

Abstract
Shockwave therapy is based on generating a very intense energy in a very short period of time. It creates a mechanical pressure over the affected tissues that leads to an increased cellular permeability, thus increasing the microcirculation and the cellular metabolism. Therefore, the healing process is accelerated. Lateral epicondylitis represents a common arm injure, which usually affects early to late middle-aged patients, more common and with a longer evolution period in women, characterized by inflammation of the arm muscles’ tendon insertion and manifests with pain on elbow extension and forearm rotation. Our study aims to investigate the efficacity of the shockwave therapy in comparison with a classical treatment of local and systemic drugs. The 50 patients were evenly split into two groups. The diagnosis of lateral epicondylitis was based on exhaustive physical examination. Enthesis evaluation was performed through power Doppler ultrasound. The pain was quantified using the visual analogue scale for pain intensity. All parameters were evaluated at diagnosis and after 30 days, following treatment. One group received shockwave therapy, while the other group received nonsteroidal anti-inflammatory drugs and local topics associated with laser and ultrasound application. The results of our study report that both groups experienced significant improvement after treatment. The shockwave therapy recorded a higher improvement rate in all the parameters. Consequently, this new non-invasive, effective and safe technique can be successfully used in the treatment of abarticular pathology of the elbow.
Keywords: lateral epicondylitis, shockwave therapy, musculoskeletal ultrasound, visual analogue scale
Introduction
Lateral epicondylitis (LE) or “tennis elbow” is one of the most common arm injuries, which usually affects patients aged between 30 and 60 years, being more common and having a longer evolution period in women [1,2,3].
Although its etiology is partly elucidated, hereditary, chemical, vascular and hormonal factors are incriminated, as well as the aging process [4].
This condition is generally self-limited, but some patients may experience persistent symptoms that can be refractory to treatment.
It represents a major challenge due to its difficult treatment and susceptibility to recurrence, with an average duration of the typical episode being reported between six months and two years.
It usually appears by overusing the common finger tendon at its insertion in the arm, induced by repetitive, monotonous, rapid and excessive movements of the dominant hand [5,6,7].
Diagnosis is simple and can be confirmed by tests used in current practice, such as Tomsen test, handgrip dynamometer testing, Mill's test, the chair test, and the coffee cup test [8,9].
We can also use imaging means to identify LE, for instance musculoskeletal ultrasound, a non-invasive complex, accurate diagnostic method for the study of musculoskeletal movements during flexion-extension maneuvers or muscle contraction-relaxation and power Doppler exploration for the evaluation of inflammatory or tumor lesions [10,11].
Although the diagnosis of this condition is relatively simple, its management involves a plethora of medical and physiotherapeutic interventions based on different theoretical mechanisms of action.
The basic principles of treatment include pain reduction, accelerating the healing process, avoiding arm overload and returning the patient to the daily life activities.
Conservative treatment through rest, aggravating activities avoidance and behavioral change, usually leads to the remission of symptoms [12,13].
Nonsteroidal anti-inflammatory drugs (NSAIDs) can be used to control pain and improve short-term functionality.
Topical nitrates are also effective in reducing pain in LE and can also, stimulate collagen production by increasing local blood flow leading to the healing of tendon lesions.
Ultrasound and laser therapy are safe therapeutic alternatives that have an analgesic effect and improve the performance of daily activities, leading to a higher patient satisfaction [14].
Extracorporeal shockwave therapy (SWT) is a newly introduced method for tennis elbow management, its non-invasive nature and low rate of complications have increased the frequency of its use [15].
Its effectiveness has been demonstrated in LE refractory to other non-surgical therapeutic procedures [16].
Matherial and Method
Our study was performed as a multi-centered prospective investigation aiming at the efficiency determination of SWT in the treatment of patients diagnosed with LE.
After we obtained the approval of the local ethics committee, a total of 50 patients aged between 35-80 years who had previously never received SWT were included in the study.
The exclusion criteria for our study were the following: the existence of another different elbow disorder, cervical or upper extremity pathology, history of elbow joint surgery, rupture of the elbow tendon, neurological disease, limited range of motion of the joint due to known upper limb fracture, hemostatic disorder, malignancy, local or systemic infection and implanted pacemaker.
The diagnosis of LE was based on exhaustive physical examination. Enthesis evaluation through power Doppler ultrasound (PDUS) was performed by the same rheumatologist, unaware of the clinical evaluation, visual analogue scale (VAS) for the pain intensity and laboratory findings, at diagnosis and after 30 days, following treatment.
Ultrasound was executed using an Esaote MyLabSix equipment with a multifrequency linear array transducer (6-18 MHz).
The lateral aspect of the elbow was examined, patient positioned with elbows in extension, thumb up, palms of the hands together, visualizing the common extensor tendon on its long axis, using coronal planes with the cranial edge of the probe placed on the lateral epicondyle and short-axis planes over the insertion for LE.
Besides the ultrasound evaluation at diagnosis we considered measuring the maximum thickness of the common extensor tendon (CET) on the lateral epicondyle and the power Doppler (PD) signal semiquantitatively on a 0 to 3 scale, before and after treatment.
Following the clinical assessment, VAS intensity and musculoskeletal ultrasound, we split the patients in two homogenous study groups (25 members each) taking into account the severity of the disorder.
Before initiating the treatment, all the patients agreed and signed the informed consent forms.
For the first group we used SWT applied with a BTL-5000SWT equipment using the W-0108 program for LE.
The settings used were continuous shocks with 2 bar pressure and a frequency of 10Hz (2000 shocks).
The treatment was performed in five sessions with a five day break in-between.
After identifying the painful sites, SWT was started with 400 shocks at 2 bars with a frequency of 5Hz around the most painful area.
Subsequently, the painful spot was treated with 1000 shocks and another 400 shocks were successively applied to the forearm muscles.
The treatment received by the second group consisted in the administration of NSAIDs and local topics associated with laser and ultrasound applications.
Results
Mean values for all parameters are included in Table 1.
Table 1.
Mean values for the evaluated parameters
| Shockwave Therapy (n=25) | NSAIDs + Local Topics + Laser + Ultrasound (n=25) | Comparison between the two methods [%] | |
| VAS Mean (0 days) [mm] | 70.80 | 61.60 | 38.20 |
| VAS Mean (30 days) [mm] | 28.40 | 38.80 | |
| Improvment [%] | 59.89 | 37.01 | |
| CET Mean Thickness (0 days) [mm] | 6.1 | 6.2 | 44.66 |
| CET Mean Thickness (30 days) [mm] | 4.5 | 5.3 | |
| Improvment [%] | 26.23 | 14.52 | |
| PD Mean Scale (0 days) | 2.5 | 2.2 | 40.78 |
| PD Mean Scale (30 days) | 0.8 | 1.3 | |
| Improvment [%] | 69.35 | 41.07 |
Our results (Fig. 1) show great improvement on both therapies with a higher effectiveness in favor of the shockwave treatment (26.23% improvement in CET thickness for the SWT in comparison with 14.52% for the alternative one).
Figure 1.
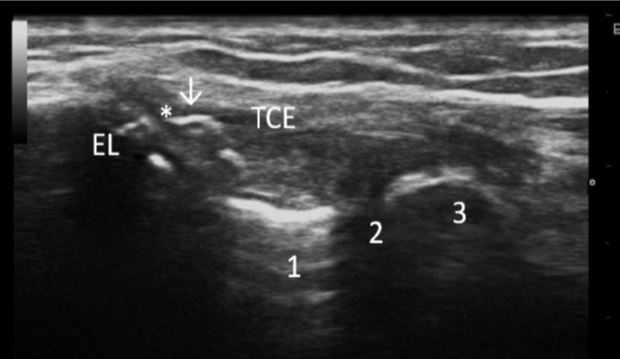
Common extensor tendon, long axis scan. Structures: 1-humeral capitellum; 2-radio-capitellar joint; 3-radial head; TCE-common extensor tendon; EL- lateral epicondyle; *-hypoechoic area; ↓-entesophytes and calcifications; the aspect pleads for calcific enthesopathy in a patient with lateral epicondylitis
The patients in the first group reported a decrease of mean VAS from 70.8mm to 28.4mm (59.89% decrease), while the patients in the second group reported only a reduction in mean from 61.6mm to 38.8mm (37.01% reduction).
The results regarding the PD scale (Fig. 2) also show a great decline for the SWT with a decrease from a mean of 2.5 to 0.8 (69.35%).
Figure 2.
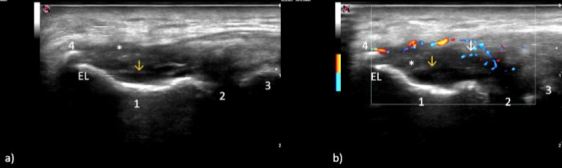
Common extensor tendon, longitudinal scan. Structures: a) Gray scale; b) power Doppler imaging; 1-humeral capitellum; 2-radio-capitellar joint; 3-radial head; 4-entesophyte; *-common extensor tendon; LE-lateral epicondyle; ↓ power Doppler signal; ↓-radial collateral ligament; enlarged insertion on the lateral epicondyle of the common extensor tendon, hypoechoic areas with loss of fibrillar pattern, anechoic areas representative for fibrillar ruptures, marked entheseal and tendinous inhomogeneity with hypervascularity-grade 2 power Doppler signal, a common ultrasound aspect found in lateral epicondylitis
The PD scale for the second group has diminished as well, from 2.2 to 1.3 (41.07% decrease).
The results are graphically represented bellow (Fig. 3, 4, 5).
Figure 3.
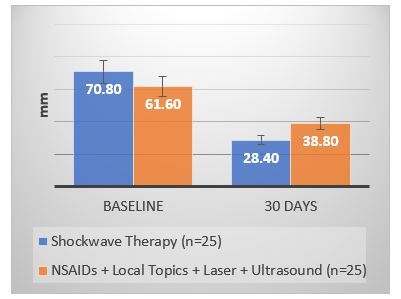
VAS decrease after 30 days treatment in both groups
Figure 4.
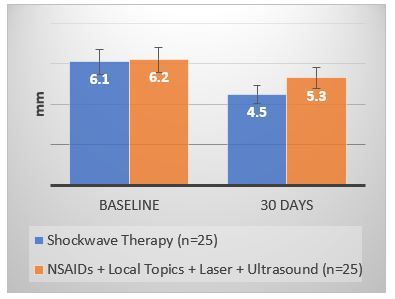
CET thickness decrease after 30 days treatment in both groups
Figure 5.
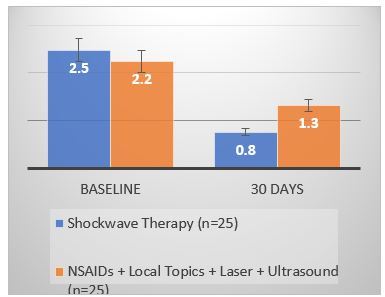
PD scale reduction after 30 days treatment in both groups
All parameters decreased significantly in comparison with pretreatment values (P<0.05).
Discussion
In this study, we investigated the ultrasound appearance and VAS in patients diagnosed with LE following two different therapeutic paths.
The pathology, also known as “tennis elbow” is caused by chronic microtrauma secondary to repetitive overuse that determines progressive degeneration and/or partial tears of the common extensor tendon (tendinopathy) [17] or to damage to the bone insertion (enthesopathy) [18,19,20].
The extensor carpi radialis brevis is the more commonly affected. According to Outcome Measures in Rheumatology (OMERACT) ultrasound group enthesopathy is defined as “abnormal hypoechoic (loss of normal fibrillar architecture) and/or thickened tendon or ligament at its bony attachment (may occasionally contain hyperechoic foci consistent with calcification), seen in two perpendicular planes that may exhibit Doppler signal [21,22] and/or bony changes, including enthesophytes, erosions, or irregularity” [23-26].
We have found several studies which report the favorable effect of SWT in patients with LE and the success rate ranged from 68% to 91% [27-30].
Shockwaves are acoustic waves that carry an increased level of energy to the painful areas of the musculoskeletal tissues in patients with subacute and chronic conditions. The kinetic energy of the projectile is determined by the compressed air and is taken over by the transmitter and subsequently by the tissues of the affected area. The energy transmitted to the affected tissues stimulates the processes of bone, tendons and soft tissues regeneration [31,32].
One of SWT beneficial effects is the formation of new blood vessels. Blood nutrient intake is necessary to start and maintain rejuvenation processes of affected tissue.
By applying SWT, partial ruptures of capillary vessels from the tendons and bones will increase, which will consequently stimulate the expression of growth factors such as endothelial nitric oxide synthase, endothelial vascular growth factor and morphogenetic bone protein.
As a result of these mechanisms, the development, growth and remodeling of arterioles is stimulated, with direct involvement in enhancing the blood supply of nutrients and oxygen to the affected tissues leading to a faster healing of localized lesions in the bones and tendons [33].
Chronic inflammation occurs when the inflammatory response is not completely stopped and may cause chronic pain by affecting the healthy tissue.
Through SWT, the activity of mast cells is increased.
The activation of these cells will result in the production of proinflammatory compounds (chemokines, cytokines) that initially accentuate the inflammatory process and then stimulate the healing and regeneration processes of the affected tissue [34,35].
The production of a sufficient amount of collagen is necessary for the reconstruction of the affected musculoskeletal and ligamentous structures.
Applying SWT accelerates collagen synthesis and causes the new collagen fibers to have a longitudinal distribution in order to increase tendon density and strength [36].
P substance is an important neurotransmitter that mediates pain and is generally associated with chronic and persistent chronic pain.
Applying SWT leads to a decrease in the P substance concentration, with direct involvement in pain reduction and stimulation of nociceptive fibers [37].
In our study, in the treatment of LE, we observed short-term effectiveness of SWT on both subjective clinical parameters as VAS, and imaging parameters as ultrasound evaluation (CET thickness, power Doppler scale).
A significant pain reduction (P<0.05) was recorded in all the patients who benefited from this therapy.
Furthermore, SWT also increased the quality of life in these patients.
Pain relief on the VAS scale was found to be greater with a mean of 59.89% in all patients who received SWT compared to an average decrease of 37.01% encountered in patients treated with drugs and standard physiotherapy procedures.
The ultrasound imaging parameters also reported a significant improvement of the inflammatory process quantified by means of CET thickness and PD scale (P<0.05).
The CET thickness improvement found in the first group was an average of 26.23%, compared to the improvement in the second group of 14.52%.
The PD scale has recorded an average improvement of 69.35% in the shockwave treatment group, while the group that received drugs and traditional procedures has recorded an improvement of only 41.07%.
Conclusions
In conclusion, SWT is a relatively new and non-invasive, effective, convenient and safe therapeutic procedure.
The rate of complications is low and negligible.
The therapeutic effect is cumulative and requires, in most cases, three to five sessions.
Frequently, patients experience pain relief after the first treatment session.
The use of SWT in lateral epicondylitis provided superior results compared to the classical physical therapies and allows for the reduction of pain and temporary inability to work in these patients.
References
- 1.Vicenzino B, Wright A. Lateral epicondylalgia I: Epidemiology, pathophysiology, aetiology and natural history. Phys Ther Rev. 1996;1(1):23–34. [Google Scholar]
- 2.Allander E. Prevalence, incidence and remission rates of some common rheumatic diseases and syndromes. Scand J Rheumatol. 1974;3(3):145–153. doi: 10.3109/03009747409097141. [DOI] [PubMed] [Google Scholar]
- 3.Kivi P. The etiology and conservative treatment of humeral epicondylitis. Scand J Rehabil Med. 1982;15(1):37–41. [PubMed] [Google Scholar]
- 4.Nirschl RP, Pettrone FA. Tennis elbow. The surgical treatment of lateral epicondylitis. J Bone Joint Surg Am. 1979;61(6A):832–839. [PubMed] [Google Scholar]
- 5.Kamien M. A rational management of tennis elbow. Sports Med. 1990;9(3):173–191. doi: 10.2165/00007256-199009030-00005. [DOI] [PubMed] [Google Scholar]
- 6.Nirschl RP. The etiology and treatment of tennis elbow. J Sports Med. 1974;2(6):308–323. doi: 10.1177/036354657400200602. [DOI] [PubMed] [Google Scholar]
- 7.Meyer NJ, Walter F, Haines B, Orton D, Daley RA. Modeled evidence of force reduction at the extensor carpi radialis brevis origin with the forearm support band. J Hand Surg Am. 2003;28(2):279–287. doi: 10.1053/jhsu.2003.50045. [DOI] [PubMed] [Google Scholar]
- 8.Pienimäki T, Tarvainen T, Siira P, Malmivaara A, Vanharanta H. Associations between pain, grip strength, and manual tests in the treatment evaluation of chronic tennis elbow. Clin J Pain. 2002;18(3):164–170. doi: 10.1097/00002508-200205000-00005. [DOI] [PubMed] [Google Scholar]
- 9.Haker E. Lateral epicondylalgia: diagnosis, treatment and evaluation. Crit Rev Phys Rehabil Med. 1993;5:129–154. [Google Scholar]
- 10.Krogh TP, Fredberg U, Ammitzbøl C, Ellingsen T. Ultrasonographic characteristics of the common extensor tendon of the elbow in asymptomatic individuals: Thickness, color Doppler activity, and bony spurs. Orthop J Sports Med. 2017;5(5):2325967117704186–2325967117704186. doi: 10.1177/2325967117704186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Toprak U, Baskan B, Ustuner E, Oten E, Altin L, Karademir MA, Bodur H. Common extensor tendon thickness measurements at the radiocapitellar region in diagnosis of lateral elbow tendinopathy. Diagn Interv Radiol. 2012;18:566–570. doi: 10.4261/1305-3825.DIR.5575-12.2. [DOI] [PubMed] [Google Scholar]
- 12.Trudel D, Duley J, Zastrow I, Kerr EW, Davidson R, MacDermid JC. Rehabilitations for patients with lateral epicondylitis: A systematic review. J Hand Ther. 2004;17(2):243–266. doi: 10.1197/j.jht.2004.02.011. [DOI] [PubMed] [Google Scholar]
- 13.Traistaru R, Alexandru DO, Kamal D, Kamal KC, Rogoveanu OC, Postolache P. Boswellia derivates and rehabilitation program in knee osteoarthritis patients. Rev Chim. 2018;69(11):4105–4108. [Google Scholar]
- 14.Smidt N, Assendelft W, Arola H, Malmivaara A, Green S, Buchbinder R, van der, Bouter L. Effectiveness of physiotherapy for lateral epicondylitis: A systematic review. Ann Med. 2003;35(1):51–62. doi: 10.1080/07853890310004138. [DOI] [PubMed] [Google Scholar]
- 15.Furia JP. Safety and efficacy of extracorporeal shock wave therapy for chronic lateral epicondylitis. Am J Orthop. 2005;34(1):13–19. [PubMed] [Google Scholar]
- 16.Stasinopoulos D, Johnson MI. Effectiveness of extracorporeal shock wave therapy for tennis elbow (lateral epicondylitis) Br J Sports Med. 2005;39(3):132–136. doi: 10.1136/bjsm.2004.015545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Clarke AW, Ahmad M, Curtis M, Connell DA. Lateral elbow tendinopathy: Correlation of ultrasound findings with pain and functional disability. Am J Sports Med. 2010;38(6):1209–1214. doi: 10.1177/0363546509359066. [DOI] [PubMed] [Google Scholar]
- 18.Resnick D, Niwayama G. Entheses and enthesopathy. Anatomical, pathological, and radiological correlation. Radiology. 1983;146(1):1–9. doi: 10.1148/radiology.146.1.6849029. [DOI] [PubMed] [Google Scholar]
- 19.Shaibani A, Workman R, Rothschild BM. The significance of enthesopathy as a skeletal phenomenon. Clin Exp Rheumatol. 1993;11(4):399–403. [PubMed] [Google Scholar]
- 20.Benjamin M, Rufai A, Ralphs JR. The mechanism of formation of bony spurs (enthesophytes) in the achilles tendon. Arthritis Rheum. 2000;43(3):576–583. doi: 10.1002/1529-0131(200003)43:3<576::AID-ANR14>3.0.CO;2-A. [DOI] [PubMed] [Google Scholar]
- 21.duToit C, Stieler M, Saunders R, Bisset L, Vicenzino B. Diagnostic accuracy of power Doppler ultrasound in patients with chronic tennis elbow. Br J Sports Med. 2008;42(11):872–876. doi: 10.1136/bjsm.2007.043901. [DOI] [PubMed] [Google Scholar]
- 22.Krogh TP, Fredberg U, Christensen R, Stengaard-Pedersen K, Ellingsen T. Ultrasonographic assessment of tendon thickness, doppler activity and bony spurs of the elbow in patients with lateral epicondylitis and healthy subjects: a reliability and agreement study. Ultraschall Med. 2013;34(05):468–474. doi: 10.1055/s-0033-1335951. [DOI] [PubMed] [Google Scholar]
- 23.Walz DM, Newman JS, Konin GP, Ross G. Epicondylitis: Pathogenesis, imaging, and treatment. Radiographics. 2010;30(1):167–184. doi: 10.1148/rg.301095078. [DOI] [PubMed] [Google Scholar]
- 24.De Maeseneer, Brigido MK, Antic M, et al. Ultrasound of the elbow with emphasis on detailed assessment of ligaments, tendons, and nerves. Eur J Radiol. 2015;84(4):671–681. doi: 10.1016/j.ejrad.2014.12.007. [DOI] [PubMed] [Google Scholar]
- 25.Jaén-Díaz JI, Cerezo-López E, López-de Castro, Mata-Castrillo M, Barceló-Galíndez JP, De la, Balius-Mata R. Sonographic findings for the common extensor tendon of the elbow in the general population. J Ultrasound Med. 2010;29(12):1717–1724. doi: 10.7863/jum.2010.29.12.1717. [DOI] [PubMed] [Google Scholar]
- 26.Radunovic G, Vlad V, Micu MC, Nestorova R, Petranova T, Porta F, Annamaria I. Ultrasound assessment of the elbow. Med Ultrason. 2012;14(2):141–146. [PubMed] [Google Scholar]
- 27.Melegati G, Tornese D, Bandi M, Rubini M. Comparison of two ultrasonographic localization techniques for the treatment of lateral epicondylitis with extracorporeal shock wave therapy: A randomized study. Clin Rehabil. 2004;18(4):366–370. doi: 10.1191/0269215504cr762oa. [DOI] [PubMed] [Google Scholar]
- 28.Ko JY, Chen HS, Chen LM. Treatment of lateral epicondylitis of the elbow with shock waves. Clin Orthop. 2001;387:60–67. doi: 10.1097/00003086-200106000-00008. [DOI] [PubMed] [Google Scholar]
- 29.Rompe JD, Decking J, Schoellner C, Theis C. Repetitive low-energy shock wave treatment for chronic lateral epicondylitis in tennis players. Am J Sports Med. 2004;32(3):734–743. doi: 10.1177/0363546503261697. [DOI] [PubMed] [Google Scholar]
- 30.Spacca G, Necozione S, Cacchio A. Radial shock wave therapy for lateral epicondylitis: A prospective randomised controlled single-blind study. Europa Medicophysica. 2005;41(1):17–25. [PubMed] [Google Scholar]
- 31.Ogden JA, Tóth-Kischkat A, Schultheiss R. Principles of shock wave therapy. Clin Orthop. 2001;387:8–17. doi: 10.1097/00003086-200106000-00003. [DOI] [PubMed] [Google Scholar]
- 32. Siebert W , Buch M, editors. Extracorporeal shock waves in orthopaedics . Berlin : Springer Verlag ; 1997 . pp. 1– 248. [Google Scholar]
- 33.Kuo YR, Wang CT, Wang FS, Chiang YC, Wang CJ. Extracorporeal shock-wave therapy enhanced wound healing via increasing topical blood perfusion and tissue regeneration in a rat model of STZ-induced diabetes. Wound Repair Reg. 2009;17(4):522–530. doi: 10.1111/j.1524-475X.2009.00504.x. [DOI] [PubMed] [Google Scholar]
- 34.Wang CJ, Ko JY, Chan YS, Weng LH, Hsu SL. Extracorporeal shockwave for chronic patellar tendinopathy. Am J Sports Med. 2007;35(6):972–978. doi: 10.1177/0363546506298109. [DOI] [PubMed] [Google Scholar]
- 35.Rogoveanu OC, Calina D, Cucu MG, Burada F, Docea AO, Sosoi S, Stefan E, Ioana M, Burada E. Association of cytokine gene polymorphisms with osteoarthritis susceptibility. Exp Ther Med. 2018;16(3):2659–2664. doi: 10.3892/etm.2018.6477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Haupt G, Haupt A, Ekkernkamp A, Gerety B, Chvapil M. Influence of shockwave on fracture healing. J Urol. 1992;39(6):529–532. doi: 10.1016/0090-4295(92)90009-l. [DOI] [PubMed] [Google Scholar]
- 37.Lian O, Dahl J, Ackermann PW, Frihagen F, Engebretsen L, Bahr R. Pronociceptive and antinociceptive neuromediators in patellar tendinopathy. Am J Sports Med. 2006;34(11):1801–1808. doi: 10.1177/0363546506289169. [DOI] [PubMed] [Google Scholar]