
Figure 1.
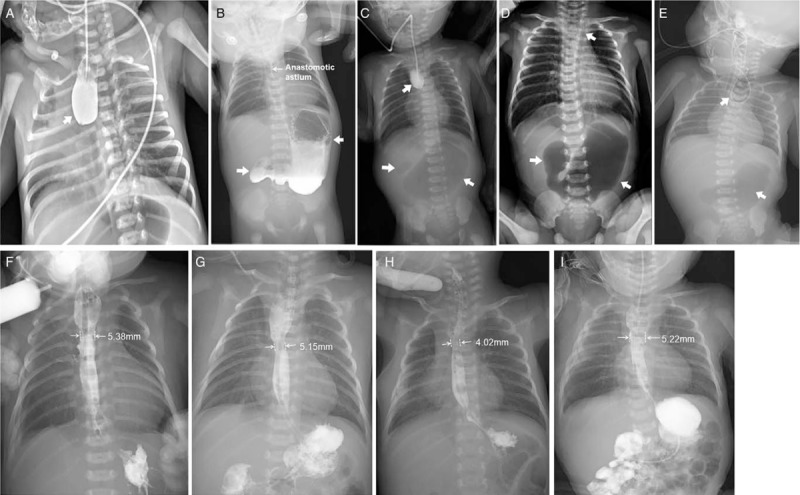
The X-ray series films of the 4 patients with esophageal and duoenal anomalies. Patient 1: esophageal radiography confirmed esophageal atresia (arrow; A); upper gastrography confirmed the presence of esophageal anastomosis patency on the ninth day after the first stage operation and demonstrated a large dilated stomach and the absence of distal bowel gas (arrows; B); and a repeat upper gastrointestinal imaging confirmed esophageal stoma after “diamond-shape” anastomosis during follow-up (F). Patient 2: esophageal radiography revealed esophageal atresia and a distended stomach with no distal bowel gas (arrows; C), suggesting duodenal obstruction and no vertebral anomalies; and a repeat upper gastrointestinal imaging confirmed esophageal stoma after “diamond-shape” anastomosis during follow-up (G). Patient 3: A preoperative X-ray film demonstrating showing combined coiled-up of NGT in the upper esophageal pouch and large gastric bubble with no distal bowel gas (arrows; D); and a repeat upper gastrointestinal imaging confirmed esophageal stoma after “diamond-shape” anastomosis during follow-up (H). Patient 4: a combined chest and abdominal X-ray demonstrated that the nasogastric tube was in the upper esophageal pouch. Vertebral anomalies and a large gastric bubble with no distal bowel gas were observed, suggesting tracheoesophageal fistula/esophageal atresia complicated with duodenal obstruction (E); and a repeat upper gastrointestinal imaging confirmed the presence of esophageal and duodenal anastomosis patency well during follow-up (I).