
Fig. 1.
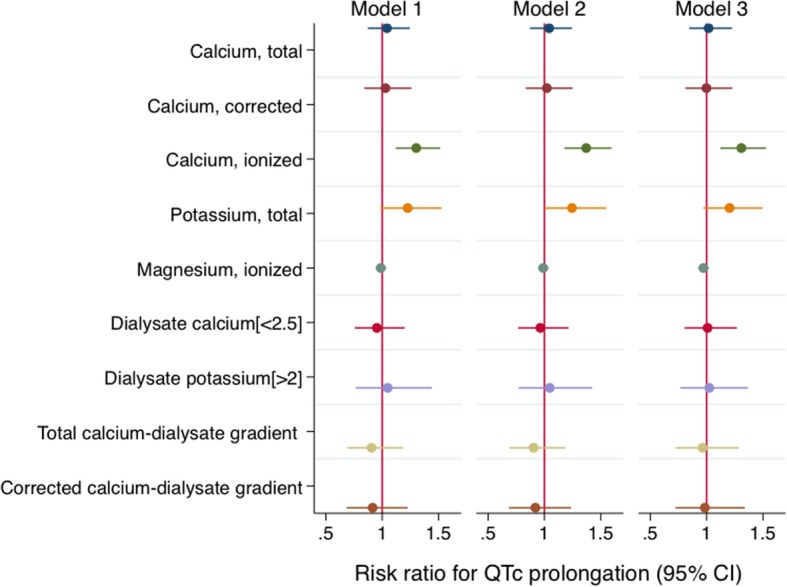
Associations of serum, dialysate, and serum-dialysate gradient measures with the risk of QTc prolongation at baseline in 330 incident dialysis participants.* Total calcium, per 1 mg/dl decrease; corrected calcium, per 1 mg/dl decrease; ionized calcium, per 0.1 mmol/l decrease; potassium, per 1 mEq/l decrease; magnesium, per 0.1 mEq/l decrease; dialysate calcium [< 2.5] = dialysate calcium < 2.5 mEq/l in reference to 2.5 mEq/l; dialysate potassium [> 2] = dialysate potassium > 2 mEq/l in reference to 2 mEq/l; total calcium-dialysate gradient, per 1 mEq/l increase in difference; corrected calcium-dialysate gradient, per 1 mEq/l increase in difference. Model 1 includes the main exposure (one of serum, dialysate, or gradient measurements). Model 2 includes model 1, age, sex, and ethnicity. Model 3 includes model 2, Charlson comorbidity index, non-dialysis systolic blood pressure, left ventricular mass index, and use of antihypertensive medication, renin-angiotensin-aldosterone system blockade, cinacalcet, and QT-prolonging medication. Models with ionized calcium and magnesium also include serum pH