

Abstract
Background
Eczema is a chronic skin disease characterised by dry skin, intense itching, inflammatory skin lesions, and has a considerable impact on quality of life. Moisturisation is an integral part of treatment, but it is unclear if moisturisers are effective.
Objectives
To assess the effects of moisturisers for eczema.
Search methods
We searched the following databases to December 2015: Cochrane Skin Specialised Register, CENTRAL, MEDLINE, Embase, LILACS, and GREAT. We searched five trials registers and checked references of included and excluded studies for further relevant trials.
Selection criteria
Randomised controlled trials in people with eczema.
Data collection and analysis
We used standard Cochrane methodological procedures.
Main results
We included 77 studies (mean duration: 6.7 weeks; 6603 participants, mean age: 18.6 years). Thirty‐six studies were at high risk of bias, 34 at unclear risk, and seven at low risk. Twenty‐four studies assessed our primary outcome of participant‐assessed disease severity, 13 assessed satisfaction, and 41 assessed adverse events. Secondary outcomes included investigator‐assessed disease severity (addressed in 65 studies), skin barrier function (29), flare prevention (16), quality of life (10), and corticosteroid use (eight). Adverse events reporting was limited (smarting, stinging, pruritus, erythema, folliculitis).
Six studies evaluated moisturiser versus no moisturiser. Participant‐assessed disease severity and satisfaction were not assessed. Moisturiser use yielded lower SCORing Atopic Dermatitis (SCORAD) scores than no moisturiser (3 studies, 276 participants; mean difference (MD) ‐2.42, 95% confidence interval (CI) ‐4.55 to ‐0.28), but the minimal important difference (MID) was unmet. Moisturiser use resulted in fewer flares (2 studies, 87 participants; RR 0.40, 95% CI 0.23 to 0.70), prolonged time to flare (median: 180 versus 30 days), and reduced use of topical corticosteroids (2 studies, 222 participants; MD ‐9.30 g, 95% CI ‐15.3 to ‐3.27). There was no clear difference in adverse events (1 study, 173 participants; risk ratio (RR) 15.34, 95% CI 0.90 to 261.64). Evidence for these outcomes was low quality.
With Atopiclair, 174/232 participants reported improvement in disease severity versus 27/158 using vehicle (3 studies; RR 4.51, 95% CI 2.19 to 9.29). Atopiclair decreased itching (4 studies, 396 participants; MD ‐2.65, 95% CI ‐4.21 to ‐1.09) and achieved more frequent satisfaction (2 studies, 248 participants; RR 2.14, 95% CI 1.58 to 2.89), fewer flares (3 studies, 397 participants; RR 0.18, 95% CI 0.11 to 0.31), and lower Eczema Area and Severity Index (EASI) scores (4 studies, 426 participants; MD ‐4.0, 95% CI ‐5.42 to ‐2.57), but the MID was unmet. The number of participants reporting adverse events was not statistically different (4 studies, 430 participants; RR 1.03, 95% CI 0.79 to 1.33). Evidence for these outcomes was moderate quality.
Participants reported skin improvement more frequently with urea‐containing cream than placebo (1 study, 129 participants; RR 1.28, 95% CI 1.06 to 1.53; low‐quality evidence), with equal satisfaction between the two groups (1 study, 38 participants; low‐quality evidence). Urea‐containing cream improved dryness (investigator‐assessed) (1 study, 128 participants; RR 1.40, 95% CI 1.14 to 1.71; moderate‐quality evidence), and produced fewer flares (1 study, 44 participants; RR 0.47, 95% CI 0.24 to 0.92; low‐quality evidence), but caused more adverse events (1 study, 129 participants; RR 1.65, 95% CI 1.16 to 2.34; moderate‐quality evidence).
Three studies assessed glycerol‐containing moisturiser versus vehicle or placebo. More participants in the glycerol group noticed skin improvement (1 study, 134 participants; RR 1.22, 95% CI 1.01 to 1.48; moderate‐quality evidence), which also included improved investigator‐assessed SCORAD scores (1 study, 249 participants; MD ‐2.20, 95% CI ‐3.44 to ‐0.96; high‐quality evidence), but the MID was unmet. Participant satisfaction was not addressed. The number of adverse events reported was not statistically significant (2 studies, 385 participants; RR 0.90, 95% CI 0.68 to 1.19; moderate‐quality evidence).
Four studies investigated oat‐containing moisturisers versus no treatment or vehicle. No significant differences between groups were reported for participant‐assessed disease severity (1 study, 50 participants; RR 1.11, 95% CI 0.84 to 1.46; low‐quality evidence), satisfaction (1 study, 50 participants; RR 1.06, 95% CI 0.74 to 1.52; very low‐quality evidence), or investigator‐assessed disease severity (3 studies, 272 participants; standardised mean difference (SMD) ‐0.23, 95% CI ‐0.66 to 0.21; low‐quality evidence). In the oat group, there were fewer flares (1 study, 43 participants; RR 0.31, 95% CI 0.12 to 0.7; low‐quality evidence) and reduced use of topical corticosteroids (2 studies, 222 participants; MD ‐9.30g, 95% CI 15.3 to ‐3.27; low‐quality evidence), but more adverse events (1 study, 173 participants; Peto odds ratio (OR) 7.26, 95% CI 1.76 to 29.92; low‐quality evidence).
We compared all moisturisers to placebo, vehicle, or no moisturiser. Participants considered moisturisers to be more effective for reducing eczema (5 studies, 572 participants; RR 2.46, 95% CI 1.16 to 5.23; low‐quality evidence) and itch (7 studies, 749 participants; SMD ‐1.10, 95% CI ‐1.83 to ‐0.38) than control. Participants in both treatment arms reported comparable satisfaction (3 studies, 296 participants; RR 1.35, 95% CI 0.77 to 2.26; low‐quality evidence). Moisturisers led to lower investigator‐assessed disease severity scores (12 studies, 1281 participants; SMD ‐1.04, 95% CI ‐1.57 to ‐0.51; high‐quality evidence) and fewer flares (6 studies, 607 participants; RR 0.33, 95% CI 0.17 to 0.62; moderate‐quality evidence), without a difference in adverse events (10 studies, 1275 participants; RR 1.03, 95% CI 0.82 to 1.30; moderate‐quality evidence).
Topical active treatment combined with moisturiser was more effective than active treatment alone in reducing investigator‐assessed disease severity scores (3 studies, 192 participants; SMD ‐0.87, 95% CI ‐1.17 to ‐0.57; moderate‐quality evidence) and flares (1 study, 105 participants; RR 0.43, 95% CI 0.20 to 0.93), and was preferred by participants (both low‐quality evidence). There was no clear difference in number of adverse events (1 study, 125 participants; RR 0.39, 95% CI 0.13 to 1.19; very low‐quality evidence). Participant‐assessed disease severity was not addressed.
Authors' conclusions
Most moisturisers showed some beneficial effects; prolonging time to flare, reducing the number of flares and the amount of topical corticosteroids needed to achieve similar reductions in eczema severity. Moisturisers combined with active treatment gave better results than active treatment alone. We did not find reliable evidence that one moisturiser is better than another.
Plain language summary
Emollients and moisturisers for eczema
Review question
Do emollients and moisturisers help control eczema?
Background
Eczema is a chronic (long‐lasting) skin disorder. Its main symptoms are dry skin and intense itching. Affected areas appear red, with crusts and scratches, and may ooze fluid. Moisturisers are considered important in eczema treatment, but there is uncertainty about how well they work, and whether any one moisturiser works better ‐ and is preferable ‐ to another.
Study characteristics
We searched the medical literature up to December 2015, and identified 77 relevant studies with 6603 participants, with mainly mild to moderate eczema. Participant age ranged from four months to 84 years (mean: 18.6 years). Most studies lasted between two and six weeks; a few lasted six months.
Forty‐six studies received funding from pharmaceutical companies.
Key results
Most moisturisers appeared to be effective. Twenty‐four studies reported participant‐assessed eczema severity. Only 13 studies assessed participant satisfaction with the moisturiser. Side effects (adverse events) were reported in 41 studies, although this information was often limited (mainly smarting, stinging, itch, redness). Most studies evaluated physician‐assessed severity of eczema (65 studies). Other outcomes addressed were skin barrier function (29 studies), flare prevention (16), quality of life (10), and corticosteroid use (8).
According to physicians, moisturisers reduced eczema severity compared with no moisturiser (3 studies), but the reduction was too small to be considered meaningful for patients. Moisturiser use resulted in fewer flares (2 studies), and reduced the need for topical corticosteroids (2 studies). Participant‐assessed eczema severity and satisfaction were not evaluated. There was no difference in the number of adverse events reported.
Participants thought Atopiclair (containing glycyrrhetinic acid) was more than four times more effective at improving eczema‐severity than the control (i.e. identical looking, but without glycyrrhetinic acid) (3 studies). However, physicians did not identify a meaningful difference for patients. Atopiclair led to greater reduction of itch (4 studies), more frequent participant satisfaction (2 studies), and fewer flares (3 studies). The number of reported adverse events was similar in each group.
Four studies evaluated urea‐containing cream. Participants using urea cream reported improvement more often than those using control (1 study). Satisfaction ratings in both groups were comparably positive (1 study). Urea‐containing cream improved dryness more often (physician assessment) (1 study) and led to fewer flares (1 study), but with more adverse events reported.
Three studies assessed glycerol‐containing moisturiser versus control. More participants in the glycerol group considered their skin to be improved (1 study), as did physicians, but these differences were not meaningful for patients. Participant satisfaction was not addressed. There was no difference in the number of adverse events reported.
Four studies investigated oat‐containing moisturisers versus no treatment or control. No differences between groups were observed for participant‐assessed improvement (1 study), participant satisfaction (1 study), or physician‐assessed improvement (3 studies). However, the oat group had fewer flares (1 study), and a reduced need for topical corticosteroids (2 studies). Oat creams caused more adverse events.
When we compared all moisturisers against no moisturiser or control, overall, participants considered moisturisers to be more than twice as effective in improving eczema than no moisturiser or control (5 studies), and more effective for itch (7 studies). Participants in both treatment arms reported comparable satisfaction (3 studies). According to physicians, moisturisers decreased eczema severity more than the control (12 studies), and led to fewer flares (6 studies). There were no differences between groups for the number of adverse events reported.
According to physicians, topical corticosteroids were more effective at improving eczema when used with a moisturiser, rather than used alone (3 studies), and also reduced the number of flares (1 study). This combination was also favoured by participants, though participant‐assessed disease severity was not addressed. There was no difference in the number of adverse events reported.
Quality of the evidence
There was high certainty evidence for physician‐assessed disease severity for glycerol‐containing creams versus control and all moisturisers versus control. For most other outcomes across comparisons, there was low to moderate certainty evidence. The most important reasons for lowering the certainty of evidence were risk of bias in studies (e.g. no blinding, or missing data), or too few participants, which leads to less precise results.
Summary of findings
Summary of findings 1. Moisturisers versus no treatment (no moisturiser).
| Moisturisers versus no moisturiser for eczema | ||||||
| Patient or population: people with eczema Setting: dermatology departments in hospitals Intervention: moisturisers Comparison: no treatment (no moisturiser) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with no moisturiser | Risk with moisturisers | |||||
| Change from baseline in disease severity according to participants ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| Participant satisfaction ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| Number of participants reporting an adverse event Follow‐up: mean 2 months | Study population | RR15.34 (0.90 to 261.64) | 173 (1 RCT) 1 | ⊕⊕⊝⊝ LOW2, 3 | 8/91 versus 0/82 reported an adverse event. Peto OR 7.26 (95% CI 1.76 to 29.92). 3 adverse events were reported to be mild, 3 moderate, and 2 were severe leading to treatment discontinuation. No adverse events were reported in the study of Simpson 2013 (within‐participant). |
|
|
1 per 100 (0.5/82)a |
9 per 100 (1 to100) |
|||||
| Change from baseline in disease severity as assessed by the investigators Assessed with: SCORAD Scale from: 0 to 103 (higher = worse) Follow‐up: range 4 weeks to 2 months | The mean change from baseline in disease severity as assessed by the investigators ranged from ‐2.4 to ‐19.5 | The mean change from baseline in disease severity as assessed by the investigators in the intervention group was 2.42 lower (4.55 lower to 0.28 lower) | ‐ | 276 (3 RCTs) 4 | ⊕⊕⊝⊝ LOW2, 5 | Reductions from baseline in Giordano‐Labadie 2006 and Grimalt 2007 met MID (= 8.7 Schram 2012) in both treatment arms. There was greater severity of disease in these studies than in Patrizi 2014. A MD of ‐2.42, although statistically significant, is not clinically important. |
| Number of participants who experienced a flare Follow‐up: mean 6 months | Study population | RR 0.40 (0.23 to 0.70) | 87 (2 RCTs) 6 | ⊕⊕⊝⊝ LOW2,7 | There were fewer flares in the moisturiser groups. The rate of flare in the control group was 3.74 times the rate in the moisturiser group (hazard ratio (HR) 3.74, 95% CI 1.86 to 7.50; P = 0.0002). | |
| 67 per 100 | 27 per 100 (15 to 47) | |||||
| Amount of corticosteroids used Follow‐up: range 6 weeks to 2 months | The mean amount of corticosteroids used ranged from 22.73 g to 62.1 g | The mean amount of corticosteroids used in the intervention group was 9.30 g less (15.30 g less to 3.27 g less) | ‐ | 222 (2 RCTs) 8 | ⊕⊕⊝⊝ LOW9, 10 | P = 0.003. There was a statistically significant difference showing that the use of moisturisers decreased the use of topical corticosteroids to achieve similar reductions in SCORAD. |
| Change from baseline in health‐related quality of life Assessed with: CDLQI (Giordano‐Labadie 2006), IDQOL (Grimalt 2007) Scale from: 0 to 30 Follow‐up: range 6 weeks to 2 months | ‐ | The mean change from baseline in health‐related quality of life in the intervention group calculated as the SMD was 0.15 lower (0.55 lower to 0.24 higher) | ‐ | 177 (2 RCTs) 8 | ⊕⊕⊝⊝ LOW2, 7 | There was no statistically significant difference in change from baseline of quality of life between the 2 treatment arms. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CDLQI: Children's Dermatology Life Quality Index; CI: confidence interval; IDQOL: Infant’s Dermatitis Quality of Life Index; MD: mean difference; MID: minimal important difference;OR: odds ratio; RR: risk ratio; SCORAD: scoring atopic dermatitis; SMD: standardised mean difference | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aWe had to put a value other than 0 in GRADEproGDT to calculate the risk with no moisturiser in relation to the RR, and we chose 0.5 (after discussion with the GRADE working Group). GRADEproGDT then calculates the risk with moisturiser.
2Downgraded one level due to high risk of bias because of performance and detection bias.
3Downgraded one level due to serious imprecision (wide confidence interval, low occurrence of events).
4Giordano‐Labadie 2006, Grimalt 2007, Patrizi 2014.
5Downgraded one level for serious inconsistency (I² = 68%), caused by Grimalt 2007.
7Downgraded one level for serious imprecision (small sample size).
8Giordano‐Labadie 2006, Grimalt 2007.
9Downgraded one level for serious inconsistency (I² = 68%). In the study of Giordano‐Labadie 2006, far more topical corticosteroids were used and the difference between the two arms was much larger.
10Downgraded one level for serious imprecision (wide confidence interval).
Summary of findings 2. Atopiclair versus vehicle.
| Atopiclair versus vehicle for eczema | ||||||
| Patient or population: people with eczema Setting: dermatology departments in hospitals Intervention: Atopiclair Comparison: vehicle | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with vehicle | Risk with Atopiclair | |||||
| Change from baseline in disease severity according to participants (number of participants who considered their skin to have improved) Assessed with: Likert scale, good improvement to total resolution Follow‐up: range 43 days to 50 days | Study population | RR 4.51 (2.19 to 9.29) | 390 (3 RCTs) 1 | ⊕⊕⊕⊝ MODERATE2 | Participants considered Atopiclair more effective than its vehicle. NNTB = 2, 95% CI 1 to 2 | |
| 17 per 100 | 77 per 100 (37 to 100) | |||||
| Participant satisfaction Follow‐up: mean 50 days | Study population | Not estimable | 248 (2 RCTs) 3 | ⊕⊕⊕⊝ MODERATE4 |
Abramovits 2008: 119/145 (Atopiclair) vs 28/73 (vehicle) wished to continue (RR 2.14, 95% CI 1.58 to 2.89; P < 0.00001; NNTB = 2; 95% CI 2 to 3). Belloni 2005: 5/15 vs 0/15 would use again (Peto OR 10.18, 95% CI 1.54 to 67.23; P = 0.02) |
|
| Not pooled | Not pooled | |||||
| Number of participants reporting an adverse event Follow‐up: range 43 days to 50 days | Study population | RR 1.03 (0.79 to 1.33) | 430 (4 RCTs) 5 | ⊕⊕⊕⊝ MODERATE6 | The number of participants reporting adverse events was not statistically different between the 2 groups. | |
| 33 per 100 | 34 per 100 (26 to 44) | |||||
| Change from baseline in disease severity according to the investigators Assessed with: EASI Scale from: 0 to 72 (higher = worse) Follow‐up: range 43 days to 50 days | The mean change from baseline in disease severity according to the investigators ranged from ‐1.7 to 0.84 | The mean change from baseline in disease severity according to the investigators in the intervention group was 4 lower (5.42 lower to 2.57 lower) | ‐ | 426 (4 RCTs) 5 | ⊕⊕⊕⊝ MODERATE7 | Although there is a statistically significant difference in favour of Atopiclair, the difference between the treatment group is not clinically important (MID EASI is 6.6 (Schram 2012)). |
| Number of participants who experienced a flare Follow‐up: range 43 days to 50 days | Study population | RR 0.18 (0.11 to 0.31) | 397 (3 RCTs) 8 | ⊕⊕⊕⊝ MODERATE9 | Participants in the Atopiclair group experienced fewer flares than the vehicle group (NNTB 3, 95% CI 3 to 5). | |
| 35 per 100 | 6 per 100 (4 to 11) | |||||
| Change in use of topical active treatment ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| Change from baseline in health‐related quality of life ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; EASI: Eczema Area Severity Index; MID: minimal important difference; NNTB: number needed to treat for an additional beneficial outcome; OR: odds ratio;RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1Abramovits 2008, Belloni 2005, Boguniewicz 2008.
2Downgraded one level for serious imprecision (wide confidence interval).
3Abramovits 2008, Belloni 2005.
4Downgraded one level for serious indirectness, as outcomes did not exactly match participant satisfaction.
5Abramovits 2008, Belloni 2005, Boguniewicz 2008, Patrizi 2008.
6Downgraded one level for serious imprecision (small sample size and CI includes no difference (1) and appreciable harm (1.25)).
7Downgraded one level for serious inconsistency (I² = 51%), caused by Boguniewicz 2008, which showed a larger effect size.
8Abramovits 2008, Boguniewicz 2008, Patrizi 2008.
9Downgraded one level for risk of bias (Abramovits 2008: high risk for attrition bias, Boguniewicz 2008: unclear risk of bias for allocation concealment blinding and incomplete outcome data, and Patrizi 2008: at unclear risk of bias due to incomplete outcome data).
Summary of findings 3. Urea‐containing moisturisers versus vehicle, placebo or no moisturiser.
| Urea‐containing moisturiser versus vehicle, placebo or no moisturiser for eczema | ||||||
| Patient or population: people with eczema Setting: dermatology departments in hospitals Intervention: urea‐containing moisturiser Comparison: vehicle, placebo or no treatment (no moisturiser) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with vehicle, placebo or no moisturiser | Risk with urea‐ containing moisturiser | |||||
|
Change from baseline in disease severity according to the participants (number of participants who considered their skin to have improved) Assessed with: Likert scale Follow‐up: mean 4 weeks |
Study population | RR 1.28 (1.06 to 1.53) | 129 (1 RCT) 1 | ⊕⊕⊝⊝ LOW2, 3 | P = 0.0009. NNTB = 5 (95% CI 3 to 18). Participants considered that urea‐containing moisturiser provided more improvement than placebo cream without urea. In Wilhelm 1998 (n = 77, within‐participant design), 61% considered that the side treated with urea cream showed moderate to very good improvement, and 48.1% felt the vehicle‐treated side showed moderate to very good improvement. |
|
| 70 per 100 | 89 per 100 (74 to 100) | |||||
|
Participant satisfaction Assessed with: Likert scale Follow‐up: mean 4 weeks |
‐ | 38 (1 RCT) 4, 5 |
⊕⊕⊝⊝ LOW6 | Smell, spreadability, penetration into the skin, and skin feel were assessed. None of these features were assessed as being better on the urea‐treated side than on the vehicle‐treated side. For details, see comparison 2b under Effects of interventions. | ||
| Number of participants reporting an adverse event Follow‐up: mean 4 weeks | Study population | RR 1.65 (1.16 to 2.34) | 129 (1 RCT) 1 | ⊕⊕⊕⊝ MODERATE3 | P = 0.005; NNTH = 4, 95% CI 2 to 11.There were fewer adverse events in the group treated with placebo cream. | |
| 39 per 100 | 65 per 100 (46 to 92) | |||||
|
Change from baseline in disease severity according to the investigators (number of participants who improved according to the investigators) Assessed with: DASI (Serup 1995) Follow‐up: mean 4 weeks |
Study population | RR 1.40 (1.14 to 1.71) | 129 (1 RCT) 1 | ⊕⊕⊕⊝ MODERATE3 | The assessments of the investigators were in line with the assessments of the participants. P = 0.001; NNTB = 4, 95% CI 3 to 9. The within‐participant study of Wilhelm 1998 demonstrated a mean of the paired differences of ‐0.57 (95% CI ‐1.14 to 0.0) in favour of urea moisturiser (lower score being better), and is more or less in line with the parallel‐design study of Lodén 2002. |
|
| 64 per 100 | 89 per 100 (73 to 100) | |||||
| Number of participants who experienced a flare Follow‐up: mean 6 months | Study population | RR 0.47 (0.24 to 0.92) | 44 (1 RCT) 7 | ⊕⊕⊝⊝ LOW3, 8 | P = 0.03; NNTB = 3, 95% CI 2 to 11 The rate of flare in the group that did not use a moisturiser was 3.2 times the rate in the group treated with urea cream (HR 3.2, 95% CI 1.3 to 7.8; P < 0.01). |
|
| 68 per 100 | 32 per 100 (16 to 63) | |||||
| Change in use of topical active treatment ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| Change from baseline in health‐related quality of life ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; DASI: dry skin area and severity index; RR: risk ratio; HR: hazard ratio; NNTB: number needed to treat for an additional beneficial outcome; NNTH: number needed to treat for one additional harmful outcome | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
2Downgraded one level for serious indirectness, the study of Lodén 2002 had a parallel study design and the study of Wilhelm 1998 had a within‐participant design.
3Downgraded one level for serious imprecision (small sample size).
5Within‐participant design.
6Downgraded two levels for very serious imprecision (very small sample size).
8Downgraded one level for risk of bias as Wirén 2009 was assessed as at high risk of bias as the study was not blinded.
Summary of findings 4. Glycerin/glycerol‐containing moisturisers versus vehicle or placebo.
| Glycerin/glycerol‐containing moisturiser versus vehicle or placebo for eczema | ||||||
| Patient or population: people with eczema Setting: dermatology departments in hospitals Intervention: glycerin/glycerol‐containing moisturiser Comparison: vehicle or placebo | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with vehicle or placebo | Risk with glycerol‐containing moisturiser | |||||
| Change from baseline in disease severity as assessed by the participants (number of participants who considered their dry skin to have improved) Assessed with: Likert scale Follow‐up: mean 4 weeks | Study population | RR 1.22 (1.01 to 1.48) | 134 (1 RCT) 1 | ⊕⊕⊕⊝ MODERATE2 | Participants considered glycerol‐containing moisturiser more effective for improving dry skin than placebo cream (P = 0.03; NNTB = 6, 95% CI 3 to 60) | |
| 70 per 100 | 85 per 100 (70 to 100) | |||||
| Participant satisfaction ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| Number of participants reporting an adverse event Follow‐up: mean 4 weeks | Study population | RR 0.90 (0.68 to 1.19) | 385 (2 RCTs) 3 | ⊕⊕⊕⊝ MODERATE4 | The adverse events were mild to moderate and consisted of smarting, erythema, pruritus, or burning. | |
| 35 per 100 | 32 per 100 (24 to 42) | |||||
| Change from baseline in disease severity as assessed by the investigators Assessed with: SCORAD Scale from: 0 to 103 (higher = worse) Follow‐up: mean 4 weeks | The mean change from baseline in disease severity as assessed by the investigators was ‐3.1 | The mean change from baseline in disease severity as assessed by the investigators in the intervention group was 2.2 lower (3.44 lower to 0.96 lower) | ‐ | 249 (1 RCT) 5 | ⊕⊕⊕⊕ HIGH | P = 0.0005, but does not meet the MID (which is 8.2 for objective SCORAD (Schram 2012)). The study of Breternitz 2008 had a within‐participant design and confirmed these data. The mean of the paired differences was ‐1.10, CI 95% ‐1.63 to ‐0.57. In Lodén 2002, in the glycerol group 58/68 showed improvement in 'dryness' of the skin versus 42/66 in the vehicle group (RR 1.34, 95% CI 1.09 to 1.65; P = 0.0006, NNTB 5, 95% CI 3 to 14) |
| Number of participants who experienced a flare ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| Change in use of topical active treatment ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| Change from baseline in health‐related quality of life ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MID: minimal important difference; NNTB: number needed to treat for an additional beneficial outcome; RR: risk ratio; SCORAD: scoring atopic dermatitis | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
2Downgraded one level for serious imprecision (lower bound of CI approaches 1).
3Lodén 2002 and Boralevi 2014.
4Downgraded one level for serious imprecision (small sample size and CI includes appreciable benefit (0.75) and no difference (1)).
Summary of findings 5. Oat‐containing moisturisers versus vehicle or no moisturiser.
| Oat‐containing moisturiser versus vehicle or no moisturiser | ||||||
| Patient or population: people with eczema Setting: dermatology departments in hospitals Intervention: oat‐containing moisturiser Comparison: vehicle or no treatment (no moisturiser) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with vehicle or no moisturiser | Risk with oat‐containing moisturiser | |||||
|
Change from baseline in disease severity as assessed by the participants (number of participants who considered their skin to have improved) Assessed with: Likert scale Follow‐up: mean 8 weeks |
Study population | RR 1.11 (0.84 to 1.46) | 50 (1 RCT) 1 | ⊕⊕⊝⊝ LOW2 | P = 0.45. Participants did not consider that the oat‐containing moisturiser was more effective than the control treatment (occlusive vehicle). | |
| 76 per 100 | 84 per 100 (64 to 100) | |||||
| Participant satisfaction Assessed with: number of participants who agreed via a questionnaire Follow‐up: mean 8 weeks | Study population | RR 1.06 (0.74 to 1.52) | 50 (1 RCT) 1 | ⊕⊝⊝⊝ VERY LOW3, 4 | P = 0.76. Participants were not more satisfied with oat‐containing moisturiser than with the occlusive vehicle. | |
| 68 per 100 | 72 per 100 (50 to 100) | |||||
| Number of participants reporting an adverse event Follow‐up: mean 6 weeks | Study population | RR 15.34 (0.90 to 261.64) | 173 (1 RCT) 7 | ⊕⊕⊝⊝ LOW5, 6 | 8/91 versus 0/82 reported an adverse event. Peto OR 7.26 (95% CI 1.76 to 29.92). 3 adverse events were reported to be mild, 3 moderate, and 2 severe leading to treatment discontinuation. | |
| 1 per 100 (0.5/82)a | 9 per 100 (1 to 100) | |||||
| Change from baseline in disease severity as assessed by the investigators Assessed with: SCORAD and EASI Follow‐up: range 6 weeks to 8 weeks | ‐ | The mean change from baseline in disease severity in the intervention group calculated as the SMD was 0.23 lower (0.66 lower to 0.21 higher) | ‐ | 272 (3 RCTs) 8 | ⊕⊕⊝⊝ LOW9, 10 | P = 0.30. There was no statistically significant difference according to the investigators between the 2 treatment arms. |
| Number of participants who experienced a flare Follow‐up: mean 6 months | Study population | RR 0.31 (0.12 to 0.77) | 43 (1 RCT) 11 | ⊕⊕⊝⊝ LOW5, 12 | P = 0.01; NNTB = 2, 95% CI 1 to 5. The HR for rate of flare was 4.74 (95% CI 1.57 to 14.34; P = 0.006) in favour of the oat‐containing cream. | |
| 65 per 100 | 20 per 100 (8 to 50) | |||||
| Total amount of topical corticosteroids used Follow‐up: range 6 weeks to 2 months | The mean total amount of topical corticosteroids used ranged from 22.73 g to 62.1 g | The mean total amount of topical corticosteroids used in the intervention group was 9.3 g lower (15.3 g less to 3.27 g less) | ‐ | 222 (2 RCTs) 13 | ⊕⊕⊝⊝ LOW14, 15 | P = 0.003. There is a statistically significant difference showing that the use of moisturisers decreased the use of topical corticosteroids to achieve similar reductions in disease severity. |
| Change from baseline in health‐related quality of life Assessed with: CDLQI (Giordano‐Labadie 2006), IDQOL (Grimalt 2007), DLQI (Nebus 2009) Scale from: 0 to 30 (higher = worse) Follow‐up: range 6 weeks to 2 months | ‐ | The mean change from baseline in health‐related quality of life in the intervention group calculated as the SMD was 0.09 lower (0.37 lower to 0.19 higher) | ‐ | 226 (3 RCTs) 8 | ⊕⊕⊝⊝ LOW16, 17 | There was no statistically significant difference in change from baseline in quality of life between the 2 treatment arms. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; CDLQI: Children's Dermatology Life Quality Index; DLQI: Dermatoloqy Quality of Life Index; EASI: Eczema Area and Severity Index; HR: hazard ratio; IDQOL: Infant’s Dermatitis Quality of Life Index; MID: minimal important difference;NNTB: number needed to treat for an additional beneficial outcome; OR: odds ratio; RR: risk ratio; SCORAD: scoring atopic dermatitis; SMD: standardised mean difference | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aWe had to put a value other than 0 in GRADEproGDT to calculate the risk with no moisturiser in relation to the RR, and we chose 0.5 (after discussion with the GRADE working Group). GRADEproGDT then calculates the risk with moisturiser.
2Downgraded two levels level for very serious imprecision (small sample size and CI includes no effect (1) and appreciable benefit (1.25)).
3Downgraded one level for serious indirectness as the outcome was more about soothing and calming of the skin and not really participant satisfaction.
4Downgraded two levels for very serious imprecision as the CI includes both no effect, and benefit of both oat‐containing cream as well as of the vehicle.
5Downgraded one level for risk of bias because of performance and detection bias.
6Downgraded one level for serious imprecision (wide confidence interval, low occurrence of events).
8Giordano‐Labadie 2006, Grimalt 2007, Nebus 2009.
9Downgraded one level for serious inconsistency (I² = 65%), caused by Giordano‐Labadie 2006, which was the study showing a favourable result for the oat‐containing creams whilst the other studies showed no difference between the treatment arms.
10Downgraded one level for serious imprecision; the CI creates uncertainty with the effect, ranging from moderate effect to small harmful effect.
11Weber 2015.
12Downgraded one level for serious imprecision (small sample size).
13Giordano‐Labadie 2006 and Grimalt 2007.
14Downgraded one level for serious inconsistency (I² = 68%). In the study of Giordano‐Labadie 2006, far more topical corticosteroids were used and the difference between the two arms was much larger.
15Downgraded one level for serious imprecision (wide confidence interval).
16Downgraded one level for serious risk of bias because of performance, detection, and attrition bias.
17Downgraded one level for serious imprecision (the CI creates uncertainty with the effect, ranging from small effect to small harmful effect).
Summary of findings 6. All moisturisers compared to vehicle, placebo or no moisturiser for eczema.
| All moisturisers compared to vehicle, placebo or no moisturiser for eczema | ||||||
| Patient or population: people with eczema Setting: dermatology departments in hospitals Intervention: all moisturisers Comparison: vehicle, placebo or no moisturiser | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with vehicle, placebo or no moisturiser | Risk with all moisturisers | |||||
| Change from baseline in disease severity as assessed by the participants (number of participants who considered their skin to have improved) Assessed with: Likert scale Follow‐up: range 4 weeks to 8 weeks | Study population | RR 2.46 (1.16 to 5.23) | 572 (5 RCTs) 1 | ⊕⊕⊝⊝ LOW2, 3 | Participants considered the use of a moisturiser to be more effective than vehicle/placebo or no moisturiser. P = 0.02, NNTB = 2, 95% CI 2 to 3 | |
| 37 per 100 | 91 per 100 (43 to 100) | |||||
| Participant satisfaction Assessed with: Likert scale Follow‐up: range 6 weeks to 8 weeks | Study population | RR 1.35 (0.77 to 2.36) | 298 (3 RCTs) 4 | ⊕⊕⊝⊝ LOW5, 6 | P = 0.29. According to the participants, there was no difference between the 2 treatment arms for this outcome. Results are supported by the within‐participant study (Bohnsack 1997). | |
| 48 per 100 | 65 per 100 (37 to 100) | |||||
| Number of participants reporting an adverse event Follow‐up: range 4 weeks to 6 months | Study population | RR 1.03 (0.82 to 1.30) | 1275 (10 RCTs) 7 | ⊕⊕⊕⊝ MODERATE8 | There was no statistically significant difference in number of participants experiencing an adverse event. | |
| 23 per 100 | 24 per 100 (19 to 30) | |||||
| Change from baseline in disease severity as assessed by the investigators Assessed with: EASI, SCORAD, objective SCORAD Follow‐up: range 4 weeks to 6 months | ‐ | The mean change from baseline in disease severity as assessed by the investigators in the intervention group calculated as the SMD was 1.04 lower (1.57 lower to 0.51 lower) | ‐ | 1281 (12 RCTs) 9 | ⊕⊕⊕⊕ HIGH10 | P < 0.0001 The investigators considered the use of moisturisers to be more beneficial than the vehicle, placebo, or no moisturiser. However, clinical impact was unclear. |
| Number of participants who experienced a flare Follow‐up: range 6 weeks to 6 months | Study population | RR 0.33 (0.17 to 0.62) | 607 (6 RCTs) 11 | ⊕⊕⊕⊝ MODERATE12 | P = 0.006; NNTB = 4, 95% CI 3 to 5. The rate of flare in the control group was 3.74 times the rate in the moisturiser group based on Weber 2015 and Wirén 2009 (HR 3.74, 95% CI 1.86 to 7.50; P = 0.0002 in favour of moisturiser). | |
| 41 per 100 | 13 per 100 (7 to 25) | |||||
| Total amount of topical corticosteroids used Follow‐up: range 6 weeks to 2 months | The mean amount of corticosteroids used ranged from 22.73 g to 62.1 g | The mean amount of corticosteroids used in the intervention group was 9.30 g less (15.30 g less to 3.27 g less) | ‐ | 222 (2 RCTs) 13 | ⊕⊕⊝⊝ LOW3, 14 | P = 0.003. There was a statistically significant difference showing that the use of moisturisers decreased the use of topical corticosteroids to achieve similar reductions in eczema severity. |
| Change from baseline in health‐related quality of life Assessed with: CDLQI, IDQOL and DFI Scale from: 0 to 30 Follow‐up: range 6 weeks to 6 months | ‐ | The mean change from baseline in health‐related quality of life in the intervention group calculated as the SMD was 0.39 lower (0.9 lower to 0.12 higher) | ‐ | 300 (3 RCTs) 15 | ⊕⊕⊝⊝ LOW16, 17, 18 | The effect on quality of life ranges from a moderate effect on quality of life in favour of moisturisers to no difference between the groups. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CDLQI: Children's Dermatology Life Quality Index; CI: confidence interval; DFI: Dermatitis Family Impact; EASI: Eczema area and severity index; HR: hazard ratio; IDQOL: Infant’s Dermatitis Quality of Life Index; MID: minimal important difference;NNTB: number needed to treat for an additional beneficial outcome; RR: risk ratio; SCORAD: scoring atopic dermatitis; SD: standard deviation; SMD: standardised mean difference | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1Abramovits 2008, Belloni 2005, Boguniewicz 2008, Lodén 2002, Nebus 2009.
2Downgraded one level for inconsistency (I² = 95%), which was in part caused studies by studies at risk for attrition bias (Abramovits 2008 and Boguniewicz 2008).
3Downgraded one level for serious imprecision (wide confidence interval).
4Abramovits 2008, Belloni 2005, Nebus 2009.
5Downgraded one level for serious inconsistency (I² = 83%). All heterogeneity was removed when a study at high risk of bias was excluded (Abramovits 2008); we did not double count for risk of bias.
6Downgraded one level for serious imprecision (CI interval includes no effect (1) and appreciable benefit (1.25)).
7Abramovits 2008, Belloni 2005, Boguniewicz 2008, Boralevi 2014, Gayraud 2015, Grimalt 2007, Korting 2010, Lodén 2002, Patrizi 2008, Tan 2010.
8Downgraded one level for imprecision (CI interval included no difference (1) and appreciable harm (1.25)).
9Abramovits 2008, Belloni 2005, Boguniewicz 2008, Boralevi 2014, Gayraud 2015, Giordano‐Labadie 2006, Grimalt 2007, Korting 2010, Nebus 2009, Patrizi 2008, Patrizi 2014, Tan 2010.
10We did not downgrade for inconsistency as all sensitivity analyses show a clear positive effect of moisturisers.
11Abramovits 2008, Boguniewicz 2008, Gayraud 2015, Patrizi 2008, Weber 2015, Wirén 2009.
12Downgraded one level for serious inconsistency (I² = 73%), which was caused by the studies at unclear to high risk of bias showing better results.
13Giordano‐Labadie 2006, Grimalt 2007.
14Downgraded one level for serious inconsistency (I² = 68%). In the study of Giordano‐Labadie 2006, far more topical corticosteroids were used and the difference between the two arms was much larger.
15Gayraud 2015, Giordano‐Labadie 2006, Grimalt 2007.
16We did not downgrade for risk of bias, as, although there was attrition bias in Grimalt 2007, it did not impact the overall result, and even reduced the direction of effect.
17Downgraded one level for serious inconsistency (I² = 79%), it might have no effect at all, signal around 0.
18Downgraded one level for serious imprecision (CI includes moderate effect in favour of moisturisers as well as no difference).
Summary of findings 7. Licochalcone‐containing moisturiser versus hydrocortisone acetate 1% cream for eczema.
| Licochalcone‐containing moisturiser versus hydrocortisone acetate1% cream for eczema | ||||||
| Patient or population: people with eczema Setting: dermatology departments in hospitals Intervention: licochalcone‐containing moisturiser Comparison: hydrocortisone acetate 1% cream | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with hydrocortisone acetate 1% cream | Risk with licochalcone‐containing moisturiser | |||||
| Change from baseline in disease severity according to participants ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| Number of participants who rated treatment satisfaction as good to excellent Assessed with: Likert scale Follow‐up: mean 4 weeks | ‐ | ‐ | ‐ | 30 (1 RCT) 1 | ⊕⊕⊝⊝ LOW2, 3 | On both treatment sides, 22/30 participants rated their satisfaction good to excellent with no difference between either side. |
| Number of participants reporting an adverse event Follow‐up: range 1 weeks to 4 weeks | ‐ | ‐ | ‐ | 18 (1 RCT) 4 | ⊕⊕⊝⊝ LOW5, 6 | Both Udompataikul 2011 and Wanakul 2013 reported no adverse events on any side during the study. Side effects in Angelova‐Fischer 2014 (within‐participant study) were skin tightness, itch, and scaling on both sides. 9 side effects were reported on each forearm (n = 18). |
| Change from baseline in disease severityas assessed by the investigators Assessed with: SCORAD Scale from: 0 to 103 (higher = worse) Follow‐up: range 1 weeks to 4 weeks | The mean disease severity as assessed by the investigators ranged from ‐3.50 to ‐21.29 | The mean disease severity as assessed by the investigators in the intervention group was 0.08 higher (1.96 lower to 2.13 higher) | ‐ | 96 (3 RCTs) 4 | ⊕⊕⊝⊝ LOW7, 8 | There was no statistically significant difference between the 2 treatments, which is in accordance with the data for participant satisfaction. |
| Number of participants who experienced a flare Follow‐up: mean 4 weeks | ‐ | ‐ | ‐ | 30 (1 RCT) 1 | ⊕⊕⊝⊝ LOW9, 10 | 3/30 experienced a flare on the side treated with licochalcone and 6/30 on the contralateral side treated with hydrocortisone acetate 1%. |
| Change in use of active topical treatment ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| Change from baseline in quality of life ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio; RR: risk ratio; SCORAD: scoring atopic dermatitis | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1Within‐participant study Udompataikul 2011.
2We did not downgrade for detection bias as the participants were not blinded, but they considered treatments equally satisfactory.
3Downgraded two levels for serious imprecision (very small sample size).
4Within‐participant study Angelova‐Fischer 2014.
5Not downgraded for risk of bias (participants in Angelova‐Fischer 2014 and Udompataikul 2011 were not blinded) as there was no difference between the both treatment arms regarding reporting adverse events.
6Downgraded two levels for very serious imprecision (very small sample size).
7We did not downgrade for detection bias as investigators were blinded.
8Downgraded two levels for very serious inconsistency (I² = 85%); it could benefit both treatments. We therefore did not downgrade further for imprecision. Differences in study duration, and, in Angelova‐Fischer 2014, only forearms were treated.
9Downgraded one level for serious imprecision (small sample size and as we downgraded for risk of bias, we only downgraded once for imprecision for this outcome).
10Downgraded one level for risk of bias (no blinding of participants).
Summary of findings 8. Vehicle treatment + daily moisturiser compared to fluticasone propionate twice weekly + daily moisturiser.
| Vehicle treatment + daily moisturiser compared to fluticasone propionate twice weekly + daily moisturiser for eczema | ||||||
| Patient or population: people with eczema Setting: dermatology departments in hospitals Intervention: vehicle treatment + daily moisturiser Comparison: fluticasone propionate twice weekly + daily moisturiser | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with fluticasone propionate twice weekly + moisturiser | Risk with vehicle treatment + moisturiser | |||||
| Change from baseline in disease severity as assessed by the participants (number of participants reporting good to excellent result) Follow‐up: mean 20 weeks | Study population | RR 0.45 (0.34 to 0.59) | 348 (1 RCT) 1 | ⊕⊕⊕⊕ HIGH | NNTB = 3, 95% CI 2 to 3, in favour of fluticasone propionate twice weekly + daily moisturiser | |
| 71 per 100 | 32 per 100 (24 to 42) | |||||
| Participant satisfaction ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| Number of participants reporting an adverse event Follow‐up: range 16 weeks to 20 weeks | Study population | RR 0.51 (0.22 to 1.14) | 718 (4 RCTs) 2 | ⊕⊕⊝⊝ LOW3, 4 | Although there was a trend favouring the vehicle treatment + daily moisturiser, the 2 comparisons of Berth‐Jones 2003 implied that they might be equally safe (no adverse events in either group). | |
| 22 per 100 | 11 per 100 (5 to 25) | |||||
| Change from baseline in disease severityas assessed by the investigators Assessed with: Objective SCORAD Scale from: 0 to 83 Follow‐up: mean 16 weeks | 75 (1 RCT)5 |
⊕⊕⊕⊝ MODERATE6 | There were reporting inconsistencies in the paper between the data table and text regarding the increase in SCORAD in the twice‐weekly fluticasone propionate + daily moisturiser group. These were reported as 7.1 in the table and as 3.8 in the text. In the vehicle + daily moisturiser group, the increase was 12.2 in both table and text. |
|||
| Number of participants who experienced a flare Follow‐up: range 16 weeks to 20 weeks | Study population | RR 2.17 (1.51 to 3.11) | 718 (4 RCTs) 2 | ⊕⊕⊕⊝ MODERATE7 | NNTB = 3, 95% CI 2 to 3. Twice‐weekly fluticasone propionate combined with moisturiser resulted in fewer flares than moisturiser alone. HR of rate of flare 3.69, 95% CI 1.80 to 7.55 in favour of fluticasone propionate twice weekly + daily moisturiser | |
| 28 per 100 | 61 per 100 (43 to 88) | |||||
| Change in use of topical active treatment ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| Change from baseline in quality of life ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; HR: hazard ratio; NNTB: number needed to treat for an additional beneficial outcome; RR: risk ratio; SCORAD: scoring atopic dermatitis | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
2Berth‐Jones 2003 (two comparisons), Glazenburg 2009, Hanifin 2002.
3Downgraded one level for serious inconsistency (I² = 67%); as there were no adverse events in both comparisons in Berth‐Jones 2003 in both treatment arms, they could be equally safe.
4Downgraded one level for serious imprecision (CI includes appreciable benefit and no difference).
5Glazenburg 2009 (See 'Comments').
6Downgraded one level for serious imprecision (small sample size).
7Downgraded one level for serious inconsistency (I² = 72%).
Summary of findings 9. Topical active treatment in combination with moisturiser compared to topical active treatment alone.
| Topical active treatment in combination with moisturiser compared to topical active treatment alone for eczema | ||||||
| Patient or population: people with eczema Setting: dermatology departments in hospitals Intervention: active treatment in combination with moisturiser Comparison: active treatment alone | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with active treatment alone | Risk with active treatment in combination with moisturiser | |||||
| Change from baseline in disease severity according to participants ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| Participant satisfaction Follow‐up: range 3 weeks to 4 weeks | ‐ | ‐ | 201 (2 RCTs) 1 2 | ⊕⊕⊝⊝ LOW3, 4 | Hanifin 1998: 96% of 78 preferred the combination treatment and just 4% the active treatment 'only'. Simpson 2011: 84.3% to 96.7% of 123 felt that the addition of the RestoraDerm to the routine use of their topical steroids "reduces inflammation, relieves dry and itchy skin, provides long lasting hydration, leaves skin protected and maintains healthy skin". | |
|
Number of participants reporting an adverse event Follow‐up: mean 3 weeks |
Study population | RR 0.39 (0.13 to 1.19) | 125 (1 RCT) 5 | ⊕⊝⊝⊝ VERY LOW6, 7, 8 | Draelos 2008: no adverse events. Hanifin 1998 (within‐participant): 10 participants reported burning and stinging on the side treated with desonide 0.05% combined with moisturiser versus 11 on the other side treated with only desonide 0.05%. | |
| 16 per 100 | 6 per 100 (2 to 19) | |||||
| Change from baseline in disease severity as assessed by the investigators Assessed with: SCORAD (Msika 2008); EASI (Wu 2014) Follow‐up: mean 3 weeks | ‐ | The mean change from baseline in disease severity as assessed by the investigators in the intervention group calculated as the SMD0.87 lower (1.17 lower to 0.57 lower) | ‐ | 192 (3 RCTs) 9 | ⊕⊕⊕⊝ MODERATE10 | According to the assessments of the investigators, adding a moisturiser to topical active treatment is more effective than topical active treatment alone. |
| Number of participants who experienced a flare Follow‐up: mean 3 weeks | Study population | RR 0.43 (0.20 to 0.93) | 105 (1 RCT) 5 | ⊕⊕⊝⊝ LOW11, 12 | Adding a moisturiser to active treatment reduced the number of flares (NNTB = 6, 95% CI 3 to 57). | |
| 31 per 100 | 13 per 100 (6 to 29) | |||||
| Change in amount of use topical active treatment ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | This outcome was not assessed in any of the studies. |
| Change from baseline in health‐related quality of life Assessed with: IDQOL Scale from: 0 to 30 follow‐up: mean 3 weeks | The mean change from baseline in health‐related quality of life ranged from ‐2.07 to ‐3.17 | The mean change from baseline in health‐related quality of life in the intervention group was 1.31 lower (2.7 lower to 0.09 higher) | ‐ | 67 (2 RCTs) 13 | ⊕⊕⊝⊝ LOW12, 14 | The study duration of 3 weeks was short; there was no difference in changes from baseline in quality of life between the 2 treatment groups. Results of DFI confirmed this (MD ‐1.03, 95% CI ‐2.47 to 0.42) |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; DFI: Dermatitis Family Impact; EASI: Eczema Area and Severity Index; IDQOL: Infant’s Dermatitis Quality of Life Index; RR: risk ratio; SCORAD: scoring atopic dermatitis; SMD: standardised mean difference | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1Within‐participant design.
3Downgraded one level for serious risk of detection bias (no blinding of participants).
4Downgraded one level for serious indirectness as in both studies satisfaction was not really assessed.
5Wu 2014.
6Downgraded one level for risk of bias. Hanifin 1998 and Wu 2014 were assessed as being at a high risk of bias.
7Downgraded one level for serious indirectness for different reporting on adverse events including outcome definitions.
8Downgraded one level for serious imprecision (small sample size, too few adverse events, and wide CI).
9Msika 2008 (2 comparisons), Wu 2014.
10Downgraded one level for risk of bias (no blinding of outcome assessors).
11Downgraded one level for risk of bias (attrition bias (17/62) in the control group).
12Downgraded one level for serious imprecision (small sample size).
13Msika 2008 (2 comparisons).
14Downgraded one level for risk of bias (no blinding of participants).
Background
We have listed relevant terms in the glossary of terms in Table 10.
1. Glossary of terms.
| Term | Definition |
| Adverse events | Unwanted side effects of using medication |
| Allergic contact dermatitis | A form of eczema after contact with a substance (an allergen) that produces (elicits) an immune‐mediated response in the skin |
| Allergic rhinitis | 'Hay fever': inflammation of the nose caused by allergens such as house dust mite, animals, pollen. Symptoms include sneezing, itchiness in the nose, watery eyes, runny or blocked nose |
| Ameliorate | Improve, to make something (such as a problem) better |
| Atopy | The individual's genetic predisposition to develop allergic reactions such as eczema, allergic rhinitis and asthma. Atopy often involves production of IgE antibodies against allergens such as, for example, house dust mite, animals, grass and tree pollen, and food proteins. |
| Bacteria | Also referred to as germs, bacteria are tiny micro‐organisms that are invisible to the eye. They are found everywhere and can be harmful, e.g. causing infections, or helpful, e.g. aiding digestion of food |
| Ceramides | Lipid (fatty) molecules found in the lipid bilayer of the intercellular matrix (see `Intercellular lipid matrix' below) |
| Colonisation | The point at which an Infection begins, when an organism successfully enters the body, grows and multiplies |
| Control | The alternative treatment, placebo, or absence of treatment against which the intervention of interest in the review is compared |
| Corneodesmosomes | Any of a class of proteins that hold corneocytes (cells in the epidermis, or outer layers of the skin) together; their degradation leads to desquamation (see 'Desquamation' below) |
| DASI | Dry skin area and severity index: a tool used to evaluate dryness and severity of dry skin (Serup 1995) |
| Desquamation | Skin peeling |
| Dizygotic | Non‐identical twins, i.e. twins formed from two different eggs fertilised by separate sperm cells, are referred to as dizygotic. |
| DLQI | Dermatology Life Quality Index: an assessment tool to evaluate the impact of eczema and its treatment on quality of life (Finlay 1994) |
| EASI | Eczema Area and Severity Index: a tool used to measure the extent (area) and severity of eczema (Hanifin 2001) |
| Emollients | The terms `emollients' and `moisturisers' are often used interchangeably. But, since 'emollient' sometimes refers to a specific ingredient that soothes the skin, it is more appropriate to use the term 'moisturiser'. Emollients are included within ointments, creams, lotions, gels, bath oils and sprays, and are used to keep the skin soft and supple and reduce scaling. Application to the skin reduces water loss by covering it with a protective film. They can be used frequently and might ease itching |
| Epidermis | The outermost layers of cells in the skin which consist mainly of keratinocytes that mature to become corneocytes |
| Exacerbation | Periods of worsening the symptoms and signs of eczema |
| Excoriation | Abrasion, scratched skin |
| Extensor | The opposite site of a flexure point, i.e. the outer side of, for example elbow, knee or wrist |
| Filaggrin | An epidermal barrier protein |
| Flare | Periods of worsening of eczema symptoms and signs, or escalation in use of medication (Thomas 2015) |
| Flexural dermatitis | Eczema at the flexure points (inner sides) of elbow, knees, wrists, groin and armpits |
| Gene | Part of DNA that encodes a protein involved in body function |
| Genome‐wide linkage study | An established tool to map inherited diseases |
| Humectant | Substance or product that is 'water loving' and draws water towards it |
| Hygroscopic | Absorbing water |
| Hypersensitivity | An exaggerated immune response toward an allergen (for example pollen, house dust mite, but also for contact allergens such as nickel and fragrances) |
| IgE (immunoglobulin E) | A class of antibody that is important in defence against parasitic disease, and plays a key role in the disease process of allergic diseases. People with eczema often have an increased level of IgE in their blood |
| Immune response | The process through which the body identifies and defends itself against bacteria, viruses and other harmful agents |
| Intercellular lipid matrix | Space surrounding corneocytes with stacked layers of lipids |
| Lesion | A region or area of damaged skin |
| Lesional | Concerning lesions, or accompanied by lesions |
| Lichenification | Skin thickening |
| Moisturisers | Ointments, creams, lotions, gels, bath oils and sprays that are used to keep the skin soft and supple and reduce scaling. Application to the skin reduces water loss and covers it with a protective film. Moisturisers can be used frequently and might ease itching. |
| Monozygotic | Identical twins, i.e. twins who develop from a single fertilised egg (zygote) that splits to form two identical embryos, are referred to as monozygotic (in contrast to dizygotic twins (see above)). |
| Objective | Something observed and verified by physician or investigator by visible physical signs or laboratory tests (i.e. based on facts, not emotions or feelings) |
| Objective‐ SCORAD | Objective ‐ SCORing Atopic Dermatitis is a clinical scoring system, that uses the SCORAD system and excludes subjective symptoms, which cannot be measured accurately, such as daytime itching (pruritus) and sleep loss (Kunz 1997) |
| Occlusive | Describes an agent or process that seals something off |
| Over‐the‐counter (OTC) medicines | Medicines that can be bought without a prescription |
| Papulovesicular | Relating to an eruption of papules (clearly defined (circumscribed), solid elevations of skin with no visible fluid) and vesicles (small fluid‐filled sacs on the skin) |
| Pathogenesis | Origin of disease and how it develops |
| Pathognomonic biomarker | A specific indicator for a disease |
| Photochemotherapy (PUVA) | PUVA is a combination treatment of a drug (psoralen) with ultraviolet A (UVA) light. The psoralen makes the skin temporarily more sensitive to the ultraviolet light |
| Phototherapy | Treatment with ultraviolet light (UVB or UVA) |
| Placebo | A 'dummy' or fake medicine that has no expected benefit. In this review placebo means, in accordance with the terminology used by the investigators, a moisturiser without the ingredient considered to be the most beneficial, and so, of a different composition than the moisturiser being studied. Use of placebo treatments allows patients and staff to be blinded, as the placebo and active treatments appear the same, so it is impossible to tell which has been used. |
| POEM | The Patient Oriented Eczema Measure is a self‐assessment tool for monitoring eczema severity, based on signs and symptoms (Charman 2004) |
| PO‐SCORAD | The Patient‐Oriented SCORing Atopic Dermatitis (PO‐SCORAD) index is a self‐assessment score for patients to evaluate their eczema, based on subjective and objective criteria from the SCORAD (see also SCORAD below) (Stalder 2011) |
| Preservative | A natural or synthetic ingredient added to products such as foods, pharmaceuticals, paints, biological samples, wood, etc. which help to prevent decomposition caused by microbial growth or by undesirable chemical changes |
| Propylene glycol | Propylene glycols attract water and by enhancing skin penetration they behave as moisturisers to improve the appearance of the skin |
| Protease | An enzyme that breaks down proteins (via proteolysis) |
| Pruritus | Itch |
| Quality of life | The general well‐being of individuals and societies. Health‐Related Quality of Life (HRQoL) looks at quality of life in relation to health |
| QoLIAD | Quality of Life Index for Atopic Dermatitis (QoLIAD). An assessment tool to evaluate the impact of eczema and its treatment on quality of life (Whalley 2004) |
| Remission | A temporary or permanent decrease or absence of the symptoms and signs of disease activity |
| Sensitisation | Exposure to an allergen that results in the development of hypersensitivity, i.e. an increased or disproportionate response to the allergen |
| SCORAD‐index | An assessment tool used by clinicians to evaluate the extent and severity of eczema (SCORing Atopic Dermatitis) (European Task Force on Atopic Dermatitis 1993) |
| Staphyloccocus aureus | A type of bacterium that is often found on the skin |
| Subjective | Something experienced by the participant not perceived by the investigator or physician |
| TEWL | Trans‐epidermal water loss (TWL or TEWL) is the quantity of water that diffuses through and evaporates from the epidermis |
| Topical corticosteroid | Corticosteroids applied to the skin; these are effective in controlling inflammation and used to treat eczema and many other skin conditions |
| Urea | Urea absorbs water, helps to reduce the amount of water lost though the skin and increases skin penetration of other substances. It softens the horny layer and also has anti‐itch (anti‐pruritic) properties. |
| Vehicle | In this review 'vehicle' means a moisturiser that has the same composition as the studied moisturiser, but lacks the ingredient that is considered to be the most beneficial |
| Volar | The inside surface of the forearm, i.e. the same side as the palm of the hand |
| Xerosis | Dry skin |
Description of the condition
Definition
Atopic eczema, which is also known as atopic dermatitis, eczema, flexural eczema or neurodermatitis, is a chronic inflammatory skin disease that can present with frequent spontaneous flares and remissions (Bos 2010; Eichenfield 2014a; Weidinger 2016). It is a heterogeneous, highly variable skin disease with a broad range of presentations, and is characterised principally by dry skin, intense itching, and inflammatory skin lesions (Andersen 2015; Bieber 2008; Weidinger 2016). Atopic eczema has a typical age‐related distribution (Möhrenschlager 2006), and in all of the age categories, itching can result in sleep deprivation and have a considerable impact on quality of life (Bieber 2008; Weidinger 2016).
There is long‐standing and continuing debate as to whether atopic eczema is truly atopic (Flohr 2004; Flohr 2008; Williams 2005; Williams 2006). Atopy is associated with an increased level of immunoglobulin E (IgE) antibodies against common inhaled allergens (sensitisation) (Flohr 2004), but there does not seem to be an absolute relationship between IgE levels and atopic dermatitis, as the percentage of people with atopic dermatitis that show allergic sensitisation to aeroallergens varies widely from 30% to 80% (Eichenfield 2014a; Flohr 2004; Flohr 2008). The development of atopic eczema followed by the development of allergic sensitisation, asthma or food allergy is often called the 'atopic march' (Boguniewicz 2011; Eichenfield 2014a), but this is not a universal occurrence (Eichenfield 2014a; Williams 2006), and it has been postulated that the sequence might even be reversed (such as the onset of asthma before the onset of eczema) (Dharmage 2014). We will use the term 'eczema' throughout the review in agreement with the 'Revised nomenclature for allergy for global use' (Johansson 2004).
Epidemiology
A number of recent studies have reported that the lifetime prevalence of eczema at the global level continues to show a steady but measurable increase (Flohr 2014; Nutten 2015; Weidinger 2016). These findings largely concur with an earlier systematic review of epidemiological studies, covering the period 1990 to 2010, which concluded that although there was "no consistent overall global trend", prevalence has increased in some parts of the world (Deckers 2012; Haileamlak 2005). In an investigation into whether childhood eczema prevalence was on the increase worldwide, researchers evaluated data from Phases One (1991 to 2002) and Three (1999 to 2004) of the International Study of Asthma and Allergies in Childhood (ISAAC), and reported that "the epidemic of eczema seems to be levelling or decreasing in some countries with previously high prevalence rates" (Odhiambo 2009; Williams 2008). It is generally recognised that the limitations and reliability of most of these epidemiological data are in part dependent on the complexities associated with assessing global trends over time, as well as on the diversity of outcome and diagnostic measures used to gather the data (Flohr 2009).
Prevalence rates vary between and within countries and are reported to range between 15% and 30% in children, and between 2% and 10% in adults (Bieber 2008; Mack Correa 2012; Silverberg 2013). Most of these data have been derived from questionnaires; however, the validity and reliability of using questionnaires to obtain prevalence data for eczema in non‐English speaking and low‐ and middle‐income countries has recently been questioned (Flohr 2009; Hogewoning 2012).
The first manifestations of eczema usually occur in early infancy, with approximately 60% of cases developing during the first year of life (Bieber 2008; Eichenfield 2014a; Nutten 2015; Weidinger 2016), and with up to 90% of individuals experiencing an onset of eczema before the age of five (Bieber 2008; Eichenfield 2014a; Nutten 2015). However, eczema can also develop in adult life (late‐onset eczema) (Bieber 2008; Eichenfield 2014a). Several studies have reported that up to 70% of affected children have either a resolution or a marked improvement of their eczema before adolescence (Bieber 2008; Eichenfield 2014a; Weidinger 2016). The recent PEER study (Pediatric Eczema Elective Registry), which consisted mainly of children with mild to moderate eczema, also indicated that eczema probably does not resolve fully in the majority of children who have it to a mild or moderate degree, but is most likely a lifelong disease (Margolis 2014).
Eczema constitutes a major public health issue, and was ranked as the skin condition with the highest burden of disease expressed as disability‐adjusted life years (DALYs) in the Global Burden of Disease Study 2010 (Murray 2012). Furthermore, it has been estimated that the overall economic costs associated with eczema are not dissimilar to those for asthma (Jenner 2004; Nutten 2015; Williams 2005).
Symptoms
The cardinal features of eczema are dry skin and intense itch accompanied by persistent subsequent scratching, which become part of a continuous itch‐scratch cycle (Bieber 2008; Eichenfield 2014a). In addition, the presence of red, irritated, scaly patches on the skin that sometimes become infected, coupled with sleep disturbances and difficulties concentrating at school and at work, can have a significant impact on the quality of life of affected individuals (Lewis‐Jones 2006; Nutten 2015).
Risk factors and aetiology
Although the precise aetiology is yet to be determined conclusively, a number of potential risk factors and possible causative associations have been acknowledged for eczema (Bieber 2008; Eichenfield 2014a; Weidinger 2016). Genetic and environmental factors have been implicated and remain a continuing subject of debate, as does the lack of certainty regarding the balance of impact of these risk factors, and whether they should be considered as interdependent, cumulative or sequentially independent (Cork 2009; Flohr 2008; Flohr 2014). Indeed, it remains unclear how the increased prevalence can be explained by genetic factors alone, and whether these increases in prevalence may reflect more recent changes at an environmental level that appear to have a key role in the disease process (Cork 2006).
Genetic risk factors, which have been evaluated in several observational studies, showed a higher concordance rate in monozygotic (identical) twins than dizygotic (fraternal) twins (Bieber 2008; Nutten 2015), and people with a family history of atopic disease are at increased risk of developing eczema (Boguniewicz 2011; Eichenfield 2014a). Discussion of candidate gene association studies and genome‐wide linkage studies, as well as the concepts of innate and adaptive immunity is beyond the scope of this review, but more information can be found in the literature (Bieber 2008; Boguniewicz 2011; Weidinger 2016).
Important genetic risk factors have been identified and are the focus of ongoing research. The most significant of these are loss‐of‐function mutations in the filaggrin gene (FLG), which has the propensity to influence skin barrier function and transepidermal water loss (TEWL) (Flohr 2014; Palmer 2006). When the skin barrier functions normally it prevents water loss through the skin, and also protects against the penetration of irritants, allergens and pathogenic microbes (Elias 2014; Moncrieff 2013). Filaggrin is a key protein in epidermal differentiation, and is therefore crucial for skin barrier integrity (Nutten 2015; Palmer 2006). This protein, which is expressed in the outer layers of the epidermis, has multiple functions, one of which is hydration of the stratum corneum (Elias 2014; Kezic 2008). Filaggrin is degraded into hygroscopic, free amino acids, some of which generate natural moisturising factors (NMF) that maintain epidermal hydration (Kezic 2008; Moncrieff 2013). However, not all people suffering from eczema appear to have FLG mutations, and not all people with FLG mutations have eczema (Eichenfield 2014a; Nutten 2015). Further breakdown of the skin barrier can be caused by proteases ‐ enzymes normally involved in homeostasis and restoration of the skin barrier ‐ in the stratum corneum. Protease levels are increased in people with eczema (by genetic and environmental factors) (Cork 2006; Elias 2014). Proteases released by the bacterium Staphylococcus aureus (S aureus) can also add measurably to the disruption of the skin barrier and enhance microbial invasion (Cork 2009; Elias 2014). While the skin of 5% to 30% of people without eczema is colonised with S aureus, colonisation occurs in 60% to 100% of people with eczema (Petry 2013). In addition, the toxins produced by S aureus can exacerbate skin inflammation, and contribute to disease severity (Bieber 2008; Chung 2008; Elias 2011; Petry 2013).
Recent findings in skin biology suggest that skin barrier defects might be a crucial initiator of disease activity in eczema (Palmer 2006; Simpson 2014). Researchers and eczema experts continue to debate whether impaired barrier function is secondary to the inflammatory response in people with eczema (inside‐outside hypothesis) (Leung 2000), or if xerosis, caused by barrier dysfunction, should be considered to be the driver of disease activity (outside‐inside hypothesis) (Chamlin 2002; Cork 2006; Elias 2011; Elias 2014). The stratum corneum is central to the normal functioning of the skin barrier. In people with eczema, both lesional skin and non‐lesional skin demonstrate a reduced barrier function (Janssens 2012; van Smeden 2014b). Skin barrier function is largely dependent on the intercellular lipid matrix in the stratum corneum, which is composed of corneocytes (dead, flattened cells containing NMF), which are protected externally by a cornified cell envelope and are surrounded by a lipid matrix in what has been described as a 'bricks and mortar' structure (Caussin 2008; Rawlings 2014; van Smeden 2014b). The 'bricks' are held together by corneodesmosomes and the intercellular matrix (lipid bilayers) (Rawlings 2014; van Smeden 2014b, respectively). This lipid matrix consists of free fatty acids, ceramides and cholesterol. Studies have demonstrated that in eczema the amount, concentration, and chain length of ceramide and free fatty acids ‐ as well as the organisation of the lipids within the matrix ‐ are altered; and the amount of lipids is reduced in both lesional and non‐lesional skin (Elias 2014; Janssens 2012; van Smeden 2014a; van Smeden 2014b). In healthy skin, three components regulate hydration by inhibiting water loss: the intercellular lipid matrix, the fully matured corneocytes bound by the corneodesmosomes, and the NMF within the corneocytes (Rawlings 2005; Rawlings 2014). Skin barrier disruption in people with eczema makes the skin more susceptible to the penetration of allergens, irritants and microbes (Boguniewicz 2011; Flohr 2014; van Smeden 2014a). Furthermore, TEWL is increased when skin barrier function is impaired, and people with eczema demonstrate elevated TEWL in both lesional and non‐lesional skin (Janssens 2012; van Smeden 2014b).
Environmental factors such as aeroallergens, microbial exposure, diet, climate, antibiotics, smoking, pollution, skin irritants, hard water, improved hygiene, and number of siblings have also been implicated in the development of eczema (Eichenfield 2014a; Hogewoning 2010; Flohr 2014; Lee 2007; Mack Correa 2012).
Clinical findings and diagnosis
Three age‐related clinical phases can be observed for eczema (Bieber 2008; Möhrenschlager 2006; Weidinger 2016). The infantile phase is characterised by the appearance of lesions on the cheeks and scalp, but the whole body may be affected (Bieber 2008; Weidinger 2016). In childhood, the flexural areas of the knee and elbows are generally affected, but the wrists, ankles and buttocks can also be involved (Bieber 2008; Weidinger 2016). In adolescents and adults, the neck and face are most commonly affected, with a more diffuse scaling, erythema, and lichenification (Bieber 2008; Weidinger 2016). In people with a dark skin type (i.e. Asians, Carribeans or Africans) there is a predilection more often for the extensor surfaces to be affected instead of the flexor surfaces and "discoid (circular) or follicular (around hair follicles) patterns may be more common" (NICE 2007). Also, the severity of erythema might be more difficult to assess in darker skin types.
In the acute stage, eczema is characterised clinically by itching, diffuse redness, oozing papulovesicular lesions and crusts, and is often accompanied by secondary infection with S aureus (Mack Correa 2012; Weidinger 2016; Williams 2005). The chronic stage is typified by lichenification, excoriations and very dry skin with a more specific involvement of the elbow and knee folds, wrists, ankles, face and neck (Möhrenschlager 2006; Williams 1994).
Physical examination continues to be the best way to diagnose eczema because diagnosis is based on an array of clinical findings, and there is no single pathognomonic biomarker that can be used to make the diagnosis (Andersen 2015; Eichenfield 2014a; Weidinger 2016; Williams 2005). The most frequently used clinical criteria for the diagnosis of eczema are those developed by Hanifin and Rajka in 1980 (Hanifin 1980). These criteria are based on clinical experience and were developed via a consensus approach. The UK Diagnostic Criteria for Atopic Dermatitis Working Party has refined the criteria of Hanifin and Rajka further by developing a core set of six diagnostic criteria, which are especially suitable for use in epidemiological and clinical studies (Eichenfield 2014a; Williams 1994; Williams 1996).
Description of the intervention
Management strategies for eczema include both active treatments that address the inflammatory lesions and adjunctive therapies to optimise skin barrier function and prevent flare‐ups (Eichenfield 2014a; Eichenfield 2014b; Ring 2012a). Further recommended measures include advice on: bathing practices; avoidance of triggers such as irritants (e.g. wool, soap), allergens (such as aeroallergens, food allergens, contact allergens), environmental factors (e.g. humidity), and non‐irritating clothing; together with education about eczema, its treatments and how to apply these (Eichenfield 2014b; Ring 2012a; Sidbury 2014a; Weidinger 2016).
Topical corticosteroids are still the cornerstone of anti‐inflammatory therapy in the management of eczema (Eichenfield 2014b; Ring 2012a). However, under‐use of topical corticosteroids ‐ out of a fear of skin thinning or possible growth retardation ‐ are well‐known problems (Charman 2000). Other frequently used topical anti‐inflammatory treatments include coal tar applications and topical calcineurin inhibitors (non‐steroidal immune modulators) such as tacrolimus and pimecrolimus (Eichenfield 2014b; Ring 2012a). The beneficial effects of sunlight for eczema are well recognised, and so phototherapy or photo(chemo)therapy are periodically used as an alternate form of treatment (Ring 2012b; Sidbury 2014b). Systemic immunosuppressive treatments such as ciclosporin, mycophenolate mofetil, methotrexate, azathioprine, and systemic steroids (used in the short term for severe flares) are mainly indicated in people with moderate to severe eczema that does not respond sufficiently well to topical treatments and phototherapy (Haeck 2011; Ring 2012b; Sidbury 2014b). Antimicrobials can be used to treat infected eczema, but preferably only in the short term, as this treatment may foster the development of antibiotic resistance, and thus far, there is no reliable evidence of a beneficial effect when it is used in non‐infected eczema (Bath‐Hextall 2010; Eichenfield 2014b). Although antihistamines are widely prescribed for people with eczema, there is a lack of evidence that they reduce itching (van Zuuren 2014). However, sedative antihistamines may prove useful for improving sleep (Sidbury 2014b).
Some other interventions for eczema have been covered by other Cochrane Reviews (Apfelbacher 2013; Ashcroft 2007; Bamford 2013; Bath‐Hextall 2008; Bath‐Hextall 2010; Bath‐Hextall 2012; Birnie 2002; Boyle 2006; Cury Martins 2015; Ersser 2014; Gu 2013; Nankervis 2015), while some topics are under development and currently published as protocols (Calderon 2010; Futamura 2014; Jadotte 2014; Küster 2015; Moed 2012).
Emollients and moisturisers
The terms 'emollient' and 'moisturiser' are used interchangeably and lack consistency in their use in the literature (Penzer 2012). However, in essence an emollient is an ingredient of a moisturiser (Rawlings 2004). Therefore, it would be more appropriate to use the term 'moisturiser', and this will be used throughout this review.
As dry skin (xerosis) is the most important disease feature for eczema, skin moisturisation may constitute an integral part of standard treatment for all severities of eczema (Bieber 2008; Eichenfield 2014b). Moisturising the skin might be sufficient to control mild eczema, but could also form part of the treatment regimen for more severe eczema, and may have a role in the possible prevention of eczema flare‐ups (Eichenfield 2014b; Moncrieff 2013; Sidbury 2014a; Weber 2015).
The functions of moisturisers are to reduce the dryness of skin, decrease TEWL, improve comfort and reduce itch (Lodén 2012; Rawlings 2004). Moisturising components can be hydrophilic or lipophilic (Caussin 2008; Caussin 2009a). Hydrophilic components are predominantly important for skin hydration (Caussin 2008), whilst lipophilic components are designed to remain on the surface of the skin as an occlusive (waterproofing) layer that prevents evaporation of water and assists barrier recovery (Caussin 2008). Moisturisers can include humectants (e.g. urea, glycerol, lactic acid) which help increase the attraction and retention of water by the stratum corneum; occlusives (e.g. petrolatum, mineral oil, dimethicone) that form a layer on the skin surface and prevent TEWL; and emollients (lanolin, glycerol stearate, glyceryl stearate, soy sterols) to soften the skin and make it smoother (Eichenfield 2014b; Lodén 2003; Lodén 2012; Rawlings 2004). Recently, the notional term 'prescription emollient devices' (PED) was introduced; this is a class of topical agents developed to "target specific defects in skin barrier function" in people with eczema (Eichenfield 2014b). These PEDs contain various mixtures and ratios of lipids, ceramides, fatty acids, and natural anti‐inflammatory agents such as glycyrrhetinic acid, as well as other ingredients to alleviate itching and inflammation (Mack Correa 2012).
Studies to evaluate the use of moisturisers in primary prevention of eczema in high risk (atopic) families have been conducted, and are ongoing, but these are beyond the scope of our review (e.g. Kvenshagen 2014; Simpson 2010; Simpson 2014).
There are a number of different formulations of moisturisers, such as oil‐in‐water creams, water‐in‐oil creams, ointments, lotions, oils, gels, sprays and emulsions, and the choice of formulation used will depend on the severity of the skin condition and the patient's preferences (Eichenfield 2014b; Lodén 2003). Furthermore, moisturisers can be categorised as leave‐on (directly applied) moisturisers, soap substitutes and bath moisturisers. In this review we will focus on the leave‐on moisturisers.
Usually moisturisers need to be applied two to three times a day (Eichenfield 2014b), in amounts of up to "150‐200 g per week in young children and up to 500g in adults" (Ring 2012a). It is preferable to apply moisturisers after bathing (Eichenfield 2014b). The repetitive application of topical treatments is time consuming, and the use of adequate amounts of moisturiser is often restricted due to cost, especially since there is no reimbursement in most countries (Nutten 2015; Ring 2012a; Williams 2005). Possible side effects include irritation and contact allergy for certain ingredients (Eichenfield 2014b; Lodén 2003; Lodén 2012; Ring 2012a). The ideal moisturiser should be pleasant to use, restore the skin barrier and soften skin effectively, avoid additives that can irritate or sensitise ‐ such as fragrance and perfume ‐ and contain just a few ingredients (Eichenfield 2014b; Weidinger 2016).
How the intervention might work
Since Palmer 2006, a growing understanding that gene‐expressed skin barrier impairment may play a key role in the pathogenesis of eczema has reinforced the importance of developing specific treatments with the capacity to either restore barrier function or to ameliorate further damage, or both (Boguniewicz 2011; Elias 2014; Moncrieff 2013).
Moisturisers are directed towards improving the skin barrier function by delivering lipids and water to the stratum corneum (Lodén 2003; Moncrieff 2013; Simpson 2010). Restoring barrier function might also improve antimicrobial defence in the skin of people with eczema, and so have a beneficial effect on disease activity (Elias 2014). Moisturisers containing hydrophilic components mostly include low‐molecular‐weight hygroscopic substances such as glycerol and urea. It is assumed that, because of their low molecular weight, these substances penetrate the stratum corneum, where they subsequently act as humectants (Sagiv 2003), mimicking the role of NMF (Caussin 2008). Moisturisers containing more lipophilic components include compounds that are water insoluble, such as fatty acids, waxes, and triglycerides (Caussin 2009a). These are unlikely to penetrate the skin due to their high molecular weight (Caussin 2009a), so serve as occlusive agents that prevent TEWL. However, if they penetrate into the stratum corneum, they may restore barrier function by interacting with the lipid matrix (Caussin 2009b; Ghadially 1992). Although adjuvant constituents such as ceramides, cholesterol and fatty acids may be included in moisturisers, it is unclear if these actually improve the efficacy of the moisturisers (Moncrieff 2013).
Why it is important to do this review
Severe eczema remains difficult to treat and some of the treatments offered can be problematic and associated with adverse side effects (Eichenfield 2014b; Ring 2012a; Ring 2012b; Sidbury 2014b). Moisturisers are widely prescribed as the basis of eczema management, as they are relatively inexpensive, have a favourable safety profile, and can improve the appearance and symptoms of the dry skin (xerosis) (Eichenfield 2014b; Moncrieff 2013; NICE 2007; Ring 2012a; SIGN 2011). However, their application is time consuming ‐ possibly a life‐long requirement ‐ and moisturisers can be smelly, messy and stick to clothing (Eichenfield 2014b). Some preparations are known to cause skin reactions such as stinging and burning, which can result in poor adherence, while others may contain sensitising ingredients, which can lead to contact dermatitis (Eichenfield 2014b; Lodén 2003; Lodén 2012; Ring 2012a). The use of moisturisers still fails to meet the expectations of people with eczema (Rawlings 2014; Santer 2013; Santer 2016).
A perceived advantage of moisturiser use is that it may restrict the need to use topical corticosteroids to more severe eczema only, or during exacerbations and flare‐ups, while at the same time improving disease control (Harcharik 2014; Lucky 1997; Moncrieff 2013; Msika 2008; Weber 2015). Moisturisers may also reduce the number of flares (Moncrieff 2013; Sidbury 2014a), which we hope to confirm with this review. At present it is not clear which, if any, moisturiser is effective at particular body sites, and whether one moisturiser is preferable to another according to people with eczema.
The plans for this review were published as a protocol with the title 'Emollients and moisturisers for eczema' (van Zuuren 2016).
Objectives
To assess the effects of moisturisers for eczema.
Methods
Criteria for considering studies for this review
Types of studies
We have only included randomised controlled trials (RCTs).
Types of participants
People of any age with a clinical diagnosis of eczema (or 'atopic eczema' or 'atopic dermatitis') as diagnosed by a dermatologist, physician or other specialist healthcare practitioner using the standardised diagnostic criteria of Hanifin and Rajka (Hanifin 1980), the UK Working Party's diagnostic criteria for atopic dermatitis (Williams 1994), or other recognised diagnostic criteria.
We excluded trials where the participants suffered from other types of eczema such as contact dermatitis, nummular eczema or dyshidrotic eczema.
Types of interventions
All types of moisturisers alone or in combination versus:
active treatment e.g. topical corticosteroids;
another moisturiser;
'placebo' moisturiser (moisturiser, but with a different composition and without the assumed effective ingredient);
vehicle (has same composition as the moisturiser it is compared with, but without the assumed effective ingredient);
combination of moisturiser and active treatment;
or no treatment.
Types of outcome measures
Acronyms are included in the glossary of terms in Table 10. We have searched the website of Core Outcome Measures in Effectiveness Trials (COMET) (www.comet-initiative.org) to help us define some of the outcomes. A full set of core outcome measures has not yet been defined, although the Eczema Area and Severity Index (EASI), the objective SCORing Atopic Dermatitis (SCORAD) scale, and the Patient Oriented Eczema Measure (POEM) are the scales recommended for use in studies (Schmitt 2007; Schmitt 2014).
Primary outcomes
Change in disease severity from baseline as assessed by study participants using a recognised or validated rating scale (e.g. POEM and Patient Oriented SCORAD (PO‐SCORAD)), visual analogue scale (VAS) score, Likert scale, or similar scale. If data were available we evaluated change in scores for itch separately.
Participant satisfaction using any generic Likert scale or similar scale.
Adverse events (proportion of participants reporting an adverse event); we reviewed the nature of adverse events (e.g. itching, stinging, sensitisation) and reported them narratively.
Secondary outcomes
Change in disease severity from baseline as assessed by investigators using a recognised or validated rating scale (e.g. SCORAD and EASI), VAS score, Likert scale, or similar scale.
Prevention of flares (measured as time to first flare).
Change in use of topical active treatment (e.g. corticosteroids or topical immune modulators, tar).
Changes in skin barrier function as assessed by TEWL.
Change in health‐related quality of life (HRQoL) using a recognised or validated rating scale (e.g. the Dermatology Life Quality Index (DLQI), Children’s DLQI, and the Quality of Life Index for Atopic Dermatitis (QoLIAD)).
Timing of outcomes
We considered measurements taken for up to one week to be short‐term; between one and four weeks to be medium‐term; and after four weeks to be long‐term. We reported end of study data, and there were no other data that could be cohesively grouped into other specific time periods.
Outcomes for 'Summary of findings' tables
We produced 'Summary of findings' tables for the main comparisons that included the following outcomes (listed according to priority):
participant‐assessed change in disease severity from baseline;
participant satisfaction;
adverse events;
investigator‐assessed change in disease severity from baseline;
prevention of flares;
change in use of topical active treatment;
change in HRQoL.
We produced these tables using the GRADEpro GDT program.
Search methods for identification of studies
We aimed to identify all relevant randomised controlled trials (RCTs) regardless of language or publication status (published, unpublished, in press, or in progress).
Electronic searches
We searched the following databases up to 17 December 2015:
the Cochrane Skin Specialised Register using the search strategy in Appendix 1;
the Cochrane Central Register of Controlled Trials (CENTRAL; 2015, Issue 11, in the Cochrane Library) using the strategy in Appendix 2;
MEDLINE via Ovid (from 1946) using the strategy in Appendix 3;
Embase via Ovid (from 1974) using the strategy in Appendix 4; and
LILACS (Latin American and Caribbean Health Science Information database, from 1982) using the strategy in Appendix 5.
We searched the Global Resource of EczemA Trials (GREAT database) on 21 December 2015 using the strategy in Appendix 6. GREAT is produced by the Centre of Evidence Based Dermatology, and accessed at: www.greatdatabase.org.uk.
Trials registers
Two review authors (EvZ and ZF) searched the following trials registers on 16 February 2016 using the following search terms: 'eczema', 'emollient', 'ointment', 'cream', 'moisturizer' and 'moisturiser':
the ISRCTN registry (www.isrctn.com/);
ClinicalTrials.gov (www.clinicaltrials.gov);
the Australian New Zealand Clinical Trials Registry (www.anzctr.org.au);
the World Health Organization International Clinical Trials Registry Platform (apps.who.int/trialsearch/); and
the EU Clinical Trials Register (www.clinicaltrialsregister.eu).
Searching other resources
References from published studies
Two review authors (EvZ and ZF) examined the bibliographies of the included and excluded studies for further references to potentially eligible studies.
Adverse effects
We did not perform a separate search for adverse effects of the target intervention. However, we examined and reported the data on adverse effects from the included studies.
Correspondence
Trial investigators were contacted (by EvZ and ZF) and asked to provide missing data or clarify study details (see Table 11).
2. Contact with investigators.
| Study ID | Response | Additional | Comment |
| Abramovits 2008 | Emails sent: 26 June 2014, 7 February 2016, 12 February 2016, 26 February 2016, 12 March 2016, 19 March 2016, to dra@dermcenter.us Regarding allocation concealment and method of blinding Replies received: 24 March 2016 with responses; 29 March 2016 with additional information |
Yes | ‐ |
| Angelova‐Fischer 2014 | Emails sent: 13 February 2016, 26 February 2016, to irena.angelova‐fischer@uk‐sh.de Regarding sequence generation and allocation concealment Reply received: 1 March 2016 with response to sequence generation Several emails sent regarding allocation concealment, but this remains unclear |
Yes | ‐ |
| Belloni 2005 | stefano.veraldi@unimi.it no need to contact, but this is recent email for future update of the review | Not applicable | ‐ |
| Berents 2015 | Email sent: 13 February 2016, to t.l.berents@medisin.uio.no Regarding sequence generation and allocation concealment Email received: 15 February 2016 with responses |
Yes | ‐ |
| Berth‐Jones 2003 | Emails sent: 13 February 2016, 26 February 2016, to johnberthjones@aol.com Regarding method of blinding Email received: 27 February 2016 with responses |
Yes | ‐ |
| Bissonnette 2010 | Emails sent: 12 May 2014, 14 June 2014, 21 January 2016, to rbissonnette@innovaderm.ca and sophie.seite@loreal.com Regarding sequence generation, allocation concealment and method of blinding Replies received: 2 February 2015 and 15 February 2016; received all responses and additional material |
Yes | ‐ |
| Boguniewicz 2008 | Emails sent: 14 February 2016, 26 February 2016, 12 March 2016, 19 March 2016, to boguniewiczm@njhealth.org. Also did not reply to questions about the Abramovits 2008 study Regarding allocation concealment and method of blinding, EASI scores at day 43 and subjects/care givers assessment of global response at day 43 in vehicle group No reply received |
Not applicable | ‐ |
| Boralevi 2014 | Emails sent: 15 February 2016, 26 February 2016, 12 March 2016, 26 March 2016, to franck.boralevi@chu‐bordeaux.fr Regarding P‐VAS scores, SCORAD, Objective SCORAD, and HI at day 28 as well as SDs Replies received: 31 March 2016 and 5 April 2016 responses and additional information |
Yes | ‐ |
| Breternitz 2008 | Emails sent: May 2014, 15 February 2016, to elsner@derma‐jena.de and joachim.fluhr@charite.de Regarding sequence generation, allocation concealment and method of blinding, mean SCORAD, TEWL, capacitance and SDs Replies received: 16 May 2014 and 15 February 2016, received responses and additional information |
Yes | ‐ |
| Danby 2011 | Emails sent: 15 February 2016, 26 February 2016, 15 March 2016, 19 March 2016, to s.danby@sheffield.ac.uk Regarding sequence generation, allocation concealment, method of blinding, TEWL values and SDs after 2 weeks, number of dropouts, numbers of male/female and age of participants Reply received: 22 March 2016 with responses to our questions |
Yes | ‐ |
| De Belilovsky 2011 | Email sent: 16 February 2016 to philippe.msika@airliquide.com and clarence.de‐belilovsky@wanadoo.fr Regarding allocation concealment and method of blinding Replies received: 24 February 2016 and 12 March 2016 from cbaudouin@expanscience.com and bernard@clinreal.com, with responses to our questions |
Yes | ‐ |
| Draelos 2008 | Emails sent: 16 February 2016, 12 March 2016, 19 March 2016, 26 March 2016, to zdraelos@northstate.net Regarding allocation concealment and method of blinding No reply received |
Not applicable | ‐ |
| Draelos 2009 | Emails sent: 19 February 2016, 12 March 2016, 19 March 2016, 26 March 2016, to zdraelos@northstate.net Regarding allocation concealment and method of blinding, more precise baseline data and data at end of study means and SDs No reply received |
Not applicable | ‐ |
| Draelos 2011 | Emails sent: 19 February 2016, 12 March 2016, 19 March 2016, 26 March 2016, to zdraelos@northstate.net Regarding sequence generation, allocation concealment, method of blinding, precise baseline data and data at end of study, means and SDs, Participant assessments of target site skin appearance for redness, peeling, dryness, stinging/burning, and overall skin irritation, sponsoring and declaration of interest No reply received |
Not applicable | ‐ |
| Emer 2011 | Emails sent: 5 March 2016, 12 March 2016, 19 March 2016, 26 March 2016 to Jason Emer (email not current anymore), with last 2 emails to A Frankel (afrankelmd@gmail.com) Regarding sequence generation, allocation concealment, method of blinding, colour version of pdf and SDs at week 4 No reply received |
Not applicable | ‐ |
| Faergemann 2009 | Emails sent: 7 March 2016, 12 March 2016, to jan.faergemann@derm.gu.se Regarding sequence generation, allocation concealment, method of blinding, more precise data Reply received: 12 March 2015 "it is so long time ago that I performed this study so I do not remember. I retired last November 2015 and I do not have assess to any data now." |
No | ‐ |
| Gayraud 2015 | Email sent 9 March 2016 to e.jourdan@bioderma.com Regarding sequence generation, allocation concealment, method of blinding and incomplete data Reply received: 14 March 2014 with responses to our questions |
Yes | ‐ |
| Giordano‐Labadie 2006 | Email sent: 13 May 2014 to giordano.labadie.f@chu‐toulouse.fr, frederic.cambazard@chu‐st‐etienne.fr, gerard.guillet@chu‐poitiers.fr, patrick.combemale@lyon.unicancer.fr, and valerie.mengeaud@pierre‐fabre.com Regarding sequence generation and allocation concealment Reply received: 26 May 2014 with responses to our questions |
Yes | ‐ |
| Glazenburg 2009 | Emails sent:14 March 2016, 19 March 2016, 26 March 2016, 3 April 2016, to a.oranje@inter.nl.net Regarding allocation concealment, method of blinding and inconsistencies in text page 64 and table 1 No reply received |
Not applicable | ‐ |
| Grimalt 2007 | Email sent: 13 April 2014, to grimalt@ub.edu, frederic.cambazard@chu‐st‐etienne.fr, valerie.mengeaud@pierre‐fabre.com Regarding sequence generation and allocation concealment Reply received: 24 June 2015, after several emails we received responses to everything we asked for |
Yes | ‐ |
| Hagströmer 2006 | Email sent: 17 April 2016, to lena.hagstromer@karolinska.se (no longer correct, no more recent email, so sent again to lennart.emtestam@medhs.ki.se, but this is also no longer correct) Regarding sequence generation, allocation concealment and baseline data for TEWL and corneometry No recent email addresses could be found |
Not applicable | ‐ |
| Hamada 2008 | We could not find a current email address of any of the authors listed | Not applicable | ‐ |
| Hlela 2015 | Emails sent: 18 March 2016, 26 March 2016, 3‐4 February 2016,10 April 2016, to n.khumalo@uct.ac.za Regarding sequence generation and allocation concealment, frequency of use, precise data after 3 months (means and SDs), more data on adverse events No reply received |
Not applicable | ‐ |
| Janmohamed 2014 | Emails sent: 19 March 2016, 26 March 2016, 3 April 2016, to a.oranje@inter.nl.net Regarding allocation concealment, method of blinding, exact data for POEM and quality of life at baseline, and SCORAD, POEM and quality of life at day 28 No reply received |
Not applicable | ‐ |
| Jirabundansuk 2014 | Emails sent: 8 January 2016, 24 January 2016, 12 February 2016, 8 April 2016, 18 April 2016, to umontree@yahoo.com Regarding sequence generation and allocation concealment No reply received |
Not applicable | ‐ |
| Kircik 2009 | Email sent: 19 March 2015, to wedoderm@yahoo.com Regarding full text publication Reply received: 21 March 2015, Principal investigator could not remember anymore |
No | ‐ |
| Kircik 2014 | Email sent: 19 March 2015, to wedoderm@yahoo.com Regarding sequence generation, allocation concealment, method of blinding, exact TEWL values and corneometry with SDs at week 4 Reply received: 21 March 2016 with responses to some of our questions, the rest was no longer accessible |
Yes and No | We did not receive exact data |
| Korting 2010 | Email sent: 20 March 2016, to H.C.Korting@lrz.uni‐muenchen.de Regarding allocation concealment and blinding Email address is no longer correct, and further searches showed that he died in 2012. None of the other authors could be contacted |
Not applicable | ‐ |
| Laumann 2006 | Emails sent: 20 March 2016, 26 March 2016, to a‐laumann@northwestern.edu, susanlboone@gmail.com dwest@northwestern.edu Regarding sequence generation, allocation concealment, method of blinding and precise study data Reply received: 26 March 2016 with responses to our questions |
Yes | ‐ |
| Marseglia 2014 | Emails sent: 15 April 2016, 19 April 2016, 23 April 2016, 30 April 2016, to massimo.milani@isdin.com Regarding allocation concealment and blinding Reply received: 2 May 2016 with responses to our questions |
Yes | ‐ |
| Miller 2011 | Email sent: 14 May 2014, to afleisch@wfubmc.edu. Latest email address is alan.fleischer1961@gmail.com (since October 2015) Regarding sequence generation and allocation concealment Reply received: 14 May 2014 with responses to our questions |
Yes | ‐ |
| Msika 2008 | Email sent: 15 May 2014, to pmsika@expanscience.com, clarence.de‐belilovsky@wanadoo.fr, npiccardi@rd.loreal.com Regarding sequence generation, stratifying, allocation concealment, means and SDs for some outcomes and clarification about data losses for the following outcomes in particular IDQOL, DFI, IGE Reply received: 30 June 2014 with additional information |
Yes | ‐ |
| Namazova‐Baranova 2012 | Email sent: 30 June 2014, to julia.levina@mail.ru and lsnamazova@yandex.ru Regarding clarification of correct citation i.e. author string/journal page numbers to the 2 citations listed in Included studies, plus sequence generation, allocation concealment and method of blinding Reply received: 30 June 2014 and 5 July 2014, with responses to our questions |
Yes | ‐ |
| Nebus 2009 | Emails sent: 2 January 2016, 5 January 2016, 15 January 2016, 20 January 2016, to Fowlerjoe@msn.com, wwallo@its.jnj.com, Jnebus@its.jnj.com Regarding missing data of control, and clarification regarding study design, and data regarding EASI, IGA Repy received: 20 January 2016 from Dr Nebus with responses to our questions and additional documents |
Yes | ‐ |
| Noh 2011 | Email sent: 7 January 2016, to kwanglee@yuhs.ac Regarding sequence generation and allocation concealment Reply received: 18 January 2016, from sminno@gmail.com, with responses to our questions |
Yes | ‐ |
| Nuñez 2013 | Email sent: 26 March 2016, to CNunez1@its.jnj.com Regarding sequence generation, allocation concealment, method of blinding, dropouts, EASI, VAS scores at baseline and day 21 and additional study details Replies received: 26 March 2016, and 30 March 2016 with responses to our questions |
Yes | ‐ |
| Park 2014 | Emails sent: 26 March 2016, 3 April 2016, 10 April 2016, 16 April 2016, to Dr Seo: joon@cnu.ac.kr Regarding sequence generation, allocation concealment, method of blinding and precise data of IGA, VAS, TEWL and corneometry with SD at 4 weeks No reply received |
Not applicable | ‐ |
| Patrizi 2008 | Emails sent: 27 March 2016, 3 April 2016, 10 April 2016, to annalisa.patrizi@unibo.it Regarding sequence generation, allocation concealment, method of blinding and precise data of EASI at day 43, and data of appraisal patients Reply received: 12 April 2016, with responses regarding sequence generation, allocation concealment and blinding, but not the rest. 14 April 2016 we sent mails to the sponsor at PPrioglio@sinclairpharma.com (no longer working) and pprioglio@sinclairpharma.it No further details retrieved |
In part | ‐ |
| Patrizi 2014 | Email sent 27 March 2016, 3 April 2016 jennifer.theunis@pierre‐fabre.com. Regarding sequence generation, allocation concealment, and precise data of TEWL at day 43, and to which group drop‐out was randomised Response 7 April 2016 we received responses to our questions |
Yes | ‐ |
| Peltonen 2014 | Email sent 28 March 2016, 3 April 2016, 10 April 2016, 16 April 2016 jarmo.laihia@utu.fi Regarding allocation concealment, precise data at baseline,day 10 and 28 for TEWL, PGA, EASI, adverse events in Cis UCA group and in vehicle No reply received |
Not applicable | ‐ |
| Peserico 2008 | Email sent: 29 March 2016, to thomas.bieber@ukb.uni‐bonn.de Regarding sequence generation, allocation concealment, method of blinding as one group had two different tubes, precise data at baseline and week 16 for VAS, EASI, DLQI and CDLQI Reply received: 30 March 2016, saying that cannot help us, the study was too long ago, and Schering Dermatology does not exist anymore. Intendis (the pharmaceutical company) did not reply |
No | ‐ |
| Shi 2015 | Email sent: 2 April 2016, to rksivamani@ucdavis.edu, vivian.shi918@gmail.com Regarding sequence generation, allocation concealment, differences between publication and protocol and exact baseline values for data after 15, 30 and 60 minutes for TEWL, and corneometry Reply received: 12 April 2016, with responses to our questions |
Yes | ‐ |
| Simpson 2011 | Email sent: 18 May 2014, to simpsone@ohsu.edu, SOTIRIOS‐PAUL.GEORGANTOPOULOS@galderma.com Regarding sequence generation and allocation concealment, mean reduction in EASI and corresponding standard deviations at day 28, and dropouts Reply received: 18 July 2014, with responses to our questions |
Yes | ‐ |
| Simpson 2013 | Emails sent: 2 April 2016, 10 April 2016, 16 April 2016, 23 April 2016, to simpsone@ohsu.edu, Nabil.kerrouche@galderma.com, Delphine.KEROB@galderma.com Regarding exact baseline values (and SD) at day 28 for dryness scale, TEWL, and corneometry Reply received: 2 May 2016, with responses to our questions and additional information |
Yes | ‐ |
| Sugarman 2009 | Email sent: 3 April 2016, to pediderm@yahoo.com Regarding sequence generation, allocation concealment, method of blinding, precise data at baseline and day 28 for IGA and patient/family self‐assessments Reply received: 4 April 2016, with responses to our questions and additional information |
Yes | ‐ |
| Szczepanowska 2008 | Email sent: 14 May 2014, to adi_medicalis@go2.pl, Adam Reich Regarding sequence generation and allocation concealment Reply received: 16 May 2014, with responses to our questions |
Yes | Quasi randomised, exclude |
| Takeuchi 2012 | Emails sent: 3 April 2016, 10 April 2016, 16 April 2016, 23 April 2016, 30 April 2016, to takeuchs@dermatol.med.kyushu‐u.ac.jp Regarding sequence generation and allocation concealment, and SCORAD (mean and SD) at start maintenance phase and at day 28 No reply received |
Not applicable | ‐ |
| Tan 2010 | Emails sent: 3 April 2016, 10 April 2016, to wptan@nsc.com.sg Regarding allocation concealment Reply received: 11 April 2016, with response to our question |
Yes | ‐ |
| Tripodi 2009 | Email sent: 8 April 2016, to salvatore.tripodi@gmail.com Regarding allocation concealment Reply received: 8 April 2016, with response to our question |
Yes | ‐ |
| Udompataikul 2011 | Emails sent: 2 July 2014, 7 July 2014, 24 January 2016, 12 February 2016, 8 April 2016, 18 April 2016, to umontree@yahoo.com (mpatai@yahoo.com is no longer in use) Regarding sequence generation, allocation concealment and standard deviations (or SEM) of the SCORAD at baseline, week 2, week 4 and week 6? Reply received: 18 April 2016, with some data but no information regarding sequence generation, or allocation concealment and there were no data for week 6 |
In part | ‐ |
| Weber 2015 | Email sent: 10 April 2016, to tweberQbdfusa.com Regarding sequence generation and allocation concealment Reply received: 15 April 2016, with responses to our questions |
Yes | ‐ |
| Wirén 2009 | Email sent: 15 April 2016, to marie.loden@eviderm.se, karin.wiren@omega‐pharma.se Regarding sequence generation and allocation concealment Reply received: 20 April 2016, with responses to our questions |
Yes | ‐ |
| Wu 2014 | Emails sent: 5 January 2016, 15 January 2016, 31 January 2016, 12 February 2016, 10 April 2016, to zwq4791@163.com Regarding sequence generation and allocation concealment No reply received |
Not applicable | ‐ |
| Åkerström 2015 | Emails sent: 10 April 2016, 16 April 2016, to petra.skare@aconordic.com Regarding allocation concealment, method of blinding, SCORAD values at start maintenance phase and follow‐up, item EQ‐5D Reply received: 18 April 2016, with responses to our questions |
Yes | ‐ |
Abbreviations
CDLQI: Children’s Dermatology Life Quality Index DLQI: Dermatology Life Quality Index EASI: eczema area and severity index EQ‐5D: a measure of health‐related quality of life that was developed by the EuroQol group that includes the five dimensions of mobility, self‐care, usual activities, pain/discomfort, and anxiety/depression HI: hydration index IGA: Investigator Global Assessment IGE: Immunoglobulin E POEM: Patient‐Oriented Eczema Measure P‐VAS: Pruritus visual analogue scale SCORAD: scoring atopic dermatitis SD: standard deviation SEM: standard error of the mean TEWL: transepidermal water loss
Data collection and analysis
Some parts of the methods section of this review uses text that was originally published in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We followed the published protocol for this Cochrane Review (van Zuuren 2016).
Selection of studies
Two authors (EvZ and ZF) independently assessed the titles and abstracts of studies identified from the searches and, if necessary, obtained and reviewed them in full text to evaluate whether they met the inclusion criteria. We resolved disagreement through discussion and, when necessary, by the judgement of a third author (AL). We excluded studies that did not meet our inclusion criteria. We have reported the number of reports retrieved, the number of both included and excluded studies and the reasons for exclusion in a flow diagram (Figure 1), as described in the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) statement (Liberati 2009).
1.
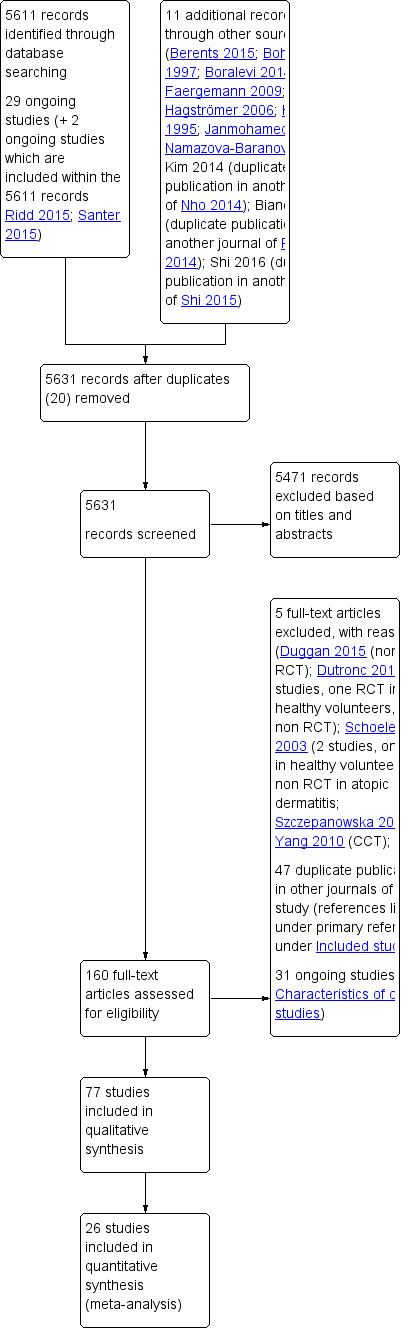
Study flow diagram
Data extraction and management
Two review authors (EvZ and ZF) collected study details and outcome data independently with a piloted data extraction form. Disagreements were resolved through discussion or a third author (RC).
The following details were extracted.
Methods: study design, blinding of participants, investigators and outcome assessors, setting, date of study conduct and study duration.
Participants: number randomised, gender, inclusion and exclusion criteria, number of dropouts and reasons for losses to follow‐up, baseline data.
Interventions: description of treatment arms, dosage or application frequency, duration of intervention.
Outcomes: timing of assessments and outcomes as reported by trial authors.
Funding source as reported.
Declarations of interest.
One review author (EvZ) added these details into the Characteristics of included studies tables in Review Manager (RevMan) 5 (RevMan 2014), and these were checked by another review author (ZF).
Assessment of risk of bias in included studies
Two review authors (EvZ and ZF) independently assessed the risk of bias of each individual included study using the Cochrane tool for assessing risk of bias (Higgins 2011). Inconsistencies were resolved through discussion or by involving a third author (RC). The 'Risk of bias' tool addresses the following domains:
method of sequence generation;
method of allocation concealment;
blinding of investigators and participants;
blinding of outcome assessors;
presence of incomplete outcome data;
presence of selective reporting; and
other bias such as, for example, baseline imbalance.
For each study we categorised each domain as being at a low risk of bias, high risk of bias or unclear risk of bias. We determined the overall risk of bias of each study as follows:
low risk of bias when all domains were assessed as being at low risk (plausible bias unlikely to seriously alter the results);
unclear risk of bias when at least one domain was classified as being at unclear risk (plausible bias that raises some doubt about the results);
high risk of bias when at least one domain was judged as being at high risk (plausible bias that seriously weakens confidence in the results).
Measures of treatment effect
Dichotomous data
We calculated risk ratios (RR) with their associated 95% confidence interval (CI) for dichotomous data. When the RR was statistically significant (95% CI did not overlap 1) we computed the number needed to treat for an additional beneficial outcome (NNTB) or number needed to treat for an additional harmful outcome (NNTH) on the basis of the combined RR value, applying the overall event rate in the placebo groups as a proxy for baseline risk.
Continuous data
We calculated mean differences (MD) with their associated 95% CI for continuous data when the eligible trials used the same instrument to measure a given construct. In cases where different measurement instruments were used, we calculated standardised mean differences (SMDs). Clinically, for HRQoL measures, an effect size (SMD) of 0.2 is considered small, 0.5 is considered moderate, and 0.8 or more is considered large (Bliddal 2009).
Time‐to‐event data
We expressed results for time‐to‐event outcome data as hazard ratios (HR). Conducting a meta‐analysis using summary information from published papers can often be problematic. We obtained the estimates of log hazard ratios and the corresponding standard errors from the reports (either from confidence intervals or reported P values) and applied them in meta‐analyses using the generic inverse variance method (Tierney 2007). We estimated the corresponding standard error (from the log‐scale), which enabled us to use the generic inverse variance method in RevMan 5. In future updates, if situations arise where we only have a contrast between groups (e.g. a difference) with an explicit P value, we will estimate the standard error, based on a Wald test (Wald 1943).
Unit of analysis issues
In studies with a parallel‐group design, the unit of analysis was the participant.
Cross‐over studies
We only included the first treatment period of cross‐over trials, due to possible carryover effects.
Studies with multiple treatment groups
We included studies with multiple treatment arms and these have been included as pair‐wise comparisons following the recommendations in Chapter 16, section 16.5.4 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Within‐participant studies
We included within‐participant studies following the recommendation in Chapter 16, section 16.4.4 in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). For continuous outcomes reported from within‐participant designs we used the mean of the paired differences (i.e. we handled the unit of analysis as a pair of observations rather than two independent observations). We calculated the summary statistics ‐ outside RevMan 5 – and reported and presented these using the inverse variance property feature. Matched group designs enrol pairs of subjects, and in analysis, use the difference score between 'subject' and 'sibling'. In dermatology this study design is applied when different sides of the body are compared; thus, it is not the 'matching subjects' that are compared but the matching sides of the body. The standard deviation (SD) of the difference is computed by summing the two SDs, and then subtracting a term that includes the correlation (rho) between the two scores on the same individual (Borenstein 2009). For pragmatic reasons we decided a priori to assume that the correlation between 'within‐participant' measures was 0.7 for all studies reporting paired samples.
We had limited analyses for binary outcomes, therefore we only reported proportions or percentages of the body sides without calculating RRs, principally because the data could not be analysed in a way that takes into account the within‐participant nature of the study design.
Dealing with missing data
We contacted trial investigators and sponsors for details of missing data for studies that were less than 10 years old. Whenever possible we used results from the intention‐to‐treat (ITT) population for both continuous and dichotomous data. For dichotomous data, we assumed that the missing participants experienced a poor outcome (imputation on basis of the worst‐case scenario).
For continuous data, we extracted the mean change from baseline and corresponding SD, or, where applicable, the after‐value scores. When necessary, we approximated means and measures of dispersion from figures in the reports.
Assessment of heterogeneity
We assessed both clinical and statistical diversity to determine if data from studies could meaningfully be combined and entered into a meta‐analysis. We assessed clinical heterogeneity by exploring variability in participants, interventions and outcomes. For the meta‐analysis we used standard random‐effects meta‐analysis as the default option (DerSimonian 1986), and applied the fixed‐effect model for the purpose of sensitivity analysis. The random‐effects model assumes that the true treatment effect differs from study to study and provides an estimate of the average treatment effect, rather than assuming all studies are estimating the same (fixed) treatment effect (Riley 2011). We assessed heterogeneity across the studies by using the I² statistic, which describes the percentage of total variation across trials that is due to heterogeneity rather than chance (Higgins 2011). An I² of 50% to 90% may represent considerable heterogeneity and 75% to 100%, represents substantial heterogeneity. We conducted meta‐analyses according to the protocol independently of the observed I². Based on the recommendations of the Grading of Recommendations Assessment, Development and Evaluation working group (GRADE), we considered downgrading the quality of the evidence for serious inconsistency if I² was above 50%, and also took other considerations for downgrading into account. One consequence of using random‐effects models as the default (these models weigh studies more equally than a fixed‐effect analysis) is that in the presence of small‐study effects (in which the intervention effect is more beneficial in the smaller studies) the random‐effects estimate of the intervention effect will appear more beneficial than the fixed‐effect estimate. In order to explore whether there was evidence of small‐study effects, we performed sensitivity analyses to examine how the results of the meta‐analysis changed when we compared the fixed‐effect and random‐effects estimates of the intervention effect. If the estimates were similar, then any small‐study effects had little effect on the estimate of the intervention effect (Chapter 10.4.4.1 Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Assessment of reporting biases
There was only one outcome for which we had more than 10 studies entered in a meta‐analysis (one secondary outcome in comparison 2f). We generated a funnel plot for this outcome to check for asymmetry (which may suggest publication and small study effect biases) (Higgins 2011), however we did not detect asymmetry in the funnel plot for this specific outcome (disease severity as assessed by the investigators).
Data synthesis
Two review authors (EvZ and ZF) analysed the data in RevMan 5 using a random‐effects model, following the recommendations in Chapter 9 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Where outcomes of interest were rare, we followed the recommendations of Bradburn 2007 and used Peto odds ratios to compare the intervention and comparator groups. We planned to undertake meta‐analyses using Mantel‐Haenszel risk differences. However, this was not required, as we had no meta‐analysis for outcomes that were rare. In future updates when we can perform meta‐analyses for these outcomes, we will report results with 95% CI and forest plots for both statistical measures so that findings can be compared.
Where we estimated results for individual studies with low numbers of events (fewer than 10 in total) or where the total sample size was less than 30 participants, we reported the proportion of events in each group, together with a P value from a Fisher's exact test.
We applied the GRADE approach for the main comparisons (Schünemann 2013), in order to rate the quality of the evidence for the prespecified outcomes (see Outcomes for 'Summary of findings' tables under Types of outcome measures) (Guyatt 2013a; Guyatt 2013b).
Subgroup analysis and investigation of heterogeneity
According to our protocol we planned to undertake the following stratified analyses for the primary outcomes to explore whether different study characteristics could be considered as effect modifiers:
age of participants (e.g. children versus adults) (subset of participants);
disease severity (mild versus severe eczema) (subset of participants);
atopic versus non‐atopic eczema (subset of participants); and
presence of filaggrin gene mutations versus no filaggrin gene mutations (subset of participants).
However, we did not find enough studies to carry out any subgroup analysis.
Sensitivity analysis
We carried out sensitivity analyses to examine the effects of excluding studies at high risk of bias, as well as different stratified analyses to explore heterogeneity. To do this we performed stratified analyses for the overall risk of bias, defined as low risk (low for all domains), high risk (high for one or more domains), and unclear risk (unclear for one or more domains).
In the presence of small‐study effects, that is where the intervention effect appears more beneficial in smaller studies, use of a random‐effects estimate of intervention effect produces a more beneficial result than a fixed‐effect estimate. Therefore, we assessed the influence of small‐study effects on the results of meta‐analyses in which there was evidence of between‐study heterogeneity (I² > 0), by comparing the fixed‐effect and random‐effects estimates of the intervention effect (i.e. if the estimates were similar, then any small‐study effects had little effect on the intervention effect estimate) (Chapter 10 Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011)).
Where possible, we performed a stratified analysis to compare study results from preregistered trials (e.g. available on ClinicalTrials.gov) with those without an available prespecified protocol.
Results
Description of studies
See Characteristics of included studies and Characteristics of excluded studies.
Results of the search
Our searches of the various databases retrieved 5611 records for studies, two of which were protocols for ongoing trials. The searches of the trials registers identified a further 29 ongoing studies, and we found 11 additional references through other resources, including the bibliographies of included and excluded studies. After removal of 20 duplicate records, we screened 5631 references for eligibility. We excluded 5471 studies through assessment of their titles and abstracts, and we obtained full‐text copies of the remaining 160 studies. Among the 160 studies there were 47 duplicate studies (multiple publications of the same study; i.e. studies published as well in another journal or presented as an abstract or poster during a conference). We excluded five studies with reasons detailed in Characteristics of excluded studies; a further 31 are ongoing trials (see Characteristics of ongoing studies). We included the remaining 77 studies in the review (see Characteristics of included studies). For details of our screening process, see the study flow diagram (Figure 1).
Thirteen studies had to be translated into English from Chinese (Gao 2008; Wu 2014; Yang 2010), German (Bohnsack 1997; Gehring 1996; Puschmann 2003; Thumm 2000; Wilhelm 1998), Japanese (Hamada 2008; Shiratori 1977), Korean (Kim 2014 (full publication of Nho 2014) and Noh 2011), and French (Larregue 1996), prior to further assessment (see Acknowledgements).
Included studies
We included 77 studies, with a total of 6603 participants, in the review. The number of participants for whom gender was reported (2986 women and 2311 men) were fairly comparable, but gender was not reported for the remaining 1306 participants.
Characteristics of the trial setting and methods
Within the 77 included RCTs:
seven compared a moisturiser with no treatment (no moisturiser) (Giordano‐Labadie 2006; Grimalt 2007; Hagströmer 2006; Patrizi 2014; Simpson 2013; Weber 2015; Wirén 2009);
15 were placebo‐ or vehicle‐controlled (Abramovits 2008; Belloni 2005; Boguniewicz 2008; Bohnsack 1997; Boralevi 2014; Breternitz 2008; Gayraud 2015; Gehring 1999; Hamada 2008; Korting 2010; Larregue 1996; Nebus 2009; Peltonen 2014; Tan 2010; Wilhelm 1998);
four multi‐armed studies made comparisons between placebo or vehicle as well as another moisturiser (Lodén 2002; Patrizi 2008; Shiratori 1977; Thumm 2000);
15 studies compared moisturisers against active treatments (topical corticosteroids or topical immunomodulators) (Angelova‐Fischer 2014; Berth‐Jones 2003; De Belilovsky 2011; Emer 2011; Frankel 2011; Gehring 1996; Glazenburg 2009; Hanifin 2002; Janmohamed 2014; Jirabundansuk 2014; Peserico 2008; Sugarman 2009; Takeuchi 2012; Udompataikul 2011; Wanakul 2013);
seven studies compared active treatment combined with moisturisers against active treatment alone (Draelos 2008; Gao 2008; Hanifin 1998; Kircik 2009; Msika 2008; Simpson 2011; Wu 2014);
the remaining 29 studies compared one moisturiser with another moisturiser.
Thirty‐eight studies were conducted in a single centre, mostly dermatology departments of hospitals, whilst 40 studies were multicentre studies. The majority of studies were conducted in Europe (42), followed by the USA and Canada (20), Asia (14), and Africa (1).
Characteristics of the participants
The studies mainly included participants with mild to moderate eczema; the criteria of the UK Working Party (Williams 1994), and of Hanifin and Rajka (Hanifin 1980), were the most widely used diagnostic criteria. Sample sizes were relatively small and ranged from six to 552 participants with the majority of studies including between 20 and 60 participants.
The ages of the participants varied across the studies, with a range of four months to 84 years, and an overall mean of 18.6 years.
Characteristics of the interventions
The studies evaluated a wide range of different moisturisers (see Table 12), but very few compared similar interventions. Duration of interventions lasted from a single 10‐minute application of a treatment to application several times a day for up to six months, but two to six weeks was the most common duration of study, with a mean of 6.7 weeks.
3. Comparisons of moisturisers.
| MOISTURISER VERSUS VEHICLE, PLACEBO OR NO TREATMENT | ||||
| Moisturisers versus no treatment (i.e. no moisturiser) | ||||
| Study | Intervention | Comparator | Within‐participant? | Active treatment allowed? |
| Grimalt 2007 | Exomega lotion (oat) twice daily 6 weeks | No treatment for 6 weeks | No | Moderate‐ and high‐potency corticosteroids allowed |
| Giordano‐Labadie 2006 | Exomega moisturising milk (oat) twice daily for 2 months | No treatment for 2 months | No | Moderate‐ and high‐potency corticosteroids allowed |
| Weber 2015 | Eucerin Eczema Relief body cream (oat and licochalcone) once a day for 6 months + cleanser | Only cleanser for 6 months | No | Eucerin Eczema Relief Instant Therapy allowed for active lesions, |
| Wirén 2009 | Canoderm (urea 5%) twice daily 6 months | No treatment 6 months | No | Permitted only at areas other than target lesion |
| Simpson 2013 | Cethaphil Restoraderm Body moisturiser (ceramide precursors etc) twice daily 27 days | No treatment 27 days | Yes | No |
| Patrizi 2014 | Emollient balm twice daily for 28 days | Hygiene product for 28 days | No | Not mentioned |
| Atopiclairversus vehicle | ||||
| Study | Intervention | Comparator | Within‐participant? | Active treatment allowed? |
| Abramovits 2008 | Atopiclair three times daily for 50 days | Vehicle three times daily for 50 days | No | No |
| Belloni 2005 | Atopiclair three times daily for 21 days | Vehicle three times daily for 21 days | No | Oral medication continued |
| Boguniewicz 2008 | Atopiclair three times daily for 43 days | Vehicle three times daily for 43 days | No | If really needed, low‐potency topical corticosteroids allowed |
|
Patrizi 20083‐arm (1st comparison) As Atopiclair 'light' is not marketed and clearly less effective, it is not included in the comparison Atopiclair versus vehicle. The comparison Atopiclair 'light' versus vehicle (2nd comparison) will therefore not be further discussed |
Atopiclair three times daily for 43 days | Vehicle three times daily for 43 days | No | If really needed, low‐potency topical corticosteroid allowed |
| Other moisturisers versus vehicle or placebo | ||||
| Urea‐containing moisturisers | ||||
| Study | Intervention | Comparator | Within‐participant? | Active treatment allowed? |
| Bohnsack 1997 | Laceran (10% urea) twice daily for 4 weeks | Vehicle twice daily for 4 weeks | Yes | No |
| Wirén 2009 | Canoderm (urea 5%) twice daily for 6 months | No treatment for 6 months | No | Only at other areas than target lesion |
| Wilhelm 1998 | Laceran (10% urea) twice daily for 4 weeks | Vehicle twice daily for 4 weeks | Yes | No |
| Lodén 20023 arm (1st comparison) | Urea saline 4% cream once daily for 30 days | Placebo (cream base) cream once daily for 30 days | No | Topical steroids allowed |
| Glycerol‐containing moisturisers | ||||
| Lodén 20023 arm (2nd comparison) | Glycerol 20% once daily for 30 days | Placebo (cream base) once daily for 30 days | No | Topical steroids allowed |
| Boralevi 2014 | Dexeryl (glycerol 15%) twice daily for 4 weeks | Vehicle without glycerol twice daily for 4 weeks | No | If really needed, moderate‐potency topical corticosteroid allowed |
| Breternitz 2008 | Glycerol 20% twice daily for 4 weeks | Vehicle without glycerol twice daily for 4 weeks | Yes | No |
| Oat‐containing moisturisers | ||||
| Grimalt 2007 | Exomega lotion (oat) twice daily for 6 weeks | No treatment for 6 weeks | No | Moderate‐ and high‐potency corticosteroids allowed |
| Giordano‐Labadie 2006 | Exomega moisturising milk (oat) twice daily for 2 months | No treatment for 2 months | No | Moderate‐ and high‐potency corticosteroids allowed |
| Nebus 2009 | Oatmeal based occlusive cream twice daily for 8 weeks | Occlusive vehicle for 8 weeks | No | Topical medications allowed |
| Weber 2015 | Eucerin Eczema Relief body cream (oat and licochalcone) once a day for 6 months + cleanser | Cleanser only for 6 months | No | Eucerin Eczema Relief Instant Therapy was allowed for active lesions |
| Remaining moisturisers versus vehicle or placebo | ||||
| Larregue 1996 | Ammonium lactate 6% in water‐in‐oil emulsion twice daily for 4 weeks | Vehicle twice daily for 4 weeks | Yes | No |
| Korting 2010 | Pale sulfonated 4% shale oil cream three times daily for 4 weeks | Vehicle three times daily for 4 weeks | No | No |
| Gayraud 2015 | Atoderm Intensive cream twice daily for 6 months | Moisturiser base twice daily for 6 months | No | Topical corticosteroid and immunomodulators could be continued |
| Tan 2010 | Triclosan 1% moisturiser twice daily for 41 days | Vehicle cream twice daily for 41 days | No | Low‐potency corticosteroid allowed |
| Thumm 20003 arm (1st comparison) | Hippophae rhamnoides 10% cream for 4 weeks | Placebo cream for 4 weeks | No | No |
| Thumm 20003 arm (2nd comparison) | Hippophae rhamnoides 20% cream for 4 weeks | Placebo cream for 4 weeks | No | No |
| Oils versus placebo | ||||
| Gehring 1999study 1 | Primrose oil amphilic o/w emulsion twice daily for 4 weeks | Placebo oil twice daily for 4 weeks | Yes | No |
| Gehring 1999study 2 | Primrose oil amphilic w/o emulsion twice daily for 4 weeks | Placebo oil twice daily for 4 weeks | Yes | No |
| Hamada 2008 | Camellia oil spray for 2 weeks | Purified water spray for 2 weeks | No | All allowed without changing |
| ONE MOISTURISER VERSUS ANOTHER MOISTURISER | ||||
| Study | Intervention | Comparator | Within‐participant? | Active treatment allowed? |
| Patrizi 20083 arm (3rd comparison) | Atopiclair three times daily for 43 days | Atopiclair 'light' three times daily for 43 days | No | If really needed, low‐potency topical corticosteroid allowed |
| Miller 20113 arm (1st comparison) | Atopiclair three times daily for 3 weeks | EpiCeram three times daily for 3 weeks | No | No |
| Miller 20113 arm (2nd comparison) | Atopiclair three times daily for 3 weeks | Aquaphor (petrolatum 41%, glycerol, lanolin etc.), three times daily for 3 weeks | No | No |
| Miller 20113 arm (3rd comparison) | EpiCeram (high ceramides) three times daily for 3 weeks | Aquaphor three times daily for 3 weeks | No | No |
| Draelos 2011 | EpiCeram twice daily for 4 weeks | Hyalotopic (hyaluronic acid, glycerol, propylene glycol etc) twice daily for 4 weeks | Yes | No |
| Nuñez 2013 | EpiCeram twice daily for 3 weeks | Oatmeal‐containing cream twice daily for 3 weeks | No | No |
| Kircik 2014 | EpiCeram for 4 weeks | Eucerin for 4 weeks | Yes | No |
| Laumann 2006 | MimyX + Eucerin twice daily for 12 weeks | Eucerin cream twice daily for 12 weeks | Yes | If really needed, low‐potency topical corticosteroid allowed |
| Draelos 2009 | Albolene twice daily for 4 weeks | MimyX twice daily for 4 weeks | Yes | Low‐potency topical corticosteroid allowed |
| Fredriksson 1975(2 studies) | Aquacare twice daily for 4 weeks | Calmurid twice daily for 4 weeks | Yes | No |
| Namazova‐Baranova 2012 | Locobase repair twice daily for a year | Atoderma twice daily for a year | No | Moderate‐potency topical corticosteroid allowed |
| Åkerström 2015 | Canoderm (urea 5%) twice daily for 6 months | Miniderm (no urea) twice daily for 6 months | No | No |
| Bissonnette 2010 | Urea 5% moisturiser twice daily for 6 weeks | Urea 10% lotion for 6 weeks | No | Topical steroids allowed |
| Hagströmer 2001 | Urea 4% + NaCl in o/w twice daily for 2 weeks | Urea 4% in o/w twice daily for 2 weeks | Yes | No |
| Lodén 20023 arm (3rd comparison) | Glycerol 20% once daily for 30 days | Urea saline 4% cream once daily for 30 days | No | Topical corticosteroids allowed |
| Faergemann 2009 | Propyless (20% propylene glycol) twice daily for 2 weeks | Fenuril (urea 4% and NaCl 4%) twice daily for 2 weeks | Yes | No |
| Noh 2011 | Ceramide‐containing moisturiser twice daily for 6 weeks | Control moisturiser (?) twice daily for 6 weeks | No | Topical corticosteroids allowed |
| Tripodi 2009 | Furfuryl palmitate‐enriched moisturiser twice daily for 2 weeks | Moisturiser twice daily for 2 weeks | No | No |
| Marseglia 2014 | Pro‐AMP cream (rhamnosoft ceramides) twice daily for 4 weeks | Hydrating cream (glycerol, vaseline, paraffin twice daily for 4 weeks | No | No |
| Thumm 20003 arm (3rd comparison) | Hippophae rhamnoides 10% cream for 4 weeks | Hipophae rhamnoides 20% cream for 4 weeks | No | No |
| Park 2014 | Lactobacillus sakei‐containing moisturiser twice daily for 4 weeks | Control moisturiser for 4 weeks | Yes | Topical corticosteroids allowed |
| Evangelista 2014 | Virgin coconut oil twice daily for 8 weeks | Mineral oil twice daily for 8 weeks | No | No |
| Verallo‐Rowell 2008 | Virgin coconut oil twice daily for 4 weeks | Virgin olive oil twice daily for 4 weeks | No | No |
| Shi 2015 | Bleach bath with moisturiser on one occasion | Water bath with moisturiser on one occasion | No | No |
| MOISTURISERS VERSUS ACTIVE TREATMENT | ||||
| Moisturisers versus topical corticosteroids | ||||
| Study | Intervention | Comparator | Within‐participant? | Active treatment allowed? |
| Within‐participant studies comparing licochalcone containing moisturiser versus hydrocortisone | ||||
| Angelova‐Fischer 2014 | O/W formulation containing licochalcone A (Glycyrrhiza Inflata root extract) twice daily for 1 week | Hydrocortisone cream twice daily for 1 week | Yes | No |
| Udompataikul 2011 | Licochalcone twice daily for 6 weeks | Hydrocortisone cream twice daily for 6 weeks | Yes | No |
| Wanakul 2013 | Licochalcone twice daily for 4 weeks | Hydrocortisone cream twice daily for 4 weeks | Yes | No |
| Parallel studies comparing moisturisers versus topical corticosteroids | ||||
| De Belilovsky 2011 | Stelatopia (2% sunflower oil distillate, fatty acids, ceramides) twice daily for 3 weeks | Hydrocortisone butyric propionate twice daily for 3 weeks | No | No |
| Sugarman 2009 | EpiCeram twice daily for 4 weeks | Fluticasone 0.5% cream twice a day for 4 weeks | No | No (Cetaphil lotion applied to uninvolved lesions) |
| Janmohamed 2014 | 20% petrolatum in cetomacrogol + wet wrap for 4 weeks | Mometasone furoate 0.1% + wet wrap for 4 weeks | No | No |
| Gehring 1996 | w/o emulsion Excipial twice a day for 1 week | Hydrocortisone 1% in w/o emulsion (Excipial) twice daily for 1 week | No | No |
| Jirabundansuk 2014 | Moisturiser containing spent grain wax, spinose kernel oil, etc. twice a day for 4 weeks | Hydrocortisone 1% cream twice a day for 4 weeks | Yes | No |
| Peserico 2008 | Moisturiser (Advabase) twice a day for 16 weeks | Methylprednisolone aceponate cream 2 days a week, on other days used moisturiser twice a day for 16 weeks | No | No |
| Moisturiser versus topical immunomodulators | ||||
| Emer 2011 | Eletone (high lipid) three times daily for 4 weeks | Pimecrolimus three times daily for 4 weeks | Yes | No |
| Takeuchi 2012 | Moisturiser therapy (?) for 4 weeks | Tacrolimus for 4 weeks | No | No |
| Frankel 2011 | Hyalotopic (ceramide) three times daily for 4 weeks | Pimecrolimus twice a day for 4 weeks | Yes | No |
| VEHICLE + MOISTURISER VERSUS TOPICAL CORTICOSTEROID + MOISTURISER | ||||
| Berth‐Jones 20034 arm (1st comparison) | Vehicle cream twice weekly + moisturiser for 16 weeks | Fluticasone propionate 0.05% cream twice weekly + moisturiser for 16 weeks | No | No |
|
Berth‐Jones 20034 arm (2nd comparison) We did not consider other possible comparisons of the 4 arms important for this review |
Vehicle ointment twice weekly + moisturiser for 16 weeks | Fluticasone propionate 0.005% ointment twice weekly + moisturiser for 16 weeks | No | No |
| Hanifin 2002 | Vehicle twice a week + moisturiser for 20 weeks | Fluticasone propionate 0.05% cream twice weekly + moisturiser for 20 weeks | No | No |
| Glazenburg 2009 | Placebo ointment twice weekly + moisturiser for 16 weeks | Fluticasone propionate 0.005% ointment twice weekly + moisturiser for 16 weeks | No | No |
| TOPICAL ACTIVE TREATMENT + MOISTURISER VERSUS TOPICAL ACTIVE TREATMENT ALONE | ||||
| Study | Intervention | Comparator | Within‐participant? | Active treatment allowed? |
| Draelos 20083 arm (1st comparison) | Fluocinonide 0.05% twice a day + ceramide cleanser+ moisturising cream for 4 weeks | Fluocinonide 0.05% twice a day plus cleansing bar for 4 weeks | No | No |
|
Draelos 20083 arm (2nd comparison) 3rd possible comparison did not include moisturiser i.e. fluocinonide + cleansing bar vs fluocinonide + ceramide cleanser |
Fluocinonide 0.05% twice a day + ceramide cleanser+ moisturising cream for 4 weeks | Fluocinonide 0.05% twice a day plus ceramide cleanser for 4 weeks | No | No |
| Wu 2014 | Moisturising and softening cream + flumethasone ointment twice a day for 3 weeks | Flumethasone ointment twice a day for 3 weeks | No | No |
| Simpson 2011 study D | Restoraderm moisturiser twice a day + topical corticosteroids for 4 weeks | Routine use of topical corticosteroids for 4 weeks | Yes | No |
| Hanifin 1998 | Desonide 0.05% twice a day + three times daily moisturiser for 3 weeks | Desonide 0.05% cream twice a day for 3 weeks | Yes | No |
| Msika 20085 arm (1st comparison) | Desonide 0.05% twice a day plus moisturiser + sunflower oil 2% twice a day for 21 days | Desonide 0.05% twice a day for 21 days | No | No |
|
Msika 20085 arm (2nd comparison) We did not consider other possible comparisons of the 5 arms to be important for this review |
Desonide 0.05% once daily plus moisturiser + sunflower oil 2% twice a day for 21 days | Desonide 0.05% once daily for 21 days | No | No |
| Gao 2008 | BoPao cream + 10% urea ointment once a day or twice a day for 2 weeks | BoPao cream only (antifungal/anti‐inflammatory cream) | No | No |
o/w: oil in water
w/o: water in oil
Fourteen of the 77 included studies provided no usable data (see Table 13). The reasons for this were: that the study report was unclear about how many participants were randomised to each treatment arm; or reported no precise outcome data, so the data could only be estimated from figures; or there were no separate data for healthy participants and atopic participants; or the study did not address our prespecified outcomes; or the reports were posters with limited information. We were either unsuccessful in our attempts to obtain data from the principal investigators of these 14 cases (see Table 11), or the studies were more than 10 years old, which made a response to enquiries unlikely.
4. Included studies with no usable or irretrievable data.
| Study ID | Interventions & comparisons | N | Comments |
| Andersson 1999 | 5% urea as active substance versus 4% urea and 4% NaCl | 50 | The data were reported in box‐and‐whisker plots, and no precise data were provided, too much estimation |
| Berents 2015 | Emollient + fresh expressed milk versus moisturiser only | 9 | None of our outcomes were assessed |
| Danby 2011 | Aqueous cream BP versus Oilatum Junior Bath additive | 38 | Poster with limited information. The principal investigator said, "The study itself was a purely mechanistic study, and not meant to provide clinical evidence" |
| Ferreira 1998 | Nioleol (10% primrose oil, 8%‐9% γ‐linolenic acid) versus Uriage (borage oil and 24% γ‐linolenic acid) versus Atopic (35%‐40% γ‐linolenic acid) versus Atoderm control moisturiser once daily for 12 weeks |
23 | Unclear how many participants were randomised to each arm |
| Hagströmer 2006 | Proderm versus no treatment | 24 | No baseline data nor end value data were reported. The data were reported in box‐and‐whisker plots, and were not interpretable |
| Harper 1995 | Oilatum Plus versus Oilatum Emollient | 30 | Unclear how many participants were randomised to each arm, inconsistencies in reporting of data |
| Hlela 2015 |
Study 1 Emulsifying ointment with aqueous cream versus emulsifying ointment with baby oil Study 2 Cetomacrogol versus emulsifying ointment versus glycerol/petrolatum versus petroleum jelly |
120 | Frequency of use during day or week were not reported. There were quite some inconsistencies in text and figures. Study 2 reported no end data, just that all scores tended to decline. We mailed investigators numerous times to clarify study details, but received no response. |
| Kircik 2009 | Midpotency corticosteroid cream versus midpotency corticosteroid cream combined with a hydrolipid cream | 6 | Poster with limited information, principal investigator was not able to provide missing study details |
| Lodén 2001 | Glycerol 20% cream versus 4% urea and 4% NaCl | 110 | Unclear how many participants were randomised to each arm. The data all need to be estimated from box‐and‐whisker plots, too much estimation |
| Nho 2014 | PPARα activator and ceramide versus moisturiser without these ingredients | 31 | Only 5 participants with eczema included, no individual patient data, not our prespecified outcomes |
| Peltonen 2014 | Cis‐urocanic acid 5% emulsion cream versus control vehicle | 14 | Data provided need to be estimated from figures (for transepidermal water loss (TEWL)), or no precise data were provided other than that there were no significant differences. We mailed investigators numerous times to clarify study details, but received no response |
| Pigatto 1996 | Cream containing 10% urea versus control cream | 70 | Unclear how many were randomised to each treatment arm, no separate data for healthy subjects and atopic subjects |
| Puschmann 2003 | Two different formulations of polidocanol‐ and urea‐containing creams against each other | 54 | Unclear how many were randomised to each treatment arm, no separate data for healthy subjects and atopic subjects |
| Shiratori 1977 | Urea 10% ointment versus base OR versus urea 20% ointment | 552 | The data were confusingly reported in this study and did not lend themselves to further analysis. As the study was 39 years old we have not contacted the investigators for data |
Characteristics of the outcome measures
Our primary outcome, participant‐assessed disease severity, was addressed in only 24 studies, which mostly used a 3‐ to 6‐point Likert scale. However, three studies used a validated instrument. The Gayraud 2015 study applied the Patient‐Oriented SCORing Atopic Dermatitis (PO‐SCORAD) scale (Stalder 2011), and the Hlela 2015 and Janmohamed 2014 studies used the Patient Oriented Eczema Measure (POEM) (Charman 2004). A total of 23 studies evaluated changes in itch scores, which were predominantly measured with a visual analogue scale (VAS). Satisfaction was assessed in 13 studies with either a Likert scale, VAS or a questionnaire. Adverse events were reported in 41 studies, however, information was mostly limited or generic in nature (e.g. "Only five adverse events were possibly or probably related to the study products with three of them of mild intensity and all of them related to the skin" (Bissonnette 2010)).
One of our secondary outcomes, investigator‐assessed disease severity, was addressed in 65 studies and, as with the participant assessments, was predominantly evaluated with a Likert scale alone or in combination with validated instruments such as the Eczema Area and Severity Index (EASI) and SCORAD. Fourteen studies assessed disease severity with EASI (Hanifin 2001), and 25 studies used the SCORAD (European Task Force on Atopic Dermatitis 1993). Prevention of flares (lengthening the time to first flare) was investigated in 16 studies, mostly after eczema had been stabilised with active treatment. The least assessed outcome was 'change in use of topical active treatment' which was only addressed in eight studies. Twenty‐nine studies assessed changes in skin barrier function by TEWL, followed by corneometry, to measure skin hydration. The remaining secondary outcome 'change in health‐related quality of life' was covered in 10 studies. All of the studies used validated instruments except Bissonnette 2010 which used a 22‐item questionnaire. De Belilovsky 2011, Grimalt 2007 and Msika 2008 used two instruments (the Infant’s Dermatitis Quality of Life index (IDQOL) (Lewis‐Jones 2001), and the Dermatitis Family Impact questionnaire (DFI) (Lawson 1998)). Gayraud 2015 used the Children's Dermatology Life Quality Index (CDLQI) as an additional instrument (Lewis‐Jones 1995). Hlela 2015 and Janmohamed 2014 applied the IDQOL, Giordano‐Labadie 2006 used the CDLQI, Nebus 2009 the Dermatology Quality of Life Index (DLQI) (Finlay 1994), and Åkerström 2015 the EQ‐5D (The EuroQol Group 1990).
Many of the included studies in this review reported additional outcomes of potential clinical relevance, but they were not directly relevant to the prespecified objectives of this review. Examples of such outcomes included reduction in S aureus (Angelova‐Fischer 2014; Verallo‐Rowell 2008), tolerability (Bissonnette 2010; Draelos 2008; Grimalt 2007; Korting 2010; Larregue 1996; Marseglia 2014; Puschmann 2003; Wilhelm 1998), cosmetic acceptability (Bissonnette 2010; Faergemann 2009; Fredriksson 1975), and onset and duration of itch relief (Boguniewicz 2008).
Declaration of interest and funding
A total of 46 of the 77 studies reported the source of their funding, which was mostly from the pharmaceutical industry, and 27 of these studies declared conflicts of interest. Some studies did not report funding, although the product under investigation was manufactured by a pharmaceutical company that employed one or more of the investigators, which would make the prospect of pharmaceutical company funding more likely (Abramovits 2008; Andersson 1999; Bissonnette 2010; Bohnsack 1997; Giordano‐Labadie 2006).
Some studies reported that there was no conflict of interest, but indicated that some of the investigators were employees of the manufacturer of the moisturiser under investigation (Andersson 1999; Bohnsack 1997; De Belilovsky 2011; Giordano‐Labadie 2006; Glazenburg 2009; Hanifin 1998; Hanifin 2002; Lodén 2001; Lodén 2002; Msika 2008; Thumm 2000; Wilhelm 1998; Wirén 2009).
Nine studies did not report funding (or were not funded by the pharmaceutical industry) and had no apparent conflict of interest (Berents 2015; Evangelista 2014; Hagströmer 2006; Hamada 2008; Hlela 2015; Park 2014; Shi 2015; Takeuchi 2012; Verallo‐Rowell 2008). The older studies generally did not report funding or conflicts of interest, as these declarations were not a requirement at that time; this made it impossible for us to draw conclusions about whether these studies were industry sponsored or were free of conflicts of interest (e.g. Ferreira 1998; Fredriksson 1975; Gehring 1996; Gehring 1999; Larregue 1996; Pigatto 1996; Shiratori 1977).
Excluded studies
We excluded five studies after evaluation of their full text; most were excluded because they were not RCTs (see details Characteristics of excluded studies).
Risk of bias in included studies
We assessed each of the six domains of the Cochrane 'Risk of bias' tool for every included study (see 'Risk of bias' table corresponding to the individual studies in Characteristics of included studies). Risk of bias is also presented in Figure 2 (the 'Risk of bias' graph) and Figure 3 (the 'Risk of bias' summary).
2.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies
3.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study
Seven studies received an overall assessment of low risk of bias as we judged all domains in the 'Risk of bias' tool to be at low risk (plausible bias unlikely to alter the results seriously) (Åkerström 2015; Belloni 2005; Boralevi 2014; Gayraud 2015; Miller 2011; Nebus 2009; Tan 2010). We assessed 36 studies as being at high risk of bias because we considered one or more domains to be at a high risk of bias (plausible bias that weakens confidence in the results seriously). We classified the remaining 34 studies as being at an unclear risk of bias (plausible bias that raises some doubt about the results).
Allocation
In 44 studies the method used to generate the allocation sequence was clearly described, and allowed a clear assessment of whether the method would produce comparable groups; most of these studies used computer‐generated randomisation codes. The remaining 33 studies were reported to be randomised, but did not provide further details about the methods of random sequence generation used.
Allocation concealment was ensured in 32 studies. Central allocation by pharmaceutical companies and deliveries of sequentially numbered, de‐identified containers or tubes of identical appearance were the most frequently used methods to secure this. We considered allocation concealment to be at a high risk of bias in one study, as the principal investigator informed us that there was no concealment of allocation (Danby 2011). We judged this domain to be at unclear risk of bias for the other 44 studies, as these did not report the method of allocation concealment used.
Blinding
Lack of blinding was the single most important reason for which we judged studies to be at a high risk of bias.
Sixteen studies had no blinding, or incomplete or inadequate blinding, and we therefore judged the domain for performance bias as being at high risk. We judged 21 studies to be at low risk of bias for this domain, as these provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received. Methods we considered to provide adequate blinding included the use of similar containers, tubes or boxes with similar looking moisturisers, and comparative treatments and similar application frequencies. Forty studies did not describe the method of blinding, or described it inadequately, and therefore we considered the domain as being at unclear risk of bias.
Twenty‐three studies ensured blinding of the outcomes assessors, and it was unlikely that the blinding could have been broken. For 29 studies we judged blinding of outcome assessors as being at high risk of bias. This number is clearly higher than for the domain of performance bias. This was mainly due to the fact that although some studies were labelled as investigator‐blinded, the participants were not blinded, yet the study design included participant‐assessed outcomes. We judged 25 studies to be at an unclear risk of detection bias, largely due to the lack of detail reported about the methods of blinding.
Incomplete outcome data
For 52 studies there was no evidence of incomplete reporting of outcome data, or missing data were limited and balanced between the treatment arms, therefore we judged this domain to be at a low risk of bias. For six studies we considered this domain to be at a high risk of bias (Abramovits 2008; Berents 2015; Grimalt 2007; Noh 2011; Tripodi 2009; Wu 2014), mainly because of high dropout rates combined with per‐protocol analysis, an unbalanced number of dropouts, or because outcome data were missing (such as incomplete outcome data from questionnaires). We assessed the remaining 19 studies as being at an unclear risk of bias.
Selective reporting
The prespecified outcomes and those mentioned in the Methods section appeared to have been reported adequately in the majority of studies (66). In four studies one or more predefined outcomes were not addressed in the Results section (Draelos 2011; Larregue 1996; Laumann 2006; Takeuchi 2012), and we considered that this presented a high risk of bias for this domain. For the other seven studies there was either limited reporting of an outcome, or insufficient information available to permit us to make a 'Risk of bias' judgement.
Other potential sources of bias
We considered the domain of other bias to be at low risk of bias in 67 studies. We assessed this domain as being at unclear risk of bias for 10 studies; there was some baseline imbalance in three studies (Breternitz 2008; Hlela 2015; Verallo‐Rowell 2008), and, in the remaining seven studies, there was insufficient information available to permit us to make a clear judgement (e.g. poster abstract) (Danby 2011; Gao 2008; Kircik 2009; Laumann 2006; Nho 2014; Nuñez 2013; Pigatto 1996).
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7; Table 8; Table 9
A total of 63 studies contributed to comparisons as listed below. Some studies contributed to more than one comparison. As stated above, 14 studies provided no usable data (Table 13).
We provide a summary of the comparisons we made, and the categories within them, below for ease of navigation (see Table 12). Some studies appear in more than one category.
Comparison 1: moisturisers versus no treatment (i.e. no moisturiser) (six studies)
Comparison 2: moisturisers versus vehicle, placebo or no treatment (2a to 2g): subdivided as follows.
2a ‐ Atopiclair (glycyrrhetinic acid‐containing moisturiser) versus vehicle (four studies);
2b ‐ Urea‐containing moisturisers versus vehicle, placebo or no treatment (i.e. no moisturiser) (four studies);
2c ‐ Glycerol (glycerine)‐containing moisturisers versus vehicle or placebo (three studies);
2d ‐ Oat‐containing moisturisers versus vehicle or no treatment (four studies);
2e‐I to 2e‐VI ‐ Remainder of moisturisers versus vehicle or placebo (five studies, one reference included three treatment arms (Thumm 2000));
2f ‐ All moisturisers versus vehicle, placebo or no treatment (14 studies);
2g ‐ Oil versus placebo (three studies (one reference: Gehring 1999 included two studies).
To ensure consistency with the terminology used by the investigators, we have used their wording and refer to 'placebo' or 'vehicle' accordingly. It is important to know that a placebo is also a moisturiser, but with a different composition and without the ingredient assumed to be effective, while a vehicle has the same composition as the moisturiser it is compared with, but without the ingredient assumed to be effective. As both placebo and vehicle have moisturising properties, they might have a beneficial effect on the skin barrier and thus might decrease disease severity.
Comparison 3: one moisturiser versus another moisturiser (3a to 3x, 22 studies, one reference included two studies (Fredriksson 1975), and one reference included three treatment arms (Miller 2011)).
Comparison 4: moisturisers versus active treatment:
4a ‐ Licochalcone‐containing cream versus hydrocortisone acetate 1% cream (three studies);
4b‐I to 4b‐VI ‐ Other moisturisers versus topical corticosteroids (six studies);
4c‐ Moisturisers versus topical immunomodulators (three studies).
Comparison 5: vehicle in combination with a moisturiser versus topical corticosteroids in combination with a moisturiser (three studies, one reference included four treatment arms (Berth‐Jones 2003)).
Comparison 6: topical active treatment in combination with a moisturiser versus topical active treatment only (six studies).
Where small‐study bias was suspected in the meta‐analyses, we used a fixed‐effect model sensitivity analyses for pooled data and we present the estimates in Table 14. We also performed stratified analyses for 'Risk of bias' domain for pooled data (where there were three or more studies) and the results are presented in Table 15. We could not perform a stratified analysis to compare study results from trials that were preregistered (e.g. available on ClinicalTrials.gov (www.clinicaltrials.gov)) with those without an available prespecified protocol because, a limited number of studies included in the meta‐analyses were preregistered.
5. Table of fixed‐effect sensitivity analyses.
| Analysis | Comparison | MD/RR/HR/SMD | 95% confidence interval | P value |
|
Analysis 1.1 Change from baseline in SCORAD |
Moisturisers versus no treatment Pooled data |
MD ‐2.51 | ‐3.66 to ‐1.37 | P < 0.0001 |
|
Analysis 1.2 Number of participants experiencing a flare |
Moisturisers versus no treatment Pooled data |
RR 0.39 | 0.22 to 0.68 | P = 0.0008 |
|
Analysis 1.4 Amount of topical steroids used |
Moisturisers versus no treatment Pooled data for the first 3 to 4 weeks |
MD ‐5.34 | ‐7.79 to ‐2.89 | P < 0.0001 |
| Moisturisers versus no treatment Single study data last 3 to 4 weeks |
MD 0.50 | ‐4.70 to 5.70 | P = 0.85 | |
| Moisturisers versus no treatment Pooled data for 6 to 8 weeks |
MD ‐8.11 | ‐11.00 to ‐5.22 | P < 0.00001 | |
|
Analysis 1.5 Change from baseline in quality of life |
Moisturisers versus no treatment Pooled data |
SMD ‐0.14 | ‐0.44 to 0.16 | P = 0.35 |
|
Analysis 2.1 Number of participants who experienced good improvement to total resolution |
Atopiclair versus vehicle Pooled data |
RR 4.16 | 2.96 to 5.86 | P < 0.00001 |
|
Analysis 2.2 Change from baseline itch measured on a VAS |
Atopiclair versus vehicle Pooled data |
MD ‐2.08 | ‐2.35 to ‐1.81 | P < 0.00001 |
|
Analysis 2.3 Number of participants reporting an adverse event |
Atopiclair versus vehicle Pooled data |
RR 1.04 | 0.80 to 1.35 | P = 0.78 |
|
Analysis 2.4 Change from baseline in EASI |
Atopiclair versus vehicle Pooled data |
MD ‐4.05 | ‐5.00 to ‐3.10 | P < 0.00001 |
|
Analysis 2.5 Number of participants experiencing a flare |
Atopiclair versus vehicle Pooled data |
RR 0.18 | 0.11 to 0.31 | P < 0.00001 |
|
Analysis 3.1 Change from baseline in skin capacitance |
Urea‐containing versus vehicle | MD 3.13 | 2.13 to 4.13 | P < 0.00001 |
|
Analysis 4.1 Numbers of participants reporting an adverse event |
Glycerol versus placebo cream Pooled data |
RR 0.89 | 0.67 to 1.18 | P = 0.46 |
|
Analysis 5.1 Change in disease severity as assessed by the investigators |
Oat‐containing cream versus vehicle or no treatment Pooled data |
SMD ‐0.19 | ‐0.43 to 0.05 | P = 0.12 |
|
Analysis 5.2 Change from baseline in quality of life |
Oat‐containing cream versus vehicle or no treatment Pooled data |
SMD ‐0.09 | ‐0.35 to 0.17 | P = 0.51 |
|
Analysis 6.1 Number of participants that experienced improvement |
All moisturisers versus vehicle, placebo or no treatment Pooled data |
RR 2.20 | 1.84 to 2.62 | P < 0.00001 |
|
Analysis 6.2 Change from baseline in itch |
All moisturisers versus vehicle, placebo or no treatment Pooled data |
SMD ‐0.88 | ‐1.04 to ‐0.72 | P < 0.00001 |
|
Analysis 6.3 Number of participants that expressed treatment satisfaction |
All moisturisers versus vehicle, placebo or no treatment Pooled data |
RR 1.69 | 1.35 to 2.11 | P < 0.00001 |
|
Analysis 6.4 Number of participants reporting an adverse event |
All moisturisers versus vehicle, placebo or no treatment Pooled data |
RR 1.06 | 0.88 to 1.27 | P = 0.56 |
|
Analysis 6.5 Change in disease severity as assessed by the investigators |
All moisturisers versus vehicle, placebo or no treatment Pooled data |
SMD ‐0.62 | ‐0.73 to ‐0.51 | P < 0.00001 |
|
Analysis 6.6 Number of participants experiencing a flare |
All moisturisers versus vehicle, placebo or no treatment Pooled data |
RR 0.35 | 0.26 to 0.47 | P < 0.00001 |
|
Analysis 6.7 Change from baseline in quality of life |
All moisturisers versus vehicle, placebo or no treatment Pooled data |
SMD ‐0.40 | ‐0.64 to ‐0.17 | P = 0.0006 |
|
Analysis 7.1 Change from baseline in TEWL |
Primrose oil versus placebo oil Pooled data |
MD ‐0.34 | ‐1.44 to 0.76 | P = 0.55 |
|
Analysis 7.2 Change from baseline in skin hydration |
Primrose oil versus placebo oil Pooled data |
MD 0.34 | ‐2.54 to 3.21 | P = 0.82 |
|
Analysis 8.1 Change from baseline in itch (VAS) |
Licochalcone versus hydrocortisone Pooled data |
MD ‐0.37 | ‐0.75 to ‐0.00 | P = 0.05 |
|
Analysis 8.2 Change from baseline in SCORAD |
Licochalcone versus hydrocortisone Pooled data |
MD ‐0.12 | ‐0.77 to 0.54 | P = 0.73 |
|
Analysis 8.3 Change from baseline in TEWL |
Licochalcone versus hydrocortisone Pooled data |
MD ‐2.04 | ‐3.60 to ‐0.49 | P = 0.010 |
|
Analysis 10.1 Number of participants reporting an adverse event |
Vehicle plus moisturiser versus fluticasone propionate plus moisturiser Pooled data |
RR 0.60 | 0.42 to 0.85 | P = 0.004 |
|
Analysis 10.2 Number of participants experiencing a flare |
Vehicle plus moisturiser versus fluticasone propionate plus moisturiser Pooled data |
RR 2.27 | 1.91 to 2.71 | P < 0.00001 |
|
Analysis 10.3 Hazard ratio for rate of flare |
Vehicle plus moisturiser versus fluticasone propionate plus moisturiser Pooled data |
HR 3.67 | 2.78 to 4.84 | P < 0.00001 |
|
Analysis 11.1 Change in disease severity as assessed by the investigators |
Active treatment in combination with a moisturiser versus active treatment only Pooled data |
SMD ‐0.87 | ‐1.17 to ‐0.57 | P = 0.00001 |
|
Analysis 11.2 Change in quality of life IDQOL |
Active treatment in combination with a moisturiser versus active treatment only Pooled data |
MD ‐1.31 | ‐2.70 to 0.09 | P = 0.07 |
|
Analysis 11.3 Change of quality of life DFI |
Active treatment in combination with a moisturiser versus active treatment only Pooled data |
MD ‐1.03 | ‐2.47 to 0.42 | P = 0.17 |
Abbreviations
DFI: dermatitis family impact EASI: eczema area and severity index IDQOL: infant's dermatitis quality of life; HR: hazard ratio MD: mean difference RR: risk ratio SCORAD: scoring atopic dermatitis SMD: standardised mean difference TEWL: transepidermal water loss VAS: visual analogue scale
6. Table with stratified analyses per domain of risk of bias.
| MOISURISER VERSUS NO MOISTURISER | ||||||
| Change from baseline in SCORAD | ||||||
| Variable | Number of studies | Number of participants in moisturiser group | Number of participants in control group | MD (95% CI) | Heterogeneity I² | P value |
| All trials (Giordano‐Labadie 2006; Grimalt 2007; Patrizi 2014) | 3 | 141 | 135 | ‐2.42 (‐4.55 to ‐0.28) | 68% | P = 0.03 |
| Sequence generation | ||||||
| Low risk (all trials) | 3 | 141 | 135 | ‐2.42 (‐4.55 to ‐0.28) | 68% | P = 0.03 |
| Allocation concealment | ||||||
| Low risk (all trials) | 3 | 141 | 135 | ‐2.42 (‐4.55 to ‐0.28) | 68% | P = 0.03 |
| Blinding of participants and personnel | ||||||
| High risk (all trials) | 3 | 141 | 135 | ‐2.42 (‐4.55 to ‐0.28) | 68% | P = 0.03 |
| Blinding of outcome assessment | ||||||
| High risk (all trials) | 3 | 141 | 135 | ‐2.42 (‐4.55 to ‐0.28) | 68% | P = 0.03 |
| Incomplete outcome data | ||||||
| Low risk (Giordano‐Labadie 2006; Patrizi 2014) | 2 | 63 | 65 | ‐3.39 (‐4.73 to ‐2.05) | 0% | P < 0.00001 |
| High risk (Grimalt 2007) | 1 | 78 | 70 | ‐0.16 (‐2.36 to 2.04) | NA | P = 0.89 |
| Selective reporting | ||||||
| Low risk (all trials) | 3 | 141 | 135 | ‐2.42 (‐4.55 to ‐0.28) | 68% | P = 0.03 |
| Other bias | ||||||
| Low risk (all trials) | 3 | 141 | 135 | ‐2.42 (‐4.55 to ‐0.28) | 68% | P = 0.03 |
| ATOPICLAIR VERSUS VEHICLE | ||||||
| Number of participants who considered their skin to have improved | ||||||
| Variable | Number of studies | Number of participants in Atopiclair group | Number of participants in vehicle group | RR (95% CI) | Heterogeneity I² | P value |
| All trials (Abramovits 2008; Belloni 2005; Boguniewicz 2008) | 3 | 232 | 158 | 4.51 (2.19 to 9.29) | 64% | P < 0.0001 |
| Sequence generation | ||||||
| Low risk (all trials) | 3 | 232 | 158 | 4.51 (2.19 to 9.29) | 64% | P < 0.0001 |
| Allocation concealment | ||||||
| Low risk (Abramovits 2008; Belloni 2005) | 2 | 160 | 88 | 3.09 (2.08 to 4.59) | 0% | P < 0.00001 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | 8.06 (3.95 to 16.42) | NA | P < 0.00001 |
| Blinding of participants and personnel | ||||||
| Low risk (Abramovits 2008; Belloni 2005) | 2 | 160 | 88 | 3.09 (2.08 to 4.59) | 0% | P < 0.00001 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | 8.06 (3.95 to 16.42) | NA | P < 0.00001 |
| Blinding of outcome assessment | ||||||
| Low risk (Abramovits 2008; Belloni 2005) | 2 | 160 | 88 | 3.09 (2.08 to 4.59) | 0% | P < 0.00001 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | 8.06 (3.95 to 16.42) | NA | P < 0.00001 |
| Incomplete outcome data | ||||||
| Low risk (Belloni 2005; Boguniewicz 2008) | 2 | 87 | 85 | 6.95 (3.69 to 13.07) | 0% | P < 0.00001 |
| High risk (Abramovits 2008) | 1 | 145 | 73 | 3.02 (2.00 to 4.56) | NA | P < 0.00001 |
| Selective reporting | ||||||
| Low risk (all trials) | 3 | 232 | 158 | 4.51 (2.19 to 9.29) | 64% | P < 0.0001 |
| Other bias | ||||||
| Low risk (all trials) | 3 | 232 | 158 | 4.51 (2.19 to 9.29) | 64% | P < 0.0001 |
| Change from baseline in itch measured on a VAS | ||||||
| Variable | Number of studies | Number of participants in Atopiclair group | Number of participants in vehicle group | MD (95% CI) | Heterogeneity I² | P value |
| All trials (Abramovits 2008; Belloni 2005; Boguniewicz 2008; Patrizi 2008) | 4 | 235 | 161 | ‐2.65 (‐4.21 to ‐1.09) | 97% | P = 0.0008 |
| Sequence generation | ||||||
| Low risk (all trials) | 4 | 235 | 161 | ‐2.65 (‐4.21 to ‐1.09) | 97% | P = 0.0008 |
| Allocation concealment | ||||||
| Low risk (Abramovits 2008; Belloni 2005; Patrizi 2008) | 3 | 163 | 91 | ‐2.25 (‐3.83 to ‐0.68) | 95% | P = 0.005 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | ‐3.80 (‐4.36 to ‐3.24) | NA | P < 0.00001 |
| Blinding of participants and personnel | ||||||
| Low risk (Abramovits 2008; Belloni 2005; Patrizi 2008) | 3 | 163 | 91 | ‐2.25 (‐3.83 to ‐0.68) | 95% | P = 0.005 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | ‐3.80 (‐4.36 to ‐3.24) | NA | P < 0.00001 |
| Blinding of outcome assessment | ||||||
| Low risk (Abramovits 2008; Belloni 2005; Patrizi 2008) | 3 | 163 | 91 | ‐2.25 (‐3.83 to ‐0.68) | 95% | P = 0.005 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | ‐3.80 (‐4.36 to ‐3.24) | NA | P < 0.00001 |
| Incomplete outcome data | ||||||
| Low risk (Belloni 2005; Boguniewicz 2008; Patrizi 2008) | 3 | 106 | 104 | ‐2.33 (‐4.13 to ‐0.52) | 97% | P = 0.01 |
| High risk ((Abramovits 2008) | 1 | 129 | 57 | ‐3.70 (‐4.66 to ‐2.74) | NA | P < 0.00001 |
| Selective reporting | ||||||
| Low risk (all trials) | 4 | 235 | 161 | ‐2.65 (‐4.21 to ‐1.09) | 97% | P = 0.0008 |
| Other bias | ||||||
| Low risk (all trials) | 4 | 235 | 161 | ‐2.65 (‐4.21 to ‐1.09) | 97% | P = 0.0008 |
| Change from baseline in EASI | ||||||
| Variable | Number of studies | Number of participants in Atopiclair group | Number of participants in vehicle group | MD (95% CI) | Heterogeneity I² | P value |
| All trials (Abramovits 2008; Belloni 2005; Boguniewicz 2008; Patrizi 2008) | 4 | 251 | 175 | ‐4.00 (‐5.42 to ‐2.57) | 51% | P < 0.00001 |
| Sequence generation | ||||||
| Low risk (all trials) | 4 | 251 | 175 | ‐4.00 (‐5.42 to ‐2.57) | 51% | P < 0.00001 |
| Allocation concealment | ||||||
| Low risk Abramovits 2008; Belloni 2005; Patrizi 2008) | 3 | 179 | 105 | ‐3.36 (‐4.47 to ‐2.25) | 0% | P < 0.00001 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | ‐5.99 (‐7.85 to ‐4.13) | NA | P < 0.00001 |
| Blinding of participants and personnel | ||||||
| Low risk Abramovits 2008; Belloni 2005; Patrizi 2008) | 3 | 179 | 105 | ‐3.36 (‐4.47 to ‐2.25) | 0% | P < 0.00001 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | ‐5.99 (‐7.85 to ‐4.13) | NA | P < 0.00001 |
| Blinding of outcome assessment | ||||||
| Low risk Abramovits 2008; Belloni 2005; Patrizi 2008) | 3 | 179 | 105 | ‐3.36 (‐4.47 to ‐2.25) | 0% | P < 0.00001 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | ‐5.99 (‐7.85 to ‐4.13) | NA | P < 0.00001 |
| Incomplete outcome data | ||||||
| Low risk (Belloni 2005) | 1 | 15 | 15 | ‐3.30 (‐5.67 to ‐0.93) | NA | P = 0.006 |
| Unclear risk (Boguniewicz 2008; Patrizi 2008) | 2 | 91 | 89 | ‐4.42 (‐7.73 to ‐1.10) | 77% | P = 0.009 |
| High risk (Abramovits 2008) | 1 | 145 | 71 | ‐3.62 (‐5.06 to ‐2.18) | NA | P < 0.0001 |
| Selective reporting | ||||||
| Low risk (all trials) | 4 | 251 | 175 | ‐4.00 (‐5.42 to ‐2.57) | 51% | P < 0.00001 |
| Other bias | ||||||
| Low risk (all trials) | 4 | 251 | 175 | ‐4.00 (‐5.42 to ‐2.57) | 51% | P < 0.00001 |
| OAT‐CONTAINING MOISTURISERS VERSUS VEHICLE OR NO TREATMENT (NO MOISTURISER) | ||||||
| Change from baseline in disease severity as assessed by the investigators (EASI and SCORAD) | ||||||
| Variable | Number of studies | Number of participants in oat‐containing moisturiser group | Number of participants in control group | SMD (95% CI) | Heterogeneity I² | P value |
| All trials (Giordano‐Labadie 2006; Grimalt 2007; Nebus 2009) | 3 | 138 | 134 | ‐0.23 (‐0.66 to 0.21) | 65% | P = 0.30 |
| Sequence generation | ||||||
| Low risk (all trials) | 3 | 138 | 134 | ‐0.23 (‐0.66 to 0.21) | 65% | P = 0.30 |
| Allocation concealment | ||||||
| Low risk (all trials) | 3 | 138 | 134 | ‐0.23 (‐0.66 to 0.21) | 65% | P = 0.30 |
| Blinding of participants and personnel | ||||||
| Low risk (Nebus 2009) | 1 | 25 | 25 | 0.01 (‐0.55 to 0.56) | NA | P = 0.98 |
| High risk (Giordano‐Labadie 2006; Grimalt 2007) | 2 | 113 | 109 | ‐0.33 (‐0.98 to 0.32) | 81% | P = 0.32 |
| Blinding of outcome assessment | ||||||
| Low risk (Nebus 2009) | 1 | 25 | 25 | 0.01 (‐0.55 to 0.56) | NA | P = 0.98 |
| High risk (Giordano‐Labadie 2006; Grimalt 2007) | 2 | 113 | 109 | ‐0.33 (‐0.98 to 0.32) | 81% | P = 0.32 |
| Incomplete outcome data | ||||||
| Low risk (Giordano‐Labadie 2006; Nebus 2009) | 2 | 60 | 64 | ‐0.36 (‐1.03 to 0.32) | 71% | P = 0.30 |
| High risk (Grimalt 2007) | 1 | 78 | 70 | ‐0.02 (‐0.35 to 0.30) | NA | P = 0.98 |
| Selective reporting | ||||||
| Low risk (all trials) | 3 | 138 | 134 | ‐0.23 (‐0.66 to 0.21) | 65% | P = 0.30 |
| Other bias | ||||||
| Low risk (all trials) | 3 | 138 | 134 | ‐0.23 (‐0.66 to 0.21) | 65% | P = 0.30 |
| Effect | ||||||
| No difference (Grimalt 2007; Nebus 2009) | 2 | 103 | 95 | ‐0.02 (‐0.29 to 0.26) | 0% | P = 0.91 |
| Difference in favour of oat‐containing moisturiser (Giordano‐Labadie 2006) | 1 | 35 | 39 | ‐0.69 (‐1.16 to ‐0.22) | NA | P = 0.004 |
| Change from baseline in quality of life | ||||||
| Variable | Number of studies | Number of participants in oat‐containing moisturiser group | Number of participants in control group | SMD (95% CI) | Heterogeneity I² | P value |
| All trials (Giordano‐Labadie 2006; Grimalt 2007; Nebus 2009) | 3 | 110 | 116 | ‐0.09 (‐0.37 to 0.19) | 12% | P = 0.53 |
| Sequence generation | ||||||
| Low risk (all trials) | 3 | 110 | 116 | ‐0.09 (‐0.37 to 0.19) | 12% | P = 0.53 |
| Allocation concealment | ||||||
| Low risk (all trials) | 3 | 110 | 116 | ‐0.09 (‐0.37 to 0.19) | 12% | P = 0.53 |
| Blinding of participants and personnel | ||||||
| Low risk (Nebus 2009) | 1 | 25 | 25 | 0.10 (‐0.46 to 0.65) | NA | P = 0.74 |
| High risk (Giordano‐Labadie 2006; Grimalt 2007) | 2 | 85 | 91 | ‐0.16 (‐0.55 to 0.24) | 42% | P = 0.44 |
| Blinding of outcome assessment | ||||||
| Low risk (Nebus 2009) | 1 | 25 | 25 | 0.10 (‐0.46 to 0.65) | NA | P = 0.74 |
| High risk (Giordano‐Labadie 2006; Grimalt 2007) | 2 | 85 | 91 | ‐0.16 (‐0.55 to 0.24) | 42% | P = 0.44 |
| Incomplete outcome data | ||||||
| Low risk (Giordano‐Labadie 2006; Nebus 2009) | 2 | 60 | 64 | ‐0.17 (‐0.63 to 0.29) | 39% | P = 0.48 |
| High risk (Grimalt 2007) | 1 | 50 | 52 | 0.03 (‐0.36 to 0.41) | NA | P = 0.89 |
| Selective reporting | ||||||
| Low risk (all trials) | 3 | 110 | 116 | ‐0.09 (‐0.37 to 0.19) | 12% | P = 0.53 |
| Other bias | ||||||
| Low risk (all trials) | 3 | 110 | 116 | ‐0.09 (‐0.37 to 0.19) | 12% | P = 0.53 |
| ALL MOISTURISERS VERSUS VEHICLE TO PLACEBO OR NO MOISTURISER | ||||||
| Number of participants who considered their skin to have improved | ||||||
| Variable | Number of studies | Number of participants in moisturiser group | Number of participants in control group | RR (95% CI) | Heterogeneity I² | P value |
| All studies (Abramovits 2008; Belloni 2005; Boguniewicz 2008; Lodén 2002; Nebus 2009) | 5 | 323 | 249 | 2.46 (1.16 to 5.23) | 95% | P = 0.02 |
| Sequence generation | ||||||
| Low risk (Abramovits 2008; Belloni 2005; Boguniewicz 2008; Nebus 2009 | 4 | 257 | 183 | 3.10 (0.98 to 9.82) | 95% | P = 0.05 |
| Unclear risk (Lodén 2002) | 1 | 66 | 66 | 1.24 (1.03 to 1.49) | NA | P = 0.02 |
| Allocation concealment | ||||||
| Low risk (Abramovits 2008; Belloni 2005; Nebus 2009) | 3 | 185 | 113 | 2.19 (0.75 to 6.39) | 95% | P = 0.15 |
| Unclear risk (Boguniewicz 2008; Lodén 2002) | 2 | 138 | 136 | 3.11 (0.25 to 38.71) | 98% | P = 0.98 |
| Blinding of participants and personnel | ||||||
| Low risk (Abramovits 2008; Belloni 2005; Nebus 2009) | 3 | 185 | 113 | 2.19 (0.75 to 6.39) | 95% | P = 0.15 |
| Unclear risk (Boguniewicz 2008; Lodén 2002) | 2 | 138 | 136 | 3.11 (0.25 to 38.71) | 98% | P = 0.98 |
| Blinding of outcome assessment | ||||||
| Low risk (Abramovits 2008; Belloni 2005; Nebus 2009) | 3 | 185 | 113 | 2.19 (0.75 to 6.39) | 95% | P = 0.15 |
| Unclear risk (Boguniewicz 2008; Lodén 2002) | 2 | 138 | 136 | 3.11 (0.25 to 38.71) | 98% | P = 0.98 |
| Incomplete outcome data | ||||||
| Low risk (Belloni 2005; Lodén 2002; Nebus 2009) | 3 | 106 | 106 | 1.23 (0.94 to 1.62) | 48% | P = 0.13 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | 8.06 (3.95 to 16.42) | NA | P < 0.00001 |
| High risk (Abramovits 2008) | 1 | 145 | 73 | 3.02 (2.00 to 4.56) | NA | P < 0.00001 |
| Selective reporting | ||||||
| Low risk (all trials) | 5 | 323 | 249 | 2.46 (1.16 to 5.23) | 95% | P = 0.02 |
| Other bias | ||||||
| Low risk (all trials) | 5 | 323 | 249 | 2.46 (1.16 to 5.23) | 95% | P = 0.02 |
| Change from baseline in itch | ||||||
| Variable | Number of studies | Number of participants in moisturiser group | Number of participants in control group | SMD (95% CI) | Heterogeneity I² | P value |
| All studies (Abramovits 2008; Belloni 2005; Boguniewicz 2008; Boralevi 2014; Nebus 2009; Patrizi 2008; Patrizi 2014) | 7 | 412 | 337 | ‐1.10 (‐1.83 to ‐0.38) | 94% | P = 0.003 |
| Sequence generation | ||||||
| Low risk (all trials) | 7 | 412 | 337 | ‐1.10 (‐1.83 to ‐0.38) | 94% | P = 0.003 |
| Allocation concealment | ||||||
| Low risk (Abramovits 2008; Belloni 2005; Boralevi 2014; Nebus 2009; Patrizi 2008; Patrizi 2014) | 6 | 340 | 267 | ‐0.89 (‐1.56 to ‐0.23) | 91% | P = 0.009 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | ‐2.22 (‐2.64 to ‐1.80) | NA | P < 0.00001 |
| Blinding of participants and personnel | ||||||
| Low risk (Abramovits 2008; Belloni 2005; Boralevi 2014; Nebus 2009; Patrizi 2008) | 5 | 312 | 241 | ‐0.98 (‐1.79 to ‐0.18) | 93% | P < 0.00001 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | ‐2.22 (‐2.64 to ‐1.80) | NA | P < 0.00001 |
| High risk (Patrizi 2014) | 1 | 28 | 26 | ‐0.52 (‐1.06 to 0.03) | NA | P = 0.06 |
| Blinding of outcome assessment | ||||||
| Low risk (Abramovits 2008; Belloni 2005; Boralevi 2014; Nebus 2009; Patrizi 2008) | 5 | 312 | 241 | ‐0.98 (‐1.79 to ‐0.18) | 93% | P < 0.00001 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | ‐2.22 (‐2.64 to ‐1.80) | NA | P < 0.00001 |
| High risk (Patrizi 2014) | 1 | 28 | 26 | ‐0.52 (‐1.06 to 0.03) | NA | P = 0.06 |
| Incomplete outcome data | ||||||
| Low risk (Belloni 2005; Boralevi 2014; Nebus 2009; Patrizi 2014) | 4 | 192 | 191 | ‐0.38 (‐0.94 to 0.17) | 80% | P = 0.18 |
| Unclear risk (Boguniewicz 2008; Patrizi 2008) | 2 | 91 | 89 | ‐2.29 (‐2.67 to ‐1.91) | 0% | P < 0.00001 |
| High risk (Abramovits 2008) | 1 | 129 | 57 | ‐1.33 (‐1.67 to ‐0.99) | NA | P < 0.00001 |
| Selective reporting | ||||||
| Low risk (all trials) | 7 | 412 | 337 | ‐1.10 (‐1.83 to ‐0.38) | 94% | P = 0.003 |
| Other bias | ||||||
| Low risk (all trials) | 7 | 412 | 337 | ‐1.10 (‐1.83 to ‐0.38) | 94% | P = 0.003 |
| Number of participants who expressed treatment satisfaction | ||||||
| Variable | Number of studies | Number of participants in moisturiser group | Number of participants in control group | RR (95% CI) | Heterogeneity I² | P value |
| All trials (Abramovits 2008; Belloni 2005; Nebus 2009) | 3 | 185 | 113 | 1.35 (0.77 to 2.36) | 83% | P = 0.29 |
| Sequence generation | ||||||
| Low risk (all trials) | 3 | 185 | 113 | 1.35 (0.77 to 2.36) | 83% | P = 0.29 |
| Allocation concealment | ||||||
| Low risk (all trials) | 3 | 185 | 113 | 1.35 (0.77 to 2.36) | 83% | P = 0.29 |
| Blinding of participants and personnel | ||||||
| Low risk (all trials) | 3 | 185 | 113 | 1.35 (0.77 to 2.36) | 83% | P = 0.29 |
| Blinding of outcome assessment | ||||||
| Low risk (all trials) | 3 | 185 | 113 | 1.35 (0.77 to 2.36) | 83% | P = 0.29 |
| Incomplete outcome data | ||||||
| Low risk (Belloni 2005; Nebus 2009) | 2 | 40 | 40 | 1.04 (0.77 to 1.42) | 0% | P = 0.79 |
| High risk (Abramovits 2008) | 1 | 145 | 73 | 2.14 (1.58 to 2.89) | NA | P < 0.00001 |
| Selective reporting | ||||||
| Low risk (all trials) | 3 | 185 | 113 | 1.35 (0.77 to 2.36) | 83% | P = 0.29 |
| Other bias | ||||||
| Low risk (all trials) | 3 | 185 | 113 | 1.35 (0.77 to 2.36) | 83% | P = 0.29 |
| Number of participants who reported an adverse event | ||||||
| Variable | Number of studies | Number of participants in moisturiser group | Number of participants in control group | RR (95% CI) | Heterogeneity I² | P value |
| All trials (Abramovits 2008; Belloni 2005; Boguniewicz 2008; Boralevi 2014; Gayraud 2015; Grimalt 2007; Korting 2010; Lodén 2002; Patrizi 2008; Tan 2010) | 10 | 680 | 595 | 1.03 (0.82 to 1.30) | 21% | P = 0.80 |
| Sequence generation | ||||||
| Low risk (Abramovits 2008; Belloni 2005; Boguniewicz 2008; Boralevi 2014; Gayraud 2015; Grimalt 2007; Korting 2010; Patrizi 2008; Tan 2010) | 9 | 614 | 529 | 0.96 (0.74 to 1.24) | 16% | P = 0.76 |
| Unclear risk (Lodén 2002) | 1 | 66 | 66 | 1.31 (0.89 to 1.91) | NA | P = 0.17 |
| Allocation concealment | ||||||
| Low risk ((Abramovits 2008; Belloni 2005; Boralevi 2014; Gayraud 2015; Grimalt 2007; Korting 2010; Patrizi 2008; Tan 2010) | 7 | 491 | 411 | 1.00 (0.65 to 1.55) | 35% | P = 0.99 |
| Unclear risk (Boguniewicz 2008; Korting 2010; Lodén 2002) | 3 | 189 | 184 | 1.08 (0.82 to 1.43) | 15% | P = 0.59 |
| Blinding of participants and personnel | ||||||
| Low risk (Abramovits 2008; Belloni 2005; Boralevi 2014; Gayraud 2015; Patrizi 2008; Tan 2010) | 6 | 400 | 329 | 0.94 (0.72 to 1.24) | 0% | P = 0.67 |
| Unclear risk (Boguniewicz 2008; Lodén 2002) | 2 | 138 | 136 | 1.11 (0.83 to 1.48) | 26% | P = 0.49 |
| High risk (Grimalt 2007; Korting 2010) | 2 | 142 | 130 | 2.27 (0.06 to 90.70) | 80% | P = 0.66 |
| Blinding of outcome assessment | ||||||
| Low risk (Abramovits 2008; Belloni 2005; Boralevi 2014; Gayraud 2015; Patrizi 2008; Tan 2010) | 6 | 400 | 329 | 0.94 (0.72 to 1.24) | 0% | P = 0.67 |
| Unclear risk (Boguniewicz 2008; Lodén 2002) | 2 | 138 | 136 | 1.11 (0.83 to 1.48) | 26% | P = 0.49 |
| High risk (Grimalt 2007; Korting 2010) | 2 | 142 | 130 | 2.27 (0.06 to 90.70) | 80% | P = 0.66 |
| Incomplete outcome data | ||||||
| Low risk (Belloni 2005; Boralevi 2014; Gayraud 2015; Korting 2010; Lodén 2002; Tan 2010) | 6 | 352 | 350 | 0.99 (0.70 to 1.40) | 23% | P = 0.96 |
| Unclear risk (Boguniewicz 2008; Patrizi 2008) | 2 | 92 | 90 | 0.95 (0.69 to 1.30) | 0% | P = 0.73 |
| High risk (Abramovits 2008; Grimalt 2007) | 2 | 236 | 155 | 3.04 (0.24 to 38.72) | 71% | P = 0.39 |
| Selective reporting | ||||||
| Low risk (all trials) | 10 | 680 | 595 | 1.03 (0.82 to 1.30) | 21% | P = 0.80 |
| Other bias | ||||||
| Low risk (all trials) | 10 | 680 | 595 | 1.03 (0.82 to 1.30) | 21% | P = 0.80 |
| Change in disease severity as assessed by the investigators | ||||||
| Variable | Number of studies | Number of participants in moisturiser group | Number of participants in control group | SMD (95% CI) | Heterogeneity I² | P value |
| All studies (Abramovits 2008; Belloni 2005; Boguniewicz 2008; Boralevi 2014; Gayraud 2015; Giordano‐Labadie 2006; Grimalt 2007; Korting 2010; Nebus 2009; Patrizi 2008; Patrizi 2014; Tan 2010) | 12 | 683 | 598 | ‐0.65 (‐0.89 to ‐0.41) | 75% | P < 0.00001 |
| Sequence generation | ||||||
| Low risk (all trials) | 12 | 683 | 598 | ‐0.65 (‐0.89 to ‐0.41) | 75% | P < 0.00001 |
| Allocation concealment | ||||||
| Low risk (Abramovits 2008; Belloni 2005; Boralevi 2014; Gayraud 2015; Giordano‐Labadie 2006; Grimalt 2007; Nebus 2009; Patrizi 2008; Patrizi 2014; Tan 2010) | 10 | 561 | 481 | ‐0.53 (‐0.76 to ‐0.30) | 66% | P = 0.009 |
| Unclear risk (Boguniewicz 2008; Korting 2010) | 2 | 122 | 117 | ‐1.15 (‐1.43 to ‐0.88) | 0% | P < 0.00001 |
| Blinding of participants and personnel | ||||||
| Low risk (Abramovits 2008; Belloni 2005; Boralevi 2014; Gayraud 2015; Nebus 2009; Patrizi 2008; Tan 2010) | 7 | 420 | 346 | ‐0.53 (‐0.77 to ‐0.30) | 52% | P < 0.00001 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | ‐1.04 (‐1.39 to ‐0.69) | NA | P < 0.00001 |
| High risk ( Giordano‐Labadie 2006; Grimalt 2007; Korting 2010; Patrizi 2014) | 4 | 191 | 182 | ‐0.77 (‐1.41 to ‐0.12) | 88% | P = 0.02 |
| Blinding of outcome assessment | ||||||
| Low risk (Abramovits 2008; Belloni 2005; Boralevi 2014; Gayraud 2015; Nebus 2009; Patrizi 2008; Tan 2010) | 7 | 420 | 346 | ‐0.53 (‐0.77 to ‐0.30) | 52% | P < 0.00001 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | ‐1.04 (‐1.39 to ‐0.69) | NA | P < 0.00001 |
| High risk (Giordano‐Labadie 2006; Grimalt 2007; Korting 2010; Patrizi 2014) | 4 | 191 | 182 | ‐0.77 (‐1.41 to ‐0.12) | 88% | P = 0.02 |
| Incomplete outcome data | ||||||
| Low risk (Belloni 2005; Boralevi 2014; Gayraud 2015; Giordano‐Labadie 2006; Korting 2010; Nebus 2009; Patrizi 2014; Tan 2010 | 8 | 369 | 368 | ‐0.66 (‐0.96 to ‐0.36) | 71% | P < 0.0001 |
| Unclear risk (Boguniewicz 2008; Patrizi 2008) | 2 | 91 | 89 | ‐0.93 (‐1.29 to ‐0.57) | 17% | P < 0.00001 |
| High risk (Abramovits 2008; Grimalt 2007) | 2 | 223 | 141 | ‐0.41 (‐1.17 to 0.35) | 92% | P = 0.29 |
| Selective reporting | ||||||
| Low risk (all trials) | 12 | 683 | 598 | ‐0.65 (‐0.89 to ‐0.41) | 75% | P < 0.00001 |
| Other bias | ||||||
| Low risk (all trials) | 12 | 683 | 598 | ‐0.65 (‐0.89 to ‐0.41) | 75% | P < 0.00001 |
| Number of participants who experienced a flare | ||||||
| Variable | Number of studies | Number of participants in moisturiser group | Number of participants in control group | RR (95% CI) | Heterogeneity I² | P value |
| All studies (Abramovits 2008; Boguniewicz 2008; Gayraud 2015; Patrizi 2008; Weber 2015; Wirén 2009) | 6 | 341 | 266 | 0.33 (0.17 to 0.62) | 73% | P = 0.0006 |
| Sequence generation | ||||||
| Low risk (all trials) | 6 | 341 | 266 | 0.33 (0.17 to 0.62) | 73% | P = 0.0006 |
| Allocation concealment | ||||||
| Low risk (Abramovits 2008; Gayraud 2015; Patrizi 2008; Weber 2015; Wirén 2009) | 5 | 269 | 196 | 0.33 (0.15 to 0.71) | 78% | P = 0.005 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | 0.29 (0.12 to 0.68) | NA | P = 0.005 |
| Blinding of participants and personnel | ||||||
| Low risk (Abramovits 2008; Gayraud 2015; Patrizi 2008) | 3 | 227 | 151 | 0.27 (0.06 to 1.20) | 89% | P = 0.09 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | 0.29 (0.12 to 0.68) | NA | P = 0.005 |
| High risk (Weber 2015; Wirén 2009) | 2 | 42 | 45 | 0.40 (0.23 to 0.70) | 0% | P = 0.001 |
| Blinding of outcome assessment | ||||||
| Low risk (Abramovits 2008; Gayraud 2015; Patrizi 2008) | 3 | 227 | 151 | 0.27 (0.06 to 1.20) | 89% | P = 0.09 |
| Unclear risk (Boguniewicz 2008) | 1 | 72 | 70 | 0.29 (0.12 to 0.68) | NA | P = 0.005 |
| High risk (Weber 2015; Wirén 2009) | 2 | 42 | 45 | 0.40 (0.23 to 0.70) | 0% | P = 0.001 |
| Incomplete outcome data | ||||||
| Low risk (Gayraud 2015; Weber 2015; Wirén 2009) | 3 | 104 | 106 | 0.54 (0.31 to 0.92) | 47% | P = 0.02 |
| Unclear risk (Boguniewicz 2008; Patrizi 2008) | 2 | 92 | 89 | 0.26 (0.12 to 0.57) | 0% | P = 0.0007 |
| High risk (Abramovits 2008) | 1 | 145 | 71 | 0.14 (0.07 to 0.28) | NA | P < 0.00001 |
| Selective reporting | ||||||
| Low risk (all trials) | 6 | 341 | 266 | 0.33 (0.17 to 0.62) | 73% | P = 0.0006 |
| Other bias | ||||||
| Low risk (all trials) | 6 | 341 | 266 | 0.33 (0.17 to 0.62) | 73% | P = 0.0006 |
| Change from baseline in quality of life | ||||||
| Variable | Number of studies | Number of participants in moisturiser group | Number of participants in control group | SMD (95% CI) | Heterogeneity I² | P value |
| All trials (Gayraud 2015; Giordano‐Labadie 2006; Grimalt 2007) | 3 | 146 | 154 | ‐0.39 (‐0.90 to 0.12) | 79% | P = 0.13 |
| Sequence generation | ||||||
| Low risk (all trials) | 3 | 146 | 154 | ‐0.39 (‐0.90 to 0.12) | 79% | P = 0.13 |
| Allocation concealment | ||||||
| Low risk (all trials) | 3 | 146 | 154 | ‐0.39 (‐0.90 to 0.12) | 79% | P = 0.13 |
| Blinding of participants and personnel | ||||||
| Low risk (Gayraud 2015) | 1 | 62 | 61 | ‐0.81 (‐1.18 to ‐0.44) | NA | P < 0.0001 |
| High risk (Giordano‐Labadie 2006; Grimalt 2007) | 2 | 84 | 93 | ‐0.15 (‐0.55 to 0.24) | 42% | P = 0.44 |
| Blinding of outcome assessment | ||||||
| Low risk (Gayraud 2015) | 1 | 62 | 61 | ‐0.81 (‐1.18 to ‐0.44) | NA | P < 0.0001 |
| High risk (Giordano‐Labadie 2006; Grimalt 2007) | 2 | 84 | 93 | ‐0.15 (‐0.55 to 0.24) | 42% | P = 0.44 |
| Incomplete outcome data | ||||||
| Low risk (Gayraud 2015; Giordano‐Labadie 2006) | 2 | 97 | 100 | ‐0.62 (‐1.04 to ‐0.19) | 52% | P = 0.004 |
| High risk (Grimalt 2007) | 1 | 49 | 54 | 0.03 (‐0.36 to 0.41) | NA | P = 0.89 |
| Selective reporting | ||||||
| Low risk (all trials) | 3 | 146 | 154 | ‐0.39 (‐0.90 to 0.12) | 79% | P = 0.13 |
| Other bias | ||||||
| Low risk (all trials) | 3 | 146 | 154 | ‐0.39 (‐0.90 to 0.12) | 79% | P = 0.13 |
| LICOCHALCONE‐CONTAINING MOISTURISERS VERSUS HYDROCORTISONE ACETATE 1% CREAM | ||||||
| Change from baseline in disease severity as assessed by the investigators (SCORAD) | ||||||
| Variable | Number of studies | Number of participants in licochalcone group | Number of participants in hydrocortisone group | MD (95% CI) | Heterogeneity I² | P value |
| All trials (Angelova‐Fischer 2014; Udompataikul 2011; Wanakul 2013) | 3 | 96 (within‐participant) | 96 (within‐participant) | 0.08 (‐1.96 to 2.13) | 85% | P = 0.94 |
| Sequence generation | ||||||
| Low risk (Angelova‐Fischer 2014; Wanakul 2013) | 2 | 70 (within‐participant) | 70 (within‐participant) | ‐0.90 (‐2.85 to 1.05) | 82% | P = 0.32 |
| Unclear risk (Udompataikul 2011) | 1 | 26 (within‐participant) | 26 (within‐participant) | 2.57 (0.59 to 4.55) | NA | P = 0.01 |
| Blinding of participants and personnel | ||||||
| Low risk (Wanakul 2013) | 1 | 52 (within‐participant) | 52 (within‐participant) | ‐2.00 (‐3.47 to ‐0.53) | NA | P = 0.008 |
| Unclear risk (Angelova‐Fischer 2014; Udompataikul 2011) | 2 | 44 (within‐participant) | 44 (within‐participant) | 1.12 (‐1.38 to 3.61) | 82% | P = 0.38 |
| Blinding of outcome assessment | ||||||
| Low risk (Wanakul 2013) | 1 | 52 (within‐participant) | 52 (within‐participant) | ‐2.00 (‐3.47 to ‐0.53) | NA | P = 0.008 |
| High risk (Angelova‐Fischer 2014; Udompataikul 2011) | 2 | 44 (within‐participant) | 44 (within‐participant) | 1.12 (‐1.38 to 3.61) | 82% | P = 0.38 |
| Incomplete outcome data | ||||||
| Low risk (Angelova‐Fischer 2014; Wanakul 2013) | 2 | 70 (within‐participant) | 70 (within‐participant) | ‐0.90 (‐2.85 to 1.05) | 82% | P = 0.32 |
| Unclear risk (Udompataikul 2011) | 1 | 26 (within‐participant) | 26 (within‐participant) | 2.57 (0.59 to 4.55) | NA | P = 0.01 |
| Selective reporting | ||||||
| All studies | 3 | 96 (within‐participant) | 96 (within‐participant) | 0.08 (‐1.96 to 2.13) | 85% | P = 0.94 |
| Other bias | ||||||
| All studies | 3 | 96 (within‐participant) | 96 (within‐participant) | 0.08 (‐1.96 to 2.13) | 85% | P = 0.94 |
| VEHICLE TREATMENT + MOISTURISER VERSUS FLUTICASONE TREATMENT TWICE WEEKLY + MOISTURISER | ||||||
| Number of participants reporting an adverse event | ||||||
| Variable | Number of studies | Number of participants in vehicle + moisturiser group | Number of participants in fluticasone propionate + moisturiser group | RR (95% CI) | Heterogeneity I² | P value |
| All studies (Berth‐Jones 2003 (2 studies); Glazenburg 2009; Hanifin 2002) | 4 | 312 | 406 | 0.51 (0.22 to 1.14) | 67% | P = 0.10 |
| Sequence generation | ||||||
| Low risk (Berth‐Jones 2003 (2 studies); Glazenburg 2009) | 3 | 193 | 177 | 0.30 (0.12 to 0.73) | NA | P = 0.008 |
| Unclear risk (Hanifin 2002) | 1 | 119 | 229 | 0.70 (0.48 to 1.04) | NA | P = 0.08 |
| Allocation concealment | ||||||
| Low risk (Berth‐Jones 2003 (2 studies)) | 2 | 157 | 138 | Not estimable | NA | NA |
| Unclear risk (Glazenburg 2009; Hanifin 2002) | 2 | 155 | 268 | 0.51 (0.22 to 1.14) | 67% | P = 0.10 |
| Blinding of participants and personnel | ||||||
| Low risk (Berth‐Jones 2003 (2 studies)) | 2 | 157 | 138 | Not estimable | NA | NA |
| Unclear risk (Glazenburg 2009; Hanifin 2002) | 2 | 155 | 268 | 0.51 (0.22 to 1.14) | 67% | P = 0.10 |
| Blinding of outcome assessment | ||||||
| Low risk (Berth‐Jones 2003 (2 studies)) | 2 | 157 | 138 | Not estimable | NA | NA |
| Unclear risk (Glazenburg 2009; Hanifin 2002) | 2 | 155 | 268 | 0.51 (0.22 to 1.14) | 67% | P = 0.10 |
| Incomplete outcome data | ||||||
| Unclear risk (all studies) | 4 | 312 | 406 | 0.51 (0.22 to 1.14) | 67% | P = 0.10 |
| Selective reporting | ||||||
| Low risk (all studies) | 4 | 312 | 406 | 0.51 (0.22 to 1.14) | 67% | P = 0.10 |
| Other bias | ||||||
| Low risk (all studies) | 4 | 312 | 406 | 0.51 (0.22 to 1.14) | 67% | P = 0.10 |
| Number of participants experiencing a flare | ||||||
| Variable | Number of studies | Number of participants in vehicle + moisturiser group | Number of participants in fluticasone propionate + moisturiser group | RR (95% CI) | Heterogeneity I² | P value |
| All studies (Berth‐Jones 2003 (2 studies); Glazenburg 2009; Hanifin 2002) | 4 | 312 | 406 | 2.17 (1.51 to 3.11) | 74% | P < 0.0001 |
| Sequence generation | ||||||
| Low risk (Berth‐Jones 2003 (2 studies); Glazenburg 2009) | 3 | 193 | 177 | 2.02 (1.24 to 3.30) | 76% | P = 0.005 |
| Unclear risk (Hanifin 2002) | 1 | 119 | 229 | 2.62 (2.03 to 3.39) | NA | P < 0.00001 |
| Allocation concealment | ||||||
| Low risk (Berth‐Jones 2003 (2 studies)) | 2 | 157 | 138 | 2.17 (0.88 to 5.37) | 88% | P = 0.09 |
| Unclear risk (Glazenburg 2009; Hanifin 2002) | 2 | 155 | 268 | 2.27 (1.62 to 3.19) | 54% | P < 0.00001 |
| Blinding of participants and personnel | ||||||
| Low risk (Berth‐Jones 2003 (2 studies)) | 2 | 157 | 138 | 2.17 (0.88 to 5.37) | 88% | P = 0.09 |
| Unclear risk (Glazenburg 2009; Hanifin 2002) | 2 | 155 | 268 | 2.27 (1.62 to 3.19) | 54% | P < 0.00001 |
| Blinding of outcome assessment | ||||||
| Low risk (Berth‐Jones 2003 (2 studies)) | 2 | 157 | 138 | 2.17 (0.88 to 5.37) | 88% | P = 0.09 |
| Unclear risk (Glazenburg 2009; Hanifin 2002) | 2 | 155 | 268 | 2.27 (1.62 to 3.19) | 54% | P < 0.00001 |
| Incomplete outcome data | ||||||
| Unclear risk (all studies) | 4 | 312 | 406 | 2.17 (1.51 to 3.11) | 74% | P < 0.0001 |
| Selective reporting | ||||||
| Low risk (all studies) | 4 | 312 | 406 | 2.17 (1.51 to 3.11) | 74% | P < 0.0001 |
| Other bias | ||||||
| Low risk (all studies) | 4 | 312 | 406 | 2.17 (1.51 to 3.11) | 74% | P < 0.0001 |
| Hazard ratio for rate of flare | ||||||
| Variable | Number of studies | Number of participants in fluticasone propionate + moisturiser group | Number of participants in vehicle + moisturiser group | HR (95% CI) | Heterogeneity I² | P value |
| All studies (Berth‐Jones 2003 (2 studies); Glazenburg 2009; Hanifin 2002) | 4 | 406 | 312 | 3.69 (1.80 to 7.55) | 85% | P = 0.0004 |
| Sequence generation | ||||||
| Low risk (Berth‐Jones 2003 (2 studies); Glazenburg 2009) | 3 | 177 | 193 | 2.84 (1.44 to 5.61) | 76% | P = 0.003 |
| Unclear risk (Hanifin 2002) | 1 | 229 | 119 | 7.70 (4.62 to 12.84) | NA | P < 0.00001 |
| Allocation concealment | ||||||
| Low risk (Berth‐Jones 2003 (2 studies)) | 2 | 138 | 157 | 3.26 (1.09 to 9.74) | 87% | P = 0.03 |
| Unclear risk (Glazenburg 2009; Hanifin 2002) | 2 | 268 | 155 | 4.16 (1.21 to 14.31) | 89% | P = 0.02 |
| Blinding of participants and personnel | ||||||
| Low risk (Berth‐Jones 2003 (2 studies)) | 2 | 138 | 157 | 3.26 (1.09 to 9.74) | 87% | P = 0.03 |
| Unclear risk (Glazenburg 2009; Hanifin 2002) | 2 | 268 | 155 | 4.16 (1.21 to 14.31) | 89% | P = 0.02 |
| Blinding of outcome assessment | ||||||
| Low risk (Berth‐Jones 2003 (2 studies)) | 2 | 138 | 157 | 3.26 (1.09 to 9.74) | 87% | P = 0.03 |
| Unclear risk (Glazenburg 2009; Hanifin 2002) | 2 | 268 | 155 | 4.16 (1.21 to 14.31) | 89% | P = 0.02 |
| Incomplete outcome data | ||||||
| Unclear risk (all studies ) | 4 | 406 | 312 | 3.69 (1.80 to 7.55) | 85% | P = 0.0004 |
| Selective reporting | ||||||
| Low risk (all studies) | 4 | 406 | 312 | 3.69 (1.80 to 7.55) | 85% | P = 0.0004 |
| Other bias | ||||||
| Low risk (all studies) | 4 | 406 | 312 | 3.69 (1.80 to 7.55) | 85% | P = 0.0004 |
NA not applicable; MD mean difference; SMD standardised mean difference; RR risk ratio; HR hazard ratio
Analyses are only shown when we were able to pool data of at least two studies.
(1) Moisturisers versus no treatment (i.e. no moisturiser)
Six studies (413 participants) evaluated this comparison (Giordano‐Labadie 2006; Grimalt 2007; Patrizi 2014; Simpson 2013; Weber 2015; Wirén 2009); however, in Patrizi 2014 and Weber 2015, the comparator consisted of a cleaning product only. Study duration varied from four weeks in the Patrizi 2014 and Simpson 2013 studies, to six months in the Weber 2015 and Wirén 2009 studies. Four studies were conducted in children (Giordano‐Labadie 2006; Grimalt 2007; Patrizi 2014; Weber 2015), and the other two, in adults (Simpson 2013; Wirén 2009). The participants in these studies had predominantly mild to moderate eczema.
The Simpson 2013 study, which was reported only as 'investigator‐blinded', included mainly investigator‐assessed outcomes, but because the method of blinding was not clearly specified, we judged it to be at unclear risk of bias. None of the other studies were blinded; therefore, we assessed them as being at a high risk of bias.
In Giordano‐Labadie 2006 and Grimalt 2007, application of moderate to strong topical corticosteroids was allowed in both treatment arms, whilst in Weber 2015, 'Eucerin Eczema Relief Instant Therapy' was allowed on active lesions, and Wirén 2009 allowed topical corticosteroids on areas other than the target lesions.
See also Table 1.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed in any of the studies; however, 'itch' was evaluated in Patrizi 2014 (54 participants) on a 4‐point Likert scale (0 to 3), with a higher score indicating more severe itch. The mean change from baseline in itch in the emollient balm group (28 participants) was ‐1.24 (standard deviation (SD) 0.77) compared to ‐0.76 (SD 1.05) in the control group (26 participants), with a mean difference (MD) of ‐0.48 (95% confidence interval (CI) ‐0.97 to 0.01; P = 0.06).
Participant satisfaction
This outcome was not assessed in any of the studies.
Adverse events
Two studies reported some data on adverse events (Grimalt 2007; Simpson 2013). In Grimalt 2007, 8/91 participants reported adverse events in the active treatment group compared to 0/82 in the control group after six weeks (Peto odds ratio (OR) 7.26, 95% CI 1.76 to 29.92; P = 0.006). The P value of Fisher's Exact Test was 0.0071. Three adverse events were reported to be mild, three moderate, and two were severe, which led to treatment discontinuation. No further details were provided other than "all the adverse events spontaneously resolved without sequel." The Simpson 2013 study had a within‐participant design, in which the legs of 20 participants were randomised, and there were no treatment‐related adverse events experienced on either leg.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
Disease severity was assessed using the SCORing Atopic Dermatitis (SCORAD) index (scale: 0 to 103, higher scores indicate worse eczema) in three studies, with a total of 276 participants (Giordano‐Labadie 2006; Grimalt 2007; Patrizi 2014). In both Giordano‐Labadie 2006 and Grimalt 2007, moderate to strong topical corticosteroids were allowed in both treatment arms, and the participants in these two studies had higher baseline SCORAD scores, which indicated more severe disease, than those in Patrizi 2014. The baseline SCORAD values in Giordano‐Labadie 2006 were 25.96 (SD 7.67) in the moisturiser group and 23.3 (SD 7.63) in the non‐treated group; in Grimalt 2007, these baseline values were 35.63 (SD 11.92) versus 35.96 (SD 10.50) and in Patrizi 2014, 11.7 (SD 3.1) versus 10.2 (SD 3.3), which explains the considerable heterogeneity observed with the pooled data. The MD between the pooled moisturiser groups and control groups was ‐2.42 (95% CI ‐4.55 to ‐0.28; P = 0.03; I² = 68%; Analysis 1.1), favouring the moisturiser group. However, the minimal important difference (MID) for the SCORAD is estimated to be 8.7 (Schram 2012), and therefore this difference, although statistically significant, is not clinically relevant. As Giordano‐Labadie 2006 and Grimalt 2007 used topical corticosteroids in both treatment arms, the SCORAD decreased in each arm in a very substantial way and met the MID in both arms (but without meeting MID between arms). Grimalt 2007 was the only study that did not show a difference between the two treatments, while the other two studies with smaller sample sizes did show a difference (although did not meet MID). However, baseline differences in eczema severity as well as the use of topical corticosteroids might be responsible for this difference. All three studies were assessed as being at an overall high risk of bias due to lack of blinding, therefore, we did not conduct sensitivity analyses for overall risk of bias. However, when we conducted further stratified analyses for the individual domains of risk of bias, our repeat analysis showed no heterogeneity following the exclusion of Grimalt 2007, which was also judged to be at high risk of bias for incomplete outcome data (MD ‐3.39, 95% CI ‐4.73 to ‐2.05; P < 0.00001; I² = 0%; Table 15).
1.1. Analysis.

Comparison 1: Moisturisers versus no treatment (i.e. no moisturiser), Outcome 1: Change from baseline in SCORAD
The Simpson 2013 study, which had a within‐participant design (20 participants), used a dryness scale (0 to 4, with higher scores being worse) for assessment of this outcome. The mean change from baseline was ‐1.15 (SD 0.41) on the side treated with moisturiser versus ‐0.91 (SD 0.58) on the side that received no treatment. The mean of the paired differences was statistically significant at ‐0.24 (95% CI ‐0.42 to ‐0.06). This small difference in favour of moisturiser is unlikely to be clinically important.
Prevention of flares (lengthening the time to first flare)
Both Weber 2015 and Wirén 2009 (total of 87 participants) had a study duration of six months and assessed the efficacy of reducing the risk of flare. Combining data from the two studies, a total of 11/42 participants experienced a flare in the moisturiser group over a period of six months compared to 30/45 in the control group (risk ratio (RR) 0.40, 95% CI 0.23 to 0.70; P = 0.001; number needed to treat for an additional beneficial outcome (NNTB) = 3, 95% CI 2 to 5; Analysis 1.2). The RR showed a significant difference in favour of the moisturiser group. In both studies, the median time to flare in the moisturiser group was more than 180 days versus 28 days and 30 days for the control groups (Weber 2015 and Wirén 2009, respectively). The rate of flare in the control group was 3.74 times the rate in the moisturiser group (hazard ratio (HR) 3.74, 95% CI 1.86 to 7.50; P = 0.0002, I²= 0%; Analysis 1.3). These data indicate that with the use of moisturisers there are fewer flares, and the time to flare is lengthened.
1.2. Analysis.

Comparison 1: Moisturisers versus no treatment (i.e. no moisturiser), Outcome 2: Number of participants experiencing a flare
1.3. Analysis.

Comparison 1: Moisturisers versus no treatment (i.e. no moisturiser), Outcome 3: Rate of flare
Change in use of topical active treatment
Two of the studies in this comparison measured the amount of topical corticosteroids used (Giordano‐Labadie 2006; Grimalt 2007).
In Giordano‐Labadie 2006, data were available from 35/37 participants in the moisturiser group. The mean amount of topical corticosteroids (moderate and strong, class 2 and 3 respectively) used in the first part of the study (days 0 to 28) was 24.5 g (SD 12.51) in the moisturiser group, compared to 38 g (SD 18.63) in the control group (39 participants) (MD ‐13.50 g, 95% CI ‐20.67 to ‐6.33; P = 0.0002), which was a 35% reduction in the use of topical corticosteroids in the moisturiser group. This corresponded with a 50% reduction in SCORAD in the moisturiser group and a 48.7% reduction in SCORAD in the control group, demonstrating that the control group had to apply more topical corticosteroids to reach a similar reduction in SCORAD. From day 28 until day 56, 24.6 g (SD 9.89) was used in the moisturiser group versus 24.1 g (SD 12.85) in the control group, which is almost identical for both groups (MD 0.50 g, 95% CI ‐4.70 to 5.70; P = 0.85). The reduction in SCORAD was greater in the moisturiser group (Analysis 1.1), but the difference was not clinically relevant (see the 'Change from baseline in disease severity as assessed by the investigators' section).
In the first three weeks of the Grimalt 2007 study, 4.86 g (SD 8.57) of high‐potency topical corticosteroids was used in the moisturiser group (based on 78/91 participants) compared to 8.87 g (SD 11.46) in the control group (based on 70/82 participants) (MD ‐4.01 g, 95% CI ‐7.30 to ‐0.72; P = 0.02), which corresponds to a 45.2% reduction in the use of strong‐potency topical corticosteroids in the moisturiser group compared to the control group. The amount of moderate‐potency topical corticosteroids used was 4.66 g (SD 5.74) in the moisturiser group versus 4.91 g (SD 6.27) in the control group (MD ‐0.25 g, 95% CI ‐2.19 to 1.69; P = 0.80), which, in contrast to the use of strong‐potency topical corticosteroids, was not statistically significant. The total amount of high‐potency corticosteroids used over six weeks was 8.56 g (SD 15.37) in the moisturiser group and 14.7 g (SD 17.47) in the control group (MD ‐6.14 g, 95% CI ‐11.47 to ‐0.81; P = 0.02). Although this is a statistically significant difference, it did not hold true for the moderate‐potency topical corticosteroids, for which the amount used in the moisturiser group was 7.43 g (SD 9.98) versus 8.03 g (SD 10.29) in the control group (MD ‐0.60 g, 95% CI ‐3.87 to 2.67; P = 0.72). The amount of topical corticosteroids used from weeks three to six was not specified separately.
Analysis 1.4 is subgrouped by length of treatment. In the first few weeks, both studies showed a non‐statistically significant difference in favour of the moisturiser groups for the amount of corticosteroids used (MD ‐8.25 g, 95% CI ‐17.22 to 0.72; P = 0.07; I² = 82%), but no difference was seen in the last three to four weeks (MD 0.50 g, 95% CI ‐4.70 to 5.70) (data from Giordano‐Labadie 2006 only). However, the mean difference in the total amount of corticosteroids used over six to eight weeks was ‐9.30 g (95% CI ‐15.33 to ‐3.27; P = 0.003; I² = 68%). This is a statistically significant difference showing that the use of moisturisers decreased the need for topical corticosteroids. For this analysis in Grimalt 2007, data for both the moderate‐ and high‐potency corticosteroids were combined. The amount of total topical corticosteroids used in both treatment groups was much higher in Giordano‐Labadie 2006, which may explain the substantial heterogeneity.
1.4. Analysis.

Comparison 1: Moisturisers versus no treatment (i.e. no moisturiser), Outcome 4: Amount of topical steroids used
Changes in skin barrier function
Three studies reported data on transepidermal water loss (TEWL) (Patrizi 2014; Simpson 2013; Wirén 2009). The Wirén 2009 study only reported that "the difference in TEWL between the groups after three weeks of maintenance treatment did not reach statistical significance." Simpson 2013 had a within‐participant design, and therefore we did not pool the data with Patrizi 2014. A reduction in TEWL score equates to an improvement in skin barrier function. In Patrizi 2014, the mean change from baseline in TEWL at day 28 was ‐12.50 g/m²/h (SD 12.81) in the moisturiser group (28 participants) compared to 1.13 g/m²/h (SD 12.09) in the control group (26 participants), with a MD of ‐13.63 g/m²/h (95% CI ‐20.27 to ‐6.99; P < 0.0001).
In Simpson 2013 (a within‐participant design with 20 participants), the mean changes from baseline in TEWL were ‐1.59 g/m²/h (SD 0.97) on the moisturiser side and ‐0.42 g/m²/h (SD 1.13) on the control side, which were both minimal changes (statistically significant mean of the paired differences: ‐1.17 g/m²/h (95% CI ‐1.52 to ‐0.82)). In this study, measurement of skin capacitance was evaluated with a corneometer and showed an improvement of 16.91 units (SD 6.31) on the moisturiser side and 3.3 units (SD 3.86) on the control side (statistically significant mean of the paired differences: 13.61 units, 95% CI 11.60 to 15.60).
Change in health‐related quality of life
Change in health‐related quality of life was assessed in two studies (Giordano‐Labadie 2006; Grimalt 2007). Giordano‐Labadie 2006 used the Children's Dermatology Life Quality Index (CDLQI) with scoring ranging from 0 to 30. Scores between 0 and 1 indicate no effect on quality of life, while scores between 19 and 30 indicate an extremely large negative effect on quality of life (Lewis‐Jones 1995). In the moisturiser group the score had changed by ‐0.84 (SD 0.43) at day 56 and by ‐0.41 (1.50) in the control group. Grimalt 2007 used the Infant's Dermatitis Quality of Life Index (IDQOL) (Lewis‐Jones 2001), and the Dermatitis Family Impact (DFI) questionnaires (Lawson 1998), with scores in both ranging from 0 (no quality of life impairment) to 30 (most serious quality of life impairment). The mean change from baseline on the IDQOL was ‐2.57 (SD 35.51) in the moisturiser group (data only available for 49/91 participants) and ‐3.41 (SD 26.70) in the control group (data for 54/82 participants only). The standardised mean difference (SMD) in change from baseline quality of life between the moisturiser group and the control group was ‐0.15 (95% CI ‐0.55 to 0.24; P = 0.44; I² = 42%; Analysis 1.5). The reductions in scores in each treatment arm for both studies were small and not clinically important with no statistically significant difference between groups. The data from the second questionnaire in Grimalt 2007 (DFI) were in agreement with this analysis. For the DFI, the mean changes were ‐2.82 (SD 35.79) in the moisturiser group and ‐2.89 (SD 30.10) in the control group with a MD of 0.07 (95% CI ‐12.77 to 12.91; P = 0.99). A possible explanation for the statistical heterogeneity (I² = 42%) between the two treatments might be that in Grimalt 2007 40% of the participants did not complete the questionnaires, and this domain was therefore assessed as being at high risk of attrition bias.
1.5. Analysis.

Comparison 1: Moisturisers versus no treatment (i.e. no moisturiser), Outcome 5: Change from baseline in quality of life
(2) Moisturisers versus vehicle, placebo or no treatment (i.e. no moisturiser)
2a Atopiclair (containing glycyrrhetinic acid) three times a day versus vehicle three times a day
Four studies with a total of 450 participants reported data on this comparison (Abramovits 2008; Belloni 2005; Boguniewicz 2008; Patrizi 2008). We assessed the Belloni 2005 study as being at a low risk of bias, Abramovits 2008 at high risk of bias, and the other two at unclear risk of bias. Study duration ranged from 21 days (Belloni 2005), through 43 days (Boguniewicz 2008; Patrizi 2008), up to 50 days (Abramovits 2008). Both Boguniewicz 2008 and Patrizi 2008 were conducted in children, Belloni 2005 included children and adults, and Abramovits 2008 only investigated adults. All of the participants included in these studies had mild to moderate eczema.
In Boguniewicz 2008 and Patrizi 2008, low‐potency topical corticosteroids were allowed in both treatment arms, but only if really needed. Patrizi 2008 was a three‐arm study (see also comparison 3a, we did not consider Atopiclair light versus vehicle, as Atopiclair light was never marketed).
See also Table 2.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Three studies reported the number of participants who experienced improvement rated as good improvement to total resolution (Abramovits 2008; Belloni 2005; Boguniewicz 2008); this showed that 174/232 in the Atopiclair group experienced good improvement to total resolution versus 27/158 in the vehicle group (RR 4.51, 95% CI 2.19 to 9.29; P < 0.0001; I² = 64%; NNTB = 2, 95% CI 1 to 2; Analysis 2.1). When we removed the study with the smallest sample size (Belloni 2005), the effect estimate increased slightly showing that the meta‐analysis findings were robust. We conducted a sensitivity analysis based on these three studies. When we excluded the Abramovits 2008 study (which was at high risk of bias) from the analysis, our repeat analysis showed no residual heterogeneity (RR 6.95, 95% CI 3.69 to 13.07; P < 0.00001; I² = 0%; NNTB = 2, 95% CI 1 to 2).
2.1. Analysis.

Comparison 2: Atopiclair versus vehicle, Outcome 1: Number of participants who experienced good improvement to total resolution
Itch was addressed in all four studies via a visual analogue scale (VAS) that ran from 0 cm to 10 cm, with score of 0 indicating no itch. There was a significant reduction in itch in favour of the Atopiclair moisturiser group with a MD of ‐2.65 cm (95% CI ‐4.21 to ‐1.09; P = 0.0008; I² = 97%; Analysis 2.2). The only study at low risk of bias, Belloni 2005, showed a smaller effect, which might have been caused by the shorter treatment duration (three weeks versus six to seven weeks in the other studies). None of the sensitivity analyses (stratified by risk of bias or effect size) reduced the heterogeneity to a minimum.
2.2. Analysis.

Comparison 2: Atopiclair versus vehicle, Outcome 2: Change from baseline in itch measured on a VAS
Participant satisfaction
At the end of the Abramovits 2008 study, 119/145 participants were willing to continue treatment with Atopiclair, while only 28/73 wished to continue with vehicle (RR 2.14, 95% CI 1.58 to 2.89; P < 0.00001; NNTB = 2, 95% CI 2 to 3). In Belloni 2005, the participants were asked about their willingness to use the treatment again; 9/15 in both groups indicated that they 'might' (RR 1.00, 95% CI 0.56 to 1.79; P = 1.00), and 5/15 in the Atopiclair group indicated that they 'would' use it again versus 0/15 in the vehicle group (Peto OR 10.18, 95% CI 1.54 to 67.23; P = 0.02). The P value of the Fisher's Exact Test was 0.0421. This outcome was not assessed in Boguniewicz 2008, and in Patrizi 2008, no data were reported other than P values indicating the participants' desire to continue on the treatment, which read "P < 0.001 in favour of Atopiclair".
Adverse events
All four studies addressed adverse events. There was no statistically significant difference in the number reporting an adverse event in either group with 84/252 adverse events in the Atopiclair group and 59/178 in the vehicle group (RR 1.03, 95% CI 0.79 to 1.33; P = 0.83; I² = 0%; Analysis 2.3). As no adverse events were reported in either group in Belloni 2005, we repeated our analysis adding one adverse event in each group for this study, and the RR was 1.03 (95% CI 0.79 to 1.33), which made no difference.
2.3. Analysis.

Comparison 2: Atopiclair versus vehicle, Outcome 3: Number of participants reporting an adverse event
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
This outcome was assessed in all four studies with the EASI (for which the score rating runs from 0 to 72, with higher scores being worse (Hanifin 2001)), with a MD of ‐4.00 (95% CI ‐5.42 to ‐2.57; P < 0.00001; I² = 51%; Analysis 2.4) in favour of Atopiclair. The MID for the EASI is estimated at 6.6 (Schram 2012), and therefore the difference was not clinically relevant. Removing both of the studies with smaller sample sizes did slightly increase the MD (Belloni 2005; Patrizi 2008), therefore, we can conclude that the meta‐analysis is robust. The stratified sensitivity analyses per domain of risk of bias concluded that Boguniewicz 2008 demonstrated the greatest effect size, as well as being the only study in which there was uncertainty regarding the efficacy of the allocation concealment and of the blinding (see Table 15).
2.4. Analysis.

Comparison 2: Atopiclair versus vehicle, Outcome 4: Change from baseline in EASI
Prevention of flares (lengthening the time to first flare)
Occurrence of flares was measured as the number of participants who needed rescue medication in three of the four studies (Abramovits 2008; Boguniewicz 2008; Patrizi 2008). In the Atopiclair treatment arm, 15/237 of the participants experienced a flare versus 56/160 in the vehicle group, showing benefit in the treatment arm (RR 0.18, 95% CI 0.11 to 0.31; P < 0.00001; I² = 0%; NNTB = 3, 95% CI 3 to 5; Analysis 2.5). The study at high risk of bias, Abramovits 2008, did not appreciably alter the effect estimate In the sensitivity analysis (Analysis 2.5).
2.5. Analysis.

Comparison 2: Atopiclair versus vehicle, Outcome 5: Number of participants experiencing a flare
Change in use of topical active treatment
This outcome was not assessed in any of the studies.
Changes in skin barrier function
This outcome was not assessed in any of the studies.
Change in health‐related quality of life
This outcome was not assessed in any of the studies.
2b Urea‐containing moisturisers versus vehicle, placebo or no treatment (i.e. no moisturiser)
Four studies, with a total of 362 adult participants, examined urea‐containing cream versus vehicle, placebo, or no treatment (Bohnsack 1997; Lodén 2002; Wilhelm 1998; Wirén 2009). We assessed three of these as being at an unclear risk of bias (Bohnsack 1997; Lodén 2002; Wilhelm 1998), and the fourth as being at high risk of bias due to lack of blinding (Wirén 2009). The Bohnsack 1997, Lodén 2002, and Wilhelm 1998 studies were four weeks long, and Wirén 2009 had a duration of six months (this study is featured in Comparison 1 also). The objective of the Wirén 2009 study was to explore time to flare after treatment; treatment success was obtained in certain target areas with betamethasone valerate 0.1% (a steroid) and moisturiser, and Canoderm cream (containing urea) was compared with no treatment in the subsequent maintenance phase. Bohnsack 1997 and Wilhelm 1998 had a within‐participant design and did not allow topical treatments, while Lodén 2002 and Wirén 2009 did allow topical steroids in either treatment arm (though in Wirén 2009 they were permitted at areas other than the target areas during the maintenance phase). Lodén 2002 was a three‐armed study (see Comparisons 2c and 3o).
See Table 3.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed in Bohnsack 1997 and Wirén 2009. In Lodén 2002, 56/63 participants in the group treated with urea‐containing cream (4% urea and 4% sodium chloride) rated the dryness of their skin as improved versus 46/66 in the group treated with placebo (for ingredients, see Notes in Characteristics of included studies for Lodén 2002), with a statistically significant difference in favour of the urea‐containing cream (RR 1.28, 95% CI 1.06 to 1.53; P = 0.009; NNTB = 5, 95% CI 3 to 18).
Sixty‐one per cent of the 77 participants in the Wilhelm 1998 within‐participant study considered that the side treated with 10% urea cream showed moderate to very good improvement compared to 48.1% who felt that the side treated with vehicle showed moderate to good improvement. Itch was also assessed in this study, with 54.5% reporting improvement of itch on the side treated with urea cream and 45.5% reporting improvement on the vehicle side.
Participant satisfaction
Only Bohnsack 1997 assessed participant satisfaction, specifically smell, spreadability, penetration into the skin, and the feel of the skin, using a 4‐point Likert scale (1 = unsatisfactory, 2 = satisfactory, 3 = good, 4 = very good). Thirty‐two of the 38 participants thought the side treated with 10% urea cream smelt 'satisfactory to good', and 31/38 considered that the vehicle side smelt 'satisfactory' (RR 1.07, 95% CI 0.79 to 1.44; P = 0.68). Spreadability was assessed as 'satisfactory to very good' by 35/38 participants for the 10% urea cream and by 37/38 for the vehicle (RR 0.94, 95% 0.78 to 1.14; P = 0.55). Penetration into the skin was assessed as 'satisfactory to very good' by 26/38 participants for the 10% urea cream and as 'satisfactory to good' by 32/38 participants for the vehicle (RR 0.81, 95% CI 0.57 to 1.17; P = 0.26). Twenty‐seven out of 38 participants considered the feel of the skin on the 10% urea‐treated side as 'satisfactory to good', and 32/38 considered it to be 'satisfactory to good' on the vehicle‐treated side (RR 0.88, 95% CI 0.63 to 1.22; P = 0.43).
Adverse events
Only the Lodén 2002 trial assessed adverse events. Smarting was reported by 41/63 participants in the urea cream group and by 26/66 participants in the placebo group (RR 1.65, 95% CI 1.16 to 2.34; P = 0.005; NNTH = 4, 95% CI 2 to 11), which is a statistically significant difference in favour of the placebo cream.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
This outcome was not assessed in Wirén 2009. The Lodén 2002 study used the dry skin area and severity index (DASI) to assess disease severity (score from 4 to 20, with higher scores being worse) (Serup 1995). After four weeks, 56/63 in the urea cream‐treated group had improved, and 42/66 in the placebo cream group (RR 1.40, 95% CI 1.14 to 1.71; P = 0.001; NNTB = 4, 95% CI 3 to 9); this result favoured the urea‐containing cream and was consistent with the participant assessments.
The within‐participant Bohnsack 1997 study used a combined score for all participants to assess dryness (4‐point Likert scale (0 to 3); 0 = fine shiny skin surface, 1 = dry matte skin surface, 2 = mild scaling, 3 = obvious mild to moderate scaling). The combined total score for all 38 participants decreased from 91 to 63 on the side treated with 10% urea cream and from 88 to 70 on the vehicle side. The investigators of the study reported that this was not a statistically significant difference.
The within‐participant Wilhelm 1998 study used a sum score to assess change in disease severity (erythema, dryness, induration, papules, with each item scoring from 0 to 4, with higher values being worse). The mean change from baseline in the sum score after four weeks was ‐1.90 (SD 3.5) on the side treated with urea‐containing cream and ‐1.33 (SD 2.11) on the side treated with vehicle, with the mean of the paired differences being ‐0.57 (95% CI ‐1.14 to 0.0).
Prevention of flares (lengthening the time to first flare)
Only Wirén 2009 examined time to first flare. During the six‐month period of the trial, 7/22 of the 5% urea cream group experienced a flare compared with 15/22 of the no moisturiser group, which favours the use of moisturiser (RR 0.47, 95% CI 0.24 to 0.92; P = 0.03; NNTB = 3, 95% CI 2 to 11). In this study, the median time to flare was more than 180 days in the urea cream group versus 30 days for the no moisturiser group. The rate of flare in the no moisturiser group was 3.2 times that in the urea cream group (HR 3.2, 95% CI 1.3 to 7.8; P = 0.01). (See the data analysis for Wirén 2009 in Analysis 1.3). These data demonstrate that urea cream reduced the number of flares and prolonged time to flare compared to not using a moisturiser.
Change in use of topical active treatment
This outcome was not assessed in any of the studies.
Changes in skin barrier function
Bohnsack 1997 and Wilhelm 1998 (both within‐participant studies) assessed skin hydration with a corneometer in a total of 115 participants. In Bohnsack 1997, hydration increased over four weeks by 12 arbitrary units (SD 7.21) on the side treated with 10% urea cream and by 15.20 units (SD 7.92) on the vehicle‐treated side. In Wilhelm 1998 the changes were 11.80 (SD 6.90) arbitrary units on the side treated with urea cream and 6.20 (SD 6.58) units on the side treated with vehicle (pooled data showed a MD 1.23, 95% CI ‐7.39 to 9.86; P = 0.78; I² = 98%; Analysis 3.1). Improvements in skin hydration were seen in both arms, with the studies just showing slightly different results, with Bohnsack 1997 favouring vehicle and Wilhelm 1998 favouring the urea cream.
3.1. Analysis.

Comparison 3: Urea‐containing moisturiser versus vehicle, Outcome 1: Change from baseline in skin capacitance
The Wirén 2009 study measured TEWL, and the investigators reported that "the difference in TEWL between the groups after three weeks of maintenance treatment did not reach statistical significance."
Change in health‐related quality of life
This outcome was not assessed in any of the studies.
2c Glycerol‐containing moisturisers versus vehicle or placebo
The participants in the three studies that evaluated glycerol‐containing moisturises against vehicle or placebo had mild to moderate eczema (409 participants) (Boralevi 2014; Breternitz 2008; Lodén 2002). The duration of all three studies was four weeks. The Boralevi 2014 study enrolled 251 children aged from two to six years and allowed topical corticosteroids only if they were really needed; we assessed it as being at low risk of bias. The Breternitz 2008 study was a within‐participant study (24 participants), conducted in people aged between 15 and 49 years, in which no concomitant treatments were permitted; we assessed it as being at an unclear risk of bias. Lodén 2002 was a three‐armed study of 197 adults (see also Comparisons 2b and 3o) that did not permit additional use of topical corticosteroids; we assessed it as being at an unclear risk of bias.
See Table 4.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Only Lodén 2002 evaluated participant‐assessed disease severity and rated the improvement in dryness of the skin. In the group treated with glycerol 20% cream, 58/68 participants considered their skin to have improved in terms of dryness versus 46/66 in the placebo cream group, with a RR of 1.22 (95% CI 1.01 to 1.48; P = 0.03; NNTB = 6, 95% CI 3 to 60), showing greater improvement in the glycerol group.
In the Boralevi 2014 study, the participants scored itch on a 10 cm VAS (with higher values being worse): in the 124 children treated with glycerol 15% cream, the mean change from baseline in itch was ‐1.72 cm (SD 2.01), while in the 125 children treated with placebo cream, the mean change was ‐1.11 cm (SD 1.93), which were both small changes but slightly favoured the glycerol group (MD ‐0.61 cm, 95% CI ‐1.10 to ‐0.12; P = 0.01).
Participant satisfaction
This outcome was not assessed in any of the studies.
Adverse events
Two studies reported data on adverse events (Boralevi 2014; Lodén 2002). There was no statistically significant difference in the number of adverse events between the two treatment groups (RR 0.90, 95% CI 0.68 to 1.19; P = 0.45; I² = 0%; Analysis 4.1). The adverse events were mild to moderate and consisted of smarting, erythema, pruritus, or burning.
4.1. Analysis.

Comparison 4: Glycerin cream versus placebo cream, Outcome 1: Number of participants reporting an adverse event
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
In Boralevi 2014, the investigators assessed disease severity with the objective SCORAD (Kunz 1997). The mean change from baseline was ‐5.3 (SD 5.3) in the 124 participants treated with glycerol cream versus a change of ‐3.1 (SD 4.7) in the 125 participants treated with vehicle cream (MD ‐2.20, 95% ‐3.44 to ‐0.96; P = 0.0005), which is a statistically significant difference in favour of the glycerol‐containing cream, but this value does not meet the MID of 8.2 for the objective SCORAD (Schram 2012).
Breternitz 2008 had a within‐participant design with 24 participants. The mean change from baseline in SCORAD was ‐1.10 (SD 1.57) on the side treated with glycerol 20% cream, and 0.0 (SD 1.83) on the side treated with vehicle (mean of the paired differences: ‐1.10, CI 95% ‐1.63 to ‐0.57), which favoured the glycerol‐containing cream.
The investigators in Lodén 2002 evaluated skin dryness with the DASI (Serup 1995), and stated that there were "no differences between the groups in DASI scores". Despite this, in the glycerol group, 58/68 showed improvement in dryness of the skin versus 42/66 in the vehicle group (RR 1.34, 95% CI 1.09 to 1.65; P = 0.0006; NNTB = 5, 95% CI 3 to 14), which is in accordance with the participant assessments and favoured the glycerol cream.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed in any of the studies.
Change in use of topical active treatment
This outcome was not assessed in any of the studies.
Changes in skin barrier function
In Boralevi 2014, the hydration index was measured with corneometry and showed a mean change of 11.14 units (SD 10.21) in the glycerol group (120 participants) versus 5.56 units (SD 9.88) in the vehicle group (121 participants) (MD 5.58 units, 95% CI 3.04 to 8.12; P < 0.0001), showing glycerol was more effective at improving hydration.
In the within‐participant study (24 participants) of Breternitz 2008, the mean change in TEWL was ‐5.80 g/m²/h (SD 4.95) on the side treated with glycerol cream versus 7.20 g/m²/h (SD 11.01) on the side treated with vehicle, with a statistically significant mean of the paired differences of ‐13 g/m²/h (95% CI ‐16.33 to ‐9.67) in favour of glycerol cream. Furthermore, the mean change from baseline in hydration was 12.40 units (SD 6.2) on the glycerol cream side versus 5.30 units (SD 5.77) on the vehicle cream side (statistically significant mean of the paired differences: 7.10 units, 95% CI 5.24 to 8.96).
Change in health‐related quality of life
This outcome was not assessed in any of the studies.
2d Oat‐containing moisturisers versus vehicle or no treatment (i.e. no moisturiser)
Four studies (344 participants) reported data on oat‐containing moisturisers versus no treatment or vehicle (Giordano‐Labadie 2006; Grimalt 2007; Nebus 2009; Weber 2015). Three of these four studies are also reported under Comparison 1 (Giordano‐Labadie 2006; Grimalt 2007; Weber 2015). Only Nebus 2009 compared oat‐containing moisturiser versus occlusive vehicle, whilst the comparison in the other studies was no moisturiser. Study duration was six weeks for Grimalt 2007, eight weeks for Giordano‐Labadie 2006 and Nebus 2009, and six months for Weber 2015.
The Giordano‐Labadie 2006, Grimalt 2007, and Weber 2015 studies were conducted in children, and Nebus 2009 included both children (above 12 years of age) and adults. All participants had predominantly mild to moderate eczema.
We assessed Nebus 2009 as being at low risk of bias, but the other three studies were not blinded, and we therefore assessed them as being at a high risk of bias.
The Giordano‐Labadie 2006, Grimalt 2007, and Nebus 2009 studies allowed application of moderate to strong topical corticosteroids in both treatment arms, and Weber 2015 allowed application of 'Eucerin Eczema Relief Instant Therapy' to active lesions.
See Table 5.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was only assessed in Nebus 2009, in which 50 participants reported how effective the creams were in hydrating and alleviating eczema. There was no difference between the two treatment groups for two assessments: 21/25 participants in the oat‐containing cream group considered the moisturiser to be effective in hydrating skin versus 19/25 in the occlusive vehicle group (RR 1.11, 95% CI 0.84 to 1.46; P = 0.45), while 18/25 in the oat‐containing cream group felt eczema was alleviated versus 16/25 in the occlusive vehicle group (RR 1.13, 95% CI 0.77 to 1.65; P = 0.55).
Itch was assessed on a 5‐point Likert scale (0 to 4, with a higher score being worse) in Nebus 2009. The mean change from baseline was ‐0.78 (SD 0.76) in the oat‐containing cream group (25 participants) versus ‐1.20 (SD 1.01) in the occlusive vehicle group (25 participants) (MD 0.42, 95% CI ‐0.08 to 0.92; P = 0.10).
Participant satisfaction
This outcome was only assessed in Nebus 2009, where there was equal satisfaction in the two groups with the treatments; 18/25 participants in the oat‐containing cream group indicated that the cream was soothing and calmed the discomfort versus 17/25 in the occlusive vehicle group (RR 1.06, 95% CI 0.74 to 1.52; P = 0.76).
Adverse events
At six weeks in the Grimalt 2007 trial, 8/91 participants reported adverse events in the oat‐containing cream group compared to 0/82 in the no moisturiser control group (Peto OR 7.26, 95% CI 1.76 to 29.92; P = 0.006). The P value of Fisher's Exact Test was 0.0071. Three adverse events were reported to be mild, three moderate, and two severe, which led to treatment discontinuation. No further details were provided other than "all the adverse events spontaneously resolved without sequel." None of the other studies addressed this outcome.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The investigators in three studies evaluated disease severity (Giordano‐Labadie 2006; Grimalt 2007; Nebus 2009). Two of the studies, Giordano‐Labadie 2006 and Grimalt 2007, used the SCORAD to measure disease severity, and Nebus 2009 used the EASI. The SMD in change from baseline in disease severity was ‐0.23 (95% CI ‐0.66 to 0.21; P = 0.30; I² = 65%; Analysis 5.1). However, when we conducted further analyses based on individual domains of risk of bias in addition to a stratified analysis adjusting for effect size ‐ which eliminated the heterogeneity ‐ Giordano‐Labadie 2006 showed a greater effect than the other two studies, but did not alter the conclusion (Table 15).
5.1. Analysis.

Comparison 5: Oat‐containing cream versus vehicle or no treatment, Outcome 1: Change in disease severity as assessed by the investigators (SCORAD and EASI)
Prevention of flares (lengthening the time to first flare)
Only Weber 2015 evaluated flaring: 4/20 participants in the oat‐containing cream group experienced a flare versus 15/23 in the no moisturiser control group (RR 0.31, 95% CI 0.12 to 0.77; P = 0.01; NNTB = 2, 95% CI 1 to 5), favouring the use of oat‐containing cream. The median time to flare was more than 180 days for the group treated with oat‐containing cream versus 28 days for the no moisturiser group. The HR for rate to flare was 4.74 (95% CI 1.57 to 14.34; P = 0.006; Analysis 1.3) in favour of the oat‐containing cream.
Change in use of topical active treatment
Two of the four studies provided data for this outcome, Giordano‐Labadie 2006 and Grimalt 2007. These have been discussed under Comparison 1, and only the conclusion is repeated here. Pooled data that demonstrated a statistically significant reduction in use of topical corticosteroids in the moisturiser groups, where a smaller amount was required to achieve a similar reduction in eczema severity, are presented in Analysis 1.4. Total topical corticosteroid usage was much higher in both treatment groups in Giordano‐Labadie 2006, which explains the substantial heterogeneity.
Changes in skin barrier function
This outcome was not assessed in any study.
Change in health‐related quality of life
Three studies assessed change from baseline in quality of life (Giordano‐Labadie 2006; Grimalt 2007; Nebus 2009) (details of Giordano‐Labadie 2006 and Grimalt 2007 appear in Comparison 1 and Analysis 1.5). Giordano‐Labadie 2006 used the CDLQI; Grimalt 2007, the IDQOL; and Nebus 2009 used the Dermatology Quality of Life Index (DLQI) (Finlay 1994). The SMD for changes from baseline in quality of life was ‐0.09 (95% CI ‐0.37 to 0.19; P = 0.53; I² = 12%; Analysis 5.2).
5.2. Analysis.

Comparison 5: Oat‐containing cream versus vehicle or no treatment, Outcome 2: Change from baseline in quality of life
2e Remainder of moisturisers versus vehicle, placebo or no treatment (i.e. no moisturiser)
2e‐I Ammonium lactate‐containing moisturiser (6%) versus vehicle
One study compared twice daily application of ammonium lactate (6%) in water in oil emulsion with vehicle that was also applied twice daily (Larregue 1996). This within‐participant trial had 46 participants (six to 12 years old), who had had moderate eczema for four weeks. We assessed the study as being at a high risk of bias. Very limited data were provided, and no additional treatment was allowed.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Although this was a prespecified outcome and should have been measured with a questionnaire filled in by the parents, the data were not reported. (See the 'Risk of bias' assessment in Characteristics of included studies).
Participant satisfaction
The trial did not assess this outcome.
Adverse events
The trial did not assess this outcome.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
Larregue 1996 assessed desquamation and xerosis, lichenification, and hyperkeratosis on a 4‐point Likert scale (0 = normal, to 3 = severe), and summed the results for all participants into a total score. At the start of the study, the total score for desquamation and xerosis in 44/46 participants on the side treated with ammonium lactate was 74, which decreased to 34 over a period of four weeks. On the vehicle side of the body, the score was 76 at baseline and 35 at the end of the study, showing a minimal difference between the two treatments on either side of the body. Data for lichenification showed a decrease of 21 on the side treated with ammonium lactate and a decrease of 19 on the vehicle side. Hyperkeratosis decreased by 23 on the side treated with ammonium lactate and by 18 on the vehicle side. The authors reported that both treatments were effective in reducing erythema and papules.
Prevention of flares (lengthening the time to first flare)
The trial did not assess this outcome.
Change in use of topical active treatment
The trial did not assess this outcome.
Changes in skin barrier function
The trial did not assess this outcome.
Change in health‐related quality of life
The trial did not assess this outcome.
2e‐II Pale sulfonated 4% shale oil cream versus vehicle
One study compared application of pale sulfonated 4% shale oil (PSSO) with application of vehicle, both applied three times daily (Korting 2010). The trial included 99 children who had had mild to moderate eczema for four weeks. We assessed the study as being at a high risk of bias. No other treatments for eczema were allowed during the study period.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
The trial did not assess this outcome.
Participant satisfaction
The trial did not assess this outcome.
Adverse events
Two out of the 51 participants treated with PSSO reported adverse events (both reported itch and erythema) versus 4/48 treated with vehicle (Peto OR 0.46, 95% CI 0.09 to 2.40; P = 0.36). The P value of Fisher's Exact Test was 0.4270. The adverse events in the vehicle group included one case each of a bacterial super‐infection; erythema and itch; erythema, itch and spreading of eczema; and worsening of eczema.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
This outcome was assessed with EASI (score rating from 0 to 72, with a higher score being worse) (Hanifin 2001). In the PSSO group (50 participants), the mean change from baseline in EASI was ‐8.90 (SD 4.96) compared to ‐1.30 (SD 6.40) in the vehicle group (47 participants) (MD ‐7.60, 95% CI ‐9.89 to ‐5.31; P < 0.00001). The MID of the EASI is 6.6 (Schram 2012), and therefore the reduction in the PSSO group was a clinically important reduction, as was the difference between the two groups.
Prevention of flares (lengthening the time to first flare)
The trial did not assess this outcome.
Change in use of topical active treatment
The trial did not assess this outcome.
Changes in skin barrier function
The trial did not assess this outcome.
Change in health‐related quality of life
The trial did not assess this outcome.
2e‐III Atoderm Intensive cream versus moisturiser base
One study compared twice daily application of Atoderm Intensive cream with moisturiser base, also applied twice daily, over six months (Gayraud 2015). The trial enrolled 130 children with mild to moderate eczema. We assessed the study as being at a low risk of bias. Participants were permitted to continue using their prescribed medication for eczema, as long as the usage remained stable.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Participants assessed disease severity with the patient‐oriented SCORAD (Stalder 2011). The mean change from baseline was ‐5.70 (SD 5.59) in the 62 participants treated with Atoderm Intensive cream versus ‐2.70 (SD 5.66) in the 61 treated with the moisturiser base, with a MD of ‐3.00 (95% CI ‐4.99 to ‐1.01; P = 0.003) in favour of Atoderm Intensive cream.
Participant satisfaction
The trial did not assess this outcome.
Adverse events
Five out of the 65 participants randomised to Atoderm Intensive cream reported adverse events (warm sensation, pruritus, stinging, pain, erythema, flare‐up) versus 7/65 in the moisturiser base group (pruritus, mild warm sensation, mild flare‐ups, mild or moderate erythema and papules) (RR 0.71, 95% CI 0.24 to 2.13; P = 0.55).
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
Investigators used the SCORAD (score 0 to 103, with higher scores being worse) to assess disease severity. The mean change from baseline was ‐3.70 (SD 3.79) in the 62 participants treated with Atoderm Intensive cream versus 0 (SD 5.60) in the 61 treated with the moisturiser base, with a MD of ‐3.70 (95% CI ‐5.39 to ‐2.01; P < 0.0001). Although this difference clearly favoured Atoderm Intensive cream, it did not meet the estimated MID of 8.7 (Schram 2012).
Prevention of flares (lengthening the time to first flare)
In the Atoderm Intensive cream group, 18/62 of the participants experienced a flare versus 22/61 in the control group (RR 0.80, 95% CI 0.48 to 1.34; P = 0.41). The time to flare was 59 days (SD 11) in the Atoderm Intensive cream group compared to 39 days (SD 12) in the moisturiser base group (MD 20.00 days, 95% CI 15.93 to 24.07; P < 0.00001), and favoured Atoderm Intensive cream. In addition, the investigators reported that "overall, severity of flares had decreased by 49% in SBT [Atoderm Intensive cream] complex group compared to 15% in the emollient base group."
Change in use of topical active treatment
Change in use of topical active treatment was evaluated through reporting the mean number of treatment days during flares. The usage of topical corticosteroids was 4.3 days (SD 1.10) in the Atoderm Intensive cream group (62 participants) versus 4.8 days (SD 1.0) in the moisturiser base group (61 participants) (MD ‐0.50 day, 95% CI ‐0.87 to ‐0.13; P = 0.008). The difference in usage of topical immunomodulators was 1.6 days (SD 0.6) versus 3.8 days (SD 1.0) (MD ‐2.20 days, 95% CI ‐2.49 to ‐1.91; P < 0.00001), respectively. The usage of oral antihistamines was 0.5 days (SD 0.3) versus 3.5 days (SD 1.6), respectively (MD ‐3.00, 95% CI ‐3.41 to ‐2.59; P < 0.00001), which favoured the Atoderm Intensive cream.
Changes in skin barrier function
The trial did not assess this outcome.
Change in health‐related quality of life
For children under four years of age, quality of life was assessed with the IDQOL (0 = no quality of life impairment, 30 = highest quality of life impairment), and for children over four years of age, it was assessed with the CDLQI (score 0 to 30: 0 to 1 = no effect on quality of life, 19 to 30 = extremely large effect on quality of life). In addition, the DFI questionnaire was used to assess quality of life in all of the participants and their parents (0 = no quality of life impairment, 30 = highest quality of life impairment).
In children under four years of age, the mean change in IDQOL was ‐4.90 (SD 4.69) in the 47 children on Atoderm Intensive cream versus ‐1.00 (SD 2.90) in the 36 children treated with the moisturiser base (MD ‐3.90, 95% CI ‐5.54 to ‐2.26; P < 0.00001). For children over four years of age, the mean change from baseline in CDLQI was ‐0.70 (SD 1.64) in the 15 children treated with Atoderm Intensive cream versus ‐0.50 (SD 2.12) in the 25 treated with moisturiser base (MD ‐0.20, 95% CI ‐1.56 to 1.16; P = 0.77).
All children were included in the assessments of the DFI, where the mean change from baseline was ‐4.40 (SD 2.49) in the 62 children treated with Atoderm Intensive cream versus ‐2.2 (SD 2.88) in the 61 treated with moisturiser base (MD ‐2.20, 95% CI ‐3.78 to ‐0.62; P = 0.006). While this was a statistically significant difference in favour of Atoderm Intensive cream, and although the MID of the DFI has not yet been established, this difference is unlikely to be clinically important.
2e‐IV Triclosan 1% moisturiser twice daily versus vehicle cream twice daily
Triclosan 1% moisturiser was evaluated in a single study we assessed as being at low risk of bias, which included 60 children and adults with mild to moderate eczema (Tan 2010). The study duration was 41 days, and usage of low‐potency topical corticosteroids was allowed in both treatment arms.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
The trial did not assess this outcome.
Participant satisfaction
The trial did not assess this outcome.
Adverse events
Three of the 30 participants who used triclosan 1% moisturiser experienced transient stinging pain after application compared to 1/30 of those who used the vehicle cream (Peto OR 2.87, 95% CI 0.38 to 21.44; P = 0.30). The P value of Fisher's Exact Test was 0.6120.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The investigators measured disease severity with SCORAD. The mean change from baseline was ‐12.67 (SD 7.7) in the triclosan 1% moisturiser group and ‐11.69 (SD 7.7) in the vehicle cream group (MD ‐0.98, 95% CI ‐4.88 to 2.92; P = 0.62). Both reductions met the MID of 8.7 (Schram 2012), but with no important difference between the two groups.
Prevention of flares (lengthening the time to first flare)
The trial did not assess this outcome.
Change in use of topical active treatment
The mean amount of topical corticosteroids used for the duration of the study varied substantially between groups, with 22 g used in the triclosan 1% moisturiser group and 44.2 g used in the vehicle cream group; the vehicle cream group required twice the amount of corticosteroids to achieve a reduction in SCORAD similar to that seen in the triclosan 1% moisturiser group.
Changes in skin barrier function
The trial did not assess this outcome.
Change in health‐related quality of life
The trial did not assess this outcome.
2e‐V Hippophae rhamnoides 10% cream versus placebo cream
Thumm 2000 was a three‐armed study with a total of 43 adult participants with mild to moderate eczema (see Comparisons 2e‐VI and 3t). The study compared sea buckthorn oil (Hippophae rhamnoides) 10% cream, with H rhamnoides 20% cream, and with placebo. H rhamnoides cream also contains beeswax, paraffin, and glycerol and was applied for four weeks. We assessed the study as being at an unclear risk of bias.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Disease severity was not assessed by the participants, although itch was assessed on a VAS. No precise data were reported, other than that there were improvements in the severity of itch in both groups, with the H rhamnoides 10% group showing greater improvement than the placebo group.
Participant satisfaction
The trial did not assess this outcome.
Adverse events
The trial did not assess this outcome.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The investigators assessed disease severity with the SCORAD. No standard deviations were reported, but in the H rhamnoides 10% cream group (17 participants) the SCORAD decreased by 9.52 and by 13.76 in the placebo cream group (19 participants). Both scores indicate clinically relevant reductions (MID for the SCORAD is 8.7 (Schram 2012)), with the placebo group apparently doing better.
Prevention of flares (lengthening the time to first flare)
The trial did not assess this outcome.
Change in use of topical active treatment
The trial did not assess this outcome.
Changes in skin barrier function
TEWL showed a decrease of 10.20 g/m²/h in the H rhamnoides 10% cream group and a decrease of 11.37 g/m²/h in the placebo cream group. No standard deviations were provided. Skin hydration improved in both arms by 8 and 10.15 units, respectively. Hence, there were only small differences between the groups for both TEWL and skin hydration.
Change in health‐related quality of life
The Thumm 2000 study used the DLQI to measure changes in quality of life (score 0 to 30, with a higher score indicating a greater impairment of quality of life). The mean change from baseline was ‐2.74 for the H rhamnoides 10% cream group and ‐3.79 in the placebo cream group. Previously, the MID of DLQI varied between three and five, but an MID of four is the currently recommended value for inflammatory skin diseases (Basra 2015).
2e‐VI Hippophae rhamnoides 20% cream versus placebo cream
This is the second comparison in Thumm 2000 (see Comparisons 2e‐V and 3t).
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Disease severity was not assessed by the participants, but itch was assessed on a VAS. No precise data were reported, other than that there were improvements in the severity of itch in both groups, with the H rhamnoides 20% group showing greater improvement than the placebo group.
Participant satisfaction
The trial did not assess this outcome.
Adverse events
The trial did not assess this outcome.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The investigators assessed disease severity with the SCORAD. No standard deviations were provided, but in the H rhamnoides 20% cream group (17 participants) the SCORAD decreased by 10.98 and by 13.76 in the placebo cream group (19 participants). Both are both clinically important reductions (MID for the SCORAD is 8.7 (Schram 2012)). The size of reduction that was reported in the placebo group was quite remarkable.
Prevention of flares (lengthening the time to first flare)
The trial did not assess this outcome.
Change in use of topical active treatment
The trial did not assess this outcome.
Changes in skin barrier function
TEWL showed a decrease of 10.59 g/m²/h in the H rhamnoides 20% cream group and a decrease of 11.37 g/m²/h in the placebo cream group. No standard deviations were provided. Skin hydration improved in both arms by 14.84 and 10.15 units, respectively. Hence, there were only small differences between the groups for both TEWL and skin hydration.
Change in health‐related quality of life
The mean change from baseline in DLQI was ‐3.67 for the H rhamnoides 20% cream group and ‐3.79 for the placebo cream group. Until recently the MID of DLQI varied between three and five, but an MID of four is the currently recommended value for inflammatory skin diseases (Basra 2015).
2f All moisturisers (2a‐2e) versus vehicle, placebo, or no treatment (i.e. no moisturiser)
All of the studies listed under Comparisons 2a up to 2e‐VIII provided data for this overall comparison for at least one of the outcomes.
See Table 6.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was addressed in five studies for which the data could be pooled (Abramovits 2008; Belloni 2005; Boguniewicz 2008; Lodén 2002; Nebus 2009); Lodén 2002 provided data on two different treatment arms versus placebo, and therefore we pooled the data from the two active treatment arms and have partitioned them in the analyses (to avoid double counting). The number of participants who considered that their eczema had improved was 252/323 in the moisturiser group versus 92/249 in the control group, which favoured the use of moisturiser (RR 2.46, 95% CI 1.16 to 5.23; P = 0.02; I² = 95%; NNTB = 2, 95% CI 1 to 3; Analysis 6.1). From a clinical point of view, the result of the Nebus 2009 study appeared to be an outlier, but removing this study had little effect on the effect estimate. Removing the study with the smallest sample size did not alter the results (Belloni 2005).
6.1. Analysis.

Comparison 6: All moisturisers versus vehicle, placebo or no treatment (no moisturiser), Outcome 1: Number of participants who experienced improvement
Seven studies assessed itch (Abramovits 2008; Belloni 2005; Boguniewicz 2008; Boralevi 2014; Nebus 2009; Patrizi 2008; Patrizi 2014). Six of these used a VAS scale, and Patrizi 2014 used a 4‐point Likert scale. The SMD was ‐1.10 (95% CI ‐1.83 to ‐0.38; P < 0.00001; I² = 94%; Analysis 6.2), and favoured moisturiser. Again, the Nebus 2009 study, which had a smaller sample size, appeared to be an outlier, but the removal of this study did not have an important effect on the overall effect estimate. The stratified sensitivity analyses by domain of risk of bias (Table 15) and effect size (analyses not shown) did not minimise the degree of heterogeneity. Stratified analyses that compared study results from the single prospectively registered trial, Boralevi 2014, with those without a published prespecified protocol (remainder of trials included for this outcome) did not alter the degree of heterogeneity (analysis not shown).
6.2. Analysis.

Comparison 6: All moisturisers versus vehicle, placebo or no treatment (no moisturiser), Outcome 2: Change from baseline in itch
Participant satisfaction
Only three studies reported data on participant satisfaction with the treatment (Abramovits 2008; Belloni 2005; Nebus 2009). In the moisturiser group, 146/185 expressed satisfaction to a certain extent with the treatment and also indicated their willingness to use it again, versus 54/113 in the control group (RR 1.35, 95% CI 0.77 to 2.36; P = 0.29; I² = 83%; Analysis 6.3). The stratified analyses based on individual domains demonstrated that Abramovits 2008, which was assessed as being at high risk of bias (due to high risk of attrition bias) and also showed the greatest effect estimate, was responsible for all of the heterogeneity (see Table 15).
6.3. Analysis.

Comparison 6: All moisturisers versus vehicle, placebo or no treatment (no moisturiser), Outcome 3: Number of participants who expressed treatment satisfaction
The Bohnsack 1997 study (within‐participant design) included 38 participants and assessed smell, spreadability, penetration into the skin, and skin feeling. The results are summarised under Comparison 2b, but there was no difference between the two treatments for any of these features, which confirms the results from the other three studies that we pooled (Analysis 6.3).
Adverse events
Ten studies reported on the number of participants who experienced an adverse event (Abramovits 2008; Belloni 2005; Boguniewicz 2008; Boralevi 2014; Gayraud 2015; Grimalt 2007; Korting 2010; Lodén 2002; Patrizi 2008; Tan 2010). We took the number of participants who reported an adverse event in the two active treatment arms of Lodén 2002 together and partitioned them (numerator and denominator) to avoid double‐counting. In total, 170/680 participants treated with a moisturiser reported an adverse event compared to 139/595 in the control arms with a RR of 1.03 (95% CI 0.82 to 1.30; P = 0.80; I² = 21%; Analysis 6.4), which was not a statistically significant difference. As Belloni 2005 did not report adverse events in either treatment arm, we repeated our analysis when one adverse event was added in both groups, which resulted in a RR of 1.03 (95% CI 0.83 to 1.27), showing no difference between groups. Our repeat analysis no longer showed heterogeneity when we pooled data from studies at low risk of bias only (Table 15).
6.4. Analysis.

Comparison 6: All moisturisers versus vehicle, placebo or no treatment (no moisturiser), Outcome 4: Number of participants reporting an adverse event
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
Twelve studies provided usable data for this outcome (Abramovits 2008; Belloni 2005; Boguniewicz 2008; Boralevi 2014; Gayraud 2015; Giordano‐Labadie 2006; Grimalt 2007; Korting 2010; Nebus 2009; Patrizi 2008; Patrizi 2014; Tan 2010), measured with different instruments, and showed a SMD of ‐0.65 (95% CI ‐0.89 to ‐0.41; P < 0.00001; I² = 75%; Analysis 6.5), which is a significant difference in favour of the moisturiser group. Further exploration of the heterogeneity to detect publication bias and small‐study effects revealed no evidence of funnel plot asymmetry (Figure 4). In addition, our stratified sensitivity analyses by domain of risk of bias did not reduce the heterogeneity to a minimum (Table 15). Only the Boralevi 2014 study had a prospectively registered protocol.
6.5. Analysis.

Comparison 6: All moisturisers versus vehicle, placebo or no treatment (no moisturiser), Outcome 5: Change in disease severity as assessed by the investigators
4.

Funnel plot of comparison 5: All moisturisers versus vehicle, placebo or no treatment (no moisturiser), outcome: 5.5 Change in disease severity as assessed by the investigators
The investigators in the within‐participant Bohnsack 1997 study reported a combined total score for all 38 participants, which, over four weeks, showed a reduction in total score of 28 on the urea cream‐treated side versus a reduction of 18 on the vehicle‐treated side. (For further details, see Comparison 2b). The within‐participant Wilhelm 1998 study used a sum score that included erythema, dryness, induration, and papules (each item scored from 0 to 4, with higher scores being worse) in the assessment of this outcome. The mean change from baseline in the sum score after four weeks was ‐1.90 (SD 3.5) on the side treated with urea cream and ‐1.33 (SD 2.11) on the side treated with vehicle, with a mean of the paired differences of ‐0.57 (95% CI ‐1.14 to 0.0).
Prevention of flares (lengthening the time to first flare)
Six studies examined occurrence of flares (Abramovits 2008; Boguniewicz 2008; Gayraud 2015; Patrizi 2008; Weber 2015; Wirén 2009). The number of participants who experienced a flare in the moisturiser group was 44/341 versus 108/266 in the control group (RR 0.33, 95% CI 0.17 to 0.62; P = 0.0006; I² = 73%; NNTB = 4, 95% CI 3 to 5; Analysis 6.6); this result favoured use of moisturiser. The Gayraud 2015 study was the only one that did not show a difference between the treatment arms. Removing this study from the meta‐analysis altered the result only slightly. In this trial, the moisturiser base in the placebo arm appeared to be quite effective as well, possibly because it included glycerol, which might explain this effect.
6.6. Analysis.

Comparison 6: All moisturisers versus vehicle, placebo or no treatment (no moisturiser), Outcome 6: Number of participants experiencing a flare
The only two studies that addressed time to flare were Weber 2015 and Wirén 2009; both studies lasted six months, and the results have already been discussed under Comparison 1. There was a statistically significant difference in favour of the moisturiser groups for risk of flare (HR 3.74, 95% CI 1.86 to 7.50; P = 0.0002; I²= 0%; Analysis 1.3).
Change in use of topical active treatment
The assessments for this outcome have been presented in Comparison 1 and include two studies that evaluated the amount of topical steroid used (Giordano‐Labadie 2006; Grimalt 2007, see Analysis 1.4). See Comparison 2e‐III too (Gayraud 2015), which evaluated the number of treatment days and not the amount of topical active treatment used.
Changes in skin barrier function
Seven of the studies did not provide data that could be pooled for this outcome. Boralevi 2014 reported on the skin hydration index; Patrizi 2014 on TEWL; Breternitz 2008 and Simpson 2013 (within‐participants studies) both reported TEWL. SDs were not reported in Thumm 2000 for TEWL and skin capacitance. Both Bohnsack 1997 and Wilhelm 1998 evaluated skin capacitance (Analysis 3.1). All of the results on skin barrier function have been presented in the comparisons listed above (1, 2b, 2c, 2e‐V, and 2e‐VI).
Change in health‐related quality of life
Three studies provided usable data for this outcome (Gayraud 2015; Giordano‐Labadie 2006; Grimalt 2007). Gayraud 2015 used three separate measuring instruments. We chose to use the DFI, as that was the only instrument that covered the whole population, whilst the other two instruments assessed children on the basis of their age. Giordano‐Labadie 2006 used the CDLQI, and Grimalt 2007 used the IDQOL. (See Comparisons 1 and 2e‐III.) In the three studies, the SMD for the change from baseline in quality of life was ‐0.39 (95% CI ‐0.90 to 0.12; P = 0.13; I² = 79%; Analysis 6.7). We assessed Gayraud 2015 as being at a low risk of bias, and it demonstrated the largest effect size; we assessed the other two studies as being at a high risk of bias. Furthermore, as already stated under Comparison 1, in Grimalt 2007, 40% of the participants did not complete the questionnaires, and we assessed this domain as being at high risk of attrition bias, which might further explain some of the heterogeneity (Table 15).
6.7. Analysis.

Comparison 6: All moisturisers versus vehicle, placebo or no treatment (no moisturiser), Outcome 7: Change from baseline in quality of life
2g Oil versus placebo
Three studies compared oil versus placebo and provided limited data: Gehring 1999, which reported two studies, and Hamada 2008. We assessed all of the studies as being at an unclear risk of bias. The two Gehring 1999 studies assessed evening primrose oil in different vehicles on adults, and the Hamada 2008 study assessed camellia oil versus water in both children and adults. The Gehring 1999 studies had a within‐participant design, with a treatment period of four weeks during which no other treatments were allowed. The Hamada 2008 study had a two‐week duration, a parallel design, and allowed all concomitant treatments.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed by any study.
Participant satisfaction
This outcome was not assessed by any study.
Adverse events
Only the Hamada 2008 study addressed this outcome; no adverse events were reported in the 30 participants who used camellia oil spray or in the nine who applied water spray.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
This outcome was not assessed in the Gehring 1999 studies, but was assessed in Hamada 2008 by means of a 5‐point Likert scale. The investigators considered that the camellia oil spray treatment was effective, or very effective, in 8/30 participants, and that water spray was effective, or very effective, in 2/9 of the participants (RR 1.20, 95% CI 0.31 to 4.67; P = 0.79).
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed by any study.
Change in use of topical active treatment
This outcome was not assessed by any study.
Changes in skin barrier function
The two Gehring 1999 within‐participant studies (data on 20 and 19 participants) evaluated TEWL and skin hydration. For TEWL, the MD was ‐0.34 g/m²/h (95% CI ‐1.44 to 0.76; P = 0.94; I² = 0%; Analysis 7.1), showing no difference in results between the two treatments. The measurements with corneometry showed a similar result with an MD of 0.34 (95% CI ‐2.54 to 3.21; P = 0.82; I² = 0%; Analysis 7.2).
7.1. Analysis.

Comparison 7: Evening primrose oil versus placebo oil, Outcome 1: Change from baseline in TEWL
7.2. Analysis.

Comparison 7: Evening primrose oil versus placebo oil, Outcome 2: Change from baseline in skin hydration
Change in health‐related quality of life
This outcome was not assessed by any study.
(3) One moisturiser versus another moisturiser
3a Atopiclair three times daily versus Atopiclair 'light' three times daily (both containing glycyrrhetinic acid)
Patrizi 2008, a three‐armed study with 60 children, at unclear risk of bias, evaluated this comparison over 29 days (see Comparison 2a too). Atopiclair light contains the same key ingredients as Atopiclair, but at a lower concentration and with no preservatives. The study included children between the ages of two and 17 years with mild to moderate eczema. Additional low‐potency topical corticosteroids were allowed in both treatment arms as part of a rescue regimen when really needed.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Disease severity was not assessed by the participants, but itch (pruritus) was assessed on a VAS (0 cm to 10 cm, with higher values being worse). The VAS showed a reduction of 2.6 cm (SD 0.9) in the Atopiclair group (19 participants) versus a reduction of 0.23 cm (SD 0.9) in the Atopiclair light group (19 participants), with a mean difference of ‐2.37 cm (95% CI ‐2.94 to ‐1.80; P < 0.00001) in favour of the Atopiclair group.
Participant satisfaction
Participants' or caregivers' 'appraisal of acceptability of study substance' and wish to continue was a prespecified outcome. The principal investigators reported that there was a statistically significant difference in favour of Atopiclair, citing a P value of less than 0.0001, but provided no further details, and the contact person for the study was unable to provide us with further information (see Table 11).
Adverse events
In both groups, 2/20 participants reported an adverse event that was mild or moderate in severity (Peto OR 1.00, 95% CI 0.13 to 7.69; P = 1.00). The P value of Fisher's Exact Test was 1.000.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The review authors estimated data for this outcome from a figure that showed a change in EASI (score from 0 to 72, with higher scores being worse). The Atopiclair group (19 participants) showed a reduction of ‐4.3 (SD 3.3) and the Atopiclair light group (19 participants) showed a reduction of ‐0.8 (SD 5.53), with a MD of ‐3.50 (95% CI ‐6.40 to ‐0.60; P = 0.02).
Prevention of flares (lengthening the time to first flare)
This was reported as the need for rescue medication in the event of a flare. One of the 20 participants in the Atopiclair group experienced a flare and needed rescue medication compared to 9/18 in the Atopiclair light group (RR 0.10, 95% CI 0.01 to 0.71; P = 0.02; NNTB = 2, 95% CI 1 to 5), which was statistically significant in favour of Atopiclair.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was not assessed.
3b Atopiclair (containing glycyrrhetinic acid) three times daily versus EpiCeram (containing ceramides, cholesterol and free fatty acids) three times daily
Miller 2011 conducted a three‐arm study (39 participants in total), which we assessed as being at a low risk of bias, to evaluate Atopiclair, EpiCeram and Aquaphor Healing Ointment (Aquaphor Healing Ointment is considered in Comparisons 3c and 3d). The study duration was 43 days; no other eczema treatment was allowed during the study. The study was conducted in children with mild to moderate eczema.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Participants did not assess disease severity, but itch was scored on a VAS from 0 mm to 100 mm (0 = no itch and 100 = the most intense itch imaginable). The mean change from baseline in itch was ‐5.73 mm (SD 15.54) in the 13 participants treated with Atopiclair and ‐20.35 mm (SD 36.21) for the 13 participants in the EpiCeram group, with a MD of 14.62 mm (95% CI ‐6.80 to 36.04; P = 0.18).
Participant satisfaction
This outcome was not assessed.
Adverse events
This was not a predefined outcome in this study, but the investigators reported that there were no serious adverse events in any group.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The mean change from baseline as measured with the EASI (score from 0 to 72, higher being worse) was ‐1.36 (SD 2.22) in the Atopiclair group and ‐0.95 (SD 1.91) in the EpiCeram group, which were both minimal reductions (MD ‐0.41, 95% CI ‐2.00 to 1.18; P = 0.61). The MID for the EASI is estimated at 6.6 (Schram 2012), and therefore the reductions reported are not considered clinically relevant.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was not assessed.
3c Atopiclair (containing glycyrrhetinic acid) three times daily versus Aquaphor (containing petrolatum, cera microcristallina, panthenol, glycerol, bisabolol) three times daily
This comparison includes the Aquaphor Healing Ointment arm of the Miller 2011 study, the EpiCeram arm is not considered here, but is included in Comparisons 3b and 3d.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Disease severity was not assessed, but itch was assessed on a VAS from 0 mm to 100 mm. The mean change from baseline for itch was ‐5.73 mm (SD 15.54) in the 13 participants on Atopiclair compared to ‐24.86 mm (SD 13.74) in the 13 participants treated with Aquaphor (MD 19.13 mm, 95% CI 7.85 to 30.41; P = 0.0009), which is statistically significant in favour of Aquaphor.
Participant satisfaction
This outcome was not assessed.
Adverse events
This was not a predefined outcome in this study, but the investigators reported that there were no serious adverse events in any of the intervention groups.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
Investigators assessed disease severity with the EASI. The mean change from baseline was ‐1.36 (SD 2.22) in the Atopiclair group and ‐2.90 (SD 2.23) in the Aquaphor group (MD 1.54, 95% CI ‐0.17, 3.25; P = 0.08). These were both small improvements.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was not assessed.
3d EpiCeram (containing ceramides, cholesterol and free fatty acids) three time daily versus Aquaphor (containing petrolatum, cera microcristallina, panthenol, glycerol, bisabolol) three time daily
This is the third comparison in the Miller 2011 study (see Comparisons 3b and 3c too).
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Disease severity was not assessed in this study, but reduction of itch was assessed on a VAS from 0 mm to 100 mm. The mean change from baseline for itch was ‐20.35 mm (SD 36.21) in the 13 participants treated with EpiCeram compared to a change of ‐24.86 mm (SD 13.74) in the 13 participants of the Aquaphor group (MD 4.51 mm, 95% CI ‐16.54 to 25.56; P = 0.67).
Participant satisfaction
This outcome was not assessed.
Adverse events
This was not a predefined outcome in this study, but the investigators reported that there were no serious adverse events in any of the intervention groups.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The investigators assessed disease severity with the EASI; the reductions in EASI were small in both arms and not clinically meaningful. The MID for the EASI is estimated at 6.6 (Schram 2012). The change from baseline in EASI score in the EpiCeram group (13 participants) was ‐0.95 (SD 1.91) and ‐2.90 (SD 2.23) in the Aquaphor group (13 participants), with a MD of 1.95 (95% CI 0.35 to 3.55; P = 0.02), which, although not a clinically important difference, does favour Aquaphor.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was not assessed.
3e EpiCeram (containing ceramides, cholesterol and free fatty acids) twice daily versus Hyalotopic (hyaluronic acid‐based emollient foam) twice daily
Only one within‐participant study (20 participants) that we judged to be at a high risk of bias compared these two interventions over four weeks (Draelos 2011). Participants had to have at least moderate eczema. No additional treatment for eczema was allowed during the study period.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Although this was a prespecified outcome, measured on a 6‐point Likert scale, these data were not reported, and we failed in our attempts to receive clarification (see Table 11 and 'Risk of bias' assessment under Characteristics of included studies). In this study, data were available for 18 participants; 6/18 felt that EpiCeram worked better while the remaining 12/18 felt Hyalotopic worked better.
Participant satisfaction
The participants expressed a preference for Hyalotopic foam over EpiCeram; 10/18 wished to continue with Hyalotopic foam, compared to 8/18 who wished to continue with EpiCeram. Thirteen thought that Hyalotopic foam had less odour, were willing to spend more money on it, found that it rubbed in more easily, and that it was more moisturising. In addition, 14 considered that Hyalotopic foam spread more easily and was easier to use than EpiCeram.
Adverse events
No adverse events occurred on either side of the participants' bodies.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
Disease severity was assessed on a 6‐point Likert scale (0 = none, 5 = severe). No standard deviations were reported, but we estimated from a figure that on the EpiCeram side, the score went from 2.95 (3 = moderate) to 1.55 (minimal‐mild), and on the Hyalotopic foam side from 2.95 to 1.1, which are reductions of 47.5% and 62.7%, respectively.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was not assessed.
3f EpiCeram (containing ceramides, cholesterol and free fatty acids) twice daily versus colloidal oatmeal cream twice daily
One study, which we assessed as being at unclear risk of bias, was reported as a poster presentation and therefore provided limited data for this comparison (Nuñez 2013). The study was conducted over three weeks and included 49 participants. Following email contact, the principal investigator provided us with most of the missing study details (see Table 11). The study was conducted in African American children with mild to moderate eczema. No additional treatment for eczema was allowed during the study period.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed in this study, but itch was assessed on a VAS (0 cm to 10 cm, with higher scores indicating more itch). The mean change in baseline for itch was ‐0.20 cm (SD 2.03) in the 24 participants treated with EpiCeram versus 0.5 cm (SD 2.3) in the 25 participants who used the colloidal oatmeal cream, with a MD of ‐0.70 cm (95% CI ‐1.91 to 0.51; P = 0.26).
Participant satisfaction
This outcome was not assessed.
Adverse events
This outcome was not assessed.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The change in EASI (score 0 to 72, with higher scores being worse) over three weeks was ‐2.20 (SD 3.81) in the EpiCeram group (24 participants) versus ‐2.40 (SD 1.17) in the colloidal oatmeal cream group (25 participants), which are both small reductions; the MD was 0.20 (95% CI ‐1.39 to 1.79; P = 0.81).
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was not assessed.
3g EpiCeram (containing ceramides, cholesterol and free fatty acids) versus Eucerin lotion (petrolatum‐based)
One small within‐participant pilot study evaluated these two products in 10 participants over a period of four weeks (Kircik 2014). The study was assessed as being at unclear risk of bias and mainly provided very limited data on barrier function. The application frequency of the interventions was unclear in the report. Both children and adults with mild to moderate eczema were included. No other treatment for eczema was allowed during the study period.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed.
Participant satisfaction
This outcome was not assessed.
Adverse events
This outcome was not assessed.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
This outcome was not assessed.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
Barrier function assessment was based on measurement of TEWL and corneometry. We estimated the reduction from a figure, as the principal investigator was unable to provide more precise data (see Table 11). TEWL decreased by 2.2 g/m²/h on the EpiCeram side and by 1.4 g/m²/h on the Eucerin side, both of which are very small improvements.
Hydration improved by 55% on the EpiCeram side and by 37% on the Eucerin side; no further details were reported.
Change in health‐related quality of life
This outcome was not assessed.
3h MimyX cream (barrier cream containing lipids and palmitoylethanolamide (palmitamide MEA)) plus Eucerin twice daily versus Eucerin only twice daily
The data for this comparison were reported in a conference abstract (Laumann 2006). This was a within‐participant study that evaluated 74 participants over 12 weeks, that we assessed as being at a high risk of bias. The outcomes reported were predominantly assessments of participants' experience with Mimyx. The study included both children and adults with eczema in remission, but with a history of frequent flares.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was assessed by a questionnaire and data were available for 71 of the 74 participants. Overall, 37 participants (50%) considered Mimyx to be better than anything they had used before, 23 (31%) considered it similar to other products, and 11 (15%) considered it was not as good as other products.
Participant satisfaction
Satisfaction was also assessed with a questionnaire, with data available for 71/74 participants. Overall, 57 (77%) participants indicated that they were willing to continue treatment with Mimyx, while 14 (19%) did not want to continue. Mimyx was reported as 'very nice to use and pleasant' by 66 (89%) participants, while 5 (7%) considered it was 'not pleasant and too sticky'.
Adverse events
One participant at the end of the study reported mild stinging and burning with Mimyx cream.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
Although this was a prespecified outcome, this was not reported (see the 'Risk of bias' assessment under Characteristics of included studies ).
Prevention of flares (lengthening the time to first flare)
The median number of days before flare was 43 days (95% CI 37 to 78) on the Mimyx plus Eucerin side versus 29 days (95% CI 15 to 43) on the Eucerin only side, which was 48% longer for Mimyx plus Eucerin. On the Mimyx plus Eucerin side of the body, 59.5% had a flare versus 74.3% on the Eucerin only side of the body.
Change in use of topical active treatment
Rescue medication was used in 41/74 participants on the Mimyx plus Eucerin side of the body, and in 50/74 on the Eucerin only side.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was not assessed.
3i Albolene over‐the‐counter (OTC) moisturiser twice daily versus Mimyx (barrier cream containing lipids and palmitamide MEA) twice daily
A single within‐participant study of four weeks duration with 60 adult participants reported data on this comparison (Draelos 2009). We assessed this study as being at a high risk of bias. Participants with mild eczema used the moisturisers only, while participants with moderate eczema used 0.1% triamcinolone cream as well on both sides.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Although the study lasted four weeks, no end‐of‐study data were reported, and our attempts to receive clarification from the principal investigator were unsuccessful (see Table 11). Therefore, we only report data at two weeks. Disease severity was assessed on a 6‐point Likert scale (0 = none, 5 = severe). Both treatment sides started at 2.8 and reduced to 1 at two weeks, as estimated from a figure in the report.
Participant satisfaction
This outcome was not assessed.
Adverse events
There were no adverse events at either side.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
Disease severity was assessed by the investigators on the same Likert scale used by the participants. On both sides, disease severity went from 2.6 to 0.6 after two weeks. As with the participant data, there were no four‐week data reported, but similar to the participant‐assessed data, the investigator reported that at all time points, there were no differences between the two moisturisers.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was not assessed.
3j Aquacare (containing 10% urea, multisterols, phospholipids and fatty diols) twice daily versus Calmurid (containing 10% urea, betaine, and a high concentration of lactic acid) twice daily
These treatments were assessed in two within‐participant studies each with 30 participants (Fredriksson 1975 reports on two studies). We assessed both of these studies as being at an unclear risk of bias. Study duration was four weeks, and no other treatments were allowed.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed.
Participant satisfaction
Based on preference ratings, 27/60 participants in this within‐participant study preferred Aquacare, 7/60 preferred Calmurid (RR 3.50, 95% CI 1.30 to 9.41; P = 0.01; NNTB = 3, 95% CI 2 to 8), and 26/60 expressed no preference.
Adverse events
The 60 participants reported no adverse events on the Aquacare‐treated side, but reported 13 adverse events on the contralateral Calmurid‐treated side (RR 0.08, 95% CI 0.00 to 1.31; P = 0.08).
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The assessments of the investigators were in agreement with the assessments of the participants. Aquacare was considered to be the more effective treatment in 28/60 participants and Calmurid was considered more effective in 7/60 participants (RR 3.50, 95% CI 1.30 to 9.41; P = 0.01; NNTB = 3, 95% CI 2 to 8); both treatments were considered equally effective in 25 participants.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was not assessed.
3k Locobase repair (containing ceramide III, cholesterol and free fatty acids) twice daily versus Atoderma (containing glycerol, ceramides, cholesterol, vitamin E) twice daily
These moisturisers were evaluated in a single study with a duration of one year, and we assessed the study as being at a high risk of bias (Namazova‐Baranova 2012). All participants in both groups received 0.1% hydrocortisone 17‐butyrate cream one to three times a day and oral antihistamines as needed. The study was conducted in 44 children between six months and 12 years of age with eczema of moderate severity.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed.
Participant satisfaction
This outcome was not assessed.
Adverse events
None of the 44 participants reported an adverse event.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The investigators measured disease severity with SCORAD (score 0 to 103, higher score being worse). The change in SCORAD was ‐29.9 (SD 8.1) in the 22 participants on Locobase repair versus ‐27.1 (SD 7.9) in the 22 participants treated with Atoderm, both of which are substantial and clinically important reductions, but with a MD of ‐2.80 (95% CI ‐7.53 to 1.93; P = 0.25), so there was no clear difference between the groups.
Prevention of flares (lengthening the time to first flare)
The only information reported stated: "Clinically, a decrease in the recurrence of the disease and the severity of the current 1‐year follow‐up was observed."
Change in use of topical active treatment
Over the one‐year study period, the mean daily consumption of topical corticosteroid decreased by 1.6 g per day in the Locobase repair group (22 participants) and 1.7 g per day in the Atoderm group (22 participants) to achieve similar reduction in eczema severity.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
The CDLQI was used to assess changes in quality of life (score 0 to 30: 0 to 1 = no effect on quality of life, 19 to 30 = extremely large effect on quality of life). The investigators reported the degree of reduction in scores as percentages without providing the exact data. The CDLQI score reduced by ‐12.7% in the Locobase repair group (22 participants) and by ‐11.55% in the Atoderm group (22 participants), which indicates that the quality of life in both groups improved over the treatment period.
3l Canoderm (containing urea 5%) twice daily versus Miniderm (reference cream without urea) twice daily
These moisturisers were evaluated by a single study with 172 adult participants; we judged this study to be at a low risk of bias (Åkerström 2015). The study consisted of two phases. In the stabilisation phase, all participants were treated with once‐daily topical mometasone furoate cream 0.1% (Elocon) on the trunk and extremities, and hydrocortisone cream 1% on the face, groin, and armpits. In addition, in this phase of the study the participants used a medicinal moisturiser containing 20% glycerol (Miniderm). After (almost) clearing the eczema, participants entered the maintenance phase for 180 days, one group using Canoderm (containing 5% urea) and the other using Miniderm reference cream (without 20% glycerol). No topical corticosteroids were allowed.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed.
Participant satisfaction
This outcome was not assessed.
Adverse events
In the Canoderm group, 48/87 participants reported an adverse event compared to 44/85 in the Miniderm group (RR 1.07, 95% CI 0.81 to 1.41; P = 0.65). These adverse events included erythema, pruritus, and burning and were mainly considered to be mild to moderate in severity and unrelated to treatment.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
At the start of the maintenance phase (after being treated with topical corticosteroids), the SCORAD had reduced substantially to around six in both groups. At the end of the 180 days for those participants who remained 'eczema free', the mean change in SCORAD was ‐3.38 (SD 4.24) in the Canoderm group (21 participants) versus 0.44 (SD 4.07) in the Miniderm group (8 participants) (MD ‐3.82, 95% CI ‐7.17 to ‐0.47; P = 0.03), which, although it is a statistically significant difference, is not clinically relevant, as the MID for the SCORAD is estimated to be 8.7 (Schram 2012).
For those who relapsed, the mean SCORAD increased to 27.45 (SD 10.32) in the Canoderm group (66 participants) and to 30.46 (SD 12.67) in the Miniderm group (77 participants) (MD ‐3.01, 95% CI ‐6.78 to 0.76; P = 0.12).
Prevention of flares (lengthening the time to first flare)
At the end of the 180‐day maintenance phase, 21/87 of the participants in the Canoderm group had not experienced a flare, compared to 8/85 in the Miniderm group (RR 2.56, 95% CI 1.20 to 5.47; P = 0.01; NNTB = 7, 95% CI 3 to 26). The median time to flare was 22 days in the Canoderm group compared to 15 days in the Miniderm group. At day 180, 66/87 (75.8%) in the Canoderm group had a flare versus 77/85 (90.1%) in the Miniderm group, which corresponds to an absolute risk reduction of flare of 14.0% and a relative risk reduction of 15.6% with the use of Canoderm.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was measured using the EQ‐5D health questionnaire covering five dimensions (mobility, self‐care, usual activities, pain/discomfort, anxiety/depression) and a VAS that was rated 0 to 100 (100 equated to "best health you can imagine") (The EuroQol Group 1990). At the start of the maintenance phase in the Canoderm group, the score was 90 (after a period of treatment with topical corticosteroids) and 90 at the end of the study, and for those with a flare, the score reduced to 82.5. In the Miniderm group, it started at 89 and was 95 at the end of the study, but for those who experienced a flare, it dropped to 74.0.
On the EQ‐5D 5‐item instrument, the mean score was 0.945 (SD 0.137) at the beginning of the maintenance phase and 0.951 (SD 0.093) at end of study in the Canoderm group, but this score dropped to 0.881 (SD 0.154) in those with a flare. In the Miniderm group, the score at the start of the maintenance phase was 0.931 (SD 0.135), and at the end of the study and during flare, it was 0.935 (SD 0.136) and 0.851 (SD 0.152), respectively. These scores indicate that the quality of life remained relatively stable during the eczema‐free periods, but decreased during flares.
3m Urea 5% moisturiser twice daily versus urea 10% lotion twice daily
These two moisturisers were compared in one six‐week study with 100 adult participants; we assessed this study as being at an unclear risk of bias (Bissonnette 2010). The use of a stable dose of topical corticosteroids was permitted throughout the study period in both groups.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed.
Participant satisfaction
Cosmetic acceptability was assessed with a questionnaire consisting of 21 items (each scored from 0 = totally agree to 3 = totally disagree), with a lower total score indicating better acceptability. At the end of the study, 43/50 participants treated with urea 5% moisturiser had a mean score of 20.52 (SD 11.93) versus 29.75 (SD 13.03) in the 44/50 participants treated with urea 10% lotion (MD ‐9.23, 95% CI ‐14.32 to ‐‐4.14; P = 0.0004); this result favours the urea 5% moisturiser.
Adverse events
In the urea 5% group, 12/50 participants reported adverse events versus 10/50 in the urea 10% group, with a RR of 1.20 (95% CI 0.57 to 2.52; P = 0.63). The adverse events were reported to be of mild intensity.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
Investigators assessed disease severity with SCORAD (score from 0 to 103, higher score being worse). The mean change from baseline was ‐4.52 (SD 4.63) in the urea 5% group (43 participants) versus ‐4.39 (SD 5.48) in the urea 10% group (44 participants) (MD ‐0.13, 95% CI ‐2.26 to 2.00; P = 0.90).
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was not assessed.
3n Urea 4% and sodium chloride 40 mg/g in oil‐in‐water emulsion twice daily versus urea 4% in oil‐in‐water emulsion twice daily
These moisturisers were compared by one within‐participant study with a small sample size (22 participants), which we assessed as being at an unclear risk of bias (Hagströmer 2001). The study duration was two weeks, and no topical steroids were allowed. The study was conducted in adult participants with eczema, and only forearms were treated. There were minimal changes in barrier function after treatment between the two treatments.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed.
Participant satisfaction
This outcome was not assessed.
Adverse events
This outcome was not assessed.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
This outcome was not assessed.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
We had to estimate data from a figure; the change from baseline in TEWL was ‐0.60 g/m²/h (SD 1.90) on the urea 4% plus sodium chloride side versus 2.50 g/m²/h (SD 2.5) on the urea 4% only side, with a mean of the paired differences of ‐3.10 g/m²/h (95% CI ‐3.84 to ‐2.36), which is a statistically significant difference in favour of urea 4% plus sodium chloride.
Skin barrier function was also assessed with a corneometer (0 to 120, with higher measurements indicating greater hydration); the mean change from baseline was 8 arbitrary units (SD 3) on the urea 4% plus sodium chloride side versus 14 arbitrary units (SD 3.16) on the urea 4% only side, with a mean of the paired differences of ‐6.0 arbitrary units (95% CI ‐7.00 to ‐5.00), which was a statistically significant difference in favour of urea 4% only.
Change in health‐related quality of life
This outcome was not assessed.
3o Glycerol cream 20% once daily versus urea 4% cream once daily
These moisturisers constituted the third comparison in the three‐armed study conducted by Lodén 2002 (see Comparisons 2b and 2c). The study lasted 30 days and was assessed as being at an unclear risk of bias. The participants in all treatment arms were allowed to continue their use of topical corticosteroids.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
In the glycerol cream group, 58/68 participants considered the dryness of their skin to be improved versus 56/63 in the urea group with no difference between groups (RR 0.96, 95% CI 0.84 to 1.09; P = 0.54).
Participant satisfaction
This outcome was not assessed.
Adverse events
Smarting was mentioned by 27/68 in the glycerol cream group and by 41/63 in the urea cream group (RR 0.61, 95% CI 0.43 to 0.86; P = 0.005; NNTH = 4, 95% CI 2 to 11) in favour of the glycerol cream. However, the investigators stated that there "were no differences between treatment with the cream containing glycerol and urea regarding stinging, itching and experience of dryness/irritation".
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The investigators assessed dryness of skin with the DASI (score from 0 to 20, higher being worse) (Serup 1995). No exact data were provided, but the investigators stated "no differences were observed in disease severity as DASI scores between the glycerol and urea group (P = 0.787)."
The DASI score improved for 27/68 in the glycerol cream group and for 56/63 in the urea cream group, which does not agree with the assessments of the participants (RR 0.45, 95% CI 0.33 to 0.61; P < 0.00001; NNTB = 2, 95% CI 1 to 3).
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was not assessed.
3p Propyless (containing propylene glycol 20%) twice daily versus Fenuril (containing urea 4% and sodium chloride 4%) twice daily
These moisturisers were compared in a two‐week within‐participant study with 56 participants, which we assessed as being at a high risk of bias (Faergemann 2009). No other treatment was allowed. The study was conducted in adult participants with eczema and with symmetrical areas of dry skin on their lower legs.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
No exact data were provided in the report, and the investigators merely stated that "Propyless lotion resulted in statistically significantly less itching (P = 0.046) and irritation (P = 0.014). No statistical significance was observed for smarting (P = 1.0) or stinging (P = 0.75). The change in total score was statistically significantly better for Propyless lotion than for Fenuril cream (P = 0.049)."
Participant satisfaction
This outcome was not assessed.
Adverse events
Two adverse events were reported on the side treated with Propyless lotion; these were itching in one participant and eczema in another participant.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
No precise data were reported. Investigators reported improvements for both treated sides and that "there were no statistically significant differences between the two treatments with respect to the DASI [score from 0 to 20, higher being worse] evaluations" and "In total, 69% of the investigators and patients rated the overall treatment effect of Propyless as better (40%) or equal (29%) to that of Fenuril."
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This was assessed in only 20/56 participants and as with the previously reported assessments, no precise data were provided. The investigators only reported that "no (Fenuril) or almost no (decrease of 0.1 g/m2/h for Propyless) effect on TEWL was observed after treatment."
Change in health‐related quality of life
This outcome was not assessed.
3q Ceramide‐containing moisturiser twice daily versus 'control moisturiser' twice daily
This comparison was evaluated in Noh 2011, a six‐week trial in 40 children with mild to moderate eczema. We assessed the study as being at a high risk of bias. Topical corticosteroids were applied twice daily to all participants.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed.
Participant satisfaction
This outcome was not assessed.
Adverse events
This outcome was not assessed.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The investigators measured disease severity with EASI (score from 0 to 72, higher being worse). The mean change from baseline in EASI score was ‐6.65 (SD 2.79) in the ceramide‐containing moisturiser group (15 participants) and ‐7.31 (SD 2.64) in the control moisturiser group (17 participants), which are both clinically relevant reductions as the MID for the EASI is estimated at 6.6 (Schram 2012). However, the MD between groups was 0.66 (95% CI ‐1.23 to 2.55; P = 0.49), which was not a statistically significant difference.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
The amount of topical corticosteroids used (to achieve a similar reduction in eczema severity) over a six‐week period had to be estimated from a figure and was approximately 10 g in the ceramide‐containing moisturiser group and according to the figure in the report was 7.46% higher in the control moisturiser group.
Changes in skin barrier function
The mean change from baseline in TEWL was ‐14 g/m²/h (SD 12.24) in the 15 participants who were treated with the ceramide‐containing moisturiser versus ‐12 g/m²/h (SD 9.94) in the 17 participants in the control moisturiser group (MD ‐2.00 g/m2/h, 95% CI ‐9.79 to 5.79; P = 0.61).
Assessment with a corneometer showed that the hydration of the skin had improved by 17 arbitrary units (SD 13.98) in the ceramide‐containing moisturiser group (15 participants) versus 10 arbitrary units (SD 13.03) in the control moisturiser group (17 participants) (MD 7.00 arbitrary units, 95% CI ‐2.40 to 16.40; P = 0.14).
Change in health‐related quality of life
This outcome was not assessed.
3r Furfuryl palmitate enriched moisturiser twice daily versus moisturiser twice daily
These treatment options were investigated by a single study in 117 children with eczema; we assessed the study as being at a high risk of bias (Tripodi 2009). The study duration was two weeks, during which time no other treatment was allowed.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was assessed through a questionnaire completed by parents and paediatricians, and, although no exact data were reported, the investigators stated that "both paediatricians and parents rated the moisturiser cream without furfuryl palmitate to be more efficacious than the cream with furfuryl palmitate (P = 0.016)."
Participant satisfaction
This outcome was not assessed.
Adverse events
This outcome was not assessed.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
Disease severity was evaluated with SCORAD. In the furfuryl palmitate enriched moisturiser group (39 participants), the mean change from baseline in SCORAD was ‐7.10 (SD 8.42), and in the in the control group (49 participants) ‐11.60 (SD 6.13), with a MD of 4.50 (95% CI 1.35 to 7.65; P = 0.005). The MID for the SCORAD is estimated to be 8.7 (Schram 2012); therefore, the decrease in SCORAD in the control group was a clinically relevant reduction.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was not assessed.
3s PRO‐AMP cream (containing rhamsosoft, ceramides, L‐isoleucine) twice daily versus 'hydrating' cream (containing glycerol, vaseline, paraffin) twice daily
This comparison was assessed in a study we judged as being at a high risk of bias (Marseglia 2014). The moisturisers were applied to the faces (only) of 107 children with mild to moderate eczema for a period of six weeks, and no other treatments were allowed.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed.
Participant satisfaction
This outcome was not assessed.
Adverse events
This outcome was not assessed.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The EASI facial score was used to assess eczema severity; the mean change from baseline was ‐5.10 (SD 1.58) in the PRO‐AMP cream group (72 participants) and ‐2.70 (SD 1.84) in the control group (35 participants) (MD ‐2.40, 95% CI ‐3.11 to ‐1.69; P < 0.00001). Sixty‐three of the 72 participants in the PRO‐AMP cream group achieved treatment success (i.e. Investigator Global assessment (IGA) score < 1: where 0 = clear, 1 = almost clear, 2 = mild disease, 3 = moderate disease, 4 = severe) versus 20/35 in the control arm (RR 1.53, 95% CI 1.13 to 2.07; P = 0.005; NNTB = 3, 95% CI 2 to 8), this result favours the PRO‐AMP cream.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was not assessed.
3t Hippophae rhamnoides 10% cream versus Hippophae rhamnoides 20% cream
This is the third comparison of the Thumm 2000 three‐armed study with 43 participants (see Comparisons 2e‐V and 2e‐VI too). Sea buckthorn oil (Hippophae rhamnoides) 10% and 20% cream containing beeswax, paraffin, and glycerol was applied for four weeks. We assessed this study as being at an unclear risk of bias.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Disease severity was not assessed by the participants; however, itch was assessed on a VAS. No precise data were reported other than that itch severity improved in both groups, but without a statistically significant difference between the groups.
Participant satisfaction
This outcome was not assessed.
Adverse events
This outcome was not assessed.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The investigators assessed disease severity with the SCORAD. No standard deviations were provided, but the SCORAD in the H rhamnoides 10% cream group (17 participants) decreased by 9.52, and in the H rhamnoides 20% cream group (17 participants), it decreased by 10.98. Both results indicate clinically relevant reductions (MID for the SCORAD is estimated to be 8.7 (Schram 2012)), but with no important difference between the groups.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
TEWL showed a decrease of 10.20 g/m²/h in the H rhamnoides 10% cream group (n = 17) and of 10.59 g/m²/h in the H rhamnoides 20% cream group (n = 17). No standard deviations were provided. Skin hydration improved in both arms by 8 units and 14.84 units, respectively.
Change in health‐related quality of life
The DLQI was used for measuring changes in quality of life (score 0 to 30, with a higher score indicating greater impairment of quality of life). The mean change from baseline was ‐2.74 for the H rhamnoides 10% cream group (17 participants) and ‐3.67 for the H rhamnoides 20% cream group (17 participants). Previously, the MID of the DLQI varied between three and five, but a MID of four is the current recommended value for inflammatory skin diseases (Basra 2015), therefore, these changes from baseline were not clinically important, nor was the difference between groups.
3u Lactobacillus sakei‐containing moisturiser twice daily versus 'control moisturiser' twice daily
A within‐participant study in 30 children evaluated the effect of a moisturiser that contains a vegetable‐derived lactobacillus for the treatment of eczema (Park 2014). The study duration was four weeks. We assessed the study as being at an unclear risk of bias. Continued usage of topical corticosteroids on both sides was permitted.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Disease severity was not assessed, but itch was assessed on a VAS (0 cm to 10 cm, with higher scores indicating more itch) in 28 participants. On the side treated with Lsakei‐containing moisturiser, the mean change in itch was ‐2.03 cm (SD 1.12) versus ‐1.50 cm (SD 1.11) on the control side, with a mean of the paired differences of ‐0.53 cm (95% CI ‐0.84 to ‐0.22) in favour of the side treated with Lsakei‐containing moisturiser.
Participant satisfaction
This outcome was not assessed.
Adverse events
No precise data were provided, but three participants reported mild burning and stinging on the Lsakei‐containing moisturiser side, which resolved within three days.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The investigators reported no statistically significant difference between the treatment sides (28 participants). The mean change from baseline as measured on the IGA scale (0 = clear, 4 = severe) was ‐0.85 (SD 0.44) on the L sakei‐containing moisturiser side and ‐0.71 (SD 0.42) on the control side, with a mean of the paired differences of ‐0.14 (95% CI ‐0.26 to ‐0.02) in favour of Lsakei‐containing moisturiser.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
Skin barrier function was assessed through TEWL and corneometry in the 28 participants. The mean change from baseline in TEWL was ‐15.10 (SD 5.88) g/m²/h on the Lsakei‐containing moisturiser side and ‐5.30 (SD 5.31) g/m²/h on the control side, with a statistically significant mean of the paired differences of ‐9.80 g/m²/h (95% CI ‐11.43 to ‐8.17), which favours Lsakei‐containing moisturiser. Corneometry showed an increase of 17.60 (6.83) arbitrary units versus 9.10 (6.32) arbitrary units, respectively, with a mean of the paired differences of 8.50 (95% CI 6.60 to 10.40), which was also statistically significant in favour of the Lsakei‐containing moisturiser.
Change in health‐related quality of life
This outcome was not assessed.
3v Virgin coconut oil twice daily versus mineral oil twice daily
A single eight‐week study that we assessed as being at an unclear risk of bias compared these two oils in 117 children with mild to moderate eczema (Evangelista 2014). No other treatments were allowed.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed.
Participant satisfaction
This outcome was not assessed.
Adverse events
No adverse events were reported in the virgin coconut oil group (59 participants), but five of the 58 children in the mineral oil group reported adverse events (increase in erythema, pruritus) necessitating rescue therapy with topical corticosteroids (Peto OR 0.12, 95% CI 0.02 to 0.74; P = 0.02). The P value of Fisher's Exact Test was 0.0273.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
Disease severity was measured with the SCORAD (score from 0 to 103, with higher scores being worse). Data were reported as 'moderate improvement' (30% to 75%) or 'excellent improvement' (> 75%). In the virgin coconut oil group, 28/59 participants experienced moderate improvement versus 20/58 in the mineral oil group (RR 1.38, 95% CI 0.88 to 2.15; P = 0.16). Excellent improvement was seen in 27/59 in the virgin coconut oil group and 11/58 in the mineral oil group (RR 2.41, 95% CI 1.32 to 4.40; P = 0.004; NNTB = 4, 95% CI 2 to 9), which was statistically significant in favour of virgin coconut oil.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
The change from baseline in TEWL was ‐19.71 g/m²/h (SD 12.72) in the virgin coconut oil group and ‐10.57 g/m²/h (SD 12.72) in the mineral oil group, with a MD of ‐9.14 g/m²/h (95% CI ‐13.75 to ‐4.53; P = 0.0001). The skin capacitance increased by 10.30 (SD 4.17) versus 6.18 (SD 4.17), respectively (MD 4.12, 95% CI 2.61, 5.63; P < 0.00001). Both measurements were in favour of virgin coconut oil.
Change in health‐related quality of life
This outcome was not assessed.
3w Virgin coconut oil twice daily versus virgin olive oil twice daily
These two oils were evaluated in 52 adult participants with newly diagnosed mild to 'high moderate' eczema (Verallo‐Rowell 2008). We assessed the study as being at an unclear risk of bias. The study had a four‐week duration in which no other moisturisers or products were allowed.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed.
Participant satisfaction
This outcome was not assessed.
Adverse events
This outcome was not assessed.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The investigators assessed disease severity with the objective SCORAD (Kunz 1997). The mean change from baseline was ‐16.60 (SD 4.13) in the group treated with virgin coconut oil (26 participants) compared to ‐9.90 (SD 3.84) in the virgin olive oil group (26 participants), both of which are clinically important reductions (the MID objective SCORAD is 8.2 (Schram 2012)); the MD was ‐6.70 (95% CI ‐8.87 to ‐4.53; P < 0.00001) in favour of virgin coconut oil.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was not assessed.
3x Bleach bath with moisturiser versus water bath with moisturiser once daily
The intervention under investigation for this comparison was the 'bleach bath' and not the moisturiser (Shi 2015). Reducing Staphylococcus aureus has been shown to have an effect on the disease severity of eczema (Hon 2016). The Shi 2015 study had a within‐participant design with 20 participants, 10 of whom had eczema. The study was designed to evaluate skin barrier function following bleach bath and water bath, and we assessed it as being at a high risk of bias. Immersion of the volar surface of the forearm in the bleach bath or water bath for 10 minutes was followed by the application of a moisturiser containing glycerol and petrolatum.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed.
Participant satisfaction
This outcome was not assessed.
Adverse events
This outcome was not assessed.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
This outcome was not assessed.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
Both treatments (bleach bath and water bath) had very limited effect on TEWL values and corneometry.
Immediately after the bath, the TEWL increased for both arms from 12 g/m²/h to slightly over 30 g/m²/h; however, after 15 minutes, TEWL decreased again in both volar surfaces of the forearms and remained stable over 60 minutes. After 60 minutes, the changes from baseline (from before the bath) were ‐2.15 g/m²/h (SD 6.18) on the side treated with bleach bath and moisturiser versus ‐2.63 g/m²/h (SD 5.19) on the water bath side, with a mean of the paired differences of 0.48 g/m²/h (95% CI ‐2.30 to 3.26). Assessments with the corneometer showed substantial increases from around 24 arbitrary units for both forearms at baseline, to around 60 arbitrary units immediately after the bath. Within 15 minutes, these returned to baseline values and remained stable for 60 minutes. The mean changes from baseline from before the bath were ‐1.36 arbitrary units (SD 6.85) on the bleach bath side and ‐1.84 arbitrary units (SD 6.30) on the water bath side, with a mean of the paired differences of 0.48 arbitrary units (95% CI ‐2.70 to 3.66).
Change in health‐related quality of life
This outcome was not assessed.
(4) Moisturisers versus active treatment
4a Licochalcone (containing Glycyrrhiza inflata root extract, decanediol, menthoxypropanediol and ω‐6‐fatty acids) twice daily versus hydrocortisone acetate 1% cream twice daily
Three within‐participant studies (100 participants) evaluated the efficacy of these treatments (Angelova‐Fischer 2014; Udompataikul 2011; Wanakul 2013). We could only include data for the first week from Angelova‐Fischer 2014, because after one week, all participants received licochalcone‐containing cream. This study evaluated the interventions on forearms only and included both children and adults. The Udompataikul 2011 and Wanakul 2013 studies lasted six and four weeks, respectively, and were conducted only in children. We assessed both the Angelova‐Fischer 2014 and Udompataikul 2011 studies as being at a high risk of bias, and the Wanakul 2013 as being at a unclear risk of bias. Additional treatment for eczema was not permitted in any of these studies.
See Table 7.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Disease severity was not assessed by the participants in any of the three studies. However, itch was assessed in both Angelova‐Fischer 2014 and Wanakul 2013. At one week in the Angelova‐Fischer 2014 study (18 participants), itch severity assessed on a VAS (0 cm to 10 cm, with 10 being worst imaginable itch), reduced by 1.75 cm (SD 1.82) in the arm treated with licochalcone‐containing cream and by 2.75 cm (SD 1.36) in the arm treated with hydrocortisone acetate 1% cream. The mean of the paired differences was 1.00 cm (95% CI 0.39 to 1.61). The Wanakul 2013 study (52 participants) also assessed itch with a VAS (0 cm to 10 cm). After four weeks, itch had decreased from baseline by 4.00 cm (SD 2.25) on the licochalcone‐treated side of the body and by 4.00 cm (SD 2.22) on the hydrocortisone acetate‐treated side. Both appeared to be effective in reducing itch with no difference between treatment arms (mean of the paired differences: 0.0 cm, 95% CI ‐0.47 to 0.47). Pooled data demonstrated a MD of ‐0.48 (95% CI ‐1.46 to 0.50; P = 0.34; I² = 85%; Analysis 8.1).
8.1. Analysis.

Comparison 8: Licochalcone versus hydrocortisone acetate (HCA) 1%, Outcome 1: Change from baseline in itch (VAS)
Participant satisfaction
This outcome was only assessed in Udompataikul 2011, where it was scored on a 5‐point Likert scale. Twenty‐two of the 30 participants rated their satisfaction as good to excellent, with no difference between either side.
Adverse events
Both Udompataikul 2011 and Wanakul 2013 reported no adverse events on either side during the study, however, Angelova‐Fischer 2014 reported detailed side effects based on a standardised questionnaire. There were nine side effects on the 18 forearms treated with licochalcone (erythema (1), skin dryness (1), burning (2), skin tightness (1), and itch (4)) and nine on the contralateral arm (erythema (1), scaling (1), skin dryness (1), burning (3), skin tightness (1), and itch (2)).
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
All three studies measured disease severity with SCORAD (score from 0 to 103, higher score being worse). In Angelova‐Fischer 2014 the SCORAD decreased by 3.50 (SD 2.34) in one week on the side treated with licochalcone (18 sides) and by 3.50 (SD 1.85) on the hydrocortisone acetate‐treated side (18 sides), with a mean of the paired differences of 0.0 (95% CI ‐0.78 to 0.78).
In Udompataikul 2011 (26 participants), the mean change from baseline in SCORAD after four weeks was ‐18.72 (SD 6.96) on the licochalcone side and ‐21.29 (SD 6.14) on the hydrocortisone acetate side (mean of the paired differences of 2.57, 95% CI 0.59 to 4.55). In Wanakul 2013 (52 participants), the mean changes from baseline after four weeks were ‐14.00 (SD 6.85) on the licochalcone side and ‐12.00 (SD 7.09) on the hydrocortisone acetate side (mean of the paired differences of ‐2.00 (95% CI ‐3.47 to ‐0.53)). In both studies, the reductions in both treatment arms were clinically important, as the MID was met (MID SCORAD is 8.7 (Schram 2012)). Pooled data of the mean change from baseline in SCORAD resulted in a MD of 0.08 (95% CI ‐1.96 to 2.13; P = 0.94; I² = 85%; Analysis 8.2). We explored reasons for the heterogeneity (see Table 15), and considered that the most important factor was that the effect sizes differed between the studies. Furthermore, we could only include data for the first week of the Angelova‐Fischer 2014 study, as the first week was the only randomised one, and therefore smaller reductions were reported in both treatment arms compared to the other two studies, which had a four‐week duration with a correspondingly larger treatment effect. In addition, in Angelova‐Fischer 2014only the forearms/arms were treated.
8.2. Analysis.

Comparison 8: Licochalcone versus hydrocortisone acetate (HCA) 1%, Outcome 2: Change from baseline in SCORAD
Prevention of flares (lengthening the time to first flare)
This outcome was only assessed in the Udompataikul 2011 study (30 participants), where 3/30 experienced a flare on the side treated with licochalcone and 6/30 on the side treated with hydrocortisone acetate 1%.
Change in use of topical active treatment
This outcome was not assessed in any study.
Changes in skin barrier function
Two studies assessed this outcome (Angelova‐Fischer 2014; Wanakul 2013). In Angelova‐Fischer 2014 (18 participants), the mean change from baseline in TEWL after one week was ‐9.92 g/m²/h (SD 9.08) on the licochalcone‐treated forearms and ‐12.43 g/m²/h (SD 11.17) on those treated with hydrocortisone acetate 1% (the mean of the paired differences was 2.51 g/m²/h, 95% CI ‐1.21 to 6.23). In Wanakul 2013 (52 participants), the mean change from baseline in TEWL after four weeks was ‐4.0 g/m²/h (SD 7.44) on the licochalcone side and ‐1.00 g/m²/h (SD 8.59) on the hydrocortisone acetate 1% side (the mean of the paired differences was ‐3.00 g/m²/h, 95% CI ‐4.71 to ‐1.29). Pooled data of the mean change from baseline in TEWL demonstrated a MD of ‐0.50 g/m²/h (95% CI ‐5.88 to 4.87; P = 0.85; I² = 86%; Analysis 8.3). The reductions on both treatment sides were clearly smaller after four weeks than the reductions after only one week in Angelova‐Fischer 2014. Furthermore, the differences in effect between both sides of the body were small in both studies.
8.3. Analysis.

Comparison 8: Licochalcone versus hydrocortisone acetate (HCA) 1%, Outcome 3: Change from baseline in TEWL
Change in health‐related quality of life
This outcome was not assessed in any study.
4b‐I Stelatopia (2% sunflower oil, fatty acids, ceramides) twice daily versus hydrocortisone butyric propionate 0.1% twice daily
This comparison was evaluated over three weeks in the De Belilovsky 2011 study. We assessed this study as being at a high risk of bias. It was conducted on 80 children aged four months to four years, with mild to moderate eczema.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed.
Participant satisfaction
This outcome was not assessed.
Adverse events
No participants reported adverse events.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
After three weeks, the mean change from baseline in SCORAD was ‐27.48 (SD 7.63) in the 40 participants treated with Stelatopia versus ‐26.20 (SD 9.80) in the 40 treated with hydrocortisone butyric propionate 0.1% cream (MD ‐1.28, 95% CI ‐5.13 to 2.57; P = 0.51), which was not a statistically significant difference between the groups. However, the reductions in both treatment arms were substantial and clinically important, as the MID for SCORAD is estimated at 8.7 (Schram 2012).
Prevention of flares (lengthening the time to first flare)
The investigators 'agreed' or 'strongly agreed' (assessment based on a 5‐point Likert scale) that the frequency of flares was reduced in 37/40 participants treated with Stelatopia versus 32/40 treated with hydrocortisone butyric propionate 0.1% cream (RR 1.16, 95% CI 0.97 to 1.38; P = 0.11).
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was evaluated with two instruments for all 80 participants: the IDQOL (scores range from 0 (no quality of life impairment) to 30 (highest quality of life impairment)) showed mean changes from baseline of ‐8.48 (SD 3.54) in the Stelatopia group versus ‐6.50 (SD 3.61) in the hydrocortisone butyric propionate 0.1% cream group, with a MD of ‐1.98 (95% CI ‐3.55 to ‐0.41; P = 0.01) in favour of Stelatopia. The second instrument used was the DFI questionnaire; the data reported from this supported the results of the IDQOL. The mean change from baseline in DFI was ‐7.47 (SD 3.64) in the Stelatopia group compared to ‐4.85 (SD 3.16) in the hydrocortisone butyric propionate 0.1% cream group, with a MD of ‐2.62 (95% CI ‐4.11 to ‐1.13; P = 0.0006).
4b‐II EpiCeram twice daily versus fluticasone 0.05% cream twice daily
One four‐week study of 121 participants aged between six months and 18 years evaluated these treatments (Sugarman 2009). We assessed this study as being at a high risk of bias. All participants had moderate to severe eczema, and no other treatments were allowed.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Participants judged any improvement on a 3‐point Likert scale (no change, improved, worsening), and the mean change from baseline in 53/59 participants in the EpiCeram group was ‐0.90 (SD 0.61) compared to ‐0.87 (SD 0.65) in 59/62 treated with fluticasone 0.05% cream, with a MD of ‐0.03 (95% CI ‐0.26 to 0.20; P = 0.80).
Participants assessed itch on a VAS (0 cm to 10 cm) and reported that itch was reduced by 3.3 cm in the EpiCeram group (59 participants) and by 3.7 cm in the fluticasone 0.05% group (54 participants). No SDs were provided.
Participant satisfaction
This outcome was not assessed.
Adverse events
The participants did not report any serious adverse events in either group, but no further details regarding other possible treatment‐related adverse events were reported.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
Investigators used the SCORAD. The mean change from baseline in SCORAD was ‐18.7 (SD 7.8) in the 53 participants in the EpiCeram group versus ‐22.2 (SD 7.8) in the fluticasone 0.05% group (59 participants) (MD 3.50, 95% CI 0.61 to 6.39; P = 0.02). Both reductions were clinically important, as the MID for the SCORAD is estimated at 8.7 (Schram 2012), but the difference between the two treatments, although statistically significant, is not clinically important.
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was not assessed.
4b‐III 20% petrolatum in cetomacrogol combined with wet wrap versus diluted mometasone furoate 0.1% combined with wet wrap
Only one study compared wet wrap in combination with a petrolatum‐cetomacrogol moisturiser in one group and diluted mometasone furoate 0.1% ointment in the other (Janmohamed 2014). We assessed this study as being at an unclear risk of bias. The duration of the study was four weeks; it included 39 children aged between six months and 10 years with severe eczema (objective SCORAD 40 (± 5)) (Kunz 1997). The reporting of data in this trial was suboptimal, and our attempts to obtain clarification of missing and incomplete data were unsuccessful (see Table 11).
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Participants or parents applied the Patient‐Oriented Eczema Measure (POEM) (score: 0 to 28, higher score being worse) to assess this outcome. However, we had to estimate the data from a figure, and despite numerous attempts to contact the investigators, we did not obtain more precise data. Estimated reductions were 11 in the petrolatum‐cetomacrogol moisturiser group (16 participants) and 15.3 in the mometasone furoate 0.1% ointment group, which according to the investigators was not a statistically significant difference. Both reductions were clinically important as the MID for the POEM is estimated at 3.4 (Schram 2012).
Participant satisfaction
This outcome was not assessed.
Adverse events
In the petrolatum‐cetomacrogol moisturiser group, 7/20 children reported an adverse event (folliculitis (2), secondary infected eczema (2), the beginning of decubitus due to the mask (2), decubitus at mask (1)) versus 12/19 in the mometasone furoate 0.1% ointment group (folliculitis (9), severe folliculitis (1), decubitus at mask (2)) (RR 0.55, 95% CI 0.28 to 1.10; P = 0.09).
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
Investigators used the objective SCORAD, and as with the POEM, we had to estimate the data from a figure as no precise data were provided. Estimated reductions were 20 in the petrolatum‐cetomacrogol moisturiser group (16 participants) and 29.8 in the mometasone furoate 0.1% ointment group (20 participants), which are both substantial reductions (MID for objective SCORAD is 8.2 (Schram 2012)). The investigators reported "a difference of 9.927 (3.68 SE) and a P value of 0.0028".
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was assessed with the IDQOL, and again we had to estimate data from a figure. The IDQOL reduced by 4 in the 16 children on petrolatum‐cetomacrogol moisturiser versus a reduction of 12 in the 19 children on mometasone furoate 0.1% ointment. The authors reported that this difference was statistically significant ("P = 0.0002").
4b‐IV Water‐in‐oil emulsion Excipial twice daily versus hydrocortisone 1% in a water‐in‐oil emulsion
These treatments were examined in a single one‐week study with 69 adult participants (Gehring 1996). We assessed the study as being at an unclear risk of bias; no other treatments were allowed. Six participants dropped out overall, but it was unclear from which groups they came.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
'Roughness' of the skin was assessed with a VAS scale (1 cm to 10 cm, with higher being better). In the 31 participants in the Excipial moisturiser group, the mean change from baseline was 2.19 cm (SD 1.31) versus 2.60 cm (SD 0.98) in the 32 participants treated with hydrocortisone 1% (MD ‐0.41 cm, 95% CI ‐0.98 to 0.16; P = 0.16).
Participant satisfaction
This outcome was not assessed.
Adverse events
This outcome was not assessed.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The investigators assessed redness on a scale from one to four, with a lower score being better. The mean change from baseline in the 31 participants in the Excipial moisturiser group was ‐0.84 (SD 0.66) compared to ‐1.00 (SD 0.52) in the 32 participants in the hydrocortisone 1% group (MD 0.16, 95% CI ‐0.13 to 0.45; P = 0.29). Roughness was assessed with the same scale of one to four, and this demonstrated a change from baseline of ‐0.97 (SD 0.59) versus ‐1.06 (SD 0.46), respectively, with a MD of 0.09 (95% CI ‐0.18 to 0.36; P = 0.52).
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
The data reporting TEWL had to be estimated from a figure and showed a reduction of 8.2 g/m²/h in the Excipial moisturiser group (31 participants) versus 8 g/m²/h in the hydrocortisone group (32 participants), which are similar reductions.
Change in health‐related quality of life
This outcome was not assessed.
4b‐V Moisturiser containing spent grain, Vitellaria paradoxa (formerly Butyrospermum parkii) extract plus Argania spinosa kernel oil twice daily versus hydrocortisone acetate1% cream twice daily
The four‐week Jirabundansuk 2014 study examined these treatments in 31 children between two and 15 years of age, with mild to moderate eczema, using a within‐participant design. We assessed the study as being at a high risk of bias. No other treatments were allowed.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Twenty‐nine children or their parents reported change in disease severity on a 4‐point Likert scale (excellent, good, fair, unchanged). After four weeks, 89.7% rated the outcome on the side treated with the moisturiser as good to excellent compared to 93.1% on the side treated with hydrocortisone acetate 1% cream.
Participant satisfaction
This outcome was not assessed.
Adverse events
The investigators stated that "no specific adverse events were reported".
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The investigators measured disease severity in 29 participants with the SCORAD (score 0 to 103, higher score being worse). Both treatment sides showed clinically important reductions (MID SCORAD is estimated at 8.7 (Schram 2012)). On the side treated with the moisturiser, the mean change from baseline was ‐17.92 (SD 5) and on the side treated with hydrocortisone acetate 1% cream the change was ‐18.22 (SD 4.74), with a mean of the paired differences of 0.30 (95% CI ‐1.07 to 1.67), which was not a statistically significant difference between the two treatments.
Prevention of flares (lengthening the time to first flare)
After the four‐week treatment period, the moisturiser group continued for a further four weeks with the moisturiser, whilst the hydrocortisone acetate 1% group switched to the cream base for the following four weeks. No recurrences were seen in either group. However, the investigators also reported that "as for the relapse rates, it was 17.2% on the HC [hydrocortisone] cream side, and 10.3% on the S [moisturiser] cream side (P = 0.500)." It was not clear to us what the difference between recurrence and relapse might be.
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
This outcome was not assessed.
4b‐VI Advabase twice daily versus methylprednisolone aceponate cream two days a week plus moisturiser for remaining five days
The Peserico 2008 study commenced with an open‐label acute treatment phase of four weeks in which participants ‐ 12 years and older with moderate to severe eczema ‐ were treated with once‐daily methylprednisolone aceponate cream (MPA) and once‐daily moisturiser (Advabase). The second part of the study was a randomised phase that included 221 participants and had a duration of 16 weeks. In this phase, one treatment arm used only moisturiser (Advabase) and the other used MPA for two consecutive days a week and moisturiser for the remaining five days a week. We assessed the study as being at an unclear risk of bias.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
Disease severity was not assessed, but itch was assessed on a VAS (0 mm to 100 mm, higher being worse). The investigators were not able to provide us with SDs. The VAS scores increased during the second (maintenance) phase in the Advabase moisturiser group (109 participants) by 23.3 mm and in the MPA cream group (112 participants) by 5.5 mm. Authors reported "P < 0.001".
Participant satisfaction
This outcome was not assessed.
Adverse events
In the Advabase moisturiser group, 26/109 participants reported an adverse event compared to 17/112 in the MPA cream group (RR 1.57, 95% CI 0.91 to 2.73; P = 0.11). Investigators reported that "no AEs [adverse events] during the MP [maintenance phase] were considered [to be] related to the study drug".
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
The mean increase in EASI (score from 0 to 72, higher score is worse) during the maintenance phase was 2.97 in the Advabase moisturiser group versus 0.5 in the MPA cream group. The trial authors reported "P < 0.001". The MID for the EASI is 6.6 (Schram 2012), and therefore the difference between the two treatments was not clinically important.
Prevention of flares (lengthening the time to first flare)
During the 16‐week phase of maintenance therapy, 36/109 participants experienced a flare in the moisturiser group compared to 16/112 in the MPA cream group, a result that favours MPA cream (RR 2.31, 95% CI 1.37 to 3.91; P = 0.002; NNTH = 5, 95% CI 3 to 13). The rate of flare in the moisturiser group was 3.5 times the rate of flare in the MPA cream group (HR 3.5, 95% CI 1.91 to 6.43; P < 0.0001; Analysis 9.1). Twice‐weekly use of topical corticosteroid cream on consecutive days combined with use of moisturiser reduced the rate of flare compared to the use of moisturiser alone (see Comparison 5 too).
9.1. Analysis.

Comparison 9: Advabase versus MPA cream twice weekly and emollient, Outcome 1: Rate of flare
Change in use of topical active treatment
This outcome was not assessed.
Changes in skin barrier function
This outcome was not assessed.
Change in health‐related quality of life
No precise data were provided for this outcome, and the investigators were not able to provide missing trial details; however, they reported that, "The DLQI total score improved under MPA treatment by 0.6 points, mainly due to improvements in the categories 'leisure' (1.6 points) and 'personal relationships' (1.2 points) but worsened in all categories (by 4.4 to 13.8 points) in the moisturiser group. Similarly, the CDLQI had better results in the MPA group in all categories assessed (data not shown)."
4c Moisturisers versus topical immunomodulators
Three four‐week studies, that we assessed as being at a high risk of bias, evaluated different moisturisers against topical immunomodulators (Emer 2011; Frankel 2011; Takeuchi 2012). Both children and adults were included and all participants had mild to moderate eczema. Emer 2011 and Frankel 2011 used a within‐participant design. Emer 2011 included 20 participants and compared Eletone (high in lipids) three times a day on one side of the body with pimecrolimus cream three times a day on the other side of the body. Frankel 2011 included 30 participants and compared application of Hyalotopic (ceramide foam) to one side of the body with twice daily application of pimecrolimus cream to the other side. The Takeuchi 2012 study started with an induction phase in which the 70 participants received tacrolimus. They were moved to the maintenance phase only when the VAS score (0 mm to 100 mm, higher score is worse) reduced by more than 20 mm (43 participants). The application frequency of the moisturiser and the tacrolimus was not stated.
Trial details were missing and data were inadequately reported In all three studies; we made numerous attempts to contact the investigators to clarify missing study details, but were unsuccessful (see Table 11).
Primary outcomes
Change from baseline in disease severity as assessed by the participants
In Emer 2011 (within‐participant design), 20 participants compared moisturiser with pimecrolimus on a 4‐point Likert scale (0 to 3, higher scores being worse). The score reduced by 1.45 on the side treated with moisturiser, and by 1.42 on the side treated with pimecrolimus. Frankel 2011 (within‐participant design) provided no precise data; the investigators reported only that "subject self‐assessment scores decreased quadratically from week 0 to week 4 for both study treatment groups (P = 0.0001). However, there was no statistically significant difference between the pimecrolimus cream and ceramide‐hyaluronic acid emollient foam [moisturiser] group in subject self‐assessment scores (P = 0.7093)." Itch (measured on a VAS) was reduced by 54.6% versus 56.4%, respectively.
In Takeuchi 2012, itch was assessed by means of a VAS (0 mm to 100 mm). The mean change from baseline was ‐31.40 mm (SD 10.66) in the moisturiser group (21 participants) versus 1.50 mm (SD 12.61) in the tacrolimus group (23 participants) (MD 29.90 mm, 95% CI 23.02 to 36.78; P < 0.00001), which favours the moisturiser group.
Participant satisfaction
This outcome was assessed only in Frankel 2011. The investigators of this within‐participant study reported that 68% of the 28 participants preferred Hyalotopic, while 32% preferred pimecrolimus cream.
Adverse events
The Emer 2011 and Frankel 2011 studies did not report any adverse events on either side of the body. In Takeuchi 2012, adverse events were not assessed during the maintenance phase. In the induction phase, a transient burning sensation was reported in 32/69 participants after application of tacrolimus.
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
Takeuchi 2012 failed to report data on the SCORAD (see 'Risk of bias' table in Characteristics of included studies for this study). The Emer 2011 study assessed this outcome in 20 participants using a 6‐point Likert scale (0 to 5, higher values indicating worse). The mean score reduced by 2.11 on the side treated with moisturiser and by 2.16 on the side treated with pimecrolimus. Frankel 2011 reported that there was an improvement of 67.9% in the IGA (score 0 to 5, higher being worse) on the side treated with Hyalotopic and an improvement of 63.1% on the side treated with pimecrolimus (28 participants).
Prevention of flares (lengthening the time to first flare)
This outcome was not assessed in these studies.
Change in use of topical active treatment
This outcome was not assessed in these studies.
Changes in skin barrier function
This outcome was not assessed in these studies.
Change in health‐related quality of life
This outcome was not assessed in these studies.
5 Vehicle cream/ointment twice weekly combined with daily moisturiser versus fluticasone propionate cream (0.05%)/ointment (0.005%) twice weekly combined with daily moisturiser
Three studies with similar designs evaluated these treatments (Berth‐Jones 2003; Glazenburg 2009; Hanifin 2002). We assessed the three studies as being at an unclear risk of bias. All three started with a stabilisation phase of four weeks in which all participants were treated with fluticasone propionate (FP) 0.005% ointment (Berth‐Jones 2003 FP 0.05% cream in one treatment arm). They then entered a 16‐week (Berth‐Jones 2003; Glazenburg 2009), or 20‐week (Hanifin 2002), randomised maintenance phase. The participants had recurring moderate to severe eczema at entry to the studies. Berth‐Jones 2003 was a four‐arm study; we considered only two of its comparisons to be important for this review, i.e. 1) vehicle cream twice weekly combined with daily moisturiser versus FP cream combined with daily moisturiser, and 2) vehicle ointment twice weekly combined with daily moisturiser versus FP ointment combined with daily moisturiser. This study had 376 participants who were 12 to 65 years of age. The Glazenburg 2009 study included 90 children aged four to 10 years, and Hanifin 2002 included 372 participants aged from three months to 65 years. The objective of these studies was to establish whether intermittent use of FP added to a moisturiser could reduce the rate of flare over time.
See Table 8.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was assessed only in Hanifin 2002, which used a 6‐point Likert scale. Thirty‐eight of the 119 participants in the vehicle group reported a good to excellent result compared to 163/229 in the FP group, with a significant difference in favour of intermittent FP (RR 0.45, 95% CI 0.34 to 0.59; P < 0.00001; NNTB = 3, 95% CI 2 to 3).
Participant satisfaction
This outcome was not assessed in these studies.
Adverse events
All three studies reported adverse events. The number of participants in the vehicle group reporting adverse events did not demonstrate a statistically significant difference when compared with the participants in the FP group (RR 0.51, 95% CI 0.22 to 1.14; P = 0.61; I² = 67%; Analysis 10.1). No adverse events were reported in Berth‐Jones 2003, so we repeated our analysis, adding one adverse event to all treatment arms, which produced an RR of 0.60 (95% CI 0.41 to 0.90; P = 0.01), which is in favour of vehicle plus moisturiser. The investigators in Berth‐Jones 2003 stated that "during the maintenance phase investigators made no reports of visual signs of skin changes and of atrophy". Comparison of the two other studies showed that there were more adverse events in the FP group in Glazenburg 2009 than in Hanifin 2002. In Glazenburg 2009, very few participants reported skin‐related adverse events, and skin atrophy was not observed. In both studies, viral infections were reported mostly as adverse events. We assessed all three studies as being at an unclear risk of bias overall, therefore, we did not conduct sensitivity analyses for overall risk of bias. We conducted further stratified analyses for the individual domains of risk of bias (see Table 15), but the heterogeneity was not reduced.
10.1. Analysis.

Comparison 10: Vehicle + daily moisturiser versus fluticasone propionate (FP) + daily moisturiser, Outcome 1: Number of participants reporting an adverse event
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
Only the Glazenburg 2009 study assessed this outcome. There was inconsistency between the data reported in the text regarding the objective SCORAD, the corresponding data in the table, and a comment made by the investigators, "Overall a statistically significant difference was observed between treatment groups (P = 0.021)." The increase in SCORAD in the twice weekly FP plus moisturiser group was reported as 7.1 in the data table and as 3.8 in the text. This would appear to be an unintentional error, but we were unable to clarify or analyse the data further due to a lack of response from the corresponding author (see Table 11). The increase for the vehicle plus moisturiser group was 12.2, which was reported consistently in both table and text.
Prevention of flares (lengthening the time to first flare)
The number of participants who experienced a flare was reported in all three studies. In the vehicle group (combined with moisturiser) 203/312 participants had flared after 16 to 20 weeks, whilst in the FP plus moisturiser group only 115/406 had flared (RR 2.17, 95% CI 1.51 to 3.11; P < 0.0001; I² = 74%; NNTB = 3, 95% CI 2 to 3, Analysis 10.2). We explored reasons for the high level of heterogeneity using stratified analyses for effect size as well as for 'Risk of bias' domain, but all studies had an overall unclear risk of bias. One study had a smaller effect size, that is, the second comparison of Berth‐Jones 2003 in which vehicle ointment was compared with FP ointment. The investigators in Berth‐Jones 2003 stated that "the difference between the two formulations was significant (P = 0.002), with a hazard ratio of 2.9 (1.5 to 5.9), indicating that patients using the cream formulation were approximately one third as likely to have a flare as those using the ointment." The other sensitivity analyses according to 'Risk of bias' domain did not lead to further reductions in heterogeneity (Table 15).
10.2. Analysis.

Comparison 10: Vehicle + daily moisturiser versus fluticasone propionate (FP) + daily moisturiser, Outcome 2: Number of participants experiencing a flare
The median time to flare in Berth‐Jones 2003 was 6.1 weeks for both vehicle plus moisturiser groups and more than 16 weeks for both FP plus moisturiser groups. In Glazenburg 2009, the median time to flare was 2.6 weeks in the vehicle plus moisturiser group versus more than 16 weeks in the FP plus moisturiser group, while in Hanifin 2002 the median times were 4.7 weeks and more than 20 weeks, respectively. The rate of flare in the vehicle plus moisturiser group was 3.69 times the rate in the FP plus moisturiser group (HR 3.69, 95% CI 1.80 to 7.55; P = 0.0004; I² = 85%; Analysis 10.3).
10.3. Analysis.

Comparison 10: Vehicle + daily moisturiser versus fluticasone propionate (FP) + daily moisturiser, Outcome 3: Rate of flare
These results indicate that intermittent use of FP (0.05%) cream or FP (0.005%) ointment in combination with a moisturiser is more effective than moisturiser alone to reduce the rate of flare.
Change in use of topical active treatment
This outcome was not assessed in any study.
Changes in skin barrier function
This outcome was not assessed in any study.
Change in health‐related quality of life
This outcome was not assessed in any study.
6 Topical active treatment in combination with a moisturiser versus topical active treatment only
Six studies (648 participants) evaluated whether combining an active treatment, such as a topical corticosteroid, with a moisturiser would be more effective than an active treatment alone (Draelos 2008; Gao 2008; Hanifin 1998; Msika 2008; Simpson 2011; Wu 2014). These studies investigated whether moisturisers have an add‐on effect. We assessed all of the studies as being at a high risk of bias, with the exception of Draelos 2008, which we assessed as being at an unclear risk of bias. Study duration varied from two weeks in Gao 2008, to four weeks in Draelos 2008 and Simpson 2011. The Gao 2008 and Msika 2008 studies were conducted in children; Wu 2014, in adults; and the other studies included both children and adults. All participants suffered from mild to moderate eczema.
Two studies had a within‐participant design (Hanifin 1998; Simpson 2011). Draelos 2008 was a three‐arm study, and Msika 2008 was a five‐arm study. Only two comparisons from each of these two studies contributed to the present overarching comparison.
See Table 9.
Primary outcomes
Change from baseline in disease severity as assessed by the participants
This outcome was not assessed in any study.
Participant satisfaction
This outcome was assessed in two within‐participant studies only (Hanifin 1998; Simpson 2011). In Hanifin 1998 (78 participants), 96% preferred the combination of desonide 0.05% lotion twice daily with moisturiser three times a day, and only 4% preferred desonide 0.05% only. In Simpson 2011, 84.3% to 96.7% of the 123 participants (per‐protocol population) were cited as saying that the addition of the moisturiser, RestoraDerm, to the routine use of their topical steroids "reduces inflammation, relieves dry and itchy skin, provides long lasting hydration, leaves skin protected and maintains healthy skin".
Adverse events
This outcome was assessed by three studies (Draelos 2008; Hanifin 1998; Wu 2014). Draelos 2008 (60 participants) did not report any adverse events in any of the three study arms (i.e. fluocinonide 0.05% combined with a multilamellar vesicular emulsion (MVE) ceramide moisturiser, fluocinonide 0.05% combined with a MVE ceramide‐containing liquid cleanser and fluocinonide 0.05% with a mild cleansing bar). After one week, In Hanifin 1998 (80 participants, within‐participant design), 10 participants reported burning and stinging on the side treated with desonide 0.05% combined with moisturiser versus 11 reports for the side treated with desonide 0.05% alone. After three weeks, none of the participants reported burning and stinging in the combined treatment side versus two on the desonide 0.05% lotion only side. In Wu 2014, 4/63 participants treated with flumethasone ointment combined with moisturiser reported burning, redness, or greasiness versus 10/62 treated with only flumethasone ointment (RR 0.39, 95% CI 0.13 to 1.19; P = 0.10).
Secondary outcomes
Change from baseline in disease severity as assessed by the investigators
We could combine data from two of the studies (Msika 2008; Wu 2014). We included two possible comparisons from the five‐arm Msika 2008 study: desonide 0.05% twice daily combined with moisturiser containing 2% sunflower oil oleodistillate (17 participants) versus desonide 0.05% twice daily (18 participants); and desonide 0.05% once daily combined with moisturiser containing 2% sunflower oil oleodistillate (17 participants) versus desonide 0.05% once daily (15 participants). Msika 2008 assessed disease severity with SCORAD. The investigators in Wu 2014 used the EASI to assess disease severity. The reductions in disease severity in both treatment arms in all of the three comparisons met the MID (estimated at 8.7 for SCORAD, and 6.6 for EASI (Schram 2012)), but the combination of active treatment (topical corticosteroid) plus a moisturiser was only slightly more effective than active treatment alone with a SMD ‐0.87 (95% CI ‐1.17 to ‐0.57; P < 0.00001; I² = 0%; Analysis 11.1), and the difference between the interventions was not clinically important (i.e. the difference between treatment arms did not meet the MID for any of the three comparisons).
11.1. Analysis.

Comparison 11: Active treatment in combination with a moisturiser versus active treatment only, Outcome 1: Change in disease severity as assessed by the investigators
In Draelos 2008, the reductions in IGA were 2.7 for the fluocinonide 0.05% plus MVE ceramide moisturiser group (20 participants), 2.2 for the fluocinonide 0.05% plus MVE ceramide‐containing liquid cleanser group (20 participants), and 1.4 for the fluocinonide 0.05% with a mild cleansing bar group (20 participants).
In Gao 2008, BoPao plus urea 10% ointment (101 participants) was compared against BoPao alone (95 participants). The investigators stated that BoPao cream was categorised as an "inflammatory and antifungal cream [exact meaning unclear due to translation issues] for treatment of eczema", and we were unable to locate any more information about this cream. Treatment was reported to be effective in 89/101 participants on combination therapy compared to 70/95 on BoPao only (RR 1.20, 95% CI 1.04 to 1.38; P = 0.01; NNTB = 7, 95% CI 4 to 28).
In the within‐participant Hanifin 1998 study (78 participants), 70% showed marked improvement to 'clear' on the side treated with desonide 0.05% plus moisturiser compared to 55% on the side treated with desonide only (authors stated "P < 0.01"). Simpson 2011, the other within‐participant study (121 participants), used the EASI. Reductions in EASI were 1.28 (SD 1.94) on the combined treatment side versus 1.01 (SD 1.50) on the side that received active treatment only, with a statistically significant mean of the paired differences of ‐0.27 (95% CI ‐0.52 to ‐0.02) favouring combined treatment.
All studies showed that the combination of active treatment with a moisturiser was more effective (statistically significant) than active treatment alone.
Prevention of flares (lengthening the time to first flare)
This outcome was only assessed in one study (Wu 2014). In the combined treatment group, 8/60 participants experienced a flare versus 14/45 in the group on active treatment only (RR 0.43, 95% CI 0.20 to 0.93; P = 0.03; NNTB = 6, 95% CI 3 to 57), which favoured combined treatment.
Change in use of topical active treatment
This outcome was not assessed in any study.
Changes in skin barrier function
This outcome was assessed in Simpson 2011 only, via corneometry. Skin hydration improved by 5.4 arbitrary units on the side treated with topical corticosteroids plus RestoraDerm, and by 3 arbitrary units on the side treated solely with topical corticosteroids, which were both small improvements.
Change in health‐related quality of life
Only Msika 2008 evaluated this outcome, and used the IDQOL. We combined the results of the two comparisons within this study, and there was no statistically significant difference in change from baseline in quality of life between desonide 0.05% treatment plus a moisturiser versus desonide 0.05% alone (MD ‐1.31, 95% CI ‐2.70 to 0.09; P = 0.07; I² = 0%; Analysis 11.2). These data were confirmed with assessments of the DFI (MD ‐1.03, 95% CI ‐2.47 to 0.42; P = 0.17; I² = 0%; Analysis 11.3).
11.2. Analysis.

Comparison 11: Active treatment in combination with a moisturiser versus active treatment only, Outcome 2: Change in quality of life IDQOL
11.3. Analysis.

Comparison 11: Active treatment in combination with a moisturiser versus active treatment only, Outcome 3: Change in quality of life DFI
Discussion
Summary of main results
We included 77 studies with a total of 6603 participants in this review. Only seven of these studies compared moisturisers versus no moisturisers, which is probably the most important and highly informative comparison to use when assessing the efficacy of moisturisers in people with eczema. In the 15 studies that compared a moisturiser with a placebo or vehicle, the placebos and vehicles were also moisturisers, but lacked the ingredient that was considered to be the most effective in the moisturiser. These comparisons, although valuable, do not provide us with crucial information about how effective the tested moisturiser is by itself, as the placebo or vehicle might decrease disease severity. Indeed, in some studies the placebo or vehicle performed better than the moisturiser under investigation (e.g. 10% and 20% Hippophae rhamnoides cream versus placebo (Thumm 2000), and furfuryl palmitate‐enriched moisturiser versus the moisturiser without furfuryl palmitate (Tripodi 2009)).
There were 29 single study comparisons that evaluated one moisturiser versus another moisturiser; these provide information on whether one moisturiser is more effective than another, but do not inform us about the efficacy of a moisturiser by itself. However, in some instances both treatment arms showed clinically important reductions from baseline in disease severity (meeting minimal important differences (MID)) suggesting that both were similarly effective. It is worth mentioning the Åkerström 2015 study (assessed as being at low risk of bias), which compared a barrier‐strengthening moisturiser containing 5% urea against a reference cream without urea. This study started with a stabilisation phase in which active treatment (mometasone) was used until the eczema was (almost) cleared. During the maintenance phase of 180 days (with no active treatment), fewer participants in the group using barrier‐strengthening moisturiser with 5% urea experienced a flare compared to those using the reference cream, and the time to flare was considerably lengthened (15 compared to 22 days). Furthermore, two studies at unclear risk of bias that were conducted in the Philippines, evaluated oils as a moisturiser (Evangelista 2014; Verallo‐Rowell 2008). In Evangelista 2014 virgin coconut oil was compared to mineral oil, and in Verallo‐Rowell 2008 virgin coconut oil to virgin olive oil. In both studies the oils showed clinically important reductions in disease severity in both treatment arms, but virgin coconut oil appeared to be more effective in both studies.
The Sugarman 2009 study (at high risk of bias), which fits under the overarching comparison of moisturisers versus active treatment, indicated that the ceramide‐containing barrier cream (EpiCeram) showed a large reduction in the SCORing Atopic Dermatitis Index (SCORAD) (18.7) over a four‐week period, which is a clinically important reduction (MID SCORAD is 8.7 (Schram 2012)). However, several other studies (Comparisons 3b, 3d, 3e, and 3f) that evaluated the same ceramide‐containing barrier cream showed inconsistent results in improvements in eczema, which varied from very small improvements to more important clinical reductions. Another study, Jirabundansuk 2014 (high risk of bias), which evaluated a moisturiser containing spent grain, Vitellaria paradoxa (formerly Butyrospermum parkii) extract and Argania spinosa kernel oil together with other ingredients also demonstrated a reduction in SCORAD of 17.92, which is a clinically important reduction. This appeared to indicate that such a moisturiser might have an anti‐inflammatory effect, but it is equally possible that this may be due to the effective moisturising action of the product.
Three studies were conducted to assess whether twice weekly topical fluticasone propionate in combination with a moisturiser was more effective than moisturiser alone (plus the vehicle of the fluticasone propionate) in preventing flares, which is important for people with eczema who experience frequent flares. The seven studies that compared topical active treatment with a moisturiser versus active treatment alone provide us with insight into the add‐on efficacy of moisturisers when applying topical active treatment.
In general most of the moisturisers that were evaluated appeared to show at least some beneficial effect as assessed by our predefined outcomes, however the extent of the effects varied widely across the included studies.
Our primary outcome 'participant‐assessed disease severity' was addressed in only a third (24) of the studies and itch was assessed in 23 studies. In most instances only small reductions were seen in the outcome change from baseline in itch (Comparisons 1, 2b, 2c, 2d, and 2e), and these were usually based on assessments with visual analogue scales (VAS). Noteworthy improvements in itch occurred with Atopiclair, which showed a statistically significant difference compared to its vehicle (Comparison 2a). Possibly more importantly, pooled data for all of the moisturisers versus control (Comparison 2f) showed a large effect on reduction of itch in favour of the use of moisturisers. However, apart from the fact that there was a high degree of inconsistency in the data, the clinical relevance of this effect is difficult to interpret. As yet no MID has been established for itch on VAS scales, and the studies that contributed data to this outcome used a range of different scales. Based on a recent publication, the MID of the VAS for itch lies within a two to three point decrease (Reich 2016).
Only 13 studies assessed 'participant satisfaction with treatment'. These did not report in detail about specific preferences and did not elaborate about which moisturisers are preferable for daytime use and which for night‐time use, or whether choices vary depending on the season (e.g. winter versus summer). The secondary outcome 'change in health‐related quality of life' was only covered in 10 of the 77 studies. As eczema is a chronic disease with a clear impact on quality of life (Lewis‐Jones 2006; Nutten 2015), the significance of relevant patient‐reported outcomes (PROs) would appear to have been underestimated in the majority of studies.
The reporting of adverse events, although included in over half of the studies (41/77), was not informative, and most comments about these events were limited and quite generic. Most of the adverse events that were reported with moisturisers consisted of smarting, stinging, pruritus and erythema, and sometimes folliculitis.
The most assessed outcome, assessed in 65 of the 77 studies, was our prespecified secondary outcome 'investigator‐assessed disease severity'; 25 studies evaluated this with the SCORAD index (European Task Force on Atopic Dermatitis 1993), and 14 with the Eczema Area and Severity Index (EASI) (Hanifin 2001), which is the core outcome instrument for measuring clinician‐reported signs in eczema studies (Schmitt 2014). The remaining studies used Likert scales or other instruments. The other secondary outcomes assessed in studies included prevention of flares (16 studies); change in use of topical active treatment (eight studies); and changes in barrier function (29 studies).
Pooling of data for the prespecified outcomes of our review was limited, mainly because of the wide variety of comparisons, which were often assessed only by single studies. We have provided 'Summary of findings' tables for those comparisons we consider to be the most important and where data could be pooled.
For the comparison 'moisturisers versus no moisturiser' (Table 1), there was low quality evidence of a statistically significant difference favouring moisturisers over no moisturiser for the outcome 'change from baseline in disease severity as assessed by the investigators' based on the SCORAD. However, the SCORAD MID of 8.7 was not met (Schram 2012). There was also low quality evidence that more adverse events occurred in the moisturiser group than in the no moisturiser group, which was not totally unexpected. We reported two important observations (both low quality evidence); firstly, that there was a clinically relevant and statistically significant difference in favour of moisturisers for rate of flare which was reduced to almost a quarter (0.27), with a prolonged time to flare; and secondly, when moisturisers were used, a smaller quantity of topical corticosteroids was needed to achieve a greater reduction in SCORAD. However, this difference in SCORAD did not meet the MID. There were no statistically significant differences between the groups for changes in quality of life (low quality evidence).
There was moderate quality evidence for the efficacy and safety of Atopiclair over its vehicle for all the outcomes evaluated by the studies (Table 2). Both participants and investigators were in agreement that Atopiclair was the more effective, but the difference in investigator scores with the EASI did not meet the MID of 6.6 (Schram 2012). In addition, participants in the Atopiclair group experienced fewer flares than those in the vehicle group. Atopiclair contains glycyrrhetinic acid, which, as summarised in Abramovits 2008, "has anti‐inflammatory effects, possibly mediated through inhibition of 11‐β‐hydroxysteroid dehydrogenase, an enzyme that interconverts active cortisol to and from inactive cortisone; this inhibition may increase the cortisol available for binding to local glucocorticoid receptors, including in the skin". Atopiclair reduced itch more effectively than its vehicle and the difference might be clinically important (Reich 2016), on the basis of the MID described above.
There was low to moderate quality evidence for several outcomes assessed in the comparison of urea‐containing moisturisers versus vehicle, placebo or no moisturiser (Table 3). Both participants and investigators considered urea‐containing cream to be more effective than its control, but there were fewer adverse events in the control group. It is fairly widely acknowledged that urea can cause transient burning and stinging after application. The use of urea‐containing moisturiser reduced the rate of flare by one‐third (0.31) (low quality evidence).
The effects of glycerol (glycerine) are summarised in Table 4. There was moderate to high quality evidence for the outcomes assessed. Both participants and investigators considered glycerol‐containing moisturiser to be more effective than vehicle or placebo cream. However, for the investigator‐assessed change in disease severity, the 8.2 SCORAD MID was not met between the two treatment arms.
When oat‐containing creams were compared to vehicle or no moisturiser there was no difference between the two treatment arms for participant‐ and investigator‐assessed change in disease severity (low to very low quality evidence) (Table 5). In contrast there were statistically significantly fewer flares in the oat‐containing moisturiser group, and the rate of flare was reduced by a factor of almost five (0.21), which was quite remarkable. Furthermore, smaller amounts of corticosteroids were needed in the oat‐containing moisturiser group than in the control group. However, more adverse events were reported in the oat‐containing moisturiser group.
Table 6 compares all moisturisers to vehicle, placebo or no moisturiser, and the quality of evidence ranges from low to high. Participants considered the use of a moisturiser to be more effective than the control (low quality evidence), and this was confirmed by the judgement of the investigators in 12 studies (high quality evidence). There was low quality evidence of no difference in participant satisfaction or in the number of participants experiencing an adverse event between the two treatment arms. There was a statistically significant difference in the number of participants who experienced a flare which was three times lower in the moisturiser group (moderate quality evidence), and rate of flare was nearly reduced by a factor of four (0.27). The data showed that the use of moisturisers decreased use of topical corticosteroids without compromising reductions in disease severity (low quality evidence). There was no statistically significant difference in changes in quality of life between the two treatment groups (low quality evidence). Pooled data from seven studies showed that the use of moisturisers had a large effect on itch compared to the control group. However, due to considerable heterogeneity in the results, the use of different assessment scales, and the fact that the clinical relevance of this outcome is difficult to estimate, caution must be exercised in interpreting these data.
Three within‐participant studies compared a licochalcone‐containing moisturiser with topical hydrocortisone acetate 1% cream (Table 7). These studies showed that there were no statistically significant differences between the treatment effect, satisfaction, adverse events and number of participants who experienced a flare (all low quality evidence). In Udompataikul 2011 the study investigators stated that "licochalcone A, a major phenolic constituent of liquorice species Glycyrrhiza inflata, has lately been reported to possess anti‐inflammatory and antimicrobial properties". The investigators in Angelova‐Fischer 2014 indicated that "licochalcone A suppress the production of pro‐inflammatory mediators and cytokines such as PGE2, LTB4, IL‐6 and TNF‐α in in vitro systems relevant to the skin such as dermal fibroblasts, granulocytes, dendritic cells and human skin equivalents". It is interesting to note that moisturisers with non‐steroidal anti‐inflammatory properties, such as these licochalcone‐containing moisturisers (as well as Atopiclair), would appear to have similar effects to low potency topical corticosteroids.
Four trials that investigated vehicle treatment combined with a moisturiser compared to fluticasone propionate twice weekly in combination with a moisturiser mainly addressed the potential benefits of the twice weekly fluticasone propionate in preventing flares (Table 8). There was high quality evidence that participants considered twice weekly fluticasone propionate more effective than the control treatment in achieving good to excellent improvement. Furthermore, twice weekly fluticasone propionate in combination with a moisturiser was shown to be effective in reducing flares compared to a moisturiser with vehicle treatment (moderate quality of evidence), and reduced the rate of flare to almost a quarter (0.27). There was no statistically significant difference between the intervention groups for the number of participants who reported an adverse event (low quality evidence).
The last comparison for which we were able to pool data was topical active treatment in combination with a moisturiser versus topical active treatment alone, summarised in Table 9. There was low quality evidence that participants were more satisfied with the combined therapy, and moderate quality evidence from the investigators that adding a moisturiser to topical active treatment was more effective than topical active treatment alone. There was no difference in the number of adverse events (very low quality of evidence) and, based on one study, the addition of a moisturiser to topical active treatment reduced the number of participants who experienced a flare. There was no difference in change of quality of life (low quality of evidence), but it is likely that the three‐week study duration was probably too short to detect a difference.
The results of the 29 studies that assessed change from baseline in skin barrier function showed wide and inconsistent variation of small to substantial improvements.
The overall conclusion from the various comparisons is that moisturisers are effective at reducing rate of flare, can prolong time to flare, reduce the use of topical corticosteroids, and, when combined with topical active treatment, lead to better results than active treatment alone. However, the quality of evidence varied from low to high, and the MID for the investigators' assessments based on (objective) SCORAD and EASI was not met.
Overall completeness and applicability of evidence
Although we were able to include 77 studies, the majority (70/77) were at unclear to high risk of bias, and very few studies compared similar interventions.
The comparison that would be expected to provide the most reliable information about the efficacy of moisturisers in eczema was moisturiser versus no moisturiser, but this was only addressed in seven studies (six provided usable data). The low quality evidence from these studies indicated that the use of moisturisers was more effective, but not clinically important (investigator‐reported), than no moisturiser and resulted in fewer flares, a prolonged time to flare and a reduced need for topical corticosteroids to reach comparable reductions in eczema severity.
The 29 studies that compared one moisturiser with another moisturiser (23 provided usable data) were all evaluated in single studies with different treatment arms, which did not permit pooling of their data. Although it was clear from some of these studies that improvements were experienced in one or both treatment arms (participant‐reported, investigator‐reported, or both), these studies mainly indicated that moisturisers might have a similar effect to each other, or that one moisturiser might be better than another, though evidence for this was based on a single study ‐ often with a small sample size‐ and mostly at an unclear to high risk of bias. It also demonstrated the heterogeneous performance of moisturisers, which, as was emphasised by Danby and colleagues, has a notable impact on the treatment of eczema, and its long‐term control (Danby 2016).
There was moderate quality evidence that Atopiclair, urea‐containing moisturisers and glycerol‐containing moisturiser (high quality evidence for investigators’ assessment) were more effective than their control (no moisturiser, vehicle or placebo), although the MID for investigator assessments was not met. Both Atopiclair and urea‐containing moisturisers reduced the number of flares (this outcome was not assessed in the comparisons with glycerol‐containing moisturisers).
The overall conclusion, according to both participants (low quality evidence) and investigators (high quality evidence), when all comparisons of moisturiser versus vehicle, placebo or no moisturiser were combined, was that moisturisers are effective, can reduce flares (moderate quality evidence), and have a corticosteroid‐sparing effect.
Adding moisturisers to an active topical treatment resulted in better clinical results than topical active treatment alone, which is an encouragement for the continued use of moisturisers during eczema flare‐ups (moderate quality evidence). Twice weekly fluticasone propionate added to daily use of moisturisers reduced the likelihood of flares over time, and has key implications for daily practice, particularly in people with eczema who experience frequent flare‐ups. Furthermore, the use of moisturisers decreased usage and the need for topical corticosteroids, which is another important outcome. There was low quality evidence that licochalcone was as effective as hydrocortisone acetate 1% cream.
The majority of moisturisers considered in this systematic review included a large array of ingredients (see Notes sections in Characteristics of included studies), which made it impossible to distinguish clearly between hydrophilic and hydrophobic moisturisers, or, indeed, between humectant, emollient and occlusive moisturisers. Uncertainty about the exact proportions of these ingredients in a moisturiser does not permit a clear distinction to be made, especially as the proportions are rarely mentioned in the labelling or packaging. The quantity of certain ingredients can also affect the way a moisturiser feels on the skin. Some ingredients in a moisturiser enhance its ability to remain on the skin (e.g. petrolatum), while others (e.g. oils) transfer quickly to clothes or bed linen. Temperature can influence the viscosity of moisturisers, which is crucially important for application on the skin, as the higher the viscosity of the moisturiser, the more difficult it is to smear and spread on the skin, which can cause friction and lead to friction‐related adverse events. Once all of these aspects are taken into account, as well as dryness, day or night‐time, the seasons, the weather, and even the clothes that are worn, people with eczema will express a variety of preferences in different situations. The ideal moisturiser should be easy to spread on the skin, have no smell, contain no irritating or sensitising ingredients, be cosmetically acceptable without excessive sticking to clothes and bed linen, and be affordable for people with eczema.
This review does not address the importance of educating people with eczema on how to apply moisturisers, how much to use or how often to use them. Cork and colleagues demonstrated that correct and adequate instructions in usage "of the treatments resulted in an 800% increase in the use of emollients, a reduction in disease severity as assessed with six area, six sign atopic dermatitis severity score (SASSAD) (89% reduction compared with baseline) and no overall increase in the use of topical steroids" (Cork 2003a). The importance of education as part of the management strategy has also been emphasised by several other investigators (Arkwright 2013; Ersser 2014; Mason 2013; Oakley 2016). Another shortcoming of the studies in this review was the lack of detailed reporting of adverse events, which meant that we could not conclude which moisturiser might be preferable for avoiding adverse events. None of the studies reported aspects such as the smell, stickiness or greasiness of the moisturiser, but rather adverse effects such as pruritus, stinging, smarting or increase in erythema. We are still unable to confirm how often moisturisers need to be applied, although it is more generally acknowledged that this should be at least once a day and preferably more frequently. Current recommended quantities of moisturisers range from 250 g to 500 g per week (Moncrieff 2013; NICE 2007; Wollenberg 2016).
Quality of the evidence
Limitations in study design and implementation
Although we only included randomised controlled trials (RCTs), we assessed most studies as being at either unclear risk or high risk of bias (for details see the Risk of bias in included studies). The method of sequence generation was described in detail in slightly more than half of the studies and allocation concealment in just under half, so for the remaining studies we judged these domains as being at unclear risk of bias. The lack of (adequate) blinding was the most frequent reason for us giving studies an overall assessment of a high risk of bias. In addition, in one‐third of the studies (25/77) there was a degree of incomplete data reporting, which did not permit a full and accurate interpretation of the study results.
In 33 instances investigators or pharmaceutical companies were helpful in providing us with missing study details (seeTable 11). We were not successful in obtaining any response from investigators or industry in 13 cases, despite repeated attempts to clarify missing study details. We did not seek further clarification for 21 studies, mainly because publication was more than 10 years ago, or because we were unable to locate a current email addresses for any of the investigators.
Inconsistency of the results
Most of the comparisons included in this review were assessed in single studies, which did not allow us to assess consistency of results across studies for the various moisturisers. For several comparisons where pooling of data was possible, we observed substantial heterogeneity for one or more outcomes. In Comparison 1 (moisturiser versus no moisturiser; Table 1), one study, Giordano‐Labadie 2006, was responsible for substantial heterogeneity for the outcome 'amount of corticosteroid used' (I² = 68%), as far more topical corticosteroids were used in both treatment arms than in the other study (Grimalt 2007). This was surprising, especially when considering that disease severity at baseline was markedly worse in the Grimalt 2007 study. (See Table 5 and Table 6).
In Comparison 2a (Atopiclair versus vehicle; Table 2), we observed substantial heterogeneity (I² = 51%) for the outcome 'change from baseline in disease severity as assessed by the investigators'. This was mainly caused by the Boguniewicz 2008 study, which showed a greater effect size and was the only study in which there was uncertainty regarding the efficacy of the allocation concealment and of the blinding. We observed considerable heterogeneity (97%) for the outcome 'change from baseline in itch', but the reasons for this remain unexplained.
In Comparison 2d (oat‐containing moisturiser versus vehicle or no moisturiser; Table 5), there was substantial heterogeneity for the outcome 'change from baseline in disease severity as assessed by the investigators' (I² = 65%). We explored the heterogeneity by conducting further sensitivity analyses based on individual domains of risk of bias in addition to carrying out a stratified analysis adjusting for effect size. This heterogeneity appeared to be caused by Giordano‐Labadie 2006, which showed a greater effect than the other two studies, and, although its exclusion from the analysis eliminated the heterogeneity, it did not alter the conclusions (Table 15).
In Comparison 2f (all moisturisers versus vehicle, placebo or no moisturiser; Table 6), five studies contributed to the outcome 'change from baseline in disease severity as assessed by the participants'. There was considerable inconsistency (I² = 95%) between the studies, which was in part reduced through sensitivity analyses based on risk of bias domain, especially with our sensitivity analysis for risk of attrition bias. For the outcome 'change from baseline in itch' the same held true (I² = 94%), but the heterogeneity remained unexplained. For the outcome 'participant satisfaction' (I² = 83%), the repeat sensitivity analysis no longer showed heterogeneity after we excluded a study at high risk of bias (Abramovits 2008). Pooled data for the outcome 'number of participants who experienced a flare' also demonstrated heterogeneity (I² = 73%), with those studies that had been judged to be at an unclear to high risk of bias showing better results. Considerable heterogeneity was also seen for the outcome 'change from baseline in quality of life' (I² = 79%). Gayraud 2015 was the only study at low risk of bias and demonstrated the largest effect size, whilst we assessed the other two studies as being at a high risk of bias (Giordano‐Labadie 2006; Grimalt 2007). Furthermore, in the Grimalt 2007 study, 40% of participants did not complete the questionnaires, and therefore we assessed this domain as being at high risk of attrition bias, which might explain some of the heterogeneity.
In Comparison 4a (licochalcone‐containing moisturiser versus hydrocortisone acetate 1% cream) the pooled data from two within‐participant studies for the outcome 'change from baseline in itch' demonstrated considerable heterogeneity (I² = 85%). There was a difference in study duration (four weeks for Wanakul 2013 versus one week for Angelova‐Fischer 2014), and a difference in application sites, as Wanakul 2013 used the two sides of the body, while Angelova‐Fischer 2014 used a straight comparison between the two forearms, which could explain the inconsistency. These explanations are also applicable for the outcome 'change from baseline in transepidermal water loss' (I² = 86%). In addition, there was a similar degree of inconsistency (I² = 85%) for 'change from baseline in disease severity as assessed by the investigators', which was addressed in three studies (see Table 7). We explored possible explanations for the heterogeneity (see Table 15), and considered that the most important explanation was that the effect sizes differed between the three studies. We could only include data for the first week of the Angelova‐Fischer 2014 study, as only the first week was randomised, and therefore smaller reductions were reported in both treatment arms than in the other two studies that had four‐week durations and correspondingly larger treatment effects (Udompataikul 2011; Wanakul 2013).
In Comparison 5 (vehicle twice weekly combined with daily moisturiser versus fluticasone propionate twice weekly combined with daily moisturiser; Table 8), there was substantial heterogeneity for the number of participants reporting an adverse event (I² = 67%). No adverse events were reported in either of the two comparisons included in Berth‐Jones 2003, while in the other two studies adverse events were reported in both arms, with a predominance in the fluticasone propionate treatment arm. There was also substantial heterogeneity for the number of participants experiencing a flare (I² = 72%). One study had a smaller effect size (i.e. the second comparison of Berth‐Jones 2003 in which vehicle ointment was compared with fluticasone propionate ointment), removal of the study from the analysis reduced some, but not all, of the heterogeneity. The investigators in Berth‐Jones 2003 stated that "the difference between the two formulations was significant (P = 0.002), with a hazard ratio of 2.9 (1.5 to 5.9), indicating that patients using the cream formulation were approximately one third as likely to have a flare as those using the ointment." We also observed considerable heterogeneity in the pooled data of the three studies for this comparison in the hazard ratio for rate of flare (I² = 85%), which remained unexplained (see sensitivity analyses in Table 14 and Table 15).
Indirectness of the evidence
The participants in the included studies had mostly mild to moderate eczema according to prespecified criteria (see Types of participants) and, therefore, were a reasonably representative group that matched our inclusion criteria. However, only a limited number of studies evaluated the most informative outcome for this review, which was whether moisturisers are effective (and safe) in people with eczema; i.e. by comparing moisturiser versus no moisturiser, though many of the comparisons provided us with indirect evidence (e.g. moisturiser versus another moisturiser).
Patient‐reported outcomes (PROs) have been a target of increasing interest for the last 30 years. Data derived from PROs have demonstrated improvements in communication and decision‐making between physicians and patients, and can lead to greater satisfaction with a chosen treatment regimen (Nelson 2015). However, PROs for this clinical topic appear not to have been adequately appreciated, especially with regard to participant satisfaction with the use of moisturisers ‐ which can be sticky, greasy, smelly, and time‐consuming to apply. Frequently the included studies based inferences on simple questions ("Which one do you prefer?" or "Do you want to continue?") instead of addressing satisfaction with treatment, and this provided us with a reason to downgrade the quality of the evidence for indirectness in Table 2, Table 5 and Table 9.
Imprecision of the results
Together with inconsistency, imprecision was the most frequent reason for downgrading the quality of evidence for predefined outcomes in the 'Summary of findings' tables. Small sample sizes and low occurrence of events leading to wide confidence intervals caused us to downgrade for imprecision for one or more outcomes in all of the 'Summary of findings' tables.
Publication bias
We included a number of abstracts from conference proceedings, most of which subsequently appeared as full text publications. However, among the ongoing trials, which were often industry‐sponsored, there were a number of studies that had completed a few years ago, but have not been published, which tends to suggest that these trials showed no, or marginal, benefit for the moisturiser under investigation. Furthermore, we identified 47 duplicate publications for the same study data (Figure 1). Comparison 2f (all moisturisers versus control) was the single comparison for which we had more than 10 studies addressing an outcome; 12 studies contributed to the outcome 'change in disease severity as assessed by the investigators'; the funnel plot showed no asymmetry (Figure 4).
Potential biases in the review process
Although we took numerous steps to reduce publication bias through systematic searching and inclusion of studies published in languages other English, it is possible that the analyses in this review are based on an incomplete set of the data collected and analysed in the original trials. We made every attempt to contact investigators for missing trial data, sometimes six times over a six‐month period. However, despite our numerous attempts, we received no response for 13 studies and so were unable to obtain clarification of some of the missing trial details and study data (see Table 11). Data from studies that had a within‐participant design could not be adjusted accurately. The absence of a correlation coefficient for these studies meant that we could not analyse the data in a way that took account of the within‐participant nature of the design. For a limited number of dichotomous outcomes the results have been presented narratively, and for continuous data our decision to apply a pragmatic correlation coefficient to adjust continuous data from within‐participant studies may not reflect the true nature of the within‐person correlation.
Agreements and disagreements with other studies or reviews
Our extensive searches identified several reviews and guidelines, a practice statement and a dissertation that addressed the efficacy and usefulness of moisturisers in the treatment of eczema (Eichenfield 2014b; Hoare 2000; Katayama 2014; Lindh 2015; Mack Correa 2012; Moncrieff 2013; Nankervis 2016; NICE 2007; Oakley 2016; Penzer 2012; Ring 2012a; SIGN 2011; Silverberg 2014; Sirikudta 2013; Wollenberg 2016).
A general conclusion that can be drawn from the reviews and guidelines is that consistent, frequent, and generous use of moisturisers is necessary to restore or maintain the skin barrier. Their recommendations indicate that physicians should advise their patients to use moisturisers in large amounts (250 g to 500 g per week), preferably after bathing or showering. Educational programmes, supportive information and guidance were considered to be essential for moisturisers to achieve an optimal benefit. There was general agreement that people with eczema should have the opportunity to choose between different moisturisers and, more specifically, those that are most suitable for their own skin. Several of these reviews and guidelines referred to the studies of Cork 2003b and Danby 2011b, which stated that aqueous cream BP (or other leave‐on moisturisers containing sodium lauryl sulphate) should not be used as a leave‐on moisturiser in eczema, as this has been shown to have a negative impact on the skin barrier. Furthemore, some recent studies have questioned or discouraged the use of oils as they can damage the skin barrier, or impair skin barrier maturation in neonates (Cooke 2016; Danby 2013; Kanti 2014).
A comprehensive systematic review of treatments for atopic eczema was conducted in 2000 as a part of the NHS Health Technology Assessment (HTA) Programme (Hoare 2000). Only five RCTs were retrieved at that time and the authors of that review concluded that although moisturiser "may have beneficial actions, there is an urgent need to answer several basic questions about their use, preferably through industry‐independent RCTs". They also provided a summary of the research gaps in addition to the top 10 questions that required addressing in future RCTs. Recently, a systematic scoping review that provides an update to this review has been published; this has a search date of August 2013 (Nankervis 2016). The reviewers acknowledged that the number of RCTs evaluating moisturisers had increased considerably, with the addition of 15 studies since 2000, but that still these studies were poorly designed, with small sample sizes and short follow‐up periods, and reporting of results was frequently inadequate. The 'Risk of bias' assessment of the included studies in this HTA update was somewhat limited compared to our review, and did not include an evaluation of reporting bias and attrition bias. The authors discussed the studies in detail with respect to benefits, harms and overall implications for research and practice, but did not perform meta‐analysis or provide a rating of the quality of the evidence. The conclusions were "that the trial evidence was not clear enough to make recommendations with regard to using emollients to reduce the severity of eczema and prevent flares or to reduce the need for other eczema treatments". Our current review builds on the scoping review by reporting moderate to low quality evidence for the efficacy of moisturisers to prevent flares, as well as low quality evidence that moisturisers reduce the need for topical corticosteroids to attain similar reductions in eczema severity.
Another more recent systematic review, which had a broader scope than our review, summarised the clinical effectiveness of moisturisers in atopic dermatitis and related disorders, and also included participants with irritant hand dermatitis and ichthyosis vulgaris (Lindh 2015). Our search retrieved 45 more studies that addressed eczema, which might be because we conducted more extensive searches for studies in additional databases. Although a 'Risk of bias' assessment was conducted in the Lindh 2015 review, supportive judgements and justifications for those judgements were often lacking. However in our review we were quite successful at contacting principal investigators, and consequently our judgements for the various 'Risk of bias' domains differed in a number of instances. The authors of the Lindh 2015 review considered that the efficacy for urea‐based preparation was most well‐documented and concluded that they had "found convincing evidence that moisturizer treatment is beneficial for AD [atopic dermatitis] and related disorders". Although we are in general in concordance with the conclusion of the review ‐ that moisturiser treatment is beneficial ‐ a rating of the quality of evidence by the reviewers was lacking.
An evidence‐based treatment update for atopic dermatitis was published in 2014 (Silverberg 2014). This systematic review included randomised controlled trials as well as systematic reviews, complied with the PRISMA statement, and covered the period from 2011 until August 2013.However, the searches were restricted to MEDLINE only. There were clear inclusion and exclusion criteria and GRADE was used to assess the quality of evidence, but only for the systematic reviews retrieved by the search, which did not include any for moisturisers. The time span was quite limited (2.5 years) and only one RCT was included and a full critical appraisal was not carried out. The review reached no clear conclusions on the efficacy of moisturisers.
We identified and evaluated several narrative reviews, such as the Mack Correa 2012 review, which described the role of moisturisers in eczema management and summarised studies conducted with moisturisers, but did not appraise the studies that were selected critically. The narrative Sirikudta 2013 review provided a general overview of active ingredients in moisturisers, including those in popular over‐the‐counter moisturisers, and those that are supposed to have an anti‐inflammatory effect such as Vitellaria paradoxa (shea butter; formerly Butyrospermum parkii), glycyrrhetinic acid and licochalcone A (from Glycyrrhiza inflata), as well as a list of moisturising properties of the active ingredients. Our Cochrane Review included studies that evaluated moisturisers containing these ingredients.
Moncrieff 2013 is a consensus statement on the use of emollients in dry‐skin conditions that summarised current data and practice, and emphasised that there is evidence that urea‐containing creams enhance efficacy, prolong time to flare, and are topical corticosteroid‐sparing when compared to not using a moisturiser. The statement covers seven key topics, and concludes with consensus‐based conclusions and recommendations that are consistent with the findings of our review. An additional important conclusion was that the efficacy of a moisturiser is dependent on the adherence to treatment of people suffering from eczema, and that informed, shared decision making based on a spectrum of moisturisers, is key to optimising moisturiser treatment.
Preparation of the eczema treatment guideline of the American Academy of Dermatology included an extensive search across various databases (Eichenfield 2014a). Its authors based the evidence on the 'Strength of Recommendations Taxonomy' (SORT), where levels of evidence for individual studies are graded on a 3‐point scale and recommendations are formulated according to the best available evidence (graded A, B, C). This guideline reported that there is strong evidence that the use of moisturisers can reduce disease severity and the need for pharmacological treatment, and that, therefore, their use should be an integral part of eczema treatment. The number of studies included to evaluate the efficacy of moisturisers was much smaller than in our review, but the results and conclusions of the guideline are in broad agreement with our findings.
Katayama 2014, a Japanese guideline, was not very informative regarding moisturisers for eczema; it contained no evidentiary support from clinical trials, ratings of the quality of evidence or gradings of strengths of recommendations, but mainly reported that moisturisers are recommended and useful to prevent flares. The guideline, however, did provide a warning that "urea preparations should be used with caution, as they can stimulate an eroded surface or strongly inflammatory skin".
Similarly, the Canadian Practical Guide for treatment and management of eczema did not involve a robust methodological approach, but mainly indicated that moisturising of the skin is a fundamental part of treatment for eczema (Lynde 2005).
The National Institute for Health and Clinical Excellence (NICE) guideline only addressed eczema in children from birth to 12 years old (NICE 2007). The recommendations support the daily use of moisturisers for all eczema severities based on children’s need and preferences. Data from a limited number of RCTs that investigated the efficacy of moisturisers were summarised in evidence tables. Follow‐up searches (surveillance review) were conducted up to 2013 and concluded there was no new evidence that might have an impact on the clinical recommendations. In July 2016 it was decided not to update this guideline further (www.nice.org.uk/Guidance/CG57).
The guideline from the European Dermatology Forum, European and the European Academy of Dermatology and Venereology (EADV), the European Task Force on Atopic Dermatitis (ETFAD), European Federation of Allergy (EFA), the European Society of Pediatric Dermatology (ESPD), and the Global Allergy and Asthma European Network (GA2LEN) (Ring 2012a), reported that there was "limited evidence‐based proof" for using moisturisers. Different ingredients in moisturisers were described, together with their benefits and harms, but these guidelines did not undertake any 'Risk of bias' assessments or any appraisal of the methodological quality of the included studies.
The Scottish Intercollegiate Guidelines Network (SIGN) guideline presented conclusions based on the Hoare 2000 systematic review, and provided levels of evidence, graded recommendations (A to D), and identified good practice points for the various eczema treatments (SIGN 2011). Its authors concluded that people with eczema should have continuous treatment with moisturisers, and should continue moisturiser treatment during treatment with topical corticosteroids. Furthermore, twice weekly maintenance treatment with topical corticosteroids should be considered in people with moderate to severe eczema with frequent flares (based on the Berth‐Jones 2003 study).
An overview of how moisturisers should be used in practice, how they work, and what type of moisturisers are available, was summarised in a best practice statement produced by the British Dermatology Nursing Group (BDNG) in association with Dermatological Nursing (Penzer 2012). The statements made in this publication were supported by studies or guidelines, and are in concordance with the conclusions we draw in this Cochrane Review.
A recent paper entitled 'Views on unwanted effects of leave‐on emollients and experiences surrounding their incidence' addressed the results of a survey amongst 210 people with eczema and their carers (Oakley 2016). This study aimed to gain a greater understanding of unwanted events associated with moisturisers, and whether these might influence adherence. The findings of this survey are consistent with the results our review, as we found that participants' satisfaction with moisturisers was only assessed in 13/77 studies and that reporting of adverse events was inconsistent, without clear distinction between adverse events and unwanted events. In the Oakley 2016 survey 126/185 responders reported that they had experienced unwanted effects with the use of moisturisers (stinging was most reported), and 90/126 stopped using the moisturiser because of this unwanted effect. Oakley 2016 stated that these results confirm that poor adherence is related to unwanted effects, which underlines the importance of patient satisfaction with moisturisers in both clinical practice and future research.
Authors' conclusions
Implications for practice.
Treatment for eczema encompasses active treatments to address active inflammatory lesions, management strategies to minimise triggers, life style measures and education about eczema, but also adjunctive therapies to optimise skin barrier function and to prevent flare‐ups. The use of moisturisers has always been an integral part of eczema treatment and there was an unmet need for summarising the overall evidence about their effects. This review included 77 studies from which, although we assessed most as being at unclear to high risk of bias, we have been able to draw the following conclusions:
There is low quality evidence that applying moisturisers is effective in reducing disease severity compared to not using moisturisers (investigator‐assessed outcome), although not to a clinically important extent, as the minimal important difference (MID) was not met. However, use of moisturisers reduced the number of participants who experienced a flare, prolonged the time to flare, reduced the rate of flare by a factor of almost four and reduced the total amount of topical corticosteroids that would have been needed to achieve similar reductions in the SCORing Atopic Dermatitis Index (SCORAD), all of which are clinically important.
There is moderate quality evidence that Atopiclair is more effective than vehicle (investigator and participant assessments), but the MID was not met. It had an important effect on itch and on reduction of flares.
There is low to moderate quality evidence that urea‐containing creams are more effective than no moisturiser, placebo or vehicle (based on both investigator and participant assessments), and reduced rate of flare by a third, but with more adverse events. Efficacy was confirmed by one study, at low risk of bias, conducted over 180 days, that showed that barrier‐strengthening moisturiser with 5% urea reduced the number of participants who experienced a flare, and increased time to flare in comparison to the reference cream.
There is moderate to high quality evidence that glycerol‐containing moisturisers are more effective than 'vehicle' or placebo (investigator and participant assessments), but the MID was not met.
There is low to very low quality evidence that there is no difference in efficacy between oat‐containing cream and vehicle or no moisturiser (investigator and participant assessments), and more adverse events were seen. However, the use of oat‐containing creams reduced flares by a third, rate of flare to a fifth, and reduced the need to apply topical corticosteroids.
There is high quality evidence that the use of moisturisers is more effective (investigator assessments) than the use of no moisturiser, vehicle or placebo (controls). Use of moisturisers had a large beneficial effect on itch compared to controls. However, due to considerable heterogeneity in the results, the use of different assessment scales and because the clinical relevance of this outcome is difficult to estimate, caution must be exercised in interpreting these data. Use of moisturiser reduced flares by a third, and rate of flare to almost a quarter. Reduced amounts of topical corticosteroids were needed when moisturisers were used.
There is low quality evidence that licochalcone‐containing cream is as effective as hydrocortisone acetate 1% cream (investigator assessments).
There is high quality evidence that twice weekly fluticasone propionate plus a moisturiser provides more effective eczema control than a moisturiser alone (participant assessments), and moderate quality evidence that it reduces the number of flares by a factor of two, and reduces the rate of flare to almost a quarter.
There is moderate quality evidence that combining topical active treatment with a moisturiser is more effective than treatment with active treatment alone (investigator assessments). There is also low quality evidence that participants were more satisfied with the combined treatment.
There were no differences between treatments for the number of participants experiencing an adverse event (except for urea‐ and oat‐containing creams), or in self‐assessed quality of life.
Reductions in itch were generally small, except with Atopiclair, where the effect seemed larger and clinically important.
Improvements in skin barrier function varied from small to more substantial improvements, but these were inconsistent across studies.
Overall, considering the various included studies and comparisons in this review we can conclude that the efficacy of moisturisers varied from minimal to substantial.
Moisturisers appeared to have a beneficial effect, but the extent of the effect varied widely, and in only a few studies did moisturisers produce a reduction in disease severity that met the MID. There is no convincing evidence that moisturisers improve eczema when used alone. However, the overall conclusion is that moisturisers are safe, prevent flares, prolong time to flare, reduce the amount of topical corticosteroids needed, and that topical active treatment is more effective when used in combination with moisturisers.
This review does not inform us about the importance of education in how to apply moisturisers, in particular how often they need to be applied and how much to use. However, since moisturisers reduce flares, prolong the time to flare, decrease the necessity for topical corticosteroids and increase the efficacy of active treatment, it makes clinical sense to encourage adherence to moisturiser therapy. This is especially important as moisturiser therapy is time consuming and often required throughout life, as eczema is a chronic condition.
This review provides no information about which moisturisers might be preferred for different parts of the body, or preferred during different seasons or personal circumstances, or which moisturisers best fit the actual disease status (acute or chronic) or severity (mild, moderate or severe). There is no evidence to support a 'one size fits all' approach. Therefore, clinical decisions about choices of moisturiser should be based on the available evidence, and take into account the experiences and preferences of the person with eczema.
Implications for research.
There was substantial variation in the way the included studies were conducted, and in their quality of reporting. Standardisation of outcome reporting, as suggested by the Core Outcome Measures in Effectiveness Trials (COMET) Initiative, would improve the assessment and comparison of relevant outcomes significantly (www.comet-initiative.org). The Harmonising Outcome Measures in Eczema (HOME) initiative has defined and agreed a core set of domains, i.e. symptoms, signs, quality of life and long term control (www.nottingham.ac.uk/homeforeczema/index.aspx), while the Eczema Area and Severity Index (EASI) and the Patient Oriented Eczema Measure (POEM) have been agreed on as the best outcome measures for signs and symptoms, respectively. EASI, the objective SCORAD and POEM are scales recommended for studies (Schmitt 2007; Schmitt 2014). Of the 77 studies in this Cochrane Review, 14 used EASI, 25 used SCORAD (with objective SCORAD used in just four), and two used POEM, so there are clear opportunities for improved uniformity in future studies. The MIDs of SCORAD, objective SCORAD, EASI and POEM that were used in this review were based on the Schram 2012 study. Only the MID of POEM has been investigated in another study (Gaunt 2016), which determined a value of around 3, while we used 3.4 (Schram 2012). The MIDs of (objective) SCORAD and EASI have not been confirmed in other studies yet. As MIDs may vary by population and context (Schram 2012), further research is needed to confirm or adjust MIDs for relevant outcome measures.
In this review we were unable to conclude specifically that some of the moisturisers, or some ingredients in moisturisers, are better than others, as most head to head comparisons had been evaluated in single studies, which generally had small sample sizes. Since moisturisers can contain many different ingredients, more research is needed about their effects, and also about their safety on lesional and non‐lesional skin of people with eczema, including their potential for sensitisation and absorption (Halling‐Overgaard 2016). We were not able to conclude that the use of moisturisers is sufficient to treat (very) mild eczema, which therefore needs future research. In addition, more research is needed on the benefit of moisturisers in the different phases of the disease (i.e. acute, chronic and between flares), including the amounts and frequency of application that give the best results. This should yield information about adequate use of moisturisers and active treatment, and enable prevention of under‐ and over‐treatment with moisturisers or topical active treatments (such as corticosteroids), or both. The paediatric population is of especial importance, since the prevalence of eczema in this group is much higher than in adults, as are the negative consequences of under‐ and over‐treatment. Another area of consideration for further research is the possibility of increasing the efficacy of moisturisers by ensuring adherence through proper and timely information and education, and increasing self‐management skills.
Reporting of adverse events in future research needs to be more complete, with clear explanations of what is considered to be an adverse or unwanted event. Since in (acute) eczema almost everything applied to lesional skin causes transient stinging and erythema (Ring 2012a), thought needs to be given to whether this should be judged as an adverse event, or whether it should be classed as an adverse event only when the stinging and erythema persist over a longer period of time. The reporting of unwanted effects such as smell and stickiness, and difficulty in smearing and spreading, as adverse events hampers proper data collection about adverse events, although this information can be very useful for evaluating the suitability of a moisturiser. Almost half of the studies in this Cochrane Review did not report on adverse events, most probably because moisturisers are not always seen by investigators as treatment, but as more basic 'innocent' maintenance. Clinicians may fail to consider that this 'maintenance' is life long. The acceptability of a substance that smells, is sticky, ruins clothes, leaves traces on furniture and bed linen, and is expensive for people with eczema to purchase in the large quantities required, is an important area to consider. The distinction between these unwanted effects and treatment‐related adverse events is frequently blurred in the published research. Therefore reporting on such unwanted effects in addition to 'real' adverse events is to be recommended. Ideally, both patient satisfaction with the moisturisers and the acceptability of them in daily use should be included in patient‐assessed outcomes of studies.
Future randomised controlled trials should be rigorously designed and conducted, with adequate reporting on methodological aspects as well as complete and transparent reporting according to the Consolidated Standards of Reporting Trials (CONSORT) statement. This will improve critical appraisal and interpretation as well as assessment of the validity of the results.
Feedback
Eczema and Moisturisers, 12 April 2017
Summary
A comment was that while agreeing with their conclusion, in reality it is not that simple. Using the amount of creams and emollient every month that are prescribed would require frequent bathing to get it all off and then renew it. Their skin would not tolerate it, and it would come out in an eczematous rash. Putting on more than can be massaged in results in the layer left on top attracting dust and the skin overheating. Little and often as needed is the key. Also, what suits one person's skin one year, or season, may not the next. Every skin is different, so I hope moisturisers aren't restricted. Some of the cheaper creams such as Aqueous Cream and E45 which contains Lanolin should, in my opinion, not be on the prescription list.
The authors agree with the comments made.
Reply
We are in agreement with the comments made. We have discussed these issues in the Discussion under Overall completeness and applicability of evidence: "The majority of moisturisers considered in this systematic review included a large array of ingredients (see Notes sections in Characteristics of included studies), which made it impossible to distinguish clearly between hydrophilic and hydrophobic moisturisers, or, indeed, between humectant, emollient and occlusive moisturisers. Uncertainty about the exact proportions of these ingredients in a moisturiser does not permit a clear distinction to be made, especially as the proportions are rarely mentioned in the labelling or packaging. The quantity of certain ingredients can also affect the way a moisturiser feels on the skin. Some ingredients in a moisturiser enhance its ability to remain on the skin (e.g. petrolatum), while others (e.g. oils) transfer quickly to clothes or bed linen. Temperature can influence the viscosity of moisturisers, which is crucially important for application on the skin, as the higher the viscosity of the moisturiser, the more difficult it is to smear and spread on the skin, which can cause friction and lead to friction‐related adverse events. Once all of these aspects are taken into account, as well as dryness, day or night‐time, the seasons, the weather, and even the clothes that are worn, people with eczema will express a variety of preferences in different situations. The ideal moisturiser should be easy to spread on the skin, have no smell, contain no irritating or sensitising ingredients, be cosmetically acceptable without excessive sticking to clothes and bed linen, and be affordable for people with eczema.
This review does not address the importance of educating people with eczema on how to apply moisturisers, how much to use or how often to use them. Cork and colleagues demonstrated that correct and adequate instructions in usage "of the treatments resulted in an 800% increase in the use of emollients, a reduction in disease severity as assessed with six area, six sign atopic dermatitis severity score (SASSAD) (89% reduction compared with baseline) and no overall increase in the use of topical steroids" (Cork 2003a). The importance of education as part of the management strategy has also been emphasised by several other investigators (Arkwright 2013; Ersser 2014; Mason 2013; Oakley 2016). Another shortcoming of the studies in this review was the lack of detailed reporting of adverse events, which meant that we could not conclude which moisturiser might be preferable for avoiding adverse events. None of the studies reported aspects such as the smell, stickiness or greasiness of the moisturiser, but rather adverse effects such as pruritus, stinging, smarting or increase in erythema. We are still unable to confirm how often moisturisers need to be applied, although it is more generally acknowledged that this should be at least once a day and preferably more frequently. Current recommended quantities of moisturisers range from 250 g to 500 g per week (Moncrieff 2013; NICE 2007; Wollenberg 2016)."
We have also discussed these issues under Implications for practice: "This review does not inform us about the importance of education in how to apply moisturisers, in particular how often they need to be applied and how much to use. However, since moisturisers reduce flares, prolong the time to flare, decrease the necessity for topical corticosteroids and increase the efficacy of active treatment, it makes clinical sense to encourage adherence to moisturiser therapy. This is especially important as moisturiser therapy is time consuming and often required throughout life, as eczema is a chronic condition.
This review provides no information about which moisturisers might be preferred for different parts of the body, or preferred during different seasons or personal circumstances, or which moisturisers best fit the actual disease status (acute or chronic) or severity (mild, moderate or severe). There is no evidence to support a 'one size fits all' approach. Therefore, clinical decisions about choices of moisturiser should be based on the available evidence, and take into account the experiences and preferences of the person with eczema."
The ingredient in the Aequous cream is sodium lauryl sulphate, which is mentioned under Agreements and disagreements with other studies or reviews.
Contributors
Our Co‐ordinating Editor Hywel Williams, our Feedback Editor Urbà González and the lead author Esther van Zuuren in discussion with co‐authors.
What's new
| Date | Event | Description |
|---|---|---|
| 29 July 2020 | Amended | A minor typographical error was amended. |
History
Protocol first published: Issue 3, 2016 Review first published: Issue 2, 2017
| Date | Event | Description |
|---|---|---|
| 16 August 2017 | Amended | Further copy‐editing amendments. |
| 10 May 2017 | Feedback has been incorporated | Authors responded to feedback referring to the text of the review. Please see Feedback section for details. |
Acknowledgements
We would like to thank Masaki Futamura from the Department of Pediatrics Nagoya Medical Center, Nagoya Japan for his translation of Hamada 2008 from Japanese into English.
We thank Kyung‐Hwa Seo, Senior Researcher, Research Institute for Healthcare Policy of Korean Medical Association, and Doctorate student, Department of Medical Sciences, Ewha Woman's University, Seoul, South Korea, for his translation of Noh 2011 from Korean into English.
We would like to thank Professor Ching‐Chi Chi from the Department of Dermatology & Centre for Evidence Based Medicine, Ms Yu‐Shiun Tsai, Department of Medical Education, and Dr Yu‐Jung Chen, Department of Traditional Chinese Medicine all from Chang Gung Memorial Hospital, Chiayi, Taiwan for the translation of Wu 2014; Yang 2010 from Chinese into English.
We would like to thank all principal investigators as well as pharmaceutical companies who were so helpful in addressing our questions and clarifying missing study details (see Table 11).
The editorial base of the Cochrane Skin Group wish to thank Hywel Williams, the Cochrane Dermatology Editor for this review; Thomas Chu, the statistical editor; Ching‐Chi Chi, the methods editor; the clinical referees, Sandra Lawton and Miriam Santer; and the consumer referee, Amanda Roberts, as well as Megan Prictor, who copy‐edited the protocol for the review, and Elizabeth Royle who copy‐edited the review.
Appendices
Appendix 1. Cochrane Skin Specialised Register (CRS) search strategy
(dermatitis or eczema or neurodermatitis) and (emollient* or moisturis* or moisturiz* or lubricant* or ointment* or cream* or oil* or bath* or steroid* or corticosteroid*)
Appendix 2. CENTRAL (Cochrane Library) search strategy
#1 MeSH descriptor: [Dermatitis] explode all trees #2 dermatitis:ti,ab,kw #3 MeSH descriptor: [Eczema] explode all trees #4 eczema:ti,ab,kw #5 MeSH descriptor: [Neurodermatitis] explode all trees #6 neurodermatitis:ti,ab,kw #7 MeSH descriptor: [Dermatitis, Atopic] explode all trees #8 {or #1‐#7} #9 MeSH descriptor: [Emollients] explode all trees #10 emollient*:ti,ab,kw #11 (moisturis* or moisturiz*):ti,ab,kw #12 MeSH descriptor: [Lubricants] explode all trees #13 lubricant*:ti,ab,kw #14 MeSH descriptor: [Ointments] explode all trees #15 ointment*:ti,ab,kw #16 cream*:ti,ab,kw #17 MeSH descriptor: [Skin Cream] explode all trees #18 MeSH descriptor: [Oils] explode all trees #19 oil*:ti,ab,kw #20 bath*:ti,ab,kw #21 MeSH descriptor: [Baths] explode all trees #22 corticosteroid*:ti,ab,kw #23 steroid*:ti,ab,kw #24 MeSH descriptor: [Steroids] explode all trees #25 {or #9‐#24} #26 #8 and #25
Appendix 3. MEDLINE (Ovid) search strategy
1. exp Dermatitis/ 2. dermatitis.ti,ab. 3. exp Eczema/ 4. eczema.ti,ab. 5. exp Neurodermatitis/ 6. neurodermatitis.ti,ab. 7. exp Dermatitis, Atopic/ 8. or/1‐7 9. emollient$.ti,ab. or exp Emollients/ 10. moisturis$.ti,ab. 11. moisturiz$.ti,ab. 12. lubricant$.ti,ab. or exp Lubricants/ 13. ointment$.ti,ab. or exp Ointments/ 14. cream$.ti,ab. 15. exp Skin Cream/ 16. exp Oils/ or oil$.ti,ab. 17. bath$3.ti,ab. or exp Baths/ 18. corticosteroid$.ti,ab. 19. exp Steroids/ or steroid$.ti,ab. 20. or/9‐19 21. randomized controlled trial.pt. 22. controlled clinical trial.pt. 23. randomized.ab. 24. placebo.ab. 25. clinical trials as topic.sh. 26. randomly.ab. 27. trial.ti. 28. 21 or 22 or 23 or 24 or 25 or 26 or 27 29. exp animals/ not humans.sh. 30. 28 not 29 31. 8 and 20 and 30
[Lines 21‐30: Cochrane Highly Sensitive Search Strategy for identifying randomized trials in MEDLINE: sensitivity‐ and precision‐maximizing version (2008 revision)]
Appendix 4. Embase (Ovid) search strategy
1. exp ECZEMA/ 2. eczema.ti,ab. 3. exp DERMATITIS/ 4. dermatitis.ti,ab. 5. exp atopic dermatitis/ 6. exp NEURODERMATITIS/ 7. neurodermatitis.ti,ab. 8. or/1‐7 9. exp emollient agent/ 10. emollient$.ti,ab. 11. (moisturis$ or moisturiz$).ti,ab. 12. exp lubricating agent/ 13. lubricant$.ti,ab. 14. exp ointment/ 15. ointment$.ti,ab. 16. cream$.ti,ab. 17. exp skin cream/ 18. oil$1.ti,ab. 19. exp bath/ 20. bath$3.ti,ab. 21. exp corticosteroid/ 22. corticosteroid$.ti,ab. 23. exp steroid/ 24. steroid$.ti,ab. 25. or/9‐24 26. crossover procedure.sh. 27. double‐blind procedure.sh. 28. single‐blind procedure.sh. 29. (crossover$ or cross over$).tw. 30. placebo$.tw. 31. (doubl$ adj blind$).tw. 32. allocat$.tw. 33. trial.ti. 34. randomized controlled trial.sh. 35. random$.tw. 36. or/26‐35 37. exp animal/ or exp invertebrate/ or animal experiment/ or animal model/ or animal tissue/ or animal cell/ or nonhuman/ 38. human/ or normal human/ 39. 37 and 38 40. 37 not 39 41. 36 not 40 42. 8 and 25 and 41
Appendix 5. LILACS search strategy
(dermatitis or eczema or eccema or neurodermatitis or neurodermitis) and (emollient$ or moisturis$ or moisturiz$ or oil$ or bath$ or cream$ or lubricant$ or steroid$ or corticosteroid$ or emoliente$ or crema$ or esteroide$ or corticoesteroide$ or ointment$) We searched using the Controlled clinical trials topic‐specific query filter and the above terms.
Appendix 6. GREAT search strategy
emollient* or oil* or ointment* or lubricant* or cream* or bath* or moisturis* or moisturiz* or corticosteroid* or steroid* These terms combined with 'all intervention fields'.
This search was limited to intervention fields only.
Data and analyses
Comparison 1. Moisturisers versus no treatment (i.e. no moisturiser).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1.1 Change from baseline in SCORAD | 3 | 276 | Mean Difference (IV, Random, 95% CI) | ‐2.42 [‐4.55, ‐0.28] |
| 1.2 Number of participants experiencing a flare | 2 | 87 | Risk Ratio (M‐H, Random, 95% CI) | 0.40 [0.23, 0.70] |
| 1.3 Rate of flare | 2 | 87 | Hazard Ratio (IV, Random, 95% CI) | 3.74 [1.86, 7.50] |
| 1.4 Amount of topical steroids used | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.4.1 Amount of topical corticosteroids first 3‐4 weeks | 2 | 222 | Mean Difference (IV, Random, 95% CI) | ‐8.25 [‐17.22, 0.72] |
| 1.4.2 Amount of topical corticosteroids used last 3‐4 weeks | 1 | 74 | Mean Difference (IV, Random, 95% CI) | 0.50 [‐4.70, 5.70] |
| 1.4.3 Total amount of topical corticosteroids used in 6 to 8 weeks | 2 | 222 | Mean Difference (IV, Random, 95% CI) | ‐9.30 [‐15.33, ‐3.27] |
| 1.5 Change from baseline in quality of life | 2 | 177 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.15 [‐0.55, 0.24] |
Comparison 2. Atopiclair versus vehicle.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 2.1 Number of participants who experienced good improvement to total resolution | 3 | 390 | Risk Ratio (M‐H, Random, 95% CI) | 4.51 [2.19, 9.29] |
| 2.1.1 Number of participants who experienced good improvement to total resolution (low risk of bias) | 1 | 30 | Risk Ratio (M‐H, Random, 95% CI) | 4.00 [1.01, 15.81] |
| 2.1.2 Number of participants who experienced good improvement to total resolution (unclear risk of bias) | 1 | 142 | Risk Ratio (M‐H, Random, 95% CI) | 8.06 [3.95, 16.42] |
| 2.1.3 Number of participants who experienced good improvement to total resolution (high risk of bias) | 1 | 218 | Risk Ratio (M‐H, Random, 95% CI) | 3.02 [2.00, 4.56] |
| 2.2 Change from baseline in itch measured on a VAS | 4 | 396 | Mean Difference (IV, Random, 95% CI) | ‐2.65 [‐4.21, ‐1.09] |
| 2.2.1 Change from baseline in itch measured on a VAS (low risk of bias) | 1 | 30 | Mean Difference (IV, Random, 95% CI) | ‐0.80 [‐1.20, ‐0.40] |
| 2.2.2 Change from baseline in itch measured on a VAS (unclear risk of bias) | 2 | 180 | Mean Difference (IV, Random, 95% CI) | ‐3.10 [‐4.47, ‐1.73] |
| 2.2.3 Change from baseline in itch measured on a VAS (high risk of bias) | 1 | 186 | Mean Difference (IV, Random, 95% CI) | ‐3.70 [‐4.66, ‐2.74] |
| 2.3 Number of participants reporting an adverse event | 4 | 430 | Risk Ratio (M‐H, Random, 95% CI) | 1.03 [0.79, 1.33] |
| 2.4 Change from baseline in EASI | 4 | 426 | Mean Difference (IV, Random, 95% CI) | ‐4.00 [‐5.42, ‐2.57] |
| 2.4.1 Change from baseline in EASI (low risk of bias) | 1 | 30 | Mean Difference (IV, Random, 95% CI) | ‐3.30 [‐5.67, ‐0.93] |
| 2.4.2 Change from baseline in EASI (unclear risk of bias) | 2 | 180 | Mean Difference (IV, Random, 95% CI) | ‐4.42 [‐7.73, ‐1.10] |
| 2.4.3 Change from baseline in EASI (high risk of bias) | 1 | 216 | Mean Difference (IV, Random, 95% CI) | ‐3.62 [‐5.06, ‐2.18] |
| 2.5 Number of participants experiencing a flare | 3 | 397 | Risk Ratio (M‐H, Random, 95% CI) | 0.18 [0.11, 0.31] |
| 2.5.1 Number of participants experiencing a flare (unclear risk of bias) | 2 | 181 | Risk Ratio (M‐H, Random, 95% CI) | 0.26 [0.12, 0.57] |
| 2.5.2 Number of participants experiencing a flare (high risk of bias) | 1 | 216 | Risk Ratio (M‐H, Random, 95% CI) | 0.14 [0.07, 0.28] |
Comparison 3. Urea‐containing moisturiser versus vehicle.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 3.1 Change from baseline in skin capacitance | 2 | Mean Difference (IV, Random, 95% CI) | 1.23 [‐7.39, 9.86] |
Comparison 4. Glycerin cream versus placebo cream.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 4.1 Number of participants reporting an adverse event | 2 | 385 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.68, 1.19] |
Comparison 5. Oat‐containing cream versus vehicle or no treatment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 5.1 Change in disease severity as assessed by the investigators (SCORAD and EASI) | 3 | 272 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.23 [‐0.66, 0.21] |
| 5.1.1 Change in disease severity as assessed by the investigator (EASI) (low risk of bias) | 1 | 50 | Std. Mean Difference (IV, Random, 95% CI) | 0.01 [‐0.55, 0.56] |
| 5.1.2 Change in disease severity as assessed by the investigators (SCORAD) (high risk of bias) | 2 | 222 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.33 [‐0.98, 0.32] |
| 5.2 Change from baseline in quality of life | 3 | 226 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.09 [‐0.37, 0.19] |
| 5.2.1 Change from baseline in quality of life (low risk of bias) | 1 | 50 | Std. Mean Difference (IV, Random, 95% CI) | 0.10 [‐0.46, 0.65] |
| 5.2.2 Change from baseline in quality of life (high risk of bias) | 2 | 176 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.16 [‐0.55, 0.24] |
Comparison 6. All moisturisers versus vehicle, placebo or no treatment (no moisturiser).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 6.1 Number of participants who experienced improvement | 5 | 572 | Risk Ratio (M‐H, Random, 95% CI) | 2.46 [1.16, 5.23] |
| 6.1.1 Number of participants who experienced improvement (low risk of bias) | 2 | 80 | Risk Ratio (M‐H, Random, 95% CI) | 1.86 [0.41, 8.31] |
| 6.1.2 Number of participants who experienced improvement (unclear risk of bias) | 2 | 274 | Risk Ratio (M‐H, Random, 95% CI) | 3.11 [0.25, 38.71] |
| 6.1.3 Number of participants who experienced improvement (high risk of bias) | 1 | 218 | Risk Ratio (M‐H, Random, 95% CI) | 3.02 [2.00, 4.56] |
| 6.2 Change from baseline in itch | 7 | 749 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.10 [‐1.83, ‐0.38] |
| 6.2.1 Change from baseline in itch (low risk of bias) | 3 | 329 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.36 [‐1.16, 0.43] |
| 6.2.2 Change from baseline in itch (unclear risk of bias) | 2 | 180 | Std. Mean Difference (IV, Random, 95% CI) | ‐2.29 [‐2.67, ‐1.91] |
| 6.2.3 Change from baseline in itch (high risk of bias) | 2 | 240 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.95 [‐1.75, ‐0.16] |
| 6.3 Number of participants who expressed treatment satisfaction | 3 | 298 | Risk Ratio (M‐H, Random, 95% CI) | 1.35 [0.77, 2.36] |
| 6.3.1 Number of participants who expressed treatment satisfaction (low risk of bias) | 2 | 80 | Risk Ratio (M‐H, Random, 95% CI) | 1.04 [0.77, 1.42] |
| 6.3.2 Number of participants who expressed treatment satisfaction (high risk of bias) | 1 | 218 | Risk Ratio (M‐H, Random, 95% CI) | 2.14 [1.58, 2.89] |
| 6.4 Number of participants reporting an adverse event | 10 | 1275 | Risk Ratio (M‐H, Random, 95% CI) | 1.03 [0.82, 1.30] |
| 6.4.1 Number of participants reporting an adverse event (low risk of bias) | 4 | 471 | Risk Ratio (M‐H, Random, 95% CI) | 0.83 [0.58, 1.18] |
| 6.4.2 Number of participants reporting an adverse events (unclear risk of bias) | 3 | 314 | Risk Ratio (M‐H, Random, 95% CI) | 1.08 [0.82, 1.42] |
| 6.4.3 Number of participants reporting an adverse events (high risk of bias) | 3 | 490 | Risk Ratio (M‐H, Random, 95% CI) | 1.35 [0.37, 4.96] |
| 6.5 Change in disease severity as assessed by the investigators | 12 | 1281 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.65 [‐0.89, ‐0.41] |
| 6.5.1 Change in disease severity as assessed by the investigators (low risk of bias) | 5 | 512 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.45 [‐0.74, ‐0.15] |
| 6.5.2 Change in disease severity as assessed by the investigators (unclear risk of bias) | 2 | 180 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.93 [‐1.29, ‐0.57] |
| 6.5.3 Change in disease severity as assessed by the investigators (high risk of bias) | 5 | 589 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.77 [‐1.23, ‐0.30] |
| 6.6 Number of participants experiencing a flare | 6 | 607 | Risk Ratio (M‐H, Random, 95% CI) | 0.33 [0.17, 0.62] |
| 6.6.1 Number of participants experiencing a flare (low risk of bias) | 1 | 123 | Risk Ratio (M‐H, Random, 95% CI) | 0.80 [0.48, 1.34] |
| 6.6.2 Number of participants experiencing a flare (unclear risk of bias) | 2 | 181 | Risk Ratio (M‐H, Random, 95% CI) | 0.26 [0.12, 0.57] |
| 6.6.3 Number of participants experiencing a flare (high risk of bias) | 3 | 303 | Risk Ratio (M‐H, Random, 95% CI) | 0.27 [0.12, 0.59] |
| 6.7 Change from baseline in quality of life | 3 | 300 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.39 [‐0.90, 0.12] |
| 6.7.1 Change from baseline in quality of life (low risk of bias) | 1 | 123 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.81 [‐1.18, ‐0.44] |
| 6.7.2 Change from baseline in quality of life (high risk of bias) | 2 | 177 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.15 [‐0.55, 0.24] |
Comparison 7. Evening primrose oil versus placebo oil.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 7.1 Change from baseline in TEWL | 1 | Mean Difference (IV, Random, 95% CI) | ‐0.34 [‐1.44, 0.76] | |
| 7.2 Change from baseline in skin hydration | 1 | Mean Difference (IV, Random, 95% CI) | 0.34 [‐2.54, 3.21] |
Comparison 8. Licochalcone versus hydrocortisone acetate (HCA) 1%.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 8.1 Change from baseline in itch (VAS) | 2 | Mean Difference (IV, Random, 95% CI) | ‐0.48 [‐1.46, 0.50] | |
| 8.1.1 Change from baseline in itch (VAS) (unclear risk of bias) | 1 | Mean Difference (IV, Random, 95% CI) | 0.00 [‐0.47, 0.47] | |
| 8.1.2 Change from baseline in itch (VAS) (high risk of bias) | 1 | Mean Difference (IV, Random, 95% CI) | ‐1.00 [‐1.61, ‐0.39] | |
| 8.2 Change from baseline in SCORAD | 3 | Mean Difference (IV, Random, 95% CI) | 0.08 [‐1.96, 2.13] | |
| 8.2.1 Change from baseline in SCORAD (unclear risk of bias) | 1 | Mean Difference (IV, Random, 95% CI) | ‐2.00 [‐3.47, ‐0.53] | |
| 8.2.2 Change from baseline in SCORAD (high risk of bias) | 2 | Mean Difference (IV, Random, 95% CI) | 1.12 [‐1.38, 3.61] | |
| 8.3 Change from baseline in TEWL | 2 | Mean Difference (IV, Random, 95% CI) | ‐0.50 [‐5.88, 4.87] | |
| 8.3.1 Change from baseline in TEWL (unclear risk of bias) | 1 | Mean Difference (IV, Random, 95% CI) | ‐3.00 [‐4.71, ‐1.29] | |
| 8.3.2 Change from baseline in TEWL (high risk of bias) | 1 | Mean Difference (IV, Random, 95% CI) | 2.51 [‐1.21, 6.23] |
Comparison 9. Advabase versus MPA cream twice weekly and emollient.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 9.1 Rate of flare | 1 | Hazard Ratio (IV, Random, 95% CI) | Totals not selected |
Comparison 10. Vehicle + daily moisturiser versus fluticasone propionate (FP) + daily moisturiser.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 10.1 Number of participants reporting an adverse event | 3 | 718 | Risk Ratio (M‐H, Random, 95% CI) | 0.51 [0.22, 1.14] |
| 10.2 Number of participants experiencing a flare | 3 | 718 | Risk Ratio (M‐H, Random, 95% CI) | 2.17 [1.51, 3.11] |
| 10.3 Rate of flare | 3 | 723 | Hazard Ratio (IV, Random, 95% CI) | 3.69 [1.80, 7.55] |
Comparison 11. Active treatment in combination with a moisturiser versus active treatment only.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 11.1 Change in disease severity as assessed by the investigators | 2 | 192 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.87 [‐1.17, ‐0.57] |
| 11.2 Change in quality of life IDQOL | 1 | 67 | Mean Difference (IV, Random, 95% CI) | ‐1.31 [‐2.70, 0.09] |
| 11.3 Change in quality of life DFI | 1 | 67 | Mean Difference (IV, Random, 95% CI) | ‐1.03 [‐2.47, 0.42] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Abramovits 2008.
| Study characteristics | ||
| Methods | Randomised, double‐blind, vehicle‐controlled study Setting Multicentre (10) in USA Date of study Unspecified. Duration of intervention: 50 days |
|
| Participants | N = 218 (127 female, 91 male) Mean age = 44.5 years (18 to 84 years) Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 218 (MAS063DP group = 145, vehicle group = 73) Withdrawals/losses to follow‐up 32 overall (14.6%); MAS063DP group = 16/145 (11%), vehicle group = 16/73 (21.9%)
Baseline data Duration of the current episode of atopic dermatitis ranging from 5 days to 58 years. The most common atopic dermatitis pattern was constant or frequent (80% of participants) and with no seasonal course (66%) Mean EASI: MAS063DP group 5.76 (SD 4.68), vehicle group 6.03 (SD 6.62) Mean itch (VAS): MAS063DP group 7.51 (SD 1.6), vehicle group 7.05 (SD 1.62) |
|
| Interventions |
Intervention
Comparator
Topical corticosteroids, immunomodulators, antihistamines, non‐steroidal anti‐inflammatory drugs and phototherapy were excluded during a washout period prior to treatment initiation and during the study. |
|
| Outcomes | Assessments (5): at baseline, days 8, 22, 36, and 50 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared. However, the product under research is produced by Sinclair Pharma Ltd, Godalming, UK | |
| Declaration of interest | Almost all investigators were investigators or consultants (or both) of Sinclair Pharma Ltd, as well as of Graceway Pharmaceuticals, LCC and received compensations | |
| Notes | MAS063DP (Atopiclair, Sinclair Pharma Ltd, Godalming, UK) contains glycyrrhetinic acid, which is believed to contribute to the cream's antipruritic and anti‐inflammatory properties. It inhibits the enzyme 11β‐hydroxysteroid dehydrogenase (11β‐HSD), responsible for the metabolism of cortisol into cortisone. Glycyrrhetinic acid, has a chemical structure related to cortisone and has been shown to potentiate the action of hydrocortisone on skin. Further ingredients include: aqua, ethylhexyl palmitate, Vitellaria paradoxa (formerly called Butyrospermum parkii), pentylene glycol, arachidyl alcohol, behenyl alcohol, arachidyl glucoside, glyceryl stearate, PEG‐100 stearate, butylene glycol, glycyrrhetinic acid, capryloyl glycine, bisabolol, tocopher acetate, carbomer, ethylhexylglycerin, piroctone olamine, sodium hydroxide, allantoin, DMDM hydantoin, Vitis vinifera, sodium hyaluronate, disodium EDTA, ascorbyl tetraisopalmitate, propyl gallate, telmesteine We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 328) and (page 237 of 2006 publication): "Patients were randomized (2:1)" "Patients were assigned a study number according to their entry into the study and following a computer generated randomization code". Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: central allocation via pharmaceutical company, sequentially numbered tubes of identical appearance. Comment: central allocation, de‐identified tubes. Allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 327): "double‐blind..." Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. After email communication: "tubes of drug or placebo/vehicle looking identical" Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page 327): "double‐blind..." Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty with regard to the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. After email communication: "tubes of drug or placebo/vehicle looking identical" Blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 32 (14.6%) overall, MAS063DP (Atopiclair) group = 16/145 (11%), vehicle group = 16/73 (21.9%). Per‐protocol analysis. Comment: the total number of dropouts was unbalanced between the groups, which, combined with a per‐protocol analysis represents a high risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appears to be free from other forms of bias. |
Andersson 1999.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐controlled study Setting Department of Medical Sciences, University Hospital, Uppsala, and ACO Hud AB, Stockholm, Sweden Date of study February to April, not clear which year. Duration of intervention: 30 days |
|
| Participants | N = 50 (38 female, 12 male) Age = 18 to 55 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 50 (5% urea (Canoderm) group = 25, 4% urea (Fenuril) group = 25) Withdrawals/losses to follow‐up 2/50 (4%)
Baseline data Not reported |
|
| Interventions |
Intervention
Comparator
Allowed to continue use of topical corticosteroids |
|
| Outcomes | Assessments (3): baseline, days 15 and 31 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared, however, 1 of the products under research is produced by ACO Hud AB, Sweden | |
| Declaration of interest | None declared. Dr Lodén was an employee of ACO Hud AB, the manufacturer of the principal intervention | |
| Notes | Fenuril (Pharmacia AB, Sweden) contained 4% urea and 4% NaCl as water‐binding substances in an oil‐in‐water emulsion, pH about 5. Other ingredients were liquid paraffin, PEG‐ 5‐glyceryl stearate, cetyl alcohol, stearyl alcohol, stearic acid, trometamol, methyl para‐hydroxybenzoate, propyl para‐hydroxybenzoate, hydrochloric acid and water
Canoderm (ACO Hud AB, Sweden) contained 5% urea in an oil‐in‐water emulsion, pH about 5. Other ingredients were fractionated coconut oil, cetearyl alcohol, PEG‐20 stearate, hydrogenated canola oil, propylene glycol, carbomer, methicone, hard paraffin, glyceryl poly‐methacrylate, propylparaben, methylparaben, sodium lactate, lactic acid, glyceryl stearate, polyoxyethylene stearate, cetyl acetate, oleyl acetate, acetylated lanolin alcohols and water As the study was 17 years old we did not contact the investigators for data. The data all needed to be estimated from box‐and whisker plots, which made them difficult to use (Table 13). The adverse events were addressed in a separate publication (Lodén 1999 added in 'References to studies' under the primary publication Andersson 1999) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 165): "randomized double‐blind study" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 165): "double‐blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 165): "double‐blind" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty with the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2/50 (4%) withdrew for "reasons not related to treatment" in Fenuril group. Per‐protocol analysis. Comment: low number of losses to follow‐up, and despite use of per‐protocol analysis, considered to be at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Angelova‐Fischer 2014.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, active‐controlled, within‐participant study Setting Department of Dermatology, University of Lübeck, Lübeck, Germany Date of study Unspecified. Duration of intervention: 1 week, followed by 3 weeks' treatment with 'moisturiser only' |
|
| Participants | N = 20 (16 female, 4 male) Age = 12 to 65 years, median age = 26.2 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 20, to either forearm (within‐participant) Withdrawals/losses to follow‐up 2/20 (10%)
Baseline data Mean local SCORAD: O/W formulation group 7.0, hydrocortisone group 6.5 Mean itch severity (VAS): O/W formulation group 3.5, hydrocortisone group 3.75 Mean TEWL (g/m²/h): O/W formulation group 16.47, hydrocortisone group 16.28 |
|
| Interventions |
Intervention
Comparator
After 1 week both arms were treated with the O/W (oil in water) formulation and no other treatment |
|
| Outcomes | Assessments (3): baseline, days 7 and 28 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 9): "The study was funded by Beiersdorf AG" | |
| Declaration of interest | Quote (page 9): "I, Angelova‐Fischer has been investigator for and received honoraria as a speaker from Beiersdorf AG" [sic] | |
| Notes | Licochalcone A is an extract from Glycyrrhiza inflata that has anti‐inflammatory properties. After 1 week both arms were treated with a moisturiser, therefore we have only included data from the first week We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 10): "were randomized to receive" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "random number table" Comment: probably done. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: this remains unclear. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 10): "investigator‐blinded" Comment: the report did not provide sufficient detail about the specific measures used to blind study personnel from knowledge of which intervention a participant received on each forearm, to permit a clear judgement, and participants were not blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote (page 10): "investigator‐blinded". Outcomes were investigator‐assessed as well as participant‐assessed. Comment: there was uncertainty about the effectiveness of blinding of outcomes assessors (healthcare providers) during the study, and participants were not blinded. The outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2/20 (10%), 2 excluded in the second and fourth study weeks because of worsening of the skin condition outside the test area that required topical treatment. Comment: as we only included data from the first week we judged this as being at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free from other forms of bias. |
Belloni 2005.
| Study characteristics | ||
| Methods | Randomised, double‐blind, vehicle‐controlled study Setting European Institute of Dermatology, Milan, Italy Date of study Unspecified. Duration of intervention: 22 days, with follow‐up of 2 weeks |
|
| Participants | N = 30 (14 female, 16 male) Age = 13 to 43 years, median age = 22.5 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 30 (MAS063D group = 15, vehicle group = 15) Withdrawals/losses to follow‐up All participants finished the study protocol Baseline data Eczema severity and location of the lesions, disease duration and current episode were comparable |
|
| Interventions |
Intervention
Comparator
Participants receiving systemic medication (antihistamines, corticosteroids, NSAIDs, or other topical and systemic investigational drugs) were maintained on their medications at a constant dose throughout the study. Participants receiving topical medications (e.g. topical antihistamines, corticosteroids, NSAIDs) were taken off the medication in a washout period of 7 days, so that no participants were using these medications 7 days before the study or during it. Washout period for phototherapy and tranquillisers was 4 weeks and 5 days respectively. |
|
| Outcomes | Assessments (5): baseline, days 8, 15, 22 and 36 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 35): "The study was supported by a grant from Sinclair Pharmaceuticals, Godalming, Surrey, UK" | |
| Declaration of interest | None declared | |
| Notes | Participants receiving topical medications (e.g. topical antihistamines, corticosteroids, NSAIDs) were taken off the medication in a washout period. See in Notes section of Characteristics of included studies of Abramovits 2008 for details on Atopiclair | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 32): "Randomisation was carried out in blocks of six patients using a random number generator in Microsoft Excel". Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | Quote (page 32): "Patients were randomised to receive MAS063D or vehicle‐only control, according to their order of entry into the study. MAS063D and control were presented in identical, blindly, pre‐labelled containers. Each container was labelled with patient's study number and patients, observers and all trial personnel were blinded to study code". Comment: central allocation, de‐identified drug containers. Allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 32): "The jars containing MAS063D or control were presented blindly, labelled with identical directions for use..." Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page 32): "The jars containing MAS063D or control were presented blindly, labelled with identical directions for use..." Outcomes were investigator‐assessed as well as participant‐assessed. Blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Berents 2015.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, controlled, within‐participant study Setting Multicentre (3), baby clinics in Oslo, Norway Date of study 2008 to 2011; duration of intervention: 4 weeks |
|
| Participants | N = 9 (6 female, 3 male) Mean age = 18.5 months Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 9, however contralateral eczema spots were randomised (18 spots left/right) (within‐participant) Withdrawals/losses to follow‐up 3/9 participants (33.3%)
Baseline data Mean SCORAD: 35 (range 22‐45) |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (5): baseline, weeks 1, 2, 3 and 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | Quote (page 6): "The authors declare that they have no competing interests" | |
| Notes | None of our outcomes were addressed (Table 13). Apobase creme contains: aqua, paraffinum liquidum, petrolatum, cetearyl alcohol, ceteareth‐20, ceteareth‐12, sodium gluconate, caprylyl glycol, phenoxyethanol, and has a total lipid content of 30% We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (pages 2‐3): "Another physician, who did not see the child, was responsible for the randomization". Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: " Physician 1 prepared 12 letters, 6 right and 6 left, with treatment information. These were then folded, so the information was hidden. Thereafter one and one was randomly drawn and included into envelopes numbered 1‐12. Finally these envelopes were sealed. This procedure was performed physically outside the clinical department where physician 2 works. Physician 1 was the only one with access to the randomization code." Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | Quote (page 3): "The child was given a randomization number and the mothers were then informed on which side to apply the fresh expressed human milk and emollient, and on which side to apply emollient alone".
The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "Physician 2 received one sealed, numbered envelope, for each new included patient, from physician 1". Comment: allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 2): "physician‐blinded" Comment: The report did not provide sufficient detail about the specific measures used to blind study personnel from knowledge of which intervention a participant received, to permit a clear judgement. After email communication: "Physician 2 delivered the sealed envelope with the correct patient number, to the mother. The mother opened the sealed envelope outside the sight of physician 2. If she had any questions she could talk to physician 1 by telephone, without physician 2 listening. This happened once". Comment: the report provided sufficient detail about the measures used to blind study personnel from knowledge of which intervention a participant received. However, participants were not blinded and so we judged this study as being at an unclear risk of bias. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcomes were investigator‐assessed. Blinding of the outcomes assessors was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 3/9 (33.3%). Per‐protocol analysis. Comment: high number of losses to follow‐up, combined with per‐protocol analysis meant we considered this study to be at a high risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was available (NCT02381028), and the prespecified outcomes and those mentioned in the methods section appear to have been reported. |
| Other bias | Low risk | Comment: the study appears to be free from other forms of bias. |
Berth‐Jones 2003.
| Study characteristics | ||
| Methods | Randomised, double‐blind, active‐controlled study Setting Multicentre (39), 6 countries in Europe Date of study Recruitment January 1998 to July 1999. Duration of intervention: 4 weeks for stabilisation phase, and 16 weeks maintenance phase. We only included the data from the maintenance phase. |
|
| Participants | N = 376 (205 female, 171 male) Mean age = 28.8 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 376 (fluticasone cream once daily group = 95, fluticasone cream twice daily group = 91, fluticasone ointment once daily group = 100, fluticasone ointment twice daily group = 90) Withdrawals/losses to follow‐up Stabilisation phase: 83/376 overall (22%); fluticasone cream once daily group = 19/95, fluticasone cream twice daily group = 15/91, fluticasone ointment once daily group = 23/100, fluticasone ointment twice daily group = 26/90, reasons reported (2/83, however, entered into the maintenance phase) Maintenance phase:
Baseline data Mean extent of atopic dermatitis (%): fluticasone cream once daily group 28.8% (SD 19), fluticasone cream twice daily group 17.7% (SD 16.2), fluticasone ointment once daily group 17.5% (SD 14.6), fluticasone ointment twice daily group 18.4% (SD 16.1) Median TIS score: fluticasone cream once daily group 5.0 (range 4‐6), fluticasone cream twice daily group 5.0 (range 4‐9), fluticasone ointment once daily group 5.0 (range 4‐7), fluticasone ointment twice daily group 5.0 (range 4‐7) |
|
| Interventions | Initially the flare was stabilised with fluticasone propionate cream 0.05% or fluticasone propionate ointment 0.005%, once or twice daily, for 4 weeks. After that the maintenance phase continued as follows: Intervention
Comparator 1
Intervention 2
Comparator 2
|
|
| Outcomes | Assessments (7): baseline, weeks 2 and 4 (end of stabilisation phase), weeks 2, 6, 10 and 16 (end maintenance phase) Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 6): "Funding: Glaxo Wellcome (now GlaxoSmithKline) R & D, United Kingdom" | |
| Declaration of interest | Quote (page 6): "Competing interests: CP is employed full time by GlaxoSmith‐Kline" | |
| Notes | The moisturiser was a cetomacrogol‐based cream We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 2): "Investigators at each centre allocated patients to treatment groups in equal numbers according to a computer generated randomisation code. The block size for the study was eight, and each recruiting centre received 16 treatment allocation numbers". Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | Quote (page 2): "Investigators at each centre allocated patients to treatment groups in equal numbers according to a computer generated randomisation code. The block size for the study was eight, and each recruiting centre received 16 treatment allocation numbers". Comment: form of central allocation, probably done. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 1 and 2): "double‐blind" and "Patients who achieved remission (see assessments) then entered a maintenance phase and, using the same formulation as in the stabilisation phase, applied fluticasone propionate or its placebo base on two successive evenings per week for up to 16 weeks". Comment: the report did not provide sufficient detail about the specific measures, used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. After email communication: "blinding was achieved using matching tubes containing either active medication or vehicle alone". Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page 1 and 2): "double‐blind" and "Patients who achieved remission (see assessments) then entered a maintenance phase and, using the same formulation as in the stabilisation phase, applied fluticasone propionate or its placebo base on two successive evenings per week for up to 16 weeks". Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study, insufficient information to permit a clear judgement. After email communication: "blinding was achieved using matching tubes containing either active medication or vehicle alone". Blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Loss to follow‐up in stabilisation phase 83/376 (22%), reasons reported, balanced between groups, intention‐to‐treat and per‐protocol analysis. Discontinued in maintenance phase 27/295 (9.2%); fluticasone cream twice weekly plus moisturiser = 5/70, vehicle cream twice weekly plus moisturiser = 7/84, fluticasone ointment twice weekly plus moisturiser = 6/68, vehicle ointment twice weekly plus moisturiser 9/73); Reasons: lost to follow‐up (11), withdrew consent (3), protocol violation (7), adverse events (4), other (2). Intention‐to treat analysis. "We conducted all analyses on an intention to treat basis (all subjects were included in the analysis if they were randomised and applied the study medication at least once)." Without further information regarding the maintenance phase (the number initially randomised, does not match the number in the maintenance phase). |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Bissonnette 2010.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐controlled study Setting Multicentre, Montreal Quebec, Canada Date of study March 2007 to October 2007. Duration of intervention: 42 days |
|
| Participants | N = 100 (71 female, 29 male) Mean age = 36.1 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 100 (urea 5% moisturiser group = 50, urea 10% lotion group = 50) Withdrawals/losses to follow‐up 12/100 overall (12%); 6 in each group discontinued treatment
Baseline data Mean SCORAD: 5% moisturiser group 20.35 (SD 5.81), 10% lotion group 21.4 (SD 4.96) |
|
| Interventions |
Intervention
Comparator
Washout period: topical immuno modulators and phototherapy (2 weeks), PUVA and systemic treatment (4 weeks) Use of topical corticosteroids permissible if frequency of application constant for 2 weeks prior to start of study and throughout |
|
| Outcomes | Assessments (3): day 3; day 21 phone call to verify compliance and tolerability; day 42 follow‐up visit, efficacy and safety Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared, but 2 investigators are employed by La Roche‐Posay Laboratoire Pharmaceutique, Asnières Cedex, France | |
| Notes | Iso‐Urea, La Roche‐Posay Laboratoire Pharmaceutique, Asnières Cedex, France. Ingredients: aqua ⁄/water, Vitellaria paradoxa (formerly called Butyrospermum parkii; shea butter), glycerol, cyclohexasiloxane, urea, paraffinum liquidum ⁄ mineral oil, sodium lactate, cetearyl alcohol, PEG‐100 stearate, glyceryl stearate, propylene glycol, glycine, tocopherol, stearic acid, myristic acid, palmitic acid, bisabolol, triethanolamine, dimethicone, dimethiconol, disodium EDTA, hydroxyethyl piperazine ethane sulfonic acid, xanthan gum, acrylates ⁄ C10‐30 alkyl acrylate crosspolymer, citric acid, chlorhexidine digluconate, phenoxyethanol, methylparaben, propylparaben, fragrance 10% urea lotion contains: aqua, urea, sodium lactate, paraffinum liquidum, octyldodecanol, caprylic ⁄ capric triglyceride, isopropyl palmitate, glycerol, PEG‐7 hydrogenated castor oil, benzyl alcohol, methoxy PEG‐22 ⁄ docecyl glycol copolymer, PEG‐45 ⁄ dodecyl glycol copolymer, dimethicone, magnesium sulfate, lactic acid, ozokerite, PEG‐2 hydrogenated castor oil, sorbitan isostearate, hydrogenated castor oil We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 17): "Subjects were randomized (1:1)" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "The allocation sequence was generated by an independent statistician" "Individuals were randomised by a computer‐generated list, which was maintained centrally " Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "Individuals were randomised by a computer‐generated list, which was maintained centrally. Treatments were assigned to consecutive patients in a sequential order". Comment: form of central allocation, probably done. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 17 ): "double‐blind..." Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. After email communication: "Two copies of the randomisation list were prepared: one was used by for the labeling of the tubes performed by the sponsor (tubes were designated for each patient ‐ All tubes were equal in weight, and similar in appearance) and the other one was kept by the sponsor until the end of the study". Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page 17 ): "double‐blind..." Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. After email communication: blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 12/100 (12%); 6 in each group discontinued treatment. Reasons reported. Per‐protocol analysis (88/100) Missing data for 4 participants on: SCORAD, cosmetic acceptability and quality of life questionnaire. Comment: balanced and moderate number of dropouts at follow‐up, combined with the per‐protocol analysis, poses an unclear risk of bias for this domain. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appear to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Boguniewicz 2008.
| Study characteristics | ||
| Methods | Randomised, double‐blind, vehicle‐controlled study Setting Multicentre (7), Dermatology and Pediatric departments, children's hospitals in USA Date of study November 2005 to May 2006. Duration of intervention: 43 days |
|
| Participants | N = 142 (74 female, 68 male) Mean age = 5 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 142 (MAS063DP group = 72, vehicle group = 70) Withdrawals/losses to follow‐up 36/142 overall (25.4%); MAS063DP group = 19/72 (26.3%), vehicle group = 17/70 (24.2%)
Baseline data IGA of atopic dermatitis mild: MAS063DP group (37/72), vehicle group (37/70) IGA of atopic dermatitis moderate: MAS063DP group (35/72), vehicle group (33/70) Itch (VAS score) mean: MAS063DP group 6.2 (SD 11.7), vehicle group 6.7 (SD 1.7) |
|
| Interventions |
Intervention
Comparator
If clinically indicated, a low potency rescue topical steroid was prescribed for participants by the study investigator |
|
| Outcomes | Assessments (6): baseline, days 3, 8, 22, 29, 43 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 854): "This work was sponsored by Sinclair Pharmaceuticals Ltd (Surrey, UK)" | |
| Declaration of interest | None declared | |
| Notes | Quote (page 855): "Patients and caregivers agreed to refrain from using other topical and systemic medications (including phototherapy) during the wash‐out and study periods. A washout period of 7 or 14 days was used for patients on topical and systemic medications, respectively, including topical and systemic corticosteroids, topical calcineurin inhibitors, antihistamines,and phototherapy". See Notes of Characteristics of included studies of Abramovits 2008 for details of Atopiclair We mailed investigators numerous times to clarify study details, but received no response (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 855): "Eligible subjects were randomized to receive either MAS063DP or vehicle in a 1:1 ratio according to a computer generated code" Comment: probably done. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 855): "double‐blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 17 ): "double‐blind..." Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 36/142 (25.4%); MAS063DP group = 19/72 (26.3%), vehicle group 17/70 (24.2%), reasons reported. Both per‐protocol and intention‐to‐treat analysis. Comment: the percentage of drop‐outs exceeded 20%, however, the investigators provided both a per‐protocol and an intention‐to‐treat analysis (last observation carried forward). We judged this as being at an unclear risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Bohnsack 1997.
| Study characteristics | ||
| Methods | Randomised, double‐blind, placebo‐controlled, within‐participant study Setting BioSkin Institut für dermatologische Forschung und Enwicklung, Hamburg, Germany Date of study Unspecified. Duration of intervention: 4 weeks, followed by a 5‐month open phase for dermal tolerance |
|
| Participants | N = 41 (31 female, 10 male) Mean age = 31 years Inclusion criteria of the trial
Exclusion criteria of the trial
RandomisedN = 41, to either forearm (within‐participant) Withdrawals/losses to follow‐up3/41 (7.3%), worsening eczema (1), other reasons unrelated to the study (2) Baseline dataCorneometry mean units: urea 10% lotion side 40.4 (SD 6.6), vehicle side 40.0 (SD 8.0) Combined total eczema score for all participants: urea 10% lotion side 91, vehicle side 88 |
|
| Interventions |
Intervention
Comparator
No other treatments and moisturising shower and bath products were allowed. |
|
| Outcomes | Assessments (6): baseline, days 8, 15, 22, 29 and 32
Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared, however, 1 of the products under research is from Beiersdorf AG, Hamburg, Germany | |
| Declaration of interest | None declared, however 2 of the investigators are employees of Beiersdorf AG, Hamburg, Germany, the manufacturer of the principal intervention | |
| Notes | As the study was 19 years old we did not contact the investigators for data | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 35): “randomisiert zugeordnet” (translation: assigned randomly) Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 34): "double‐blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received on each forearm, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 34): "double‐blind" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 3/41 (7.3%) withdrew for worsening of the skin condition (1) and reasons not related to treatment (2). Per‐protocol analysis Comment: low number of losses to follow‐up, and although per‐protocol analysis, considered as being at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Boralevi 2014.
| Study characteristics | ||
| Methods | Randomised, double‐blind, vehicle‐controlled study Setting Multicentre in France (4 centres), Estonia (5 centres), Lithuania (5 centres), Poland (9 centres), and Romania (7) Date of study November 2011 to May 2012. Duration of the intervention 28 days with a follow‐up (open‐label) period of 46 days |
|
| Participants | N = 251 (122 female, 127 male and 2 gender unknown) Mean age = 4 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 251 (V0034CR01B moisturiser group = 125, vehicle group= 126) Withdrawals/losses to follow‐up 10/251 overall (4%); V0034CR01B group = 5/125, vehicle group = 5/126
Baseline data Mean objective SCORAD: V0034CR01B group 11.7 (SD 2.1), vehicle group 11.2 (SD 2.1) Mean itch (VAS): V0034CR01B group 2.8 (SD 2.2), vehicle group 2.5 (SD 1.9) Mean corneometry units: V0034CR01B group 29.1 (SD 10.3), vehicle group 29.4 (SD 11.3) |
|
| Interventions |
Intervention
Comparator
In case of atopic dermatitis flares, the test treatment had to be applied in the morning and a moderately potent corticosteroid 0.1% desonide in the evening until complete resolution of inflammatory skin lesions |
|
| Outcomes | Assessments (5): days 1, 7, 14, 21 and 28 Outcomes of the trial(as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 1456): "This study was funded by Pierre Fabre" | |
| Declaration of interest | Quote (page 1456): "F.B. received consulting fees and fees for participation in review activities from Pierre Fabre. M.S.A. and A.D. are employees of Pierre Fabre. G.T. received consulting fees from Pierre Fabre. H.R., A.K. and M.B. declare no conflicts of interest related to this article" | |
| Notes | We only included the double‐blind period of 28 days. Ingredients of V0034CR01B moisturiser: glycerol 15%, liquid and soft paraffin 10%, glycerol monostearate, stearic acid, polydimethylcyclosiloxane, silicone oil, macrogol 600, trolamine, propyl parahydroxybenzoate and purified water We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 1457): "During the double‐blind period, patients were randomized 1:1 using a computer‐generated and ‐validated list to be treated for 28 days..." Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | Quote (page 1457): "The randomization list was generated by the Clinical Pharmacology Department using proprietary software and with parallel groups and a block size of four, and the list was validated by the Biometry Department. Treatments were provided in identical, sequentially numbered containers and were assigned to patients by investigators on the basis of the sequence number". Comment: central allocation, de‐identified drug containers. Allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 1457): "Treatments were provided in identical, sequentially numbered containers and were assigned to patients by investigators on the basis of the sequence number. Thus, patients, investigators and pharmacists were blinded to which treatment (emollient or vehicle) was supplied". Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcomes were investigator‐assessed as well as participant‐assessed. Comment: blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 10/251 (4%): V0034CR01B group = 5, vehicle group = 5. Intention‐to‐treat analysis. Comment: the low total number of drop‐outs, balanced between the groups combined with a intention‐to‐treat analysis, meant we considered this study to be at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was available (EudraCT number 2011‐003295‐37), and the prespecified outcomes and those mentioned in the methods section did not all appear to have been reported. VAS data on pruritus are missing and very limited data on SCORAD and objective SCORAD are available. Comment: initially we judged this as being at a high risk of bias. After email communication: we received all necessary data. Comment: subsequently, we judged this as being at a low risk of bias. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Breternitz 2008.
| Study characteristics | ||
| Methods | Randomised, double‐blind, placebo‐controlled, within‐participant study Setting Department of Dermatology, Friedrich Schiller University, Jena, Germany Date of study November 2004 to March 2006. Duration of intervention: 4 weeks |
|
| Participants | N = 24 (8 female, 16 male) Mean age = 23 years (range 15‐49 years) Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 24, to either forearm (within‐participant) Withdrawals/losses to follow‐up No losses to follow‐up reported Baseline data The eczema on both forearms was of comparable severity Mean adaptation of SCORAD: glycerol 20% side 2.9 (SD 1.3), vehicle side 3.2 (SD 1.3) Mean TEWL (g/m²/h): glycerol 20% side 18.4 (SD 8.2), vehicle side 26.6 (SD 17.3) |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (7): baseline, weeks 1, 2, 3, 4, 5 and 6 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 44): "This study was supported by Spirig AG, Egerkingen, Switzerland" | |
| Declaration of interest | None declared, but 1 of the investigators was an employee of Spirig AG | |
| Notes | Assessment were performed 12 hours after last application and after a washout period of 2 weeks. It remains unclear if this is a product being developed by this company. The glycerol cream contained 20% glycerol (200 mg/g) and the following ingredients: aqua, cetearyl alcohol, isopropyl myristate, paraffinum liquidum, PEG‐40 hydrogenated castor oil, glyceryl behenate, glyceryl dibehenate, tribehenin, citric acid, sodium citrate, methylparaben, propylparaben. The composition of the placebo was identical but without glycerol We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 40): "According to a randomization list, the right or left forearm was selected..." Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "The randomization list was generated from the sponsor of the study not being part of the study during the trial". Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: initially there was insufficient information to permit a clear judgement. After email communication: "we received just A and B labelled tubes and allocated them according to the randomization list to each of the arms". Comment: central allocation, de‐identified drug containers. Allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 39): "...double‐blind..." .."The composition of the placebo was identical without glycerol" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. After email communication: "The study was fully double‐blinded until the statistical analysis was finalized. Both creams had the identical consistence and filled in identical tubes by the sponsor of the study". Comment: the email communication provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page 39): "...double‐blind..." Outcomes were investigator‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. After email communication: "The study was fully double‐blinded until the statistical analysis was finalized. Both creams had the identical consistence and filled in identical tubes by the sponsor of the study". Blinding of the outcomes assessors, key personnel, was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported. |
| Selective reporting (reporting bias) | Low risk | Quote (page 41): trial registered on European Clinical Trials Database (EudraCT (2004‐004443‐22)), protocol not accessible. The prespecified outcomes and those mentioned in the methods section appear to have been reported. |
| Other bias | Unclear risk | Baseline differences in TEWL and erythema in favour of active treatment group. |
Danby 2011.
| Study characteristics | ||
| Methods | Randomised, controlled, within‐participant study Setting The University of Sheffield, South Yorkshire, UK Date of study Unspecified. Duration of intervention: 2 weeks |
|
| Participants | N = 38 (29 female, 9 male) Mean age = 32 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 50, to either forearm (within‐participant) Withdrawals/losses to follow‐up 7/38, reasons unrelated to the trial Baseline data Mean TEWL (g/m²/h): Aqueous cream BP 12.868 (SD 3.253), Oilatum Junior Bath additive 12.819 (SD 3.446) |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (2): baseline and week 2 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 45): "This study was funded by a research grant from Stiefel, a GSK company" | |
| Declaration of interest | None declared | |
| Notes | Poster abstract. Little information was provided. We received responses to our request for study details (Table 11; Table 13). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 44): "randomized comparison" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "with a randomization list" Comment: probably done. |
| Allocation concealment (selection bias) | High risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: initially, there was insufficient information to permit a clear judgement. After email communication: "no concealment" Comment: subsequently, we judged this as at a high risk of bias. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Nothing reported regarding blinding. Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received on each forearm, to permit a clear judgement. After email communication: "no blinding" Comment: the outcome was likely to be influenced by the lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcomes were investigator‐assessed.
Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. After email communication: "no blinding" Comment: the outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Nothing reported, little information provided. Comment: there was insufficient information to permit a clear judgement. |
| Selective reporting (reporting bias) | Unclear risk | Comment: there was insufficient information to permit a clear judgement. |
| Other bias | Unclear risk | Comment: there was insufficient information to permit a clear judgement. |
De Belilovsky 2011.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, active‐controlled study Setting Multicentre in Spain, 12 dermatologists in private practices Date of study August to October 2007. Duration of intervention: 3 weeks |
|
| Participants | N = 80 (44 female, 36 male) Mean age = 2.3 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 80 (STELATOPIA moisturiser = 40, hydrocortisone butyric‐propionate cream group = 40) Withdrawals/losses to follow‐up No losses to follow‐up reported Baseline data Mean SCORAD: STELATOPIA moisturiser 36.86 (SD 12.01), hydrocortisone butyric‐propionate cream group 37.19 (SD 15.28) |
|
| Interventions |
Intervention
Comparator
All children also received a body hygiene product in its marketed form (STELATOPIA milky bath oil, Mustela; Laboratoires Expanscience), to be used at least once every other day |
|
| Outcomes | Assessments (3): baseline, weeks 1 and 3 Outcomes of the trial(as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 364): "This study was supported by Laboratoires Expanscience, R&D Center, France. Dr C. de Belilovsky was supported and paid by Laboratoires Expanscience for managing the project" | |
| Declaration of interest | Quote (page 364): "The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper". Several authors were employees of Laboratoires Expanscience, the manufacturer of the primary intervention. | |
| Notes | STELATOPIA moisturiser, Mustela; Laboratoires Expanscience, France contains: 2% sunflower oleodistillate, essential fatty acids, bio‐ceramides, β‐sitosterol and a complex of emulsifying sugars We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (360): "were randomly assigned by the dermatologists" and "following a chronologic order of inclusion on a randomized attribution list" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: initially, there was insufficient information to permit a clear judgement. After email communication: allocation was controlled by the Clinical Reseach Organisation. Comment: form of central allocation. Allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (360): "single‐blind" and "observation blinded" Comment: the report alone did not provide sufficient detail about the specific measures used to blind study personnel from knowledge of which intervention a participant received, to permit a clear judgement. After email communication: "Anonymous sealed identical packaging provided by the Clinical Reseach Organisation" Comment: the report provided sufficient detail about the measures used to blind study personnel from knowledge of which intervention a participant received, however, participants were not blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote (360): "single‐blind" and "observation blinded" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: blinding of the outcomes assessors, was ensured, but participants and parents were not blinded. The outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Draelos 2008.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, active‐controlled study Setting Dermatology Clinic, High Point, North Carolina, USA Date of study Unspecified. Duration of intervention: 4 weeks |
|
| Participants | N = 60 (gender not reported) Age range = 5 to 80 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 60 (fluocinonide cream 0.05% + cleansing bar group = 20, fluocinonide cream 0.05% + MVE liquid cleanser group = 20, fluocinonide cream 0.05% + MVE liquid cleanser + MVE moisturising cream = 20) Withdrawals/losses to follow‐up No losses to follow‐up reported Baseline data Mean Global Disease Severity: fluocinonide cream 0.05% + cleansing bar group = 3.0, fluocinonide cream 0.05% + MVE liquid cleanser group = 3.1, fluocinonide cream 0.05% + MVE liquid cleanser + MVE moisturising cream = 3.0 |
|
| Interventions |
Intervention
Comparator 1
Comparator 2
Participants underwent a 4‐week oral and topical eczema treatment washout period before study entry |
|
| Outcomes | Assessments (4): baseline, weeks 1, 2, and 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 87): "This study was supported by an unrestricted educational grant from Coria Laboratories, Ltd" | |
| Declaration of interest | Quote (page 87): "The author reports no conflict of interest" | |
| Notes | MVE = multilamellar vesicular emulsion. Quote (page 87): "In MVE, there are concentric layers of oil‐in‐water emulsions, which are referred to as vesicles. The vesicles are unfolded when placed in contact with the skin surface to release ceramides; cholesterol; free fatty acids; phytosphingosine; and other moisturising ingredients, such as dimethicone, glycerol, and hyaluronic acid, onto the skin surface" We mailed investigators numerous times to clarify study details, but received no response (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 88): "Subjects were randomized to 1 of 3 balanced treatment groups of 20 subjects each" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Participants were not blinded, unclear if physicians were blinded. Comment: the report did not provide sufficient detail about the specific measures used to blind study personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 89): "Blinded investigator assessments" Outcomes were (mainly) investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of healthcare providers during the study, and participants and parents were not blinded. Insufficient information to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Draelos 2009.
| Study characteristics | ||
| Methods | Randomised, investigated‐blinded, 'other moisturiser'‐controlled, within‐participant study Setting Dermatology Clinic, High Point, North Carolina, USA Date of study Unspecified. Duration of intervention: 4 weeks |
|
| Participants | N = 60 (gender not reported) Age > 18 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 60 to either forearm or leg (within‐participant) Withdrawals/losses to follow‐up 1/60 (1.7%)
Baseline data The groups were properly balanced at baseline between arm and leg target sites and eczema severity, as no statistically significant differences between groups were present at baseline. Mean participant‐assessed disease severity (6‐point Likert scale): Albolene side 2.8, MimyX side 2.8 Mean investigator‐assessed disease severity (6‐point Likert scale): Albolene side 2.6, MimyX side 2.6 |
|
| Interventions |
Intervention
Comparator
In people with moderate eczema, treatment was combined with 0.1% triamcinolone acetonide |
|
| Outcomes | Assessments (4): baseline, weeks 1, 2, and 4 Outcomes of the trial(as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 40): "This study was funded through an unrestricted grant from DSE Healthcare Solutions, which manufactures Albolene, one of the products evaluated in this research" | |
| Declaration of interest | None declared | |
| Notes | Albolene, Clarion Brands Inc contains mineral oils, petrolatum, paraffin, ceresin and betacarotene. Mimyx, Stiefel, Coral Gables, FL, contains lipids (triglycerides, phospholipids), squalene, phytosterole, and N‐palmitoylethanolamide (has anti‐inflammatory effect) We mailed the investigator numerous times to clarify study details, but received no response (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 41): "were asked to use the OTC moisturizer twice daily to the randomized right or left target limb and an Rx device to the other randomized target limb" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 41): "The study could only be investigator blinded, as it was not possible to make the two study moisturizers appear identical, since the products were studied as currently marketed". Participants were not blinded. Comment: the report did not provide sufficient detail about the specific measures used to blind study personnel from knowledge of which intervention a participant received on each body part, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote (page 41): "The study could only be investigator blinded" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of healthcare providers during the study, and participants and parents were not blinded. The outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1/60 (1.7%), reason reported. Per‐protocol analysis. Comment: low number of losses to follow‐up, and although per‐protocol analysis, considered as at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Draelos 2011.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐controlled, within‐participant study Setting Dermatology Clinic, High Point, North Carolina, USA Date of study Unspecified. Duration of intervention: 4 weeks |
|
| Participants | N = 20 (all female) Mean age was not reported Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 20 to either body site (within‐participant) Withdrawals/losses to follow‐up 2/20 (10%)
Baseline data Mean overall severity score 2 = mild, 3 = moderate: hyaluronic acid‐based emollient foam 2.9, ceramide‐containing emulsion cream 2.9 |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (3): baseline, weeks 2 and 4 Outcomes of the trial(as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared | |
| Notes | EpiCeram contains a blend of ceramides, cholesterol and free fatty acids. Hyalotopic contains water, glycerol, ethylhexyl palmitate, cetearyl alcohol, Theobroma grandiflorum seed butter, petrolatum, dimethicone, parabens, tocopherol acetate and sodium hyalorunate We mailed the investigator numerous times to clarify study details, but received no response (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 186): "This single‐centered, double‐blinded, randomized, split body study" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 186): "double‐blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study personnel from knowledge of which intervention a participant received on each part of the body, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 186): "Blinded investigator ratings" and "double‐blind" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2/20 (10%), worsening atopic dermatitis at all sites (1), lost to follow‐up (1). Per‐protocol analysis. Comment: low number of losses to follow‐up, and although per‐protocol analysis, considered as at a low risk of bias. |
| Selective reporting (reporting bias) | High risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared not to be all reported. Results on participant assessments of target site skin appearance for redness, peeling, dryness, stinging/burning, and overall skin irritation were missing. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Emer 2011.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, active‐controlled, within‐participant study Setting Outpatient clinic of Dermatology Clinical Trials Center, Mount Sinai School of Medicine, New York, USA Date of study September 2009 to March 2010. Duration of intervention: 4 weeks |
|
| Participants | N = 20 (gender not reported) Age range = 14 to 50 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 20 to either body site (within‐participant) Withdrawals/losses to follow‐up No losses to follow‐up reported. Baseline data PGA mild: Eletone N = 2, pimecrolimus N = 2 PGA moderate: Eletone N = 15, pimecrolimus N = 15 PGA severe: Eletone N = 3, pimecrolimus N = 3 Mean PGA (0‐5): Eletone side 3.08, pimecrolimus side 3.03 Mean participants' self‐assessment (0‐3): Eletone side 2.32, pimecrolimus side 2.33 |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (3): baseline, weeks 2 and 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 741): "Funding Sources: Fernadale Laboratories" | |
| Declaration of interest | Quote (page 471): "The authors have no relevant conflict of interest to disclose" | |
| Notes | Eletone contains a high lipid content that utilizes a specialized hydrolipid technology, a reverse‐phase formulation of 70% lipids dispersed in 30% outer phase of water We mailed investigators numerous times to clarify study details, but received no response (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 737): "medication was randomized in a 1:1 ratio" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 737): "investigator blinded" and "subsequently dispensed by an unblinded study coordinator to ensure investigator blindness" Comment: the report did not provide sufficient detail about the specific measures used to blind study personnel from knowledge of which intervention a participant received on each part of the body, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote (page 737): "investigator‐blinded". Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (healthcare providers) during the study, and participants were not blinded. The outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Evangelista 2014.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐controlled study Setting Dermatology Outpatient Department of the Jose R Reyes Memorial Medical Center, Manila, Philippines Date of study March 2011 to June 2012. Duration of intervention: 8 weeks |
|
| Participants | N = 117 (50 female, 47 male and 20 gender unknown) Mean age = 4.5 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 117 (virgin coconut oil group = 59, mineral oil group = 58) Withdrawals/losses to follow‐up 16/117 overall (13.7%); virgin coconut oil group = 5/59 (8.5%), mineral oil group = 11/58 (19.0%)
Reasons for withdrawal
Baseline data Mean SCORAD index: virgin coconut oil group 13.28, mineral oil group 12.29 Mean TEWL (g/m²/h): virgin coconut oil group 26.68, mineral oil group 24.12 Mean skin capacitance (corneometry units): virgin coconut oil group 32.00, mineral oil group 31.31 |
|
| Interventions |
Intervention
Comparator
All parents were asked to give the participating children a bath once daily with warm water for 5–10 minutes and to apply the assigned oil immediately after bathing and at night. |
|
| Outcomes | Assessments (4): baseline, weeks 2, 4 and 8 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | Quote (page 100): "Conflicts of interest: None" | |
| Notes | Parents were advised not to give or apply any other medication (excluding multivitamins) or moisturiser during the study period. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 102): "The study statistician generated a list of random numbers using the table of random numbers" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | Quote (page 102): "uniform opaque plastic bottles" and "The bottles were coded (A or B) by the pharmacist" and "An assigned resident, who was blinded to the codes, allocated the treatments randomly using the list and dispensed the packaged bottles accordingly. The codes were not disclosed to the investigators until the end of the study". Comment: central allocation, de‐identified uniform bottles. Allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 102): "Both VCO and mineral oil were obtained from local companies. They were repackaged into uniform opaque plastic bottles with a small opening to mask the color and scent of both oils. There are no other apparent differences between the oils as both are clear, colorless, and of similar viscosity. The bottles were coded (A or B) by the pharmacist". Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page 102): "Both VCO and mineral oil were obtained from local companies. They were repackaged into uniform opaque plastic bottles with a small opening to mask the color and scent of both oils. There are no other apparent differences between the oils as both are clear, colorless, and of similar viscosity. The bottles were coded (A or B) by the pharmacist". Outcomes were investigator‐assessed as well as participant‐assessed. Blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 16/117 (13.7%), virgin coconut oil group = 5/59 (8.5%), mineral oil group = 11/58 (19.0%), reasons reported. Intention‐to‐treat analysis. Comment: the total number of dropouts were unbalanced between the groups and although combined with a intention‐to‐treat analysis, represents an unclear risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free from other forms of bias. |
Faergemann 2009.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, 'other moisturiser'‐controlled within‐participant study Setting 2 Dermatology departments Sahlgrenska University Hospital, Göteborg and University Hospital MAS, Malmö, Sweden Date of study October to March unclear which years. Duration of intervention: 2 weeks |
|
| Participants | N = 56 (39 female, 17 male) Mean age = 46 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 56 to either leg (within‐participant) Withdrawals/losses to follow‐up 1/56 (1.8%) before start of treatment Baseline data Nothing reported |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (2): baseline and week 2 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 307): "This study was supported by Schering‐Plough AB, Sweden and writing of the article was supported by TFS Trial Form Support, Sweden" | |
| Declaration of interest | Quote (page 307): "Conflict of interest: Petter Olsson is an employee of Schering‐Plough AB, Sweden" | |
| Notes | The investigator was not able to provide us with more information on study details (Table 11). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 305‐6): "according to randomization 1:1 ratio" and "The subjects were randomized into two groups (1:1)" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 305): "Single‐blind" and "The allocation of treatment was known to the patients but not to the investigator" Comment: the report did not provide sufficient detail about the specific measures used to blind study personnel from knowledge of which intervention a participant received on each leg, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote (page 305): "Single‐blind" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (healthcare providers) during the study. Participants were not blinded. The outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1/56 (1.8%) before start of treatment. Intention‐to‐treat analyses. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Ferreira 1998.
| Study characteristics | ||
| Methods | Randomised, 'other moisturiser'‐controlled study Setting Dermatology Department, Hospital do Desterro, Lisbon, Portugal Date of study Unspecified. Duration of intervention: 12 weeks |
|
| Participants | N = 23 (7 female, 16 male) Mean age = 9.7 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 23 (unclear how many to each group) Withdrawals/losses to follow‐up Nothing reported Baseline data Mean xerosis scores: Nioleol group 26.6 (SD 22.5), Atopic group 23.3 (SD 17.5), Uriage group 30.0 (SD 28.2), Atoderm group 33.3 (SD 27.3) Mean pruritus scores: Nioleol group 14 (SD 11.4), Atopic group 13.5 (SD 12.1), Uriage group 11.7 (SD 9.8), Atoderm group 14.6 (SD 10.5) Mean cutaneous hydration units: Nioleol group 109 (SD 15.6), Atopic group 107 (SD 12.8), Uriage group 108 (SD 21.3), Atoderm group 99 (SD 16.8) Mean TEWL (g/m²/h): Nioleol group 9.25 (SD 3.5), Atopic group 9.05 (SD 4.3), Uriage group 9.05 (SD 2.4), Atoderm group 8.15 (SD 3.0) |
|
| Interventions |
Intervention
Comparator 1
Comparator 2
Comparator 3
|
|
| Outcomes | Assessments (8): baseline, weeks 1, 2, 3 4, 6, 8 and 12 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared | |
| Notes | Atoderm, Bioderma, Laboratoire Dermatologique contains: aqua, mineral oil (paraffinum liquidum), glycerol, cetearyl isonanoate, glyceryl stearate, PEG‐100 stearate, myreth‐3 myristate, steareth‐21, tocopheryl acetate, mannitol, xylitol, rhamnose, fructo‐oligosaccharides, laminaria ochroleuca extract, cyclopentasiloxane, cyclohexasiloxane, triethanolamine, cetyl alcohol, palmitic acid, stearic acid, acrylates/C10‐30 alkyl acrylate crosspolymer, caprylic/capric trygliceride, disoidum EDTA, phenoxyethanol, chlorphenesin, sodium hydroxide As the study was 18 years old we have not contacted the investigators for missing trial data. As it is unclear how many were randomised to each group, this study is included in Table 13 |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 139): "They were randomised into four groups" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No reporting of measures used to blind study participants and personnel from knowledge of which intervention a participant received. Comment: the outcome was likely to be influenced by the lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | No blinding reported. Outcomes were investigator‐assessed as well as participant‐assessed. Comment: the outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Nothing reported, unclear how many were randomised to each group. Comment: there was insufficient information to permit a clear judgement. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Frankel 2011.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, active‐controlled, within‐participant study Setting Outpatient clinic of Dermatology Clinical Trials Center, Mount Sinai School of Medicine, New York, USA Date of study March 2010 to October 2010. Duration of intervention: 4 weeks |
|
| Participants | N = 30 (gender not reported) Age range = 4 to 69 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 30 to either body site (within‐participant) Withdrawals/losses to follow‐up 2/30 (6.7%) reasons unreported Baseline data Mean IGA: Hylatopic side 2.62 (SE 0.14), pimecrolimus side 2.62 (SE 0.14) |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (3): baseline, weeks 2 and 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 671): "Study support was provided by Onset Dermatologics" | |
| Declaration of interest | Quote (page 671): "The authors have no relevant financial conflicts of interest to disclose" | |
| Notes | Hyalotopic contains water, glycerol, ethyl‐hexyl palmitate, cetearyl alcohol, Theobroma grandiflorum seed butter, petrolatum, dimethicone, parabens, tocopherol acetate and sodium hyaluronate We mailed investigators numerous times to clarify study details, but received no response (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 669): "were screened and randomized in a 1:1 ratio" Quote (page 668): "A randomized list was created to determine which side the subject applied..." Comment: probably done |
| Allocation concealment (selection bias) | Unclear risk | Quote (page 668): "The list was only available to the un‐blinded study coordinator" The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 668): "investigator‐blinded" "subsequently dispensed by an unblinded study coordinator to ensure investigator blindness". Participants were not blinded. Comment: the report did not provide sufficient detail about the specific measures used to blind study personnel from knowledge of which intervention a participant received on each part of the body, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote (page 668): "investigator‐blinded". Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (healthcare providers) during the study, and participants were not blinded. The outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2/30 (6.7%); reasons unreported. Per‐protocol analysis. Comment: low number of losses to follow‐up, and although per‐protocol analysis considered as at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was available (NCT01202149), and the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Fredriksson 1975.
| Study characteristics | ||
| Methods | Two randomised, double‐blind, 'other moisturiser'‐controlled, within‐participant studies Setting Two Dermatology clinics of the Central Hospitals Västerás and Sundsvall, Sweden Date of study During winter 1972‐73. Duration of interventions: 4 weeks |
|
| Participants | N = 2 studies of 30 (gender not reported) Mean age not reported Inclusion criteria of the trials
Exclusion criteria of the trials
Randomised N = 2 studies of 30, to either side of the body (within‐participant) Withdrawals/losses to follow‐up No losses to follow‐up reported Baseline data Nothing reported |
|
| Interventions |
Intervention
Comparator
No other treatments were permitted |
|
| Outcomes | Assessments (3): baseline, weeks 2 and 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared | |
| Notes | Quote (page 442): "Aquacare® is a moisturising emulsion containing 10% urea, multi sterols, phospholipids and fatty diols. Calmurid® contains 10% urea, betaine, and a high content lactic acid" As the study was 41 years old we have not contacted the investigators for data. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 443): "after being randomly marked left and right" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | Quote (page 443): "Tubes containing 90 gm of Aquacare HP Cream and Calmurid Cream were packed into identical cartons after being randomly marked left and right". Unclear who packed the tubes and if allocation was indeed concealed to the investigators. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 443): "These were dispensed in a double‐blind fashion" and "Tubes containing 90 gm of Aquacare HP Cream and Calmurid Cream were packed into identical cartons after being randomly marked left and right". Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received on each part of the body, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page 443): "These were dispensed in a double‐blind fashion" and "Tubes containing 90 gm of Aquacare HP Cream and Calmurid Cream were packed into identical cartons after being randomly marked left and right". Outcomes were investigator‐assessed as well as participant‐assessed. Blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported. Data presented on all randomised participants. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Gao 2008.
| Study characteristics | ||
| Methods | Randomised, active‐controlled study Setting Hospital in China Date of study Unspecified. Duration of intervention: 2 weeks |
|
| Participants | N = 196 (108 female, 88 male) Mean age = 4 months Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 196 (BoPao + 10% urea ointment = 101, BoPao cream only = 95) Withdrawals/losses to follow‐up Nothing reported Baseline data Disease duration 14 days in BoPao + 10% urea cream and 10 days in Bopao only group |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (2): baseline and week 2 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared | |
| Notes | We were unable to retrieve the correct email address for Dr Gao | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 294): translation: "randomly divided" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No reporting of measures used to blind study participants and personnel from knowledge of which intervention a participant received. Comment: the outcome was likely to be influenced by the lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | No blinding reported. Outcomes were investigator‐assessed as well as participant‐assessed. Comment: the outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Nothing reported, there seems to have been an intention‐to‐treat analysis. Comment: we judged this as at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Unclear risk | Comment: there was insufficient information to permit a clear judgement. |
Gayraud 2015.
| Study characteristics | ||
| Methods | Randomised, double‐blind, placebo‐controlled study Setting Investigational site in Poland Date of study March 2012 to June 2013. Duration of intervention: 6 months |
|
| Participants | N = 130 (56 female, 67 male and 7 gender unknown) Mean age = 5 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 130 (65 to either group) Withdrawals/losses to follow‐up 7/165 overall (4.2%); SBT complex = 3/65 (4.6%), moisturiser base 4/65 (6.2%)
Baseline data Mean SCORAD: SBT complex 26.5 (SE 0.9), moisturiser base 26.4 (SE 1.0) Mean PO SCORAD: SBT complex 32.1 (SE 1.9), moisturiser base 32.4 (SE 1.7) |
|
| Interventions |
Intervention
Comparator
Quote (page 108): "Alternately or adjunctively to their conventional topical AD treatment (topical corticosteroids or calcineurin inhibitors such as pimecrolimus or tacrolimus). AD treatments were prescribed at selection visit, prior to entering the study. Subjects were not allowed to alter their prescribed AD medication regimen and to continue concomitantly their current moisturiser or moisturising products" |
|
| Outcomes | Assessments (4): baseline, days 56, 112 and 168 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 112): "The study was granted by Laboratoire Bioderma, France" | |
| Declaration of interest | Quote (page 112): "All authors are employees of Laboratoire Bioderma, Lyon, France" | |
| Notes | Quote (page 108): "SBT complex contains vitamin B3 palmitoyl ethanolamide (PEA) an anti‐pruritus agent, sucro‐esters, β‐sitosterol an anti‐inflammatory agent and zinc known for its antibacterial action against Staphylococcus aureus" We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 108): "Subjects were randomized at the investigational site in a 1:1 way" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "The allocation sequence was generated under SAS v9.2 statistical software" Comment: probably done |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "The allocation sequence was provided to the study center before the beginning of the study. This list assigned each of the product code to a subject number. The complete list was available for the investigator from the beginning of the study. The participants didn't see the allocation sequence. It was impossible for them to guess which product they or the following subjects received". Comment: central allocation. Allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 165): "double‐blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. After email communication: "The tested products were packaged identically in white plastic bottle with pomp dispenser [SIC], with the exact same labeling. The color and texture of both topical products were the same: white emulsion. The only difference between both product were the identification code BIXXXVX. Neither the investigator nor the caregivers knew the nature of the products used (tested product or placebo). The investigator and CRO staff was just following the randomization list to allocate the product without knowing if it was the tested product or the placebo. The nature of the products was only known by the Sponsor" Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcomes were investigator‐assessed as well as participant‐assessed.
Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement After email communication: blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 7/165 (4.2%); SBT complex = 3/65 (4.6%), moisturiser base 4/65 (6.2%). Per‐protocol analysis Comment: low number of losses to follow‐up, and although per‐protocol analysis considered as at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Gehring 1996.
| Study characteristics | ||
| Methods | Randomised, double‐blind, active‐controlled study Setting Dermatology clinic, Karlsruhe, Germany Date of study Unspecified. Duration of intervention: 2 weeks |
|
| Participants | N = 69 (39 female, 24 male and 6 gender unknown) Mean age = 27 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 69 (water‐in‐oil emulsion group = 31, water‐in‐oil emulsion plus hydrocortisone group = 32) Withdrawals/losses to follow‐up 6/69 (8.7%) unclear from which group
Baseline data Mean roughness according to participants: 3.97 (SD 2.12) water‐in‐oil emulsion group, 4.31 (SD 1.57) hydrocortisone group Mean itch according to participants: 4.65 (SD 2.51) water‐in‐oil emulsion group, 4.72 (SD 2.46) hydrocortisone group Mean redness according to physicians: 2.23 (SD 0.80) water‐in‐oil emulsion group, 1,97 (SD 0.82) hydrocortisone group Mean roughness according to physicians: 3.42 (SD 0.62) water‐in‐oil emulsion group, 3.13 (SD 0.71) hydrocortisone group Mean TEWL (g/m²/h): 24 water‐in‐oil emulsion group, 20 hydrocortisone group |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (3): baseline, weeks 1 and 2 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared | |
| Notes | Excipial U lipo lotion, Spirig Pharma, Erkingen, Germany contains: urea 4%, lipids 36% We have only included the first week of the trial. As the study was 20 years old we have not contacted the investigators for data. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 554): "randomized double‐blind study design" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 165): "double‐blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcomes were investigator‐assessed as well as participant‐assessed.
Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 6/69 (8.7%) unclear from which group. Per‐protocol analysis. Comment: low number of losses to follow‐up, and although per‐protocol analysis considered as at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Gehring 1999.
| Study characteristics | ||
| Methods | Two randomised, double‐blind, vehicle‐controlled, within‐participant studies Setting Dermatology Clinc, Karlsruhe, Germany Date of study Unspecified. Duration of intervention: 4 weeks with 1 week follow up |
|
| Participants | Study 1: N = 20 (14 female, 6 male); Study 2: N = 20 (18 female, 2 male) Mean age study 1 = 25.1 years, mean age study 2 = 22.9 years Inclusion criteria of the trials
Exclusion criteria of the trial
Randomised Study 1: N = 20 to either forearm (within‐participant); Study 2: N = 20 to either forearm (within‐participant) Withdrawals/losses to follow‐up No losses to follow‐up in study 1 1/20 lost to follow‐up in Study 2 due to acute exacerbation of eczema Baseline data Study 1 mean TEWL (g/m²/h): 1.38, corneometry 4.8 Study 2 mean TEWL (g/m²/h): 1.50, corneometry 1.9 |
|
| Interventions | Study 1 Intervention
Comparator
Study 2 Intervention
Comparator
|
|
| Outcomes | Assessments (6): baseline, weeks 1, 2, 3, 4 and 5 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared | |
| Notes | Ingredients Study 1: evening primrose oil 30.0 ml, glycerol monostearate 4.0 ml, cetyl alcohol 6.0 ml, polyoxyethylene glycerol monostearate 7.0 ml, glycerol 15.0 ml, propylene glycol 10.0 ml, purified water to 150.0 ml Ingredients Study 2: evening primrose oil 20%, aqua, paraffinum liquidum, caprylic/capric triglyceride, urea, myristyl lactate, dimethicone, methoxy PEG‐22/dodecyl, glycol copolymer, sodium lactate, PEG‐7 hydrogenated castor oil, sorbitan isostearate, PEG‐2 hydrogenated castor oil, ozokerite, hydrogenated castor oil, chlorhexidine, triclosan, lactic acid, perfume As the study was 17 years old, we have not contacted the investigators for data |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 636): "a vehicle‐controlled, randomised, double‐blind trial" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 165): "double‐blind" and "taken from containers labelled "RIGHT" and "LEFT". The vehicle was similar in both active treatment and placebo arms. Comment: the report provided sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received on each forearm, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Outcomes were investigator‐assessed. Blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up in Study 1, but 1/20 lost to follow‐up in Study 2 due to acute exacerbation of eczema. Per‐protocol analysis. Comment: low number of losses to follow‐up, and although per‐protocol analysis considered as at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Giordano‐Labadie 2006.
| Study characteristics | ||
| Methods | Randomised, controlled (inactive) study Setting Department of Dermatology Hôpital Purpan Toulouse, France Date of study Unspecified. Duration of intervention: 2 months |
|
| Participants | 76 children (gender not reported) Mean age = 4 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 76 (active treatment group = 37, non‐treated group = 39) Withdrawals/losses to follow‐up No losses to follow‐up reported, after email contact it appeared that there were 2 losses in Exomega group Baseline data Mean SCORAD: active treatment group 25.96 (SD 7.67), non‐treated group 23.3 (SD 7.63) Mean CLQI: active treatment group 2.24 (SD 0.25), non‐treated group 1.59 (SD 0.7) |
|
| Interventions | Both groups received a cleansing bar (A‐Derma, Pierre Fabre Laboratories) Intervention
Comparator
Use of strong/moderate topical corticosteroids allowed. No other moisturiser permitted |
|
| Outcomes | Assessments (3): baseline, days 28 and 56 Outcomes of the trial(as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared. However, the product under research comes from the Pierre Fabre Research Institute, the manufacturer of the drug under investigation | |
| Declaration of interest | None declared, but 1 of the investigators was an employee of Pierre Fabre Research Institute, the manufacturer of the drug under investigation | |
| Notes | Washout period of 1 week before study started Exomega milk contains: evening primrose oil, Rhealba oat extract, chlorphenizine, phenoxyethanol, butyl hydroxy toluene, glycols, paraffin jelly, paraffin oil, shea butter We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 79): "randomized..." Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "The randomization was generated by the means of a program created with SAS® software" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "Sequence generation, has been done centrally by the pharmaceutical company" Comment: probably done. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote (page 79 ): "It was packaged in unidentifiable 200 ml bottles" After email communication: "The investigators were not blind because they could see the products when they were handed over to the patients" Comment: no similar placebo intervention in control group. The outcome was likely to be influenced by the lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote (page 79): "It was packaged in unidentifiable 200 ml bottles"
Outcomes were investigator‐assessed as well as participant‐assessed. Comment: no similar placebo intervention in control group. The outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported. After email communication: "2 subjects were losses in Exomega group between D0 and D28" Comment: we judged this to be at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Glazenburg 2009.
| Study characteristics | ||
| Methods | Two‐phase study, the maintenance phase of which was randomised, double‐blind, and placebo‐controlled Setting Multicentre (N = 13) in the Netherlands (N = 12) and Belgium (N = 1) Date of study Unspecified. Duration of first phase 4 weeks (not randomised), then a 16‐week randomised phase |
|
| Participants | N = 90 (52 female, 38 male) Mean age = 5.7 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 90, in maintenance phase N = 75 (fluticasone group = 39, placebo group = 36) Withdrawals/losses to follow‐up 3/90 in first phase; serious adverse event (1), withdrawal of consent (1), lost to follow‐up (1) 12/87 (13.8%) in maintenance phase; target TIS > 1 (9), consent withdrawn (1), target TIS ≤ 1 at the original lesion but target TIS > 1 at another lesion (1) and exacerbation of atopic dermatitis (1) between the end of the acute phase and the start of the maintenance phase Baseline data at maintenance phase Mean TIS score: for both groups 0 Mean objective SCORAD: fluticasone group 3.6, placebo group 7.0 |
|
| Interventions | Acute phase; all children received twice daily fluticasone propionate 0.005% ointment over 4 weeks on all originally affected sites, even if no visible signs of atopic dermatitis were detectable, and on all newly occurring lesions. Standard moisturiser was supplied for use as required.
We only included the maintenance phase of this study. Intervention
Comparator
During maintenance phase a moisturiser was applied twice daily. On days when study medication was applied, moisturiser was applied only in the morning |
|
| Outcomes | Assessments (7): baseline, weeks 4, 6, 8, 12, 16 and 20 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 66): "This study was conducted with financial support from GlaxoSmithKline, London, UK" | |
| Declaration of interest | None declared, but the lead author is an employee of GlaxoSmithKline, Zeist, The Netherlands, the manufacturer of fluticasone propionate 0.005% ointment | |
| Notes | We included only the randomised maintenance phase We mailed investigators numerous times to clarify study details, as there was inconsistency in the data reported regarding objective SCORAD, in the text and the corresponding data in the table, which was also not in agreement with a comment made by the investigators "overall a statistically significant difference was observed between treatment groups (P = 0.021)". However, we received no response (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 60): "Randomization was achieved by a computer‐generated scheme and performed by the statistician" Comment: probably done. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 60): "double‐blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 60): "double‐blind" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 12/87 (13.8%) in maintenance phase, reasons reported. Per‐protocol analysis. Comment: balanced and moderate number of drop‐outs combined with the per‐protocol analysis poses an unclear risk of bias for this domain. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Grimalt 2007.
| Study characteristics | ||
| Methods | Randomised, controlled (inactive) study Setting Multicentre, 41 dermatologists in France Date of study January 2004 to end July 2004. Duration of intervention: 6 weeks |
|
| Participants | N = 173 (69 female, 93 male and 11 gender unknown) Mean age = 6 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised 173 (moisturiser group = 91, no moisturiser group = 82) Withdrawals/losses to follow‐up 25/173 overall (14.5%); moisturiser group (13), no moisturiser group (12)
Baseline data Mean SCORAD index: moisturiser group 35.63 (SE 1.25); no moisturiser group 35.96 (SE 1.16) |
|
| Interventions | Both groups received a "hygiene product ‐ pain dermatologique" Intervention
Comparator
Inflammatory lesions in both groups were treated with topical corticosteroids of high [micronized desonide 0.1% cream (Locatop, Laboratoires P. Fabre)] or moderate potency [desonide 0.1% cream (Locapred,Laboratoires P. Fabre)], or both, according to the investigators' regular practice |
|
| Outcomes | Assessments (3): baseline, days 21 and 42 Outcomes of the trial(as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 66): "This work was supported by the Institut de Recherche Pierre Fabre, France" | |
| Declaration of interest | None declared, but 1 of the investigators was an employee of Pierre Fabre Research Institute, the manufacturer of the drug under investigation | |
| Notes | Outcomes assessment parent proxy reports Exomega lotion, Laboratoires Pierre Fabre, France, mainly contains water, petrolatum, shea butter, evening primrose oil, glycerol, paraffin oil, niacinamide, butylene glycol, benzoic acid, carbomer and also specific active Rhealba oat extracts that had previously demonstrated potential beneficial effects on skin inflammation We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 62): "randomly allocated..." "according to a randomization list on the basis of their order of inclusion" After email communication: "the list was provided from the promotors of the study." "A randomisation list was established by Pierre Fabre Biometric Department. The randomization was generated by the means of a program created with SAS® software" "randomization was perform in blocks of 4" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. After email communication: "The study products were labelled with the subject number according the randomization, and each center have to follow and attribute the subject number in the chronological order of arrival at the randomization visit. The entry order of the subjects in the study and the following of the randomization has been checked and validated during the blind review of the study." Comment: central allocation, judged as at a low risk of bias. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote (page 62 ): "This emollient was packed in unidentifiable 400‐ml bottles" After email communication: "We prepared the study product RV2478B and the hygiene product as the following; emollient group received hygiene product and RV2478B milk...non‐treated group hygiene product alone" Comment: no corresponding intervention or placebo in control group, uncertainty that knowledge of the allocated intervention was adequately prevented during the study. The outcome was likely to be influenced by the lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | No corresponding intervention or placebo in control group. Outcomes investigator‐assessed as well as by participants' carers. Comment: the outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 7/91 in moisturiser group and 4/82 in the no moisturiser group, were excluded from the analysis reasons reported (9/173 no follow‐up data, 2/173 late exclusions). Incomplete outcome data: 103/173 IDQOL and 102/173 DFI questionnaires completed Comment: we judged this as being at a high risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appear to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Hagströmer 2001.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐controlled, within‐participant study Setting Section of Dermatology and Venereology, Department of Medicine, Karolinska Institutet at Huddinge University Hospital, Stockholm, Sweden Date of study January to May 1998. Duration of intervention: 2 weeks |
|
| Participants | N = 22 (16 female, 6 male) Mean age = 32 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 22 to either forearm (within‐participant) Withdrawals/losses to follow‐up No losses to follow‐up reported Baseline data Mean TEWL (mg/m²/h): NaCl 40 mg/g and urea 40 mg/g in an oil‐in‐water emulsion side 7.5 (SD 3), urea side 6 (SD 2.5) Mean corneometry units: NaCl 40 mg/g and urea 40 mg/g in an oil‐in‐water emulsion side 54 (SD 4), urea side 51 (SD 5) |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (3): baseline, weeks 1 and 2 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 33): "This study was supported by grants from the Swedish Council for Work Life Research, the Swedish Society of Medicine, Karolinska Institutet, Edvard Welander Foundation, Finsen Foundation, Åke Wiberg Foundation, Tore Nilson Foundation for Medical Research and Pharmacia Upjohn Sweden AB" | |
| Declaration of interest | None declared | |
| Notes | With the exception of the NaCl and urea, the other ingredients in the emulsions were identical, namely liquid paraffin, PEG‐5 glyceryl stearate, cetyl alcohol, stearyl alcohol, stearic acid, trometamol, methylparaben, propylparaben, hydrochloric acid and water. Both creams were prepared by Pharmacia & Upjohn Sweden AB, Stockholm, Sweden As the study was 15 years old we have not contacted the investigators for data |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 28): "The study was comparative, double‐blind and randomised" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 28): "The study was comparative, double‐blind and randomised" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received on each forearm, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcomes were investigator‐assessed as well as participant‐assessed.
Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appear to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Hagströmer 2006.
| Study characteristics | ||
| Methods | Randomised, controlled (no treatment), within‐participant study Setting Department of Medicine, Section of Dermatology and Venereology, Karolinska Institutet at Huddinge University Hospital, Stockholm, Sweden Date of study Unspecified. Duration of the intervention 3 weeks |
|
| Participants | N = 24 (20 female, 4 male) Mean age = 35 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 24 to either forearm (within‐participant) Withdrawals/losses to follow‐up No losses to follow‐up reported Baseline data Nothing reported |
|
| Interventions |
Intervention
Comparator
During the study, the participants were allowed to wash in the usual manner, but not to use any other skin care products on their arms |
|
| Outcomes | Assessments (3): baseline, days 10 and 21 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | Quote (page 272): "None declared" | |
| Notes | The study also included 20 healthy participants Proderm, Ponsus Pharma AB, Stockholm, Sweden contains: dimethicone (< 1%), glycerol (1% to 5%), stearic acid (5% to10%), propylene glycol (5% to 10%), polyvinyl pyrolidone (1% to 5%), polysorbate 20 (1% to 5%), triethanolamine (1% to 5%), methyl‐, butyl‐, ethyl‐ and propylparabens, and purified water (approximately 80%) We failed to contact any of the investigators of this study. No baseline data nor end value data were reported. The data were reported in box‐and‐whisker plots, and were not interpretable (Table 13). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 273): "a randomized forearm" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding reported. Comment: the outcome was likely to be influenced by the lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | No blinding reported. Outcomes were investigator‐assessed. Comment: the outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appear to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Hamada 2008.
| Study characteristics | ||
| Methods | Randomised, double‐blind, placebo‐controlled, cross‐over study Setting Multicentre (5), Dermatological clinics in Fukuoka Prefecture of Japan Date of study March to June 2006. Duration of intervention: 4 weeks (cross‐over after 2 weeks) |
|
| Participants | N = 42 (26 female, 13 male and 3 gender unknown) Mean age = 17.9 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 42 (camellia oil first group = 30, purified water first group = 9, 3 unknown) Withdrawals/losses to follow‐up 3/42 (7.1%), reasons not reported Baseline data Mild eczema: camellia oil first group 17 participants, purified water group 4 participants Moderate eczema: camellia oil first group 13 participants, purified water group 5 participants |
|
| Interventions |
Intervention
Comparator
Any treatments including topical ointments (e.g. corticosteroids) and oral medications (e.g. antihistamine, corticosteroids) were allowed without changing during the trial |
|
| Outcomes | Assessments (2): baseline and week 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared | |
| Notes | We only included the first 2 weeks, before cross‐over. Except for disease severity, no separate data were provided at the end of 2 weeks, only after 4 weeks | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 218): "randomized controlled study" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 214): "double‐blind" (translated) Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 214): "double‐blind" (translated) Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information provided to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 3/42 (7.1%), reasons not reported. Per‐protocol analysis. Comment: low number of losses to follow‐up, and although a per‐protocol analysis we considered this to be at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appear to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Hanifin 1998.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, active‐controlled, within‐participant study Setting Multicentre (unclear how many centres) in US Date of study Unspecified. Duration of intervention: 3 weeks |
|
| Participants | N = 80 (51 female, 29 males) Mean age = 24.4 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 80 to either body side (within‐participant) Withdrawals/losses to follow‐up 2/80 (2.5%)
Baseline data "The overall severity (mean total sign and symptom) scores were similar for both sides" |
|
| Interventions |
Intervention
Comparator
In order to standardise the cleansing regimen, all participants were provided with a non‐medicated cleansing bar (Cetaphil Gentle Cleansing bar, Galderma Laboratories, Inc) |
|
| Outcomes | Assessments (3): baseline, weeks 1 and 3 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 232): "This study was financially supported by Galderma Laboratories Inc, Fort Worth, Texas" | |
| Declaration of interest | None declared, but 1 of the investigators was an employee at Galderma Laboratories the manufacturer of the desonide lotion (DesOwen), the moisturiser and the cleansing bar | |
| Notes | The moisturiser (Cetaphil Moisturising cream, Galderma Laboratories, Inc, Forth Worth, Texas) possesses humectant, emollient and occlusive properties and contains: aqua, glycerol, petrolatum, dicaprylyl ether, dimethicone, glyceryl stearate, cetyl alcohol, Prunus amygdalus (synonym: Prunus dulcis) (sweet almond) oil, PEG‐30 stearate, tocopheryl acetate, acrylates/C10‐30 alkyl acrylate crosspolymer, dimethiconol, benzyl alcohol, phenoxyethanol, glyceryl acrylate/acrylic acid copolymer, propylene glycol, disodium EDTA, sodium hydroxide As the study was 18 years old we did not contact the investigators for data |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 228): "Treatments were randomly assigned by a third party" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 227): "investigator‐blinded", however, participants were not blinded. Comment: the report did not provide sufficient detail about the specific measures used to blind study personnel from knowledge of which intervention a participant received on each part of the body, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote (page 227): "investigator‐blinded". Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (healthcare providers) during the study, and participants were not blinded. The outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2/80 (2.5%), reasons reported. Per‐protocol analysis. Comment: low number of losses to follow‐up, and although per‐protocol analysis, we considered this to be at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appear to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Hanifin 2002.
| Study characteristics | ||
| Methods | Three‐phase study in which the maintenance phase was randomised, double‐blind, and had an active control Setting Multicentre (16) in USA and Canada Date of study Unspecified. Duration of intervention: Stabilisation phase was up to 4 weeks and maintenance phase was 20 weeks |
|
| Participants | N = 372 entered the stabilisation phase (216 female, 156 male), and 348 entered the maintenance phase (more than half the population was female) Mean age = 16.8 years (7.1 years for children and 35.9 years for adults) Inclusion criteria of the trial
For entrance in maintenance phase
Exclusion criteria of the trial
Randomised N = 348 (maintenance phase; fluticasone propionate group = 229, vehicle group = 119) Withdrawals/losses to follow‐up Lost to follow‐up: 44/348 overall (12.6%); fluticasone propionate group = 32/229 (14%), vehicle group = 12/119 (10%) Relapse: 110/348 overall (31.6%); fluticasone propionate group = 27/229 (11.8%), vehicle group = 83/119 (69.7%) Baseline data Moderate eczema 63%, mean Rajka and Langeland Severity Grading score was 7 for all participants, approximately 3/4 of the population suffered continuously from atopic dermatitis without remission |
|
| Interventions | All participants entered an open‐label stabilisation phase of up to 4 weeks' duration on twice daily fluticasone propionate 0.05% cream and used a moisturiser at least once a day Maintenance phase Intervention
Comparator
It is unclear which moisturiser was used |
|
| Outcomes | Assessments Maintenance phase(7): 'baseline', weeks 2, 4, 8, 12, 16 and 20, then 'follow‐up phase' Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 536): "This study (FPC40002) was conducted with a grant from Glaxo Wellcome Inc., Research Triangle Park, NC, U.S.A." | |
| Declaration of interest | None declared, but 1 of the investigators was an employee of Glaxo Wellcome Inc, the manufacturer of the fluticasone propionate cream | |
| Notes | For participants who completed the maintenance phase on intermittent fluticasone propionate 0.05% cream without a relapse, the intermittent fluticasone propionate 0.05% cream dosing/moisturiser regimen was extended for a further 24 weeks in a subsequent follow‐up phase As the study was 14 years old we have not contacted the investigators for data |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 147): "Subjects who entered the second part of the study were randomized (2: 1 within each age stratum)" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 147): "double‐blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcomes were investigator‐assessed as well as participant‐assessed.
Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information provided to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 44/348 (12.6%) were lost to follow‐up; fluticasone propionate group = 32/229 (14%), vehicle group = 12/119 (10%). Intention‐to‐treat analysis. Comment: balanced but moderate number of drop‐outs (although an intention‐to‐treat analysis), poses an unclear risk of bias for this domain. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appear to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Harper 1995.
| Study characteristics | ||
| Methods | Randomised, double‐blind, controlled, cross‐over study Setting Out‐patient Dermatology Clinic at Queen Elizabeth Hospital for Children, London, UK Date of study Unspecified. Duration of intervention: two 4‐week periods (cross‐over study) with 2‐week separation |
|
| Participants | N = 30 (17 female, 9 male and 4 gender unknown) Mean age = 4.5 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 30 (unclear how many to each arm) Withdrawals/losses to follow‐up 4/30 (13.3%)
Baseline data Therapeutic control was adequate for 10 patients and 'marginal with exacerbations in 16' |
|
| Interventions |
Intervention
Comparator
Use of other bath additives was not allowed. Emulsifying ointment or aqueous cream were used as a soap substitute in all cases throughout the study period. Pre‐study topical therapy was continued unaltered during the study |
|
| Outcomes | Assessments (3): baseline, weeks 2 and 4 (then cross‐over phase) Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared, but under acknowledgements "Also Dennis Joseph from Stiefel for his contribution" | |
| Declaration of interest | None declared | |
| Notes | Oilatum Plus includes triclosan and benzalkonium chloride. We have only included the first 4 weeks before the cross‐over part As the study was 21 years old we have not contacted the investigators for data Inconsistency of reporting of number of participants; stated on 2nd page that 32 patients (88%) experienced at least 3 exacerbations. Number randomised to each arm was unclear and there are inconsistencies in data reporting (Table 13). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 42): "The order in which the two preparations were used was determined by a computer generated random code" Comment: probably done. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 42): "double‐blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcomes were investigator‐assessed as well as participant‐assessed.
Comment: uncertainty about the effectiveness of blinding of outcome assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 4/30, reasons reported, unclear how many participants randomised to each arm, and inconsistent reporting of number of participants throughout study. Intention‐to treat‐analysis. Comment: we judged this as being at an unclear risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appear to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Hlela 2015.
| Study characteristics | ||
| Methods | Two randomised, investigator‐blinded, 'other moisturiser'‐controlled, studies Setting Red Cross Children's War Memorial Hospital, Cape Town, South Africa Date of study February 2013 to July 2013. Duration of intervention: 3 months |
|
| Participants | N = 120: Study 1 N = 40 (17 female, 20 male and 3 gender unknown); Study 2 N = 80 (37 female, 36 male and 7 gender unknown) Mean age = 5.6 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 120: Study 1 N = 40 (aqueous cream group = 20, baby oil group = 20), Study 2 N = 80 (cetomacrogol group = 20, emulsifying ointment group = 20, glycerol/petroleum group = 20, petroleum group = 20) Withdrawals/losses to follow‐up Study 1: 3/40 (7.5%); 3 lost to follow‐up in baby oil group Study 2: 7/80 (8.8%); cetomacrogol group (3), emulsifying ointment group (0), glycerol/petroleum group (1), petroleum group (3) Baseline data Study 1: mean SCORAD: aqueous cream group 33.11 (SD 16.82), baby oil group 23.02 (SD 11.79) Study 1: mean POEM: aqueous cream group 11.50 (SD 7.97), baby oil group 9.00 (SD 5.06) Study 1: mean NESS: aqueous cream group 9.50 (SD 3.25), baby oil group 10.20 (SD 1.96) Study 1: mean IDQOL aqueous cream group 7.00 (SD 4.86), baby oil group 6.45 (SD 4.78) Study 2: mean SCORAD: cetomacrogol group 24.78 (SD 16.90), emulsifying ointment group 28.40 (SD 16.16), glycerol/petroleum group 21.52 (SD 15.24), petroleum group 26.77 (SD 12.09) Study 2 mean POEM: cetomacrogol group 9.47 (SD 6.02), emulsifying ointment group 9.10 (SD 4.56), glycerol/petroleum group 9.75 (SD 7.23), petroleum group 11.29 (SD 7.06) Study 2 mean NESS: cetomacrogol group 9.35 (SD 2.40), emulsifying ointment group 9.85 (SD 2.83), glycerin/petroleum group 9.25 (SD 3.64), petroleum group 10.00 (SD 3.35) Study 2 mean IDQOL: cetomacrogol group 7.23 (SD 4.48), emulsifying ointment group 7.25 (SD 5.84), glycerin/petroleum group 7.35 (SD 6.75), petroleum group 6.76 (SD 3.72) |
|
| Interventions | Study 1 Intervention
Comparator
All the participants in study 1 used emulsifying ointment as a moisturiser Study 2 Intervention
Comparator 1
Comparator 2
Comparator 3
All participants in Study 2 washed with baby oil and applied this as soap instead of aqueous cream. All the participants in both studies continued to use clinic‐prescribed topical steroids during the study period, and brought back all tubes so that the amount used during the previous month could be recorded at every visit. |
|
| Outcomes | Assessments (4): baseline, months 1, 2 and 3 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 738): "The study was investigator initiated, and all emollients were requested from and donated by Sekpharma (SA), a generic medicine supply company" | |
| Declaration of interest | None declared | |
| Notes | Frequency of use during day or week were not reported. There were some inconsistencies between text and figures. No end data were reported for Study 2, just stated that all scores tended to decline. We mailed investigators numerous times to clarify study details, but received no response (Table 11; Table 13). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 781): "Patients were randomised using an automatic online enrolment system in a 1:1 ratio for study 1 or a 1:1:1:1 ratio for study 2" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 781): "single (assessor)‐blind trial" Comment: the report did not provide sufficient detail about the specific measures used to blind study personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote (page 781): "single (assessor)‐blind trial" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (healthcare providers) during the study, and participants were not blinded. The outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Study 1: 3/40 (7.5%): 3 lost to follow‐up in baby oil group. Study 2: 7/80 (8.8%): cetomacrogol group (3), emulsifying ointment group (0), glycerol/petroleum group (1), petroleum group (3). Per‐protocol analysis |
| Selective reporting (reporting bias) | Unclear risk | The protocol for the study was available (NCT02084472) and the prespecified outcomes and those mentioned in the Methods section appear to have been reported. However, for Study 2 very few data were provided ("all mean scores tended to decline over time", without providing the data). |
| Other bias | Unclear risk | There was baseline imbalance in SCORAD for study 1, but not for the other disease severity scores. Comment: we judged this as at an unclear risk of bias. |
Janmohamed 2014.
| Study characteristics | ||
| Methods | Randomised, double‐blind, active‐controlled study Setting Multicentre (4), dermatology outpatient clinics in Rotterdam, the Netherlands Date of study February 2009 to February 2012. Duration of intervention: 4 weeks |
|
| Participants | N = 39 (14 female, 25 male) Mean age = 3.4 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 39 (corticosteroid group = 19, placebo group = 20) Withdrawals/losses to follow‐up 4/39 (9.8%); all in placebo group
Baseline data Mean objective SCORAD was 35 to 40 or higher (indicating severe eczema) on 2 measuring points before start of treatment Mean objective SCORAD: corticosteroid group 43.8, vehicle group 43.0 Mean POEM: corticosteroid group 23, placebo group 22 (estimated from figure) Mean IDQOL: corticosteroid group 17, placebo group 14 (estimated from figure) |
|
| Interventions |
Intervention
Comparator
For the face, mometasone furoate 0.1% ointment was diluted 1:19, although pimecrolimus 1% cream was used in some participants. For the body, a 1:3 dilution was used Participants were not allowed to use other moisturisers or topical agents |
|
| Outcomes | Assessments (5): baseline, days 1, 4, 7, 14 and 28 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 1076): "Nonrestricted funds were received from Schering‐Plough BV, Fagron, Astellas, Molnlycke, Aardbeesie Project (www.aardbeesie.nl), and Foundation for Pediatric Dermatology Rotterdam (www.pediatric‐dermatology.com)" | |
| Declaration of interest | Quote (page 1076): "Conflicts of interest: None declared" | |
| Notes | We mailed investigators numerous times to clarify study details, but received no response (Table 11). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 1077): "Computerized randomization was performed by our statistician" Comment: probably done. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 1076): "double‐blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 1076): "double‐blind" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 4/39 (9.8%); all in placebo group, reasons reported. Per‐protocol analysis. Comment: low number of losses to follow‐up, and although per‐protocol analysis, we considered this study to be at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was available (EudraCT Number: 2007‐005232‐81) and the prespecified outcomes and those mentioned in the Methods section appear to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Jirabundansuk 2014.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, active‐controlled, within‐participant study Setting Skin Center, Faculty of Medicine, Srinakharinwirot University, Bangkok, Thailand Date of study Unspecified. Duration of intervention: 4 weeks |
|
| Participants | N = 31 (11 female, 18 male and 2 gender unknown) Mean age = 4.3 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 31 to either body site (within‐participant) Withdrawals/losses to follow‐up 2/31 (6.5%) lost to follow‐up Baseline data Mean SCORAD: spinosa kernel oil cream side 25.6 (SD 7.9), hydrocortisone cream side 25.7 (SD 7.5) |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (4): baseline, weeks 2, 4 and 8 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 824): "The authors wish to thank Hoe Pharmaceutical Sdn Bhd for their support of the experimental S [spinosa kernel oil] cream for this research" | |
| Declaration of interest | Quote (page 824): "Potential conflicts of interest: None" | |
| Notes | The spinosa kernel oil cream consisted of linoleic acid (omega‐6), oleic acid, palmitic acid, stearic acid, polyphenols, tocopherols, phenolic acid, and squalene. Cream base was comprised of butylene glycol, mineral oil, ethylhexyl stearate, tocopheryl acetate, sodium polyacrylate | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 821): "All patients who met eligible criteria were randomized. The randomization schedule was prepared by a third party" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 821): "randomized assessment blind controlled trial" and "The cassettes of both agents were similar in shape and color, however they were labeled as 'left' or 'right'." On the hydrocortisone side two different tubes or cassettes were used compared to one tube or cassette on the S [spinosa kernel oil] cream side. The trialists state "assessment blind", but did not report on the blinding of participants. Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received on each side of the body, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote (page 821): "randomized assessment blind controlled trial" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of healthcare providers during the study and participants and parents seem not to be blinded. The outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2/31 (6.5%) lost to follow‐up. Per‐protocol analysis. Comment: low number of losses to follow‐up, and although per‐protocol analysis, we considered this trial to be at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appear to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Kircik 2009.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, active‐controlled, within‐participant pilot study Setting Indiana University Medical Center, Indianapolis, USA Date of study Unspecified. Duration of intervention: 4 weeks |
|
| Participants | N = 6 (gender not reported) Mean age not reported Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 6 to either body side (within‐participant) Withdrawals/losses to follow‐up Nothing reported Baseline data Nothing reported |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (2): baseline and week 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page AB67): "Commercial support: Poster production sponsored by Ferndale Laboratories, Inc" | |
| Declaration of interest | None declared | |
| Notes | Poster abstract. Little information was provided, PI was not able to provide more study data (Table 11), therefore the study is moved to Table 13 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page AB67): "were randomized" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 1482): "investigator‐blinded study" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received on each side of the body, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcomes were investigator‐assessed and participant‐assessed.
Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants and healthcare providers) during the study. Insufficient information to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Nothing reported, little information provided. Comment: there was insufficient information to permit a clear judgement. |
| Selective reporting (reporting bias) | Unclear risk | Comment: there was insufficient information to permit a clear judgement. |
| Other bias | Unclear risk | Comment: there was insufficient information to permit a clear judgement. |
Kircik 2014.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, 'other moisturiser'‐controlled, within‐participant study Setting Icahn School of Medicine at Mount Sinai, New York, USA Date of study Unspecified. Duration of intervention: 4 weeks |
|
| Participants | N = 10 (6 female, 4 male) Mean age = 31 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 10 to either body side (within‐participant) Withdrawals/losses to follow‐up None reported Baseline data Mean IGA scores: 2 (5 participants), 3 (5 participants) |
|
| Interventions |
Intervention
Comparator
Frequency of application not reported |
|
| Outcomes | Assessments (2): baseline and week 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 1484): "This study is funded by Puracap Pharmaceutical, LLC. " | |
| Declaration of interest | Quote (page 1484): "Dr. Kircik has served as an advisor, investigator, and consultant for Puracap Pharmaceutical, LLC" | |
| Notes | EpiCeram contains a blend of ceramides, cholesterol and free fatty acids Most data had to be estimated from graphs, principal investigator was not able to provide us with more exact study data (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 1482): "Subjects were randomized at a 1:1 ratio" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "pre scheduled list by the CRO" [Clinical research organisation] Comment: probably done. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 1482): "investigator‐blind study" Comment: the report did not provide sufficient detail about the specific measures used to blind study personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 1482): "investigator‐blind study" Outcomes were investigator‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (healthcare providers) during the study. Insufficient information to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appear to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Korting 2010.
| Study characteristics | ||
| Methods | Randomised, vehicle‐controlled study Setting Multicentre (3), outpatient centres in Cologne, Kiel and Heilbronn, Germany Date of study October 2003 and January 2005. Duration of intervention: 4 weeks |
|
| Participants | N = 99 (39 female, 58 male and 2 gender unknown) Mean age = 3.5 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 99 (pale sulfonated shale oil (PSSO) = 51, vehicle = 48) Withdrawals/losses to follow‐up 2/99 (2%), 1 participant in each group did not appear for any follow‐up visits 7/99 (11.7%) "were excluded from per‐protocol analysis"
Baseline data Mild eczema: PSSO group 35 participants, vehicle group 37 participants Moderate eczema: PSSO group 15 participants, vehicle group 10 participants Mean EASI: PSSO group 13.4 (SD 3.7), vehicle group 13.0 (SD 3.1) |
|
| Interventions |
Intervention
Comparator
Accompanying medications of any kind (systemic or topical) were not permitted. The use of skin care products on areas of unaffected skin was allowed as usual |
|
| Outcomes | Assessments (4): baseline, weeks 1, 2 and 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 1176): "The preparation of this article was supported by an educational grant to Dr Schöllmann." | |
| Declaration of interest | Quote (page 1176): "Prof. Korting collaborates with Ichthyol‐Gesellschaft, Hamburg, in the development of topical drugs for skin diseases. Dr Cholcha and Dr Wolff are employed by the company that supported this multicentre study but do not have any personal financial interest in the research described in the manuscript" | |
| Notes | Quote (page 1177): "The verum product was an oil‐in‐water cream with sodium bituminosulfonate 4%, pale (trade name: Ichthosin cream; manufacturer: Ichthyol‐Gesellschaft, Hamburg, Germany). The vehicle was a correspondingly coloured cream without an active ingredient, containing propylene glycol, glycerol monostearate, cetyl alcohol, medium chain triglycerides, macrogol‐1000‐glycerol monostearate, white vaseline, purified water, and – for adjustment to the verum regarding colour – additionally spirit caramel and quinoline yellow." The lead author died in 2012 and the other authors could not be contacted |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 1177‐ 8): "The randomization occurred in blocks of 2 with a randomizing ratio of 1:1" and "Block randomization was chosen and calculated with the validated program RanCode (version 3.6, IDV Gauting, Germany)" Comment: probably done. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No reporting of measures used to blind study participants and personnel from knowledge of which intervention a participant received. Comment: the outcome was likely to be influenced by the lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | No blinding reported. Outcomes were investigator‐assessed as well as participant assessed. Comment: the outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2/99 (2%), 1 from each group did not appear for any follow‐up visit and were excluded from intention‐to treat analysis. Although 7 others appeared to have violated the protocol, these seem to have been included in the analyses. Comment: low number of losses to follow‐up, and although per‐protocol analysis, we considered this to be at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appear to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Larregue 1996.
| Study characteristics | ||
| Methods | Randomised, double‐blind, vehicle‐controlled, within‐participant study Setting Multicentre (4) in France and Italy Date of study Unspecified. Duration of intervention: 4 weeks |
|
| Participants | N = 46 (21 female, 25 male) Age range 6 to 12 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 46 to either body side (within‐participant) Withdrawals/losses to follow‐up 2/46 (4.3%), exacerbation (1), personal reasons (1) Baseline data Nothing reported |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (3): baseline, weeks 2 and 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared | |
| Notes | The emulsion contained almond oil, olive oil, gamma oryzanol and alpha tocopherol As the study was 20 years old we did not contact the investigators for data |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 720): "une etude clinique randomisée" (translation: randomised clinical study) Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 720): "double‐aveugle" (translation: double‐blind): pre‐coded tubes and the investigator was not aware of content. Products were identical except for the lactic acid. Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received on each body side, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page 720): "double‐aveugle" (translation: double‐blind): pre‐coded tubes and the investigator was not aware of content. Products were identical except for the lactic acid. Outcomes were investigator‐assessed as well as participant‐assessed. Blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2/46 (4.3%), exacerbation (1), personal reasons (1). Per‐protocol analysis. Comment: low number of losses to follow‐up, and although per‐protocol analysis, we considered this to be at a low risk of bias. |
| Selective reporting (reporting bias) | High risk | The following predefined outcomes were not addressed; pruritus, and efficacy according to the parents and only P value provided for erythema,papules and excoriations. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Laumann 2006.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, controlled, within‐participant study Setting Multicentre (6) USA Date of study Unspecified. Duration of intervention: 12 weeks |
|
| Participants | N = 74 (42 female, 32 male) Mean age = 26 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 74 to either body side (within‐participant) Withdrawals/losses to follow‐up 8/74 (10.8%)
Baseline data Nothing reported |
|
| Interventions |
Intervention
Comparator
Rescue medication (triamcinolone cream 0.1%) was provided in the event of flare |
|
| Outcomes | Assessments (7): baseline, weeks 2, 4, 6, 8, 10 and 12 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared but product under investigation was from Stiefel Labs Inc | |
| Declaration of interest | None declared | |
| Notes | MimyX cream contains purified water, olive oil, glycerol, pentylene glycol, palm glycerides, vegetable oil, hydrogenated lecithin, squalane, betaine, palmitamide MEA, hydroxyethyl cellulose, sodium carbomer, carbomer, xanthan gum Poster abstract. Little information was provided. We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 45): "Subjects were randomized" and "randomly assigned to one of two groups" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "each subject was assigned a number in numerical sequence of entry. This number was used to enter a computer‐generated assignment to each of the two groups" Comment: probably done |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: Central allocation by sponsor and "The study products were dispensed in opaque bags" Comment: central allocation, de‐identified study products. Allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 45): "investigator blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study personnel from knowledge of which intervention a participant received on each side of the body, to permit a clear judgement. After email communication: "investigators were blinded and the containers were not labeled with what it contained" and "The study products were dispensed in opaque bags" Comment: blinding of investigators was ensured, but participants were not blinded. We judged this as an unclear risk of bias. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page 45): "investigator blind" Outcomes were investigator‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (healthcare providers) during the study. Insufficient information to permit a clear judgement. After email communication: "investigators were blinded and the containers were not labeled with what it contained" and "The study products were dispensed in opaque bags" Blinding of the outcomes assessors was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 8/74 (10.8%), reasons reported. Intention‐to‐treat analysis. |
| Selective reporting (reporting bias) | High risk | Erythema, pruritus, and papulation/induration/oedema assessment and BSA assessment were predefined outcomes that were not addressed in the Results. |
| Other bias | Unclear risk | Comment: there was insufficient information to permit a clear judgement. |
Lodén 2001.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐controlled study Setting Multicentre (4) in Stockholm (2), Uppsala, Linköping, Sweden Date of study Specified February to April but unclear which year. Duration of intervention: 30 days |
|
| Participants | N = 110 (93 female, 16 male and 1 gender unknown) Mean age = 34 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 110 (unclear how many randomised to each arm) Withdrawals/losses to follow‐up 1/110 (< 1 %) dropped out, unclear from which group Baseline data Nothing reported |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (2): baseline and day 31 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared, however, study was probably sponsored by ACO Hud AB, Sweden (see Andersson 1999; Lodén 2002). | |
| Declaration of interest | None declared. Dr Lodén was an employee of ACO Hud AB. | |
| Notes | Unclear how many participants were randomised to each arm, and also how frequently the treatments were applied. The data were estimated from box and whisker plots, which made them difficult to use (Table 13). As the study was 15 years old, we did not contact the investigators for data |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 201): "randomized, double‐blind" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 201): "double‐blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcomes were investigator‐assessed.
Comment: uncertainty about the effectiveness of blinding of outcomes assessors (healthcare providers) during the study. Insufficient information to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1/110 (< 1 %) dropped out, unclear from which group. Per‐protocol analysis. Comment: low number of losses to follow‐up, and although per‐protocol analysis, we considered to be at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Lodén 2002.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐ and placebo‐controlled study Setting Multicentre in Stockholm, Uppsala, Linköping, Göteborg, Umeå and Malmö, Sweden Date of study February‐April, unclear which year. Duration of intervention: 30 days |
|
| Participants | N = 197 (151 female, 46 male) Mean age = 33 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 197 (glycerol group = 68, urea group = 63, placebo group = 66) Withdrawals/losses to follow‐up Not reported Baseline data Not reported |
|
| Interventions |
Intervention
Comparator 1
Comparator 2
The participants were allowed to continue use of topical corticosteroids |
|
| Outcomes | Assessments (3): baseline, weeks 2 and 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 47): "The study was sponsored by Aco Hud AB, Stockholm, Sweden" | |
| Declaration of interest | None declared. Dr Lodén was an employee of ACO Hud AB. | |
| Notes | The glycerol cream contained 20% glycerol, aqua, petrolatum, cream, canola, mineral oil, cetearyl alcohol, glyceryl stearate, dimethicone, PEG‐100 stearate, glyceryl polymethacrylate, cholesterol, propylene glycol, methylparaben and propylparaben. In the placebo cream, glycerol was replaced with water. The urea cream contained 4% urea and 4% NaCl as water‐binding substances in an oil‐in‐water emulsion, pH about 5. Other ingredients were paraffin liquidum, PEG‐5‐glyceryl‐stearate, cetyl alcohol, stearyl alcohol, stearic acid, trometamol, methylparaben, propylparaben, hydrochloric acid and water As the study was 14 years old we did not contact the investigators for data |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 45): "were randomized into three groups" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 45): "double‐blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 45): "double‐blind" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No drop‐outs reported. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Marseglia 2014.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, 'other moisturiser'‐controlled study Setting Multicentre (5), dermatology departments in Pavia, Bargamo, Bari, Sassudo and Milan, Italy Date of study January to May 2013. Duration of intervention: 6 weeks |
|
| Participants | N = 107 (48 female, 59 male) Mean age = 6 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 107 (pro‐AMP group = 72, placebo group = 35) Withdrawals/losses to follow‐up No losses to follow‐up reported Baseline data Mean eczema severity score: pro‐AMP group 6.1 (SD 2.5), placebo group 5.3 (SD 3) |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (3): baseline, weeks 3 and 6 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 274): "This was a non‐profit study" and "Isdin Srl has kindly provided the products used in the trial" | |
| Declaration of interest | Quote (page 274): "MM is an employee of Isdin Srl. He was involved in the study design and in the manuscript preparation" and "The other authors have declared no conflict of interest" | |
| Notes | Nutratopic Pro‐AMP cream contains 2.5% rhamnosoft (Biosaccharide GUM‐2), ceramides (ceramide 3), and 2% ILE (Isdin Barcelona, Spain) We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 272): "Computer‐generated number randomization list was used" "with imbalanced treatment allocation 2:1" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "Concealment was obtained using sealed envelopes" Comment: allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 272): "assessor blinded" Comment: the report did not provide sufficient detail about the specific measures used to blind study personnel from knowledge of which intervention a participant received, to permit a clear judgement and parents and participants seem not to be blinded. After email communication: "Physicians performing the first visit with treatment allocation were not the physicians performing the follow up visits. The latter were not aware of the type of treatment". Comment: the report provided sufficient detail about the measures used to blind study personnel from knowledge of which intervention a participant received. However, participants were not blinded and so we judged this as being at an unclear risk of bias. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote (page 272): "assessor blinded" Outcomes were investigator‐assessed as well as participant assessed. Comment: blinding of the outcomes assessors, was ensured, and it was unlikely that the blinding could have been broken, however, participants and parents seem not to have been blinded. The outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was available (NTR4084) and the prespecified outcomes and those mentioned in the methods section appear to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Miller 2011.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐controlled study Setting Wake Forest University Health Sciences Clinical Studies Center, North Carolina, USA Date of study Not reported. Duration of intervention: 3 weeks |
|
| Participants | N = 39 (22 female, 17 male) Mean age = 7.9 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 39 (BRC‐Gly group = 13, BRC‐Cer group = 13, OTC‐Pet group = 13) Withdrawals/losses to follow‐up 1/39 (2.5%) of OTC‐Pet group due to disease flaring Baseline data Disease severity was comparable in the 3 groups Mean itch (VAS): BRC‐Gly group 51.68 (SD 23.42), BRC‐Cer group 50.77 (SD 24.34), OTC‐Pet group 58.27 (SD 18.05) Mean EASI: BRC‐Gly group 4.05 (SD 3.68), BRC‐Cer group 4.23 (SD 2.34), OTC‐Pet group 5.30 (SD 3.70) |
|
| Interventions |
Intervention
Comparator 1
Comparator 2
|
|
| Outcomes | Assessments (3): baseline, days 7 and 21 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Text in the submitted version that was deleted in the published version read: "This study was supported by Beiersdorf, Inc". | |
| Declaration of interest | Text in the submitted version that was deleted in the published version read: "Dr Fleischer has received research, speaking and/or consulting support from Astellas, Centocor, Amgen, Galderma, Stiefel, Medicis and Intendis. Dr Weber is an employee of Beiersdorf Inc". | |
| Notes | Oral antihistamines were allowed if not initiated or discontinued during study. Compliance was monitored with a diary. See Notes of Characteristics of included studies of Abramovits 2008 for details on Atopiclair and of Draelos 2011 for details on EpiCeram. Aquaphor Healing Ointment contains petrolatum, cera microcristallina, panthenol, glycerol, bisabolol. We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 531 ): "were randomized 1:1:1..." Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "This was an investigator‐initiated protocol. The clinical studies coordinator, who did no assessments, followed a randomization chart obtained online for trichotomization into 3 groups. On this chart the coordinator followed the next randomization" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "No person involved in any clinical assessment had access to the randomization scheme. There were no sealed envelopes" Comment: reasonable to assume allocation adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 535): "Each of the moisturizers was distributed in a plain white jar so that subjects and investigators were blinded..." Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page 535): "Each of the moisturizers was distributed in a plain white jar so that subjects and investigators were blinded...". After email communication:"No person involved in any clinical assessment had access to the randomization scheme" Comment: Outcomes were investigator‐assessed as well as participant assessed. Blinding of participants and key study personnel was ensured, and it is unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1/39 (2.5%) of OTC‐Pet group, reason reported. Per‐protocol analysis. Comment: low number of losses to follow‐up, and although per‐protocol analysis, we considered this to be at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was available (NCT01093469), and the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Msika 2008.
| Study characteristics | ||
| Methods | Randomised, active‐controlled study Setting Multi‐centre (20 paediatricians) in France Date of study March to June 2003. Duration of intervention: 3 weeks |
|
| Participants | N = 90 children (41 female, 45 male and 4 gender unknown)
Mean age = 16 months (range: 4 to 48 months) Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 90 (Group A = 18, Group B = 17, Group C = 15, Group D = 17, Group E = 19, unclear = 4) Withdrawals/losses to follow‐up 4/90 (4.4%): unclear from which groups, lost to follow‐up (1), prematurely stopped the study for their own convenience (not for side effects) (2), forms incorrectly filled out or incomplete (1) Baseline data Mean SCORAD index: Group A 33.28, Group B 34.60, Group C 34.50, Group D 35.18, Group E 35.91 |
|
| Interventions |
Intervention (Group A)
Comparator 1 (Group B)
Comparator 2 (Group C)
Comparator 3 (Group D)
Comparator 4 (Group E)
|
|
| Outcomes | Assessments (3): baseline, days 7 and 21 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared, but 3 investigators were employees of Laboratoires Expanscience, Epernon, France, manufacturer of the product under research | |
| Notes | STELATOPIA moisturiser, Mustela; Laboratoires Expanscience, France contains: 2% sunflower oleodistillate, essential fatty acids, bio‐ceramides, β‐sitosterol and a complex of emulsifying sugars We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 607): "randomly assigned...". "Each study center received one test kit containing five treatments. The five treatment options studies were successively allocated to patients according to chronological order of entry in the study. Patients were randomized based on chronological order of entry in the study" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "there was randomized attribution list, the order of attribution to different subjects was pre‐determined in a balanced fashion, following the attribution list" Comment: probably done |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: Central allocation, identical packages "On this pack, was only printed the number of chronological attribution to follow. The doctor did not know what was inserted in this pack (what protocol of emollient and steroid)" Comment: reasonable to assume allocation adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No reporting of measures used to blind study participants and personnel from knowledge of which intervention a participant received. Comment: the outcome was likely to be influenced by the lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | No blinding reported. Outcomes were investigator‐assessed as well as participant assessed. Comment: the outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported. After email communication: "One was lost to follow‐up. Two stopped prematurely the study for their own convenience (not for side effect). One file was not correctly filled and incomplete and was excluded from the analysis. So, we studied 86 children." Per‐protocol analysis. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Namazova‐Baranova 2012.
| Study characteristics | ||
| Methods | Open randomised, 'other moisturiser'‐controlled study Setting Institute of Preventive Pediatrics and Rehabilitation Scientific Center of Children's Health RAMS, Moscow, Russia Date of study Unspecified. Duration of intervention: 1 year |
|
| Participants | N = 44 (24 female, 20 male) Age range: 6 months to 12 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 44 (Locobase Repair group = 22, Atoderm group = 22) Withdrawals/losses to follow‐up 4/44 (9%); Locobase Repair group due to respiratory infection (1), Atoderm group due to protocol violation (1), worsening skin (2) Baseline data Median SCORAD: Locobase Repair group 38.3, Atoderm group 36.6 Mean daily consumption of topical corticosteroid: Locobase Repair group 2.8 g, Atoderm group 3.0 g Mean CDLQI: Locobase Repair group 15.83, Atoderm group 15.35 |
|
| Interventions |
Intervention
Comparator
As a basic therapy the participants received 0.1% hydrocortisone 17‐butyrate cream (Locoid) 1 to 3 times a day as needed. Systemic therapy in both groups was of antihistamines (cetirizine, levocetirizine) in dosages for age |
|
| Outcomes | Assessments (4): baseline, months 1, 6 and 12 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared | |
| Notes | Locobase Repair contains petrolatum, water, paraffin, liquid paraffin, glycerol, sorbitan oleate, carnauba wax, cholesterol, ceramides 3, oleic acid, palmitic acid, carbomer, tromethamine. Atoderm contains vaseline‐glycerol complex in dispersed state, sodium salt of EDTA, vitamin E, phenoxyethanol, parabens We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (translated from Russian): "All the children were randomly assigned into 2 groups of 22 people each" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "a computer generated randomisation list was used" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "sealed envelops for allocation, provided by research department" Comment: reasonable to assume allocation adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No reporting of measures used to blind study participants and personnel from knowledge of which intervention a participant received. Comment: the outcome was likely to be influenced by the lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | No blinding reported. Outcomes were investigator‐assessed as well as participant assessed. Comment: the outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 4/44 (9%), reasons reported, per‐protocol analysis. Comment: low number of losses to follow‐up, and although per‐protocol analysis, we considered this to be at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Nebus 2009.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐controlled study Setting Multicentre (2) in USA Date of study Unspecified. Duration of intervention: 8 weeks |
|
| Participants | N = 50 (gender not reported) Mean age = 29.8 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 50 (oatmeal group = 25, occlusive vehicle group = 25) Withdrawals/losses to follow‐up 3/50 (6%): all in occlusive vehicle group Baseline data IGA score: oatmeal group 2.58, occlusive vehicle group 2.58 Mean EASI: oatmeal group 6.55 (SD 5.10), occlusive vehicle 8.87 (SD 6.10) Mean DLQI: oatmeal group 5.96 (SD 5.80), occlusive vehicle 7.46 (SD 4.29) |
|
| Interventions |
Intervention
Comparator
Participants were allowed to use their normal topical medications for their atopic dermatitis |
|
| Outcomes | Assessments (3): baseline weeks 2, 4 and 8 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page AB67) "Commercial support: 100% sponsored by Johnson and Johnson Consumer Products Worldwide" | |
| Declaration of interest | None declared, but several investigators were employees of Johnson and Johnson Consumer Products Worldwide, the manufacturer of the drug under investigation | |
| Notes | Poster abstract with limited details provided. We received responses to our request for study details (Table 11). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page AB67): "multicenter, double‐blinded, randomized clinical study" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "The randomization was generated by SAS by a statistician. The method used to assign patients to treatment was a block design. Subjects were assigned in a 1:1 ratio to the two treatments, with a block size of 4." Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "The treatment codes (M and C) were kept in a sealed envelope by our clinical supplies department. The tubes were randomized labeled prior to sending to the investigator ‐ so subjects were dispensed treatment according to enrollment/randomization order. Both treatment creams were in the same 6 oz. beige tube, same cap color. Both creams were basically the same color and unfragranced". Comment: central allocation, de‐identified tubes. Allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page AB67): "double‐blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. After email communication: "Both treatment creams were in the same 6 oz. beige tube, same cap color. Both creams were basically the same color and unfragranced" Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page AB67): "double‐blind" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. After email communication: "Both treatment creams were in the same 6 oz. beige tube, same cap color. Both creams were basically the same color and unfragranced" Blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 3/50 (6%), all in the occlusive vehicle group. Intention‐to‐treat analysis performed. Comment: we considered this trial to be at a low risk of bias because the total number of dropouts was low, and intention‐to‐treat analysis was performed. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. We received additional information from the principal investigator. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Nho 2014.
| Study characteristics | ||
| Methods | Randomised, 'other moisturiser'‐controlled, within‐participant study Setting Multicentre, Korea Date of study Unspecified |
|
| Participants | N = 31, 5 participants had atopic dermatitis (gender not reported) Mean age not reported Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 31 to either side of the face (within‐participant), 5 participants had atopic dermatitis Withdrawals/losses to follow‐up Nothing reported Baseline data Nothing reported |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (2): baseline and week 2 Outcomes of the trial (as reported)
|
|
| Funding source | None declared | |
| Declaration of interest | None declared, but 3 authors were employees of R&I Center, Cosmax Co. Ltd, the manufacturer of the drug under investigation | |
| Notes | Three PPARα activators used (Euryale ferox, Euphorbia lathyris, Rosa multiflora) Only 5 participants met our inclusion criteria. No individual patient data (Table 13) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page S95): "were randomly applied on half of the face" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Nothing reported regarding blinding. Comment: the outcome was likely to be influenced by the lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Nothing reported regarding blinding. Outcomes were investigator‐assessed. Comment: the outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Little information provided. Comment: there was insufficient information to permit a clear judgement. |
| Selective reporting (reporting bias) | Unclear risk | Comment: there was insufficient information to permit a clear judgement. |
| Other bias | Unclear risk | Comment: there was insufficient information to permit a clear judgement. |
Noh 2011.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐controlled study Setting Department of Dermatology and Cutaneous Biology Research Institute, Yonsei University College of Medicine, Seoul, Korea Date of study Unspecified. Duration of intervention: 6 weeks |
|
| Participants | N = 40 (17 female, 23 male) Mean age = 12.95 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 40 (ceramide containing moisturiser group = 20, control moisturiser group = 20) Withdrawals/losses to follow‐up 8/40 overall (20%): ceramide containing moisturiser group (5), control moisturiser group (3)
Baseline data Mean EASI: ceramide containing moisturiser group 10.45 (SE 1.17), control moisturiser group 9.51 (SE 1.02) Mean TEWL (g/m²/h): ceramide containing moisturiser group 45 (SE 5), control moisturiser group 42 (SE 4) Mean corneometry units: ceramide containing moisturiser group 18 (SE 2), control moisturiser group 24 (SE 3) |
|
| Interventions |
Intervention
Comparator
Corticosteroid cream also applied (Zemaderm) twice daily for 6 weeks |
|
| Outcomes | Assessments (3): baseline, weeks 3 and 6 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared | |
| Notes | Atobarrier cream, ceramide‐containing moisturiser, APDDR‐0801. APDDR‐0801 is the research name of in the Atobarrier cream We received responses to our request for study details (Table 11) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 227): "randomized, controlled, double‐blinded" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "block randomization method" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "central randomization independent of researcher who's doing enrollment and also used coded container" Comment: central allocation, de‐identified drug containers. Allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 227): "double‐blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 227): "double‐blind" Outcomes were investigator‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 8/40 (20%); ceramide containing moisturiser group (5), control moisturiser group (3). Per‐protocol analysis. Comment: the total number of dropouts, combined with a per‐protocol analysis represented a high risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Nuñez 2013.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐controlled study Setting Multicentre (USA) Date of study Unspecified. Duration of intervention: 3 weeks |
|
| Participants | N = 49 (gender not reported) Age = 2 to 15 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 49 (colloidal oatmeal group = 25, prescription barrier repair cream group = 24) Withdrawals/losses to follow‐up 7/49 (14.3%), unclear from which group(s) Baseline data Mean EASI: colloidal oatmeal group 3.56 (SD 1.8), prescription barrier repair cream group 3.15 (SD 2.5) Mean VAS itch: colloidal oatmeal group 1.4 (SD 2.3), prescription barrier repair cream group 1.4 (SD 3.3) |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (4): baseline, weeks 1, 2 and 3 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page AB73): "This study was sponsored by Johnson & Johnson Consumer Companies, Inc." | |
| Declaration of interest | None declared, but 4 investigators were employees of Johnson & Johnson Consumer Companies, Inc, the manufacturer of the drug under investigation | |
| Notes | See Notes section of Characteristics of included studies of Draelos 2011 for details on EpiCeram. We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page AB73): "randomly assigned" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "Eligible subjects were randomly assigned to one of the two investigational products in a 1:1 ratio. The randomization scheme was generated by the Sponsor using the random number generating procedure in SAS (Statistical Analysis System) package" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "Eligible subjects were randomized in a sequential order. That is, the smallest random code in the randomization list was picked up and assigned to the next eligible subject. Thus, both subjects and investigator couldn't foresee the upcoming treatment assignment. J&J Clinical supply team completely overwrapped the products with plain white labels with study information printed on the white label. That would include randomization number, study site, PI phone number and instructions for use. We did not repackage the products from their original container" Comment: central allocation, de‐identified tubes. Allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Nothing reported regarding blinding. Comment: the outcome was likely to be influenced by the lack of blinding. After email communication: "double‐blind, products were overwrapped and randomization number and instructions for use were included on the overwrapped label" Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Nothing reported regarding blinding. Outcomes were investigator‐assessed and participant‐assessed. Comment: the outcome measurement was likely to be influenced by the lack of blinding. After email communication: "double‐blind, products were overwrapped and randomization number and instructions for use were included on the overwrapped label". Blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Little information provided. Comment: there was insufficient information to permit a clear judgement. After email communication: 7/49 (14.3%), unclear from which group. Intention‐to treat analysis Comment: we judged this as being at an unclear risk of bias. |
| Selective reporting (reporting bias) | Unclear risk | Comment: there was insufficient information to permit a clear judgement. After email communication: "The study was part of protocol (NCT01326910), there was an additional outcome provided in the protocol "Investigator's Global Atopic Dermatitis Assessment" Comment: as this was a poster presentation, and the sub‐study has not yet been published in full, we judged this as being at an unclear risk of bias. |
| Other bias | Unclear risk | Comment: there was insufficient information to permit a clear judgement. |
Park 2014.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐controlled, within‐participant study Setting Department of Dermatology, Chungnam National University School of Medicine, Daejeon, Korea Date of study June to November 2011. Duration of intervention: 4 weeks |
|
| Participants | N = 30 (20 female, 10 male) Mean age = 14.2 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 30 to either side of the body (within‐participant) Withdrawals/losses to follow‐up 2/30 (6.7%) lost to follow‐up Baseline data Mean IGA: treatment side 2.75 (SD 0.70), control side 2.71 (SD 0.66) Mean VAS: treatment side 6.53 (SD 1.77), control side 6.50 (SD 1.75) Mean TEWL (g/m²/h): treatment side 37.10 (SD 9.30), control side 34.30 (SD 8.40) Mean skin capacitance: treatment side 27.40 (SD 10.80), control side 28.90 (SD 10.00) |
|
| Interventions |
Intervention
Comparator
Continued use of antihistamines and topical steroids was permitted |
|
| Outcomes | Assessments (4): baseline, weeks 1, 2 and 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 155): "This study was supported by a grant from the Korea Ministry of Health and Welfare (A091121)" | |
| Declaration of interest | None declared | |
| Notes | We mailed investigators numerous times for more precise study details, but received no response (Table 11). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 151): "was randomly assigned" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 150): "double‐blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received on each part of the body, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcomes were investigator‐assessed as well as participant‐assessed.
Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2/30 (6.7%) lost to follow‐up. Per‐protocol analysis. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Patrizi 2008.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐ and vehicle‐controlled study Setting Two dermatological sites, Department of Specialistic and Experimental Clinical Medicine, Division of Dermatology, University of Bologna, Bologna, San Gallicano Dermatological Institute, Rome, Italy Date of study February 2005 to April 2006. Duration of intervention: 43 days |
|
| Participants | N = 60 (30 female, 30 male) Mean age = 5.5 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 60 (MAS063DP (Atopiclair) group = 20, MAS060 (Atopiclair light) group = 20, vehicle group = 20) Withdrawals/losses to follow‐up 14/60 overall (23.3%): MAS063DP group = 1/20 (5%), MAS060 group = 7/20 (35%), vehicle group = 6/20 (30%)
Baseline data Number of participants with:
|
|
| Interventions |
Intervention 1
Comparator 1
Comparator 2
Participants had to observe a 7‐ or 14‐day washout period if appropriate, and had to refrain from using other medications for the treatment of atopic dermatitis during the study. The use of other topical or systemic medications for the treatment of atopic dermatitis, and phototherapy were not permitted during the washout and study period. If atopic dermatitis was poorly controlled to the degree that additional therapy/rescue regimen was needed, then either hydrocortisone butyrate 0.1% or desonide 0.5% cream were allowed twice daily for 1 week. The use for rescue medication was an end‐point of the study |
|
| Outcomes | Assessments (7): baseline, days 1, 8, 15, 22, 29 and 43 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 625): "This study was supported by Sinclair Pharmaceuticals Ltd, Godalming Business Centre, Woolsack way, Godalming, GU7 1XW Surrey, UK" | |
| Declaration of interest | None declared | |
| Notes | MAS063DP = Atopiclair. See Notes section of Characteristics of included studies of Abramovits 2008 for details on Atopiclair. MAS060 = Atopiclair light, a water‐in‐oil formulation containing the same key ingredients of MAS063DP, but at lower concentration and with no preservatives Participants were also provided with a specific non medicated, fragrance‐free cleanser (Cetaphil; Galderma, Alby‐Sur‐Cheran, France) for the entire study duration |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 620): "The randomization list was generated by computer" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: sponsor provided numbered identical boxes containing the different products. Comment: central allocation, de‐identified boxes. Allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 620): "the tubes were labelled in a double‐blind manner" and "MAS063DP, MAS060 and vehicle were similar in consistency and in colour". Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page 620): "Investigators, patients and caregivers remained blinded" and "MAS063DP, MAS060 and vehicle were similar in consistency and in colour".
Outcomes were investigator‐assessed as well as participant‐assessed. Blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 14/60 (23.3%): MAS063DP group = 1/20 (5%), MAS060 group = 7/20 (35%), vehicle group = 6/20 (30%). Intention‐to‐treat analysis based on 57/60. Comment: although 'modified' intention‐to‐treat analysis, the high number of losses to follow‐up posed an unclear risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Patrizi 2014.
| Study characteristics | ||
| Methods | Randomised, open, controlled study Setting Multicentre (3) in Italy and Romania Date of study Unspecified. Duration of intervention: 28 days |
|
| Participants | N = 55 (gender not reported) Mean age = 2.5 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 55 (emollient balm group = 28, control group = 27) Withdrawals/losses to follow‐up 1/55 (1.8%), from control group Baseline data Mean SCORAD: emollient balm group 11.7 (SD 3.1), control group 10.2 (SD 3.3) Mean pruritus intensity: emollient balm group 1.67 (SD 1.20), control group 1.77 (SD 1.52) Mean TEWL (g/m²/h): emollient balm group 35.46 (SD 20.90), control group 21.55 (SD 9.43) |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (3): baseline, days 15 and 28 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 170 of co‐publication Bianchi 2016, under primary reference): "The study was funded and conducted by Pierre Fabre Dermo‐Cosmetique" | |
| Declaration of interest | Quote (page 170 of co‐publication Bianchi 2016, under primary reference): "P. Bianchi, J. Theunis, C. Casas, C. Villeneuve, C. Phulpin, A. Bacquey, D. Redoules, V. Mengeaud, and A‐M Schmitt are employees of Pierre Fabre Dermo‐ Cosmetique. The principal investigator, Dr. Patrizi, signed a contract with Pierre Fabre Dermo‐Cosmetique for this study" | |
| Notes | The study product (Avene Xeracalm balm; Pierre Fabre Dermo Cosmetique, Boulogne, France) was an oil‐in‐water emulsion. The associated hygiene product (emollient cleansing gel; Trixera; Pierre Fabre Dermo, Boulogne, France) was indicated for dry and atopic skin and was used for bathing and then rinsed off once a day. We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 170 of co‐publication Bianchi 2016): "were randomized to receive" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "The randomization list was generated by the Pierre Fabre Biometrie Department. Our statistical department used a specific software to generate the randomization list" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "The randomization list was not given to the investigator. Only sponsor had access to this list and could see it" Comment: central allocation, allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote (page AB62): "open, randomized" Comment: the outcome was likely to be influenced by the lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote (page AB62): "open, randomized" Outcomes were investigator‐assessed and participant‐assessed. Comment: the outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 1/55 (1.8%), from control group. Per‐protocol analysis. Comment: low number of losses to follow‐up, and although per‐protocol analysis considered as at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Peltonen 2014.
| Study characteristics | ||
| Methods | Three randomised, double‐blind, vehicle‐controlled, within‐participant studies, only 1 of which was in atopic dermatitis Setting Department of Physiology, Institute of Biomedicine, University of Turku, Turku, Finland Date of study October 2008 to May 2009. Duration of intervention: 28 days |
|
| Participants | N = 14 (9 female, 5 male) Mean age = 28 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 14 to either forearm (within‐participant) Withdrawals/losses to follow‐up 2/14 (14.3%): withdrew consent (1), and worsening eczema (1) Baseline data Mild atopic dermatitis: 10/13 Moderate atopic dermatitis: 3/13 |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (3): baseline, weeks 2 and 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 420): "The 3 studies were funded by BioCis Pharma Ltd" | |
| Declaration of interest | Quote (page 420): "The authors LP, LL, and JKL were employees of BioCis Pharma Ltd at the time the studies were conducted. LL and JKL are also shareholders and patent inventors for BioCis Pharma Ltd" | |
| Notes | 5% (w/w) cis‐UCA emulsion cream (BioCis Pharma, Turku, Finland) and the same vehicle emulsion cream base (Orion, Espoo, Finland). The cream base contained aqua, decyl oleate, cetearyl alcohol, glycerol, sodium cetearyl sulphate, and methyl paraben. Both products were pH 6.5. Data needed to be estimated from figures (TEWL), otherwise no precise data were provided other than the statement that "there were no significant differences." We mailed investigators numerous times for more precise study details, but received no response (Table 11; Table 13). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 415): Randomisation was performed by computer‐generated (SAS System, Cary, NC, USA) lists by a randomisation expert with no clinical involvement in the trials" Comment: probably done. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 415): "the investigators, and the study site personnel were blinded for the identity of the treatments" and "The products were packed in identical tubes labelled for either arm for each subject number" Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page 415) "The products were packed in identical tubes labelled for either arm for each subject number" Blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 2/14 (14.3%): withdrew consent (1), and worsening eczema (1). Per‐protocol analysis Comment: moderate number of dropouts at follow‐up combined with the per‐protocol analysis posed an unclear risk of bias for this domain. |
| Selective reporting (reporting bias) | Unclear risk | The protocol for the study was available (Eudra‐2008‐005075‐10). Not all the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. Data on skin swelling, formation of papules, formation of vesicles or bullae, and scaling were missing. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Peserico 2008.
| Study characteristics | ||
| Methods | Two‐phase randomised, double‐blind, active‐controlled study Setting Multicentre (20) in Germany, Italy and Spain Date of study August 2005 to January 2006. Duration of intervention: acute treatment phase of up to 4 weeks and a 16‐week maintenance phase |
|
| Participants | N = 249 in acute treatment phase, and 221 in maintenance phase (142 female, 79 male) Mean age = 30.9 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 221 (moisturiser group = 109, MPA group = 112) Withdrawals/losses to follow‐up 8/221 overall (3.6%): moisturiser group = 3, MPA group = 5
Baseline data at start maintenance phase Mean EASI: moisturiser group 1.4, MPA group 1.6 Mean itching: moisturiser group 8.7, MPA group 10.1 |
|
| Interventions | First phase open‐label methylprednisolone aceponate (MPA) cream once a day as well as open‐label moisturiser once a day for a maximum of 4 weeks Second, maintenance phase: Intervention
Comparator
|
|
| Outcomes | Assessments (5): baseline, weeks 2, 6, 10 and 16 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 806): "This study was sponsored by Intendis GmbH, Berlin" | |
| Declaration of interest | None declared, but 1 of the authors was an employee at Intendis GmbH, Berlin, manufacturer of Advabase | |
| Notes | Advabase, Intendis GmbH, Berlin, Germany contains aqua, decyl oleate, glyceryl stearate, caprylic/capric/stearic triglyceride, glycerol, cetearyl alcohol, hydrogenated coco‐glycerides, benzyl alcohol, disodium EDTA, BHT We had email communication with the corresponding author, but he could not help us with missing trial details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 802): "Randomization at the end of the AP [acute treatment phase] was carried out in blocks according to the patients' arrival at the study centre and aimed to achieve a 1:1 randomization ratio overall and within each centre" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 801): "double‐blind" and "MP medication was packed in identical tubes to ensure blinding" In view of the difference in number of tubes (1 or 2) in the interventions groups it remains unclear if blinding was effective. Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 801): "double‐blind" and "MP medication was packed in identical tubes to ensure blinding". In view of the difference in number of tubes (1 or 2) in the interventions groups it remains unclear if blinding was effective. Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 8/221 (3.6%); moisturiser group = 3, MPA group = 5. Both intention‐to‐treat analysis and per‐protocol analysis. Comment: low number of losses to follow‐up, and combined with both intention‐to‐treat as well as per‐protocol analysis meant we considered this trial as being at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Pigatto 1996.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐controlled study Setting Department of Dermatology, University and Ospedale Maggiore IRCCS of Milan, Milan, and S Gallicano Dermatological Institute, Rome, Italy Date of study Unspecified. Duration of intervention: 1 month |
|
| Participants | N = 70 (30 healthy adults: 8 female, 22 male, and 40 adults with atopic dermatitis: 10 female, 30 male) Age range = 27 to 45 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 70 unclear how many randomised to each treatment arm Withdrawals/losses to follow‐up Not reported Baseline data Not reported |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (2): baseline, week 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared | |
| Notes | Cream containing urea (Laceran, Beiersdorf AG) and Essex Base Cream containing white petrolatum, paraffin, cresol chloride and polyethylene glycol (Schering‐Plough) Unclear how many were randomised to each treatment arm, no separate data for healthy and atopic adults (Table 13) As the study was 20 years old we did not contact the investigators for data. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 171): "The patients and controls were assigned randomly to one or the other treatment" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 171): "Patients, normal controls and the physicians (AB and CC) who examined them were blind to the treatments" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 171): "Patients, normal controls and the physicians (AB and CC) who examined them were blind to the treatments" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Nothing reported, little information provided. Comment: there was insufficient information to permit a clear judgement. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Unclear risk | Comment: there was insufficient information to permit a clear judgement. |
Puschmann 2003.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐controlled study Setting Klinik für Dermatologie und Venereologie der Universität Lubeck, Germany Date of study Unspecified. Duration of intervention: 2 weeks |
|
| Participants | N = 54 (20 healthy participants, 34 participants with atopic dermatitis, gender not reported) Mean age not reported Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 54 unclear how many to each treatment arm Withdrawals/losses to follow‐up 5/54 (9.3%) reasons unreported Baseline data Nothing reported |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (3): baseline, weeks 1 and 2 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared, but Dr Puschmann was employed by HERMAL, the manufacturer of the moisturiser under investigation, therefore the trial was likely to have been funded by HERMAL Kurt Herrmann GmbH & Co, Reinbek | |
| Declaration of interest | None declared, but Dr Puschmann was employed by HERMAL Kurt Herrmann GmbH & Co, Reinbek, the manufacturer of the moisturiser under investigation | |
| Notes | Commercial cream contains polidocanol 3% and urea 5%, water, octyl dodecanol, polymethylphenylsiloxane, stearin palm, dimethicone, glycerol, paraffin, hexadecyl palmitate, polysorbate 40, carbomer, benzyl alcohol, and trometamol. The products differ chiefly in the number of carbomers the molecules contain. Unclear how many were randomised to each treatment arm, no separate data for healthy participants and atopic participants (Table 13) As the study was 13 years old we did not contact the investigators for data. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 78): "einer doppelblinden, randomisierten" (translation: double‐blind, randomised) Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 78): "doppelblinden" (translation: double‐blind) Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 78): "doppelblinden" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 5/54 dropouts (9.3%): reasons unreported, unclear from which treatment arm(s) they came, little information provided. Per‐protocol analysis. Comment: there was insufficient information to permit a clear judgement. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Shi 2015.
| Study characteristics | ||
| Methods | Randomised, participant‐blinded, controlled, within‐participant study Setting Multicentre, Sacramento, California, USA Date of study January 2014 to May 2015. Duration of the intervention 10 minutes |
|
| Participants | N = 20 of which 10 had atopic dermatitis and 10 were healthy subjects (9 female, 11 male) Mean age = 26.3 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 20 to either forearm (within‐participant) Withdrawals/losses to follow‐up No losses to follow‐up reported Baseline data of 10 participants with atopic dermatitis Severity of eczema: mild (n = 5), moderate (n = 3), severe (n = 2) Mean TEWL (g/m²/h): bleach side 12.58 (SD 8.74), water side 11.89 (SD 8.64) Mean corneometry units: bleach side 23.66 (SD 11.38), water side 24.47 (SD 10.44) |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (4): baseline, 15 minutes, 30 and 60 minutes Outcomes of the trial(as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page AB76): "Commercial support: None identified" | |
| Declaration of interest | None declared | |
| Notes | Poster abstract. We received responses to our request for study details (Table 11). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page AB76): "randomized controlled study" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "The allocation sequence was generated a priori with binary randomization generator." Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication (and in Shi 2016): "The randomization was performed prior to recruitment by the study coordinator, and stored in sealed envelopes that were not opened until the subject was recruited by the investigators." Comment: allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | According to protocol (NCT02594969 available at clinicaltrials.gov): "participant‐blinded" and "Participants remained blinded to the water or dilute hypochlorite immersion". Investigators were not blinded. Comment: the outcome was likely to be influenced by the lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Outcomes were investigator‐assessed. Comment: the outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up. |
| Selective reporting (reporting bias) | Low risk | The protocol was available (NCT02594969 available at clinicaltrials.gov), and the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Shiratori 1977.
| Study characteristics | ||
| Methods | Randomised, double‐blind, active‐ and vehicle‐controlled, within‐participant study Setting Multicentre (25) in Japan Date of study Unspecified. Duration of intervention: 4 weeks with 2 months of follow‐up |
|
| Participants | N = 552 (gender not reported) Mean age not reported Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 552 to either side of the body (within‐participant) Withdrawals/losses to follow‐up 61/552 (11%), unclear from which groups, due to:
Baseline data of per‐protocol population Ichtyosis vulgaris (137), senile xerosis (170), atopic skin (184) |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (5): baseline, weeks 1, 2, 3 and 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared | |
| Notes | The data were confusingly reported in this study and did not lend themselves to further analysis (Table 13). As the study was 39 years old we did not contact the investigators for data. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 104): "doubleblind randomised control trial" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 104): "doubleblind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received on each side of the body, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 104): "doubleblind" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 61/552 (11%), unclear from which groups. Per‐protocol analysis. Comment: we judged this to be at an unclear risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Simpson 2011.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, controlled, within‐participant study (study D) Setting Multi‐centre (3) in USA Date of study Unspecified. Duration of intervention: 4 weeks |
|
| Participants | N = 127 (gender not reported) Mean age not reported Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 127 to either side of the body (within‐participant) Withdrawals/losses to follow‐up 4/127 (3%), reasons unreported Baseline data Mean corneometry units: Cetaphil RestoraDerm moisturiser side 42.5, control 41.8 |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (5): days 0, 7, 14, 21 and 28 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 748): "The studies were supported by Galderma R & D" | |
| Declaration of interest | Quote (page 748): "Dr Simpson is a consultant for Galderma. Dr Dutronc is an employee of Galderma" | |
| Notes | This reference includes data on 4 studies, of which only study D matched our inclusion criteria Cetaphil RestoraDerm contains aqua, glycerol, caprylic/capric triglyceride, Helianthus annus (sunflower) seed oil, pentylene glycol, Vitellaria paradoxa (formerly called Butyrospermum parkii; shea butter), sorbitol, cyclopentasiloxane, cetearyl alcohol, behenyl alcohol, glyceryl stearate, tocopheryl acetate, hydroxypalmitoyl sphinganine, niacinamide, allantoin, panthenol, arginine, disodium ethylene dicocamide PEG‐15 disulfate, glyceryl stearate citrate, sodium PCA, ceteareth‐20, sodium polyacrylate, caprylyl glycol, citric acid, dimethiconol, disodium EDTA, sodium hyaluronate, cetyl alcohol We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 745): "...randomized..." Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "This was a left/right comparison study, comparing treatment with Cetaphil cream on one side of the body versus no treatment on the contralateral side. The allocation of treatments (Cetaphil cream or no treatment) was randomized and the allocation sequence was generated by an independent statistician" Comment: probably done |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "The study medications were dispensed by someone other than the investigator designated as Study Drug Dispenser. The randomization list was secured in a locked cabinet and in an electronic file with restricted access to only the designated personnel directly responsible for labelling and handling the study medications, until the study database was locked and ready to be unblinded." Comment: reasonable to assume allocation adequately concealed. We judged this as at a low risk of bias. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 745): "evaluator‐blinded" Comment: participants were not blinded. The report provided insufficient detail about the measures used to blind study personnel from knowledge of which intervention a participant received on each side of the body, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote (page 745): "evaluator‐blinded"
Outcomes were investigator‐assessed and participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (healthcare providers) during the study, and participants were not blinded. The outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 4/127 (3%), reasons unreported. Per‐protocol analysis. Comment: low number of losses to follow‐up, and although per‐protocol analysis, we considered this to be at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Simpson 2013.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, controlled (inactive), within‐participant study Setting Pro‐DERM Institute in Germany Date of study December 2010 to February 2011. Duration of intervention: 27 days |
|
| Participants | N = 20 (16 female, 4 male) Mean age = 40.9 years Inclusion criteria of the trial
Exclusion criteria of the trial1
Randomised N = 20 to either leg (within‐participant) Withdrawals/losses to follow‐up No losses to follow‐up reported Baseline data Mean dryness: CRM‐treated area 2.05 (SD 0.63), untreated area 2.07 (SD 0.63) Mean skin hydration (corneometry units): CRM‐treated area 17.77 (SD 5.24), untreated area 18.25 (SD 5.91) Mean TEWL (g/m²/h): CRM‐treated area 5.15 (SD 1.53), untreated area 15.32 (SD 1.73) |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (2): baseline and day 28 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared but the manufacturer of the drug under investigation is Galderma, R&D, Sophia Antipolis, France | |
| Declaration of interest | Quote (page 125): "Dr. Simpson is a consultant for Galderma, and Dr. Böhling and Mr. Bielfeldt received investigator fees for this research study. Ms. Bosc and Mr. Kerrouche are employees of Galderma" | |
| Notes | Cetaphil Restoraderm Body Moisturiser (CRM – Galderma S.A.) contains filaggrin breakdown products (components of NMF), ceramide precursor, and niacinamide, fatty acids, humectants, filmogenic substances, emollients, and shea butter. CRM contains no fragrances and has a pH of approximately 5.5 We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 122): "statistician generated a randomization list" and "randomly assigned to the right or left lower leg (for each subject, one 4x4 cm area treated with CRM and one symmetric untreated control area) with a block size of four subjects" Comment: probably done |
| Allocation concealment (selection bias) | Low risk | Quote (page 122): "a statistician generated a randomization list and each bottle of product was identified by a randomization number and was labeled with the side to be treated...The randomization list was kept under restricted access until the study database was locked and ready to be unblinded for statistical analyses" Comment: central allocation, de‐identified bottles. Allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 122): "investigator‐blinded"; participants were not blinded. Comment: the report did not provide sufficient detail about the specific measures used to blind study personnel from knowledge of which intervention a participant received on each leg, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 122): "investigator‐blinded"; participants were not blinded. Outcomes were (mainly) investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Sugarman 2009.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, active‐controlled study Setting Multicentre (5) in USA Date of study December 2006 to February 2007. Duration of intervention: 4 weeks |
|
| Participants | N = 121 (73 female, 48 male) Mean age = 7.1 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 121 (barrier repair group = 59, fluticasone group = 62) Withdrawals/losses to follow‐up 12/121 overall (9.9%); barrier repair group = 6/59, fluticasone group 3/62
Baseline data Mean SCORAD: barrier repair group 37.2, fluticasone group 33.8 Mean self‐assessment: barrier repair group 0.1 (SD 0.40), fluticasone group 0.11 (SD 0.46) |
|
| Interventions |
Intervention
Comparator
Cetaphil lotion was applied to clinically uninvolved areas twice daily |
|
| Outcomes | Assessments (3): baseline, days 14 and 28 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 1110): "company‐sponsored study (Ceragenix Corporation, Dever, CO) | |
| Declaration of interest | Quote (page 1110): "Neither of the authors is a consultant or shareholder at Ceragenix" | |
| Notes | See Notes section of Characteristics of included studies of Draelos 2011 for details on EpiCeram. We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 1107): "were assigned randomly at entry" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "A central randomization schedule was produced providing random allocation to the two treatment groups. A block size of 4 will be used in the generation of the randomization code" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "central allocation by sponsor" Comment: allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 1106): "investigator‐blinded". Participants were not blinded, quote (page 1107) "the subjects could not be blinded" Comment: the report did not provide sufficient detail about the specific measures used to blind study personnel from knowledge of which intervention a participant received, to permit a clear judgement. After email communication: "The person dispensing the study medication and performing ongoing study medication accountability will NOT perform any of the efficacy assessments required by the protocol" Comment: the report provided sufficient detail about the measures used to blind study personnel from knowledge of which intervention a participant received, however, participants were not blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote (page 1106): "investigator‐blinded" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: blinding of the outcomes assessors, was ensured but participants and parents were not blinded. The outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 12/121 (9.9%), reasons reported. Intention‐to‐treat analysis. Comment: low number of losses to follow‐up, combined with intention‐to‐treat analysis, meant we considered this domain to be at a low risk of bias. |
| Selective reporting (reporting bias) | Unclear risk | The protocol for the study was available (NCT00616538) and the prespecified outcome "Patient/family self assessments of improvement" and "IGA" mentioned in the methods section was inadequately reported ("demonstrated highly significant improvement") Comment: we judged this as being at an unclear risk of bias. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Takeuchi 2012.
| Study characteristics | ||
| Methods | Two‐phase, randomised, open‐label, active‐controlled study Setting Multicentre (8) in Japan Date of study Unspecified. Induction phase 1‐4 weeks, maintenance phase > 4 weeks |
|
| Participants | N = 70 (37 female, 33 male) Mean age = 31 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 70 (induction phase: moisturiser group = 35, tacrolimus group = 35; maintenance phase moisturiser group = 21, tacrolimus group = 23) Withdrawals/losses to follow‐up Induction phase 2/70 (2.9%): 1 in each group and in 24 the VAS‐itch score did not reduce by more than 20 and did not make it to maintenance phase, 1 refused to continue Maintenance phase 1/43 (2.3%): in moisturiser group Baseline data Mean itch (VAS): moisturiser group 19.3 (SD 16.7), tacrolimus group 28.1 (SD 15.4) |
|
| Interventions | Phase 1: induction phase, all participants received topical tacrolimus (0.03% < 16 years old and 0.1% otherwise). Moisturisers twice daily in addition to usual topical corticosteroid treatment (maximum use, 10 g/week). Participants who showed a reduced VAS‐itch score by > 20 points were considered to show relief from pruritus, and only these induction therapy responders proceeded into maintenance treatment Phase 2: maintenance phase Intervention
Comparator
|
|
| Outcomes | Assessments (2): baseline and day 28 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 150): "This work was supported by research grants from the Ministry of Health, Labour and Welfare, Japan" | |
| Declaration of interest | None declared | |
| Notes | We only include data on phase 2, the maintenance phase of the study We mailed investigators numerous times for more precise study details, but received no response (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 146): "random allocated" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote (page 144): "open‐label" Comment: the outcome was likely to be influenced by the lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote (page 144): "open‐label" Outcomes were investigator‐assessed as well as participant assessed. Comment: the outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | We only include data on maintenance phase, 1/43 dropped out in the moisturiser group. Without further information regarding the maintenance phase (the number initially randomised, do not match the number in the maintenance phase). |
| Selective reporting (reporting bias) | High risk | Atopic dermatitis severity score (SCORAD), was a predefined outcome in the Methods section, but was not reported for the maintenance phase. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Tan 2010.
| Study characteristics | ||
| Methods | Randomised, double‐blind, vehicle‐controlled study Setting National Skin Centre, Singapore Date of study Unspecified. Duration of intervention: 41 days |
|
| Participants | N = 60 (21 female, 39 male) Mean age = 18 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 60 (study cream group = 30, vehicle group = 30) Withdrawals/losses to follow‐up No losses to follow‐up Baseline data Mild atopic dermatitis (number of participants): study cream group (7), vehicle group (7) Moderate atopic dermatitis (number of participants): study cream group (23), vehicle group (23) Mean SCORAD: study cream group 28.85, vehicle group 29.51 |
|
| Interventions | For ethical reasons and recruitment effectiveness, all participants were provided with 0.025% betamethasone valerate cream, for the first 27 days. Following this, participants who still had persistent eczema were allowed to continue use of the steroid if necessary, which most did. Intervention
Comparator
Participants were provided with emulsifying ointment as cleansers throughout the study period and were instructed not to use any systemic or topical antibiotics, antibacterial soap or antibacterial shampoo until the end of study |
|
| Outcomes | Assessments (4): baseline, days 14, 27 and 41 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page e109): "This study was sponsored by Hygieia Healthcare Ltd" | |
| Declaration of interest | None declared | |
| Notes | All participants underwent a washout period of 1 week during which no topical corticosteroid was allowed. We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page e110): "Patients were assigned to one of two treatment groups according to a computer‐generated randomization list, stratified according to disease severity" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "Pharmaceutical company prepared identical labelled bottles" Comment: central allocation, de‐identified bottles. Allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page e109 and e110): "double‐blind" and "All study personnel and physicians remained blinded to allocation of treatment until completion of data analysis. Both the study cream and vehicle were odourless, of the same appearance and consistency, and provided in identical bottles" Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page e109 and e110): "double‐blind" and "All study personnel and physicians remained blinded to allocation of treatment until completion of data analysis. Both the study cream and vehicle were odourless, of the same appearance and consistency, and provided in identical bottles" Outcomes were investigator‐assessed as well as participant‐assessed. Blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Thumm 2000.
| Study characteristics | ||
| Methods | Randomised, double‐blind, active‐ and placebo‐controlled study Setting Klinikum Mannheim gGmbH, Universitätsklinikum, Fakultät für Klinische Medizin Mannheim der Universität Heidelberg, Germany Date of study Unspecified. Duration of intervention: 4 weeks |
|
| Participants | N = 58 (40 female, 18 male) Mean age = 31.1 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 58 (sea buckthorn oil (Hippophae rhamnoides oil) 10 % group = 17, sea buckthorn oil 20% group = 17, placebo group = 19, 5 unclear) Withdrawals/losses to follow‐up 5/58 (8.6%), reasons unreported and unclear from which groups Baseline data Nothing reported |
|
| Interventions |
Intervention
Comparator 1
Comparator 2
Application frequency unclear |
|
| Outcomes | Assessments (5): baseline, weeks 1, 2, 3 and 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared, but 1 of the authors was an employee of Weleda AG, Schwabisch Gmund, the manufacturer of the product under investigation | |
| Notes | As the study was 16 years old we have not contacted the investigators for data | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 285): "randomized" and on page 287 "nach dem Zufallsprinzip" (translation: at random) Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 285): "double blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Outcomes were investigator‐assessed as well as participant‐assessed.
Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 5/58 (8.6%) lost to follow‐up, reasons unreported and unclear from which groups. Per‐protocol analysis Comment: low number of losses to follow‐up, and although per‐protocol analysis, we considered this domain to be at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Tripodi 2009.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐controlled study Setting Multicentre Rome, Italy Date of study Unspecified. Duration of intervention: 2 weeks |
|
| Participants | N = 117 (46 female, 71 male) Mean age = 4.3 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 117 (furfuryl palmitate enriched moisturiser group = 57, moisturiser group = 60) Withdrawals/losses to follow‐up 29/117 overall (24.8%); furfuryl palmitate enriched moisturiser group 18/57, moisturiser group 11/60
Baseline data Mean SCORAD: furfuryl palmitate enriched moisturiser group 28.1 (SD 10.6), moisturiser group 25.6 (SD 10.1) |
|
| Interventions |
Intervention
Comparator
Treatment with systemic or topical corticosteroids, topical immunomodulators, and topical or oral antihistamines was not allowed. |
|
| Outcomes | Assessments (3): baseline, weeks 1 and 2 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared, however, quote (page 207): "Both products were provided by the same manufacturer (ICIM International Srl, Milan, Italy)" | |
| Declaration of interest | None declared | |
| Notes | Moisturiser containing various antioxidant molecules (superoxide dismutase, 18‐ß‐glycyrrhetinic acid, vitamin E, and α‐bisabolol). Furfuryl palmitate enriched formulation was same moisturiser with addition of furfuryl palmitate We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 206): "Randomization was performed using a computer‐generated list" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "Each tube had a letter "A" or "B", and we assigned the cream preparation to the patients on the basis of computer randomization list made directly by the Producer and sent to the each center before starting the trial. Obviously the investigators did not know if "A" or "B" was the active or not" Comment: central allocation, de‐identified tubes; allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 207): "The study was double blind, with the key code disclosed only after statistical evaluations. The 2 topical products had an identical color, smell, and consistency and were indistinguishable to both parents and examining pediatricians" Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page 207): "The study was double blind, with the key code disclosed only after statistical evaluations. The 2 topical products had an identical color, smell, and consistency and were indistinguishable to both parents and examining pediatricians" Outcomes were investigator‐assessed as well as participant‐assessed. Blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 29/117 (24.8%) lost to follow‐up; furfuryl palmitate‐enriched moisturiser group 18/57, moisturiser group 11/60, reasons reported. Per‐protocol analysis. Comment: the total number of dropouts, combined with a per‐protocol analysis represents a high risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Udompataikul 2011.
| Study characteristics | ||
| Methods | Randomised, investigator‐blinded, active‐controlled, within‐participant study Setting Skin Center, Faculty of Medicine, Srinakharinwirot University, Bangkok, Thailand Date of study Unspecified. Study duration 6 weeks |
|
| Participants | N = 30 (12 female, 14 male and 4 gender unknown)
Mean age = 5.8 years (2 months to 10 years) Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 30 to either body side (within‐participant) Withdrawals/losses to follow‐up 4/30 (13%): bacterial folliculitis (1) incomplete follow‐up (3) Baseline data Mean SCORAD: licochalcone A side 28.28, hydrocortisone acetate 1% side 28.52 |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (6): efficacy for the first 4 weeks; 2 weeks of relapse‐rate Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared. However, the study design is identical ‐ with a similar comparison with licochalcone ‐ to Angelova‐Fischer 2014 and Wanakul 2013, which were sponsored by Beiersdorf. | |
| Declaration of interest | Quote (page 660): "No conflict of interest" | |
| Notes | Licochalcone in ceramide and linoleic acid lipid base formulation (Eucerin Soothing lotion 12% omega, Beiersdorf, Germany). Licochalcone A is an extract from Glycyrrhiza inflata (Chinese liquorice) that has anti‐inflammatory property We received several responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 661): "Treatment was randomly assigned by a third party" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | Quote (page 661): "The trial codes were broken only after data were analyzed" The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 660‐661): "investigator‐blinded and "The tubes were similar in shape and colour" Comment: the report provided sufficient detail about the measures used to blind study personnel from knowledge of which intervention a participant received on each side of the body, however, participants were not blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote (page 660): "investigator‐blinded" Outcomes were investigator and participant‐assessed. Blinding of key study personnel was ensured, and it is unlikely that the blinding could have been broken, however participants were not blinded. Comment: we judged this domain to be at a high risk of bias. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 4/30 (13%) lost to follow‐up; bacterial folliculitis (1) incomplete follow‐up (3) low number, and per‐protocol analysis. Comment: moderate number of losses to follow‐up, combined with per‐protocol analysis, so we considered domain to be at an unclear risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | The study appears to be free of other forms of bias. |
Verallo‐Rowell 2008.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐controlled study Setting Two outpatient dermatology clinics Makati City, Philippines Date of study Unspecified. Study duration 4 weeks |
|
| Participants | N = 52 (25 female, 27 male) Mean age = 32 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 52 (virgin coconut oil group = 26, virgin olive oil group = 26) Withdrawals/losses to follow‐up No dropouts or protocol violators Baseline data Mean objective SCORAD: virgin coconut oil group 39.2 (SD 6.4), virgin olive oil group 36.6 (SD 6.3) Colonisation with Stapylococcus aureus: virgin coconut oil group 20/26, virgin olive oil group 12/26 |
|
| Interventions |
Intervention
Comparator
No other moisturisers, creams, or oil‐based products were allowed |
|
| Outcomes | Assessments (2): baseline and week 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 309): "the randomization key, and the codes were carried out by the pharmacist of Skin Sciences Laboratory, Inc., and was disclosed to the investigators only at the end of the study" and "underwent simple concealed random allocation (by drawing rolled pieces of paper labeled "A" or "B") to control or treatment arms by the two dermatology residents, both of whom were blind to the codes" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | Quote (page 309): "the randomization key, and the codes were carried out by the pharmacist of Skin Sciences Laboratory, Inc., and was disclosed to the investigators only at the end of the study" and "repackaged in uniform medicinal opaque plastic bottles with a small opening to mask the color and scent of both oils" Comment: central allocation, de‐identified bottles; allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 208‐209): "double‐blind" and "repackaged in uniform medicinal opaque plastic bottles with a small opening to mask the color and scent of both oils" Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement of low risk. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page 208‐209): "double‐blind" and "repackaged in uniform medicinal opaque plastic bottles with a small opening to mask the color and scent of both oils" Outcomes were investigator‐assessed. Comment: the report provided sufficient detail about the measures used to blind outcomes assessors from knowledge of which intervention a participant received, to permit a clear judgement of low risk. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote (page 311 ): "There were no dropouts or protocol violators" |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the outcomes mentioned in the Methods section appeared to have been reported. |
| Other bias | Unclear risk | There was baseline imbalance regarding colonisation with S aureus in favour of the virgin oil group (77% versus 46%). |
Wanakul 2013.
| Study characteristics | ||
| Methods | Randomised, double‐blind, active‐controlled, within‐participant study Setting Multicentre (4) in Bangkok, Thailand Date of study March 2010 to December 2011. Duration of intervention: 4 weeks followed by 4 weeks open label licochalcone A |
|
| Participants | N = 55 (28 female, 27 male) Mean age = 3.1 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 55 to either side of the body (within‐participant) Withdrawals/losses to follow‐up 3/55 (5.5%), reasons unreported Baseline data Mean SCORAD: licochalcone side 26 (SD 8.8), hydrocortisone 1% side 26 (SD 9.8) Mean TEWL (g/m²/h): licochalcone side 29 (SD 12.1), hydrocortisone 1% side 27 (SD 14.0) |
|
| Interventions |
Intervention
Comparator
After 4 weeks both sides were treated with licochalcone A lotion. We only include the first 4 randomised weeks. |
|
| Outcomes | Assessments (3): baseline, weeks 2 and 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 1140): "The present study was supported by Beiersdorf (Thailand) Co. Ltd. The sponsor had no influence on study design, data collection, and data analyses" | |
| Declaration of interest | None declared | |
| Notes | Licochalcone in ceramide and linoleic acid lipid base formulation (Eucerin Soothing lotion 12% omega, Beiersdorf, Germany). Licochalcone A is an extract of Glycyrrhiza inflata (Chinese liquorice) that has anti‐inflammatory property | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 1136): "The assignment of applying the test substance was performed by block randomization by the principal investigator to all four sites before the present study was started" Comment: probably done. |
| Allocation concealment (selection bias) | Unclear risk | Quote (page 1136): "These code numbers were assigned sequentially so that the patients were enrolled in each site" and "supplied in similar containers" Comment: although this suggests central allocation with delivering de‐identified containers to the 4 study sites, the principal investigator generated the randomisation sequence and it remains unclear whether the allocation sequence was adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 1136): "During the present study, investigators and patients were blinded regarding the use of either moisturizer containing Lic A lotion or 1% hydrocortisone lotion, which were supplied in similar containers" Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received on each side of the body, to permit a clear judgement of low risk. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page 1136): "During the present study, investigators and patients were blinded regarding the use of either moisturizer containing Lic A lotion or 1% hydrocortisone lotion, which were supplied in similar containers" Outcomes were investigator‐assessed as well as participant‐assessed. Blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 3/55 (5.5%) lost to follow‐up, reasons unreported. Per‐protocol analysis Comment: low number of losses to follow‐up, and although per‐protocol analysis, we considered this domain to be at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the outcomes mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | The study appears to be free of other forms of bias. |
Weber 2015.
| Study characteristics | ||
| Methods | Randomised, controlled (inactive), study Setting Single dermatology centre, Colorado Springs, CO, USA Date of study Unspecified. Duration of intervention: 6 months (study consisted of 3 phases, we only included the second, i.e. the maintenance phase) |
|
| Participants | N = 45 (21 female, 24 male) Mean age = 3.5 years (7 months to 11 years 5 months) Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 45 (moisturiser group = 21, control group = 24) Withdrawals/losses to follow‐up 2/45 overall (4.4%); moisturiser group 1/21, control group 1/24
Baseline data "The eczema history questionnaire completed at baseline showed that 78% of subjects had flared 3 to 4 times in the previous 12 months, while 18% had flared 1 to 2 times during this time period" |
|
| Interventions | Washout phase of 2 weeks, then maintenance phase Intervention
Comparator
In case of acute therapy for active atopic dermatitis lesions Eucerin Eczema Relief Instant Therapy was provided and participants entered the Treatment phase for 4 weeks |
|
| Outcomes | Assessments (4): baseline, weeks 2, 6 and until flare Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared but 3 of the authors were employees of Beiersdorf, therefore it is most likely that the study was funded by Beiersdorf | |
| Declaration of interest | Quote (page 485): "Teresa M. Weber PhD is an employee of Beiersdorf Inc, the manufacturer of Eucerin Eczema Relief Body Creme and Eucerin Eczema Relief Flare Treatment. Alexander Filbry PhD and Frank Rippke MD are employees of BeiersdorfAG. Frank Samaria MD and Michael J. Babcock MD have no conflicts of interest to declare" | |
| Notes | Eucerin Eczema Relief Body Creme, Seiersdorf, Wilton, CT contains 1% colloidal oatmeal, licochalcone A (anti‐inflammatory property), ceramide 3, an epidermal barrier Iipid, aqua, glycerol, castor‐oil‐plant (Ricinus communis) seed oil, mineral oil, cetyl alcohol, glyceryl sterate, caprylic/capric triglyceride, octyldodecanol, cetyl palmitate, PEG‐40 stearate, Chinese liquorice (Glycyrrhiza inflata) root extract, 2‐hexanediol, phenoxyethanol, piroctone olamine, caprylyl glycol, ethylhexylglycerin, benzyl alcohol, citric acid We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 479): "randomly assigned" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "In order to enroll subjects across the inclusion age range and to assure approximately equal age distribution in the two treatment cells (moisturizer vs. no moisturizer), subjects were randomized into 3 age groups, 3 months up to 12 months, >12 months to 24 months, and >24 months to 12 years. Therefore the study coordinator created 3 randomization lists (1 per age group) with subject number codes" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "treatment cell allocation and product distribution was handled separately, in a different part of the clinical site from the examination rooms, away from the investigator. The investigator was not involved in cell allocation, nor dispensing the treatment supplies" Comment: form of central allocation. Allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No reporting of measures used to blind study participants and personnel from knowledge of which intervention a participant received. Comment: the outcome was likely to be influenced by the lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | No blinding reported. Outcomes were investigator‐assessed. Comment: the outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2/45 (4.4%): moisturiser group 1/21, control group 1/24. Per‐protocol analysis. Comment: low number of losses to follow‐up, and although per‐protocol analysis considered to be at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the outcomes mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | The study appears to be free of other forms of bias. |
Wilhelm 1998.
| Study characteristics | ||
| Methods | Randomised, double‐blind, vehicle‐controlled, within‐participant study Setting ProDERM Institut für Angewandte Dermatologische Forschung, Schenefeld, Germany Date of study Unspecified. Duration of the intervention 4 weeks |
|
| Participants | N = 80 (58 female, 22 male) Mean age not reported Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 80 to either body side (within‐participant) Withdrawals/losses to follow‐up 3/80 (3.8%), reasons unreported Baseline data 65% experience acute episode of atopic dermatitis within last year, 72.5% suffered from moderate to severe itch Mean sum score of erythema, dryness, induration/papules: urea cream side 4.05, vehicle side 4.11 Mean corneometry: urea cream side 48.6 (SD 9.1), vehicle side 48.2 (SD 10.0) |
|
| Interventions |
Intervention
Comparator
During the study no systemic treatments with corticosteroids, antihistamines, NSAIDs, cytostatic drugs or immunotherapy, nor topical treatments were permitted |
|
| Outcomes | Assessments (4): baseline, weeks 1, 2 and 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared, but 1 of the investigators was an employee of Beiersdorf, Hamburg, Germany, the manufacturer of the drug under investigation | |
| Notes | Vehicle contains: benzyl alcohol, paraffin, sodium lactate, magnesium stearate, ceresin, glyceryl diisostearate, isopropyl palmitate, wool alcohols, magnesium sulphate, purified water | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote (page 26): "randomised" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote (page 165): "double‐blind" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received on each side of the body, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Quote (page 165): "double‐blind" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 3/80 (3.4%), reasons unreported. Per‐protocol analysis. Comment: low number of losses to follow‐up, and although per‐protocol analysis considered as at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the prespecified outcomes and those mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | Comment: the study appeared to be free of other forms of bias. |
Wirén 2009.
| Study characteristics | ||
| Methods | Randomised, controlled (inactive) study Setting Multicentre (5), dermatology outpatient clinics in Sweden Date of study Unspecified. Duration of intervention: 3 weeks for treatment phase, and 6 months maintenance phase. We only include the data from the maintenance phase |
|
| Participants | N = 44 (32 female, 12 male) Mean age = 33.5 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised for maintenance phase N = 44 (moisturiser group = 22, no moisturiser = 22) Withdrawals/losses to follow‐up No losses to follow‐up reported Baseline data Mean TEWL (g/m²/h): moisturiser group 11.9, no moisturiser 14.1 |
|
| Interventions | Treatment phase: 3 weeks betamethasone valerate 0.01% cream (Betnoderm or Betnovat) (55) Maintenance phase: Intervention
Comparator
Concomitant treatment of other body areas with other topical preparations (e.g. cosmetics and corticosteroids) was allowed throughout the study |
|
| Outcomes | Assessments (2): baseline and week 3 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared, but the drug under investigation is manufactured by ACO HUD NORDIC AB, Upplands Väsby, Sweden | |
| Declaration of interest | Quote (page 1267): "None declared", but the first author was an employee of ACO HUD NORDIC AB, Upplands Väsby, Sweden, the manufacturer of the drug under investigation | |
| Notes | Betnoderm ACO HUD AB, Upplands Väsby, Sweden or Betnovat GlaxoSmithKline, Solna, Sweden Canoderm cream 5%, ACO HUD NORDIC AB, Upplands Väsby, Sweden; oil‐in‐water emulsion containing fractionated coconut oil, emulsifying wax, hydrogenated canola oil, propylene glycol, carbomer, dimethicone, hard paraffin, glycerol polymetacrylate, propyl‐ and methyl parahydroxybenzoate, sodium lactate solution, lactic acid, glyceryl stearate, polyoxyethylene stearate, purified water The co‐publication, Hjalte 2010, under the primary reference, contains economic outcomes We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 1268): "randomized" Comment: insufficient detail was reported about the method used to generate the allocation sequence to allow a clear assessment of whether it would produce comparable groups. After email communication: "Randomisation was performed by the Sponsor and there was one randomisation list for each part of the study. The randomization was computer aided (Excel). The investigator kept the randomisation lists in a sealed envelope only to be opened in case of a SAE. When patients were included in the first part of the study, patients received a chronological identification number and received one of the interventional drugs labelled with the chronological identification number. If patients were eligible for the part two of the study, then they were to receive either Canoderm or no treatment, also according to the predetermined randomization list. In this part of the study, blocked randomization (balanced within blocks of 20) were used to ensure equal number of Canoderm treatment and no treatment" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. After email communication: "The investigator kept the randomisation lists in a sealed envelope only to be opened in case of a SAE..." (see above) and "The Sponsor dispensed the intervention labelled with appropriate identification number" Comment: central allocation; allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No reporting of measures used to blind study participants and personnel from knowledge of which intervention a participant received. Comment: the outcome was likely to be influenced by the lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | No blinding reported. Outcomes were investigator‐assessed. Comment: the outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No losses to follow‐up reported. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the outcomes mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | The study appears to be free of other forms of bias. |
Wu 2014.
| Study characteristics | ||
| Methods | Randomised, active‐controlled study Setting Department of Dermatology, Guangxi Minzu Hospital, Nanning, China Date of study February 2012 to July 2013. Duration of intervention: 3 weeks with 2 weeks of follow‐up |
|
| Participants | N = 125 (62 female, 63 male) Mean age = 47 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 125 (pilot group = 63, control group = 62) Withdrawals/losses to follow‐up 20/125 overall (16%): pilot group 3/63, control group 17/62; reasons unreported Baseline data Mean disease duration: pilot group 18.5 months (SD 35.7), control group 20.3 months (SD 34.6) Mean EASI: pilot group 18.9 (SD 0.86), control group 17.94 (SD 0.71) |
|
| Interventions |
Intervention
Comparator
|
|
| Outcomes | Assessments (6): baseline, weeks 1, 2, 3, 5 and 8 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | None declared | |
| Declaration of interest | None declared | |
| Notes | We mailed investigators numerous times to clarify study details, but received no response (Table 11). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Translated "Allocated by using a random number table" Comment: probably done. |
| Allocation concealment (selection bias) | Unclear risk | The method used to conceal the allocation sequence, that is to determine whether intervention allocations could have been foreseen in advance of, or during, enrolment, was not reported. Comment: there was insufficient information to permit a clear judgement. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No reporting of measures used to blind study participants and personnel from knowledge of which intervention a participant received. Comment: the outcome was likely to be influenced by the lack of blinding. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | No blinding reported. Outcomes were investigator‐assessed as well as participant‐assessed. Comment: the outcome measurement was likely to be influenced by the lack of blinding. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 20/125 (16%): pilot group 3/63, control group 17/62, reasons unreported. Per‐protocol analysis. Comment: moderate dropout rate, but very unbalanced, which, combined with per‐protocol analyses, poses a high risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was not available, but the outcomes mentioned in the Methods section appeared to have been reported. |
| Other bias | Low risk | The study appears to be free of other forms of bias. |
Åkerström 2015.
| Study characteristics | ||
| Methods | Randomised, double‐blind, 'other moisturiser'‐controlled study Setting Multicentre (15) in Finland, Noway and Sweden Date of study September 2011 to September 2012. After the stabilisation phase, participants entered the randomised maintenance phase of 180 days. We only include the data from the maintenance phase |
|
| Participants | N = 172 (101 female, 71 male) Mean age = 28 years Inclusion criteria of the trial
Exclusion criteria of the trial
Randomised N = 172 (barrier‐strengthening moisturiser = 87, reference cream = 85) Withdrawals/losses to follow‐up 7/172 overall (4.1%): barrier‐strengthening moisturiser 3/87 (3.4%), reference cream 4/85 (4.7%)
Baseline data stabilisation phase Mean SCORAD: barrier‐strengthening moisturiser 35.62 (SD 12.24), reference cream 37.68 (SD 13.56) Baseline data maintenance phase: Mean SCORAD: barrier‐strengthening moisturiser 6.14 (SD 6.38), reference cream 5.97 (SD 5.84) |
|
| Interventions | Stabilisation phase: once‐daily topical mometasone furoate cream 0.1% (Elocon, Merck Sharp & Dohme B.V, Netherlands) on the trunk and extremities and/or hydrocortisone acetate cream 1% (Hyderm ACO Hud Nordic, Upplands Väsby, Sweden) on the face, groin and armpits. In addition, participants used a medicinal moisturiser containing 20% glycerol (Miniderm, ACO Hud Nordic, Upplands Väsby, Sweden) Maintenance phase Intervention
Comparator
|
|
| Outcomes | Assessments (4): baseline, end of stabilisation phase (visit 2), relapse visit (visit 3), day 180 (visit 4) Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
|
| Funding source | Quote (page 591): "This study was sponsored by ACO Hud Nordic AB, an Omega Pharma Company and partly funded by the Knowledge Foundation, Sweden. The sponsor was responsible for the study design, co‐ordination and collection of data provided by the investigators. The authors were responsible for data analysis, manuscript preparation and the decision to submit the manuscript for publication" | |
| Declaration of interest | Quote (page 591):"U.Å., K.W. and P.S. are employees of ACO Hud Nordic AB. M.G. was an employee at ACO Hud Nordic AB at the time when the study was conducted. Å.S. participated as principal investigator, but did not receive any personal compensation. S.R. has acted as an expert and/or given lectures for ACO Hud Nordic AB, Dignity Sciences, and Astellas Pharma Europe. M.B. has acted as an expert and/or given lectures for ACO Hud Nordic AB. M.L. has acted as a paid consultant to ACO Hud Nordic AB and has received funding for research carried out in this work.”L.K., none declared. L.R., none declared. T.L., none declared" | |
| Notes | Canoderm (ACO Hud Nordic, Sweden), an oil‐in‐water emulsion containing 5% urea, fractionated coconut oil, polysorbate 60, hydrogenated canola oil, propylene glycol, carbomer, dimethicone, hard paraffin, glyceryl polymethacrylate, propyl‐ and methyl parahydroxybenzoate, sodium lactate, lactic acid, glyceryl stearate, polyoxyethylene stearate, cetostearyl alcohol and purified water. The reference cream was Miniderm without glycerol (ACO Hud Nordic, Upplands Väsby, Sweden) and contains white soft paraffin, hydrogenated canola oil, light liquid paraffin, glyceryl stearate, polyoxyethylene stearate, cetostearyl alcohol, hard paraffin, dimethicone, cholesterol, propyl‐ and methyl parahydroxybenzoate and purified water. We received responses to our request for study details (Table 11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote (page 588): "Randomization to test cream and reference cream groups in 1:1, was performed according to a randomization list, with a block size of 4, and stratified for country with one randomization list for each country" and "The randomization was prepared by an independent statistician using a validated SAS® program" Comment: probably done. |
| Allocation concealment (selection bias) | Low risk | Quote (page 558): "The patients were provided with a randomization number" and "All study personnel at the clinics and the sponsor staff remained blinded during the maintenance part of the study" Comment: there was insufficient information to permit a clear judgement. After email communication: "The clinics received sealed envelopes containing individual treatment codes. The Investigator kept the envelopes in a secure, limited‐access location to prevent inadvertent breaking of the blind" Comment: central allocation; allocation appears to have been adequately concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote (page 557‐8): "double‐blind" and "All study personnel at the clinics and the sponsor staff remained blinded during the maintenance part of the study" Comment: the report did not provide sufficient detail about the specific measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. After email communication: "The test cream and the reference cream used in the maintenance phase were produced by Bioglan, Malmö, Sweden. The creams were packaged in identical plastic pump jars of 500 g and in tubes of 100 g" and "Before the products were distributed to the patients, they were also be labelled with the randomisation number" Comment: the report provided sufficient detail about the measures used to blind study participants and personnel from knowledge of which intervention a participant received, to permit a clear judgement. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote (page 557‐8): "double‐blind" and "All study personnel at the clinics and the sponsor staff remained blinded during the maintenance part of the study" Outcomes were investigator‐assessed as well as participant‐assessed. Comment: uncertainty about the effectiveness of blinding of outcomes assessors (participants/healthcare providers) during the study. Insufficient information to permit a clear judgement After email communication:(see domain above) Blinding of the outcomes assessors, key personnel, and participants was ensured, and it was unlikely that the blinding could have been broken. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 7/172 (4.1%); barrier‐strengthening moisturiser 3/87 (3.4%), reference cream 4/85 (4.7%), reasons reported. Intention‐to‐treat analysis. Comment: low number of losses to follow‐up, combined with intention‐to‐treat analysis, so considered to be at a low risk of bias. |
| Selective reporting (reporting bias) | Low risk | The protocol for the study was available (EudraCT Number: 2011‐001068‐23) and the prespecified outcomes and those mentioned in the Methods section appear to have been reported. |
| Other bias | Low risk | The study appears to be free of other forms of bias. |
AD: atopic dermatitis ADSI: Atopic Dermatitis Severity Index BHT: butylated hydroxytoluene BSA: body surface area CDLQI: Children’s Dermatology Life Quality Index cis‐UCA: cis urocanic acid DASI: dry skin area and severity index DFI: Dermatitis Family Impact DLQI: dermatology quality of life index EASI: eczema area and severity index ECG: electrocardiograph EDTA: ethylenediaminetetraacetic acid GCS: Global Change Scale GIS: Global Impression Scale HI: hydration index HPA: hypothalamic‐pituitary‐adrenal IDQOL: the Infant’s Dermatitis Quality of Life index IGA: investigator Global Assessment ILE: L‐isoleucine MEA: monoethanolamine MPA: methylprednisolone aceponate MVE: multilamellar vesicular emulsion NESS: Nottingham Atopic Eczema Severity Score NSAIDs: non‐steroidal anti‐inflammatories OTC: over‐the‐counter PPARα: peroxisome proliferator‐activated receptor alpha PCA: pyrrolidone carboxylic acid PEG: polyethylene glycol PGA: Physician Global Assessment PUVA: photochemotherapy, a type of ultraviolet radiation treatment POEM: Patient‐Oriented Eczema Measure QoL: quality of life SCORAD: scoring atopic dermatitis TEWL: transepidermal water loss TIS: three item severity score UVA, UVB: types of ultraviolet light VAS: visual analogue scale VCO: virgin coconut oil VOO: virgin olive oil
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Duggan 2015 | After reading full text, appeared to be a report on BATHE trial, BEEP study and CLOTHES trial and no primary research |
| Dutronc 2011B | Two studies, one RCT in healthy volunteers, second study observational in atopic dermatitis |
| Schoelermann 2003 | Report on two studies, one was a CCT in atopic dermatitis |
| Szczepanowska 2008 | CCT: email communication with investigators confirmed participants were allocated by alternation. "We included patients consecutively and every second patient was assigned to one group, while the others to the second treatment group" |
| Yang 2010 | After translation, appeared to be a CCT |
Abbreviations
BATHE: Bath Additives in the Treatment of cHildhood Eczema (see Santer 2015) BEEP: Barrier Enhancement for Eczema Prevention CCT: controlled clinical trial CLOTHES: Clothing for the relief of Eczema Symptoms RCT: randomised controlled trial
Characteristics of ongoing studies [ordered by study ID]
ACTRN12615000782538.
| Study name | A randomised, double blind, placebo controlled comparative trial of ceramide cream and ceramide cleanser in the management of moderate eczema in adults |
| Methods | Randomised, double‐blind, placebo‐controlled study, Braeside Vic, Australia |
| Participants | N = 100 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments (2): baseline, day 28 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | Not yet recruiting (website accessed 08‐02‐2016) |
| Contact information | Dr Kerryn Greive (kerryng@egopharm.com) |
| Notes |
ACTRN12615000920594.
| Study name | A randomised double blinded placebo controlled study investigating Atopis for the improvement of skin health in subjects with eczema |
| Methods | Randomised, double‐blind, placebo‐controlled study in St Rangiora, Christchurch, New Zealand |
| Participants | N = 60 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments (3): baseline, weeks 2, and 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | 04‐09‐2015, follow‐up complete (website accessed 08‐02‐2016) |
| Contact information | Dr Iona Weir (iona@decima.co.nz) and Dr Simon Carson (simon@sctrials.co.nz) |
| Notes | No study results posted |
ACTRN12615001343594.
| Study name | Pilot study comparing two moisturisers, Emulsifying ointment B.P. and Epaderm topical ointment in children with eczema |
| Methods | Randomised, double‐blind, controlled within‐participant study in Wellington, New Zealand |
| Participants | N = 60 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments (5): baseline, weeks 2, 4, 6 and 8 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | Recruiting (website accessed 08‐02‐2016) |
| Contact information | Marina.Dzhelali@ccdhb.org.nz and thorsten.stanley@otago.ac.nz |
| Notes |
ChiCTR‐IOR‐15007139.
| Study name | Effect and efficacy of a linoleic acid‐ceramide containing moisturizer as an adjunctive therapy in the treatment of atopic dermatitis: a randomized controlled trial |
| Methods | Randomised controlled trial in Shanghai |
| Participants | N = 10 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments unclear Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | 2003, completed (website accessed 11‐02‐2016) |
| Contact information | Xia Li (drlixia@126.com) and Jie Zheng (jie‐zheng2001@126.com) |
| Notes | No study results posted. Similar study in chronic eczema is ongoing ChiCTR‐IOR‐15007140 with 29 participants in each treatment arm. However, unclear if this is atopic eczema |
EudraCT2004‐002926‐23.
| Study name | Evaluation of the impact of the moisturizing milk RV2478B on the use of corticoids and on quality of life, in a population of children with atopic dermatitis |
| Methods | Open, randomised controlled study in Italy |
| Participants | N = 210 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments unclear Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | 2004, completed (website accessed 09‐02‐2016) |
| Contact information | Not provided, sponsor is Pierre Fabre Médicament |
| Notes | Very little information provided; no study results posted |
EudraCT2005‐003396‐21.
| Study name | Long‐term management of atopic dermatitis with the moisturiser V0034 CR. A randomised, placebo‐controlled, parallel‐groups, double‐blind study in infants and children |
| Methods | Randomised controlled trial in Estonia, Finland, Germany, Latvia |
| Participants | N = 300 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments (5): baseline, days 7, 14, 21 and 28 Outcomes of the trial (as reported) To evaluate the overall benefit of a regular treatment by the moisturiser V0034CR in the management of atopic dermatitis: reduction of corticosteroids consumption, reduction of flares
*Denotes outcomes prespecified for this review |
| Starting date | 3‐11‐2005, completed (website accessed 09‐02‐2016) |
| Contact information | Not provided, sponsor is Pierre Fabre Médicament, however, see www.fda.gov/iceci/enforcementactions/warningletters/ucm211391.htm |
| Notes | Not clear from the website if desonide cream was used in both arms. No study results posted |
EudraCT2006‐000877‐30.
| Study name | A 6 week, multi centre study to evaluate the efficacy and safety of E45 complete moisturiser therapy and E45 itch relief cream in the treatment of mild to moderate atopic eczema compared to a patient's normal moisturiser regime defined as the frequent use of moisturisers (not containing lauromacrogols) listed in the BNF (Harbour Study) |
| Methods | Randomised controlled trial in UK |
| Participants | N = 180 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator 1
Comparator 2
|
| Outcomes | Assessments (3): baseline, days 7 and 21 Outcomes of the trial(as reported) To compare the efficacy of E45 complete moisturiser therapy against an unchanged moisturiser regime along with the role of E45 anti itch cream in controlling itch. This will be evaluated through validated quality of life questionnaires, IGA and diary cards.
*Denotes outcomes prespecified for this review |
| Starting date | 27‐4‐2006, ongoing (website accessed 16‐2‐2016) |
| Contact information | Reckitt Benckiser Healthcare International, no further contact details available |
| Notes |
EudraCT2007‐002133‐36.
| Study name | A multicenter, randomized, double‐blind clinical study to examine the efficacy and safety of Zarzenda in comparison to Elidel in the management of mild to moderate atopic dermatitis in children and adolescents |
| Methods | Randomised, double‐blind, active‐controlled study, multicentre in Germany, Spain and Italy |
| Participants | N = 80 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments (unspecified): baseline and at each visit (information unclear) Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | Completed in Germany and Italy, but still ongoing in Spain (website accessed 09‐02‐2016) |
| Contact information | Not provided, sponsor is INTENDIS GmbH |
| Notes | Zardenda is another name for Atopiclair. No study results posted |
EudraCT2008‐003485‐25.
| Study name | Impact of the V0034CR 01B moisturiser on atopic dermatitis symptoms in children. A randomised, placebo‐controlled, parallel‐groups, double‐blind study |
| Methods | Randomised controlled trial in Estonia, France, Germany, Italy, Latvia, Lithuania |
| Participants | N= 550 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention (not clear from the study protocol on the website if desonide cream was used in both arms)
Comparator
|
| Outcomes | Assessments (unspecified): baseline and at each visit (information unclear) Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | October 2008, completed in all countries except in France (ongoing) (website accessed 09‐02‐2016) |
| Contact information | Not provided, sponsor is Pierre Fabre Médicament |
| Notes | No study results posted |
EudraCT2008‐006844‐21.
| Study name | Evaluation of a developmental ‘long lasting’ moisturiser in subjects with dry skin |
| Methods | Randomised, double‐blind, controlled, within‐participant study in UK |
| Participants | N = 40 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments: unclear Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | 2008, completed (website accessed 09‐02‐2016) |
| Contact information | Not provided, sponsor is Dermal Laboratories Ltd |
| Notes | No study results posted |
EudraCT2009‐010609‐35.
| Study name | Is treatment with moisturisers always beneficial? Comparative biophysical and molecular biological studies of the skin barrier function in patients with atopic dermatitis, ichthyosis vulgaris and X‐linked ichthyosis |
| Methods | Randomised, investigator‐blinded, controlled study in Sweden |
| Participants | N = 60 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator 1
Comparator 2
|
| Outcomes | Assessments (2): baseline, week 4 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | 2009, ongoing (website accessed 09‐02‐2016) |
| Contact information | Department of Medical Sciences, Dermatology and Venerology, Uppsala University, Uppsala Sweden, no further details provided |
| Notes |
EudraCT2009‐016572‐78.
| Study name | Arm immersion test to compare the skin effects of routine bathing with and without the use of an emollient bath additive |
| Methods | Randomised, investigator‐blinded, controlled within‐participant study in UK |
| Participants | N = 24 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments unclear Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | 2010, not recruiting (website accessed 12‐02‐2016) |
| Contact information | Sponsor Dermal Laboratories Ltd UK |
| Notes |
EudraCT2012‐004621‐24.
| Study name | Moisturisers in the management of atopic dermatitis in children: prevention of flares |
| Methods | Randomised, open, controlled study in Lithuania and Estonia |
| Participants | N = 409 Inclusion criteria of the trial Boys or girls, presenting with the following criteria (V1):
After treatment of the current flare, the following are required for randomisation (V2):
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator 1
Comparator 2
|
| Outcomes | Assessments (4): baseline, days 28, 56 and 84 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | 2013, completed (website accessed 09‐02‐2016) |
| Contact information | Pierre Fabre Médicament, Carine Fabre (carine.fabre@pierre‐fabre.com) |
| Notes | V0034CR = Dexeryl. A flare will be defined as the following: measurable increased extent or intensity of lesions in < 2 weeks under continued treatment (in this case: moisturiser or no moisturiser), corresponding to a significant increase (> 25%) in medical score (SCORAD or last PO‐SCORAD) or to the introduction of a new line of therapy (topical corticosteroid). No study results posted |
EudraCT2014‐001026‐16.
| Study name | Randomised, double‐blind, bilateral comparison of two moisturisers in patients with dry skin |
| Methods | Randomised, double‐blind, controlled within‐participant study in the UK |
| Participants | N = 20 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments (16): baseline, days 1 until 5 (3 times a day) Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | 2014, completed (website accessed 09‐02‐2016) |
| Contact information | Dermal Laboratories Limited, Amanda Wigens, clinical@dermal.co.uk |
| Notes | No study results posted |
ISRCTN97515110.
| Study name | Investigating whether topical application of a non toxic molecule improves epidermal pH and barrier function in atopic dermatitis |
| Methods | Randomised, vehicle‐controlled study in UK |
| Participants | Not specified |
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments (7): baseline and then weekly up to 6 weeks Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | 01‐09‐2008, completed (website accessed 8‐2‐2016) |
| Contact information | Dr Neil Gibbs (neil.gibbs@manchester.ac.uk) |
| Notes | No study results posted |
JPRN‐UMIN000005158.
| Study name | Randomized controlled trial to evaluate clinical efficacy of once‐ or twice‐daily skin care with moisturiser for prevention of atopic dermatitis exacerbation |
| Methods | Randomised, investigator‐blinded, controlled study in Japan |
| Participants | N = 150 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments unclear Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | 2011, recruiting (website accessed 12‐02‐2016 |
| Contact information | Yukihiro Ohya, National Center for Child Health and Development, Okura, Setagayaku, Tokyo, Japan |
| Notes | No further details regarding skin care regimen being tested |
JPRN‐UMIN000010009.
| Study name | Study to evaluate the efficacy of conventional topical therapy for atopic dermatitis based on filaggrin‐gene mutations |
| Methods | Randomised, double‐blind controlled study in Japan |
| Participants | N = 30 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
Treatment includes steroid ointment and tacrolimus ointment |
| Outcomes | Assessments unclear Outcomes of the trial(as reported)
*Denotes outcomes prespecified for this review |
| Starting date | 2012, still recruiting (website accessed 12‐02‐2016) |
| Contact information | Osamu Mizuno (osmizuno@tk9.so‐net.ne.jp) |
| Notes | Applying split‐plot design, multiple factors randomised. 4 sites at each cubital fossa and popliteal fossa are used as independent sites. First randomisation factor is presence or absence of filaggrin gene mutation. Second factor is combination of the usage or non‐usage of moisturiser and treatment. Treatment includes steroid ointment and tacrolimus ointment |
JPRN‐UMIN000017957.
| Study name | The effect of moisturizer on both sweating function and sensitive skin in patients with atopic dermatitis, a randomized comparative study |
| Methods | Randomised, double‐blinded, placebo‐controlled study in Osaka, Japan |
| Participants | N = 25 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments unclear Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | June 2015 |
| Contact information | Hiroyuki Murota (h‐murota@derma.med.osaka‐u.ac.jp) |
| Notes | No study results posted |
NCT00180141.
| Study name | Control of therapy with Elidel vs placebo in patients with atopic dermatitis using bioengineering methods |
| Methods | Randomised, double‐blind, controlled study in Dresden, Germany |
| Participants | N = 24 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments: unclear Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | April 2005, completed (website accessed 10‐02‐2016) |
| Contact information | Roland Aschoff, MD Department of Dermatology. Medical Faculty, Technical University Dresden, Germany |
| Notes | No study results posted |
NCT00576238.
| Study name | A multi‐centre, parallel, randomised study of the skin tolerance of betamethasone creams on atopic eczema and the influence of moisturiser treatment on the recurrence of eczema |
| Methods | Randomised, double‐blind, controlled study in Sweden |
| Participants | N = 55 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator 1
|
| Outcomes | Assessments (3): baseline, week 3 and month 6 Outcomes of the trial (as reported) To study the:
*Denotes outcomes prespecified for this review |
| Starting date | January 2004, completed (website accessed 11‐02‐2016) |
| Contact information | Principal investigator Berit Berne Hudkliniken, Akademiska sjukhuset, Uppsala, Sweden |
| Notes | No study results posted |
NCT00828412.
| Study name | A randomised, investigator‐blind, six‐week, parallel group, multicenter pilot study to compare the safety and efficacy of EpiCeram skin barrier emulsion and desonide cream 0.05% in the twice daily treatment of paediatric subjects with moderate atopic dermatitis |
| Methods | Randomised, investigator‐blinded, controlled study in the USA |
| Participants | N = 100 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments (2): baseline and week 6 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | March 2009, completed (website accessed 10‐02‐2016) |
| Contact information | Promius Pharma LCC, Joanne Fraser (joannefraser@promiuspharma.com) |
| Notes | Few data are available for one outcome |
NCT01779258.
| Study name | Moisturisers in the management of atopic dermatitis in children: Prevention of flares |
| Methods | Randomised controlled open‐label trial in Estonia, France, Lithuania, Poland, Romania |
| Participants | N = 347 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator 1
Comparator 2
|
| Outcomes | Assessments: baseline and further time points unclear Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | February 2013, completed (website accessed 10‐2‐2016) |
| Contact information | Pierre Fabre Medicament. No further details available |
| Notes | No study results posted |
NCT01781663.
| Study name | Efficacy of KAM2904 face cream and KAM3008 body lotion treatment in children with atopic dermatitis (AD) |
| Methods | Randomised, double‐blind, controlled trial in Spain |
| Participants | N = 156 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments (4): baseline, week 2, 4 and 6 Outcomes of the trial (as reported)
|
| Starting date | February 2013, completed (website accessed 10‐02‐2016) |
| Contact information | Miri Sani (mirisani@013.net) |
| Notes | No study results posted |
NCT01915914.
| Study name | A randomized, open‐label, comparative study to evaluate an intermittent dosing regimen of fluticasone propionate 0.05% cream (twice per week) in reducing the risk of relapse when added to regular daily moisturization using PHYSIOGEL lotion in paediatric subjects with stabilized atopic dermatitis |
| Methods | Open, 2‐phase, randomised controlled study in China |
| Participants | N = 107 Inclusion criteria of the trial
Exclusion criteria of the trial (in the acute phase)
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments: baseline and further time points unclear Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | December 2013, completed (website accessed 10‐02‐2016) |
| Contact information | GlaxoSmithKline. No further details available |
| Notes | No study results posted |
NCT02028546.
| Study name | The effect of bathing and moisturizers on skin hydration in atopic dermatitis: an in vivo study |
| Methods | Randomised, investigator‐blinded, controlled, cross‐over study in Thailand |
| Participants | N = 22 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator 1
Comparator 2
Comparator 3
The same 4 regimens were repeated with soaking an arm with mild cleanser All regimens were completed in all participants with 2 visits (7 days between visits) |
| Outcomes | Assessments: at baseline and every 30 minutes for 120 minutes after each regimen Outcomes of the trial(as reported)
*Denotes outcomes prespecified for this review |
| Starting date | January 2013, completed (website accessed 11‐02‐2016) |
| Contact information | Arisa Kaewkes, MSc dermatology Skin center, Faculty of Medicine, Srinakharinwirot University |
| Notes | No study results posted |
NCT02286700.
| Study name | Skin effects of a topical amino acid moisturizing cream and desonide in atopic dermatitis |
| Methods | Randomised, double‐blind, controlled study in Boston, USA |
| Participants | N = 42 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments (4): baseline, week 1, 2 and 3 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | November 2014, still recruiting (website accessed 10‐2‐2016) |
| Contact information | Barbara A Green, RPh (bgreen@neostrata.com) and Justine K Gostomski, MS (jgostomski@neostrata.com) |
| Notes |
NCT02376049.
| Study name | An explorative clinical trial to evaluate an intra patient comparison design of topical agents in adults with mild to moderate atopic dermatitis |
| Methods | Randomised, double‐blind, controlled study in Israel and Canada |
| Participants | N = 30 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator 1
Comparator 2
Comparator 3
|
| Outcomes | Assessments (2): baseline and week 2 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | February 2015, completed (website accessed 11‐02‐2016) |
| Contact information | Principal investigator Emma Guttmann, MD, Icahn Scool of Medicine |
| Notes | No study results posted |
NCT02589392.
| Study name | Effect of Cetaphil Restoraderm moisturizer on very dry skin in children with a controlled atopic dermatitis:a randomised, parallel group study |
| Methods | Randomised, investigator‐blinded controlled study in China and the Phillipines |
| Participants | N = 120 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
|
| Outcomes | Assessments (2): baseline and week 12 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | May 2015, still recruiting (website accessed 11‐2‐2016) |
| Contact information | Philippe Martel (philippe.martel@galderma.com) and Stéphanie Leclerc (stephanie.leclerc@galderma.com) |
| Notes |
NTR4541.
| Study name | Efficacy of a skin barrier repair cream (Dermalex Eczema) in atopic dermatitis patients ‐ EDA |
| Methods | Randomised, double‐blind, controlled, within‐participant study in the Netherlands |
| Participants | N = 100 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator 1
Comparator 2
|
| Outcomes | Assessments unclear Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | May 2014, recruiting (website accessed 12‐02‐2016) |
| Contact information | SA Koppes (s.a.koppes@amc.nl) |
| Notes |
Ridd 2015.
| Study name | Choice Of Moisturiser in Eczema Treatment (COMET) |
| Methods | Randomised, investigator‐blinded, controlled study Setting University of Bristol, UK Date of study June 2014 to July 2015. Duration 3 months |
| Participants | N = 160 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator 1
Comparator 2
Comparator 3
Children will attend appointments for their eczema as normal and use other medications (for example, topical corticosteroids) as normally directed. Co‐prescribing of other leave on moisturisers and bath additives will be discouraged, but allowed |
| Outcomes | Assessments (4): baseline, months 1, 2 and 3 Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | June 2014. Completed (website accessed 8‐2‐2016) |
| Contact information | Dr Victoria J Wilson (Victoria.Wilson@bristol.ac.uk) |
| Notes | Feasability study. No study results posted |
Santer 2015.
| Study name | Bath additives for the treatment of childhood eczema |
| Methods | Open, randomised controlled study Setting Multicentre general practitioner practices in England and Wales, UK Date of study Unspecified. Duration 1 year |
| Participants | N = 423 Inclusion criteria of the trial
Exclusion criteria of the trial
|
| Interventions |
Intervention
Comparator
Standard care includes advice to use leave‐on moisturisers regularly, plus intermittent topical corticosteroids if required |
| Outcomes | Assessments (25): baseline and then weekly up to 16 weeks, thereafter monthly Outcomes of the trial (as reported)
*Denotes outcomes prespecified for this review |
| Starting date | The recruitment was expected to start in November 2014 (website accessed 8‐2‐2016) |
| Contact information | Kate Martinson, Trial Manager (k.martinson@soton.ac.uk) |
| Notes | Trial registration number: ISRCTN84102309 |
Abbreviations
ADSI: Atopic Dermatitis Severity Index BNF: British National Formulary BSA: body surface area CDLQI: Children’s Dermatology Life Quality Index COPD: chronic obstructive pulmonary disease DELP: Brandname of the gel under research DFI: Dermatitis Family Impact questionnaire EASI: eczema area and severity index IDQOL: Infant's Dermatitis Quality of Life Index IGA: Investigator Global Assessment NSAIDs: non‐steroidal anti‐inflammatories UVA and UVB: types of ultraviolet light POEM: Patient‐Oriented Eczema Measure PO SCORAD: Patient Oriented SCORAD PSGA: Physician Static Global Assessment SCORAD: scoring atopic dermatitis SGA: Subjective Global Assessment TADSI: Target Lesion Atopic Dermatitis Severity Index TEWL: transepidermal water loss TIS: three item severity score UVA, UVB: types of ultraviolet light VAS: visual analogue scale
Differences between protocol and review
We have added 'vehicle' as comparator under Types of interventions. For clarity, under Effects of interventions we added: "To ensure consistency with the terminology used by the investigators, we used the wording for placebo or vehicle accordingly. It is important to know that a placebo is also a moisturiser, but with a different composition and without the assumed effective ingredient; a vehicle has the same composition as the moisturiser it is compared with, but without the assumed effective ingredient. As both placebo and vehicle have moisturising properties they might have a beneficial effect on the skin barrier and thus might decrease disease severity."
The text under Measures of treatment effect, Unit of analysis issues (within‐participant studies), Assessment of heterogeneity and Assessment of reporting biases has been amended slightly to provide improved clarification, but without and substantive change made to the content.
We removed the last sentence Dealing with missing data "Whenever possible, we used results based on an ITT analysis" as this was already mentioned in first paragraph.
In the protocol we stated under Assessment of heterogeneity "However, based on the GRADE Working Group approach (GRADE) we will rate down for very serious inconsistency if the I² is above 75%". Rating down the quality of evidence also depends on how much other items have been downgraded. The GRADE Handbook states "Reviewers should grade the quality of the evidence by considering both the individual factors in the context of other judgments they made about the quality of evidence for the same outcome. In such a case, you should pick one or two categories of limitations which you would offer as reasons for downgrading and explain your choice in the footnote. You should also provide a footnote next to the other factor, you decided not to downgrade, explaining that there was some uncertainty, but you already downgraded for the other factor and further lowering the quality of evidence for this outcome would seem inappropriate" (Schünemann 2013). Therefore, we have made the following post hoc changes to the protocol; "However, based on the recommendations of the Grading of Recommendations Assessment, Development and Evaluation working group (GRADE) we considered rating down for serious inconsistency if the I² was above 50%, taking into account other considerations for rating down the quality of evidence."
The text under Data synthesis has changed slightly as although we planned to undertake meta‐analyses using Mantel‐Haenszel risk differences, this was not applicable. In future updates when we can perform meta‐analyses we will report results including 95% confidence intervals and forest plots for both Peto OR and Mantel‐Haenszel risk differences so that findings can be compared.
In the Subgroup analysis and investigation of heterogeneity we were not able to conduct our planned stratified analyses, as we had no studies that addressed disease severity (mild versus severe eczema), atopic versus non‐atopic eczema, or presence of filaggrin gene mutations versus no filaggrin gene mutations and, although some studies were conducted only in children and others only in adults, none of the comparisons allowed stratified analyses for age for the primary outcomes.
In the Sensitivity analysis section we planned to assess the influence of small‐study effects on the results of a meta‐analysis, but this was only applicable in Comparison 1 for the outcome 'amount of active topical treatment used' (Analysis 1.4). Also in this section we were not able to perform a stratified analysis to compare study results from preregistered trials (e.g. available on Clinicaltrials.gov) with those without an available prespecified protocol as planned because none of the studies included in meta‐analyses were preregistered.
Contributions of authors
EvZ was the contact person with the editorial base. EvZ co‐ordinated contributions from co‐authors and wrote the final draft of the review. EvZ and ZF screened papers against eligibility criteria. EvZ and ZF obtained data on ongoing and unpublished studies. EvZ translated German and French studies. EvZ and ZF assessed 'Risk of bias' of the studies. EvZ and ZF extracted data for the review and sought additional information about papers. EvZ and ZF entered data into RevMan 5. EvZ, ZF and RC analysed and interpreted data. EvZ, ZF and RC worked on the methods sections. EvZ, ZF, AL and BA drafted the clinical sections of the background and responded to the clinical comments of the referees. EvZ, ZF, and RC responded to the methodology and statistics comments of the referees. BA was the consumer co‐author and checked the review for readability and clarity, as well as ensuring outcomes are relevant to consumers. EvZ is the guarantor of the update.
Disclaimer
This project was supported by the National Institute for Health Research (NIHR), via Cochrane Infrastructure funding and Cochrane Incentive funding to the Cochrane Skin Group. The views and opinions expressed herein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, National Health Service or the Department of Health.
Sources of support
Internal sources
No sources of support supplied
External sources
-
Oak Foundation, Denmark
The Parker Institute (RC) is supported by grants from the Oak Foundation, a philantropic/non‐profit organisation.
-
The National Institute for Health Research (NIHR), UK
The NIHR, UK, is the largest single funder of the Cochrane Skin Group.
Declarations of interest
Esther J van Zuuren: nothing to declare. Zbys Fedorowicz: nothing to declare. Adriana Lavrijsen: nothing to declare. Robin Christensen: nothing to declare. Bernd Arents: nothing to declare. Matthew Ridd (referee of the protocol): "I am chief investigator on a feasibility trial comparing four commonly used emollients in children with eczema (not yet published but likely to be included in this review). I have recently submitted an application for funding to take this study to a full trial." Sandra Lawton (referee of the protocol): "I have received an honorarium for speaking at meetings from Genus, Almirall, and Thornton & Ross Ltd, and for reviewing an educational programme for Bayer."
Edited (no change to conclusions)
References
References to studies included in this review
Abramovits 2008 {published data only}
- Abramovits W, Boguniewicz M, Adult Atopiclair Study Group. A multicenter, randomized, vehicle-controlled clinical study to examine the efficacy and safety of MAS063DP (Atopiclair) in the management of mild to moderate atopic dermatitis in adults. Journal of Drugs in Dermatology 2006;5(3):236-44. [PMID: ] [PubMed] [Google Scholar]
- Abramovits W, Hebert A, Boguniewicz M. A multicenter randomized, vehicle-controlled, double-blind clinical study to examine the safety and efficacy of MAS063DP in the management of AD. Journal of the American Academy of Dermatology 2006;54(Suppl 3):AB84. [PubMed] [Google Scholar]
- *.Abramovits W, Hebert AA, Boguniewicz M, Kempers SE, Tschen E, Jarratt MT, et al. Patient-reported outcomes from a multicenter, randomized, vehicle-controlled clinical study of MAS063DP (Atopiclair) in the management of mild-to-moderate atopic dermatitis in adults. Journal of Dermatological Treatment 2008;19(6):327-32. [PMID: ] [DOI] [PubMed] [Google Scholar]
Åkerström 2015 {published data only}
- Åkerström U, Reitamo S, Langeland T, Berg M, Rustad L, Korhonen L. Comparison of moisturizing creams for the prevention of atopic dermatitis relapse: a randomized double-blind controlled multicentre clinical trial. Acta Dermato-Venereologica 2015;95(5):587-92. [PMID: ] [DOI] [PubMed] [Google Scholar]
Andersson 1999 {published data only}
- *.Andersson A-C, Lindberg M, Lodén M. The effect of two urea-containing creams on dry, eczematous skin in atopic patients. I. Expert, patient and instrumental evaluation. Journal of Dermatological Treatment 1999;10(3):165-9. [Google Scholar]
- Lodén M, Andersson AC, Lindberg M. The effect of two urea-containing creams on dry, eczematous skin in atopic patients. Journal of Dermatological Treatment 1999;10(3):171-5. [Google Scholar]
Angelova‐Fischer 2014 {published data only}
- Angelova-Fischer I, Neufang G, Jung K, Fischer TW, Zillikens D. A randomized, investigator-blinded efficacy assessment study of stand-alone emollient use in mild to moderately severe atopic dermatitis flares. Journal of the European Academy of Dermatology and Venereology : JEADV 2014;28(Suppl 3):9-15. [PMID: ] [DOI] [PubMed] [Google Scholar]
Belloni 2005 {published data only}
- Belloni G, Pinelli S, Veraldi S. A randomised, double-blind, vehicle-controlled study to evaluate the efficacy and safety of MAS063D (Atopiclair) in the treatment of mild to moderate atopic dermatitis. European Journal of Dermatology 2005;15(1):31-6. [PMID: ] [PubMed] [Google Scholar]
Berents 2015 {published data only}
- Berents TL, Rønnevig J, Søyland E, Gaustad P6, Nylander G, Løland BF. Topical treatment with fresh human milk versus emollient on atopic eczema spots in young children: a small, randomized, split body, controlled, blinded pilot study. BMC Dermatology 2015;15:7. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Berth‐Jones 2003 {published data only}
- *.Berth-Jones J, Damstra RJ, Golsch S, Livden JK, Van Hooteghem O, Allegra F, et al. Twice weekly fluticasone propionate added to emollient maintenance treatment to reduce risk of relapse in atopic dermatitis: randomised, double blind, parallel group study. BMJ 2003;326(7403):1367. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glazenburg E, Graham-Brown R, Hanifin J, Berth-Jones J, Meer J. Intermittent dosing with topical fluticasone propionate delays the time to relapse in adults and children with chronic atopic dermatitis - two randomised controlled studies. Journal of Investigative Dermatology 2001;117(2):533. [Google Scholar]
Bissonnette 2010 {published data only}
- Bissonnette R, Maari C, Provost N, Bolduc C, Nigen S, Rougier A, et al. A double-blind study of tolerance and efficacy of a new urea-containing moisturizer in patients with atopic dermatitis. Journal of Cosmetic Dermatology 2010;9(1):16-21. [PMID: ] [DOI] [PubMed] [Google Scholar]
Boguniewicz 2008 {published data only}
- Boguniewicz M, Eichenfield L, Hebert A, Jarratt M. A multicenter, randomized, vehicle-controlled clinical study to examine the efficacy and safety of MAS063DP nonsteroidal cream in the management of mild to moderate atopic dermatitis in infants and children. Journal of the American Academy of Dermatology 2007;56(2):AB69. [Google Scholar]
- *.Boguniewicz M, Zeichner JA, Eichenfield LF, Hebert AA, Jarratt M, Lucky AW et al. MAS063DP is effective monotherapy for mild to moderate atopic dermatitis in infants and children: a multicenter, randomized, vehicle-controlled study. The Journal of Pediatrics 2008;152(6):854-9. [PMID: ] [DOI] [PubMed] [Google Scholar]
Bohnsack 1997 {published data only}
- Bohnsack K, Tausch I, Gassmuller J, Rippke F. Efficacy on the symptom "dry skin"and long-term dermal tolerance of Laceran Lotion 10% urea in patients with atopic dermatitis [Wirksamkeit auf das Symptom "trockene Haut" und Langzeitveträglichkeit von Laceran Lotion 10% Urea bei Patienten mit Atopischem Ekzem]. Zeitschrift fur Hautkrankheiten 1997;72(1):34-9. [Google Scholar]
Boralevi 2014 {published data only}
- Boralevi F, Saint Aroman M, Delarue A, Raudsepp H, Kaszuba A, Bylaite M, et al. Long-term emollient therapy improves xerosis in children with atopic dermatitis. Journal of the European Academy of Dermatology and Venereology : JEADV 2014;28(11):1456-62. [DOI: 10.1111/jdv.12314] [PMID: ] [DOI] [PubMed] [Google Scholar]
Breternitz 2008 {published data only}
- Breternitz M, Kowatzki D, Langenauer M, Elsner P, Fluhr JW. Placebo-controlled, double-blind, randomized, prospective study of a glycerol-based emollient on eczematous skin in atopic dermatitis: biophysical and clinical evaluation. Skin Pharmacology and Physiology 2008;21(1):39-45. [PMID: ] [DOI] [PubMed] [Google Scholar]
Danby 2011 {published data only}
- *.Danby S, Al Enezi T, Chittock J, Kennedy K, Sultan A, Cork M. A randomized comparison of aqueous cream and Oilatum Junior bath additive on skin barrier function in atopic dermatitis. British Journal of Dermatology 2011;165(Suppl 1):44-5. [DOI] [PubMed] [Google Scholar]
- Danby S, Al Enezi T, Chittock J, Kennedy K, Sultan A, Cork M. A randomized comparison of aqueous cream and Oliatum junior bath additive on skin barrier function in atopic dermatitis. British Journal of Dermatology 2011;165(1):115. [DOI] [PubMed] [Google Scholar]
De Belilovsky 2011 {published data only}
- De Belilovsky C, Baudouin C, Bredif S, Chadoutaud B, Msika P. Sunflower oleodistillate: A topical PPAR-alpha (peroxisome proliferator-activated receptors) agonist developed for atopic dermatitis. Journal of Investigative Dermatology 2011;131(S1):S141. [Google Scholar]
- De Belilovsky C, Chadoutaud B, Baudouin C, Msika P. Sunflower oleodistillate: A topical PPAR-alpha agonist developed for atopic dermatitis. Journal of the American Academy of Dermatology 2011;64(2 Suppl 1):AB58. [Google Scholar]
- De Belilovsky C, Msika P, Menu F, Baudouin C, Chadoutaud B. Natural PPAR-alpha agonist and atopic dermatitis: From research to clinical efficacy. European Journal of Pediatric Dermatology 2010;20(1):63. [Google Scholar]
- *.De Belilovsky C, Roo-Rodriguez E, Baudouin C, Menu F, Chadoutaud B, Msika P. Natural peroxisome proliferator-activated receptor-alpha agonist cream demonstrates similar therapeutic response to topical steroids in atopic dermatitis. Journal of Dermatological Treatment 2011;22(6):359-65. [PMID: ] [DOI] [PubMed] [Google Scholar]
Draelos 2008 {published data only}
- Draelos ZD. The effect of ceramide-containing skin care products on eczema resolution duration. Cutis 2008;81(1):87-91. [PMID: ] [PubMed] [Google Scholar]
Draelos 2009 {published data only}
- Draelos ZD. An evaluation of prescription device moisturizers. Journal of Cosmetic Dermatology 2009;8(1):40-3. [PMID: ] [DOI] [PubMed] [Google Scholar]
Draelos 2011 {published data only}
- Draelos ZD. A clinical evaluation of the comparable efficacy of hyaluronic acid-based foam and ceramide-containing emulsion cream in the treatment of mild-to-moderate atopic dermatitis. Journal of Cosmetic Dermatology 2011;10(3):185-8. [PMID: ] [DOI] [PubMed] [Google Scholar]
Emer 2011 {published data only}
- Emer JJ, Frankel A, Sohn A, Lebwohl M. A bilateral comparison study of pimecrolimus cream 1% and a topical medical device cream in the treatment of patients with atopic dermatitis. Journal of Drugs in Dermatology 2011;10(7):735-43. [PMID: ] [PubMed] [Google Scholar]
Evangelista 2014 {published data only}
- *.Evangelista MT, Abad-Casintahan F, Lopez-Villafuerte L. The effect of topical virgin coconut oil on SCORAD index, transepidermal water loss, and skin capacitance in mild to moderate pediatric atopic dermatitis: a randomized, double-blind, clinical trial. International Journal of Dermatology 2014;53(1):100-8. [PMID: ] [DOI] [PubMed] [Google Scholar]
- Evangelista MTP, Casintahan FA, Villafuerte LL. The effect of topical virgin coconut oil on SCORAD, transepidermal water loss and skin capacitance in mild to moderate pediatric atopic dermatitis: A randomized, double-blind clinical trial. In: Conference: 2013 Annual American Contact Dermatitis Society, ACDS Meeting Miami Beach, FL United States. 2013.
Faergemann 2009 {published data only}
- *.Faergemann J, Olsson P, Svensson A. A randomized, single-blind comparison of the efficacy, tolerability and cosmetic acceptance of Propyless or Fenuril treatment of patients with dry skin. Acta Dermato-Venereologica 2009;89(3):305-7. [PMID: ] [DOI] [PubMed] [Google Scholar]
- Faergemann J, Svensson A. A randomised investigator-blind study comparing the efficacy, tolerability and cosmetic acceptance of Propyless and Fenuril on dry skin. Journal of the European Academy of Dermatology and Venereology : JEADV 2005;19(Suppl 2):196-7. [Google Scholar]
Ferreira 1998 {published data only}
- *.Ferreira MJ, Fiadeiro T, Silva M, Soares AP. Electrical conductance: a controversial parameter in the evaluation of emollients in atopic dermatitis. Skin Research and Technology 1998;4(3):138-41. [DOI: 10.1111/j.1600-0846.1998.tb00099.x] [DOI] [PubMed] [Google Scholar]
- Ferreira MJ, Fiadeiro T, Silva M, Soares AP. Topical gamma-linolenic acid therapy in atopic dermatitis. A clinical and biometric evaluation. Allergo Journal 1998;7(4):213-6. [Google Scholar]
Frankel 2011 {published data only}
- Frankel A, Sohn A, Emer J, Lebwohl M. Bilateral comparison study of pimecrolimus cream 1% and a ceramide-hyaluronic acid based emollient foam in the treatment of patients with atopic dermatitis. Journal of the American Academy of Dermatology 2011;64(2 Suppl 1):AB59. [PubMed] [Google Scholar]
- *.Frankel A, Sohn A, Patel RV, Lebwohl M. Bilateral comparison study of pimecrolimus cream 1% and a ceramide-hyaluronic acid emollient foam in the treatment of patients with atopic dermatitis. Journal of Drugs in Dermatology 2011;10(6):666-72. [PMID: ] [PubMed] [Google Scholar]
Fredriksson 1975 {published data only}
- Fredriksson T, Gip L. Urea creams in the treatment of dry skin and hand dermatitis. International Journal of Dermatology 1975;14(6):442-4. [PMID: ] [DOI] [PubMed] [Google Scholar]
Gao 2008 {published data only}
- Gao Y. Effectiveness observation on moisturizer for infant eczema. China Journal of Leprosy and Skin Diseases [Zhong Guo Ma Feng Pi Fu Bing Za Zhi] 2008;24(4):294. [Google Scholar]
Gayraud 2015 {published data only}
- Gayraud F, Imko-Walczuk, Sayag M, Jourdan E. Comparative, randomized, double-blinded study assessing the efficacy of a new kind of dermocosmetic product containing skin barrier therapy on infants and children with moderate atopic dermatitis. Journal of the German Society of Dermatology 2014;12(Suppl 2):14. [Google Scholar]
- *.Gayraud F, Sayag M, Jourdan E. Efficacy and tolerance assessment of a new type of dermocosmetic in infants and children with moderate atopic dermatitis. Journal of Cosmetic Dermatology 2015;14(2):107-12. [PMID: ] [DOI] [PubMed] [Google Scholar]
Gehring 1996 {published data only}
- Gehring W, Gloor M. Treatment of the atopic dermatitis with a water-in-oil emulsion with or without the addition of hydrocortisone - Results of a controlled double-blind randomized study using clinical evaluation and bioengineering methods [Behandlung der neurodermitis atopica mit einer W/O-Emulsion mit und ohne Hydrocortison - Ergebnisse einder klinisch u. meßmethodische controllierten randomisierten Doppelblindstudie]. H+G Zeitschrift für Hautkrankheiten 1996;71(7):554-60. [Google Scholar]
Gehring 1999 {published data only}
- Gehring W, Bopp R, Rippke F, Gloor M. Effect of topically applied evening primrose oil on epidermal barrier function in atopic dermatitis as a function of vehicle. Arzneimittel-Forschung 1999;49(7):635-42. [DOI] [PubMed] [Google Scholar]
Giordano‐Labadie 2006 {published data only}
- Giordano Labadie F, Cambazard F, Guillet C, Combemale P, Mengeaud V. Interest of a moisturizer milk containing oat rhealba extracts in atopic dermatitis. In: 20th World Congress of Dermatology Paris 1st- 5th of July. P0203 edition. 2002.
- *.Giordano-Labadie F, Cambazard F, Guillet G, Combemale P, Mengeaud V. Evaluation of a new moisturizer (Exomega milk) in children with atopic dermatitis. Journal of Dermatological Treatment 2006;17(2):78-81. [PMID: ] [DOI] [PubMed] [Google Scholar]
Glazenburg 2009 {published data only}
- *.Glazenburg EJ, Wolkerstorfer A, Gerretsen AL, Mulder PG, Oranje AP. Efficacy and safety of fluticasone propionate 0.005% ointment in the long-term maintenance treatment of children with atopic dermatitis: differences between boys and girls? Pediatric Allergy and Immunology 2009;20(1):59-66. [PMID: ] [DOI] [PubMed] [Google Scholar]
- Glazenburg EJ, Wolkerstorfer A, Gerretsen AL, Oranje AP. Twice weekly topical fluticasone propionate delays the time to relapse in children with chronic atopic dermatitis. Journal of the European Academy of Dermatology and Venereology : JEADV 2003;17(Suppl 3):184. [Google Scholar]
Grimalt 2007 {published data only}
- Grimalt R, Cambazard F. Evaluation of the corticosteroid-sparing effect of a new emollient in 162 atopic infants. In: 4th European Association of Dermatology and Venereology (EADV) Spring Symposium Saariselka, Lapland, Finland. February 9-12th. 2006:P-009.
- *.Grimalt R, Mengeaud V, Cambazard F, Study IG . The steroid-sparing effect of an emollient therapy in infants with atopic dermatitis: a randomized controlled study. Dermatology 2007;214(1):61-7. [PMID: ] [DOI] [PubMed] [Google Scholar]
- Josse M, Mengeaud V, Durosier V, Sibaud V, Grimalt R, Cambazard F. Evaluation of the Corticosteroid-Sparing Effect of an Emollient Milk in a Large Population of Infants Affected by Atopic Dermatitis. Journal of Investigative Dermatology 2005;125(3):612. [Google Scholar]
Hagströmer 2001 {published data only}
- Hagströmer L, Nyrén M, Emstesam L. Urea and sodium chloride in moisturisers for dry atopic skin: A double-blind, randomised, placebo-controlled study. Journal of the European Academy of Dermatology and Venereology : JEADV 1999;12(Suppl 2):S160. [Google Scholar]
- *.Hagströmer L, Nyrén M, Emtestam L. Do urea and sodium chloride together increase the efficacy of moisturisers for atopic dermatitis skin? A comparative, double-blind and randomised study. Skin Pharmacology and Applied Skin Physiology 2001;14(1):27-33. [PMID: ] [DOI] [PubMed] [Google Scholar]
- Hagströmer L, Nyrén M, Emtestam L. Moisturisers for dry atopic skin: a double-blind, randomised, placebo-controlled study. Contact Dermatitis 2000;42(Suppl):52. [Google Scholar]
Hagströmer 2006 {published data only}
- Hagströmer L, Kuzmina N, Lapins J, Talme T, Emtestam L. Biophysical assessment of atopic dermatitis skin and effects of a moisturizer. Clinical and Experimental Dermatology 2006;31(2):272-7. [PMID: ] [DOI] [PubMed] [Google Scholar]
Hamada 2008 {published data only}
- Hamada M, Gyoutoku T, Sato S, Matsuda T, Kinukawa N, Furue M. The usefulness of camellia oil spray for treatment of atopic dermatitis. Nishinihon Journal of Dermatology 2008;70(2):213-8. [Google Scholar]
Hanifin 1998 {published data only}
- Hanifin JM, Hebert AA, Mayes S, Paller A, Sheretz EF, Wagner Aetal. Bilateral regimen comparison of desonide lotion, 0.05% vs desonide lotion, 0.05% plus a moisturizing cream in patients with atopic dermatitis. In: Australasian Journal of Dermatology. Vol. 38. 1997:233.
- *.Hanifin JM, Hebert AA, Mays SR, Paller A, Sherertz EF, Wagner AM, et al. Effects of a low-potency corticosteroid lotion plus a moisturizing regimen in the treatment of atopic dermatitis. Current Therapeutic Research, Clinical and Experimental 1998;59(4):227-33. [Google Scholar]
Hanifin 2002 {published data only}
- Glazenburg EJ, Meer JB. Safety of fluticasone propionate. Journal of the European Academy of Dermatology and Venereology : JEADV 2002;16(Suppl 1):P2-34. [Google Scholar]
- Hanifin J, Berth-Jones J. Consensus from 4 studies—use of twice weekly fluticasone propionate can maintain remission in moderate to severe atopic dermatitis. Journal of Investigative Dermatology 2003;121(1):199. [Google Scholar]
- *.Hanifin J, Gupta AK, Rajagopalan R. Intermittent dosing of fluticasone propionate cream for reducing the risk of relapse in atopic dermatitis patients. British Journal of Dermatology 2002;147(3):528-37. [PMID: ] [DOI] [PubMed] [Google Scholar]
Harper 1995 {published data only}
- Harper J. Double-blind comparison of an antiseptic oil-based bath additive (Oilatum Plus) with regular Oilatum (Oilatum emollient) for the treatment of atopic eczema. In: Lever R, Levy J, editors(s). The Bacteriology of Eczema. Round Table Series 37 edition. Vol. 37. London: The Royal Society of Medicine Press Ltd, 1995:42-7. [Google Scholar]
Hlela 2015 {published data only}
- Hlela C, Lunjani N, Gumedze F, Kakande B, Khumalo NP. Affordable moisturisers are effective in atopic eczema: A randomised controlled trial. South African Medical Journal 2015;105(9):780-4. [DOI] [PubMed] [Google Scholar]
Janmohamed 2014 {published data only}
- Janmohamed SR, Gutermuth J, Oranje AP. The wet-wrap method with diluted corticosteroids versus emollients in children with atopic dermatitis-a prospective, randomized, double-blind, placebo controlled trial. Journal of Investigative Dermatology 2015;135(S2):S38. [DOI] [PubMed] [Google Scholar]
- *.Janmohamed SR, Oranje AP, Devillers AC, Rizopoulos D, Praag MC, Van Gysel, et al. The proactive wet-wrap method with diluted corticosteroids versus emollients in children with atopic dermatitis: a prospective, randomized, double-blind, placebo-controlled trial. Journal of the American Academy of Dermatology 2014;70(6):1076-82. [PMID: ] [DOI] [PubMed] [Google Scholar]
Jirabundansuk 2014 {published data only}
- Jirabundansuk P, Ophaswongse S, Udompataikul M. Comparative trial of moisturizer containing spent grain wax, Butyrospermum parkii extract, Argania spinosa kernel oil vs. 1% hydrocortisone cream in the treatment of childhood atopic dermatitis. Journal of the Medical Association of Thailand 2014;97(8):820-6. [PMID: ] [PubMed] [Google Scholar]
Kircik 2009 {published data only}
- Kircik L. Skin barrier function and hydration effects of hydrolipid cream alone and in combination in the treatment of mild to moderate atopic dermatitis: Investigator-blinded, split-body, pilot study results. Journal of the American Academy of Dermatology 2009;62(3 Suppl 1):AB67. [Google Scholar]
Kircik 2014 {published data only}
- Kircik LH. Effect of skin barrier emulsion cream vs a conventional moisturizer on transepidermal water loss and corneometry in atopic dermatitis: a pilot study. Journal of Drugs in Dermatology 2014;13(12):1482-4. [PMID: 25607793] [PubMed] [Google Scholar]
Korting 2010 {published data only}
- Korting HC, Schöllmann C, Cholcha W, Wolff L, Collaborative SG . Efficacy and tolerability of pale sulfonated shale oil cream 4% in the treatment of mild to moderate atopic eczema in children: a multicentre randomized vehicle-controlled trial. Journal of the European Academy of Dermatology and Venereology : JEADV 2010;24(10):1176-82. [PMID: ] [DOI] [PubMed] [Google Scholar]
Larregue 1996 {published data only}
- Larregue M, Devaux J, Audebert C, Gelmetti DR. A double-blind controlled study on the efficacy and tolerability of 6% ammonium lactate cream in children with atopic dermatitis. Nouvelles Dermatologiques 1996;15(10):720-1. [Google Scholar]
Laumann 2006 {published data only}
- Laumann A, Lai S, Lucky AW, Schlessinger J, Jarratt M Jones TM, et al. The efficacy and safety of MimyX Cream in reducing the risk of relapse in atopic dermatitis. Journal of Investigative Dermatology 2006;126(Suppl 1s):45. [Google Scholar]
Lodén 2001 {published data only}
- Lodén M, Andersson AC, Andersson C, Frödin T, Oman H, Lindberg M. Instrumental and dermatologist evaluation of the effect of glycerine and urea on dry skin in atopic dermatitis. Skin Research and Technology 2001;7(4):209-13. [PMID: ] [PubMed] [Google Scholar]
Lodén 2002 {published data only}
- Lodén M, Andersson AC, Anderson C, Bergbrant IM, Frödin T, Ohman H, et al. A double-blind study comparing the effect of glycerin and urea on dry, eczematous skin in atopic patients. Acta Dermato-Venereologica 2002;82(1):45-7. [PMID: ] [DOI] [PubMed] [Google Scholar]
Marseglia 2014 {published data only}
- Marseglia A, Licari A, Agostinis F, Barcella A, Bonamonte D, Puviani M, et al. Local rhamnosoft, ceramides and L-isoleucine in atopic eczema: a randomized, placebo controlled trial. Pediatric Allergy and Immunology 2014;25(3):271-5. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Miller 2011 {published data only}
- Miller DW, Clark AR, Fleischer AB, Yentzer BA, Koch SB. An over the counter moisturizer is as clinically effective as, and more cost-effective than, prescription barrier creams in the treatment of children with mild to moderate atopic dermatitis. Journal of the American Academy of Dermatology 2011;64(2 Suppl 1):AB57. [PubMed] [Google Scholar]
- *.Miller DW, Koch SB, Yentzer BA, Clark AR, O'Neill JR, Fountain J, et al. An over-the-counter moisturizer is as clinically effective as, and more cost-effective than, prescription barrier creams in the treatment of children with mild-to-moderate atopic dermatitis: a randomized, controlled trial. Journal of Drugs in Dermatology 2011;10(5):531-7. [PMID: ] [PubMed] [Google Scholar]
Msika 2008 {published data only}
- Msika C, De Belilovsky C, Menu F, Baudouin C, Chadoutaud B. Natural PPAR-alpha agonist and atopic dermatitis: From research to clinical efficacy. Contact Dermatitis 2010;63(Suppl 1):68. [Google Scholar]
- Msika P, De Belilovsky C, Chadoutaud IB, Nicolas JF. New Natural PPAR-a agonist for childhood atopic dermatitis: Dermocorticoid-sparing and quality of life improvement. Journal of Investigative Dermatology 2006;126(Suppl 3):S102. [Google Scholar]
- Msika P, De Belilovsky C, Chadoutaud IB, Nicolas JF. New natural PPAR-a agonist for childhood atopic dermatitis: Dermocorticoid- sparing and quality of life improvement. Journal of the American Academy of Dermatology 2007;56(2):AB67. [Google Scholar]
- Msika P, De Belilovsky C, Menu F, Baudouin C, Chadoutaud B. Natural PPAR-alpha agonist and Atopic dermatitis: From research to clinical efficacy. Journal of Investigative Dermatology 2010;130(10):2524. [Google Scholar]
- Msika P, De Belilovsky C, Menu F, Baudouin C, Chadoutaud B. Natural PPAR-alpha agonist and atopic dermatitis: From research to clinical efficacy. Journal of Investigative Dermatology 2010;130(Suppl 1):S54. [Google Scholar]
- *.Msika P, De Belilovsky C, Piccardi N, Chebassier N, Baudouin C, Chadoutaud B. New emollient with topical corticosteroid-sparing effect in treatment of childhood atopic dermatitis: SCORAD and quality of life Improvement. Pediatric Dermatology 2008;25(6):606-12. [PMID: ] [DOI] [PubMed] [Google Scholar]
- Msika P, Piccirilli A, Piccardi N, Choulot JC, Chadoutaud, B. Steroid sparing effect of an emollient in the treatment of mild to moderate eczema. Pediatric Dermatology 2004;21(3):382. [Google Scholar]
Namazova‐Baranova 2012 {published data only}
- Namazova-Baranova L, Vishneva E, Levina J, Torshkhoeva R, Alekseeva A, Efendieva K, et al. Combined therapy of atopic dermatitis in children. Allergy 2012;67(Suppl 96):181-2. [Google Scholar]
- *.Namazova-Baranova LS, Vishneva EA, Torshhoeva RM, Dzagoeva ZN, Alexeeva AA, Levina JG, et al. Non-steroidal topical medications in the treatment of atopic dermatitis in children. Pediatric Pharmacology [Pediatricheskaya farmakologiya] 2012;9(1):66-70. [Google Scholar]
Nebus 2009 {published data only}
- Nebus J, Nystrand G, Fowler J, Wallo W. A daily oat-based skin care regimen for atopic skin. Journal of the American Academy of Dermatology 2009;62(3 Suppl 1):AB67. [Google Scholar]
Nho 2014 {published data only}
- Kim YS, Jung YL, Youm JK, Park JH, Bae YI, Lee SH. The effects of peroxisome proliferator activated receptor α (PPARα) activator on patients with facial erythema. Korean Journal of Dermatology 2014;52(8):608-14. [Google Scholar]
- *.Nho Y, Kim H, Jung Y, Kim S, Kim Y, Lee Setal. A combination of PPARα activator and ceramide improves red face originated from variable skin diseases. Journal of Investigative Dermatology 2014;134(S1):S95. [Google Scholar]
Noh 2011 {published data only}
- Noh S, Jung JY, Park WS, Koh HJ, Lee KH. The Steroid-sparing Effect of an Emollient APDDR-0801 in Patients with Atopic Dermatitis. Korean Journal of Dermatology 2011;49(3):227-33. [Google Scholar]
Nuñez 2013 {published data only}
- Nuñez C, Hogan D, Humphrey M, Zhang P, Lisante T, Doshi U. A colloidal oatmeal OTC cream is as clinically effective as a prescription barrier repair cream for the management of mild to moderate atopic dermatitis in African American children. Journal of the American Academy of Dermatology 2013;68(4 Suppl 1):AB73. [Google Scholar]
Park 2014 {published data only}
- Park SB, Im M, Lee Y, Lee JH, Lim J, Park YH, et al. Effect of emollients containing vegetable-derived lactobacillus in the treatment of atopic dermatitis symptoms: split-body clinical trial. Annals of Dermatology 2014;26(2):150-5. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Patrizi 2008 {published data only}
- Patrizi A, Capitanio B, Neri I, Giacomini F, Sinagra JL, Raone B, et al. A double-blind, randomized, vehicle-controlled clinical study to evaluate the efficacy and safety of MAS063DP (ATOPICLAIR[trademark]) in the management of atopic dermatitis in paediatric patients. Pediatric Allergy and Immunology 2008;19(7):619-25. [PMID: ] [DOI] [PubMed] [Google Scholar]
Patrizi 2014 {published data only}
- Bianchi P, Theunis J, Casas C, Villeneuve C, Patrizi A, Phulpin C, et al. Effects of a New Emollient-Based Treatment on Skin Microflora Balance and Barrier Function in Children with Mild Atopic Dermatitis. Pediatric Dermatology 2016;33(2):165-71. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bianchi P, Villeneuve C, Theunis J, Casas C, Patrizi A, Bacquey A, et al. Evaluation of a novel emollient balm containing Aquaphilus dolomiae extract in atopic dermatitis children: Effect on clinical parameters, skin barrier and microflora. Journal of Investigative Dermatology 2014;134(Suppl 1):S96. [Google Scholar]
- *.Patrizi A, Bacquey A, Schmitt AM, Decoster CJ, Phulpin C, Theunis J, et al. Clinical and biometrologic evaluation of a novel emollient balm containing an Aquaphilus dolomiae extract in 1-to 4-year-old children suffering from atopic dermatitis: International,multicenter, randomized versus control group study. Journal of the American Academy of Dermatology 2014;70(5 Suppl 1):AB62. [Google Scholar]
Peltonen 2014 {published data only}
- Peltonen JM, Pylkkänen L, Jansén CT, Volanen I, Lehtinen T, Laihia JK, et al. Three randomised phase I/IIa trials of 5% cis-urocanic acid emulsion cream in healthy adult subjects and in patients with atopic dermatitis. Acta Dermato-Venereologica 2014;94(4):415-20. [PMID: ] [DOI] [PubMed] [Google Scholar]
Peserico 2008 {published data only}
- Peserico A, Städtler G, Sebastian M, Fernandez RS, Vick K, Bieber T. Reduction of relapses of atopic dermatitis with methylprednisolone aceponate cream twice weekly in addition to maintenance treatment with emollient: a multicentre, randomized, double-blind, controlled study. British Journal of Dermatology 2008;158(4):801-7. [PMID: ] [DOI] [PubMed] [Google Scholar]
Pigatto 1996 {published data only}
- Pigatto PD, Bigardi AS, Cannistraci C, Picardo M. 10% urea cream (Laceran) for atopic dermatitis: A clinical and laboratory evaluation. Journal of Dermatological Treatment 1996;7(3):171-5. [Google Scholar]
Puschmann 2003 {published data only}
- Puschmann M, Melzer A, Welzel J. Extensive treatment of itching, dry dermatoses with a polidocanol-urea-combination. Aktuelle Dermatologie 2003;29(3):77-81. [Google Scholar]
Shi 2015 {published data only}
- *.Shi VY, Foolad N, Ornelas JN, Hassoun L, Monico G, Takeda N, et al. Comparing the effect of bleach and water baths on skin barrier function in atopic dermatitis: a split-body randomized controlled trial. British Journal of Dermatology 2016;175(1):212-4. [PMID: ] [DOI] [PubMed] [Google Scholar]
- Shi VY, Foolad N, Takeda N, Hassoun L, Johal R, Saric S, et al. The effect of dilute bleach bath and moisturizers on skin barrier function in atopic dermatitis. Journal of the American Academy of Dermatology 2015;72(Suppl 1):AB76. [Google Scholar]
Shiratori 1977 {published data only}
- Shiratori A, Ikazi M, Tamada T, Sato Y, Igarashi R, Ishikawa H, et al. A double-blind study on clinical efficacy of urea ointment. Rinsho Hyoka (Clinical Evaluation) 1977;5(1):103-25. [Google Scholar]
Simpson 2011 {published data only}
- Dutronc Y, Guennoun M. Hydration potential of a new body moisturizer. Journal of the American Academy of Dermatology 2011;64(2 Suppl 1):AB58. [Google Scholar]
- *.Simpson E, Dutronc Y. A new body moisturiser increases skin hydration and improves atopic dermatitis symptoms among children and adults. Journal of Drugs in Dermatology 2011;10(7):744-9. [PMID: ] [PubMed] [Google Scholar]
- Simpson E Dutronc Y Caveney S. A new body moisturizer increases skin hydration among children and adults with atopic dermatitis symptoms. Seminars in Cutaneous Medicine and Surgery 2012;31(1):A5. [Google Scholar]
Simpson 2013 {published data only}
- *.Simpson E, Böhling A, Bielfeldt S, Bosc C, Kerrouche N. Improvement of skin barrier function in atopic dermatitis patients with a new moisturizer containing a ceramide precursor. Journal of Dermatological Treatment 2013;24(2):122-5. [PMID: ] [DOI] [PubMed] [Google Scholar]
- Simpson E. Improvement of skin barrier function in atopic dermatitis patients with a new moisturizer containing a ceramide precursor. Journal of the American Academy of Dermatology 2013;68(4 Suppl 1):AB77. [DOI] [PubMed] [Google Scholar]
Sugarman 2009 {published data only}
- Sugarman IL, Parish LJ. A topical physiologic lipid-based, barrier repair formulation (Epiceram™ cream) is highly effective monotherapy for moderate-to-severe pediatric atopic dermatitis: a multicenter, investigator-blinded trial comparing a barrier repair formulation, Epiceram™, to fluticasone proprionate (Cutivate®) cream. Journal of Investigative Dermatology 2008;128(Suppl 1):S54. [Google Scholar]
- *.Sugarman JL, Parish LC. Efficacy of a lipid-based barrier repair formulation in moderate-to-severe pediatric atopic dermatitis. Journal of Drugs in Dermatology 2009;8(12):1106-11. [PMID: ] [PubMed] [Google Scholar]
Takeuchi 2012 {published data only}
- *.Takeuchi S, Saeki H, Tokunaga S, Sugaya M, Ohmatsu H, Tsunemi Y, et al. A randomized, open-label, multicenter trial of topical tacrolimus for the treatment of pruritis in patients with atopic dermatitis. Annals of Dermatology 2012;24(2):144-50. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Takeuchi S, Saeki H, Tokunaga S, Torii H, Nakamura K, Soma Y, et al. A randomized,multicenter trial of topical tacrolimus for treatment of pruritus in patients with atopic dermatitis. Acta Dermato-Venereologica 2009;89:704. [Google Scholar]
- Takeuchi S Furue M. Itch control in atopic dermatitis. In: New Trends in Allergy VII and 6th Georg Rajka Symposium on Atopic Dermatitis, Munich, Germany. 2010.
Tan 2010 {published data only}
- Tan WP, Goon A, Suresh S, Tey HL, Chiam LY. A randomized double-blind controlled trial to compare a triclosan-containing emollient with vehicle for the treatment of atopic dermatitis. Journal of the American Academy of Dermatology 2010;60(3 Suppl 1):AB70. [DOI] [PubMed] [Google Scholar]
- *.Tan WP, Suresh S, Tey HL, Chiam LY, Goon AT. A randomized double-blind controlled trial to compare a triclosan-containing emollient with vehicle for the treatment of atopic dermatitis. Clinical and Experimental Dermatology 2010;35(4):e109-12. [PMID: ] [DOI] [PubMed] [Google Scholar]
Thumm 2000 {published data only}
- Thumm EJ, Stoss M, Bayerl C, Schürholz T. Randomized trial to study efficacy of a 20% and 10% Hippophae rhamnoides containing creme used by patients with mild to intermediate atopic dermatitis [Überprüfung der Wirksamkeit einer 20%igen und 10%igen Sanddornkernölcreme bei Patienten mit leichter bis mittelgradiger atopischer Dermatitis]. Aktuelle Dermatologie 2000;26(8-9):285-90. [Google Scholar]
Tripodi 2009 {published data only}
- Tripodi S, Di Rienzo Businco A, Panetta V, Pingitore G, Volterrani A, Frediani T, et al. Lack of efficacy of topical furfuryl palmitate in pediatric atopic dermatitis: a randomized double-blind study. Journal of Investigational Allergology & Clinical Immunology 2009;19(3):204-9. [PMID: ] [PubMed] [Google Scholar]
Udompataikul 2011 {published data only}
- Udompataikul M, Srisatwaja W. Comparative trial of moisturizer containing licochalcone A vs. hydrocortisone lotion in the treatment of childhood atopic dermatitis: a pilot study. Journal of the European Academy of Dermatology and Venereology: JEADV 2011;25(6):660-5. [PMID: ] [DOI] [PubMed] [Google Scholar]
Verallo‐Rowell 2008 {published data only}
- Verallo-Rowell VM, Dillague KM, Syah-Tjundawan BS. Novel antibacterial and emollient effects of coconut and virgin olive oils in adult topic dermatitis. Dermatitis 2008;19(6):308-15. [PMID: ] [PubMed] [Google Scholar]
Wanakul 2013 {published data only}
- Wananukul S, Chatproedprai S, Chunharas A, Limpongsanuruk W, Singalavanija S, Chantorn R. Comparison study of moisturiser containing licochalcone A and 1%hydrocortisone in the treatment of childhood atopic dermatitis. Allergy 2012;67(Suppl 96):634. [PubMed] [Google Scholar]
- *.Wananukul S, Chatproedprai S, Chunharas A, Limpongsanuruk W, Singalavanija S, Nitiyarom R, et al. Randomized, double-blind, split-side, comparison study of moisturizer containing licochalcone A and 1% hydrocortisone in the treatment of childhood atopic dermatitis. Journal of the Medical Association of Thailand 2013;96(9):1135-42. [PMID: ] [PubMed] [Google Scholar]
Weber 2015 {published data only}
- Weber TM, Samarin F, Babcock MJ, Filbry A, Arrowitz CE, Rippke E. A novel daily moisturizing cream for effective management of mild to moderate atopic dermatitis in infants and children. Journal of the American Academy of Dermatology 2015;72(5 Suppl 1):AB73. [Google Scholar]
- *.Weber TM, Samarin F, Babcock MJ, Filbry A, Rippke F. Steroid-Free Over-the-Counter Eczema Skin Care Formulations Reduce Risk of Flare, Prolong Time to Flare, and Reduce Eczema Symptoms in Pediatric Subjects With Atopic Dermatitis. Journal of Drugs in Dermatology 2015;14(5):478-85. [PMID: ] [PubMed] [Google Scholar]
Wilhelm 1998 {published data only}
- Wilhelm KP, Schölermann A, Bohnsack K, Wilhelm D, Rippke F. Efficacy and tolerability of a topical preparation containing 10% urea in patients with atopic dermatitis [Wirksamkeit und Verträglichkeit einer topischer Zubereitung mit 10% Urea (Laceran® Salbe 10% Urea bei Neurodermitis]. Aktuelle Dermatologie 1998;24(1-2):26-30. [Google Scholar]
Wirén 2009 {published data only}
- Hjalte F, Asseburg C, Tennvall GR. Cost-effectiveness of a barrier-strengthening moisturizing cream as maintenance therapy vs. no treatment after an initial steroid course in patients with atopic dermatitis in Sweden--with model applications for Denmark, Norway and Finland. Journal of the European Academy of Dermatology and Venereology : JEADV 2010;24(4):474-80. [PMID: PMID: 19793150] [DOI] [PubMed] [Google Scholar]
- *.Wirén K, Nohlgård C, Nyberg F, Holm L, Svensson M, Johannesson A, et al. Treatment with a barrier-strengthening moisturizing cream delays relapse of atopic dermatitis: a prospective and randomized controlled clinical trial. Journal of the European Academy of Dermatology and Venereology: JEADV 2009;23(11):1267-72. [PMID: ] [DOI] [PubMed] [Google Scholar]
Wu 2014 {published data only}
- Wu Y-Q, Pan J-S, Zhao W-Q. Clinical observation of moisture and softening cream (MSC) combined with compound flumetasone ointment for chronic eczema. Journal of Clinical Dermatology 2014;43(7):434-6. [Google Scholar]
References to studies excluded from this review
Duggan 2015 {published data only}
- Duggan C. Eczema on trial. Journal of Family Health 2015;25(3):10, 12. [PubMed] [Google Scholar]
Dutronc 2011B {published data only}
- Dutronc Y. Irritation potential and cosmetic acceptability of a new body moisturizer. Journal of the American Academy of Dermatology 2011;64(2 Suppl 1):AB58. [Google Scholar]
Schoelermann 2003 {published data only}
- Schölermann A. 10% urea: an effective moisturizer in various dry skin conditions. In: 20th World Congress of Dermatology Paris 1st to 5th July. 2002- P0259.
- *.Schoelermann A, Fibry A, Rippke F. 10% urea: an effective moisturizer in various dry skin conditions. British Journal of Dermatology 2003;149(Suppl 64):79. [Google Scholar]
Szczepanowska 2008 {published data only}
- Szczepanowska J, Reich A, Szepietowski JC. Emollients improve treatment results with topical corticosteroids in childhood atopic dermatitis: a randomized comparative study. Pediatric Allergy and Immunology 2008;19(7):614-8. [PMID: ] [DOI] [PubMed] [Google Scholar]
Yang 2010 {published data only}
- Yang XY, Xu LM, Zhou AM, Wen H, Wu Y, Hao F, et al. The adjuvant treatment of atopic dermatitis with medical skin preparation containing extracts from Portulaca oleracea and avocado. Journal of Clinical Dermatology 2010;39(7):460-2. [Google Scholar]
References to ongoing studies
ACTRN12615000782538 {published data only}
- ACTRN12615000782538. A randomised, double blind, placebo controlled comparative trial of Ceramide Cream and Ceramide Cleanser in the management of moderate eczema in adults. apps.who.int/trialsearch/Trial2.aspx?TrialID=ACTRN12615000782538 Date first received: 28 July 2015.
ACTRN12615000920594 {published data only}
- ACTRN12615000920594. A randomised double blinded placebo controlled study investigating Atopis for the improvement of skin health in subjects with eczema. apps.who.int/trialsearch/Trial2.aspx?TrialID=ACTRN12615000920594 Date first received: 2 September 2015.
ACTRN12615001343594 {published data only}
- ACTRN12615001343594. Epaderm ointment in children with eczema [Pilot study comparing two emollients, Emulsifying ointment B.P. and Epaderm topical ointment in children with eczema]. apps.who.int/trialsearch/Trial2.aspx?TrialID=ACTRN12615001343594 Date first received: 9 December 2015.
ChiCTR‐IOR‐15007139 {published data only}
- ChiCTR-IOR-15007139. Effect andEfficacy of a Linoleic Acid-Ceramide Containing Moisturizer in atopic dermatitis [Effect and Efficacy of a Linoleic Acid-Ceramide Containing Moisturizer as an adjunctive therapy in the treatment of atopic dermatitis:A Randomized Controlled Trial]. apps.who.int/trialsearch/Trial2.aspx?TrialID=ChiCTR-IOR-15007139 Date first received: 31 August 2015.
EudraCT2004‐002926‐23 {published data only}
- EudraCT 2004-002926-23. Evaluation of the impact of the moisturizing milk RV2478B on the use of corticoids and on quality of life, in a population of children with atopic dermatitis. clinicaltrialsregister.eu/ctr-search/trial/2004-002926-23/IT Date first received: 15 January 2007.
EudraCT2005‐003396‐21 {published data only}
- EudraCT2005-003396-21. Long-term management of atopic dermatitis with the emollient V0034 CR. A randomised, placebo-controlled, parallel-groups, double-blind study in infants and children. clinicaltrialsregister.eu/ctr-search/search?query=2005-003396-21.
EudraCT2006‐000877‐30 {published data only}
- EudraCT2006-000877-30. A 6 week, multi centre study to evaluate the efficacy and safety of E45 complete emollient therapy and E45 itch relief cream in the treatment of mild to moderate atopic eczema compared to a patients normal emollient regime defined as the frequent use of emollient/s (not containing lauromacrogols) listed in the BNF. - Harbour Study. clinicaltrialsregister.eu/ctr-search/search?query=2006-000877-30.
EudraCT2007‐002133‐36 {published data only}
- EudraCT2007-002133-36. A multicenter, randomized, double-blind clinical study to examine the efficacy and safety of Zarzenda® in comparison to Elidel® in the management of mild to moderate atopic dermatitis in children and adolescents. clinicaltrialsregister.eu/ctr-search/search?query=2007-002133-36.
EudraCT2008‐003485‐25 {published data only}
- EudraCT2008-003485-25. Impact of the V0034CR 01B emollient on atopic dermatitis symptoms in children. A randomised, placebo-controlled, parallel-groups, double-blind study. clinicaltrialsregister.eu/ctr-search/trial/2008-003485-25/DE Date first received: 12 September 2008.
EudraCT2008‐006844‐21 {published data only}
- EudraCT2008-006844-21. Evaluation of a developmental ‘long lasting’ emollient in subjects with dry skin. clinicaltrialsregister.eu/ctr-search/trial/2008-006844-21/GB.
EudraCT2009‐010609‐35 {published data only}
- EudraCT2009-010609-35. Is treatment with emollients always beneficial? Comparative biophysical and molecular biological studies of the skin barrier function in patients with atopic dermatitis, ichthyosis vulgaris and x-linked ichthyosis. clinicaltrialsregister.eu/ctr-search/trial/2009-010609-35/SE.
EudraCT2009‐016572‐78 {published data only}
- EudraCT2009-016572-78. Arm immersion test to compare the skin effects of routine bathing with and without the use of an emollient bath additive. clinicaltrialsregister.eu/ctr-search/search?query=eudract_number:2009-016572-78 Date first received: 17 March 2010.
EudraCT2012‐004621‐24 {published data only}
- EudraCT2012-004621-24. Emollients in the management of atopic dermatitis in children: prevention of flares. www.clinicaltrialsregister.eu/ctr-search/search?query=2012-004621-24.
EudraCT2014‐001026‐16 {published data only}
- EudraCT2014-001026-16. Randomised, double-blind, bilateral comparison of two emollients in patients with dry skin. clinicaltrialsregister.eu/ctr-search/search?query=2014-001026-16.
ISRCTN97515110 {published data only}
- ISRCTN97515110. Investigating whether topical application of a non toxic molecule improves epidermal pH and barrier function in atopic dermatitis. isrctn.com/ISRCTN97515110 Date first received: 21 October 2010.
JPRN‐UMIN000005158 {published data only}
- JPRN-UMIN000005158. Randomized controlled trial to evaluate clinical efficacy of once- or twice-daily skin care with emollient for prevention of atopic dermatitis exacerbation. apps.who.int/trialsearch/Trial2.aspx?TrialID=JPRN-UMIN000005158 Date first received: 7 March 2011.
JPRN‐UMIN000010009 {published data only}
- JPRN-UMIN000010009. Study to evaluate the efficacy of conventional topical therapy for atopic dermatitis based on Filaggrin-gene mutations. http://apps.who.int/trialsearch/Trial2.aspx?TrialID=JPRN-UMIN000010009.
JPRN‐UMIN000017957 {published data only}
- JPRN-UMIN000017957. The effect of moisturizer on both sweating function and sensitive skin in patients with atopic dermatitis, a randomized comparative study. apps.who.int/trialsearch/Trial2.aspx?TrialID=JPRN-UMIN000017957 Date first received: 18 June 2015.
NCT00180141 {published data only}
- NCT00180141. Elidel-study: Elidel in patients with atopic dermatitis [Control of therapy with Elidel vs placebo in patients with atopic dermatitis using bioengineering methods]. clinicaltrials.gov/ct2/show/study/NCT00180141 Date first received: 12 September 2005.
NCT00576238 {published data only}
- NCT00576238. Skin tolerance study of betamethasone creams in atopic eczema and the preventative properties of a moisturiser [A multi centre, parallel, randomised study of the skin tolerance of betamethasone creams on atopic eczema and the influence of moisturiser treatment on the recurrence of eczema]. clinicaltrials.gov/ct2/show/NCT00576238?term=NCT00576238&rank=1 Date first received: 18 December 2007.
NCT00828412 {published data only}
- NCT00828412. Comparison of the efficacy and safety of two topical creams for pediatric atopic dermatitis [A randomized, investigator-blind, six-week, parallel group, multicenter pilot study to compare the safety and efficacy of EpiCeram skin barrier emulsion and desonide cream 0.05% in the twice daily treatment of pediatric subjects with moderate atopic dermatitis]. clinicaltrials.gov/show/NCT00828412 Date first received: 21 January 2009.
NCT01779258 {published data only}
- NCT01779258. Emollients in the management of atopic dermatitis [Emollients in the management of atopic dermatitis in children: Prevention of flares]. clinicaltrials.gov/show/NCT01779258 Date first received: 28 January 2013.
NCT01781663 {published data only}
- NCT01781663. Efficacy of KAM2904 face cream and KAM3008 body lotion treatment in children with atopic dermatitis (AD). clinicaltrials.gov/ct2/show/NCT01781663 Date first received: 29 January 2013.
NCT01915914 {published data only}
- NCT01915914. A randomized, open-label, comparative study to evaluate an intermittent dosing regimen of fluticasone propionate 0.05% cream (twice per week) in reducing the risk of relapse when added to regular daily moisturization using PHYSIOGEL lotion in paediatric subjects with stabilized atopic dermatitis. clinicaltrials.gov/show/NCT01915914 Date first received: 27 June 2013.
NCT02028546 {published data only}
- NCT02028546. The effect of bathing and moisturizers on skin hydration in atopic dermatitis: an in vivo study. clinicaltrials.gov/ct2/show/NCT02028546 Date first received: 19 December 2013.
NCT02286700 {published data only}
- NCT02286700. Skin effects of a topical amino acid moisturizing cream and desonide in atopic dermatitis [A randomized, double-blind, active control, 5 week study to evaluate the safety and skin effects of a new, twice-daily, topically applied amino acid moisturizing cream vs. desonide cream in adult atopic dermatitis]. clinicaltrials.gov/ct2/show/study/NCT02286700 Date first received: 4 November 2014.
NCT02376049 {published data only}
- NCT02376049. A clinical trial to compare topical agents in adults with mild to moderate atopic dermatitis (AD) [An explorative clinical trial to evaluate an intra patient comparison design of topical agents in adults with mild to moderate atopic dermatitis]. clinicaltrials.gov/ct2/show/NCT02376049 Date first received: 25 February 2015.
NCT02589392 {published data only}
- NCT02589392. Cetaphil Restoraderm effect on young children with atopic dermatitis [Effect of Cetaphil® Restoraderm® moisturizer on very dry skin in children with a controlled atopic dermatitis: a randomised, parallel group study]. clinicaltrials.gov/ct2/show/NCT02589392 Date first received: 23 October 2015.
NTR4541 {published data only}
- NTR4541. Efficacy of Dermalex Eczema in atopic dermatitis patients [Efficacy of a skin barrier repair cream (Dermalex Eczema) in atopic dermatitis patients - EDA]. www.trialregister.nl/trialreg/admin/rctview.asp?TC=4541 Date first received: 28 April 2014.
Ridd 2015 {published data only}
- Ridd MJ, Redmond NM, Hollinghurst S, Ball N, Shaw L, Guy R, et al. Choice of Moisturiser for Eczema Treatment (COMET): study protocol for a randomized controlled trial. Trials 2015;16:304. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Santer 2015 {published data only}
- Santer M, Rumsby K, Ridd MJ, Francis NA, Stuart B, Chorozoglou M, et al. Bath additives for the treatment of childhood eczema (BATHE): protocol for multicentre parallel group randomised trial. BMJ Open 2015;5(10):e009575. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Additional references
Andersen 2015
Apfelbacher 2013
- Apfelbacher CJ, Zuuren EJ, Fedorowicz Z, Jupiter A, Matterne U, Weisshaar E. Oral H1 antihistamines as monotherapy for eczema. Cochrane Database of Systematic Reviews 2013, Issue 2. Art. No: CD007770. [DOI: 10.1002/14651858.CD007770.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Arkwright 2013
- Arkwright PD, Motala C, Subramanian H, Spergel J, Schneider LC, Wollenberg A, et al. Management of difficult-to-treat atopic dermatitis. Journal of Allergy and Clinical Immunology: In Practice 2013;1(2):142-51. [PMID: ] [DOI] [PubMed] [Google Scholar]
Ashcroft 2007
- Ashcroft DM, Chen L-C, Garside R, Stein K, Williams HC. Topical pimecrolimus for eczema. Cochrane Database of Systematic Reviews 2007, Issue 4. Art. No: CD005500. [DOI: 10.1002/14651858.CD005500.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bamford 2013
- Bamford JTM, Ray S, Musekiwa A, Gool C, Humphreys R, Ernst E. Oral evening primrose oil and borage oil for eczema. Cochrane Database of Systematic Reviews 2013, Issue 4. Art. No: CD004416. [DOI: 10.1002/14651858.CD004416.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Basra 2015
- Basra MK, Salek MS, Camilleri L, Sturkey R, Finlay AY. Determining the minimal clinically important difference and responsiveness of the Dermatology Life Quality Index (DLQI): further data. Dermatology 2015;230(1):27-33. [PMID: ] [DOI] [PubMed] [Google Scholar]
Bath‐Hextall 2008
- Bath-Hextall FJ, Delamere FM, Williams HC. Dietary exclusions for established atopic eczema. Cochrane Database of Systematic Reviews 2008, Issue 1. Art. No: CD005203. [DOI: 10.1002/14651858.CD005203.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bath‐Hextall 2010
- Bath-Hextall FJ, Birnie AJ, Ravenscroft JC, Williams HC. Interventions to reduce Staphylococcus aureus in the management of atopic eczema: an updated Cochrane review. British Journal of Dermatology 2010;163(1):12-26. [PMID: ] [DOI] [PubMed] [Google Scholar]
Bath‐Hextall 2012
- Bath-Hextall FJ, Jenkinson C, Humphreys R, Williams HC. Dietary supplements for established atopic eczema. Cochrane Database of Systematic Reviews 2012, Issue 2. Art. No: CD005205. [DOI: 10.1002/14651858.CD005205.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bieber 2008
- Bieber T. Atopic dermatitis. New England Journal of Medicine 2008;358(14):1483-94. [PMID: ] [DOI] [PubMed] [Google Scholar]
Birnie 2002
- Birnie AJ, Bath-Hextall FJ, Ravenscroft JC, Williams HC. Interventions to reduce Staphylococcus aureus in the management of atopic eczema. Cochrane Database of Systematic Reviews 2002, Issue 4. Art. No: CD003871. [DOI: 10.1002/14651858.CD003871] [DOI] [PubMed] [Google Scholar]
Bliddal 2009
- Bliddal H, Christensen R. The treatment and prevention of knee osteoarthritis: a tool for clinical decision-making. Expert Opinion on Pharmacotherapy 2009;10(11):1793-804. [PMID: ] [DOI] [PubMed] [Google Scholar]
Boguniewicz 2011
- Boguniewicz M, Leung DYM. Atopic dermatitis: a disease of altered skin barrier and immune dysregulation. Immunological Reviews 2011;242(1):233–46. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Borenstein 2009
- Borenstein M, Hedges LV, Higging JPT, Rothstein HR. Introduction to Meta-Analysis. John Wiley & Sons, Ltd, 2009. [Google Scholar]
Bos 2010
- Bos JD, Brenninkmeijer EE, Schram ME, Middelkamp-Hup MA, Spuls PI, Smitt JH. Atopic eczema or atopiform dermatitis. Experimental Dermatology 2010;19(4):325-31. [PMID: ] [DOI] [PubMed] [Google Scholar]
Boyle 2006
- Boyle RJ, Bath-Hextall FJ, Leonardi-Bee J, Murrell DF, Tang MLK. Probiotics for treating eczema. Cochrane Database of Systematic Reviews 2006, Issue 3. Art. No: CD006135. [DOI: 10.1002/14651858.CD006135] [DOI] [PubMed] [Google Scholar]
Bradburn 2007
- Bradburn MJ, Deeks JJ, Berlin JA, Russell Localio A. Much ado about nothing: a comparison of the performance of meta-analytical methods with rare events. Statistics in Medicine 2007;26(1):53-77. [PMID: ] [DOI] [PubMed] [Google Scholar]
Calderon 2010
- Calderon MA, Boyle RJ, Nankervis H, García Núñez I, Williams HC, Durham S. Specific allergen immunotherapy for the treatment of atopic eczema. Cochrane Database of Systematic Reviews 2010, Issue 10. Art. No: CD008774. [DOI: 10.1002/14651858.CD008774] [DOI] [PMC free article] [PubMed] [Google Scholar]
Caussin 2008
- Caussin J, Gooris GS, Bouwstra JA. FTIR studies show lipophilic moisturizers to interact with stratum corneum lipids, rendering the more densely packed. Biochimica et Biophysica Acta 2008;1778(6):1517-24. [PMID: ] [DOI] [PubMed] [Google Scholar]
Caussin 2009a
- Caussin J. Skin, dry skin and moisturization. In: Doctoral thesis: Stratum corneum hydration : mode of action of moisturizers on a molecular level. Leiden: Division of Drug Delivery Technology (LACDR), Faculty of Science, Leiden University, 2009:7-21. [Google Scholar]
Caussin 2009b
- Caussin J, Rozema E, Gooris GS, Wiechers JW, Pavel S, Bouwstra JA. Hydrophilic and lipophilic moisturizers have similar penetration profiles but different effects on SC water distribution in vivo. Experimental Dermatology 2009;18(11):954-61. [PMID: ] [DOI] [PubMed] [Google Scholar]
Chamlin 2002
- Chamlin SL, Kao J, Frieden IJ, Sheu MY, Fowler AJ, Fluhr JW. Ceramide-dominant barrier repair lipids alleviate childhood atopic dermatitis: changes in barrier function provide a sensitive indicator of disease activity. Journal of the American Academy of Dermatology 2002;47(2):198-208. [PMID: ] [DOI] [PubMed] [Google Scholar]
Charman 2000
- Charman CR, Morris AD, Williams HC. Topical corticosteroid phobia in patients with atopic eczema. British Journal of Dermatology 2000;142(5):931-6. [PMID: ] [DOI] [PubMed] [Google Scholar]
Charman 2004
- Charman CR, Venn AJ, Williams HC. The patient-oriented eczema measure: development and initial validation of a new tool for measuring atopic eczema severity from the patients' perspective. Archives of Dermatology 2004;140(12):1513-9. [PMID: ] [DOI] [PubMed] [Google Scholar]
Chung 2008
- Chung HJ, Jeon HS, Sung H, Kim MN, Hong SJ. Epidemiological characteristics of methicillin-resistant Staphylococcus aureus isolates from children with eczematous atopic dermatitis lesions. Journal of Clinical Microbiology 2008;46(3):991-5. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Cooke 2016
- Cooke A, Cork MJ, Victor S, Campbell M, Danby S, Chittock J, et al. Olive oil, sunflower oil or no oil for baby dry skin or massage: A pilot, assessor-blinded, randomized controlled trial (the Oil in Baby SkincaRE [OBSeRvE] Study). Acta Dermato-Venereologica 2016;96(3):323-30. [PMID: 26551528] [DOI] [PubMed] [Google Scholar]
Cork 2003a
- Cork MJ, Britton J, Butler L, Young S, Murphy R, Keohane SG. Comparison of parent knowledge, therapy utilization and severity of atopic eczema before and after explanation and demonstration of topical therapies by a specialist dermatology nurse. British Journal of Dermatology 2003;149(3):582-9. [PMID: ] [DOI] [PubMed] [Google Scholar]
Cork 2003b
- Cork MJ, Timmins J, Holden C, Carr J, Berry V, Tazi-Ahnini R, et al. An audit of adverse drug reactions to aqueous cream in children with atopic eczema. Pharmaceutical Journal 2003;271:747-8. [Google Scholar]
Cork 2006
- Cork MJ, Robinson DA, Vasilopoulos Y, Ferguson A, Moustafa M, MacGowan A et al. New perspectives on epidermal barrier dysfunction in atopic dermatitis: gene-environment interactions. Journal of Allergy & Clinical Immunology 2006;118(1):3-21. [PMID: ] [DOI] [PubMed] [Google Scholar]
Cork 2009
- Cork MJ, Danby SG, Vasilopoulos Y, Hadgraft J, Lane ME, Moustafa M. Epidermal barrier dysfunction in atopic dermatitis. Journal of Investigative Dermatology 2009;129(8):1892-908. [PMID: ] [DOI] [PubMed] [Google Scholar]
Costa 1989
- Costa C, Rilliet A, Nicolet M, Saurat JH. Scoring atopic dermatitis: the simpler the better? Acta Dermato-Venereologica 1989;69(1):41-5. [PMID: ] [PubMed] [Google Scholar]
Cury Martins 2015
- Cury Martins J, Martins C, Aoki V, Gois AFT, Ishii HA, da Silva EMK. Topical tacrolimus for atopic dermatitis. Cochrane Database of Systematic Reviews 2015, Issue 7. Art. No: CD009864. [DOI: 10.1002/14651858.CD009864.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Danby 2011b
- Danby SG, Al-Enezi T, Sultan A, Chittock J, Kennedy K, Cork MJ. The effect of aqueous cream BP on the skin barrier in volunteers with a previous history of atopic dermatitis. British Journal of Dermatology 2011;165(2):329-34. [PMID: ] [DOI] [PubMed] [Google Scholar]
Danby 2013
- Danby SG, AlEnezi T, Sultan A, Lavender T, Chittock J, Brown K, et al. Effect of olive and sunflower seed oil on the adult skin barrier: implications for neonatal skin care. Acta Dermato-Venereologica 2013;30(1):42-50. [PMID: ] [DOI] [PubMed] [Google Scholar]
Danby 2016
- Danby SG, Chalmers J, Brown K, Williams HC, Cork MJ. A functional mechanistic study of the effect of emollients on the structure and function of the skin barrier. British Journal of Dermatology 2016;175(5):1011-9. [PMID: ] [DOI] [PubMed] [Google Scholar]
Deckers 2012
- Deckers IA, McLean S, Linssen S, Mommers M, Schayck CP, Sheikh A. Investigating international time trends in the incidence and prevalence of atopic eczema 1990-2010: a systematic review of epidemiological studies. PloS One 2012;7(7):e39803. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
DerSimonian 1986
- DerSimonian R, Laird N. Meta-analysis in clinical trials. Controlled Clinical Trials 1986;7(3):177-88. [PMID: ] [DOI] [PubMed] [Google Scholar]
Dharmage 2014
- Dharmage SC, Lowe AJ, Matheson MC, Burgess JA, Allen KJ, Abramson MJ. Atopic dermatitis and the atopic march revisited. Allergy 2014;69(1):17-27. [PMID: ] [DOI] [PubMed] [Google Scholar]
Diepgen 1989
- Diepgen TL, Fartasch M, Hornstein OP. Evaluation and relevance of atopic basic and minor features in patients with atopic dermatitis and in the general population. Acta Dermato-Venereologica. Supplementum 1989;144:50-4. [PMID: ] [DOI] [PubMed] [Google Scholar]
Diepgen 1996
- Diepgen TL, Sauerbrei W, Fartasch M. Development and validation of diagnostic scores for atopic dermatitis incorporating criteria of data quality and practical usefulness. Journal of Clinical Epidemiology 1996;49(9):1031-8. [PMID: ] [DOI] [PubMed] [Google Scholar]
Eichenfield 2014a
- Eichenfield LF, Tom WL, Chamlin SL, Feldman SR, Hanifin JM, Simpson EL, et al. Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis. Journal of the American Academy of Dermatology 2014;70(2):338-51. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Eichenfield 2014b
- Eichenfield LF, Tom WL, Berger TG, Krol A, Paller AS, Schwarzenberger K. Guidelines of care for the management of atopic dermatitis: section 2. Management and treatment of atopic dermatitis with topical therapies. Journal of the American Academy of Dermatology 2014;71(1):116-32. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Elias 2011
- Elias PM, Wakefield JS. Therapeutic implications of a barrier-based pathogenesis of atopic dermatitis. Clinical Reviews in Allergy & Immunology 2011;41(3):282-95. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Elias 2014
- Elias PM. Lipid abnormalities and lipid-based repair strategies in atopic dermatitis. Biochimica et Biophysica Acta 2014;1841(3):323-30. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Emerson 2000
- Emerson RM, Charman CR, Williams HC. The Nottingham Eczema Severity Score: preliminary refinement of the Rajka and Langeland grading. British Journal of Dermatology 2000;142(2):288-97. [PMID: ] [DOI] [PubMed] [Google Scholar]
Ersser 2014
- Ersser SJ, Cowdell F, Latter S, Gardiner E, Flohr C, Thompson AR, et al. Psychological and educational interventions for atopic eczema in children. Cochrane Database of Systematic Reviews 2014, Issue 1. Art. No: CD004054. [DOI: 10.1002/14651858.CD004054.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
European Task Force on Atopic Dermatitis 1993
- No authors listed. Severity scoring of atopic dermatitis: the SCORAD index. Consensus Report of the European Task Force on Atopic Dermatitis. Dermatology 1993;186(1):23-31. [PMID: ] [DOI] [PubMed] [Google Scholar]
Finlay 1994
- Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)-a simple practical measure for routine clinical use. Clinical and Experimental Dermatology 1994;19(3):210-6. [PMID: ] [DOI] [PubMed] [Google Scholar]
Flohr 2004
- Flohr C, Johansson SG, Wahlgren CF, Williams H. How atopic is atopic dermatitis? Journal of Allergy & Clinical Immunology 2004;114(1):150-8. [PMID: ] [DOI] [PubMed] [Google Scholar]
Flohr 2008
- Flohr C, Weiland SK, Weinmayr G, Björkstén B, Bråbäck L, Brunekreef B, et al. The role of atopic sensitization in flexural eczema: findings from the International Study of Asthma and Allergies in Childhood Phase Two. Journal of Allergy & Clinical Immunology 2008;121(1):141-7. [PMID: ] [DOI] [PubMed] [Google Scholar]
Flohr 2009
- Flohr C, Weinmayr G, Weiland SK, Addo-Yobo E, Annesi-Maesano I, Björkstén B, et al. How well do questionnaires perform compared with physical examination in detecting flexural eczema? Findings from the International Study of Asthma and Allergies in Childhood (ISAAC) Phase Two. British Journal of Dermatology 2009;161(4):846-53. [PMID: ] [DOI] [PubMed] [Google Scholar]
Flohr 2014
- Flohr C, Mann J. New insights into the epidemiology of childhood atopic dermatitis. Allergy 2014;69(1):3-16. [PMID: ] [DOI] [PubMed] [Google Scholar]
Futamura 2014
- Futamura M, Ferguson L, Vakirlis E, Kojima R, Roberts A, Mori R. Leukotriene receptor antagonists for atopic eczema. Cochrane Database of Systematic Reviews 2014, Issue 7. Art. No: CD011224. [DOI: 10.1002/14651858.CD011224] [DOI] [PMC free article] [PubMed] [Google Scholar]
Gaunt 2016
- Gaunt DM, Metcalfe C, Ridd M. The Patient-Oriented Eczema Measure in young children: responsiveness and minimal clinically important difference. Allergy 2016;71(11):1620-5. [DOI: 10.1111/all.12942] [PMID: ] [DOI] [PMC free article] [PubMed]
Ghadially 1992
- Ghadially R, Halkier-Sorensen L, Elias PM. Effects of petrolatum on stratum corneum structure and function. Journal of the American Academy of Dermatology 1992;26(3 Pt 2):387-96. [PMID: ] [DOI] [PubMed] [Google Scholar]
GRADEpro GDT [Computer program]
- GRADEpro GDT. Version accessed September 2016. Hamilton (ON): GRADE Working Group, McMaster University, 2015.
Gu 2013
- Gu S, Yang AWH, Xue CCL, Li CG, Pang C, Zhang W, et al. Chinese herbal medicine for atopic eczema. Cochrane Database of Systematic Reviews 2013, Issue 9. Art. No: CD008642. [DOI: 10.1002/14651858.CD008642.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Guyatt 2013a
- Guyatt GH, Oxman AD, Santesso N, Helfand M, Vist G, Kunz R. GRADE guidelines: 12. Preparing summary of findings tables-binary outcomes. Journal of Clinical Epidemiology 2013;66(2):158-72. [PMID: ] [DOI] [PubMed] [Google Scholar]
Guyatt 2013b
- Guyatt GH, Thorlund K, Oxman AD, Walter SD, Patrick D, Furukawa TA. GRADE guidelines: 13. Preparing summary of findings tables and evidence profiles-continuous outcomes. Journal of Clinical Epidemiology 2013;66(2):173-83. [PMID: ] [DOI] [PubMed] [Google Scholar]
Haeck 2011
- Haeck IM, Knol MJ, Ten Berge O, Velsen SG, Bruin-Weller MS, Bruijnzeel-Koomen CA. Enteric-coated mycophenolate sodium versus cyclosporin A as long-term treatment in adult patients with severe atopic dermatitis: a randomized controlled trial. Journal of the American Academy of Dermatology 2011;64(6):1074-84. [PMID: ] [DOI] [PubMed] [Google Scholar]
Haileamlak 2005
- Haileamlak A, Dagoye D, Williams H, Venn AJ, Hubbard R, Britton J, et al. Early life risk factors for atopic dermatitis in Ethiopian children. Journal of Allergy & Clinical Immunology 2005;115(2):370-6. [PMID: ] [DOI] [PubMed] [Google Scholar]
Halling‐Overgaard 2016
Hanifin 1980
- Hanifin JM, Rajka G. Diagnostic features of atopic dermatitis. Acta Dermato-Venereologica 1980;92(Suppl):44-7. [Google Scholar]
Hanifin 2001
- Hanifin JM, Thurston M, Omoto M, Cherill R, Tofte SJ, Graeber M. The eczema area and severity index (EASI): assessment of reliability in atopic dermatitis. EASI Evaluator Group. Experimental Dermatology 2001;10(1):11-8. [PMID: ] [DOI] [PubMed] [Google Scholar]
Harcharik 2014
- Harcharik S, Emer J. Steroid-sparing properties of emollients in dermatology. Skin Therapy Letter 2014;19(1):5-10. [PMID: ] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane-handbook.org.
Hoare 2000
- Hoare C, Li Wan Po A, Williams H. Systematic review of treatments for atopic eczema. Health Technology Assessment 2000;4(37):1-191. [PMID: ] [PMC free article] [PubMed] [Google Scholar]
Hogewoning 2010
- Hogewoning AA, Larbi IA, Addo HA, Amoah AS, Boakye D, Hartgers F, et al. Allergic characteristics of urban schoolchildren with atopic eczema in Ghana. Journal of the European Academy of Dermatology & Venereology 2010;24(12):1406-12. [PMID: ] [DOI] [PubMed] [Google Scholar]
Hogewoning 2012
- Hogewoning AA, Bouwes Bavinck JN, Amoah AS, Boakye DA, Yazdanbakhsh M, Kremsner PG, et al. Point and period prevalences of eczema in rural and urban schoolchildren in Ghana, Gabon and Rwanda. Journal of the European Academy of Dermatology & Venereology 2012;26(4):488-94. [PMID: ] [DOI] [PubMed] [Google Scholar]
Holm 2007
- Holm EA, Wulf HC, Thomassen L, Jemec GB. Assessment of atopic eczema: clinical scoring and noninvasive measurements. British Journal of Dermatology 2007;157(4):674-80. [PMID: ] [DOI] [PubMed] [Google Scholar]
Hon 2016
- Hon KL, Tsang YC, Lee VW, Pong NH, Ha G, Lee ST, et al. Efficacy of sodium hypochlorite (bleach) baths to reduce Staphylococcus aureus colonization in childhood onset moderate-to-severe eczema: A randomized, placebo-controlled cross-over trial. Journal of Dermatological Treatment 2016;27(2):156-62. [PMID: ] [DOI] [PubMed] [Google Scholar]
Jadotte 2014
- Jadotte YT, Santer M, Vakirlis E, Schwartz RA, Bauer A, Gundersen DA, et al. Complementary and alternative medicine treatments for atopic eczema. Cochrane Database of Systematic Reviews 2014, Issue 1. Art. No: CD010938. [DOI: 10.1002/14651858.CD010938] [DOI] [Google Scholar]
Janssens 2012
- Janssens M, Smeden J, Gooris GS, Bras W, Portale G, Caspers PJ, et al. Increase in short-chain ceramides correlates with an altered lipid organization and decreased barrier function in atopic eczema patients. Journal of Lipid Research 2012;53(12):2755-66. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Jenner 2004
- Jenner N, Campbell J, Marks R. Morbidity and cost of atopic eczema in Australia. Australian Journal of Dermatology 2004;45(1):16-22. [PMID: ] [DOI] [PubMed] [Google Scholar]
Johansson 2004
- Johansson SG, Bieber T, Dahl R, Friedmann PS, Lanier BQ, Lockey RF, et al. Revised nomenclature for allergy for global use: Report of the Nomenclature Review Committee of the World Allergy Organization, October 2003. Journal of Allergy & Clinical Immunology 2004;113(5):832-6. [PMID: ] [DOI] [PubMed] [Google Scholar]
Kanti 2014
- Kanti V, Grande C, Stroux A, Bührer C, Blume-Peytavi U, Garcia Bartels N. Influence of sunflower seed oil on the skin barrier function of preterm infants: a randomized controlled trial. Dermatology 2014;229(3):230-9. [PMID: ] [DOI] [PubMed] [Google Scholar]
Katayama 2014
- Katayama I, Kohno Y, Akiyama K, Aihara M, Kondo N, Saeki H, et al. Japanese Guideline for Atopic Dermatitis 2014. Allergology International 2014;63(3):377-98. [PMID: ] [DOI] [PubMed] [Google Scholar]
Kezic 2008
- Kezic S, Kemperman PM, Koster ES, Jongh CM, Thio HB, Campbell LE, et al. Loss-of-function mutations in the filaggrin gene lead to reduced level of natural moisturizing factor in the stratum corneum. Journal of Investigative Dermatology 2008;128(8):2117-9. [PMID: ] [DOI] [PubMed] [Google Scholar]
Kunz 1997
- Kunz B, Oranje AP, Labrèze L, Stalder JF, Ring J, Taïeb A. Clinical validation and guidelines for the SCORAD index: consensus report of the European Task Force on Atopic Dermatitis. Dermatology 1997;195(1):10-9. [PMID: ] [DOI] [PubMed] [Google Scholar]
Kvenshagen 2014
- Kvenshagen BK, Carlsen KH, Mowinckel P, Berents TL, Carlsen KC. Can early skin care normalise dry skin and possibly prevent atopic eczema? A pilot study in young infants. Allergologia et Immunopathologia 2014;42(6):539-43. [PMID: ] [DOI] [PubMed] [Google Scholar]
Küster 2015
- Küster D, Spuls PI, Flohr C, Smith C, Hooft L, Deckert S et al. Effects of systemic immunosuppressive therapies for moderate-to-severe eczema in children and adults. Cochrane Database of Systematic Reviews 2015, Issue 11. Art. No: CD011939. [DOI: 10.1002/14651858.CD011939] [DOI] [Google Scholar]
Langan 2006
- Langan SM, Thomas KS, Williams HC. What is meant by a 'flare' in atopic dermatitis? A systematic review and proposal. Archives of Dermatology 2006;142(9):1190-6. [PMID: ] [DOI] [PubMed] [Google Scholar]
Lawson 1998
- Lawson V, Lewis-Jones MS, Finlay AY, Reid P, Owens RG. The family impact of childhood atopic dermatitis: the Dermatitis Family Impact Questionnaire. British Journal of Dermatology 1998;138(1):107-13. [PMID: ] [DOI] [PubMed] [Google Scholar]
Lee 2007
- Lee YL, Li CW, Sung FC, Yu HS, Sheu HM, Guo YL. Environmental factors, parental atopy and atopic eczema in primary-school children: a cross-sectional study in Taiwan. British Journal of Dermatology 2007;157(6):1217-24. [PMID: ] [DOI] [PubMed] [Google Scholar]
Leung 2000
- Leung DY. Atopic dermatitis: new insights and opportunities for therapeutic intervention. Journal of Allergy & Clinical Immunology 2000;105(5):860-76. [PMID: ] [DOI] [PubMed] [Google Scholar]
Lewis‐Jones 1995
- Lewis-Jones MS, Finlay AY. The Children's Dermatology Life Quality Index (CDLQI): initial validation and practical use. British Journal of Dermatology 1995;132(6):942-9. [PMID: ] [DOI] [PubMed] [Google Scholar]
Lewis‐Jones 2001
- Lewis-Jones MS, Finlay AY, Dykes PJ. The Infants' Dermatitis Quality of Life Index. British Journal of Dermatology 2001;144(1):104-10. [PMID: ] [DOI] [PubMed] [Google Scholar]
Lewis‐Jones 2006
- Lewis-Jones S. Quality of life and childhood atopic dermatitis: the misery of living with childhood eczema. International Journal of Clinical Practice 2006;60(8):984-92. [PMID: ] [DOI] [PubMed] [Google Scholar]
Liberati 2009
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Medicine 2009;6(7):e1000100. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Lindh 2015
- Lindh JD, Bradley M. Clinical effectiveness of moisturizers in atopic dermatitis and related disorders: A systematic review. American Journal of Clinical Dermatology 2015;16(5):341-59. [PMID: ] [DOI] [PubMed] [Google Scholar]
Lodén 2003
- Lodén M. Role of topical emollients and moisturizers in the treatment of dry skin barrier disorders. American Journal of Clinical Dermatology 2003;4(11):771-88. [PMID: ] [DOI] [PubMed] [Google Scholar]
Lodén 2012
- Lodén M. Effect of moisturizers on epidermal barrier function. Clinics in Dermatology 2012;30(3):286-96. [PMID: ] [DOI] [PubMed] [Google Scholar]
Lucky 1997
- Lucky AW, Leach AD, Laskarzewski P, Wenck H. Use of an emollient as a steroid-sparing agent in the treatment of mild to moderate atopic dermatitis in children. Pediatric Dermatology 1997;14(4):321-4. [PMID: ] [DOI] [PubMed] [Google Scholar]
Lynde 2005
- Lynde C, Barber K, Claveau J, Gratton D, Ho V, Krafchik B, et al. Canadian practical guide for the treatment and management of atopic dermatitis. Journal of Cutaneous Medicine and Surgery 2005;8(Suppl 5):1-9. [PMID: ] [DOI] [PubMed] [Google Scholar]
Mack Correa 2012
- Mack Correa MC, Nebus J. Management of patients with atopic dermatitis: the role of emollient therapy. Dermatology Research & Practice 2012;2012:836931. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Margolis 2014
- Margolis JS, Abuabara K, Bilker W, Hoffstad O, Margolis DJ. Persistence of mild to moderate atopic dermatitis. Journal of the American Academy of Dermatology 2014;150(6):593-600. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Mason 2013
- Mason JM, Carr J, Buckley C, Hewitt S, Berry P, Taylor J, et al. Improved emollient use reduces atopic eczema symptoms and is cost neutral in infants: before-and-after evaluation of a multifaceted educational support programme. BMC Dermatology 2013;13:7. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Moed 2012
- Moed H, Yang Q, Oranje AP, Panda S, Wouden JC. Different strategies for using topical corticosteroids for established eczema. Cochrane Database of Systematic Reviews 2012, Issue 10. Art. No: CD010080. [DOI: 10.1002/14651858.CD010080] [DOI] [Google Scholar]
Moncrieff 2013
- Moncrieff G, Cork M, Lawton S, Kokiet S, Daly C, Clark C. Use of emollients in dry-skin conditions: consensus statement. Clinical & Experimental Dermatology 2013;38(3):231-8. [PMID: ] [DOI] [PubMed] [Google Scholar]
Murray 2012
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380(9859):2197-223. [PMID: ] [DOI] [PubMed] [Google Scholar]
Möhrenschlager 2006
- Möhrenschlager M, Darsow U, Schnopp C, Ring J. Atopic eczema: what's new? Journal of the European Academy of Dermatology & Venereology 2006;20(5):503-11. [PMID: ] [DOI] [PubMed] [Google Scholar]
Nankervis 2015
- Nankervis H, Pynn EV, Boyle RJ, Rushton L, Williams HC, Hewson DM, et al. House dust mite reduction and avoidance measures for treating eczema. Cochrane Database of Systematic Reviews 2015, Issue 1. Art. No: CD008426. [DOI: 10.1002/14651858.CD008426.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Nankervis 2016
- Nankervis H, Thomas KS, Delamere FM, Barbarot S, Rogers NK, Williams HC. Scoping systematic review of treatments for eczema. Southampton (UK): NIHR Journals Library. Programme Grants for Applied Research 2016;4(7):1-480. [27280278] [PubMed] [Google Scholar]
Nelson 2015
- Nelson EC, Eftimovska E, Lind C, Hager A, Wasson JH, Lindblad S. Patient reported outcome measures in practice. British Medical Journal 2015;350:g7818. [PMID: ] [DOI] [PubMed] [Google Scholar]
NICE 2007
- National Institute for Health and Clinical Excellence (NICE). Atopic eczema in under 12s: diagnosis and management (CG57) 2007. www.nice.org.uk/guidance/cg57 (accessed prior to 5 October 2016).
Nutten 2015
- Nutten S. Atopic dermatitis: global epidemiology and risk factors. Annals of Nutrition & Metabolism 2015;66(Suppl 1):8-16. [PMID: ] [DOI] [PubMed] [Google Scholar]
Oakley 2016
- Oakley R, Lawton S. Views on unwanted effects of leave-on emollients and experiences surrounding their incidence. Dermatological Nursing 2016;15(4):38-43.
Odhiambo 2009
- Odhiambo JA, Williams HC, Clayton TO, Robertson CF, Asher MI, ISAAC Phase Three Study Group. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. Journal of Allergy & Clinical Immunology 2009;124(6):1251-8. [PMID: ] [DOI] [PubMed] [Google Scholar]
Palmer 2006
- Palmer CN, Irvine AD, Terron-Kwiatkowski A, Zhao Y, Liao H, Lee SP, et al. Common loss-of-function variants of the epidermal barrier protein filaggrin are a major predisposing factor for atopic dermatitis. Nature Genetics 2006;38(4):441-6. [PMID: ] [DOI] [PubMed] [Google Scholar]
Penzer 2012
- Penzer R. Best practice in emollient therapy: a statement for health care professionals. Dermatological Nursing 2012;11(4):4-19. [Google Scholar]
Petry 2013
- Petry V, Lipnharski C, Bessa GR, Silveira VB, Weber MB. Prevalence of community-acquired methicillin-resistant Staphylococcus aureus and antibiotic resistance in patients with atopic dermatitis in Porto Alegre, Brazil. International Journal of Dermatology 2013;53(6):731-5. [PMID: ] [DOI] [PubMed] [Google Scholar]
Rajka 1989
- Rajka G, Langeland T. Grading of the severity of atopic dermatitis. Acta Dermato-venereologica. Supplementum 1989;144:13-14. [PMID: ] [DOI] [PubMed] [Google Scholar]
Rawlings 2004
- Rawlings AV, Canestrari DA, Dobkowski B. Moisturizer technology versus clinical performance. Dermatologic Therapy 2004;17(Suppl 1):49-56. [PMID: ] [DOI] [PubMed] [Google Scholar]
Rawlings 2005
- Rawlings AV, Matts PJ. Stratum corneum moisturization at the molecular level: an update in relation to the dry skin cycle. Journal of Investigative Dermatology 2005;124(6):1099-110. [PMID: ] [DOI] [PubMed] [Google Scholar]
Rawlings 2014
- Rawlings AV. Molecular basis for stratum corneum maturation and moisturization. British Journal of Dermatology 2014;171(Suppl 3):19-28. [PMID: ] [DOI] [PubMed] [Google Scholar]
Reich 2016
- Reich A, Riepe C, Anastasiadou Z, Mędrek K, Augustin M, Szepietowski JC. Itch assessment with visual analogue scale and numerical rating scale: determination of minimal clinically important difference in chronic itch. Acta Dermato-Venereologica 2016;96(7):978-80. [DOI: 10.2340/00015555-2433] [PMID: ] [DOI] [PubMed]
RevMan 2014 [Computer program]
- Review Manager (RevMan). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Riley 2011
- Riley RD, Higgins JP, Deeks JJ. Interpretation of random effects meta-analyses. BMJ 2011;342:d549. [PMID: ] [DOI] [PubMed] [Google Scholar]
Ring 2012a
- Ring J, Alomar A, Bieber T, Deleuran M, Fink-Wagner A, Gelmetti C. Guidelines for treatment of atopic eczema (atopic dermatitis) part I. Journal of the European Academy of Dermatology and Venereology : JEADV 2012;26(8):1045-60. [PMID: ] [DOI] [PubMed] [Google Scholar]
Ring 2012b
- Ring J, Alomar A, Bieber T, Deleuran M, Fink-Wagner A, Gelmetti C. Guidelines for treatment of atopic eczema (atopic dermatitis) Part II. Journal of the European Academy of Dermatology and Venereology : JEADV 2012;26(9):1176-93. [PMID: ] [DOI] [PubMed] [Google Scholar]
Saeki 2009
- Saeki H, Furue M, Furukawa F, Hide M, Ohtsuki M, Katayama I, et al. Guidelines for management of atopic dermatitis. Journal of Dermatology 2009;36(10):563-77. [PMID: ] [DOI] [PubMed] [Google Scholar]
Sagiv 2003
- Sagiv AE, Marcus Y. The connection between in vitro water uptake and in vivo skin moisturization. Skin Research & Technology 2003;9(4):306-11. [PMID: ] [DOI] [PubMed] [Google Scholar]
Santer 2013
- Santer M, Burgess H, Yardley L, Ersser SJ, Lewis-Jones S, Muller I, et al. Managing childhood eczema: qualitative study exploring carers' experiences of barriers and facilitators to treatment adherence. Journal of Advanced Nursing 2013;69(11):2493-501. [PMID: 23528163] [DOI] [PubMed] [Google Scholar]
Santer 2016
- Santer M, Muller I, Yardley L, Lewis-Jones S, Ersser S, Little P. Parents' and carers' views about emollients for childhood eczema: qualitative interview study. BMJ Open 2016;6(8):e011887. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Schmitt 2007
- Schmitt J, Langan S, Williams HC. What are the best outcome measurements for atopic eczema? A systematic review. Journal of Allergy & Clinical Immunology 2007;120(6):1389-98. [PMID: ] [DOI] [PubMed] [Google Scholar]
Schmitt 2014
- Schmitt J, Spuls PI, Thomas KS, Simpson E, Furue M, Deckert S, et al. The Harmonising Outcome Measures for Eczema (HOME) statement to assess clinical signs of atopic eczema in trials. Journal of Allergy & Clinical Immunology 2014;134(4):800-7. [PMID: ] [DOI] [PubMed] [Google Scholar]
Schram 2012
- Schram ME, Spuls PI, Leeflang MM, Lindeboom R, Bos JD, Schmitt J. EASI, (objective) SCORAD and POEM for atopic eczema: responsiveness and minimal clinically important difference. Allergy 2012;67(1):99-106. [PMID: ] [DOI] [PubMed] [Google Scholar]
Schünemann 2013
- Schünemann H, Brożek J, Guyatt G, Oxman A, editors The GRADE Working Group. GRADE handbook for grading quality of evidence and strength of recommendations. www.guidelinedevelopment.org/handbook (accessed before 5 October 2016);(2013).
Serup 1995
- Serup J. EEMCO guidance for the assessment of dry skin(xerosis) and ichthyosis: clinical scoring systems. Skin Research and Technology 1995;1(3):109-114. [DOI] [PubMed] [Google Scholar]
Sidbury 2014a
- Sidbury R, Tom WL, Bergman JN, Cooper KD, Silverman RA, Berger TG. Guidelines of care for the management of atopic dermatitis: Section 4. Prevention of disease flares and use of adjunctive therapies and approaches. Journal of the American Academy of Dermatology 2014;71(6):1218-33. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sidbury 2014b
- Sidbury R, Davis DM, Cohen DE, Cordoro KM, Berger TG, Bergman JN. Guidelines of care for the management of atopic dermatitis: section 3. Management and treatment with phototherapy and systemic agents. Journal of the American Academy of Dermatology 2014;71(2):327-49. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
SIGN 2011
- Scottish Intercollegiate Guidelines Network (SIGN). Management of atopic eczema in primary care. SIGN publication no.125, 2011. www.sign.ac.uk/guidelines/fulltext/125/index.html (accessed 6 January 2016).
Silverberg 2013
- Silverberg JI, Hanifin JM. Adult eczema prevalence and associations with asthma and other health and demographic factors: a US population-based study. Journal of Allergy & Clinical Immunology 2013;132(5):1132-8. [PMID: ] [DOI] [PubMed] [Google Scholar]
Silverberg 2014
- Silverberg JL. Atopic dermatitis: an evidence-based treatment update. American Journal of Clinical Dermatology 2014;15(3):149-64. [PMID: ] [DOI] [PubMed] [Google Scholar]
Simpson 2010
- Simpson EL, Berry TM, Brown PA, Hanifin JM. A pilot study of emollient therapy for the primary prevention of atopic dermatitis. Journal of the American Academy of Dermatology 2010;63(4):587-93. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Simpson 2014
- Simpson EL, Chalmers JR, Hanifin JM, Thomas KS, Cork MJ, McLean WH, et al. Emollient enhancement of the skin barrier from birth offers effective atopic dermatitis prevention. Journal of Allergy & Clinical Immunology 2014;134(4):818-23. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sirikudta 2013
- Sirikudta W, Kulthanan K, Varothai S, Nuchkull P. Moisturizers for patients with atopic dermatitis: an overview. Journal of Allergy and Therapy 2013;4(4):1-7. [DOI: 10.4172/2155-6121.1000143] [DOI] [Google Scholar]
Stalder 2011
- Stalder JF, Barbarot S, Wollenberg A, Holm EA, De Raeve L, Seidenari S, et al. Patient-Oriented SCORAD (PO-SCORAD): a new self-assessment scale in atopic dermatitis validated in Europe. Allergy 2011;66(8):1114-21. [PMID: ] [DOI] [PubMed] [Google Scholar]
The EuroQol Group 1990
- The EuroQol Group. EuroQol-a new facility for the measurement of health-related quality of life. Health Policy 1990;16(3):199-208. [PMID: ] [DOI] [PubMed] [Google Scholar]
Thomas 2015
- Thomas KS, Stuart B, O'Leary CJ, Schmitt J, Paul C, Williams HC, et al. Validation of treatment escalation as a definition of atopic eczema flares. PLoS One 2015;10(4):e0124770. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Tierney 2007
- Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007;8:16. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
van Smeden 2014a
- Smeden J, Janssens M, Kaye EC, Caspers PJ, Lavrijsen AP, Vreeken RJ, et al. The importance of free fatty acid chain length for the skin barrier function in atopic eczema patients. Experimental Dermatology 2014;23(1):45-52. [PMID: ] [DOI] [PubMed] [Google Scholar]
van Smeden 2014b
- Smeden J, Janssens M, Gooris GS, Bouwstra JA. The important role of stratum corneum lipids for the cutaneous barrier function. Biochimica et Biophysica Acta 2014;1841(3):295-313. [PMID: ] [DOI] [PubMed] [Google Scholar]
van Zuuren 2014
- Zuuren EJ, Apfelbacher CJ, Fedorowicz Z, Jupiter A, Matterne U, Weisshaar E. No high level evidence to support the use of oral H1 antihistamines as monotherapy for eczema: a summary of a Cochrane systematic review. Systematic Reviews 2014;13(3):25. [PMID: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wald 1943
- Wald A. Tests of statistical hypotheses concerning several parameters when the number of observations is large. Transactions of the American Mathematical Society 1943;54:426-82. [Google Scholar]
Weidinger 2016
Whalley 2004
- Whalley D, McKenna SP, Dewar AL, Erdman RA, Kohlmann T, Niero M, et al. A new instrument for assessing quality of life in atopic dermatitis: international development of the Quality of Life Index for Atopic Dermatitis (QoLIAD. British Journal of Dermatology 2004;150(2):274-83. [PMID: ] [DOI] [PubMed] [Google Scholar]
Williams 1994
- Williams HC, Burney PG, Hay RJ, Archer CB, Shipley MJ, Hunter JJ, et al. The U.K. Working Party's Diagnostic Criteria for Atopic Dermatitis. I. Derivation of a minimum set of discriminators for atopic dermatitis. British Journal of Dermatology 1994;131(3):383-96. [PMID: ] [DOI] [PubMed] [Google Scholar]
Williams 1996
- Williams HC, Burney PG, Pembroke AC, Hay RJ. Validation of the U.K. diagnostic criteria for atopic dermatitis in a population setting. U.K. Diagnostic Criteria for Atopic Dermatitis Working Party. British Journal of Dermatology 1996;135(1):12-7. [PMID: ] [PubMed] [Google Scholar]
Williams 2005
- Williams HC. Clinical practice. Atopic dermatitis. New England Journal of Medicine 2005;352(22):2314-24. [PMID: ] [DOI] [PubMed] [Google Scholar]
Williams 2006
- Williams H, Flohr C. How epidemiology has challenged 3 prevailing concepts about atopic dermatitis. Journal of Allergy & Clinical Immunology 2006;118(1):209-13. [PMID: ] [DOI] [PubMed] [Google Scholar]
Williams 2008
- Williams H, Stewart A, Mutius E, Cookson W, Ross Anderson H, and the International Study of Asthma and Allergies in Childhood (ISAAC) Phase one and Three Study Groups. Is eczema really on the increase worldwide? Journal of Allergy & Clinical Immunology 2008;121(4):947-54. [EMBASE: 2008158035] [DOI] [PubMed] [Google Scholar]
Wolkerstorfer 1999
- Wolkerstorfer A, Waard van der Spek FB, Glazenburg EJ, Mulder PG, Oranje AP. Scoring the severity of atopic dermatitis: three item severity score as a rough system for daily practice and as a pre-screening tool for studies. Acta Dermato-Venereologica 1999;79(5):356-9. [PMID: ] [DOI] [PubMed] [Google Scholar]
Wollenberg 2016
- Wollenberg A, Oranje A, Deleuran M, Simon D, Szalai Z, Kunz B, et al. ETFAD/EADV Eczema task force 2015 position paper on diagnosis and treatment of atopic dermatitis in adult and paediatric patients. Journal of the European Academy of Dermatology and Venereology : JEADV 2016;30(5):729-47. [PMID: ] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
van Zuuren 2016
- Zuuren EJ, Fedorowicz Z, Lavrijsen A, Christensen R, Arents B. Emollients and moisturisers for eczema. Cochrane Database of Systematic Reviews 2016, Issue 3. Art. No: CD012119. [DOI: 10.1002/14651858.CD012119] [DOI] [PMC free article] [PubMed] [Google Scholar]