
Figure 4.
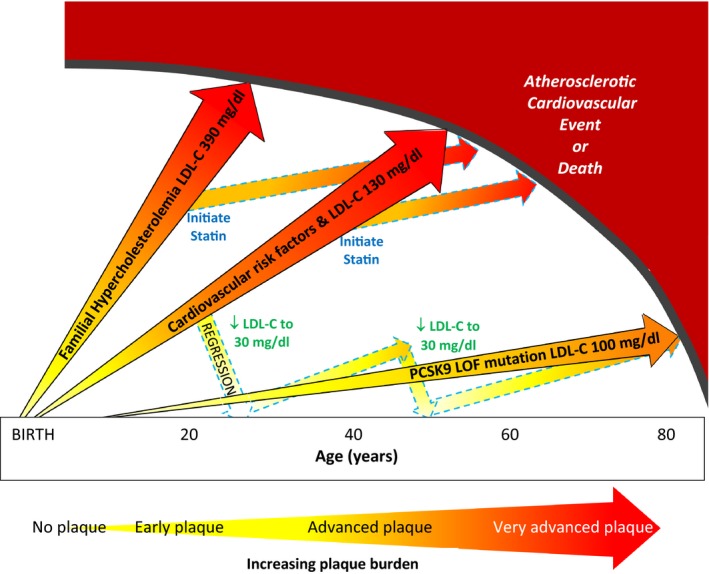
Life course trajectory of atherosclerotic progression is illustrated for individuals at very high, high, and low risk of atherosclerotic cardiovascular disease events (ASCVD). (1) individuals with heterozygous familial hypercholesterolemia who have severe LDL‐C elevation from birth have markedly accelerated atherosclerosis and premature onset of clinical ASCVD events; (2) individuals with cardiovascular risk factors from young adulthood and “average” LDL‐C levels of 130 mg/dL are more likely to experience clinical ASCVD events in early and middle age; and (3) individuals with a proprotein convertase subtilisin/kexin type 9 PCSK9 loss‐of‐function (PCSK9 LOF) mutation have lower LDL‐C levels throughout the lifespan and may be at markedly reduced risk of clinical ASCVD events. LDL‐C lowering with statins can stabilize and modestly regress plaque but does not eradicate the plaque burden and remain at increased risk of clinical ASCVD events. Intensive LDL‐C lowering to 20 to 40 mg/dL may have a greater impact on plaque regression in earlier stages of plaque. A new paradigm of “regression” treatment with intensive LDL‐C lowering earlier in the course of atherosclerosis or at younger ages could then be followed by intermittent retreatment to “maintain” a low plaque burden until late in life. LDL‐C indicates low‐density lipoprotein cholesterol (to convert to mmol/L divide by 38.65 mg/dL); PCSK9 LOF indicates proprotein convertase subtilisin/kexin type 9 loss‐of‐function mutation.