

Abstract
Background
Seasonal affective disorder (SAD) is a seasonal pattern of recurrent major depressive episodes that most commonly occurs during autumn or winter and remits in spring. The prevalence of SAD ranges from 1.5% to 9%, depending on latitude. The predictable seasonal aspect of SAD provides a promising opportunity for prevention. This review ‐ one of four reviews on efficacy and safety of interventions to prevent SAD ‐ focuses on second‐generation antidepressants (SGAs).
Objectives
To assess the efficacy and safety of SGAs (in comparison with other SGAs, placebo, light therapy, melatonin or agomelatine, psychological therapies or lifestyle interventions) in preventing SAD and improving patient‐centred outcomes among adults with a history of SAD.
Search methods
We searched Ovid MEDLINE (1950‐ ), Embase (1974‐ ), PsycINFO (1967‐ ) and the Cochrane Central Register of Controlled Trials (CENTRAL) to 19 June 2018. An earlier search of these databases was conducted via the Cochrane Common Mental Disorders Controlled Trial Register (CCMD‐CTR) (all years to 11 August 2015). Furthermore, we searched the Cumulative Index to Nursing and Allied Health Literature, Web of Science, the Cochrane Library, the Allied and Complementary Medicine Database and international trial registers (to 19 June 2018). We also conducted a grey literature search and handsearched the reference lists of included studies and pertinent review articles.
Selection criteria
For efficacy, we included randomised controlled trials (RCTs) on adults with a history of winter‐type SAD who were free of symptoms at the beginning of the study. For adverse events, we planned to include non‐randomised studies. Eligible studies compared a SGA versus another SGA, placebo, light therapy, psychological therapy, melatonin, agomelatine or lifestyle changes. We also intended to compare SGAs in combination with any of the comparator interventions versus placebo or the same comparator intervention as monotherapy.
Data collection and analysis
Two review authors independently screened abstracts and full‐text publications, extracted data and assessed risk of bias of included studies. When data were sufficient, we conducted random‐effects (Mantel‐Haenszel) meta‐analyses. We assessed statistical heterogeneity by calculating the Chi2 statistic and the Cochran Q. We used the I2 statistic to estimate the magnitude of heterogeneity. We assessed publication bias by using funnel plots.We rated the strength of the evidence using the system developed by the GRADE Working Group.
Main results
We identified 3745 citations after de‐duplication of search results and excluded 3619 records during title and abstract reviews. We assessed 126 full‐text papers for inclusion in the review, of which four publications (on three RCTs) providing data from 1100 people met eligibility criteria for this review. All three RCTs had methodological limitations due to high attrition rates.
Overall, moderate‐quality evidence indicates that bupropion XL is an efficacious intervention for prevention of recurrence of depressive episodes in people with a history of SAD (risk ratio (RR) 0.56, 95% confidence interval (CI) 0.44 to 0.72; 3 RCTs, 1100 participants). However, bupropion XL leads to greater risk of headaches (moderate‐quality evidence), insomnia and nausea (both low‐quality evidence) when compared with placebo. Numbers needed to treat for additional beneficial outcomes (NNTBs) vary by baseline risks. For a population with a yearly recurrence rate of 30%, the NNTB is 8 (95% CI 6 to 12). For populations with yearly recurrence rates of 50% and 60%, NNTBs are 5 (95% CI 4 to 7) and 4 (95% CI 3 to 6), respectively.
We could find no studies on other SGAs and no studies comparing SGAs with other interventions of interest, such as light therapy, psychological therapies, melatonin or agomelatine.
Authors' conclusions
Available evidence indicates that bupropion XL is an effective intervention for prevention of recurrence of SAD. Nevertheless, even in a high‐risk population, three out of four people will not benefit from preventive treatment with bupropion XL and will be at risk for harm. Clinicians need to discuss with patients advantages and disadvantages of preventive SGA treatment, and might want to consider offering other potentially efficacious interventions, which might confer a lower risk of adverse events. Given the lack of comparative evidence, the decision for or against initiating preventive treatment of SAD and the treatment selected should be strongly based on patient preferences.
Future researchers need to assess the effectiveness and risk of harms of SGAs other than bupropion for prevention of SAD. Investigators also need to compare benefits and harms of pharmacological and non‐pharmacological interventions.
Plain language summary
Antidepressants for prevention of winter depression
Why is this review important?
Many people in northern latitudes suffer from winter blues, which occurs as a reaction to reduced sunlight. Three‐quarters of those affected are women. Lethargy, overeating, craving for carbohydrates and depressed mood are common symptoms. In some people, winter blues becomes depression, which seriously affects their daily lives. Up to two‐thirds experience depressive symptoms every winter.
Who will be interested in this review?
• Anyone who has experienced winter depression.
• Relatives and friends of people who have experienced winter depression.
• General practitioners, psychiatrists and pharmacists.
• Professionals working in adult mental health services.
What questions does this review aim to answer?
In light of the seasonal pattern and the high rate of recurrence, beginning antidepressant therapy in early autumn (fall) when people are still free of depressive symptoms can prevent the onset of depressed mood. The goal of this review is to examine whether benefits outweigh harms of antidepressants when they are used in healthy people with a history of winter depression to prevent onset of depression the next winter. To date, this question has not been examined in a systematic way.
Which studies were included in the review?
We searched databases up to June 2018 for studies on antidepressants given to prevent winter depression. Of 3745 records, we found three randomised controlled studies including 1100 people who received bupropion extended‐release (only one of many available antidepressants, but the only one licensed for prevention of winter depression) or placebo. We found no studies on other antidepressants.
What does evidence from the review reveal?
In populations with a high risk of developing a new depressive episode in the next winter, results show that antidepressants can prevent winter depression in about one in four people. In populations with a lower risk of recurrence, antidepressants can prevent a new depressive episode in one of eight people. The other seven people suffer from winter depression despite treatment or would not have suffered from winter depression anyway. People using antidepressants are at slightly higher risk of experiencing headaches, nausea or insomnia when compared with people not taking antidepressants.
Doctors need to discuss with patients the advantages and disadvantages of antidepressants and other potentially preventive treatments for winter depression, such as light treatment, psychological therapies or lifestyle interventions. As no available studies have compared these treatments, the decision for or against preventive treatment of SAD and the treatment selected should be strongly based on patient preferences.
What should happen next?
Review authors recommend that future studies should directly compare antidepressants against other treatments, such as light therapy, psychological therapies or other drugs to determine the best treatment for preventing winter depression.
Summary of findings
Summary of findings for the main comparison. Bupropion XL versus placebo for prevention of SAD.
| Bupropion XL versus placebo for prevention of SAD | ||||||
| Patient or population: adults with a history of SAD who do not fulfil criteria for major depressive disorder Settings: any setting Intervention: bupropion XL Comparison: placebo | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Placebo | Bupropion XL | |||||
| Incidence of SAD (SIGH‐SAD score ≥ 20) Follow‐up: 4 to 6 months |
Low | RR 0.56 (0.44 to 0.72) | 1100 (3 RCTs) | ⊕⊕⊕⊝ Moderatea | All 3 studies were funded by GlaxoSmithKline, the producer of bupropion XL | |
| 300 per 1000 | 165 per 1000 (129 to 213) | |||||
| Moderate | ||||||
| 500 per 1000 | 275 per 1000 (215 to 355) | |||||
| High | ||||||
| 600 per 1000 | 330 per 1000 (258 to 426) | |||||
| Overall rate of adverse events Follow‐up: 4 to 6 months |
Study population | RR 1.02 (0.97 to 1.08) |
1048 (3 RCTs) | ⊕⊕⊕⊝ Moderateb | ||
| 834 per 1000 | 858 per 1000 | |||||
| Headache Follow‐up: 4 to 6 months |
Study population | RR 1.26 (1.02 to 1.56) | 1048 (3 RCTs) | ⊕⊕⊕⊝ Moderateb | ||
| 270 per 1000 | 340 per 1000 (275 to 421) | |||||
| Insomnia Follow‐up: 4 to 6 months |
Study population | RR 1.46 (1.10 to 1.93) | 1048 (3 RCTs) | ⊕⊕⊝⊝ Lowb,c | ||
| 133 per 1000 | 194 per 1000 (146 to 257) | |||||
| Nausea Follow‐up: 4 to 6 months |
Study population | RR 1.63 (1.12 to 2.38) | 1048 (3 RCTs) | ⊕⊕⊝⊝ Lowb,c | ||
| 76 per 1000 | 124 per 1000 (85 to 180) | |||||
| Diarrhoea Follow‐up: 4 to 6 months |
Study population | RR 1.04 (0.66 to 1.64) | 1048 (3 RCTs) | ⊕⊕⊝⊝ Lowb,c | ||
| 67 per 1000 | 69 per 1000 (44 to 109) | |||||
| Discontinuation due to adverse events Follow‐up: 4 to 6 months |
Study population | RR 1.68 (0.74 to 3.79) | 1048 (3 RCTs) | ⊕⊕⊝⊝ Lowb,c | ||
| 47 per 1000 | 79 per 1000 (35 to 178) | |||||
| *The basis for the assumed risk (e.g. median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; HAM‐D: Hamilton Rating Scale for Depression; RCT: randomised controlled trial; SAD: seasonal affective disorder; SIGH‐SAD: Structured Interview Guide for the Hamilton Depression Rating Scale, Seasonal Affective Disorders | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate Very low quality: we are very uncertain about the estimate | ||||||
aDowngraded by one level for risk of bias because of high attrition rates in all 3 studies. bDowngraded by one level for risk of bias because assessment of adverse events was limited to spontaneously reported adverse events. cDowngraded by one level because the number of events did not reach optimal information size.
Background
Description of the condition
Seasonal affective disorder (SAD) is a seasonal pattern of recurrent major depressive episodes that most commonly occurs during autumn or winter and remits in spring or summer (Rosenthal 1984). In addition to the predictable seasonal pattern of depression, persons suffering from SAD commonly experience atypical symptoms including hypersomnia, carbohydrate craving with increased appetite and weight gain and extreme fatigue (Sohn 2005). Prevalence of SAD is estimated at around 10% in northern latitudes (Byrne 2008). In the USA, it ranges from 1.5% in southern Florida to about 9% in northern regions (Rosen 1990). SAD is a multifactorial condition. Chronobiological mechanisms related to circadian rhythms, melatonin, serotonin turnover and photoperiodism (length of dark hours relative to light hours in a 24‐hour period) are thought to play a role in SAD (Ciarleglio 2011; Levitan 2007). A quintessential and especially impairing quality of this illness is its high risk of recurrence and persistence. Approximately two‐thirds of those diagnosed with SAD will face recurrence of these distressing symptoms the following winter (Rodin 1997). In the five to 11 years following initial diagnosis, 22% to 42% of people still suffer from SAD, and 33% to 44% develop a non‐seasonal pattern in subsequent episodes; the disorder resolves completely in only 14% to 18% of people (Magnusson 2005; Schwartz 1996). Indeed, many people who suffer from SAD experience this type of depression every year, which makes it particularly amenable to preventive treatment (Westrin 2007).
Description of the intervention
Various interventions such as second‐generation antidepressants (SGAs), light therapy (e.g. bright white light, dawn simulation), melatonin or agomelatine, psychological therapies and lifestyle interventions have been used for prevention of SAD. Of these, SGAs have become the pharmacological treatment of choice for depressive disorders. SGAs can be classified into three groups: selective serotonin reuptake inhibitors (SSRIs: citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, sertraline); serotonin and norepinephrine reuptake inhibitors (SNRIs: desvenlafaxine, duloxetine, levomilnacipran, milnacipran, venlafaxine); and others (bupropion, mirtazapine, nefazodone, reboxetine, trazodone, vilazodone, vortioxetine). Although most SGAs have been approved in most countries for treatment of major depressive disorders, only one (bupropion XL (extended‐release)) is currently licensed for use in preventing SAD (Modell 2005).
How the intervention might work
SGAs work through their effects on neurotransmitters in the central nervous system. SSRIs act by selectively inhibiting reuptake of serotonin (5‐hydroxy‐tryptamine (5‐HT)) at the presynaptic neuronal membrane. SNRIs are potent inhibitors of serotonin and norepinephrine reuptake. Other SGAs include mirtazapine, which is believed to enhance central noradrenergic and serotonergic activity as an alpha‐adrenergic, 5‐HT2 and 5‐HT3 receptor antagonist, and bupropion, a relatively weak inhibitor of neuronal uptake of noradrenaline and dopamine (Foley 2006). Reboxetine is a noradrenaline reuptake inhibitor that does not act on serotonin (Kent 2000). Nefazodone is believed to inhibit neuronal uptake of serotonin and norepinephrine and to block postsynaptic 5‐HT2A‐receptors (Davis 1997). Trazodone appears to produce its primary antidepressant effects by inhibiting serotonin reuptake, but it also acts as a 5‐HT2A‐ and 5‐HT2C‐receptor blocker and inhibits α1‐adrenoreceptors and histamine‐1‐receptors (Stahl 2009).
Much research into the causes of SAD has focused on the role of circadian rhythms and melatonin (Lam 2006). Early morning bright light exposure is a common and effective short‐term treatment for SAD (Golden 2005). On the neurochemical level, changes in both serotonergic and catecholaminergic transmitter systems seem to play a key role in this disorder (Neumeister 2001). Targeting these monoaminergic systems with serotonin, noradrenaline or dopamine reuptake inhibition provides biological plausibility for the mechanism of action of SGAs.
The rationale for using SGAs for prevention of SAD is based on the efficacy of SGAs for treatment of SAD (Thaler 2010). Starting treatment with SGAs early in the season, when people are still well, might lead to reduced disturbance in serotonergic and catecholaminergic transmitter systems (Neumeister 2001).
Why it is important to do this review
The predictable seasonal aspect of SAD provides a specific and promising opportunity for prevention. However, both patients and clinicians face much uncertainty in their collaborative decisions in selecting a preventive intervention (Westrin 2007). Although a recent Cochrane Review assessed efficacy and risk of harms of SGAs for short‐term treatment of SAD (Thaler 2010), to date no review has determined the efficacy, effectiveness and risk of harms of SGAs for preventing recurrent SAD.
Our findings are intended to provide insights into (1) available evidence on benefits and harms of competing interventions for prevention of SAD, with respect to patient‐centred outcomes, and (2) gaps in the evidence base that need to inform future research needs.
This is one of four reviews of interventions used to prevent SAD. The others focus on light therapy (Nussbaumer 2015), agomelatine and/or melatonin (Kaminski‐Hartenthaler 2015), and psychological therapies (Forneris 2015), as preventive interventions.
Objectives
To assess the efficacy and safety of SGAs (in comparison with other SGAs, placebo, light therapy, melatonin or agomelatine, psychological therapies or lifestyle interventions) in preventing SAD and improving patient‐centred outcomes among adults with a history of SAD.
Methods
Criteria for considering studies for this review
Types of studies
Efficacy (beneficial effects)
We included randomised controlled trials (RCTs; including cross‐over studies and cluster‐randomised trials) of SGAs for prevention of SAD.
Adverse effects
We included the following.
RCTs (including cross‐over studies and cluster‐randomised trials) of SGAs for prevention of SAD.
Non‐randomised controlled studies such as non‐randomised trials, prospective cohort studies or case‐control studies of SGAs for prevention of SAD.
Types of participants
Participant characteristics
Male and female adults (≥ 18 years of age) of all races, ethnicities and cultural groups with a history of SAD who do not fulfil the criteria for a current major depressive episode.
Diagnosis
We defined SAD according to the Diagnostic and Statistical Manual of Mental Disorders (DSM‐5; APA 2013), as a seasonal pattern of recurrent major depressive episodes. However, we restricted our focus to winter‐type SAD (i.e. major depression in autumn/winter with full remission in spring/summer), and we did not include people with bipolar disorder with a seasonal pattern. We included studies that used definitions from prior versions of the DSM (APA 1980; APA 1987; APA 2000).
Comorbidities
We excluded studies that enrolled participants with depressive disorder due to another medical condition. We planned to include populations at risk of SAD with common comorbidities (e.g. diabetes, cardiovascular disease) that are not the cause of the depressive episode.
Setting
We included studies conducted in all settings.
Subset data
We intended to include studies that provided data on subsets of participants of interest, as long as the subsets met our eligibility criteria. We did not include studies with 'mixed' populations if investigators did not adequately stratify data with respect to our populations of interest.
Types of interventions
Experimental interventions
We included the following SGAs.
Selective serotonin reuptake inhibitors (SSRIs): citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, sertraline.
Serotonin and norepinephrine reuptake inhibitors (SNRIs): desvenlafaxine, duloxetine, levomilnacipran, milnacipran, venlafaxine.
Other: bupropion, mirtazapine, nefazodone, reboxetine, trazodone, vilazodone, vortioxetine.
We planned to include combination therapies of SGAs versus any of the comparator interventions listed below. We applied no restrictions on dosing nor on length of treatment.
Comparator interventions
We were interested in comparisons of SGAs with:
placebo;
another SGA from the list above;
light therapy;
melatonin or agomelatine;
psychological therapies; and
lifestyle interventions (e.g. exercising, making the environment sunnier (open blinds), spending regular time outside, adapting nutrition (low‐fat diet, reduced refined sugars).
We also planned to compare SGAs in combination with any of the comparator interventions listed above versus placebo, or the same comparator intervention as monotherapy (see Data extraction and management).
Types of outcome measures
We included studies that met the above inclusion criteria regardless of whether they reported on the following outcomes. In consultation with clinical experts during the protocol stage of the review, we selected the following outcomes a priori.
Primary outcomes
The primary outcome for benefit was incidence of SAD, measured as the proportion of participants with a SIGH‐SAD (Structured Interview Guide for the Hamilton Depression Rating Scale, Seasonal Affective Disorders (Williams 2002)) of 20 or higher.
The primary outcome for harms was the overall rate of adverse events related to preventive interventions.
Secondary outcomes
Severity of the SAD episode or SAD‐related symptoms, as measured by a validated tool (e.g. Hamilton Depression Rating Scale (Hamilton 1960)).
Quality of life, as measured by a validated quality of life tool (e.g. Short Form (SF)‐36 (Ware 1992)).
Quality of interpersonal and social functioning, as measured by a validated tool (e.g. the Range of Impaired Functioning Tool (LIFE–RIFT) (Leon 1999)).
Proportion of participants with serious adverse events.
Rates of discontinuation of preventive intervention due to adverse events.
Overall rate of discontinuation.
Timing of outcome assessment
Depending on available data, we planned to synthesise outcomes at different time points (e.g. short‐term, medium‐term and long‐term) throughout an entire six‐month period of risk during an autumn/winter season.
Hierarchy of outcome measures
Our main focus was patient‐centred outcomes (i.e. outcomes that patients notice and care about). If several measures assessed the same outcome, we consulted with clinical experts a priori regarding the validity and reliability of individual outcome measures and prioritised accordingly.
Search methods for identification of studies
Cochrane Common Mental Disorders Controlled Trials Register (CCMD‐CTR)
The Cochrane Common Mental Disorders (CCMD) Group maintains a specialised register of randomised controlled trials (RCTs), the CCMD‐CTR. This register contains over 40,000 reference records (reports of RCTs) for anxiety disorders, depression, bipolar disorder, eating disorders, self‐harm, and other mental disorders within the scope of this Group. The CCMD‐CTR is a partially studies‐based register with more than 50% of reference records tagged to approximately 12,500 individually PICO‐coded study records. Reports of trials for inclusion in the register are collated from (weekly) generic searches of MEDLINE (1950‐), Embase (1974‐) and PsycINFO (1967‐), quarterly searches of the Cochrane Central Register of Controlled Trials (CENTRAL), and review‐specific searches of additional databases. Reports of trials are also sourced from international trial registries, drug companies, the handsearching of key journals, conference proceedings, and other (non‐Cochrane) systematic reviews and meta‐analyses. Details of CCMD's core search strategies (used to identify RCTs) can be found on the Group's website, with an example of the core MEDLINE search displayed in Appendix 1.
The CCMD‐CTR is current to June 2016 only, with the move of the editorial base from the University of Bristol to York.
Electronic searches
The searches for this review are up‐to‐date as of 19 June 2018. Details of all searches conducted between April 2013 and June 2018 are described below.
The Information Specilaist with the Cochrane Common Mental Disorders Group (CCMD) ran an initial search of their Group's Specialised Registers (CCMD‐CTR‐Studies and CCMD‐CTR‐References) (all years to 12 April 2013) using terms for condition only. An updated search was performed onto 11 August 2015, prior to the first publication of this review.
("seasonal affective disorder*" or "seasonal depression" or "seasonal mood disorder*" or "winter depression" or SIGH‐SAD*).
In addition, we conducted our own searches of the following electronic databases (to 26 May 2014) to ensure that no studies had been missed by the CCMD‐CTR (Appendix 2).
International Pharmaceutical Abstracts.
Cumulative Index to Nursing and Allied Health Literature (CINAHL).
Web of Science (former Web of Knowledge: includes Web of Science, Current Contents Connect, Conference Proceedings Citation Index, BIOSIS, Derwent Innovations Index, Data Citation Index, SciELO Citation Index) (all available years).
The Cochrane Library.
Allied and Complementary Medicine Database (AMED).
We also searched international trial registries via the World Health Organization trials portal (ICTRP) and ClinicalTrials.gov to identify unpublished or ongoing studies.
We did not restrict searches by date, language and publication status.
In June 2018, CCMD's Information Specialist updated the search for studies on all of the databases listed above (Appendix 3), with the exception of International Pharmaceutical Abstracts. The search of these databases was necessary as the CCMD‐CTR was out of date at the time (current to June 2016 only).
Searching other resources
Grey literature
To detect additional studies, we checked the following sources.
IFPMA (International Federation of Pharmaceutical Manufacturers and Associations) Clinical Trials Portal.
OpenGrey.
National Institute of Health RePORTER.
Health Services Research Projects in Progress (HSRProj).
Hayes Inc. Health Technology Assessment.
The New York Academy of Medicine Grey Literature Index.
Conference Papers Index.
European Medicines Agency.
Drugs@FDA (Food and Drug Administration).
National Registry of Evidence‐Based Programs and Practices (NREPP) (no longer available online).
Reference lists
We handsearched the references of all included studies and pertinent review articles.
Correspondence
We contacted trialists, subject matter experts and pharmaceutical companies to ask for information on unpublished or ongoing studies, or to request additional trial data.
Data collection and analysis
Selection of studies
Two review authors independently screened the titles and abstracts of all studies identified by the searches. We retrieved full‐text copies of all studies that potentially met the inclusion criteria as determined by this initial assessment, and two review authors independently screened them to determine their eligibility.
If the two review authors did not reach consensus, they discussed disagreements and resolved them through consultation with a third party. We contacted study authors if relevant information was missing. We tracked all results in an EndNote X8 database.
We recorded the selection process in sufficient detail to complete a PRISMA flow diagram (Moher 2009) and Characteristics of included studies tables.
Data extraction and management
Two review authors independently extracted study characteristics and outcome data using a data collection form that had been piloted on at least two studies in the review. We resolved discrepancies by reaching consensus or by involving another review author. We reported whether studies were detected by a search of databases of published studies, by handsearch or by a search of grey literature.
We extracted the following study characteristics.
Methods: study design, duration of study, details of any 'run‐in' period, duration of treatment period, number of study centres and locations, study setting, withdrawals and dates of studies.
Participants: number of participants, mean age, age range, proportion of women, number of prior depressive episodes, diagnostic criteria, inclusion criteria and exclusion criteria.
Interventions: intervention, comparison, concomitant interventions and excluded interventions.
Outcomes: primary and secondary outcomes specified and collected and time points reported.
Notes: funding for studies and notable conflicts of interest of study authors.
We noted in the Characteristics of included studies table if outcome data were not reported in a useable way. We resolved disagreements by reaching consensus or by involving a third person. One review author transferred data into the Review Manager file (Review Manager 2014). We double‐checked that data were entered correctly by comparing data presented in the systematic review versus those provided in the study reports. A second review author spot‐checked study characteristics for accuracy against the trial report.
Main planned comparisons
SGAs versus placebo.
SGAs versus other SGAs.
SGAs versus light therapy.
SGAs versus psychological therapies.
SGAs versus lifestyle interventions.
SGAs versus melatonin or agomelatine.
SGAs plus comparator intervention (as listed in Types of interventions) versus placebo.
SGAs plus comparator intervention (as listed in Types of interventions) versus the same comparator intervention as monotherapy (e.g. SGAs plus light therapy versus light therapy alone).
Assessment of risk of bias in included studies
Two review authors independently assessed risk of bias of included randomised trials using the Cochrane 'Risk of bias' tool, as described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). This tool includes assessment of random sequence generation; allocation concealment; blinding of participants, personnel and outcome assessors; incomplete outcome data; selective reporting; and other potential threats to validity. Specifically, we assessed attrition in these trials and reasons for attrition, particularly when attrition rates between two groups in a trial differed substantially. In addition, we assessed whether all relevant outcomes for the trial were reported in the published articles. We assigned each domain as high risk of bias, low risk of bias or unclear risk of bias. Review authors resolved discrepancies by reaching consensus or by consulting with a third review author.
For non‐randomised studies, we planned to use the Newcastle‐Ottawa scale, involving selection of cases or cohorts and controls, adjustment for confounders, methods of outcomes assessment, length of follow‐up and statistical analysis (Wells 2009).
Measures of treatment effect
We used data extracted from the original studies to construct 2 × 2 tables for dichotomous outcomes. When multiple studies allowed for quantitative analysis, we planned to calculate the risk ratio (RR) with 95% confidence intervals (CIs) for each outcome. We chose RR as an effect measure because for decision makers, RRs are easier to interpret than odds ratios (ORs), particularly when event rates are high.
We planned to pool continuous data using the mean difference (MD) if an outcome was measured on the same scale, or the standardised mean difference (SMD) if an outcome was measured on different scales. If available, we planned to use final measurements rather than changes from baseline to estimate differences between treatments. When it was considered necessary to use both change and post‐intervention scores within a comparison, we would have presented these by subgroup using the MD rather than the SMD.
For time‐to‐event data, we planned to calculate a pooled hazard ratio when this was available, or to dichotomise data at multiple time points into response/no response (e.g. at one week, at two weeks, at four weeks, etc.).
We intended to use the same time points as specified under 'Timing of outcomes assessment' to form the basis for dichotomisation into response/no response.
For non‐randomised studies, we planned to use adjusted treatment effects if available.
Unit of analysis issues
Cluster‐randomised trials
To incorporate cluster‐randomised trials, we intended to reduce the size of each trial to its 'effective sample size'. If intracluster correlation coefficients had not been reported, we planned to find external estimates from similar studies. We intended to undertake sensitivity analysis to assess the impact of including such trials.
Cross‐over trials
To avoid carry‐over effects, we planned to include data only from the first period of cross‐over studies.
Studies with multiple treatment groups
For included trials that consisted of multiple treatment groups (e.g. differing doses of one SGA versus placebo, or of multiple SGAs versus placebo), we planned to include data for the treatment arms and to halve data from the placebo arm, or to collapse the data for different doses into one group when this was clinically appropriate (Hansen 2009).
Dealing with missing data
We used intention‐to‐treat (ITT) analysis when data were missing for participants who dropped out of trials before completion. When data regarding an outcome of interest were not reported, we planned to contact authors of publications or the pharmaceutical company that funded the study to obtain missing results. We documented all correspondences.
Assessment of heterogeneity
We used the Cochran Chi2 test (Q‐test) to assess heterogeneity. We considered a P value less than 0.10 as statistically significant. We used the I2 statistic to estimate the degree of heterogeneity. This measure describes the percentage of total variation across studies that results from heterogeneity rather than from chance. We interpreted the importance of heterogeneity in terms of its magnitude and direction of effects. We did not consider thresholds; instead we adopted the overlapping bands, as suggested in the Cochrane Handbook for Systematic Reviews of Interventions. For example, we considered an I2 value between 0% and 40% as probably not important, between 30% and 60% as representing moderate heterogeneity, between 50% and 90% as representing substantial heterogeneity and between 75% and 100% as representing considerable heterogeneity (Higgins 2011).
Assessment of reporting biases
If we had found more than 10 studies, we planned to perform a funnel plot analysis. A funnel plot is a graph used to detect publication bias. We wanted to look at whether the largest studies were near the average with small studies spread on both sides of the average. Variations from this assumption can indicate the existence of publication bias, but asymmetry may not necessarily be caused by publication bias. In addition, we intended to use Kendell's tau (Begg 1994), Egger's regression intercept (Egger 1997), and Fail‐Safe N (Rosenthal 1979), to assess reporting biases.
Data synthesis
We analysed data using Review Manager 5 software (Review Manager 2014), and GRADEpro GDT (GRADEpro GDT 2015). We pooled data for meta‐analyses when participant groups were similar and when studies assessed the same treatments with the same comparator and had similar definitions of outcome measures over a similar duration of treatment.
We used Mantel‐Haenszel random‐effects models to combine results because baseline event rates in control groups varied by almost 10 percentage points despite identical study protocols for the included RCTs. For comparisons for which fixed effect models also seemed viable, we employed both models to determine differences between random effects and fixed effect meta‐analyses.
We rated the strength of the evidence by using the system developed by the GRADE Working Group (Guyatt 2011).
Subgroup analysis and investigation of heterogeneity
Sex, age, history of non‐seasonal major depressive episodes and psychiatric comorbidities are potential effect measure modifiers for prevention of SAD. If data had been sufficient, we planned to conduct subgroup analyses for the primary outcome measures. We planned to conduct subgroup analyses based on:
men versus women;
history of non‐seasonal major depressive disorder versus no history of non‐seasonal major depressive disorder;
younger than 65 years of age versus 65 years of age or older; and
Axis I, Axis II comorbidities versus no Axis I, Axis II comorbidities.
Sensitivity analysis
We conducted sensitivity analyses to test the robustness of decisions made during the review process.
We planned to conduct sensitivity analyses:
excluding small studies (i.e. studies with fewer than 30 participants);
excluding studies with high risk of bias (i.e. studies that had been rated as having high risk of bias in one or more domains);
excluding studies published only in abstract form;
with adjusted versus unadjusted results; and
excluding cluster‐randomised trials.
'Summary of findings' tables
We assessed the quality of the evidence using the GRADE approach and presented the results in a 'Summary of findings' table for our main comparisons and outcomes (as listed in Types of outcome measures). We did not stratify populations into low‐, medium‐ and high‐risk populations. For 'assumed risk', we used prevalence studies from countries in northern latitudes (e.g. Scandinavia, Canada, northern USA) in which SAD leads to substantial burden of disease.
We used GRADEpro GDT to rate the quality of evidence and to prepare the 'Summary of findings' table (GRADEpro GDT 2015).
Results
Description of studies
Results of the search
We identified 3745 citations through electronic searches and reviews of reference lists after de‐duplication of search results. We excluded 3619 records during title and abstract reviews. We included 126 articles for full‐text review and assessed them for eligibility. We included three studies (4 records) in this review. The PRISMA flow chart documents the disposition of the literature in this review (Figure 1). Under Excluded studies, we describe in greater detail the reasons for excluding these studies.
1.
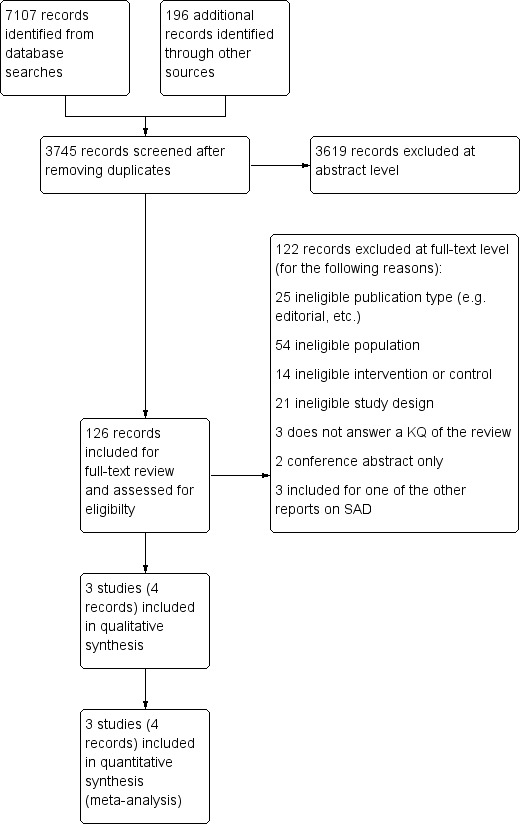
PRISMA flow chart.
Included studies
We included three RCTs (identified by the CCMD‐CTR, by ClinicalTrials.gov and published in a single manuscript (Modell 2005): WELL 100006, n = 512; WELL AK130930, n = 277; WELL AK130936, n = 311) comparing bupropion XL versus placebo for prevention of SAD. All three trials were funded by GlaxoSmithKline, the producer of bupropion XL. Records from the GlaxoSmithKline clinical trials database (www.gsk‐studyregister.com), provided additional data on these RCTs (WELL 100006; WELL AK130930; WELL AK130936). We found no additional non‐randomised studies that assessed risk of harms.
In the following section, we present study characteristics and results in greater detail (see also Characteristics of included studies).
Design
The three included RCTs were multicentre, double‐blinded, placebo‐controlled studies (WELL 100006; WELL AK130930; WELL AK130936). With the exception of a few differences (e.g. primary outcomes, allowed time to travel to sunny destinations), these trials had identical protocols. They enrolled participants between the months of September and November and lasted until spring (March) of the following year.
Sample sizes
Overall, trials included 1100 participants with a history of SAD. All three studies were powered at 90% to detect a difference in end of treatment depression‐free rates of 12%.
Setting
The three studies were conducted at 151 sites in northern USA or Canada, located between 38.5 and 61 degrees northern latitude.
Participants
Participants were adults with a history of SAD who were non‐depressed at enrolment into the study. Most participants were female (70%), had an average age of 42 years and reported, on average, 13 previous episodes of SAD. Eighty‐nine per cent of the study population was white. Participants were excluded if they had medical problems; a history of an eating disorder, bipolar I disorder, schizophrenia or other psychotic disorders; concomitant anxiety disorder; recurrent summer depressions; or recent drug or alcohol abuse; or had been treated for depression since the preceding winter or used psychoactive medications within three weeks of study entry.
Participants were recruited through the media and by referral from clinical practices. During the trials, participants were asked to refrain from using light therapy and from travelling to a sunny destination for longer than five days (seven days in one study).
Interventions
Participants initially received bupropion XL 150 mg every morning or matching placebo for one week. Thereafter, investigators increased the dose to 300 mg per day unless the individual did not tolerate the higher dose. Beginning the first week of spring, the dose was reduced to 150 mg per day, and treatment was subsequently discontinued.
Outcomes
The primary outcome in two of the three studies was time to onset of major depressive disorder (MDD) (WELL AK130930; WELL AK130936). The primary outcome in the third study was the difference in depression‐free participants at the end of the study. Investigators used the Seasonal Pattern Assessment Questionnaire and the SIGH‐SAD to evaluate participants during the course of the study. Recurrence of depression was defined as:
a score ≥ 20 on the SIGH‐SAD during two subsequent weeks; or
clinical depression (based on DSM‐IV) that required treatment.
Participants who became depressed were withdrawn from the study.
In all three trials, investigators assessed spontaneously reported adverse events without using a standardised instrument.
Excluded studies
Overall, we excluded 122 records at full‐text review level. Characteristics of excluded studies shows all records that narrowly missed the inclusion criteria for this systematic review. We excluded studies because included participants already had depressive symptoms when the study started. The study that was included in the review on light therapy (Nussbaumer 2015), is mentioned in Characteristics of excluded studies, where we have explained why it is not included in this review.
Ongoing studies
We identified no ongoing studies.
Studies awaiting classification
No studies are currently awaiting classification.
Risk of bias in included studies
For details on risk of bias judgements for each study, see Characteristics of included studies. We present graphical representations of overall risk of bias in included studies in Figure 2 and Figure 3.
2.
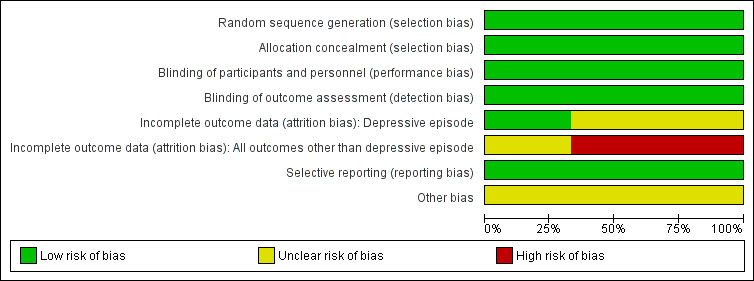
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
In all three trials, we rated this domain as low risk of bias. Participants were randomly assigned through block randomisation (block sizes of four). Researchers achieved allocation concealment with central randomisation, telephone registration and automated medication ordering.
Blinding
In all three trials, blinding was achieved with identically looking bupropion XL and placebo pills. We rated this domain as low risk of bias for all three trials.
Incomplete outcome data
Overall attrition rates and post‐randomisation exclusion rates were high for all three studies. For example, in one study, 53% of participants in the placebo group and 41% in the bupropion XL group discontinued treatment. Investigators excluded 48 participants (9%) from ITT analyses (WELL 100006). We present detailed attrition rates for each study under Characteristics of included studies. We rated risk of bias for this domain as high for two studies (WELL 100006; WELL AK130930), and as unclear for one study (WELL AK130936).
As specified a priori, participants who became depressed were withdrawn from the study. Consequently, high attrition rates will not affect onset of depression and discontinuation rates as outcomes. However, high attrition rates will pose a risk of bias for other outcomes such as adverse events.
Selective reporting
Reported outcomes match outcomes listed in clinicaltrials.gov. We rated this domain as low risk of bias for all three studies.
Other potential sources of bias
All three studies were funded by the producers of bupropion XL. How or to what extent potential funding bias has an impact on trial results remains unclear. We rated risk of funding bias as unclear for all three trials.
Effects of interventions
See: Table 1
We could conduct a meta‐analysis only for SGAs versus placebo. We were not able to undertake the following planned comparisons as no data were available.
SGAs versus other SGAs.
SGAs versus light therapy.
SGAs versus melatonin or agomelatine.
SGAs versus psychological therapies.
SGAs versus lifestyle interventions.
SGAs plus comparator intervention (as listed under 'Types of interventions') versus placebo.
SGAs plus comparator intervention (as listed under 'Types of interventions') versus the same comparator intervention as monotherapy (e.g. SGAs plus light therapy versus light therapy alone).
Comparison 1. SGAs versus placebo
Three studies, including 1042 participants, contributed data to this comparison (WELL 100006; WELL AK130930; WELL AK130936). However, information from these studies was limited to bupropion XL compared with placebo. We could find no eligible studies on other SGAs. Table 1 provides information on treatment effects and quality of evidence for relevant outcomes.
Primary outcomes
1.1 Incidence of SAD
Numbers of participants who experienced onset of a depressive episode are conflicting in available publications (WELL 100006; WELL AK130930; WELL AK130936). For our meta‐analyses, we used numbers that reflect the most conservative findings.
Across the three studies, fewer participants treated with bupropion XL than placebo experienced onset of a major depressive episode during the winter months (15% versus 27%; risk ratio (RR) 0.56, 95% confidence interval (CI) 0.44 to 0.72; 3 RCTs, 1100 participants, moderate‐quality evidence; see Analysis 1.1). The published article reported Kaplan‐Meier survival analyses that favoured bupropion XL over placebo in all three studies but reached statistical significance in only one study (Modell 2005). On the basis of the meta‐analysis presented in Analysis 1.1, we calculated numbers needed to treat for additional beneficial outcomes (NNTBs) for different baseline recurrence rates. For a population with a yearly recurrence rate of 30%, the NNTB is 8 (95% CI 6 to 12). In other words, eight people need to be treated with bupropion XL during the winter season to avoid the onset of a depressive episode in one person. For populations with yearly recurrence rates of 50% and 60%, NNTBs are 5 (95% CI 4 to 9) and 4 (95% CI 3 to 6), respectively. A fixed effect model rendered similar results as the random effects model.
1.1. Analysis.
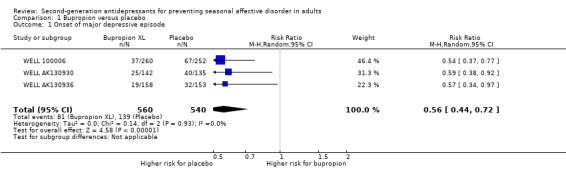
Comparison 1 Bupropion versus placebo, Outcome 1 Onset of major depressive episode.
1.2 Overall rate of adverse events
The risk of experiencing any adverse events during the course of a study was similar between participants treated with bupropion XL and those given placebo (85% versus 83%; RR 1.02, 95% CI 0.97 to 1.08; 3 RCTs, 1048 participants, moderate‐quality evidence; see Analysis 1.2). The risk of several specific adverse events, however, was higher for those treated with bupropion XL than for those given placebo. Specifically, participants taking bupropion XL had higher risk for headaches (34% versus 27%; RR 1.26, 95% CI 1.02 to 1.56; 3 RCTs, 1048 participants, moderate‐quality evidence; see Analysis 1.3), insomnia (20% versus 13%; RR 1.46, 95% CI 1.10 to 1.93; 3 RCTs, 1048 participants, low‐quality evidence; see Analysis 1.4), and nausea (13% versus 8%; RR 1.63, 95% CI 1.12 to 2.38; 3 RCTs, 1048 participants, low‐quality evidence; see Analysis 1.5).
1.2. Analysis.
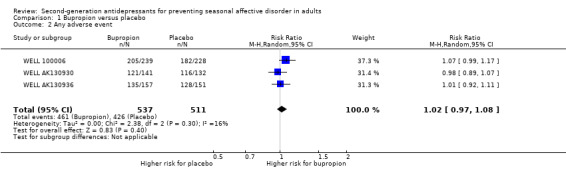
Comparison 1 Bupropion versus placebo, Outcome 2 Any adverse event.
1.3. Analysis.
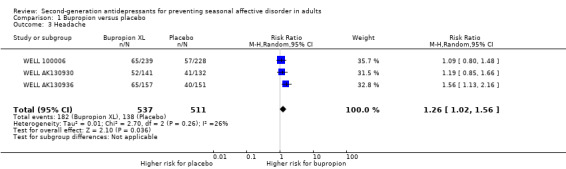
Comparison 1 Bupropion versus placebo, Outcome 3 Headache.
1.4. Analysis.
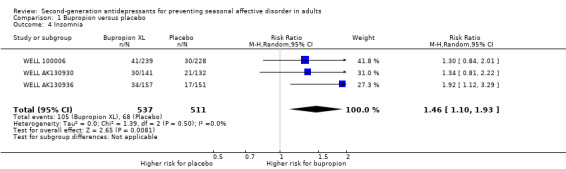
Comparison 1 Bupropion versus placebo, Outcome 4 Insomnia.
1.5. Analysis.
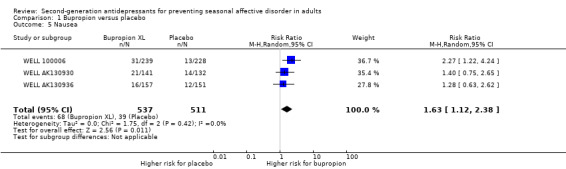
Comparison 1 Bupropion versus placebo, Outcome 5 Nausea.
The risk of diarrhoea was similar between participants taking bupropion XL and those given placebo (7% versus 7%; RR 1.04, 95% CI 0.66 to 1.64; 3 RCTs, 1048 participants, low‐quality evidence; see Analysis 1.6). Fixed effect models rendered similar results as random effects models.
1.6. Analysis.
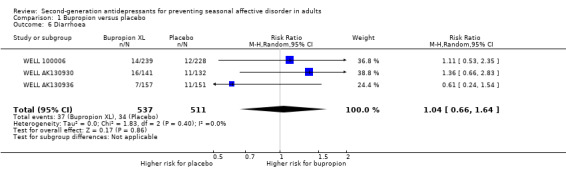
Comparison 1 Bupropion versus placebo, Outcome 6 Diarrhoea.
Secondary outcomes
1.3 Severity of SAD or SAD‐related symptoms
We found no eligible evidence addressing this outcome.
1.4 Quality of life
We found no eligible evidence addressing this outcome.
1.5 Quality of interpersonal and social functioning
We found no eligible evidence addressing this outcome.
1.6 Proportion of participants with serious adverse events
Across the three included studies, two participants treated with bupropion XL and one given placebo developed serious adverse events. Participants taking bupropion XL suffered from supraventricular tachycardia and duodenal ulcer bleeding, and the individual given placebo from goitre.
1.7 Rates of discontinuation due to adverse events
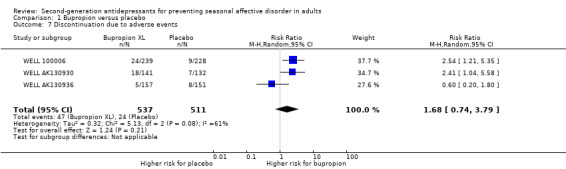
Rates of discontinuation due to adverse events were numerically higher for participants taking bupropion XL than for those given placebo (9% versus 5%; RR 1.68, 95% CI 0.74 to 3.79; 3 RCTs, 1048 participants, low‐quality evidence; see Analysis 1.7). Because of high heterogeneity, we did not employ a fixed effect model.
1.7. Analysis.
Comparison 1 Bupropion versus placebo, Outcome 7 Discontinuation due to adverse events.
1.8 Overall rate of discontinuation
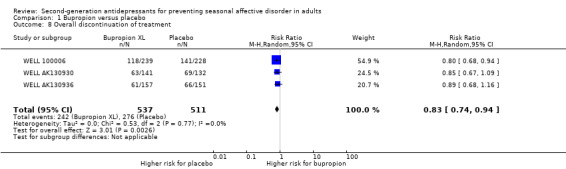
Overall rates of discontinuation were higher for participants in the placebo group than for those in the bupropion XL group (45% versus 54%; RR 0.83, 95% CI 0.74 to 0.94; 3 RCTs, 1048 participants, low‐quality evidence; see Analysis 1.8). However, this difference is attributable in part to the higher incidence of SAD in the placebo group. Participants who had an onset of MDD were withdrawn from the study as defined a priori in the study protocols. When participants with onset of MDD were not taken into consideration, overall discontinuation rates were high but similar between participants treated with bupropion XL and those given placebo (30% versus 28%). A fixed effect model rendered similar results as the random effects model.
1.8. Analysis.
Comparison 1 Bupropion versus placebo, Outcome 8 Overall discontinuation of treatment.
Subgroup analyses
Data were insufficient for subgroup analyses.
Sensitivity analyses
Data were insufficient for sensitivity analyses.
Reporting bias
Statistical methods did not indicate publication bias. As a result of the small number of included studies, such statistical approaches are unreliable and have to be interpreted cautiously. We did not detect outcomes reporting bias when we compared reported outcomes with those presented a priori in study protocols.
Discussion
Summary of main results
Bupropion XL is an efficacious intervention provided to prevent recurrence of depressive episodes in people with a history of seasonal affective disorder (SAD) (risk ratio (RR) 0.56, 95% confidence interval (CI) 0.44 to 0.72). Benefits must be balanced against risks of adverse events when treatment with bupropion XL is provided. Overall adverse event rates were similar between participants treated with bupropion XL and those given placebo. However, bupropion XL led to higher risk of headaches, insomnia and nausea, which might influence adherence to treatment. Weighing of benefits against harms will be influenced by the risk of a person experiencing a recurrence of depression with onset of autumn (fall) and winter. Numbers needed to treat for additional benefit vary by baseline risk. In the three included randomised controlled trials (RCTs), about 30% of participants given placebo experienced a recurrence of SAD. Eight (at least six but up to 12) people need to be treated during winter months to prevent new onset of depression in one person. In other words, seven individuals will experience no benefit from treatment but will be exposed to risk of harm. In populations with higher risks of recurrence, NNTBs are lower. Table 1 presents beneficial and adverse treatment effects and the respective quality of evidence for the main outcomes.
Overall completeness and applicability of evidence
A major limitation of our report is that our evidence is limited to bupropion XL, which has been compared only with placebo. We found no studies on other SGAs nor on other comparators of interest. However, bupropion XL is the only antidepressant that is currently licensed for use in SAD.
Populations included in the studies that met our eligibility criteria do not reflect the broad spectrum of people who experience SAD. Studies excluded participants who had medical problems; a history of an eating disorder, bipolar I disorder, schizophrenia or other psychotic disorders; concomitant anxiety disorder; recurrent summer depressions; or recent drug or alcohol abuse; or had been treated for depression since the preceding winter or had used psychoactive medications within three weeks of study entry. In addition, most study participants were white and female. Although subgroup analyses revealed no differences in treatment effects for members of other ethnicities and for males, these analyses might lack power; therefore, some uncertainty about applicability remains.
Finally, recurrence rates in the placebo groups of the three included trials were lower than in other studies, which report that up to two‐thirds of those diagnosed with SAD will face recurrence of a depressive episode the following winter (Rodin 1997).
Quality of the evidence
We graded the quality of evidence for available efficacy outcomes (incidence of SAD, reduction of points on the Structured Interview Guide for the Hamilton Depression Rating Scale, Seasonal Affective Disorders (SIGH‐SAD)) as moderate. The quality of evidence was limited by high attrition rates in all three trials and thus was downgraded for risk of bias.
We graded the quality of evidence for outcomes on harms as moderate and low. Quality of evidence was compromised by high attrition rates, event rates that did not fulfil the optimal information size and the fact that assessment of harms was limited to spontaneously reported adverse events.
Potential biases in the review process
Our eligibility criteria included non‐randomised studies for assessment of harms because methods research indicates that rare but potentially serious adverse events are not covered well in RCTs. Despite extensive literature searches, we identified no non‐randomised studies for any of the eligible interventions. Evidence derived from systematic reviews on populations other than those suffering from SAD suggests that bupropion XL is associated with risk for serious adverse events such as seizures or increased suicidal ideation, particularly among young adults (Gartlehner 2008).
If information provided in full‐text articles was unclear or missing, we attempted to contact study authors for clarification. However, the yield of this effort was small. Despite multiple attempts to contact study authors, few replied or were able to provide missing information.
All three included studies were funded by the producer of bupropion XL. Whether or to what extent funding bias had an impact on study results remains unclear.
Finally, publication bias and selective outcomes reporting are potential limitations for any systematic review. Although we searched for grey and unpublished literature, the extent and impact of reporting biases in this body of evidence are impossible to determine.
Agreements and disagreements with other studies or reviews
To our knowledge, no other studies have addressed this research question.
Authors' conclusions
Implications for practice.
Available evidence indicates that bupropion XL is an effective intervention for prevention of recurrence of seasonal affective disorder (SAD). Nevertheless, even in a high‐risk population, three out of four people will not benefit from preventive treatment with bupropion XL and will be at risk for harm. Clinicians need to discuss with patients advantages and disadvantages of preventive second‐generation antidepressant (SGA) treatment and to offer other potentially efficacious interventions, such as light treatment, psychological therapies or lifestyle interventions, which might have lower risks of adverse events. Given the lack of comparative evidence, the decision for or against initiating preventive treatment of SAD and the choice of treatment should be strongly based on patient preferences.
Implications for research.
To date, no comparative effectiveness research is available on best strategies for prevention of SAD. Future researchers must compare SGAs versus other treatment options, such as melatonin or agomelatine, light therapy, psychological therapies or lifestyle interventions to determine the comparative benefits and harms of competing preventive interventions, and to take patient‐relevant outcomes, such as functional capacity and quality of life into consideration. Also, future studies should be funded by independent sponsors that have no commercial interests.
What's new
| Date | Event | Description |
|---|---|---|
| 15 April 2019 | Amended | Minor correction made to the PRISMA diagram. |
History
Protocol first published: Issue 9, 2014 Review first published: Issue 11, 2015
| Date | Event | Description |
|---|---|---|
| 15 March 2019 | New citation required but conclusions have not changed | Review updated |
| 15 March 2019 | New search has been performed | We updated the searches on 19 June 2018; we did not identify any new trials. |
Acknowledgements
We would like to thank Evelyn Auer and Sandra Hummel for providing administrative support during the course of this review. We would also like to thank Angela Kaminski‐Hartenthaler, Julia Hoffmann, and Jeffrey H Sonis for their support when conducting the former version of this Cochrane Review.
CRG Funding Acknowledgement: The National Institute for Health Research (NIHR) is the largest single funder of the Cochrane Common Mental Disorders Group.
Disclaimer: the views and opinions expressed herein are those of the review authors and do not necessarily reflect those of the NIHR, the National Health Service (NHS) or the Department of Health and Social Care.
Appendices
Appendix 1. CCMDCTR: Core MEDLINE search
The search strategy listed below is the weekly OVID Medline search which was used to inform the Group’s specialised register (to June 2016). It is based on a list of terms for all conditions within the scope of the Cochrane Common Mental Disorders Group plus a sensitive RCT filter.
OVID MEDLINE search strategy, used to inform the Cochrane Common Mental Disorders Group's Specialised Register A weekly search alert based on condition + RCT filter only 1. [MeSH Headings]: eating disorders/ or anorexia nervosa/ or binge‐eating disorder/ or bulimia nervosa/ or female athlete triad syndrome/ or pica/ or hyperphagia/ or bulimia/ or self‐injurious behavior/ or self mutilation/ or suicide/ or suicidal ideation/ or suicide, attempted/ or mood disorders/ or affective disorders, psychotic/ or bipolar disorder/ or cyclothymic disorder/ or depressive disorder/ or depression, postpartum/ or depressive disorder, major/ or depressive disorder, treatment‐resistant/ or dysthymic disorder/ or seasonal affective disorder/ or neurotic disorders/ or depression/ or adjustment disorders/ or exp antidepressive agents/ or anxiety disorders/ or agoraphobia/ or neurocirculatory asthenia/ or obsessive‐compulsive disorder/ or obsessive hoarding/ or panic disorder/ or phobic disorders/ or stress disorders, traumatic/ or combat disorders/ or stress disorders, post‐traumatic/ or stress disorders, traumatic, acute/ or anxiety/ or anxiety, castration/ or koro/ or anxiety, separation/ or panic/ or exp anti‐anxiety agents/ or somatoform disorders/ or body dysmorphic disorders/ or conversion disorder/ or hypochondriasis/ or neurasthenia/ or hysteria/ or munchausen syndrome by proxy/ or munchausen syndrome/ or fatigue syndrome, chronic/ or obsessive behavior/ or compulsive behavior/ or behavior, addictive/ or impulse control disorders/ or firesetting behavior/ or gambling/ or trichotillomania/ or stress, psychological/ or burnout, professional/ or sexual dysfunctions, psychological/ or vaginismus/ or Anhedonia/ or Affective Symptoms/ or *Mental Disorders/ 2. [Title/ Author Keywords]: (eating disorder* or anorexia nervosa or bulimi* or binge eat* or (self adj (injur* or mutilat*)) or suicide* or suicidal or parasuicid* or mood disorder* or affective disorder* or bipolar i or bipolar ii or (bipolar and (affective or disorder*)) or mania or manic or cyclothymic* or depression or depressive or dysthymi* or neurotic or neurosis or adjustment disorder* or antidepress* or anxiety disorder* or agoraphobia or obsess* or compulsi* or panic or phobi* or ptsd or posttrauma* or post trauma* or combat or somatoform or somati#ation or medical* unexplained or body dysmorphi* or conversion disorder or hypochondria* or neurastheni* or hysteria or munchausen or chronic fatigue* or gambling or trichotillomania or vaginismus or anhedoni* or affective symptoms or mental disorder* or mental health).ti,kf. 3. [RCT filter]: (controlled clinical trial.pt. or randomized controlled trial.pt. or (randomi#ed or randomi#ation).ab,ti. or randomly.ab. or (random* adj3 (administ* or allocat* or assign* or class* or control* or determine* or divide* or distribut* or expose* or fashion or number* or place* or recruit* or subsitut* or treat*)).ab. or placebo*.ab,ti. or drug therapy.fs. or trial.ab,ti. or groups.ab. or (control* adj3 (trial* or study or studies)).ab,ti. or ((singl* or doubl* or tripl* or trebl*) adj3 (blind* or mask* or dummy*)).mp. or clinical trial, phase ii/ or clinical trial, phase iii/ or clinical trial, phase iv/ or randomized controlled trial/ or pragmatic clinical trial/ or (quasi adj (experimental or random*)).ti,ab. or ((waitlist* or wait* list* or treatment as usual or TAU) adj3 (control or group)).ab.) 4. (1 and 2 and 3)
Records are screened for reports of RCTs within the scope of the Cochrane Common Mental Disorders Group. Secondary reports of RCTs are tagged to the appropriate study record. Similar weekly search alerts are also conducted on OVID Embase and PsycINFO, using relevant subject headings (controlled vocabularies) and search syntax, appropriate to each resource.
Appendix 2. Database searches 2014
PubMed 26.05.2014
| Search | Query | Items found |
| #1 | Search "Seasonal Affective Disorder"[Mesh] | 1061 |
| #2 | Search "seasonal affective disorder"[All Fields] | 1415 |
| #3 | Search seasonal affective disorder* | 1451 |
| #4 | Search "seasonal depression"[All Fields] | 162 |
| #5 | Search seasonal mood disorder* | 10 |
| #6 | Search "winter depression" | 248 |
| #7 | Search SIGH‐SAD | 61 |
| #8 | Search (#1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7) | 1555 |
| #9 | Search (#8 AND 2013/05:2014[dp]) | 46 |
The Cochrane Library 26.05.2014
| ID | Search | Hits |
| #1 | seasonal affective disorder (Word variations have been searched) | 312 |
| #2 | winter blues (Word variations have been searched) | 25 |
| #3 | seasonal depression | 295 |
| #4 | seasonal mood disorder | 134 |
| #5 | winter depression | 256 |
| #6 | SIGH‐SAD | 39 |
| #7 | {or #1‐#6} Publication Date from 2013 to 2014 | 69 |
EMBASE 26.05.2014
| No. | Query | Results |
| #1 | 'seasonal affective disorder'/exp AND [humans]/lim AND [embase]/lim | 640 |
| #3 | 'seasonal affective disorder'/mj | 484 |
| #4 | #1 OR #3 | 831 |
| #5 | #4 AND [2013‐2014]/py | 79 |
PsycINFO, AMED, IPA, CINAHL (via EBSCO HOST) 26.05.2014
| # | Query | Limiters/Expanders | Last Run Via | Results |
| S1 | seasonal affective disorder | Limiters ‐ Published Date: 20130501‐ | Interface ‐ EBSCOhost Research Databases | 39 |
| Search modes ‐ Boolean/Phrase | Search Screen ‐ Advanced Search | |||
| Database ‐ PsycINFO;AMED ‐ The Allied and Complementary Medicine Database;CINAHL with Full Text;International Pharmaceutical Abstracts |
Web of Knowledge (via UNC) 28.05.2014
| Set | Results | |
| # 5 | 69 | #4 AND #1 |
| Timespan=2013‐2014 | ||
| Search language=English | ||
| # 4 | Approximately | #3 OR #2 |
| 1,107,073 | Timespan=2013‐2014 | |
| Search language=English | ||
| # 3 | Approximately | TOPIC: (treatment) |
| 975,242 | Timespan=2013‐2014 | |
| Search language=English | ||
| # 2 | Approximately | TOPIC: (prevention) |
| 188,628 | Timespan=2013‐2014 | |
| Search language=English | ||
| # 1 | 165 | TOPIC: ("seasonal affective disorder") |
| Timespan=2013‐2014 | ||
| Search language=English |
Appendix 3. Database searches 2018
Summary of searches (19‐June‐2018)
CCMD Register, n = 8
CENTRAL, n = 30
MEDLINE, n = 233
Embase, n = 301
PsycINFO, n = 154
International Pharmaceutical Abstracts, (database unavailable)
CINHAL, n = 77
Web of Knowledge, n = 489
AMED, n = 1
Total = 1293 Duplicates removed = 607 Number to screen = 686
Database search strategies
CCMD‐CTR (searched via Cochrane CRS) Date searched: Tuesday, 19th June 2018 (Register current to June 2016, only) Hits: 303 (8 in scope for this update) 1"seasonal affective disorder" AND INREGISTER (277) 2seasonal affective disorder* AND INREGISTER (280) 3"seasonal depression" AND INREGISTER34 4 seasonal mood disorder* AND INREGISTER (6) 5 "winter depression" AND INREGISTER (72) 6 SIGH‐SAD AND INREGISTER (48) 7 #1 OR #2 OR #3 OR #4 OR #5 OR #6 (303) Cochrane CENTRAL searched The Cochrane Library (Wiley interface) Data parameters: Issue 5 of 12, May 2018 Date searched: Tuesday, 19th June 2018 Hits: 363 (30 in scope for this update) #1 MeSH descriptor: [Seasonal Affective Disorder] explode all trees 172 #2 "seasonal affective disorder" 364 #3 seasonal affective disorder* 397 #4 "seasonal depression" 46 #5 seasonal mood disorder* 199 #6 "winter depression" 85 #7 SIGH‐SAD 55 #8 (#1 or #2 or #3 or #4 or #5 or #6 or #7) 452 Notes: Of 452 returned from searching The Cochrane Library, 363 were records from CENTRAL. Records dating pre‐2015 were visually inspected and manually removed.
Ovid MEDLINE(R) Epub Ahead of Print, In‐Process & Other Non‐Indexed Citations, Ovid MEDLINE(R) Daily and Ovid MEDLINE(R) Data parameters: 1946 to Present Date searched: Tuesday, 19th June 2018 Hits: 233 1 Seasonal Affective Disorder/1180 2 "seasonal affective disorder".ti,ab,kw,ot.1206 3 seasonal affective disorder*.ti,ab,kw,ot.1277 4 "seasonal depression".ti,ab,kw,ot.188 5 seasonal mood disorder*.ti,ab,kw,ot.12 6 "winter depression".ti,ab,kw,ot.272 7 SIGH‐SAD.ti,ab,kw,ot.78 8 (1 or 2 or 3 or 4 or 5 or 6 or 7) 1790 9 (2015* or 2016* or 2017* or 2018*).yr,ed. 4792024 10 (8 and 9) 233
Embase (Ovid Interface) Data parameters: 1974 to 2018 June 18 Date searched: Tuesday, 19th June 2018 Hits: 301 1 Seasonal Affective Disorder/ 1239 2 "seasonal affective disorder".ti,ab,kw,ot. 1528 3 seasonal affective disorder*.ti,ab,kw,ot. 1618 4 "seasonal depression".ti,ab,kw,ot. 246 5 seasonal mood disorder*.ti,ab,kw,ot. 23 6 "winter depression".ti,ab,kw,ot. 334 7 SIGH‐SAD.ti,ab,kw,ot. 92 8 (1 or 2 or 3 or 4 or 5 or 6 or 7) 2297 9 (2015* or 2016* or 2017* or 2018*).yr,ed. 4907927 10 (8 and 9) 301
PsycINFO (Ovid) Data parameters: 2002 to June Week 2 2018 Date searched: Tuesday, 19th June 2018 Hits: 154 1 Seasonal Affective Disorder/ 484 2 "seasonal affective disorder".ti,ab,kw,ot. 511 3 seasonal affective disorder*.ti,ab,kw,ot. 529 4 "seasonal depression".ti,ab,kw,ot. 94 5 seasonal mood disorder*.ti,ab,kw,ot. 6 6 "winter depression".ti,ab,kw,ot. 72 7 SIGH‐SAD.ti,ab,kw,ot. 53 8 (1 or 2 or 3 or 4 or 5 or 6 or 7) 690 9 (2015* or 2016* or 2017* or 2018*).yr,ed. 633488 10 (8 and 9) 154
CINAHL via EBSCOHost Data parameters: 1937‐Current Date searched: Tuesday, 19th June 2018 Hits: 77 S9 (S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7) Limiters: Published Date (20150101 ‐ 20180631) 77 S8 (S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7) 454 S7 TI SIGH‐SAD OR AB SIGH‐SAD 15 S6 TI "winter depression" OR AB "winter depression" 24 S5 TI seasonal mood disorder* OR AB seasonal mood disorder* 16 S4 TI "seasonal depression" OR AB "seasonal depression" 43 S3 TI Seasonal Affective Disorder* OR AB Seasonal Affective Disorder* 287 S2 TI "Seasonal Affective Disorder" OR AB "Seasonal Affective Disorder" 276 S1 (MM "Seasonal Affective Disorder") 365
Web of Science (Web of Science Core Collection, BIOSIS, Data citation Index, KCI Korean Journal Database, MEDLINE, Russian Science Citation Database, SciELO Citation Index)* Data parameters: 1900 to Present Date searched: Tuesday, 19th June 2018 Hits: 489 #8 TOPIC ((#6 OR #5 OR #4 OR #3 OR #2 OR #1) Refined by: PUBLICATION YEARS (2018 OR 2017 OR 2016 OR 2015) 489 #7 TOPIC (#6 OR #5 OR #4 OR #3 OR #2 OR #1) 3819 #6 TOPIC (SIGH‐SAD) 84 #5 TOPIC ("winter depression") 790 #4 TOPIC (seasonal mood disorder*) 1525 #3 TOPIC ("seasonal depression") 267 #2 TOPIC (Seasonal Affective Disorder*) 3355 #1 TOPIC ("Seasonal Affective Disorder") 3007
Notes: In the 2015 review, which these searches update, Web of Knowledge was searched. Web of Knowledge (containing includes Web of Science, Current Contents Connect, Conference Proceedings Citation Index, BIOSIS, Derwent Innovations Index, Data Citation Index, SciELO Citation Index) has been discontinued. This search was the closest representation of the previous search.
Allied and Complementary Medicine Database (AMED) Data parameters: 1985 to June 2018 Date searched: Tuesday, 19th June 2018 Hits: 1 1 Seasonal Affective Disorder/ 0 2 "seasonal affective disorder".ti,ab,kw,ot. 28 3 seasonal affective disorder*.ti,ab,kw,ot. 28 4 "seasonal depression".ti,ab,kw,ot. 2 5 seasonal mood disorder*.ti,ab,kw,ot. 0 6 "winter depression".ti,ab,kw,ot. 4 7 SIGH‐SAD.ti,ab,kw,ot. 2 8 (1 or 2 or 3 or 4 or 5 or 6 or 7) 32 9 (2015* or 2016* or 2017* or 2018*).yr,ed. 22289 10 (8 and 9) 1
Trials registers WHO International Clinical Trials Registry Platform (ICTRP) searched via: http://apps.who.int/trialsearch/Default.aspx search date: Tuesday, 19th June 2018 seasonal n = 113 records for 49 trials. These records were visually inspected and 20 records were retained for screening SIGH‐SAD n = 0 Clinical Trials.Gov searched via: https://www.clinicaltrials.gov/ct2/home search date: Tuesday, 19th June 2018 Records were visually inspected and records 2015‐current when exported to Endnote. Search field: Condition or Disease seasonal affective n = 3 seasonal depression n = 3 (being duplicates of the above) SIGH‐SAD n = 0
Data and analyses
Comparison 1. Bupropion versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Onset of major depressive episode | 3 | 1100 | Risk Ratio (M‐H, Random, 95% CI) | 0.56 [0.44, 0.72] |
| 2 Any adverse event | 3 | 1048 | Risk Ratio (M‐H, Random, 95% CI) | 1.02 [0.97, 1.08] |
| 3 Headache | 3 | 1048 | Risk Ratio (M‐H, Random, 95% CI) | 1.26 [1.02, 1.56] |
| 4 Insomnia | 3 | 1048 | Risk Ratio (M‐H, Random, 95% CI) | 1.46 [1.10, 1.93] |
| 5 Nausea | 3 | 1048 | Risk Ratio (M‐H, Random, 95% CI) | 1.63 [1.12, 2.38] |
| 6 Diarrhoea | 3 | 1048 | Risk Ratio (M‐H, Random, 95% CI) | 1.04 [0.66, 1.64] |
| 7 Discontinuation due to adverse events | 3 | 1048 | Risk Ratio (M‐H, Random, 95% CI) | 1.68 [0.74, 3.79] |
| 8 Overall discontinuation of treatment | 3 | 1048 | Risk Ratio (M‐H, Random, 95% CI) | 0.83 [0.74, 0.94] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
WELL 100006.
| Methods | Randomised controlled trial (multicentre: 47 centres in northern portions of the USA) | |
| Participants | 512 adult participants with a history of MDD with a seasonal pattern (autumn/winter pattern) who scored < 7 on the HAM‐D‐17 and < 10 on the SIGH‐SAD at baseline | |
| Interventions | Bupropion XL 150 to 300 mg every morning from autumn (starting September to November) until the first week of spring | |
| Outcomes | Recurrence of MDD, time to depressive episode, mean change from baseline on the SIGH‐SAD, HAM‐D 17 total score, SIGH‐SAD 7‐item subscale score, adverse events | |
| Funding source | The study was funded by GlaxoSmithKline | |
| Dates | The study was conducted from September 2003 to June 2004 | |
| Declaration of interest | All but one study author were employees of GlaxoSmithKline | |
| Notes | This publication was identified through a systematic literature search of electronic databases | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisation (blocks of 4) |
| Allocation concealment (selection bias) | Low risk | Telephone registration and automated medication ordering |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Matching placebo tablets |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Matching placebo tablets |
| Incomplete outcome data (attrition bias) Depressive episode | Low risk | 48 participants (9%) were excluded from ITT analyses: 22 in the bupropion XL group, 26 in the placebo group. Those who developed a depressive episode were withdrawn from the study |
| Incomplete outcome data (attrition bias) All outcomes other than depressive episode | High risk | Overall, 58% of participants in the placebo group and 47% in the bupropion XL group discontinued treatment. 48 participants (9%) were excluded from ITT analyses |
| Selective reporting (reporting bias) | Low risk | Outcomes in the study protocol are also reported as results |
| Other bias | Unclear risk | This study was funded by the producer of bupropion XL |
WELL AK130930.
| Methods | Randomised controlled trial (multicentre: 43 centres in the USA and 8 in Canada) | |
| Participants | 277 adult participants with a history of MDD with a seasonal pattern (autumn/winter pattern) who scored < 7 on the HAM‐D‐17 and < 10 on the SIGH‐SAD at baseline | |
| Interventions | Bupropion XL 150 to 300 mg every morning from autumn (starting September to November) until the first week of spring | |
| Outcomes | Primary outcome: time to onset of seasonal MDD (defined as SIGH‐SAD > 20 or investigators' judgement of the need for treatment based on DSM‐IV criteria) Secondary outcomes: proportion of participants with recurrence of MDD, mean change from baseline on SIGH‐SAD, HAM‐D 17 total score, SIGH‐SAD 7‐item subscale score, modified visual analogue pain assessment score, adverse events |
|
| Funding source | This study was funded by GlaxoSmithKline | |
| Dates | This study was conducted from September 2002 to June 2003 | |
| Declaration of interest | All but one study author were employees of GlaxoSmithKline | |
| Notes | This publication was identified through a systematic literature search of electronic databases | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisation (blocks of 4) |
| Allocation concealment (selection bias) | Low risk | Telephone registration and automated medication ordering |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Matching placebo tablets |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Matching placebo tablets |
| Incomplete outcome data (attrition bias) Depressive episode | Unclear risk | 5 participants (2%) were excluded from ITT analyses: 2 in the bupropion XL group, 3 in the placebo group. Overall dropout rates were not reported; overall, 52% of participants in the placebo group and 42% in the bupropion XL group discontinued treatment |
| Incomplete outcome data (attrition bias) All outcomes other than depressive episode | High risk | Overall, 52% of participants in the placebo group and 42% in the bupropion XL group discontinued treatment; 5 (2%) were excluded from ITT analyses |
| Selective reporting (reporting bias) | Low risk | Outcomes in the study protocol are also reported as results |
| Other bias | Unclear risk | This study was funded by the producer of bupropion XL |
WELL AK130936.
| Methods | Randomised controlled trial (multicentre: 48 centres in the USA, 7 centres in Canada) | |
| Participants | 311 adult participants with a history of MDD with a seasonal pattern (autumn/winter pattern) who scored < 7 on the HAM‐D‐17 and < 10 on the SIGH‐SAD at baseline | |
| Interventions | Bupropion XL 150 to 300 mg every morning from autumn (starting September to November) until the first week of spring | |
| Outcomes | Primary outcome: time to onset of seasonal MDD (defined as SIGH‐SAD > 20 or investigators' judgement of the need for treatment based on DSM‐IV criteria) Secondary outcomes: proportion of participants with recurrence of MDD, mean change from baseline on the SIGH‐SAD, HAM‐D 17 total score, SIGH‐SAD 7‐item subscale score, modified visual analogue pain assessment score, adverse events |
|
| Funding source | This study was funded by GlaxoSmithKline | |
| Dates | This study was conducted from September 2002 to June 2003 | |
| Declaration of interest | All but one study author were employees of GlaxoSmithKline | |
| Notes | This publication was identified through a systematic literature search of electronic databases | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisation (blocks of 4) |
| Allocation concealment (selection bias) | Low risk | Telephone registration and automated medication ordering |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Matching placebo tablets |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Matching placebo tablets |
| Incomplete outcome data (attrition bias) Depressive episode | Unclear risk | 5 participants (2%) were excluded from ITT analyses: 2 in the bupropion XL group, 3 in the placebo group. Overall, 34% of those in the placebo group and 41% in the bupropion XL group discontinued treatment |
| Incomplete outcome data (attrition bias) All outcomes other than depressive episode | Unclear risk | Overall, 34% of participants in the placebo group and 41% in the bupropion XL group discontinued treatment; 5 (2%) were excluded from ITT analyses |
| Selective reporting (reporting bias) | Low risk | Outcomes in the study protocol are also reported as results |
| Other bias | Unclear risk | This study was funded by the producer of bupropion XL |
HAM‐D: Hamilton Rating Scale for Depression ITT: intention‐to‐treat MDD: major depressive disorder SAD: seasonal affective disorder SIGH‐SAD‐SR: Hamilton Depression Rating Scale‐Seasonal Affective Disorders self‐rating version
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Martiny 2004 | This study included participants who already had symptoms when the study started. Investigators treated them with citalopram or placebo and investigated relapse prevention of SAD. As participants already had depressive symptoms when treatment was started, this study was not relevant for inclusion in this systematic review |
| Meesters 1999 | This study investigated different types of light therapy for prevention of SAD. This study is included in the systematic review on efficacy and safety of light therapy for SAD prevention; however, as it does not investigate efficacy nor safety of SGAs as preventive treatment, this study is not relevant for inclusion in this systematic review |
| Thorell 1999 | This study investigated relapse prevention, not prevention of SAD. Included participants already had symptoms when the study started |
SAD: seasonal affective disorder SGAs: second‐generation antidepressants
Differences between protocol and review
We reclassified vilazodone from 'SSRIs' to 'other antidepressants' because it is also a partial 5‐HT1A‐receptor agonist.
Contributions of authors
GG and BN drafted and revised the review text; MvN ran grey literature searches. BG, DW and CF provided clinical expertise for the Background section. BN, GG, BG, CF, AG, LM, JW, LL screened records on title/abstract and full‐text level. GG, BN extracted data and assessed the risk of bias of the included study and conducted the GRADE assessment. All authors reviewed the manuscript and provided feedback on individual drafts.
Sources of support
Internal sources
Internal funds of Cochrane Austria, Austria.
External sources
No sources of support supplied
Declarations of interest
Gerald Gartlehner ‐ no conflict of interest
Barbara Nussbaumer‐Streit ‐ no conflict of interest
Bradley N Gaynes ‐ no conflict of interest
Catherine A Forneris ‐ no conflict of interest
Laura C Morgan ‐ no conflict of interest
Amy Greenblatt ‐ no conflict of interest
Jörg Wipplinger ‐ no conflict of interest
Linda J Lux ‐ no conflict of interest
Megan G Van Noord ‐ no conflict of interest
Dietmar Winkler ‐ has received lecture fees from Angelini Pharmaceuticals, Lundbeck Pharmaceuticals and Pro Mente Austria and has received authorship honoraria from Medizin Medien Austria.
Edited (no change to conclusions)
References
References to studies included in this review
WELL 100006 {published and unpublished data}
- GlaxoSmithKline. A 7‐month, multicenter, randomized, double‐blind, placebo‐controlled comparison of 150‐300mg/day of extended‐release bupropion hydrochloride (WELLBUTRIN XL) and placebo for the prevention of seasonal affective disorder in subjects with a history of seasonal affective disorder followed by an 8‐week observational follow‐up phase. GSK ‐ Clinical Study Register [www.gsk‐clinicalstudyregister.com] 2003.
- Modell JG, Rosenthal NE, Harriett AE, Krishen A, Asgharian A, Foster VJ, et al. Seasonal affective disorder and its prevention by anticipatory treatment with bupropion XL. Biological Psychiatry 2005;58(8):658‐67. [DOI] [PubMed] [Google Scholar]
WELL AK130930 {published and unpublished data}
- GlaxoSmithKline. A 7‐month, multicenter, randomized, double‐blind, placebo‐controlled comparison of 150‐300mg/day of extended‐release bupropion hydrochloride (WELLBUTRIN XL) and placebo for the prevention of seasonal affective disorder in subjects with a history of seasonal affective disorder followed by an 8‐week observational follow‐up phase. GSK ‐ Clinical Study Register [www.gsk‐clinicalstudyregister.com] 2003.
- Modell JG, Rosenthal NE, Harriett AE, Krishen A, Asgharian A, Foster VJ, et al. Seasonal affective disorder and its prevention by anticipatory treatment with bupropion XL. Biological Psychiatry 2005;58(8):658‐67. [DOI] [PubMed] [Google Scholar]
WELL AK130936 {published and unpublished data}
- GlaxoSmithKline. A 7‐month, multicenter, randomized, double‐blind, placebo‐controlled comparison of 150‐300mg/day of extended‐release bupropion hydrochloride (WELLBUTRIN XL) and placebo for the prevention of seasonal affective disorder in subjects with a history of seasonal affective disorder followed by an 8‐week observational follow‐up phase. GSK ‐ Clinical Study Register [www.gsk‐clinicalstudyregister.com] 2004.
- Modell JG, Rosenthal NE, Harriett AE, Krishen A, Asgharian A, Foster VJ, et al. Seasonal affective disorder and its prevention by anticipatory treatment with bupropion XL. Biological Psychiatry 2005;58(8):658‐67. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Martiny 2004 {published data only}
- Martiny K, Lunde M, Simonsen C, Clemmensen L, Poulsen DL, Solstad K, et al. Relapse prevention by citalopram in SAD patients responding to 1 week of light therapy. A placebo‐controlled study. Acta Psychiatrica Scandinavica 2004;109:230‐4. [DOI] [PubMed] [Google Scholar]
Meesters 1999 {published data only}
- Meesters Y, Beersma DG, Bouhuys AL, Hoofdakker RH. Prophylactic treatment of seasonal affective disorder (SAD) by using light visors: bright white or infrared light?. Biological Psychiatry 1999;46:239‐46. [DOI] [PubMed] [Google Scholar]
Thorell 1999 {published data only}
- Thorell LH, Kjellman B, Arned M, Lindwall‐Sundel K, Walinder J, Wetterberg L. Light treatment of seasonal affective disorder in combination with citalopram or placebo with 1‐year follow‐up. International Clinical Psychopharmacology 1999;14 Suppl 2:S7‐11. [PubMed] [Google Scholar]
Additional references
APA 1980
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd Edition. Washington, DC: American Psychiatric Association, 1980. [Google Scholar]
APA 1987
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 3rd Edition. Washington, DC: American Psychiatric Association, 1987. [Google Scholar]
APA 2000
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (text revision). 4th Edition. Washington, DC: American Psychiatric Association, 2000. [Google Scholar]
APA 2013
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th Edition. Washington, DC: American Psychiatric Association, 2013. [Google Scholar]
Begg 1994
- Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994;50:1088‐101. [PubMed] [Google Scholar]
Byrne 2008
- Byrne B, Brainard GC. Seasonal affective disorder and light therapy. Sleep Medicine Clinics 2008;3(2):307–15. [Google Scholar]
Ciarleglio 2011
- Ciarleglio CM, Resuehr HES, McMahon DG. Interactions of the serotonin and circadian systems: nature and nurture in rhythms and blues. Neuroscience 2011;197:8‐16. [DOI] [PubMed] [Google Scholar]
Davis 1997
- Davis R, Whittington R, Bryson HM. Nefazodone. A review of its pharmacology and clinical efficacy in the management of major depression. Drugs 1997;53:608‐36. [DOI] [PubMed] [Google Scholar]
Egger 1997
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a simple graphical test. BMJ 1997;315:629‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Foley 2006
- Foley KF, DeSanty KP, Kast RE. Bupropion: pharmacology and therapeutic applications. Expert Review of Neurotherapeutics 2006;6:1249‐65. [DOI] [PubMed] [Google Scholar]
Forneris 2015
- Forneris CA, Nussbaumer B, Kaminski‐Hartenthaler A, Morgan LC, Gaynes BN, Sonis JH, et al. Psychological therapies for preventing seasonal affective disorder. Cochrane Database of Systematic Reviews 2015, Issue 11. [DOI: 10.1002/14651858.CD011270.pub2] [DOI] [PubMed] [Google Scholar]
Gartlehner 2008
- Gartlehner G, Thieda P, Hansen RA, Gaynes BN, Deveaugh‐Geiss A, Krebs EE, et al. Comparative risk for harms of second‐generation antidepressants: a systematic review and meta‐analysis. Drug Safety 2008;31(10):851‐65. [DOI] [PubMed] [Google Scholar]
Golden 2005
- Golden RN, Gaynes BN, Ekstrom RD, Hamer RM, Jacobsen FM, Suppes T, et al. The efficacy of light therapy in the treatment of mood disorders: a review and meta‐analysis of the evidence. American Journal of Psychiatry 2005;162(4):656‐62. [DOI] [PubMed] [Google Scholar]
GRADEpro GDT 2015 [Computer program]
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015.
Guyatt 2011
- Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. Journal of Clinical Epidemiology 2011;64(4):383‐94. [DOI] [PubMed] [Google Scholar]
Hamilton 1960
- Hamilton M. A rating scale for depression. Journal of Neurology, Neurosurgery and Psychiatry 1960;23:56‐62. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hansen 2009
- Hansen RA, Moore CG, Dusetzina SB, Leinwand BI, Gartlehner G, Gaynes B. Controlling for drug dose in systematic review and meta‐analysis: a case study of effect of antidepressant dose. Medical Decision Making 2009;29(1):91‐103. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Kaminski‐Hartenthaler 2015
- Kaminski‐Hartenthaler A, Nussbaumer B, Forneris CA, Morgan LC, Gaynes BN, Sonis JH, et al. Melatonin and agomelatine for preventing seasonal affective disorder. Cochrane Database of Systematic Reviews 2015, Issue 11. [DOI: 10.1002/14651858.CD011271.pub2] [DOI] [PubMed] [Google Scholar]
Kent 2000
- Kent JM. SNaRIs, NaSSAs, NaRIs: new agents for the treatment of depression. Lancet 2000;355(9207):911‐8. [DOI] [PubMed] [Google Scholar]
Lam 2006
- Lam RW, Levitt AJ, Levitan RD, Enns MW, Morehouse R, Michalak EE, et al. The Can‐SAD study: a randomized controlled trial of the effectiveness of light therapy and fluoxetine in patients with winter seasonal affective disorder. American Journal of Psychiatry 2006;163(5):805‐12. [DOI] [PubMed] [Google Scholar]
Leon 1999
- Leon AC, Solomon DA, Mueller TI, Turvey CL, Endicott J, Keller MB. The Range of Impaired Functioning Tool (LIFE‐RIFT): a brief measure of functional impairment. Psychological Medicine 1999;29(4):869‐78. [DOI] [PubMed] [Google Scholar]
Levitan 2007
- Levitan RD. The chronobiology and neurobiology of winter seasonal affective disorder. Dialogues in Clinical Neuroscience 2007;9(3):315‐24. [DOI] [PMC free article] [PubMed] [Google Scholar]
Magnusson 2005
- Magnusson A, Partonen T. The diagnosis, symptomatology, and epidemiology of seasonal affective disorder. CNS Spectrums 2005;10(8):625‐34. [DOI] [PubMed] [Google Scholar]
Modell 2005
- Modell JG, Rosenthal NE, Harriett AE, Krishen A, Asgharian A, Foster VJ, et al. Seasonal affective disorder and its prevention by anticipatory treatment with bupropion XL. Biological Psychiatry 2005;58(8):658‐67. [DOI] [PubMed] [Google Scholar]
Moher 2009
- Moher D, Liberati A, Tetzlaff J, Altman DG. The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta‐Analyses: The PRISMA Statement. PLoS Medicine 2009;6(7):e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
Neumeister 2001
- Neumeister A, Konstantinidis A, Praschak‐Rieder N, Willeit M, Hilger E, Stastny J, et al. Monoaminergic function in the pathogenesis of seasonal affective disorder. International Journal of Neuropsychopharmacology 2001;4:409‐20. [DOI] [PubMed] [Google Scholar]
Nussbaumer 2015
- Nussbaumer B, Kaminski‐Hartenthaler A, Forneris CA, Morgan LC, Sonis JH, Gaynes BN, et al. Light therapy for preventing seasonal affective disorder. Cochrane Database of Systematic Reviews 2015, Issue 11. [DOI: 10.1002/14651858.CD011269.pub2] [DOI] [PubMed] [Google Scholar]
Review Manager 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rodin 1997
- Rodin I, Thompson C. Seasonal affective disorder. Advances in Psychiatric Treatment 1997;3:352‐9. [Google Scholar]
Rosen 1990
- Rosen LN, Targum SD, Terman M, Bryant MJ, Hoffman H, Kasper SF. Prevalence of seasonal affective disorder at four latitudes. Psychiatry Research 1990;31:131‐44. [DOI] [PubMed] [Google Scholar]
Rosenthal 1979
- Rosenthal R. The "file‐drawer problem" and tolerance for null results. Psychological Bulletin 1979;86:638‐41. [Google Scholar]
Rosenthal 1984
- Rosenthal NE, Sack DA, Gillin JC, Lewy AJ, Goodwin FK, Davenport Y, et al. Seasonal affective disorder. A description of the syndrome and preliminary findings with light therapy. Archives of General Psychiatry 1984;41(1):72‐80. [DOI] [PubMed] [Google Scholar]
Schwartz 1996
- Schwartz PJ, Brown C, Wehr TA, Rosenthal NE. Winter seasonal affective disorder: a follow‐up study of the first 59 patients of the National Institute of Mental Health Seasonal Studies Program. American Journal of Psychiatry 1996;153(8):1028‐36. [DOI] [PubMed] [Google Scholar]
Sohn 2005
- Sohn CH, Lam RW. Update on the biology of seasonal affective disorder. CNS Spectrums 2005;10(8):635‐46. [DOI] [PubMed] [Google Scholar]
Stahl 2009
- Stahl SM. Mechanism of action of trazodone: a multifunctional drug. CNS Spectrums 2009;14:536‐46. [DOI] [PubMed] [Google Scholar]
Thaler 2010
- Thaler K, Delivuk M, Chapman A, Gaynes BN, Kaminski A, Gartlehner G. Second‐generation antidepressants for seasonal affective disorder. Cochrane Database of Systematic Reviews 2011, Issue 12. [DOI: 10.1002/14651858.CD008591.pub2] [DOI] [PubMed] [Google Scholar]
Ware 1992
- Ware JE Jr, Sherbourne CD. The MOS 36‐item short‐form health survey (SF‐36). I. Conceptual framework and item selection. Medical Care 1992;30(6):473‐83. [PubMed] [Google Scholar]
Wells 2009
- Wells GA, Shea B, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta‐analyses. www.ohri.ca/programs/clinical_epidemiology/oxford.htm 2009.
Westrin 2007
- Westrin A, Lam RW. Long‐term and preventative treatment for seasonal affective disorder. CNS Drugs 2007;21(11):901‐9. [DOI] [PubMed] [Google Scholar]
Williams 2002
- Williams JBW, Link MJ, Rosenthal NE, Terman M. Structured Interview Guide for the Hamilton Depression Rating Scale ‐ Seasonal Affective Disorder version (SIGH‐SAD). New York: New York State Psychiatric Institute, 2012. [Google Scholar]
References to other published versions of this review
Gartlehner 2014
- Gartlehner G, Nussbaumer B, Gaynes BN, Forneris CA, Morgan LC, Kaminski‐Hartenthaler A, et al. Second‐generation antidepressants for preventing seasonal affective disorder. Cochrane Database of Systematic Reviews 2014, Issue 9. [DOI: 10.1002/14651858.CD011268] [DOI] [PubMed] [Google Scholar]
Gartlehner 2015
- Gartlehner G, Nussbaumer B, Gaynes BN, Forneris CA, Morgan LC, Kaminski‐Hartenthaler A, et al. Second‐generation antidepressants for preventing seasonal affective disorder in adults. Cochrane Database of Systematic Reviews 2015, Issue 11. [DOI: 10.1002/14651858.CD011268.pub2] [DOI] [PubMed] [Google Scholar]