
Fig. 1.
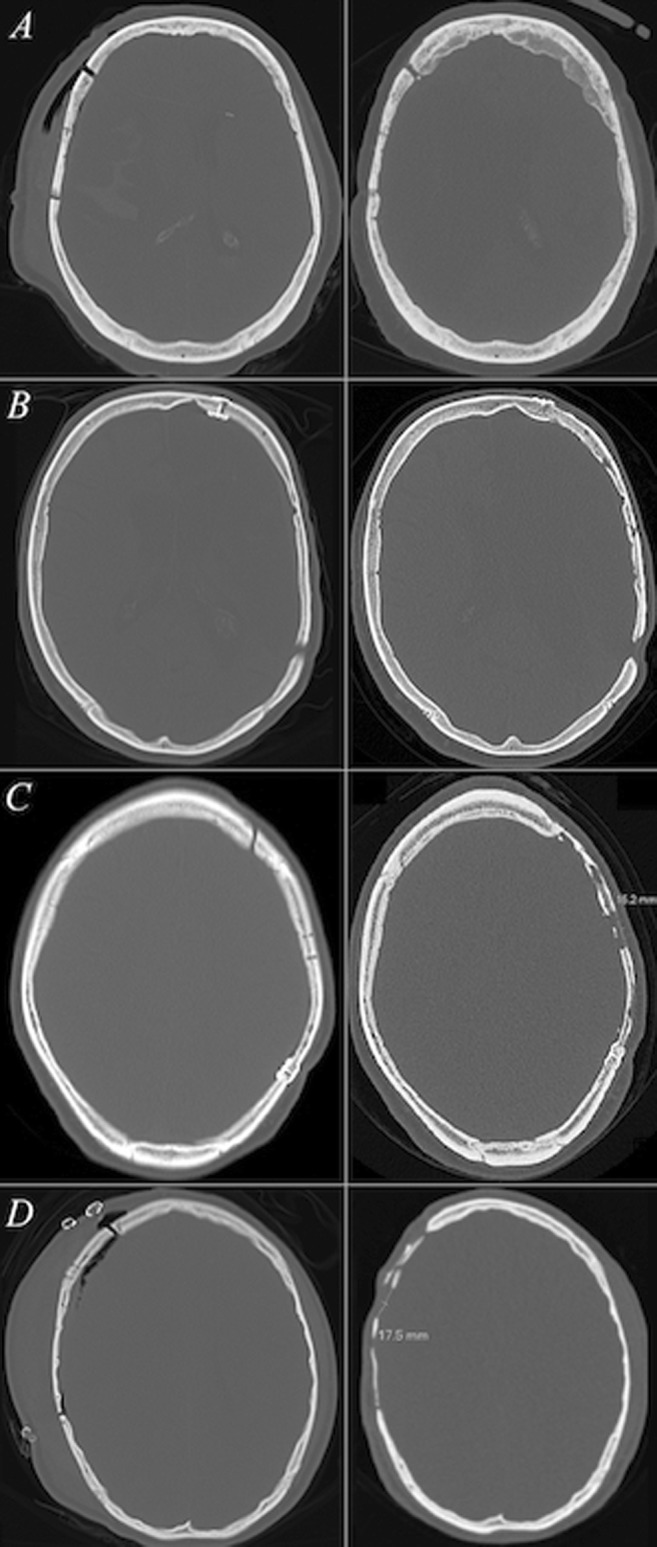
CT slices with bone window settings depict the initial postoperative and follow-up bone flap statuses (left and right columns, respectively) of four cranioplasty patients with different levels of bone flap resorption. Each row comprises one patient. In a, the follow-up bone flap status was given a mean Oulu resorption score of 0 (grade 0) as no signs of bone flap resorption were visible. The bone flap status of the patient in b was given a mean Oulu resorption score of 1.33 (grade I)—though the follow-up bone volume remained ≥ 75%, relatively mild bone flap resorption manifesting as multiple non-perforating cortical irregularities on both sides of the autograft was visible. More notable signs of bone flap resorption are depicted in c, where the follow-up status of the cranioplasty was graded a mean Oulu resorption score of 8 (grade II). The postoperative bone volume had decreased to 25–75% of the original volume along with diffuse resorptive changes on the bone flap area and a bicortical perforation exceeding 1 cm in diameter. Yet, the autograft had remained somewhat fixed to the cranium. In d, the cranioplasty had failed and the mean Oulu resorption score was 9 (grade III). The follow-up bone flap volume was < 25% of the original, bicortical perforations larger than 1.0 cm were noted and the resorptive changes within the bone flap were diffuse. Neither of the surgeons recommended further interventions for patients a or b. For the patient c, one surgeon recommended a neurosurgical consultation and for the patient d, both surgeons recommended consultation of a neurosurgeon and additionally a re-cranioplasty evaluation due to bone flap failure