

Abstract
Background
Short (or small) saphenous vein (SSV) varices occur as a result of an incompetent sapheno‐popliteal junction, where the SSV joins the popliteal vein, resulting in reflux in the SSV; they account for about 15% of varicose veins. Untreated varicose veins may sometimes lead to ulceration of the leg, which is difficult to manage. Traditionally, treatment was restricted to surgery or conservative management. Since the 1990s, however, a number of minimally invasive techniques have been developed; these do not normally require a general anaesthetic, are day‐case procedures with a quicker return to normal activities and avoid the risk of wound infection which may occur following surgery. Nerve injury remains a risk with thermal ablation, but in cases where it does occur, the injury tends to be transient.
Objectives
To compare the effectiveness of endovenous laser ablation (EVLA), radiofrequency ablation (RFA) and ultrasound‐guided foam sclerotherapy (UGFS) versus conventional surgery in the treatment of SSV varices.
Search methods
The Cochrane Vascular Information Specialist searched the Specialised Register (last searched 17 March 2016) and the Cochrane Central Register of Controlled Trials (CENTRAL; 2016, Issue 2). We searched clinical trials databases for details of ongoing or unpublished studies.
Selection criteria
We considered all randomised controlled trials (RCTs) comparing EVLA, endovenous RFA or UGFS with conventional surgery in the treatment of SSV varices for inclusion.
Data collection and analysis
We independently reviewed, assessed and selected trials that met the inclusion criteria; any disagreements were resolved by discussion. We extracted data and used the Cochrane's tool for assessing risk of bias. When the data permitted, we performed either fixed‐effect meta‐analyses with odds ratios (ORs) and 95% confidence intervals (CIs) or random‐effects meta‐analyses where there was moderate to significant heterogeneity.
Main results
We identified three RCTs, all of which compared EVLA with surgery; one also compared UGFS with surgery. There were no trials comparing RFA with surgery. The EVLA versus surgery comparison included 311 participants: 185 received EVLA and 126 received surgery. In the UGFS comparison, each treatment group contained 21 people. For several outcomes in the EVLA comparison, only a single study provided relevant data; as a result, the current review is limited in its ability to demonstrate meaningful results for some planned outcomes. The quality of evidence according to GRADE was moderate to low for the outcome measures in the EVLA versus surgery comparison, but low for the UGFS versus surgery comparison. Reasons for downgrading in the EVLA versus surgery comparison were risk of bias (for some outcomes, the outcome assessors were not blinded; and in one study the EVLA‐surgery allocation of 2:1 did not appear to be prespecified); imprecision (data were only available from a single small study and the CIs were relatively wide); indirectness (one trial reported results at six months rather than one year and was inadequately powered for SSV varices‐only analysis). Reasons for downgrading in the UGFS versus surgery comparison were imprecision (only one trial offered UGFS and several participants were missing from the analysis) and a limitation in design (the study was inadequately powered for SSV participants alone).
For the EVLA versus surgery comparison, recanalisation or persistence of reflux at six weeks occurred less frequently in the EVLA group than in the surgery group (OR 0.07, 95% CI 0.02 to 0.22; I2 = 51%; 289 participants, 3 studies, moderate‐quality evidence). Recurrence of reflux at one year was also less frequent in the EVLA group than in the surgery group (OR 0.24, 95% CI 0.07 to 0.77; I2 = 0%; 119 participants, 2 studies, low‐quality evidence). For the outcome clinical evidence of recurrence (i.e. presence of new visible varicose veins) at one year, there was no difference between the two treatment groups (OR 0.54, 95% CI 0.17 to 1.75; 99 participants, 1 study, low‐quality evidence). Four participants each in the EVLA and surgery groups required reintervention due to technical failure (99 participants, 1 study, moderate‐quality evidence). There was no difference between the two treatment groups for disease‐specific quality of life (QoL) (Aberdeen Varicose Veins Questionnaire) either at six weeks (mean difference (MD) 0.15, 95% CI ‐1.65 to 1.95; I2 = 0%; 265 participants, 2 studies, moderate‐quality evidence), or at one year (MD ‐1.08, 95% CI ‐3.39 to 1.23; 99 participants, 1 study, low‐quality evidence). Main complications reported at six weeks were sural nerve injury, wound infection and deep venous thrombosis (DVT) (one DVT case in each treatment group; EVLA: 1/161, 0.6%; surgery 1/104, 1%; 265 participants, 2 studies, moderate‐quality evidence).
For the UGFS versus surgery comparison, there were insufficient data to detect clear differences between the two treatment groups for the two outcomes recanalisation or persistence of reflux at six weeks (OR 0.34, 95% CI 0.06 to 2.10; 33 participants, 1 study, low‐quality evidence), and recurrence of reflux at one year (OR 1.19, 95% CI 0.29 to 4.92; 31 participants, 1 study, low‐quality evidence). No other outcomes could be reported for this comparison because the study data were not stratified according to saphenous vein.
Authors' conclusions
Moderate‐ to low‐quality evidence exists to suggest that recanalisation or persistence of reflux at six weeks and recurrence of reflux at one year are less frequent when EVLA is performed, compared with conventional surgery. For the UGFS versus conventional surgery comparison, the quality of evidence is assessed to be low; consequently, the effectiveness of UGFS compared with conventional surgery in the treatment of SSV varices is uncertain. Further RCTs for all comparisons are required with longer follow‐up (at least five years). In addition, measurement of outcomes such as recurrence of reflux, time taken to return to work, duration of procedure, pain, etc., and choice of time points during follow‐up should be standardised such that future trials evaluating newer technologies can be compared efficiently.
Plain language summary
Endovenous ablation therapy (laser or radiofrequency) or foam sclerotherapy versus open surgery for the treatment of short saphenous varicose veins
Background
Varicose veins (varices) are enlarged veins occurring below the skin's surface, usually in the legs. One‐third of the UK population may be affected. They can be painful and itchy, the surrounding skin may change colour, and occasionally they may bleed; in some people, untreated varicose veins may lead to ulceration. Varicose veins occur due to leaky valves within the veins. Traditionally, they were treated with surgery to remove the veins. Newer techniques require neither vein removal, nor a general anaesthetic; they may involve less pain after the procedure and have a lower risk of complications, resulting in quicker recovery and return to normal activities. Endovenous laser ablation (EVLA) and radiofrequency ablation (RFA) are methods that seal the main leaking vein. They are performed using a local anaesthetic; a probe is passed into the vein: either a tiny laser or radiofrequency makes the wall of the vein heat up causing the vein to clot off and seal. With ultrasound‐guided foam sclerotherapy (UGFS), a foam is injected into the veins; the foam pushes the blood away, causing thickening and scarring of the inside of the vein so that it becomes blocked.
Study characteristics and key results
We searched for all randomised controlled trials to March 2016 that compared at least one of the newer techniques with surgery, when treating short saphenous vein (SSVs; found in the lower leg) varices. We found three trials comparing EVLA with surgery; one trial compared UGFS with surgery, but none reported RFA. The main measures (outcomes) were recanalisation (blood flowing in the veins again) or persistence of reflux (due to failure of treatment) at six weeks; recurrence of reflux at one year; clinical evidence of recurrence (presence of new varicose veins) at one year; repeat treatment due to failure; quality of life (QoL) at six weeks and one year after the treatment; and complications after treatment.
The EVLA versus surgery comparison included 311 participants: 185 received EVLA and 126 received surgery. In the UGFS comparison, each treatment group contained 21 people. For several outcomes in the EVLA comparison, only one study provided data; consequently, this review has limited ability to demonstrate meaningful results for some planned outcomes.
EVLA versus surgery: there was less recanalisation or persistence of reflux at six weeks and less recurrence of reflux at one year in the EVLA group; however, there were insufficient data to report clear differences in clinical recurrence at one year. One trial reported four participants in each group required further treatment. There was no difference between treatments in QoL. Although some participants had postoperative complications (e.g., sural nerve injury (the sural nerve is in the calf), infection, deep venous thrombosis (DVT; blood clots in veins), inflammation of the wall of the vein), most complications improved without treatment and the two cases of DVT resolved after treatment with medicines.
UGFS versus surgery: there were insufficient data to detect clear differences between treatment groups for recanalisation or persistence of reflux at six weeks and recurrence of reflux at one year. Data were not available for other outcomes.
Quality of the evidence
For the EVLA comparison, the quality of evidence was moderate for recanalisation or persistence of reflux, QoL and complications, all at six weeks, and retreatment due to technical failure, but low for recurrence of reflux, QoL and clinical evidence of recurrence after one year. The quality of evidence was downgraded due to imprecision (small number of trials with few participants) and bias (outcome assessors aware of treatment allocation in some studies and one study recruited insufficient participants with SSV). For the UGFS comparison, evidence was low quality because one study (with few participants with SSV) offered UGFS and several participants were missing from the analysis.
The main difficulty with this review was lack of data: we found a small number of trials and two trials had substantial amounts of unavailable data. Further well‐designed studies are needed.
Summary of findings
Background
Description of the condition
Abnormally dilated veins are termed varicose veins (varices). They are commonly noted in the lower limbs and may be seen either as dilated and tortuous veins or as palpable veins under the skin. Approximately one‐third of the population in the UK is affected by varicose veins (NICE 2013).
Varicose veins predominantly occur as a result of either an incompetent sapheno‐femoral junction, where the great (long) saphenous vein (GSV) joins the femoral vein, or an incompetent sapheno‐popliteal junction (SPJ), where the short (small) saphenous vein (SSV) joins the popliteal vein. Incompetence of the sapheno‐femoral junction leads to reflux in the GSV and incompetence in the SPJ leads to reflux in the SSV. Approximately 15% of varicose veins are due to SSV reflux (Almgren 1990).
In addition to the obvious finding of abnormally dilated veins, participants with varicose veins may present with a variety of symptoms such as pain, itching and skin changes. Untreated varicose veins in some of these participants may lead to ulceration, which is difficult to manage.
Varicose veins due to SSV incompetence are traditionally managed by a conventional surgical procedure, where an incision is made in the popliteal fossa, and the SSV and SPJ are identified. The SPJ is then disconnected and a short segment of the SSV is either resected or stripped. Two‐thirds of surgeons in the UK perform conventional surgery on the SPJ as described; however, some variations do exist (Winterborn 2004). Although this procedure is considered the gold standard, there is a complication rate of 5% (Winterborn 2004), and associated risks such as recurrence and disabling nerve injury make this surgery challenging (Sam 2004).
Description of the intervention
Since the 1990s, minimally invasive techniques have been developed to treat sapheno‐femoral junction and GSV incompetence. These include endovenous laser ablation (EVLA), radiofrequency ablation (RFA) and ultrasound‐guided foam sclerotherapy (UGFS). These techniques have been extensively used in the treatment of sapheno‐femoral junction and GSV reflux (Nesbitt 2014; Rigby 2009), and the National Institute for Health and Care Excellence (NICE) clinical guideline considers them safe in the management of varicose veins (NICE 2013).
In EVLA, under ultrasound guidance, a bare‐tipped or jacketed laser optical fibre is inserted into the vein from a distal point towards the junction, gentle pressure applied over the vein and the laser activated. This results in heat coagulation of the blood in the vein. The fibre is then slowly withdrawn and the vein becomes occluded.
In RFA, under ultrasound guidance, a catheter electrode is inserted into the vein and the tip placed close to the junction. When activated, heat generated from the electrode results in closure of the vein.
In UGFS, a sclerosant agent turned into foam is injected into the affected vein, where the foam displaces the blood. The irritant nature of the sclerosant causes inflammation of the endothelium and sub‐endothelium layers of the vein wall, resulting in fibrosis and occlusion of the vein.
EVLA and RFA are day‐case procedures and performed under tumescent local anaesthesia, where local anaesthetic is injected around the vein, along the length of intervention. UGFS is also a day‐case procedure and does not require any anaesthesia. Patients are allowed to ambulate immediately following the procedure and are discharged within hours of treatment. Furthermore, the risks of wound infection and nerve injury may be abated or significantly reduced due to the mode of these interventions.
Why it is important to do this review
In addition to the known risks of conventional surgery, there is concern about its success in dealing with SPJ and SSV reflux. One review comparing treatment for SSV varices showed variation in the success rate of conventional surgery, which ranged between 24% and 100% (Tellings 2011). Therefore, it is important to explore the alternative treatment modalities, such as EVLA, RFA or UGFS, which are now commonly used in the management of GSV varices. The Tellings 2011 review included non‐randomised, heterogeneous studies; however, it did show that minimally invasive techniques tend to have a higher success rate compared to conventional surgery.
EVLA and RFA have been shown to be as effective as conventional surgery in the management of GSV varices (Nesbitt 2014). However, their role in the management of SSV varices has not been thoroughly evaluated. The outcomes of this review, which will assess the role of EVLA, RFA and UGFS, will be useful in clinical decision‐making.
Objectives
To compare the effectiveness of endovenous laser ablation (EVLA), radiofrequency ablation (RFA) and ultrasound‐guided foam sclerotherapy (USFS) versus conventional surgery in the treatment of SSV varices.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) comparing EVLA or RFA or UGFS with conventional surgery in the treatment of SSV varices. We accepted all published RCTs and presumed operator competence, unless defined in the article as a learning‐curve report.
Types of participants
We included men and women aged 18 years and over who received treatment for SSV varices.
Types of interventions
Interventions
Endovenous laser ablation therapy (EVLA).
Endovenous radiofrequency ablation (RFA).
Ultrasound‐guided foam sclerotherapy (UGFS).
Comparator
Conventional surgery.
Types of outcome measures
Primary outcomes
Recanalisation or persistence of reflux at six weeks.
Recurrence of reflux at one year.
We considered persistence of reflux at six weeks after the procedure as being due to technical failure of the intervention. We used duplex ultrasound (DUS) reflux of greater than 0.5 seconds as the definition for reflux.
Clinical evidence of recurrence (i.e. presence of new visible varicose veins).
Reintervention (due to technical failure).
We considered failure to obliterate as technical failure and not as recurrence, and any intervention to deal with this as reintervention.
We distinguished between further treatment of the SSV and adjuvant tributary treatment (e.g. delayed phlebectomy).
Secondary outcomes
Quality of life (QoL, determined by pre‐ and postprocedure QoL scores).
Postoperative pain.
We assessed pain using either visual analogue scale (VAS) scores, postoperative analgesia requirements or participant complaints, as reported by the trialists.
Complications (such as postprocedural deep venous thrombosis (DVT), thermal injury, sural nerve injury, wound infection, haematoma, pigmentation or skin bruising, and phlebitis).
We regarded postoperative cutaneous injury or sural nerve injury as thermal‐related injuries.
Healing of ulcers.
Hospital stay.
Return to work.
In addition, we reported on the type of anaesthesia and the duration of the procedure, if these data were available.
Search methods for identification of studies
Electronic searches
The Cochrane Vascular Information Specialist (CIS) searched the Specialised Register (March 2016). In addition, the CIS searched the Cochrane Register of Studies (CRS) (www.metaxis.com/CRSWeb/Index.asp) (Cochrane Central Register of Controlled Trials (CENTRAL) (2016, Issue 2)). See Appendix 1 for details of the search strategy used to search the CRS. The Specialised Register is maintained by the CIS and is constructed from weekly electronic searches of MEDLINE, Embase, CINAHL and AMED, and through handsearching relevant journals. The full list of the databases, journals and conference proceedings which have been searched, as well as the search strategies used, are described in the Specialised Register section of the Cochrane Vascular module in the Cochrane Library (www.cochranelibrary.com).
The CIS searched the following trial databases for details of ongoing and unpublished studies using the terms in Appendix 2:
World Health Organization International Clinical Trials Registry (apps.who.int/trialsearch/);
ClinicalTrials.gov (clinicaltrials.gov/);
ISRCTN Register (www.isrctn.com/).
Searching other resources
We scrutinised the reference lists of relevant articles retrieved by the electronic searches for additional citations.
In addition, we checked reference lists in published reviews on varicose veins, and various health services research‐related resources via the internet. These included health economics and health technology assessment (HTA) organisations and guideline‐producing agencies: NICE (guidance.nice.org.uk/) and the Scottish Intercollegiate Guidelines Network (SIGN) (www.sign.ac.uk/guidelines/index.html). Further, we sought trial reports through examination of the proceedings from the following meetings:
Vascular Society of Great Britain and Ireland (2005, 2007 to 2014);
Association of Surgeons of Great Britain and Ireland (2003 to 2015);
British Society of Interventional Radiology (2007 to 2015);
American Venous Forum (2007 to 2016);
The Society for Vascular Surgery (2009 to 2015);
European Society for Vascular Surgery (2007), and contents pages of all issues of the European Journal of Vascular and Endovascular Surgery (January 2003 to April 2016).
Data collection and analysis
Selection of studies
Two review authors (SP and MH) independently evaluated trials for inclusion. Any disagreements were resolved by discussion.
Data extraction and management
Two review authors (SP and MH) independently extracted data using a proforma designed by Cochrane Vascular. Any disagreements were resolved by discussion.
Assessment of risk of bias in included studies
Two review authors (SP and MH) independently assessed the quality of the included studies by using Cochrane's 'Risk of bias' tool (Higgins 2011). This tool provides a standard protocol for allowing judgements to be made on sequence generation, allocation methods, blinding, incomplete outcome data, selective outcome reporting and any other relevant biases. For each of these six items, we assessed the risk of bias as 'low risk', 'high risk' or 'unclear risk', with the 'unclear risk' of bias indicating either a lack of information or uncertainty over the potential for bias. Any disagreements were resolved by discussion with the Managing Editor of Cochrane Vascular.
Measures of treatment effect
We used odds ratio (OR) and 95% confidence interval (CI) as the measure of treatment effect for each dichotomous outcome. Where there were sufficient data, we calculated a summary statistic for each outcome using either a fixed‐effect or random‐effects model. We analysed continuous scales of measurement in continuous form (i.e. mean difference, MD) and 95% CI.
Unit of analysis issues
For all outcomes, we considered each individual participant as the unit of analysis.
Dealing with missing data
Where possible, we carried out analysis on an intention‐to‐treat (ITT) basis. In cases of incomplete or missing data from trials, we contacted the trialists for the required information. Where such an attempt to obtain information was unsuccessful, we presented the available data without undertaking meta‐analysis.
Assessment of heterogeneity
We assessed heterogeneity in the data and cautiously explored it using the characteristics of the studies, particularly assessments of quality. We used the I2 statistic to assess heterogeneity with an I2 value of 25% to 50% indicating low heterogeneity, 50% to 75% moderate heterogeneity and greater than 75% significant heterogeneity.
Assessment of reporting biases
We intended to test for publication bias using funnel plots if we included more than 10 studies in the review (Higgins 2011).
Data synthesis
Where direct comparisons could be made, we presented data as OR or MD. We examined studies for heterogeneity and used a random‐effects model in case of significant heterogeneity (I2 > 75%); otherwise we used a fixed‐effect model. We presented data that could not be pooled in tabular form. We performed statistical analyses according to the statistical guidelines for reviews outlined in Cochrane Vascular's module using Review Manager 5 (RevMan 2014).
Subgroup analysis and investigation of heterogeneity
We intended to analyse foam sclerotherapy as a generic procedure unless we identified significant differences between trials reporting outcomes for different agents. In such a case, we planned to perform a subgroup analysis.
For EVLA, we planned to perform a subgroup analysis of 800 nm to 980 nm versus 1000 nm to 1500 nm wavelengths, if sufficient data were available.
We also planned to note optical fibre tip data and to perform a subgroup analysis if sufficient data were available.
Sensitivity analysis
If any trials were judged to be of high risk of bias, we planned to perform a sensitivity analysis to assess outcomes with and without the trials that were of high risk of bias.
If participants in some of the identified trials had undergone simultaneous treatment for both SSV as well as GSV incompetence, we planned to perform a sensitivity analysis (where possible) excluding such participants.
We planned to undertake sensitivity analyses by excluding those studies that were not adequately powered (e.g. if a trial included participants with GSV varices or SSV varices or both, then only the subset of those recruited to the trial who had SSV varices would be included in this review, whereas the estimated sample‐size calculation for adequate power would be based on the inclusion of all participants).
'Summary of findings' tables
We used the GRADE approach to interpret findings (Langendam 2013), and for each comparison we presented the seven main outcomes of the review, using the GRADEpro GDT software (GRADEpro GDT 2015). We included the following outcomes in the 'Summary of findings' tables: recanalisation or persistence of reflux at six weeks; recurrence of reflux at one year; clinical evidence of recurrence at one year; reintervention (due to technical failure); disease‐specific QoL (Aberdeen Varicose Veins Questionnaire, AVVQ) at six weeks and one year; and complications at six weeks. For each outcome, the quality of the evidence was graded as high, moderate, low or very low; RCTs were graded as high‐quality evidence, and then downgraded by one level for each of the following factors that were present: limitations in the study design and implementation, indirectness of evidence, unexplained heterogeneity or inconsistency of results, imprecision of results and high probability of publication bias (GRADE Working Group 2004).
Results
Description of studies
Results of the search
See Figure 1.
1.
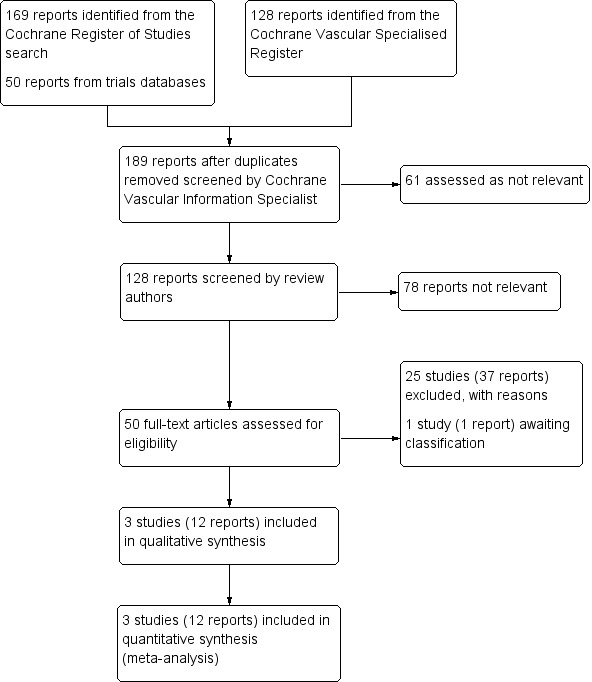
Study flow diagram.
After removing duplicates, the review authors initially screened 128 records by reviewing their title and abstract; we removed 78 records as they were not relevant and downloaded, read and assessed the full text of 50 records for eligibility. At this stage, we excluded 25 studies (37 records) (see Excluded studies and Characteristics of excluded studies for reasons for exclusion of the study). We included three studies (12 records) in the qualitative/quantitative analysis (see Included studies for a list of the records attached to each study, and Characteristics of included studies for a summary of each study). One study is awaiting classification, as we were unable to locate the paper.
Screening of health economics and HTA organisations, guideline‐producing agencies (NICE and SIGN) and proceedings of conferences for relevant abstracts did not result in any additional reports.
Included studies
Three studies fulfilled the necessary criteria for inclusion in this review (CLASS; HELP 2; VESPA). See Characteristics of included studies table for a summary of each study and an assessment of the risk of bias. All three studies were prospective RCTs: one recruited from a single UK hospital (HELP 2), one from two hospitals in the Netherlands (VESPA), and one from 11 hospitals in the UK (CLASS) (although only eight centres offered EVLA, so the EVLA versus surgery comparison was restricted to recruitment from these eight centres). Recruitment periods for the three studies ranged from October 2005 to October 2012.
Two studies solely recruited participants with SSV varices (HELP 2; VESPA), whereas CLASS recruited participants with GSV varices, SSV varices, or a combination of GSV and SSV varices. All three studies compared EVLA with conventional surgery, and CLASS compared UGFS with surgery. CLASS also compared UGFS with EVLA, but this comparison is not part of this review. No studies compared endovenous RFA with surgery.
The total number of participants included in the EVLA versus conventional surgery comparison was 311: 185 underwent EVLA and 126 underwent surgery. HELP 2 allocated 53 participants to EVLA and 53 participants to surgery; VESPA used a 2:1 allocation, with 118 participants undergoing EVLA and 57 undergoing surgery. In CLASS, 14 participants with SSV varices underwent EVLA and 16 underwent surgery in the eight‐hospital comparison. For the UGFS versus surgery comparison (in the 11‐centre CLASS study), there were 21 participants in each group.
The primary outcome measure for two studies was early technical success. This was defined in HELP 2 as the abolition of SSV reflux due to SPJ incompetence at six weeks after the procedure on DUS assessment (and reflux was defined as a retrograde flow of 1 second or more on spectral Doppler after augmentation); VESPA used thresholds of greater than 0.5 seconds to define incompetence of the superficial venous system (greater than 0.8 seconds in the case of deep veins). CLASS reported early technical success as a secondary outcome. CLASS defined reflux as greater than 1 second on DUS. HELP 2 also recorded clinical evidence of recurrence.
The primary outcome measures for the third study (CLASS) examined QoL at six months after treatment; participants completed three different questionnaires, one of which was disease‐specific, and the other two were generic QoL. HELP 2 reported results from the same three questionnaires as secondary outcomes, and VESPA reported results from the disease‐specific questionnaire, and one of the generic QoL questionnaires.
All studies reported on postoperative pain, although they each used different types of measurement scales and different time points; they each recorded time to return to work, procedure duration and postprocedural complications at six weeks. Two studies supplied information about postoperative analgesia (HELP 2; VESPA), length of stay in hospital (CLASS; HELP 2), participants' satisfaction with cosmetic appearance (HELP 2; VESPA), and Venous Clinical Severity Score (VCSS) (CLASS; HELP 2).
In HELP 2 and VESPA, there was a higher percentage of women (191/281, i.e. 68%) and the mean age of participants ranged from 47 years to 52 years. The length of follow‐up ranged from six weeks after the intervention to two years (HELP 2). The VESPA study has so far only published interim results for the first six weeks of follow‐up; in the trial register, the length of follow‐up is recorded as one year.
Excluded studies
See Characteristics of excluded studies table for the full list of excluded studies and the reasons for exclusion.
In total, we excluded 25 studies from this review (Ariyoshi 1996; Beale 2005; Campos 2015; Chant 1972; Compagna 2010; Doran 1975; Einarsson 1993; Figueiredo 2009; Flessenkamper 2012; HELP 1; Hobbs 1974; ISRCTN06552809; ISRCTN08060326; Iwamoto 2003; Jakobsen 1979; Kalodiki 2012; Liu 2011; MESSI trial 2014; Ogawa 2008; REACTIV trial 2006; Seddon 1973; Shouler 1989; VEDICO trial 1998; Wilhelmi 2009; Wright 2006). Some studies were excluded for multiple reasons. We summarise here the main reasons for exclusion. In four studies, the participant population being studied was different to the one specified in the protocol for this review (Beale 2005; Compagna 2010; HELP 1; ISRCTN08060326); in four studies, there was no mention of participants with SSV varices (Campos 2015; Flessenkamper 2012; Seddon 1973; Wilhelmi 2009); and in another two, the study did not distinguish between participants with GSV varices and SSV varices (Figueiredo 2009; Ogawa 2008). The study design in one study differed to the design specified in the protocol for this review (Wright 2006); in four studies the intervention was not one of the three specified for this review (Ariyoshi 1996; Iwamoto 2003; Kalodiki 2012; Liu 2011); in three studies, the comparator was not conventional surgery (ISRCTN06552809; MESSI trial 2014; VEDICO trial 1998); and in seven studies, the method of sclerotherapy used was not UGFS (Chant 1972; Doran 1975; Einarsson 1993; Hobbs 1974; Jakobsen 1979; REACTIV trial 2006; Shouler 1989).
Risk of bias in included studies
Detailed risk of bias assessments for each of the three studies are reported in the 'Risk of bias' section of the Characteristics of included studies table; in addition, see Figure 2 and Figure 3 for summaries of the methodological quality of these studies.
2.
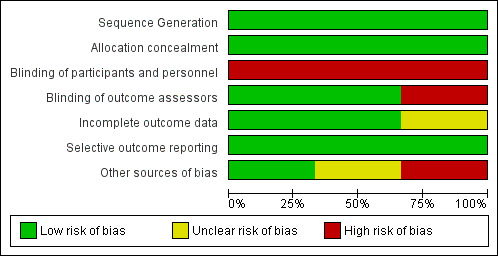
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.
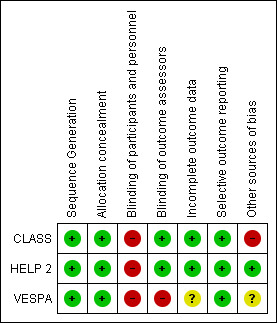
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
The review authors judged the risk of selection bias for the three included studies as low, as each study reported adequate methods for random sequence generation and allocation concealment (CLASS; HELP 2; VESPA).
Blinding
Blinding of participants and personnel was not possible in these three studies; consequently, the review authors judged the risk of performance bias as high.
It was not possible to blind postoperative assessors to the procedure that the participants had undergone. However, two studies were at low risk of detection bias since the trial authors were aware of the risk and had attempted to address it by using "independent accredited vascular technologists rather than by the surgeons who had performed the treatment" (CLASS) and objective validated instruments to record clinical outcomes, and both disease‐specific and generic QoL instruments that had all been validated to measure efficacy of venous treatment (HELP 2). The third study did not address the issue of blinding of outcome assessors, and the review authors judged it at high risk of detection bias (VESPA).
Incomplete outcome data
In two studies, the number of participants was clearly stated for each outcome reported, and the review authors judged the risk of attrition bias as low (CLASS; HELP 2). In the third study, the review authors judged the risk of attrition bias as unclear, as 7% of the participants were unaccounted for in the analysis of the success rate of the procedure, and other outcomes were reported as means, with no indication of the number of participants contributing to the outcome (VESPA).
Selective reporting
There was no evidence of reporting bias in the three studies. The protocol was available for one study (CLASS), and all prespecified outcomes were reported; for the other two studies, all outcomes specified in the trial register were reported (HELP 2; VESPA), although the VESPA report was an interim report and the report for one‐year results is still awaited.
Other potential sources of bias
One study was at low risk of any other bias, since its authors explicitly reported that its sample‐size calculation was based on the primary outcome, and that it was underpowered for a "detailed QoL analysis (secondary outcomes) and therefore cannot confirm or refute any true benefit of EVLA over surgery in this area" (HELP 2). Another study was at unclear risk of other forms of bias, since its 2:1 (EVLA:surgery) allocation of participants was not explicitly reported in either the trial register or the methods section (VESPA). The third study was potentially underpowered and at high risk of bias because it recruited participants with either GSV or SSV varices (or both), and recruited very few participants with SSV varices (CLASS).
Effects of interventions
Summary of findings for the main comparison. Endovenous laser ablation compared to conventional surgery for short saphenous vein varices.
| Endovenous laser ablation compared to conventional surgery for short saphenous vein varices | ||||||
|
Patient or population: people requiring intervention for short saphenous vein varices Setting: hospital day‐case vascular surgery department Intervention: EVLA Comparison: conventional surgery | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with conventional surgery | Risk with EVLA | |||||
| Recanalisation or persistence of reflux at 6 weeks | Study population | OR 0.07 (0.02 to 0.22) | 289 (3 RCTs) | ⊕⊕⊕⊝ Moderate1 | ‐ | |
| 250 per 1000 | 23 per 1000 (7 to 68) | |||||
| Recurrence of reflux at 1 year | Study population | OR 0.24 (0.07 to 0.77) | 119 (2 RCTs) | ⊕⊕⊝⊝ Low2 | ‐ | |
| 242 per 1000 | 71 per 1000 (22 to 197) | |||||
| Clinical evidence of recurrence after 1 year | Study population | OR 0.54 (0.17 to 1.75) | 99 (1 RCT) | ⊕⊕⊝⊝ Low3 | ‐ | |
| 176 per 1000 | 104 per 1000 (35 to 273) | |||||
| Reintervention (due to technical failure) | See comments | See comments | ‐ | 99 (1 RCT) |
⊕⊕⊕⊝ Moderate4 | 4 participants in EVLA group required further treatment: 1 had second EVLA, 3 UGFS 4 participants in surgery group required further treatment: 3 had EVLA, 1 ultrasound‐guided perforator ligation |
| Disease‐specific QoL (AVVQ) at 6 weeks | The mean disease‐specific QoL (AVVQ) at 6 weeks was 8.75 | The mean disease‐specific QoL at 6 weeks was 8.95 | ‐ | 265 (2 RCTs) | ⊕⊕⊕⊝ Moderate5 | The mean difference between the disease‐specific QoL (AVVQ) in both groups at 6 weeks was 0.15 (‐1.65 to 1.95). (AVVQ range: 0 = no impact on QoL; 100 = greatest possible impact on QoL) |
| Disease‐specific QoL (AVVQ) at 1 year | The mean disease‐specific QoL (AVVQ) at 1 year was 5.3 | The mean disease‐specific QoL (AVVQ) at 1 year was 4.22 | ‐ | 99 (1 RCT) | ⊕⊕⊝⊝ Low3 | The mean difference between the disease‐specific QoL (AVVQ) at 1 year in both groups was ‐1.08 (‐3.39 to 1.23). (AVVQ range: 0 = no impact on QoL; 100 = greatest possible impact on QoL) |
| Complications at 6 weeks | See comments | See comments | ‐ | 265 (2 RCTs) |
⊕⊕⊕⊝ Moderate6 | Main complications reported were sural nerve injury at 6 weeks (11/161 EVLA; 30/104 surgery), wound infection; 2 cases of DVT (1e in each group). See Table 6 for detailed information |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). AVVQ: Aberdeen Varicose Veins Questionnaire; CI: confidence interval; EVLA: endovenous laser ablation; OR: odds ratio; QoL: quality of life; RCT: randomised controlled trial; UGFS: ultrasound‐guided foam sclerotherapy. | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Downgraded one level due to risk of bias: limitation of power in one study, and a 2:1 EVLA:surgery allocation that did not appear to be prespecified in another study. 2 Downgraded one level due to risk of bias and one level for potential concerns relating to imprecision and indirectness, since one study reported outcomes at six months rather than one year. 3 Downgraded one level for risk of bias and one level for imprecision (n = 99). 4 Downgraded one level for imprecision (n = 99). 5 Downgraded one level for risk of bias. Decision taken not to downgrade for imprecision because the mean difference between the two treatments was negligible on the total AVVQ range (0 to 100). 6 Downgraded one level for imprecision in one study.
Summary of findings 2. Ultrasound‐guided foam sclerotherapy compared to conventional surgery for short saphenous vein varices.
| Ultrasound‐guided foam sclerotherapy compared to conventional surgery for short saphenous vein varices | ||||||
|
Patient or population: people requiring intervention for short saphenous vein varices Setting: hospital day‐case vascular surgery department Intervention: UGFS Comparison: conventional surgery | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with conventional surgery | Risk with UGFS | |||||
| Recanalisation or persistence of reflux at 6 weeks | Study population | OR 0.34 (0.06 to 2.10) | 33 (1 RCT) | ⊕⊕⊝⊝ Low1 | ‐ | |
| 294 per 1000 | 124 per 1000 (24 to 467) | |||||
| Recurrence of reflux at 1 year | Study population | OR 1.19 (0.29 to 4.92) | 31 (1 RCT) | ⊕⊕⊝⊝ Low1 | Follow‐up for this outcome was only available for 6 months in this trial | |
| 429 per 1000 | 472 per 1000 (179 to 787) | |||||
| Clinical evidence of recurrence after 1 year | See comments | See comments | Not estimable | 31 (1 RCT) | ‐ | Clinical evidence not stratified by GSV/SSV |
| Reintervention (due to technical failure) | See comments | See comments | Not estimable | 31 (1 RCT) | ‐ | Reintervention not stratified by GSV/SSV |
| Disease‐specific QoL (AVVQ) at 6 weeks | See comments | See comments | Not estimable | 33 (1 RCT) | ‐ | QoL not stratified by GSV/SSV |
| Disease‐specific QoL (AVVQ) at 1 year | See comments | See comments | Not estimable | 31 (1 RCT) | ‐ | QoL not stratified by GSV/SSV |
| Complications at 1 year | See comments | See comments | Not estimable | 31 (1 RCT) | ‐ | Complications not stratified by GSV/SSV |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). AVVQ: Aberdeen Varicose Veins Questionnaire; CI: confidence interval; GSV: great saphenous vein; OR: odds ratio; QoL: quality of life; RCT: randomised controlled trial; SSV: short saphenous vein; UGFS: ultrasound‐guided foam sclerotherapy. | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Downgraded by one level for imprecision (only one trial in this review offered UGFS) and one level for limitation in design as the study was inadequately powered for participants with SSV varices alone.
Nearly all the outcome measures prespecified in our protocol, and the Methods section, were presented in the original trial report for CLASS; however, the CLASS authors did not stratify their results according to GSV/SSV for most outcomes. We contacted the study authors with a request for data pertaining to participants with SSV varices and, although the study authors responded positively to our request for stratified data, it had not been received by the time of completion of this review. As a consequence, we are unable to provide data for CLASS, in either treatment comparison, for the following outcomes:
clinical evidence of recurrence at one year;
QoL AVVQ scores;
QoL EQ‐5D scores;
QoL 36‐item Short Form (SF‐36) scores;
postoperative pain;
postoperative complications;
duration of hospital stay;
return to work;
duration of procedure.
In the VESPA trial, data were only available for the first six weeks of follow‐up; we contacted the study authors who responded positively to our request for data up to one year after intervention (according to the study protocol), but data were not received by the time of completion of this review. As a consequence, we are unable to provide data for VESPA, in the EVLA versus surgery comparison, for:
recurrence of reflux at one year;
all QoL scores at one year.
Primary outcomes
Recanalisation or persistence of reflux at six weeks
Ultrasound was used to determine recanalisation. The three studies used different thresholds for definition of reflux: reflux was defined as: a retrograde flow of 1 second or more on spectral Doppler after augmentation (HELP 2); greater than 0.5 seconds for incompetence of the superficial venous system (and greater than 0.8 seconds for deep veins) (VESPA); and greater than 1 second (CLASS).
Endovenous ablation therapy versus surgery
All three studies evaluated recanalisation or persistence of reflux (CLASS; HELP 2; VESPA). At six weeks, there were significantly fewer instances in the EVLA (3/173 participants) group compared to surgery (29/116 participants). In the fixed‐effect meta‐analysis, there was a statistically significant difference between the two groups: the OR for recanalisation or persistence of reflux at six weeks was 0.07 in favour of EVLA (95% CI 0.02 to 0.22; P < 0.00001, I2 = 51%, moderate‐quality evidence) (Analysis 1.1).
1.1. Analysis.
Comparison 1 Endovenous laser ablation (EVLA) versus conventional surgery, Outcome 1 Recanalisation or persistence of reflux at 6 weeks.
Foam sclerotherapy versus surgery
Only one study compared UGFS with conventional surgery (CLASS). Of the 21 participants randomised to each group and who underwent the procedure, data at six weeks were available for 16 participants in the UGFS group and 17 in the surgery group. In the UGFS group, there were two incidences of recanalisation or persistence of reflux at six weeks compared to five participants in the surgical group; the OR of recanalisation or persistence of reflux at six weeks when UGFS was compared with surgery was 0.34 (95% CI 0.06 to 2.10; P = 0.25, low‐quality evidence), showing no statistically significant difference between the two treatment groups (Analysis 2.1).
2.1. Analysis.
Comparison 2 Ultrasound‐guided foam sclerotherapy (UGFS) versus conventional surgery, Outcome 1 Recanalisation or persistence of reflux at 6 weeks.
Recurrence of reflux at one year
Endovenous ablation therapy versus surgery
Recurrence of reflux at one year was determined by recanalisation on ultrasound. One‐year follow‐up data were available from HELP 2 only; CLASS reported six‐month follow‐up data and data from VESPA could not be obtained (Analysis 1.2). In the CLASS trial, at six months, reflux was observed in 1/9 participants in the EVLA group, and 5/11 participants in the surgery group (OR 0.15, 95% CI 0.01 to 1.64). In HELP 2, reflux was observed in 3/48 participants in the EVLA group and 10/51 participants in the surgery group (OR 0.27, 95% CI 0.07 to 1.06). Pooled data suggested a significantly higher number of recurrences in the surgery group compared to the EVLA group (OR 0.24, 95% CI 0.07 to 0.77; P = 0.02, I2 = 0%, low‐quality evidence).
1.2. Analysis.
Comparison 1 Endovenous laser ablation (EVLA) versus conventional surgery, Outcome 2 Recurrence of reflux at 1 year.
HELP 2 also published two‐year follow‐up data, which provided no evidence of a difference between the number of recurrences in surgery (15/44 participants) and EVLA (8/44 participants) (OR 0.43, 95% CI 0.16 to 1.15; P = 0.09) (Analysis 1.3).
1.3. Analysis.
Comparison 1 Endovenous laser ablation (EVLA) versus conventional surgery, Outcome 3 Recurrence of reflux at 2 years.
Foam sclerotherapy versus surgery
In the CLASS study, at the clinic six months after the procedure, there was no significant difference in the incidence of reflux between UGFS (8/17 participants) and surgery (6/14 participants) groups (OR 1.19, 95% CI 0.29 to 4.92, low‐quality evidence) (Analysis 2.2).
2.2. Analysis.
Comparison 2 Ultrasound‐guided foam sclerotherapy (UGFS) versus conventional surgery, Outcome 2 Recurrence of reflux at 6 months.
Clinical evidence of recurrence at one year
The most common clinical evidence of recurrence was the presence of new visible varicose veins.
Endovenous ablation therapy versus surgery
In HELP 2, there was clinical evidence of recurrence one year after the procedure in 5/48 participants in the EVLA group, and 9/51 in the surgical group. The OR for clinical evidence of recurrence one year after the procedure when EVLA was compared with surgery was 0.54 (95% CI 0.17 to 1.75, low‐quality evidence), demonstrating no difference between the two treatment groups (Analysis 1.4). VESPA did not report this outcome. In the CLASS study, results for this outcome were not presented separately for people with SSV varices; therefore, results for this outcome are not available from that study.
1.4. Analysis.
Comparison 1 Endovenous laser ablation (EVLA) versus conventional surgery, Outcome 4 Clinical evidence of recurrence after 1 year.
Foam sclerotherapy versus surgery
In the CLASS study, results for this outcome were not presented separately for people with SSV varices; therefore, results are not available for this outcome.
Reintervention (due to technical failure)
Endovenous ablation therapy versus surgery
Neither CLASS nor VESPA reported reintervention (due to technical failure).
In HELP 2, four participants randomised to EVLA required further treatment: one participant underwent a second EVLA, and three participants underwent UGFS; in the surgical group, three participants underwent EVLA and one participant had ultrasound‐guided perforator ligation.
Foam sclerotherapy versus surgery
CLASS did not report results for this outcome separately for people with SSV varices; therefore, results are not available for this outcome.
Secondary outcomes
Quality of life
All included studies measured QoL with at least two different participant‐reported questionnaires ‐ the disease‐specific AVVQ and the generic EuroQoL Group 5‐Dimension Self‐Report Questionnaire (EQ‐5D) (CLASS; HELP 2; VESPA). In addition, two studies used a second participant‐reported generic questionnaire ‐ the Medical Outcomes SF‐36 (CLASS; HELP 2).
Quality of life ‐ Aberdeen Varicose Veins Questionnaire
AVVQ scores range from 0 (no impact on QoL) to 100 (greatest possible impact on QoL).
Endovenous ablation therapy versus surgery
See Table 3 for a breakdown of results over time by study. In the HELP 2 study, both groups reported a slight increase in the AVVQ score one week after the procedure (i.e. a slight deterioration), but thereafter there was a steady decrease in scores for both treatment groups during the first year after the procedure, indicating a steady and continuing improvement (P < 0.001). There was no statistically significant difference between the AVVQ scores of the two treatment groups at each time point.
1. Disease‐specific quality of life scores (AVVQ) over follow‐up: EVLA versus surgery.
| Time point | HELP 2 | VESPA | ||||
| AVVQ scores (mean (SD)) | P value§ | AVVQ scores (mean (SD)) | P value§§ | |||
| EVLA | Surgery | EVLA | Surgery | |||
| Baseline | 13.2 (6.0) | 14.5 (6.0) | 0.215 | 16.0 (10.0) | 11.9 (5.9) | nr |
| 1 week | 16.2 (6.2) | 17.9 (6.4) | 0.092 | 16.8 (7.7)* | 16.4 (8.9)* | nr |
| 6 weeks | 8.8 (7.2) | 8.8 (5.5) | 0.996 | 9.0 (7.7) | 8.7 (8.0) | nr |
| 12 weeks | 5.1 (4.9) | 5.2 (5.3) | 0.787 | ‐ | ‐ | nr |
| 52 weeks | 4.2 (6.0) | 5.3 (5.7) | 0.327 | ‐ | ‐ | nr |
*These scores were measured at 2 weeks after the procedure' §Student t‐test for intergroup analysis' §§Individual P values were not reported, but the authors reported there were no significant differences between the groups (P < 0.001).
AVVQ: Aberdeen Varicose Veins Questionnaire; EVLA: endovenous laser ablation; nr: not recorded.
In the VESPA study, there were no statistically significant differences in AVVQ scores between the two groups, and in both groups the scores decreased significantly between the two‐ and six‐week appointments, indicating an improvement in disease‐specific QoL (P < 0.001).
The CLASS study did not report results for QoL measured by AVVQ separately for people with SSV varices; therefore, results were not available.
When we pooled the six‐week AVVQ scores for HELP 2 and VESPA, there was no evidence of a difference in AVVQ score between the two procedures; the MD in AVVQ scores between the interventions was 0.15 (95% CI ‐1.65 to 1.95; I2 = 0%, P = 0.87; moderate‐quality evidence) (Analysis 1.5). The only study that reported AVVQ scores at one year was HELP 2; however, there was insufficient evidence of a difference between EVLA and surgery (MD in AVVQ scores ‐1.08 (95% CI ‐3.39 to 1.23, low‐quality evidence) (Analysis 1.6)).
1.5. Analysis.
Comparison 1 Endovenous laser ablation (EVLA) versus conventional surgery, Outcome 5 Disease‐specific QoL (AVVQ) at 6 weeks.
1.6. Analysis.
Comparison 1 Endovenous laser ablation (EVLA) versus conventional surgery, Outcome 6 Disease‐specific QoL (AVVQ) at 1 year.
Foam sclerotherapy versus surgery
The CLASS study did not report results for QoL measured by AVVQ separately for people with SSV varices; therefore, results were not available.
Quality of life ‐ EuroQoL Group 5‐Dimension Questionnaire
EQ‐5D is a standardised measure of health status developed by the EuroQoL Group to provide a simple, generic measure of health for clinical and economic appraisal. The EQ‐5D has five dimensions (mobility, self‐care, usual activities, pain/discomfort and anxiety/depression), and each dimension has 3 levels (no problems, some problems and extreme problems); level 1 represents the best score.
Endovenous ablation therapy versus surgery
See Table 4 for a breakdown of results over time by study. We noted that the EQ‐5D values were very different between the VESPA trial and the other two studies (CLASS; HELP 2), and query therefore whether the conversion of the EQ‐5D questionnaire to the EQ‐5D Index was calculated in the same way for the English and Dutch versions. For this reason, we decided not to pool the EQ‐5D results in a meta‐analysis. The CLASS study did not report results for QoL measured by EQ‐5D separately for people with SSV varices; therefore, results were not available.
2. Generic quality of life scores (EQ‐5D) over follow‐up: EVLA versus surgery.
| Time point | HELP 2 | VESPA | ||||
| EQ‐5D (median (IQR)) | P value | EQ‐5D (mean (SD)) | P value | |||
| EVLA | Surgery | EVLA | Surgery | |||
| Baseline | 0.81 (0.73 to 1.0) | 0.88 (0.80 to 1.0) | 0.249 | 0.20 (0.19) | 0.19 (0.19) | nr |
| 1 week | 0.80 (0.70 to 1.0) | 0.77 (0.69 to 0.88) | 0.256 | 0.20 (0.22) | 0.15 (0.13) | nr |
| 6 weeks | 1.0 (0.84 to 1.0) | 1.0 (0.81 to 1.0) | 0.802 | 0.09 (0.16) | 0.12 (0.16) | nr |
| 12 weeks | 0.97 (0.76 to 1.0) | 1.0 (0.85 to 1.0) | 0.095 | nr | nr | nr |
| 52 weeks | 0.93 (0.78 to 1.0) | 1.0 (0.81 to 1.0) | 0.119 | nr | nr | nr |
EQ‐5D EuroQoL 5‐Dimension; EVLA Endovenous laser ablation; nr: not recorded.
In the HELP 2 study, there was no significant difference between the index scores of each treatment group at each time point. At six weeks, both groups had a median score of 1 (best possible), which the surgery group maintained at 12 weeks and one year; the EVLA group median was 0.97 at 12 weeks and 0.93 at one year.
The VESPA study used the Dutch version of the EQ‐5D. The authors reported "No significant differences were seen between the two groups. Scores for both groups were significantly improved over time (P = 0.017)."
Foam sclerotherapy versus surgery
The CLASS study did not report QoL measured by EQ‐5D separately for people with SSV varices; therefore, results were not available.
Quality of life ‐ 36‐Item Short‐Form Health Survey
The SF‐36 measures QoL across eight emotional and physical domains, with scores ranging from 0 (worst QoL) to 100 (best QoL); physical and mental summary scores may also be calculated.
Endovenous ablation therapy versus surgery
See Table 5 for a breakdown of results over time by study. In the HELP 2 study, across five of the eight SF‐36 domains, both groups achieved higher scores in the SF‐36 over time (i.e. better functioning). In the general health domain, although the score of the EVLA group reflected an improvement between weeks one and six, the score at the end of the year was slightly lower than that at six weeks. In the vitality and mental health domains, the deterioration for the EVLA group occurred after 12 weeks; however, the surgery group maintained an improvement in scores throughout the year.
3. Generic quality of life scores (SF‐36) over follow‐up: EVLA versus surgery.
| SF‐36 domain | Time point | HELP 2 | ||
| EVLA (median (IQR)) | Surgery (median (IQR)) | P value | ||
| Physical functioning | Baseline | 90 (75 to 100) | 90 (70 to 100) | 0.891 |
| 1 week | 80 (61 to 95) | 70 (50 to 90) | 0.095 | |
| 6 weeks | 95 (75 to 100) | 95 (85 to 100) | 0.708 | |
| 12 weeks | 95 (80 to 100) | 95 (85 to 100) | 0.766 | |
| 52 weeks | 95 (78 to 100) | 95 (85 to 100) | 0.896 | |
| Role physical | Baseline | 100 (50 to 100) | 100 (50 to 100) | 0.969 |
| 1 week | 50 (0 to 100) | 50 (0 to 100) | 0.277 | |
| 6 weeks | 100 (31 to 100) | 100 (25 to 100) | 0.644 | |
| 12 weeks | 100 (50 to 100) | 100 (75 to 100) | 0.779 | |
| 52 weeks | 100 (75 to 100) | 100 | 0.502 | |
| Bodily pain | Baseline | 74 (51 to 84) | 74 (42 to 88) | 0.826 |
| 1 week | 62 (41 to 84) | 52 (41 to 74) | 0.325 | |
| 6 weeks | 84 (62 to 100) | 74 (54 to 100) | 0.469 | |
| 12 weeks | 84 (62 to 100) | 84 (62 to 100) | 0.483 | |
| 52 weeks | 84 (62 to 100) | 84 (62 to 100) | 0.280 | |
| General health | Baseline | 77 (53 to 84) | 77 (52 to 87) | 0.606 |
| 1 week | 77 (56 to 82) | 77 (53 to 92) | 0.341 | |
| 6 weeks | 77 (57 to 89) | 82 (67 to 92) | 0.175 | |
| 12 weeks | 75 (62 to 87) | 77 (65 to 91) | 0.403 | |
| 52 weeks | 72 (57 to 87) | 82 (67 to 93) | 0.077 | |
| Vitality | Baseline | 55 (46 to 75) | 65 (50 to 80) | 0.072 |
| 1 week | 63 (45 to 74) | 60 (45 to 74) | 0.690 | |
| 6 weeks | 68 (45 to 80) | 70 (60 to 85) | 0.325 | |
| 12 weeks | 70 (45 to 80) | 70 (50 to 80) | 0.774 | |
| 52 weeks | 65 (50 to 75) | 75 (54 to 85) | 0.136 | |
| Social functioning | Baseline | 100 (75 to 100) | 100 (75 to 100) | 0.420 |
| 1 week | 88 (63 to 100) | 75 (50 to 100) | 0.082 | |
| 6 weeks | 100 (75 to 100) | 100 (63 to 100) | 0.198 | |
| 12 weeks | 100 (75 to 100) | 100 (75 to 100) | 0.877 | |
| 52 weeks | 100 (75 to 100) | 100 (78 to 100) | 0.364 | |
| Role emotional | Baseline | 100 (75 to 100) | 100 | 0.820 |
| 1 week | 100 (67 to 100) | 100 | 0.498 | |
| 6 weeks | 100 | 100 | 0.582 | |
| 12 weeks | 100 (67 to 100) | 100 | 0.155 | |
| 52 weeks | 100 | 100 | 0.510 | |
| Mental health | Baseline | 78 (60 to 87) | 80 (72 to 88) | 0.167 |
| 1 week | 78 (65 to 92) | 84 (68 to 91) | 0.680 | |
| 6 weeks | 80 (68 to 92) | 84 (76 to 92) | 0.369 | |
| 12 weeks | 84 (72 to 92) | 88 (74 to 92) | 0.456 | |
| 52 weeks | 80 (68 to 90) | 88 (72 to 92) | 0.071 | |
EVLA: endovenous laser ablation; SF‐36: 36‐Item Short Form Health Survey.
The VESPA study did not use the SF‐36 to measure QoL. The CLASS study did not report QoL measured by SF‐36 separately for people with SSV varices; therefore, results were not available.
Foam sclerotherapy versus surgery
The CLASS study did not report QoL measured by SF‐36 separately for people with SSV varices; therefore, results were not available.
Postoperative pain ‐ Visual Analogue Scale scores
Endovenous ablation therapy versus surgery
CLASS and HELP 2 measured pain on a VAS from 0 (no pain) to 10 (worst pain imaginable), and VESPA measured pain on a VAS from 0 (no pain) to 100 (worst pain imaginable). The CLASS study did not report results for postoperative pain measured using a VAS separately for people with SSV varices; therefore, results were not available.
In HELP 2, participants kept a pain diary for the seven days immediately following the procedure. For the first day, participants in the EVLA group recorded a median pain score of 1.5 (interquartile range (IQR) 0.9 to 3.6), in contrast to participants in the surgery group who recorded a median pain score of 2.9 (IQR 0.9 to 5.8). During the week, the level of pain declined each day, but pain scores for the EVLA group were lower than those for the surgery group. The study authors reported that the difference in pain between the two groups was statistically significant for days four to seven (day four, P = 0.025; day five, P = 0.008; day six, P = 0.033; day seven, P = 0.042), although there was no difference in the frequency of analgesia intake.
VESPA recorded pain caused by varicose veins at baseline and at one, two and six weeks. One week after the procedure, mean scores were 31 (EVLA group) and 18 (surgery group); by week six, these scores were 6 (EVLA group) and 9 (surgery group).
Foam sclerotherapy versus surgery
The CLASS study did not report results for postoperative pain measured using a VAS separately for people with SSV varices; therefore, results were not available.
Postoperative pain ‐ postoperative analgesia
Endovenous ablation therapy versus surgery
The CLASS trial did not report postoperative analgesia use. In HELP 2, there was no difference in the frequency of analgesia intake between participants in the EVLA and surgery groups, but there were no further details. VESPA reported that participants "were prescribed analgesia (acetaminophen [paracetamol] and non‐steroidal anti‐inflammatory drugs)", but there were no further details of postprocedural analgesia.
Foam sclerotherapy versus surgery
The CLASS trial did not report postoperative analgesia.
Postoperative pain ‐ participant complaints
Endovenous ablation therapy versus surgery
None of the studies reported participant complaints of postoperative pain (CLASS; HELP 2; VESPA).
Foam sclerotherapy versus surgery
The CLASS trial did not report participant complaints of postoperative pain.
Postoperative complications
Endovenous ablation therapy versus surgery
All three studies reported postoperative complications. The CLASS study did not report postoperative complications separately for people with SSV varices; therefore, results were not available. See Table 6 for further details. DVT was recorded for 1/161 participants in the EVLA group and 1/104 participants in the surgery group. In both participants, the DVT had completely resolved after three to six months of oral anticoagulation, with ultrasound demonstrating a competent deep venous system with no clinical evidence of pulmonary embolism (265 participants, 2 studies, moderate‐quality evidence).
4. Postprocedural complications: EVLA versus surgery.
| Complication | Treatment group | HELP 2 | VESPA | ||
| n | % | n | % | ||
| DVT | EVLA | 0 | 0 | 1/110 | < 1 |
| Surgery | 1/52 | 2 | 0 | 0 | |
| Thermal injury | EVLA | nr | nr | nr | nr |
| Surgery | nr | nr | nr | nr | |
| Sural nerve injury at 6 weeks | EVLA | 4/51 | 8 | 7/110 | 6 |
| Surgery | 14/52 | 27 | 16/52 | 31 | |
| Sural nerve injury at 52 weeks | EVLA | 2/48 | 4 | nr | nr |
| Surgery | 5/52 | 10 | nr | nr | |
| Wound infection | EVLA | 0 | 0 | 0 | 0 |
| Surgery | 1/52 | 2 | 6/52 | 11 | |
| Haematoma | EVLA | 0 | 0 | nr | nr |
| Surgery | 2/52 | 4 | nr | nr | |
| Pigmentation/skin bruising | EVLA | 2/51 | 4 | nr | nr |
| Surgery | 0 | 0 | nr | nr | |
| Phlebitis | EVLA | 3/51 | 6 | nr | nr |
| Surgery | 1/52 | 2 | nr | nr | |
DVT: deep venous thrombosis; EVLA: endovenous laser ablation; n: number of participants; nr: not reported.
In HELP 2, 8% of participants in the EVLA group and 27% of participants in the surgery group reported sural nerve injury at six weeks, and VESPA reported similar percentages; in both groups, most of these cases improved spontaneously. A small number of participants reported wound infection (surgery group, 2% in HELP 2, and 11% in VESPA), and HELP 2 reported haematoma, pigmentation or skin bruising and phlebitis.
The only complications listed in the VESPA trial were DVT; neurological complications such as numbness, hyperaesthesia and paraesthesia; and wound infection; it was not clear whether there were other complications, but they were not recorded, or whether these were the only complications encountered.
Foam sclerotherapy versus surgery
The CLASS study did not report results for postoperative complications separately for people with SSV varices; therefore, results were not available.
Healing of ulcers
Endovenous ablation therapy versus surgery
None of the studies reported healing of ulcers (CLASS; HELP 2; VESPA).
Foam sclerotherapy versus surgery
The CLASS trial did not report healing of ulcers.
Duration of hospital stay
Endovenous ablation therapy versus surgery
Although the procedures in the HELP 2 trial were intended to be performed as day‐case procedures, 1/53 participants in the EVLA group and 4/53 participants in the surgery group required an overnight stay after the intervention (the surgical participants were unsuitable for day‐case general anaesthesia).
The VESPA study did not report duration of hospital stay. The CLASS study did not report duration of hospital stay separately for people with SSV varices; therefore, results for this outcome were not available.
Foam sclerotherapy versus surgery
The CLASS study did not report duration of hospital stay separately for people with SSV varices; therefore, results were not available.
Return to work
Endovenous ablation therapy versus surgery
Although each study reported information regarding the length of time taken to return to work after interventional treatment, they used different methods to present this information, and, therefore, a meta‐analysis was not possible.
In HELP 2, the median time from treatment date to return to work was seven days (IQR 3 to 14 days) for the EVLA group, and 21 days (IQR 13 to 24 days) for the surgery group; the study authors reported that participants allocated to EVLA returned to work more quickly than participants who had received surgery (P < 0.001).
The VESPA trial, by contrast, asked participants at the two‐week clinic whether they had returned to work: 3/118 (2.4%) people in the EVLA group and 6/57 (11%) people in the surgery group had not returned to work within two weeks of the procedure as a result of the intervention they had received. The study authors reported that "these percentages were significantly different (P < 0.05)."
The CLASS study did not report results for return to work separately for people with SSV varices; therefore, results were not available.
Foam sclerotherapy versus surgery
The CLASS study did not report results for return to work separately for people with SSV varices; therefore, results were not available.
Type of anaesthesia
Endovenous ablation therapy versus surgery
Table 7 shows the types of anaesthesia used in each trial for the different interventions. All studies used a local tumescent anaesthesia for EVLA; among the surgery groups, studies used general, regional or spinal anaesthesia (CLASS; HELP 2; VESPA).
5. Type of anaesthesia.
| Study | Intervention | Type of anaesthesia |
| CLASS | EVLA | Local tumescent |
| Surgery | General or regional | |
| UGFS | ‐ | |
| HELP 2 | EVLA | Local tumescent |
| Surgery | General | |
| VESPA | EVLA | Local tumescent |
| Surgery | General or spinal |
EVLA: endovenous laser ablation; UGFS: ultrasound‐guided foam sclerotherapy.
Foam sclerotherapy versus surgery
The CLASS trial reported that either general or regional anaesthesia was used in the surgery group, and no anaesthesia was required for UGFS (Table 7).
Duration of procedure
Endovenous ablation therapy versus surgery
All studies reported duration of procedure. However, a meta‐analysis could not be performed because the VESPA data recorded mean time without reported standard deviations, and SSV varices data from CLASS were not received in time for the analysis. In HELP 2, the procedure took about one hour (mean time for EVLA was 58.5 minutes compared with 63.6 minutes for surgery) (Analysis 1.7). However, the authors of the VESPA trial reported that EVLA was significantly quicker to perform than surgery (21 minutes with EVLA versus 35 minutes with surgery, P < 0.001). The CLASS study did not report results for this outcome separately for people with SSV varices; therefore, results for duration of procedure were not available.
1.7. Analysis.
Comparison 1 Endovenous laser ablation (EVLA) versus conventional surgery, Outcome 7 Duration of procedure (minutes).
Foam sclerotherapy versus surgery
The CLASS study did not report results for duration of procedure separately for people with SSV varices; therefore, results were not available.
Subgroup analysis and sensitivity analysis
It was not possible to perform the planned subgroup analyses, due to a lack of data. Similarly, the sensitivity analyses specified in the protocol could not be undertaken.
The only sensitivity analyses that we were able to undertake related to the recanalisation or persistence of reflux at six weeks and the recurrence of reflux at one year in the EVLA versus surgery comparison. In each case, we removed data from the CLASS trial from the meta‐analyses, as that trial included participants with GSV varices or SSV varices (or both) and so was underpowered when we analysed only data for participants with SSV varices. When we pooled the results from HELP 2 and VESPA, the OR for recurrence of reflux at six weeks was 0.03 (95% CI 0.01 to 0.17; I2 = 0%, P < 0.0001), which still demonstrates that there were fewer recurrences of reflux for participants who had undergone EVLA, compared to participants who had conventional surgery. When we removed CLASS from the meta‐analysis for recurrence of reflux at one year, only HELP 2 contributed data; the OR for HELP 2 was 0.27 (95% CI 0.07 to 1.06), which did not quite achieve statistical significance (P = 0.06).
Discussion
Summary of main results
Endovenous ablation therapy versus surgery
For the primary outcome of recanalisation or persistence of reflux at six weeks after intervention, all three included studies favoured EVLA, and the pooled meta‐analysis demonstrated that there were fewer occurrences of recanalisation or persistence of reflux among the EVLA participants than the surgery participants at six weeks (P < 0.00001). Pooled analysis of two studies suggested that recurrence of reflux was higher at one year in the surgery group compared to EVLA (P = 0.02). Only one study reported clinical recurrence at one year showing no difference between the two treatment groups. Similarly, information about reintervention was limited to one study, with the same percentage in each group requiring further interventional treatment.
Only two studies provided data regarding QoL. Although there was no statistically significant difference between the two treatment groups, the mean disease‐specific QoL (AVVQ) scores for participants within each group indicated an improvement over time. Examination of the generic QoL (EQ‐5D) scores showed there was no significant difference between the two treatment groups in the two studies, but in one study the median scores in the surgery group maintained an improvement between six weeks and one year, whereas those scores in the EVLA group began to deteriorate slightly and consistently after six weeks. The second study reported that scores for both groups improved over time. With regard to postoperative pain as measured by VAS, in two studies, it diminished over time for both groups; however, in one study, the EVLA group consistently reported less pain than the surgery group, with the same level of analgesia, during the week immediately following intervention, whereas in the other study, the EVLA group reported a higher level of pain in the first two weeks, but slightly less pain than the surgery group at six weeks.
The two studies reported few complications. However, the percentages of participants in each trial that reported neurological complications at six weeks was similar, with complications affecting a larger percentage of the group who had received surgery. One study reported a greater percentage of participants in the surgery group had a wound infection than the other study.
All the studies used tumescent anaesthesia for EVLA, and a mixture of general anaesthetic only or general and either regional or spinal anaesthetic for conventional surgery. The duration of the procedure varied between the two studies, which might imply that different end‐points were used; possibly the fact that different anaesthesia was used in the surgery group might account for one group reporting that EVLA was significantly quicker to perform than surgery. Although the studies used different methods to measure participants returning to work, both studies reported that the EVLA group returned to work faster than the surgery group.
Foam sclerotherapy versus surgery
There were insufficient data to detect clear differences between the two groups for the outcome recanalisation or persistence of reflux at six weeks, although UGFS did appear to have a potentially lower recurrence rate. However, for reflux recurrence rate at one year, the surgery group appeared to have a slight advantage (again, there were insufficient data to discern a clear difference). There were no data for the other outcomes, as the study authors had not stratified their results by saphenous vein; the trialists expressed willingness to supply the requested data, but this was not received by the time the review was submitted for publication.
Overall completeness and applicability of evidence
This Cochrane Review included three studies; two were designed exclusively for adults with SSV varices (HELP 2; VESPA), whereas the third was designed for adults with either GSV varices or SSV varices, or both (CLASS). Two studies included only participants with unilateral varicose veins (HELP 2; VESPA). The third study included participants with bilateral SSV varices and nominated their worst leg to be their 'study leg' (CLASS). However, the fact that participants with bilateral SSV varices were included in one trial is likely to be less of a problem for the present review as there were very few participants from that trial with SSV varices, and the trial data available related to recurrence of reflux rather than outcomes that are most likely to be adversely affected by people with bilateral SSV varices, such as QoL, time of duration or return to work.
The review describes two of the three prespecified comparisons, but as none of the studies assessed endovenous RFA, it has not been possible to compare this treatment with conventional surgery.
Only one trial described UGFS (CLASS), although all the centres in that trial offered both treatments: thus, there were 21 participants with SSV varices in each treatment group. This is a very small number of participants and the original sample‐size calculation for this comparison estimated a sample size of 770 participants (385 in each group) would be required for at least 90% power at a 5% significance level to detect a change of 0.25 standard deviations in QoL questionnaires. Therefore, any results from this comparison should be viewed as purely exploratory findings and there is a significant potential for type II errors. In addition, many analyses in this study were not stratified according to GSV varices or SSV varices, and therefore data were missing for some outcomes. We contacted the trialists of the CLASS study, and they responded positively to our request for data pertaining to participants with SSV varices; however, stratified data had not been received by the time of completion of this review.
All three studies described EVLA and conventional surgery, although in the CLASS trial only eight of the 11 centres offered EVLA. In this comparison, 311 participants were randomised: 185 participants were treated with EVLA and 126 with conventional surgery. Although the number of participants included in this comparison was not large, it was nevertheless possible to pool the data and perform a meta‐analysis for some outcomes. In one study, data were only available for the first six weeks of follow‐up (VESPA); we contacted the authors and they also responded positively to our request for data up to one year after intervention (according to the study protocol), but data had not been received by the time of completion of this review. It should be noted that final follow‐up for CLASS was six months after intervention, rather than one year; therefore, it is possible that recurrence of reflux in Analysis 1.2 is underestimated for this trial.
Although not a prespecified outcome of this review, we noted that none of the three included studies reported on neovascularisation, which could be a potential cause of recurrence.
Quality of the evidence
We judged the quality of the evidence in the comparison of EVLA versus conventional surgery to be low to moderate, predominantly because only three studies were included in this review. All the studies were RCTs, and in four of the outcomes, the quality of evidence was downgraded by one level due either to risk of bias (the outcome assessors were not blinded, although some studies had tried to address this problem) or due to imprecision (data were only available from one study for certain outcomes). For three outcomes, the quality of the evidence was downgraded by two levels for risk of bias and either imprecision (for some outcomes data were only available from one small study), or indirectness (since for one study outcome data were only available at six months) (see Table 1).
The second comparison, UGFS versus surgery, included only one study and data were only available for two of the primary outcomes. The quality of the evidence for the two outcomes recanalisation or persistence of reflux at six weeks and recurrence of reflux at six months was low: both outcomes were downgraded by one level as only one trial in this review offered UGFS and the study was inadequately powered for SSV varices, and by another level because several of the participants were unaccounted for (for recurrence of reflux at six months, outcomes for 25% of participants (and 33% of participants in the surgery group) were not reported) (see Table 2).
Potential biases in the review process
We undertook extensive searches of databases for studies on SSV varices, and we searched meticulously by hand for reports of trials in reference lists of reviews on varicose veins, health services research‐related resources and abstracts in relevant conference proceedings. We duplicated both the screening of titles, abstracts and full papers, and the assessment of risk of bias and data extraction, and we resolved any disagreements by discussion, to restrict any potential bias.
Although all studies included in this review stated that their analyses would be conducted on an ITT basis, which normally uses the number of people who were randomised, in several studies a number of individuals dropped out between randomisation and intervention (in one study because it became apparent that some of the randomised participants were not eligible for inclusion in the trial because of the size of their veins or because they were later discovered to have recurrent varicose veins); in these studies, those participants who actually received interventional treatment were the total number included in the analysis, rather than the number who were initially randomised.
Although the three studies predominantly reported most of the same outcomes, in several instances the method used to measure a particular outcome, such as pain or return to work, differed so widely between studies that it was impossible to include the outcome in a meta‐analysis. In such cases, we reported the outcomes in the text and presented results in a table, where appropriate. For one QoL outcome, the EQ‐5D results were so different for one study that we queried whether the same method for calculating the EQ‐5D index had been employed by all the studies, or whether the Dutch and English versions of EQ‐5D were not comparable. We did not pool the results for this QoL outcome in a meta‐analysis, because we believed it would be inappropriate.
There were some discrepancies with the definition of certain outcomes among the studies, which is a potential source of bias. For example, the definition of reflux used different thresholds in all three studies: reflux was defined as a retrograde flow of 1 second or more on spectral Doppler after augmentation (HELP 2); greater than 0.5 seconds for incompetence of the superficial venous system (and greater than 0.8 seconds for deep veins) (VESPA); and greater than 1 second (CLASS). Some outcomes, such as time taken to return to work, were recorded in different ways; although the results for each study have been reported, it has not been possible to pool the data in a meta‐analysis.
We noted that studies generally reported absence of reflux as well as recurrence of reflux and we acknowledge that absence of reflux may be an outcome that is easier to interpret and as a consequence this outcome should be included in an update of this review.
We contacted the authors of two studies to request further data (CLASS; VESPA); in both cases, they agreed in principle, but the data were not available in time to be included in this review. This has resulted in limited analyses being included in this review.
Agreements and disagreements with other studies or reviews
There have been several systematic reviews and meta‐analyses published since the late 2000s: however, most examine either varicose veins in general (Carroll 2014; Leopardi 2009; Murad 2011; Nelzén 2015), or GSV varices and SSV varices combined (Hoggan 2009; van den Bos 2009), or are restricted to GSVs (Brar 2010; Luebke 2008; Siribumrungwong 2012) and do not report findings specifically for SSV varices. To our knowledge the only recent literature review that is restricted to SSV varices is Tellings 2011, which systematically reviewed the literature for papers describing RCTs, non‐randomised controlled trials and all types of observational studies that investigated at least one treatment technique. The authors identified 17 such papers, and calculated the success rate of surgery from four studies (47.8%) and the combined success rate of 10 EVLA studies and two UGFS studies (94.9%) (one identified surgery study could not be used). When Tellings 2011 compared the two success rates using the chi‐squared test, the minimally invasive procedures had a statistically higher success rate than surgery (P < 0.001), although there was heterogeneity. We included none of the papers that Tellings 2011 identified in our review, but their results are compatible with our outcome of recurrence of reflux, and the percentage of DVT in both groups was similar to that reported in this review.
Authors' conclusions
Implications for practice.
Low‐ to moderate‐quality evidence exists to suggest that recanalisation or persistence of reflux at six weeks and recurrence of reflux at one year are less frequent when endovenous laser ablation (EVLA) is performed, compared with conventional open surgery. For the ultrasound‐guided foam sclerotherapy (UGFS) versus conventional surgery comparison, we assessed the quality of evidence as low; consequently, the effectiveness of UGFS compared with conventional surgery in the treatment of short saphenous vein (SSV) varices is uncertain.
Implications for research.
The objective of this review was to compare the effectiveness of EVLA, radiofrequency ablation (RFA) and UGFS with conventional surgery in the treatment of SSV varices. However, because we found no trials that reported RFA, it has only been possible to report and analyse the results of two of these comparisons (one of which, UGFS, was only reported in a single small trial).
Although this review included three studies, they each contained a relatively small number of participants. To compound this difficulty, one study did not present their results stratified by type of saphenous vein and as a consequence most outcomes relating to quality of life, pain and return to work for people with SSV varices have not been reported, and a second study has so far only reported six weeks' follow‐up. As a result, statistical analyses of certain prespecified outcomes in this review could not be undertaken since, in several instances, only one study could be evaluated. Furthermore, since different measures were used to record certain outcomes such as pain and return to work, it precluded the pooling of results in meta‐analysis.
Continued research with well‐designed randomised controlled trials (RCTs) comparing minimally invasive endovenous procedures with conventional surgery in the treatment of SSV varices is required. In particular, future trials should aim to extend the follow‐up period to a minimum of two years and ideally five years or longer, as there is a hint in one study that for some of the minimally invasive endovenous procedures, the rate of reflux recurrence over time might be similar to or even higher than the recurrence rate for surgery over the same time period. In addition, there should be a standardisation of definitions in future work: for example, as discussed above, the three studies in this review used different thresholds in the definition of reflux (see Potential biases in the review process). Although it is not possible to blind participants and trial personnel to the interventional treatment allocated, when designing future RCTs consideration should be given to blinding outcome assessors or using independent outcome assessors rather than the clinician who performed the intervention. However, one researcher noted that future recruitment to a new RCT that compares minimally invasive endovenous procedures with open surgery may be more difficult, because clinical equipoise has become rarer as more research has been conducted (Nandhra 2015 in HELP 2). Future trials evaluating other minimally invasive techniques such as mechanico‐chemical ablation and VenaSeal™ glue where tumescent anaesthesia is not required might provide more evidence on the effective treatment of SSV varices.
Acknowledgements
The review authors would like to thank Cochrane Vascular for support in the preparation of the review, and for designing and running the search strategy. The review authors would also like to thank Professor G Stansby for his clinical input.
Appendices
Appendix 1. Cochrane Register of Studies (CRS) search strategy
| #1 | MESH DESCRIPTOR Varicose Veins EXPLODE ALL TREES | 744 |
| #2 | (varicos* near3 (vein* or veno*)):TI,AB,KY | 751 |
| #3 | (tortu* near3 (vein* or veno*)):TI,AB,KY | 6 |
| #4 | (incomp* near3 (vein* or veno* or saphenous or valv*)):TI,AB,KY | 83 |
| #5 | (insuffic* near3 (vein* or veno* or saphenous)):TI,AB,KY | 127 |
| #6 | (((saphenous or vein* or veno*) near3 reflux)):TI,AB,KY | 119 |
| #7 | MESH DESCRIPTOR Saphenous Vein EXPLODE ALL TREES WITH QUALIFIERS SU | 194 |
| #8 | (GSV or CVI or SSV):TI,AB,KY | 272 |
| #9 | MESH DESCRIPTOR Venous Insufficiency EXPLODE ALL TREES | 375 |
| #10 | #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 | 1595 |
| #11 | MESH DESCRIPTOR Sclerotherapy EXPLODE ALL TREES | 430 |
| #12 | MESH DESCRIPTOR Sclerosing Solutions EXPLODE ALL TREES | 371 |
| #13 | MESH DESCRIPTOR Sodium Tetradecyl Sulfate | 37 |
| #14 | MESH DESCRIPTOR Saline Solution, Hypertonic | 406 |
| #15 | MESH DESCRIPTOR Ethanolamines EXPLODE ALL TREES | 10578 |
| #16 | sclero*:TI,AB,KY | 7905 |
| #17 | (polydocanol or polidocanol):TI,AB,KY | 194 |
| #18 | saline:TI,AB,KY | 17864 |
| #19 | (ethanolamine near2 oleate):TI,AB,KY | 63 |
| #20 | (sodium near2 morrhuate):TI,AB,KY | 19 |
| #21 | sotradecol:TI,AB,KY | 6 |
| #22 | (aetoxisclerol or aethoxysclerol):TI,AB,KY | 15 |
| #23 | (aetoxiskerol or aethoxyskerol):TI,AB,KY | 1 |
| #24 | Turbofoam:TI,AB,KY | 2 |
| #25 | (foam* or microfoam*):TI,AB,KY | 1205 |
| #26 | varisolve:TI,AB,KY | 2 |
| #27 | MESH DESCRIPTOR Laser Therapy EXPLODE ALL TREES | 3129 |
| #28 | (endovenous or EVLA or EVLT):TI,AB,KY | 225 |
| #29 | (radiofrequency or RFA):TI,AB,KY | 1659 |
| #30 | laser* :TI,AB,KY | 9989 |
| #31 | ablation* :TI,AB,KY | 3380 |
| #32 | obliteration*:TI,AB,KY | 241 |
| #33 | MESH DESCRIPTOR Catheter Ablation | 1034 |
| #34 | #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24 OR #25 OR #26 OR #27 OR #28 OR #29 OR #30 OR #31 OR #32 OR #33 | 49548 |
| #35 | MESH DESCRIPTOR Vascular Surgical Procedures EXPLODE ALL TREES | 12073 |
| #36 | MESH DESCRIPTOR Ligation | 522 |
| #37 | surgi*:TI,AB,KY | 49395 |
| #38 | ligat*:TI,AB,KY | 1729 |
| #39 | strip*:TI,AB,KY | 1464 |
| #40 | phlebectom*:TI,AB,KY | 53 |
| #41 | #35 OR #36 OR #37 OR #38 OR #39 OR #40 | 61003 |
| #42 | #10 AND #34 AND #41 | 169 |
| #43 | * NOT SR‐PVD:CC | 914767 |
| #44 | #42 AND #43 | 66 |
Appendix 2. Trials registries searches
WHO
47 records for 45 trials found for: short saphenous or SSV
Clinicaltrials.gov
48 studies found for: short saphenous OR SSV
ISRCTN
2 results short saphenous or SSV
Data and analyses
Comparison 1. Endovenous laser ablation (EVLA) versus conventional surgery.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Recanalisation or persistence of reflux at 6 weeks | 3 | 289 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.07 [0.02, 0.22] |
| 2 Recurrence of reflux at 1 year | 2 | 119 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.24 [0.07, 0.77] |
| 3 Recurrence of reflux at 2 years | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4 Clinical evidence of recurrence after 1 year | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 5 Disease‐specific QoL (AVVQ) at 6 weeks | 2 | 265 | Mean Difference (IV, Fixed, 95% CI) | 0.15 [‐1.65, 1.95] |
| 6 Disease‐specific QoL (AVVQ) at 1 year | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7 Duration of procedure (minutes) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected |
Comparison 2. Ultrasound‐guided foam sclerotherapy (UGFS) versus conventional surgery.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Recanalisation or persistence of reflux at 6 weeks | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2 Recurrence of reflux at 6 months | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
CLASS.
| Methods |
Study design: multicentre prospective randomised controlled trial Country: UK Setting/location: vascular surgery departments in 11 hospitals (11 centres provided data for UGFS vs surgery; 8 centres provided data for EVLA vs surgery) Source of funding: supported by a grant from the Health Technology Assessment Programme of the National Institute for Health Research (06/45/02). The Health Services Research Unit is funded by the Chief Scientist Office of the Scottish Government Health Directorate. Intention‐to‐treat analysis: yes |
|
| Participants |
Number of participants randomised: total 798 (EVLA, 212; surgery, 294; UGFS, 292) Number of participants analysed: total 785 (EVLA, 210; surgery, 289; UGFS, 286) Exclusions postrandomisation: total 13 (EVLA, 2; surgery, 5; UGFS, 6) LTFU (after 1 year): not reported Age ‐ mean (range): EVLA vs surgery comparison: EVLA: 49.7 years (18 to 80); surgery: 48.4 years (22 to 85) UGFS vs surgery comparison: UGFS: 49.0 years (19 to 78); surgery: 49.2 years (22 to 85) Sex (% female): EVLA vs surgery comparison: EVLA: 57%; surgery: 57% UGFS vs surgery comparison: UGFS: 57%; surgery: 56% Inclusion criteria: aged ≥ 18 years; presence of unilateral or bilateral primary symptomatic varicose veins (CEAP grade ≥ 2); and GSV or SSV reflux > 1 second on duplex ultrasonography Exclusion criteria: current DVT; acute superficial‐venous thrombosis; a diameter of the main truncal saphenous vein of < 3 mm or > 15 mm; tortuous veins considered to be unsuitable for EVLA; contraindications to the use of foam or to general or regional anaesthesia; pregnancy or breastfeeding; inability to complete study questionnaires; needle phobia |
|
| Interventions |
EVLA: "The laser fibre was fired continuously during stepwise or continuous withdrawal, aiming to achieve a target delivery of at least 70 J/cm. EVLA was carried out under local anaesthetic." Foam sclerotherapy: "Foam was produced with the use of the Tessari technique at a ratio of 0.5 ml of sodium tetradecyl sulfate (STS) to 1.5 ml of air (3% STS for saphenous veins and 1% for varicosities, with a maximum of 12 ml of foam per session). The use of STS is licensed, but the trial involved its off‐license use as a foam rather than as its manufactured liquid form." Surgery (control): "Surgery consisted of proximal ligation and stripping (of the GSV only) and concurrent phlebectomies." Surgical treatment was performed under a general or regional anaesthetic. Duration: follow‐up at 6 and 26 weeks |
|
| Outcomes |
Primary outcomes: participant‐reported disease‐specific QoL, measured with the use of the AVVQ; participant‐reported generic (i.e. general) QoL, measured at 6 months after treatment with the EQ‐5D and the SF‐36; and 5‐year estimated cost‐effectiveness, measured as cost per quality‐adjusted life‐year gained. Secondary outcomes: clinical success at 6 weeks and 6 months, as measured by the proportion of participants with residual varicose veins (assessed by the participant and the nurse), VCSS and complications (assessed by the surgeon or nurse); QoL according to the AVVQ, EQ‐5D and SF‐36 at 6 weeks; the EQ‐5D VAS and the 8 SF‐36 domains at 6 weeks and 6 months; and ablation rates of the main trunks of the saphenous vein according to DUS at 6 weeks and 6 months, assessed using a standardised technique and reporting tool by independent, accredited vascular technologists. SSV reflux definition: SSV reflux was defined as > 1 second on DUS |
|
| Notes | Participants were recruited between November 2008 and October 2012 from 11 hospitals in the UK. In 8 centres, the treatment options available were EVLA, UGFS and conventional surgery; at these centres, participants underwent randomisation with even assignments to these 3 treatment options. However, in the other 3 centres, EVLA was not available, and in these 3 centres, participants underwent randomisation with even assignment to either UGFS or surgery. Thus, in the analysis of results from this study, in the UGFS vs surgery comparison, data from 11 hospitals were included in the analysis, whereas in the EVLA vs surgery comparison, data from 8 hospitals were included. This study included participants with GSV varices and SSV varices, but for this review, we included only SSV varices data. Many of the analyses in this trial were not stratified according to GSV or SSV, and therefore data were missing for some outcomes. The authors of the trial were contacted and responded positively to our request for data pertaining to participants with SSV varices; however, data had not been received by the time this review was ready for submission. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Sequence Generation | Low risk | Quote: "A computer‐generated randomisation system was used and was managed by the Centre for Healthcare Randomised Trials, University of Aberdeen, Aberdeen, United Kingdom." |
| Allocation concealment | Low risk | Quote: "Treatments were assigned with the use of a minimisation algorithm that included centre, age (< 50 years or ≥ 50 years), sex, reflux of either the great or the small saphenous veins (or both), and the presence or absence of unilateral or bilateral varicose veins." In the HTA Report (p. 14), "The aim was to keep participants blinded to their treatment allocation until around 2 weeks prior to their treatment. Around 2 weeks prior to their treatment, an appointment for treatment was issued by the hospital; at this time the trial office also informed the participant of his or her randomisation. However, at some sites, local processes meant that participants were informed of their randomisation by site staff in advance of this. The delay in informing participants about their treatment allocation was an attempt to minimise the possibility of unequal dropout between the arms." |
| Blinding of participants and personnel All outcomes | High risk | Quote: "Blinding with respect to the treatment used was not feasible." "... we determined whether ablation was complete or partial on the basis of duplex ultrasound scans obtained by independent, accredited vascular technologists rather than by the surgeons who had performed the treatment" (p. 1225) Judgement comment: lack of blinding may be less detrimental in this study, since groups are EVLA vs surgery and UGFS vs surgery, rather than surgery vs placebo |
| Blinding of outcome assessors All outcomes | Low risk | Quote: "it was not feasible for the participants or assessors to be kept unaware of the assigned treatment." "... we determined whether ablation was complete or partial on the basis of duplex ultrasound scans obtained by independent, accredited vascular technologists rather than by the surgeons who had performed the treatment" (p. 1225) Judgement comment: used independent assessors |
| Incomplete outcome data All outcomes | Low risk | Although there were some missing AVVQ scores at 6 months, the study authors performed sensitivity analyses, imputing the missing scores for different scenarios of missingness. For each sensitivity analysis, the effect size differed from that included in the main analysis by a negligible amount and each result was statistically significant |
| Selective outcome reporting | Low risk | Judgement comment: study protocol available and all of study's prespecified (primary and secondary) outcomes were reported either in NEJM paper, BJS paper or HTA report as prespecified |
| Other sources of bias | High risk | Judgement comment: the study may be underpowered as calculations were made on abolition of saphenous reflux, but did not specify whether GSV or SSV. Further, a very small number of participants had SSV reflux |
HELP 2.
| Methods |
Study design: prospective randomised controlled trial Country: UK Setting/location: participants presenting to a tertiary referral vascular surgical department at Hull Royal Infirmary Source of funding: "The primary funding source for this study was internal University funding. Diomed/Angiodynamics (Cambridge, United Kingdom) also provided 50% of a research nurse's salary over a 12‐month period to facilitate our work, but had no involvement or influence in the design, data collection/analysis, writing of the report, or in the decision to submit for publication. Diomed/Angiodynamics does not have access to any unpublished data." Intention‐to‐treat analysis: not applicable; participants had the treatment to which they were randomly assigned |
|
| Participants |
Number of participants randomised: total 106 participants (EVLA, 53; surgery, 53) Number of participants analysed: 52 participants in each group (week 1); EVLA, 51; surgery, 52 (week 6); EVLA, 50; surgery, 51 (week 12); EVLA, 48; surgery, 51 (week 52) Exclusions postrandomisation: 0 LTFU (after 1 year): EVLA, 4; surgery, 2 Age ‐ mean (SD): EVLA, 47.8 years (12.2); surgery, 47.5 years (12.9) Sex (% female): EVLA, 64%; surgery, 76% Inclusion criteria: primary, symptomatic, unilateral varicose veins, with isolated SPJ incompetence, causing reflux into the SSV Exclusion criteria: reflux in the GSV axis or deep veins on DUS examination; previous treatment of ipsilateral varicose veins; deep venous obstruction; aged < 18 years; pregnancy; impalpable foot pulses and inability to give informed consent or complete questionnaires during participation in the trial |
|
| Interventions |
EVLA: "A bare‐tipped 600‐nm laser fibre was introduced via a catheter, and laser energy was delivered using an 810‐nm diode laser generator (Diomed / Angiodynamics, Cambridge, UK) at 14 W power aiming for an energy delivery of 80 to 100 J/cm." Surgery (control): "All surgical procedures involved formal exploration of the popliteal fossa under general anaesthesia, predominantly undertaken as day case procedures. Saphenopopliteal ligation was attempted followed by inversion stripping of the SSV." Duration: follow‐up at 1, 6, 12 and 52 weeks |
|
| Outcomes |
Primary outcomes: early technical success, defined as abolition of SSV reflux at 6 weeks postprocedure on DUS assessment. Clinical recurrence (defined as "clinically evident varicose veins at least 3 mm in diameter not present at 1 or 6 weeks but becoming apparent during subsequent follow‐up") in first year following treatment: in surgery group 9 participants (incompetent SSV: 8; incompetent anterior accessory saphenous vein: 1); in EVLA group 5 participants (recanalisation: 2; incompetent antero‐lateral thigh branch and calf perforator: 1; incompetent posterior thigh perforator: 1; incompetent calf perforator: 1). Secondary outcomes: "Post‐procedural pain scores were recorded by the participant in a pain diary, using an unmarked 10‐cm VAS (0, no pain; 10, worst imaginable pain) daily for the first week, alongside the requirement for supplementary analgesia, the time taken to return to work and normal activity post‐procedure. Patient satisfaction with the cosmetic outcome and with the overall intervention was recorded on 10‐cm unmarked VAS (0, completely unsatisfied; 10, completely satisfied) at 12 and 52 weeks." The VCSS (a continuous scale from 0, representing no clinical evidence of venous disease, to a maximum of 30) was used to demonstrate changes in clinical severity over time. Disease‐specific QoL was assessed using the AVVQ, which measures the QoL impairment directly associated with venous disease; this is scored from 0 (no impact upon QoL) to a theoretical maximum of 100. Generic QoL was assessed using 2 instruments: SF‐36 was used to produce a health profile across 8 physical and psychological domains, each scored from 0 (worst possible) to 100 (best possible); the EQ‐5D was used to derive a single index valuation. SSV reflux definition: incompetence on DUS defined as retrograde flow of ≥ 1 second on spectral Doppler after augmentation. |
|
| Notes | Participants recruited between October 2005 and January 2010 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Sequence Generation | Low risk | Quote: "Following informed written consent, eligible patients were randomised using sealed, opaque envelopes to receive either surgery or EVLA." Judgement comment: does not state whether envelopes were sequentially numbered or not, but clinician had no knowledge of which treatment group was allocated until the envelope was opened |
| Allocation concealment | Low risk | Quote: "Following informed written consent, eligible patients were randomised using sealed, opaque envelopes to receive either surgery or EVLA." Judgement comment: does not state whether envelopes were sequentially numbered or not, but clinician had no knowledge of which treatment group was allocated until the envelope was opened |
| Blinding of participants and personnel All outcomes | High risk | Quote: "Because of the nature of the interventions, it was not possible to blind the investigators or patients to the treatment methods." |
| Blinding of outcome assessors All outcomes | Low risk | Quote: "One of the limitations of this study is that the patients, surgeons, and assessors could not be blinded to the technique used due to the nature of these interventions. Risk of observer bias was, however, reduced as much as possible by recording outcomes (both primary and secondary) with objective, validated instruments, and standardised protocols employed by assessors with relevant qualifications and experience. The QoL outcomes were also independently reported by patients, and the use of both disease‐specific and generic instruments provided a valid and reliable strategy to assess patient‐reported health states after treatment of their venous disease." |
| Incomplete outcome data All outcomes | Low risk | Judgement comment: Figure 1 showed number of participants analysed at each of the 4 time points: at 52 weeks, 5 (10%) LTFU in EVLA group and 2 (4%) LTFU in surgery group (but no explanation as to why they were missing) |
| Selective outcome reporting | Low risk | Judgement comment: all outcomes reported as planned (e.g. Table 4 reported all mean (SD) QoL measures over all prespecified time points); Figure 1 gave number of participants in each group whose data were analysed) |
| Other sources of bias | Low risk | Adequately powered for primary outcomes, but under‐powered for secondary outcomes, as stated in the Discussion of study report |
VESPA.
| Methods |
Study design: multicentre prospective randomised controlled trial Country: the Netherlands Setting/location: 2 teaching hospitals Source of funding: AngioCare BV Intention‐to‐treat analysis: yes |
|
| Participants |
Number of participants randomised: 189 participants Number of participants analysed: 175 treated (and analysed): EVLA, 118 (67%); surgery (ligation of the SPJ), 57 (33%) Exclusions postrandomisation: 14 participants cancelled their planned procedure for personal reasons LTFU (after 1 year): not stated Age ‐ mean (range): EVLA, 52 years (21 to 79); surgery, 51 years (19 to 73) Sex (% female): EVLA, 73%; surgery, 54% Inclusion criteria: valvular incompetence of the SPJ and SSV shown by DUS; aged > 18 years; CEAP severity classification of C2 to C6; informed consent; and minimum length of 10 cm of incompetent SSV Exclusion criteria: occlusion of the deep venous system; pregnancy; recurrent incompetence after previous ligation or EVLA of the SSV; tortuous SSV on DUS; SSV diameter < 2 mm; history of arterial insufficiency (ankle‐brachial index < 0.8 or absence of peripheral pulsations); simultaneous incompetence of the GSV and inability to understand the Dutch language |
|
| Interventions |
EVLA: "An 810‐nm Diomed (Andover, Mass) laser in continuous mode was used. Pullback speed was at a rate of 2 mm per second, with active power of 14 W. Laser energy was delivered with minimally 70 J/cm." Surgery (control): ligation of the SPJ performed under general/spinal anaesthesia. In prone position, a transverse incision was made in the popliteal fossa. The SSV was identified and dissected toward the SPJ; it was ligated and excised over a length of 3 cm to 5 cm. Duration: follow‐up at 1, 2, 6, 12 and 52 weeks |
|
| Outcomes |
Primary outcome: residual or recurrent incompetence or recanalisation of the SPJ and SSV, determined by DUS after 1 year (recurrence); if DUS showed incompetence of the treated segment after 6 weeks, it was considered as procedural failure. Secondary outcomes: morbidity: all participants were checked at the outpatient clinic after 2, 6, 12 and 52 weeks, with DUS at 6 and 52 weeks; QoL: AVVQ and the Dutch‐translated EQ‐5D completed at 2, 6, 12 and 52 weeks; BIQ filled out at 2 and 52 weeks; pain scored on a 0 to 100 VAS (0 = no pain, 100 = worst possible pain), preoperatively and at weeks 1, 2, 6, 12 and 52 weeks postoperatively; return to work was noted at 2 weeks postprocedure; difficulty and duration of the procedure; and neurological complications at 2 and 6 weeks postoperatively. SSV reflux definition: in DUS scanning, a threshold of > 0.5 seconds was used to define incompetence of the superficial venous system; for deep veins, a threshold of > 0.8 seconds was used; and for perforator veins, a threshold of > 0.35 seconds was used in the semi‐supine position. |
|
| Notes | According to the entry in the Netherlands trial register, participants were recruited between November 2008 and October 2010, although this was not confirmed in the study paper. Data were only available for the first 6 weeks of follow‐up; the authors were contacted and responded positively to our request for data up to 1 year after intervention (in accordance with the study protocol); however, data had not been received by the time the review was ready to be submitted for publication. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Sequence Generation | Low risk | Quote: "Patients were randomized using a computer‐generated randomization list prepared by the trial statistician." |
| Allocation concealment | Low risk | Quote: "The statistician provided the trial coordinator with randomization envelopes, and after inclusion, patients were randomized to conventional ligation of the SPJ or EVLA of the SSV." |
| Blinding of participants and personnel All outcomes | High risk | Judgement comment: no mention of blinding in text |
| Blinding of outcome assessors All outcomes | High risk | Judgement comment: no mention of blinding in text |
| Incomplete outcome data All outcomes | Unclear risk | Judgement comment: in Table III, 13 participants were unaccounted for: 8 in EVLA group and 5 in surgery group. Pain scores are given in Table IV, AVVQ in Table V, Euro QoL‐5D in Table VI, and body image in Table VII: however, these were all mean values and no indication of number of participants for each group at each time point |
| Selective outcome reporting | Low risk | Judgement comment: all results described in Methods section were presented up to 6‐week period (as stated in Introduction). Authors were contacted for results after 1 year and responded positively to our request for data up to 1 year after intervention (in accordance with the study protocol); however, data had not been received by the time the review was ready to be submitted for publication |
| Other sources of bias | Unclear risk | Judgement comment: allocation ratio of 2:1 (EVLA vs surgery) should have been reported more explicitly in the Methods (and Protocol), although the authors stated in the Statistical analysis section that a "twofold amount of patients were assigned to the EVLA group to enable statistical analysis within this group." |
AVVQ: Aberdeen Varicose Veins Questionnaire; BIQ: Body Image Questionnaire; BJS: British Journal of Surgery; CEAP: clinical, etiological, anatomical and pathophysiological classification system; DUS: duplex ultrasound; DVT: deep venous thrombosis; EQ‐5D: EuroQol 5‐Dimension Self‐Report Questionnaire; EVLA: endovenous laser ablation; GSV: great saphenous vein; HTA: Health Technology Assessment; IQR: interquartile range; LTFU: lost to follow‐upNEJM: New England Journal of Medicine; QoL: quality of life; SD: standard deviation; SF‐36: Medical Outcomes Study 36‐item Short Form Health Survey; SPJ: sapheno‐popliteal junction; SSV: short saphenous vein; UGFS: ultrasound‐guided foam sclerotherapy; VAS: visual analogue scale; VCSS: Venous Clinical Severity Score.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Ariyoshi 1996 | Intervention did not meet the eligibility criteria: sclerotherapy + surgery vs surgery alone; no mention of people with SSV varices |
| Beale 2005 | Participant population did not meet the eligibility criteria: GSV |
| Campos 2015 | No mention of people with SSV varices |
| Chant 1972 | Injection/compression sclerotherapy was used, not UGFS; did not distinguish between GSV varices and SSV varices |
| Compagna 2010 | Participant population did not meet the eligibility criteria: GSV |
| Doran 1975 | Wrong intervention: Fegan's compression‐injection method of sclerotherapy was used; did not distinguish between GSV varices and SSV varices |
| Einarsson 1993 | Wrong intervention: compression sclerotherapy vs surgery; did not distinguish between GSV varices and SSV varices |
| Figueiredo 2009 | Did not distinguish between GSV varices and SSV varices. After extensive discussion between the authors of the Cochrane Review for GSV varices (Nesbitt 2014), and the authors of this trial, we excluded the trial from the Cochrane Review because many aspects remained unclear. For this reason, and the fact that there would appear to be only 2 participants with SSV varices in each group (UGFS and surgery), the joint decision of the review authors (SP and MH) was also to exclude this trial from the present Cochrane Review |
| Flessenkamper 2012 | No mention of people with SSV varices |
| HELP 1 | Participant population did not meet the eligibility criteria: GSV |
| Hobbs 1974 | Fegan's injection‐compression sclerotherapy was used, not UGFS |
| ISRCTN06552809 | Comparator did not meet the eligibility criteria RFA vs pharmaco‐mechanical ablation (ClariVein) |
| ISRCTN08060326 | Participant population did not meet the eligibility criteria: GSV |
| Iwamoto 2003 | Intervention and participant population did not meet the eligibility criteria: compression sclerotherapy and GSV |
| Jakobsen 1979 | Fegan's injection‐compression sclerotherapy was used, not UGFS; groups were injection‐compression sclerotherapy alone vs minor surgery + injection‐compression sclerotherapy vs surgery alone |
| Kalodiki 2012 | Intervention and participant population did not meet the eligibility criteria: UGFS + sapheno‐femoral ligation vs surgery and GSV |
| Liu 2011 | Intervention and participant population did not meet the eligibility criteria: intravenous catheter‐guided laser ablation vs stab avulsion and GSV |
| MESSI trial 2014 | Comparator did not meet the eligibility criteria: mechano‐chemical endovenous ablation vs RFA |
| Ogawa 2008 | Did not distinguish between GSV varices and SSV varices; there were only 8/92 participants with SSV varices |
| REACTIV trial 2006 | Sclerotherapy was not UGFS: injection sclerotherapy vs conservative management; injection sclerotherapy vs surgery; surgery vs conservative management; did not distinguish between GSV varices and SSV varices |
| Seddon 1973 | No mention of people with SSV varices; compressive sclerotherapy was used, not UGFS |
| Shouler 1989 | Injection sclerotherapy was used, not UGFS; focus was on the compression stockings |
| VEDICO trial 1998 | Participant population and comparator did not meet the eligibility criteria: GSV and sclerotherapy alone vs sclerotherapy + surgery vs surgery alone |
| Wilhelmi 2009 | No mention of people with SSV varices |
| Wright 2006 | Study design did not meet the eligibility criteria: participants assessed and assigned to either surgery or sclerotherapy group (as alternative treatment). Then randomised to Varisolve technique or the chosen treatment alternative ‐ so 2 cohorts: Varisolve vs surgery and Varisolve vs sclerotherapy |
GSV: great saphenous vein; RFA: radiofrequency ablation; SSV: short saphenous vein; UGFS: ultrasound‐guided foam sclerotherapy.
Characteristics of studies awaiting assessment [ordered by study ID]
Boisseau 2015.
| Methods | |
| Participants | |
| Interventions | |
| Outcomes | |
| Notes | We were unable to locate this paper. |
Differences between protocol and review
The search that the Cochrane Vascular Information Specialist ran for the review differed slightly from that stated in the Cochrane protocol, to reflect current Cochrane guidelines. For this reason, we excluded the Current Controlled Trials and the Nederlands Trials register in the list of resources searched, but included ISRCTN Register (www.isrctn.com/) in the resources searched for this review.
When searching other resources for potential information about trials that had not yet been published, the years of the proceedings from certain association meetings differed from the protocol, in accordance with the availability of resources.
We have changed the wording of the first primary outcome, from "Recurrence of reflux at six weeks (determined by recanalisation on ultrasound)" to "Recanalisation or persistence of reflux at six weeks" since this describes the outcome more accurately, and we no longer categorise recurrence of reflux into total, segmental or none.
We have changed the end‐point for short‐term follow‐up from one month, as specified in the protocol, to six weeks because six weeks appears to be common practice.
We have clarified the outcome "Clinical evidence of recurrence (i.e. presence of visible varicose veins)" to become "Clinical evidence of recurrence (i.e. presence of new visible varicose veins)."
The unit of analysis now for all outcomes is the participants and not limbs, as was originally stated in the protocol for outcomes such as recurrence or reintervention, where bilateral procedures are possible.
For the outcome recurrence of reflux, we have deviated from the original protocol and present results for one and two years to explore whether the early results of treatment are maintained in medium‐term follow‐up. In quality of life analysis, the protocol specified no time points; we decided to include data for six weeks, six months and one year.
Results from studies that include great saphenous vein (GSV) varices and SSV varices will be underpowered in this review, since we have only included data from a subset of participants in the trial, whereas the sample‐size estimation for adequate power for the trial was based on the inclusion of participants with GSV varices, SSV varices or both types of varicose vein. Where such studies are included in meta‐analyses in this review, we have conducted sensitivity analyses and excluded these studies; these sensitivity analyses were not specified in the protocol.
Contributions of authors
SP: selected studies for inclusion, extracted data, assessed the quality of studies and wrote the review.
MH: selected studies for inclusion, extracted data, assessed the quality of studies, performed data analysis and wrote the review.
PDD: contributed to the review.
Sources of support
Internal sources
No sources of support supplied
External sources
-
National Institute for Health Research (NIHR), UK.
This project was supported by the NIHR, via Cochrane Incentive scheme award funding to Cochrane Vascular (15/81/09). The views and opinions expressed therein are those of the review authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, National Health Service or the Department of Health.
-
Chief Scientist Office, Scottish Government Health Directorates, The Scottish Government, UK.
The Cochrane Vascular editorial base is supported by the Chief Scientist Office.
Declarations of interest
SP: none known.
MH: none known.
PDD is a director of Vasacare Ltd, a specialist vascular services provider. He has received sponsorship to attend proprietary training in the use of ClariVein mechano‐chemical ablation and VenaSeal (Sapheon Inc) vein adhesive.
New
References
References to studies included in this review
CLASS {published data only}
- Brittenden J. Randomised controlled trial comparing foam sclerotherapy, alone or in combination with endovenous laser therapy, with conventional surgery as a treatment for varicose veins (ISRCTN 51995477). www.controlled‐trials.com/ISRCTN51995477 Date first received: 25 February 2008.
- Brittenden J, Cotton SC, Elders A, Ramsay CR, Norrie J, Burr J, et al. A randomized trial comparing treatments for varicose veins. New England Journal of Medicine 2014;371(13):1218‐27. [DOI] [PubMed] [Google Scholar]
- Brittenden J, Cotton SC, Elders A, Tassie E, Scotland G, Ramsay CR, et al. Clinical effectiveness and cost‐effectiveness of foam sclerotherapy, endovenous laser ablation and surgery for varicose veins: results from the Comparison of LAser, Surgery and foam Sclerotherapy (CLASS) randomised controlled trial. Health Technology Assessment (Winchester, England) 2015;19(27):1‐341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- ISRCTN51995477. The CLASS study. Comparison of LAser, Surgery and foam Sclerotherapy. Research protocol (Protocol 09PRT/2275; EudraCT 2008‐001069‐26) Randomised controlled trial comparing foam sclerotherapy, alone or in combination with endovenous laser therapy, with conventional surgery as a treatment for varicose veins. NIHR Health Technology Assessment Programme www.nets.nihr.ac.uk/__data/assets/pdf_file/0004/51448/PRO‐06‐45‐02.pdf (accessed 12 July 2016).
- Tassie E, Scotland G, Brittenden J, Cotton SC, Elders A, Campbell MK, et al. Cost‐effectiveness of ultrasound‐guided foam sclerotherapy, endovenous laser ablation or surgery as treatment for primary varicose veins from the randomized CLASS trial. British Journal of Surgery 2014;101:1532‐40. [DOI] [PubMed] [Google Scholar]
HELP 2 {published data only}
- ISRCTN56883670. EVLT for sapheno‐popliteal incompetence and SS reflux: a RCT. www.isrctn.com/ISRCTN56883670 Date first received: 29 September 2006.
- NCT00841178. Endovenous laser therapy (EVLT) for sapheno‐popliteal incompetence and short saphenous vein (SSV) reflux: a RCT. clinicaltrials.gov/ct2/show/NCT00841178 Date first received: 10 February 2009.
- Nandhra S, El‐Sheikha J, Carradice D, Wallace T, Souroullas P, Samuel N, et al. A randomized clinical trial of endovenous laser ablation versus conventional surgery for small saphenous varicose veins. Journal of Vascular Surgery 2015;61(3):741‐6. [DOI] [PubMed] [Google Scholar]
- Samuel N, Carradice D, Mekako AI, Wallace T, Hatfield J, Chetter IC. Randomised trial of endovenous laser ablation versus surgery for small saphenous varicose veins. The Vascular Society of Great Britain & Ireland Yearbook 2011 2011:82.
- Samuel N, Carradice D, Wallace T, Mekako A, Hatfield J, Chetter I. Randomized clinical trial of endovenous laser ablation versus conventional surgery for small saphenous varicose veins. Annals of Surgery 2013;257(3):419‐26. [DOI] [PubMed] [Google Scholar]
VESPA {published data only}
- NTR1554. VESPA trial: endovenous laser treatment versus crossectomy of the small saphenous vein. www.trialregister.nl/trialreg/admin/rctview.asp?TC=1554 Date first received: 24 November 2008.
- Roopram AD, Lind MY, Brussel JP, Terlouw‐Punt LC, Birnie E, Smet AA, et al. Endovenous laser ablation versus conventional surgery in the treatment of small saphenous vein incompetence. Journal of Vascular Surgery: Venous and Lymphatic Disorders 2013;1(4):357‐63. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Ariyoshi 1996 {published data only}
- Ariyoshi H, Kambayashi J‐I, Tominaga S, Hatanaka T. The possible risk of lower‐limb sclerotherapy causing an extended hypercoagulable state. Surgery Today 1996;26(5):323‐7. [DOI] [PubMed] [Google Scholar]
Beale 2005 {published data only}
- Beale R, Theivacumar N, Mavor AID, Gough MJ. Endovenous laser treatment (EVLT) or surgery of varicose veins? A randomised controlled trial in patients with saphenofemoral and long saphenous incompetence. Yearbook 2005, The Vascular Society of Great Britain & Ireland. 2005:Abstract 77.
Campos 2015 {published data only}
- Campos W, Torres IO, Silva ES, Casella IB, Puech‐Leao P. A prospective randomized study comparing polidocanol foam sclerotherapy with surgical treatment of patients with primary chronic venous insufficiency and ulcer. Annals of Vascular Surgery 2015;29(6):1128‐35. [DOI] [PubMed] [Google Scholar]
Chant 1972 {published data only}
- Beresford SAA, Chant ADB, Jones HO, Piachaud D, Weddell JM. Varicose veins: a comparison of surgery and injection/compression sclerotherapy. Lancet 1978;1(8070):921‐4. [DOI] [PubMed] [Google Scholar]
- Chant ADB, Jones HO, Weddell JM. Varicose veins: a comparison of surgery and injection/compression sclerotherapy. Lancet 1972;2:1188‐91. [DOI] [PubMed] [Google Scholar]
- Piachaud D, Weddell JM. The economics of treating varicose veins. International Journal of Epidemiology 1972;1(3):287‐94. [DOI] [PubMed] [Google Scholar]
Compagna 2010 {published data only}
- Compagna R, Vito D, Rossi R, Fappiano F, Magistris L, Sodano L, et al. A prospective randomised controlled trial comparing foam sclerotherapy combined with sapheno‐femoral ligation to surgical treatment of varicose veins. European Surgical Research 2010;45(3‐4):267. [Google Scholar]
Doran 1975 {published data only}
- Doran FSA, White M. A clinical trial designed to discover if the primary treatment of varicose veins should be by Fegan's method or by an operation. British Journal of Surgery 1975;62:72‐6. [DOI] [PubMed] [Google Scholar]
Einarsson 1993 {published data only}
- Einarsson E, Eklof B, Neglén P. Sclerotherapy or surgery as treatment for varicose veins: a prospective randomized study. Phlebology 1993;8:22‐6. [Google Scholar]
- Neglén P, Einarsson E, Eklof B. The functional long‐term value of different types of treatment for saphenous vein incompetence. Journal of Cardiovascular Surgery 1993;34:295‐301. [PubMed] [Google Scholar]
Figueiredo 2009 {published data only}
- Figueiredo M, Araujo S, Barros N Jr, Miranda F Jr. Results of surgical treatment compared with ultrasound‐guided foam sclerotherapy in patients with varicose veins: a prospective randomised study. European Journal of Vascular and Endovascular Surgery 2009;38(6):758‐63. [DOI] [PubMed] [Google Scholar]
Flessenkamper 2012 {published data only}
- Flessenkamper I, Stenger D, Hartmann M, Roll S. Saphenofemorale neoreflux after endovenous laser therapy, high ligation/stripping or high ligation/laser therapy. Interim results of a prospective randomized controlled multicentre trial [Saphenofemoraler neoreflux nach lasertherapie, crossektomie/stripping oder crossektomie/ lasertherapie. Interimsergebnisse einer prospektiven randomisierten Multizenterstudie]. Phlebologie 2012;41(6):289‐94. [Google Scholar]
HELP 1 {published data only}
- Carradice D, Mekako A, Hatfield J, Chetter I. Recurrent varicose veins are more common following surgery than EVLT ‐ results of a randomised controlled trial. The Vascular Society of Great Britain & Ireland Yearbook 2009. 2009:86.
- Carradice D, Mekako AI, Hatfield J, Chetter IC. A randomised trial of EVLT vs surgery for varicose veins. The Vascular Society of Great Britain & Ireland Yearbook 2008. 2008:91.
- Carradice D, Wallace T, Gohil R, Chetter I. A comparison of the effectiveness of treating those with and without the complications of superficial venous insufficiency. Annals of Surgery 2014;260(2):396‐401. [DOI] [PubMed] [Google Scholar]
- Carradice D, Wallace T, Samuel N, Gohil R, Chetter I. A comparison of the effectiveness of treating those with and without the complications of superficial venous insufficiency. Vascular Society of Great Britain and Ireland Annual General Meeting. 2012:38.
Hobbs 1974 {published data only}
- Hobbs JT. Surgery and sclerotherapy in the treatment of varicose veins. A random trial. Archives of Surgery 1974;109:793‐6. [DOI] [PubMed] [Google Scholar]
- Hobbs JT. Surgery or sclerotherapy for varicose veins. 10 year results of a random trial. In: Tesi M, Dormandy JA editor(s). Superficial and Deep Venous Diseases of the Lower Limbs / Surgical Therapy. Turin: Panminerva Medica, 1984:243‐8. [Google Scholar]
- Hobbs JT. The treatment of varicose veins. A random trial of injection‐compression therapy versus surgery. British Journal of Surgery 1968;55(10):777‐80. [DOI] [PubMed] [Google Scholar]
ISRCTN06552809 {published data only}
- ISRCTN06552809. VNUS vs ClariVein for varicose veins. www.isrctn.com/ISRCTN06552809 Date first received: 22 July 2012.
ISRCTN08060326 {published data only}
- ISRCTN08060326. Endovenous laser ablation (EVLA), radio frequency (RF), foam sclerotherapy and stripping for treatment of varicose veins. www.isrctn.com/ISRCTN08060326 Date first received: 31 July 2009.
Iwamoto 2003 {published data only}
- Iwamoto S, Ikeda M, Kawasaki T, Monden M. Treatment of varicose veins: an assessment of intraoperative and postoperative compression sclerotherapy. Annals of Vascular Surgery 2003;17(3):290‐5. [DOI] [PubMed] [Google Scholar]
Jakobsen 1979 {published data only}
- Jakobsen BH. The value of different forms of treatment for varicose veins. British Journal of Surgery 1979;66:182‐4. [DOI] [PubMed] [Google Scholar]
Kalodiki 2012 {published data only}
- Kalodiki E, Lattimer CR, Azzam M, Shawish E, Bountouroglou D, Geroulakos G. Long‐term results of a randomized controlled trial on ultrasound‐guided foam sclerotherapy combined with saphenofemoral ligation vs standard surgery for varicose veins. Journal of Vascular Surgery 2012;55(2):451‐7. [DOI] [PubMed] [Google Scholar]
Liu 2011 {published data only}
- Liu P, Ren S, Yang Y, Liu J, Ye Z, Lin F. Intravenous catheter‐guided laser ablation: a novel alternative for branch varicose veins. International Surgery 2011;96(4):331‐6. [DOI] [PubMed] [Google Scholar]
MESSI trial 2014 {published data only}
- Boersma D, Eekeren RR, Kelder HJ, Werson DA, Holewijn S, Schreve MA, et al. Mechanochemical endovenous ablation versus radiofrequency ablation in the treatment of primary small saphenous vein insufficiency (MESSI trial): study protocol for a randomized controlled trial. Trials 2014;15:421. [DOI: 10.1186/1745-6215-15-421] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ogawa 2008 {published data only}
- Ogawa T, Hoshino S, Makimura S, Shigematsu H, Azuma N, Sasajima T, et al. Endovenous laser ablation compared with stripping ‐ multicenter RCT in Japan. American Venous Forum Annual Meeting; 2008 Feb; Charleston, SC, USA. 2008.
REACTIV trial 2006 {published data only}
- Michaels JA, Campbell WB, Brazier JE, MacIntyre JB, Palfreyman SJ, Ratcliffe J, et al. Randomised clinical trial, observational study and assessment of cost‐effectiveness of the treatment of varicose veins (REACTIV trial). Health Technology Assessment (Winchester, England) 2006;10(13):1‐196. [DOI] [PubMed] [Google Scholar]
Seddon 1973 {published data only}
- Seddon J. The management of varicose veins. British Journal of Surgery 1973;60(5):345‐7. [DOI] [PubMed] [Google Scholar]
Shouler 1989 {published data only}
- Shouler PJ, Runchman PC. Varicose veins: optimum compression after surgery and sclerotherapy. Annal of the Royal College of Surgeons of England 1989;71:402‐4. [PMC free article] [PubMed] [Google Scholar]
VEDICO trial 1998 {published data only}
- Belcaro G, Cesarone MR, Renzo A, Brandolini R, Coen L, Acerbi G, et al. Foam‐sclerotherapy, surgery, sclerotherapy, and combined treatment for varicose veins: a 10‐year, prospective, randomized, controlled, trial (VEDICO trial). Angiology 2003;54(3):307‐15. [DOI] [PubMed] [Google Scholar]
- Belcaro G, Christopoulos D, Vasdekis S. Treatment of superficial venous incompetence with the SAVAS technique. (Section ambulatoire des varices avec sclerotherapie). A four year randomised, controlled trial comparing venous hemodynamic and costing after SAVAS, sclerotherapy and the dentist's technique. Journal des Maladies Vasculaires 1991;16:23‐7. [PubMed] [Google Scholar]
- Belcaro G, Dugall M, Vasdekis S, Christopoulos D, Laurora G, Nicolaides AN, et al. Comparison between endovascular sclerotherapy, surgery and surgery plus sclerotherapy in the treatment of superficial vein insufficiency. A randomized study on 10 years follow‐up. Angeiologie 1998;50(1):57‐61. [Google Scholar]
- Belcaro G, Nicolaides AN, Ricci A, Dugall M, Errichi BM, Vasdekis S, et al. Endovascular sclerotherapy, surgery, and surgery plus sclerotherapy in superficial venous incompetence: a randomized, 10‐year follow‐up trial ‐ final results. Angiology 2000;51(7):529‐34. [DOI] [PubMed] [Google Scholar]
Wilhelmi 2009 {published data only}
- Wilhelmi M, Hoch A, Hoch W, Pichlmaier AM, Teebken OE, Bisdas T, et al. Effectiveness and clinical outcome following endovenous therapy of primary varicose veins: first results of a randomised, prospective study comparing the VNUS closure fast system, 980nm and 1470nm lasers and conventional surgery. XVI World Congress of the Union Internationale de Phlebologie Abstract Book. 2009.
Wright 2006 {published data only}
- Wright D. European randomized controlled trial of Varisolve® PD microfoam compared with alternative therapy in management of moderate‐to‐severe varicose veins: preliminary results. UIP World Congress Chapter Meeting; 2003 Aug 27‐31; San Diego, CA. 2003.
- Wright D, Gobin JP, Bradbury AW, Coleridge‐Smith P, Spoelstra H, Berridge D, et al. Varisolve polidocanol microfoam compared with surgery or sclerotherapy in the management of varicose veins in the presence of trunk vein incompetence: European randomized controlled trial. Phlebology 2006;21(4):180‐90. [Google Scholar]
References to studies awaiting assessment
Boisseau 2015 {published data only}
- Boisseau M. A randomized trial comparing treatments for varicose veins. Angeiologie 2015;66:60‐1. [Google Scholar]
Additional references
Almgren 1990
- Almgren B, Eriksson I. Valvular incompetence in superficial, deep and perforator veins of limbs with varicose veins. Acta Chirugica Scandinavica 1990;156(1):69‐74. [PubMed] [Google Scholar]
Brar 2010
- Brar R, Nordon IM, Hinchliffe RJ, Loftus IM, Thompson MM. Surgical management of varicose veins: meta‐analysis. Vascular 2010;18(4):205‐20. [DOI] [PubMed] [Google Scholar]
Carroll 2014
- Carroll C, Hummel S, Leaviss J, Ren S, Stevens JW, Cantrell A, et al. Systematic review, network meta‐analysis and exploratory cost‐effectiveness model of randomized trials of minimally invasive techniques versus surgery for varicose veins. British Journal of Surgery 2014;101:1040‐52. [DOI] [PubMed] [Google Scholar]
GRADE Working Group 2004
- GRADE Working Group 2004. Grading quality of evidence and strength of recommendations. BMJ 2004;328:1490‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
GRADEpro GDT 2015 [Computer program]
- GRADEpro GDT. GRADEpro Guideline Development Tool (GRADEpro GDT). Hamilton (ON): GRADE Working Group, McMaster University, 2015.
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
Hoggan 2009
- Hoggan BL, Cameron AL, Maddern JJ. Systematic review of endovenous laser therapy versus surgery for the treatment of saphenous varicose veins. Annals of Vascular Surgery 2009;23:277‐87. [DOI] [PubMed] [Google Scholar]
Langendam 2013
- Langendam M, Akl EA, Dahm P, Glasziou P, Guyatt G, Schünemann HJ. Assessing and presenting summaries of evidence in Cochrane Reviews. Systematic Reviews 2013;2:81. [DOI] [PMC free article] [PubMed] [Google Scholar]
Leopardi 2009
- Leopardi D, Hoggan BL, Fitridge RA, Woodruff PWH, Maddern GJ. Systematic review of treatments for varicose veins. Annals of Vascular Surgery 2009;23:264‐76. [DOI] [PubMed] [Google Scholar]
Luebke 2008
- Luebke T, Brunkwall J. Systematic review and meta‐analysis of endovenous radiofrequency obliteration, endovenous laser therapy, and foam sclerotherapy for primary varicosis. Journal of Cardiovascular Surgery 2008;49:213‐33. [PubMed] [Google Scholar]
Murad 2011
- Murad MH, Coto‐Yglesias F, Zumaeta‐Garcia M, Elamin MB, Duggirala MK, Erwin PJ, et al. A systematic review and meta‐analysis of the treatments of varicose veins. Journal of Vascular Surgery 2011;53:49S‐65S. [DOI] [PubMed] [Google Scholar]
Nelzén 2015
- Nelzén O, Cervin A, Daxberg E‐L, Drott C, Gelin J, Persson J, et al. Endovenous interventions on varicose veins of the leg [Endovenösa interventioner mot åderbråck]. Göteborg: Västra Götalandsregionen, Sahlgrenska Universitetssjukhuset, HTA‐centrum. Regional activity‐based HTA 2015; Vol. 77.
Nesbitt 2014
- Nesbitt C, Bedenis R, Bhattacharya V, Stansby G. Endovenous ablation (radiofrequency and laser) and foam sclerotherapy versus open surgery for great saphenous vein varices. Cochrane Database of Systematic Reviews 2014, Issue 7. [DOI: 10.1002/14651858.CD005624.pub3] [DOI] [PubMed] [Google Scholar]
NICE 2013
- National Institute for Health and Care Excellence. Varicose veins in the legs. The diagnosis and management of varicose veins [CG168], 2013. www.nice.org.uk/nicemedia/live/14226/64566/64566.pdf (accessed 14 August 2013). [PubMed]
RevMan 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rigby 2009
- Rigby KA, Palfreyman SSJ, Beverley C, Michaels JA. Surgery versus sclerotherapy for the treatment of varicose veins. Cochrane Database of Systematic Reviews 2009, Issue 1. [DOI: 10.1002/14651858.CD004980] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sam 2004
- Sam RC, Silverman SH, Bradbury AW. Nerve injuries and varicose vein surgery. European Journal of Vascular and Endovascular Surgery 2004;27(2):113‐20. [DOI] [PubMed] [Google Scholar]
Siribumrungwong 2012
- Siribumrungwong B, Noorit P, Wilasrusmee C, Attia J, Thakkinstian A. A systematic review and meta‐analysis of randomised controlled trials comparing endovenous ablation and surgical intervention in patients with varicose vein. European Journal of Vascular and Endovascular Surgery 2012;44:214‐23. [DOI] [PubMed] [Google Scholar]
Tellings 2011
- Tellings SS, Ceulen RP, Sommer A. Surgery and endovenous techniques for the treatment of small saphenous varicose veins: a review of the literature. Phlebology 2011;26(5):179‐84. [DOI] [PubMed] [Google Scholar]
van den Bos 2009
- Bos R, Arends L, Kockaert M, Neumann M, Nijsten T. Endovenous therapies of lower extremity varicosities: a meta‐analysis. Journal of Vascular Surgery 2009;49:230‐9. [DOI] [PubMed] [Google Scholar]
Winterborn 2004
- Winterborn RJ, Campbell WB, Heather BP, Earnshaw JJ. The management of short saphenous varicose veins: a survey of the members of the vascular surgical society of Great Britain and Ireland. European Journal of Vascular and Endovascular Surgery 2004;28(4):400‐3. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Paravastu 2013
- Paravastu SCV, Dodd PDF. Endovenous ablation therapy (LASER or radiofrequency) or foam sclerotherapy versus conventional surgical repair for short saphenous varicose veins. Cochrane Database of Systematic Reviews 2013, Issue 12. [DOI: 10.1002/14651858.CD010878] [DOI] [PMC free article] [PubMed] [Google Scholar]