

Abstract
Background
Acute respiratory tract infections (ARTIs) are common in children and can involve both upper and lower airways. Many children experience frequent ARTI episodes or recurrent respiratory tract infections (RRTIs) in early life, which creates challenges for paediatricians, primary care physicians, parents and carers of children.
In China, Astragalus (Huang qi), alone or in combination with other herbs, is used by Traditional Chinese Medicine (TCM) practitioners in the form of a water extract, to reduce the risk of ARTIs; it is believed to stimulate the immune system. Better understanding of the therapeutic mechanisms of Astragalus may provide insights into ARTI prevention, and consequently reduced antibiotic use.
Objectives
To assess the effectiveness and safety of oral Astragalus for preventing frequent episodes of acute respiratory tract infections (ARTIs) in children in community settings.
Search methods
We searched the Cochrane Central Register of Controlled Trials (CENTRAL, Issue 12, 2015), MEDLINE (Ovid) (1946 to 31 December 2015), Embase (Elsevier) (1974 to 31 December 2015), AMED (Ovid) (1985 to 31 December 2015), Chinese National Knowledge Infrastructure (CNKI) (1979 to 31 December 2015) and Chinese Scientific Journals full text database (CQVIP) (1989 to 31 December 2015), China Biology Medicine disc (CBM 1976 to 31 December 2015) and Wanfang Data Knowledge Service Platform (WanFang) (1998 to 31 December 2015).
Selection criteria
We included randomised controlled trials (RCTs) comparing oral Astragalus as a sole Chinese herbal preparation with placebo to prevent frequent episodes of ARTIs in children.
Data collection and analysis
We used standard Cochrane methodological procedures for this review. We assessed search results to identify relevant studies. We planned to extract data using standardised forms. Disagreements were to be resolved through discussion. Risk of bias was to be assessed using the Cochrane 'Risk of bias' tool. We planned to use mean difference (MD) or standardised mean difference (SMD) for continuous data and risk ratio (RR) or odds ratio (OR) to analyse dichotomous data, both with 95% confidence intervals (CIs).
Main results
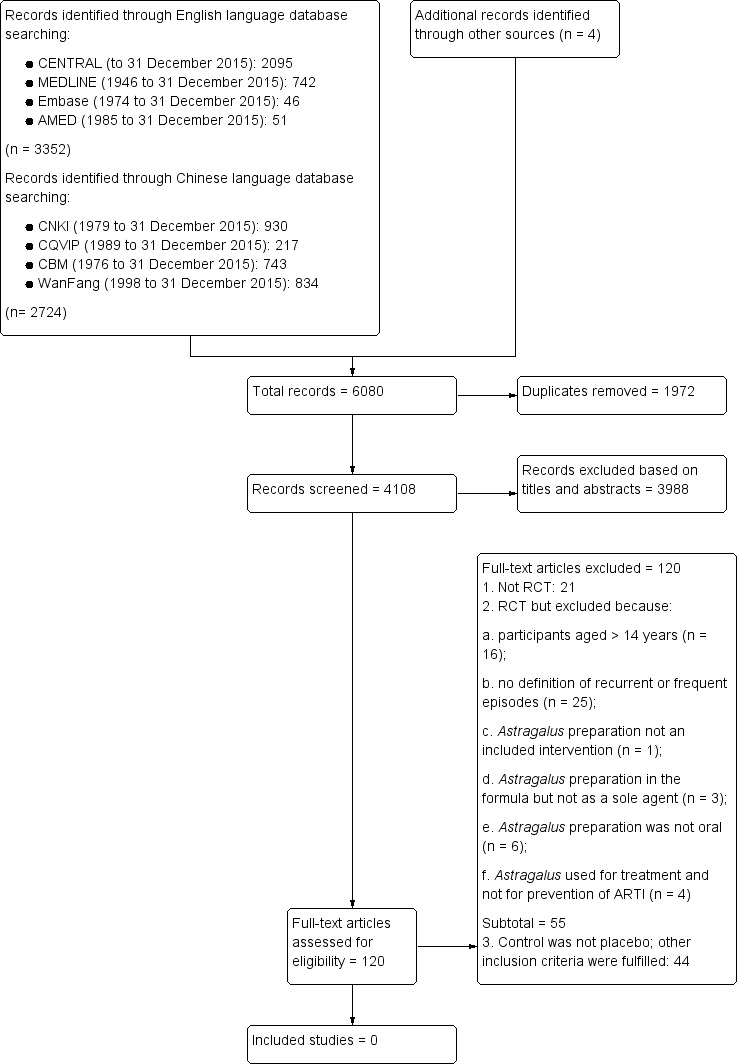
We identified 6080 records: 3352 from English language databases, 2724 from Chinese databases, and four from other sources. Following initial screening and deduplication, we obtained 120 full‐text papers for assessment. Of these, 21 were not RCTs; 55 did not meet the inclusion criteria because: participants were aged over 14 years; definition was not included for recurrent or frequent episodes;Astragalus preparation was not an intervention; Astragalus preparation was in the formula but was not the sole agent; the Astragalus preparation was not administered orally; or Astragalus was used for treatment rather than prevention of ARTI. A further 44 studies were excluded because they were not placebo‐controlled, although other inclusion criteria were fulfilled.
No RCTs met our inclusion criteria.
Authors' conclusions
We found insufficient evidence to enable assessment of the effectiveness and safety of oral Astragalus as a sole intervention to prevent frequent ARTIs in children aged up to 14 years.
Plain language summary
Can oral Astragalus (Huang qi) prevent frequent acute respiratory tract infections in children?
Review question
We assessed evidence for the benefits and harms of oral Astragalus used alone to prevent frequent episodes of acute respiratory infections (ARTIs) in children aged up to 14 years, compared to a dummy treatment. ARTIs include colds, sore throats, laryngitis, influenza, bronchitis and pneumonia.
Background
Many therapies are used to prevent ARTIs, especially in children. Astragalus, is a widely used and available herbal therapy that has been used for thousands of years in China to help prevent ARTIs. It is thought to boost immunity. Almost one in five children experience frequent ARTIs and treatment accounts for up to 75% of all prescribed antibiotics for children. Because most ARTIs are caused by viruses, antibiotics are not effective in treating these illnesses.
Search date
We searched the literature up to 31 December 2015.
Study characteristics
We identified 6080 potentially relevant records. After removing duplicate records, and those that did not meet our inclusion criteria, we obtained 120 full‐text studies. We carefully assessed these studies for possible inclusion. We excluded most studies because: they presented unclear diagnosis criteria; Astragalus preparation was used with other agents; or Astragalus was not compared with a dummy treatment. No studies met our inclusion criteria and so we were unable to analyse any results.
Study funding sources
We could not assess study funding sources.
Key results
We did not find any studies that compared use of oral Astragalus alone with a dummy treatment to prevent frequent episodes of ARTI in children aged up to 14 years. Well‐designed, conducted and reported studies investigating this issue are needed to enable assessment in the future.
Quality of the evidence
We could not assess evidence quality.
Background
Description of the condition
Acute respiratory tract infection (ARTI) is a frequent childhood illness that can involve both upper and lower airways (WHO 1998). ARTIs include common cold, influenza, otitis media, sinusitis, tonsillitis, laryngitis, pharyngitis, bronchitis and pneumonia (CPSCMA 1999). Symptoms include nasal congestion and discharge, sneezing, sore throat, cough, sputum production, shortness of breath, chest pain and fever. Managing ARTIs is a continuing challenge for paediatricians and primary care physicians (CPSCMA 1999; Heikkinen 2003).
On average, children aged under two years experience about six common colds each year (Kvaerner 2000; Leder 2003; Monto 1993; Monto 2002), and healthy children under six years of age may experience up to five respiratory tract infections annually (Griffin 2004). A cohort study observed the history of respiratory infections among children living in urban areas in Germany, and indicated that the mean cumulative number of ARTIs in the first 12 years of life was 21.90 ± 9.00 episodes (Grüber 2008). In high‐income countries, up to 25% of children aged up to one year, and 18% of children between the ages of one and four years, experience frequent ARTI episodes or RRTIs (Bellanti 1997); these are characterised as recurrent airway inflammation caused by infectious agents (Martino 2007).
In China, the definition of 'frequency' is based on age and disease type in accordance with Chinese guidelines (CPSCMA 2008; Table 1). This definition was developed by the respiratory group of the Paediatrics Committee Chinese Medical Association in 1988 (Hu 1988) and updated in 2007 (CPSCMA 2008). All criteria emphasise infection frequency and requires the absence of underlying pathological conditions such as primary or secondary immunodeficiency, cystic fibrosis, airway malformations or immotile‐cilia syndrome.
1. Definition of frequent episodes of respiratory tract infection.
| Age (years) | Recurrent URTI (episodes per year) | Recurrent LRTI (episodes per year) | |
| Recurrent tracheitis or bronchitis | Recurrent pneumonia | ||
| Birth to 2 years of age | 7 | 3 | 2 |
| 2 to 5 years of age (> 2 years and < 5 years) | 6 | 2 | 2 |
| 5 to 14 years of age (> 5 years and < 14 years) | 5 | 2 | 2 |
Abbreviations: LRTI ‐ lower respiratory tract infection; URTI ‐ upper respiratory tract infection
Although factors influencing the aetiology of ARTIs are not always readily identifiable, viral agents are typically responsible for infection. Over 200 different viruses have been associated with ARTIs (Mäkelä 1998). Consequently, vaccination is theoretically an effective way to prevent some ARTIs in children; however, the high frequency of genetic exchange among different strains or subtypes, and high rates of nucleotide substitution, increase the difficulty of developing vaccines that remain persistently effective (Brichacek 1996; O'Brien 1995).
Description of the intervention
There are a number of non‐specific preventative strategies for children with frequent ARTI episodes: general hygiene methods (Martino 2007); physical interventions (Jefferson 2009); administration of vitamin A and zinc (Kartasurya 2012), vitamin C (Hemilä 2013), or vitamin D supplements (Jolliffe 2013); probiotics (Hao 2015); homeopathic medicines (Steinsbekk 2005a; Steinsbekk 2005b); and immunostimulants (Del‐Rio‐Navarro 2012).
Traditional Chinese Medicine (TCM) follows a theoretical and methodological pathway, that differs from Western medicine, to assess cause, diagnosis and treatment. TCM may give new insight into preventive measures for children with frequent ARTI episodes. A main TCM treatment principle is to strengthen the Zheng Qi (a concept of the body's ability to self‐regulate, pathogen resistance and self‐recovery) and eliminate Evil Qi (pathogens). This emphasises the importance of immune system functioning of patients and assumes that strengthening patients' immune systems might prevent and control infections. Certain herbs have been found to affect the distribution and expression of cytokines and their receptors in the immune system (Patwardhan 2005). Astragalus (Huang qi), a herb widely used to strengthen Qi, is widely available in supermarkets in China. For many centuries, Astragalus, alone or in combination with other herbs, has been used by TCM practitioners in the form of a water extract to prevent respiratory infections and to correct a condition called 'Qi deficiency', which typically includes symptoms such as: feelings of weakness, fatigue, apathy, poor appetite and vulnerability to respiratory infections (WHO 2007). In daily clinical TCM practice, there are different routes of administration, such as injection, self‐made oral water extraction, oral liquid and oral granules. The dosage or equivalent of raw Astragalus varies from 10 g/day to 20 g/day and is adjusted according to age. In this review, we focused on all kinds of oral Astragalus preparations, however, we did not include parenteral preparations due to their limited use in children for ARTIs.
How the intervention might work
A study has suggested that Astragalus confers some immune‐stimulating effects, including promoting white blood cell production, accelerating peripheral blood mononuclear cells and cytokine proliferation (Wang 2002). Hou 1981 found that healthy people who received oral Astragalus (8 g per day) for two months experienced significant improvement in the interferon‐inducing ability of blood cells compared with control group participants. Two months after therapy ceased, the interferon‐inducing ability remained significantly higher in the Astragalus group. In another study, Astragalus extract was prescribed to healthy adults for 20 consecutive days and increases were observed in immune parameters such as immunoglobulin (Ig) M, IgE and cyclic adenosine monophosphate (IBMSCAMS 1979). Nie 2009b demonstrated that Astragalus could decrease soluble interleukin‐2 receptor (sIL‐2R) and interleukin‐8 levels, while increasing IgA, IgM and IgG levels in patients experiencing recurrent upper respiratory tract infections (URTIs). Based on these findings, Astragalus may have a biological basis for use in preventing ARTIs in children.
Why it is important to do this review
ARTIs in children impose significant social and financial burdens, particularly when parental time off work is considered, in addition to healthcare costs (Fendrick 2003; Hollinghurst 2008). A third of children in the USA and UK visit primary care physicians for ARTIs or related symptoms each year (Fendrick 2003; Hay 2005). Up to 75% of all antibiotics prescribed for children are for ARTIs, despite their mainly viral aetiology (Doan 2012). Overuse of antibiotics for children in primary care can induce bacterial resistance (Costelloe 2010), which may result in medicalisation of illness whereby patients are more likely to consult when similar symptoms recur – creating a cycle that exacerbates inappropriate use of antibiotics (Andrews 2012). Despite being mostly self‐limiting illnesses, ARTIs remain a common cause of hospitalisation for children in high‐income countries, and a major cause of death in low‐income countries (Culebras 2013). Consequently, there are many social, financial and health reasons for preventing ARTI. Complementary and alternative medicine interventions may provide novel and efficient solutions.
Until the early nineteenth century in China, only TCM was practiced, and consequently it played an important role in healthcare. The popularity of TCM practice is increasing outside of China. According to recent national survey data, 60% to 75% of populations in Singapore, Japan, Taiwan and Korea consult TCM practitioners at least once per year (Cheung 2011). The USA is now the second largest consumer of TCM products (after China) where expenditure in 2010 was USD 7.6 billion (Cheung 2011). This indicates that interest in the potential of herbal treatments is widespread. The potential impact on public health is unknown, but could be substantial, given that herbal products can be purchased at pharmacies, supermarkets and health food stores.
Astragalus is a herb, extensively used both in clinical practice and as a food supplement in daily life in China. Although it is widely used to prevent ARTI in children who experience frequent episodes, no definitive conclusions about its effectiveness have been determined. Safety is an important concern, especially in the context of medications for children. Allergic reactions to Astragalus injections have been reported, and the safety of oral Astragalus preparation remains unclear (Fu 2009; Hu 2008; Xiong 2002).
Six Cochrane Reviews relate to herbal medicine and ARTI (Del‐Rio‐Navarro 2012; Huang 2012b; Jiang 2012; Jiang 2013; Liu 2012; Wu 2007); however, none focus on oral Astragalus for ARTI in children. Four of these reviews focused on the therapeutic effect of Astragalus rather than its prophylactic potential, or in reducing ARTI incidence (Huang 2012b; Jiang 2012; Liu 2012; Wu 2007). Del‐Rio‐Navarro 2012 focused on preventing respiratory tract infection in children, but the intervention was not related to Astragalus.
Our aim was to assess the effectiveness and safety of Astragalus for preventing frequent ARTIs in children in community settings, where Astragalus preparations were used as sole oral agents. We planned to assess ARTI frequency during the study period as the primary outcome.
Objectives
To assess the effectiveness and safety of oral Astragalus for preventing frequent episodes of acute respiratory tract infections (ARTIs) in children in community settings.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials (RCTs) that compared oral Astragalus prescription as a sole Chinese herbal preparation, with placebo, to prevent frequent episodes of acute respiratory tract infection (ARTI) in children. We did not include trials in which Astragalus was one of multiple components in Traditional Chinese Medicine (TCM), such as Yupingfeng, BuZhongYiQiTang, etc.
Types of participants
We included children aged up to 14 years (without chronic disease) who experienced frequent ARTIs and were in community settings.
Frequency was defined in accordance with the current Chinese guideline (CPSCMA 2008; Table 1). We excluded trials that included participants who had asthma, asthmatic bronchitis, allergy and atopy, recurrent spastic laryngitis, tuberculosis, idiopathic pulmonary haemosiderosis, bronchiolitis obliterans with organising pneumonia, eosinophilic pneumonia, sequoiosis or idiopathic interstitial pneumonia.
Types of interventions
Astragalus preparation as the sole agent, administered orally. We excluded formulas with multiple herbs even if they included Astragalus.
Astragalus preparation prescribed alone or as an adjunct for at least four weeks. Adjunctive treatment was only relevant if Astragalus could be isolated as the intervention: concurrent treatment was permitted, such as additional symptomatic treatment, but this needed to follow guidelines, and needed to be the same in both intervention and control groups.
Control group participants received placebo. We excluded trials comparing other active interventions.
No limit on the duration of treatment or follow‐up.
Types of outcome measures
Primary outcomes
The primary outcome was acute respiratory tract infection (ARTI) frequency in children during the study period.
The diagnostic criteria for ARTI were in accordance with the Chinese Paediatrics Antibiotics Application Guideline of Acute Respiratory Tract Infection (CPSCMA 1999). We accepted a broad definition of ARTI, using different specific diagnoses, such as the common cold, influenza, sinusitis, tonsillitis, laryngitis, pharyngitis, bronchitis and pneumonia. ARTI could be either clinically confirmed or self‐reported by parents in studies.
Secondary outcomes
Fever clearance time. This refers to the time from commencing treatment until body temperature returns to normal; self‐reported by parents or reported by clinicians based on formal thermometer readings. We did not include causes of fever other than ARTI in the fever clearance time.
Respiratory symptom clearance time. This refers to the time from commencing treatment until respiratory symptoms resolve, such as cough and sputum reported by parents or clinicians. We planned to evaluate clearance time for each respiratory symptom.
-
Immune system indicator changes referred to changes in:
serum immunoglobulins such as IgG, IgA, or IgM; or
peripheral blood counts; or
percentage of immunocompetent cells such as haematopoietic progenitor cell, or antigen three T lymphocytes.
Adverse events. We planned to report all adverse events during medication administration and frequency of severe adverse events during the study period, including hospitalisations and deaths, and additional medications used in both groups.
Search methods for identification of studies
Electronic searches
We searched the Cochrane Central Register of Controlled Trials (CENTRAL, Issue 12 2015) (Appendix 1), MEDLINE (Ovid) (1946 to 31 December 2015) (Appendix 2), Embase (Elsevier) (Appendix 3) (1974 to 31 December 2015), AMED (Ovid) (1985 to 31 December 2015) (Appendix 4), Chinese National Knowledge Infrastructure (CNKI) (1979 to 31 December 2015) (Appendix 5) and Chinese Scientific Journals full text database (CQVIP) (1989 to 31 December 2015) (Appendix 6), China Biology Medicine disc (CBM 1976 to 31 December 2015) (Appendix 7) and Wanfang Data Knowledge Service Platform (WanFang) (1998 to 31 December 2015) (Appendix 8).
We applied the strategy described in Appendix 2 to search MEDLINE. We combined the MEDLINE search with the Cochrane Highly Sensitive Search Strategy for identifying randomised trials (Lefebvre 2011). We adapted the search strategy to search the other databases. We did not impose language, date or publication limits.
Searching other resources
We searched the trials registries: Current Controlled Trials (www.controlled‐trials.com), National Research Register (www.nihr.ac.uk), Chinese Clinical Trial Register (www.chictr.org), World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) (WHO ICTRP) (www.who.int/ictrp/en), and ClinicalTrials.gov for completed and ongoing trials (www.clinicaltrials.gov). We planned to search the references of included studies. We attempted to identify the grey literature by searching reviews, conference proceedings and academic degree dissertations. Our search identified relevant studies published up to 31 December 2015.
Data collection and analysis
Selection of studies
Two review authors (Zhang L, Liu ZZ) scanned all titles and abstracts found in the searches. We retrieved potentially eligible studies as full‐text articles and the same review authors independently assessed eligibility for inclusion. We resolved disagreements by reaching consensus after rechecking source papers and following discussion with a third review author (Liu XS). We recorded the selection process in sufficient detail to complete a PRISMA flow diagram (Figure 1; Moher 2009), and Characteristics of excluded studies table.
1.
Study flow diagram
Data extraction and management
We designed a data extraction form based on the checklist of items for data collection in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), and as proposed by Cochrane Acute Respiratory Infections. We included information on source, eligibility, study methods, participants, intervention details, outcomes and results. All review authors reviewed the form, which was piloted using a sample of studies, and revised to produce the final version. Two review authors independently extracted data from the included trials. When more than one publication of a study existed, we planned to group reports together and to only use the publication with the most complete data in analyses. We planned to contact trial authors for study details and additional information for incomplete results in the available reports, if needed. We resolved disagreements by discussion, and when necessary, by consulting a third review author.
Assessment of risk of bias in included studies
We planned that two review authors would independently assess risk of bias of each included trial using the Cochrane 'Risk of bias' tool (Higgins 2011). Risk of bias tool domains are:
random sequence generation;
allocation concealment;
blinding of participants and personnel;
blinding of outcome assessment;
incomplete outcome data;
selective outcome reporting; and
other sources of bias.
We planned to assign a quality rating for each domain for all included studies as high, low or unclear risk of bias.
Measures of treatment effect
We were to analyse data using Review Manager 5 (RevMan 2014). We planned to use mean difference (MD) or standardised mean difference (SMD) for continuous data, and risk ratio (RR) or odds ratio (OR) to analyse dichotomous data, both with 95% confidence intervals (CIs).
Unit of analysis issues
The individual participant was to be the unit of analysis. If the unit of analysis was not the same as the unit of randomisation, we were to adjust the outcomes for clustering based on the intra‐cluster correlation as outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). For cross‐over trials, we were only to include data from the first period. For multiple treatment groups, we were to combine all relevant experimental intervention groups of the study into a single test group and combine all relevant control intervention groups into a single control group. We were to subject different units of analysis to a sensitivity analysis.
Dealing with missing data
We planned to obtain additional information as required by contacting study authors and to include information obtained in the review. We were to investigate attrition rates. Analyses were to be based on an intention‐to‐treat approach. We were to impute missing data. For missing dichotomous outcomes, we were to assume that they were ineffective in both treatment and control groups. For missing continuous outcomes, we were to try to obtain participant data by contacting authors and to impute missing data using the last observation carried forward approach (Higgins 2011). If we failed to obtain additional data, we were to perform an available‐case analysis.
Assessment of heterogeneity
We planned to assess heterogeneity among trials in two steps. First, we were to assess face value heterogeneity by comparing trial populations, settings and methods. Secondly, we were to assess statistical heterogeneity using a Chi² test and the I² statistic (Higgins 2003). An I² statistic value of 25%, 50% and 75% refers to low, medium and high levels of heterogeneity, respectively. If heterogeneity were to be present, we would have examined the methodological and clinical characteristics of the included trials to explore the possible causes. We were to then conduct subgroup analyses and summarise our findings. If we had failed to identify the possible causes of heterogeneity, we were not to perform a meta‐analysis. Instead, we were to use a qualitative approach to present the results.
Assessment of reporting biases
We planned to construct funnel plots if more than 10 studies were included to assess risk of publication bias. Because factors other than publication bias (such as study quality) might lead to an asymmetrical funnel plot, we were to perform Egger's test using STATA 11.0 software (StataCorp, USA) (Stata 2009), to detect funnel plot asymmetry.
Data synthesis
We planned to use a random‐effects model to synthesise all data, regardless of heterogeneity among the studies. We planned to test for publication bias by constructing a funnel plot or other corrective analytical methods, depending on numbers of included studies.
GRADE and 'Summary of findings' table
We planned to create a 'Summary of findings' table using the following outcomes: ARTI frequency, fever clearance time, respiratory symptom clearance time, effectiveness rate and adverse events. We were to use the GRADE approach to rate the quality of the body of evidence based on five considerations: study limitations, consistency of effect, imprecision, indirectness and publication bias (Atkins 2004). We planned to use methods and recommendations introduced in Section 8.5 and Chapter 12 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), and the GRADE Handbook (www.guidelinedevelopment.org/handbook), using GRADEpro GDT software (GRADEpro GDT 2014). We planned to justify all decisions to downgrade or upgrade the quality of studies in footnotes, and to make comments to aid readers' understanding of the review, where necessary. We were to use Review Manager 5 for all calculations (RevMan 2014).
Subgroup analysis and investigation of heterogeneity
We planned to perform subgroup analyses based on interventions and treatment duration. Clinical heterogeneity among interventions could be related to the different doses and types of Astragalus preparations, such as decoction of dried Astragalus, powder capsule of dried Astragalus, capsule of Astragalus extracts, etc. If the onset of clinical effect and how long the effect would last were still unclear, we were to perform a subgroup analysis by stratifying by treatment duration and time of follow‐up to investigate the appropriate duration of treatment.
Sensitivity analysis
We planned to perform a sensitivity analysis by stratifying studies at low, high and unclear risk of bias to explore the impact of risk of bias on the pooled estimate, and to investigate potential methodological heterogeneity. We were also to perform a sensitivity analysis with the available data to assess the impact of imputation. Analyses were not possible because no studies were found to be eligible for inclusion.
Results
Description of studies
Results of the search
Searches identified a total of 6080 records: 3352 from English language databases, 2724 from Chinese databases, and four from other sources (Figure 1). After removing 1972 duplicate records, we assessed the remaining 4108, and excluded 3988 records based on titles and abstracts. We retrieved 120 full‐text records and assessed them for inclusion.
Included studies
We did not identify any studies that met our inclusion criteria for this review.
Excluded studies
We excluded 120 studies, of these, 21 studies were not RCTs. We excluded a further 55 records because: participants were aged over 14 years (n = 16); no definition was included for recurrent or frequent episodes (n = 25); Astragalus preparation was not an intervention (n = 1); Astragalus preparation was in the formula, but not a sole agent (n = 3); Astragalus preparation was not oral (n = 6); and Astragalus was used for treatment rather than ARTI prevention (n = 4). We excluded 44 records because the control was not a placebo, although other inclusion criteria were fulfilled.
We identified no ongoing studies.
Risk of bias in included studies
We were unable to conduct a 'Risk of bias' assessment because no studies were identified that met our inclusion criteria.
Effects of interventions
We did not identify any studies that met our inclusion criteria for this review.
Discussion
Frequent acute respiratory tract infection (ARTI) episodes are common during childhood. Caring for children with ARTIs consumes considerable medical, parental and carer resources. In China, Astragalus (Huang qi) has traditionally been used to prevent ARTI. Although Astragalus is widely used and widely available in China, its effectiveness and safety have not been evaluated systematically in the context of ARTI prevention.
We aimed to assess the effectiveness and safety of oralAstragalus for preventing frequent ARTI episodes among children in community settings. However, we did not identify any studies that met our inclusion criteria. We found a gap in the evidence: well‐designed and well‐conducted randomised controlled trials (RCTs) investigating oral Astragalus to prevent frequent ARTI in children are needed to inform assessment of safety and efficacy.
A limitation of this review is that definitions of ARTI and episode frequency were not well defined. We did not find a definition for 'acute', nor whether there were differences in how episodes of upper and lower airway infections were counted, nor length of intervals between episodes. This is problematic because it can result in over‐ or underestimation of numbers of ARTI episodes reported.
Another limitation was that ARTI frequency in children was the only primary outcome; ARTI severity and duration are also very important to evaluate the effect of prevention. Instruments such as the Wisconsin Upper Respiratory Symptom Survey for Kids (WURSS‐K) and the Canadian Acute Respiratory Infection and Flu Scale (CARFIS) have been developed to enable evaluation of severity and duration of RTIs among children (Fischer 2014; Jacobs 2000; Shepperd 2004; www.fammed.wisc.edu/wurss). WURSS‐K is a self‐report quality of life instrument for children, designed to assess the negative impact of acute URTI. WURSS‐K is completed by children and focuses on the impact of quality of life; CARFIS is used by parents and focuses on ARTI severity. Both instruments could be used in future studies looking at the preventive effect of Astragalus for children with frequent episodes of ARTI.
We did not capture the exact ingredients of the intervention in the inclusion criteria. As a natural product, the method of plant extraction and whether the product is standardised will determine the proportion of constituents and dose, thus influencing effectiveness and safety of oral Astragalus preparations. The aspects of standardisation of oral Astragalus preparation should be considered, such as which part of the plant was used, species, age, size, growing conditions, medicinal preparations/extract methods, proportion of constituents, and storage methods of Astragalus (Natural Medicines 2016), all of which have implication for future research.
Summary of main results
We did not identify any RCTs that investigated the effectiveness and safety of oralAstragalus compared with placebo to prevent frequent episodes of ARTIs in children.
Overall completeness and applicability of evidence
We did not identify any RCTs for inclusion.
Quality of the evidence
We did not identify any RCTs for inclusion.
Potential biases in the review process
We found no studies that met our inclusion criteria; our search strategies were comprehensive, and It is unlikely that we missed potentially eligible studies. We included two additional Chinese language databases (CBM and Wanfang) than planned in the protocol, to extend our search and capture all potential studies.
We planned to include only placebo‐controlled studies and ARTI was to be clinically confirmed or self‐reported by patients. Since patient‐reported occurrence of ARTI is subjective, placebo was nominated as the only control that would avoid expectation and measurement bias. We did not find any studies that were placebo‐controlled, and surmised that difficulties in obtaining ethics approval, especially in trials for children, limited this objective. Obtaining informed consent could be challenging because of reluctance by parents and carers to consent to children's participation in the knowledge that they may be allocated to the placebo arm. Of the 44 studies that fulfilled all inclusion criteria, except being placebo‐controlled, most were add‐on design studies (Huang qi + concurrent treatment versus concurrent treatment). Further evaluation of the add‐on effect might be possible by reviewing these studies.
Agreements and disagreements with other studies or reviews
We found no studies or systematic reviews that investigated the effectiveness and safety of oral Astragalus in preventing frequent ARTIs in children. Current evidence is diverse in study design but all support oral Astragalus in preventing ARTIs in children, such as the 44 non‐placebo‐controlled RCTs excluded from this review, and a mini systematic review embedded in a case report of Huang qi (Astragalus) granules in upper respiratory tract infection (URTI) prevention in children with nephrotic syndrome (Zou 2013).
Authors' conclusions
Implications for practice.
Although oral Astragalus (Huang qi) has been used to prevent acute respiratory tract infection (ARTI) for many years, no placebo‐controlled randomised controlled trial (RCT) evidence is available to help guide practice, family decisions about care, or healthcare policy in relation to oral Astragalus for preventing frequent ARTI episodes among children in community settings.
Implications for research.
Large, well‐designed RCTs investigating the safety and efficacy of oral Astragalus to prevent frequent ARTIs in children are needed. In future studies, add‐on placebo designs (Huang qi + concurrent treatment versus placebo + concurrent treatment) may help to prevent children not receiving any treatment. Consideration should be taken to include:
the use of WRUSS‐K and CARFIS instruments to evaluate quality of life and disease severity, rather than ARTI frequency;
a clear definition of 'acute' in relation to respiratory tract infection, and stating the interval between respiratory tract infection episodes used to define separate episodes;
standardising ingredients and dosage of oralAstragalus used in children and ensuring the placebo is adequately masked to replicate the smell and taste of oral Astralagus;
systemic markers of immune function to see the potential mechanism; and
if a placebo is not applicable, pragmatic research in real world practice to evaluate the preventive and safety effects of oral Astragalus in children with frequent ARTIs.
Acknowledgements
We thank Cochrane Acute Respiratory Infections for their assistance with this Cochrane Review. The authors would also like to thank Suzanne Cunliffe, Lily Lai, George Lewith, David King, Viviana Rodriguez and Susan Smith for their comments on the protocol; and Ann Fonfa, Eleana Villanueva, George Lewith, Mio Hu, Treasure McGuire, Viviana Rodriguez and Susan Smith for their comments on the review. We would also like to thank Oliver Dyar for checking grammar and commenting on this review. We acknowledge Jiasheng Huang and Jiawei He for their management and editing of text and data in this review. We thank Liz Dooley, Kerry Dwan, Ann Jones and other editors for their editing work on this review.
Appendices
Appendix 1. CENTRAL search strategy
1 MeSH descriptor: [Astragalus Plant] explode all trees
2 Astraga*
3 MeSH descriptor: [Astragalus membranaceus] explode all trees
4 Huang Qi
5 Huangqi
6 Milkvetch
7 #1 OR #2 OR #3 OR #4 OR #5 OR #6
8 MeSH descriptor: [Drugs, Chinese Herbal] explode all trees
9 MeSH descriptor: [Medicine, East Asian Traditional] explode all trees
10 MeSH descriptor: [Phytotherapy] explode all trees
11 MeSH descriptor: [Herbal Medicine] explode all trees
12 MeSH descriptor: [Plants, Medicinal] explode all trees
13 MeSH descriptor: [Plant Preparations] explode all trees
14 (Chinese) AND ((Prescription*) OR (Preparation*) OR (extract*) OR (herb*) OR (medicin*) OR (drug*) OR (plant*) OR (botanical*))
15 #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14
16 MeSH descriptor: [Respiratory Tract Infections] explode all trees
17 (acute OR upper OR lower) AND ((respiratory infection*) OR (respiratory tract infection*))
18 (pharyngit*) OR (tracheit*) OR (bronchit*) OR (pneumon*)
19 (common cold*) OR (coryza) OR (influenza*) OR (flu) OR (otitis media*) OR (sinusit*) OR (tonsillit*) OR (laryngit*) OR (pharyngit*) OR (bronchit*) OR (pneumon*) OR (sore throat*) OR (sneez*) OR (cough*) OR ((nasal or nose) AND (congest* or discharg*))
20 #16 OR #17 OR #18 OR #19
21 #15 and #20
22 #7 OR #21
Appendix 2. MEDLINE (Ovid) search strategy
1 exp Astragalus Plant/
2 Astragal*.mp.
3 "A. membranaceus".mp.
4 "huang qi".mp.
5 huangqi.mp.
6 vetch.mp.
7 or/1‐6
8 Drugs, Chinese Herbal/
9 exp Medicine, East Asian Traditional/
10 Phytotherapy/
11 Herbal Medicine/
12 Plants, Medicinal/
13 plant preparations/ or plant extracts/
14 (chinese adj5 (herb* or medicin* or drug* or plant* or botanical*)).mp.
15 or/8‐14
16 exp Respiratory Tract Infections/
17 ((acute or upper or lower) adj2 (respiratory infection* or respiratory tract infection*)).mp.
18 (pharyngit* or tracheit* or bronchit* or pneumon*).mp.
19 (common cold* or coryza or influenza* or flu or otitis media* or sinusit* or tonsillit* or laryngit* or pharyngit* or bronchit* or pneumon* or sore throat* or sneez* or cough* or ((nasal or nose) adj2 (congest* or discharg*))).mp.
20 or/16‐19
21 15 and 20
22 7 or 21
23 randomized controlled trial.pt.
24 controlled clinical trial.pt.
25 randomized.ab.
26 placebo.ab.
27 clinical trials as topic.sh.
28 randomly.ab.
29 trial.ti.
30 or/23‐29
31 exp animals/ not humans.sh.
32 30 not 31
33 22 and 32
Appendix 3. Embase (Elsevier) search strategy
1 Astragalus (plant)'/exp
2 Astragal*
3 "A. membranaceus"
4 "huang qi"
5 "huangqi"
6 vetch
7 #1 OR #2 OR #3 OR #4 OR #5 OR #6
8 Chinese herb'/exp
9 oriental medicine'/exp
10 phytotherapy'/exp
11 'herbal medicine'/exp
12 medicinal plant'/exp
13 ('plant medicinal product'/exp) or ('plant extract'/exp)
14 chinese NEXT/5 (herb* or medicin* or drug* or plant* or botanical*)
15 #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14
16 respiratory tract infection'/exp
17 respiratory AND infection* OR (respiratory AND tract AND infection*)
18 pharyngit* or tracheit* or bronchit* or pneumon*
19 common cold* or coryza or influenza* or flu or otitis media* or sinusit* or tonsillit* or laryngit* or pharyngit* or bronchit* or pneumon* or sore throat* or sneez* or cough* or ((nasal or nose) NEXT/2 (congest* or discharg*))
20 #16 AND #17 AND #18 AND #19
21 #15 and #20
22 #7 or #21
23 [randomized controlled trial]/lim
24 [controlled clinical trial]/lim
25 randomized:ab
26 placebo:ab
27 clinical trial (topic)'/exp
28 randomly:ab
29 trial:ti
30 #23 OR #24 OR #25 OR #26 OR #27 OR #28 OR #29
31 animal'/exp not 'human'/exp
32 #30 not #31
33 #22 and #32
Appendix 4. AMED (Ovid) search strategy
1 exp Astragalus Plant/
2 Astragal*.mp.
3 "A. membranaceus".mp.
4 "huang qi".mp.
5 huangqi.mp.
6 vetch.mp.
7 or/1‐6
8 Drugs, Chinese Herbal/
9 exp Medicine, East Asian Traditional/
10 Phytotherapy/
11 Herbal Medicine/
12 Plants, Medicinal/
13 plant preparations/ or plant extracts/
14 (chinese adj5 (herb* or medicin* or drug* or plant* or botanical*)).mp.
15 or/8‐14
16 exp Respiratory Tract Infections/
17 ((acute or upper or lower) adj2 (respiratory infection* or respiratory tract infection*)).mp.
18 (pharyngit* or tracheit* or bronchit* or pneumon*).mp.
19 (common cold* or coryza or influenza* or flu or otitis media* or sinusit* or tonsillit* or laryngit* or pharyngit* or bronchit* or pneumon* or sore throat* or sneez* or cough* or ((nasal or nose) adj2 (congest* or discharg*))).mp.
20 or/16‐19
21 15 and 20
22 7 or 21
23 randomized controlled trial.pt.
24 controlled clinical trial.pt.
25 randomized.ab.
26 placebo.ab.
27 clinical trials as topic.sh.
28 randomly.ab.
29 trial.ti.
30 or/23‐29
31 exp animals/ not humans.sh.
32 30 not 31
33 22 and 32
Appendix 5. CNKI search strategy
SU=("呼吸道感染"+"感冒"+"流感"+"喉炎"+"咽炎"+"肺炎"+"肺部感染"+"鼻炎"+"鼻窦炎"+"扁桃体炎"+"气管炎"+"结核"+"百日咳") AND SU=("黄芪"+"北芪"+"黄耆"+"北耆") AND SU=("临床观察"+"临床评估"+"临床试验"+"临床效果"+"临床研究"+"疗效"+"评价研究"+"前瞻性"+"随访"+"对比研究"+"多中心"+"随机"+"对照"+"病例报告"+"病例研究"+"病例分析"+"病例报道")
Appendix 6. CQVIP search strategy
题名或关键词
M(题名或关键词)=(呼吸道感染+感冒+流感+喉炎+咽炎+肺炎+肺部感染+鼻炎+鼻窦炎+扁桃体炎+气管炎+结核+百日咳)*(黄芪+北芪+黄耆+北耆)*(临床观察+临床评估+临床试验+临床效果+临床研究+疗效+评价研究+前瞻性+随访+对比研究+多中心+随机+对照+病例报告+病例研究+病例分析+病例报道)
文摘
R(文摘)=(呼吸道感染+感冒+流感+喉炎+咽炎+肺炎+肺部感染+鼻炎+鼻窦炎+扁桃体炎+气管炎+结核+百日咳)*(黄芪+北芪+黄耆+北耆)*(临床观察+临床评估+临床试验+临床效果+临床研究+疗效+评价研究+前瞻性+随访+对比研究+多中心+随机+对照+病例报告+病例研究+病例分析+病例报道)
Appendix 7. CBM search strategy
#1:(((((("呼吸道感染"[常用字段:智能]) OR "感冒"[常用字段:智能]) OR "流感"[常用字段:智能]) OR "喉炎"[常用字段:智能]) OR "咽炎"[常用字段:智能]) OR "肺炎"[常用字段:智能]) OR "肺部感染"[常用字段:智能]
#2:((((("鼻炎"[常用字段:智能]) OR "鼻窦炎"[常用字段:智能]) OR "扁桃体炎"[常用字段:智能]) OR "气管炎"[常用字段:智能]) OR "结核"[常用字段:智能]) OR "百日咳"[常用字段:智能]
#3:(#2) OR (#1)
#4:((("黄芪"[常用字段:智能]) OR "北芪"[常用字段:智能]) OR "黄耆"[常用字段:智能]) OR "北耆"[常用字段:智能]
#5:((((((("临床观察"[常用字段:智能]) OR "临床评估"[常用字段:智能]) OR "临床试验"[常用字段:智能]) OR "临床效果"[常用字段:智能]) OR "临床研究"[常用字段:智能]) OR "疗效"[常用字段:智能]) OR "评价研究"[常用字段:智能]) OR "前瞻性"[常用字段:智能]
#6:(((((((("随访"[常用字段:智能]) OR "对比研究"[常用字段:智能]) OR "多中心"[常用字段:智能]) OR "随机"[常用字段:智能]) OR "对照"[常用字段:智能]) OR "病例报告"[常用字段:智能]) OR "病例研究"[常用字段:智能]) OR "病例分析"[常用字段:智能]) OR "病例报道"[常用字段:智能]
#7:(#6) OR (#5)
#8:(#7) AND (#4) AND (#3)
Appendix 8. Wanfang search strategy
主题词
主题:("呼吸道感染"+"感冒"+"流感"+"喉炎"+"咽炎"+"肺炎"+"肺部感染"+"鼻炎"+"鼻窦炎"+"扁桃体炎"+"气管炎"+"结核"+"百日咳") AND 主题:("黄芪"+"北芪"+"黄耆"+"北耆") AND 主题:("临床观察"+"临床评估"+"临床试验"+"临床效果"+"临床研究"+"疗效"+"评价研究"+"前瞻性"+"随访"+"对比研究"+"多中心"+"随机"+"对照"+"病例报告"+"病例研究"+"病例分析"+"病例报道")
Characteristics of studies
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Bai 2005 | Not placebo‐controlled |
| Chen 1996 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; participants were aged over 14 years; intervention aimed for treatment, not prevention |
| Chen 2001 | RTIs investigated, but not defined as recurrent or frequent episodes; not oral Astragalus preparation |
| Chen 2003 | Not placebo‐controlled |
| Chen 2008a | RTIs investigated, but not defined as recurrent or frequent episodes; non‐RCT |
| Chen 2008b | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; intervention aimed for treatment, not prevention |
| Chen 2009 | Not placebo‐controlled |
| Chen 2010 | Not oral Astragalus preparation |
| Cui 2010 | RTIs investigated, but not defined as recurrent or frequent episodes; not oral Astragalus preparation; intervention aimed for treatment, not prevention |
| Deng 2000 | Not placebo‐controlled |
| Deng 2004 | Not placebo‐controlled |
| Du 1992 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; intervention aimed for treatment, not prevention |
| Feng 2001 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; participants were aged over 14 years; intervention aimed for treatment, not prevention |
| Feng 2009 | RTIs investigated, but not defined as recurrent or frequent episodes |
| Gao 1993 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; participants were aged over 14 years; intervention aimed for treatment, not prevention |
| Gao 2007 | Not placebo‐controlled |
| Guan 2011 | Not placebo‐controlled |
| Guo 2008 | Non‐RCT |
| Han 2000 | Not placebo‐controlled |
| Han 2011 | Not placebo‐controlled |
| He 2014 | Non‐RCT |
| Hu 1984 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; intervention aimed for treatment, not prevention |
| Huang 2000 | Not placebo‐controlled |
| Huang 2004a | No data; Only for treatment not for prevention |
| Huang 2004b | Not placebo‐controlled |
| Huang 2012a | Not oral Astragalus preparation; intervention aimed for treatment, not prevention |
| Huo 1994 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; intervention aimed for treatment, not prevention |
| Ikeda 1988 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; non‐RCT; intervention aimed for treatment, not prevention |
| Ji 1996 | RTIs investigated, but not defined as recurrent or frequent episodes; Astragalus preparation not administered as sole agent; participants were aged over 14 years; intervention aimed for treatment, not prevention |
| Jin 1997 | Not oral Astragalus preparation; intervention aimed for treatment, not prevention |
| Jin 2009 | Astragalus preparation not administered as sole agent; intervention aimed for treatment, not prevention |
| Jin 2013 | Not placebo‐controlled |
| Kang 1992 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; intervention aimed for treatment, not prevention |
| Ke 2005 | Non‐RCT |
| Li 1989 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation;participants were aged over 14 years; intervention aimed for treatment, not prevention |
| Li 1994a | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; non‐RCT; intervention aimed for treatment, not prevention |
| Li 1994b | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; intervention aimed for treatment, not prevention |
| Li 1999 | RTIs investigated, but not defined as recurrent or frequent episodes; intervention aimed for treatment, not prevention |
| Li 2001 | RTIs investigated, but not defined as recurrent or frequent episodes; Astragalus preparation not administered as sole agent; participants were aged over 14 years; intervention aimed for treatment, not prevention |
| Li 2002 | Not placebo‐controlled |
| Li 2004 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; intervention aimed for treatment, not prevention |
| Li 2008 | Not placebo‐controlled |
| Li 2013 | Not placebo‐controlled |
| Li 2015 | Not oral Astragalus preparation; intervention aimed for treatment, not prevention |
| Lin 2001 | Not placebo‐controlled |
| Lin 2003 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; intervention aimed for treatment, not prevention |
| Lin 2012 | Not placebo‐controlled |
| Liu 1992 | Non‐RCT; intervention aimed for treatment, not prevention |
| Liu 2002 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; intervention aimed for treatment, not prevention |
| Liu 2003 | Not placebo‐controlled |
| Liu 2004a | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; participants were aged over 14 years; intervention aimed for treatment, not prevention |
| Liu 2004b | RTIs investigated, but not defined as recurrent or frequent episodes; not oral Astragalus preparation; intervention aimed for treatment, not prevention |
| Liu 2004c | Not placebo‐controlled |
| Liu 2010 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; intervention aimed for treatment, not prevention |
| Liu 2011 | Not placebo‐controlled |
| Liu 2014 | RTIs investigated, but not defined as recurrent or frequent episodes; not oral Astragalus preparation; intervention aimed for treatment, not prevention |
| Lu 2006 | RTIs investigated, but not defined as recurrent or frequent episodes; non‐RCT |
| Lu 2009 | Not placebo‐controlled |
| Lu 2012 | RTIs investigated, but not defined as recurrent or frequent episodes; Astragalus preparation not administered as sole agent; participants were aged over 14 years; intervention aimed for treatment, not prevention |
| Lu 2013 | Not placebo‐controlled |
| Luan 2001 | Not placebo‐controlled |
| Luo 1994 | RTIs investigated, but not defined as recurrent or frequent episodes; Astragalus preparation not administered as sole agent; participants were aged over 14 years |
| Luo 2013 | Not placebo‐controlled |
| Nie 2009a | Not oral Astragalus preparation |
| Peng 1991 | RTIs investigated, but not defined as recurrent or frequent episodes; Astragalus preparation not administered as sole agent; participants were aged over 14 years; intervention aimed for treatment, not prevention |
| Peng 2006 | Intervention aimed for treatment, not prevention |
| Peng 2012 | RTIs investigated, but not defined as recurrent or frequent episodes; intervention aimed for treatment, not prevention |
| Qi 2000 | RTIs investigated, but not defined as recurrent or frequent episodes; Astragalus preparation not administered as sole agent; participants were aged over 14 years; intervention aimed for treatment, not prevention |
| Qiu 2004 | Non‐RCT |
| Ruan 2013 | Not placebo‐controlled |
| Shen 1988 | Non‐RCT; intervention aimed for treatment, not prevention |
| Sheng 2010 | Not placebo‐controlled |
| Shi 2006 | RTIs investigated, but not defined as recurrent or frequent episodes; participants were aged over 14 years |
| Song 2008 | Not placebo‐controlled |
| Su 1988 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; intervention aimed for treatment, not prevention |
| Su 1994 | RTIs investigated, but not defined as recurrent or frequent episodes; Astragalus preparation not administered as sole agent; intervention aimed for treatment, not prevention |
| Wang 1997 | Non‐RCT; Astragalus preparation not administered as sole agent |
| Wang 2001 | Not placebo‐controlled |
| Wang 2008a | RTIs investigated, but not defined as recurrent or frequent episodes; non‐RCT |
| Wang 2008b | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; intervention aimed for treatment, not prevention |
| Wang 2009 | Not placebo‐controlled |
| Wang 2010 | Only for treatment not for prevention |
| Wang 2013 | Not placebo‐controlled |
| Wang 2014 | Not placebo‐controlled |
| Wang 2015 | Not placebo‐controlled |
| Wei 2000 | Not oral Astragalus preparation |
| Wu 1996 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; participants were aged over 14 years; intervention aimed for treatment, not prevention |
| Wu 2003 | Non‐RCT |
| Wu 2011 | RTIs investigated, but not defined as recurrent or frequent episodes; non‐RCT; intervention aimed for treatment, not prevention |
| Xia 2007 | RTIs investigated, but not defined as recurrent or frequent episodes; intervention aimed for treatment, not prevention |
| Xiao 1988 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; intervention aimed for treatment, not prevention |
| Xiao 2014 | Not placebo‐controlled |
| Xie 2015 | Intervention aimed for treatment, not prevention |
| Xu 1994 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; participants were aged over 14 years; intervention aimed for treatment, not prevention |
| Xu 1997 | Astragalus preparation not administered as sole agent |
| Xu 2004 | Non‐RCT; not oral Astragalus preparation |
| Yang 1992 | RTIs investigated, but not defined as recurrent or frequent episodes; Astragalus preparation not administered as sole agent; participants were aged over 14 years; intervention aimed for treatment, not prevention |
| Yang 1998 | Not placebo‐controlled |
| Yang 2001 | Not placebo‐controlled |
| Yang 2008 | Non‐RCT |
| Yu 2005 | Non‐RCT |
| Zeng 2009 | RTIs investigated, but not defined as recurrent or frequent episodes |
| Zhang 1995 | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; intervention aimed for treatment, not prevention |
| Zhang 1999 | Not placebo‐controlled |
| Zhang 2000 | Intervention aimed for treatment, not prevention |
| Zhang 2012 | Not placebo‐controlled |
| Zhang 2013 | Not placebo‐controlled |
| Zhao 2000a | RTIs investigated, but not defined as recurrent or frequent episodes; not Astragalus preparation; participants were aged over 14 years; intervention aimed for treatment, not prevention |
| Zhao 2000b | Non‐RCT |
| Zhao 2003 | Not placebo‐controlled |
| Zhao 2007 | Not oral Astragalus preparation |
| Zheng 2013 | RTIs investigated, but not defined as recurrent or frequent episodes; not oral Astragalus preparation; intervention aimed for treatment, not prevention |
| Zhong 2012 | Not placebo‐controlled |
| Zhou 2005 | RTIs investigated, but not defined as recurrent or frequent episodes; non‐RCT |
| Zhou 2009a | Not placebo‐controlled |
| Zhou 2009b | Non‐RCT |
| Zhou 2012 | Not placebo‐controlled |
| Zhu 2014a | Astragalus preparation not administered as sole agent |
| Zhu 2014b | RTIs investigated, but not defined as recurrent or frequent episodes; Astragalus preparation not administered as sole agent; non‐RCT |
| Zou 2000 | Not placebo‐controlled |
Differences between protocol and review
We added two Chinese language databases (CBM and Wanfang) to extend our search to capture all potential studies. Planned analyses could not be conducted because no studies met our inclusion criteria.
Contributions of authors
Guobin Su and Xusheng Liu drafted the review. Xiankun Chen and Zhuangzhu Liu developed and ran the search strategy. Lihong Yang and La Zhang independently extracted data and obtained copies of studies. Xindong Qin and Jueyao Liang entered data into Review Manager 5. Zhuangzhu Liu and Zehuai Wen assessed studies for inclusion and planned to assess risk of bias. Xinfeng Guo was the third review author who planned to select which studies to include when disagreements existed. Cecilia Stålsby Lundborg contributed to the development of data analysis strategies and acted as a general adviser. Xusheng Liu acted as guarantor for the review and planned to perform data analysis. All authors provided comments on this review and approved the final version.
Sources of support
Internal sources
-
Guangdong Provincial Hospital of Chinese Medicine, China.
This review is supported by a research grant from a project between the Guangdong Provincial Hospital of Chinese Medicine in China and the Department of Public Health Sciences, Karolinska Institutet in Sweden.
External sources
-
Provincial Administration of Traditional Chinese Medicine, Guangdong Province, China.
This review is supported by a research fund for developing Guangdong Province as a competitive province of traditional Chinese medicine (NO. 20151245) by the Provincial Administration of Traditional Chinese Medicine, Guangdong Province, China.
-
China Scholarship Council, China.
Guobin Su is supported by China Scholarship Council. (NO. 201508440214)
Declarations of interest
Guobin Su: none known. Xiankun Chen: none known. Zhuangzhu Liu: none known. Lihong Yang: none known. La Zhang: none known. Cecilia Stålsby Lundborg: none known. Zehuai Wen: none known. Xinfeng Guo: none known. Xindong Qin: none known. Jueyao Liang: none known. Xusheng Liu: none known.
New
References
References to studies excluded from this review
Bai 2005 {published data only}
- Bai SX, Ji YY, Tang XF, Lu GQ, Li L. Observation in the curative effect of Astragalus decoction on children with recurrent respiratory tract infection. Chinese Journal for Clinicians 2005;33(3):28‐9. [Google Scholar]
Chen 1996 {published data only}
- Chen, M. Therapy of combining traditional Chinese and Western medicine for chronic bronchitis acute episodes in 45 cases. Shandong Journal of Traditional Chinese Medicine 1996;15(3):120‐1. [Google Scholar]
Chen 2001 {published data only}
- Chen FL. 36 cases of paediatric asthmatic bronchitis treated with traditional Chinese medicine and Western Medicine. Chinese Journal of Rural Medicine and Pharmacy 2001;8(11):28. [Google Scholar]
Chen 2003 {published data only}
- Chen J, Chen H. Clinical observation of Astragalus granule in treatment of children with recurrent respiratory tract infection. Liaoning Journal of Traditional Chinese Medicine 2003;30(3):204‐5. [Google Scholar]
Chen 2008a {published data only}
- Chen J, Chen SQ. Clinical observation of Huangqi granule preventing infection in children with nephropathy syndrome. Chinese Journal of Integrated Traditional and Western Medicine 2008;28(3):467‐9. [Google Scholar]
Chen 2008b {published data only}
- Chen WJ. Integrated traditional and western medicine for treating children with acute purulent tonsillitis in 46 cases. Chinese Journal of Information on Traditional Chinese Medicine 2008;15(2):61‐2. [Google Scholar]
Chen 2009 {published data only}
- Chen CB, Wang M, Wang XP. Clinical observation of Huaiqihuang granule in the treatment of children with recurrent respiratory tract infection. Modern Journal of Integrated Chinese Traditional and Western Medicine 2009;18(32):3958‐9. [Google Scholar]
Chen 2010 {published data only}
- Chen ZD. Curative effect of the adjunctive therapy of Astragalus injection combined with iron zinc calcium amino acid in recurrent respiratory tract infection. China Modern Medicine 2010;17(35):62. [Google Scholar]
Cui 2010 {published data only}
- Cui Y, Mao JL. Clinical analysis of 55 cases of capillary bronchitis treated by Astragalus injection. Qinghai Medical Journal 2010;40(12):62‐3. [Google Scholar]
Deng 2000 {published data only}
- Deng GN, Zhao M. Study on infection and immune function of the triple prevention of recurrent respiratory tract infection. Medical Journal of Communications 2000;14(2):135. [Google Scholar]
Deng 2004 {published data only}
- Deng Y, Fan Y, Huang WH, Li LJ. Clinical observation on Huangqi and Heluo oral liquid in the treatment of children with recurrent respiratory tract infection. Chinese Journal of Integrated Traditional and Western Medicine 2004;24(6):552‐3. [PubMed] [Google Scholar]
Du 1992 {published data only}
- Du YJ. Treating 43 infantile pneumonia cases with Pneumonia mixture. Liaoning Journal of Traditional Chinese Medicine 1992;11:32‐3. [Google Scholar]
Feng 2001 {published data only}
- Feng YL, Liu CT, Li YH. Randomized controlled study on the sequential therapy in the treatment of lower respiratory tract infection. Chinese Journal of Pharmacoepidemiology 2001;10(2):57‐8. [Google Scholar]
Feng 2009 {published data only}
- Feng YZ, Li Y, Pan HM, Dong Y. Clinical study of huanerjin's effect on repeated respiratory tract infection in bronchial asthma children. Chinese Journal of Asthma 2009;3(2):126‐8. [Google Scholar]
Gao 1993 {published data only}
- Gao ZQ, Tang PJ. Integrative medicine therapy for chronic pharyngitis. Chinese Journal of Integrated Traditional and Western Medicine 1993;8:498‐9. [Google Scholar]
Gao 2007 {published data only}
- Gao XF, Man YG. The preventive effect of Radix Astragali on recurrent respiratory tract infection. Journal of Jining Medical College 2007;30(1):68‐9. [Google Scholar]
Guan 2011 {published data only}
- Guan LM, Zhang LL, Luan HX, Wang KH. Curative effect observation of Astragalus particles in the treatment of 160 cases of recurrent respiratory tract infection in children. Journal of China Traditional Chinese Medicine Information 2011;3(23):246. [Google Scholar]
Guo 2008 {published data only}
- Guo JX, Wang YS. The prevention and treatment of 56 cases of recurrent respiratory tract infection with Astragalus granule. Modern Journal of Integrated Traditional Chinese and Western Medicine 2008;17(35):5420. [Google Scholar]
Han 2000 {published data only}
- Han H, Liu JX, Zhang YP. 100 cases of recurrent respiratory tract infection treated with transfer factor combined with Huangqi in children. Journal of Pediatric Pharmacy 2000;6(1):36. [Google Scholar]
Han 2011 {published data only}
- Han XM, Mu WH. Application of Astragalus particles combined with Lysine and Vitamin B12 granules in the treatment and prevention of children recurrent respiratory tract infection. World Health Digest Medical Periodical 2011;8(28):204‐5. [Google Scholar]
He 2014 {published data only}
- He ZP, Zhang CX, Liu ZF. Clinical observation of two different formulations of Astragalus in treatment of children with recurrent respiratory tract infection. Journal of Frontiers of Medicine 2014;12(34):181. [Google Scholar]
Hu 1984 {published data only}
- Hu JX. Analysis of the therapeutical effect of 529 cases with infantile pneumonia. Journal of Integrated Traditional Medicine 1984;4(11):672‐4. [PubMed] [Google Scholar]
Huang 2000 {published data only}
- Huang H. Astragalus in preventing recurrent respiratory tract infection. Chinese Journal of Information on TCM 2000;7(4):60. [Google Scholar]
Huang 2004a {published data only}
- Huang Y, Xu PJ. Clinical effect of Astragalus granule in treatment of children with recurrent respiratory tract infection. Proceedings of the Fifth Young and Middle‐aged Symposium. 2004; Vol. 1:99.
Huang 2004b {published data only}
- Huang Y, Liang Q, Xu PJ. Clinical observation of Astragalus Injection in treating recurrent respiratory tract infections in children. Modern Journal of Integrated Traditional Chinese and Western Medicine 2004;13(18):2411. [Google Scholar]
Huang 2012a {published data only}
- Huang Fu JX. A clinical research on the effect of Astragalus Injection on immune function in children. Medical Information 2012;25(4):127‐8. [Google Scholar]
Huo 1994 {published data only}
- Huo XJ. Treating 28 cases of severe pneumonia with the combination of Chinese and Western medical treatment in children. Liaoning Journal of Traditional Chinese Medicine 1994;21(1):36. [Google Scholar]
Ikeda 1988 {published data only}
- Ikeda K, Takasaka T. Treatment of secretory otitis media with kampo medicine. Archives of Oto‐rhino‐laryngology 1988;245(4):234‐6. [DOI] [PubMed] [Google Scholar]
Ji 1996 {published data only}
- Ji HH, Zhou DW. Treating chronic sinusitis with integrated traditional Chinese and Western medicine in 62 cases. Shanxi Journal of Traditional Chinese Medicine 1996;12(4):17‐8. [Google Scholar]
Jin 1997 {published data only}
- Jin YH, Xiao YM, Chen PL, Yao GY, Lu JC. Effect of Astragalus on T cell subsets for children with recurrent respiratory tract infection. Shanghai Medical & Pharmaceutical Journal 1997;3:24‐5. [Google Scholar]
Jin 2009 {published data only}
- Jin YS. Observation of Huangqi Guizhi Decoction in the treatment of children with recurrent respiratory tract infection. Modern Journal of Integrated Traditional Chinese and Western Medicine 2009;18(2):146. [Google Scholar]
Jin 2013 {published data only}
- Jin YF, Huang XH, Chen Y. Astragalus particles adjust the immune function repeated respiratory tract infection children 258 cases of observation. Shanghai Journal of Preventive Medicine 2013;4:193‐7. [Google Scholar]
Kang 1992 {published data only}
- Kang CH, Zhang YY, Bi BL, Li H, Ai LF, Huang RF, et al. Clinical study on supportive treating acute infantile pneumonia with medicated diet KT. Liaoning Journal of Traditional Chinese Medicine 1992;4:29‐30. [Google Scholar]
Ke 2005 {published data only}
- Ke QP, Guo YH. 80 cases of recurrent respiratory tract infection treated with combination of TCM and Western Medicine in Children. Henan Traditional Chinese Medicine 2005;25(9):55‐6. [Google Scholar]
Li 1989 {published data only}
- Li ZG, Cui Q, Zhang ZF. Contrast observation on the effect of Ru Er decoction combined with acupuncture for acute tonsillitis. Journal of Guiyang College of Traditional Chinese Medicine 1989;3:37‐8. [Google Scholar]
Li 1994a {published data only}
- Li YP, Jiang CG. Mixture of making lung calm in treating 50 cases of children with acute lower respiratory tract infection. Journal of Nanjing College of Traditional Chinese Medicine 1994;10(1):31‐2. [Google Scholar]
Li 1994b {published data only}
- Li YX, Zhang YH. Clinical observation of Chinese medicine for infantile pneumonia. Chinese Journal of Integrated Traditional and Western Medicine 1994;9:573. [Google Scholar]
Li 1999 {published data only}
- Li LQ. Nuclear casein, observe huangqijing prevention of bronchiolitis. Journal of Medical Theory and Practice 1999;12(9):542‐3. [Google Scholar]
Li 2001 {published data only}
- Li GQ, Song QQ, Qi WS, Yang XJ, Xiong KM, Zhao B. Integrative medicine for acute senile bacterial pneumonia in 49 cases. Chinese Journal of Information on Traditional Chinese Medicine 2001;8(7):68‐9. [Google Scholar]
Li 2002 {published data only}
- Li YZ, Liu YH, Sun GF. 81 cases of recurrent respiratory tract infection treated with Astragalus in children. Chinese Community Doctors 2002;18(24):36. [Google Scholar]
Li 2004 {published data only}
- Li J, Chen DD. Treating 76 cases of mycoplasma pneumonia with the combination of traditional Chinese and Western therapy. Chinese Journal of Information on Traditional Chinese Medicine 2004;11(1):74. [Google Scholar]
Li 2008 {published data only}
- Li XZ. Clinical observation of Astragalus particles in prevention and treatment of recurrent respiratory tract infections in children. Chinese Journal of Misdiagnostics 2008;8(28):6871‐2. [Google Scholar]
Li 2013 {published data only}
- Li XJ. Clinical research on treating 50 cases of RRTI in children in the integrative medicine. Clinical Journal of Chinese Medicine 2013;5(21):25‐6. [Google Scholar]
Li 2015 {published data only}
- Li X. Research on curative effect of traditional Chinese medicine treating low‐grade fever of children caused by respiratory system infection. Pakistan Journal of Pharmaceutical Sciences 2015;25(4):1457‐60. [PubMed] [Google Scholar]
Lin 2001 {published data only}
- Lin XZ. To observe the curative effect of 130 cases of huangqijing oral liquid in the treatment of children with recurrent respiratory tract infection. Henan Traditional Chinese Medicine 2001;21(1):57‐8. [Google Scholar]
Lin 2003 {published data only}
- Lin DH, Ma X, Yang H, Chen K. Clinical observation of traditional Chinese medicine for treating mycoplasma pneumonia. Chinese Journal of Information on Traditional Chinese Medicine 2003;10(11):42‐3. [Google Scholar]
Lin 2012 {published data only}
- Lin JY. Treatment of 61 cases of recurrent respiratory tract infection with Huang‐Qi‐Jing oral liquid. China's Naturopathy 2012;20(7):46. [Google Scholar]
Liu 1992 {published data only}
- Liu WY, Li F, Yu GY. Study on children with recurrent respiratory tract infection of peripheral blood NK cell activity and T cell subsets. Journal of Mudanjiang Medical College 1992;13(2):96‐8. [Google Scholar]
Liu 2002 {published data only}
- Liu D, Lv J, Yang Q. The observation of antivirus pill for treating 50 childhood upper respiratory infection. Tian Jin Pharmacy 2002;14(6):54. [Google Scholar]
Liu 2003 {published data only}
- Liu SH, Li CP, Xue WH. A clinical research on treatment of infant recurrent respiratory infection with combination of traditional Chinese medicine and western medicine. Journal of Binzhou Medical College 2003;26(02):98‐100. [Google Scholar]
Liu 2004a {published data only}
- Liu T. Treating 105 cases of enduring cough after cold with syndrome differentiation treatment. Chinese Journal of Information on Traditional Chinese Medicine 2004;11(9):824‐5. [Google Scholar]
Liu 2004b {published data only}
- Liu MH, Zhou S. Analysis of the clinical curative effect of Astragalus Injection in adjuvant treatment of infantile bronchiolitis. Jiangxi Medical Journal 2004;39(1):40‐1. [Google Scholar]
Liu 2004c {published data only}
- Liu WC, Li CY. To observe the curative effect of Huangqi with zinc on children with recurrent respiratory tract infection. Zhongguo Shiyong Xiangcun Yisheng Zazhi 2004;11(4):37. [Google Scholar]
Liu 2010 {published data only}
- Liu DJ, Zheng B, Cai BH, Zhou WM, Yu BX. Traditional Chinese and Western medicine treatment of mycoplasmal pneumonia in children and the serum cytokine changes. Journal of Southern Medical University 2010;30(3):626‐7, 630. [PubMed] [Google Scholar]
Liu 2011 {published data only}
- Liu J. Curative effect observation of Astragalus particles in the treatment of children recurrent respiratory tract infection. Journal of China Traditional Chinese Medicine Information 2011;3(18):156. [Google Scholar]
Liu 2014 {published data only}
- Liu GS, Yu DF, Li MZ. Curative observation of combination therapy of antibiotics and Astragalus Injection in the treatment of children upper respiratory tract infection. Journal of Mathematical Medicine 2014;27(6):712‐3. [Google Scholar]
Lu 2006 {published data only}
- Lu W. XQM treated Astragalus in the treatment of respiratory tract infection in children. Journal of Medical Forum 2006;27(17):90‐2. [Google Scholar]
Lu 2009 {published data only}
- Lu J. Clinical observation of 50 cases of Huangqi treating children with recurrent respiratory tract infection. Chinese Journal of Ethnomedicine and Ethnopharmacy 2009;8:117. [Google Scholar]
Lu 2012 {published data only}
- Lu ZM, Qian XH, Chen ZW, Zhang CH, Guo LS, Chen J. Prospective clinical study of radix astragali and its compound prescription for treatment of beta‐thalassemia in children. Chinese Journal of Contemporary Pediatrics 2012;5:344‐9. [PubMed] [Google Scholar]
Lu 2013 {published data only}
- Lu JZ. Clinical evaluation of the combination treatment of children with recurrent respiratory tract infection. Journal of Clinical Pulmonary Medicine 2013;3:478‐9. [Google Scholar]
Luan 2001 {published data only}
- Luan H, Feng JH. Effect of Huangqi essence oral liquid In children with repeated respiratory infection. Medical Journal of Qilu 2001;2:107‐8. [Google Scholar]
Luo 1994 {published data only}
- Luo KQ, Yang JS, Luo JZ, Wang GZ. Treatment of chronic suppurative maxillary sinusitis with integrated Chinese and Western medicine. Chinese Journal of Integrated Traditional and Western Medicine 1994;10(14):631. [Google Scholar]
Luo 2013 {published data only}
- Luo P, Wang H. Curative effect observation of Astragalus particles in treating children recurrent respiratory tract infection. Journal of Community Medicine 2013;17:31‐2. [Google Scholar]
Nie 2009a {published data only}
- Nie QF, Yi P. The effect of Astragalus on SIL‐2R, IL‐8 and Ig with repeated respiratory tract infection patients. Chinese Journal of Cellular and Molecular Immunology 2009;4(25):362‐3. [Google Scholar]
Peng 1991 {published data only}
- Peng X, Zheng S. Sinusitis mixture combined with ultrasonic atomization in treating chronic sinusitis in 35 cases. Chinese Journal of Modern Developments in Traditional Medicine 1991;8:467. [Google Scholar]
Peng 2006 {published data only}
- Peng RF. Clinical observation of Astragalus in treatment of children with recurrent respiratory tract infection. Modern Journal of Integrated Traditional Chinese and Western Medicine 2006;17:2348‐9. [Google Scholar]
Peng 2012 {published data only}
- Peng Y, Zhang Y, Yuan LZ. Curative effect of Huangqi oral liquid in preventing recurrent myocarditis caused by respiratory tract infection. Lishizhen Medicine and Materia Medica Research 2012;7:1832‐3. [Google Scholar]
Qi 2000 {published data only}
- Qi W, Ren A, Zhang S. Dynamic changes of serum pro‐inflammatory cytokines and anti‐inflammatory cytokines in patients with acute infection and the effect of Chinese herbal medicine intervention. Chinese Journal of Integrated Traditional & Western Medicine 2000;11:824‐7. [PubMed] [Google Scholar]
Qiu 2004 {published data only}
- Qiu YT, Zhou C, Li RH, Lin SY, Zeng L. To observe the curative effect of Huangqi granule in adjuvant treatment of children with recurrent respiratory tract infection. Journal of Practical Medicine 2004;7:850‐1. [Google Scholar]
Ruan 2013 {published data only}
- Ruan WH, Huang ML, He XL, Zhang F, Tao HB. Effects of huangqi and bear bile on recurrent parotitis in children: a new clinical approach. Journal of Zhejiang University ‐ Science B (Biomedicine & Biotechnology) 2013;3:253‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Shen 1988 {published data only}
- Shen SP, Yang HZ, Xu YZ. Astragalus extract oral low dose of prevention of 100 cases of respiratory tract infection in children. Jiangsu TCM 1988;9:32. [Google Scholar]
Sheng 2010 {published data only}
- Sheng L. Preventive effect of Astragalus on recurrent episodes of recurrent respiratory tract infection. China Modern Medicine 2010;35:96. [Google Scholar]
Shi 2006 {published data only}
- Shi W, Gao P, Li J, Feng YS. To observe the preventive effect of Astragalus in the common cold. Clinical Journal of Medical Officer 2006;2:247‐8. [Google Scholar]
Song 2008 {published data only}
- Song ZY. Astragalus essence oral liquid and cod liver oil 38 cases of prevention and treatment of infantile repeated respiratory infection. Chinese Community Doctors 2008;21:131. [Google Scholar]
Su 1988 {published data only}
- Su BG. Therapeutic effects of TCM‐WM on pneumonia in newborn baby with respiratory repeated pause. Chinese Journal of Modern Developments in Traditional Medicine 1988;3:182‐2. [Google Scholar]
Su 1994 {published data only}
- Su XQ. Clinical Observation of treating upper respiratory tract infectional cough with 'Jiang Du Ke' ‐ with case reports of 88 cases. Journal of Chengdu College of Traditional Chinese Medicine 1994;4:21‐5. [Google Scholar]
Wang 1997 {published data only}
- Wang WY, Liu Y, Li SG, Yue YE. Effect of Fuzheng Jianpi on immune function in children with recurrent respiratory tract infection. Chinese Journal of Traditional Medical Science and Technology 1997;2:73‐4. [Google Scholar]
Wang 2001 {published data only}
- Wang CY, Jiang C, Mao Q. Observation on the effect of oral fluid of Astragalus Essence in the prevention and treatment of 32 cases of infantile recurrent respiratory tract infection. Journal of Practical Traditional Chinese Medicine 2001;3:34‐5. [Google Scholar]
Wang 2008a {published data only}
- Wang J. Huangqi, BCG‐PSN preventive effect observation of children with asthmatic bronchitis. Journal of Huaihai Medicine 2008;26:429‐30. [Google Scholar]
Wang 2008b {published data only}
- Wang XL. Effect comparison of pedo‐mycoplasma pneumonia treated with integrated traditional and Western medicine or little hormone. Modern Journal of Integrated Traditional Chinese and Western Medicine 2008;5(17):667‐8. [Google Scholar]
Wang 2009 {published data only}
- Wang SF, Wang JZ, Kong XM. Clinical observation of 120 cases of Astragalus in treatment of children with recurrent respiratory tract infection. Chinese Journal of Coal Industry Medicine 2009;3:453. [Google Scholar]
Wang 2010 {published data only}
- Wang SP, Chen GQ, Xiao HF, Wang J. Curative effect and observation of Astragalus essence combined with Shinsbo on treating children recurrent respiratory tract infection. Modern Chinese Doctor 2010;7:38‐9. [Google Scholar]
Wang 2013 {published data only}
- Wang XY, Wu QL, Li J. Clinical observation on treating children with recurrent respiratory tract infection by licorzinc. Clinical Journal of Chinese Medicine 2013;19:73‐4. [Google Scholar]
Wang 2014 {published data only}
- Wang XP. Curative effect observation on 40 cases of children with recurrent respiratory tract infection treated with the combination of the oral fluid of Astragalus Essence and pidotimod. Shanxi Medical Journal 2014;19:2300‐1. [Google Scholar]
Wang 2015 {published data only}
- Wang MH, Gao H. Curative effect observation of integrated traditional Chinese and western medicine in the prevention and treatment of children recurrent respiratory tract infection. Chinese Journal of Clinical Rational Drug Use 2015;11:37‐8. [Google Scholar]
Wei 2000 {published data only}
- Wei XZ. To investigate the effect of Astragalus and vitamins curative effect in the treatment of recurrent respiratory tract infection. Medical Journal of Communications 2000;4:345‐6. [Google Scholar]
Wu 1996 {published data only}
- Wu L. The treatment of TCM‐WM on Sinusitis for 80 cases. Chinese Journal of Integrated Traditional and Western Medicine 1996;6:30. [Google Scholar]
Wu 2003 {published data only}
- Wu WQ. Clinical observation on prevention and treatment of 68 children of recurrent respiratory tract infection with Astragalus granule. China Journal of Modern Medicine 2003;1(4):11. [Google Scholar]
Wu 2011 {published data only}
- Wu JL. The two drugs cost‐effect analysis for the treatment of upper respiratory tract infection. Chinese Manipulation & Rehabilitation Medicine 2011;24:138. [Google Scholar]
Xia 2007 {published data only}
- Xia WH. Effect of mycoplasma pneumoniae infection on immune function in children treated with integrated traditional Chinese and Western medicine. Journal of Clinical and Experimental Medicine 2007;12:90‐1. [Google Scholar]
Xiao 1988 {published data only}
- Xiao LX, Li WZ, Wang SF. Curative effective observation on treating infantile acute respiratory tract infection with Chinese medicine. Jiangxi Journal of Traditional Chinese Medicine 1988;3:27. [Google Scholar]
Xiao 2014 {published data only}
- Xiao XF, Li YP, Feng YB, Zhang X. Clinical experience of the combination therapy of Astragalus particles and levamisole in treatment of children recurrent respiratory infection. Medical Information 2014;23:432. [Google Scholar]
Xie 2015 {published data only}
- Xie M, Lue XY. Clinical efficacy of Astragalus Particles in treating children recurrent respiratory tract infection of ying‐wei disharmony type. Journal of Pediatrics of Traditional Chinese Medicine 2015;4:20‐2. [Google Scholar]
Xu 1994 {published data only}
- Xu JJ. Effective analysis of Chinese medicine adding ibuprofen for acute pharyngitis in 80 cases. Chinese Journal of Integrated Traditional and Western Medicine 1994;8:477. [Google Scholar]
Xu 1997 {published data only}
- Xu B. A clinical study of new Sanliangban oral liquid in preventing and treating children with recurrent respiratory tract infection. Journal of Zhejiang College of TCM 1997;4:29‐31. [Google Scholar]
Xu 2004 {published data only}
- Xu Y, Hu Y. Clinical observation of Astragalus Injection in treating recurrent respiratory tract infections in children. Qilu Pharmaceutical Affairs 2004;4:56. [Google Scholar]
Yang 1992 {published data only}
- Yang TG. Clinical observation of integrated traditional Chinese and Western medicine for acute episode of chronic bronchitis in 115 cases. Jiangsu Journal of Traditional Chinese Medicine 1992;6:8‐9. [Google Scholar]
Yang 1998 {published data only}
- Yang ZZ, Ji CY, Feng L. Curative effect observation of Huangqi oral liquid for 78 cases of recurrent respiratory tract infection In children. Shanghai Medical & Pharmaceutical Journal 1998;5:13‐4. [Google Scholar]
Yang 2001 {published data only}
- Yang J, Liu ZF. Clinical observation of Astragalus in treatment of children with recurrent respiratory tract infection. Chinese Journal of Integrated Traditional and Western Medicine 2001;1:73. [Google Scholar]
Yang 2008 {published data only}
- Yang SP, Dong H, Wu YC, Su H, Wu YJ, Huang AP. Clinical effect of Milkvetch extract oral liquid in preventing and treating children's recurrent respiratory tract infection. Chinese Journal of Integrated Traditional and Western Medicine 2008;6:544‐7. [PubMed] [Google Scholar]
Yu 2005 {published data only}
- Yu CJ, Wang JH, Wang Y. To observe the curative effect of Huangqi Granule on prevention and treatment of recurrent respiratory tract infection. Central Plains Medical Journal 2005;15:73. [Google Scholar]
Zeng 2009 {published data only}
- Zeng FR, Zeng FZ. Curative effect of Chinese medicine Huangqi on the adjunctive therapy of bronchial asthma complicated with recurrent respiratory infection in children. Hubei Journal of Traditional Chinese Medicine 2009;12:11‐2. [Google Scholar]
Zhang 1995 {published data only}
- Zhang WL. Integrated traditional Chinese and Western medicine for infantile gasping bronchitis in 500 cases. Jiangxi Journal of Traditional Chinese Medicine 1995;3:52‐7. [Google Scholar]
Zhang 1999 {published data only}
- Zhang WX. Prevention and treatment of recurrent respiratory tract infection in children with integrated traditional Chinese and Western Medicine. Journal of Bengbu Medical College 1999;6:465‐6. [Google Scholar]
Zhang 2000 {published data only}
- Zhang JJ. Astragalus essence oral liquid on the immune function of infantile repeated respiratory infection. Zhejiang Journal of Integrated Traditional Chinese and Western Medicine 2000;2:96‐7. [Google Scholar]
Zhang 2012 {published data only}
- Zhang YQ. Treatment of recurrent respiratory tract infections with astragalus particles. Medical Journal of West China 2012;1:36‐7. [Google Scholar]
Zhang 2013 {published data only}
- Zhang Y. Huangqi oral liquid combined with levamisol for the prevention of children recurrent respiratory tract infection. Chinese Journal of Practical Medicine 2013;40:121. [Google Scholar]
Zhao 2000a {published data only}
- Zhao HY. Therapeutic effect of integration of traditional Chinese medicine and western medicine on chronic pharyngitis. Hebei Journal of Traditional Chinese Medicine 2000;7(22):539‐40. [Google Scholar]
Zhao 2000b {published data only}
- Zhao JF, Wang SW, Zhang TL. Combined with weierben huangqijing treatment of 69 cases of recurrent respiratory tract infection. Journal of Pediatric Pharmacy 2000;3:19. [Google Scholar]
Zhao 2003 {published data only}
- Zhao LP, Yin SM. Curative effect and immunologic effect of astragalus extract in treatment of children with recurrent respiratory tract infection. Modern Jorunal of Integrated Traditional Chinese and Western Medicine 2003;19:2035‐6. [Google Scholar]
Zhao 2007 {published data only}
- Zhao CQ. Clinical observation of 50 cases of Huangqi Injection in prevention and treatment of children with recurrent respiratory tract infection. Public Medical Forum Magazine 2007;2:84. [Google Scholar]
Zheng 2013 {published data only}
- Zheng HL. Astragalus injection for the treatment of children refractory pneumonia with experience of 58 cases. Chinese and Foreign Medical Research 2013;22:26‐7. [Google Scholar]
Zhong 2012 {published data only}
- Zhong ZY, Zhong YH, Huang XM. Curative effect observation of Astragalus decoction combined with western medicine in the treatment of children recurrent respiratory tract infection. People's Military Surgeon 2012;2:147‐8. [Google Scholar]
Zhou 2005 {published data only}
- Zhou AY, Huang XZ. Clinical observation of Astragalus in prevention and treatment of children with recurrent respiratory tract infection. Strait Pharmaceutical Journal 2005;4:159‐60. [Google Scholar]
Zhou 2009a {published data only}
- Zhou YH. Observation of the Astragalus essence adjusting immune function in children's recurrent respiratory tract infections. Chinese Community Doctors 2009;10:109‐10. [Google Scholar]
Zhou 2009b {published data only}
- Zhou QH. Levamisole combined with Astragalus oral liquid to observe the curative effect of the treatment of 50 cases of children with recurrent respiratory tract infection. China Healthcare Frontiers 2009;16:60. [Google Scholar]
Zhou 2012 {published data only}
- Zhou YD. Curative effect analysis of Astragalus particles in the prevention and treatment of 34 cases of children with recurrent respiratory tract infection. Health Required 2012;5:263‐3. [Google Scholar]
Zhu 2014a {published data only}
- Zhu XP. Analysis of curative effect on treating recurrent respiratory tract infection with combination of Chinese traditional and Western medicine. Modern Chinese Doctor 2014;8:119‐20, 134. [Google Scholar]
Zhu 2014b {published data only}
- Zhu DJ, Wei YB. A clinical study on the treatment of recurrent respiratory tract infection with combination of integrated Chinese and Western medicines. Asia‐Pacific Traditional Medicine 2014;24:80‐1. [Google Scholar]
Zou 2000 {published data only}
- Zou LY. Astragalus essence oral liquid prevention and treatment of 50 cases of infantile repeated respiratory infection. Fujian Journal of Traditional Chinese Medicine 2000;3:20. [Google Scholar]
Additional references
Andrews 2012
- Andrews T, Thompson M, Buckley DI, Heneghan C, Deyo R, Redmond N, et al. Interventions to influence consulting and antibiotic use for acute respiratory tract infections in children: a systematic review and meta‐analysis. PloS One 2012;7:303‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Atkins 2004
- Atkins D, Best D, Briss PA, Eccles M, Falck‐Ytter Y, Flottorp S, et al. GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ 2004;328(7454):1490. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bellanti 1997
- Bellanti JA. Recurrent respiratory tract infections in paediatric patients. Drugs 1997;54(Suppl 1):1‐4. [DOI] [PubMed] [Google Scholar]
Brichacek 1996
- Brichacek B, Swindells S, Janoff EN, Pirruccello S, Stevenson M. Increased plasma human immunodeficiency virus type 1 burden following antigenic challenge with pneumococcal vaccine. Journal of Infectious Diseases 1996;174:1191‐9. [DOI] [PubMed] [Google Scholar]
Cheung 2011
- Cheung F. TCM: Made in China. Nature 2011;480(7378):S82‐3. [DOI] [PubMed] [Google Scholar]
Costelloe 2010
- Costelloe C, Metcalfe C, Lovering A, Mant D, Hay AD. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta‐analysis. BMJ 2010;340:c2096. [DOI] [PubMed] [Google Scholar]
CPSCMA 1999
- Chinese Paediatric Society of Chinese Medical Association. Chinese paediatrics antibiotics application guideline of acute respiratory tract infection. Chinese Journal of Paediatrics 1999;37(12):748‐50. [Google Scholar]
CPSCMA 2008
- Chinese Paediatric Society of Chinese Medical Association. Guideline: the clinical concept and management principle of recurrent respiratory tract infection. Chinese Journal of Paediatrics 2008;46(2):108‐10. [PubMed] [Google Scholar]
Culebras 2013
- Culebras E, Betriu C, Vazquez‐Cid E, Lopez‐Varela E, Rueda S, Picazo JJ. Detection and genotyping of human respiratory viruses in clinical specimens from children with acute respiratory tract infections. Revista Espanola de Quimioterapia 2013;26:47‐50. [PubMed] [Google Scholar]
Del‐Rio‐Navarro 2012
- Del‐Rio‐Navarro BE, Espinosa‐Rosales FJ, Flenady V, Sienra‐Monge JJL. Immunostimulants for preventing respiratory tract infection in children. Evidence‐Based Child Health 2012;7(2):629‐717. [DOI: 10.1002/ebch.1833] [DOI] [PMC free article] [PubMed] [Google Scholar]
Doan 2012
- Doan Q, Enarson P, Kissoon N, Klassen TP, Johnson DW. Rapid viral diagnosis for acute febrile respiratory illness in children in the Emergency Department. Cochrane Database of Systematic Reviews 2012, Issue 5. [DOI: 10.1002/14651858.CD006452.pub3] [DOI] [PubMed] [Google Scholar]
Fendrick 2003
- Fendrick AM, Monto AS, Nightengale B, Sarnes M. The economic burden of non‐influenza‐related viral respiratory tract infection in the United States. Archives of Internal Medicine 2003;163(4):487‐94. [DOI] [PubMed] [Google Scholar]
Fischer 2014
- Fischer JB, Prasad PA, Coffin SE, Alpern ER, Mistry RD. Canadian Acute Respiratory Illness and Flu Scale (CARIFS) for clinical detection of influenza in children. Clinical Pediatrics 2014;53(12):1174‐80. [PUBMED: 25009116] [DOI] [PubMed] [Google Scholar]
Fu 2009
- Fu SF, Zhang JH, Shang HC, Gao XM. Analysis on case suffered from adverse reactions of Huangqi injection. Drug Evaluation Research 2009;32(1):54‐61. [Google Scholar]
GRADEpro GDT 2014 [Computer program]
- GRADE Working Group, McMaster University. GRADEpro GDT. Version accessed prior to 20 November 2016. Hamilton (ON): GRADE Working Group, McMaster University, 2014.
Griffin 2004
- Griffin MR, Walker FJ, Iwane MK, Weinberg GA, Staat MA, Erdman DD, et al. Epidemiology of respiratory infections in young children: insights from the new vaccine surveillance network. Pediatric Infectious Disease Journal 2004;23(Suppl 11):188‐92. [DOI] [PubMed] [Google Scholar]
Grüber 2008
- Grüber C, Keil T, Kulig M, Roll S, Wahn U, Wahn V, MAS‐90 Study Group. History of respiratory infections in the first 12 yr among children from a birth cohort. Pediatric Allergy and Immunology 2008;19(6):505‐12. [DOI] [PubMed] [Google Scholar]
Hao 2015
- Hao B, Dong BR, Wu T. Probiotics for preventing acute upper respiratory tract infections. Cochrane Database of Systematic Reviews 2015, Issue 2. [DOI: 10.1002/14651858.CD006895.pub3] [DOI] [PubMed] [Google Scholar]
Hay 2005
- Hay AD, Heron J, Ness A, ALSPAC study team. The prevalence of symptoms and consultations in pre‐school children in the Avon Longitudinal Study of Parents and Children (ALSPAC): a prospective cohort study. Family Practice 2005;22(4):367‐74. [DOI] [PubMed] [Google Scholar]
Heikkinen 2003
- Heikkinen T, Jarvinen A. The common cold. Lancet 2003;361(9351):51‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hemilä 2013
- Hemilä H, Chalker E. Vitamin C for preventing and treating the common cold. Cochrane Database of Systematic Reviews 2013, Issue 1. [DOI: 10.1002/14651858.CD000980.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327(7414):557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Hollinghurst 2008
- Hollinghurst S, Gorst C, Fahey T. Measuring the financial burden of acute cough in pre‐school children: a cost of illness study. Family Practice 2008;9(10):1‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hou 1981
- Hou YD, Ma GL, Wu SH. Effect of Radix Astragali seu Hedysari on the interferon system. Chinese Medical Journal 1981;1:35‐40. [PubMed] [Google Scholar]
Hu 1988
- Hu YJ. The national pediatrics respiratory disease academic conference summary: diagnosis criteria of recurrent respiratory tract infection. Chinese Journal of Pediatrics 1988;26:41‐2. [Google Scholar]
Hu 2008
- Hu H, Zhou XQ, Rao YH. Analysis of reports of ADR induced by Huangqi injection. Anhui Medical and Pharmaceutical Journal 2008;12:1261‐2. [Google Scholar]
Huang 2012b
- Huang Y, Wu T, Zeng L, Li S. Chinese medicinal herbs for sore throat. Cochrane Database of Systematic Reviews 2012, Issue 3. [DOI: 10.1002/14651858.CD004877.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
IBMSCAMS 1979
- Institute of Basic Medical Sciences, the Chinese Academy of Medical Sciences. Immunity parameters and blood cAMP changes in normal persons after ingestion of Radix Astragali. National Medical Journal of China 1979;59:31‐4. [Google Scholar]
Jacobs 2000
- Jacobs B, Young NL, Dick PT, Ipp MM, Dutkowski R, Davies HD, et al. Canadian Acute Respiratory Illness and Flu Scale (CARIFS): development of a valid measure for childhood respiratory infections. Journal of Clinical Epidemiology 2000;53(8):793‐9. [PUBMED: 10942861] [DOI] [PubMed] [Google Scholar]
Jefferson 2009
- Jefferson T, Mar C, Dooley L, Ferroni E, Al‐Ansary LA, Bawazeer GA, et al. Physical interventions to interrupt or reduce the spread of respiratory viruses: systematic review. BMJ 2009;339:b.3675. [DOI] [PMC free article] [PubMed] [Google Scholar]
Jiang 2012
- Jiang L, Li K, Wu T. Chinese medicinal herbs for acute bronchitis. Cochrane Database of Systematic Reviews 2012, Issue 2. [DOI: 10.1002/14651858.CD004560.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Jiang 2013
- Jiang L, Deng L, Wu T. Chinese medicinal herbs for influenza. Cochrane Database of Systematic Reviews 2013, Issue 3. [DOI: 10.1002/14651858.CD004559.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Jolliffe 2013
- Jolliffe DA, Griffiths CJ, Martineau AR. Vitamin D in the prevention of acute respiratory infection: systematic review of clinical studies. Journal of Steroid Biochemistry and Molecular Biology 2013;136:321‐9. [DOI] [PubMed] [Google Scholar]
Kartasurya 2012
- Kartasurya MI, Ahmed F, Subagio HW, Rahfiludin MZ, Marks GC. Zinc combined with vitamin A reduces upper respiratory tract infection morbidity in a randomised trial in preschool children in Indonesia. British Journal of Nutrition 2012;108(12):2251‐60. [DOI] [PubMed] [Google Scholar]
Kvaerner 2000
- Kvaerner KJ, Nafstad P, Jaakkola JJ. Upper respiratory morbidity in preschool children: a cross‐sectional study. Archives of Otolaryngology Head and Neck Surgery 2000;126(10):1201‐6. [DOI] [PubMed] [Google Scholar]
Leder 2003
- Leder K, Sinclair MI, Mitakakis TZ, Hellard ME, Forbes A. A community‐based study of respiratory episodes in Melbourne, Australia. Australian and New Zealand Journal of Public Health 2003;27(4):399‐404. [DOI] [PubMed] [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Liu 2012
- Liu X, Zhang M, He L, Li Y. Chinese herbs combined with Western medicine for severe acute respiratory syndrome (SARS). Cochrane Database of Systematic Reviews 2012, Issue 10. [DOI: 10.1002/14651858.CD004882.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Martino 2007
- Martino M, Ballotti S. The child with recurrent respiratory infections: normal or not?. Pediatric Allergy and Immunology 2007;Suppl 18:13‐8. [DOI] [PubMed] [Google Scholar]
Moher 2009
- Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta‐Analyses: The PRISMA Statement. BMJ 2009;339:2535. [PMC free article] [PubMed] [Google Scholar]
Monto 1993
- Monto AS, Sullivan KM. Acute respiratory illness in the community. Frequency of illness and the agents involved. Epidemiology and Infection 1993;110:145‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Monto 2002
- Monto AS. Epidemiology of viral respiratory infections. American Journal of Medicine 2002;112(Suppl 6A):4‐12. [DOI] [PubMed] [Google Scholar]
Mäkelä 1998
- Mäkelä MJ, Puhakka T, Ruuskanen O, Leinonen M, Saikku P, Kimpimäki M, et al. Viruses and bacteria in the etiology of the common cold. Journal of Clinical Microbiology 1998;36(2):539‐42. [DOI] [PMC free article] [PubMed] [Google Scholar]
Natural Medicines 2016
- Natural Medicines. Natural Medicines ‐ Astragalus. www.naturaldatabase.therapeuticresearch.com/nd/PrintVersion.aspx?id=963&AspxAutoDetectCookieSupport=1 (accessed 9 September 2016).
Nie 2009b
- Nie LF, Yi Ping. Huangqi influence SIL‐2R, IL‐8 and immuno‐globin in patient with recurrent respiratory tract infection. Chinese Journal of Cellular and Molecular Immunology 2009;25(4):362‐3. [Google Scholar]
O'Brien 1995
- O'Brien WA, Grovit‐Ferbas K, Namazi A, Ovcak‐Derzic S, Wang HJ, Park J, et al. Human immunodeficiency virus‐type 1 replication can be increased in peripheral blood of seropositive patients after influenza vaccination. Blood 1995;86(3):1082‐9. [PubMed] [Google Scholar]
Patwardhan 2005
- Patwardhan B, Gautam M. Botanical immuno drugs: scope and opportunities. Drug Discovery Today 2005;10(7):495‐502. [DOI] [PMC free article] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Shepperd 2004
- Shepperd S, Perera R, Bates S, Jenkinson C, Hood K, Harnden A, et al. A children's acute respiratory illness scale (CARIFS) predicted functional severity and family burden. Journal of Clinical Epidemiology 2004;57(8):809‐14. [PUBMED: 15485733] [DOI] [PubMed] [Google Scholar]
Stata 2009 [Computer program]
- StataCorp. Stata. Version 11.0. USA: StataCorp, 2009.
Steinsbekk 2005a
- Steinsbekk A, Fønnebø V, Lewith G, Bentzen N. Homeopathic care for the prevention of upper respiratory tract infections in children: a pragmatic, randomised, controlled trial comparing individualised homeopathic care and waiting‐list controls. Complementary Therapies in Medicine 2005;13(4):231‐8. [DOI] [PubMed] [Google Scholar]
Steinsbekk 2005b
- Steinsbekk A, Bentzen N. Self treatment with one of three self selected, ultra molecular homeopathic medicines for the prevention of upper respiratory tract infections in children. A double‐blind randomised placebo controlled trial. British Journal of Clinical Pharmacology 2005;59(4):447‐55. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wang 2002
- Wang RT, Shan BE, Li QX. Extracorporeal experimental study on immuno‐modulator activity of Astragalus membranaceus extract. Zhongguo Zhong Xi Yi Jie He Za Zhi [Chinese Journal of Integrated Traditional and Western Medicine] 2002;6:453‐6. [PubMed] [Google Scholar]
WHO 1998
- World Health Organization. Acute respiratory infections: the forgotten pandemic. Bulletin of the World Health Organization 1998;76(1):101‐7. [PMC free article] [PubMed] [Google Scholar]
WHO 2007
- World Health Organization. WHO international standard terminologies on traditional medicine in the Western Pacific Region. World Health Organization, Western Pacific Region, 2007. [Google Scholar]
Wu 2007
- Wu T, Zhang J, Qiu Y, Xie L, Liu GJ. Chinese medicinal herbs for the common cold. Cochrane Database of Systematic Reviews 2007, Issue 1. [DOI: 10.1002/14651858.CD004782.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Xiong 2002
- Xiong HL. Advances in clinical application of Astragalus membranaceus and drug adverse reaction. Pharmaceutical Care and Research 2002;2(3):180‐2. [Google Scholar]
Zou 2013
- Zou C, Su GB, Wu YC, Lu FH, Mao W, Liu XS. Astragalus in the prevention of upper respiratory tract infection in children with nephrotic syndrome: evidence‐based clinical practice. Evidence‐Based Complementary Alternative Medicine 2013;2013:352130. [DOI: 10.1155/2013/352130] [DOI] [PMC free article] [PubMed] [Google Scholar]
References to other published versions of this review
Su 2015
- Su G, Chen X, Liu Z, Yang L, Zhang L, Stålsby Lundborg C, et al. Oral Astragalus (Huang qi) for preventing frequent episodes of acute respiratory tract infection in children. Cochrane Database of Systematic Reviews 2015, Issue 11. [DOI: 10.1002/14651858.CD011958] [DOI] [PMC free article] [PubMed] [Google Scholar]