
Figure 1.
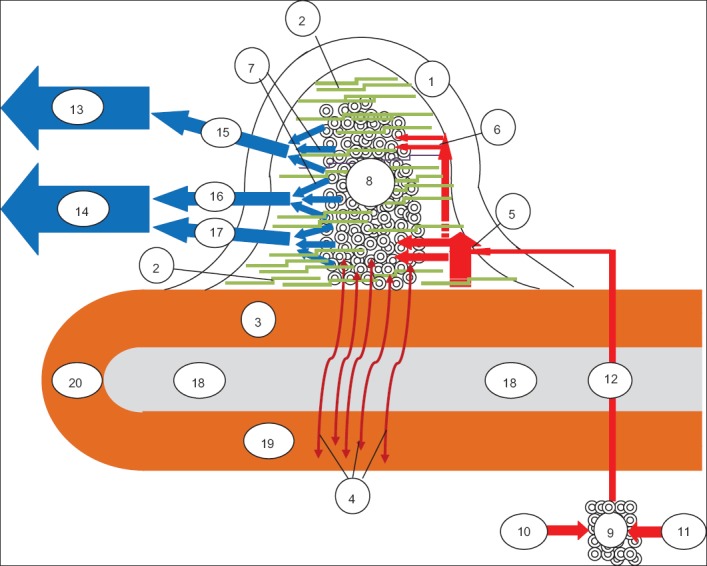
A proposed schematic representation of the anatomy of the anal cushion. Anal cushion consists of a non-vascular part (the transitional epithelium – 1, the submucosal connective tissue – 2 and the muscle of Treitz, which has 2 elements, the anal submucosal muscle – 3 and the mucosal suspensory ligament or Park’s ligament - 4) and a vascular part (the small arterioles - 5, the tiny arterioles – 6, the tiny venules – 7 and the direct arteriolar-venular anastomoses between arterioles and venules, that form a subcutaneous spongy network of capillaries, the sinusoids – 8). Arterial blood from the retrorectal plexus - 9 (formed by the SRA -10 and MRA -11) supplies the sinusoidal plexus via 3 terminal arterial branches (here one of them is shown - 12). Before turning into sinusoids - 8, the terminal branch subdivides into small - 5 and tiny - 6 arterioles in the lamina propria. These small and tiny arterioles are the source of bleeding, when the anal cushion is transformed to an anal nodule. Sinusoid drainage is accomplished via tiny venules - 7, which direct venous blood both to the portal circulation – 13 (through the SRV -15) and to the systemic circulation – 14 (mainly through the MRV-16 and to a lesser extent through the IRV -17). The cluster of sinusoids is tightly fixed to the inner anal sphincter -18 by the anal submucosal muscle -3 and by the submucosal connective tissue - 2 (which extends between the sinusoidal anastomoses) and to the conjoined longitudinal muscle -19 by the mucosal suspensory ligament -4. According to several researchers, anal submucosal muscle -3 is thought to represent the continuity of the conjoined longitudinal muscle -19; the latter is believed to form a loop -20 at the lower end of the internal anal sphincter (based on references 5,7,8,10,12-20) IRV, inferior rectal vein; MRA, middle rectal artery; MRV, middle rectal vein; SRA, superior rectal artery; SRV, superior rectal vein