
Figure 1.
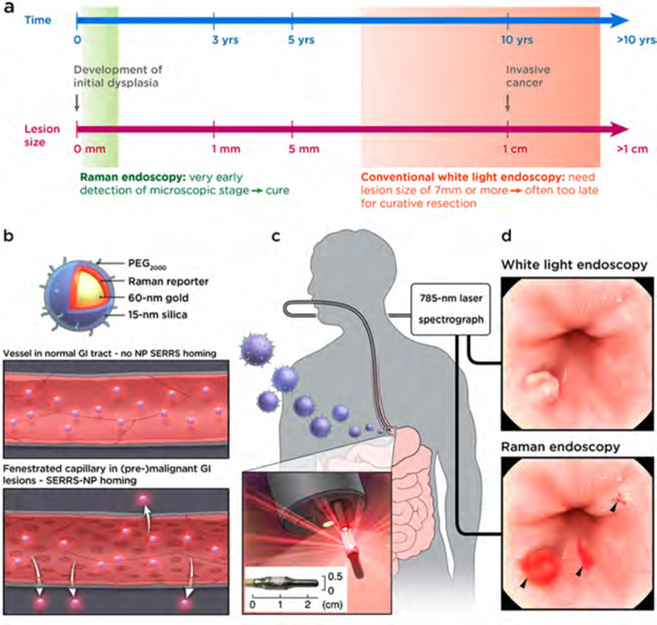
Concept of contrast-enhanced Raman imaging of gastrointestinal lesions. In contrast to white-light endoscopy, very small premalignant lesions, microscopic malignant lesions, and otherwise occult (flat) lesions can be detected. (a) Comparison of lesion detectability between SERRS-NP-enhanced Raman endoscopy and conventional white-light endoscopy currently used in the clinic. While white-light endoscopy requires lesions to be at least 5−7 mm in size to be detectable, Raman endoscopy can detect lesions at 0.5−1.0 mm. Depending on the growth characteristics of different GI tumors, Raman endoscopy has the potential to “catch” lesions much earlier, at a premalignant stage where localized lesion removal could result in cures (depicted time line is approximated for colon cancer; there are large variations, and other GI tumors can grow much faster). (b) Rendered cross-section diagram of the SERRS-NPs used. (c) Envisioned clinical use: intravenously injected SERRS-NPs specifically accumulate in (pre-) malignant lesions. Given the very high sensitivity of detecting the SERRS-NPs and their specific accumulation via the EPR effect, specific targeting moieties are not required. Thus, this approach may be a universal detection strategy for (pre-) malignant GI tract lesions. Raman-scattered photons are recorded by the Raman endoscope with a rotating mirror, enabling it to acquire two two-dimenstional images of the GI tract lumen: a Raman image that is superimposed on the surface topology of the luminal surface. Inset: The distal end of the circumferentially scanning Raman endoscope includes a rotating mirror that distributes the laser circumferentially along the luminal surface of the colon. As the Raman endoscope is designed to fit into the instrument channel of a clinical white-light endoscope currently used in the clinic, concomitant dual-modal white-light/Raman imaging can be acquired in the same endoscopic session. Data are analyzed and collected by the spectrograph and CCD image sensor, respectively. (d) Illustration of the acquired imaging data. The traditional white-light endoscope can visualize polypoid lesions above a certain size (usually a size of >5−7 mm is required). However, the Raman signals from the SERRS-NP fingerprint enable detection of much smaller lesions. Of note, the SERRS detection does not depend on the lesion morphology or molecular markers, so that even flat lesions (usually missed with conventional white-light endoscopy) can be visualized. This graphic was created by the MSKCC Graphic Department, and permission for use obtained.