

Abstract
Background
Managed withdrawal is a necessary step prior to drug‐free treatment or as the endpoint of substitution treatment.
Objectives
To assess the effects of buprenorphine versus tapered doses of methadone, alpha2‐adrenergic agonists, symptomatic medications or placebo, or different buprenorphine regimens for managing opioid withdrawal, in terms of the intensity of the withdrawal syndrome experienced, duration and completion of treatment, and adverse effects.
Search methods
We searched the Cochrane Central Register of Controlled Trials (CENTRAL, Issue 11, 2016), MEDLINE (1946 to December week 1, 2016), Embase (to 22 December 2016), PsycINFO (1806 to December week 3, 2016), and the Web of Science (to 22 December 2016) and handsearched the reference lists of articles.
Selection criteria
Randomised controlled trials of interventions using buprenorphine to modify the signs and symptoms of withdrawal in participants who were primarily opioid dependent. Comparison interventions involved reducing doses of methadone, alpha2‐adrenergic agonists (clonidine or lofexidine), symptomatic medications or placebo, and different buprenorphine‐based regimens.
Data collection and analysis
We used standard methodological procedures expected by Cochrane.
Main results
We included 27 studies involving 3048 participants. The main comparators were clonidine or lofexidine (14 studies). Six studies compared buprenorphine versus methadone, and seven compared different rates of buprenorphine dose reduction. We assessed 12 studies as being at high risk of bias in at least one of seven domains of methodological quality. Six of these studies compared buprenorphine with clonidine or lofexidine and two with methadone; the other four studies compared different rates of buprenorphine dose reduction.
For the comparison of buprenorphine and methadone in tapered doses, meta‐analysis was not possible for the outcomes of intensity of withdrawal or adverse effects. However, information reported by the individual studies was suggestive of buprenorphine and methadone having similar capacity to ameliorate opioid withdrawal, without clinically significant adverse effects. The meta‐analyses that were possible support a conclusion of no difference between buprenorphine and methadone in terms of average treatment duration (mean difference (MD) 1.30 days, 95% confidence interval (CI) −8.11 to 10.72; N = 82; studies = 2; low quality) or treatment completion rates (risk ratio (RR) 1.04, 95% CI 0.91 to 1.20; N = 457; studies = 5; moderate quality).
Relative to clonidine or lofexidine, buprenorphine was associated with a lower average withdrawal score (indicating less severe withdrawal) during the treatment episode, with an effect size that is considered to be small to moderate (standardised mean difference (SMD) −0.43, 95% CI −0.58 to −0.28; N = 902; studies = 7; moderate quality). Patients receiving buprenorphine stayed in treatment for longer, with an effect size that is considered to be large (SMD 0.92, 95% CI 0.57 to 1.27; N = 558; studies = 5; moderate quality) and were more likely to complete withdrawal treatment (RR 1.59, 95% CI 1.23 to 2.06; N = 1264; studies = 12; moderate quality). At the same time there was no significant difference in the incidence of adverse effects, but dropout due to adverse effects may be more likely with clonidine (RR 0.20, 95% CI 0.04 to 1.15; N = 134; studies = 3; low quality). The difference in treatment completion rates translates to a number needed to treat for an additional beneficial outcome of 4 (95% CI 3 to 6), indicating that for every four people treated with buprenorphine, we can expect that one additional person will complete treatment than with clonidine or lofexidine.
For studies comparing different rates of reduction of the buprenorphine dose, meta‐analysis was possible only for treatment completion, with separate analyses for inpatient and outpatient settings. The results were diverse, and we assessed the quality of evidence as being very low. It remains very uncertain what effect the rate of dose taper has on treatment outcome.
Authors' conclusions
Buprenorphine is more effective than clonidine or lofexidine for managing opioid withdrawal in terms of severity of withdrawal, duration of withdrawal treatment, and the likelihood of treatment completion.
Buprenorphine and methadone appear to be equally effective, but data are limited. It remains possible that the pattern of withdrawal experienced may differ and that withdrawal symptoms may resolve more quickly with buprenorphine.
It is not possible to draw any conclusions from the available evidence on the relative effectiveness of different rates of tapering the buprenorphine dose. The divergent findings of studies included in this review suggest that there may be multiple factors affecting the response to the rate of dose taper. One such factor could be whether or not the initial treatment plan includes a transition to subsequent relapse prevention treatment with naltrexone. Indeed, the use of buprenorphine to support transition to naltrexone treatment is an aspect worthy of further research.
Most participants in the studies included in this review were male. None of the studies reported outcomes on the basis of sex, preventing any exploration of differences related to this variable. Consideration of sex as a factor influencing response to withdrawal treatment would be relevant research for selecting the most appropriate type of intervention for each individual.
Plain language summary
Buprenorphine for managing opioid withdrawal
Review question
We reviewed the evidence about the effect of buprenorphine for managing withdrawal in people who are dependent on opioid drugs (for example, heroin or pharmaceutical opiates).
Background
Managed withdrawal, or detoxification, is a required first step for long‐term treatment of opioid dependence. The combination of uncomfortable symptoms and intense craving makes completion of opioid withdrawal difficult for most people. Buprenorphine is one of the medications used to manage withdrawal from opioid drugs. This review considered whether buprenorphine is more effective than methadone in tapered doses, or better than clonidine or lofexidine, which are other medications that have been commonly used for managing opioid withdrawal.
Search date
The evidence is current to December 2016.
Study characteristics
We identified 27 randomised controlled trials (clinical studies where people are randomly put into one of two or more treatment groups), involving 3048 opioid‐dependent participants. For 21 studies the average age of participants was in the range 25 to 40 years − in one study the average age was 47 years, while in two studies involving adolescents, the average age of participants was in the range 17 to 20 years (3 studies did not report the average age of participants). In four studies, all or nearly all participants were male, while in three studies less than half the participants were male. In most studies males comprised between one half and three‐quarters of participants, a balance that is typical of the population of people who are opioid dependent. Fourteen of the studies took place in the USA, while the remaining studies were in eight other countries. The studies compared buprenorphine with methadone (6 studies), clonidine or lofexidine (14 studies), or different rates of buprenorphine dose reduction (7 studies).
Fourteen studies reported funding from sources other than industry; in seven studies funding or medications were provided by a pharmaceutical company. The funding source was unclear for seven studies.
Key results
Compared to clonidine or lofexidine, people receiving buprenorphine for opioid withdrawal will have less severe signs and symptoms, be likely to stay in treatment longer, experience fewer side effects, and be more likely to complete the scheduled period of treatment. The effectiveness of buprenorphine is probably similar to tapered doses of methadone, but we are uncertain whether withdrawal symptoms resolve more quickly with buprenorphine. We are also uncertain whether rapid reduction in the dose of buprenorphine is more effective than slow reduction and whether this depends on the context of withdrawal.
Quality of the evidence
We assessed the quality of the evidence to be very low to moderate for the comparison of buprenorphine versus clonidine or lofexidine, low to moderate for the comparison of buprenorphine versus methadone, and very low to low for the comparison of different rates of dose reduction. Further evidence could change the findings, particularly for buprenorphine compared to methadone and for different rates of reduction of buprenorphine dose.
Summary of findings
Background
Description of the condition
Dependence on opioid drugs (heroin, pharmaceutical opiates) is a major health and social issue in most societies. Globally, around 0.2% of adults report unsanctioned use of opioid drugs (Gowing 2015). Despite this low prevalence of opioid use, unsanctioned use of opioid drugs contributes more to the burden of disease than other illicit psychoactive drugs. The burden to the individual user and the community of opioid dependence arises from premature mortality and disability associated with dependent use, with the greatest impact in younger populations of drug users (Gowing 2015), transmission of human immunodeficiency virus (HIV) and hepatitis C, healthcare costs, crime and law enforcement costs, and less tangible costs of family disruption and lost productivity (Mark 2001).
Treatment is central for reducing the harms incurred by individuals and the community from opioid dependence. Managed withdrawal, or detoxification, by itself is not an effective treatment for dependence (Lipton 1983; Mattick 1996). Rates of completion of withdrawal treatment tend to be low, and rates of relapse to opioid use following detoxification are high (Broers 2000; Gossop 1989a; Vaillant 1988). However, withdrawal remains a required first step for many forms of long‐term treatment such as residential rehabilitation and naltrexone maintenance (Kleber 1982). It may also represent the endpoint of an extensive period of substitution treatment with methadone or buprenorphine. As such, the availability of managed withdrawal is essential to an effective and comprehensive treatment system.
The signs and symptoms of the opioid withdrawal syndrome include irritability, anxiety, apprehension, muscular and abdominal pains, chills, nausea, diarrhoea, yawning, lacrimation, sweating, sneezing, rhinorrhoea, general weakness, and insomnia. Symptoms of the opioid withdrawal syndrome usually begin two to three half‐lives after the last opioid dose, that is, 6 to 12 hours for short‐acting opioids such as heroin and morphine, and 36 to 48 hours for long‐acting opioids such as methadone. Following cessation of a short half‐life opioid, symptoms reach peak intensity within two to four days, with most of the obvious physical withdrawal signs no longer observable after 7 to 14 days (Jaffe 1997; Mattick 1996). As with the onset of withdrawal, the duration also varies with the half‐life of the opioid used and the duration of regular use (Tetrault 2009). Opioid withdrawal syndrome is rarely life‐threatening or associated with significant aberrations of mental state (Farrell 1994), but the combination of uncomfortable symptoms and intense craving makes completion of withdrawal treatment difficult for most people (Mattick 1996; Tetrault 2009).
Description of the intervention
For many years routine procedures for managing opioid withdrawal involved suppression of withdrawal with methadone and gradual reduction of the methadone dose (Kleber 1982). This approach derived from observations that the withdrawal syndrome from methadone was milder, though longer, than that from morphine. Methadone's high oral bioavailability, efficacy, and long duration of withdrawal relief (24 to 36 hours) were additional factors that contributed to its widespread use in specialist withdrawal programmes.
Ambivalence to the use of a drug of dependence to treat opioid dependence, government restrictions on prescription of methadone, and consumer dislike of the protracted nature of methadone withdrawal limited, to some extent, the use of methadone for managing opioid withdrawal (Farrell 1994). One widely used non‐opioid alternative, the alpha2‐adrenergic agonist clonidine, can also ameliorate some signs and symptoms of opioid withdrawal (Gossop 1988), but it is associated with adverse effects of sedation and hypotension. Dissatisfaction with methadone and clonidine drove the development of a variety of alternative approaches, in particular buprenorphine.
How the intervention might work
This review assesses the partial agonist, buprenorphine, for managing the signs and symptoms of opioid withdrawal. Research activity has primarily focused on the use of buprenorphine as an alternative medication for opioid substitution treatment, but today physicians often use buprenorphine for managing withdrawal. The rationale behind this treatment approach is that the morphine‐like effects of buprenorphine will suppress the physical signs and symptoms of withdrawal, but people will only experience limited withdrawal signs and symptoms because buprenorphine is a partial agonist (Banys 1994).
There is a complex range of variables that can potentially influence the course and subjective severity of withdrawal, including the type of opioid used, dose taken, concomitant use of other drugs including alcohol, duration of use, general physical health, and psychological factors, such as the reasons for undertaking withdrawal and fear of withdrawal (Farrell 1994; Phillips 1986; Preston 1985). Outcomes of a withdrawal episode may also be influenced by a prior period of substitution treatment, since such treatment is likely to result in a degree of stabilisation in health and social functioning that may facilitate successful withdrawal. Where information is available, we have considered the influence of these variables.
The first, or acute, phase of withdrawal is followed by a period of about six months of a secondary or protracted withdrawal syndrome. This protracted syndrome is characterised by a general feeling of reduced well‐being, which is reflected in measurable abnormal physiological functioning. During this phase, people may periodically experience strong cravings for opioids. Some authors consider that the malaise associated with protracted abstinence is a major factor in relapse (Satel 1993). The protracted nature of withdrawal typically makes the dependence recovery period lengthy and responsive to a range of factors, both social and treatment related. The types of intervention offered following the acute phase of withdrawal to promote recovery and prevent relapse are substantially different from those offered for managing withdrawal and may include psychological and lifestyle counselling, support groups, and pharmacological and medical treatment. We have excluded this long‐term aspect of treatment of opioid dependence from this review because of its substantially different nature.
Why it is important to do this review
This review is one of a series relating to managing opioid withdrawal. Other reviews consider the use of alpha2‐adrenergic agonists (Gowing 2016), the administration of opioid antagonists with minimal sedation (Gowing 2009), their administration under heavy sedation or anaesthesia (Gowing 2010), the use of tapered doses of methadone (Amato 2013), inpatient versus other settings (Day 2005), detoxification treatments for adolescents (Minozzi 2014), and psychosocial and pharmacological treatments for opioid detoxification (Amato 2011).
Objectives
To assess the effects of buprenorphine versus tapered doses of methadone, alpha2‐adrenergic agonists, symptomatic medications or placebo, or different buprenorphine regimens for managing opioid withdrawal, in terms of the intensity of the withdrawal syndrome experienced, duration and completion of treatment, and adverse effects.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled clinical trials that provided detailed information on the type and dose of drugs used and the characteristics of participants treated. Studies also had to provide information on the nature of withdrawal signs and symptoms experienced, the occurrence of adverse effects, or the rates of completion of the treatment episode.
Types of participants
We included studies that involved participants who were primarily opioid dependent and underwent managed withdrawal.
Types of interventions
Experimental interventions involved the administration of buprenorphine for ameliorating the signs and symptoms of opioid withdrawal.
We excluded studies that combined buprenorphine with opioid antagonists administered in order to induce withdrawal. This method of managing withdrawal is covered by a separate Cochrane Review (Gowing 2009).
Comparison interventions involved tapered doses of methadone, alpha2‐adrenergic agonists, symptomatic medications or placebo, or buprenorphine‐based regimens differing in amount, duration, or rate of taper of buprenorphine. For the purpose of this review, we define symptomatic medications as benzodiazepines, antiemetics, antidiarrhoeals, antipsychotics, antispasmodics, muscle relaxants, or non‐opioid analgesics, administered in combination as needed, or according to a defined regimen.
Types of outcome measures
Primary outcomes
We assessed the included studies on the basis of a number of measures.
Intensity of withdrawal (with consideration to peak withdrawal scores and average withdrawal score over the duration of withdrawal treatment).
Duration of treatment.
Nature and incidence of adverse effects.
Completion of treatment.
Interventions aimed at the management of acute opioid withdrawal are typically of short duration. As a result, structured psychological therapies are generally not provided as adjuncts to interventions for managing withdrawal, but the episode of withdrawal management does provide the opportunity to inform people who are opioid dependent about the options for further treatment, and to encourage them to engage in treatment appropriate to their needs. The longer the duration of treatment, the more opportunities there are for interaction between treatment services and people who are opioid dependent. The relative time in treatment is also an indicator of the relative acceptability to participants of the interventions being compared. For these reasons, we considered duration of treatment in addition to treatment completion rates.
It is difficult to differentiate adverse effects of treatment from the signs and symptoms of opioid withdrawal. We defined adverse effects as clinically significant signs and symptoms of opioid withdrawal (such as vomiting and diarrhoea) plus any incidents that are not typical components of the opioid withdrawal syndrome (hypotension, dry mouth). Early experience with clonidine, which was developed as a hypotensive agent, was that low blood pressure was a common adverse effect of clonidine treatment. This review therefore considered the occurrence of hypotension or symptoms of hypotension, withholding doses of medication and cessation of treatment as adverse effects.
Secondary outcomes
We also sought to assess data on the number of participants engaged in further treatment following completion of the withdrawal intervention. As indicated in the Background, managed withdrawal by itself is not an effective treatment for dependence. Hence we consider engagement in further treatment to be an outcome of interest.
Search methods for identification of studies
All searches included non‐English language literature. We assessed studies with English abstracts on the basis of the abstract. If we thought the study was likely to meet inclusion criteria, we translated it sufficiently to extract study methods and results.
Electronic searches
We searched the Cochrane Central Register of Controlled Trials (CENTRAL, Issue 11, 2016), MEDLINE (1946 to December week 1, 2016), Embase (to 22 December 2016), PsycINFO (1806 to December week 3, 2016), and the Web of Science (to 22 December 2016).
We developed a search strategy to retrieve references for all the Cochrane Reviews relating to the management of opioid withdrawal in one operation. We adapted the strategy to each of the major databases and the supporting platform. See Appendix 1; Appendix 2; Appendix 3; Appendix 4; Appendix 5.
Searching other resources
We also searched:
the reference lists of all relevant papers to identify further studies;
some of the main electronic sources of ongoing trials: National Research Register; Current Controlled Trials (www.controlled‐trials.com); ClinicalTrials.gov (clinicaltrials.gov); Osservatorio Nazionale sulla Sperimentazione Clinica dei Medicinali (oss‐sper‐clin.agenziafarmaco.it); and Trialsjournal.com (www.trialsjournal.com);
conference proceedings likely to contain trials relevant to the review.
We contacted investigators to seek information about unpublished or incomplete trials.
Data collection and analysis
Selection of studies
One reviewer (LG) assessed each potentially relevant study for inclusion according to the identified inclusion and exclusion criteria. All reviewers confirmed the inclusion and exclusion decisions.
Data extraction and management
We developed a form for recording data on the outcomes of interest, taking into account the different ways that studies might report such data. The outcomes specified in the form were:
intensity of withdrawal (peak withdrawal score, overall withdrawal score, number with severe withdrawal, other data such as amount of adjunct medication);
duration of withdrawal treatment (days in treatment, other data such as number retained in treatment at a defined point);
adverse effects (number experiencing any adverse effects, number with hypotensive effects, number withdrawn from treatment due to adverse effects, other);
completion of treatment (number completing the scheduled period of treatment, number abstinent at completion of treatment);
postdetoxification (number engaged in further treatment, other such as number abstinent at follow‐up).
One reviewer (LG or DM) extracted key information, in consultation with other review authors where there was any uncertainty. We summarised key findings of studies descriptively in the first instance and considered the capacity for quantitative meta‐analysis. We contacted study authors if we required additional information to include studies in meta‐analyses.
Assessment of risk of bias in included studies
We assessed the methodological quality of included studies according to the approach recommended in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). This was based on the evaluation of seven specific methodological domains (namely, sequence generation, allocation concealment, blinding of participants and providers, blinding of outcome assessors, incomplete outcome data, selective outcome reporting, and 'other' issues). For each study, we analysed the seven domains, described them as reported in the study and provided a final judgement on the likelihood of bias in terms of low, high, or unclear risk of bias. We based these judgements on the criteria indicated by Higgins 2011 and their applicability to the addiction field.
We considered blinding separately for subjective and objective outcomes. Lack of blinding is a source of serious risk of bias for subjective outcomes but is less significant with objective outcomes, such as completion of treatment and duration of treatment. We only considered incomplete outcome data for intensity of withdrawal and the nature and incidence of adverse effects. Retention in treatment (duration of treatment) and completion of treatment are frequently primary outcome measures in addiction research. See Appendix 6 for a detailed description of the criteria we considered in the 'Risk of bias' assessment.
Details of the assessments of risk of bias are included in the Characteristics of included studies.
Measures of treatment effect
For dichotomous data (e.g. number completing treatment), we calculated risk ratios (RR), and for continuous data with consistent methods of measurement (e.g. time in treatment), we calculated mean differences (MD). For continuous data with differences between studies in the method of measurement (e.g. withdrawal scores), we calculated standardised mean differences (SMD). According to the approach recommended in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), we interpreted SMD of 0.2 to indicate a small effect size, SMD of 0.5 to indicate a moderate effect size, and SMD of 0.8 to indicate a large effect size. We used 95% confidence intervals (CI) to express the uncertainty in each result.
Unit of analysis issues
Where there were trials with multiple arms, we excluded any arms that involved an intervention not defined by the inclusion criteria for this review. Where there were trials with several arms relevant to meta‐analyses, we combined data involving different buprenorphine regimens after checking that the outcomes for the groups were similar.
Assessment of heterogeneity
We assessed statistical heterogeneity using the Chi2 test and its P value, by visual inspection of the forest plots, and through the I2 statistic. A P value of the test lower than 0.10 or an I2 statistic of at least 50% indicated a significant statistical heterogeneity.
Data synthesis
We used Review Manager 5 (RevMan 5) for statistical analyses (RevMan 2014). In all analyses, we used a random‐effects model. We used GRADEpro GDT to prepare the 'Summary of findings' tables (GRADEpro GDT).
Subgroup analysis and investigation of heterogeneity
This review also aimed to consider the following potential sources of heterogeneity through subgroup analyses, as this approach is considered to be associated with less risk of bias.
Drug of dependence and severity of dependence (as indicated by duration and level of use).
Polydrug use.
Concurrent physical and psychiatric illness.
Precipitants to the withdrawal episode.
Nature of the treatment setting.
Nature of adjunct treatment, including other medications to manage symptoms.
The nature of studies that met the inclusion criteria has limited such analyses. Subgroup analysis was possible only for treatment setting in the comparison of buprenorphine with an alpha2 ‐adrenergic agonist (clonidine or lofexidine).
Sensitivity analysis
We did not use risk of bias as a criterion for inclusion in the review. However, we assessed the impact of risk of bias through sensitivity analyses. This involved considering the overall estimate of effect when both including and excluding studies with a high risk of bias in meta‐analysis. We undertook sensitivity analyses where there were at least three studies providing data on the outcome, and where we assessed at least two of these studies as being at low or unclear risk of bias for that outcome. The only domain for which we performed sensitivity analyses was performance and detection bias in subjective outcomes (Analysis 2.1; Analysis 2.2).
2.1. Analysis.
Comparison 2 Buprenorphine versus clonidine, Outcome 1 Mean peak withdrawal score.
2.2. Analysis.
Comparison 2 Buprenorphine versus clonidine, Outcome 2 Mean overall withdrawal score.
Summary of findings table
We assessed the overall quality of the evidence for the primary outcome using the GRADE system. The GRADE Working Group developed a system for grading the quality of evidence that takes into account issues not only related to internal validity but also to external validity, such as directness of results (Atkins 2004; Guyatt 2008a; Guyatt 2008b; Guyatt 2011). The 'Summary of findings' tables present the main findings of a review in a transparent and simple tabular format. In particular, they provide key information concerning the quality of evidence, the magnitude of effect of the interventions examined and the sum of available data on the main outcomes.
The GRADE system assigns grades of evidence as follows.
High: we are very confident that the true effect lies close to that of the estimate of the effect.
Moderate: we are moderately confident in the effect estimate; the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low: our confidence in the effect estimate is limited; the true effect may be substantially different from the estimate of the effect.
Very low: we have very little confidence in the effect estimate; the true effect is likely to be substantially different from the estimate of effect.
We downgraded the quality of the studies for the following reasons.
Serious (−1) or very serious (−2) study limitation for risk of bias.
Serious (−1) or very serious (−2) inconsistency between study results.
Some (−1) or major (−2) uncertainty about directness (the correspondence between the population, the intervention, or the outcomes measured in the studies actually found and those under consideration in our systematic review).
Serious (−1) or very serious (−2) imprecision of the pooled estimate.
Publication bias strongly suspected (−1).
In some situations it is possible to increase grading, but this did not apply to this review.
Results
Description of studies
Results of the search
As indicated in the flow diagram (Figure 1), we identified 3573 records relevant to the management of opioid withdrawal in general. Of these, we excluded 3269 on the basis of title and abstract. We assessed 304 full‐text articles, excluding 192 (without listing reasons). We provide reasons for excluding a further 63 articles (45 studies) that appeared to be relevant, and 49 articles (27 studies) satisfied all the criteria to be included in the review.
1.
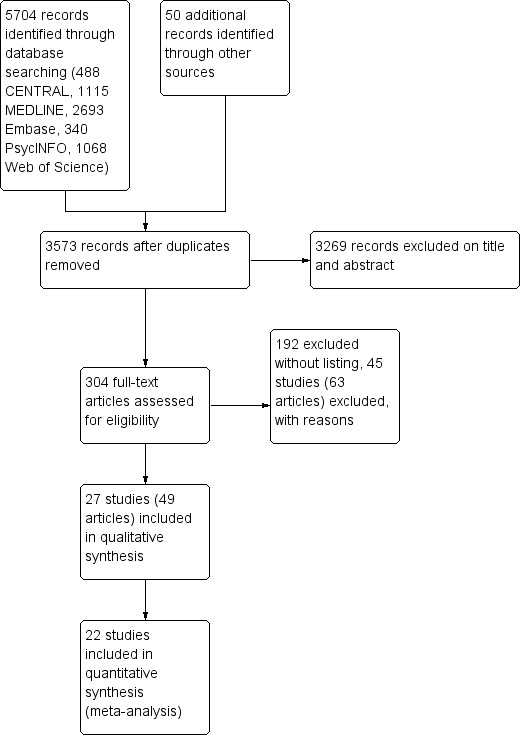
Study flow diagram.
Included studies
Twenty‐seven studies (49 reports) involving 3048 participants met the inclusion criteria for this review (see Characteristics of included studies). In total, 2172 participants received buprenorphine.
One study was partially randomised − the first 14 participants were randomly allocated, and the remaining 9 participants had access to the rapid dose reduction regimen only (Wang 1996). We included only the 14 randomly allocated participants in this review. The other studies were randomised controlled trials.
Three studies received some financial support from a pharmaceutical company, and a further three studies reported receiving study medications from a pharmaceutical company. Thirteen studies reported funding from sources other than industry; in seven studies, funding arrangements were unclear.
Major comparisons
The 27 studies made eligible comparisons that fell into three main groups.
Buprenorphine versus tapered doses of methadone (6 studies).
Buprenorphine versus an alpha2‐adrenergic agonist (14 studies) − Raistrick 2005 used the adrenergic agonist lofexidine, while the other studies used clonidine.
Different rates of reduction of buprenorphine (7 studies).
Umbricht 2003 included both clonidine and methadone comparisons, and we consider those results in both relevant comparisons (1 and 2).
In addition, Oreskovich 2005 compared different starting doses of buprenorphine, and Schneider 2000 compared buprenorphine versus oxazepam. As there were no other studies making these comparisons, we do not consider these studies further. This review focuses on the three major comparisons.
Three studies compared regimens that were not defined by the inclusion criteria for this review. Janiri 1994 included a group treated with lefetamine; O'Connor 1997 included a group treated with clonidine plus naltrexone − a separate Cochrane Review assesses this approach (Gowing 2009); and Collins 2005 included a group receiving antagonist‐induced withdrawal under anaesthesia − also covered by a separate Cochrane Review (Gowing 2010). We excluded these groups from the review.
Treatment setting
Buprenorphine versus tapered doses of methadone
Four of the six studies provided treatment on an inpatient basis. One of these studies took place in an AIDS service, participants having been admitted for acute medical illness (Umbricht 2003). Wright 2011 took place in a prison setting, through the prison healthcare centre ‐ in this setting participants would have had less access to opioid drugs than in an outpatient setting, but would have had less supervision than in an inpatient setting. Only Bickel 1988 provided treatment on an outpatient basis.
Buprenorphine versus clonidine or lofexidine
Ten of the 14 studies provided treatment on an inpatient basis. As indicated above, Umbricht 2003 took place in an AIDS service. Ling 2005 included two separate studies: one in an inpatient and one in an outpatient setting.
Different rates of buprenorphine dose reduction
Two of the seven studies provided treatment on an inpatient basis − in Assadi 2004 participants were admitted to an addiction unit, while participants in Hopper 2005 were residents in a therapeutic community. Amass 1994 and Sigmon 2013 provided treatment on an outpatient basis with participants attending a clinic on a daily basis for medication, in Ling 2009 participants attended a clinic once weekly, and Marsch 2016 initially required participants to attend the clinic daily, but after 20 enrolments this was varied to enable participants to attend two to three times weekly. The report for Wang 1996 does not give this detail, but as the scheduled study duration was 12 weeks, we assume that it was undertaken on an outpatient basis.
Participant characteristics
For 21 studies the average age of participants was in the range 25 to 40 years. In one study (Hopper 2005) the average age was 47 years, while in two studies involving adolescents (Marsch 2005, Marsch 2016), the average age of participants was in the range 17 to 20 years. Three studies (O'Connor 1997, Ponizovsky 2006, Wang 1996) did not report the average age of participants.
In 17 of the 27 studies most or all participants were withdrawing from heroin alone or heroin and methadone. In two studies most participants were withdrawing from heroin, but a minority were using opium (Assadi 2004; Nigam 1993). One study was notable in that most participants were withdrawing from prescription opioids (57% oxycodone, 39% buprenorphine) (Sigmon 2013). The remaining seven studies did not report details of the nature of opioid drugs being used, although two studies excluded people dependent on methadone (Bickel 1988; Ling 2009), and two studies compared different rates of buprenorphine taper following a period of substitution treatment with buprenorphine (Amass 1994; Wang 1996). Hence participants in these two studies were effectively withdrawing from buprenorphine.
We had intended to compare outcomes for studies involving participants withdrawing from heroin versus those withdrawing from methadone, but the nature of studies meeting the inclusion criteria did not support this analysis.
There was considerable variability between studies in approach to the use of non‐opioid drugs. Four of the studies excluded participants abusing or dependent on any psychotropic drugs other than opioids (Collins 2005; Janiri 1994; Lintzeris 2002, Nigam 1993). Assadi 2004 and Umbricht 2003 excluded alcohol dependence; Oreskovich 2005 and Wright 2011 excluded people using drugs other than opioids if medically supervised withdrawal was required, and Ponizovsky 2006 excluded people also dependent on benzodiazepines or alcohol. Participants in Amass 1994 and Petitjean 2002 who were dependent on other drugs, in addition to opioids, underwent selective detoxification prior to the study of opioid withdrawal. In Hopper 2005, 60% were also cocaine dependent. All participants in Seifert 2002 and Schneider 2000 were polydrug users.
Opioid use is generally more common amongst men than women. However, in Cheskin 1994 and Marsch 2005, fewer than half the participants were men. In Umbricht 2003, 44% of the group treated with methadone were men, compared to 71% and 69% in the buprenorphine and clonidine groups, respectively. In four studies, authors reported that all participants were men, or they were most likely all men (Bickel 1988; Hussain 2015; Nigam 1993; Ziaaddini 2012). The significance of sex for managing opioid withdrawal is unclear, and hence the potential confounding effect of this variability in gender composition between the studies is also unclear. None of the studies report outcomes on the basis of sex, preventing further exploration of this aspect.
Nigam 1993 (undertaken in India) differed in that all participants used heroin (or opium) by inhalation, a route of administration that is likely to result in lower levels of dependence (Strang 1999). Furthermore, 92% of participants in Nigam 1993 and 70% of participants in Hussain 2015 (also undertaken in India) were employed, a situation that is generally unusual for heroin users from Western countries. Marsch 2005 and Marsch 2016 differed from other studies in that all participants were adolescents.
Fourteen of the studies took place in the USA, while three took place in Germany, two each in the UK, India, and Iran, and one each in Australia, Israel, Italy, and Switzerland.
Treatment regimens
Buprenorphine has low bioavailability when administered orally (Elkader 2005). When used for treating opioid dependence, buprenorphine is most commonly administered sublingually. In early studies of buprenorphine for opioid dependence, participants received buprenorphine sublingually as a solution (Chawarski 2005). Subsequently tablet preparations were developed containing either buprenorphine alone or buprenorphine plus naloxone, a combination that is intended to reduce the risk of recreational and inappropriate use (Larance 2011). More recently a film preparation containing buprenorphine plus naloxone has become available for improved placement under the tongue and reduced risk of recreational use (Lintzeris 2013).
Nine of the 27 studies included in the review reported using sublingual buprenorphine tablets, and a further five studies used the combination buprenorphine‐naloxone tablets. One study (Marsch 2016) commenced participants on sublingual buprenorphine tablets, and transferred them to combination buprenorphine‐naloxone tablets once stable. None of the studies considered for this review used the film preparation.
Three studies reported administering buprenorphine as a sublingual solution (Amass 1994; Bickel 1988; Cheskin 1994), and three studies administered buprenorphine as intramuscular injections (Assadi 2004; Janiri 1994; Umbricht 2003). Participants in Umbricht 2003 had been admitted to hospital for acute medical conditions, and the intramuscular route may have been preferable in this population, but the preparations in the other studies probably reflected a lack of access to sublingual tablets at the time the studies were undertaken.
Six studies did not report details of the buprenorphine preparation administered (Collins 2005; Schneider 2000; Seifert 2002; Steinmann 2008; Wang 1996; Wright 2011).
A number of factors, including route of administration, influence the bioavailability of buprenorphine (Chiang 2003; Strain 2004). Given this complexity, we have not attempted to calculate equivalent doses for buprenorphine used as different formulations and via different routes.
Buprenorphine versus tapered doses of methadone
These six studies varied in both dose of buprenorphine and the scheduled duration of treatment. Umbricht 2003 used the shortest regimen: 3.6 mg buprenorphine (intramuscular) on day 1, tapered to 1.2 mg on day 3. Petitjean 2002 and Seifert 2002 administered buprenorphine in tapered doses over periods of around 10 days; Petitjean 2002 used maximum doses of 16 mg/d (as sublingual tablets), while Seifert 2002 administered maximum doses of 4 mg/d (unspecified route and formulation). Bickel 1988, Steinmann 2008 and Wright 2011 administered buprenorphine over 20 to 21 days, with maximum doses of 2 mg/d (sublingual solution, Bickel 1988), 8 mg/d (unspecified preparation, Wright 2011), or 16 mg/d (unspecified preparation, Steinmann 2008).
Buprenorphine versus alpha2 ‐adrenergic agonists (clonidine or lofexidine)
Two of the 14 studies administered buprenorphine intramuscularly. Janiri 1994 administered 0.9 mg/d for two days and tapered the dose over the next two days. Umbricht 2003 used much higher doses: 3.6 mg on day 1 to 1.2 mg on day 3, tapering the dose by reducing the frequency of injections (from every 4 h on day 1 to every 8 h on day 3). Eight studies administered buprenorphine sublingually, using maximum doses ranging from 1.2 mg/d as buprenorphine tablet in Nigam 1993 to 16 mg/d as buprenorphine/naloxone tablet in Ling 2005. Lintzeris 2002 and Ziaaddini 2012 tailored doses, within limits, in response to individual need; the other studies used fixed‐dose regimens.
Collins 2005 administered a single 8 mg dose of buprenorphine (sublingual, preparation not specified) on the first day of a scheduled three‐day hospitalisation, with naltrexone commenced at 12.5 mg on day 2. O'Connor 1997 also used buprenorphine (3 mg sublingual, preparation not specified) as a transition to naltrexone treatment − participants received combination clonidine plus naltrexone following three days of buprenorphine treatment.
Cheskin 1994, O'Connor 1997 and Umbricht 2003 administered buprenorphine for three days, Janiri 1994, for four days; Lintzeris 2002, Oreskovich 2005, and Ziaaddini 2012, for five days; Marsch 2005 and Raistrick 2005, for seven days; Ponizovsky 2006, Hussain 2015, and Nigam 1993, for 10 days; and Ling 2005, for 13 days.
Different rates of buprenorphine dose reduction
The seven studies that compared different rates of dose‐tapering with buprenorphine varied considerably in the treatment regimens.
The scheduled duration of treatment for the two studies that provided treatment on an inpatient basis (Assadi 2004 and Hopper 2005) was short compared to the studies undertaken on an outpatient basis. For this reason, we separated studies according to treatment setting for analyses.
In Assadi 2004 participants in the experimental group received 4 × 1.5 mg doses of buprenorphine (intramuscular) on the afternoon of day 1, and 4 × 1.5 mg doses (intramuscular) on the morning of day 2, giving a total dose of 12 mg. The comparison group received 3 mg (intramuscular) on day 1, tapered to 0.6 mg on day 5.
Hopper 2005 used a similarly short, high dose regimen, with one group receiving buprenorphine only on day 1 (sublingual tablet, 8 mg followed by 24 mg after 30 min). The comparison group received 32 mg of buprenorphine over three days.
The five studies undertaken in outpatient settings differed in the period of stabilisation on buprenorphine prior to dose‐tapering, the starting dose of buprenorphine and the duration of taper.
In Amass 1994, participants were stabilised on 8 mg buprenorphine for 28 days and the dose was tapered over 12 days or 36 days.
In Ling 2009, the stabilisation period was one month, with a flexible starting dose, and the taper was over seven or 28 days.
In Marsch 2016, the stabilisation period and starting dose was flexible, and the taper was over 28 days or 56 days.
In Sigmon 2013, the stabilisation period was two weeks, with a flexible starting dose, and the taper was over one, two or four weeks.
In Wang 1996, there was no specified stabilisation period, the starting dose was 8 mg and the dose was tapered over 14 days or 8 weeks.
For the purposes of this review, the treatment regimen with buprenorphine tapered over a shorter period of time was defined as "rapid", while the comparison group was defined as "slow". In Sigmon 2013 there was no difference in outcomes for the groups with the buprenorphine dose tapered over one or two weeks; data from these groups were combined as "rapid" dose taper.
Excluded studies
Forty‐five studies (63 reports) did not meet the criteria for inclusion in this review (see Characteristics of excluded studies). The reasons for exclusion were: comparison of interventions other than those defined by the inclusion criteria (17 studies); methodology other than randomised controlled trials (7 studies); no treatment comparison (6 studies); interventions not primarily based on alleviating withdrawal (9 studies), and insufficient data on outcomes defined by the inclusion criteria (14 studies). Some studies fulfilled more than one criteria for exclusion.
Risk of bias in included studies
For summary results of the judged risk of bias across the included studies for each domain, see Figure 2 and Figure 3.
2.
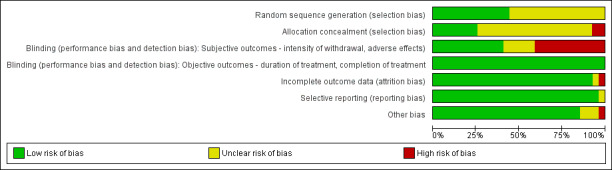
Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies.
3.
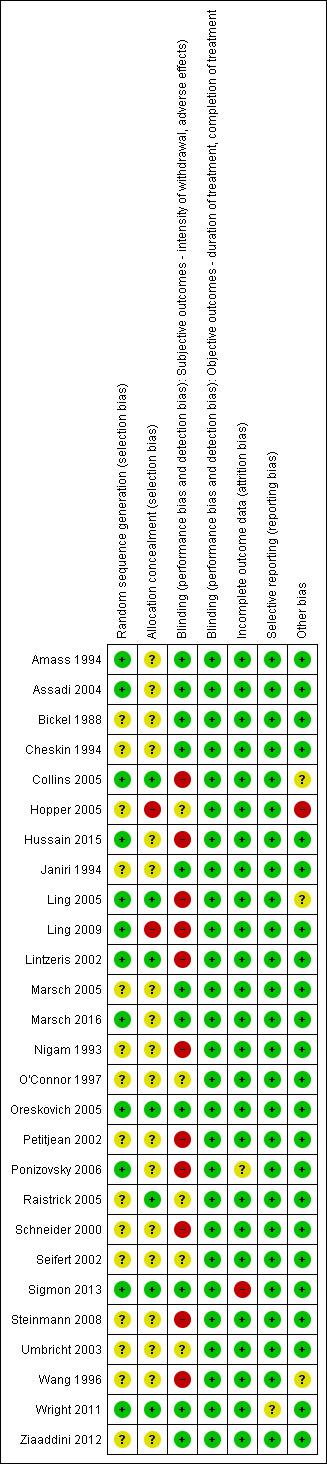
Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
Allocation
We judged five of the six studies comparing buprenorphine versus methadone to be at uncertain risk of bias due to the reporting of insufficient information on the method of random sequence generation and allocation concealment. We judged the other study in this group to be at low risk of allocation bias (Wright 2011).
Similarly we judged 10 of the 14 studies comparing buprenorphine with an alpha2‐adrenergic agonist to be at uncertain risk of bias because of insufficient information on the method of random sequence generation, allocation concealment, or both. We judged the other four studies in this group to be at a low risk of allocation bias.
We judged two of the seven studies comparing different rates of reduction of buprenorphine to be at high risk of allocation bias, as neither of these studies concealed the group allocation (Hopper 2005; Ling 2009). We assessed only Sigmon 2013 to be at low risk of allocation bias; we deemed the risk of bias to be uncertain for the other four studies in this group.
Blinding
We considered the risk of performance and detection bias for objective outcomes (duration and completion of treatment) to be low for all studies, as these outcomes are unlikely to be affected by an awareness of group allocation. This section therefore focuses on the risk of assessment bias in relation to subjective outcomes (intensity of withdrawal, occurrence, and severity of adverse effects).
We judged the following studies to be at high risk of bias due to a lack of blinding.
Two of the six studies comparing buprenorphine versus tapered doses of methadone (Petitjean 2002; Steinmann 2008).
Six of the 14 studies comparing buprenorphine versus an alpha2‐adrenergic agonist (Collins 2005; Hussain 2015; Ling 2005; Lintzeris 2002; Nigam 1993; Ponizovsky 2006).
Two of the seven studies comparing different rates of reduction of buprenorphine (Ling 2009; Wang 1996).
We judged the risk of bias to be uncertain in the following studies.
Two studies comparing buprenorphine versus methadone (Seifert 2002; Umbricht 2003).
Three studies comparing buprenorphine versus an alpha2‐adrenergic agonist (O'Connor 1997; Raistrick 2005; Umbricht 2003).
We judged the risk of bias to be low in all other studies.
Incomplete outcome data
Retention (duration of treatment) and completion of treatment are primary outcome measures for opioid withdrawal interventions. Hence we only considered the risk of bias due to incomplete data for the outcomes of intensity of withdrawal and adverse effects.
We judged the risk of bias to be high for Sigmon 2013 and uncertain for Ponizovsky 2006. We judged the risk of bias to be low in all other studies.
Selective reporting
We judged the risk of bias to be uncertain for Wright 2011 due to data on adverse effects being collected but not reported. We judged the risk of bias to be low in all other studies.
Other potential sources of bias
We judged the risk of bias to be high for Hopper 2005 as all participants were resident in a therapeutic community. This may have resulted in selection of a highly motivated group who would have done well whatever the treatment.
Collins 2005 and Ling 2005 were both stopped early due to clear benefits from one of the interventions being compared. Potentially this could have introduced bias, but it is difficult to determine the extent of risk.
We also judged Wang 1996 to be at uncertain risk of bias, as there was little information available to assess this study.
Effects of interventions
See: Table 1; Table 2; Table 3
Summary of findings for the main comparison. Buprenorphine vs methadone for managing opioid withdrawal.
| Buprenorphine versus methadone for managing opioid withdrawal | |||||
| Patient or population: Adults with opioid dependence Setting: Inpatient or outpatient Intervention: Buprenorphine Comparison: Methadone | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with methadone | Risk with buprenorphine | ||||
| Mean days in treatment | The mean days in treatment in the methadone group was 10.8 or 48.5 days. | The mean days in treatment in the buprenorphine group was 1.3 more (8.1 less to 10.7 more) than in the methadone group. | — | 82 (2 RCTs) | ⊕⊕⊝⊝ Lowa,b |
| Completion of withdrawal treatment | Study population | RR 1.04 (0.91 to 1.20) | 457 (5 RCTs) | ⊕⊕⊕⊝ Moderateb | |
| 528 per 1000 | 549 per 1000 (481 to 634) | ||||
| Moderate | |||||
| 534 per 1000 | 555 per 1000 (486 to 641) | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RCT: randomised controlled trial; RR: risk ratio; OR: odds ratio. | |||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||||
aStudies were conducted in different settings (inpatient and outpatient). bSmall number of participants (N < 300).
Summary of findings 2. Buprenorphine vs alpha2‐adrenergic agonists for managing opioid withdrawal.
| Buprenorphine vs alpha2‐adrenergic agonists for managing opioid withdrawal | |||||
| Patient or population: Adults or adolescents with opioid dependence Setting: Inpatient or outpatient Intervention: Buprenorphine Comparison: Alpha2‐adrenergic agonists (clonidine or lofexidine) | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with alpha2‐adrenergic agonists | Risk with buprenorphine | ||||
| Mean peak withdrawal score, assessed with various scales | Not able to be summarised due to different means of assessment | The mean peak withdrawal score was lower in the buprenorphine group, indicating less severity, with a standardised mean difference of 0.43, which is a moderate effect size | SMD ‐0.43 (‐0.74 to ‐0.13) | 521 (6 RCTs) | ⊕⊝⊝⊝ Very lowa,b,c,d |
| Mean overall withdrawal score, with various methods of assessment | Not able to be summarised due to different means of assessment | The mean overall withdrawal score was lower in the buprenorphine group, indicating less severity, with a standardised mean difference of 0.43, which is a moderate effect size | SMD ‐0.43 (‐0.58 to ‐0.28) | 902 (7 RCTs) | ⊕⊕⊕⊝ Moderatea |
| Mean days in treatment (with varying scheduled duration) | Mean days in treatment ranged across studies from 21% to 70% of scheduled treatment duration | Mean days in treatment ranged across studies from 25% to 97% of scheduled treatment duration, with a standardised mean difference of 0.92, which is a large effect size. | SMD 0.92 (0.57 to 1.27) | 558 (4 RCTs) | ⊕⊕⊕⊝ Moderatec,d |
| Number experiencing adverse effects | Study population | RR 0.93 (0.70 to 1.26) | 493 (3 RCTs) | ⊕⊝⊝⊝ Very lowa,b,c | |
| 289 per 1000 | 269 per 1000 (202 to 364) | ||||
| Moderate | |||||
| 127 per 1000 | 118 per 1000 (89 to 160) | ||||
| Number with treatment stopped due to adverse effects | Study population | RR 0.20 (0.04 to 1.15) | 134 (3 RCTs) | ⊕⊕⊝⊝ Lowb | |
| 90 per 1000 | 18 per 1000 (4 to 103) | ||||
| Moderate | |||||
| 79 per 1000 | 16 per 1000 (3 to 91) | ||||
| Number completing withdrawal treatment | Study population | RR 1.59 (1.23 to 2.06) | 1264 (11 RCTs) | ⊕⊕⊕⊝ Moderated | |
| 453 per 1000 | 721 per 1000 (558 to 934) | ||||
| Moderate | |||||
| 536 per 1000 | 852 per 1000 (659 to 1000) | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RCT: randomised controlled trial; RR: risk ratio; OR: odds ratio. | |||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||||
aRisk of bias in blinding of subjective outcomes. bSmall number of events (n < 300). cDifferent treatment settings (outpatient and inpatient). dHeterogeneity > 60%.
Summary of findings 3. Rapid vs slow taper of buprenorphine dose for managing opioid withdrawal.
| Rapid versus slow taper of buprenorphine dose for managing opioid withdrawal | |||||
| Patient or population: Adults or adolescents with opioid dependence Setting: Inpatient or outpatient Intervention: Rapid Comparison: Slow dose taper | |||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | |
| Risk with slow dose taper | Risk with rapid taper | ||||
| Completion of withdrawal treatment − Inpatient | Study population | RR 1.00 (0.84 to 1.18) | 60 (2 RCTs) | ⊕⊕⊝⊝ Lowa | |
| 900 per 1000 | 900 per 1000 (756 to 1000) | ||||
| Moderate | |||||
| 900 per 1000 | 900 per 1000 (756 to 1000) | ||||
| Completion of withdrawal treatment − Outpatient | Study population | RR 0.86 (0.44 to 1.70) | 647 (4 RCTs) | ⊕⊝⊝⊝ Very lowb,c | |
| 594 per 1000 | 511 per 1000 (261 to 1000) | ||||
| Moderate | |||||
| 636 per 1000 | 547 per 1000 (280 to 1000) | ||||
| Number abstinent at completion of dose taper − Inpatient | Study population | RR 1.00 (0.81 to 1.23) | 40 (1 RCT) | ⊕⊕⊝⊝ Lowa,d | |
| 900 per 1000 | 900 per 1000 (729 to 1000) | ||||
| Moderate | |||||
| 900 per 1000 | 900 per 1000 (729 to 1000) | ||||
| Number abstinent at completion of dose taper − Outpatient | Study population | RR 0.94 (0.39 to 2.24) | 619 (4 RCTs) | ⊕⊝⊝⊝ Very lowb,c | |
| 320 per 1000 | 301 per 1000 (125 to 717) | ||||
| Moderate | |||||
| 337 per 1000 | 317 per 1000 (131 to 755) | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval;RCT: randomised controlled trial; RR: risk ratio; OR: odds ratio. | |||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | |||||
aSmall number of events (n < 300). bHigh degree of heterogeneity (>75%). cMost studies small. dOnly one study.
We present results in three sections according to the nature of the comparison: tapered doses of methadone, alpha2‐adrenergic agonist (clonidine or lofexidine), and different rates of buprenorphine dose reduction. We subdivide each of these sections into parts addressing the outcomes of interest to this review: intensity of withdrawal, duration of withdrawal treatment (indicative of both duration of withdrawal and retention in treatment), nature and incidence of adverse effects, and completion of treatment.
Buprenorphine versus tapered doses of methadone
Intensity of withdrawal
Meta‐analysis was not possible for this outcome.
Petitjean 2002 reported no difference in total withdrawal severity, but significantly higher withdrawal scores on day 8 in the buprenorphine group and on days 13 and 16 in the methadone group. Based on the graph presented in the trial report, the average withdrawal score was high in the buprenorphine group to day 12 (the average duration of the buprenorphine taper) before rapidly declining, while in the methadone group the withdrawal score increased steadily to day 16 (the taper was completed on average in 15 days) then declined.
Seifert 2002 presented data as graphs only. These show withdrawal scores to be significantly lower in the buprenorphine group on days 8 and 14. Scores of clinical impression were also significantly lower on days 7 and 14.
Bickel 1988 and Umbricht 2003 found no significant difference between the buprenorphine and methadone groups.
Steinmann 2008 and Wright 2011 did not report data on withdrawal severity.
Duration of withdrawal treatment
Two studies reported data on the average length of stay in treatment (Analysis 1.1). There is no significant difference in the average length of time in treatment in either study (MD 1.30 days, 95% CI −8.11 to 10.72; N = 82; studies = 2). We assessed the quality of evidence for this outcome as low (Table 1).
1.1. Analysis.
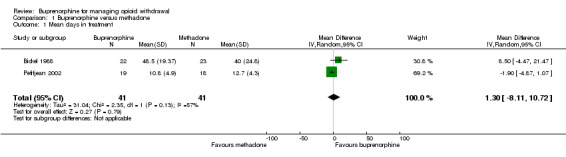
Comparison 1 Buprenorphine versus methadone, Outcome 1 Mean days in treatment.
Seifert 2002 and Steinmann 2008 did not report data on retention in treatment. In Umbricht 2003 the duration of treatment was determined by the acute condition for which the participant was admitted to hospital, rather than by completion of withdrawal treatment. In Wright 2011, the prison setting meant that duration of treatment was potentially affected by a range of factors unrelated to the type of treatment.
Nature and incidence of adverse effects
Three studies stated there were no significant adverse effects in either buprenorphine or methadone groups (Bickel 1988; Seifert 2002; Umbricht 2003). Other studies did not comment on adverse effects.
Completion of treatment
Five studies provided data on completion of treatment (Analysis 1.2). The combined result shows no difference between buprenorphine and methadone in terms of completion of withdrawal treatment (RR 1.04, 95% CI 0.91 to 1.20; N = 457; studies = 5). We assessed the quality of evidence for this outcome as moderate (Table 1).
1.2. Analysis.
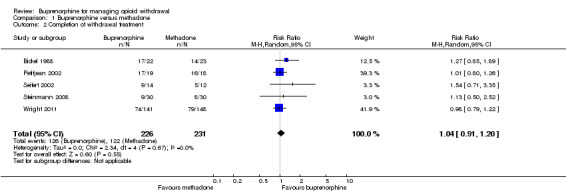
Comparison 1 Buprenorphine versus methadone, Outcome 2 Completion of withdrawal treatment.
In Umbricht 2003, the duration of hospital stay depended on the acute condition for which the participant was admitted to hospital, and completion of withdrawal treatment was not relevant.
Buprenorphine versus alpha2‐adrenergic agonists
Intensity of withdrawal
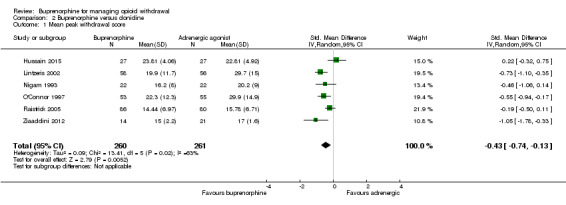
Six studies reported a mean peak withdrawal score (Analysis 2.1). In five of the six studies, the mean peak withdrawal score was lower for those treated with buprenorphine, compared to those treated with an alpha2‐adrenergic agonist. The studies differed in the scale used to assess withdrawal severity, preventing the direct comparison of withdrawal scores across studies, but in all studies a higher score indicates more severe withdrawal. The effect size has instead been estimated as a standardised mean difference. The combined result moderately favours buprenorphine (SMD −0.43, 95% CI −0.74 to −0.13; N = 521; studies = 6). We assessed the quality of evidence for this outcome as very low (Table 2), in part due to the high level of unexplained heterogeneity (I2 = 63%).
We assessed three of the studies as being at high risk of bias for this outcome (Hussain 2015; Lintzeris 2002; Nigam 1993). When we excluded these three studies in a sensitivity analysis, the combined result remained moderately in favour of buprenorphine (SMD −0.50, 95% CI −0.92 to −0.09; N = 309; studies = 6).
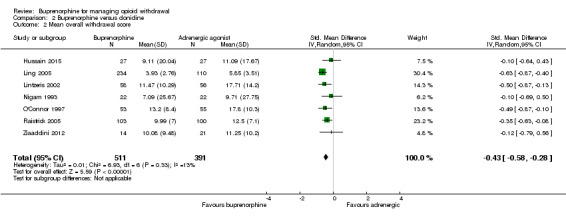
A mean overall withdrawal score was reported, or able to be calculated, for seven studies (Analysis 2.2). In all seven studies the mean withdrawal score was lower for those treated with buprenorphine, compared to those treated with an alpha2‐adrenergic agonist. We combined data from inpatient and outpatient groups in Ling 2005 in this analysis. The combined result favours buprenorphine with a moderate effect size (SMD −0.43, 95% CI −0.58 to −0.28; N = 902; studies = 7). We assessed the quality of evidence for this outcome as moderate (Table 2).
We assessed four of the studies as being at high risk of bias for this outcome (Hussain 2015; Ling 2005; Lintzeris 2002; Nigam 1993). When we excluded these four studies in a sensitivity analysis, the combined result remained significant in favour of buprenorphine with a moderate effect size (SMD −0.37, 95% CI −0.58 to −0.16).
Five other studies also reported less severe withdrawal in those treated with buprenorphine but did not report data in a form that could be included in analyses.
Cheskin 1994 reported the mean total (area under the curve) opioid withdrawal symptom score as being 88% higher in the clonidine‐treated group compared to the buprenorphine‐treated group in the first three days.
Janiri 1994 stated that buprenorphine was significantly more effective than clonidine in suppressing withdrawal.
Oreskovich 2005 reported that 10 of 20 (50%) participants receiving buprenorphine and 1 of 9 (11%) receiving clonidine achieved a suppression of withdrawal in the first 24 hours of treatment. In addition authors stated that Clinical Opiate Withdrawal Scale (COWS) scores were significantly lower in the buprenorphine group over the five days of treatment.
Marsch 2005 stated that those in the buprenorphine group reported more positive effects of medication.
Ponizovsky 2006 did not rate the severity of withdrawal during the detoxification period; however, after the 10‐day detoxification period both the clonidine and buprenorphine groups had similar ratings on the Clinical Global Impression (CGI) scale, with both groups displaying normal to borderline mental illness scores. The CGI scale is a brief assessment providing the clinician's view of a patient's global functioning, taking into account psychosocial circumstances, symptoms, and behaviour. The assessment is comprised of a one‐item measure evaluating the severity of psychopathology from 1 to 7 and the change in psychopathology using a similar scale, after the initiation of treatment.
In two studies there was no significant difference in withdrawal severity for groups treated with buprenorphine versus clonidine (Collins 2005; Umbricht 2003).
Duration of withdrawal treatment
Four studies reported data on length of treatment (Analysis 2.3). Collins 2005 reported the average weeks in treatment, encompassing the period of inpatient treatment and subsequent naltrexone maintenance treatment. We included these data (converted from weeks to days) in the inpatient subcategory, as this was the setting for detoxification. Ling 2005 studied separate groups in inpatient and outpatient settings − we included both sets of data as two studies in the analysis. Oreskovich 2005 compared two buprenorphine regimens with clonidine. We combined the data and converted results from hours to days prior to analysis. As the studies differed in the scheduled duration of treatment, we calculated a standardised mean difference rather than directly comparing the average days in treatment.
2.3. Analysis.
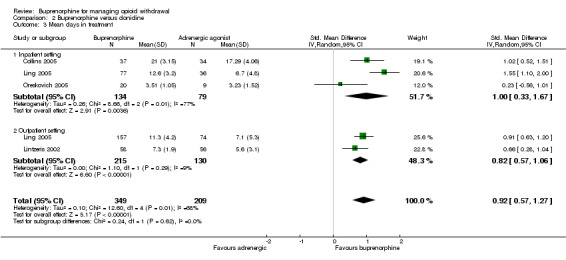
Comparison 2 Buprenorphine versus clonidine, Outcome 3 Mean days in treatment.
Based on these four studies, participants receiving buprenorphine were likely to be retained in treatment for significantly longer than those receiving clonidine (SMD 0.92, 95% CI 0.57 to 1.27; N = 558; studies = 5). The effect size is large for both inpatient and outpatient settings. We assessed the quality of evidence for this outcome as moderate (Table 2).
O'Connor 1997 used eight‐day treatment protocols. The clonidine group received naltrexone on day eight. The buprenorphine group received buprenorphine for three days, then clonidine plus naltrexone, with a dose of 50 mg naltrexone scheduled for day five. Authors did not report the mean length of stay, but there was a comparison of retention in treatment at day 8, the first day on which participants in both treatment protocols had completed detoxification. The authors found no significant difference between the groups, with 65% of those who received clonidine only, and 60% of the buprenorphine group remaining in treatment.
In Umbricht 2003 the duration of treatment was determined by the acute medical condition that led to hospital admission, and not opioid withdrawal. Authors did not report data on treatment duration.
In Ziaaddini 2012, withdrawal managed with buprenorphine or clonidine was a precursor to relapse prevention treatment with naltrexone. The reported duration of treatment included both the withdrawal phase and the subsequent period of naltrexone treatment.
The remaining seven studies did not discuss duration of treatment (Cheskin 1994; Hussain 2015; Janiri 1994; Marsch 2005; Nigam 1993; Ponizovsky 2006; Raistrick 2005).
Nature and incidence of adverse effects
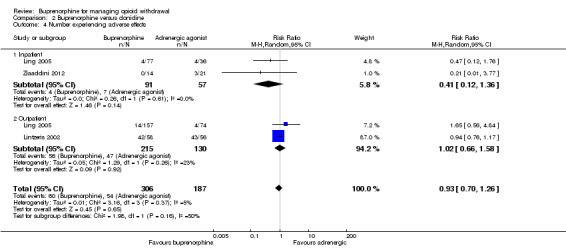
Three studies reported the number of participants who experienced adverse effects (Analysis 2.4). Ling 2005 comprised two separate studies, one in outpatient and one in inpatient settings, and we consider data as two studies in the analysis. The data suggest no significant difference between buprenorphine and an alpha2‐adrenergic agonist in terms of the number of participants experiencing adverse effects (RR 0.93, 95% CI 0.70 to 1.26; N = 493; studies = 4). In addition, Collins 2005 stated there were no serious adverse effects in either the buprenorphine or clonidine group. We assessed the quality of evidence for this outcome as very low (Table 2)
2.4. Analysis.
Comparison 2 Buprenorphine versus clonidine, Outcome 4 Number experiencing adverse effects.
A number of studies included discussion of the nature of adverse effects experienced.
Hussain 2015 reported dizziness and dry mouth as common adverse effects in those treated with clonidine, whereas the buprenorphine group experienced headache, constipation, and nausea. Similarly, Nigam 1993 reported giddiness, dry mouth, and constipation in the clonidine group, and nausea, vomiting, and constipation in the buprenorphine group. In Lintzeris 2002, headache was the most commonly reported adverse effect in the buprenorphine group, compared to dizziness and lethargy in those treated with clonidine.
Ling 2005 included continued substance abuse or overdose that resulted in overnight hospitalisation in their definition of adverse events. Fourteen of 157 (8.9%) outpatients receiving buprenorphine experienced serious adverse effects, 10 of which were ongoing substance abuse or overdose. In contrast, 4 of 74 (5.4%) in the clonidine group experienced serious adverse events, 1 of which was ongoing substance abuse. Ling 2005 also reported mean adverse events (± standard deviation (SD)) per participant per day in both inpatients: 1.5 (± 0.8) events for the buprenorphine group versus 2.4 (± 1.6) events for the clonidine group; and in outpatients: 0.7 (± 0.8) events for the buprenorphine group versus 1.2 (± 1.6) events for the clonidine group.
Cheskin 1994 reported a lower respiratory rate, and higher sedation in the buprenorphine group during the three days of treatment. Janiri 1994 reported no significant difference in heart rate or blood pressure. Oreskovich 2005 reported the proportion of occasions when practitioners withheld doses of clonidine (or placebo) due to hypotension: on day 2, physicians withheld 18.4% of the doses in the high dose buprenorphine group, 30.3%in the low dose buprenorphine group, and 38.5% in the clonidine group. On day 3, the proportions were 30.3%, 22.9%, and 38.1%, respectively. As noted by Oreskovich 2005, investigators did not expect to see hypotension in the buprenorphine group; there was no statistically significant difference in the rate of low diastolic blood pressure between the three groups.
These data suggest no significant difference between buprenorphine and clonidine in the incidence of adverse effects, but there are differences in the nature of associated adverse effects and potentially in the severity of adverse effects experienced.
In Ponizovsky 2006 the presence of adverse effects was measured using the Distress Scale for Adverse Symptoms (DSAS) which comprises 22 common adverse effects, each rates 0 (none) to 4 (extreme) for severity. Scores (mean ± SD) were significantly lower for participants receiving buprenorphine (1.81 ± 1.32) compared to those receiving clonidine (6.01 ± 1.42).
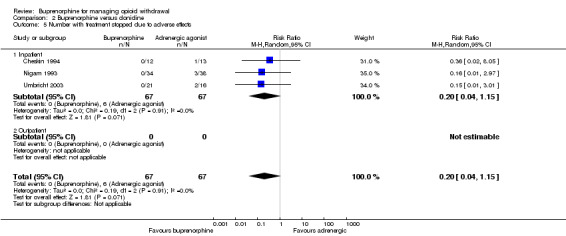
Three studies, all taking place in an inpatient setting, reported the number of participants stopping treatment due to adverse effects (Analysis 2.5). This occurred only for the clonidine groups in all three studies (RR 0.20, 95% CI 0.04 to 1.15). However, given the small number of events, we rated the quality of evidence for this outcome as low (Table 2).
2.5. Analysis.
Comparison 2 Buprenorphine versus clonidine, Outcome 5 Number with treatment stopped due to adverse effects.
Collins 2005 reported that no participants in either the buprenorphine or clonidine groups stopped treatment because of adverse effects.
Three studies did not discuss adverse effects (Marsch 2005; O'Connor 1997; Raistrick 2005).
Completion of treatment
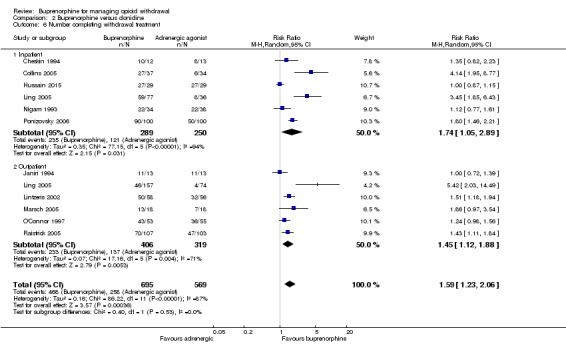
We present data on the number of participants who completed the study or the scheduled period of treatment in Analysis 2.6. Two studies reported the number of participants who received a 50 mg dose of naltrexone (Collins 2005; O'Connor 1997). We interpreted these data as indicating the number of participants completing withdrawal treatment, but that may represent a more stringent definition of completion than is the case for other studies. The combined result indicates an advantage for buprenorphine over clonidine in terms of completion of withdrawal treatment in both inpatient (RR 1.74, 95% CI 1.05 to 2.89; N = 539; studies = 6) and outpatient (RR 1.45, 95% CI 1.12 to 1.88; N = 725; studies = 6) settings. The overall result (RR 1.59, 95% CI 1.23 to 2.06; N = 1264; studies = 12) translates to a number needed to treat for an additional beneficial outcome of 4 (95% CI 2.8 to 6.7), indicating that for every four people treated with buprenorphine, we can expect that one additional person will complete treatment than with clonidine. We assessed the quality of evidence for this outcome as moderate (Table 2).
2.6. Analysis.
Comparison 2 Buprenorphine versus clonidine, Outcome 6 Number completing withdrawal treatment.
In one study, discharge from hospital depended on the acute condition leading to admission, not by completion of withdrawal treatment − 25 of 31 participants in the study were discharged from hospital prior to completion of withdrawal (Umbricht 2003). The remaining study did not report data on completion of treatment (Oreskovich 2005).
Five studies reported outcomes following completion of the study intervention.
In Lintzeris 2002, 47 of 58 (81%) in the buprenorphine group engaged in some form of postwithdrawal treatment, compared with 37 of 56 (66%) in the clonidine group. In the 28 days following completion of the study intervention, participants in the buprenorphine group received a mean (± SD) of 19.0 (± 11.2) days of treatment, compared to 11.0 (± 11.0) days for participants in the clonidine group.
In Collins 2005, detoxification was followed by naltrexone maintenance treatment. In the buprenorphine group, 9 of 37 (24%) were retained in treatment for 12 weeks, compared to 3 of 34 (9%) in the clonidine group. This difference may be due at least in part to the treatment protocols, with the buprenorphine group receiving the first dose of naltrexone while still in hospital, whereas the clonidine group did not receive it until after hospital discharge.
In Raistrick 2005, 37 of 92 (40%) in the buprenorphine group reported abstinence at one‐month follow‐up, compared to 26 of 82 (32%) in the lofexidine group. At this time, 6.5% in the buprenorphine group and 8.5% in the lofexidine group were receiving a substitute prescription, while 14.1% and 8.5%, respectively, were prescribed naltrexone.
In Marsch 2005, 61% of the buprenorphine group and 5% of the clonidine group initiated treatment with naltrexone.
In Ziaaddini 2012, 52% of participants in the clonidine group commenced naltrexone treatment and remained in treatment for an average of 70.2 days, compared to 53% of participants in the buprenorphine group, who remained in naltrexone treatment for an average of 66.7 days.
Different rates of buprenorphine dose reduction
As noted in Description of studies, the scheduled duration of treatment was shorter for the studies in this group that were undertaken in an inpatient versus outpatient setting. For this reason, we consider results separately according to this variable.
Intensity of withdrawal
No meta‐analysis was possible for this outcome.
Inpatient studies
Assadi 2004 administered buprenorphine over two or five days and found no significant differences in withdrawal severity. However, peak withdrawal occurred earlier with the more rapid treatment protocol, and participants in this group used more adjunct medication.
Hopper 2005 administered buprenorphine over one or three days, and found no significant differences in withdrawal scores or the use of adjunct medications.
Outpatient studies
Amass 1994 tapered buprenorphine over 12 or 36 days in an outpatient setting. While there was no difference in observers' assessment of withdrawal severity, the rate of increase in participant‐rated withdrawal severity was significantly greater in the rapid taper group.
Ling 2009 tapered buprenorphine over 7 or 28 days in an outpatient setting. There were no significant differences between the groups in withdrawal ratings, but participants in the rapid taper group used less concomitant medications.
Sigmon 2013 tapered buprenorphine over one, two, or four weeks in an outpatient setting. Authors reported that those in the four‐week taper group experienced a relatively mild and stable course of withdrawal whereas those in the one‐ and two‐week taper groups experienced a sharp increase in withdrawal during the week following the last dose of buprenorphine. There were no differences between the groups in the use of ancillary medications.
Wang 1996 did not rate withdrawal severity. However, authors reported that all participants in the rapid taper group experienced muscle aches, and most had lengthy insomnia. Participants reported prolonged symptoms even with adjunct medication. In contrast, participants in the gradual reduction group had minimal complaints.
Marsch 2016 did not discuss withdrawal severity.
Duration of withdrawal treatment
No meta‐analysis was possible for this outcome.
Inpatient studies
In Assadi 2004, both groups were scheduled to remain in inpatient treatment for 10 days, with buprenorphine tapered over two or five days during this time. The reported average time in treatment was 9.5 (± 1.8) days for the rapid taper group, compared to 9.8 (± 0.9) days for the five‐day group.
Hopper 2005 did not report data on the average duration of treatment.
Outpatient studies
Marsch 2016 reported an average 37.5 days in treatment for the group with buprenorphine tapered over 56 days, compared to an average 26.4 days for the group with buprenorphine tapered over 28 days. However, the authors also noted a significant effect of the frequency of clinic attendance, with an average 17.3 days in treatment for those required to attend the clinic daily compared to an average 46.7 days for those required to attend on 2 or 3 days each week. No other studies reported data on the average duration of treatment, although Amass 1994 reported that rapid dropout occurred in the rapid taper group once the detoxification phase commenced.
Nature and incidence of adverse effects
No meta‐analysis was possible for this outcome.
Inpatient studies
Assadi 2004 reported no significant difference between the two‐day and five‐day treatment regimens in terms of total adverse effects profile, and no significant difference in any specific adverse effect. They did note that blood levels of one liver enzyme (alanine transaminase, or ALT) had a greater increase from baseline in the group who received the five‐day treatment, but there are multiple factors that can impact liver enzymes, and this difference may not have been related to the buprenorphine regimen.
Hopper 2005 did not comment on adverse effects.
Outpatient studies
Amass 1994, Ling 2009 and Sigmon 2013 did not comment on adverse effects. Wang 1996 stated there were none reported. Marsch 2016 reported that no trial‐specific serious adverse events occurred.
Completion of treatment
We used subgroup analysis to consider data from studies undertaken in inpatient and outpatient settings separately. Due to the substantially different treatment regimens used in the two types of setting, we did not calculate an overall estimate of effect.
Inpatient studies
Two studies reported the number of participants who completed treatment (Analysis 3.1). There was no effect of the rate of dose taper on completion of treatment (RR 1.00, 95% CI 0.84 to 1.18; N = 60; studies = 2). We assessed the quality of evidence for this outcome as low (Table 3).
3.1. Analysis.
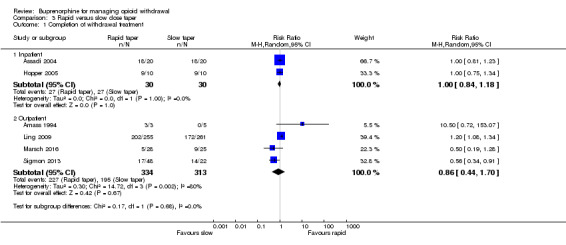
Comparison 3 Rapid versus slow dose taper, Outcome 1 Completion of withdrawal treatment.
Assadi 2004 confirmed abstinence by a naloxone challenge test at the completion of treatment (Analysis 3.2), finding no effect of the rate of dose taper (RR 1.00, 95% CI 0.81 to 1.23; N = 40; studies = 1). Hopper 2005 did not report the number of participants who were abstinent at the completion of treatment. We assessed the quality of evidence for this outcome as low (Table 3).
3.2. Analysis.
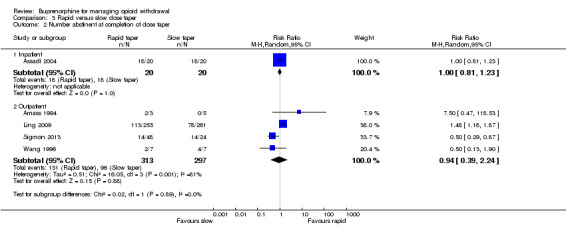
Comparison 3 Rapid versus slow dose taper, Outcome 2 Number abstinent at completion of dose taper.
In Assadi 2004, the total scheduled stay in hospital was 10 days, and naltrexone treatment was available as aftercare. Authors reported no data on this aspect.
Hopper 2005 took place in a residential therapeutic community and presumably study participants subsequently continued in the residential programme. Retention at 14 days was 7 of 10 participants in the 1‐day group and 5 of 10 in the 3‐day group.
Outpatient studies
Four studies that took place in an outpatient setting reported the number of participants who completed treatment (Analysis 3.1). Sigmon 2013 compared treatment regimens with buprenorphine tapered over one, two, or four weeks. We combined data from the one‐ and two‐week regimens prior to entry into the analyses to make the data comparable with that of the other studies.
There was no effect of the rate of dose taper on completion of treatment (RR 0.86, 95% CI 0.44 to 1.70; N = 647; studies = 4; I2 = 80%) However, there is a high degree of heterogeneity in this result, which is likely to reflect the diverse nature of the studies. This, and the small number of participants involved, resulted in our rating the quality of evidence for this outcome as very low (Table 3).
Wang 1996 did not clearly report the number of participants who completed treatment.
Four studies reported the number of participants abstinent at the completion of treatment (Analysis 3.2). Marsch 2016 reported that a higher percentage of scheduled urine tests were opioid negative in the group with buprenorphine tapered over 56 days compared with the group with the dose tapered over 28 days (35% versus 17%) but this outcome was also influenced by the frequency of clinic attendance with 20.6% of opioid‐negative urine samples for those required to attend daily, versus 66.2% for those required to attend 2 to 3 days a week. Based on Analysis 3.2, there was no effect of the rate of dose taper on the likelihood of abstinence at completion of treatment (RR 0.94, 95% CI 0.39 to 2.24; N = 610; studies = 4; I2 = 81%). Again there is substantial heterogeneity, and we assessed the quality of evidence for this outcome as being very low (Table 3).
Only Sigmon 2013 reported any data on engagement in ongoing treatment. In this study, participants received naltrexone as a second phase of treatment, from the end of the buprenorphine taper to week 12. Eleven of 22 in the four‐week taper group and 10 of 48 in the other groups were retained in treatment to the end of this phase of the study.
Discussion
Summary of main results
Buprenorphine versus tapered doses of methadone
Data comparing buprenorphine versus methadone in tapered doses for managing opioid withdrawal remains limited but are suggestive of buprenorphine and methadone having similar capacity to ameliorate opioid withdrawal, without significant adverse effects. The available data suggest there is no significant difference between buprenorphine and methadone in terms of average treatment duration or rates of completion of withdrawal treatment. We assessed the quality of evidence as low to moderate (Table 1).
There remains a possibility that the pattern of withdrawal symptoms may be different when managing it with buprenorphine versus methadone (Cameron 2001). In Seifert 2002, withdrawal severity was rated only on days 0 (baseline), 2, 8, and 14, while both buprenorphine and methadone were tapered over 11 days. These three assessment points are not sufficient to provide a clear indication of the pattern of withdrawal. Petitjean 2002 reported withdrawal scores on a daily basis up to day 18, while buprenorphine was tapered over an average of 12 days, and methadone an average of 15 days. A feature of managed withdrawal with tapered doses of methadone is that peak withdrawal severity occurs at the end of the methadone taper (Gossop 1989b). The pattern of withdrawal severity for the group treated with methadone in Petitjean 2002 is consistent with this, showing a steady climb in severity to peak around day 15. In contrast, for the buprenorphine group, withdrawal severity is high early in treatment and declines rapidly after day 10. Seifert 2002 also reported that withdrawal scores were significantly lower in the buprenorphine group in the latter stages of treatment. Furthermore, Lintzeris 2002 reported that after ceasing buprenorphine, 5 out of 53 experienced mild and/or transient withdrawal, and 4 of 53 reported moderately severe 'rebound' withdrawal (i.e. the re‐emergence of withdrawal symptoms after ceasing use of the medication for managing withdrawal). These data suggest that most individuals treated with tapered doses of buprenorphine do not experience rebound withdrawal after cessation of buprenorphine. The finding that buprenorphine has similar capacity as methadone for suppressing withdrawal signs and symptoms is consistent with findings in relation to maintenance treatment (Mattick 2014). Overall, however, more information is required on the patterns of withdrawal associated with tapered doses of buprenorphine and methadone in order to draw conclusions on the relative effectiveness of these drugs in terms of amelioration of the signs and symptoms of opioid withdrawal.
Buprenorphine versus alpha2‐adrenergic agonists
The withdrawal scores and descriptive reporting of the withdrawal syndrome experienced by participants support a conclusion that buprenorphine is more effective than alpha2‐adrenergic agonists in ameliorating the signs and symptoms of opioid withdrawal, both in terms of the peak average withdrawal score and the average daily withdrawal score over the withdrawal episode. We assessed the quality of evidence as low to moderate (Table 2).
Available data suggest that, compared to alpha2‐adrenergic agonists, buprenorphine is associated with greater retention in treatment, as indicated by a longer mean duration of treatment, in both inpatient and outpatient settings, with moderate quality of evidence (Table 2). The clinical significance of a longer period of time in treatment is that it increases the opportunity for interventions to encourage engagement in further treatment following the episode of managed withdrawal.
There was no significant difference between buprenorphine and alpha2‐adrenergic agonists (clonidine or lofexidine) in terms of the number of participants experiencing adverse effects. The nature of adverse effects experienced appears to differ, with dizziness, dry mouth, and lethargy being particularly common with alpha2‐adrenergic agonists and headache being most prominent with buprenorphine, while dropout from treatment because of adverse effects was somewhat more likely with alpha2‐adrenergic agonists. The small number of events and the small number of studies providing data led us to assess the quality of evidence on adverse effects as low to very low (Table 2).
Completion of withdrawal treatment is significantly more likely when managing withdrawal with buprenorphine compared to an alpha2‐adrenergic agonist, in either an inpatient or an outpatient setting. The overall result translates to a number needed to treat for an additional beneficial outcome of 4 (95% CI 3 to 6), indicating that for every four people treated with buprenorphine, we can expect that one additional person will complete treatment than with clonidine or lofexidine. We assessed the quality of evidence as moderate (Table 2).
Data on engagement in postdetoxification treatment is limited, but four of the five studies reporting information suggest somewhat higher rates of engagement in further treatment following withdrawal managed with buprenorphine versus clonidine or lofexidine. The exception was Ziaaddini 2012, where rates of engagement in naltrexone treatment following withdrawal were similar between buprenorphine and clonidine groups. In contrast, the findings of Collins 2005, Marsch 2005, and Raistrick 2005 suggest higher rates of initiation of naltrexone treatment following withdrawal managed with buprenorphine versus an alpha2‐adrenergic agonist.
Different rates of dose reduction
Based on the two studies undertaken in an inpatient setting with short periods (five days or less) of treatment with buprenorphine, it appears that the rate of taper of the buprenorphine dose may have no significant effect on the intensity of withdrawal or the completion of treatment (Assadi 2004; Hopper 2005). However, the small number of studies and the differing nature of the inpatient settings (a hospital ward in Assadi 2004, and a residential treatment facility in Hopper 2005) make any findings highly uncertain (Table 3).
Five studies undertaken in outpatient settings compared buprenorphine regimens of longer duration (up to 56 days). Meta‐analysis of withdrawal scores was not possible, but qualitative comments made by the authors of the studies suggest that there is a more marked increase in withdrawal associated with more rapid rates of tapering of the buprenorphine dose. There were no data on the average duration of treatment, and most studies did not comment on adverse effects. It seems unlikely for there to be differences in the nature or incidence of adverse effects based on the rate of taper of the buprenorphine dose. There was considerable variability between these four studies in rates of completion of withdrawal treatment and abstinence at completion, with low quality evidence (Table 3). Two of the four studies were small, exploratory studies, reporting limited data (Amass 1994; Wang 1996). Ling 2009, Marsch 2016 and Sigmon 2013 were larger studies but produced differing results: Ling 2009 found that completion of withdrawal treatment was more likely with a more rapid taper of the dose of buprenorphine, while Sigmon 2013 and Marsch 2016 found that completion of withdrawal treatment was more likely with a slower taper of the dose of buprenorphine. Marsch 2016 involved adolescents, tapered buprenorphine over 28 or 56 days, and found that the frequency of clinic attendance also affected completion rates. In Sigmon 2013, the use of buprenorphine to manage withdrawal was the first phase of the study. In the second phase, study participants received naltrexone maintenance treatment (plus buprenorphine placebo). Participants in Ling 2009 were offered naltrexone treatment as aftercare, but it was not incorporated into the study protocol as a standard component of treatment. The findings in relation to abstinence at completion of the buprenorphine dosing regimen are similarly divergent.
These findings leave the question of whether buprenorphine dose should be tapered rapidly or slowly unanswered and introduce the possibility that it may depend on the context of withdrawal.
Overall completeness and applicability of evidence
Most (14 of 26) of the studies included in this review compared buprenorphine with clonidine (13 studies) or lofexidine (1 study), usually in an inpatient setting (10 studies), for managing withdrawal from heroin alone or heroin and methadone, in relatively short episodes of treatment (3 to 13 days). In this context, the finding that buprenorphine is more effective than clonidine in ameliorating the signs and symptoms of opioid withdrawal, prolonging the duration of treatment, and increasing the likelihood of completion of treatment, is reasonably robust.
Fewer studies (six) compared buprenorphine versus methadone in tapered doses, while the treatment settings were more diverse, and the scheduled duration of treatment tended to be longer (up to 21 days). Historically, methadone was widely used in withdrawal management with a short‐term goal of abstinence, particularly in outpatient settings, but currently the predominant use of methadone is in opioid substitution treatment where the immediate aims are retention in treatment, reduction of illicit opioid use and harms related to opioid use, and improvement of the quality of life, with abstinence a longer‐term goal (WHO 2009). The small number of studies comparing buprenorphine and methadone for managing opioid withdrawal is likely to be a reflection of the predominant use of methadone in opioid substitution treatment.
The small number of studies comparing different dose tapering schedules of buprenorphine, and the diverse findings, indicate that there is still much to learn about how to maximise the effectiveness of buprenorphine when it comes to managing opioid withdrawal in various settings and contexts. There is still very little information about managing withdrawal after a period of substitution treatment with buprenorphine, or indeed methadone, and postwithdrawal arrangements, such as transition to naltrexone, may affect preference for rapid or slow rate of dose taper.
Quality of the evidence
Buprenorphine versus tapered doses of methadone
Six studies involving 436 participants compared buprenorphine versus tapered doses of methadone. Meta‐analysis was possible for only two outcomes, mean days in treatment (2 studies) and number of participants completing withdrawal (5 studies). Study findings were reasonably consistent − we downgraded the quality of the evidence primarily due to the diverse settings in which the studies took place and the small numbers of participants. We assessed the quality of evidence on the duration of treatment as low, and on completion of withdrawal treatment as moderate (Table 1).
Buprenorphine versus alpha2‐adrenergic agonists
Fourteen studies investigated this comparison in 750 people receiving buprenorphine and 615 receiving an alpha2‐adrenergic agonist (103 with lofexidine). Meta‐analysis was possible for the intensity of withdrawal (peak withdrawal score and average withdrawal score across the treatment episode), duration of treatment, adverse effects (number of participants experiencing adverse effects, and number with treatment stopped due to adverse effects), and completion of treatment. All 14 studies contributed to at least one of the meta‐analyses. We assessed the quality of evidence as very low to moderate (Table 2) for the six meta‐analyses for the following reasons.
Analysis 2.1, mean peak withdrawal score, very low quality due to the risk of bias in the assessment of subjective outcomes, and small number of events.
Analysis 2.2, mean overall withdrawal score, moderate quality due to the risk of bias in the assessment of subjective outcomes.
Analysis 2.3, mean days in treatment, moderate quality due to different settings and heterogeneity in results.
Analysis 2.4, participants experiencing adverse effects, very low quality due to the risk of bias in the assessment of subjective outcomes, different settings, and small number of events.
Analysis 2.5, participants with treatment stopped due to adverse effects, low quality due to the small number of events.
Analysis 2.6, participants completing treatment, moderate quality due to heterogeneity in results.
Different rates of dose reduction
Seven studies involving 730 participants investigated this comparison. Meta‐analysis was possible only for outcomes of number of participants completing treatment, and number abstinent at completion, and we undertook separate meta‐analyses for inpatient (2 studies) and outpatient (5 studies) settings, as there were substantial differences in treatment regimens between the two. We assessed the quality of evidence as low or very low due to the small number of events, the small size of most of the studies, and heterogeneity in the results. As a result, we have little confidence in the findings for this comparison.
Potential biases in the review process
We did not detect any publication bias and believe that the search strategy was thorough and the study selection and data extraction processes, unbiased. We calculated the mean overall withdrawal score for some studies comparing buprenorphine with an alpha2‐adrenergic agonist using data reported in the studies, and this may have introduced some error.
Agreements and disagreements with other studies or reviews
We are not aware of any other systematic reviews addressing the effectiveness of buprenorphine for managing opioid withdrawal. The finding that buprenorphine has similar efficacy to methadone in terms of the capacity to ameliorate the signs and symptoms of opioid withdrawal is consistent with the findings of another Cochrane Review of the effectiveness of buprenorphine for opioid substitution treatment (Mattick 2014).
Authors' conclusions
Implications for practice.
Buprenorphine is more effective than clonidine or lofexidine in reducing the signs and symptoms of opioid withdrawal, retaining patients in withdrawal treatment, and in supporting the completion of withdrawal treatment. Buprenorphine may be associated with less dropout due to adverse effects. This finding holds for both inpatient and outpatient settings, particularly for withdrawal from heroin. The use of buprenorphine to manage withdrawal may also be associated with higher rates of engagement in postdetoxification treatment.
Buprenorphine and methadone in tapered doses appear to have similar efficacy in managing opioid withdrawal, but limited data leave open the possibility that the pattern and timeframe of withdrawal experienced may differ.
It is not possible to draw any conclusions from the available evidence on the relative effectiveness of different rates of tapering the buprenorphine dose or on factors that might determine a preference for rapid or slow rate of dose taper. It is possible that postwithdrawal arrangements, such as transition to relapse prevention treatment with naltrexone, may affect preference for the rate of taper of the buprenorphine dose during withdrawal.
Implications for research.
The studies included in this review that compared buprenorphine with reducing doses of methadone were predominantly undertaken in inpatient settings. One of the advantages of both buprenorphine and methadone for managing opioid withdrawal is the possibility of extending the episode into substitution treatment if the individual finds it too difficult to achieve abstinence. This makes buprenorphine and methadone particularly suited to outpatient settings, where there is a greater risk of illicit opioid use during treatment. However, the use of buprenorphine and methadone in this way would blur any distinction between withdrawal management and substitution treatment. Given that both buprenorphine and methadone have been shown to be effective for long‐term opioid substitution treatment, the value of research comparing the two medications in treatments with a short timeframe is questionable.
It is not possible, on the basis of the studies included in this review, to assess the effectiveness of buprenorphine for managing withdrawal from methadone or pharmaceutical opioids versus heroin. It is of interest that most of the studies comparing buprenorphine with clonidine or lofexidine involved participants withdrawing from heroin, whereas most of the studies comparing buprenorphine with methadone involved participants who were all withdrawing from other opiates. The transition from methadone to buprenorphine can be associated with precipitated withdrawal (Johnson 2003). This is generally managed by delaying commencement of buprenorphine until the emergence of withdrawal symptoms (Gowing 2014), but this approach adds some complexity to the use of buprenorphine for managing methadone withdrawal. Given this, more information on the relative effectiveness of buprenorphine for managing withdrawal from heroin compared to methadone and other opioid drugs would be of value.
A notable feature of the studies included in this review is the diversity of treatment regimens, with maximum doses ranging from 0.3 mg to 3.6 mg as intramuscular injections, and from 1.2 mg to 16 mg as sublingual tablets. Furthermore, other approaches have been and are being investigated. These include the use of a single, high dose (32 mg) of buprenorphine (Ang‐Lee 2006; Kutz 2002), depot preparations of buprenorphine (Sigmon 2004; Sobel 2004), and preparations for transdermal delivery of buprenorphine (Lanier 2007; Lanier 2008). These approaches may offer ways of providing a gradual taper of buprenorphine dose with minimal supervision and are of potential value in outpatient settings. However, controlled trials have yet to test their effectiveness for managing opioid withdrawal.
Many aspects of the treatment protocol, including doses, frequency, and duration of buprenorphine administration, require further research to determine the most effective way to use buprenorphine for managing opioid withdrawal. Researchers should assess effectiveness in terms of objective signs and subjective symptoms that are typical of the acute phase of withdrawal, the nature of residual signs and symptoms that are not effectively suppressed by buprenorphine, the occurrence of adverse effects, and the completion of withdrawal treatment, using objective criteria such as negative urine tests (particularly for outpatient withdrawal) and/or naloxone challenges. Studies should take into account the influence of variables such as the route of administration for heroin use (inhalation or intravenous), the nature and severity of dependence (including heroin versus methadone), the setting in which withdrawal occurs, and the linkage to further treatment (such as naltrexone maintenance).
What's new
| Date | Event | Description |
|---|---|---|
| 9 February 2017 | New citation required and conclusions have changed | New studies, new analyses, discussion and conclusions changed |
| 23 December 2016 | New search has been performed | Updated search. |
History
Protocol first published: Issue 2, 2000 Review first published: Issue 3, 2000
| Date | Event | Description |
|---|---|---|
| 22 April 2009 | New search has been performed | new assessment of included studies, conclusions changed |
| 19 November 2008 | New citation required and conclusions have changed | New search, new trials, conclusions changed |
| 25 March 2008 | Amended | Converted to new review format. |
| 3 January 2006 | New citation required and conclusions have changed | Substantive amendment |
Acknowledgements
Dr Rajat Ray and Associate Professor Rolley E Johnson provided additional information on studies included in the review (Nigam 1993 and Cheskin 1994, respectively).
Dr Zhao Chengzheng and Dr Liang Jianhui translated and assisted with assessment of two studies considered for this review that were published in Chinese (He 1999; Jia 2001). Dr Reinhard Bornemann assisted with the assessment of a study considered for this review that was published in German (Steinmann 2008).
Dr Hao Wei provided additional information on the nature of WeiniCom, a Chinese herbal preparation that was the comparison treatment for Hao 2000.
We thank Sylvia Minozzi for her very thorough quality assessment of this review.
Appendices
Appendix 1. CENTRAL search strategy
#1 (opiate or opioid or heroin or narcotic) near/2 (abuse or addiction or dependence):ti,ab,kw in Trials
#2 MeSH descriptor: [Opioid‐Related Disorders] explode all trees
#3 #1 or #2
#4 MeSH descriptor: [Substance Withdrawal Syndrome] explode all trees
#5 detoxification:ti,ab,kw in Trials
#6 #4 or #5
#7 #3 and #6
Appendix 2. MEDLINE search strategy via Ovid Online
exp Opioid‐Related Disorders/
((opiate$ or opioid$ or heroin$ of narcot$) adj2 (abus$ or depend$)).ti,ab
exp Substance Withdrawal Syndrome/
(detoxifi$ or desintoxi$ or disintoxi$ or disintossi$).ti,ab
1 or 2
3 or 4
5 and 6
exp clinical trial/ or exp comparative study/
random$.ti,ab
exp Double‐Blind Method/
(double adj2 blind).ti,ab
8 or 9 or 10 or 11
7 and 12
Limit 13 to humans
Appendix 3. EMBASE search strategy
#1 'opiate addiction'/exp
#2 'heroin dependence'/exp
#3 (opiate* or opioid* or heroin* or narcot*) NEAR/2 (abus* or depend*)
#4 'withdrawal syndrome'/exp
#5 detoxifi*.ab,ti or desintoxi*.ab,ti or disintoxi*.ab,ti or disintossi*.ab,ti
#6 'drug detoxification'/exp
#7 #1 or #2 or #3
#8 #4 or #5 or #6
#9 #7 and #8
#10 'clinical study'/exp
#11 random*.ab,ti
#12 'double blind procedure'
#13 double NEAR/1 blind
#14 #10 or #11 or #12 or #13
#15 #9 and #14 AND [humans]/lim
Appendix 4. PsycINFO search strategy via Ovid Online
exp drug dependency/
exp heroin addiction/
((opiate$ or opioid$ or heroin$ of narcot$) adj2 (abus$ or depend$)).ti,ab
exp drug withdrawal/ or exp detoxification/
(detoxifi$ or desintoxi$ or disintoxi$ or disintossi$).ti,ab
1 or 2 or 3
4 or 5
6 and 7
limit 8 to human
exp clinical trials/
random$.ti,ab
(double adj2 blind).ti,ab
10 or 11 or 12
9 and 13
Appendix 5. Web of Science search strategy
TS="opioid‐related disorders"
TS=opiate addiction
TS=opiate depend*
TS=heroin* depend*
TS=heroin* addict*
#5 or #4 or #3 or #2 or #!
TS="substance withdrawal syndrome"
TX=detox*
#8 or #7
#9 and #6
TS=clinical trial*
TS=random*
TS=double blind
#13 or #12 or #11
#14 and #10
Appendix 6. Criteria for risk of bias assessment
| Item | Judgement | Description |
| 1. Random sequence generation (selection bias) | Low risk | The investigators describe a random component in the sequence generation process such as: random number table; computer random number generator; coin tossing; shuffling cards or envelopes; throwing dice; drawing of lots; minimisation. |
| High risk | The investigators describe a non‐random component in the sequence generation process such as: odd or even date of birth; date (or day) of admission; hospital or clinic record number; alternation; judgement of the clinician; results of a laboratory test or a series of tests; availability of the intervention. | |
| Unclear risk | Insufficient information about the sequence generation process to permit judgement of low or high risk. | |
| 2. Allocation concealment (selection bias) | Low risk | Investigators enrolling participants could not foresee assignment because 1 of the following, or an equivalent method, was used to conceal allocation: central allocation (including telephone, web‐based, and pharmacy‐controlled, randomisation); sequentially numbered drug containers of identical appearance; sequentially numbered, opaque, sealed envelopes. |
| High risk | Investigators enrolling participants could possibly foresee assignments because 1 of the following method was used: open random allocation schedule (eg, a list of random numbers); assignment envelopes without appropriate safeguards (eg, if envelopes were unsealed or nonopaque or not sequentially numbered); alternation or rotation; date of birth; case record number; any other explicitly unconcealed procedure. | |
| Unclear risk | Insufficient information to permit judgement of low or high risk. This is usually the case if the method of concealment is not described or not described in sufficient detail to allow a definite judgement. | |
| 3. Blinding of participants, providers and outcome assessor (performance and detection bias) Objective outcomes |
Low risk | No blinding or incomplete blinding, but the review authors judge that the outcome is not likely to be influenced by lack of blinding. Blinding of participants, providers and outcome assessor and unlikely that the blinding could have been broken. |
| High risk | No blinding or incomplete blinding, and the outcome is likely to be influenced by lack of blinding; blinding of key study participants providers and outcome assessor attempted, but likely that the blinding could have been broken, and the outcome is likely to be influenced by lack of blinding. | |
| Unclear risk | Insufficient information to permit judgement of low or high risk. | |
| 4. Blinding of participants, providers and outcome assessor (performance and detection bias) Subjective outcomes |
Low risk | Blinding of participants, providers and outcome assessor and unlikely that the blinding could have been broken. |
| High risk | No blinding or incomplete blinding, and the outcome is likely to be influenced by lack of blinding. Blinding of key study participants, providers and outcome assessor attempted, but likely that the blinding could have been broken, and the outcome is likely to be influenced by lack of blinding. |
|
| Unclear risk | Insufficient information to permit judgement of low or high risk. | |
| 5. Incomplete outcome data (attrition bias) For all outcomes except retention in treatment or dropout |
Low risk | No missing outcome data. Reasons for missing outcome data unlikely to be related to true outcome (for survival data, censoring unlikely to be introducing bias). Missing outcome data balanced in numbers across intervention groups, with similar reasons for missing data across groups. For dichotomous outcome data, the proportion of missing outcomes compared with observed event risk not enough to have a clinically relevant impact on the intervention effect estimate. For continuous outcome data, plausible effect size (difference in means or standardized difference in means) among missing outcomes not enough to have a clinically relevant impact on observed effect size. Missing data have been imputed using appropriate methods. All randomised participants are reported/analysed in the group they were allocated to by randomisation irrespective of non‐compliance and co‐interventions (intention to treat). |
| High risk | Reason for missing outcome data likely to be related to true outcome, with either imbalance in numbers or reasons for missing data across intervention groups. For dichotomous outcome data, the proportion of missing outcomes compared with observed event risk enough to induce clinically relevant bias in intervention effect estimate. For continuous outcome data, plausible effect size (difference in means or standardised difference in means) among missing outcomes enough to induce clinically relevant bias in observed effect size. 'As‐treated' analysis done with substantial departure of the intervention received from that assigned at randomisation. |
|
| Unclear risk | Insufficient information to permit judgement of low or high risk (eg, number randomised not stated, no reasons for missing data provided; number of dropouts not reported for each group). | |
| 6 Selective reporting (reporting bias) | Low risk | The study protocol is available and all of the study's pre‐specified (primary and secondary) outcomes that are of interest in the review have been reported in the pre‐specified way. The study protocol is not available but it is clear that the published reports include all expected outcomes, including those that were pre‐specified (convincing text of this nature may be uncommon). |
| High risk | Not all of the study's pre‐specified primary outcomes have been reported. One or more primary outcomes is reported using measurements, analysis methods or subsets of the data (eg, subscales) that were not pre‐specified. One or more reported primary outcomes were not pre‐specified (unless clear justification for their reporting is provided, such as an unexpected adverse effect). One or more outcomes of interest in the review are reported incompletely so that they cannot be entered in a meta‐analysis. The study report fails to include results for a key outcome that would be expected to have been reported for such a study. |
|
| Unclear risk | Insufficient information to permit judgement of low or high risk. | |
| 9. Other bias | Low risk | Potential confounding factors identified but evenly distributed between groups. Study ceased early but with no indications of selection bias. Interventions delivered consistently. |
| High risk | Potential confounding factors unequally distributed between groups. Study ceased early with risk of selection bias. Differences in aspects of delivery of interventions. Mandatory treatment. |
|
| Unclear risk | Confounding possible but not able to be assessed. Study ceased early and unable to determine possible bias. Unclear if delivery of interventions was equivalent. |
Data and analyses
Comparison 1. Buprenorphine versus methadone.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mean days in treatment | 2 | 82 | Mean Difference (IV, Random, 95% CI) | 1.30 [‐8.11, 10.72] |
| 2 Completion of withdrawal treatment | 5 | 457 | Risk Ratio (M‐H, Random, 95% CI) | 1.04 [0.91, 1.20] |
Comparison 2. Buprenorphine versus clonidine.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Mean peak withdrawal score | 6 | 521 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.43 [‐0.74, ‐0.13] |
| 2 Mean overall withdrawal score | 7 | 902 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.43 [‐0.58, ‐0.28] |
| 3 Mean days in treatment | 4 | 558 | Std. Mean Difference (IV, Random, 95% CI) | 0.92 [0.57, 1.27] |
| 3.1 Inpatient setting | 3 | 213 | Std. Mean Difference (IV, Random, 95% CI) | 1.00 [0.33, 1.67] |
| 3.2 Outpatient setting | 2 | 345 | Std. Mean Difference (IV, Random, 95% CI) | 0.82 [0.57, 1.06] |
| 4 Number experiencing adverse effects | 3 | 493 | Risk Ratio (M‐H, Random, 95% CI) | 0.93 [0.70, 1.26] |
| 4.1 Inpatient | 2 | 148 | Risk Ratio (M‐H, Random, 95% CI) | 0.41 [0.12, 1.36] |
| 4.2 Outpatient | 2 | 345 | Risk Ratio (M‐H, Random, 95% CI) | 1.02 [0.66, 1.58] |
| 5 Number with treatment stopped due to adverse effects | 3 | 134 | Risk Ratio (M‐H, Random, 95% CI) | 0.20 [0.04, 1.15] |
| 5.1 Inpatient | 3 | 134 | Risk Ratio (M‐H, Random, 95% CI) | 0.20 [0.04, 1.15] |
| 5.2 Outpatient | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 6 Number completing withdrawal treatment | 11 | 1264 | Risk Ratio (M‐H, Random, 95% CI) | 1.59 [1.23, 2.06] |
| 6.1 Inpatient | 6 | 539 | Risk Ratio (M‐H, Random, 95% CI) | 1.74 [1.05, 2.89] |
| 6.2 Outpatient | 6 | 725 | Risk Ratio (M‐H, Random, 95% CI) | 1.45 [1.12, 1.88] |
Comparison 3. Rapid versus slow dose taper.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Completion of withdrawal treatment | 6 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.1 Inpatient | 2 | 60 | Risk Ratio (M‐H, Random, 95% CI) | 1.0 [0.84, 1.18] |
| 1.2 Outpatient | 4 | 647 | Risk Ratio (M‐H, Random, 95% CI) | 0.86 [0.44, 1.70] |
| 2 Number abstinent at completion of dose taper | 5 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 2.1 Inpatient | 1 | 40 | Risk Ratio (M‐H, Random, 95% CI) | 1.0 [0.81, 1.23] |
| 2.2 Outpatient | 4 | 610 | Risk Ratio (M‐H, Random, 95% CI) | 0.94 [0.39, 2.24] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Amass 1994.
| Methods | Randomised, double‐blind, placebo‐controlled study | |
| Participants | Setting: outpatient clinic, USA Participants: N = 8, opioid dependent by DSM‐III‐R, using unspecified opioid drugs Group sizes: group 1: N = 3; group 2: N = 5 Groups similar in withdrawal symptoms and positive urine samples during maintenance phase Average age 39.4 years 87.5% male Average duration opioid use 18.1 years, 87.5% reported i.v. use. One required benzodiazepine detoxification prior to study |
|
| Interventions | Buprenorphine solution (or placebo) administered sublingually, plus placebo pills during dose taper Buprenorphine increased to 8 mg/d over first three days, maintained for 28 days, then tapered. Group 1: 36 days (1 mg/4 days then 0.5 mg in last 4 days) Group 2: 12 days (50% every 4 days) Daily clinic attendance Both groups received behavioural counselling (2‐3 sessions of 1 h each). Vouchers for recreational items given for negative urine samples |
|
| Outcomes | Change in withdrawal scores per day, % opioid‐negative urine samples, number in treatment for full 9 weeks, % continuously abstinent by week | |
| Notes | Withdrawal rated by participants (20 signs and symptoms in prior 24 h, rated 0 (none) to 9 (severe), max score 180) and observers (8 signs, rated 0 (not at all) to 3 (severe), max score 24) Observed urine and breath alcohol samples 3 times a week. Missed urine samples considered positive Source of funding for trial not reported; report preparation supported by government (NIDA) grants |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "subjects were assigned randomly . . . by drawing lots" |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment not reported |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | Low risk | Double‐blind stated, with use of placebos. Quote: "Nursing staff who were blind to the treatment conditions completed an observer rating scale" |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | Double‐blind stated, with use of placebos, and these outcomes unlikely to be affected by awareness of treatment allocation |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "Missed (urine) samples were considered opioid positive for the purposes of data analyses." "A repeated measures analysis of variance (ANOVA) was performed to examine subject‐ and observer‐rated withdrawal, and mean percentage opioid‐negative urine samples across the treatment groups" Comment: this approach less susceptible to bias due to missing data |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Assadi 2004.
| Methods | Randomised double‐blind, placebo‐controlled trial. Concurrent dependence on alcohol exclusion criterion | |
| Participants | Setting: inpatient treatment, addiction ward of psychiatric hospital, Tehran, Iran Participants: N = 40, opioid dependent by DSM‐IV, 68% using heroin, 32% opium Group sizes: N = 20 in each group Baseline characteristics of groups similar Average age 31.5 39/40 male Average duration opioid use 9 years; 50% using by injection or multiple routes; 30% employed, 55% married |
|
| Interventions | Buprenorphine, i.m. with: Group 1: 4 × 1.5 mg between 12 pm and 6 pm day 1, 4 × 1.5 mg between 6 am and 12 pm day 2 Group 2: 2 × 1.5 mg day 1, tapered to 2 × 0.3 mg day 5 Adjunct medications (indomethacin, trazodone, chlorpromazine, hyoscine) as required. Relapse prevention treatment using naltrexone as aftercare |
|
| Outcomes | Withdrawal scores, days in treatment, number completing treatment | |
| Notes | Withdrawal assessed once per day by participants (SOWS) and observer (OOWS) Study conducted without financial support |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomly assigned . . . using a computer‐generated list of random numbers" |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment not reported |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | Low risk | Patients and staff with patient contact, and person performing clinical research assessments all blind to group allocation. Placebo used |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | Patients and staff with patient contact, and person performing clinical research assessments all blind to group allocation. Placebo used |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 10% dropout in course of study. Missing data replaced by carrying last observation forward |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Bickel 1988.
| Methods | Randomised, double‐blind, placebo‐controlled trial | |
| Participants | Setting: outpatient clinic, USA Participants: N = 45, opioid dependent, using opiates other than methadone, seeking outpatient detoxification, eligible for methadone maintenance treatment (evidence of recent injecting use part of eligibility criteria) Group sizes: group 1: N = 22; group 2: N = 23, but most analyses based on N = 17 from group 1 and N = 14 from group 2who remained in treatment at least 6 weeks Groups similar on demographics Average age 30 years All male Duration of heroin use, mean ± SD: group 1 6.7 ± 1.9 years; group 2: 9.2 ± 6.1 years |
|
| Interventions | Treatment regimens involved 3 weeks stabilisation, 4 weeks dose reduction, 6 weeks placebo dosing with: Group 1: buprenorphine, sublingual solution, 2 mg/d or Group 2: methadone, 30 mg/d, oral Daily clinic attendance All had access to supportive counselling. Scheduled 90‐day treatment |
|
| Outcomes | Mean duration in treatment, number in treatment for 6 weeks or more, graphs of retention, mean withdrawal scores and opiate positive or missing urine to week 6 | |
| Notes | Withdrawal rated by subjects 3 times a week (2 scales, each 20 symptoms rated 0‐9) Urine samples collected according to random schedule Study supported by government grants and pharmaceutical company |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were randomised, stratifying for race"; method of sequence generation not specified |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment not reported |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | Low risk | Quote: "Neither the subjects nor the nurses had information about which medication was active nor did they have any information about the dose‐reduction schedule." |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | Quote: "Neither the subjects nor the nurses had information about which medication was active nor did they have any information about the dose‐reduction schedule." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Rapid dropout from week 6, towards the end of the dose taper of the two medications, but dropout similar in two groups. Retention main outcome reported after week 6 when dropout > 30% |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Cheskin 1994.
| Methods | Randomised, double‐blind, placebo‐controlled trial | |
| Participants | Setting: inpatient, closed research ward, USA Participants: N = 25 heroin users, with evidence of recent injecting use Group sizes: group 1: N = 12; group 2: N = 13. Analysis primarily on basis of 18 who completed treatment Group similar on demographic characteristics Average age 35 years 44% male Average duration heroin use 11.5 years |
|
| Interventions | Morphine used to attenuate withdrawal on admission. Subsequent treatment with: Group 1: buprenorphine, sublingual solution, maximum of 2 mg/dose, total 17 mg over 3 days Group 2: clonidine, maximum 0.3 mg/dose, total 2.7 mg over 5 days Individual counselling twice weekly Total study period 18 days. Placebo administered after completion of active medication phase |
|
| Outcomes | Graphs of mean 'urge' and 'need' for an opioid, mean withdrawal score, number completing 10 days of treatment, reasons for cessation | |
| Notes | Visual analogue scales for rating 'urge' and 'need' for an opioid and subjective response to medication Addiction Research Centre scales assessed opioid‐like euphoria, apathetic sedation and dysphoria Daily urine screening Study funded by US government research programme |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "patients were randomly assigned" with stratification based on response to naloxone challenge test. Method of sequence generation not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment not reported |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | Low risk | Quote: "double‐blind, double‐dummy . . . design"; extended treatment period to maintain blind |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | Quote: "double‐blind, double‐dummy . . . design" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Analysis of withdrawal based on participants who completed the study. The significant difference in the first 3 days of treatment would be expected to be increased, not decreased, if dropouts had been included. |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Collins 2005.
| Methods | Randomised controlled, open‐label study | |
| Participants | Setting: clinical research centre, New York, USA. Inpatient care for 72 h of withdrawal, outpatient for 12 weeks naltrexone maintenance treatment Participants: N = 106, treatment seeking, heroin dependent by DSM‐IV Group sizes: group 1: N = 35; group 2: N = 37; group 3: N = 34 Groups similar on demographic and clinical characteristics Average age 36 72% male 40% using by injection; 36% currently married or cohabiting; 56% currently employed. Major psychiatric illness, active medical illness, dependence on alcohol or drugs other than heroin were exclusion criteria. |
|
| Interventions | Group 1 (excluded from review): nalmefene 4 mg i.v. over 30 min, naltrexone 50 mg via nasogastric tube, under propofol anaesthesia (4‐6 hours). Various adjunct medications, including octreotide Group 2: buprenorphine (sublingual, preparation not specified), 8 mg (single dose) day 1, naltrexone 12.5 mg afternoon of day 2, 25 mg 12 hours later, then 50 mg/d Group 3: clonidine, max 1.2 mg/d, discharged day 3, naltrexone 12.5 mg day 7, 25 mg day 8, then 50 mg/d. Clonidine and various adjunct medications available to all groups. Naltrexone maintenance and relapse prevention psychotherapy as aftercare |
|
| Outcomes | Graphs of withdrawal severity,.mean weeks in treatment. Number of participants completing inpatient phase, receiving at least one dose of naltrexone, receiving full 50 mg dose of naltrexone. Number retained in treatment over 12 weeks. Number retained 12 weeks who provided 2 or less opiate positive urine samples. Number experiencing serious adverse events | |
| Notes | Withdrawal assessed by SOWS, OOWS, and Clinical Institute Narcotic Assessment, 4 times a day during inpatient phase Study funded entirely by grants from US National Institutes of Health |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: ". . .using random, computer‐generated assignments, with stratification by sex. . . . In addition, the Berger‐Exner test was used to confirm that no selection bias in enrolment occurred." |
| Allocation concealment (selection bias) | Low risk | Quote: "All staff remained unaware of the randomisation sequence" |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | High risk | Patients were not blinded to treatment − sham anaesthesia not ethical. Unclear whether observers were blinded to treatment. |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | These outcomes unlikely to be affected by knowledge of treatment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up similar in three groups and main outcomes reported not sensitive to missing data |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Unclear risk | Enrollment stopped at 106 participants (target 150) "because actual differences in withdrawal severity scores and treatment retention were smaller than anticipated, leading to an impractically large recalculated sample size" Comment: it seems unlikely that the stopping of enrolment resulted in bias |
Hopper 2005.
| Methods | Randomised controlled (open‐label) trial | |
| Participants | Setting: residential therapeutic community, USA Participants: N = 20, heroin dependent by DSM‐IV Group sizes: N = 10 in each group Groups similar on demographics and drug use Average age 47 years 65% male 35% using heroin by injection (rest using nasally), 60% also cocaine dependent; 15% married, 20% employed in prior 30 days |
|
| Interventions | Buprenorphine/naloxone sublingual tablet, two dose regimens: Group 1: 8 mg plus 24 mg after 30 min on day 1 Group 2: 8 mg day 1, 16 mg day 2, 8 mg day 3 Adjunct medications available as needed Detoxification and monitoring over 7 days; follow‐up evaluations on days 14‐17 |
|
| Outcomes | Number completing 7 days of detoxification programme, number completing follow‐up evaluation, mean daily withdrawal score, use of adjunct medication | |
| Notes | Withdrawal assessed daily by Clinical Opiate Withdrawal Scale (COWS) Urine testing 4 times in 7 days of detoxification Source of funding government grants |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "patients were randomly assigned in an open‐label fashion"; method of sequence generation not reported. |
| Allocation concealment (selection bias) | High risk | Quote: "patients were randomly assigned in an open‐label fashion". |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | Unclear risk | Staff who assessed withdrawal symptoms daily were not aware of group assignments, but participants were probably aware of treatment allocation. |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | Treating staff were not aware of group assignments and these outcomes considered unlikely to be affected by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No significant difference in dropouts between groups |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | High risk | All participants were resident in a therapeutic community. This may have resulted in selection of a highly motivated group who would have done well whatever the treatment. |
Hussain 2015.
| Methods | Randomised controlled, open‐label trial | |
| Participants | Setting: inpatient treatment facility, Srinagar, India Participants: N = 58, opioid dependent by DSM‐IV, treatment seeking. Use of substances of abuse other than opioids was an exclusion criterion Group sizes: N = 29 in each group Groups similar on demographic characteristics Average age 27 years Sex not reported (probably all male) Average 6 years of abuse; 69% employed, 26% married |
|
| Interventions | Group 1: buprenorphine/naloxone, sublingual, 4.0/1.0 mg on day 1, 8.0/2.0 mg/d on days 2‐4, 4.0/1.0 mg on days days 5‐7, 2.0/0.5 mg on days 8‐10 Group 2: clonidine, oral, 0.1 mg day 1, increasing to 0.2 mg on days 2‐4, tapered from day 5, ceased on day 10 Both groups received ancillary medications on demand |
|
| Outcomes | Average daily withdrawal score, average daily craving score, participants experiencing adverse effects, number completing study | |
| Notes | Withdrawal assessed twice daily with Clinical Opiate Withdrawal Scale (COWS). Craving assessed with visual analogue scale (VAS) Source of funding not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "participants were randomised into two groups using computer generated random numbers". |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not reported |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | High risk | Quote: "open labelled study and blinding was not done" |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | These outcomes are unlikely to be affected by knowledge of the treatment group. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Low rate of attrition, and same in both groups |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Janiri 1994.
| Methods | Randomised double‐blind, placebo‐controlled trial | |
| Participants | Setting: inpatient, hospital drug dependence unit, Italy Participants: N = 39 from MMT requiring detoxification Group sizes: N = 13 in each group. Analysis based on 32/39 who completed treatment Groups stated to not differ on psychosocial and drug history data Average age 26 years 59% male Average duration opioid dependence 7.5 years, methadone maintenance 3.4 years; 56% using methadone only, 43% using methadone and heroin; polydrug use an exclusion criterion; 41% in stable job |
|
| Interventions | All stabilised on methadone, mean 23.7mg/d, tapered to 10 mg/d before study commenced Detoxification managed with: Group 1: buprenorphine intramuscularly, 0.9 mg days 1 and 2, 0.45 mg day 3, 0.15 mg day 4 Group 2: Clonidine, 0.3 to 0.9 mg/d intramuscularly, 6 days or Group 3 (excluded from review): Lefetamine, 60‐240 mg/d intramuscularly, 6 days. This group excluded from this review. Clonidine and lefetamine groups given 5 mg methadone on days 1 and 2; oral and i.m. placebos used to maintain blind, no other drugs allowed. |
|
| Outcomes | Graphs of total, objective, subjective and psychological withdrawal scores, adjusted for baseline scores Number completing treatment | |
| Notes | Withdrawal assessed by scale of Bruno and Ferracuti (12 objective, 10 subjective, 5 psychological items, each rated 0‐5). Urine screening used Source of funding not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "patients were assigned randomly to one of three groups" Comment: Method of sequence generation not reported but groups similar at baseline |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not reported |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | Low risk | Quote: withdrawal "was rated by a trained psychiatrist, who was blind to study conditions". |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | Double‐blind stated and these outcomes unlikely to be affected by knowledge of intervention |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "The 7 patients who dropped out were equally distributed among the three groups." |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Ling 2005.
| Methods | Randomised controlled open‐label trials − separate trials in outpatient and inpatient settings | |
| Participants | Setting: inpatient and outpatient, in various community treatment programmes in USA Participants: N = 113 (inpatient) and N = 231 (outpatient), heroin dependent by DSM‐IV Group sizes: group 1: N = 77; group 2: N = 36 for inpatient study, group 1: N = 157; group 2: N = 74 for outpatient study Groups similar on demographics, drug use history, except cannabis use with group 1 13.9%; group 2 2.6% meeting criteria for cannabis dependence Average age 36 (inpatient) and 39 (outpatient) 68% male Duration of heroin use more than 9 years for outpatient study, less than 7 years for inpatient study. 65% in buprenorphine groups injecting users, 70%‐94% across all groups worked full‐ or part‐time. Those codependent on other drugs not excluded |
|
| Interventions | Group 1: buprenorphine/naloxone sublingual tablet, first dose when in mild withdrawal, 4 mg day 1, with further 4 mg 1‐2 hours later, increasing to 16 mg day 3, tapering to 2 mg day 12/13 Group 2: clonidine, 0.05‐0.1 mg every 4‐6 hours day 1, plus transdermal patch from day 2, patch only from day 3, discontinued by day 13 Ancillary medications and counselling available. Medications administered daily. Scheduled duration 13 days |
|
| Outcomes | Success, defined as retention for entire study duration and opioid‐free urine on last day. Summary withdrawal, calculated as average of COWS scores across available observations. Average craving score. | |
| Notes | Observers completed COWS (11 signs) daily. Participants completed Adjective Rating Scale for Withdrawal (16 items). Craving assessed by Visual Analogue Scale. Daily urine samples. Source of funding: series of grants from US government (NIDA) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "patients were assigned randomly to bup‐nx or clonidine conditions using a 2:1 ratio in favour of buprenorphine" Comment: based on contacts with the research group, we consider it likely that the method of sequence generation was adequate. |
| Allocation concealment (selection bias) | Low risk | Method of concealment not reported, but based on our knowledge of the research group, we consider it likely that concealment of allocation would have been achieved. |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | High risk | No blinding |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | No blinding, but these outcomes unlikely to be affected by knowledge of group allocation |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Significantly more dropouts from clonidine groups, but method of analysis (ANCOVA) adjusted for missing data |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Unclear risk | Quote: "the NIDA Data and Safety Monitoring Board (DSMB) recommended that the study be halted prior to collecting the full complement of subjects for the following reasons: the large enrolment status, the consistency of findings overwhelmingly favourable toward the bup‐nx condition and the consideration that additional participant enrolment would not yield meaningful new information. Comment: while early termination of studies is associated with some risk of bias, the extent of recruitment achieved is likely to have minimised this risk |
Ling 2009.
| Methods | Randomised controlled, open‐label study. Randomisation stratified by buprenorphine dose at end of stabilisation (8, 16 or 24 mg) | |
| Participants | Setting: outpatient, 11 treatment programmes, USA Participants: N = 516, dependent on opioids other than methadone Group sizes: group 1: N = 255; group 2: N = 261 No significant differences between groups in demographics or drug use at baseline Average age 36 years 33% female About 8 years of lifetime heroin use; exclusion criteria included positive urine test for methadone or benzodiazepine, and dependence on alcohol or any drug other than opioids; 35% unemployed in month prior to baseline |
|
| Interventions | Buprenorphine/naloxone sublingual tablet (Suboxone), 4‐week stabilisation with flexible dosing for 3 weeks to establish optimal dose, fixed at that dose for week 4, then tapered: Group 1: over 7 days Group 2: over 28 days Psychosocial services as usual for both groups. Once weekly clinic attendance Maximum 5 months covering screening, induction/stabilisation, taper and follow‐up |
|
| Outcomes | Mean withdrawal and craving scores at assessment time points, number in treatment at end of taper, number with opioid‐free urine samples at end of taper and at follow‐up | |
| Notes | Participants rated withdrawal with Adjective Rating Scale (16 items each rated 0‐9). Clinicians rated withdrawal with COWS (range 0‐48). Visual analogue scale for overall withdrawal, craving and medication effectiveness. Weekly data collection to week 8. Incentive payments for each 'milestone' visit Source of funding: series of grants from US government (NIDA) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "participants were assigned randomly. . . stratified by maintenance dose at the end of the stabilization phase". Comment: This sort of randomisation would be expected to be computerised. |
| Allocation concealment (selection bias) | High risk | Quote: "Each treatment site had three sets of randomisation cards (one for each stabilisation dose) prepared in advance. Based on stabilisation dose, the top card in the appropriate stack was selected for the participant." Comment: Concealment of allocation was unlikely meaning the sequence could be easily manipulated |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | High risk | Study conducted open label |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | Study open label but these outcomes unlikely to be affected by awareness of treatment allocation |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No significant differences in baseline characteristics of those who remained in the study to the end of the taper and those who dropped out |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Lintzeris 2002.
| Methods | Randomised controlled, open‐label study | |
| Participants | Setting: outpatient, specialist clinic, Australia Participants: N = 114 heroin users, dependent by DSM‐IV Group sizes: group 1: N = 58; group 2: N = 56 Groups similar on demographics and drug use Average age 30 years 65% male About 7 years since first regular heroin use, 90% injecting users; 39% employed full‐ or part‐time, 25% married/de facto. Some polydrug use, but significant other drug dependence an exclusion criterion |
|
| Interventions | Group 1: buprenorphine, sublingual tablet, supervised single daily dose around 6 mg/d, adjusted to symptoms, ceased day 5 Group 2: clonidine 0.1‐0.15 mg 4 times a day as required plus symptomatic medications Daily clinic attendance for medication Both groups received supportive counselling during withdrawal. Naltrexone, substitution treatment or counselling available as aftercare. Scheduled duration 8 days |
|
| Outcomes | Withdrawal score, treatment retention, time in treatment, days of heroin use, adverse effects, engagement in postwithdrawal treatment | |
| Notes | Withdrawal assessed by SOWS and OOWS (Handelsman) Urine screening used Source of funding: government, buprenorphine provided by manufacturer |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "a computerized schedule was developed . . . using the technique of dynamic balanced randomisation . . . balancing treatment allocation within each site and across the study as a whole." |
| Allocation concealment (selection bias) | Low risk | Quote: "randomisation was conducted by an independent organization" |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | High risk | Quote: "patients, treatment providers and outcome assessors (were) aware of group allocation." |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | Quote: "patients, treatment providers and outcome assessors (were) aware of group allocation" but these outcomes unlikely to be affected by knowledge of group allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Difference in dropout cannot account for significant differences between buprenorphine and clonidine treatment |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Marsch 2005.
| Methods | Randomised double‐blind, placebo‐controlled trial. Participants stratified by sex and past‐month route of opiate use (injection or intranasal) | |
| Participants | Setting: outpatient, university‐based research clinic, USA Participants: N = 36 adolescents (aged 13‐18 years), opiate dependent by DSM‐IV Group sizes: N = 18 in each group Groups similar on demographics and clinical criteria at baseline Average age 17 39% male Average age 15 years at first opiate use; 53% primarily heroin users, 36% injecting users |
|
| Interventions | Group 1: buprenorphine, sublingual tablets, commenced at 6 or 8 mg/day according to body weight and opiate use, decreased 2 mg every 7 days Group 2: clonidine, 0.1 mg transdermal patches, 1 day 1, 2 days 2‐6, with optional 3rd days 4‐6, tapered after 7 days. Scheduled treatment duration 28 days Behavioural counselling 3 times a week and incentives contingent on opiate abstinence. All offered naltrexone as aftercare |
|
| Outcomes | Number completing scheduled treatment. % urine tests opioid negative. Number initiating treatment with naltrexone | |
| Notes | Withdrawal not assessed. Urine screening used Funding support from government (NIDA) and university grants |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Participants were randomly assigned"; method not reported. |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment not reported |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | Low risk | Quote: "double‐blind, double‐dummy design" |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | Quote: "double‐blind, double‐dummy design" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Retention is major outcome. Analyses of secondary outcomes based on data from first week when retention still high in both groups |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Marsch 2016.
| Methods | Randomised controlled, double‐blind trial | |
| Participants | Setting: Outpatient, in hospital‐based research clinics in New York City, USA Participants: N=53 adolescents (age 16‐24), opioid‐dependent by DSM‐IV Group sizes: (1) N=28 (2) N=25 Groups similar, except more participants in group (1) were nicotine dependent. Average age 20.5 years 58% male 58% using iv, 81% primary heroin users. Pregnancy, active significant psychiatric disorder, serious medical condition were exclusion criteria. |
|
| Interventions | Commenced on sublingual tablets containing buprenorphine only, initial dose 6 or 8 mg based on bodyweight and drug use, additional 2, 4, 6 or 8 mg if withdrawal symptoms after 1 hour. Switched to sublingual buprenorphine/naloxone when stable (after 2 days). Taper adjusted to starting dose to cease after (1) 28 or (2) 56 days. Initially daily clinic attendance required; after 20 enrolments participants able to earn take home doses and clinic attendance required 2‐3 times weekly. All received behavioural counselling and opioid abstinence incentives as adjunct therapies. |
|
| Outcomes | Abstinence as percentage of scheduled urine tests documented as negative (missed urine samples assumed to be positive) Retention as number of days with attendance at scheduled visits. |
|
| Notes | Urine samples at intake and then randomly at scheduled visits. Source of funding: grant from US government (NIDA); study medication provided by manufacturer. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "...participants were assigned randomly" "A minimum allocation procedure was used [to balance] groups on participant characteristics likely to influence treatment outcomes. |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation concealment not reported. |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | Low risk | Double‐blind stated. Quote: "...each participant received the same number of identical‐appearing tablets ... throughout the trial". No subjective outcomes reported. |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | Double‐blind stated. Quote: "...each participant received the same number of identical‐appearing tablets ... throughout the trial". |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Nigam 1993.
| Methods | Randomised controlled trial | |
| Participants | Setting: inpatient, hospital, New Delhi, India Participants: N = 72, opioid dependent by DSM‐III‐R. Published analysis based on 44 (of 72 recruited) who completed treatment. Additional information provided by authors Group sizes: group 1: N = 34; group 2: N = 38 Groups similar on demographics, drug use history, withdrawal score at entry Average age 29 All males Duration heroin use 4‐5 years, 90% heroin users (1.5 g/day), rest opium users; no intravenous users; polydrug use an exclusion criterion; 64% married, 92% employed |
|
| Interventions | Group 1: buprenorphine, initial dose 0.6 mg/d, maximum 1.2 mg/d, sublingual tablet, in 3 divided doses Group 2: clonidine, initial dose 0.3 mg/d, maximum 0.9 mg/d, oral, in 3 divided doses. Nitrazepam as adjunct medication. Scheduled duration 10 days |
|
| Outcomes | Mean daily withdrawal scores. Side effects. Completion rates from personal communication | |
| Notes | Withdrawal assessed daily using Subjective and Objective Opiate Withdrawal Scales (Handelsman). Urine screening used only for some participants Source of funding not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Authors advised that subjects were randomly assigned but did not specify the method of sequence generation. |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment not reported |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | High risk | Authors advised study not double‐blind |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | These outcomes unlikely to be affected by knowledge of group allocation |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropout similar in two groups; withdrawal score comparisons based on those who completed treatment |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
O'Connor 1997.
| Methods | Randomised, double‐blind clinical trial | |
| Participants | Setting: outpatient, primary care clinic, USA Participants: N = 162, heroin dependent. Group sizes: group 1: N = 55; group 2: N = 54; group 3: N = 53 Groups similar on sociodemographic and clinical characteristics Age range 18 to 50 years (average not reported) 71% male Average duration of heroin use > 7 years, polydrug users not excluded; 35% employed; 62% married |
|
| Interventions | Group 1: clonidine 0.1‐0.2 mg every 4 h as needed days 1‐7. 50 mg naltrexone day 8 Group 2 (excluded from review): clonidine as in group 1, 12.5 mg naltrexone day 1, increasing to 50 mg day 3 Group 3: buprenorphine 3 mg sublingually (preparation not specified) days 1‐3, then clonidine as in group 1, 25 mg naltrexone day 4, 50 mg day 5 Oxazepam, ibuprofen, ketorolac, prochlorperazine as adjunct medication Daily clinic attendance except weekends. Participants referred for further treatment following trial |
|
| Outcomes | Mean overall and peak withdrawal scores. Number retained in treatment for 8 days. Number achieving 50 mg maintenance dose naltrexone | |
| Notes | Withdrawal assessment primarily subjective symptoms Funding support: government grant (NIDA) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "participants were randomly assigned"; method of sequence generation not reported. |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment not reported |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | Unclear risk | Quote: "staff and patients were blinded to the protocols". Comment: double‐blind possibly compromised by differential symptoms |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | Quote: "staff and patients were blinded to the protocols" Comment: double‐blind possibly compromised by differential symptoms, but these outcomes unlikely to be affected by knowledge of treatment allocation |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "Retention did not differ significantly among the groups" |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | Outcome definition adjusted for differences in medication duration |
Oreskovich 2005.
| Methods | Double‐blind, double‐dummy, randomised controlled trial | |
| Participants | Setting: inpatient detoxification facility affiliated with University of Washington, USA Participants: N = 30 heroin dependent by DSM‐IV, in moderate withdrawal at time of randomisation. One participant (clonidine group) discontinued due to protocol violation − main analysis on N = 29, complete demographic data on N = 28 Group sizes: group 1: N = 10; group 2: N = 10; group 3: N = 9 Groups similar on main demographic and clinical characteristics Average age 36 63% male Average duration of heroin use 6.5 to 10.3 years; polydrug users excluded if medically supervised withdrawal required for other drug dependence; unemployed group 1 10%, group 2 50%, group 3 25% |
|
| Interventions | Buprenorphine, sublingual tablet (Subutex), or placebo in two dose regimens: Group 1: high dose: 8‐8‐8‐4‐2 mg/d or Group 2: low dose: 2‐4‐8‐4‐2 mg/d on days 1‐5 Compared with group 3:clonidine, oral, 0.2‐0.3 mg four times a day for 5 days Ancillary medications available No specific behavioural therapies during withdrawal, but participants assessed for placement in outpatient treatment after completion of the study |
|
| Outcomes | Number achieving suppression of withdrawal; mean withdrawal score; chlordiazepoxide use; mean hours to discharge; doses of medication (or placebo) withheld due to hypotension | |
| Notes | Withdrawal assessed by COWS, Adjective Rating Scale for Withdrawal, and Visual Analogue Craving Scale Funding support from University of Washington. Buprenorphine and placebo provided by pharmaceutical company |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomly assigned . . . by a computerised random numbers generator" |
| Allocation concealment (selection bias) | Low risk | Quote: "(allocation) by the offsite research pharmacist" |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | Low risk | Double‐blind, double‐dummy stated |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | Double‐blind, double‐dummy stated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Statistical methods used to adjust for missing data |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Petitjean 2002.
| Methods | Randomised, controlled (open‐label) study | |
| Participants | Setting: inpatient, specialist unit, Switzerland Participants: N = 37, opioid dependent by ICD‐10, using heroin or methadone Group sizes: group 1: N = 19; group 2: N = 18 Groups similar on sociodemographics Average age 32 years 78% male Those with concurrent alcohol or benzodiazepine dependence were detoxified before entering study |
|
| Interventions | Medication tailored to declared amount of heroin use and withdrawal signs: Group 1: buprenorphine, sublingual tablets, 8 mg/70 kg in 2 daily doses to max 16 mg/70 kg, reduced in 2 mg steps over average 12 days Group 2: oral methadone, 40 mg/70kg to max 60 mg/70kg, reduced in 10 mg steps to 30 mg/70kg, then 5 mg steps, over total 15 days on average |
|
| Outcomes | Withdrawal severity, length of stay, completion rate | |
| Notes | Withdrawal assessed by Short Opiate Withdrawal Scale. Urine testing used Source of funding not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were randomly assigned". Insufficient information reported on characteristics of groups to form a view on adequacy of sequence generation |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment not reported |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | High risk | No blinding |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | These outcomes unlikely to be affected by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropout evenly distributed between groups |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Ponizovsky 2006.
| Methods | Randomised, open‐label, controlled trial | |
| Participants | Setting: inpatient, 2 separate specialist units, Jerusalem, Israel Participants: N = 200 heroin dependent by ICD‐10 Group sizes: N = 100 in each group Detailed demographics reported only for those who completed detoxification, but authors stated there were no significant differences in sociodemographic characteristics between completers and non‐completers within each group Majority (> 60%) in each group aged between 25 and 44 years 86% male Dependence on benzodiazepines or alcohol an exclusion criterion. 19% married, 88% unemployed |
|
| Interventions | Group 1: buprenorphine (Subutex) 10 mg day 1 with extra if needed, tapered to finish day 10 Group 2: clonidine, 0.6 mg/d in divided doses, tapered from day 5 10 days detoxification followed by relapse prevention programme |
|
| Outcomes | Number completing treatment. Mean adverse effects score. Adverse effects, well‐being assessed only for those who completed 10‐day detoxification | |
| Notes | Withdrawal severity not reported Study supported in part by pharmaceutical company, and by government |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "we used a random number generator" |
| Allocation concealment (selection bias) | Unclear risk | Method of allocation not reported. Groups treated in separate hospitals. |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | High risk | No blinding |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | These outcomes unlikely to be affected by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Significantly more dropout from clonidine group. It is unclear how this difference in dropout may have affected the adverse symptoms mean score, which is the only outcome relevant to this review |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Raistrick 2005.
| Methods | Open‐label, randomised controlled trial | |
| Participants | Setting: outpatient, specialist clinic, Leeds, UK Participants: N = 210 heroin dependent by ICD‐10. Data also reported for N = 271 who opted not to be allocated randomly and chose 1 of the 2 treatments Group sizes: group 1: N = 107; group 2: N = 103 Groups similar on baseline variables (but limited data reported) Average age 28 years 75% male |
|
| Interventions | Group 1: buprenorphine, sublingual tablet, 4 mg day 1, 6‐8 mg day 2, 6 mg day 3, then tapered and ceased day 7; naltrexone offered 2 days after last buprenorphine Group 2: lofexidine, 0.4 mg 4‐hourly as needed for 4 days; co‐phenotrope, hyoscine, chlordiazepoxide, chlorpromazine as needed day 1, naltrexone 25 mg day 4 Daily clinic attendance |
|
| Outcomes | Mean daily withdrawal severity, completion rate, abstinence at 1 month | |
| Notes | Withdrawal assessed by Short Opiate Withdrawal Scale. Urine screening on completion Funding from treatment service with contribution from pharmaceutical company but without input to study design, conduct, or report |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "participants were allocated randomly"; method not reported |
| Allocation concealment (selection bias) | Low risk | Quote: "predetermined random sequence . . . held by an administrator" |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | Unclear risk | Quote: "open‐label randomised controlled trial" and "The researcher was blind to . . . the treatment regimen given" Comment: this suggests that observers, but not participants or treating staff were blind to group allocation. This introduces some risk of bias for measures completed by participants. |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | These outcomes unlikely to be affected by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Peak withdrawal scores recorded on day 2 when missing data similar in both groups (20% and 22%). No other outcome data affected by differences in dropout rates |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | More than half eligible participants chose not to enter the trial, but data reported for these cohorts and outcomes were similar to the groups randomised |
Schneider 2000.
| Methods | Randomised controlled open‐label trial | |
| Participants | Setting: inpatient detoxification ward, Hannover, Germany Participants: N = 27 methadone and/or heroin users, dependent by DSM‐IV Group sizes: group 1: N = 15; group 2: N = 12 Groups similar on sociodemographics and drug use history Average age 31 years 89% male Average duration opioid use 11.9 ± 5.4 years (group 1); 8.7 ± 5.8 years (group 2). All polydrug users. 1st inpatient detoxification for around half of the participants. |
|
| Interventions | Group 1: buprenorphine, 3 mg/d for 7 days, then tapered and ceased day 11 Group 2: oxazepam, 90 mg/d for 7 days then tapered and ceased day 15 Both groups received carbamazepine, 900 mg/d for 7 days, then tapered and ceased day 20. Total 21‐day treatment |
|
| Outcomes | Graph of withdrawal scores. Number giving 'drug not effective' as reason for dropout. Number NOT completing treatment | |
| Notes | Withdrawal assessed using Short Opiate Withdrawal Scale. Urine screening used Source of funding: Government grant. Buprenorphine provided by pharmaceutical company |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were randomly assigned"; method not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment not reported |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | High risk | Open‐label stated (authors suggest that medication effects would have revealed group allocation) |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | These outcomes unlikely to be affected by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "the difference in the dropout rate between the two treatment strategies was not significant." |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Seifert 2002.
| Methods | Double‐dummy randomised controlled trial | |
| Participants | Setting: inpatient treatment in ward for drug and alcohol abuse, Hannover, Germany Participants: N = 26, opioid dependent (methadone or heroin) by DSM‐IV Group sizes: group 1: 14; group 2: 12 Groups similar on demographics and drug use history, except 6/14 in group 1 and 10/12 in group 2 abused cannabis in addition to opioids Average age 32 years 85% male Average duration of opioid abuse about 10 years First inpatient detoxification for 19%. All polydrug users |
|
| Interventions | All given 25 mg methadone, 400 mg carbamazepine on admission then: Group 1: buprenorphine, 4 mg/d for 3 days then tapered to cease day 10, or Group 2: L‐methadone, 20 mg day 1, tapered to cease day 10 All received carbamazepine, 900 mg/d for 6 days, then tapered to cease day 14 |
|
| Outcomes | Withdrawal severity, completion rate | |
| Notes | Withdrawal assessed by Short Opiate Withdrawal Scale. Observed urine samples weekly Source of funding not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Patients were randomly assigned"; method not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment not reported |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | Unclear risk | Quote: "double‐dummy, parallel group study design" "Buprenorphine placebo was obtained from the pharmacy" Comment: it is unclear whether participants, treating personnel and observers were all blind to group allocation |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | These outcomes unlikely to be affected by blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "the difference in the dropout rate was not significant" |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Sigmon 2013.
| Methods | Randomised controlled trial, double‐blind, double dummy, with stabilisation dose, abstinence during stabilisation, cocaine use, gender, alcohol dependence, and current pain as stratification variables | |
| Participants | Setting: outpatient, research clinic, Vermont, USA Participants: N = 70, opioid dependent by DSM‐IV Group sizes: group 1: N = 24; group 2: N = 24; group 3: N = 22 Baseline characteristics of groups similar Average age 27 years 69% male Average 4.9 years of opioid abuse; primary drug of abuse oxycodone for 57%, buprenorphine for 39%; 16% used primary by intravenous injection 94% white, 63% employed full‐time, 24% ever married |
|
| Interventions | Stabilised on buprenorphine/naloxone for 2 weeks, then dose tapered: Group 1: over 1 week Group 2: over 2 weeks Group 3: over 4 weeks Participants received 5.5 sublingual tablets at each visit containing a combination of either active/placebo buprenorphine so participants and staff were blind to dose, taper and commencement of naltrexone At completion of buprenorphine taper, all groups were commenced on naltrexone, 12.5 mg day 1, 25 mg days 2 and 3, 50 mg day 4, then 50 mg/d All participants received behavioural therapy based on Community Reinforcement Approach Participants visited the clinic daily in weeks 1‐5, then 3 times a week during weeks 6‐12 |
|
| Outcomes | Participants abstinent from opioids, retention in treatment, participants receiving naltrexone, withdrawal scores | |
| Notes | Urine samples were collected three times a week. Withdrawal and craving were assessed by visual analogue scales, and the CINA Source of funding government grant (NIDA); buprenorphine and placebo provided by manufacturer through NIDA |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Participants . . . were then randomly assigned . . . Stratification variables included stabilization dose, illicit opioid abstinence during stabilization, past‐month cocaine use, sex, current alcohol dependence,and current chronic pain not reported." Comment: method of sequence generation not reported, but computerisation is likely given the number of stratification variables used |
| Allocation concealment (selection bias) | Low risk | Quote: "Doses were prepared by the hospital’s investigational pharmacy". Comment: although method of allocation concealment not specifically reported, the preparation of identical medications by the hospital pharmacy makes it likely that concealment was adequate |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | Low risk | Study stated as double‐blind with placebos used so that "neither the participants nor the staff knew the doses received, the duration of taper and the point at which naltrexone therapy began." |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | Study double‐blind and double‐dummy |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Analysis of withdrawal severity based on a subset of participants (n = 28, 40% of all participants) who were verified to be abstinent from opioids while the buprenorphine dose was being tapered |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Steinmann 2008.
| Methods | Randomised controlled trial | |
| Participants | Setting: inpatient, detoxification unit, Wasserburg, Germany Participants: N = 60 Group sizes: group 1: N = 30; group 2: N = 30 Groups similar on demographics and drug use at baseline Average age 27 years 83% male, duration of heroin use about 7 years |
|
| Interventions | Group 1: methadone, 60 mg/d, tapered 2.5‐5 mg/d. Group 2: buprenorphine, 12‐16 mg/d, tapered 0.8‐1.2 mg/d. Study duration 28 days |
|
| Outcomes | Craving, withdrawal, use of additional medication, number completing treatment | |
| Notes | Withdrawal assessed with COWS and tailored instrument (24 items) Source of funding not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "patients were randomly assigned"; method not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment not reported |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | High risk | "Due to technical reasons" there was no blinding |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | These outcomes unlikely to be affected by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "The two groups of patients did not differ . . . in the rate at which they successfully completed the trial." |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Umbricht 2003.
| Methods | Randomised, double‐blind clinical trial, with stratification on withdrawal severity, pain, CD4 T‐cell count | |
| Participants | Setting: inpatient, AIDS service, USA Participants: N = 55, HIV positive, opioid‐dependent by self‐report and physical exam, hospitalised for acute medical illness Group sizes: group 1: N = 21; group 2: N = 16; group 3. N = 18 Those in group 1 more likely to have been admitted for fever/cellulitis. Groups otherwise similar Average age 40 years 62% male Duration of heroin use around 18 years. Concurrent alcohol dependence, enrolment in MMT exclusion criteria. |
|
| Interventions | All stabilised with morphine 10 mg i.m. every 4 h as needed up to 6 h prior to enrolment in study then 3 day taper with: Group 1: buprenorphine 0.6 mg i.m. every 4 h day 1, every 6 h day 2, every 8 h day 3, Group 2: oral clonidine, 0.2 mg loading dose, 0.1 mg every 4 h day 1, every 6 h day 2, every 8 h day 3, or Group 3: oral methadone, 30 mg day 1, 20 mg day 2, 10 mg day 3. All received clonidine transdermal patch day 4 No adjunct treatment for withdrawal |
|
| Outcomes | Withdrawal severity, completion rate, adverse effects, use of supplemental morphine for pain | |
| Notes | Withdrawal assessed by Short Opiate Withdrawal Scale (participants) and Objective Opiate Withdrawal Scale (observers) Source of funding: government grant (NIDA) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "patients . . . were randomly assigned"; "patients were stratified on four characteristics". Method of sequence generation was not reported |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment not reported |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | Unclear risk | Quote: "To maintain the blind, one active medication and two inactive medications were administered to all participants." Comment: It remains unclear whether participants, treating personnel and observers were all blind to group allocation |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | These outcomes unlikely to be affected by knowledge of treatment allocation |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Statistical methods allowed for missing data and variation in time of assessment |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
Wang 1996.
| Methods | Double‐blind controlled trial, with 14/23 participants randomly allocated | |
| Participants | Setting: not stated − probably outpatient, Milwaukee, USA Participants: N = 23 who had completed maintenance phase of preliminary trial of buprenorphine Group sizes: group 1: N = 14 (N = 7 randomly allocated); group 2: N = 7 Note: this review only used data for the participants who were randomly allocated Participant characteristics not reported (conference abstract only information available) |
|
| Interventions | Buprenorphine 8 mg/d, tapered: Group 1: rapidly (14 days) Group 2: slowly (8 weeks) Placebo to total 12 weeks |
|
| Outcomes | Descriptive comments on withdrawal; completion rate | |
| Notes | Withdrawal rating scale not used. Urine screening not reported Source of funding: government grant (NIDA) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "The first 14 (patients) were randomized into two groups" Comment: method of allocation not reported. Data reported separately for the 14 participants who were allocated randomly, and the remaining 9 participants who were all allocated to group 1. |
| Allocation concealment (selection bias) | Unclear risk | Method of concealment not reported |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | High risk | Double‐blind only for those allocated randomly |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | These outcomes unlikely to be affected by lack of blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Completion of withdrawal treatment is the only outcome reported |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Unclear risk | Unable to assess (conference abstract only report available) |
Wright 2011.
| Methods | Randomised, open‐label, controlled trial | |
| Participants | Setting: healthcare services in high, but not maximum, security prisons (2 male, 1 female), England Participants: prisoners using illicit opioids, wanting to detoxify and remain abstinent, in custody at least 28 days Group sizes: group 1: N = 148; group 2: N = 141 Groups similar on baseline characteristics Median age 31 years Median duration of opioid use 10 years; 53% used primarily by injection |
|
| Interventions | Group 1: buprenorphine, sublingual (probably tablets) starting dose 8 mg, tapered to 0.4 mg at day 20 Group 2: methadone (oral, 1 mg/1 ml mixture), starting dose 30 mg, tapered to 2 mg (day 20) |
|
| Outcomes | Opioid abstinence at 8 days, 1, 3 and 6 months after detoxification. Urinalysis for opioid abstinence at 8 days postdetoxification. Factors predictive of abstinence | |
| Notes | Withdrawal severity not assessed Source of funding: government grant |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomisation sequence (with random block size) was generated using Microsoft Excel RAND function." |
| Allocation concealment (selection bias) | Low risk | Quote: "Sealed, opaque, consecutively numbered envelopes concealing the name of the allocated intervention were prepared by a researcher who had no contact with participants." |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | Low risk | Study undertaken open‐label because "blinded study would have necessitated commercial funding to develop dummy preparations . . . [and] there is also potential bias in study findings where there is a commercial funder". Because it was open‐label, subjective outcomes were not used. |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | Study undertaken open‐label, but these outcomes at less risk of bias due to awareness of treatment allocation |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Loss to follow‐up at primary outcome (abstinence at 8 days postdetoxification) similar for two groups: group 1: 24%; group 2: 29% |
| Selective reporting (reporting bias) | Unclear risk | Data collected on adverse effects but not reported |
| Other bias | Low risk | None apparent |
Ziaaddini 2012.
| Methods | Randomised, double‐blind, controlled trial | |
| Participants | Setting: inpatient psychiatric hospital, Kerman, Iran Participants: opioid dependent by DSM‐IV, randomly selected from individuals referred for detoxification Group sizes: group 1: N = 14; group 2: N = 21 Employed: 42.9% (group 1); 71.4% (group 2); groups otherwise similar Average age 25 years All male 34% married |
|
| Interventions | Group 1: buprenorphine, sublingual tablet (plus clonidine placebo), 2 mg day 1, 4 mg day 2, 6 mg day 3, 4 mg day 4, 2 mg day 5 with additional 2‐4 mg if required for severe withdrawal Group 2: clonidine, oral tablets, 0.4 mg day 1, 0.6 mg days 2 and 3, 0.2 mg days 4 and 5, plus additional 0.2‐0.4 mg/d if required for severe withdrawal Actual doses administered not reported |
|
| Outcomes | Average change in withdrawal and craving scores on days 1, 2, 3, and 5. Total days in treatment and days receiving naltrexone at follow‐up | |
| Notes | Withdrawal rated by 'psychiatric technician' with COWS (11 items rated 0‐4), and by participants with ARWS (Adjective Rating Withdrawal Scale, 16 items rated 0‐9). Craving assessed with visual analogue scale Funding source intramural |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "participants were randomly allocated to . . . detoxification group." Method of sequence generation not explained |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding (performance bias and detection bias) Subjective outcomes ‐ intensity of withdrawal, adverse effects) | Low risk | Double‐blind stated, and placebos used to maintain blind. Quote: "All drugs and placebos were assigned a code and kept by a person who was not involved in the study" |
| Blinding (performance bias and detection bias) Objective outcomes ‐ duration of treatment, completion of treatment | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "All patients took naltrexone at the end of the detoxification period" Comment: this review focuses on the detoxification period, and if all participants completed detoxification there should be no incomplete data |
| Selective reporting (reporting bias) | Low risk | None apparent |
| Other bias | Low risk | None apparent |
COWS: Clinical Opiate Withdrawal Scale; DSM‐IV: Diagnostic and Statistical Manual of Mental Health ‐ 4th edition; DSM‐III‐R: Diagnostic and Statistical Manual of Mental Health ‐ 3rd edition, Revised; i.m.: intramuscular; i.v.: intravenous; MMT: methadone maintenance treatment; OOWS: Objective Opiate Withdrawal Scale; SOWS: Subjective Opiate Withdrawal Scale.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Blondell 2008 | Randomised controlled trial comparing effect of 2 different periods of extended buprenorphine prescription following inpatient detoxification. No data on detoxification outcomes defined for this review. Not primarily about withdrawal management |
| Breen 2003 | Comparison of 3 different regimens for transferring participants from methadone to buprenorphine, with subsequent tapering of buprenorphine dose. No comparison during withdrawal phase and insufficient data on outcomes of this phase. |
| Fiellin 2014 | Randomised controlled trial comparing buprenorphine/naloxone for withdrawal management and substitution treatment. Treatment comparison is not one of the modalities included in the review |
| Fingerhood 2001 | Clonidine or buprenorphine offered consecutively for management of opioid withdrawal. Not randomised controlled trial |
| Frownfelter 2001 | Investigation of buprenorphine as an adjunct to antagonist‐induced withdrawal. The groups differed only in the timing of naltrexone administration. Treatment comparison not one defined by inclusion criteria |
| Gandhi 2003 | Randomised controlled trial comparing 2 different dose regimens of buprenorphine for management of opioid withdrawal. Groups combined for analysis of postdetoxification outcomes. No data on detoxification phase |
| Gibson 2003 | Comparison of outcomes of opioid withdrawal managed with buprenorphine in specialist clinic or primary health setting. Treatment comparison not defined by inclusion criteria |
| Gonzalez 2015 | Randomised controlled trial comparing memantine and placebo as adjuncts to buprenorphine for management of opioid withdrawal. Not one of the comparisons specified for this review |
| Hao 2000 | Treatment comparison (WeiniCom, a Chinese herbal preparation with complex pharmacology) is not one of the modalities defined by the inclusion criteria. |
| Harris 2003 | Comparison of buprenorphine and lofexidine for management of opioid withdrawal. Not a controlled study − partly retrospective; insufficient outcome data (conference abstract only) |
| He 1999 | Controlled study comparing buprenorphine plus naloxone from day 5, with tincture of opium. Unclear whether group allocation was random. Treatment comparison (tincture of opium) is not one of the modalities defined by the inclusion criteria. |
| Jain 2011 | Comparison of memantine and placebo in conjunction with buprenorphine in terms of capacity to ameliorate withdrawal induced with naloxone. Study more about pharmacology of memantine than management of withdrawal |
| Jia 2001 | Randomised controlled trial comparing methadone followed by buprenorphine versus buprenorphine alone for managing opioid withdrawal. Primary treatment approach unclear − it appears that some participants in buprenorphine only group received methadone during first few days of treatment. Comparison is not one specified for this review |
| Johnson 1989 | Preliminary report of trial comparing methadone and buprenorphine for the treatment of opioid dependence. Insufficient outcome data |
| Johnson 1992a | Comparison of buprenorphine and clonidine for management of opioid withdrawal. Insufficient data − conference abstract only. Probably preliminary report of Cheskin 1994 |
| Johnson 1992b | Randomised controlled trial comparing buprenorphine and methadone (60 or 20 mg/d) for 17 weeks of maintenance followed by 8 weeks withdrawal. Comparison not one specified for this review. Focus on maintenance rather than management of withdrawal |
| Johnson 1996 | Study of withdrawal symptoms following abrupt cessation of methadone or buprenorphine. Focus on pharmacological properties rather than management of withdrawal. Insufficient data − conference abstract only |
| Katz 2009 | Comparison of brief (5‐day) and extended (30‐day) buprenorphine treatment for outpatient management of opioid withdrawal. Data drawn from 2 previous studies comparing counselling approaches as adjuncts to buprenorphine. Not randomised controlled trial |
| Kosten 1988 | Open label study comparing 3 different dose regimens of buprenorphine in terms of illicit opiate use and withdrawal symptoms during 30 days at a fixed dose. Buprenorphine abruptly discontinued after 30 days but no data reported on this withdrawal phase. Study more about substitution treatment than management of withdrawal |
| Kosten 1991 | Reports use of buprenorphine for 30 days as transition between methadone or heroin and naltrexone, with comparison of reactions to naloxone and naltrexone. No treatment comparison for withdrawal phase |
| Law 2002 | Participants stabilised on methadone or buprenorphine then detoxified by combination of tapered methadone plus lofexidine, or tapered buprenorphine. Insufficient data (conference abstract, preliminary report) |
| Liebschutz 2014 | Randomised controlled trial comparing 5‐day buprenorphine detoxification with stabilisation on buprenorphine in hospital and linkage to outpatient opioid substitution treatment. Comparison not one specified for this review. |
| Lintzeris 2003 | Investigation of doses of buprenorphine required to suppress opioid withdrawal symptoms. No treatment comparison |
| Liu 1997 | Comparison of different dose regimens of buprenorphine, with starting dose determined by duration and dose of heroin use and severity of dependence. Not a randomised controlled trial |
| Maayan 2008 | Randomised controlled trial comparing DHEA and placebo as adjuncts to buprenorphine for management of opioid withdrawal. Analysis largely in terms of factors affecting response to DHEA treatment. Insufficient outcome data, and not primarily a study of buprenorphine |
| Meade 2010 | Randomised controlled trial comparing active and sham transcutaneous electric acupoint stimulation (TEAS) as an adjunct to inpatient detoxification managed with buprenorphine. Focus of study on drug use following detoxification. Insufficient data on withdrawal episode |
| Montoya 1994 | Comparison of naltrexone‐buprenorphine combination with buprenorphine only for managing opioid withdrawal. Investigation of pharmacology of buprenorphine and naltrexone rather than management of withdrawal |
| Pjrek 2012 | Medication selection based on judgement of treating clinician. Not randomised controlled trial. Focus on sleep parameters − insufficient data on outcomes defined for this review |
| Pycha 1994 | Comparison of 2 rates of reduction of buprenorphine dose for management of opioid withdrawal. Only information available is conference abstract − contact author advised study was never fully written up. Insufficient information on medications and characteristics of patients, insufficient outcome data |
| Reed 2007 | Participants able to choose buprenorphine or methadone for management of opioid withdrawal |
| Resnick 1992 | Randomised controlled trial comparing buprenorphine detoxification and continuation of buprenorphine substitution treatment for opioid dependence. Comparison not one of the modalities defined by the inclusion criteria |
| Rosen 1995 | Participants maintained on buprenorphine for 30 days then given challenges with naltrexone or naloxone as process of easing transition to naltrexone maintenance treatment. No treatment comparison |
| Rosenthal 2013 | Randomised controlled trial comparing active buprenorphine/naloxone implants with placebo implants and with sublingual buprenorphine/naloxone tablets. Opiate withdrawal and craving were assessed in the context of initiation of substitution (maintenance) treatment rather than managing withdrawal |
| Sanders 2013 | Randomised controlled trial comparing gabapentin and placebo as adjuncts to buprenorphine for treatment of opioid withdrawal. Intervention is not one defined by the inclusion criteria for this review |
| Sheard 2009 | Comparison of buprenorphine and dihydrocodeine for management of opioid withdrawal in prison setting. Comparison not one of the modalities defined by inclusion criteria |
| Sigmon 2004 | Randomised placebo‐controlled trial of depot preparation of buprenorphine. Focus is on effectiveness in providing opioid blockade and suppression of withdrawal, but not full withdrawal intervention |
| Sullivan 2015 | Randomised controlled trial comparing 2 different buprenorphine regimens to manage induction onto naltrexone treatment. Intervention not one defined by inclusion criteria for this review. Preliminary report (conference abstract) − insufficient outcome data |
| Tompkins 2014 | Cross‐over study assessing withdrawal syndrome following cessation of morphine or buprenorphine. No intervention to manage withdrawal |
| Umbricht 1999 | Comparison of buprenorphine‐naltrexone combination with buprenorphine followed by naltrexone for management of opioid withdrawal. Treatment comparison not one of the modalities defined by the inclusion criteria |
| Weiss 2010 | Randomised controlled trial comparing adjunct therapies with phases of buprenorphine maintenance and dose taper. Comparison not one defined by the inclusion criteria for this review |
| White 2001 | Comparison of buprenorphine and lofexidine for management of opioid withdrawal. Mixed retrospective and prospective data collection − not a controlled study |
| Williams 2002 | Reports the use of buprenorphine for management of opioid withdrawal in an outpatient setting. No treatment comparison |
| Woody 2008 | Comparison of 12 week buprenorphine maintenance and 14‐day detox in terms of positive urine samples and retention in treatment for opioid dependence. Comparison is not one of the modalities defined by the inclusion criteria |
| Wright 2007 | Randomised controlled trial comparing buprenorphine and dihydrocodeine for management of opioid withdrawal in primary care setting. Comparison not one of the modalities defined by the inclusion criteria. |
| Zhang 1993 | Comparison of buprenorphine and methadone for management of opioid withdrawal. Insufficient information on treatment regimens and outcomes |
Differences between protocol and review
The protocol and previous versions of this review included prospective controlled cohort studies as well as randomised and quasi‐randomised controlled trials. As further research has become available, we have now restricted the review to randomised and quasi‐randomised controlled trials to ensure internal validity of the review.
Contributions of authors
Linda Gowing, with assistance from Dalitso Mbewe for this update, assessed each potentially relevant study according to identified inclusion and exclusion criteria, extracted key information from included studies and compiled a first draft of the review. Co‐authors confirmed inclusion and exclusion decisions by discussion. Robert Ali and Jason White confirmed and commented on the review content.
Sources of support
Internal sources
Drug and Alcohol Services South Australia, Australia.
External sources
Commonwealth Department of Health and Ageing, Australia.
Declarations of interest
Linda Gowing: none known.
Robert Ali: none known.
Jason M White: none known.
Dalitso Mbewe: none known.
New search for studies and content updated (conclusions changed)
References
References to studies included in this review
Amass 1994 {published data only}
- Amass L, Bickel WK, Higgins ST, Hughes JR. A preliminary investigation of outcome following gradual or rapid buprenorphine detoxification. Journal of Addictive Diseases 1994;13(3):33‐45. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Assadi 2004 {published data only}
- Assadi SM, Hafezi M, Mokri A, Razzaghi EM, Ghaeli P. Opioid detoxification using high doses of buprenorphine in 24 hours: a randomised, double‐blind, controlled clinical trial. Journal of Substance Abuse Treatment 2004;27(1):75‐82. [DOI] [PubMed] [Google Scholar]
Bickel 1988 {published data only}
- Bickel WK, Johnson RE, Stitzer ML, Bigelow GE, Liebson IA, Jasinski DR. A clinical trial of buprenorphine: I. Comparison with methadone in the detoxification of heroin addicts. II. Examination of its opioid blocking properties. NIDA Research Monograph 1987;76:182‐8. [PubMed] [Google Scholar]
- Bickel WK, Stitzer ML, Bigelow GE, Liebson IA, Jasinski DR, Johnson RE. A clinical trial of buprenorphine: comparison with methadone in the detoxification of heroin addicts. Clinical Pharmacology & Therapeutics 1988;43(1):72‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Cheskin 1994 {published and unpublished data}
- Cheskin LJ, Fudala PJ, Johnson RE. A controlled comparison of buprenorphine and clonidine for acute detoxification from opioids. Drug and Alcohol Dependence 1994;36(2):115‐21. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Collins 2005 {published data only}
- Collins ED, Kleber HD, Whittington RA, Heitler NE. Anesthesia‐assisted vs buprenorphine‐ or clonidine‐assisted heroin detoxification and naltrexone induction. A randomised trial. JAMA 2005;294(8):903‐13. [DOI] [PubMed] [Google Scholar]
- Collins ED, Whittington RA, Heitler NE, Kleber HD. A randomised comparison of anaesthesia‐assisted heroin detoxification with buprenorphine‐ and clonidine‐assisted detoxifications. Drug and Alcohol Dependence 2002;66(Suppl):S35. [Google Scholar]
Hopper 2005 {published data only}
- Hopper JA, Wu J, Martus W, Pierre JD. A randomized trial of one‐day vs. three‐day buprenorphine inpatient detoxification protocols for heroin dependence. Journal of Opioid Management 2005;1(1):31‐5. [DOI] [PubMed] [Google Scholar]
Hussain 2015 {published data only}
- Hussain SS, Farhat S, Rather YH, Abbas Z. Comparative trial to study the effectiveness of clonidine hydrochloride and buprenorphine‐naloxone in opioid withdrawal: a hospital based study. Journal of Clinical and Diagnostic Research 2015;9(1):FC01‐FC4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Janiri 1994 {published data only}
- Janiri L, Mannelli P, Persico AM, Serretti A, Tempesta E. Opiate detoxification of methadone maintenance patients using lefetamine, clonidine and buprenorphine. Drug and Alcohol Dependence 1994;36(2):139‐45. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Janiri L, Mannelli P, Serretti A, Tempesta E. Low‐dose buprenorphine detoxification in long term methadone addicts. Regulatory Peptides 1994;Suppl(1):289‐90. [Google Scholar]
Ling 2005 {published data only}
- Amass L, Ling W, Freese TE, Reiber C, Annon JJ, Cohen AJ, et al. Bringing buprenorphine‐naloxone detoxification to community treatment providers: the NIDA Clinical Trials Network Field Experience. American Journal on Addictions 2004;13(Suppl):S42‐66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hillhouse M, Domier CP, Chim D, Ling W. Provision of ancillary medications during buprenorphine detoxification does not improve treatment outcomes. Journal of Addictive Diseases 2010;29(1):23‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ling W, Amass L, Shoptaw S, Annon JJ, Hillhouse M, et al. A multi‐centre randomised trial of buprenorphine‐naloxone versus clonidine for opioid detoxification: findings from the National Institute on Drug Abuse Clinical Trials Network. Addiction 2005;100(8):1090‐100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ziedonis DM, Amass L, Steinberg M, Woody G, Krejci J, Annon JJ, et al. Predictors of outcome for short‐term medically supervised opioid withdrawal during a randomized, multicenter trial of buprenorphine‐naloxone and clonidine in the NIDA clinical trials network drug and alcohol dependence. Drug and Alcohol Dependence 2009;99(1‐3):28‐36. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ling 2009 {published data only}
- Brown ES, Tirado C, Minhajuddin A, Hillhouse M, Adinoff B, Ling W, et al. Association of race and ethnicity with withdrawal symptoms, attrition, opioid use, and side‐effects during buprenorphine therapy. Journal of Ethnicity in Substance Abuse 2010;9(2):106‐14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hillhouse M, Canamar CP, Doraimani G, Thomas C, Hasson A, Ling W. Participant characteristics and buprenorphine dose. American Journal of Drug and Alcohol Abuse 2011;37(5):453‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hillhouse M, Canamar CP, Ling W. Predictors of outcome after short‐term stabilization with buprenorphine. Journal of Substance Abuse Treatment 2013;44(3):336‐42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ling W, Hillhouse M, Domier C, Doraimani G, Hunter J, Thomas C, et al. Buprenorphine tapering schedule and illicit opioid use. Addiction 2009;104(2):256‐65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nielsen S, Hillhouse M, Thomas C, Hasson A, Ling W. A comparison of buprenorphine taper outcomes between prescription opioid and heroin users. Journal of Addiction Medicine 2013;7(1):33‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saleh MI. Modeling longitudinal changes in buprenorphine treatment outcome for opioid dependence. Pharmacopsychiatry 2014;47(7):251‐8. [DOI] [PubMed] [Google Scholar]
- Saleh MI. Predictors of long term opioid withdrawal outcome after short‐term stabilization with buprenorphine. European Review for Medical and Pharmacological Sciences 2014;18(24):3935‐42. [PubMed] [Google Scholar]
Lintzeris 2002 {published data only}
- Lintzeris N, Bell J, Bammer G, Jolley DJ, Rushworth L. A randomised controlled trial of buprenorphine in the management of short‐term ambulatory heroin withdrawal. Addiction 2002;97(11):1395‐404. [DOI] [PubMed] [Google Scholar]
Marsch 2005 {published data only}
- Marsch LA, Bickel WK, Badger GJ, Stothart ME, Quesnel KJ, Stanger C, et al. Comparison of pharmacological treatments for opioid‐dependent adolescents: a randomized controlled trial. Archives of General Psychiatry 2005;62(10):1157‐64. [DOI] [PubMed] [Google Scholar]
- Moore SK, Marsch LA, Badger GJ, Solhkhah R, Hofstein Y. Improvement in psychopathology among opioid‐dependent adolescents during behavioral‐pharmacological treatment. Journal of Addiction Medicine 2011;5(4):264‐71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Motamed M, Marsch LA, Solhkhah R, Bickel WK, Badger GJ. Differences in treatment outcomes between prescription opioid‐dependent and heroin‐dependent adolescents. Journal of Addiction Medicine 2008;2(3):158‐64. [DOI] [PubMed] [Google Scholar]
Marsch 2016 {published data only}
- Marsch LA, Moore SK, Borodovsky JT, Solhkhah R, Badger GJ, et al. A randomized controlled trial of buprenorphine taper duration among opioid‐dependent adolescents and young adults. Addiction 2016;111(8):1406‐15. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Nigam 1993 {published and unpublished data}
- Nigam AK, Ray R, Tripathi BM. Buprenorphine in opiate withdrawal: a comparison with clonidine. Journal of Substance Abuse Treatment 1993;10(4):391‐4. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
O'Connor 1997 {published data only}
- O'Connor PG, Carroll KM, Shi JM, Schottenfeld RS, Kosten TR, Rounsaville BJ. Three methods of opioid detoxification in a primary care setting. A randomized trial. Annals of Internal Medicine 1997;127(7):526‐30. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Shi JM, O'Connor PG, Constantino JA, Carroll KM, Schottenfeld RS, Rounsaville BJ. Three methods of ambulatory opiate detoxification: preliminary results of a randomised clinical trial. NIDA Research Monograph 1993;132:309. [Google Scholar]
Oreskovich 2005 {published data only}
- Oreskovich MR, Saxon AJ, Ellis ML, Malte CA, Reoux JP, Knox PC. A double‐blind, double‐dummy, randomized, prospective pilot study of the partial Mu opiate agonist, buprenorphine, for acute detoxification from heroin. Drug and Alcohol Dependence 2005;77(1):71‐9. [Embase 2004536231] [DOI] [PubMed] [Google Scholar]
Petitjean 2002 {published and unpublished data}
- Petitjean S, Bardeleben U, Weber M, Ladewig D. Buprenorphine versus methadone in opiate detoxification: preliminary results. Drug and Alcohol Dependence 2002;66(Suppl):S138. [Google Scholar]
Ponizovsky 2006 {published data only}
- Ponizovsky AM, Grinshpoon A, Margolis A, Cohen R, Rosca P. Well‐being, psychosocial factors, and side‐effects among heroin‐dependent inpatients after detoxification using buprenorphine versus clonidine. Addictive Behaviors 2006;31(11):2002‐13. [DOI] [PubMed] [Google Scholar]
Raistrick 2005 {published data only}
- Raistrick D, West D, Finnegan O, Thistlewaite G, Brearley R, Banbery J. A comparison of buprenorphine and lofexidine for community opiate detoxification: results from a randomized controlled trial. Addiction 2005;100(12):1860‐7. [DOI] [PubMed] [Google Scholar]
Schneider 2000 {published data only}
- Paetzold W, Eronat V, Seifert J, Holze I, Emrich HM, Schneider U. Detoxification of poly‐substance abusers with buprenorphine. Effects on affect, anxiety, and withdrawal symptoms [Detoxifikation polytoxikomaner Patienten mit Buprenorphin. Auswirkungen auf Affektivitat, Angst und Entzugssymptomaik]. Nervenarzt 2000;71(9):722‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Schneider U, Paetzold W, Eronat V, Huber TJ, Seifert J, Wiese B, et al. Buprenorphine and carbamazepine as a treatment for detoxification of opiate addicts with multiple drug misuse: a pilot study. Addiction Biology 2000;5:65‐9. [DOI] [PubMed] [Google Scholar]
Seifert 2002 {published data only}
- Seifert J, Metzner C, Paetzold W, Borsutzky M, Ohlmeier M, Passie T, et al. Mood and affect during detoxification of opiate addicts: a comparison of buprenorphine versus methadone. Addiction Biology 2005;10(2):157‐64. [DOI] [PubMed] [Google Scholar]
- Seifert J, Metzner C, Paetzold W, Borsutzky M, Passie T, Rollnik J, et al. Detoxification of opiate addicts with multiple drug abuse: a comparison of buprenorphine vs. methadone. Pharmacopsychiatry 2002;35(5):159‐64. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Sigmon 2013 {published data only}
- Dunn KE, Saulsgiver KA, Miller ME, Nuzzo PA, Sigmon SC. Characterizing opioid withdrawal during double‐blind buprenorphine detoxification. Drug and Alcohol Dependence 2015;151:47‐55. [DOI: 10.1016/j.drugalcdep.2015.02.033] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patrick ME, Dunn KE, Badger GJ, Heil SH, Higgins ST, Sigmon SC. Spontaneous reductions in smoking during double‐blind buprenorphine detoxification. Addictive Behaviors 2014;39(9):1353‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sigmon SC, Dunn KE, Saulsgiver K, Patrick ME, Badger GJ, Heil SH, et al. A randomized, double‐blind evaluation of buprenorphine taper duration in primary prescription opioid abusers. JAMA Psychiatry 2013;70(12):1347‐54. [DOI] [PMC free article] [PubMed] [Google Scholar]
Steinmann 2008 {published data only}
- Steinmann C, Artmann S, Henneberg B, Paul HW. Should methadone or buprenorphine be preferred for opiate detoxification? [Methadon‐racemat versus buprenorphin zur stationaren entgiftungsbehandlung opiatabhangiger]. Psychiatrische Praxis 2007;34(1):S103‐5. [Google Scholar]
- Steinmann C, Artmann S, Schachtschneider A, Paul HW. Methadone versus buprenorphine for inpatient detoxification treatment [Methadon‐Racemat versus Buprenorphin zur stationaren Entgiftungsbehandlung]. Sucht 2008;54(4):217‐21. [Google Scholar]
Umbricht 2003 {published data only}
- Umbricht A, Hoover DR, Tucker MJ, Leslie JM, Chaisson RE, Preston KL. Opioid detoxification with buprenorphine, clonidine, or methadone in hospitalized heroin‐dependent patients with HIV infection. Drug and Alcohol Dependence 2003;69(3):263‐72. [DOI] [PubMed] [Google Scholar]
Wang 1996 {published data only}
- Wang RI, Young LD. Double‐blind controlled detoxification from buprenorphine. NIDA Research Monograph 1996;162:114. [Google Scholar]
Wright 2011 {published data only}
- Sheard L, Wright NMJ, Adams CE, Bound N, Rushforth B, Hart R, et al. The Leeds Evaluation of Efficacy of Detoxification Study (LEEDS) Prisons Project Study: protocol for a randomised controlled trial comparing methadone and buprenorphine for opiate detoxification. Trials 2009;10:53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wright NMJ, Sheard L, Adams CE, Rushforth BJ, Harrison W, Bound N, et al. Comparison of methadone and buprenorphine for opiate detoxification (LEEDS trial): a randomised controlled trial. British Journal of General Practice 2011;61(593):e772‐80. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ziaaddini 2012 {published data only}
- Ziaaddini H, Nasirian M, Nakhaee N. A comparison of the efficacy of buprenorphine and clonidine in detoxification of heroin‐dependents and the following maintenance treatment. Addiction and Health 2010;2(1‐2):18‐24. [PMC free article] [PubMed] [Google Scholar]
- Ziaaddini H, Nasirian M, Nakhaee N. Comparison of the efficacy of buprenorphine and clonidine in detoxification of opioid‐dependents. Addiction and Health 2012;4(3‐4):79‐86. [PMC free article] [PubMed] [Google Scholar]
References to studies excluded from this review
Blondell 2008 {published data only}
- Blondell RD, Frydrych L, Arber BC, Bashaw HL, Vexler A, Purdy CH, et al. A randomized trial of extended buprenorphine detoxification for opioid dependency. Journal of Addiction Medicine 2008;2(3):139‐46. [DOI] [PubMed] [Google Scholar]
Breen 2003 {published data only}
- Breen CL, Harris SJ, Lintzeris N, Mattick RP, Hawken L, Bell J, et al. Cessation of methadone maintenance treatment using buprenorphine: transfer from methadone to buprenorphine and subsequent buprenorphine reductions. Drug and Alcohol Dependence 2003;71(1):49‐55. [DOI] [PubMed] [Google Scholar]
Fiellin 2014 {published data only}
- Fiellin D, Cutter CJ, Moore BA, Barry D, O'Connor P, Schottenfeld RS. Primary care buprenorphine detoxification vs. maintenance for prescription opioid dependence. Drug and Alcohol Dependence 2015;146(12):e277. [Google Scholar]
- Fiellin DA, Schottenfeld RS, Cutter CJ, Moore BA, Barry DT, O'Connor PG. Primary care‐based buprenorphine taper vs maintenance therapy for prescription opioid dependence: a randomized clinical trial. JAMA Internal Medicine 2014;174(12):1947‐54. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fingerhood 2001 {published data only}
- Fingerhood MI, Thompson MR, Jasinski DR. A comparison of clonidine and buprenorphine in the outpatient treatment of opiate withdrawal. Substance Abuse 2001;22(3):193‐9. [DOI] [PubMed] [Google Scholar]
Frownfelter 2001 {published data only}
- Frownfelter J, Hopper JA. Rapid opioid detoxification using buprenorphine and naltrexone. Drug and Alcohol Dependence 2001;63(Suppl 1):S50. [Google Scholar]
Gandhi 2003 {published data only}
- Gandhi DH, Jaffe JH, McNary S, Kavanagh GJ, Hayes M, Currens M. Short‐term outcomes after brief ambulatory opioid detoxification with buprenorphine in young heroin users. Addiction 2003;98(4):453‐62. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Gibson 2003 {published data only}
- Doran CM, Shanahan M, Bell J, Gibson A. A cost‐effectiveness analysis of buprenorphine‐assisted heroin withdrawal. Drug and Alcohol Review 2004;23(2):171‐5. [DOI] [PubMed] [Google Scholar]
- Gibson AE, Doran CM, Bell JR, Ryan A, Lintzeris N. A comparison of buprenorphine treatment in clinic and primary care settings: A randomised trial. Medical Journal of Australia 2003;179(1):38‐42. [DOI] [PubMed] [Google Scholar]
Gonzalez 2015 {published data only}
- Gonzalez G, DiGirolamo G, Kolodziej ME, Smelson D, Romero‐Gonzalez M. Memantine improves buprenorphine treatment for opioid‐dependent young adults. Drug and Alcohol Dependence 2015;146:e124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gonzalez G, DiGirolamo G, Kolodziej ME, Smelson D, Romero‐Gonzalez M. Memantine improves buprenorphine treatment for opioid‐dependent young adults. Drug and Alcohol Dependence 2015;156:243‐253. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hao 2000 {published data only}
- Hao W, Zhao M. A comparative clinical study of the effect of WeiniCom, a Chinese herbal compound, on alleviation of withdrawal symptoms and craving for heroin in detoxification treatment. Journal of Psychoactive Drugs 2000;32(3):277‐84. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Harris 2003 {published data only}
- Harris L. A comparison of buprenorphine with lofexidine in the rapid opiate detoxification of patients with opiate dependency receiving treatment in a community setting. Addiction Biology 2003;8:243. [Google Scholar]
He 1999 {published data only}
- He M, Zhang H, Tang J, Tang Z, Yang D, Chen X, et al. A comparative study of buprenorphine plus naloxone vs opium tincture in the detoxification treatment of heroin dependence. Chinese Journal of Clinical Psychology 1999;4(1):10‐5. [Google Scholar]
Jain 2011 {published data only}
- Jain K, Jain R, Dhawan A. A double‐blind, double‐dummy, randomized controlled study of memantine versus buprenorphine in naloxone‐precipitated acute withdrawal in heroin addicts. Journal of Opioid Management 2011;7(1):11‐20. [DOI] [PubMed] [Google Scholar]
Jia 2001 {published data only}
- Jia Y. Effect of methadone plus buprenorphine on the alleviation of heroin withdrawal symptoms. Chinese Journal of Clinical Psychology 2001;9(1):60‐2. [Google Scholar]
Johnson 1989 {published data only}
- Johnson RE, Fudala PJ, Collins CC, Jaffe JH. Outpatient maintenance/detoxification comparison of methadone and buprenorphine. NIDA Research Monograph 1989;95:384. [MEDLINE: ] [PubMed] [Google Scholar]
Johnson 1992a {published data only}
- Johnson RE, Fudala PJ, Cheskin LR. A comparison of buprenorphine to clonidine for rapid inpatient opiate detoxification. Clinical Pharmacology & Therapeutics 1992;51(2):167. [Google Scholar]
Johnson 1992b {published data only}
- Johnson RE, Jaffe JH, Fudala PJ. A controlled trial of buprenorphine treatment for opioid dependence. JAMA 1992;267(20):2750‐5. [PubMed] [Google Scholar]
Johnson 1996 {published data only}
- Johnson RE, Eissenberg T, Alim TN, Lindquist T, Vocci FJ, Risher‐Flowers DL, et al. Comparison of the withdrawal syndromes following abrupt termination of buprenorphine and methadone. NIDA Research Monograph 1996;162:200. [Google Scholar]
Katz 2009 {published data only}
- Katz EC, Schwartz RP, King S, Highfield DA, O'Grady KE, Billings T, et al. Brief vs extended buprenorphine detoxification in a community treatment program: engagement and short‐term outcomes. American Journal of Drug and Alcohol Abuse 2009;35(2):63‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kosten 1988 {published data only}
- Kosten TR, Kleber HD. Buprenorphine detoxification from opioid dependence: a pilot study. Life Sciences 1988;42(6):635‐41. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Kosten 1991 {published data only}
- Kosten TR, Krystal JH, Charney DS, Price LH, Morgan CH, Kleber HD. Opioid antagonist challenges in buprenorphine maintained patients. Drug and Alcohol Dependence 1990;25(1):73‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Kosten TR, Krystal JH, Charney DS, Price LH, Morgan CH, Kleber HD. Rapid detoxification from opioid dependence. American Journal of Psychiatry 1989;146(10):1349. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Kosten TR, Morgan C, Kleber HD. Phase II clinical trials of buprenorphine: detoxification and induction onto naltrexone. NIDA Research Monograph 1992;121:101‐19. [MEDLINE: ] [PubMed] [Google Scholar]
- Kosten TR, Morgan C, Kleber HD. Treatment of heroin addicts using buprenorphine. American Journal of Drug and Alcohol Abuse 1991;17(2):119‐28. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Law 2002 {published data only}
- Law FD, Myles JS, Nutt DJ. BD RCT of Suboxone (buprenorphine/naloxone) vs. methadone/lofexidine for stabilization and withdrawal of low‐dose outpatient opiate addicts. Drug and Alcohol Dependence 2002;66(Suppl 1):S100. [Google Scholar]
- Myles J, Law F, Raybould T. A double‐blind randomised controlled trial of buprenorphine/naloxone (suboxone) versus methadone/lofexidine for the detoxification of opiate‐dependent addicts. Drug and Alcohol Dependence 2000;60(Suppl 1):S156. [Google Scholar]
Liebschutz 2014 {published data only}
- Cushman PA, Anderson BJ, Moreau M, Stein MD, Liebschutz JM. Buprenorphine initiation and linkage to outpatient buprenorphine treatment does not reduce frequency of injection drug use for inpatient opioid‐dependent injection drug users: results of a randomized clinical trial. Journal of General Internal Medicine 2015;30:S114‐S5. [Google Scholar]
- Liebschutz J, Crooks D, Herman D, Anderson B, Meshesha L, Dossabhoy S, et al. Initiating buprenorphine maintenance for opiate‐dependent hospitalized patients: a randomized controlled trial. Journal of General Internal Medicine 2013;28:S108‐9. [Google Scholar]
- Liebschutz JM, Crooks D, Herman D, Anderson B, Tsui J, Meshesha LZ, et al. Buprenorphine treatment for hospitalized, opioid‐dependent patients: a randomized clinical trial. JAMA Internal Medicine 2014;174(8):1369‐76. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lintzeris 2003 {published data only}
- Lintzeris N, Bammer G, Rushworth L, Jolley DJ, Whelan G. Buprenorphine dosing regime for inpatient heroin withdrawal: a symptom‐triggered dose titration study. Drug and Alcohol Dependence 2003;70(3):287‐94. [DOI] [PubMed] [Google Scholar]
Liu 1997 {published data only}
- Liu ZM, Cai ZJ, Wang XP, Ge Y, Li CM. Rapid detoxification of heroin dependence by buprenorphine. Acta Pharmacologica Sinica 1997;18(2):112‐4. [PubMed] [Google Scholar]
Maayan 2008 {published data only}
- Maayan R, Touati‐Werner D, Shamir D, Yadid G, Friedman A, Eisner D, et al. The effect of DHEA complementary treatment on heroin addicts participating in a rehabilitation program: a preliminary study. European Neuropsychopharmacology 2008;18(6):406‐13. [DOI] [PubMed] [Google Scholar]
Meade 2010 {published data only}
- Meade CS, Lukas SE, McDonald LJ, Fitzmaurice GM, Eldridge JA, Merrill N, et al. A randomized trial of transcutaneous electric acupoint stimulation as adjunctive treatment for opioid detoxification. Journal of Substance Abuse Treatment 2010;38(1):12‐21. [DOI] [PMC free article] [PubMed] [Google Scholar]
Montoya 1994 {published data only}
- Montoya ID, Mann DJ, Ellison PA, Lange WR, Preston KL. Inpatient medically supervised opioid withdrawal, with buprenorphine alone and in combination with naltrexone. Clinical Pharmacology and Therapeutics 1994;55(2):131. [Google Scholar]
Pjrek 2012 {published data only}
- Pjrek E, Frey R, Naderi‐Heiden A, Strnad A, Kowarik A, Kasper S, et al. Actigraphic measurements in opioid detoxification with methadone or buprenorphine. Journal of Clinical Psychopharmacology 2012;32(1):75‐82. [DOI] [PubMed] [Google Scholar]
Pycha 1994 {published and unpublished data}
- Pycha C, Resnick RB, Galanter M. Buprenorphine: rapid and slow dose‐reductions for heroin detoxification. NIDA Research Monograph 1994;141:453. [Google Scholar]
Reed 2007 {published data only}
- Reed LJ, Glasper A, Wet CJ, Bearn J, Gossop M. Comparison of buprenorphine and methadone in the treatment of opiate withdrawal: possible advantages of buprenorphine for the treatment of opiate‐benzodiazepine codependent patients?. Journal of Clinical Psychopharmacology 2007;27(2):188‐92. [DOI] [PubMed] [Google Scholar]
Resnick 1992 {published data only}
- Resnick RB, Galanter M, Pycha C, Cohen A, Grandison P, Flood N. Buprenorphine: an alternative to methadone for heroin dependence treatment. Psychopharmacology Bulletin 1992;28(1):109‐13. [MEDLINE: ] [PubMed] [Google Scholar]
Rosen 1995 {published data only}
- Rosen M, Kosten TR. Detoxification and induction onto naltrexone. In: Cowan A, Lewis JW editor(s). Buprenorphine: Combatting Drug Abuse with a Unique Opioid. New York: Wiley‐Liss, 1995. [Google Scholar]
Rosenthal 2013 {published data only}
- Rosenthal RN, Ling W, Casadonte P, Vocci F, Bailey GL, Kampman K, et al. Buprenorphine implants for treatment of opioid dependence: randomized comparison to placebo and sublingual buprenorphine/naloxone. Addiction 2013;108(12):2141‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sanders 2013 {published data only}
- Sanders NC, Mancino MJ, Gentry WB, Guise JB, Bickel WK, Thostenson J, et al. Randomized, placebo‐controlled pilot trial of gabapentin during an outpatient, buprenorphine‐assisted detoxification procedure. Experimental and Clinical Psychopharmacology 2013;21(4):294‐302. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sheard 2009 {published data only}
- Sheard L, Adams CE, Wright NMJ, El‐Sayeh H, Dalton R, Tompkins CNE. The Leeds Evaluation of Efficacy of Detoxification Study (LEEDS) prisons project pilot study: protocol for a randomised controlled trial comparing dihydrocodeine and buprenorphine for opiate detoxification. Trials 2007;8:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheard L, Wright NMJ, El‐Sayeh HG, Adams CE, Li R, Tompkins CNE. The Leeds Evaluation of Efficacy of Detoxification Study (LEEDS) prisons project: a randomised controlled trial comparing dihydrocodeine and buprenorphine for opiate detoxification. Substance Abuse Treatment, Prevention, and Policy 2009;4:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sigmon 2004 {published data only}
- Sigmon SC, Wong CJ, Chausmer AL, Liebson IA, Bigelow GE. Evaluation of an injection depot formulation of buprenorphine: placebo comparison. Addiction 2004;99(11):1439‐49. [DOI] [PubMed] [Google Scholar]
Sullivan 2015 {published data only}
- Sullivan MA, Bisaga A, Carpenter K, Mariani JJ, Mishlen K, Nunes EV. Long‐acting injectable naltrexone induction: a randomized trial of outpatient opioid detoxification with naltrexone vs buprenorphine. Drug and Alcohol Dependence 2015;146:e112. [DOI] [PMC free article] [PubMed] [Google Scholar]
Tompkins 2014 {published data only}
- Tompkins D, Smith MT, Mintzer MZ, Campbell CM, Strain EC. A double blind, within subject comparison of spontaneous opioid withdrawal from buprenorphine versus morphine. Journal of Pharmacology and Experimental Therapeutics 2014;348(2):217‐26. [DOI] [PMC free article] [PubMed] [Google Scholar]
Umbricht 1999 {published data only}
- Umbricht A, Montoya ID, Hoover DR, Demuth KL, Chiang CT, Preston KL. Naltrexone shortened opioid detoxification with buprenorphine. Drug and Alcohol Dependence 1999;56(3):181‐90. [DOI] [PubMed] [Google Scholar]
Weiss 2010 {published data only}
- Weiss RD, Potter JS, Fiellin DA, Byrne M, Connery HS, Dickinson W, et al. Adjunctive counseling during brief and extended buprenorphine‐naloxone treatment for prescription opioid dependence: a 2‐phase randomized controlled trial. Archives of General Psychiatry 2011;68(12):1238‐46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weiss RD, Potter JS, Provost SE, Huang Z, Jacobs P, Hasson A, et al. A multi‐site, two‐phase, Prescription Opioid Addiction Treatment Study (POATS): Rationale, design, and methodology. Contemporary Clinical Trials 2010;31(2):189‐99. [DOI] [PMC free article] [PubMed] [Google Scholar]
White 2001 {published data only}
- White R, Alcorn R, Feinmann C. Two methods of community detoxification from opiates: an open‐label comparison of lofexidine and buprenorphine. Drug and Alcohol Dependence 2001;65(1):77‐83. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Williams 2002 {published data only}
- Williams H, Remedios A, Oyefeso A, Bennett J. Buprenorphine detoxification treatment for heroin dependence: a preliminary experience in an outpatient setting. Irish Journal of Psychological Medicine 2002;19(3):80‐3. [DOI] [PubMed] [Google Scholar]
Woody 2008 {published data only}
- Hill KP, Bennett HE, Griffin ML, Connery HS, Fitzmaurice GM, Subramaniam G, et al. Association of cannabis use with opioid outcomes among opioid‐dependent youth. Drug and Alcohol Dependence 2013;132(1‐2):342‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meade CS, Weiss RD, Fitzmaurice GM, Poole SA, Subramaniam GA, Patkar AA, et al. HIV risk behavior in treatment‐seeking opioid‐dependent youth: results from a NIDA clinical trials network multisite study. Journal of Acquired Immune Deficiency Syndromes 2010;55(1):65‐72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Polsky D, Glick HA, Yang J, Subramaniam GA, Poole SA, Woody GE. Cost‐effectiveness of extended buprenorphine‐naloxone treatment for opioid‐dependent youth: data from a randomized trial. Addiction 2010;105(9):1616‐24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Subramaniam GA, Warden D, Minhajuddin A, Fishman MJ, Stitzer ML, Adinoff B, et al. Predictors of abstinence: National Institute of Drug Abuse multisite buprenorphine/naloxone treatment trial in opioid‐dependent youth. Journal of the American Academy of Child and Adolescent Psychiatry 2011;50(11):1120‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Warden D, Subramaniam GA, Carmody T, Woody GE, Minhajuddin A, Poole SA, et al. Predictors of attrition with buprenorphine/naloxone treatment in opioid dependent youth. Addictive Behaviors 2012;37(9):1046‐53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilcox CE, Bogenschutz MP, Nakazawa M, Woody GE. Compensation effects on clinical trial data collection in opioid‐dependent young adults. American Journal of Drug and Alcohol Abuse 2012;38(1):81‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woody GE, Poole SA, Subramaniam G, Dugosh K, Bogenschutz M, Abbott P, et al. Extended vs short‐term buprenorphine‐naloxone for treatment of opioid‐addicted youth. JAMA 2008;300(17):2003‐11. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wright 2007 {published data only}
- Oldham NS, Wright NM, Adams CE, Sheard L, Tompkins CN. The Leeds Evaluation of Efficacy of Detoxification Study (LEEDS) project: an open‐label pragmatic randomised control trial comparing the efficacy of differing therapeutic agents for primary care detoxification from either street heroin or methadone [ISRCTN07752728]. BMC Family Practice 2004;5(1):9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wright NM, Sheard L, Tompkins CN, Adams CE, Allgar VL, Oldham NS. Buprenorphine versus dihydrocodeine for opiate detoxification in primary care: a randomised controlled trial. BMC Family Practice 2007;8:3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Zhang 1993 {published data only}
- Zhang R, Li J, Wan W. Comparative study of buprenorphine and methadone in the treatment of heroin addicts. Chinese Journal of Neurological and Mental Diseases 1993;19(5):295‐96. [Google Scholar]
Additional references
Amato 2011
- Amato L, Minozzi S, Davoli M, Vecchi S, Ferri M, Mayet S. Psychosocial and pharmacological treatments versus pharmacological treatments for opioid detoxification. Cochrane Database of Systematic Reviews 2011, Issue 9. [DOI: 10.1002/14651858.CD005031.pub2] [DOI] [PubMed] [Google Scholar]
Amato 2013
- Amato L, Davoli M, Ferri M, Ali R. Methadone at tapered doses for the management of opioid withdrawal. Cochrane Database of Systematic Reviews 2013, Issue 2. [DOI: 10.1002/14651858.CD003409.pub4] [DOI] [Google Scholar]
Ang‐Lee 2006
- Ang‐Lee K, Oreskovich MR, Saxon AJ, Jaffe C, Meredith C, Ellis ML, et al. Single dose of 24 milligrams of buprenorphine for heroin detoxification: an open‐label study of five inpatients. Journal of Psychoactive Drugs 2006;38(4):505‐12. [DOI] [PubMed] [Google Scholar]
Atkins 2004
- Atkins D, Best D, Briss PA, Eccles M, Falck‐Ytter Y, Flottorp S, et al. GRADE working group. Grading quality of evidence and strength of recommendations. BMJ 2004;328(7454):1490‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Banys 1994
- Banys P, Clark HW, Tusel DJ, Sees K, Stewart P, Mongan L, et al. An open trial of low dose buprenorphine in treating methadone withdrawal. Journal of Substance Abuse Treatment 1994;11(1):9‐15. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Broers 2000
- Broers B, Giner F, Dumont P, Mino A. Inpatient opiate detoxification in Geneva: follow‐up at 1 and 6 months. Drug and Alcohol Dependence 2000;58(1):85‐92. [DOI] [PubMed] [Google Scholar]
Cameron 2001
- Cameron D, Allen D, Galway K. A pilot study of the effectiveness of buprenorphine and methadone as detoxication agents when choice is given to the consumer. Journal of Substance Use 2001;6(2):101‐9. [Google Scholar]
Chawarski 2005
- Chawarski MC, Moody DE, Pakes J, O'Connor PG, Schottenfeld RS. Buprenorphine tablet versus liquid: a clinical trial comparing plasma levels, efficacy and symptoms. Journal of Substance Abuse Treatment 2005;29:307‐12. [DOI] [PubMed] [Google Scholar]
Chiang 2003
- Chiang CN, Hawks RL. Pharmacokinetics of the combination tablet of buprenorphine and naloxone. Drug and Alcohol Dependence 2003;70(Suppl):S39‐S47. [DOI] [PubMed] [Google Scholar]
Day 2005
- Day E, Ison J, Strang J. Inpatient versus other settings for detoxification for opioid dependence. Cochrane Database of Systematic Reviews 2005, Issue 2. [DOI: 10.1002/14651858.CD004580.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Elkader 2005
- Elkader A, Sproule B. Buprenorphine: clinical pharmacokinetics in the treatment of opioid dependence. Clinical Pharmacokinetics 2005;44(7):661‐80. [DOI] [PubMed] [Google Scholar]
Farrell 1994
- Farrell M. Opiate withdrawal. Addiction 1994;89(11):1471‐5. [DOI] [PubMed] [Google Scholar]
Gossop 1988
- Gossop M. Clonidine and the treatment of the opiate withdrawal syndrome. Drug and Alcohol Dependence 1988;21(3):253‐9. [DOI] [PubMed] [Google Scholar]
Gossop 1989a
- Gossop M, Green L, Phillips G, Bradley B. Lapse, relapse and survival among opiate addicts after treatment. A prospective follow‐up study. British Journal of Psychiatry 1989;154:348‐53. [DOI] [PubMed] [Google Scholar]
Gossop 1989b
- Gossop M, Griffiths P, Bradley B, Strang J. Opiate withdrawal symptoms in response to 10 day and 21 day methadone withdrawal programmes. British Journal of Psychiatry 1989;154:360‐3. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Gowing 2009
- Gowing L, Ali R, White J. Opioid antagonists with minimal sedation for the management of opioid withdrawal. Cochrane Database of Systematic Reviews 2009, Issue 4. [DOI: 10.1002/14651858.CD002021.pub3] [DOI] [Google Scholar]
Gowing 2010
- Gowing LR, Ali RL, White JM. Opioid antagonists under heavy sedation or anaesthesia for opioid withdrawal. Cochrane Database of Systematic Reviews 2010, Issue 2. [DOI: 10.1002/14651858.CD002022.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Gowing 2014
- Gowing L, Ali R, Dunlop A, Farrell M, Lintzeris N. National Guidelines for Medication‐Assisted Treatment of Opioid Dependence. Commonwealth of Australia, 2014. www.nationaldrugstrategy.gov.au/internet/drugstrategy/Publishing.nsf/content/ng‐mat‐op‐dep accessed prior to 18 January 2017. [Online ISBN: 978‐1‐74241‐945‐9]
Gowing 2015
- Gowing LR, Ali RL, Allsop S, Marsden J, Turf EE, West R, et al. Global statistics on addictive behaviours: 2014 status report. Addiction 2015;110(6):904‐19. [DOI: 10.1111/add.12899] [DOI] [PubMed] [Google Scholar]
Gowing 2016
- Gowing LR, Farrell M, Ali RL, White JM. Alpha2‐adrenergic agonists for the management of opioid withdrawal. Cochrane Database of Systematic Reviews 2016, Issue 5. [DOI: 10.1002/14651858.CD002024.pub5] [DOI] [PMC free article] [PubMed] [Google Scholar]
GRADEpro GDT [Computer program]
- GRADE Working Group, McMaster University. GRADEpro GDT. Version accessed prior to 17 January 2017. Hamilton (ON): GRADE Working Group, McMaster University, 2014.
Guyatt 2008a
- Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck‐Ytter Y, Alonso‐Coello P, et al GRADE working group. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008;336(7560):924‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Guyatt 2008b
- Guyatt GH, Oxman AD, Kunz R, Vist GE, Falck‐Ytter Y, Schünemann HJ, GRADE Working Group. Rating quality of evidence and strength of recommendations: What is "quality of evidence" and why is it important to clinicians?. BMJ 2008;336(7651):955‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Guyatt 2011
- Guyatt G, Oxman AD, Akl EA, Kunz R, Vist G, Brozek J, et al GRADE working group. GRADE guidelines 1. Introduction‐GRADE evidence profiles and summary of findings tables. Journal of Clinical Epidemiology 2011;64(4):383‐94. [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Jaffe 1997
- Jaffe JH, Knapp CM, Ciraulo DA. Opiates: Clinical Aspects. In: Lowinson JH, Ruiz P, Millman RB, Langrod JG editor(s). Substance Abuse: A Comprehensive Textbook. 3rd Edition. Baltimore: Williams & Wilkins, 1997. [Google Scholar]
Johnson 2003
- Johnson RE, Strain EC, Amass L. Buprenorphine: how to use it right. Drug and Alcohol Dependence 2003;70(Suppl 2):S59‐S77. [DOI] [PubMed] [Google Scholar]
Kleber 1982
- Kleber HD, Riordan CE. The treatment of narcotic withdrawal: a historical review. Journal of Clinical Psychiatry 1982;43(6):30‐4. [PubMed] [Google Scholar]
Kutz 2002
- Kutz I, Reznik V. Heroin detoxification with a single high dose of buprenorphine. Israel Journal of Psychiatry and Related Sciences 2002;39(2):113‐9. [PubMed] [Google Scholar]
Lanier 2007
- Lanier RK, Umbricht A, Harrison JA, Nuwayser ES, Bigelow GE. Evaluation of a transdermal buprenorphine formulation in opioid detoxification. Addiction 2007;102(10):1648‐56. [DOI] [PubMed] [Google Scholar]
Lanier 2008
- Lanier RK, Umbricht A, Harrison JA, Nuwayser ES, Bigelow GE. Opioid detoxification via single 7‐day application of a buprenorphine transdermal patch: an open‐label evaluation. Psychopharmacology (Berlin) 2008;198(2):149‐58. [DOI] [PMC free article] [PubMed] [Google Scholar]
Larance 2011
- Larance B, Degenhardt L, Lintzeris N, Bell J, Winstock A, Dietze P, et al. Post‐marketing surveillance of buprenorphine‐naloxone in Australia: diversion, injection and adherence with supervised dosing. Drug and Alcohol Dependence 2011;118(2‐3):265‐73. [DOI] [PubMed] [Google Scholar]
Lintzeris 2013
- Lintzeris N, Leung SY, Dunlop AJ, Larance B, White N, Rivas GR, et al. A randomised controlled trial of sublingual buprenorphine‐naloxone film versus tablets in the management of opioid dependence. Drug and Alcohol Dependence 2013;131(1‐2):119‐26. [DOI] [PubMed] [Google Scholar]
Lipton 1983
- Lipton D, Maranda M. Detoxification from heroin dependency: an overview of method and effectiveness. Advances in Alcohol and Substance Abuse 1983;2(1):31‐55. [Google Scholar]
Mark 2001
- Mark TL, Woody GE, Juday T, Kleber HD. The economic costs of heroin addiction in the United States. Drug and Alcohol Dependence 2001;61(2):195‐206. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Mattick 1996
- Mattick RP, Hall W. Are detoxification programmes effective?. Lancet 1996;347(8994):97‐100. [DOI] [PubMed] [Google Scholar]
Mattick 2014
- Mattick RP, Breen C, Kimber J, Davoli M. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database of Systematic Reviews 2014, Issue 2. [DOI: 10.1002/14651858.CD002207.pub4] [DOI] [Google Scholar]
Minozzi 2014
- Minozzi S, Amato L, Davoli M. Detoxification treatments for opiate dependent adolescents. Cochrane Database of Systematic Reviews 2014, Issue 4. [DOI: 10.1002/14651858.CD006749.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Phillips 1986
- Phillips GT, Gossop M, Bradley B. The influence of psychological factors on the opiate withdrawal syndrome. British Journal of Psychiatry 1986;149:235‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Preston 1985
- Preston KL, Bigelow GE. Pharmacological advances in addiction treatment. International Journal of the Addictions 1985;20(6‐7):845‐67. [DOI] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Satel 1993
- Satel SL, Kosten TR, Schuckit MA, Fischman MW. Should protracted withdrawal from drugs be included in DSM‐IV?. American Journal of Psychiatry 1993;150(5):695‐704. [DOI] [PubMed] [Google Scholar]
Sobel 2004
- Sobel B‐FX, Sigmon SC, Walsh SL, Johnson RE, Liebson IA, Nuwayser ES, et al. Open‐label trial of an injection depot formulation of buprenorphine in opioid detoxification. Drug and Alcohol Dependence 2004;73(1):11‐22. [DOI] [PubMed] [Google Scholar]
Strain 2004
- Strain EC, Moody DE, Stoller KB, Walsh SL, Bigelow GE. Relative bioavailability of different buprenorphine formulations under chronic dosing conditions. Drug and Alcohol Dependence 2004;74:37‐43. [DOI] [PubMed] [Google Scholar]
Strang 1999
- Strang J, Griffiths P, Powis B, Gossop M. Heroin chasers and heroin injectors: differences observed in a community sample in London, UK. American Journal on Addictions 1999;8(2):148‐60. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
Tetrault 2009
- Tetrault JM, O'Connor PG. Management of opioid intoxication and withdrawal. In: Ries RK, Fiellin DA, Miller SC, Siatz R editor(s). Principles of Addiction Medicine. 4th Edition. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins, 2009:589‐606. [Google Scholar]
Vaillant 1988
- Vaillant GE. What can long‐term follow‐up teach us about relapse and prevention of relapse in addiction?. British Journal of Addiction 1988;83(10):1147‐57. [DOI] [PubMed] [Google Scholar]
WHO 2009
- World Health Organization. Guidelines for the Psychosocially Assisted Pharmacological Treatment of Opioid Dependence. Geneva: World Health Organization, 2009. [ISBN 978 92 4 154754 3] [PubMed] [Google Scholar]
References to other published versions of this review
Gowing 2004
- Gowing L, Ali R, White JM. Buprenorphine for the management of opioid withdrawal. Cochrane Database of Systematic Reviews 2004, Issue 4. [DOI: 10.1002/14651858.CD002025.pub4] [DOI] [PubMed] [Google Scholar]
Gowing 2006
- Gowing L, Ali R, White JM. Buprenorphine for the management of opioid withdrawal. Cochrane Database of Systematic Reviews 2006, Issue 2. [DOI: 10.1002/14651858.CD002025.pub4] [DOI] [PubMed] [Google Scholar]
Gowing 2009a
- Gowing L, Ali R, White JM, Mbewe D. Buprenorphine for the management of opioid withdrawal. Cochrane Database of Systematic Reviews 2009, Issue 3. [DOI: 10.1002/14651858.CD002025.pub4] [DOI] [PubMed] [Google Scholar]