

Abstract
Background
Nicotine replacement therapy (NRT) aims to replace nicotine from cigarettes to ease the transition from cigarette smoking to abstinence. It works by reducing the intensity of craving and withdrawal symptoms. Although there is clear evidence that NRT used after smoking cessation is effective, it is unclear whether higher doses, longer durations of treatment, or using NRT before cessation add to its effectiveness.
Objectives
To determine the effectiveness and safety of different forms, deliveries, doses, durations and schedules of NRT, for achieving long‐term smoking cessation, compared to one another.
Search methods
We searched the Cochrane Tobacco Addiction Group trials register, and trial registries for papers mentioning NRT in the title, abstract or keywords. Date of most recent search: April 2018.
Selection criteria
Randomized trials in people motivated to quit, comparing one type of NRT use with another. We excluded trials that did not assess cessation as an outcome, with follow‐up less than six months, and with additional intervention components not matched between arms. Trials comparing NRT to control, and trials comparing NRT to other pharmacotherapies, are covered elsewhere.
Data collection and analysis
We followed standard Cochrane methods. Smoking abstinence was measured after at least six months, using the most rigorous definition available. We extracted data on cardiac adverse events (AEs), serious adverse events (SAEs), and study withdrawals due to treatment. We calculated the risk ratio (RR) and the 95% confidence interval (CI) for each outcome for each study, where possible. We grouped eligible studies according to the type of comparison. We carried out meta‐analyses where appropriate, using a Mantel‐Haenszel fixed‐effect model.
Main results
We identified 63 trials with 41,509 participants. Most recruited adults either from the community or from healthcare clinics. People enrolled in the studies typically smoked at least 15 cigarettes a day. We judged 24 of the 63 studies to be at high risk of bias, but restricting the analysis only to those studies at low or unclear risk of bias did not significantly alter results, apart from in the case of the preloading comparison. There is high‐certainty evidence that combination NRT (fast‐acting form + patch) results in higher long‐term quit rates than single form (RR 1.25, 95% CI 1.15 to 1.36, 14 studies, 11,356 participants; I2 = 4%). Moderate‐certainty evidence, limited by imprecision, indicates that 42/44 mg are as effective as 21/22 mg (24‐hour) patches (RR 1.09, 95% CI 0.93 to 1.29, 5 studies, 1655 participants; I2 = 38%), and that 21 mg are more effective than 14 mg (24‐hour) patches (RR 1.48, 95% CI 1.06 to 2.08, 1 study, 537 participants). Moderate‐certainty evidence (again limited by imprecision) also suggests a benefit of 25 mg over 15 mg (16‐hour) patches, but the lower limit of the CI encompassed no difference (RR 1.19, 95% CI 1.00 to 1.41, 3 studies, 3446 participants; I2 = 0%). Five studies comparing 4 mg gum to 2 mg gum found a benefit of the higher dose (RR 1.43, 95% CI 1.12 to 1.83, 5 studies, 856 participants; I2 = 63%); however, results of a subgroup analysis suggest that only smokers who are highly dependent may benefit. Nine studies tested the effect of using NRT prior to quit day (preloading) in comparison to using it from quit day onward; there was moderate‐certainty evidence, limited by risk of bias, of a favourable effect of preloading on abstinence (RR 1.25, 95% CI 1.08 to 1.44, 9 studies, 4395 participants; I2 = 0%). High‐certainty evidence from eight studies suggests that using either a form of fast‐acting NRT or a nicotine patch results in similar long‐term quit rates (RR 0.90, 95% CI 0.77 to 1.05, 8 studies, 3319 participants; I2 = 0%). We found no evidence of an effect of duration of nicotine patch use (low‐certainty evidence); 16‐hour versus 24‐hour daily patch use; duration of combination NRT use (low‐ and very low‐certainty evidence); tapering of patch dose versus abrupt patch cessation; fast‐acting NRT type (very low‐certainty evidence); duration of nicotine gum use; ad lib versus fixed dosing of fast‐acting NRT; free versus purchased NRT; length of provision of free NRT; ceasing versus continuing patch use on lapse; and participant‐ versus clinician‐selected NRT. However, in most cases these findings are based on very low‐ or low‐certainty evidence, and are the findings from single studies.
AEs, SAEs and withdrawals due to treatment were all measured variably and infrequently across studies, resulting in low‐ or very low‐certainty evidence for all comparisons. Most comparisons found no evidence of an effect on cardiac AEs, SAEs or withdrawals. Rates of these were low overall. Significantly more withdrawals due to treatment were reported in participants using nasal spray in comparison to patch in one trial (RR 3.47, 95% CI 1.15 to 10.46, 922 participants; very low certainty) and in participants using 42/44 mg patches in comparison to 21/22 mg patches across two trials (RR 4.99, 95% CI 1.60 to 15.50, 2 studies, 544 participants; I2 = 0%; low certainty).
Authors' conclusions
There is high‐certainty evidence that using combination NRT versus single‐form NRT, and 4 mg versus 2 mg nicotine gum, can increase the chances of successfully stopping smoking. For patch dose comparisons, evidence was of moderate certainty, due to imprecision. Twenty‐one mg patches resulted in higher quit rates than 14 mg (24‐hour) patches, and using 25 mg patches resulted in higher quit rates than using 15 mg (16‐hour) patches, although in the latter case the CI included one. There was no clear evidence of superiority for 42/44 mg over 21/22 mg (24‐hour) patches. Using a fast‐acting form of NRT, such as gum or lozenge, resulted in similar quit rates to nicotine patches. There is moderate‐certainty evidence that using NRT prior to quitting may improve quit rates versus using it from quit date only; however, further research is needed to ensure the robustness of this finding. Evidence for the comparative safety and tolerability of different types of NRT use is of low and very low certainty. New studies should ensure that AEs, SAEs and withdrawals due to treatment are both measured and reported.
Plain language summary
What is the best way to use nicotine replacement therapy to quit smoking?
Background
Nicotine replacement therapy (NRT) is a medicine that is available as skin patches, chewing gum, nasal and oral sprays, inhalers, lozenges and tablets that deliver nicotine to the brain. The aim of NRT is to replace the nicotine that people who smoke usually get from cigarettes, so the urge to smoke is reduced and they can stop smoking altogether. We know that NRT improves a person's chances of stopping smoking, and that people use it to quit. This review looks at the different ways to use NRT to quit smoking, and which of these work best to quit smoking for six months or longer.
Study characteristics
This review includes 63 trials covering 41,509 participants. All studies were conducted in people who wanted to quit smoking, and most were conducted in adults. People who enrolled in the studies typically smoked at least 15 cigarettes a day at the start of the studies. Studies lasted for at least six months.The evidence is up to date to April 2018.
Key results
Using nicotine patch and another type of NRT (such as gum or lozenge) together made it 15% to 36% more likely that a person would successfully stop smoking than if they used one type of NRT alone. People were also more likely to quit successfully if they used higher‐dose nicotine patches (containing 25 mg (worn over 16 hours) or 21 mg (worn over 24 hours) of nicotine compared to 15 mg (worn over 16 hours) or 14 mg of nicotine (worn over 24 hours)) or higher‐dose nicotine gum (containing 4 mg of nicotine compared to 2 mg of nicotine). Using NRT before a quit day as well as after may help more people to quit than only using it after, but more evidence is needed to strengthen this conclusion. However, people who smoke have the same chances of quitting successfully whether they use a nicotine patch to quit or another type of NRT, such as gum, lozenge or nasal spray.
We also looked at how long NRT should be used for, whether NRT should be used on a schedule or as wanted, and whether more people stop smoking when NRT is provided for free versus if they have to pay for it. However, more research is needed to answer these questions.
Most studies did not look at safety. Where studies did look at safety, very few people experienced negative effects of NRT. Evidence from another review shows that NRT is a safe medication.
Quality of the evidence
There is high‐certainty evidence that combination NRT works better than a single form of NRT, that higher‐dose nicotine gum works better than lower‐dose gum, and that there is no difference in effect between different types of NRT (such as gum or lozenge). This means that future research is very unlikely to change our conclusions. This is because the evidence is based on a large number of participants, and the studies were well‐conducted. However, the quality of the evidence was moderate, low or very low for all of the other questions we looked at. This means that our findings may change when more new research is carried out. In most cases this is because there were not enough studies, there were problems with the design of studies that do exist, and these studies were too small. We rated all of the evidence looking at the safety of using NRT in different ways to be low or very low quality, because many studies did not report on safety.
Summary of findings
Background
Description of the condition
Tobacco use is one of the leading causes of preventable illness and death worldwide, accounting for over seven million deaths annually (GBD 2015 Risk Factors Collaborators 2016). Extrapolation based on current smoking trends suggests that without widespread quitting approximately 400 million tobacco‐related deaths will occur between 2010 and 2050, mostly among current smokers (Jha 2011). Most smokers would like to stop (CDC 2017); however, quitting tobacco use is difficult. This is because users develop both a psychological and physiological dependence on smoking. The physiological dependence is caused by a component of tobacco called nicotine (McNeill 2017).
Description of the intervention
Nicotine replacement therapy (NRT) is a medication formulated for absorption through the oral mucosa (chewing gum, lozenges, sublingual tablets, inhaler/inhalator), nasal mucosa (spray), or skin (transdermal patches). Nicotine patches are worn on the body and deliver a nicotine dose slowly and passively through the skin. They do not replace any of the behavioural activities of smoking. In contrast, the other types of NRT mimic some of the hand‐to‐mouth actions of smoking or provide an oral substitute, or do both, and are faster‐acting, but require more effort on the part of the user. Transdermal patches are available in several different doses, and deliver between 5 mg and 52.5 mg of nicotine over a 24‐hour period, resulting in plasma levels similar to the trough levels seen between cigarettes in heavy smokers (Fiore 1992). Some brands of patch are designed to be worn for 24 hours, whilst others are to be worn for 16 hours each day. Nicotine gum is available in both 2 mg and 4 mg strengths, and nicotine lozenges are available in 1 mg, 1.5 mg, 2 mg and 4 mg strengths, although the amount of nicotine absorbed by the user is less than the original dose. The availability of NRT products on prescription or for over‐the‐counter purchase varies from country to country. Table 8 summarizes the products currently licensed in the United Kingdom.
1. Nicotine replacement therapies available in the UK.
| Type | Available doses |
| Nicotine transdermal patches | Worn over 16 hours: 5 mg, 10 mg, 15 mg, 25 mg doses Worn over 24 hours: 7 mg, 14 mg, 20 mg, 21 mg, 30 mg dosesa |
| Nicotine chewing gum | 2 mg and 4 mg doses |
| Nicotine sublingual tablet | 2 mg dose |
| Nicotine lozenge | 1 mg, 1.5 mg, 2 mg and 4 mg doses |
| Nicotine inhalation cartridge plus mouthpiece | Cartridge containing 10 mg |
| Nicotine metered nasal spray | 0.5 mg dose/spray |
| Nicotine oral spray | 1 mg dose/spray |
Information extracted from British National Formulary
a35 mg/24‐hour and 53.5 mg/24‐hour patches available in other regions.
How the intervention might work
When a person stops using tobacco, the aim of NRT is to replace the nicotine that the smoker would have been receiving, without the additional harmful elements of tobacco (McNeill 2017). This should reduce the motivation to smoke and the physiological and psychomotor withdrawal symptoms often experienced during an attempt to stop smoking, thereby increasing the likelihood of remaining abstinent (West 2001). Nicotine undergoes first‐pass metabolism in the liver, reducing the overall bio‐availability of swallowed nicotine pills. A pill that could reliably produce high enough nicotine levels in the central nervous system would risk causing adverse gastrointestinal effects. This is why NRT was formulated for absorption through the skin or oral/nasal mucosa.
None of the available NRT products delivers such high doses of nicotine as quickly as cigarettes. The average cigarette delivers between 1 and 3 mg of nicotine and the typical pack‐a‐day smoker absorbs 20 to 40 mg of nicotine each day (Henningfield 2005). However, despite this, there is high‐certainty well‐accepted evidence that NRT helps some people to stop smoking. A recent Cochrane Review comparing any NRT product to control for smoking cessation identified 133 studies, with 64,640 participants eligible for inclusion in the main meta‐analysis. This resulted in a risk ratio (RR) of 1.55 (95% confidence interval (CI) 1.49 to 1.61; high‐certainty evidence) (Hartmann‐Boyce 2018). In addition, many clinical guidelines recommend NRT as a first‐line treatment for people seeking pharmacological help to stop smoking (West 2000; Woolacott 2002; Italy ISS 2004; Le Foll 2005; NZ MoH 2007; Fiore 2008; Zwar 2011).
Why it is important to do this review
The aforementioned Cochrane Review comparing NRT to control (Hartmann‐Boyce 2018) was first published over 20 years ago, in 1996 (Silagy 1996), and has been regularly updated since then. Despite the number of included studies more than doubling over this time, the main effect estimate has remained stable. This most recent publication is therefore intended to be the final time the Cochrane Tobacco Addiction Group will review the evidence comparing NRT to placebo or to no pharmacotherapy, as our confidence in this effect estimate is high, and unlikely to be changed by further research.
However, this is not to say that all questions about NRT have been answered. Evidence is still needed comparing different forms, deliveries, doses, durations and schedules of NRT, to see whether the effectiveness of NRT differs when used in different ways, and therefore whether it is possible to use NRT in specific ways to maximize success. These issues used to be considered in the aforementioned review of NRT versus control, but as the Cochrane Tobacco Addiction Group has decided to stop updating evidence comparing NRT to control we have decided to split the previous original version of this review (Stead 2012) into two reviews. Studies comparing NRT to control can now be found in Hartmann‐Boyce 2018, and studies comparing different types of NRT use will be reviewed here.
As well as comparing different types and uses of NRT, there are other questions that would still benefit from further research. These are covered in the following separate Cochrane Reviews, which we will continue to update: comparing NRT to other pharmacotherapies (Hughes 2014; Cahill 2016); testing the efficacy of NRT in special populations where we may reasonably hypothesize that its effectiveness differs from that in the general population, such as pregnant women (Coleman 2015) and adolescents (Fanshawe 2017); and testing the effectiveness and safety of electronic cigarettes containing nicotine, which we do not include in this review, but could be considered a form of NRT (Hartmann‐Boyce 2016).
Objectives
To determine the effectiveness and safety of different forms, deliveries, doses, durations and schedules of nicotine replacement therapy (NRT), for achieving long‐term smoking cessation, compared to one another.
Methods
Criteria for considering studies for this review
Types of studies
Randomized controlled trials, including cluster‐randomized trials and quasi‐randomized trials (i.e. trials where treatment allocation was not truly random).
Types of participants
We include people of any age who smoked and were motivated to quit, irrespective of the setting from which they were recruited or their initial level of nicotine dependence. We include studies that randomized therapists, rather than smokers, provided that the specific aim of the study was to examine the effect of different types of NRT use on smoking cessation. We have not included trials that randomized physicians or other therapists to receive an educational intervention, which included encouraging their patients to use NRT, but have reviewed them separately (Carson 2012).
Types of interventions
Any form, dose, duration, schedule of NRT use (this could include any type of NRT, i.e. gum, transdermal patches, nasal and oral spray, inhalers and tablets or lozenges). Eligible comparisons were any other form(s), dose(s), duration(s), schedule(s) of NRT use (this could also include any type of NRT).
The terms 'inhaler' and 'inhalator' (an oral device which delivers nicotine to the mouth by inhalation, for absorption through the buccal mucosa) are used interchangeably in the literature. We have used the term 'inhaler' throughout the rest of this review.
Studies were not eligible for inclusion if one of the study arms received an additional intervention component that could not be separated from the NRT intervention, making it impossible to establish whether any effect found was as a result of the difference in NRT use or the additional component. We have not included trials that evaluated the effect of NRT for individuals who were attempting to reduce the number of cigarettes smoked rather than to quit. They are covered by a separate review of harm reduction approaches (Lindson‐Hawley 2016).
Types of outcome measures
Primary outcomes
1) Smoking cessation. This review evaluates the effects of different NRT regimens on smoking cessation. We therefore excluded trials that did not assess smoking cessation as an outcome, and also those that followed participants for less than six months, in line with the standard methods of the Cochrane Tobacco Addiction Group. For each study, we chose the strictest available criteria to define abstinence. For example, in studies where biochemical validation of cessation was available, only those participants who met the criteria for biochemically confirmed abstinence were regarded as being abstinent. Wherever possible, we chose a measure of sustained cessation rather than point prevalence. We regard people who were lost to follow‐up as being continuing smokers (West 2005). 2) Adverse events (AEs) and serious adverse events (SAEs). Number of participants reporting cardiac AEs (as defined by study authors, but including fast or irregular heartbeat, chest pain, myocardial infarction or stroke), any SAEs, and withdrawing due to effects of the treatment where they are reported. We report cardiac AEs rather than AEs in general, as NRT is generally deemed to be safe, but cardiac AEs have been identified as a particular area of concern (Hartmann‐Boyce 2018). We did not exclude studies if they did not report AEs.
Search methods for identification of studies
Electronic searches
We searched the specialized register of the Cochrane Tobacco Addiction Group on 30 April 2018 for any reports of trials making reference to the use of NRT of any type, by searching for 'NRT', or 'nicotine' near to terms for nicotine replacement products in the title, abstract or keywords. The most recent issues of the databases included in the register as searched for the current update of this review were:
Cochrane Central Register of Controlled trials (CENTRAL), issue 3, 2018;
MEDLINE (via OVID) to update 20180404;
Embase (via OVID) to week 201814;
PsycINFO (via OVID) to update 20180326.
The search strategy for the Register is given in Appendix 1. For details of the searches used to create the specialized register see the Cochrane Tobacco Addiction Group's website. The trials register also includes trials identified by handsearching of abstract books from meetings of the Society for Research on Nicotine and Tobacco.
For previous versions of the original review we performed searches of additional databases: Cancerlit, Health Planning and Administration, Social Scisearch, Smoking & Health, and Dissertation Abstracts. Since the searches did not produce any additional trials we did not search these databases after December 1996.
Searching other resources
We searched the following trial registries: clinicaltrials.gov and www.who.int/ictrp/, from inception to 30 April 2018, using the term 'nicotine replacement therapy'. During preparation of the first version of the original review (Silagy 1996), we also sent letters to manufacturers of NRT preparations. Since this did not result in additional data we have not repeated the exercise for subsequent updates.
Data collection and analysis
Selection of studies
In previous versions of the original review (Silagy 1996; Silagy 2001; Silagy 2002; Silagy 2004; Stead 2008), one review author screened records retrieved by searches, to exclude papers that were not reports of potentially relevant studies. For the last two updates (Stead 2012 and this version), two review authors independently screened references to establish eligibility. References were screened in two stages. First, we screened titles and abstracts for eligibility (JHB, NL, SC), then for those that appeared to be eligible or eligibility was still unclear we retrieved full‐text reports. Two review authors (from JHB, NL, SC) then went on to independently screen each report for eligibility. Where there were any disagreements on eligibility between the two review authors the third review author was asked to screen the studies. We did not exclude studies based on the language of publication.
We list reports that linked to potentially relevant studies but did not report the outcomes of interest along with the main study report in the 'References to studies' section. The primary reference to the study is indicated, and for most studies we use the first author and year as the study identifier corresponds to the primary reference.
Data extraction and management
Two review authors (SC and WY) independently extracted data from the published reports and abstracts. We resolved disagreements by discussion or referral to a third party (NL). We made no attempt to blind these individuals either to the results of the primary studies or to which treatment participants received. We examined reports published only in non‐English language journals with the assistance of translators.
We extracted the following data from each study where available:
Study characteristics: references, study registration details, country, funder, author conflicts of interest, design including unit of randomization.
Recruitment methods: setting, eligibility criteria.
Participant characteristics: number randomized, gender, baseline measures, such as cigarettes per day, any measure of levels of dependence (such as the Fagerström Test for Cigarette Dependence (FTCD; Fagerström 2012)).
Intervention and comparator details: type of NRT, dosage, schedule of use, other details on methods.
Common behavioural support/intervention: mode of delivery, number of sessions, length of support sessions, any other available information.
Smoking abstinence outcome: definition of abstinence used, whether biochemical validation took place and how this was defined, number abstinent in each arm, number randomized to each arm, attrition rates.
AE/SAE outcome: whether AEs/SAEs were measured, when they were measured, number of participants reporting a cardiac AE in each arm, number of participants reporting a serious AE in each arm, number of withdrawals in each arm due to allocated treatment.
Risk of bias: information related to any of the risk of bias domains outlined below, information related to any other potential biases identified.
Assessment of risk of bias in included studies
We assessed included studies for risks of selection bias (methods of randomized sequence generation and allocation concealment), performance and detection bias (the presence or absence of blinding), attrition bias (levels and reporting of loss to follow‐up), and any other threats to study quality, using the Cochrane 'Risk of bias' tool. For each new study in this update, two review authors (SC and WY) independently assessed each study for each domain, in accordance with 'Risk of bias' guidance developed by the Cochrane Tobacco Addiction Group to assess smoking cessation studies. Where there was any disagreement on the assessment, a third review author (NL) acted as arbiter.
Measures of treatment effect
Smoking cessation
We extracted smoking cessation rates in the intervention and control groups from the reports at six or 12 months. Since not all studies reported cessation rates at exactly these intervals, we allowed a window of six weeks at each follow‐up point. For trials without 12‐month follow‐up, we used six‐month data. For trials which also reported follow‐up at more than a year we used 12‐month outcomes in most cases (we note length of follow‐up for each study in the Characteristics of included studies table). Where both validated and self‐reported quit rates were reported we used the validated rates to calculate the study treatment effect. However, where only self‐reported data were available we used these to calculate the treatment effect.
Adverse events and serious adverse events
We extracted information on whether AEs were measured, at what time points they were measured, the number of participants reporting a cardiac AE in each arm, the number of participants reporting an SAE in each arm (using the definitions provided by study authors), and the number of withdrawals in each arm due to allocated treatment.
Following the Cochrane Tobacco Addiction Group's recommended method of data analysis for dichotomous outcomes, we used the risk ratio (RR) to summarize all of the individual trial outcomes where this was possible. Whilst there are circumstances in which odds ratios (ORs) may be preferable, there is a danger that they will be interpreted as if they are RRs, making the treatment effect seem larger (Deeks 2017).
Unit of analysis issues
We had planned to include any studies that randomized participants in clusters, i.e. cluster‐RCTs, as well as those that individually randomized participants. However, none of our included studies were cluster‐randomized.
Dealing with missing data
We treated participants who dropped out or who were lost to follow‐up after randomization as being continuing smokers. We note losses to follow‐up in the 'Risk of bias' table, and whether there was high or differential loss to follow‐up. The assumption that 'missing = smoking' gives conservative absolute quit rates, and will make little difference to the RR unless dropout rates differ substantially between groups.
Assessment of heterogeneity
We assessed clinical and methodological heterogeneity, to establish how studies should be grouped and where it was appropriate to pool studies. To assess heterogeneity statistically, we used the I2 statistic, given by the formula [(Q ‐ df)/Q] x 100%, where Q is the Chi2 statistic and df is its degrees of freedom (Higgins 2003). This describes the percentage of the variability in effect estimates that is due to heterogeneity rather than to sampling error (chance). A value greater than 50% may be considered to indicate substantial heterogeneity.
Assessment of reporting biases
Reporting bias is best assessed using funnel plots, where 10 or more RCTs contribute to an outcome (Higgins 2011). Where a meta‐analysis included 10 or more studies we therefore generated and reported on a funnel plot.
Data synthesis
Following assessment of clinical heterogeneity, we separated studies into groups testing different NRT comparisons (based on types/uses of NRT):
Patch dose
Duration of patch therapy
Effect of tapering patch dose
Combination versus single form
Duration of combination therapy
Fast‐acting NRT versus patch
Type of fast‐acting NRT
Nicotine gum dose
Fixed versus ad lib dosing schedule
NRT preloading versus standard post‐quit use
Free versus purchased NRT
Duration of free NRT
Studies were eligible to fall within more than one comparison.
Smoking cessation
Within these groups, we estimated pooled weighted averages using the Mantel‐Haenszel fixed‐effect method, to generate risk ratios (RRs) and 95% confidence intervals (CIs), where appropriate. We chose a priori to use a fixed‐effect method, as we assumed that due to the nature of the intervention there would be minimal heterogeneity in the true effect. Where only one study tested a comparison we report this narratively.
Adverse events
Within the groups above we carried out three analyses where the relevant data were available. We estimated a pooled weighted average using Mantel‐Haenszel fixed‐effect methods comparing the number of cardiac AEs, SAEs, and withdrawals due to effects of the treatment, reported between trial arms. We generated effect estimates as the RR and 95% CI where appropriate.
Subgroup analysis and investigation of heterogeneity
We split the following comparisons into subgroups, to investigate whether variations between intervention characteristics resulted in varied effects:
Patch dose: studies were split according to the dosage administered, i.e. 42/44 mg versus 21/22 mg and 21/25 mg versus 14/15 mg.
Duration of patch therapy: studies split according to duration of treatment. This ranged from 2 weeks to 52 weeks.
Combination versus single‐form: studies, split by type of combination NRT used (e.g. patch plus gum, patch plus nasal spray, etc.) and type of single NRT used (e.g. gum alone, patch alone, etc.).
Duration of combination therapy: studies split according to duration of treatment. This ranged from 2 weeks to 16 weeks.
Fast‐acting NRT versus patch: studies split by type of fast‐acting NRT used.
Type of fast‐acting NRT: studies split by type of fast‐acting NRT used in either comparison group.
4 mg versus 2 mg nicotine gum: participants split into high‐ versus low‐dependency smokers, as defined by study authors.
Fixed versus ad lib dosing schedule: studies split by the type of NRT used, i.e. gum, nasal spray.
NRT preloading versus standard post‐quit use: studies split by the type of NRT used, e.g. patch, gum, patch and gum.
Free versus purchased NRT: studies split by the type of NRT used, i.e. patch, gum.
Duration of free NRT: studies split by length of period free NRT provided. This ranged from 1 week to 8 weeks.
Sensitivity analysis
We carried out the following sensitivity analyses:
We tested the impact of removing any study judged to be at high risk of bias for any domain on the relevant meta‐analyses.
In Walker 2011 a very low proportion of participants who claimed to have quit completed verification (34%). We extracted actual verified rates and used these in our main analysis, but conducted a sensitivity analysis comparing these figures to data extrapolated from these proportions to the wider trial population, and to non‐verified rates.
'Summary of findings' table
Following standard Cochrane methodology, we created 'Summary of findings' tables including the following comparisons, which we deemed to be most clinically relevant:
Patch dose
Duration of patch therapy
Combination versus single form
Duration of combination therapy
Fast‐acting NRT versus patch
Type of fast‐acting NRT
NRT preloading versus standard post‐quit use
Also following standard Cochrane methodology (Higgins 2011), we used the five GRADE considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) to assess the certainty of the body of evidence for smoking cessation, SAEs, and treatment withdrawals, and to draw conclusions about the certainty of the evidence within the text of the review.
Results
Description of studies
Results of the search
The most recent search for this update resulted in 1502 records to be screened. After duplicates were removed 1274 records remained for title and abstract screening. We ruled out 1174 records at this stage, leaving 100 for full‐text screening. Along with the 21 new included studies, there was one ongoing study, and 78 studies excluded at the full‐text screening stage. See Figure 1 for study flow information relating to the most recent update search.
1.

Flow diagram for the 2018 search update only
Included studies
The review includes 63 studies (with 41,509 participants), 21 of which are new in this update (Kupecz 1996; Tønnesen 1996; Bolliger 2007; Hall 2009; Rey 2009; Cummings 2011; Walker 2011; Abdullah 2013; Smith 2013; Caldwell 2014; Schnoll 2015; Baker 2016; Burns 2016; Caldwell 2016; Dennis 2016; Krupski 2016; Piper 2016; Schlam 2016; Tulloch 2016; Hughes 2018; Preloading Investigators 2018). Trials were conducted in the USA (39 studies), Europe (14 studies), Australasia (4 studies), South Africa (2 studies), South America, Canada, China, and in multiple regions (1 study each). The median sample size was around 400 but ranged from 45 to 3575 participants.
Participants
Participants were typically adult cigarette smokers, with an average age of approximately 45. Six trials targeted specific populations:
Moolchan 2005 recruited adolescents.
Hall 2009 recruited participants over 50 years of age.
Kornitzer 1987 recruited only men in a workplace setting.
Cooney 2009 recruited participants who were alcohol‐dependent at the time of the study.
Kalman 2006 recruited people with a history of alcohol dependence.
Dennis 2016 recruited adult smokers diagnosed with post‐traumatic stress disorder (PTSD).
Trials typically recruited people who smoked at least 15 cigarettes a day. Although some trials included lighter smokers as well (12 of the 63 trials (19%)), the average number smoked was greater than or equal to 20 a day in most studies (46 of the 63 trials (73%)). Killen 1999 recruited people smoking 25 or more cigarettes a day and Hughes 1999 recruited only people smoking 30 or more a day. Five studies did not report the average cigarettes per day of participants.
Thirty‐one studies recruited participants directly from the community, making it the most common source of recruitment. Most participants volunteered in response to media advertisements, with one study using advertisements on internet sites (Hughes 2018). A number of studies recruited through referrals from clinicians or from healthcare clinics, such as smoking cessation clinics or quit lines, substance abuse clinics, or primary care clinics, and one study recruited from referrals to a lung health clinic (Tønnesen 2000). Two studies recruited participants from previous smoking‐cessation studies (Tønnesen 1996; Baker 2016), two from worksites (Kornitzer 1987; Kornitzer 1995) and one from universities (Schnoll 2015). A number of studies used a mixture of these approaches.
Types and uses of nicotine replacement therapy
Trials addressed a range of questions relating to the effectiveness of different types and uses of NRT. The variations on NRT use tested are listed below (some studies tested more than one NRT variant):
Patch dose (nine studies): three studies compared 25 mg to 15 mg (16‐hour) patches (Paoletti 1996; CEASE 1999; Killen 1999); one study compared 21 mg to 14 mg (24‐hour) patches (TNSG 1991); two studies compared 42 mg and 21 mg (24‐hour) patches (Kalman 2006; Rose 2010); and one study compared 44 mg to 22 mg (24‐hour) patches (Jorenby 1995). Dale 1995 and Hughes 1999 both compared three different doses; 44 mg versus 22 mg versus 11 mg (24‐hour), and 42 mg versus 35 mg versus 21 mg (24‐hour) respectively.
24‐hours‐a‐day versus 16‐hours‐a‐day patch use (one study): one trial (Daughton 1991) included a direct comparison between groups wearing the same nicotine patches (dose and delivery system not specified) over either a 16‐hour period (removing the patch at bedtime) or a 24‐hour period (continuous use, including overnight). All participants used patches for a four‐week period after the quit day.
Duration of patch therapy (seven studies): Schnoll 2015 compared 52‐week use of nicotine patches to 24‐week use and eight‐week use. CEASE 1999 compared 28‐week with 12‐week use, and Schnoll 2010a compared 24‐week with eight‐week use. Hilleman 1994 and Bolin 1999 both compared 12‐week patch use to shorter patch use, i.e. six weeks and three weeks respectively. Cummings 2011 compared six‐ to four‐ and two‐week use, and Glavas 2003 compared six‐week and three‐week patch use.
Effect of tapering patch dose (two studies): these studies compared the effect of stopping patch use abruptly at a high dose, to gradually reducing patch dose over a prolonged period of time. Hilleman 1994 did this by providing one group of participants with 21 mg patches for six weeks and providing another group of participants with 21 mg patches for four weeks, then 14 mg patches for four weeks, then 7 mg patches for another four weeks. Stapleton 1995 gave all participants a 15 mg patch for one week, then participants could choose to receive either a continued 15 mg dose or a higher 35 mg dose for a further 11 weeks. Participants were randomized within these self‐selected groups to either taper their patch dose after the 12‐week period or to receive tapered placebo patches. Participants in the active patch group therefore received a further two‐week dose of 15 mg patches, followed by two weeks of 10 mg patches, followed by two weeks of 5 mg patches. The placebo group received the equivalent placebo patches.
Combination versus single form (14 studies): combination NRT describes using nicotine patches as well as a fast‐acting form of NRT, such as gum or lozenge. Kornitzer 1995; Puska 1995; Cooney 2009 and Smith 2013 all studied patch in combination with nicotine gum. Puska 1995 compared combination therapy to gum alone, whereas the other studies compared combination therapy to patch alone. Blondal 1999 and Croghan 2003 combined patch with nasal spray. Blondal 1999 used patch alone as the comparator, whereas Croghan 2003 had a group of participants that received patch alone and a group that received nasal spray alone. Bohadana 2000; Tønnesen 2000 and Caldwell 2016 combined patches with inhaler; Caldwell 2016 compared to patch alone, Bohadana 2000 to inhaler alone, and Tønnesen 2000 compared to both patch alone and inhaler alone. Piper 2009; Smith 2009; Baker 2016 and Krupski 2016 all used patch in combination with lozenge. Baker 2016 and Krupski 2016 compared combination NRT to patch alone, whereas both Piper 2009 and Smith 2009 compared combination NRT to a group receiving patch only and a group receiving lozenge only. Finally, Caldwell 2014 combined patch with oral spray and compared this to patch use alone.
Duration of combination therapy (three studies): these studies investigated the optimum length of combination patch plus gum use. Smith 2013 compared six‐week to two‐week use, Piper 2016 compared 16‐week to eight‐week use, and Schlam 2016 compared 26‐week to eight‐week use.
Fast‐acting NRT versus patch (eight studies): fast‐acting NRT refers to the faster acting (non‐patch) formulations of NRT, such as gum, lozenge, nasal spray, etc. One study compared patch to inhaler (Tønnesen 2000), two studies compared patch to nasal spray (Croghan 2003; Lerman 2004), three studies compared patch to lozenge (Piper 2009; Smith 2009; Schnoll 2010b), and two studies compared patch to gum (Kupecz 1996; Moolchan 2005).
Type of fast‐acting NRT (one study): only Bolliger 2007 compared the effectiveness of different forms of fast‐acting NRT by comparing oral spray to gum to inhaler.
Nicotine gum dose (five studies): these studies compared 4 mg nicotine gum to 2 mg nicotine gum (Kornitzer 1987; Tønnesen 1988; Hughes 1990; Herrera 1995; Garvey 2000)
Duration of gum use (one study): Hall 2009 investigated whether duration of gum use had an effect on quit rates. The intervention group used gum for 50 weeks and the comparison group used gum for 10 weeks.
Fixed versus ad lib dosing schedule (four studies): these studies investigated whether instructions on when to use fast‐acting NRT influenced effectiveness. Goldstein 1989 and Killen 1990 provided participants with 2 mg nicotine gum, and Tønnesen 1996 and Rey 2009 provided participants with nasal spray. The fixed‐dosing groups were either asked to use one piece/puff per hour (Goldstein 1989; Killen 1990; Tønnesen 1996) or two puffs per hour (Rey 2009), regardless of cravings. The ad lib dosing groups were all asked to use their product when a craving occurred, with a maximum upper limit for daily use, i.e. 30 pieces of gum a day or 80 puffs of nasal spray.
NRT preloading versus standard post‐quit NRT use (nine studies): traditionally NRT is used from a quit date onward, after tobacco use has ceased. NRT preloading is when NRT is used before the quit day, whilst the participant is still smoking. Seven studies provided participants with nicotine patches pre‐quit day (Rose 1994; Rose 1998; Schuurmans 2004; Rose 2006; Rose 2009; Dennis 2016; Preloading Investigators 2018), and two studies included participants that used patch alone, gum alone and patch plus gum pre‐quit day (Bullen 2010; Piper 2016). The length of nicotine preloading also varied across studies. Seven studies initiated NRT use two weeks before the quit date (Rose 1994; Rose 1998; Schuurmans 2004; Rose 2006; Rose 2009; Bullen 2010; Dennis 2016), one initiated use three weeks prior to the quit date (Piper 2016), and one initiated use four weeks prior to the quit date (Preloading Investigators 2018). Following the quit date all study arms received active NRT.
Stopping patch use versus continuing patch use on relapsing (one study): Hughes 2018 tested whether the instruction to stop using a nicotine patch in the event of a smoking lapse resulted in different quit rates to the instruction to continue using a patch in the event of a lapse, in participants who were using nicotine patches after a quit day.
Free versus purchased NRT (two studies): these studies investigated whether buying NRT versus being provided with NRT free of charge resulted in different quit rates. Hughes 1991 had three study arms that all used nicotine gum. Participants were randomized to: 1) a free prescription for six months; 2) buying the gum at a cost of USD 6 per box; 3) buying the gum at a cost of USD 20 per box. Hays 1999 also randomized participants to three groups: 1) nicotine patches provided free of charge; 2) placebo patches provided free of charge; 3) nicotine patches bought by participants. The placebo patch group is excluded from this review.
Duration of free NRT (two studies): these studies provided participants with NRT free of charge for a limited period of the study, then encouraged participants to source the remainder of the treatment themselves. The length of free NRT varied between trial arms. Abdullah 2013 provided two weeks free patch or gum (depending on participant preference) in one arm and one week free in the other arm. In both arms participants were encouraged to use NRT for a total of eight to12 weeks, sourcing the remainder themselves. Burns 2016 provided participants with eight weeks of nicotine patches in one arm and four weeks in another arm. Participants were encouraged to use patches for a total of 10 weeks and to source the remainder themselves.
In addition to the comparisons above, Walker 2011 provided participants with a one‐week free NRT selection box (including one patch, gum, inhaler, sublingual tablets and oral pouches), followed by eight weeks of free participant‐selected NRT in the intervention arm. The comparison arm received eight weeks of subsidised NRT patches or gum. Tulloch 2016 provided one group of participants with nicotine patches for 10 weeks, beginning on quit day. Participants were provided with a maximum dose of 21 mg or 14 mg, depending on their baseline cigarettes per day. Dosage was then tapered from weeks seven to 10. Another group of participants self‐titrated their nicotine patch dosage to a maximum of 35 mg, and also used ad libitum nicotine gum or inhaler, for up to 22 weeks.
Excluded studies
We list studies that were potentially relevant but excluded with reasons in the Characteristics of excluded studies table. Reasons that studies were excluded at full‐text stage for this update specifically are also summarized in Figure 1. For this update most studies were excluded at full‐text screening stage because they had an ineligible comparator, for example, placebo rather than another form of NRT. Studies that compared NRT to a control intervention rather than another form or use of NRT, but met all of the other relevant inclusion criteria are included in Hartmann‐Boyce 2018. We also excluded a number of studies due to short follow‐up of the smoking abstinence outcome (i.e. less than six months).
We found one ongoing study comparing 10 weeks of declining, standard‐dose nicotine patch with 10 weeks of titrated nicotine patch, which may be relevant for inclusion when complete (NCT01622998). Further details are summarized in the Characteristics of ongoing studies table.
Risk of bias in included studies
Overall, we judged nine studies to be at low risk of bias (low risk of bias across all domains), 24 at high risk of bias (high risk of bias in at least one domain), and the remaining 30 at unclear risk of bias. A summary illustration of the 'Risk of bias' profile across trials is shown in Figure 2.
2.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
We assessed selection bias through investigating methods of random sequence generation and allocation concealment for each study. We rated 28 studies at low risk for random sequence generation, 34 at unclear risk and one at high risk (Kupecz 1996). We judged Kupecz 1996 to be at high risk as it was described as 'quasi‐experimental', with month of recruitment randomized to study arm (gum or patch), and all people recruited in each month provided with the allotted treatment. We judged 27 studies to be at low risk for allocation concealment and 36 at unclear risk.
When assessing both random sequence generation and allocation concealment, an unclear risk of bias resulted from a lack of sufficient information about methods used in studies, making it impossible to be sure whether bias was present or not.
Blinding
We assessed any risk of bias linked to blinding as one domain. However, we took into account both performance and detection bias when making this judgement. Although we are assessing a pharmaceutical treatment (NRT) in this review, there were some circumstances where the variation in treatment between arms meant it would be impossible to blind participants and study personnel by using a placebo. For example, in Abdullah 2013 the intervention being tested was the length of time NRT was supplied to participants for free (overall length of NRT use was the same). In such cases, we did not rate studies at high risk as long as participants received similar amounts of face‐to‐face contact between groups, or abstinence was biochemically verified, or both. We judged 21 studies to be at low risk of bias for this domain, 22 at unclear risk and 20 at high risk.
Incomplete outcome data
We judged studies to be at a low risk of attrition bias where the numbers of participants lost to follow‐up were clearly reported, the overall number lost to follow‐up was not more than 50%, and the difference in loss to follow‐up between groups was no greater than 20%. This is in accordance with 'Risk of bias' guidance produced by the Cochrane Tobacco Addiction Group for assessing smoking cessation studies. We found that 38 of the studies were at low risk of bias, 20 were at unclear risk and five were at high risk. In four of the five studies (Rose 2009; Caldwell 2014; Dennis 2016; Krupski 2016) at high risk, this was because overall loss to follow‐up was more than 50%. The rating of high risk in Hughes 1999 was because the study was terminated early by the sponsor, resulting in incomplete long‐term follow‐up data; losses were included in the analysis as non‐abstinent.
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7
Summary of findings for the main comparison. Combination compared to single‐form NRT for smoking cessation.
| Combination compared to single‐form NRT for smoking cessation | ||||||
| Patient or population: People who smoke Setting: Any; studies conducted in: Australasia, Europe, USA Intervention: Combination NRT (nicotine patch plus a fast‐acting form of NRT) Comparison: Single‐form NRT | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with single‐form NRT | Risk with combination | |||||
| Smoking cessation | Study population | RR 1.25 (1.15 to 1.36) | 11,356 (14 RCTs) | ⊕⊕⊕⊕ HIGHa | ‐ | |
| 139 per 1000 | 174 per 1000 (160 to 189) | |||||
| Overall SAEs | Study population | RR 4.44 (0.76 to 25.85) | 2888 (5 RCTs) | ⊕⊕⊝⊝ LOWb | ‐ | |
| 1 per 1000 | 3 per 1000 (1 to 18) | |||||
| Treatment withdrawals | Study population | RR 1.12 (0.57 to 2.20) | 3070 (5 RCTs) | ⊕⊝⊝⊝ VERY LOWb,c | ‐ | |
| 12 per 1000 | 14 per 1000 (7 to 27) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; SAEs: serious adverse events | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aWe rated most studies at low or unclear risk of bias. However, we did not downgrade the certainty of the evidence, as limiting the analysis only to studies we judged to be at low risk of bias resulted in a consistent effect estimate and 95% confidence interval. bDowngraded by two levels due to inconsistency: less than 100 events overall and confidence intervals encompass clinically significant harms as well as clinically significant benefits. cModerate unexplained statistical heterogeneity (I2 = 73%).
Summary of findings 2. Longer compared to shorter duration of combination NRT for smoking cessation.
| Longer compared to shorter duration of combination NRT for smoking cessation | ||||||
| Patient or population: People who smoke Setting: Any; studies conducted in: USA Intervention: Longer duration combination NRT (nicotine patch plus a fast‐acting form of NRT) Comparison: Shorter duration combination NRT (nicotine patch plus a fast‐acting form of NRT) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with shorter duration NRT | Risk with longer duration NRT | |||||
| Smoking cessation ‐ 16 weeks versus 8 weeks | Study population | RR 0.96 (0.75 to 1.23) | 637 (1 RCT) | ⊕⊝⊝⊝ VERY LOWa,b | ‐ | |
| 285 per 1000 | 274 per 1000 (214 to 351) | |||||
| Smoking cessation ‐ 6 weeks versus 2 weeks | Study population | RR 1.11 (0.94 to 1.31) | 987 (1 RCT) | ⊕⊕⊝⊝ LOWa,c | ‐ | |
| 351 per 1000 | 390 per 1000 (330 to 460) | |||||
| Overall SAEs ‐ 26 weeks versus 8 weeks | Study population | RR 1.63 (0.60 to 4.42) | 544 (1 RCT) | ⊕⊝⊝⊝ VERY LOWa,d | ‐ | |
| 22 per 1000 | 36 per 1000 (13 to 99) | |||||
| Overall SAEs ‐ 16 weeks versus 8 weeks | Study population | not estimable | 637 (1 RCT) | ⊕⊝⊝⊝ VERY LOWa,d | No events in either arm | |
| not estimable | not estimable | |||||
| Overall SAEs ‐ 6 weeks versus 2 weeks | Study population | not estimable | 987 (1 RCT) | ⊕⊝⊝⊝ VERY LOWa,d | No events in either arm | |
| not estimable | not estimable | |||||
| Treatment withdrawals | Study population | n/a | 0 (0 RCTs) |
n/a | None of our included studies reported usable data on these outcomes | |
| n/a | n/a | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; n/a: not applicable; SAEs: serious adverse events | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aDowngraded by one level due to risk of bias: we judged the one included study to be at high risk of bias. bDowngraded by two levels for imprecision: fewer than 300 events and confidence intervals encompass clinically significant benefit as well as clinically significant harm. cDowngraded by one level due to imprecision: confidence intervals encompass no clinically significant difference between groups as well as clinically significant benefit. dDowngraded by two levels due to imprecision: fewer than 100 events overall.
Summary of findings 3. Higher‐dose compared to lower‐dose nicotine patch for smoking cessation.
| Higher dose compared to lower dose nicotine patch for smoking cessation | ||||||
| Patient or population: People who smoke Setting: Any; studies conducted in: Australasia, Europe, USA Intervention: Higher‐dose nicotine patch Comparison: Lower‐dose nicotine patch | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with lower dose nicotine patch | Risk with higher dose | |||||
| Smoking cessation ‐ 42/44 mg vs 21/22 mg (24‐hour patches) | Study population | RR 1.09 (0.93 to 1.29) | 1655 (5 RCTs) | ⊕⊕⊕⊝ MODERATEa | ‐ | |
| 238 per 1000 | 260 per 1000 (222 to 307) | |||||
| Smoking cessation ‐ 25 mg vs 15 mg (16‐hour patches) | Study population | RR 1.19 (1.00 to 1.41) | 3446 (3 RCTs) | ⊕⊕⊕⊝ MODERATEa,b | ‐ | |
| 123 per 1000 | 146 per 1000 (123 to 173) | |||||
| Smoking cessation ‐ 21 mg vs 14 mg (24‐hour patches) | Study population | RR 1.48 (1.06 to 2.08) | 537 (1 RCT) | ⊕⊕⊕⊝ MODERATEc | ‐ | |
| 167 per 1000 | 248 per 1000 (177 to 348) | |||||
| Overall SAEs ‐ 42/44 mg vs 21/22 mg (24 hr patches) | Study population | RR 5.01 (0.87 to 28.82) | 1023 (2 RCTs) | ⊕⊕⊝⊝ LOWd,e | ‐ | |
| 2 per 1000 | 10 per 1000 (2 to 56) | |||||
| Overall SAEs ‐ 21 mg vs 14 mg (24‐hour patches) | Study population | not estimable | 537 (1 RCT) | ⊕⊕⊝⊝ LOWf | No events in either arm | |
| not estimable | not estimable | |||||
| Treatment withdrawals ‐ 42/44 mg vs 21/22 mg (24‐hour patches) | Study population | RR 4.99 (1.60 to 15.50) | 554 (2 RCTs) | ⊕⊕⊝⊝ LOWe,f | ‐ | |
| 11 per 1000 | 54 per 1000 (17 to 168) | |||||
| Treatment withdrawals ‐ 21 mg vs 14 mg (24‐hour patches) | Study population | RR 0.77 (0.36 to 1.64) | 537 (1 RCT) | ⊕⊕⊝⊝ LOWd | ‐ | |
| 55 per 1000 | 42 per 1000 (20 to 89) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; SAEs: serious adverse events | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aDowngraded by one level due to imprecision: confidence intervals encompass no difference as well as a clinically significant difference. bWe rated most studies at low or unclear risk of bias. We did not downgrade the certainty of the evidence, as limiting the analysis only to studies we judged to be at low risk of bias resulted in a consistent effect estimate and 95% confidence interval. cDowngraded by one level due to imprecision: fewer than 300 events overall. dDowngraded by two levels due to imprecision: fewer than 100 events in total and confidence intervals encompass no difference as well as a clinically significant difference. eOne of the two studies was at high risk of bias, but judged unlikely to affect this outcome. fDowngraded by two levels due to imprecision: fewer than 100 events in total.
Summary of findings 4. Longer compared to shorter duration of nicotine patch therapy for smoking cessation.
| Longer compared to shorter duration of nicotine patch therapy for smoking cessation | ||||||
| Patient or population: People who smoke Setting: Any; studies conducted in: Europe, USA Intervention: Longer duration of nicotine patch therapy Comparison: Shorter duration of nicotine patch therapy | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with shorter duration patch | Risk with longer duration patch | |||||
| Smoking cessation | Study population | n/a | 7078 (7 RCTs) |
⊕⊕⊝⊝ LOWa,b,c | We did not pool studies, due to substantial clinical heterogeneity in length of intervention and control patch duration, and two studies appeared in multiple comparisons. None of the individual comparisons detected a statistically or clinically significant difference between longer and shorter durations of patch therapy | |
| n/a | n/a | |||||
| Overall SAEs | Study population | n/a | 1173 (3 RCTs) | ⊕⊝⊝⊝ VERY LOWb,d | We did not pool studies, due to substantial clinical heterogeneity in length of intervention and control patch duration, and one study appeared in multiple comparisons. We found no significant differences in any study | |
| n/a | n/a | |||||
| Treatment withdrawals | n/a | n/a | 648 (2 RCTs) | ⊕⊝⊝⊝ VERY LOWb,d | We did not pool studies, due to substantial clinical heterogeneity in length of intervention and control patch duration. We found no significant differences in any study | |
| n/a | n/a | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). n/a: not applicable; SAEs: serious adverse events | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aDowngrade by one level due to imprecision: all individual comparisons had fewer than 300 events overall. bDowngrade by one level due to inconsistency: clinical heterogeneity between treatment durations in individual studies prevented pooling. cMost studies were at a high risk of bias for blinding but as studies did not detect significant effects we think blinding was unlikely to have contributed to the outcome. dDowngraded by two levels due to imprecision: fewer than 100 events overall.
Summary of findings 5. Fast‐acting NRT compared to nicotine patch for smoking cessation.
| Fast‐acting NRT compared to nicotine patch for smoking cessation | ||||||
| Patient or population: People who smoke Setting: Any; studies conducted in: Europe, USA Intervention: Fast‐acting NRT Comparison: Nicotine patch | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with nicotine patch | Risk with fast‐acting NRT | |||||
| Smoking cessation | Study population | RR 0.90 (0.77 to 1.05) | 3319 (8 RCTs) | ⊕⊕⊕⊕ HIGHa | ‐ | |
| 164 per 1000 | 148 per 1000 (126 to 172) | |||||
| Overall SAEs | Study population | ‐ | 1252 (4 RCTs) | ⊕⊝⊝⊝ VERY LOWb,c | Three of the four studies had no events in either arm. In the one study in which SAEs were reported (n = 642) the confidence interval was wide (RR 1.75, 95% CI 0.52 to 5.92) | |
| see comment | see comment | |||||
| Treatment withdrawals | Study population | RR 4.23 (1.54 to 11.63) | 1482 (3 RCTs) | ⊕⊝⊝⊝ VERY LOWb,d | ‐ | |
| 5 per 1000 | 23 per 1000 (8 to 63) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; SAEs: serious adverse events | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aWe rated most studies at low or unclear risk of bias. However, we did not downgrade the certainty of the evidence, as limiting the analysis only to studies we judged to be at low risk of bias resulted in a consistent effect estimate and 95% confidence interval. ˜bDowngraded by two levels due to imprecision: fewer than 100 events overall. cDowngraded by one level due to risk of bias: two of the four studies were at high risk of bias. dDowngraded by one level due to risk of bias: two of the three studies were at high risk of bias.
Summary of findings 6. Comparing types of fast‐acting NRT for smoking cessation.
| Comparing types of fast‐acting NRT for smoking cessation | ||||||
| Patient or population: People who smoke Setting: Any; study conducted in: South Africa Intervention: Fast‐acting NRT (e.g. gum, lozenge, nasal spray) Comparison: Fast‐acting NRT (e.g. gum, lozenge, nasal spray) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with fast‐acting NRT 1 | Risk with fast‐acting NRT 2 | |||||
| Smoking cessation ‐ Oral spray versus gum | Study population | RR 0.80 (0.29 to 2.19) | 75 (1 RCT) | ⊕⊝⊝⊝ VERY LOWa,b | ‐ | |
| 200 per 1000 | 160 per 1000 (58 to 438) | |||||
| Smoking cessation ‐ Oral spray versus inhaler | Study population | RR 2.00 (0.46 to 8.73) | 75 (1 RCT) | ⊕⊝⊝⊝ VERY LOWa,b | ‐ | |
| 80 per 1000 | 160 per 1000 (37 to 698) | |||||
| Smoking cessation ‐ Gum versus inhaler | Study population | RR 2.50 (0.53 to 11.70) | 50 (1 RCT) | ⊕⊝⊝⊝ VERY LOWa,b | ‐ | |
| 80 per 1000 | 200 per 1000 (42 to 936) | |||||
| Overall SAEs | Study population | n/a | 0 (0 RCTs) |
n/a | None of our included studies reported usable data on these outcomes | |
| n/a | n/a | |||||
| Treatment withdrawals | Study population | n/a | 0 (0 RCTs) |
n/a | None of our included studies reported usable data on these outcomes | |
| n/a | n/a | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; n/a: not applicable; SAEs: serious adverse events | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aDowngraded by one level due to risk of bias: we judged the one included study to be at high risk of bias. bDowngraded by two levels due to imprecision: fewer than 100 events overall.
Summary of findings 7. Preloading NRT compared to standard‐use NRT for smoking cessation.
| Preloading NRT compared to standard‐use NRT for smoking cessation | ||||||
| Patient or population: People who smoke Setting: Any; studies conducted in: Australasia, Europe, South Africa, USA Intervention: Preloading NRT Comparison: Standard‐use NRT | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with standard use NRT | Risk with preloading NRT | |||||
| Smoking cessation | Study population | RR 1.25 (1.08 to 1.44) | 4395 (9 RCTs) | ⊕⊕⊕⊝ MODERATEa | ‐ | |
| 136 per 1000 | 170 per 1000 (147 to 196) | |||||
| Overall SAEs | Study population | RR 1.11 (0.59 to 2.09) | 3908 (4 RCTs) | ⊕⊕⊝⊝ LOWb,c | ‐ | |
| 10 per 1000 | 11 per 1000 (6 to 21) | |||||
| Treatment withdrawals | Study population | RR 0.33 (0.01 to 7.95) | 80 (1 RCT) | ⊕⊝⊝⊝ VERY LOWd,e | ‐ | |
| 25 per 1000 | 8 per 1000 (0 to 199) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; SAEs: serious adverse events | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
aDowngraded by one level due to a combination of risk of bias and imprecision: we judged five of nine studies to be at high risk of bias; removing these studies from the analysis resulted in a wider confidence interval, rendering the result no longer statistically significant (the point estimate was lower but still favoured the intervention (RR 1.16)). We rated the one included study which detected a statistically significant benefit in favour of the intervention to be at high risk of bias. bDowngraded by one level due to risk of bias: we judged three of four studies to be at high risk of bias. cDowngraded by one level due to imprecision: fewer than 300 events overall. dDowngraded by one level due to risk of bias: we judged the one study to be at high risk of bias. eDowngraded by two levels due to imprecision: fewer than 100 events overall.
Patch therapy
Dose
We treated three groups of studies that compared different patch doses as separate groups for our first comparison: Patch dose; 1) 42/44 mg versus 21/22 mg patches; 2) 25 mg versus 15 mg patches; 3) 21 mg versus 14 mg patches. Although the doses included in groups 2) and 3) appear comparable, the patches used in these groups did not have comparable delivery systems, meaning the doses delivered to participants per hour were likely to be different across the two groups. The three studies comparing the 25 mg dose to the 15 mg dose (Paoletti 1996; CEASE 1999; Killen 1999) all used patches that delivered nicotine over a 16‐hourr period (to be worn during waking hours), so the doses delivered per hour were approximately 1.6 mg and 0.9 mg. However, in TNSG 1991, which compared a 21 mg dose with a 14 mg dose, the patches used delivered nicotine over 24 hours (to be worn continuously, including overnight), resulting in doses of approximately 0.9 mg and 0.6 mg per hour. The five studies comparing 42/44 mg doses with 21/22 mg doses (Dale 1995; Hughes 1999; Jorenby 1995; Kalman 2006; Rose 2010) all used patches that delivered nicotine over 24 hours, so that the approximate doses delivered per hour were 1.8 mg and 0.9 mg respectively.
When we compared 21 mg to 14 mg (24‐hour) patches, we found a statistically significant effect on smoking cessation in favour of the higher dose (risk ratio (RR) 1.48, 95% confidence interval (CI) 1.06 to 2.08, 1 study, 537 participants; Analysis 1.1). When we compared 25 mg to 15 mg (16‐hour) patches, the point estimate was in favour of the higher dose; however, the lower limit of the confidence interval was one (RR 1.19, 95% CI 1.00 to 1.41, 3 studies, 3446 participants; I2 = 0%). Finally, when we compared 42 or 44 mg to 21 or 22 mg (24‐hour) patches, the point estimate was lower, and the effect was not statistically significant (RR 1.09, 95% CI 0.93 to 1.29, 5 studies, 1655 participants; I2 = 38%). Results were not sensitive to the exclusion of one study at a high risk of bias.
1.1. Analysis.

Comparison 1 Patch dose, Outcome 1 Smoking cessation.
When we compared high‐ (25 mg) and low‐dose (15 mg) 16‐hour patches, there was no evidence of a statistically significant difference in fast or irregular heartbeat (RR 0.92, 95% CI 0.64 to 1.33, 2 studies, 3269 participants; I2 = 0%; Analysis 1.2) or myocardial infarctions (RR 0.50, 95% CI 0.05 to 5.51, 1 study, 2861 participants; Analysis 1.3). However, only two of nine studies reported cardiac AEs by trial arm (CEASE 1999; Killen 1999). Hughes 1999 reported that 8% of the 42 mg (24‐hour) patch group experienced cardiac side effects but did not report data for the other treatment arms, so could not be included in the meta‐analysis.
1.2. Analysis.

Comparison 1 Patch dose, Outcome 2 Fast or irregular heartbeat.
1.3. Analysis.
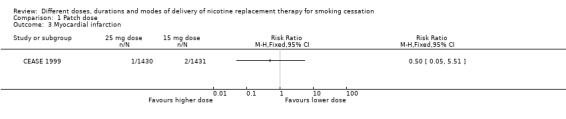
Comparison 1 Patch dose, Outcome 3 Myocardial infarction.
Only three studies comparing patch doses reported overall SAEs (TNSG 1991; Jorenby 1995; Hughes 1999). When we entered these into a meta‐analysis, there was no evidence of a statistically significant difference (RR 5.01, 95% CI 0.87 to 28.82, 3 studies, 1560 participants; I2 = 0%; Analysis 1.4).
1.4. Analysis.

Comparison 1 Patch dose, Outcome 4 Overall SAEs.
When we compared 42/44 mg versus 21/22 mg (24‐hour) patches, we found a statistically significant difference in study withdrawals due to treatment, with more withdrawals occurring in participants receiving higher‐dose patches (RR 4.99, 95% CI 1.60 to 15.50, 2 studies, 544 participants; I2 = 0%; Analysis 1.5). However, there was no evidence of a difference when we compared 21 mg to 14 mg (24‐hour) patches (RR 0.77, 95% CI 0.36 to 1.64, 1 study, 537 participants; Analysis 1.5). Two studies reported treatment withdrawals overall rather than by trial arm, with 2% (CEASE 1999) and 3% (Rose 2010) of participants withdrawing overall.
1.5. Analysis.

Comparison 1 Patch dose, Outcome 5 Treatment withdrawals.
Duration
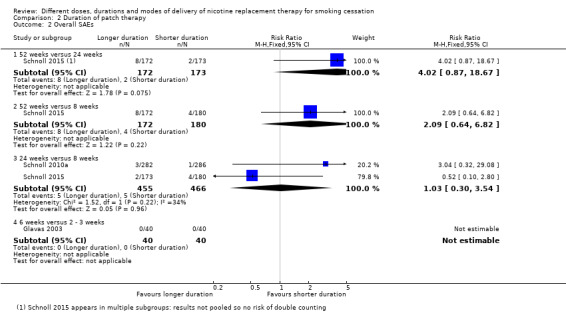
None of the comparisons based on duration of patch therapy showed a clinically or statistically significant difference for our abstinence outcome (Analysis 2.1), SAEs (Analysis 2.2) or treatment withdrawals (Analysis 2.3). Studies were so clinically heterogenous that we did not pool across subgroups. For individual subgroups the number of included studies was small and confidence intervals were generally wide, meaning we cannot rule out a clinically significant difference or conduct sensitivity analyses.
2.1. Analysis.

Comparison 2 Duration of patch therapy, Outcome 1 Smoking cessation.
2.2. Analysis.
Comparison 2 Duration of patch therapy, Outcome 2 Overall SAEs.
2.3. Analysis.

Comparison 2 Duration of patch therapy, Outcome 3 Treatment withdrawals.
Four studies comparing different durations of patch therapy reported cardiac AEs (CEASE 1999; Glavas 2003; Schnoll 2010a; Schnoll 2015). However, meta‐analysis was not possible due to a lack of reporting of events by duration of treatment (CEASE 1999), measuring AEs for different lengths of time by treatment arm (Glavas 2003), and not reporting AEs cumulatively across time points (Schnoll 2010a; Schnoll 2015). However, Glavas 2003 reported no cardiac AEs in either the three‐ or six‐week NRT groups during the time participants were on treatment. Cardiac AEs were also rare and similar between trial arms in Schnoll 2010a and Schnoll 2015 (Appendix 2).
Effect of tapering
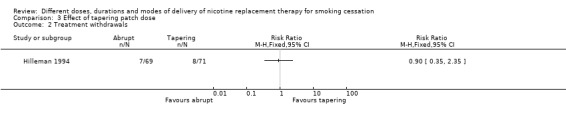
Neither of the two studies that compared the tapering of patch dose before end of treatment to abrupt withdrawal indicated any difference in effect on abstinence between the two approaches (RR 0.99, 95% CI 0.74 to 1.32, 2 studies, 264 participants; I2 = 0%; Analysis 3.1). Results were not sensitive to removing the one study at a high risk of bias. Neither of the studies reported cardiac or SAEs. Hilleman 1994 found no evidence of a difference between tapering and abrupt withdrawal on withdrawals due to treatment (RR 0.90, 95% CI 0.35 to 2.35, 1 study, 140 participants; Analysis 3.2). Stapleton 1995 reported 2% treatment withdrawals, but did not report these by trial arm and so could not be included in the meta‐analysis.
3.1. Analysis.

Comparison 3 Effect of tapering patch dose, Outcome 1 Smoking cessation.
3.2. Analysis.
Comparison 3 Effect of tapering patch dose, Outcome 2 Treatment withdrawals.
Other variations in patch use
There were two studies that tested the effects of variations in patch use that do not fall under the headings above and were not entered into a meta‐analysis.
Daughton 1991 looked at the effect of using the same nicotine patches (nicotine dose and delivery system not specified) for 24 hours a day versus 16 hours a day (in the former group participants wore patches overnight, and in the latter during waking hours only). There was no significant effect of hours of use per day on abstinence (RR 0.70, 95% CI 0.36 to 1.34, 106 participants), with 11/51 and 17/55 participants quitting in the 24‐hour and 16‐hour groups respectively (Analysis 13.1). Whilst Daughton 1991 reported common AEs, it did not report on cardiac AEs or SAEs. Overall, 1.3% of participants withdrew due to treatment, but withdrawals by treatment arm were not reported (Appendix 2).
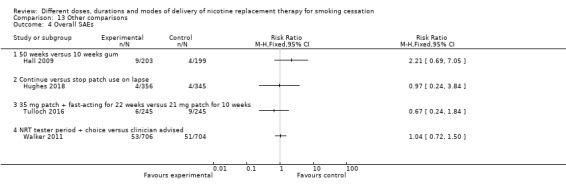
Hughes 2018 found no effect of instructing participants to continue using a patch in the event of a lapse versus instructing participants to stop using a nicotine patch in the event of a smoking lapse; 174/356 quit in the continuing group and 190/345 in the stopping group (RR 0.89, 95% CI 0.77 to 1.02, 701 participants; Analysis 13.1). Hughes 2018 found no effect of differential NRT use on SAEs (RR 0.97, 95% CI 0.24 to 3.84, 1 study, 701 participants; Analysis 13.4).
13.1. Analysis.

Comparison 13 Other comparisons, Outcome 1 Smoking cessation.
13.4. Analysis.
Comparison 13 Other comparisons, Outcome 4 Overall SAEs.
Combination therapy
Combination versus single form
Overall evidence favoured combination NRT over single‐type NRT for smoking cessation (RR 1.25, 95% CI 1.15 to 1.36, 14 studies, 11,356 participants; I2 = 4%; Analysis 4.1). When split into subgroups, this was equally true for combination therapy compared to patch alone (RR 1.23, 95% CI 1.12 to 1.36, 12 studies, 8992 participants; I2 = 32%), or to a fast‐acting form of NRT alone (RR 1.30, 95% CI 1.09 to 1.54, 6 studies, 2364 participants; I2 = 0%). There was no evidence of significant subgroup differences (I2 = 0%). Results were not sensitive to the removal of studies at a high risk of bias.
4.1. Analysis.
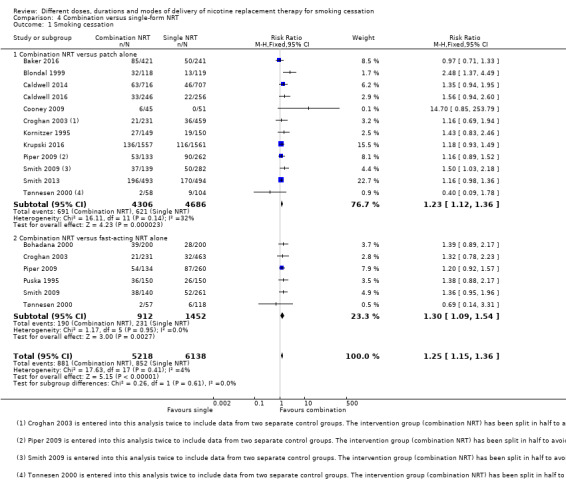
Comparison 4 Combination versus single‐form NRT, Outcome 1 Smoking cessation.
As this meta‐analysis included over 10 studies, we generated a funnel plot to investigate the likelihood of publication bias (Figure 3). The plot does not provide evidence of publication bias, but as the number of studies included is low (14 studies) this should be interpreted with caution.
3.

Funnel plot of comparison: 4 Combination versus single form NRT, outcome: 4.1 Smoking cessation.
Whilst 11 of the 14 studies comparing combination NRT to single‐type NRT reported some AE data, only two studies reported cardiac AEs (Cooney 2009; Caldwell 2016). Cooney 2009 found no significant difference between combination and single‐form NRT (RR 1.13, 95% CI 0.30 to 4.27, 1 study, 96 participants; Analysis 4.2); however, this was a single small study. Caldwell 2016 reported chest discomfort and palpitations at multiple time points but did not report these cardiac AEs cumulatively across time points and so could not be included in the meta‐analysis. However, cardiac AEs were generally similar between groups at each time point (Appendix 2).
4.2. Analysis.

Comparison 4 Combination versus single‐form NRT, Outcome 2 Any cardiac AE.
SAEs were generally rare, with seven such events across the five studies that reported SAEs by treatment arm. There was no evidence of a statistically significant difference in SAEs between combination NRT and single‐form NRT (RR 4.44, 95% CI 0.76 to 25.85, 5 studies, 2888 participants; I2 = 35%; Analysis 4.3). Although the effect size was large and in favour of single‐form NRT, the confidence intervals were wide and we cannot be certain of the direction of the effect. Subgroup analysis by type of single NRT also showed no significant difference for combination NRT versus patch (RR 11.45, 95% CI 0.64 to 205.90, 4 studies, 2313 participants; Analysis 4.3) or for combination NRT versus fast‐acting NRT (RR 1.00, 95% CI 0.06 to 15.88, 2 studies, 575 participants; Analysis 4.3). Piper 2009 (1504 participants) reported 32 SAEs not considered related to treatment over six months, but did not report these by trial arm and so could not be included in the meta‐analysis.
4.3. Analysis.

Comparison 4 Combination versus single‐form NRT, Outcome 3 Overall SAEs.
Five studies reported withdrawals due to treatment effects by trial arm. Comparing treatment withdrawals for combination NRT versus single‐form NRT, there was no evidence of a difference (RR 1.12, 95% CI 0.57 to 2.20, 5 studies, 3070 participants; Analysis 4.4). However, there was significant heterogeneity (I2 = 73%). When we divided studies into subgroups, and compared combination NRT with NRT patch, there remained no evidence of a difference (RR 2.32, 95% CI 0.99 to 5.40, 5 studies, 1982; I2 = 61%; Analysis 4.4). The same was observed when we compared combination NRT with fast‐acting forms of NRT (RR 0.14, 95% CI 0.02 to 1.08, 2 studies, 1088 participants; I2 = not estimable, as one of the studies had no events; Analysis 4.4).
4.4. Analysis.

Comparison 4 Combination versus single‐form NRT, Outcome 4 Treatment withdrawals.
Duration of combination therapy
Two of the studies testing duration of combination NRT found no difference in effect on abstinence between shorter and longer duration (Analysis 5.1), but er did not combined them in a meta‐analysis as they compared different durations of use. Piper 2016 compared 16‐week to eight‐week combination NRT use, with an RR of 0.96 (95% CI 0.75 to 1.23, 637 participants); and Smith 2013 compared six‐week to two‐week combination NRT use, with an RR of 1.11 (95% CI 0.94 to 1.31, 987 participants). Smith 2013 was a factorial trial and did not report results on duration for combination NRT only; we therefore combined study arms receiving combination and gum alone, as the authors reported there was no interaction between the two groups.
5.1. Analysis.
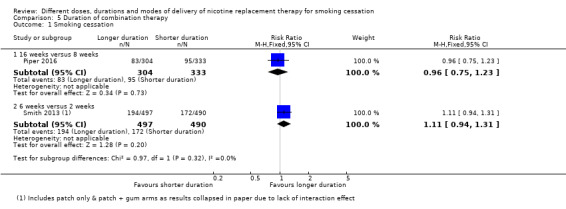
Comparison 5 Duration of combination therapy, Outcome 1 Smoking cessation.
We did not include Schlam 2016 in this analysis. The study had a factorial design and statistical interactions between factors were reported in the paper. We contacted study authors who supplied group‐by‐group quit rates. We checked to see if the odds ratio (OR) generated from this data resulted in a clinically different interpretation of the OR generated for the regression model adjusting for interactions in the paper, for the relevant comparison of 26‐ versus eight‐week use of combination NRT. The ORs were similar, but the wider confidence intervals generated from the basic quit‐rate data changed the interpretation of the results. The analysis accounting for interactions in the paper resulted in a significant effect of 26‐week gum (OR 1.40, 95% CI 1.08 to 1.82); however, this effect became non‐significant when we used the basic quit‐rate data supplied by the authors (OR 1.42, 95% CI 0.98 to 2.05, 544 participants). This suggests it would be inappropriate to use the basic quit rates to calculate RRs and 95% CIs for the duration of combination therapy comparison, ignoring the interactions detected with other intervention factors.
All three studies testing duration of combination NRT reported SAEs by trial arm (Analysis 5.2). There were no SAEs in either Piper 2016 or Smith 2013.Schlam 2016 reports no SAEs in the published paper but reports the occurrence of SAEs on ClinicalTrials.gov. The numbers given in the trial registry data do not suggest a statistically significant difference between those receiving 26 weeks of NRT compared with those receiving eight weeks (RR 1.63, 95% CI 0.60 to 4.42, 1 study, 544 participants; Analysis 5.2).
5.2. Analysis.

Comparison 5 Duration of combination therapy, Outcome 2 Overall SAEs.
None of the studies reported treatment withdrawals by trial arm.
Fast‐acting NRT versus patch
None of the studies that compared a form of fast‐acting NRT to nicotine patch found an effect on smoking cessation, whether subgrouped according to type of fast‐acting NRT or combined (RR 0.90, 95% CI 0.77 to 1.05, 8 studies, 3319 participants; I2 = 0%). There was no significant difference in effects between subgroups (effects for individual subgroups can be found in Analysis 6.1). The overall effect was not sensitive to the removal of studies judged to be at a high risk of bias.
6.1. Analysis.
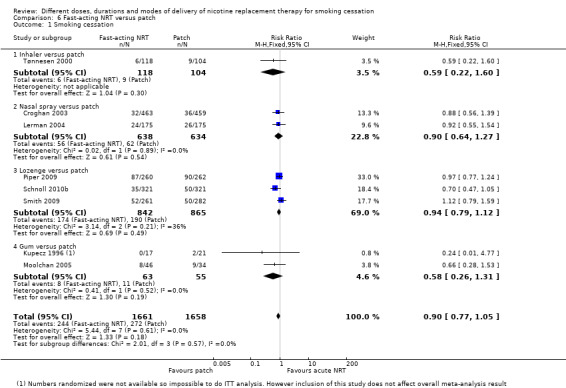
Comparison 6 Fast‐acting NRT versus patch, Outcome 1 Smoking cessation.
Only one small study reported cardiac AEs by trial arm (Kupecz 1996). In this study, there were no events in either the gum or patch groups.
Three of the four studies which reported SAEs by trial arm had no SAEs (Kupecz 1996; Tønnesen 2000; Lerman 2004). Schnoll 2010b found no evidence of a difference in SAEs between lozenge and patch (RR 1.75, 95% CI 0.52 to 5.92, 1 study, 642 participants; Analysis 6.3). Piper 2009 reported 36 SAEs over six months, but did not report these by trial arm and so could not be included in a meta‐analysis.
6.3. Analysis.

Comparison 6 Fast‐acting NRT versus patch, Outcome 3 Overall SAEs.
When comparing withdrawals due to treatment between fast‐acting NRT and NRT patches, more participants withdrew in the fast‐acting NRT groups (RR 4.23, 95% CI 1.54 to 11.63, 3 studies, 1482 participants; I2 = 0%; Analysis 6.4). We also conducted subgroup analysis by type of fast‐acting NRT. When we compared nasal spray and patch, nasal spray was associated with significantly more withdrawals (RR 3.47, 95% CI 1.15 to 10.46, 1 study, 922 participants; Analysis 6.4). There was no evidence of a significant difference in withdrawals between gum and patches (RR 11.00, 95% CI 0.63 to 191.04, 1 study, 38 participants; Analysis 6.4). There were no treatment withdrawals in either group in the study comparing lozenge with patch.
6.4. Analysis.
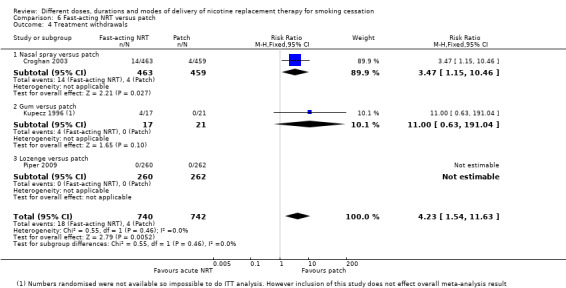
Comparison 6 Fast‐acting NRT versus patch, Outcome 4 Treatment withdrawals.
Fast‐acting NRT
Type
One small study of 100 participants (Bolliger 2007) compared smoking cessation rates across three types of fast‐acting NRT (oral spray, gum and inhaler). Confidence intervals were wide and not statistically significant for all comparisons (Analysis 7.1). Whilst this study reported some adverse event data, it did not report on cardiac AEs, SAEs or treatment withdrawals.
7.1. Analysis.

Comparison 7 Type of fast‐acting NRT, Outcome 1 Smoking cessation.
Gum dose
Five studies compared 4 mg to 2 mg gum use. Overall there was a statistically significantly greater effect of 4 mg gum use on long‐term abstinence (RR 1.43, 95% CI 1.12 to 1.83, 5 studies, 856 participants; I2 = 63%; Analysis 8.1), but with moderate statistical heterogeneity between studies. In this group of studies, authors conducted subgroup analyses to test whether effects differed between low‐ and high‐dependency smokers (this was not consistently done in other groups of studies). Our post hoc subgroup analysis found that when we split studies/participants into lower‐dependency smokers (Kornitzer 1987; Hughes 1990; Garvey 2000) and higher‐dependency smokers (Kornitzer 1987; Tønnesen 1988; Herrera 1995; Garvey 2000), with Garvey 2000 and Kornitzer 1987 split across the two subgroups, this heterogeneity reduced substantially. We found a statistically significant benefit of the 4 mg dose (RR 1.85, 95% CI 1.36 to 2.50, 4 studies, 618 participants; I2 = 13%) in high‐dependency smokers, with no evidence of an effect in low‐dependency smokers (RR 0.77, 95% CI 0.49 to 1.21, 3 studies, 238 participants; I2 = 0%). This resulted in a significant difference between subgroups (I2 = 90%). We rated none of the studies included in this analysis at high risk of bias, so a sensitivity analysis was unnecessary.
8.1. Analysis.

Comparison 8 4 mg versus 2 mg gum, Outcome 1 Smoking cessation.
One small study reported palpitations by trial arm (Tønnesen 1988). This study did not find a statistically significant difference in palpitations between 4 mg and 2 mg gum doses (RR 3.64, 95% CI 0.15 to 85.97, 1 study, 60 participants; Analysis 8.2). No studies comparing gum dose reported on SAEs. However, two studies reported withdrawals due to treatment by trial arm (Tønnesen 1988; Garvey 2000). There was no evidence of an effect of gum dose on treatment withdrawals (RR 1.08, 95% CI 0.18 to 6.36, 2 studies, 465 participants; I2 = 0%; Analysis 8.3).
8.2. Analysis.
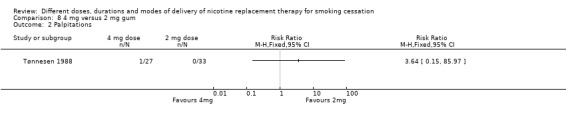
Comparison 8 4 mg versus 2 mg gum, Outcome 2 Palpitations.
8.3. Analysis.

Comparison 8 4 mg versus 2 mg gum, Outcome 3 Treatment withdrawals.
Gum duration
Hall 2009 found no significant effect of 50‐week gum use over 10‐week gum use on smoking abstinence. Eighty‐five of 203 quit in the 50‐week duration group and 80 of 199 in the 10‐week duration group (RR 1.04, 95% CI 0.82 to 1.32, 402 participants; Analysis 13.1). The study also found no evidence of a significant effect on SAEs (RR 2.21, 95% CI 0.69 to 7.05, 1 study, 402 participants; Analysis 13.4), or the sensation of midsternal pressure (RR 2.94, 95% CI 0.12 to 71.77, 1 study, 402 participants; Analysis 13.2). It did not report on other cardiac AEs or treatment withdrawals.
13.2. Analysis.

Comparison 13 Other comparisons, Outcome 2 Midsternal pressure.
Fixed versus ad lib dosing schedule
There was no statistically significant effect of fixed versus ad lib dosing of fast‐acting NRT on abstinence (RR 1.12, 95% CI 0.87 to 1.45, 4 studies, 828 participants; I2 = 8%; Analysis 9.1). Two of the studies tested dosing schedule using gum and two using nasal spray; however, neither group demonstrated an effect and subgroup differences were not significant. Removal of one study judged to be at high risk of bias did not affect the interpretation of subgroup or overall effect estimates.
9.1. Analysis.

Comparison 9 Fixed versus ad lib dose schedule, Outcome 1 Smoking cessation.
Only one small study reported cardiac AEs and SAEs (Tønnesen 1996). However, the cardiac AEs were not reported cumulatively, or by treatment arm at all time points (Appendix 2). There were no SAEs in the study.
Three studies reported withdrawals due to treatment. In Tønnesen 1996, there were no withdrawals in either the fixed‐dose or the ad lib nasal spray groups. Killen 1990 found no evidence of a difference between fixed‐dose and ad lib gum (RR 0.89, 95% CI 0.49 to 1.59, 1 study, 299 participants; Analysis 9.3).Rey 2009 reported 4% treatment withdrawals across the study, but did not report these by trial arm.
9.3. Analysis.
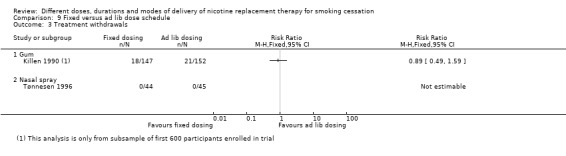
Comparison 9 Fixed versus ad lib dose schedule, Outcome 3 Treatment withdrawals.
NRT preloading versus standard post‐quit use
Overall, evidence from nine studies comparing NRT use with no NRT use before a quit day, whilst concurrently smoking, found a positive statistically significant effect of NRT preloading on abstinence (RR 1.25, 95% CI 1.08 to 1.44, 9 studies, 4395 participants; I2 = 0%; Analysis 10.1).
10.1. Analysis.
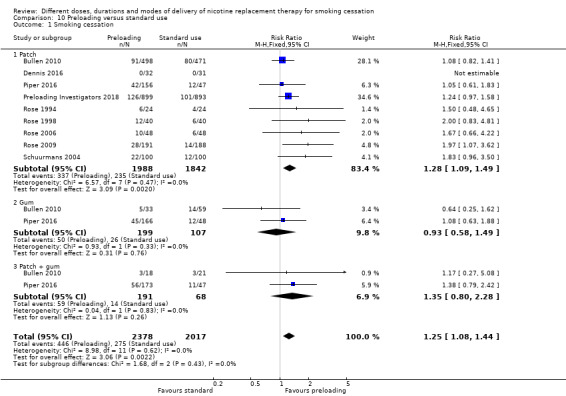
Comparison 10 Preloading versus standard use, Outcome 1 Smoking cessation.
Participants in the included studies were split into three subgroups. Those that used patch only for preloading, those that used patch plus gum and those that used gum only (Bullen 2010 and Piper 2016 were included in all three groups, as they each had distinct groups of participants who used patch alone, gum alone, or both). The significant effect of preloading was only found in those participants where patch only was used (RR 1.28, 95% CI 1.09 to 1.49, 9 studies, 3830 participants; I2 = 0%). However, the test for subgroup differences was not significant (I2 = 0%), and the numbers of participants contributing to the gum alone (306 participants) and patch plus gum (259 participants) subgroups were comparatively low, resulting in wider confidence intervals.
When the five studies judged to be at high risk of bias for at least one domain were removed from the overall analysis, the pooled effect was no longer statistically significant but the point estimate still favoured the intervention (RR 1.16, 95% CI 0.93 to 1.46, 4 studies, 1444 participants). Only one study (Rose 2009) detected a statistically significant effect of the intervention; we rated this study at high risk of bias.
One study (Preloading Investigators 2018) reported palpitations, with a statistically significant increase in palpitations found in the preloading arm (RR 2.05, 95% CI 1.15 to 3.62, 1792 participants; Analysis 10.2). One study (Bullen 2010) reported cardiac AEs, with no significant difference detected (RR 1.25, 95% CI 0.50 to 3.15, 1100 participants; Analysis 10.3). Three studies reported cardiac SAEs, and again demonstrated no statistically significant difference (RR 1.94, 95% CI 0.81 to 4.65, 3529 participants; I2 = 0%; Analysis 10.4). Four studies reported overall SAEs, and as with cardiac SAEs, found no statistically significant difference (RR 1.11, 95% CI 0.59 to 2.09, 3908 participants; I2 = 0%; Analysis 10.5). The one study (Rose 1998) reporting treatment withdrawals did not detect a significant difference (RR 0.33, 95% CI 0.01 to 7.95, 80 participants; Analysis 10.6).
10.2. Analysis.
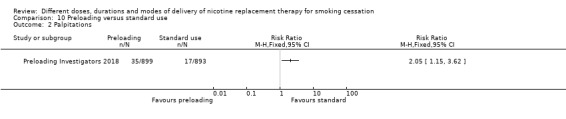
Comparison 10 Preloading versus standard use, Outcome 2 Palpitations.
10.3. Analysis.

Comparison 10 Preloading versus standard use, Outcome 3 Cardiac AEs.
10.4. Analysis.
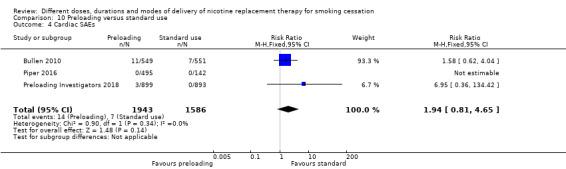
Comparison 10 Preloading versus standard use, Outcome 4 Cardiac SAEs.
10.5. Analysis.

Comparison 10 Preloading versus standard use, Outcome 5 Overall SAEs.
10.6. Analysis.
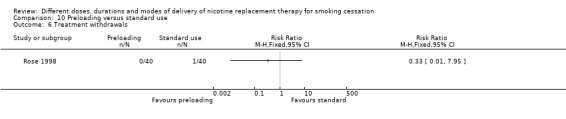
Comparison 10 Preloading versus standard use, Outcome 6 Treatment withdrawals.
Cost of NRT
Free versus purchased
One study (Hays 1999) comparing the effectiveness of free and purchased patches in an over‐the‐counter setting found no significant difference in quit rates between the two conditions (RR 1.24, 95% CI 0.77 to 1.99, 636 participants). Another small study (Hughes 1991) of the cost of nicotine gum for participants receiving brief physician advice also found no significant effect of free gum compared to close to full price gum on abstinence (RR 2.70, 95% CI 0.89 to 8.20, 104 participants), despite the fact that people who could get free gum were much more likely to obtain it. However, due to the low number of participants confidence intervals were wide, meaning we cannot rule out a significant effect. Only Hays 1999 reported cardiac AEs, finding no statistically significant difference between free and purchased patch (RR 0.55, 95% CI 0.18 to 1.61, 1 study, 636 participants; Analysis 11.2). Neither study reported on treatment withdrawals.
11.2. Analysis.

Comparison 11 Free NRT versus purchased NRT, Outcome 2 Cardiac AEs.
Duration of free NRT
Abdullah 2013 compared abstinence rates when participants were provided with two weeks versus one week of free NRT (participants were encouraged to use NRT for eight to 12 weeks in total) and found no statistically significant effect (RR 1.63, 95% CI 0.98 to 2.70, 562 participants). Burns 2016 provided participants with eight weeks versus four weeks of free NRT (participants were encouraged to use NRT for 10 weeks in total), and also found no significant effect on abstinence (RR 0.97, 95% CI 0.64 to 1.48, 1495 participants). Neither study reported AEs.
Participant‐ versus clinician‐selected NRT
Walker 2011 found that providing participants with a one‐week free NRT selection box (including one patch, gum, inhaler, sublingual tablets and oral pouches), followed by eight weeks of free participant‐selected NRT did not result in higher quit rates than providing participants with eight weeks of clinician‐selected NRT patches or gum (RR 1.28, 95% CI 0.90 to 1.83, 1410 participants). However, this RR and 95% CI are based on quit rates validated by saliva sample analysis (63/706 and 49/704 quit in the selection box and control group respectively) and a very low proportion of participants who claimed to be quit completed verification (34%). We therefore conducted a sensitivity analysis using data extrapolated from validated proportions to the wider trial population (161/706 and 136/704 quit in the selection box and control group respectively: RR 1.18, 95% CI 0.96 to 1.45, 1410 participants), and non‐verified, self‐reported quit rates (143/706 and 133/704 quit in the selection box and control group respectively: RR 1.07, 95% CI 0.87 to 1.33, 1410 participants). All three analyses resulted in statistically non‐significant between‐group differences, with no differences in clinical interpretation (Analysis 13.1). Walker 2011 also found no evidence of a difference in SAEs between groups (RR 1.04, 95% CI 0.72 to 1.50, 1 study, 1410 participants; Analysis 13.4).
Other variations in NRT use
Tulloch 2016 was not entered into any meta‐analyses. Although it compared combination patch plus fast‐acting NRT to patch alone, there were other variations in the NRT use that may have confounded the effect. The patches used in the combination arm were self‐titrated to a maximum of 35 mg and used over 22 weeks, whereas the patches in the control arm were a maximum of 21 mg (depending on cigarettes per day), used over 10 weeks with tapering of dose from week seven. The study found no significant effect of the intervention group (29/233 quit) versus the control group (23/230 quit) on abstinence (RR 1.25, 95% CI 0.75 to 2.10, 486 participants; Analysis 13.1). Similarly, the study found no statistically significant difference between the intervention and control groups for cardiac AEs (RR 0.60, 95% CI 0.14 to 2.48, 1 study, 490 participants; Analysis 13.3), for SAEs (RR 0.67, 95% CI 0.24 to 1.84, 1 study, 490 participants; Analysis 13.4) or for withdrawals due to treatment (RR 1.25, 95% CI 0.34 to 4.60, 1 study, 490 participants; Analysis 13.5).
13.3. Analysis.
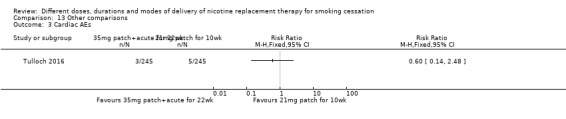
Comparison 13 Other comparisons, Outcome 3 Cardiac AEs.
13.5. Analysis.
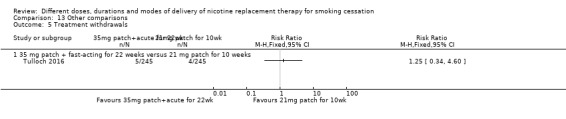
Comparison 13 Other comparisons, Outcome 5 Treatment withdrawals.
Discussion
Summary of main results
This review summarizes and evaluates the evidence investigating the relative efficacy and safety of different types of nicotine replacement therapy (NRT) use for smoking cessation, including variations in duration, dose and modes of delivery. The authors have already published a review of NRT versus controls for smoking cessation (Hartmann‐Boyce 2018), which provides high‐certainty evidence that offering nicotine replacement therapy to dependent smokers, who are prepared to try to quit, increases their chance of success over that achieved with the same level of support but without NRT. This review adds to those findings by investigating how NRT can best be used to maximize the likelihood of smoking cessation at six months or longer.
This review includes 63 studies investigating the effects of NRT dose; duration of treatment; use in combination versus single form; different types of NRT (e.g. patch versus gum, etc.); a fixed versus ad lib dosing schedule; preloading; and the provision of free NRT. All studies reported smoking abstinence at least six months following baseline; however, cardiac AEs, SAEs and withdrawals due to treatment were all measured variably and infrequently.
This review provides high‐certainty evidence that the use of combination NRT results in higher quit rates than single‐form NRT, whether that single form is a patch or a fast‐acting version, such as gum or lozenge. For patch dose comparisons we judged the evidence to be of moderate certainty, due to imprecision. Twenty‐one mg patches resulted in higher quit rates than 14 mg (24‐hour) patches, 25 mg patches resulted in higher quit rates than 15 mg (16‐hour) patches, although the confidence interval included one; there was no clear evidence of superiority for 42/44 mg over 21/22 mg (24‐hour) patches. In addition, results suggest that using 4 mg nicotine gum results in higher quit rates than using 2 mg nicotine gum. A post hoc subgroup analysis accounted for the moderate heterogeneity in the associated analysis and provided an indication that this may only be true in highly‐dependent smokers, and that 4 mg and 2 mg gum may result in similar quit rates when used by less dependent smokers. However, this finding should be treated with caution and tested in primary, adequately‐powered studies to strengthen the evidence in this area. Moderate‐certainty evidence indicates that nicotine preloading, i.e. the use of NRT prior to a quit date, results in higher quit rates than using NRT from quit day onwards; however, when the five studies (of nine) judged to be at high risk of bias were removed from the analysis the statistically significant effect did not remain. It is not possible to say conclusively that this was due to bias, and could be because removing more than half of the studies meant that the sample size reduced by more than half, making the result less precise.
We found no evidence of an effect of duration of nicotine patch use (low‐certainty evidence); 16‐hour versus 24‐hour daily patch use; duration of combination NRT use (low‐ and very low‐certainty evidence); tapering of patch dose versus abrupt patch cessation; fast‐acting NRT type (very low‐certainty evidence); duration of nicotine gum use; ad lib versus fixed dosing of fast‐acting NRT; free versus purchased NRT; length of provision of free NRT; ceasing versus continuous patch use on lapse; and participant‐ versus clinician‐selected NRT. However, this lack of evidence of an effect should not be interpreted as proof that these differing forms of NRT will result in equal quit rates. In many cases these findings are based on very low‐ or low‐certainty evidence, and the findings of single studies. The exception to this is the high‐certainty evidence which suggests that using a form of fast‐acting NRT alone, such as gum or lozenge, results in similar quit rates to using a nicotine patch.
Many studies did not report cardiac AEs separately or did not report AEs and SAEs at all. Where these were reported, there was no evidence of differential cardiac AEs or overall SAEs across comparisons, and the rates of both were low or very low overall, with the exception of one study of nicotine preloading, which found an excess of palpitations in the preloading arm. However, due to variations in reporting, we rate the evidence on which these findings were based as low or very low certainty. The number of withdrawals from trials reported to be due to treatment were also variably reported across studies, and we rated the contributing evidence to be of low and very low certainty. For most comparisons the frequency of these withdrawals was similar between groups; however, significantly more withdrawals due to treatment were reported in participants using nasal spray (3.0%) in comparison to patch (0.9%) in one trial, and in participants using 42/44 mg patches (6.1%) in comparison to 21/22 mg patches (1.1%) across two trials (low‐certainty evidence). In both cases the rates of withdrawal due to treatment were low, so their clinical relevance may be limited when considered alongside other clinical factors, such as initial patient preference and efficacy.
Overall completeness and applicability of evidence
The searches conducted for this study were broad and identified any studies where NRT was used as treatment. This is because the searches were carried out to identify eligible studies for both this review and our review of NRT versus control (no NRT) (Hartmann‐Boyce 2018). As we also screened and extracted data for trials which, based on abstract and title alone, appeared to compare NRT to control, we can be confident in our approach for identifying all studies that compared one form of NRT delivery with another, regardless of how clear this was at the first stage of eligibility screening. We also searched trial registers to identify any ongoing or completed but unpublished, registered studies comparing NRT to another form of NRT.
Although the evidence base investigating the efficacy of NRT versus control (no NRT) is considerable and judged to be stable and of high certainty (Hartmann‐Boyce 2018), the evidence base exploring the optimal methods of use is less developed. Although this review includes 63 studies, there are many comparisons of interest; in many cases the studies and participants contributing to a comparison are sparse, and further research could strengthen or change findings. Although smoking abstinence was reported in all included trials (as this was an inclusion criterion), AEs, SAEs and withdrawals due to treatment were reported rarely and inconsistently across trials, making it difficult to carry out meta‐analyses and draw conclusions.
Studies included in this review recruited smokers who were motivated to quit, who were typically adult, and smoking at least 15 cigarettes a day. Across the studies in this review, the highest mean cigarettes per day was 38. Caution should therefore be exercised when attempting to generalize results outside of these populations.
Certainty of the evidence
Of the 63 studies included in this review, we judged nine to be at low risk of bias for all domains, and 24 to be at high risk in one or more domains. In many cases we had to rate studies at an unclear risk, due to a lack of reporting of key information. In these cases it is impossible to know whether these studies were at any risk of bias or whether the information was simply not reported. To investigate the potential impact of studies that we judged to be at high risk of bias on results, we carried out sensitivity analyses, removing studies judged to be at high risk from analyses and observing the effects on results (where this was possible). In most cases this had no effect on the clinical interpretation of the analyses; however, removing the five studies judged to be at high risk of bias from the analysis of NRT preloading versus NRT use from quit day onward did affect the results. Originally the results showed a positive significant effect of NRT preloading on smoking quit rates, but after the five high‐risk studies were removed the confidence interval widened so that the effect was no longer statistically significant. We judged the only study in this comparison that detected a statistically significant effect of the intervention to be at high risk of bias. However, after removal the point estimate still favoured the intervention; removing the five studies more than halved the number of participants in the analysis, which will have contributed significantly to the imprecision of the results.
We assessed the certainty of the evidence by creating 'Summary of findings' tables and carrying out GRADE ratings for seven of the comparisons (combination versus single‐form NRT (Table 1); duration of combination therapy (Table 2); patch dose (Table 3); duration of patch use (Table 4); fast‐acting NRT versus nicotine patch (Table 5); type of fast‐acting NRT (Table 6); NRT preloading versus standard post‐quit use (Table 7), across all outcomes, where possible. Two of the seven comparisons assessed generated high‐certainty evidence for the efficacy of treatment for smoking cessation: combination versus single‐form NRT, and fast‐acting NRT versus nicotine patch. We judged the NRT preloading versus standard post‐quit use comparison to generate moderate‐certainty evidence; however, we rated the remaining efficacy comparisons to be of low or very low certainty. In all cases where data were available to contribute to any of the safety analyses for these comparisons, we rated the evidence to be of low or very low certainty. This was largely due to the fact that very few studies contributed data to these analyses and where they did the number of events were very low. Our group's policy is to present effect estimates as risk ratios, as these are easier to interpret than odds ratios, but this means that where there are no events measured in both comparison groups risk ratios cannot be calculated and therefore do not contribute to the meta‐analysis. We considered alternative statistical approaches to dealing with this data analysis but concluded that other approaches would be more difficult to interpret and that overall conclusions would not change as a result.
The main reasons for downgrading the evidence were imprecision (low overall numbers of participants and events), risk of bias (judgements of high risk that may affect the result) and heterogeneity (high statistical heterogeneity detected in meta‐analyses).
Potential biases in the review process
We consider the review process used to be robust, and do not believe we have introduced any biases. For outcome assessment, we followed the standard methods used for Cochrane Tobacco Addiction Review Group cessation reviews. Our search strategy included the Cochrane Tobacco Addiction Group Specialized Register and we were able to capture an ongoing study. However, there may be unpublished data that our searches did not uncover. We also considered participants lost to follow‐up as smokers, which is current best practice in this field of work (West 2005). Due to the limited number of studies contributing to each comparison, we were only able to create one funnel plot for the comparison of combination NRT versus single‐form NRT. This provided no evidence of publication bias, although only 14 studies contributed (a relatively small number), so this should be interpreted with caution.
Context for this review
There is high‐certainty evidence to suggest that NRT is a safe and effective treatment for quitting smoking (Hartmann‐Boyce 2018). Evidence for the effect of NRT relative to other pharmacotherapies for smoking cessation can be found in the Cochrane Reviews of nicotine agonists (Cahill 2016) and antidepressants (Hughes 2014) for smoking cessation, as well as the Cochrane overview of pharmacotherapies for smoking cessation, which also provides indirect comparisons (Cahill 2013). This evidence suggests that overall NRT is as effective a quitting aid as the antidepressant bupropion, but is less effective than the nicotine agonist varenicline. However, when different types of NRT are considered, combination NRT is as effective as varenicline. This is in line with the findings of this review, which has found high‐certainty evidence that combination NRT is more effective then single forms of NRT. US clinical practice guidelines (Fiore 2008) and NICE clinical guidelines (NICE 2018) in England are consistent with this finding, although British prescribing guidelines (BNF 2018) do not mention the combination of different forms of NRT. NICE guidance (NICE 2018) does not currently recommend nicotine preloading and explicitly recommends starting NRT on the day before the target quit date; this is not addressed in US guidance (Fiore 2008), and is not explicitly recommended in British prescribing guidance (BNF 2018). US guidelines (Fiore 2008) support the use of higher‐dose preparations of NRT in highly‐dependent smokers, as do British prescribing guidelines (BNF 2018). Less consideration has been given to the other comparisons addressed by this review. Appendix 3 highlights key elements of British prescribing guidance (BNF) as these relate to the comparisons in this review.
Authors' conclusions
Implications for practice.
Combination NRT (fast‐acting form + patch) results in approximately 15% to 36% higher long‐term quit rates than a single form of NRT.
4 mg nicotine gum results in approximately 12% to 83% higher quit rates than 2 mg nicotine gum, although there is some evidence to suggest this may vary based on nicotine dependence.
Forms of fast‐acting NRT, such as gum and lozenge, are as effective a cessation aid as nicotine patches.
There is some evidence that using 21 mg (24‐hour) nicotine patches results in higher quit rates than 14 mg (24‐hour) nicotine patches; however, further evidence could strengthen or weaken this effect.
There is some evidence that using NRT before a quit day could result in higher quit rates than beginning NRT on a quit day; however, due to potential risks of bias in the existing studies, further research could strengthen or weaken this effect.
There is insufficient evidence indicating that any other characteristics of NRT influence the efficacy of NRT for smoking cessation.
There is insufficient evidence to conclude whether different types or methods of NRT delivery result in more frequent cardiac adverse events (AEs), serious adverse events (SAEs) or withdrawals due to treatment. However, where these do occur they are rare, and NRT is generally considered to be well‐tolerated.
These conclusions all apply to smokers who are motivated to quit and who smoke approximately 15 or more cigarettes a day. There is little evidence about the role of NRT for individuals smoking fewer than 15 cigarettes a day.
Implications for research.
More high‐quality studies are needed to assess the efficacy of higher versus lower patch doses, different durations of NRT use, different types of fast‐acting NRT, and NRT preloading versus standard NRT use. In particular, well‐conducted studies examining the use of fast‐acting NRT or combination NRT for preloading would add to the existing evidence base. Studies in people smoking fewer than 15 cigarettes a day or more than 40 cigarettes a day would also add to the existing evidence base.
New studies should ensure that they measure and report on adverse events (AEs) and withdrawals due to treatment, and that these numbers are reported separately by study arm, as well as overall.
Notes
Prof Chris Silagy died in December 2001. In recognition of his major contribution he remained as first author until 2007. The authorship changed from 2008 issue 1.
Acknowledgements
This project was supported by the National Institute for Health Research, via Cochrane Infrastructure funding to the Cochrane Tobacco Addiction Group. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health. JHB is funded in part by the NIHR Oxford Biomedical Research Centre (BRC).
This review has been separated and updated from a previous Cochrane Review titled: 'Nicotine replacement therapy for smoking cessation'. Chris Silagy was the original first author and contributed to updates until his death in 2001, and was listed as an author until 2008. Godfrey Fowler was also an author until 2008. Lindsay Stead was an author from inception and was first author from 2008 to 2012; she heavily shaped this review and the comparisons within it. We also thank the many authors of included studies who have provided clarifications and extra details about their studies over the various updates and for the current version.
Jonathan Livingstone‐Banks assisted in finding studies and with editorial checks and processes for the current update. We also gratefully acknowledge peer review by Dr Katie Myers Smith (Queen Mary University of London) and Dr Sue Cooper (University of Nottingham), consumer review by Phillip Anderson and editorial review by Professor Tim Coleman (University of Nottingham).
Appendices
Appendix 1. Specialized Register search strategy
#1 NRT: TI,AB,KY,XKY,MH,EMT
#2 (nicotine NEAR2 patch*):TI,AB,KY,XKY,MH,EMT
#3 (nicotine NEAR2 gum):TI,AB,KY,XKY,MH,EMT
#4 (nicotine NEAR2 nasal spray):TI,AB,KY,XKY,MH,EMT
#5 (nicotine NEAR2 lozenge*):TI,AB,KY,XKY,MH,EMT
#6 (nicotine NEAR2 tablet*):TI,AB,KY,XKY,MH,EMT
#7 (nicotine NEAR2 sublingual):TI,AB,KY,XKY,MH,EMT
#8 (nicotine NEAR2 inhal*):TI,AB,KY,XKY,MH,EMT
#9 (nicotine NEAR2 replacement):TI,AB,KY,XKY,MH,EMT
#10 (nicotine NEAR3 therap*):TI,AB,KY,XKY,MH,EMT
#11 #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10
The specialised register was transferred from Reference Manager to the Cochrane Register of Studies in May 2012. This is the search used for the CRS: KY, XKY, MH & EMT are keyword fields.
Appendix 2. Withdrawals, cardiac adverse events (AEs) and serious adverse events (SAEs) by study
| Study ID | Withdrawals due to treatment | Cardiovascular adverse events (AEs) | Serious Adverse Events (SAEs) | Notes |
| Abdullah 2013 | Not reported | Not reported | Not reported | No AE data reported |
| Baker 2016 | Not reported | Not reported | 0/421 combination group; 0/241 patch group. | AEs measured for duration of treatment (12 weeks). Only most common AEs reported (i.e. in > 5% of participants). |
| Blondal 1999 | Not reported | Not reported | Not reported | AEs measured during treatment (at 3 months).Not reported in detail by relevant trial arms. |
| Bohadana 2000 | Not reported | Not reported | 1/200 intervention group; 1/200 control group. Both unrelated to treatment. | AEs measured at 1 year. Treatment was for 6 months. Only most common AEs reported. |
| Bolin 1999 | Not reported | Not reported | Not reported | No AEs data reported |
| Bolliger 2007 | Not reported | Not reported | Not reported | AEs measured at each visit to 1 year. Treatment was for 12 weeks. Only most common AEs reported (i.e. in > 5% of participants) |
| Bullen 2010 | Not reported | CARDIAC: 10/549 (1.8%) pre‐cessation group; 8/551 (1.5%) control group. UNSPECIFIED CHEST PAIN: 9/549 pre‐cessation group; 1/551 control group. | Number of participants: 11/549 intervention group; 7/551 control group. Total number of events: 99/549 intervention group; 109/551 control group. | AEs measured at all contacts (6 months). Cardiac AEs numerator is number of people experiencing AEs. |
| Burns 2016 | Not reported | Not reported | Not reported | No AEs data reported |
| Caldwell 2014 | Not reported | Not reported | Not reported | AEs measured at 1 year. Treatment was for 6 months. |
| Caldwell 2016 | 15/246 (6.1%) nicotine patch plus inhaler; 3/256 (1.2%) nicotine patch plus placebo inhaler | CHEST DISCOMFORT: baseline, active 3/246 vs control 1/256. One day quit, active 1/224 vs control 0/234. 1 month quit, active 2/170 vs control 0/179. 3 months quit, active 4/147 vs control 0/143. 6 months quit, active 0/128 vs control 0/119. PALPITATIONS: baseline, active 3/246 vs control 0/256. 1 day quit, active 6/224 vs control 4/234. 1 month quit, active 4/170 vs control 2/179. 3 months quit, active 1/147 vs control 2/143. 6 months quit, active 2/128 vs control 0/119 | 5/246 nicotine patch and inhaler group; 0/256 nicotine patch and placebo group. | AEs measured during treatment (6 months) |
| CEASE 1999 | 72 (2%) overall. Not reported by relevant trial arm. | PALPITATIONS and TACHYCARDIA: 32/1430 (2.3%) 25 mg group; 37/1431 (2.6%) 15 mg group | Do not report all SAEs. Not reported by length of treatment. Myocardial infarction 1/1430 25 mg group; 2/1431 15 mg group. | AEs during treatment (8 weeks). SAE measured during whole study period. Not reported in detail by relevant trial arms. |
| Cooney 2009 | 0% overall. | CARDIAC (related to treatment): 0/45 (0%) nicotine patch and active gum group; 0/51 (0%) nicotine patch and placebo gum group. | Not reported | AEs measured during treatment (6 months). |
| Croghan 2003 | 4/459 (0.9%) patch group; 14/463 (3%) spray group; 2/462 (0.4%) combined group. | Not reported | Not reported | AEs measured to 6 months . Treatment was for 6 weeks. Only most common AEs reported. "No other AEs were reported with a great deal of frequency" |
| Cummings 2011 | Not reported | Not reported | Not reported | No AE data reported |
| Dale 1995 | 1/18 (5.6%) 44 mg group; 0/17 (0%) 22 mg group. | Not reported | Not reported | AEs (nicotine toxicity only, not including cardiac) measured during first week of treatment (inpatient phase). Treatment continued for 6 weeks |
| Daughton 1991 | 2 (1.3%) participants overall. Not reported by trial arm. | Not reported | Not reported | AEs measured weekly during treatment (4 weeks). Only most common AEs reported (i.e. in > 5% of participants) |
| Dennis 2016 | Not reported | Not reported | Not reported | No AE data reported |
| Garvey 2000 | 2/203 4 mg gum group; 1/202 2 mg gum group | Not reported | Not reported | AEs not reported in detail by relevant trial arms. |
| Glavas 2003 | 1/40 3 week group (additional person withdrew as perceived treatment as ineffective); 2/40 6 week group | CARDIAC: 0/40 (0%) three week group; 0/40 (0%) six week group. | 0/40 intervention group; 0/40 control group. | AEs measured during treatment (3 weeks or 6 weeks depending on treatment group) |
| Goldstein 1989 | Not reported | Not reported | Not reported | No AE data reported |
| Hall 2009 | Not reported | MIDSTERNAL PRESSURE: 1/203 (0.5%) extended (50 week) NRT group; 0/199 (0%) in brief (10 week) NRT group. | 9/203 extended (50 week) NRT group; 4/199 brief (10 week) NRT group. CARDIAC SAEs: 4/203 extended (50 week) NRT group; 0/199 brief (10 week) NRT group. | AEs measured to week 104. Treatment was to week 50. |
| Hays 1999 | Not reported | CARDIOVASCULAR (ANGINA PECTORIS, CARDIOVASCULAR DISORDER, CHEST PAIN, AND/OR MYOCARDIAL INFARCTION): 5/321 (1.6%) free patches group; 9/315 (2.9%) pay for patches group. | SAEs not fully reported. 5 cardiovascular SAEs in trial (2 myocardial infarction: 1 in known NRT arm, 1 in placebo arm (not used in this review). | AEs measured during treatment (6 weeks) |
| Herrera 1995 | Not reported | Not reported | Not reported | Adverse effects measured daily during treatment. Tachycardia was observed. Not reported in detail by relevant trial arms. |
| Hilleman 1994 | 7/69 (10%) Fixed dose; 8/71 (11%) tapered dose | Not reported | Not reported | Some AE data reported. Time measured not reported. |
| Hughes 1990 | Not reported | Not reported | Not reported | AEs (not including cardiac) measured during treatment (at 1 week). |
| Hughes 1991 | Not reported | Not reported | Not reported | No AE data reported |
| Hughes 1999 | 3/260 (1%) 21 mg group; 8/260 (3%) 35 mg group; 16/259 (6%) 42 mg group. | CARDIAC (mostly tachycardia, vasodilation and palpitation): 8% of 42 mg group, not reported for other groups. | 3/259 42 mg group; 1/260 35 mg group; 1/260 21 mg group. | Withdrawals in first 4 months. AEs measured to 6 or 12 months depending on site. Treatment was for 16 weeks. AEs not reported in detail by relevant trial arms |
| Hughes 2018 | 9% overall. Not reported by trial arm. | Not reported | 4/356 continue patch group; 4/345 discontinue patch group. 1 SAE in each group was cardiac related. | AEs measured to 1 week post treatment (12 weeks). Only most common AEs reported. |
| Jorenby 1995 | Not reported | Not reported | 4/252 44 mg intervention group (2 cardiovascular: stroke and myocardial infarction); 0/252 control group. | AEs measured weekly during treatment (8 weeks). Only most common AEs reported. |
| Kalman 2006 | Not reported | Not reported | Not reported | AEs measured during treatment (up to 12 weeks post‐quit) |
| Killen 1990 | 21/152 (13.7%) ad lib group; 16/147 (12.5%) fixed group | Not reported | Not reported | AEs measured weekly during treatment (8 weeks). Only most common AEs reported (10 most common). |
| Killen 1999 | Not reported | IRREGULAR HEARTBEAT: 21/206 (10%) 25 mg group; 20/202 (10%) 15 mg group. SEVERE IRREGULAR HEARTBEAT: 5/206 (2.4%) 25 mg group; 6/202 (3%) 15 mg grou. | Not reported | AEs self‐reported by participants. Measured during treatment (to 6 weeks) |
| Kornitzer 1987 | Not reported | Not reported | Not reported | No AE data reported |
| Kornitzer 1995 | 1/149 (0.7%) nicotine patch and gum group; 2/150 (1.3%) nicotine patch and placebo gum group | Not reported | Not reported | AEs measured at each visit during treatment (6 months). Not reported in detail by relevant trial arms. |
| Krupski 2016 | Not reported | Not reported | Not reported | No AE data reported |
| Kupecz 1996 | 0/21 (0%) patch group; 4/17 (23%) gum group. | CARDIAC: 0/21 (0%) patch group; 0/17 (0%) gum group. | 0/21 patch group; 0/17 gum group. | AEs measured at each session to 1 year. Treatment was for 24 weeks. AEs presented here measured at 6 weeks (during treatment) |
| Lerman 2004 | Not reported | Not reported | 0/175 patch group; 0/175 spray group. | AEs measured in counselling sessions during treatment (8 weeks) |
| Moolchan 2005 | Not reported | Not reported | Not reported | AEs measured during treatment (12 weeks). Only most common AEs reported (19 most common). |
| Paoletti 1996 | Not reported | Not reported | Not reported | AEs measured at visits. Participants were asked about particular symptoms but none cardiac. Paper states, "Heart rate and blood pressure were not affected by the different treatments." |
| Piper 2009 | 0/260 (0%) lozenge group; 0/262 (0%) patch and lozenge group | Not reported | 32 SAEs in 6 months. Not reported by trial arm. | AEs measured at visits during treatment (8 weeks). No SAE were possibly related to treatment and no withdrawals due to AEs in relevant trial arms. |
| Piper 2016 | Not reported | Not reported | 0 SAEs in any group. 0 cardiac SAEs in any group. | AEs measured to 26 weeks. Not reported in detail by relevant trial arms |
| Puska 1995 | Not reported | Not reported | Not reported | AEs measured at all visits during treatment (52 weeks). Only moderate or severe AEs reported. |
| Rey 2009 | 2 (4%) participants overall. Not reported by trial arm | Not reported | Not reported | No AE data reported |
| Rose 1994 | Not reported | Not reported | Not reported | AEs measured until 1 week after treatment. Only AEs relating to mecamylamine treatment discussed. |
| Rose 1998 | 0/40 (0%) preloading group; 1/40 (2.5%) no preloading group | Not reported | Not reported | AEs measured during preloading period. 5 people withdrew for reasons unrelated to treatment. |
| Rose 2006 | Not reported | Not reported | Not reported | No AE data reported |
| Rose 2009 | Not reported | Not reported | 1/191 preloading nicotine patch group; 3/188 preloading placebo patch group. | Timing of AEs measurements not reported. AEs only reported if self‐reported severity was moderate or greater. |
| Rose 2010 | 3% overall. Not reported by trial arm. | Not reported | Not reported | AEs measured during treatment (12 weeks). Not reported in detail by relevant trial arms |
| Schlam 2016 | Not reported | Not reported | 10/275 26‐week patch group; 6/269 8‐week patch group. CARDIAC SAEs: 4/275 26‐week patch group; 5/269 8‐week patch group. | AEs measured to 1 year. Treatment was for 8 or 26 weeks. Only most common AEs reported. SAE data from clinicaltrials.gov. Paper states no SAE in trial. |
| Schnoll 2010a | 1/282 (0.4%) extended treatment group; 0/282 (0%) standard treatment group | POUNDING HEART: Week 1: 2/247 (0.8%) extended group; 3/252 (1.2%) standard group. Week 12: 0/182 (0%) extended group; 2/134 (1.5%) standard group. | 3/282 extended NRT group (including 1 myocardial infarction); 1/286 standard NRT group | AEs measured to 1 year. Treatment was for 8 or 24 weeks. AE denominators are participants followed. The myocardial infarction occurred before treatment started |
| Schnoll 2010b | Not reported | Not reported | 4/321 patch group (including 2 strokes); 7/321 lozenge group (including 1 heart disease and 1 myocardial infarction). | AEs measured to 6 months. Treatment was for 12 weeks. AEs not reported in detail by relevant trial arms. All SAE considered unrelated to study treatment (as did not occur whilst on treatment) except stroke in patch group. |
| Schnoll 2015 | Not reported | POUNDING HEART: At 12 weeks: 0/128 (0%) 8 week group; 1/137 (0.7%) 24 week group; 2/121 (1.7%) 52 week group. At 30 weeks: 2/103 (1.9%) 8 week group; 1/116 (0.9%) 24 week group; 1/103 (1.0%) 52 week group. RAPID HEARTBEAT: 1/103 (1%) 8 week group; 1/116 (0.9%) 24 week group; 0/103 (0%) 52 week group. | 4/180 8‐week patch group; 2/173 24‐week patch group; 8/172 52‐week patch group. | Cardiac AEs are not cumulative across time points. |
| Schuurmans 2004 | Not reported | Not reported | Not fully reported. One death in each group. | AEs measured at all follow‐up visits (to 6 months). Treatment was for 12 weeks. AEs not reported in detail by relevant trial arms |
| Smith 2009 | Not reported | Not reported | Not reported | No AE data reported |
| Smith 2013 | Not reported | Not reported | 0/490 2‐week NRT group; 0/497 6‐week NRT group; 0/494 patch group; 0/493 patch and gum group. | No AE data reported |
| Stapleton 1995 | 8 (2%) overall. Not reported by trial arm. | Not reported | Not reported | AEs measured at each visit. Not reported in detail by relevant trial arms. |
| Preloading Investigators 2018 | Not reported | PALPITATIONS: 35/899 (3.9%) preloading group; 17/893 (1.9%) control group | 8/899 preloading group (3 cardiac) ; 8/893 control group (0 cardiac) | AEs measured to 1 week post‐quit (1 week after preloading ceased) |
| TNSG 1991 | 11/262 (4.2%) 21 mg group; 15/275 (5.5%) 14 mg group; 1/127 (0.8%) 7 mg group | Not reported | 0 SAEs in any group | AEs not reported in detail by relevant trial arms |
| Tønnesen 1988 | 0/27 (0%) 4 mg group; 1/33 (3%) 2 mg group. | PALPITATIONS: 1/27 (3.7%) 4 mg group; 0/33 (0%) 2 mg group. | Not reported. | AEs measured in counselling sessions during treatment (either 16 or 20 weeks) |
| Tønnesen 1996 | 0/45 (0%) ad libitum group; 0/44 (0%) fixed group. | PALPITATIONS: at 1 week: 1 moderate and 1 severe overall (not spilt by treatment group). At 6 weeks: 0% in both groups. | 0 SAEs in any group. | AEs measured on treatment (up to 6 weeks) |
| Tønnesen 2000 | Not reported | Not reported | 0/109 5 mg patch group; 0/104 15 mg patch group; 0/118 inhaler group; 0/115 inhaler and 15 mg patch group | AEs measured at every follow‐up (to 12 months). Treatment could continue to 12 months |
| Tulloch 2016 | 5/245 (2%) patch and gum group; 4/245 (1.6%) patch group. | CARDIOVASCULAR (E.G PALPITATIONS, TACHYCARDIA, CHEST PAIN): 3/245 (1.2%) patch and fast‐acting NRT group; 5/245 (2%) patch only group | 6/245 patch and gum group; 9/245 patch group. | AEs measured at each appointment |
| Walker 2011 | Not reported | Not reported | 53/706 selection box group; 51/704 usual care group. | SAEs measured to 6 months. Treatment was for 8 weeks. |
Appendix 3. British National Formulary prescribing guidance for NRT as relates to comparisons in this review
| Comparison of interest | BNF recommendation | Review findings |
| Patch duration | “Individuals who smoke more than 10 cigarettes daily should apply a high‐strength patch daily for 6 ‐ 8 weeks, followed by the medium‐strength patch for 2 weeks and then the low‐strength patch for the final 2 weeks; individuals who smoke fewer than 10 cigarettes daily can usually start with the medium‐strength patch for 6 ‐ 8 weeks, followed by the low‐strength patch for 2 ‐ 4 weeks” > 10 cigarettes per day: 10 ‐ 12 weeks < 10 cigarettes per day: 8 ‐ 12 weeks |
Low‐certainty evidence of no effect of duration of nicotine patch use on smoking cessation. Studies in the review typically recruited smokers who were smoking at least 15 cigarettes per day so comparisons with BNF guidance for individuals smoking < 10 cigarettes per day cannot be made. |
| Patch dose | “Individuals who smoke more than 10 cigarettes daily should apply a high‐strength patch… individuals who smoke fewer than 10 cigarettes daily can usually start with the medium‐strength patch…” > 10 cigarettes per day: high strength (21/22/25 mg) then tapered < 10 cigarettes per day: medium strength (15 mg) then tapered |
Moderate‐certainty evidence that 21 mg patches result in higher quit rates than 14 mg 24 hr patches Moderate‐certainty evidence that 25 mg patches result in higher quit rates than 15 mg (16‐hour) patches, though the CI includes one. Moderate‐certainty evidence that 42/44 mg patches (not available in UK) are as effective as 21/22 mg patches Low‐certainty evidence of no difference of dose on SAEs or treatment withdrawals Studies in the review typically recruited smokers who were smoking at least 15 cigarettes per day so comparisons with BNF guidance for individuals smoking < 10 cigarettes per day cannot be made |
| Patch tapering | “Individuals who smoke more than 10 cigarettes daily should apply a high‐strength patch daily for 6‐8 weeks, followed by the medium‐strength patch for 2 weeks and then the low‐strength patch for the final 2 weeks; individuals who smoke fewer than 10 cigarettes daily can usually start with the medium‐strength patch for 6‐8 weeks, followed by the low‐strength patch for 2‐4 weeks” > 10 cigarettes per day: 6 ‐ 8 weeks high strength, 2 weeks medium strength, 2 weeks low strength < 10 cigarettes per day: 6 ‐ 8 weeks medium strength, 2 ‐ 4 weeks low strength. |
No evidence of difference between tapering and abrupt patch cessation on abstinence Studies in the review typically recruited smokers who were smoking at least 15 cigarettes per day so comparisons with BNF guidance for individuals smoking <10 cigarettes per day cannot be made |
| Patch 16‐hour vs 24‐hour | No reference to hours of use per day | No evidence of effect of hours of use per day on abstinence. |
| Ceasing vs continuing on lapse | “if abstinence is not achieved, or if withdrawal symptoms are experienced, the strength of the patch used should be maintained or increased until the patient is stabilised” Continue on lapse |
No evidence of effect on abstinence of instructing participants to continue using a patch versus stopping patch use, in the event of a smoking lapse. |
| Patch preloading | No specific reference but does refer to using patch prior to quit day to reduce cigarette consumption: “a slower titration schedule can be used [for patches] in individuals who are not ready to quit but want to reduce cigarette consumption before a quit attempt” |
Moderate‐certainty evidence of a positive effect of NRT preloading on abstinence. |
| Combination NRT | No reference to combination NRT | High‐certainty evidence that combination NRT results in higher long‐term quit rates, whether combination therapy was compared to patch or to an fast‐acting form of NRT. Low‐ to very low‐certainty evidence of no effect on cardiac AEs, SAEs or study withdrawals |
| Type of NRT | No recommendations on which type of NRT to use. | High‐certainty evidence of no difference between fast‐acting NRT and patch on smoking cessation Very low‐certainty evidence of no difference in effect of type of fast‐acting NRT (oral spray, gum or inhaler) on smoking cessation |
| Gum dose | “In individuals who smoke fewer than 20 cigarettes each day… 2 mg as required, chew 1 piece of gum when the urge to smoke occurs or to prevent cravings” “In individuals who smoke more than 20 cigarettes each day or who require more than 15 pieces of 2 mg strength gum each day… 4 mg as required, chew 1 piece of gum when the urge to smoke occurs or to prevent cravings, individuals should not exceed 15 pieces of 4 mg strength gum daily” > 20 cigarette a day: 4 mg < 20 cigarette a day: 2 mg |
Evidence that using 4 mg gum results in higher quit rates than 2 mg gum. A post hoc subgroup analysis found a statistically significant benefit of 4 mg dose over 2 mg dose for higher dependency smokers, but not for lower dependency smokers. |
| Duration of gum | “Treatment should continue for 3 months before reducing the dose” | No significant effect of 50 weeks gum over 10 weeks gum use on smoking cessation |
| Fixed dose vs ad lib dosing for fast‐acting NRT | Gum: “Chew 1 piece of gum when the urge to smoke occurs or to prevent cravings” Sublingual tablet: “1 [or 2] tablet[s] every 1 hour” Inhalator: “As required, the cartridges can be used when the urge to smoke occurs or to prevent cravings” Lozenges: “1 lozenge every 1‐2 hours as required, one lozenge should be used when the urge to smoke occurs” Oromucosal spray: “1‐2 sprays as required, individuals can spray in the mouth when the urge to smoke occurs or to prevent cravings” Nasal spray: “1 spray as required, individuals can spray into each nostril when the urge to smoke occurs, up to twice every hour” Advice differs by type of fast‐acting NRT. Ad lib for gum and nasal spray |
No evidence of an effect of fixed versus ad lib dosing of fast‐acting NRT (gum and nasal spray) on abstinence |
| As specified in the Methods section we only carried out GRADE assessments and created 'Summary of findings' tables for some of the comparisons (and their associated outcomes) in this review. Therefore, only some of the review findings above are accompanied by a GRADE rating of the certainty of the evidence. | ||
Data and analyses
Comparison 1. Patch dose.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Smoking cessation | 9 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 21 mg versus 14 mg (24‐hour) | 1 | 537 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.48 [1.06, 2.08] |
| 1.2 25 mg versus 15 mg (16‐hour) | 3 | 3446 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.19 [1.00, 1.41] |
| 1.3 42/44 mg versus 21/22 mg (24‐hour) | 5 | 1655 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.09 [0.93, 1.29] |
| 2 Fast or irregular heartbeat | 2 | 3269 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.92 [0.64, 1.33] |
| 3 Myocardial infarction | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4 Overall SAEs | 3 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 4.1 42/44 mg versus 21/22 mg (24‐hour) | 2 | 1023 | Risk Ratio (M‐H, Fixed, 95% CI) | 5.01 [0.87, 28.82] |
| 4.2 21 mg versus 14 mg (24‐hour) | 1 | 537 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5 Treatment withdrawals | 3 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 5.1 42/44 mg versus 21/22 mg (24‐hour) | 2 | 554 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.99 [1.60, 15.50] |
| 5.2 21 mg versus 14 mg (24‐hour) | 1 | 537 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.77 [0.36, 1.64] |
Comparison 2. Duration of patch therapy.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Smoking cessation | 7 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 52 weeks versus 24 weeks | 1 | 345 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.78 [0.53, 1.15] |
| 1.2 52 weeks versus 8 weeks | 1 | 352 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.63, 1.41] |
| 1.3 28 weeks versus 12 weeks | 1 | 2861 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.88, 1.26] |
| 1.4 24 weeks versus 8 weeks | 2 | 921 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.10 [0.84, 1.45] |
| 1.5 12 weeks versus 6 weeks | 1 | 140 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.62, 1.71] |
| 1.6 12 weeks versus 3 weeks | 1 | 98 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.26, 1.41] |
| 1.7 6 weeks versus 4 weeks | 1 | 1873 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.06 [0.85, 1.33] |
| 1.8 6 weeks versus 2 ‐ 3 weeks | 2 | 1957 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.13 [0.91, 1.40] |
| 1.9 4 weeks versus 2 weeks | 1 | 1862 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.85, 1.37] |
| 2 Overall SAEs | 3 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.1 52 weeks versus 24 weeks | 1 | 345 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.02 [0.87, 18.67] |
| 2.2 52 weeks versus 8 weeks | 1 | 352 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.09 [0.64, 6.82] |
| 2.3 24 weeks versus 8 weeks | 2 | 921 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.30, 3.54] |
| 2.4 6 weeks versus 2 ‐ 3 weeks | 1 | 80 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 3 Treatment withdrawals | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.1 24 weeks versus 8 weeks | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 6 weeks versus 2 ‐ 3 weeks | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 3. Effect of tapering patch dose.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Smoking cessation | 2 | 264 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.74, 1.32] |
| 2 Treatment withdrawals | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected |
Comparison 4. Combination versus single‐form NRT.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Smoking cessation | 14 | 11356 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.25 [1.15, 1.36] |
| 1.1 Combination NRT versus patch alone | 12 | 8992 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.23 [1.12, 1.36] |
| 1.2 Combination NRT versus fast‐acting NRT alone | 6 | 2364 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.30 [1.09, 1.54] |
| 2 Any cardiac AE | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3 Overall SAEs | 5 | 2888 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.44 [0.76, 25.85] |
| 3.1 Combination NRT versus patch alone | 4 | 2313 | Risk Ratio (M‐H, Fixed, 95% CI) | 11.45 [0.64, 205.90] |
| 3.2 Combination NRT versus fast‐acting NRT alone | 2 | 575 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.0 [0.06, 15.88] |
| 4 Treatment withdrawals | 5 | 3070 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.12 [0.57, 2.20] |
| 4.1 Combination NRT versus patch alone | 5 | 1982 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.32 [0.99, 5.40] |
| 4.2 Combination NRT versus fast‐acting NRT alone | 2 | 1088 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.14 [0.02, 1.08] |
Comparison 5. Duration of combination therapy.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Smoking cessation | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 16 weeks versus 8 weeks | 1 | 637 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.75, 1.23] |
| 1.2 6 weeks versus 2 weeks | 1 | 987 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.11 [0.94, 1.31] |
| 2 Overall SAEs | 3 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.1 26 weeks versus 8 weeks | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 16 weeks versus 8 weeks | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.3 6 weeks versus 2 weeks | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 6. Fast‐acting NRT versus patch.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Smoking cessation | 8 | 3319 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.77, 1.05] |
| 1.1 Inhaler versus patch | 1 | 222 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.59 [0.22, 1.60] |
| 1.2 Nasal spray versus patch | 2 | 1272 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.64, 1.27] |
| 1.3 Lozenge versus patch | 3 | 1707 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.79, 1.12] |
| 1.4 Gum versus patch | 2 | 118 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.58 [0.26, 1.31] |
| 2 Cardiac AEs | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3 Overall SAEs | 4 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.1 Inhaler versus patch | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Nasal spray versus patch | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.3 Lozenge versus patch | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.4 Gum versus patch | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 Treatment withdrawals | 3 | 1482 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.23 [1.54, 11.63] |
| 4.1 Nasal spray versus patch | 1 | 922 | Risk Ratio (M‐H, Fixed, 95% CI) | 3.47 [1.15, 10.46] |
| 4.2 Gum versus patch | 1 | 38 | Risk Ratio (M‐H, Fixed, 95% CI) | 11.0 [0.63, 191.04] |
| 4.3 Lozenge versus patch | 1 | 522 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
6.2. Analysis.

Comparison 6 Fast‐acting NRT versus patch, Outcome 2 Cardiac AEs.
Comparison 7. Type of fast‐acting NRT.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Smoking cessation | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.1 Oral spray versus gum | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Oral spray versus inhaler | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 Gum versus inhaler | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 8. 4 mg versus 2 mg gum.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Smoking cessation | 5 | 856 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.43 [1.12, 1.83] |
| 1.1 High‐dependency smokers | 4 | 618 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.85 [1.36, 2.50] |
| 1.2 Low‐dependency smokers | 3 | 238 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.77 [0.49, 1.21] |
| 2 Palpitations | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3 Treatment withdrawals | 2 | 465 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.08 [0.18, 6.36] |
Comparison 9. Fixed versus ad lib dose schedule.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Smoking cessation | 4 | 828 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.12 [0.87, 1.45] |
| 1.1 Gum | 2 | 689 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.22 [0.92, 1.61] |
| 1.2 Nasal spray | 2 | 139 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.67 [0.35, 1.30] |
| 2 Overall SAEs | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3 Treatment withdrawals | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.1 Gum | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Nasal spray | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
9.2. Analysis.

Comparison 9 Fixed versus ad lib dose schedule, Outcome 2 Overall SAEs.
Comparison 10. Preloading versus standard use.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Smoking cessation | 9 | 4395 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.25 [1.08, 1.44] |
| 1.1 Patch | 9 | 3830 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.28 [1.09, 1.49] |
| 1.2 Gum | 2 | 306 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.58, 1.49] |
| 1.3 Patch + gum | 2 | 259 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.35 [0.80, 2.28] |
| 2 Palpitations | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3 Cardiac AEs | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4 Cardiac SAEs | 3 | 3529 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.94 [0.81, 4.65] |
| 5 Overall SAEs | 4 | 3908 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.11 [0.59, 2.09] |
| 6 Treatment withdrawals | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected |
Comparison 11. Free NRT versus purchased NRT.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Smoking cessation | 2 | 740 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.38 [0.90, 2.13] |
| 1.1 Patch | 1 | 636 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.24 [0.77, 1.99] |
| 1.2 Gum | 1 | 104 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.7 [0.89, 8.20] |
| 2 Cardiac AEs | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected |
11.1. Analysis.

Comparison 11 Free NRT versus purchased NRT, Outcome 1 Smoking cessation.
Comparison 12. Duration of free NRT.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Smoking cessation | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 2 weeks versus 1 week patch or gum | 1 | 562 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.63 [0.98, 2.70] |
| 1.2 8 weeks versus 4 weeks patch | 1 | 1495 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.97 [0.64, 1.48] |
12.1. Analysis.
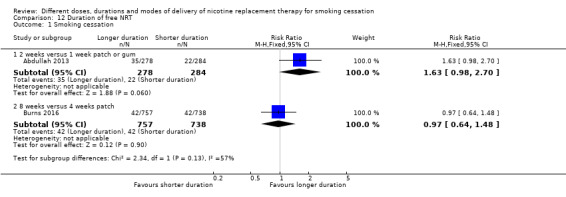
Comparison 12 Duration of free NRT, Outcome 1 Smoking cessation.
Comparison 13. Other comparisons.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Smoking cessation | 5 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 24‐hour versus 16‐hour patch | 1 | 106 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.70 [0.36, 1.34] |
| 1.2 50 weeks versus 10 weeks gum | 1 | 402 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.82, 1.32] |
| 1.3 Continue versus stop patch use on lapse | 1 | 701 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.89 [0.77, 1.02] |
| 1.4 35 mg patch + fast‐acting for 22 weeks versus 21 mg patch for 10 weeks | 1 | 486 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.25 [0.75, 2.10] |
| 1.5 NRT tester period + choice versus clinician‐advised | 1 | 4230 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.15 [1.00, 1.32] |
| 2 Midsternal pressure | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.1 50 weeks versus 10 weeks gum | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Cardiac AEs | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4 Overall SAEs | 4 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.1 50 weeks versus 10 weeks gum | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Continue versus stop patch use on lapse | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.3 35 mg patch + fast‐acting for 22 weeks versus 21 mg patch for 10 weeks | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.4 NRT tester period + choice versus clinician advised | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 Treatment withdrawals | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 5.1 35 mg patch + fast‐acting for 22 weeks versus 21 mg patch for 10 weeks | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Abdullah 2013.
| Methods | Country: China Recruitment: from a smoking cessation health centre ‐ smokers who called the booking line and attended the health centre during the study period were recruited by smoking cessation counsellor |
|
| Participants | 562 smokers: aged ≥ 16 yrs, ≥ 5 cpd, clearly motivated to quit 78.3% men; av. cpd: 18.8; av years smoking 18.5 |
|
| Interventions | 1. 2 weeks of free NRT (patch or gum according to participant preference). However, participants were encouraged to use NRT for 8 ‐ 12 weeks, sourcing the remainder themselves 2. 1 week of free NRT (patch or gum according to participant preference). However, participants were encouraged to use NRT for 8 ‐ 12 weeks, sourcing the remainder themselves |
|
| Outcomes | PPA at 6m follow‐up; CO validated (< 9 ppm) Other abstinence measures: self‐reported 7‐day pp at 6m; self‐reported 24‐hour pp at 6 m and 12 m; self‐reported continuous at 6 m and 12 m; quit for at least 24 hours at some point before 6 m and 12 m follow‐up Adverse events: not measured |
|
| Notes | 70% of participants chose patch, 30% chose gum, with similar between‐group percentages The study was funded by the Hong Kong Council on Smoking and Health (COSH). Pfizer Consumers and Novartis partially sponsored the printing cost of the clinic pamphlets and provided some free NRT samples Conflicts of interest: the authors declared no conflict of interests |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “The random numbers for group assignment were generated by the research assistant (not the counselors) of the project using a personal computer before subject recruitment.” |
| Allocation concealment (selection bias) | Low risk | Quote: “Eligible selected subjects signed the consent form and completed the baseline measures…before the counselor opened a serially numbered, opaque, and sealed envelope (SNOSE) to reveal the random assignment of each smoker to A1 or A2 group.” |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Quote: “An independent interviewer, who was unaware of the subject’s group allocation, carried out the 6 and 12 months follow‐up interview.” Participants were aware whether they were provided 1 or 2 weeks free NRT; however it would be impossible to blind for this |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropout rates at 6m were 75/278 in group 1 (2 weeks free NRT) and 83/284 in group 2 (1 week free NRT). There was therefore less than 50% dropout overall and rates were similar between groups |
Baker 2016.
| Methods | Country: USA Recruitment: participants were recruited from 2 sources: (1) by contacting participants in the authors' ongoing longitudinal study of smokers, the Wisconsin Smokers Health Study; and (2) by media and community outreach |
|
| Participants | 1086 smokers (662 in relevant trial arms): aged > 17 yrs, ≥ 5 cpd, desire to quit smoking but not engaged in smoking treatment, willingness to use the tested cessation treatments and not using e‐cigarettes 47.9% men; av. age: 48.1 yrs; av. cpd: 17; av. FTND: 4.8; av. exhaled CO: 15.1 ppm |
|
| Interventions | 1. Combination NRT: nicotine patch (12 weeks ‐ 21 mg for 8 weeks, 14 mg for 2 weeks, 7 mg for 2 weeks) and lozenge (12 weeks ‐ 2 or 4 mg based on addiction level, asked to use at least 5 lozenges a day) 2. Nicotine patch only (12 weeks ‐ 21 mg for 8 weeks, 14 mg for 2 weeks, 7 mg for 2 weeks) In both groups treatment began on quit day |
|
| Outcomes | 7‐day PPA at 52 weeks follow‐up; CO validated (≤ 5 ppm) Other abstinence measures: 7‐day PPA at 26 weeks with CO validation; self‐reported prolonged abstinence at 26 weeks (no smoking from day 7 to day 181 post‐quit day) Adverse events: measured for duration of treatment (12 weeks) |
|
| Notes | This was a 3‐arm trial comparing varenicline, nicotine patch and nicotine patch+lozenge. For the purposes of this review we are only interested in the nicotine patch and nicotine patch + lozenge groups The study was funded by grant 5R01HL109031 from the National Heart, Lung, and Blood Institute and grant K05CA139871 from the National Cancer Institute Conflicts of interest: Dr Stein reports receipt of data and safety monitoring board honoraria from Lilly and Abbott. No other disclosures were reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “Computer‐based randomization” |
| Allocation concealment (selection bias) | Low risk | Quote: “Computer‐based randomization” |
| Blinding (performance bias and detection bias) All outcomes | High risk | At risk of both performance and detection bias Quote: “Treatment assignment was unblinded” Quote: “The follow‐up telephone assessments were intended to be blinded, but a database search by interviewers could have revealed treatment assignment.” |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Overall loss to follow‐up across all 3 groups at 12 m = 22.5%. Loss to follow‐up of 22.4% in nicotine patch group and 21.6% in the combination NRT group; therefore similar between trial arms of interest. This information on losses to follow‐up was obtained directly from the study authors |
Blondal 1999.
| Methods | Country: Iceland Recruitment: community volunteers | |
| Participants | 237 smokers (≥ 1 cpd) 33% men, av. age 41 ‐ 43, av. tobacco use 25 g/day | |
| Interventions | 1. Nicotine nasal spray (NNS) (0.5 mg/dose) + 15 mg nicotine patches for 3 m, weaning over further 2 m. NNS could be continued for 1 yr 2. Placebo nasal spray + 15 mg nicotine patches on same schedule | |
| Outcomes | Sustained abstinence at 12 m (6‐yr data also reported)
Validation: CO < 10 ppm Adverse events: measured within 3 months of follow‐up (still using NRT) |
|
| Notes | 6‐yr abstinence 19/118 vs 10/119, OR 2.1 Pharmacia and Upjohn provided the drugs and placebo for this study and measured the cotinine concentrations. Conflicts of interest: TB was a consultant for Pharmacia and Upjohn, and GG and AW are employed by Pharmacia and Upjohn |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "computer generated randomisation code at a local pharmacy" |
| Allocation concealment (selection bias) | Low risk | Quote: "Pharmacy staff were blinded to the content of the bottles" |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Clinic staff, pharmacy staff and pts all blinded to assignment. Codes not broken until after data entry and analyses completed |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All pts followed up for at least 12 m |
Bohadana 2000.
| Methods | Country: France Recruitment: community volunteers | |
| Participants | 400 smokers, 18 ‐ 70 yrs, > 10 cpd, > 1 previous quit attempt, motivated 49% men, av cpd: Group 1: 26.1, Group 2: 23.5; FTND > 6 Pts required to be motivated to quit. | |
| Interventions | 1: Nicotine inhaler, 26 wks, combined with nicotine patch (15 mg/16‐hour) for first 6 wks, placebo patch for next 6 wks 2: Nicotine inhaler, 26 wks, placebo patch for first 12 wks | |
| Outcomes | Sustained abstinence at 12 m (prolonged from wk 2, no slips allowed)
Validation: CO < 10 ppm at each visit (2 wks, 6 wks, 6 m, 12 m)
(Study also reports respiratory symptoms and pulmonary function tests for completely abstinent participants) Adverse events: measured to 1‐year follow‐up (treatment ceased at 6 months) |
|
| Notes | Gender subgroup results reported 2003
This study was supported by a grant from Pharmacia and Upjohn Consumer Healthcare. Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "computer‐generated randomization code" |
| Allocation concealment (selection bias) | Low risk | Quote: "sealed randomization envelopes were provided for each subject and were held by the hospital pharmacy, which was responsible for dispensing medication" |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Described as double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses over 12 m were steep but similar in both groups, i.e. 148 from NRT group and 155 from placebo group. Losses counted as continuing smokers |
Bolin 1999.
| Methods | Country: USA Recruitment: smoking cessation clinic | |
| Participants | 98 smokers 84% men, av. age 54, av. cpd 20 | |
| Interventions | 1. Nicotine patch for 12 wks (21 mg/3 wks, 14 mg/3 wks, 7mg/3 wks) 2. Nicotine patch for 3 wks (21 mg/1 wk, 14 mg/1 wk, 7mg/1 wk) | |
| Outcomes | Continuous abstinence at 5 m (PP also recorded)
Validation: CO Adverse events: not measured |
|
| Notes | Borderline follow‐up length ‐ 20 wks from beginning of programme, 16 wks since start of NRT Funding and declarations of interest not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Participants were randomly assigned ... random assignment took place on the first day of patch administration" |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Quote: "Both participants and experimenters were unaware of assignment during the baseline phase of the study" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Dropout rates not reported; any dropouts counted as treatment failures in analysis |
Bolliger 2007.
| Methods | Country: South Africa Recruitment: by a newspaper advertisement |
|
| Participants | 100 smokers: aged ≥ 18 yrs, > 15 cpd, smoked for > 3 y, exhaled CO > 10 ppm, serious quit attempts in the past 12 m, willing to stop smoking immediately 60% men; av. age: 43.1 y; av. cpd: 23.4; av. FTND: 5.6; av. exhaled CO: 25.5 ppm |
|
| Interventions | 1. Nicotine mouth spray 2. Nicotine gum 3. Nicotine inhaler Participants in all groups were advised to use their allocated product for 12 weeks from quit day, ad libitum (recommended 6 ‐ 12 actuations/cartridges a day) |
|
| Outcomes | Continuous smoking abstinence at 6 m follow‐up (not a puff since quit day); CO‐validated (< 10 ppm) Other abstinence measures: self‐reported continuous at 12 m follow‐up; self‐reported PPA at 12 m; CO‐validated PPA at 6 m Adverse events: measured at each visit to final follow‐up at 1 year (treatment only lasted 12 weeks) |
|
| Notes | The trial was fully funded by NicoNovum AB (the pharmaceutical company who manufactured the mouth spray tested) Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not enough detail given to make a judgement Quote: “Subjects were then randomly allocated (block randomization of 4, i.e. after each block of 4 subjects, 2 were allocated to the spray, 1 to the gum and 1 to the inhaler) to the mouth spray (n = 50), the gum (n = 25) and the inhaler (n = 25) group, irrespective of their preference.” |
| Allocation concealment (selection bias) | Unclear risk | As above |
| Blinding (performance bias and detection bias) All outcomes | High risk | Open‐label trial. No description is given of any attempts to blind participants or assessors 7 participants changed their product during treatment: 2 from spray to gum and inhaler (1 each), 2 from gum to spray and inhaler (1 each), 3 from inhaler to spray (n = 2) and gum (n = 1); all 7 were considered treatment failures according to the principle of intention‐to‐treat |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Only 46% of participants attended final follow‐up (12 m), i.e. less than 50% of those randomized. There was differential dropout between groups (60% spray; 40% gum; 56% inhaler) with a 20% difference between the spray and gum groups |
Bullen 2010.
| Methods | Country: New Zealand Recruitment: callers to New Zealand Quitline | |
| Participants | 1100 smokers, motivated to quit 40% men, mean age 40, av.cpd 19 |
|
| Interventions | Trial of precessation NRT Intervention: NRT initiated 14 days before quit date, continued for 8 wks after quit date. 91% used patch only, 6% gum only, 3% both Control: NRT for 8 wks from quit date. 85% patch, 11% gum, 4% both |
|
| Outcomes | Continuous abstinence at 6 m (data supplied by 1st author) (Self‐reported 7‐day PPA at 6 m reported in paper) Validation: salivary cotinine in subgroup only. Self‐reported outcomes used in analysis Adverse events: measured at all contacts (assumed to be up to 6 months) |
|
| Notes | Participants able to select their treatment (patch, gum, or patch+gum) after discussion with adviser. Patch and gum outcomes supplied by 1st author, contribute to separate subgroups, 39 participants using combination not included in analysis. The study was funded by the Health Research Council and the Heart Foundation of New Zealand. HealthPAC approved the use of pre‐cessation NRT vouchers and the Pharmacy Guild of New Zealand supported the trial by alerting its member pharmacists to the PQNIQ trial and the special vouchers Conflicts of interest: HM has received honoraria for speaking at research symposia and received benefits in kind and travel support from, and has provided consultancy to the manufacturers of smoking cessation medications, including those that manufacture nicotine patches and gum. MG has provided consultancy to the manufacturers of smoking cessation medications, including those that manufacture nicotine patches and gum. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "People giving verbal consent by telephone were allocated randomly using central computerized randomization." |
| Allocation concealment (selection bias) | Low risk | Quote: "randomization sequence concealed until interventions were assigned" |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | No placebo. Single blinding: Quote: "Participants were aware of the group to which they were allocated but 3‐ and 6‐ month follow‐up methods were identical for all participants, and all follow‐up telephone calls and outcome verification procedures were made by research assistants blind to treatment allocation." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Similar rates of dropouts in treatment and control groups (148 treatment, 139 control). Participants lost to follow‐up included as smokers in outcome data |
Burns 2016.
| Methods | Country: USA Recruitment: by the Colorado quitline ‐ participants were recruited during regular initial quitline calls |
|
| Participants | 1495 smokers: smoking 16 ‐ 20 cpd, agreed to receive free NRT, absence of a condition requiring physician approval for NRT 40.0% men; av cpd 19.8, most smoked within 5 mins of waking and had been smoking for > 10 years |
|
| Interventions | 1. 4 weeks of free NRT (patches). However, participants were encouraged to complete 10 weeks of NRT, sourcing the remainder themselves 2. 8 weeks of free NRT (patches), shipped in 2 x 4‐week batches. Participants were required to request the second batch. Participants were encouraged to complete 10 weeks of NRT, sourcing the remainder themselves |
|
| Outcomes | Self‐reported prolonged abstinence at 6 m post‐quit day; no biochemical validation Other abstinence measures: self‐reported 7‐day and 30‐day PPA at 6 m Adverse events: not measured |
|
| Notes | Only ⅔ of group 2 (8 weeks of free NRT) accepted second 4‐week batch of NRT. Median time NRT used same in both groups (35 days) The study was funded by a Pfizer Scholar Grant in public health and the Colorado Department of Public Health and Environment contract number FLA‐11‐16830 Conflicts of interest: None |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Enrolled study participants were randomised"; but no detail given on how randomization took place |
| Allocation concealment (selection bias) | Unclear risk | As above. No detail on allocation concealment in text |
| Blinding (performance bias and detection bias) All outcomes | High risk | Quote: "Coaches ask all quitline enrolees during second and subsequent coaching calls about their NRT utilisation, and those who are eligible for a second shipment are asked whether they need it." No blinding. Although it would have been impossible to blind participants, it would have been possible to blind outcome assessors and we therefore deem this study to be at high risk of detection bias |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropout rates at 6 m were 311/738 in group 1 (4 weeks of free NRT) and 321/757 (8 weeks of free NRT). There was less than 50% dropout overall and rates were similar between groups |
Caldwell 2014.
| Methods | Country: New Zealand Recruitment: from media advertisements, clinician referrals, and a database of people interested in trying to stop smoking |
|
| Participants | 1423 smokers: aged 18 ‐ 70 years, ≥ 9 cpd, FTND ≥ 3. Ineligible if currently taking psychoactive medication/illicit drugs, drank > 28 units of alcohol a week, had hyperthyroidism/diabetes/severe renal or hepatic disease, were female and using inadequate contraception or were breastfeeding 46% men; mean age 45; av. cpd: 20; mean FTND: 6.1 |
|
| Interventions | 1. 6 m nicotine oral spray parallel to 5 m free 24‐hour nicotine patch. Each spray actuation contained 1 mg nicotine 2. 6 m placebo oral spray parallel to 5 m free 24‐hour nicotine patch. The placebo spray was dispensed in opaque bottles identical to the nicotine spray Both groups were instructed to use the spray ad libitum whenever they felt the urge to smoke, up to a maximum of 30 sprays/day Both groups received 21 mg/24‐hour nicotine patches for 18 weeks, then 14 mg/24‐hour nicotine patches for 2 weeks, and then 7 mg/24‐hour nicotine patches for 2 weeks |
|
| Outcomes | Prolonged abstinence at 12 m post‐quit day; CO‐validated (< 10 ppm). Prolonged abstinence defined as no smoking since end of grace period ‐ 4 weeks after quit day ‐ to 12m post‐quit Other abstinence measures: 7‐day PPA at 12 m follow‐up (CO‐validated) Adverse events: measured for 12 months (treatment was for 6 months) |
|
| Notes | Authors provided information on dosing schedule Funding for the study was provided by the Health Research Council of New Zealand (HRC 09/200). Active Zonnic mouth‐spray was provided by Niconovum. Placebo Zonnic was manufactured by Argenta according to instructions from Niconovum. Nicotine patches were provided without charge by the New Zealand Ministry of Health Conflicts of interest: None |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The randomization sequence was computer‐generated Quote: "Subjects were randomised centrally for all three trial sites using a random allocation algorithm built into the access database that was used for all of the data collection" |
| Allocation concealment (selection bias) | Low risk | Study participants were allocated into groups by a computer |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blinding maintained throughout trial Quote: "Active and placebo bottles were identical", "all staff remained blind to the allocation during the course of the trial" |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Dropout rates at 12 m were 612/716 for group 1 (nicotine spray + nicotine patch), and 621/707 for group 2 (placebo spray + nicotine patch). There was more than 50% dropout overall, but rates were similar between groups |
Caldwell 2016.
| Methods | Country: New Zealand Recruitment: from media advertisements, a study website, primary care practices and smoking cessation services |
|
| Participants | 502 smokers: aged 18 ‐ 70 years, ≥ 9 cpd, FTND ≥ 3 49% men; mean age: 45; av. cpd: 19; mean FTND: 6.2 |
|
| Interventions | 1. 6 m nicotine inhaler used parallel to 5 m 24‐hour nicotine patch. The nicotine inhaler contained 2 doses of nicotine lactate: 100 micrograms/puff and 200 micrograms/puff. Participants were instructed to start with the lower dose and move onto the higher dose once they had developed tolerance to the upper airway effects of the lower dose 2. 6 m placebo inhaler used parallel to 5 m 24‐hour nicotine patch. The placebo inhaler contained menthol in 2 doses to mimic the 2 doses of active inhaler and participants were also instructed to move onto the higher dose once they had developed tolerance to the upper airway effects of the lower dose Both groups were instructed to use the inhaler when they had an urge to smoke, and to have as many puffs as required to satisfy their urge (maximum 10 puffs) Both groups were instructed to use 21 mg/24‐hour nicotine patch for 18 weeks, 14 mg/24‐hour for 2 weeks, and 7 mg/24‐hour for 2 weeks |
|
| Outcomes | Prolonged abstinence (defined as not even a puff) at 6 m post‐quit date; CO‐validated at 1 m visit (≤ 10 ppm) Other abstinence measures: self‐reported 7‐day PPA at 6 m, self‐reported prolonged abstinence at 6 m Adverse events: measured for 6 months (duration of treatment) |
|
| Notes | Study funded by the Health Research Council of New Zealand (grant number 09/199) Conflicts of interest: None |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Eligible subjects were randomised to active or placebo inhaler in a 1:1 ratio by the trial database according to a sequential randomisation list that was not visible to research staff or subjects" |
| Allocation concealment (selection bias) | Low risk | Allocation concealment upheld (see quote above) |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Quote: "The database provided staff with a product code, which identified which inhaler to give to each subject. The product codes and inhalers for both groups had the same appearance...both subjects and staff were masked to treatment assignment" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropout rates at 6 m were 88/246 in group 1 (nicotine inhaler + nicotine patch), and 102/256 in group 2 (placebo inhaler + nicotine patch). There was therefore < 50% dropout overall and rates were similar between groups |
CEASE 1999.
| Methods | Country: Multicentre ‐ 36 clinic centres in 17 European countries Recruitment: community volunteers | |
| Participants | 3575 smokers (> 14 cpd) 52% men, av. age 41, av. cpd 27 (34% had previously used NRT) | |
| Interventions | Factorial design compared 2 patch doses and 2 treatment durations. Dose 15 mg or 25 mg (16‐hour), duration of active treatment 28 wks (incl 4‐wk fading) or 12 wks (incl 4‐wk fading). 1. 25 mg patch for 28 wks 2. 25 mg patch for 12 wks 3. 15 mg patch for 28 wks 4. 15 mg patch for 12 wks 5. Placebo | |
| Outcomes | Prolonged abstinence at 12 m, sustained from wk 2
Validation: expired CO < 10 ppm at each clinic visit Adverse events: SAEs measured during whole study period, but cardiac AEs reported within 8‐week treatment period |
|
| Notes | Level of support reclassified to high for 2007, because of repeated visits. Limited support at these visits
This study was sponsored by Pharmacia and Upjohn Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "A computer‐generated allocation list was prepared centrally and allocated subjects to treatment numbers". Randomization stratified by centre |
| Allocation concealment (selection bias) | Low risk | See process above |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Quote: "Active and placebo patches were identical in appearance and packaging. In order to maintain blinding, all subjects continued to use two patches for a total of 26 weeks", i.e. non‐tapered groups were switched to placebo patches |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 22% lost to 12‐m follow‐up, and 54% withdrew |
Cooney 2009.
| Methods | Country: USA Recruitment: community volunteers and referrals from substance abuse clinic |
|
| Participants | 96 alcohol‐dependent tobacco smokers (≥ 15 cpd) 75% men, av. age 45, av. cpd 25, motivated to quit, av. FTND 6, 31% veterans |
|
| Interventions | 1. Nicotine patch (titrated, 21 mg/d for 8 wks, 14 mg/d for 2 wks, 7 mg/d for 2 wks) + nicotine gum (2 mg for 24 wks, ad lib but advised 6 ‐ 20/day) 2. Nicotine patch + placebo gum (doses as above) |
|
| Outcomes | Continuous abstinence at 12 m (with 30‐day grace period immediately following quit date) Validation: CO < 10 ppm Adverse events: measured at 2 weeks, 3 months and 6 months (gum or placebo gum use continued until 6 months) |
|
| Notes | This study was supported by award number R01 AA011197 and P50 AA1563 from the National Institute on Alcohol Abuse and Alcoholism and by a MIRECC award from the Department of Veterans Affairs Conflicts of interest: JC and KS have worked as promotional speakers for Pfizer |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "urn randomization computer program that balanced the two groups for history of previous substance use treatment, age, sex, baseline drinks/drinking day and baseline cpd." |
| Allocation concealment (selection bias) | Low risk | Randomization procedure required participant characteristics to be provided before allocation assigned |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Quote: "Double blind." "Research assistants who collected these data were blind to medication assignment and did not conduct psychosocial treatments." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 26 dropouts at 12 m included as smokers; all previously verified as having relapsed |
Croghan 2003.
| Methods | Country: USA Recruitment: multicentre community volunteers | |
| Participants | 1384 smokers (≥ 15 cpd) 42% men, av. age 42, av. cpd 26 | |
| Interventions | 1. 15 mg/16‐hour nicotine patch plus 0.5 mg/dose nasal spray, max 5/hr, 40/day, for 6 wks 2. Nicotine nasal spray only 3. Nicotine patch only | |
| Outcomes | PPA at 6 m
Validation: CO Adverse events: measured to 6 months (treatment duration was 6 weeks) |
|
| Notes | This study was supported in part by Public Health Service Grants CA‐25224, CA‐37404, CA63849, CA‐35269, CA‐52352, CA‐37417, CA‐63848, CA‐35195, and CA‐35103 from the National Cancer Institute, Department of Health and Human Services. Medication was provided by McNeil Consumer Products Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomization by Mayo Clinic Co‐ordinating Centre |
| Allocation concealment (selection bias) | Low risk | Quote: "Treatment assignment was carried out using a dynamic allocation procedure" which took account of stratification by gender, cpd, yrs smoking, study site |
| Blinding (performance bias and detection bias) All outcomes | High risk | Open‐label study |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropouts reported in detail. 34% of pts completed study. Losses to follow‐up similar across groups, treated as non‐abstinent |
Cummings 2011.
| Methods | Country: USA Recruitment: from callers to the New York State Smokers’ Quit Line (NYSSQL) between July and October of 2008 |
|
| Participants | 2806 smokers: aged ≥ 18 yrs, ≥ 10 cpd, interested in using nicotine patch to help them stop smoking, no known contra‐indications to the patch, willing to make quit attempt within 2 weeks 44.3% men; av. age: 45 ‐ 54 yrs (mode); av. cpd: 20 ‐ 29 (mode); time to first cigarette: within 5 mins (mode category) |
|
| Interventions | 1. 2 weeks of free nicotine patch treatment provided 2. 4 weeks of free nicotine patch treatment provided 3. 6 weeks of free nicotine patch treatment provided All participants received the quit line’s standard cessation guide, providing tips on quitting smoking, along with information on the benefits of smoking cessation. In addition, all participants received 1 x 10‐ to 15‐minute proactive follow‐up call conducted 2 weeks after initially contacting the quit line. The counselling call was intended to help participants address barriers to quitting and prompt them to use the medications sent to them |
|
| Outcomes | Self‐reported 30‐day PPA at 7‐m follow‐up Other abstinence measures: self‐reported 7‐day PPA at 7 m No biochemical validation Adverse events: not measured |
|
| Notes | Funded by the New York State Department of Health Conflicts of interest: not reported The mean number of patches used was significantly greater in the groups that received more medication (2‐wk group: 13.0; 4‐wk group: 16.3; 6‐wk group: 20.1) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not sufficient information given Quote: “Eligible participants were assigned according to a prerandomized assignment sheet” |
| Allocation concealment (selection bias) | Unclear risk | Not sufficient information given Quote: “Eligible participants were assigned according to a prerandomized assignment sheet” |
| Blinding (performance bias and detection bias) All outcomes | High risk | Quote: “Quit line phone coaches were not aware of the callers’ group assignment.” However participants were not blinded and it is unclear whether abstinence assessors were blind to allocation |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 59.9% of participants responded to the follow‐up survey overall, with a similar response rate between groups – 58% in 2‐week group; 62% in the 4‐week group; 60% in the 6‐week group |
Dale 1995.
| Methods | Country: USA Recruitment: community volunteers and smoking clinic attenders | |
| Participants | 71 smokers stratified according to light, moderate and heavy smoking rates, and motivated to quit 44% men, av. age 48, av. cpd 26 | |
| Interventions | 1. 11 mg/24‐hour nicotine patch 2. 22 mg/24‐hour nicotine patch 3. 44 mg/24‐hour nicotine patch 4. Placebo patch for 1 wk followed by 11 or 22 mg patch for 7 wks Duration of patch use 8 wks | |
| Outcomes | PPA at 12 m
Validation: Blood cotinine Adverse events: measured daily for 6 days post‐ baseline (treatment continued for 6 weeks) |
|
| Notes | This study was supported by Lederie Laboratories, Pearl River, NY. RH, IC and KO have worked on clinical research studies funded in part by Lederle Laboratories, Elan Pharmaceutical Research Corporation, Burroughs‐Wellcome and Kabi Conflicts of interest: RH has received honoraria for educational activities from CibaGeigy Corporation, Marion Merrell Dow, Inc, and McNeil Pharmaceuticals. KO has received honoraria for educational activities from Elan Pharmaceutical Research Corporation |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "subjects ... were randomly assigned" |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Quote: "To blind the subjects, staff, and investigators, each subject simultaneously wore three patches during the 6‐day inpatient phase" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Apart from one light smoker dropping out from 44 mg group for nicotine toxicity in wk 1, apparently no dropouts |
Daughton 1991.
| Methods | Country: USA Recruitment: community volunteers at 2 sites | |
| Participants | 158 smokers (at least 1 pack cpd) 47% men, av. age 42, av. cpd 33 | |
| Interventions | 1. Nicotine patch (15 cm², 4 wks) worn for 16 hrs/day 2. Nicotine patch (15 cm², 4 wks) worn for 24 hrs/day 3. Placebo patch, 4 wks | |
| Outcomes | Sustained abstinence at 6 m
Validation: CO at 2 ‐ 4 wks (none after 4 wks) Adverse events: assessed weekly during treatment (4 weeks) |
|
| Notes | This study was funded by ALZA Corporation, California. Conflicts of interest: 3 of the authors have corporate affiliations or contractual agreements with, or own stock in, ALZA or Merrell Dow |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "All 158 study‐eligible volunteers were randomly assigned" |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Described as Quote: "double‐blind"; "All of the patches were physically identical in appearance". |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Dropouts (if any) not reported; included as treatment failures in our analysis; results presented on an ITT basis |
Dennis 2016.
| Methods | Country: USA Recruitment: from outpatient clinic referrals, and by flyers and letters advertising a study on PTSD and smoking cessation posted in local hospitals |
|
| Participants | 63 smokers: diagnosed with PTSD, age 18 ‐ 70 years, cpd ≥ 10, willing to quit within the following 30 days 46% men, av. age 42, av. cpd 17.7, mean FTND 4.1 |
|
| Interventions | 1. 2 weeks of nicotine patch (preloading) treatment pre‐quit date, followed by 6 weeks of nicotine patch and nicotine gum/lozenge from quit date 2. 2 weeks of placebo patch pre‐quit date, followed by 6 weeks of nicotine patch and nicotine gum/lozenge from quit date Initial patch dose 21 mg/24‐hour – unclear if tapered down and if so at what dose |
|
| Outcomes | 30‐day PPA at 6‐m follow‐up Validation: salivary cotinine (< 10 ng/ml) Adverse events: not measured |
|
| Notes | Participants were compensated up to USD 650 for complete participation The study was funded by the National Institutes of Health (R21CA128965; R01CA037220; R34DA038272), by the Department of Veterans Affairs (VA) Office of Research and Development (ORD) Health Services Research and Development Service (HSR&D; I01HX000132; I01HX001109), and by the VA Mid‐Atlantic Mental Illness Research, Education, and Clinical Center Conflicts of interest: none to declare |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No detail on exactly how participants were randomized Quote: "randomisation to active nicotine patch or placebo patch was stratified by gender and presence of current MDD" |
| Allocation concealment (selection bias) | Low risk | Quote: "patch allocation was concealed by maintaining a list through the pharmacy that was unavailable to study investigators and coordinators" |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Quote: “Participants were randomized…in a double blind fashion.” No detail is given on who was blinded and how exactly this occurred, but the control group received placebo patch rather than no patch |
| Incomplete outcome data (attrition bias) All outcomes | High risk | > 50% participants lost to follow‐up (18/32 in active patch group; 19/31 in placebo patch group), although similar dropout in each group |
Garvey 2000.
| Methods | Country: USA Recruitment: community volunteers | |
| Participants | 608 smokers, aged > 20, smoking > 5 cpd 49% men, av. cpd 23 | |
| Interventions | 1. 4 mg nicotine gum (recommended 9 ‐ 15 pieces), weaning from 2 m 2. 2 mg nicotine gum, use as 1 3. Placebo gum All received brief counselling (5 ‐ 10 mins) at each study visit (1, 7, 14, 30 days, 2, 3, 6, 9, 12 m) | |
| Outcomes | Sustained abstinence at 12 m (relapse defined as 7+ consecutive days or episodes of smoking)
Validation: CO ≤ 8 ppm Adverse events: not measured |
|
| Notes | This study was supported by grants DA06183 and DA10073 from the National Institute on Drug Abuse, and by the Department of Veterans Affairs Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Stratified by dependence level (high/low) and then allocated [Quote]: "using a randomized, double‐blind procedure" |
| Allocation concealment (selection bias) | Unclear risk | No further detail |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Described as double‐blind, but no further information |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Relapsers were included as failures. Dropout rates not reported |
Glavas 2003.
| Methods | Country: Croatia Recruitment: community volunteers | |
| Participants | 160 smokers | |
| Interventions | 1. Nicotine patch, 24‐hour, 25 mg/15 mg/8 mg starting dose depending on baseline cpd. 6 wks 2. Nicotine patch, 24‐hour, 25 mg/15 mg starting dose depending on baseline cpd. 3 wks 3. Placebo patch. 6 wks 4. Placebo patch 3 wks | |
| Outcomes | Abstinence at 6 m after EOT (abstinence defined as ≤ 2 cigs a wk)
Validation: CO < 11 ppm Adverse events: monitored during treatment (3 weeks in 1 group and 6 weeks in another) |
|
| Notes | Study funding information not reported Conflicts of interest: not reported Author supplied additional details in personal communication |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not stated |
| Allocation concealment (selection bias) | Low risk | Quote: "presealed numbered envelopes" |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Quote: "The envelopes were prepared well in advance and the distribution was commissioned to a nurse not taking part in the evaluation process" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not stated |
Goldstein 1989.
| Methods | Country: USA Recruitment: community volunteers | |
| Participants | 89 smokers (excluding 18 early treatment dropouts not included in results) | |
| Interventions | Factorial design of 2 types of group treatment, and 2 schedules for use of nicotine gum. Behaviour therapy arms collapsed 1. Fixed‐schedule nicotine gum (2 mg); 1 piece/hour for 1st wk with tapering over 10 wks 2. Ad lib nicotine gum; to be used when urge to smoke, max 30/day | |
| Outcomes | PPA at 6 m
Validation: Saliva cotinine < 10 ng/ml or CO < 8 ppm for people still using gum Adverse events: not measured |
|
| Notes | Each pt paid USD 130 at start of study, of which they recovered USD 30 for supplying follow‐up information
This study was funded by grant IN‐45Z from the American Cancer Society and by grant HL‐32318 from the National Heart, Lung, and Blood Institute Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not stated |
| Allocation concealment (selection bias) | Unclear risk | Quote: "each subject was assigned" |
| Blinding (performance bias and detection bias) All outcomes | High risk | Not relevant; placebo gum not used |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 18 early dropouts (16.8%) not included. Dropout rate by EOT was 7.9%, by 6 m 3.4%; losses included as failures |
Hall 2009.
| Methods | Country: USA Recruitment: from the general public through advertising, public service announcements and flyers |
|
| Participants | 402 smokers; aged ≥ 50 yrs, ≥ 10 cpd 59.7% men, av. age 56.7 yrs, av, cpd 20.5, mean FTND 4.8, av. years regular smoking 37.8 |
|
| Interventions | Factorial 2x2 design: extended NRT and extended CBT All participants completed a 12‐wk treatment programme that included group counselling, 12 wks of bupropion and 10 wks of nicotine gum (beginning on quit day). Participants were asked to taper their gum use down completely by week 12 1. Standard treatment: Participants received no further treatment after week 12 2. Extended NRT: Participants were provided with another 40 wks of nicotine gum from their quit day (a total of 50 wks of gum treatment). No CBT past 12 wks 3. Extended CBT: Participants received 11 additional CBT sessions between weeks 10 and 52. 10 weeks of NRT 4. Extended NRT & Extended CBT: Participants received an extra 40 wks of nicotine gum and an additional 11 CBT sessions following the planned quit day (total 50 wks gum treatment) |
|
| Outcomes | 7‐day PPA at 52 weeks post‐baseline; biochemically validated (CO ≤ 10 ppm and anatabine/anabasine ≤ 2 mg/ml) Other abstinence measures: 7‐day PPA at 12, 24, 64, 104 weeks post‐baseline; biochemically validated (CO ≤ 10 ppm and anatabine/anabasine ≤ 2 mg/ml) Adverse events: measured to week 104 (treatment was to week 50) |
|
| Notes | Factorial trial: Authors do not appear to have tested for any interaction between the effects of the 2 interventions tested. However, the review team carried out the same analysis, testing for an interaction at the relevant follow‐up point and found no statistically significant interaction. As there was no significant interaction between the 2 treatments tested we combine groups 1 and 3, and groups 2 and 4 for meta‐analysis, so that we could compare 50 wks extended NRT treatment to 10 wks 'standard' NRT treatment Participants were paid USD 25 per completed assessment The study was funded by the National Institute on Drug Abuse (R01 DA02538, K05 DA016752, K23 DA018691 and P50 DA 09253) Conflicts of interest: None |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “…assigned randomly to one of four experimental conditions using a computerized allocation list by the project statistician (Ms Robbins), who had no contact with participants.” |
| Allocation concealment (selection bias) | Low risk | As above, plus the following: Quote: “The assignment of individual participants by subject number was then transmitted electronically to clinical staff.” |
| Blinding (performance bias and detection bias) All outcomes | High risk | No blinding for NRT intervention |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | > 50% followed up by strictest quit time point. Similar follow‐up between groups |
Hays 1999.
| Methods | Country: USA (3 sites) Recruitment: community volunteers | |
| Participants | 958 smokers, > 15 cpd, motivated to quit 50% men, av. age 44, typically smoked 21 ‐ 40 cpd | |
| Interventions | 1. Nicotine patches (22 mg, 24‐hour for 6 wks) purchased by participants, open‐label 2. Nicotine patches (22 mg, 24‐hour for 6 wks) provided, double‐blind 3. Placebo patches provided The intervention replicated an OTC environment, with no counselling intervention and minimal study recording. Weekly visits required for CO measurement and adverse experience recording, but study sites were not in medical centres and there was no advice, counselling or interaction with medical personnel | |
| Outcomes | Abstinence at 6 m (7‐day PPA) Validation: CO ≤ 8 ppmAdverse events: measured for 6 weeks (during the treatment phase). | |
| Notes | Study was supported by Elan Pharmaceutical Research Corp, Gainesville, Ga Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Computer‐generated random schedule" |
| Allocation concealment (selection bias) | Low risk | 2‐stage process. 1. random allocation to 1 of 2 trials, i.e. open‐label pay trial or placebo‐controlled. 2. Those in placebo trial were then assigned Quote: "by means of a computer‐generated code, in blocks of 20" |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Quote: "The randomization code was not revealed to any of the investigators until completion of the study." Packaging identical |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Pts who missed follow‐up visits classified as failures. Dropout rates not reported |
Herrera 1995.
| Methods | Country: Venezuela Recruitment: community volunteers | |
| Participants | 322 smokers > 10 cpd, scoring ≥ 4 on FTND, no serious illness. Only those who were ready to quit after 4 wks of behavioural treatment were randomized 57% men, av. age ˜38, av. cpd 33 for high dependence, 16 for low dependence | |
| Interventions | Low‐dependence smokers (FTND 4 ‐ 6): 1. 2 mg nicotine gum 2. Placebo gum High‐dependence smokers (FTND 7 ‐ 11): 1. 4 mg nicotine gum plus 2. 2 mg nicotine gum Participants also randomized to starting medication with increasing dose for 1 wk before TQD, or to start at full dose on TQD ‐ there was no blinding for this | |
| Outcomes | Sustained abstinence at 2 yrs (1yr also reported)
Validation: expired CO < 6 ppm Adverse events: measured daily during treatment |
|
| Notes | Relapse between 1 and 2 yrs similar between low‐dependence groups. Higher relapse in 4 mg high‐dependence than 2 mg Funding and conflicts of interest not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not stated |
| Allocation concealment (selection bias) | Unclear risk | Stratified on dependency scores, to determine dosage. Then "randomly assigned" |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Described as double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 68 pts dropped out in Phase 1 (wks 1 ‐ 2) and 10 pts in Phase 2 (wks 4 ‐ 6), i.e. before randomization. Dropout rates not reported, but classified as relapsed "and not further analyzed" |
Hilleman 1994.
| Methods | Country: USA Recruitment: community volunteers | |
| Participants | 140 smokers (excluding a buspirone treatment group), smoking > 20 cpd, FTND ≥ 8 45% men, av. age 46, av. cpd 25 ‐ 26 | |
| Interventions | 1. Nicotine patch (21 mg/24‐hour) for 6 wks, no weaning 2. Nicotine patch, 21 mg 4 wks, weaning to 14 mg 4 wks, 7 mg 4 wks | |
| Outcomes | Abstinence at 6 m
Validation: Plasma thiocyanate Adverse events: not measured |
|
| Notes | Funding and conflicts of interest not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "open‐label, randomized" |
| Allocation concealment (selection bias) | Unclear risk | Method not stated |
| Blinding (performance bias and detection bias) All outcomes | High risk | Not relevant |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "The number of patients discontinuing therapy among the three treatment groups was not significantly different"; analyses included all randomized |
Hughes 1990.
| Methods | Country: USA Recruitment: community volunteers | |
| Participants | 78 smokers, motivated to quit 46% men, av. age 34 ‐ 44, av. cpd 24 ‐ 30 | |
| Interventions | 1. Placebo gum 2. 1 mg nicotine gum (unbuffered formula, available dose approx 0.5 mg) 3. 2 mg nicotine gum 4. 4 mg nicotine gum Gum use not recommended for longer than 3 m | |
| Outcomes | Sustained abstinence at 6 m
Validation: Independent observer report Adverse events: measured at 1 week follow‐up (within treatment) using a 13‐item side effects scale. Note none of the side effects included in the scale are cardiovascular |
|
| Notes | This study was supported by Grants DA‐03728 and DA‐04066 and Research Scientist Development Award DA‐00109 (to J.R.H.) from the National Institute on Drug Abuse. Merrell‐Dow Research Institute provided the drug for the study Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Subjects were randomly assigned" |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Quote: "in a double‐blind manner"; participants guessed which group they had been assigned to |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "Subjects unable to be contacted were counted as smokers". Losses not reported |
Hughes 1991.
| Methods | Country: USA Recruitment: primary care patients | |
| Participants | 106 smokers, motivation to quit not required 48% men, av. age 38, av.cpd 26 | |
| Interventions | 1. Free prescription for nicotine gum for up to 6 m 2. Nicotine gum at cost of USD 6/box (96 pieces 2 mg) 3. Nicotine gum at USD 20/box All participants received brief physician advice with 1 follow‐up | |
| Outcomes | Abstinence at 6 m
Validation: observer verification of all 6‐m quitters Adverse events: not measured |
|
| Notes | Tested effect of price on gum use and efficacy. We combined groups 2 and 3 to make 1 purchasing arm in meta‐analysis. Similar quit rates in the 2 combined arms
This study was supported by a grant (DA‐04066) and Research Scientist Development Award (DA‐00109) from the National Institute on Drug Abuse. Merreil‐Dow Research Institute provided nicotine gum Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated |
| Allocation concealment (selection bias) | Low risk | Quote: "Physician opened a sealed envelope" which assigned to a price group |
| Blinding (performance bias and detection bias) All outcomes | High risk | Double‐blind, as described above. But physicians knew how much each pt paid, and therefore which group they were in, so could have managed them differently (Quote: "no anecdotal evidence that this occurred") |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses at 6 m reported; all were counted as failures, but distribution across the groups not reported |
Hughes 1999.
| Methods | Country: USA (12 sites), Australia (1 site) Recruitment: community volunteers and referrals | |
| Participants | 1039 smokers (≥ 30 cpd) who had made a prior quit attempt, motivated to try again 50% men, av. age 43, av. cpd 38 | |
| Interventions | 1. 42 mg nicotine patch (24‐hour, 6 wks + 10 wks tapering) 2. 35 mg nicotine patch 3. 21 mg nicotine patch 4. Placebo patch | |
| Outcomes | Prolonged abstinence at 6 m (from 2 wks post‐quit) verified at each follow‐up visit
(12‐m follow‐up only completed for 11/13 sites)
Validation: CO ≤ 10 ppm Adverse events: measured up to 10 wks and then at 6‐m and 12‐m follow‐up. Note measurement at 12 months only occurred at some sites Treatment duration was to 16 weeks |
|
| Notes | 6‐m abstinence rates used in analyses, since not all centres completed 12‐m follow‐up due to sponsor termination of study. Denominators confirmed by author
This study was funded by ALZA and Hoechst Marion Roussel. The writing of the study was funded by a Research Scientist Development Award DA‐00109 from the National Institute on Drug Abuse Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Subjects were randomly assigned in a double‐blind manner" |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Subjects were randomly assigned in a double‐blind manner" |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Described as "double‐blind" but no further detail |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Early termination by sponsor, resulting in incomplete long‐term follow‐up data collection. Losses were included as failures |
Hughes 2018.
| Methods | Country: USA Recruitment: through internet sites, such as Craigslist, and referral by friends already enrolled |
|
| Participants | 701 smokers: aged ≥ 18 yrs, ≥ 10 cpd for ≥ 1 yr, probably or definitely intend to quit smoking in the next month, no medical caution to use of patch, no use of other nicotine or tobacco products in the last month 43.5% men; av. cpd: 19; FTND: 5.5; av. age started smoking: 17.8; any prior quit attempt: 78% |
|
| Interventions | 1. Participants advised to 'continue' nicotine patch use in the case of a lapse post‐quit day. Those in the 'continue patch' condition were told: “If you smoke after quitting, continue to use the nicotine patches. Wearing the patches will make it easier for you to return to not smoking. We know that using the patches and smoking a few cigarettes is not harmful. So, if you slip and have a cigarette after quitting, return to not smoking as soon as possible, get rid of any cigarettes you may have, and continue to use the nicotine patches. Do you have any questions or concerns about this?” To minimize adverse events participants were also told to only use the patch while smoking if they were smoking ≤ 75% of their baseline number of cpd 2. Participants advised to 'discontinue' nicotine patch use in the case of a lapse post‐quit day. Those in the discontinue patch condition were told: “If you smoke after quitting, take off your patch for the rest of the day. Using the patches while smoking may give you nicotine levels that are too high, and it's not known if patch use while smoking helps smokers quit. So, if you slip and have a cigarette after quitting, return to not smoking as soon as possible, get rid of any cigarettes you may have, but stop using the patch the day you slip, and resume use on future days only if you completely stop smoking again. Do you have any questions or concerns about this?” For both groups counsellors delivered the instructions above at least 8 times throughout the interventions, and patches were provided for 10 weeks post‐quit date. For all participants the behavioural counselling protocol was based on USPHS Clinical Practice Guidelines that emphasize the provision of social support and problem‐solving around high‐risk‐for‐lapse situations. Counselling was delivered in 6 proactive phone calls that occurred 7 and 3 days before, and 2, 7, 14, and 28 days after participants' designated quit date. The first call lasted about 20 mins; subsequent calls were 10 – 15 mins |
|
| Outcomes | Self‐reported 7‐day PPA smoking abstinence at 6 m post‐quit Other abstinence measures: Self‐reported 7‐day PPA at 4 m post‐quit Adverse events: measured to 1 week post‐treatment (12 weeks) |
|
| Notes | The study was funded by the US National Cancer Institute (Grant CA165080) Conflicts of interest: Dr. Hughes has received consulting and speaking fees from several companies that develop or market pharmacological and behavioral treatments for smoking cessation or harm reduction and from several non‐profit organizations that promote tobacco control. He also consults (without payment) to Swedish Match. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “The randomization schedule and implementation of randomization was conducted by a statistician who had no contact with participants” Quote: “Treatment condition was based on a stratified block design using the SAS procedure PLAN” |
| Allocation concealment (selection bias) | Low risk | As above |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Quote: “Neither participants, research assistants, nor counselors were blind to condition”. However, this is a trial of a behavioural instruction so blinding is impossible. Not biochemically validated, and unknown if participants aware of the treatment the other group was receiving, but both groups received the same contact. Quote: “We matched the Continue Patch and Discontinue Patch use messages on length and frequency.” Collection of outcomes (detection bias) was blinded as participants completed a survey through a phone line, entering data using the phone keypad |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 10% across conditions – reported that this did not differ between groups. 34/321 in 'continue' group did not make a quit attempt and 26/345 in 'discontinue' group ‐ similar between groups |
Jorenby 1995.
| Methods | Country: USA Recruitment: community volunteers | |
| Participants | 504 adult smokers (≥ 15 cpd) 47% men, av. age 44, av. cpd ˜27 | |
| Interventions | 1. Nicotine patch 22 mg for 6 wks then 2 wks 11 mg with minimal counselling 2. Same patch, individual counselling 3. Same patch, group counselling 4. 44 mg patch for 4 wks then 2 wks 22 mg then 2 wks 11 mg with minimal counselling 5. Same patch, individual counselling 6. Same patch, group counselling | |
| Outcomes | Abstinence (> 1 wk) at 6 m
Validation: CO < 10 ppm Adverse events: measured weekly for 8 weeks (during treatment) |
|
| Notes | This study was sponsored by a grant from Elan Pharmaceutical Research Corporation, Gainesville, Ga. Drs Jorenby, Smith, Fiore, Lewis, and Baker have worked on clinical research studies funded in part by Alza Corporation; Ciba‐Geigy Corporation; Elan Pharmaceutical Research Corporation; Lederle Laboratories; and Marion Merrell Dow, Inc. Drs Hurt, Croghan, and Hays and Mr Offord have worked on clinical research studies funded in part by Lederle Laboratories, Elan Pharmaceutical Research Corporation, BurroughsWellcome, and Kabi. Dr Fiore has received honoraria for educational activities from Ciba‐Geigy Corporation; Elan Pharmaceutical Research Corporation, Lederle Laboratories Division; Marion Merrell Dow, Inc; and Parke‐Davis Conflicts of interest: Dr Hurt has received honoraria for educational activities from Ciba‐Geigy Corporation, Marion Merrell Dow, Inc, and McNeil Pharmaceuticals. Mr Offord has received honoraria for educational activities from Elan Pharmaceutical Research Corporation. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomly assigned"; "All participants were also randomly assigned to one of the three types of counselling" |
| Allocation concealment (selection bias) | Unclear risk | Quote: "randomly assigned"; "All participants were also randomly assigned to one of the three types of counselling" |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Quote: "in a double‐blind manner" for wks 1 ‐ 4, then open‐label for wks 5 ‐ 8 |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses reported, but included as failures |
Kalman 2006.
| Methods | Country: USA Recruitment: Veterans Admin Medical Centre and community‐based substance abuse treatment facility | |
| Participants | 130 smokers (≥ 20 cpd with history of alcohol dependence and ≥ 2 m abstinence from alcohol and illicit drugs) 84% men, av. age 47, av. cpd 32 | |
| Interventions | Dose response trial 1. Nicotine patch (42 mg (2 x 21 mg)) 4 wks, then tapered for 8 wks 2. Nicotine patch (21 mg and placebo) for 4 wks then same tapering as 1 | |
| Outcomes | Abstinence at 36 wks (26 wks post‐EOT) (7 day PPA)
Validation: CO < 10 ppm Adverse events: measured during treatment (up to 12 weeks post‐quit date) |
|
| Notes | This study was supported by National Institute on Drug Abuse Research Grant R29‐DA11713‐01. GlaxoSmithKline Beecham provided the nicotine
patches for this project Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated. |
| Allocation concealment (selection bias) | Unclear risk | Quote: "pts were randomly assigned". |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | double‐blind for 4 wks, then open‐label dose tapering phase |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 10 dropped out before treatment, and 4 excluded for protocol violation. Analyses were ITT, with dropouts reported and counted as failures |
Killen 1990.
| Methods | Country: USA Recruitment: community volunteers who had abstained from smoking for 48 hrs | |
| Participants | 1218 adult smokers 48% men, av. age 43, av. cpd 25 | |
| Interventions | 1. Nicotine gum (2 mg, 8 wks) ad lib dosing 2. Nicotine gum on a fixed dose 3. Placebo gum 4. No gum Each group was also factorially randomized to 1 of 3 psychological interventions. | |
| Outcomes | PPA at 12 m (7‐day PPA)
Validation: cotinine, except participants who moved away Adverse events: measured weekly for 8 weeks (during treatment) |
|
| Notes | This study was supported by US Public Health Service grant 5 ROI CA38303 from the National Cancer Institute and by the Merrell Dow Research Institute, Cincinnati Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated. |
| Allocation concealment (selection bias) | Unclear risk | Quote: "randomly assigned" |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Quote: "Assignment to gum condition was double‐blind" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 8 deaths removed from final analyses. Pts moving out of the area were removed from the analyses. Unconfirmed claims of abstinence counted as smokers |
Killen 1999.
| Methods | Country: USA Recruitment: community volunteers responding to advertisements ‐ heavy smokers selected from responders | |
| Participants | 408 heavy smokers (> 25 cpd) 59% men, av. age 47, av. cpd 36, modified FTND score 18 | |
| Interventions | 1. 25 mg nicotine patch for 6 wks (16‐hour, no tapering) 2. 15 mg nicotine patch for 6 wks Self‐help treatment manual, short video showing patch use and placement | |
| Outcomes | Sustained abstinence at 12 m (7‐day PPA at both 6 and 12 m)
Validation: Saliva cotinine < 20 ng/ml (not required for 3 individuals not in area) Adverse events: measured at 24 hours, and 1, 2, 4, and 6 weeks (during treatment) |
|
| Notes | 85% of self‐reported quitters provided samples for validation at 12 m This study was funded by the U.S. Public Health Service Grant 1 R01 CA 68968 from the National Cancer Institute. Pharmacia and Upjohn AB (Sweden) provided the nicotine patches Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated. |
| Allocation concealment (selection bias) | Unclear risk | Quote: "Smokers ... were randomized" |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Quote: "Assignment to treatment dose was double‐blind" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Pts leaving the area were excluded from analyses; all other unconfirmed claims of abstinence were counted as failures. Losses fully reported |
Kornitzer 1987.
| Methods | Country: Belgium Recruitment: worksite primary care clinic | |
| Participants | 199 smokers (av cpd 24 ‐ 5) | |
| Interventions | 1. Nicotine gum (4 mg) for at least 3 m 2. Nicotine gum (2 mg) for same time period | |
| Outcomes | PPA at 12 m
Validation: cotinine and carboxyhaemaglobin in a subsample of participants Adverse events: not reported |
|
| Notes | Funding and conflicts of interest not reported | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated |
| Allocation concealment (selection bias) | Unclear risk | Quote: "subjects were randomised" |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Quote: "in a double‐blind way"; blinding was broken at 3 m |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Losses evident in Tables II and IV |
Kornitzer 1995.
| Methods | Country: Belgium Recruitment: worksite volunteers | |
| Participants | 374 healthy smokers (> 10 cpd for > 3 yrs), motivated to quit 61% men, av. age 40, av. cpd 25 | |
| Interventions | 1. Nicotine patch (12 wks 15 mg/16hr, 6 wks 10 mg, 6 wks 5 mg) and nicotine gum (2 mg, as required) 2. Nicotine patch and placebo gum 3. Placebo patch and placebo gum. | |
| Outcomes | Sustained abstinence at 12 m
Validation: CO < 10 ppm Adverse events: measured at each visit during treatment (6 months) |
|
| Notes | This study was supported by Pharmacia Consumer Pharma Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | See below |
| Allocation concealment (selection bias) | Low risk | Quote: "randomized list generated by a computer program". Randomization balanced between companies 2/2/1 |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Quote: "The investigator and the subjects were completely blind concerning treatment". "unblinding was never requested during the whole study" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Withdrawals counted as treatment failures. All analyses conducted on ITT basis. Dropout and withdrawal rates not reported |
Krupski 2016.
| Methods | Country: USA Recruitment: smokers who contacted the New York stop smoking quit line between March 2010 and Oct 2010 |
|
| Participants | 3118 smokers; aged ≥ 18 years, ≥ 20 cpd, 5 or 6 on Heaviness of Smoking Index, interested in using NRT to quit smoking 53% men, mode age range 45 ‐ 54 yrs, av. cpd not available but a large majority smoked > 30 cpd, 88% time to first cigarette < 5 mins |
|
| Interventions | 1. 2‐wk supply of nicotine patches plus 2‐wk supply of nicotine lozenges 2. 2‐wk supply of nicotine patches Advice to wear each patch for 24 hours, and to use lozenges consistently (every 1 ‐ 2 hours while awake) |
|
| Outcomes | Self‐reported 30‐day PPA at 7 m Other abstinence measures: self‐reported 7‐day PPA at 7 months. Validation: none Adverse events: not measured |
|
| Notes | The study was funded by New York State Smokers’ Quitline (NYS Department of Health) & Roswell Park Cancer Institute Cancer Center Support Grant (NCI grant #P30 CA016056) Conflicts of interest: Dr. Cummings provides expert testimony in litigation against cigarette manufacturers, provides consulting advice and has received grants from Pfizer, and previously served as a co‐investigator on a multi‐center trial evaluating a nicotine vaccine from Nabi Biopharmaceuticals. Dr. Mahoney has provided expert testimony in litigation against cigarette manufacturers, has received research grants and speaker fees from Pfizer and served as an investigator on a multi‐center trial evaluating the potential efficacy of a nicotine vaccine for cessation sponsored by Nabi Biopharmaceuticals. Dr. Toll has received a grant from Pfizer for medicine only |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No detail on exactly how the randomization sequence was generated or allocated Quote: "a randomised experimental design" |
| Allocation concealment (selection bias) | Unclear risk | As above |
| Blinding (performance bias and detection bias) All outcomes | High risk | No blinding and no biochemical validation of abstinence |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Only 41.6% of participants were followed up, but loss to follow‐up was similar between groups (903/1557 in group 1 and 917/1561 in group 2) |
Kupecz 1996.
| Methods | Country: USA Recruitment: smokers attending for smoking cessation treatment at the Veterans’ Affairs Medical Center in Denver between September 1992 and March 1993 (following self‐enrolment or referral by physician or nurse) were invited to participate |
|
| Participants | 45 smokers: motivated to quit 94.7% men; av. age: 50.2 yrs; av. FTND: 7; 69% living in a smoking household environment, av. pack/year history: 47.2 yrs |
|
| Interventions | 1. Nicotine patch treatment for 10 weeks (21 mg/day for 6 weeks, then 14 mg/day for 2 weeks, then 7 mg/day for 2 weeks) 2. Nicotine gum: 2 mg pieces (chewed for 20 mins) ad libitum for 12 weeks, then an individualized tapering schedule with the goal of discontinuing therapy within the next 12 weeks All participants began the above treatment on their quit date and attended 4 weekly sessions, which included contract negotiation, positive reinforcement, relaxation exercises, visual imagery, and group support. Following the cessation programme participants attended 7 follow‐up sessions |
|
| Outcomes | PPA (defined as not smoking at time of asking) 52‐wk follow‐up, validated by exhaled CO < 8 ppm Other abstinence measures: PPA at 6, 12 and 26 wks (CO‐validated) Adverse events: recorded at each session or follow‐up. Note follow‐up was to 1 year, and treatment was to 24 weeks |
|
| Notes | ITT numbers are not available. There were 7 dropouts after randomization, but how these were split across study arms is not reported, making it impossible to perform an ITT analysis. There was no response to a request for the numbers randomized Funding and conflicts of interest not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | It appears that treatment (gum or patch) was assigned randomly to the month of recruitment and then all participants recruited in that month received the allotted treatment rather than allocating treatment to individual participants Quote: “A prospective quasi‐experimental design was employed…” Quote: “During this study, patients were assigned to nicotine gum or a nicotine patch on random months.” Quote: “A random number table was used to assign which product would be used. Each month, the nicotine patch or nicotine gum was randomly assigned to participants in that group by blindly selecting the treatment from an envelope that contained both options.” |
| Allocation concealment (selection bias) | Unclear risk | Quote: “Each month, the nicotine patch or nicotine gum was randomly assigned to participants in that group by blindly selecting the treatment from an envelope that contained both options.” It is unclear whether the treatment for that month was selected before or after the participants had been enrolled for the month. If the treatment was allocated pre‐enrolment then this could have influenced allocation of individuals |
| Blinding (performance bias and detection bias) All outcomes | High risk | Not placebo‐controlled; participants were aware which intervention they were receiving |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: “Seven dropped out prior to completing the program” |
Lerman 2004.
| Methods | Country: USA Recruitment: community volunteers and referrals | |
| Participants | 350 smokers (≥ 10 cpd) (includes 51 who withdrew before treatment) 46% men, av. age 46, av. cpd 21 | |
| Interventions | 1. Nicotine patch (21 mg/24‐hour) for 8 wks incl tapering 2. Nicotine nasal spray (8 ‐ 40 doses/day, max 5/hour) for 8 wks, tapering over final 4 wks | |
| Outcomes | PPA at 6 m (Continuous no slips and prolonged lapse‐free unvalidated outcomes also reported)
Validation: CO < 10 ppm Adverse events: measured during counselling sessions during treatment (8 weeks) |
|
| Notes | This study was supported by the Transdisciplinary Tobacco Use Research Center grant P5084718 from the National Cancer Institute and the National Institute on Drug Abuse and Public Health Services Research grant M01‐RR0040 from the National Institutes of Health. Dr. Lerman was supported by the Abramson Cancer Center and Annenberg Public Policy Center. Dr. Benowitz was supported by Public Health Services grants DA02277, DA12393, and CA078703, as well as the University of California, San Francisco, Comprehensive Cancer Center. Nicotine nasal spray (Nicotrol) was provided by Pharmacia and Upjohn, Helsingborg, Sweden. Conflicts of interest: Consultancies: N. Benowitz (GlaxoSmithKline); Grants received: C. Lerman (National Cancer Institute), N. Benowitz (GlaxoSmithKline) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "computer‐generated randomization scheme", stratified by study site |
| Allocation concealment (selection bias) | Low risk | See above |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Open‐label treatment; Outcome assessment Quote: "interviewers were blinded to study group assignment". |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropouts and withdrawals fully tabulated in Fig 1. ITT analyses confined to those known to have received treatment, with dropouts included as treatment failures |
Moolchan 2005.
| Methods | Country: USA Recruitment: community volunteers | |
| Participants | 120 adolescent smokers (age 13 ‐ 17) (≥ 10 cpd), motivated to quit 30% male, av. age 15, av. cpd 19 | |
| Interventions | 1. Nicotine patch (21 mg, or 14 mg for < 20 cpd) for 6 wks +placebo gum 2. Nicotine gum (4 mg, or 2 mg for < 24 cpd) for 6 wks + placebo patch 3. Double placebo | |
| Outcomes | PPA at 6 m
Validation: CO and cotinine Adverse events: measured during treatment visits (treatment length 12 weeks) |
|
| Notes | This study was supported by funds from the National Institute on Drug Abuse, Intramural Research Program. GlaxoSmithKline (Research Triangle Park, NC) provided study medications (21‐ and 14‐mg Nicoderm, 2‐ and 4‐mg Nicorette, and placebo patch and gum) Conflicts of interest: None |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomized ... according to an algorithm held by the National Institute on Drug Abuse Pharmacy, with true replacement of the non‐completers" |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Described as "double‐blind, double‐dummy", but no further information |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up were included as failures for cessation. Losses fully reported |
Paoletti 1996.
| Methods | Country: Italy Recruitment: community volunteers | |
| Participants | 297 smokers (≥ 10 cpd), motivated to quit Stratified according to baseline cotinine levels 60% men, av. age 43, av. cpd 24 in low cotinine group (n = 120), 30 in high group (n = 177) | |
| Interventions | Stratum A (baseline cotinine < 250 ng/ml) 1. Nicotine patch (15 mg/16‐hour, 18 wks incl taper) 2. Placebo patch Stratum B (baseline cotinine > 250 ng/ml) 3. Nicotine patch 15 mg 4. Nicotine patch 25 mg | |
| Outcomes | PPA at 12 m
Validation: CO and plasma cotinine Adverse events: measured at visits. Note participants were only asked about particular symptoms (none of which are cardiac) |
|
| Notes | This study was supported by a grant from Pharmacia. Conflicts of interest: A.C. and F.M. were recipients of a fellowship at the University of Pisa, sponsored by Pharmacia |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomization stratified on plasma cotinine levels. No detail on methods used |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Described as double‐blind. All pts got 2 patches, to ensure maintenance of blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up fully reported |
Piper 2009.
| Methods | Country: USA Participants: community volunteers |
|
| Participants | 1504 smokers motivated to quit 42% men, av. age 45, av. cpd 21.4 |
|
| Interventions | 1. Nicotine lozenge 2 or 4 mg for 12 wks (based on dose‐for‐dependence level as per instructions) 2. Nicotine patch (24‐hour, 21, 14, and 7 mg titrated down over 8‐wk period post‐quit) 3. Bupropion SR (150 mg bid, 1 wk pre‐quit, 8 wks post‐quit) 4. Lozenge + patch (duration and dosage as above) 5. Bupropion + lozenge (duration and dosage as above) 6. Placebo (5 groups matched to above 5 interventions) |
|
| Outcomes | 7‐day PPA at 6 m; initial cessation Validation: CO < 10 ppm Adverse events: measured at study visits during treatment (8 weeks) |
|
| Notes | Analyses conducted using ITT This study was supported by grant P50 DA019706 from the National Institute on Drug Abuse and by grant M01 RR03186 from the General Clinical Research Centers Program of the National Center for Research Resources. Dr Piper was supported by an Institutional Clinical and Translational Science Award, University of Wisconsin–Madison (KL2 grant 1KL2RR025012‐01). Medication was provided to patients at no cost under a research agreement with GlaxoSmithKline Conflicts of interest: Dr Smith has received research support from Elan Corporation. Dr Baker has served as an investigator on research projects sponsored by pharmaceutical companies, including Sanofi‐Synthelabo, Pfizer Inc, and Nabi Biopharmaceuticals. Dr Jorenby has received research support from the National Institute on Drug Abuse, the National Cancer Institute, Pfizer Inc, Sanofi‐Synthelabo, and Nabi Biopharmaceuticals. He has received support for educational activities from the National Institute on Drug Abuse and the Veterans Administration and consulting fees from Nabi Biopharmaceuticals. Dr Fiore has received honoraria from Pfizer. He has served as an investigator on research studies at the University of Wisconsin that were funded by Pfizer, SanofiSynthelabo, GlaxoSmithKlein, and Nabi Biopharmaceuticals. In 1998, the University of Wisconsin appointed Dr Fiore to a named chair funded by an unrestricted gift to University of Wisconsin from Glaxo Wellcome |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Randomization was double‐blind and used a block randomization scheme with sex and self‐reported race as the blocking variables." |
| Allocation concealment (selection bias) | Low risk | Quote: "Staff did not know to which type(s) of medication a participant would be assigned until the moment of randomization, and study staff were blinded to whether the medication was active or placebo." |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Quote: "Double blind." Quote: "Study staff were blinded to whether the medication was active or placebo" (Type of medication (i.e. patch, gum, pill) would have been apparent to both groups). |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 90 dropouts (out of 1504). Analyses conducted using ITT. Individuals with missing data considered to be smoking |
Piper 2016.
| Methods | Country: USA Recruitment: smokers attending primary care clinics were invited to participate in a research programme to help them quit smoking |
|
| Participants | 637 smokers; aged ≥ 18 years, ≥ 5 cpd for 6 m, motivated to quit 45.4% men, av. age 45.8 yrs, av. cpd 17.7, mean FTND 4.8, baseline CO 20.3ppm, HSI 3.1 |
|
| Interventions | 2 x 2 x 2 x 2 x 2 x 2 factorial design. There were 6 intervention components tested (detailed below) that were tested in different combinations resulting in 32 study groups 1. Nicotine patches for 3 wks prior to quit date (patch preloading) vs no preloading patches 2. Nicotine gum for 3 wks prior to quit date (gum preloading) vs no preloading gum 3. Preparation counselling vs no preparation counselling 4. Intensive cessation in‐person counselling vs minimal in‐person counselling 5. Intensive cessation telephone counselling vs minimal telephone counselling 6. 16w nicotine patch and gum from quit date versus 8 weeks nicotine patch and gum from quit date For the purposes of this review we are interested in comparisons 1, 2 and 6 |
|
| Outcomes | Self‐reported 7‐day PPA at 6 m post‐quit date Self‐reported 7‐day PPA at 16 wks post‐quit date Validation: none Adverse events: measured in visits at wks ‐1 and 4, and in calls at wks 8, 16, and 26 |
|
| Notes | This study had a factorial design, and an interaction between interventions was detected. However results of a regression accounting for this have been presented in the publication and authors supplied group‐by‐group data. We checked to see if the odds ratios generated from these raw data were significantly, clinically different from those generated for the model adjusting for interactions in the paper, for comparisons 1, 2 and 6. Odds ratios were similar in all cases, and in all cases CIs indicated statistically non‐significant results. We have therefore entered raw data, supplied by authors, into meta‐analyses. This results in wider confidence intervals than the models accounting for interactions, but does not affect interpretation. The study was funded by grants 9P50CA143188 and 1K05CA139871 from the National Cancer Institute Conflicts of interest: The authors have received no direct or indirect funding from, nor do they have a connection with, the tobacco, alcohol, pharmaceutical or gaming industries or anybody substantially funded by one of these organizations. W.‐Y.L. is partially supported by a grant from Eli Lilly and Company for research that is unrelated to smoking or tobacco dependence treatment. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “Participants were randomized to treatment conditions via a database that used stratified permuted block randomization” |
| Allocation concealment (selection bias) | Low risk | Quote: “Staff were blinded to randomization until eligibility was confirmed; participants were blinded until consent was provided.” |
| Blinding (performance bias and detection bias) All outcomes | High risk | No placebos. Quote: “assessed by staff who were not involved in treatment, but were not blind to treatment assignment” |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Loss to follow‐up < 50% overall (263/637), and similar for each of 6 study comparisons |
Preloading Investigators 2018.
| Methods | Country: UK Recruitment: by GP surgeries and an NHS smoking cessation clinic |
|
| Participants | 1792 smokers: aged ≥ 18 years, motivated to quit, suitable for nicotine preloading treatment (evidenced by an addiction to smoking) 52.6% men, av. age 48.9, av. cpd 18.9, mean FTND 5.2, mean CO 23.7 ppm, mean longest previous abstinence 400.3 days, cessation support in last 6 months 32.5% |
|
| Interventions | 1. Nicotine patch for 4 weeks before quit date (nicotine preloading) 2. No nicotine patch before quit date All participants received usual care from stop‐smoking services, including pharmacotherapy, beginning 1 ‐ 2 weeks before their quit date |
|
| Outcomes | Prolonged abstinence at 12 months post‐quit, biochemically validated (CO < 10 ppm ‐ salivary cotinine or anabasine were measured instead in a minority of cases, where participants could not attend in person for validation) Other abstinence measures: 7‐day PPA at 4 wks, 6 m and 12 m Prolonged abstinence at 4 wks and 6 m Adverse events: measured to 1 week post‐quit (1 week post‐cessation of preloading) |
|
| Notes | Participants received payment for travel and inconvenience at 1 week, 6‐month and 12‐month follow‐up The study was funded by the NIHR, Health Technology Assessment programme 09/110/01. The nicotine patches for pre‐quit treatment were provided free of charge by GSK Conflicts of interest: Paul Aveyard is an NIHR senior investigator and is funded by NIHR Biomedical Research Centre and CLAHRC, Oxford. Peter Hajek and Hayden McRobbie have done consultancy for manufacturers of smoking cessation treatments and investigator‐initiated research funded by a manufacturer of smoking cessation medication. No authors have financial relationships with any organisation that may have a financial interest in the submitted work in the previous three years and no relationships or activities that could have influenced the submitted work. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “An independent statistician used Stata to generate a randomisation list…” Quote: "Participants shall be randomized to a treatment arm at their baseline visit. They will be randomized to the intervention or control (1:1 ratio) on the basis of a computer‐generated allocation sequence via the internet, with telephone backup, which will be provided by our electronic Primary Care Research Network (ePCRN)." Quote: "For very rare occasions when access to the network, and therefore database randomization is not available, we will have a backup process involving sequentially numbered, opaque, sealed envelopes for randomization." |
| Allocation concealment (selection bias) | Low risk | As above |
| Blinding (performance bias and detection bias) All outcomes | High risk | No blinding Quote: “open label trial so participants, research staff, and NHS Stop Smoking Service personnel knew the arm to which participants were assigned.” Due to UK clinical guidelines in place at the time of the study stop smoking services were less likely to prescribe varenicline to people in the intervention arm post‐quit than the control arm. Authors tested whether this difference between trial arms affected the study effect size and found that it did. As we have used raw data for our NRT preloading meta‐analysis and cannot control for this, we deem this to be a high bias risk Groups received different common behavioural support initially. However, the behavioural support in the control arm was designed to reduce bias by offering the same intensity of support in the absence of a placebo. It is not possible to know whether this behavioural support was suitably matched, and therefore whether it was successful in minimizing bias |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | > 50% followed up at strictest quit time point. Similar attrition between groups (210/899 in group 1 (preloading) and 193/893 in group 2) |
Puska 1995.
| Methods | Country: Finland Recruitment: community volunteers | |
| Participants | 300 volunteers aged 20 ‐ 65, smoking > 10 cpd for > 3 yrs, no serious illness | |
| Interventions | 1. Nicotine patch (15 mg/16‐hours, 12 wks + 6 wks taper) plus nicotine gum (2 mg at least 4 daily) 2. Placebo patch plus nicotine gum (same regimen) | |
| Outcomes | Sustained abstinence at 12 m
Validation: expired CO < 10 ppm Adverse events: measured at all study visits during treatment (treatment length 52 wks) |
|
| Notes | Funding and conflicts of interest not reported. However, 2 authors are affiliated with Pharmacia Consumer Pharma, Department of Clinical Research | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "The subjects were randomly allocated" |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Quote: "The study was carried out in a strictly double blind fashion" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up fully reported |
Rey 2009.
| Methods | Country: Switzerland Recruitment: from smokers attending an academic outpatients clinic (Department of Ambulatory Care and Community Medicine) in Western Switzerland (Lausanne) |
|
| Participants | 50 smokers: highly dependent on smoking, defined as smoking ≥ 20 cpd and/or within 30 mins of waking 72% men; av. age: 40.5 yrs; av. cpd: 29.9; av. exhaled CO: 41.5 ppm; av. years of consumption: 20.5 yrs; av. previous quit attempts: 2.7 |
|
| Interventions | 1. Nicotine nasal spray ‐ advice to use spray when a craving appeared, but to also ensure using 2 puffs an hour 2. Nicotine nasal spray ‐ advice to use spray when craving appeared only Both groups advised to use spray for 2 months from quit date and reduce use in the second month if tolerable |
|
| Outcomes | Continuous smoking abstinence at 6 m follow‐up (defined as from the beginning of nasal spray use to the end of the 6th month, occasional slips < 1 cpd tolerated) Valudation: CO ≤ 10 ppm Adverse events: not measured |
|
| Notes | Despite differing usage instructions, study arms used similar amounts of the spray: group 1 used the spray an average of 2.6 (95% C −2.7 to 7.9) more doses/day compared to group 2 Pharmacia, Switzerland provided free NNS to the participants. They were not involved in data collection, the analysis of the results, in writing or correcting the manuscript, or in deciding whether the paper should be published or not. No further information provided on study funding Conflicts of interest: None |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Prior to data collection, a pharmacist prepared a randomization list of 50 blinded shuffled paper slips including 25 As and 25 Bs which were used to assign patients to treatment groups. Each paper slip was sealed in an opaque numbered envelope. Once a patient was included in the study and baseline data was collected, the sealed envelope was opened by the investigator to reveal the patient's allocation." |
| Allocation concealment (selection bias) | Low risk | As above |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Investigators employed as much blinding as was feasible Quote: "patients were blinded to the other intervention but were aware of their own. Investigator could not be blinded, as he was to give instructions on the use of NNS. During follow‐up, the research nurse was not expressively made aware of the allocation but made all patients aware of the importance of using the spray when craving appeared. Statistician was blinded to which group received which intervention until the end of the analysis." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 24/25 participants followed up in group 1 and 25/25 in group 2. Attrition < 50% and similar in both groups |
Rose 1994.
| Methods | Country: USA Recruitment: community volunteers | |
| Participants | 48 smokers (≥ 20 cpd) 40% men, av. age 34, av. cpd 27 ‐ 29 | |
| Interventions | 2 x 2 factorial trial. Mecamylamine arms collapsed 1. Nicotine patch (21 mg/24‐hour for 2 wks before TQD) 2. Placebo After TQD both groups received active patch for 6 wks, counselling at clinic visits and self‐help materials | |
| Outcomes | Sustained abstinence at 12 m
Validation: CO ≤ 8 ppm Adverse events: measured at visits until 1 week post‐treatment |
|
| Notes | This study was supported by grant PBR‐61 from the American Cancer Society (Atlanta, Ga.); by grant DA 02665 from the National Institute on Drug Abuse (Rockville, Md.), and by the Medical Research Service of the Department of Veterans Affairs (Washington, D.C.) Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated. |
| Allocation concealment (selection bias) | Unclear risk | Not stated. |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Assessment of blinding indicated higher‐than‐chance participant awareness of treatment regimen |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropout rate reported (low) |
Rose 1998.
| Methods | Country: USA Recruitment: community volunteers | |
| Participants | 80 smokers (≥ 20 cpd) 51% men, av. age 41, av. cpd 30 | |
| Interventions | 2 x 2 factorial trial. Mecamylamine pretreatment arms collapsed 1. Nicotine patch (21 mg/24‐hour for 4 wks before TQD) 2. Placebo After TQD both groups received active patch and mecamylamine for 6 wks, counselling at clinic visits and self‐help materials | |
| Outcomes | Sustained abstinence at 6 m
Validation: CO ≤ 8 ppm Adverse events: measured at visits during treatment |
|
| Notes | This study was supported by Grant PBR‐61 from the American Cancer Society and conducted with the assistance of the Medical Research Service of the Department of Veterans Affairs Conflicts of interest: Jed E. Rose is a patent holder of the nicotine—mecamylamine combination treatment tested in this study |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "participants were randomly assigned" |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding (performance bias and detection bias) All outcomes | High risk | Placebo patches not used, but pts were blinded to mecamylamine |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Early dropouts (up to 4 wks pre‐cessation) reported, but not long‐term |
Rose 2006.
| Methods | Country: USA Recruitment: community volunteers | |
| Participants | 96 smokers (≥ 20 cpd), motivated to quit 47% men, av. age 45, av. cpd 29 | |
| Interventions | 2 x 3 x 3 factorial trial ‐ only pre‐cessation patch condition contributes to MA, other conditions collapsed 1. Nicotine patch (21 mg/24‐hour for 2 wks before TQD) 2. Placebo All participants received mecamylamine 2.5 mg twice a day for 4 wks post‐TQD, and either 0, 21 or 42 mg patch | |
| Outcomes | PPA at 6 m
Validation: CO ≤ 8 ppm Adverse events: not measured |
|
| Notes | Post‐quit conditions did not affect cessation, data not reported in paper
This study was supported by grant DA 02665 from the National Institute on Drug Abuse Conflicts of interest: Dr. Rose is an inventor named on several patent applications dealing with nicotine skin patch and combination nicotine/mecamylamine treatment, and receives royalties from sales of certain nicotine patches. Dr. Rose receives research funding from Phillip Morris USA, Inc. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Patch assignment was blinded, but not cigarette type. After quit date, all pts received mecamylamine |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 8.3% of pts dropped out before TQD, and were excluded from analyses |
Rose 2009.
| Methods | Country: USA Recruitment: community volunteers |
|
| Participants | 379 participants, smoking > 15 cpd for ≥ 3 yrs, motivated to quit 43% men, av. age 42, av. cpd 23, av. FTND 6 |
|
| Interventions | 1. Usual brand of cig + 21 mg/24‐hour patch for 2 wks pre‐quit 2. Usual brand of cig + placebo patch for 2 wks pre‐quit 3. Low tar and nic cig + 21 mg/24‐hour patch for 2 wks pre‐quit 4. Low tar and nic cig + placebo patch for 2 wks pre‐quit All groups received same treatment post‐quit: 6 wks 21 mg/24‐hour, following 2 wks 14 mg/24‐hour, remaining 2 wks 7 mg/24‐hour |
|
| Outcomes | Continuous abstinence at 6 m Validation: CO ≤ 8 ppm Adverse events: not measured |
|
| Notes | Treatment had greater effect for those with low FTND Funding provided through grant to Duke University by Philip Morris, USA Conflicts of interest: Dr. Rose has received royalties from sales of certain nicotine patches and is named as inventor on nicotine skin patch patents that expired in 2008. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "a total of 400 subjects were randomly assigned to one of four treatment groups" |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Quote: "two members of the study team…placed the required number of active or placebo patches into individual plastic bags labelled with subject number and session number… In order to maintain blinding, these members of the study team did not interact with study participants." |
| Incomplete outcome data (attrition bias) All outcomes | High risk | High number lost to follow‐up (169/379) |
Rose 2010.
| Methods | Country: USA Recruitment: community volunteers |
|
| Participants | 479 smokers of ≥ 10 cpd, motivated to quit 43% men, av. age 44, av. cpd 24 |
|
| Interventions | 1. Nicotine patch, 21 mg group: wks 1 ‐ 7 21 mg/24‐hour (1 active 21 mg/24‐hour patch, 1 placebo patch) 2. Nicotine patch, 42 mg group: wks 1 ‐ 7 42 mg/24‐hour (2 active 21 mg/24‐hour patches) TQD set at 2 wks. Wks 7 ‐ 12: all participants receive same NRT dose (wks 7 ‐ 8 21 mg/24‐hour, wks 9 ‐ 10 14 mg/24‐hour, wks 11 ‐ 12 7 mg/24‐hour) All participants provided with denicotinized cigarettes during 2‐wk pre‐cessation period to minimize adverse effects of high dose NRT |
|
| Outcomes | PPA at 6 m Validation: CO ≤ 10 ppm Adverse events: measured during treatment (treatment length 12 weeks) |
|
| Notes | Primarily a study of effects of genotype on smoking cessation Number of successful quitters at 6m obtained through communication with author Participants with difficulty sleeping instructed to remove patch at bedtime and apply new ones when they awoke. Participants with other symptoms of nicotine toxicity instructed to reduce dose This study was supported by The National Institutes of Health (NIH)– Intramural Research Program, National Institute on Drug Abuse, Department of Health and Social Services (GR Uhl); a grant to Duke University (Principal Investigator, JE Rose) from Philip Morris USA, Richmond, VA, USA Conflicts of interest: GR Uhl and JE Rose are listed as inventors for a patent application filed by Duke University based on genomic markers that distinguish successful quitters from unsuccessful quitters in data from other clinical trials. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Randomized", but method not specified |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Placebo used, method of blinding not described |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 197 lost to follow‐up before 10 wks (not known how many lost at 6 m); similar numbers across groups; participants lost to follow‐up counted as smokers |
Schlam 2016.
| Methods | Country: USA Recruitment: smokers attending primary care clinics were invited to participate in a research programme to help them quit smoking. Electronic health record technology promoted clinic staff to invite smokers to participate |
|
| Participants | 544 smokers; aged ≥ 18 years, ≥ 5 cpd for 6 months, motivated to quit 41% men, av. age 46.2, av. cpd 18.6, mean FTND 4.9, HSI 3.2, baseline CO 18.5 ppm |
|
| Interventions | 2 x 2 x 2 x 2 x 2 factorial design. There were 5 intervention components tested (detailed below) that were tested in different combinations resulting in 32 study groups 1. Nicotine patches and gum for 8 weeks starting on quit date vs nicotine patches and gum for 26 weeks starting on quit date 2. Maintenance counselling vs no maintenance counselling 3. Medication adherence counselling vs no medication adherence counselling 4. Automated adherence calls vs no adherence calls 5. Helping Hand medication dispenser with feedback and counselling vs no medication dispenser, feedback or related counselling For the purposes of this review we are only interested in comparison 1 |
|
| Outcomes | Self‐reported 7‐day PPA at 52 weeks post‐quit date Validation: none Other abstinence measures: Self‐reported 7‐day PPA at 26 weeks post‐quit date Adverse events; measured at 1, 4 and 8 weeks by completed assessments with case managers (and at 16 weeks if receiving extended medication) Also measured at weeks 16, 26, 39, and 52 during follow‐up calls with assessors |
|
| Notes | The study was funded by grants 9P50CA143188 and 1K05CA139871 from the National Cancer Institute. Conflicts of interest: The authors have received no direct or indirect funding from, nor do they have a connection with, the tobacco, alcohol, pharmaceutical or gaming industries or anybody funded substantially by one of these organizations. W.‐Y.L. is supported partially by a grant from Eli Lilly and Company for research that is unrelated to smoking or tobacco dependence treatment. This study has a factorial design and statistical interactions between factors were reported in the paper. Authors supplied group‐by‐group data. We checked to see if the odds ratios generated from these raw data were significantly, clinically different from those generated for the regression model adjusting for interactions in the paper, for comparison 1. The odds ratios were similar, but the wider confidence intervals generated from the raw data changed the interpretation of the results. The analysis accounting for interactions in the paper resulted in a significant effect of 26‐week gum, but this effect was found to be non‐significant when using raw data from the authors.We therefore have not entered raw data, supplied by authors into any analysis. We have reported this study narratively in the main text. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “Participants were randomized to one of 32 unique experimental conditions… via a database that used stratified, computer‐generated, permuted block randomization…” |
| Allocation concealment (selection bias) | Low risk | Quote: “Staff could not view the allocation sequence. The database did not reveal participants’ treatment condition to staff until participants’ eligibility was confirmed; participants were blinded to treatment condition until they provided consent.” |
| Blinding (performance bias and detection bias) All outcomes | High risk | No placebo used, therefore participants were not blinded to treatment condition. Assessors were not involved in treatment but were not blinded to treatment assignment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Attrition: 127/275 extended NRT, 129/269 standard NRT < 50%, similar in both groups |
Schnoll 2010a.
| Methods | Country: USA Recruitment: community volunteers |
|
| Participants | 575 adult smokers of > 10 cpd for > 1 yr, motivated to quit 53% men, av. age 48, av. cpd 21.1, av. FTND 5.3 |
|
| Interventions | 1. 21 mg/24‐hour patch for 24 wks 2. 21 mg/24‐hour patch for 8 wks, followed by 16 wks placebo patch |
|
| Outcomes | 7‐day PPA at 12 m (also reported for 24 wks) Validation: CO ≤ 10 ppm Adverse events: measured throughout treatment (24 weeks), and also at 52‐week follow‐up |
|
| Notes | This study was supported by a Transdisciplinary Tobacco Use Research Center Grant from the National Cancer Institute and the National Institute on Drug Abuse (P50 CA/DA84718 and P50 CA143187). Conflicts of interest: Dr. Lerman has served as a consultant to GlaxoSmithKline, one company that manufactures the nicotine patch. She has also served as a consultant or has received research funding from AstraZeneca, Pfizer, and Novartis |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "computer‐based randomization table" |
| Allocation concealment (selection bias) | Unclear risk | Not specified. |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Quote: "supply of patches was prepackaged and coded with participant information. The computer program linked the randomization to the patch supply, and only the database manager could link identification with treatment allocation." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropouts included as smokers in outcome data. Similar number of dropouts in both groups |
Schnoll 2010b.
| Methods | Coutry: USA Recruitment: Community volunteers and physician referrals |
|
| Participants | 642 treatment‐seeking smokers smoking ≥ 10 cpd 43% men, av. age 45, av. cpd 20.3, av. FTND 5.1; av. yrs smoking 26.7 |
|
| Interventions | Direct comparison of patch vs lozenge 1. Patch: 21 mg/day for first 6 wks, 14 mg/day for wks 7 + 8, 7 mg/day for wks 9 ‐ 12 2. Lozenge: 4 mg for participants who smoked first cig of day within 30 mins of waking; 2 mg for all other participants. Asked to use 9/day for first 6 wks, 5/day for wks 7 ‐ 9, 3/day for wks 10 ‐ 12 |
|
| Outcomes | 24‐hour PPA at 6 m Validation: CO ≤ 10 ppm Adverse events: measured at end of treatment (12 weeks) and at 6 m follow‐up |
|
| Notes | This study was supported by grant RSGPB‐05‐240‐01‐CPPB to Dr. Schnoll from the American Cancer Society and National Institutes of Health grant U10 101178 to Dr. Paul Engstrom. This work was also supported in part by grants: P50 CA143187, R01 CA126969, R01 DA025078, and R21 DA026889. Conflicts of interest: Dr. Ferris has received grant funding through his institution to conduct research trials for GSK and Novartis during the past 3 years |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Randomization was coordinated by Fox Chase Cancer Center and was stratified at each site." |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding (performance bias and detection bias) All outcomes | High risk | Open‐label trial and although both treatments were active, 2/3 participants had preference for patch |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 46% loss to follow‐up by 6 m, similar between groups. Missing data reported as smokers |
Schnoll 2015.
| Methods | Country: USA Recruitment: through 2 universities, by media advertisements. Eligible participants identified through initial telephone screening and in‐person evaluation |
|
| Participants | 525 smokers; aged ≥ 18 years, ≥ 10 cpd, interested in smoking cessation 49.3% men, av. age 46.4, av. cpd 17.1, mean FTND 5.1 |
|
| Interventions | 1. Nicotine patch (21 mg) for 8 weeks from target quit date 2. Nicotine patch (21 mg) for 24 weeks from target quit date 3. Nicotine patch (21 mg) for 52 weeks from target quit date |
|
| Outcomes | 7‐day PPA at 12 m Other: 7‐day PPA at 24 weeks Validation: expired CO ≤ 10 ppm Adverse events: measured at 4, 12, and 30 weeks |
|
| Notes | Funding by grants R01 DA025078 and R01 DA033681 from the National Institute on Drug Abuse and grants R01 CA165001 and P50 CA143187 from the National Cancer Institute. Conflicts of interest: Drs Schnoll and Hitsman report receiving varenicline (Chantix) and placebo free of charge from Pfizer for use in ongoing National Institutes of Health–supported clinical trials. Dr Schnoll also reports having provided consultation to Pfizer and GlaxoSmithKline. Results for each individual study arm were requested from and shared by the authors |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The statistician (E.P.W.), independently of participants, provided a computerized randomization scheme, which was stratified by site and used permuted blocks of random‐sized numbers" |
| Allocation concealment (selection bias) | Unclear risk | Insufficient information |
| Blinding (performance bias and detection bias) All outcomes | High risk | No blinding |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 40% lost to follow‐up at 12 m (47% in 8‐wk group; 35% in 24‐wk group; 38% in 52‐wk group). Therefore > 50% followed up overall and no large difference (≥ 20%) between groups |
Schuurmans 2004.
| Methods | Country: South Africa Recruitment: community volunteers | |
| Participants | 200 smokers 56% men, av. age 43, av. cpd 23 ‐ 26 | |
| Interventions | 1. Pretreatment with nicotine patch for 2 wks prior to quit date. Then active patch (15 mg) for 12 wks including weaning. 4 sessions of counselling over 10 wks 2. Pretreatment with placebo patch. Then active patch as 1 | |
| Outcomes | Sustained abstinence at 6 m
Validation: CO < 10 ppm at each visit Adverse events: measured at all follow‐up visits to 6 months (treatment duration 12 weeks) |
|
| Notes | This study was supported by a grant from the Swiss Science Foundation (MMS). Conflicts of interest: Pfizer provided medication and support with data analysis. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "a computer‐generated list" |
| Allocation concealment (selection bias) | Low risk | Quote: "Numbering of identical boxes containing patches was carried out prior to the study by a person not involved in the study" |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Quote: "The treatment code was broken only after the last follow‐up visit had been completed and the data recorded" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropouts fully recorded at all stages, ITT analyses used and participants lost to follow‐up counted as smokers |
Smith 2009.
| Methods | Country: USA Recruitment: primary care (12 clinics) |
|
| Participants | 1346 smokers of > 10 cpd for past 6 m 44% men, av. age 44, av. cpd 20.3, motivated to quit |
|
| Interventions | 1. Bupropion only (up‐titrated during wk pre‐quitting, 150 mg twice a day for 8 wks post‐quit) 2. Nicotine lozenge only (4 mg lozenge if first cig of day smoked > 30 mins after waking, 2 mg otherwise. 1 lozenge every 1 ‐ 2 hrs post‐quit wk 1 ‐ 6; 1 lozenge every 2 ‐ 4 hrs wk 7 ‐ 9; 1 lozenge every 4 ‐ 8 hrs wk 10 ‐ 12) 3. Nicotine patch only (21 mg post‐quit wk 1 ‐ 4; 14 mg wk 5 ‐ 6; 7 mg wk 7 ‐ 8) 4. Bupropion and lozenge (dosage as above) 5. Patch and lozenge (dosage as above) |
|
| Outcomes | 7‐day PPA at 6 m and number of days to relapse Validation: none Adverse events: not measured |
|
| Notes | Analyses completed on ITT basis This study was supported by National Institutes of Health grant 5P50DA019706 (Dr Baker) from the National Institute on Drug Abuse and grant 1K05CA139871 (Dr Baker) from the National Cancer Institute. Dr Piper was supported by an Institutional Clinical and Translational Science Award (UW‐Madison; KL2 grant 1KL2RR025012‐01). Medication was provided to patients at no cost under a research agreement with GlaxoSmithKline. Conflicts of interest: Dr Smith has received research support from Elan Corporation plc. Dr Jorenby has received research support from Pfizer Inc, SanofiSynthelabo, and Nabi Biopharmaceuticals and has received consulting fees from Nabi Biopharmaceuticals. Dr Fiore has received honoraria from Pfizer Inc and has served as an investigator on research studies at the University of Wisconsin that were funded by Pfizer Inc, SanofiSynthelabo, and Nabi Biopharmaceuticals. In 1998, the University of Wisconsin (UW) appointed Dr Fiore to a named Chair funded by an unrestricted gift to UW from Glaxo Wellcome. Dr Baker has served as an investigator on research projects sponsored by pharmaceutical companies including Sanofi‐Synthelabo, Pfizer Inc, and Nabi Biopharmaceuticals. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Smokers were randomized to the 5 treatment conditions within each clinic with blocking on sex and self‐identified race." |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding (performance bias and detection bias) All outcomes | High risk | Open‐label |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 158 individuals who did not pick up study medication at first point not included in analyses; 122 withdrawals and 9 deaths considered to be smoking |
Smith 2013.
| Methods | Country: USA Recruitment: callers to Wisconsin Tobacco Quitline from 1 April 2010 to 15 June 2010 |
|
| Participants | 987 smokers; aged ≥ 18 years, ≥ 10 cpd, willing to quit in next 30 days 42.4% men, av. age 41.9, av. cpd 20.7, 85% of participants' time to first cigarette was within 5 mins, mode category for number of previous quit attempts was 2 ‐ 5 |
|
| Interventions | 2 x 2 x 2 factorial design. There were 3 intervention components tested (detailed below) that were tested in different combinations resulting in 8 study groups 1. Nicotine patch vs nicotine patch and nicotine gum 2. Two weeks NRT vs 6 weeks NRT 3. Standard counselling vs medication adherence counselling For the purposes of this review, we are interested in comparisons 1 and 2 |
|
| Outcomes | 30‐day PPA at 6 m follow‐up Other: 7‐day PPA at 6 m follow‐up Validation: none Adverse events: not measured |
|
| Notes | Participants randomized to 6 weeks of NRT were sent an initial shipment of 4 weeks NRT. If they indicated interest in receiving additional NRT during a subsequent call, they were sent an additional 2 weeks supply of NRT Factorial trial. Tests were carried out for interaction effects and none of these were found to be significant. We have therefore combined study arms to provide 2 comparisons (patch vs patch+gum and 2‐wk vs 6‐wk duration) Participants received up to USD 50 for completing follow‐up assessments Study supported by National Cancer Institute grants 1RC1CA144382 and K05CA139871 Conflicts of interest: S.S.S. has served in the past 5 years as a co‐investigator on research studies at the University of Wisconsin–Madison that were funded wholly or in part by GlaxoSmithKline and Pfizer. T.B.B. has served as an investigator in the past 5 years on research studies at the University of Wisconsin– Madison that were funded in part by GlaxoSmithKline. T.B., B.M., and S.M.Z. are employees at Alere Wellbeing and also own stock in Alere Wellbeing (formerly Free & Clear, Inc.), an organization providing quitline services in Wisconsin. T.A.M. was employed by and owned stock in Free & Clear prior to being appointed Director of the Office on Smoking and Health, CDC, in September 2010. He was also an unpaid member of the Board of Directors of the nonprofit North American Quitline Consortium. T.A.M. has no current financial disclosures. M.C.F. has served in the past 5 years as an investigator on research studies at the University of Wisconsin‐Madison that were funded wholly or in part by Pfizer, GlaxoSmithKline, and Nabi. From 1997 to 2010, M.C.F. held a University of Wisconsin named Chair for the Study of Tobacco Dependence, made possible by a gift to the university from GlaxoWellcome. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The 2 × 2 × 2 design yielded eight possible treatment combinations; participants were randomly assigned to the eight treatment combinations via a list of randomized numbers generated by SAS Proc Plan (SAS Institute Inc., Cary, NC)" |
| Allocation concealment (selection bias) | Unclear risk | Quote: "After initial phone screening by quitline registration staff, participants were transferred to a Quit Coach® (trained cessation counselor) at the quitline who completed consent, a baseline survey, enrollment, randomization to treatment, and provision of prequit counseling" |
| Blinding (performance bias and detection bias) All outcomes | High risk | No blinding of participants. Staff collecting outcome data were not affiliated with the quit line, but it is unclear whether they were blind to group allocation |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | > 50% participants followed up at strictest quit time point. Similar follow‐up between arms |
Stapleton 1995.
| Methods | Country: UK Setting: primary care | |
| Participants | 1200 smokers considered by GP to be highly dependent and motivated to give up Av. cpd 23 ‐ 24 |
|
| Interventions | 1. Nicotine patch standard dose (15 mg/16‐hour for 18 wks) 2. Nicotine patch with dose increase to 25 mg at 1 wk if required 3. Placebo patch group The nicotine patch groups were further randomized to gradual tapering or abrupt withdrawal at wk 12 | |
| Outcomes | Sustained abstinence at 12 m
Validation: CO Adverse events: measured at each visit. |
|
| Notes | This study was supported by Kabi Pharmacia AB, Sweden, which also supervised and monitored procedures and data collection in the practices. Medical Research Council and Imperial Cancer Research Fund financially supported the health behaviour unit Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "a computer generated list, complied in blocks of six (four active, two placebo)" |
| Allocation concealment (selection bias) | Low risk | Numbered packages |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Quote: "Both subjects and their doctors or nurses were blind to whether the dose increase was real or placebo". Study conduct throughout was monitored by clinical research associates of the pharmaceutical company |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | ITT analyses, with losses/failures included as smokers. Number of dropouts not specified |
TNSG 1991.
| Methods | Country: USA (9 sites) Recruitment: community volunteers (treated at smoking cessation clinics) | |
| Participants | 808 unselected smokers 40% men, av. age 43, av. cpd 31 | |
| Interventions | 1. Nicotine patch (21 mg /24‐hour, 6 wks+) 2. Nicotine patch 14 mg 3. Placebo patch Abstainers at end of wk 6 entered a randomized blinded trial of weaning | |
| Outcomes | Sustained abstinence at 6 m
Validation: CO < 8 ppm Adverse events: not reported |
|
| Notes | 2 trials pooled and data relating to a 7 mg patch group used in only 1 trial omitted
Long‐term (4 ‐ 5‐yr) follow‐up data reported for 7/9 sites (Daughton 1999). These data are not used in analysis
Study was supported by Alza Corp. Conflicts of interest: Drs Christen, Hatsukami, Rennard, Lichtenstein, Heatley, Repsher, Fortmann, Killen, Hughes, and Glover and Mr Daughton have received fees from Marion Merrell Dow Ine for consultancies and honoraria for educational activities. Authors employed by Marion Merrell Dow Ine (Drs Rolf and Nowak and Messrs Ackerman and Malone) and those employed by Alza Corp (Drs Causey and Knowles and Mss Voss‐Roberts, Prather, Trunnell. and Moos) own shares of company stock. Dr Biglan's spouse owns stock in Alza Corp |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not stated: Quote: "patients were ... randomized", but members of same household received same assignment, with 1 randomly selected for inclusion in the analyses |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Described as double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "All pts were included in outcome evaluations except for the excluded members of couples (49 pts) and nine pts with major protocol infractions". Losses and withdrawals were included as treatment failures |
Tulloch 2016.
| Methods | Country: Canada Recruitment: by advertising (radio, local newspaper and posters), from people presenting to the Quit Smoking programme at the institution, and from referrals by local physicians |
|
| Participants | 737 smokers (490 in relevant trial arms); aged ≥ 18 years, ≥ 10 cpd, willing to make a quit attempt in the next 2 ‐ 4 wks 53.6% men, av. age 48.6, av. cpd 23.2, mean FTND 6.1, av. years smoked 31, av. number of previous quit attempts 4.6 |
|
| Interventions | 1. Nicotine patch for 10 wks beginning on quit day (maximum 21 mg/day or 14 mg/day depending on baseline cpd, decreasing from week 7) 2. Self‐titrated nicotine patch (maximum 35 mg/day) and ad libitum nicotine gum or inhaler for up to 22 wks |
|
| Outcomes | Validated continuous smoking abstinence from week 5 to 52 Other measures: validated 7‐day PPA at 52 wks Validation: expired CO ≤ 9 ppm Adverse events: measured at each appointment (0, 1, 3, 5, 8, 10, 22, 52 wks). Note treatment lasted either 10 or 22 wks, depending on arm |
|
| Notes | Funding from the Heart and Stroke Foundation of Ontario (Grant‐in‐Aid #6614). Conflicts of interest: AP and RR have received research grants from Pfizer. AP and BR have been paid for developing and delivering educational presentations for Pfizer. AP is on the advisory board for Pfizer and Johnson & Johnson. Not included in any meta‐analyses as any comparison would be confounded by other factors |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "After eligibility was confirmed by one of the principal investigators (HT, AP), participants were randomized to receive NRT, NRT+, or VR using a computer‐generated block randomization schedule by a statistical consultant not involved in the trial" |
| Allocation concealment (selection bias) | Low risk | Quote: "After eligibility was confirmed by one of the principal investigators (HT, AP), participants were randomized to receive NRT, NRT+, or VR using a computer‐generated block randomization schedule by a statistical consultant not involved in the trial" |
| Blinding (performance bias and detection bias) All outcomes | High risk | Participants not blinded to treatment condition Quote: “The research coordinator collecting follow‐up data at weeks 22 and 52 was blind to treatment condition.” |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | > 50% followed up at strictest quit time point (152/245 and 171/245). Similar dropout between arms. 15 and 12 participants in the arms of interest were excluded due to death or moving away |
Tønnesen 1988.
| Methods | Country: Denmark Recruitment: primary care | |
| Participants | 113 low‐ to medium‐dependence smokers, motivated to quit (19 or less on Horn‐Russell scale) 44% men, av. age 45, av. cpd 20 60 highly‐dependent smokers 42% men, av. age 45, av. cpd 26 ‐ 28 | |
| Interventions | Group A: Low/medium dependence 1. Nicotine Gum (2 mg) for 16 wks 2. Placebo Group B: High‐dependence 1. Nicotine gum 4 mg for 6 wks then 2 mg 2. Nicotine gum 2 mg | |
| Outcomes | Sustained abstinence at 12 m (24 m also reported)
Validation: CO Adverse events: measured during counselling sessions to end of treatment (either 16 or 20 weeks) |
|
| Notes | This study was supported in part by grant from the Danish National Tuberculosis Foundation. A.B. Leo, Halsingborg, Sweden and H. Lundbeck A.S., Denmark supplied the nicotine and placebo chewing gum Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Pts stratified by dependence, then Quote: "subjects on each list were then randomly assigned to treatment in blocks of two". |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Gum was packaged and produced to be indistinguishable between 2 mg, 4 mg and placebo |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants who attended 1st counselling session were included in analyses, regardless of attendance or level of gum use Only 2/173 were lost to follow‐up |
Tønnesen 1996.
| Methods | Country: Denmark Recruitment: participants who continued to smoke after participation in 2 previous NRT smoking cessation trials were invited to participate |
|
| Participants | 89 smokers: previous failed quit attempts; willing to quit completely 30.3% men; av. age: 49.5; av. cpd: 22; av. FTND: 6.1; salivary cotinine at baseline: 463.5 ng/ml |
|
| Interventions | 1. Nicotine nasal spray: advice to use ad libitum (up to 10 puffs/hour and 80 puffs/day) 2. Nicotine nasal spray: advice to use 1 puff/hour whilst awake Treatment continued for 6 m following quit day, but tapering could be initiated after 3 m |
|
| Outcomes | Continuous smoking abstinence at 12‐m follow‐up (defined as abstinence from week 2 post‐quit day to 12 m follow‐up); CO‐validated (< 10 ppm) other abstinence measures: CO‐validated continuous abstinence at 6 m; CO‐validated abstinence allowing for slips (occasionally smoking between 2 visits) at 6 and 12 m Adverse events: measured up to 6 weeks (participants using treatment at this time) |
|
| Notes | Pharmacia AB Consumer Pharma, Helsingborg, Sweden, sponsored the study and analysis of saliva for cotinine levels Conflicts of interest: Not reported Despite differing dosing instructions between groups: Quote: “Two dosage regimens were used, however, no difference was observed between the fixed and ad libitum dosing group. With a mean daily dose of 16 mg nicotine, most subjects have in fact used the NNS once every hour as prescribed.” |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: “This was an open randomized study with active NNS”. No detail on how randomization achieved |
| Allocation concealment (selection bias) | Unclear risk | As above |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Open‐label design – for this comparison blinding participants was not possible. However, the behavioural support received by the groups was the same and abstinence was biochemically validated, reducing the risk of both performance and detection bias |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Numbers lost to follow‐up not stated (no response to author request for figures) |
Tønnesen 2000.
| Methods | Country: Denmark Recruitment: referrals to lung clinic | |
| Participants | 446 smokers ≥ 10 cpd 48% men, av. age 49, av. cpd 18 | |
| Interventions | 1. 5 mg nicotine patch (placebo) 2. 15 mg (16‐hour) nicotine patch for 12 wks (up to 9 m on request) 3. Nicotine inhaler (4 ‐ 12/day ad lib) 4. Combination, 15 mg patch and inhaler | |
| Outcomes | Sustained abstinence at 12 m, (from wk 2, paper also reports PPA and with slips rates)
Validation: CO < 10 ppm at all visits Adverse events: measured at every follow‐up to 12 m (note treatment could continue to 12 m) |
|
| Notes | This study was supported by a grant from Pharmacia & Upjohn, Helsingborg, Sweden and the Danish Lung Foundation Conflicts of interest: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "a computer‐generated list with random numbers" |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Not used ‐ open‐label trial |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Non‐attenders or lost to follow‐up were included as smokers |
Walker 2011.
| Methods | Country: New Zealand Recruitment: eligible callers to New Zealand's national Quitline July 2007‐ Jan 2009 |
|
| Participants | 1410 smokers; aged ≥ 18 years, smoked first cigarette within 30 mins of waking, wanted to quit in next 2 wks 40% men, av. age 41, av. cpd 20, mean FTND 6.3, partner a current smoker 4.2%, at least 1 quit attempt in last year 29% |
|
| Interventions | 1. Free NRT selection box (including 1 patch, gum, inhaler, sublingual tablets and oral pouches) providing 1‐wk supply in total, followed by 8 wks free, participant‐selected NRT posted to participants 2. Usual quitline care ‐ 2 vouchers (1 sent at baseline and 1 at 4 wks) for 4 wks of subsidized NRT patches or gum to be redeemed at pharmacy |
|
| Outcomes | Validated 7‐day PPA (and not using NRT) at 6 m Other measures: self‐reported continuous abstinence (defined as smoking not more than 5 cigarettes since quit date) at 6 m Validation: salivary cotinine ≤ 10 ng/ml Adverse events: serious adverse events only measured to 6‐m follow‐up (treatment duration 8 weeks) |
|
| Notes | Participants randomized to NRT selection box and 8 wks of preferred NRT were mailed a 4‐wk free supply of their chosen 1 or 2 NRT products after the selection box. They were then offered the option of changing their choice of NRT at a 3‐wk follow‐up call, prior to the second supply of 4 wks free NRT being sent out A very low proportion of participants who claimed to be quit completed verification (34%). We extracted actual verified rates and used these in our main analysis but conducted a sensitivity analysis comparing these figures to data extrapolated from these proportions to the wider trial population, and to non‐verified rates. Results are reported narratively in the text Funding from Health Research Council of New Zealand and the Heart Foundation of New Zealand. NRT was purchased for the intervention arm of the study from Novartis Consumer Health Australasia Pty Ltd (patch and gum), and provided free by Johnson and Johnson Pacific (inhaler and sublingual tablet) and Niconovum (oral pouch) Conflicts of interest: All authors declare that no authors have received support from any companies for the submitted work. C.B. and H.M. have previously undertaken research on behalf of NicoNovum, but prior to the purchase of the company by R.J. Reynolds. H.M. has received honoraria for speaking at research symposia and received benefits in kind and travel support from, and has provided consultancy to the manufacturers of smoking cessation medications. N.W. has provided consultancy to the manufacturers of smoking cessation medications, received honoraria for speaking at a research meeting and received benefits in kind and travel support from a manufacturer of smoking cessation medications. M.G. has provided consultancy to the manufacturers of smoking cessation medications. All authors are currently involved in a trial looking at the effect of reduced nicotine cigarettes on smoking cessation. This trial involves the use of cigarettes which have been purchased from Vector Group Ltd. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “Participants were allocated randomly by computer, with randomization stratified, using minimization, by ethnicity (Māori versus non‐Māori), sex and level of nicotine dependence (>5 points, ≤5 points on the Fagerström score)” |
| Allocation concealment (selection bias) | Low risk | Quote: “Participants were allocated randomly by computer, with randomization stratified, using minimization, by ethnicity (Māori versus non‐Māori), sex and level of nicotine dependence (>5 points, ≤5 points on the Fagerström score)” |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Quote: “Participants were not blinded to treatment allocation”, however blinding of participants would have been impossible. “All research staff involved in outcome assessment were blinded and follow‐up assessments were identical for all participants.” |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Lost to follow‐up or withdrawn: 160/706 intervention group, 144/704 control group. Similar between groups, overall < 50% |
ALA: American Lung Association; av.: average (mean); CBT: cognitive behavioural therapy; CO: carbon monoxide in exhaled air; cpd: cigarettes per day; COPD: chronic obstructive pulmonary disease; EOT: end of treatment; FTND: Fagerström Test for Nicotine Dependence; hr hour; HSI: heaviness of smoking index; ITT: intention‐to‐treat; m: month(s); MA: meta‐analysis; OR: odds ratio; OTC: over‐the‐counter; PPA: point prevalence abstinence; ppm: parts per million; pts: participants; RTQ: reduce‐to‐quit; SC: smoking cessation; TQD: target quit date; wk: week; yr: year
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| ACTRN12612001210864 | All arms received the same NRT and instructions, but some were told that there were benefits of long‐term NRT use. Therefore between‐group differences were purely in the information provided |
| Aubin 2006 | Short‐term experimental cross‐over study of the effect of different types of nicotine patch on sleep and smoking urges. Abstinence not measured and length of follow‐up too short |
| Berlin 2011 | Trial of standard NRT dosing vs dose adaptation according to salivary cotinine. Only followed participants up to 12 weeks |
| Berlin 2012 | Main comparator was the elective MAO‐B inhibitor, EVT 302. Groups receiving NRT received the same dosing and administration across groups |
| Carpenter 2011 | Measured effect of providing NRT samples on participants not initially motivated to quit. Participants were encouraged but not required to make a practice quit attempt. Intervention participants were provided with up to 2 boxes of nicotine lozenges |
| Chan 2010 | Measured effect of counselling + 2 wks free NRT. No data on whether control group also using NRT; unclear if outcome due to counselling or free NRT |
| Dey 1999 | Compared free and paid prescription for nicotine patch. Only 14 wks follow‐up |
| Etter 2009 | Differences in the behavioural intervention (not just NRT) between arms, making it impossible to attribute any effect to use of NRT. For this reason does not meet inclusion criteria. This was included in Stead 2012, but has been removed for this update |
| Fagerström 1993 | Short‐term cross‐over trial. Endpoint withdrawal symptoms not cessation |
| Fagerström 1997 | Short‐term cross‐over trial of different types of NRT. For 2 wks smokers could choose a method, for other 2 they were randomly assigned to 1 of gum, patch, spray, inhaler or tablet. Smoking reduction assessed |
| Fagerström 2000 | Short‐term cross‐over trial comparing 2 nicotine delivery devices |
| Ferguson 2015 | Standard nicotine patch treatment vs pre‐quit patch vs varenicline. Follow‐up less than 6 m (10 weeks) |
| Finland unpublished | Only 3‐m follow‐up. Comparison of patch and nasal spray (n = 51) versus nasal spray alone (n = 50). Sustained abstinence rates 18% in each group. Used in a sensitivity analysis of combination therapies |
| Garvey 2006 | Not enough information currently available (abstract only) |
| Hajek 1999 | Follow‐up < 6 m. There were no significant differences in 12‐wk abstinence rates between gum, patch, spray or inhaler groups |
| Haustein 2003 | Trial of nicotine gum for smoking reduction in people not making a quit attempt. See Cochrane Review of harm reduction interventions (Lindson‐Hawley 2016) |
| Hollands 2013 | Intervention was informing participants that their oral NRT dose was matched to their phenotype vs genotype; NRT dose was actually the same across groups |
| Hughes 1989b | No long‐term follow‐up, primarily a trial of the effect of instructions |
| Hughes 2010 | Differences in the behavioural intervention (not just NRT) between arms, making it impossible to attribute any effect to use of NRT. For this reason does not meet inclusion criteria. This was included in Stead 2012, but has been removed for this update |
| Jibrail 2010 | Only 12 wks follow‐up. Study of NRT for smoking abstinence and relationship between CRP and depressed mood during nicotine abstinence |
| Kozak 1995 | Open‐label study in which smokers with higher nicotine dependence scores were given higher patch doses |
| Kras 2010 | Study of NRT and Hypericum perforatum extract. Only 10 wks follow‐up |
| Landfeldt 1998 | Only 12 wks follow‐up reported in abstract. No evidence of benefit from combining patch and nasal spray compared to nasal spray alone |
| Leischow 1999 | Behavioural support differed between arms, confounding effect of NRT |
| Leischow 2004 | Behavioural support differed between arms, confounding effect of NRT |
| Lu 2017 | Pre‐quit nicotine patch vs standard patch vs varenicline. Follow‐up < 6 m (4 weeks) |
| Marsh 2005 | Only 3 m follow‐up, safety study comparing 4 mg lozenge to 4 mg gum |
| McRobbie 2010 | Short‐term cross‐over study assessing withdrawal symptoms and user satisfaction |
| Minneker 1989 | Only 9 wks follow‐up |
| NCT00985985 | 4‐arm study of 2 mg lozenge versus placebo and 4 mg lozenge versus placebo. However, participants were not randomized to 4 mg or 2 mg lozenge; rather, low‐dependency smokers were allocated to 2 mg lozenge and high‐dependency smokers were allocated to 4 mg lozenge |
| NCT01592695 | Participants received tailored pharmacotherapy in both study arms. The intervention being tested was the type of behavioural support |
| NCT01892813 | Participants received tailored pharmacotherapy in both study arms. The intervention being tested was the type of behavioural support |
| NCT02147132 | Has study arms allowing comparison of standard NRT use and long‐term NRT use; however, only short‐term follow‐up planned (8 weeks) |
| NCT02271919 | Has study arms allowing comparison of combination vs single use NRT; however, only short‐term follow‐up planned (12 weeks) |
| Oncken 2009 | Study of short‐term effects (4 days) of NRT (nicotine patch and nicotine nasal spray) in pregnant smokers |
| Pomerleau 2003 | Compared extended treatment (18 wks) to 10‐wk treatment with nicotine patch. No follow‐up beyond 18 wks |
| Sachs 1995 | Only 6 wks follow‐up |
| Schneider 2004 | Short‐term cross‐over study testing 5 nicotine treatments. Participants used each medication on rising for half a day and resumed smoking each afternoon |
| Schneider 2008 | Outcome was craving and withdrawal, not abstinence |
| Shahab 2011 | Short‐term cross‐over trial of withdrawal symptom relief |
| Shiffman 2000a | Compared 10 and 6 wks of patch treatment without longer follow‐up. Main outcome was craving and withdrawal |
| Shiffman 2000b | Comparison between 24‐hour and 16‐hour patches. Assessment of craving and abstinence over 2 wks |
| Shiffman 2002 | Not a randomized trial. Compared prescription and OTC patch in different populations using different methods |
| Sutherland 1999 | Only 3‐m follow‐up. Comparison of patch and nasal spray (n = 104) versus patch alone (n = 138) or nasal spray alone (n = 138). Used in a sensitivity analysis of combination therapies |
| Tundulawessa 2010 | Only 4 wks follow‐up |
| Vikhireva 2003 | Trial of free choice of NRT product vs assigned NRT product from the outcome; no control group |
| Williams 2007 | Only short‐term outcomes reported in conference abstract. Trial terminated early when no benefit of higher dose detected in interim analysis |
OTC: over the counter; m: month(s); wk: week
Characteristics of ongoing studies [ordered by study ID]
NCT01622998.
| Trial name or title | The self‐directed titrated nicotine patch versus standard treatment for smoking cessation in smokers motivated to quit (STEP) study |
| Methods | Randomized controlled trial Country: Canada Recruitment: from the UOHI Smoking Cessation Clinic and by media advertisements |
| Participants | 303 smokers: ≥ 10 cpd; 18+ years of age; willing to set a date to quit smoking within the 30 days following the baseline assessment |
| Interventions |
All participants receive 5 x 15‐minute counselling sessions from a smoking cessation counsellor. These sessions occur at 1, 3, 5, 8 and 10 wks post‐target quit date. Counselling sessions will focus on practical counselling (problem‐solving and skills training) and social support. Level of support: high (5 counselling sessions) |
| Outcomes | Continuous smoking abstinence at 10, 26 and 52 wks follow‐up 7‐day PPA at 10, 26 and 52 wks follow‐up |
| Starting date | January 2011 |
| Contact information | Andrew Pipe, Chief, Division of Prevention and Rehabilitation, Ottawa Heart Institute Research Corporation |
| Notes | Study completed 2017, but results are not published on clinicaltrials.gov. A conference abstract published in 2017 reporting unrelated outcomes states that "future work will determine if the STEP program was effective in aiding participants in transitioning to cessation at 52‐week follow‐up". This suggests that smoking outcomes may still be awaiting publication. Emailed Dr Pipe to request further information but did not receive a response |
cpd: cigarettes per day; PPA: point prevalence abstinence; wk: week
Contributions of authors
For the most recent version of this review: JHB, NL and SC screened studies. Data extraction and 'Risk of bias' assessment were conducted by SC and WY, with NL checking for discrepancies. TRF advised on statistical considerations. The analyses and review text were updated by NL, JHB, SC and WY, with review and suggestions from all authors.
Sources of support
Internal sources
-
Nuffield Department of Primary Care Health Sciences, University of Oxford, UK.
Editorial base for the Cochrane Tobacco Addiction Group
External sources
-
National Institute for Health Research, UK.
Infrastructure funding for the Cochrane Tobacco Addiction Group
Declarations of interest
CB was involved in two included trials of NRT preloading (Bullen 2010; Walker 2011). CB did not extract the data or conduct 'Risk of bias' assessment for this trial. CB has no known competing interests in relation to the work in question. CB has received honoraria for board memberships, visiting academic work at other universities and consultancy fees for some research projects; however, these are not deemed to result in conflicts with the current work.
JHB: None known.
NL is employed by the University of Oxford to work as a Managing Editor for the Cochrane Tobacco Addiction Review Group. Core infrastructure funding for the Cochrane Tobacco Addiction Group is provided by the NIHR to the University of Oxford. NL was involved in an included trial of NRT preloading (Preloading Investigators 2018). NL did not extract the data or conduct 'Risk of bias' assessment for this trial.
SC: None known.
TRF: None known.
WY: None known.
New
References
References to studies included in this review
Abdullah 2013 {published data only}
- Abdullah AS, Hedley AJ, Chan SS, Lam TH. A randomized controlled trial of two different lengths of nicotine replacement therapy for smoking cessation. BioMed Research International 2013;Epub(961751):1‐9. [DOI: 10.1155/2013/961751] [DOI] [PMC free article] [PubMed] [Google Scholar]
Baker 2016 {published and unpublished data}
- Baker TB, Piper ME, Stein JH. Effects of nicotine patch vs varenicline vs combination nicotine replacement therapy on smoking cessation at 26 weeks: a randomized clinical trial. JAMA 2016;315(4):371‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT01553084. A comparative effectiveness and long term health study in Wisconsin smokers (NHLBI‐RO1). clinicaltrials.gov/ct2/show/study/NCT01553084?view=record (first received 13 March 2012).
Blondal 1999 {published data only}
- Blondal T, Gudmundsson LJ, Olafsdottir I, Gustavsson G, Westin A. Nicotine nasal spray with nicotine patch for smoking cessation: randomised trial with six year follow up. BMJ 1999;318(7179):285‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blondal T, Ludviksdottir D, Gudmundsson L, Olafsdottir I, Gustavsson G, Westin A. Efficacy of nicotine nasal spray added to transdermal nicotine patches in smoking cessation [Abstract]. 10th World Conference on Tobacco or Health; 1997 08 24‐28; Beijing, China. 1997:48.
Bohadana 2000 {published data only}
- Bohadana A, Nilsson F, Rasmussen T, Martinet Y. Gender differences in quit rates following smoking cessation with combination nicotine therapy: influence of baseline smoking behavior. Nicotine & Tobacco Research 2003;5(1):111‐6. [DOI] [PubMed] [Google Scholar]
- Bohadana A, Nilsson F, Rasmussen T, Martinet Y. Nicotine inhaler and nicotine patch as a combination therapy for smoking cessation ‐ A randomized, double‐blind, placebo‐controlled trial. Archives of Internal Medicine 2000;160(20):3128‐34. [DOI] [PubMed] [Google Scholar]
- Bohadana AB, Nilsson F, Martinet Y. Nicotine inhaler and nicotine patch: a combination therapy for smoking cessation. Nicotine & Tobacco Research 1999;1(2):189. [Google Scholar]
Bolin 1999 {published data only}
- Bolin LJ, Antonuccio DO, Follette WC, Krumpe P. Transdermal nicotine: the long and the short of it. Psychology of Addictive Behaviors 1999;13:152‐6. [Google Scholar]
Bolliger 2007 {published data only}
- Bolliger CT, Biljion X, Axelsson A. A nicotine mouth spray for smoking cessation: a pilot study of preference, safety and efficacy. Respiration 2007;74(2):196‐201. [DOI] [PubMed] [Google Scholar]
Bullen 2010 {published data only}
- Bullen C, Howe C, Lin RB, Grigg M, Laugesen M, McRobbie H, et al. Pre‐cessation nicotine replacement therapy: pragmatic randomized trial. Addiction 2010;105(8):1474‐83. [DOI] [PubMed] [Google Scholar]
Burns 2016 {published data only}
- Burns EK, Hood NE, Goforth E, Levinson AH. Randomised trial of two nicotine patch protocols distributed through a state quitline. Tobacco Control 2016;25(2):218‐23. [DOI: 10.1136/tobaccocontrol-2014-051843] [DOI] [PubMed] [Google Scholar]
Caldwell 2014 {published and unpublished data}
- Caldwell BO, Adamson SJ, Crane J. Combination rapid‐acting nicotine mouth spray and nicotine patch therapy in smoking cessation. Nicotine & Tobacco Research 2014;16(10):1356‐64. [DOI: 10.1093/ntr/ntu084] [DOI] [PubMed] [Google Scholar]
Caldwell 2016 {published data only}
- Caldwell BO, Crane J. Combination nicotine metered dose inhaler and nicotine patch for smoking cessation: A randomized controlled trial. Nicotine & Tobacco Research 2016;18(10):1944‐51. [DOI: 10.1093/ntr/ntw093] [DOI] [PubMed] [Google Scholar]
CEASE 1999 {published data only}
- Tønnesen P, Paoletti P, Gustavsson G, Russell MA, Saracci R, Gulsvik A, et al. Higher dosage nicotine patches increase one‐year smoking cessation rates: Results from the European CEASE trial. European Respiratory Journal 1999;13(2):238‐46. [DOI] [PubMed] [Google Scholar]
Cooney 2009 {published data only}
- Cooney NL, Cooney JL, Perry BL, Carbone M, Cohen EH, Steinberg H, et al. Smoking cessation during alcohol treatment: a randomized trial of combination nicotine patch plus nicotine gum. Addiction 2009;104(9):1588‐96. [DOI] [PMC free article] [PubMed] [Google Scholar]
Croghan 2003 {published data only}
- Croghan GA, Hurt RD, Croghan IT, Sloan J, Novotny P, Loprinzi C. Comparison of a 15 mg transdermal nicotine patch alone versus nicotine nasal spray alone versus both for smoking cessation. Journal of Addictive Diseases 1998;17:121. [Google Scholar]
- Croghan GA, Sloan JA, Croghan IT, Novotny P, Hurt RD, DeKrey WL, et al. Comparison of nicotine patch alone versus nicotine nasal spray alone versus a combination for treating smokers: A minimal intervention, randomized multicenter trial in a nonspecialized setting. Nicotine & Tobacco Research 2003;5(2):181‐7. [DOI] [PubMed] [Google Scholar]
Cummings 2011 {published data only}
- Cummings KM, Hyland A, Carlin‐Menter S, Mahoney MC, Willett J, Juster HR. Costs of giving out free nicotine patches through a telephone quit line. Journal of Public Health Management & Practice 2011;17(3):E16‐23. [DOI] [PubMed] [Google Scholar]
Dale 1995 {published data only}
- Dale LC, Hurt RD, Offord KP, Lawson GM, Croghan IT, Schroeder DR. High‐dose nicotine patch therapy ‐ percentage of replacement and smoking cessation. JAMA 1995;274(17):1353‐8. [PubMed] [Google Scholar]
- Dale LC, Schroeder DR, Wolter TD, Croghan IT, Hurt RD, Offord KP. Weight change after smoking cessation using variable doses of transdermal nicotine replacement. Journal of General Internal Medicine 1998;13(1):9‐15. [DOI] [PMC free article] [PubMed] [Google Scholar]
Daughton 1991 {published data only}
- Daughton DM, Heatley SA, Prendergast JJ, Causey D, Knowles M, Rolf CN, et al. Effect of transdermal nicotine delivery as an adjunct to low‐intervention smoking cessation therapy. A randomized, placebo‐controlled, double‐blind study. Archives of Internal Medicine 1991;151(4):749‐52. [PubMed] [Google Scholar]
- Daughton DM, Heatley SA, Prendergast JJ, Causey D, Knowles M, Rolf CN, et al. Effects of transdermal nicotine as an adjunct in smoking cessation therapy. A double‐blind randomized study controlled with placebo [Italian] [Effetti del rilascio transdermico di nicotina come terapia di supporto per lo svezzamento dal fumo di sigaretta. Uno studio randomizzato in doppio cieco con controlli trattati con placebo.]. Archivio Monaldi per le Malattie de Torace 1992;47(1‐6):17‐29. [PubMed] [Google Scholar]
Dennis 2016 {published data only}
- Dennis PA, Kimbrel NA, Dedert EA, Beckham JC, Dennis MF, Calhoun PS. Supplemental nicotine preloading for smoking cessation in posttraumatic stress disorder: Results from a randomized controlled trial. Addictive Behaviors 2016;59:24‐29. [DOI: 10.1016/j.addbeh.2016.03.004] [DOI] [PMC free article] [PubMed] [Google Scholar]
Garvey 2000 {published data only}
- Doherty K, Militello FS, Kinnunen T, Garvey AJ. Nicotine gum dose and weight gain after smoking cessation. Journal of Consulting and Clinical Psychology 1996;64(4):799‐807. [PubMed] [Google Scholar]
- Ferguson SG, Shiffman S, Rohay JM, Gitchell JG, Garvey AJ. Effect of compliance with nicotine gum dosing on weight gained during a quit attempt. Addiction 2011;106(3):651‐6. [DOI] [PubMed] [Google Scholar]
- Garvey AJ, Kinnunen T, Nordstrom BL, Utman CH, Doherty K, Rosner B, et al. Effects of nicotine gum dose by level of nicotine dependence. Nicotine & Tobacco Research 2000;2(1):53‐63. [DOI] [PubMed] [Google Scholar]
- Kinnunen T, Doherty K, Militello FS, Garvey AJ. Depression and smoking cessation ‐ characteristics of depressed smokers and effects of nicotine replacement. Journal of Consulting and Clinical Psychology 1996;64(4):791‐8. [DOI] [PubMed] [Google Scholar]
- Nordstrom BL, Kinnunen T, Utman CH, Garvey AJ. Long‐term effects of nicotine gum on weight gain after smoking cessation. Nicotine & Tobacco Research 1999;1(3):259‐68. [DOI] [PubMed] [Google Scholar]
- Shiffman S, Sembower MA, Rohay JM, Gitchell JG, Garvey AJ. Assigning dose of nicotine gum by time to first cigarette. Nicotine & Tobacco Research 2013;15(2):407‐12. [DOI] [PubMed] [Google Scholar]
Glavas 2003 {published data only}
- Glavas D, Rumboldt Z. Smoking cessation using the transdermal nicotine system [Odvikavanje od pusenja transdermalnim nikotinskim sustavom]. Lijecnicki Vjesnik 2003;125(1‐2):8‐12. [PubMed] [Google Scholar]
Goldstein 1989 {published data only}
- Goldstein MG, Niaura R, Follick MJ, Abrams DB. Effects of behavioral skills training and schedule of nicotine gum administration on smoking cessation. American Journal of Psychiatry 1989;146(1):56‐60. [DOI] [PubMed] [Google Scholar]
Hall 2009 {published data only}
- Barnett PG, Wong W, Jeffers A, Muñoz R, Humfleet G, Hall S. Cost‐effectiveness of extended cessation treatment for older smokers. Addiction 2014;109(2):314‐22. [DOI: 10.1111/add.12404] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grady ES, Humfleet GL, Delucchi KL, Reus VI, Muñoz RF, Hall SM. Smoking cessation outcomes among sexual and gender minority and nonminority smokers in extended smoking treatments. Nicotine & Tobacco Research 2014;16(9):1207‐15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall SM, Humfleet GL, Muñoz RF, Reus VI, Robbins JA, Prochaska JJ. Extended treatment of older cigarette smokers. Addiction 2009;104(6):1043‐52. [DOI: 10.1111/j.1360-0443.2009.02548.x] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hays 1999 {published data only}
- Hays JT, Croghan GA, Offord KP, Wolter TD, Nides MA, Davidson M. Over‐the‐counter (OTC) transdermal nicotine patch therapy. Journal of Addictive Diseases 1997;16:136. [Google Scholar]
- Hays JT, Croghan GA, Schroeder DR, Offord KP, Hurt RD, Wolter TD, et al. Over‐the‐counter nicotine patch therapy for smoking cessation: Results from randomized, double‐blind, placebo‐controlled and open label trials. American Journal of Public Health 1999;89(11):1701‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hays JT, Croghan IT, Offord KP, Hurt RD, Schroeder DR, Wolter TD, et al. Over the counter 22mg nicotine patch therapy for smoking cessation: results from randomized double‐blind placebo‐controlled and open label trials. Society for Research on Nicotine and Tobacco 5th Annual Meeting, 1999, San Diego (CA) 1999. [DOI] [PMC free article] [PubMed]
Herrera 1995 {published data only}
- Herrera N, Franco R, Herrera L, Partidas A, Rolando R, Fagerström KO. Nicotine gum, 2 and 4 mg, for nicotine dependence. A double‐blind placebo‐controlled trial within a behavior modification support program. Chest 1995;108(2):447‐51. [DOI] [PubMed] [Google Scholar]
Hilleman 1994 {published data only}
- Hilleman DE, Mohiuddin SM, Delcore MG. Comparison of fixed‐dose transdermal nicotine, tapered‐dose transdermal nicotine, and buspirone in smoking cessation. Journal of Clinical Pharmacology 1994;34(3):222‐4. [DOI] [PubMed] [Google Scholar]
Hughes 1990 {published data only}
- Hughes JR, Gust SW, Keenan RM, Fenwick JW. Effect of dose on nicotine's reinforcing, withdrawal‐suppression and self‐reported effects. Journal of Pharmacology and Experimental Therapeutics 1990;252(3):1175‐83. [PubMed] [Google Scholar]
Hughes 1991 {published data only}
- Hughes JR, Wadland WC, Fenwick JW, Lewis J, Bickel WK. Effect of cost on the self‐administration and efficacy of nicotine gum: a preliminary study. Preventive Medicine 1991;20(4):486‐96. [DOI] [PubMed] [Google Scholar]
Hughes 1999 {published data only}
- Hughes JR, Lesmes GR, Hatsukami DK, Richmond RL, Lichtenstein E, Jorenby DE, et al. Are higher doses of nicotine replacement more effective for smoking cessation?. Nicotine & Tobacco Research 1999;1(2):169‐74. [DOI] [PubMed] [Google Scholar]
Hughes 2018 {published data only}
- Hughes JR, Solomon LJ, Peasley‐Miklus CE, Callas PW, Fingar JR. Effectiveness of continuing nicotine replacement after a lapse: A randomized trial. Addictive Behaviors 2018;76:68‐81. [DOI: 10.1016/j.addbeh.2017.07.023] [DOI] [PubMed] [Google Scholar]
- NCT01807871. Treatment of Smoking Lapses and Relapses. https://clinicaltrials.gov/ct2/show/NCT01807871 (first posted March 8 2013).
Jorenby 1995 {published data only}
- Jorenby DE, Smith SS, Fiore MC, Hurt RD, Offord KP, Crogham IT, et al. Varying nicotine patch dose and type of smoking cessation counseling. JAMA 1995;274(17):1347‐52. [PubMed] [Google Scholar]
Kalman 2006 {published data only}
- Kalman D, Denison H, Penk W, Peer J, Kresman D, Monti P. Early findings from a treatment study of heavy smokers in alcohol recovery. Society for Research on Nicotine and Tobacco 7th Annual Meeting 2001 03 23‐23; Seattle, Washington. 2001:61. [PO2 34]
- Kalman D, Kahler CW, Garvey AJ, Monti PM. High‐dose nicotine patch therapy for smokers with a history of alcohol dependence: 36‐week outcomes. Journal of Substance Abuse Treatment 2006;30(3):213‐7. [DOI] [PubMed] [Google Scholar]
- Kalman D, Kahler CW, Tirch D, Kaschub C, Penk W, Monti PM. Twelve‐week outcomes from an investigation of high‐dose nicotine patch therapy for heavy smokers with a past history of alcohol dependence. Psychology of Addictive Behaviors 2004;18(1):78‐82. [DOI] [PubMed] [Google Scholar]
- Kalman D, Tirch D, Penk W, Denison H. An investigation of predictors of nicotine abstinence in a smoking cessation treatment study of smokers with a past history of alcohol dependence. Psychology of Addictive Behaviors 2002;16(4):346‐9. [PubMed] [Google Scholar]
- Kalman D, Tirch D, Penk W, Kaschub C. Preliminary findings from a treatment study of heavy smokers in alcohol recovery: end of treatment outcomes (PO2 38). Society for Research on Nicotine and Tobacco 8th Annual Meeting, 2002 02 20‐23; Savannah, Georgia. 2002:58.
Killen 1990 {published data only}
- Fortmann SP, Killen JD, Telch MJ, Newman B. Minimal contact treatment for smoking cessation. A placebo controlled trial of nicotine polacrilex and self‐directed relapse prevention: initial results of the Stanford Stop Smoking Project. JAMA 1988;260(11):1575‐80. [DOI] [PubMed] [Google Scholar]
- Killen JD, Fortmann SP, Newman B, Varady A. Evaluation of a treatment approach combining nicotine gum with self‐guided behavioral treatments for smoking relapse prevention. Journal of Consulting and Clinical Psychology 1990;58(1):85‐92. [DOI] [PubMed] [Google Scholar]
Killen 1999 {published data only}
- Killen JD, Fortmann SP, Davis L, Strausberg L, Varady A. Do heavy smokers benefit from higher dose nicotine patch therapy?. Experimental and Clinical Psychopharmacology 1999;7(3):226‐33. [DOI] [PubMed] [Google Scholar]
Kornitzer 1987 {published data only}
- Kornitzer M, Kittel F, Dramaix M, Bourdoux P. A double blind study of 2 mg versus 4 mg nicotine‐gum in an industrial setting. Journal of Psychosomatic Research 1987;31(2):171‐6. [DOI] [PubMed] [Google Scholar]
Kornitzer 1995 {published data only}
- Kornitzer M, Boutsen M, Dramaix M, Thijs J, Gustavsson G. Combined use of nicotine patch and gum in smoking cessation: a placebo‐controlled clinical trial. Preventive Medicine 1995;24(1):41‐7. [DOI] [PubMed] [Google Scholar]
- Kornitzer M, Boutsen M, Thijs J, Gustavsson G. Efficiency and safety of combined use of nicotine patches and nicotine gum in smoking cessation: a placebo controlled double‐blind trial. European Respiratory Journal 1993;6(Suppl 17):630S. [Google Scholar]
Krupski 2016 {published data only}
- Krupski L, Cummings MK, Hyland A, Mahoney MC, Toll BA, Carpenter MJ, et al. Cost and effectiveness of combination nicotine replacement therapy among heavy smokers contacting a quitline. Journal of Smoking Cessation 2016;11(1):50‐9. [DOI: 10.1017/jsc.2014.15] [DOI] [Google Scholar]
Kupecz 1996 {published data only}
- Kupecz D, Prochazka A. A comparison of nicotine delivery systems in a multimodality smoking cessation program. Nurse Practitioner 1996;21(2):73, 77‐8, 81. [DOI] [PubMed] [Google Scholar]
Lerman 2004 {published data only}
- Lerman C, Jepson C, Wileyto EP, Epstein LH, Rukstalis M, Patterson F, et al. Role of functional genetic variation in the dopamine D2 receptor (DRD2) in response to bupropion and nicotine replacement therapy for tobacco dependence: results of two randomized clinical trials. Neuropsychopharmacology 2006;31(1):231‐42. [DOI] [PubMed] [Google Scholar]
- Lerman C, Kaufmann V, Rukstalis M, Patterson F, Perkins K, Audrain McGovern J, et al. Individualizing nicotine replacement therapy for the treatment of tobacco dependence: a randomized trial. Annals of Internal Medicine 2004;140(6):426‐33. [DOI] [PubMed] [Google Scholar]
- Lerman C, Tyndale R, Patterson F, Wileyto EP, Shields PG, Pinto A, et al. Nicotine metabolite ratio predicts efficacy of transdermal nicotine for smoking cessation. Clinical Pharmacology and Therapeutics 2006;79(6):600‐8. [DOI] [PubMed] [Google Scholar]
- Lerman C, Wileyto EP, Patterson F, Rukstalis M, Audrain‐McGovern J, Restine S, et al. The functional mu opioid receptor (OPRM1) Asn40Asp variant predicts short‐term response to nicotine replacement therapy in a clinical trial. Pharmacogenomics Journal 2004;4(3):184‐92. [DOI] [PubMed] [Google Scholar]
- Malaiyandi V, Lerman C, Benowitz NL, Jepson C, Patterson F, Tyndale RF. Impact of CYP2A6 genotype on pretreatment smoking behaviour and nicotine levels from and usage of nicotine replacement therapy. Molecular Psychiatry 2006;11(4):400‐9. [DOI] [PubMed] [Google Scholar]
- Patterson F, Jepson C, Kaufmann V, Rukstalis M, Audrain‐McGovern J, Kucharski S, et al. Predictors of attendance in a randomized clinical trial of nicotine replacement therapy with behavioral counseling. Drug and Alcohol Dependence 2003;72(2):123‐31. [DOI] [PubMed] [Google Scholar]
Moolchan 2005 {published data only}
- Collins CC, Epstein DH, Parzynski CS, Zimmerman D, Moolchan ET, Heishman SJ. Puffing behavior during the smoking of a single cigarette in tobacco‐dependent adolescents. Nicotine & Tobacco Research 2010;12(2):164‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Franken FH, Pickworth WB, Epstein DH, Moolchan ET. Smoking rates and topography predict adolescent smoking cessation following treatment with nicotine replacement therapy. Cancer Epidemiology, Biomarkers & Prevention 2006;15(1):154‐7. [DOI] [PubMed] [Google Scholar]
- Jaszyna‐Gasior M, Schroeder JR, Thorner ED, Heishman SJ, Collins CC, Lo S, et al. Age at menarche and weight concerns in relation to smoking trajectory and dependence among adolescent girls enrolled in a smoking cessation trial. Addictive Behaviors 2009;34(1):92‐5. [DOI] [PubMed] [Google Scholar]
- Moolchan ET, Robinson ML, Ernst M, Cadet JL, Pickworth WB, Heishman SJ, et al. Safety and efficacy of the nicotine patch and gum for the treatment of adolescent tobacco addiction. Pediatrics 2005;115(4):e407‐e414. [DOI] [PubMed] [Google Scholar]
- Robinson ML, Schroeder JR, Moolchan ET. Adolescent smokers screened for a nicotine replacement treatment trial: Correlates of eligibility and enrollment. Nicotine & Tobacco Research 2006;8(3):447‐54. [DOI] [PubMed] [Google Scholar]
- Thorner‐Bantug E, Jaszyna‐Gasior M, Schroeder JR, Collins CC, Moolchan ET. Weight gain, related concerns, and treatment outcomes among adolescent smokers enrolled in cessation treatment. Journal of the National Medical Association 2009;101(10):1009‐14. [DOI] [PubMed] [Google Scholar]
Paoletti 1996 {published data only}
- Cosci F, Corlando A, Fornai E, Pistelli F, Paoletti P, Carrozzi L. Nicotine dependence, psychological distress and personality traits as possible predictors of smoking cessation. Results of a double‐blind study with nicotine patch. Addictive Behaviors 2009;34(1):28‐35. [DOI] [PubMed] [Google Scholar]
- Fornai E, Desideri M, Pistelli F, Carrozzi L, Puntoni R, Avino S, et al. Smoking reduction in smokers compliant to a smoking cessation trial with nicotine patch. Monaldi Archives for Chest Disease 2001;56(1):5‐10. [PubMed] [Google Scholar]
- Paoletti P, Fornai E, Maggiorelli F, Puntoni R, Viegi G, Carrozzi L, et al. Importance of baseline cotinine plasma values in smoking cessation: results from a double blind study with nicotine patch. European Respiratory Journal 1996;9(4):643‐51. [DOI] [PubMed] [Google Scholar]
Piper 2009 {published data only}
- Asthana A, Johnson HM, Piper ME, Fiore MC, Baker TB, Stein JH. Effects of smoking intensity and cessation on inflammatory markers in a large cohort of active smokers. American Heart Journal 2010;160(3):458‐63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bekiroglu K, Russell MA, Lagoa CM, Lanza ST, Piper ME. Evaluating the effect of smoking cessation treatment on a complex dynamical system. Drug & Alcohol Dependence 2017;180:215‐22. [DOI: 10.1016/j.drugalcdep.2017.07.037] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berg KM, Piper ME, Smith SS, Fiore MC, Jorenby DE. Defining and predicting short‐term alcohol use changes during a smoking cessation attempt. Addictive Behaviors 2015;48:52‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen LS, Bloom AJ, Baker TB, Smith SS, Piper ME, Martinez M, et al. Pharmacotherapy effects on smoking cessation vary with nicotine metabolism gene (CYP2A6). Addiction 2014;109(1):128‐37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cook JW, Lanza ST, Chu W, Baker TB, Piper ME. Anhedonia: its dynamic relations with craving, negative affect, and treatment during a quit smoking attempt. Nicotine & Tobacco Research 2017;19(6):703‐9. [DOI: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cook JW, Piper ME, Leventhal AM, Schlam TR, Fiore MC, Baker TB. Anhedonia as a component of the tobacco withdrawal syndrome. Journal of Abnormal Psychology 2015;124(1):215‐25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Delches JF, Baker TB, Lanza S, Piper ME. Early lapses in a cessation attempt: lapse contexts, cessation success, and predictors of early lapse. Nicotine & Tobacco Research 2013;15(11):1883‐91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gepner AD, Piper ME, Johnson HM, Fiore MC, Baker TB, Stein JH. Effects of smoking and smoking cessation on lipids and lipoproteins: outcomes from a randomized clinical trial. American Heart Journal 2011;161(1):145‐51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Japuntich SJ, Piper ME, Leventhal AM, Bolt DM, Baker TB. The effect of five smoking cessation pharmacotherapies on smoking cessation milestones. Journal of Consulting & Clinical Psychology 2011;79(1):34‐42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson HM, Gossett LK, Piper ME, Aeschlimann SE, Korcarz CE, Baker TB, et al. Effects of smoking and smoking cessation on endothelial function: 1‐year outcomes from a randomized clinical trial. Journal of the American College of Cardiology 2010;55(18):1988‐95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu X, Li R, Lanza ST, Vasilenko SA, Piper M. Understanding the role of cessation fatigue in the smoking cessation process. Drug and Alcohol Dependence 2013;133(2):548–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCarthy DE, Ebssa L, Witkiewitz K, Shiffman S. Paths to tobacco abstinence: A repeated‐measures latent class analysis. Journal of Consulting and Clinical Psychology 2015;83(4):696‐708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piper ME, Cook JW, Schlam TR, Jorenby DE, Baker TB. Anxiety diagnoses in smokers seeking cessation treatment: relations with tobacco dependence, withdrawal, outcome and response to treatment. Addiction 2011;106(2):418‐27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piper ME, Smith SS, Schlam TR, Fiore MC, Jorenby DE, Fraser D, et al. A randomized placebo‐controlled clinical trial of 5 smoking cessation pharmacotherapies. Archives of General Psychiatry 2009;66(11):1253‐62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piper ME, Vasilenko SA, Cook JW, Lanza ST. What a difference a day makes: differences in initial abstinence response during a smoking cessation attempt. Addiction 2016;112(2):330‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith SS, Fiore MC, Baker TB. Smoking cessation in smokers who smoke menthol and non‐menthol cigarettes. Addiction 2014;109(12):2107‐17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vasilenko SA, Piper ME, Lanza ST, Liu X, Yang J, Li R. Time‐varying processes involved in smoking lapse in a randomized trial of smoking cessation therapies. Nicotine & Tobacco Research 2014;16(Suppl 2):S135‐43. [DOI] [PMC free article] [PubMed] [Google Scholar]
Piper 2016 {published data only}
- Piper ME Schlam TR, Cook JW, Smith SS, Bolt DM, Loh WY, et al. Toward precision smoking cessation treatment I: Moderator results from a factorial experiment. Drug and Alcohol Dependence 2017;171:59‐65. [DOI: 10.1016/j.drugalcdep.2016.11.025] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piper ME, Cook JW, Schlam TR, Smith SS, Bolt DM, Collins LM, et al. Toward precision smoking cessation treatment II: Proximal effects of smoking cessation intervention components on putative mechanisms of action. Drug and Alcohol Dependence 2017;171:50‐8. [DOI: 10.1016/j.drugalcdep.2016.11.027] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piper ME, Fiore MC, Smith SS, Fraser D, Bolt DM, Collins LM, et al. Identifying effective intervention components for smoking cessation: a factorial screening experiment. Addiction 2016;111(1):129‐41. [DOI: 10.1111/add.13162] [DOI] [PMC free article] [PubMed] [Google Scholar]
Preloading Investigators 2018 {published data only}
- Lindson‐Hawley N, Coleman T, Docherty G, Hajek P, Lewis S, Lycett D, et al. Nicotine patch preloading for smoking cessation (the preloading trial): Study protocol for a randomized controlled trial. Trials 2014;15(1):1‐18. [DOI: 10.1186/1745-6215-15-296] [DOI] [PMC free article] [PubMed] [Google Scholar]
- The Preloading Investigators. Effects on abstinence of nicotine patch treatment before quitting smoking: parallel, two arm, pragmatic randomised trial. BMJ 2018;361:k2164. [DOI: 10.1136/bmj.k2164] [DOI] [PMC free article] [PubMed] [Google Scholar]
Puska 1995 {published data only}
- Puska P, Korhonen HJ, Vartiainen E, Urjanheimo EL, Gustavsson G, Westin A. Combined use of nicotine patch and gum compared with gum alone in smoking cessation: a clinical trial in North Karelia. Tobacco Control 1995;4:231‐5. [Google Scholar]
Rey 2009 {published data only}
- NCT00861276. Nicotine substitute prescribed at hourly intake or ad libitum for heavy smokers willing to wuit (SUNIC). clinicaltrials.gov/ct2/show/NCT00861276 (first received 13 March 2009).
- Rey L, Vaucher P, Secretan F, Zellweger JP, Bodenmann P. Use of nicotine substitute prescribed at hourly plus ad libitum intake or ad libitum for heavy smokers willing to quit: a randomized controlled trial. Substance Abuse Treatment, Prevention, and Policy 2009;4:12. [DOI] [PMC free article] [PubMed] [Google Scholar]
Rose 1994 {published data only}
- Rose JE, Behm FM, Westman EC, Levin ED, Stein RM, Ripka GV. Mecamylamine combined with nicotine skin patch facilitates smoking cessation beyond nicotine patch treatment alone. Clinical Pharmacology and Therapeutics 1994;56(1):86‐99. [DOI] [PubMed] [Google Scholar]
- Rose JE, Westman EC, Behm FM. Nicotine/mecamylamine combination treatment for smoking cessation [published erratum appears in Drug Development Research 1997;40:215]. Drug Development Research 1996;38:243‐56. [Google Scholar]
Rose 1998 {published data only}
- Rose JE, Behm FM, Westman EC. Nicotine‐mecamylamine treatment for smoking cessation: the role of pre‐cessation therapy. Experimental and Clinical Psychopharmacology 1998;6(3):331‐43. [DOI] [PubMed] [Google Scholar]
- Rose JE, Westman EC, Behm FM. Nicotine/mecamylamine combination treatment for smoking cessation [published erratum appears in Drug Development Research 1997;40:215]. Drug Development Research 1996;38:243‐56. [Google Scholar]
Rose 2006 {published data only}
- Rose JE, Behm FM, Westman EC, Kukovich P. Precessation treatment with nicotine skin patch facilitates smoking cessation. Nicotine & Tobacco Research 2006;8(1):89‐101. [DOI] [PubMed] [Google Scholar]
Rose 2009 {published and unpublished data}
- Rose JE. Nicotine preloading: The importance of a pre‐cessation reduction in smoking behavior. Psychopharmacology 2011;217(3):453‐4. [DOI] [PubMed] [Google Scholar]
- Rose JE, Herskovic JE, Behm FM, Westman EC. Precessation treatment with nicotine patch significantly increases abstinence rates relative to conventional treatment. Nicotine & Tobacco Research 2009;11(9):1067‐75. [DOI] [PubMed] [Google Scholar]
Rose 2010 {published and unpublished data}
- Rose JE. Nicotine preloading: The importance of a pre‐cessation reduction in smoking behavior. Psychopharmacology 2011;217(3):453‐4. [DOI] [PubMed] [Google Scholar]
- Rose JE, Behm FM, Drgon T, Johnson C, Uhl GR. Personalized smoking cessation: interactions between nicotine dose, dependence and quit‐success genotype score. Molecular Medicine 2010;16(7‐8):247‐53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Uhl GR, Drgon T, Johnson C, Ramoni MF, Behm FM, Rose JE. Genome‐wide association for smoking cessation success in a trial of precessation nicotine replacement. Molecular Medicine 2010;16(11‐12):513‐26. [DOI] [PMC free article] [PubMed] [Google Scholar]
Schlam 2016 {published data only}
- Schlam TR, Fiore MC, Smith SS, Fraser D, Bolt DM, Collins LM, et al. Comparative effectiveness of intervention components for producing long‐term abstinence from smoking: a factorial screening experiment. Addiction 2016;111(1):142‐55. [DOI: 10.1111/add.13153] [DOI] [PMC free article] [PubMed] [Google Scholar]
Schnoll 2010a {published data only}
- Lerman C, Jepson C, Wileyto EP, Patterson F, Schnoll R, Mroziewicz M, et al. Genetic variation in nicotine metabolism predicts the efficacy of extended‐duration transdermal nicotine therapy. Clinical Pharmacology and Therapeutics 2010;87(5):553‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schnoll RA, Patterson F, Wileyto EP, Heitjan DF, Shields AE, Asch DA, et al. Effectiveness of extended‐duration transdermal nicotine therapy: a randomized trial. Annals of Internal Medicine 2010;152(3):144‐51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schnoll RA, Wileyto EP, Lerman C. Extended duration therapy with transdermal nicotine may attenuate weight gain following smoking cessation. Addictive Behaviors 2012;37(4):565‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Schnoll 2010b {published data only}
- Schnoll RA, Martinez E, Tatum KL, Glass M, Bernath A, Ferris D, et al. Increased self‐efficacy to quit and perceived control over withdrawal symptoms predict smoking cessation following nicotine dependence treatment. Addictive Behaviors 2011;36(1‐2):144‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schnoll RA, Martinez E, Tatum KL, Glass M, Bernath A, Ferris D, et al. Nicotine patch vs. nicotine lozenge for smoking cessation: an effectiveness trial coordinated by the Community Clinical Oncology Program. Drug and Alcohol Dependence 2010;107(2‐3):237‐43. [DOI] [PMC free article] [PubMed] [Google Scholar]
Schnoll 2015 {published and unpublished data}
- Schnoll RA, Goelz PM, Veluz‐Wilkins A, Blazekovic S, Powers L, Leone FT, et al. Long‐term nicotine replacement therapy: a randomized clinical trial. JAMA Internal Medicine 2015;175(4):504‐11. [DOI: 10.1001/jamainternmed.2014.8313] [DOI] [PMC free article] [PubMed] [Google Scholar]
Schuurmans 2004 {published data only}
- Schuurmans MM, Diacon AH, Biljon X, Bolliger CT. Effect of pre‐treatment with nicotine patch on withdrawal symptoms and abstinence rates in smokers subsequently quitting with the nicotine patch: a randomized controlled trial. Addiction 2004;99(5):634‐40. [DOI] [PubMed] [Google Scholar]
- Schuurmans MM, Diacon AH, Biljon X, Westin A, Landfeldt B, Bolliger CT. Effect of pre‐treatment with nicotine patch on withdrawal symptoms in smokers subsequently quitting with the nicotine patch: a double‐blind randomised controlled trial. European Respiratory Society Annual Congress, Stockholm (www.ersnetsecure.org/public/prg_congres.abstract?ww_i_presentation=6711). 2002.
Smith 2009 {published data only}
- Smith SS, McCarthy DE, Japuntich SJ, Christiansen B, Piper ME, Jorenby DE, et al. Comparative effectiveness of 5 smoking cessation pharmacotherapies in primary care clinics. Archives of Internal Medicine 2009;169(22):2148‐55. [DOI] [PMC free article] [PubMed] [Google Scholar]
Smith 2013 {published data only}
- Smith SS, Keller PA, Kobinsky KH, Baker TB, Fraser DL, Bush T, et al. Enhancing tobacco quitline effectiveness: identifying a superior pharmacotherapy adjuvant. Nicotine & Tobacco Research 2012;15(3):718‐28. [10.1093/ntr/nts186] [DOI] [PMC free article] [PubMed] [Google Scholar]
Stapleton 1995 {published data only}
- Russell MA, Stapleton JA, Feyerabend C, Wiseman SM, Gustavsson G, Sawe U, et al. Targeting heavy smokers in general practice: randomised controlled trial of transdermal nicotine patches. BMJ 1993;306(6888):1308‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stapleton JA, Russell MA, Feyerabend C, Wiseman SM, Gustavsson G, Sawe U, et al. Dose effects and predictors of outcome in a randomized trial of transdermal nicotine patches in general practice. Addiction 1995;90(1):31‐42. [DOI] [PubMed] [Google Scholar]
TNSG 1991 {published data only}
- Daughton DM, Fortmann SP, Glover ED, Hatsukami DK, Heatley SA, Lichtenstein E, et al. The smoking cessation efficacy of varying doses of nicotine patch delivery systems 4 to 5 years post‐quit day. Preventive Medicine 1999;28(2):113‐8. [DOI] [PubMed] [Google Scholar]
- Ferguson SG, Gitchell JG, Shiffman S, Sembower MA. Prediction of abstinence at 10 weeks based on smoking status at 2 weeks during a quit attempt: secondary analysis of two parallel, 10‐week, randomized, double‐blind, placebo‐controlled clinical trials of 21‐mg nicotine patch in adult smokers. Clinical Therapeutics 2009;31(9):1957‐65. [DOI] [PubMed] [Google Scholar]
- Swan GE, Jack LM, Ward MM. Subgroups of smokers with different success rates after use of transdermal nicotine. Addiction 1997;92(2):207‐17. [PubMed] [Google Scholar]
- Transdermal Nicotine Study Group. Transdermal nicotine for smoking cessation. Six‐month results from two multicenter controlled clinical trials. Transdermal Nicotine Study Group. JAMA 1991;266(22):3133‐8. [PubMed] [Google Scholar]
Tulloch 2016 {published data only}
- Tulloch H, Pipe A, Els C, Aitken D, Clyde M, Corran B, Reid RD. Flexible and extended dosing of nicotine replacement therapy or varenicline in comparison to fixed dose nicotine replacement therapy for smoking cessation: Rationale, methods and participant characteristics of the FLEX trial. Contemporary Clinical Trials 2014;38(2):304‐13. [DOI: 10.1016/j.cct.2014.05.011] [DOI] [PubMed] [Google Scholar]
- Tulloch HE, Pipe AL, Clyde MJ, Reid RD, Els C. The quit experience and concerns of smokers with psychiatric illness. American Journal of Preventive Medicine 2016;50(6):709‐18. [DOI: 10.1016/j.amepre.2015.11.006] [DOI] [PubMed] [Google Scholar]
- Tulloch HE, Pipe AL, Els C, Clyde MJ, Reid RD. Flexible, dual‐form nicotine replacement therapy or varenicline in comparison with nicotine patch for smoking cessation: a randomized controlled trial. BMC Medicine 2016;14:80. [DOI: 10.1186/s12916-016-0626-2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Tønnesen 1988 {published data only}
- Tønnesen P, Fryd V, Hansen M, Helsted J, Gunnersen AB, Forchammer H, et al. Effect of nicotine chewing gum in combination with group counseling on the cessation of smoking. New England Journal of Medicine 1988;318(1):15‐8. [DOI] [PubMed] [Google Scholar]
Tønnesen 1996 {published data only}
- Tønnesen P, Mikkelsen K, Norregaard J, Jorgensen S. Recycling of hard‐core smokers with nicotine nasal spray. European Respiratory Journal 1996;9(8):1619‐23. [DOI] [PubMed] [Google Scholar]
Tønnesen 2000 {published data only}
- Tønnesen P, Mikkelsen KL. Smoking cessation with four nicotine replacement regimes in a lung clinic. European Respiratory Journal 2000;16(4):717‐22. [DOI] [PubMed] [Google Scholar]
Walker 2011 {published data only}
- Walker N, Howe C, Bullen C, Grigg M, Glover M, McRobbie H, et al. Does improved access and greater choice of nicotine replacement therapy affect smoking cessation success? Findings from a randomized controlled trial. Addiction 2011;106(6):1176‐85. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
ACTRN12612001210864 {unpublished data only}
- ACTRN12612001210864. Can using nicotine as a long‐term substitute enhance smoking cessation over using it only as a cessation aid? [An open‐label randomised pragmatic policy trial examining effectiveness of short‐term use of Nicotine Replacement Therapy (NRT) vs short‐ or long‐term use of NRT vs short‐ or long‐term use of NRT or electronic nicotine delivery systems for smoking cessation in cigarette smokers]. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?ACTRN=12612001210864 (first received 15 November 2012).
Aubin 2006 {published data only}
- Aubin HJ, Luthringer R, Demazieres A, Dupont C, Lagrue G. Comparison of the effects of a 24‐hour nicotine patch and a 16‐hour nicotine patch on smoking urges and sleep. Nicotine & Tobacco Research 2006;8(2):193‐201. [DOI] [PubMed] [Google Scholar]
Berlin 2011 {published data only}
- Berlin I, Jacob N, Coudert M, Perriot J, Schultz L, Rodon N. Adjustment of nicotine replacement therapies according to saliva cotinine concentration: the ADONIS* trial‐a randomized study in smokers with medical comorbidities. Addiction 2011;106(4):833‐43. [DOI] [PubMed] [Google Scholar]
- Berlin I, Singleton EG, Heishman SJ. Validity of the 12‐item French version of the Tobacco Craving Questionnaire in treatment‐seeking smokers. Nicotine & Tobacco Research 2010;12(5):500‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Berlin 2012 {published data only}
- Berlin I, Hunneyball IM, Greiling D, Jones SP, Fuder H, Stahl HD. A selective reversible monoamine oxidase B inhibitor in smoking cessation: effects on its own and in association with transdermal nicotine patch. Psychopharmacology 2012;223(1):89‐98. [DOI] [PubMed] [Google Scholar]
Carpenter 2011 {published data only}
- Carpenter MJ, Alberg AJ, Gray KM, Saladin ME. Motivating the unmotivated for health behavior change: a randomized trial of cessation induction for smokers. Clinical Trials 2010;7(2):157‐66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carpenter MJ, Hughes JR, Gray KM, Wahlquist AE, Saladin ME, Alberg AJ. Nicotine therapy sampling to induce quit attempts among smokers unmotivated to quit: a randomized clinical trial. Archives of Internal Medicine 2011;171(21):1901‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Chan 2010 {published data only}
- Chan SS, Leung DY, Abdullah AS, Lo SS, Yip AW, Kok WM, et al. Smoking‐cessation and adherence intervention among Chinese patients with erectile dysfunction. American Journal of Preventive Medicine 2010;39(3):251‐8. [DOI] [PubMed] [Google Scholar]
Dey 1999 {published data only}
- Dey P, Foy R, Woodman M, Fullard B, Gibbs A. Should smoking cessation cost a packet? A pilot randomized controlled trial of the cost‐effectiveness of distributing nicotine therapy free of charge. British Journal of General Practice 1999;49(439):127‐8. [PMC free article] [PubMed] [Google Scholar]
Etter 2009 {published data only}
- Etter JF, Huguelet P, Perneger TV, Cornuz J. Nicotine gum treatment before smoking cessation: a randomized trial. Archives of Internal Medicine 2009;169(11):1028‐34. [DOI] [PubMed] [Google Scholar]
Fagerström 1993 {published data only}
- Fagerström KO, Schneider NG, Lunell E. Effectiveness of nicotine patch and nicotine gum as individual versus combined treatments for tobacco withdrawal symptoms. Psychopharmacology (Berl) 1993;111(3):271‐7. [DOI] [PubMed] [Google Scholar]
Fagerström 1997 {published data only}
- Fagerström KO, Tejding R, Westin A, Lunell E. Aiding reduction of smoking with nicotine replacement medications: hope for the recalcitrant smoker?. Tobacco Control 1997;6(4):311‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fagerström 2000 {published data only}
- Fagerström KO, Hughes JR, Rasmussen T, Callas PW. Randomised trial investigating effect of a novel nicotine delivery device (Eclipse) and a nicotine oral inhaler on smoking behaviour, nicotine and carbon monoxide exposure, and motivation to quit. Tobacco Control 2000;9(3):327‐33. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ferguson 2015 {published data only}
- Ferguson SG, Walters JA, Lu W, Wells GP, Schuz N. Examination of the mechanism of action of two pre‐quit pharmacotherapies for smoking cessation. BMC Public Health 2015;15(1):1268‐73. [DOI] [PMC free article] [PubMed] [Google Scholar]
Finland unpublished {unpublished data only}
- Anon. Combination NRT; Improving efficacy in smoking cessation. McNeil Consumer Healthcare booklet, 2007. Short term outcomes reported on p17.
Garvey 2006 {unpublished data only}
- Garvey AJ, Hoskinson RA, Wadler BM, Kinnunen T, Sachs DP. Individualising nicotine patch dose to match smokers' usual nicotine intake levels (PA9‐4). Society for Research on Nicotine and Tobacco 12th Annual Meeting 2006 02 15‐18, Orlando, Florida. 2006:32.
- Mustonen TK, Spencer SM, Hoskinson RA, Sachs DPL, Garvey AJ. The influence of gender, race, and menthol content on tobacco exposure measures. Nicotine & Tobacco Research 2005;7(4):581‐90. [DOI] [PubMed] [Google Scholar]
Hajek 1999 {published data only}
- Hajek P, West R, Foulds J, Nilsson F, Burrows S, Meadow A. Randomized comparative trial of nicotine polacrilex, a transdermal patch, nasal spray, and an inhaler. Archives of Internal Medicine 1999;159(17):2033‐8. [DOI] [PubMed] [Google Scholar]
- West R, Hajek P, Foulds J, Nilsson F, May S, Meadows A. A comparison of the abuse liability and dependence potential of nicotine patch, gum, spray and inhaler. Psychopharmacology (Berl) 2000;149(3):198‐202. [DOI] [PubMed] [Google Scholar]
Haustein 2003 {published data only}
- Haustein KO, Batra A, Landfeldt B, Westin A. The effect of short‐term or long‐term reduction on smoking cessation; results from a placebo controlled smoking reduction study with the nicotine gum. Nicotine & Tobacco Research 2003;5:278. [Google Scholar]
- Pfizer. Summary of Clinical Efficacy. Application for licensing of Nicorette Inhalator/Gum for smoking reduction leading to cessation. Company data NICORE‐1013‐273‐SU.
Hollands 2013 {published data only}
- Hollands GJ, Sutton S, McDermott MS, Marteau TM, Aveyard P. Adherence to and consumption of nicotine replacement therapy and the relationship with abstinence within a smoking cessation trial in primary care. Nicotine & Tobacco Research 2013;15(9):1537‐44. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hughes 1989b {published data only}
- Hughes JR, Gulliver SB, Amori G, Mireault GC, Fenwick JF. Effect of instructions and nicotine on smoking cessation, withdrawal symptoms and self‐administration of nicotine gum. Psychopharmacology (Berl) 1989;99(4):486‐91. [DOI] [PubMed] [Google Scholar]
Hughes 2010 {published data only}
- Hughes JR, Solomon LJ, Livingston AE, Callas PW, Peters EN. A randomized, controlled trial of NRT‐aided gradual vs. abrupt cessation in smokers actively trying to quit. Drug & Alcohol Dependence 2010;111(1‐2):105‐13. [NCT00297492] [DOI] [PMC free article] [PubMed] [Google Scholar]
Jibrail 2010 {published data only}
- Jibrail JJ, Cortas NK, Sarieddine DS, Kanj NA, Zaatari GS, Daher RT. Impact of nicotine metabolite monitoring on the efficacy of smoke cessation and usefulness of sequential CRP measurements. American Journal of Respiratory Critical Care Medicine 2010;181:A2652. [Google Scholar]
Kozak 1995 {published data only}
- Kozak J, Fagerström KO, Sawe U. High‐dose treatment with the nicotine patch. International Journal of Smoking Cessation 1995;4(2):26‐8. [Google Scholar]
Kras 2010 {published data only}
- Kras M, Stough C, Scholey A, Kure C, Camfield D. Hypericum perforatum, nicotine patches and combination hypericum perforatum/nicotine patches for smoking cessation. European Neuropsychopharmacology 2010;20:S608‐9. [Google Scholar]
Landfeldt 1998 {unpublished data only}
- Landfeldt B, Kruse E, Westin A, Mattson K, Lojander J. Nicotine replacement treatment in heavy smokers: nicotine nasal spray combined with nicotine patch in a double‐blind controlled study. European Respiratory Journal 1998;12(Suppl 28):154S. [Google Scholar]
Leischow 1999 {published data only}
- Leischow SJ, Muramoto ML, Cook GN, Merikle EP, Castellini SM, Otte PS. OTC nicotine patch: effectiveness alone and with brief physician intervention. American Journal of Health Behavior 1999;23:61‐9. [Google Scholar]
Leischow 2004 {published data only}
- Leischow SJ, Ranger‐Moore J, Muramoto ML, Matthews E. Effectiveness of the nicotine inhaler for smoking cessation in an OTC setting. American Journal of Health Behavior 2004;28(4):291‐301. [DOI] [PubMed] [Google Scholar]
- Leischow SJ, Ranger‐Moore J, Muramoto ML, Matthews E. The safety and effectiveness of the nicotine inhaler for smoking cessation in an over‐the‐counter setting (POS4‐78). Society for Research on Nicotine and Tobacco 9th Annual Meeting, 2003 New Orleans, LA. 2003:100.
Lu 2017 {published data only}
- Lu W, Chappell K, Walters JA, Jacobson GA, Patel R, Schuz N, et al. The effect of varenicline and nicotine patch on smoking rate and satisfaction with smoking: an examination of the mechanism of action of two pre‐quit pharmacotherapies. Psychopharmacology 2017;234(Suppl 2):1‐8. [DOI] [PubMed] [Google Scholar]
Marsh 2005 {published data only}
- Marsh HS, Dresler CM, Choi JH, Targett DA, Gamble ML, Strahs KR. Safety profile of a nicotine lozenge compared with that of nicotine gum in adult smokers with underlying medical conditions: A 12‐week, randomized, open‐label study. Clinical Therapeutics 2005;27(10):1571‐87. [DOI] [PubMed] [Google Scholar]
McRobbie 2010 {published data only}
- McRobbie H, Thornley S, Bullen C, Lin RB, Senior H, Laugesen M, et al. A randomized trial of the effects of two novel nicotine replacement therapies on tobacco withdrawal symptoms and user satisfaction. Addiction 2010;105(7):1290‐8. [DOI] [PubMed] [Google Scholar]
Minneker 1989 {published data only}
- Minneker E, Buchkremer G, Block M. The effect of different dosages of a transdermal nicotine substitution system on the success rate of smoking cessation therapy. Methods and Findings in Experimental and Clinical Pharmacology 1989;11(3):219‐22. [PubMed] [Google Scholar]
NCT00985985 {unpublished data only}
- NCT00985985. A multi‐center, randomized, double‐blind, parallel, placebo‐controlled clinical study to evaluate efficacy and safety of nicotine mint lozenge (2mg and 4mg) in smoking cessation. www.gsk‐clinicalstudyregister.com/study/CHN‐Nicotine%20Mint%20Lozenge‐002#rs (first received July 16 2009).
- NCT00985985. Efficacy and safety study of nicotine mint lozenge (2mg and 4mg) in smoking cessation. clinicaltrials.gov/ct2/show/NCT00985985 (first received 29 September 2009).
NCT01592695 {unpublished data only}
- NCT01592695. Tailored tobacco cessation program for rural vVeterans with comorbid depression, alcoholism or obesity. clinicaltrials.gov/show/NCT01592695 (first received 11 April 2012).
NCT01892813 {unpublished data only}
- NCT01892813. Dissemination of a tailored tobacco quitline for rural veteran smokers. clinicaltrials.gov/ct2/show/NCT01892813 (first received 1 July 2013).
NCT02147132 {unpublished data only}
- NCT02147132. Pilot study of nicotine nasal spray and varenicline on smoking in methadone‐maintained patients. clinicaltrials.gov/ct2/show/NCT02147132 (first received 19 May 2014).
NCT02271919 {unpublished data only}
- NCT02271919. Varenicline and combined nicotine replacement therapy (NRT) for smoking cessation. clinicaltrials.gov/ct2/show/NCT02271919 (first received 17 October 2014).
Oncken 2009 {published data only}
- Oncken C, Campbell W, Chan G, Hatsukami D, Kranzler HR. Effects of nicotine patch or nasal spray on nicotine and cotinine concentrations in pregnant smokers. Journal of Maternal‐Fetal & Neonatal Medicine 2009;22(9):751‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Pomerleau 2003 {published data only}
- Lerman C, Audrain J, Patterson F, Kaufmann V, Rukstalis M, Wileyto EP, et al. Differential response to nicotine replacement therapies in obese and non‐obese women (PA2‐6). Society for Research on Nicotine and Tobacco 9th Annual Meeting, 2003 Orleans, LA. 2003.
- Pomerleau OF, Pomerleau CS, Marks JL, Snedecor SM, Mehringer AM, Namenek‐Brouwer RJ, et al. Prolonged nicotine patch use in quitters with past abstinence‐induced depressed mood. Journal of Substance Abuse Treatment 2003;24(1):13‐8. [DOI] [PubMed] [Google Scholar]
Sachs 1995 {published data only}
- Sachs DP. Effectiveness of the 4‐mg dose of nicotine polacrilex for the initial treatment of high‐dependent smokers. Archives of Internal Medicine 1995;155(18):1973‐80. [PubMed] [Google Scholar]
Schneider 2004 {published data only}
- Schneider NG, Olmstead RE, Nides M, Mody FV, Otte Colquette P, Doan K, et al. Comparative testing of 5 nicotine systems: initial use and preferences. Amercian Journal of Health Behavior 2004;28(1):72‐86. [DOI] [PubMed] [Google Scholar]
Schneider 2008 {published data only}
- Schneider NG, Cortner C, Gould JL, Koury MA, Olmstead RE. Comparison of craving and withdrawal among four combination nicotine treatments. Human Psychopharmacology 2008;23(6):513‐7. [DOI] [PubMed] [Google Scholar]
Shahab 2011 {published data only}
- Shahab L, McEwen A, West R. Acceptability and effectiveness for withdrawal symptom relief of a novel oral nicotine delivery device: a randomised crossover trial. Psychopharmacology 2011;216(2):187‐96. [DOI] [PubMed] [Google Scholar]
Shiffman 2000a {published data only}
- Shiffman S, Khayrallah M, Nowak R. Efficacy of the nicotine patch for relief of craving and withdrawal 7‐10 weeks after cessation. Nicotine & Tobacco Research 2000;2(4):371‐8. [DOI] [PubMed] [Google Scholar]
Shiffman 2000b {published data only}
- Shiffman S, Elash CA, Paton SM, Gwaltney CJ, Paty JA, Clark DB, et al. Comparative efficacy of 24‐hour and 16‐hour transdermal nicotine patches for relief of morning craving. Addiction 2000;95(8):1185‐95. [DOI] [PubMed] [Google Scholar]
Shiffman 2002 {published data only}
- Shiffman S, Rolf CN, Hellebusch SJ, Gorsline J, Gorodetzky CW, Chiang YK, et al. Real‐world efficacy of prescription and over‐the‐counter nicotine replacement therapy. Addiction 2002;97(5):505‐16. [DOI] [PubMed] [Google Scholar]
Sutherland 1999 {published data only}
- Anon. Combination NRT; Improving efficacy in smoking cessation. McNeil Consumer Healthcare booklet. Short term outcomes reported on p18.
- Sutherland G. A placebo‐controlled double‐blind combination trial of nicotine spray and patch. Nicotine & Tobacco Research 1999;1:186. [Google Scholar]
Tundulawessa 2010 {published data only}
- Tundulawessa Y, Yongchaiyud P, Chutrthong W, Tundulawessa K. The bioequivalent and effect of nicotine formulation gum on smoking cessation. Journal of the Medical Association of Thailand 2010;93(5):574‐9. [PubMed] [Google Scholar]
Vikhireva 2003 {published data only}
- Vikhireva O, Shalnova S, Deev A. Nicotine replacement therapy in Russia: old wine in new skins? Randomized parallel study of nicotine gum/inhaler in smoking cessation/reduction. Society for Research on Nicotine and Tobacco. Fifth European Conference. 2003 11 20‐22, Padua, Italy. 2003.
- Vikhireva O, Shalnova S, Deev A, Levshin V, Radkevich N, Kalinina A. NRT‐assisted cessation in Russia: individual and population level benefits. Society for Research on Nicotine and Tobacco 11th Annual Meeting, 2005 03 20‐23; Prague, Czech Republic. 2005.
Williams 2007 {published and unpublished data}
- Williams JM, Gandhi KK, Foulds J, Steinberg M, Lou S, Masumova F, et al. No advantage for high dose compared to regular dose nicotine patch on short‐term abstinence rates in schizophrenia (PA2‐3). Society for Research on Nicotine and Tobacco 13th Annual Meeting; 2007 02 21‐24; Austin, Texas. 2007.
References to ongoing studies
NCT01622998 {unpublished data only}
- Leblanc A, Reid R, Mark A, Tulloch H, Aitken D, Mullen K, et al. STEP‐ing up smoking cessation: weight‐related concern of participants who want to quit smoking. Obesity Facts 2017;10:207. [Google Scholar]
- NCT01622998. Self‐directed titrated transdermal nicotine patch versus standard treatment for smoking cessation (STEP). clinicaltrials.gov/ct2/show/NCT01622998 (first received 19 June 2012.
Additional references
BNF 2018
- Joint Formulary Committee. British National Formulary. 76. London: BMJ Group and Pharmaceutical Press, 2018. [Google Scholar]
Cahill 2013
- Cahill K, Stevens S, Perera R, Lancaster T. Pharmacological interventions for smoking cessation: an overview and network meta‐analysis. Cochrane Database of Systematic Reviews 2013, Issue 5. [DOI: 10.1002/14651858.CD009329.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Cahill 2016
- Cahill K, Lindson‐Hawley N, Thomas KH, Fanshawe TR, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database of Systematic Reviews 2016, Issue 5. [DOI: 10.1002/14651858.CD006103.pub7] [DOI] [PMC free article] [PubMed] [Google Scholar]
Carson 2012
- Carson KV, Verbiest ME, Crone MR, Brinn MP, Esterman AJ, Assendelft WJ, et al. Training health professionals in smoking cessation. Cochrane Database of Systematic Reviews 2012, Issue 5. [DOI: 10.1002/14651858.CD000214.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
CDC 2017
- Centers for Disease Control and Prevention. Quitting Smoking Among Adults—United States, 2000–2015. Morbidity and Mortality Weekly Report 2017;65(52):1457‐64. [DOI] [PubMed] [Google Scholar]
Coleman 2015
- Coleman T, Chamberlain C, Davey M, Cooper SE, Leonardi‐Bee J. Pharmacological interventions for promoting smoking cessation during pregnancy. Cochrane Database of Systematic Reviews 2015, Issue 12. [DOI: 10.1002/14651858.CD010078.pub2] [DOI] [PubMed] [Google Scholar]
Deeks 2017
- Deeks J, Higgins JP, Altman DG, (editors) on behalf of the Cochrane Statistical Methods Group. Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JP, Churchill R, Chandler J, Cumpston MS, editor(s), Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017), Cochrane, 2017. Available from www.training.cochrane.org/handbook.
Fagerström 2012
- Fagerström K. Determinants of tobacco use and renaming the FTND to the Fagerstrom Test for Cigarette Dependence. Nicotine & Tobacco Research 2012;14(1):75‐8. [DOI: ] [DOI] [PubMed] [Google Scholar]
Fanshawe 2017
- Fanshawe TR, Halliwell W, Lindson N, Aveyard P, Livingstone‐Banks J, Hartmann‐Boyce. Tobacco cessation interventions for young people. Cochrane Database of Systematic Reviews 2017, Issue 11. [DOI: 10.1002/14651858.CD003289.pub6] [DOI] [PMC free article] [PubMed] [Google Scholar]
Fiore 1992
- Fiore MC, Jorenby DE, Baker TB, Kenford SL. Tobacco dependence and the nicotine patch. Clinical guidelines for effective use. JAMA 1992;268(19):2687‐94. [PubMed] [Google Scholar]
Fiore 2008
- Fiore MC, Jaén CR, Baker TB, Bailey WC, Benowitz NL, Curry SJ, et al. Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville, MD: U.S. Department of Health and Human Services. Public Health Service, May 2008. [Google Scholar]
GBD 2015 Risk Factors Collaborators 2016
- GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388(10053):1659‐724. [DOI: 10.1016/S0140-6736(16)31679-8] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hartmann‐Boyce 2016
- Hartmann‐Boyce J, McRobbie H, Bullen C, Begh R, Stead LF, Hajek P. Electronic cigarettes for smoking cessation. Cochrane Database of Systematic Reviews 2016, Issue 9. [DOI: 10.1002/14651858.CD010216.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hartmann‐Boyce 2018
- Hartmann‐Boyce J, Chepkin SC, Ye W, Bullen C, Lancaster T. Nicotine replacement therapy versus control for smoking cessation. Cochrane Database of Systematic Reviews 2018, Issue 5. [DOI: 10.1002/14651858.CD000146.pub5] [DOI] [PMC free article] [PubMed] [Google Scholar]
Henningfield 2005
- Henningfield JE, Fant RV, Buchhalter AR, Stitzer ML. Pharmacotherapy for nicotine dependence. CA Cancer Journal for Clinicians 2005;55(5):281‐99. [DOI] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analysis. BMJ 2003;327(7414):557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
Hughes 2014
- Hughes JR, Stead LF, Hartmann‐Boyce J, Cahill K, Lancaster T. Antidepressants for smoking cessation. Cochrane Database of Systematic Reviews 2014, Issue 1. [DOI: 10.1002/14651858.CD000031.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Italy ISS 2004
- Osservatorio Fumo, Alcol e Droga. Linee Guida Cliniche per Promuovere la Cessazione dell’Abitudine al Fumo. Rome: Istituto Superiore di Sanita, 2004. [Google Scholar]
Jha 2011
- Jha P. Avoidable deaths from smoking: a global perspective. Public Health Reviews 2011;33(2):569‐600. [Google Scholar]
Le Foll 2005
- Foll B, Melihan‐Cheinin P, Rostoker G, Lagrue G. Smoking cessation guidelines: evidence‐based recommendations of the French Health Products Safety Agency. European Psychiatry 2005;20(5‐6):431‐41. [DOI] [PubMed] [Google Scholar]
Lindson‐Hawley 2016
- Lindson‐Hawley N, Hartmann‐Boyce J, Fanshawe TR, Begh R, Farley A, Lancaster T. Interventions to reduce harm from continued tobacco use. Cochrane Database of Systematic Reviews 2016, Issue 10. [DOI: 10.1002/14651858.CD005231.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
McNeill 2017
- McNeill A, Robson D. A man before his time: Russell's insights into nicotine, smoking, treatment and curbing the smoking problem. Addiction 2017;113(4):759‐63. [DOI: 10.1111/add.14043] [DOI] [PubMed] [Google Scholar]
NICE 2018
- National Institute for Health and Care Excellence. Stop smoking interventions and services (NG92). www.nice.org.uk/guidance/ng92/resources/stop‐smoking‐interventions‐and‐services‐pdf‐1837751801029 2018.
NZ MoH 2007
- New Zealand Ministry of Health. New Zealand Smoking Cessation Guidelines. Treatment%20Guidelines_New%20Zealand%20treatment%20guidelines%20in%20English%202007%20(1).pdf 2007 (accessed 3 April 2019).
West 2000
- West R, McNeill A, Raw M. Smoking cessation guidelines for health professionals: an update. Health Education Authority. Thorax 2000;55(12):987‐99. [DOI] [PMC free article] [PubMed] [Google Scholar]
West 2001
- West R, .Shiffman S. Effect of oral nicotine dosing forms on cigarette withdrawal symptoms and craving: a systematic review. Psychopharmacology Berl 2001;155(2):115‐22. [DOI] [PubMed] [Google Scholar]
West 2005
- West R, Hajek P, Stead L, Stapleton J. Outcome criteria in smoking cessation trials: proposal for a common standard. Addiction 2005;100(3):299‐303. [DOI: 10.1111/j.1360-0443.2004.00995.x] [DOI] [PubMed] [Google Scholar]
Woolacott 2002
- Woolacott NF, Jones L, Forbes CA, Mather LC, Sowden AJ, Song FJ, et al. The clinical effectiveness and cost‐effectiveness of bupropion and nicotine replacement therapy for smoking cessation: a systematic review and economic evaluation. Health Technology Assessment 2002;6(16):1‐245. [DOI] [PubMed] [Google Scholar]
Zwar 2011
- Zwar N, Borland R, Peters M, Litt J, Bell J, Caldwell B, et al. Supporting Smoking Cessation: A Guide for Health Professionals. Melbourne: The Royal Australian College of General Practitioners, 2011. [Google Scholar]
References to other published versions of this review
Silagy 1994a
- Silagy C, Mant D, Fowler G, Lodge M. Meta‐analysis on efficacy of nicotine replacement therapies in smoking cessation. Lancet 1994;343:139‐42. [DOI] [PubMed] [Google Scholar]
Silagy 1994b
- Silagy C, Mant D, Fowler G, Lancaster T. The effectiveness of nicotine replacement therapies in smoking cessation. Online Journal of Current Clinical Trials 1994;Doc No:113. [DOI] [PubMed] [Google Scholar]
Silagy 1996
- Silagy C, Lancaster T, Stead L, Mant D, Fowler G. Nicotine replacement therapy for smoking cessation. Cochrane Database of Systematic Reviews 1996, Issue 2. [Google Scholar]
Silagy 2001
- Silagy C, Lancaster T, Stead L, Mant D, Fowler G. Nicotine replacement therapy for smoking cessation. Cochrane Database of Systematic Reviews 2001, Issue 3. [DOI: 10.1002/14651858.CD000146] [DOI] [PubMed] [Google Scholar]
Silagy 2002
- Silagy C, Lancaster T, Stead L, Mant D, Fowler G. Nicotine replacement therapy for smoking cessation. Cochrane Database of Systematic Reviews 2002, Issue 4. [DOI: 10.1002/14651858.CD000146] [DOI] [PubMed] [Google Scholar]
Silagy 2004
- Silagy C, Lancaster T, Stead L, Mant D, Fowler G. Nicotine replacement therapy for smoking cessation. Cochrane Database of Systematic Reviews 2004, Issue 3. [DOI: 10.1002/14651858.CD000146] [DOI] [PubMed] [Google Scholar]
Stead 2008
- Stead LF, Perera R, Bullen C, Mant D, Lancaster T. Nicotine replacement therapy for smoking cessation. Cochrane Database of Systematic Reviews 2008, Issue 1. [DOI: 10.1002/14651858.CD000146.pub3] [DOI] [PubMed] [Google Scholar]
Stead 2012
- Stead LF, Perera R, Bullen C, Mant D, Hartmann‐Boyce J, Cahill K, Lancaster T. Nicotine replacement therapy for smoking cessation. Cochrane Database of Systematic Reviews 2012, Issue 11. [DOI: 10.1002/14651858.CD000146.pub4] [DOI] [PubMed] [Google Scholar]