
Figure 5.
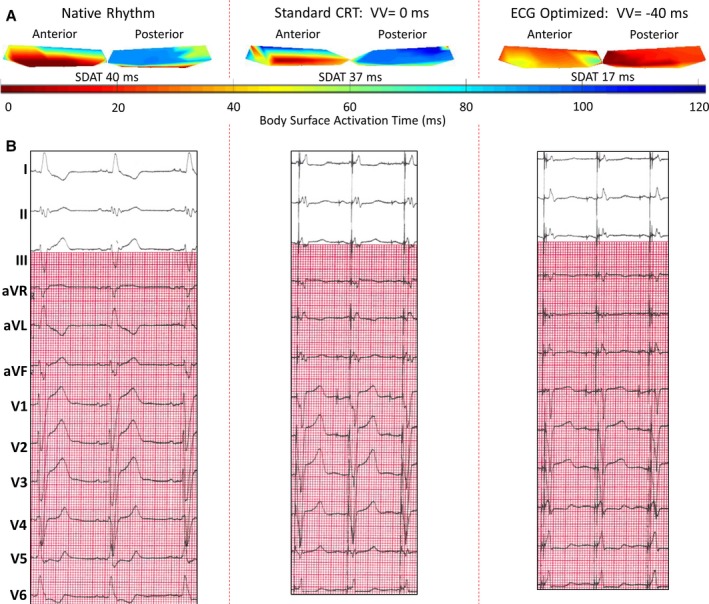
Case example: patient with inferolateral scar and optimized cardiac resynchronization therapy (CRT). Patient with previous myocardial infarction resulting in subendocardial delayed enhancement (DE) ˃75% of the basal and midinferior and inferolateral walls. The patient had an underlying left bundle branch block (LBBB) and was optimized with 12‐lead ECG to have the left ventricular (LV) lead pace 40 ms preceding the right ventricular (RV) lead. A, Body‐surface activation maps during native rhythm, at standard cardiac resynchronization therapy (CRT) programming with LV and RV leads pacing simultaneously, and at the 12‐lead ECG optimized setting. Native map shows delayed posterior electrode activation as compared with anterior electrode activation, corresponding to a dyssynchronous LBBB with a high standard deviation of activation times (SDAT) of 40 ms. Standard CRT programming resulted in only a mild benefit, with nearly similar on pattern and SDAT of 37 ms. Twelve‐lead optimization resulted in near synchronous activation and SDAT of only 17 ms. B, Changes in QRS width and morphology associated with pacing. The patient's ejection fraction (EF) increased from 22% pre‐CRT to 33% after 6 months of CRT. aVF indicates augmented vector foot; aVL, augmented vector left; aVR, augmented vector right; VV, ventricular‐ventricular.