

Abstract
Background
Approximately 50% of people with myasthenia gravis present with purely ocular symptoms, so called ocular myasthenia. Of these between 50% to 60% develop generalized disease, most within two years. Their management is controversial. This is an update of a review first published in 2006 and previously updated in 2008 and 2010.
Objectives
To assess the effects of treatments for ocular myasthenia and to answer three specific questions. Are there any treatments that impact the progression from ocular to generalized disease? Are there any treatments that improve symptoms of diplopia or ptosis? What is the frequency of adverse effects associated with treatments used?
Search methods
In this updated review, we searched the Cochrane Neuromuscular Disease Group Specialized Register (3 August 2012), CENTRAL (2012, Issue 7), MEDLINE (January 1996 to July 2012) and EMBASE (January 1974 to July 2012) for randomized controlled trials (RCTs) as well as case‐control and cohort studies. The titles and abstracts of all articles were read by both authors and the full texts of possibly relevant articles were reviewed. The references of all manuscripts included in the review were scanned to identify additional articles of relevance and experts in the field were contacted to identify additional published and unpublished data. Where necessary, we contacted authors for further information.
Selection criteria
Inclusion required meeting three criteria: (a) randomized (or quasi‐randomized) controlled study design; (b) active treatment compared to placebo, no treatment or some other treatment; and (c) results reported separately for patients with ocular myasthenia (grade 1) as defined by the Myasthenia Gravis Foundation of America.
Data collection and analysis
We collected data regarding the risk of progression to generalized myasthenia gravis, improvement in ocular symptoms, and the frequency of treatment‐related side effects.
Main results
In the original review, we identified two RCTs relevant to the treatment of ocular myasthenia, only one of which reported results in terms of the pre‐specified outcome measures used in this review. This study included only three participants and was of limited methodological quality. There were no new RCTs in searches conducted for this or previous updates. In the absence of data from RCTs, we present a review of the available observational data.
Authors' conclusions
The available randomized controlled literature does not permit any meaningful conclusions about the efficacy of any form of treatment for ocular myasthenia. Data from several reasonably good quality observational studies suggest that corticosteroids and azathioprine may be beneficial in reducing the risk of progression to generalized myasthenia gravis.
Plain language summary
Medical and surgical treatment for ocular myasthenia
Ocular myasthenia is a form of myasthenia gravis in which weakened eye muscles cause double vision or drooping eyelids. It accounts for approximately 50% of people with myasthenia gravis. Myasthenia gravis is an autoimmune disorder in which the body's own antibodies block the transmission of nerve impulses to muscles, causing fluctuating weakness and muscles that tire easily. Approximately half of people who have ocular myasthenia will go on to develop generalised myasthenia gravis and weakness affecting other muscles. For the majority of people this will be within the first two years of developing ocular symptoms.
The aims of treatment for ocular myasthenia are to return the person to a state of clear vision and to prevent the development, or limit the severity of generalised myasthenia gravis. Treatments proposed for ocular myasthenia include drugs that suppress the immune system including corticosteroids and azathioprine, thymectomy (surgical removal of the thymus gland), and acetylcholinesterase inhibitors (which increases acetylcholine to compensate for the lack of acetylcholine receptors).
Two randomised controlled trials (RCTs) relevant to the treatment of ocular myasthenia were identified in the original version of this review in 2006 and no new trials in this or previous updates. One trial included 43 ocular myasthenia participants treated with corticotropin (a type of corticosteroid) or placebo. The other only included three participants with ocular myasthenia and seven with generalised myasthenia gravis who were treated with intranasal neostigmine (an acetylcholinesterase inhibitor) or placebo. Neither trial enabled us to draw firm conclusions regarding how effective these treatments were in preventing progression to the development of generalised myasthenia gravis or in improving ocular symptoms. Several reasonably good quality non‐randomised studies favor the use of corticosteroids and azathioprine but these and other agents need to be tested in well‐designed RCTs.
Background
Myasthenia gravis (MG) is a term derived from the Greek 'myasthenia' meaning 'muscle weakness' and the Latin 'gravis' meaning 'serious'. The disease is characterized by weakness, which causes fatigue, and a distinct propensity for involvement of the ocular muscles that leads to the complaints of drooping eyelids or double vision (Oosterhuis 1997). Based on retrospective case reviews, ocular manifestations are the first sign of MG in about 50% of patients (Bever 1983; Oosterhuis 1997). Between 50% to 60% of those who initially present with ocular symptoms will progress to develop generalized muscle weakness (Bever 1983; Oosterhuis 1997) and the vast majority will do so within the first one to two years (Bever 1983; Oosterhuis 1997). Myasthenia gravis is the result of an autoimmune attack against the neuromuscular junction (Kaminski 2003; Vincent 2001). The primary antigenic target in most people is the nicotinic acetylcholine receptor (AChR) located on the post‐synaptic surface of the neuromuscular junction. Acetylcholine receptor antibodies are detected in about 90% of people with generalized MG and about 50% of patients with disease restricted to the ocular muscles, so‐called ocular myasthenia. Recently, a muscle specific kinase has been proposed as another antigenic target, but restricted ocular myasthenia appears not to occur in this group (Evoli 2003; Vincent 2003).
Treatment of ocular manifestations may be considered to have two goals: (1) to return the person to a state of clear vision and (2) to prevent, or limit the severity of, the generalization of the disease. It has been suggested that cholinesterase inhibitors may be effective in improving visual disability in 20% to 40% of people with ocular myasthenia (Evoli 2001; Oosterhuis 1997; Sommer 1997), but are not thought to have significant immunomodulatory effects that would influence generalization of the disease. Corticosteroids are frequently used in the treatment of ocular myasthenia to limit symptoms. Uncontrolled, retrospective studies (Kupersmith 1996; Kupersmith 2003; Mee 2003; Monsul 2004; Sommer 1997) suggest that treatment reduces the risk of progression to generalized disease. However, the adverse effects of such treatment have not been well characterized. For ocular myasthenia, thymectomy, a commonly applied treatment for generalized MG, has been used to a limited extent and in highly selected populations with visual disability considered to be unresponsive to other therapy. These studies report remission rates of 6% to 50% (Evoli 1988; Nakamura 1996; Schumm 1985; Sommer 1997). Generalized MG is often treated with azathioprine, cyclosporin and mycophenolate mofetil. Only azathioprine has been retrospectively evaluated as a treatment for ocular myasthenia and suggested to be beneficial (Sommer 1997).
There have been no prior systematic reviews of the treatments for ocular myasthenia. This updated review evaluates the evidence from therapeutic studies of treatments for ocular myasthenia.
Objectives
To assess the effects of treatments for ocular myasthenia and to answer three specific questions. Are there any treatments that impact the progression from ocular to generalized disease? Are there any treatments that improve symptoms of diplopia or ptosis? What is the frequency of adverse effects associated with treatments used?
Methods
Criteria for considering studies for this review
Types of studies
We included in the review all RCTs and quasi‐RCTs of any drug or surgical procedure in people with myasthenia gravis that is limited to the extra‐ocular, eyelid and orbicularis oculi muscles. We included the results from high quality observational studies (case control and cohort studies) in the Discussion.
Types of participants
We included both children and adults. We excluded participants with clinical evidence of generalized MG. Abnormalities on single fiber electromyography (EMG) did not constitute grounds for exclusion.
Types of interventions
We considered any drug treatment or surgical procedure that was compared either to no treatment or to a placebo. Drug treatments included corticosteroids, azathioprine (and other immunosuppressive agents) and acetylcholinesterase inhibitors. Surgical treatments included any form of thymectomy. We included studies that examined comparisons or combinations of these treatments.
Types of outcome measures
Primary outcomes
We considered the development of generalized MG within 12 months as the primary measure of outcome. Generalized disease was defined as the development of signs or symptoms of disease that are not limited to the extraocular, eyelid and orbicularis oculi muscles. Where possible, we had planned to calculate and compare the annual rates at which generalized disease developed.
Secondary outcomes
Secondary outcome measures included:
Improvement or resolution of symptoms due to ocular myasthenia (ptosis, diplopia) within 12 months of the start of treatment. There are no standardized criteria for determining the presence of improvement in symptoms of ocular myasthenia. We relied on each individual study's designation of whether improvement was deemed to have occurred;
The occurrence, or not of one or more serious adverse effects attributable to the treatment in the 12 month period following the start of treatment. Serious adverse events are those that are life‐threatening, fatal or require hospital admission. Where available we also gathered data about adverse events requiring treatment that are related to use of corticosteroids (including diabetes, hypertension, osteoporosis, glaucoma and peptic ulcer disease).
We selected the following outcomes for inclusion in a 'Summary of findings' table, had evidence from RCTs been available for analysis.
Development of generalized MG within 12 months.
Improvement of symptoms (diplopia or ptosis) within 12 months of treatment.
Occurrence of side effects within 12 months of treatment.
Search methods for identification of studies
Electronic searches
We searched the Cochrane Neuromuscular Disease Group Specialized Register (3 August 2012) for the following terms: myasthenia gravis, myasthenia, ocular, eye, visual, cholinergic agents, steroids, immunosuppressive agents, immunotherapy, therapy, manage, steroids, prednisolone, cortisone, azathioprine, immunosuppressants, acetylcholinest, cholinest pyridostigmine, CENTRAL (2012, Issue 7), MEDLINE (January 1966 to July 2012) and EMBASE (January 1974 to July 2012) for RCTs, case‐control and cohort studies. The detailed search strategies are listed in the appendices: CENTRAL (Appendix 1), MEDLINE (Appendix 2), EMBASE (Appendix 3).
Searching other resources
Both review authors read abstracts of all articles retrieved for potential relevance to the review. Each review author read articles that were definitely or possibly relevant in full. We also reviewed the bibliographies of the articles obtained in this way in order to identify additional articles. We contacted experts in the field in order to identify any unpublished studies that may be relevant to the review.
Data collection and analysis
Selection of studies
Both review authors independently reviewed the titles and abstracts of all articles in order to identify studies that might be relevant. Authors decided on the suitability of studies for inclusion in the review based on whether they met pre‐specified inclusion criteria. To be included in the review, studies had to meet three criteria: (a) randomized (or quasi‐randomized) controlled study design; (b) active treatment compared to placebo, no treatment or some other treatment; and (c) results reported separately for participants with ocular myasthenia (grade 1) as defined by the MG Foundation of America (Jaretzki 2000). The studies identified for inclusion were graded for their risk of bias. Disagreement between the two authors was resolved by discussion. Authors were not blinded to trial authors' names, institutional affiliation or journals of publication.
Assessment of risk of bias in included studies
Both review authors independently assessed studies for their methodology. Disagreement between the authors was resolved by discussion. We evaluated the risk of bias of RCTs using the methods described in Chapter 8 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2008). Answers to the questions "was the allocation sequence adequately generated?", "was allocation adequately concealed?", " was knowledge of the allocated intervention adequately prevented during the study?", "were incomplete outcome data adequately addressed?", "is the report of the study free of suggestion of selective reporting of outcomes?" and "was the study apparently free of other problems that could put it at a risk of bias?" were answered "yes" to indicate low risk of bias, "no" to indicate high risk of bias or "unclear" when the risk of bias was uncertain. In this version of the review these judgements are expressed as "Low risk of bias", "High risk of bias" and "Unclear risk of bias" according to the current version of RevMan and the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Data extraction and management
The review authors extracted data on study type, methodological quality, patients, interventions, outcomes and adverse events using a paper form. When necessary, attempts were made to obtain missing data from trial authors.
Analysis
Meta‐analysis was not performed as only a single RCT with suitable outcome measures was identified.
Results
Description of studies
The number of papers found by the new, current strategies are as follows: Cochrane Neuromuscular Disease Group Specialized Register 5 papers, CENTRAL 8 papers, MEDLINE 320 papers, EMBASE 40 papers.
We identified two RCTs that included participants with ocular myasthenia (Mount 1964; Badrising 1996) in the original version of this review. The characteristics of these two studies are summarized in the table Characteristics of included studies. Only one of these studies reported results in terms of the primary or secondary outcome measures that were planned for this review (Badrising 1996). In the updates in 2008, 2010 and 2012 there were no new RCTs, although a preliminary report of the Mount study was identified and added to the references.
The study by Mount 1964 included 43 patients with ocular myasthenia who were randomized to receive either an eight‐day course of corticotropin (ACTH) or placebo in a parallel‐group design. The range of ocular movement was determined from projections of photographic negatives of each eye in different positions of gaze. By marking the mid‐point of the pupil with the eye deviated to the left, to the right, upwards and downwards, and then connecting these four points with an elliptical curved line, the investigators estimated the area of eye movement. The effectiveness of therapy was determined by comparing the area of eye movement between baseline and post‐treatment time points (at 10 days, one month and three months). Results were reported separately for each eye. There was no evaluation of ocular symptoms or the risk of progression to generalized disease.
Badrising 1996 included only three participants with ocular myasthenia (and seven patients with generalized MG) who were randomized to receive a two‐week course of either intranasal neostigmine or placebo. The study had a cross‐over design without a wash out period. No primary outcome measure was specified, but the authors reported that ptosis was improved in one of the participants during treatment with neostigmine.
Risk of bias in included studies
Randomization
The risk of bias items have been summarized in Figure 1. The first study reported that participants were "randomly assigned a code number" (Mount 1964). The second study simply stated that it was a randomized trial (Badrising 1996) but further details were not reported.
1.
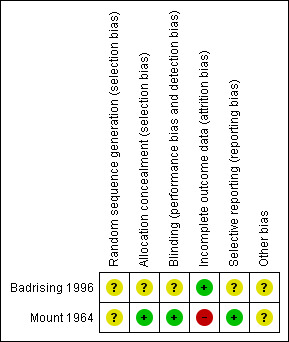
Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
Allocation concealment
In the first study identical vials containing ACTH or placebo were coded with a random number at a central office before being sent to each study site together with a list of random numbers that corresponded to the numbers on the medication vials. Patients entered into the study were assigned sequentially, based on the list of random numbers (Mount 1964). The second study contained no description of whether any attempt was made to conceal treatment allocation (Badrising 1996).
Blinding
The first study stated that the vials containing active and placebo medications were identical and that participants, nurses and attending physicians were unaware of the assigned treatment (Mount 1964). The second study simply stated that the trial was double‐blind without providing any further details (Badrising 1996).
Completeness of outcome data
Outcome data for the right eye was reported for 29 of 43 participants and for the left eye in 33 of 43 patients (Mount 1964). Results for all participants were reported in the second study (Badrising 1996).
Selective outcome reporting
In the first study investigators reported outcomes in terms of an objective measurement of eye movement (Mount 1964) as they originally proposed. The second study did not describe pre‐specified outcome measures (Badrising 1996). It is unclear, therefore, whether the report of improvement of symptoms of ptosis and diplopia represented complete reporting of outcomes.
Other potential threats to validity
Detailed information about the characteristics of study participants, that might influence response to treatment, was not reported in either study (Badrising 1996; Mount 1964).
Effects of interventions
Progression to generalized MG
Neither of the two RCTs identified by this review reported results in terms of the risk of progression to generalized MG (Badrising 1996; Mount 1964).
Improvement in ocular symptoms
A single study reported that one of three participants treated with intranasal neostigmine reported improvement in ocular symptoms (Badrising 1996). The sample size, however, was too small to draw any meaningful conclusions about the efficacy of (intranasal) acetylcholinesterase therapy.
Adverse effects
The frequency of side effects from corticotropin (ACTH) was reported in the first study (Mount 1964). ACTH was stopped in two participants (9.5%) because of an abnormal glucose tolerance test. ACTH was stopped in a single participant (4.8%) because of progressive edema of the eyelid. Other side effects that did not necessitate cessation of therapy were peripheral edema and a cushingoid face in four participants (19%) and anxiety or euphoria in six participants (28.6%).
Discussion
This systematic review of the literature identified two RCTs involving medical or surgical treatment of ocular myasthenia. There were no new trials in this update.
The results of the RCT of corticotropin versus placebo were reported in terms of the change in area of eye movements between pre‐ and post‐treatment evaluations, with the results reported separately for each eye at 12 months (Mount 1964). The odds ratios (ORs) (and 95% confidence intervals (CIs)) for improvement in area of eye movements amongst those treated with corticotropin compared to those who received placebo were 2.7 (95% CI 0.6 to 12) for the right eye and 10.3 (95% CI 1.2 to 25.2) for the left eye. The methodological quality of this study was generally good with the exception of the relatively high rate of loss to follow‐up with results reported for only 67% of right eyes and 77% of left eyes. The study results, however, were difficult to interpret because of the lack of any clinically meaningful measures of response to therapy.
The sample size of the second RCT was too small to permit any meaningful conclusions regarding the efficacy of intranasal neostigmine (Badrising 1996).
There have been no RCTs of other forms of immunosuppression (for example azathioprine, cyclosporine), thymectomy or oral acetylcholinesterase inhibitors.
This review also identified 10 observational (case control or cohort) studies that included patients with ocular myasthenia (Bhanushali 2008; Evoli 1988; Kawaguchi 2004; Kupersmith 2003; Kupersmith 2009; Mee 2003; Monsul 2004; Ortiz 2008; Papapetropoulos 2003; Papatestas 1987; Sommer 1997). It was necessary to contact the authors of three of these studies for further information (Bhanushali 2008; Evoli 1988; Kawaguchi 2004) but only two were able to provide the required data (Bhanushali 2008; Kawaguchi 2004).
The rates of progression to generalized myasthenia amongst treated and untreated patients were reported in eight of these studies (Kawaguchi 2004; Kupersmith 2003; Kupersmith 2009; Mee 2003; Monsul 2004; Ortiz 2008; Papapetropoulos 2003; Sommer 1997). Corticosteroids were used as active therapy in seven of these studies (Kupersmith 2003; Kupersmith 2009; Mee 2003; Monsul 2004; Ortiz 2008; Papapetropoulos 2003; Sommer 1997), azathioprine in two (Mee 2003; Sommer 1997) and thymectomy in one (Kawaguchi 2004). Four of the observational studies reported outcome in terms of improvement in ocular symptoms; prednisone was the active therapy in two (Bhanushali 2008; Ortiz 2008) and thymectomy was the active therapy in the other two (Kawaguchi 2004; Papatestas 1987). The methodological quality and results of these studies are summarized in Table 1 and Table 2. The quality of these studies was fairly uniform with adequate control for confounding, reasonably complete follow‐up and lack of observer blinding.
1. Observational studies with outcome of progression to generalized MG.
| Author (year) | n | Study Design | Demographics | Treatment | Treatment Schedule | Confounding | Follow‐up | Blinding | OR (95% CI) |
| Papapetropoulos (2003) | 28 7 steroids 21 no steroids | Case‐control | Mean age 48.6 Range: 15 to 80 61% male | Steroids | Gradual titration to 60 mg every other day and then tapered to lowest dose required (5 to 10 mg every other day) | Adequate Logistic regression to control for differences in age and antibody titer between the two treatment groups | Adequate Follow‐up in 100% Duration of follow‐up at least 8 years | Not done | 4.3 (0.6 to 25.9) |
| Mee (2003) | 34 11 steroids 23 no steroids | Case‐control | Mean age 55 Range: 18 to 87 56% male | Steroids | 25 mg per day (mean duration of therapy 33.5 months) | Adequate Duration of ocular symptoms, duration of follow‐up and antibody titers similar between the two treatment groups | Adequate Follow‐up in 100%. Mean duration of follow‐up 50.5 months | Not done | 0.02 (0.001 to 0.16) |
| Kupersmith (2003) | 147 58 steroids 36 no steroids | Cohort | Mean age 50 Range 2 to 80 57% male | Steroids | 10 mg per day for 2 days, 20 mg per day for 2 days, dose increased to 50 to 60 mg per day for 4 to 5 days, 40 mg per day for 1 week, 30 mg per day for 1 week, 20 mg per day for 1 week, 10 mg/20 mg every alternate day for 1 week, dose further reduced by 2.5 mg per day each week | Adequate Age and proportion of participants with elevated antibody titers similar between the two treatment groups | Inadequate Follow‐up in 64%. Mean duration of follow‐up 3.6 years (range 0.5 to 16 years) | Not done | 0.13 (0.04 to 0.45) |
| Monsul (2004) | 56 27 steroids 29 no steroids | Cohort | Mean age 53 | Steroids | 40 to 60 mg per day tapered to 2.5 to 10 mg per day over 3 to 6 months | Adequate Age and proportion of participants with elevated antibody titers similar between the two groups | Adequate Follow‐up in 100%. Minimum duration of follow‐up 24 months | Not done | 0.24 (0.06 to 0.99) |
| Sommer (1997) | 78 45 steroids 33 no steroids | Cohort | Mean age 50.6 Range 10 to 84 49% male | Steroids | Maximum dose 52 mg per day (mean duration of therapy 32 months) | Inadequate Age similar between two groups, but proportion with elevated antibody titers and with abnormal repetitive nerve stimulation different between the treatment groups | Adequate Follow‐up in 100%. Duration of follow‐up not specified. | Not done | 0.09 (0.03 to 0.29) |
| Kupersmith (2009) | 87 55 prednisone 32 no prednisone |
Cohort | Mean age Range 4 to 87 years 63% male | Steroids | 10 mg per day for 2 days, 20 mg per day for 2 days, dose increased to 50 to 60 mg per day for 7 days, dose decreased by 10mg per week to 10 mg per day, dose further reduced by 2.5 mg per day each week | Inadequate. Prednisone treated patients were those who did not refuse or had no contra‐indication to prednisone treatment. Gender distribution, age and frequency of elevated AChR antibodies were comparable between the two treatment groups. |
Adequate Follow‐up in 100%, but follow‐up duration not explicitly reported. | Not done | 0.15 (0.05 to 0.4) |
| Ortiz (2008) | 21 6 prednisone 15 no prednisone |
Cohort | Median age 2.6 Range 1.2 ‐ 4.9 | Steroids | Not specified | Inadequate. No discussion of whether the two treatment groups were comparable with respect to important potential confounding variables. | Adequate Follow‐up in 100%; mean duration 6.5 (range 2‐15.6) | Not done | 1.3 (0.09 to 17.7) |
| Sommer (1997) | 78 27 azathioprine 51 no azathioprine | Cohort | Mean age 50.6 Range 10 to 84 49% male | Azathioprine | Maximum dose 145 mg per day (mean duration of therapy 44 months) | Inadequate Age similar between two groups, but proportion with elevated antibody titers and with abnormal repetitive nerve stimulation different between the treatment groups | Adequate Follow‐up in 100%. Duration of follow‐up not specified. | Not done | 0.18 (0.05 to 0.67) |
| Kawaguchi (2005) | 75 17 thymectomy 58 no thymectomy | Cohort | Mean age 41 Range 1 to 76 35% male | Thymectomy | Adequate Age, the use of concurrent immunosuppressive therapy and duration of follow‐up were similar in the two treatment groups | Adequate Follow‐up in 100% Duration of follow‐up ranges from 58 to 86 months | Not done | 0.23 (0.012 to 4.31) |
OR: odds ratios of development of generalized MG amongst those receiving active treatment compared to those receiving control treatment.
2. Observational studies with outcome of improvement in ocular symptoms.
| Author (year) | n | Study Design | Demographics | Treatment | Confounding | Follow‐up | Blinding | OR (95% CI) |
| Bhanushali (2008) | 16 | Cohort | Median age 53.5 Range 30‐77 |
Steroids | Inadequate. No discussion of whether the two treatment groups were comparable with respect to important potential confounding variables. | Adequate Follow‐up in 100% |
Not done | 6.75 (0.93 to 49.2) |
| Ortiz (2008) | 21 | Cohort | Median age 2.6 Range 1.2 ‐ 4.9 |
Steroids | Inadequate. No discussion of whether the two treatment groups were comparable with respect to important potential confounding variables. | Adequate Follow‐up in 100%; mean duration 6.5 (range 2‐15.6) |
Not done | 0.8 (0.07 to 9.67) |
| Papatestas (1987) | 313 12 thymectomy 301 no thymectomy | Cohort | Not reported | Thymectomy | Not done | Adequate Follow‐up in 100% Duration of follow‐up not specified | Not done | 0.82 (0.18 to 3.8) |
| Kawaguchi (2005) | 75 17 thymectomy 58 no thymectomy |
Cohort | Mean age 41 Range 1‐76 35% male | Thymectomy | Adequate Age, the use of concurrent immunosuppressive therapy and duration of follow‐up were similar in the two treatment groups | Adequate Follow‐up in 100% Duration of follow‐up ranges from 58 to 86 months | Not done | 0.97 (0.27 to 3.45) |
CI: confidence interval
OR: odds ratios of improvement in ocular symptoms amongst those receiving active treatment compared to those receiving control treatment.
Among the two studies that examined the effects of oral corticosteroids on control of ocular symptoms, the point estimates of the OR favored steroids in one study (Bhanushali 2008), but not the other (Ortiz 2008); the CIs around the OR in both of these studies, spanned unity.
The point estimates of the OR in five of the seven studies that examined the effects of oral corticosteroids showed a benefit in terms of reducing the risk of progression to generalized MG (Kupersmith 2003; Kupersmith 2009; Mee 2003; Monsul 2004; Sommer 1997). The CI of the OR in the remaining two studies spanned unity (Ortiz 2008; Papapetropoulos 2003).
The two studies that examined the effects of azathioprine both showed a beneficial effect on the risk of progression to generalized MG with CIs that did not span unity (Mee 2003; Sommer 1997).
The two studies that examined the effects of thymectomy showed no benefit in terms of improvement in ocular symptoms (Kawaguchi 2004; Papatestas 1987) or risk of progression to generalized MG (Kawaguchi 2004).
Authors' conclusions
Implications for practice.
The available evidence from RCTs does not permit any firm conclusions to be drawn regarding the efficacy of acetylcholinesterase inhibitors, corticosteroids, other immunosuppressive agents or thymectomy in people with ocular myasthenia with respect to the outcome measures of improved ocular symptoms and the risk of progression to generalized MG. The data from several observational studies favor the use of corticosteroids and azathioprine but the uncontrolled nature of these reports limits the ability to draw any firm conclusions.
Implications for research.
There is a need for well‐designed randomized, placebo‐controlled studies of the efficacy of cholinesterase inhibitors, corticosteroids and other immunosuppressive agents. These studies should employ clinically relevant outcome measures such as improvement or resolution of ocular symptoms and the risk of progression to generalized MG.
In the absence of RCTs, well‐designed observational studies may shed light on the efficacy of cholinesterase inhibitors, corticosteroids and other immunosuppressive agents. These studies should control adequately for potentially confounding factors (age, the use of concomitant therapy, the duration of ocular symptoms prior to entry into the study, the duration of follow‐up following entry into the study, antibody status, and the presence of systemic abnormalities of repetitive nerve stimulation or single fiber electromyography); assess adverse effects, and should ensure that the outcome measure is ascertained in a blinded fashion in order to minimize bias.
What's new
| Date | Event | Description |
|---|---|---|
| 19 October 2017 | Amended | Trial added to Characteristics of studies awaiting classification. Information added to Published notes about the updating of this review. |
History
Protocol first published: Issue 1, 2005 Review first published: Issue 2, 2006
| Date | Event | Description |
|---|---|---|
| 17 August 2012 | New citation required but conclusions have not changed | Updated searches were reviewed. No new RCTs identified. |
| 17 August 2012 | New search has been performed | Searches updated 3 August 2012 |
| 1 March 2011 | Amended | Contact details updated. |
| 4 January 2010 | New search has been performed | New searches were run of the Cochrane NMD Group Trials Register (December 2009), MEDLINE (January 1966 to December 9 2009) and EMBASE (January 1966 to December 9 2009). No new trials were identified. Data from three new observational studies are included in the discussion and ancillary tables. |
| 2 June 2008 | Amended | Converted to new review format. |
| 25 January 2006 | New citation required and conclusions have changed | Substantive amendment |
Notes
A published, completed study (Benatar 2016) has been added to Characteristics of studies awaiting classification, pending a planned full update of the review.
Acknowledgements
The authors are grateful to Kate Jewitt and Richard Hughes at the Cochrane Neuromuscular Disease Group for their advice during the preparation of this review. We are also grateful to the late John Newsom‐Davis, Tony Swan, Philippe Gajdos and Sumit Singh for their helpful comments on an earlier draft of this review.
The editorial base of the Cochrane Neuromuscular Disease Group is supported by the MRC Centre for Neuromuscular Diseases and the Muscular Dystrophy Campaign.
Appendices
Appendix 1. CENTRAL search strategy
#1 (myasthenia*) #2 MeSH descriptor Eye Diseases explode all trees #3 ocular* or eye* or visual* #4 (#1 AND ( #2 OR #3 )) #5 MeSH descriptor Cholinergic Agents explode all trees #6 MeSH descriptor Steroids explode all trees #7 MeSH descriptor Immunosuppressive Agents explode all trees #8 MeSH descriptor Immunotherapy explode all trees #9 therap* or manag* or steroid* or prednis* or cortison* or azathioprine or immunosuppress* or acetylcholinest* or cholinest* or pyridostigmine* or thymectomy or corticotropin #10 (#5 OR #6 OR #7 OR #8 OR #9) #11 (#4 AND #10)
Appendix 2. MEDLINE (OvidSP) search strategy
Database: Ovid MEDLINE(R) <1946 to July Week 4 2012> Search Strategy: ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ 1 exp myasthenia gravis/ or myasthenia.tw. (14026) 2 (ocular$ or eye$ or visual$).mp. (696590) 3 Eye Diseases/ (31177) 4 1 and (2 or 3) (1215) 5 exp cholinergic agents/ (181786) 6 exp steroids/ (667984) 7 exp immunosuppressive agents/ (233955) 8 exp immunotherapy/ (196622) 9 (therap$ or manag$ or steroid$ or prednis$ or cortison$ or azathioprine or immunosuppress$ or acetylcholinest$ or cholinest$ or pyridostigmine$ or thymectomy or corticotropin).mp. (2947573) 10 4 and (or/5‐9) (652) 11 limit 10 to (clinical trial or consensus development conference or consensus development conference, nih or controlled clinical trial or guideline or meta analysis or multicenter study or practice guideline or randomized controlled trial) (25) 12 exp cohort studies/ (1194647) 13 (cohort$ or case‐control$ or case control$).mp. (412309) 14 [or/15‐22] (0) 15 [remove duplicates from 27] (0) 16 exp myasthenia gravis/ or myasthenia.tw. (14026) 17 (ocular$ or eye$ or visual$).mp. (696590) 18 Eye Diseases/ (31177) 19 16 and (17 or 18) (1215) 20 exp cholinergic agents/ (181786) 21 exp steroids/ (667984) 22 exp immunosuppressive agents/ (233955) 23 exp immunotherapy/ (196622) 24 (therap$ or manag$ or steroid$ or prednis$ or cortison$ or azathioprine or immunosuppress$ or acetylcholinest$ or cholinest$ or pyridostigmine$ or thymectomy or corticotropin).mp. (2947573) 25 19 and (or/20‐24) (652) 26 limit 25 to (clinical trial or consensus development conference or consensus development conference, nih or controlled clinical trial or guideline or meta analysis or multicenter study or practice guideline or randomized controlled trial) (25) 27 exp cohort studies/ (1194647) 28 (cohort$ or case‐control$ or case control$).mp. (412309) 29 25 and (27 or 28) (130) 30 randomized controlled trial.pt. (332737) 31 controlled clinical trial.pt. (84732) 32 randomized.ab. (236143) 33 placebo.ab. (133209) 34 drug therapy.fs. (1554147) 35 randomly.ab. (170059) 36 trial.ab. (244573) 37 groups.ab. (1115507) 38 or/30‐37 (2889100) 39 25 and 38 (251) 40 26 or 29 or 39 (325) 41 exp animals/ not humans.sh. (3760077) 42 40 not 41 (323) 43 remove duplicates from 42 (320)
Appendix 3. EMBASE (OvidSP) search strategy
Database: Embase <1980 to 2012 Week 30> Search Strategy: ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ 1 crossover‐procedure/ (34521) 2 double‐blind procedure/ (109963) 3 randomized controlled trial/ (326003) 4 single‐blind procedure/ (16165) 5 (random$ or factorial$ or crossover$ or cross over$ or cross‐over$ or placebo$ or (doubl$ adj blind$) or (singl$ adj blind$) or assign$ or allocat$ or volunteer$).tw. (1142094) 6 or/1‐5 (1220027) 7 exp case control study/ or exp cohort analysis/ (195500) 8 (cohort$ or case‐control$ or case control$).mp. (412724) 9 or/1‐8 (1583028) 10 exp animals/ (1782930) 11 exp humans/ (13651110) 12 10 not (10 and 11) (1333370) 13 9 not 12 (1539522) 14 limit 13 to embase (1215300) 15 myasthenia gravis/ or myasthenia$.mp. (18220) 16 (ocular or eye$ or visual$).tw. (664948) 17 eye disease/ (36079) 18 16 or 17 (683206) 19 exp immunosuppressive agent/ (479404) 20 exp immunotherapy/ (108489) 21 exp steroid/ (1005998) 22 (therap$ or manag$ or steroid$ or prednisone or prednisolone or cortison$ or azathioprine or immunosuppress$ or acetylcholinest$ or cholinest$ or pyridostigmine$ or thymectomy or corticotropin).mp. (4783156) 23 or/19‐22 (5290901) 24 14 and 15 and 18 and 23 (40)
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Badrising 1996.
| Methods | Randomized cross‐over double‐blind trial | |
| Participants | The Netherlands 3 participants (gender distribution not reported) Mean age and range not reported. | |
| Interventions | Intranasal neostigmine 4.5 mg three times per day for two weeks. | |
| Outcomes | Improvement in ocular symptoms. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Only statement is that trial was randomized |
| Allocation concealment (selection bias) | Unclear risk | No mention of whether or not allocation was concealed |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Simply state that study was double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Results are presented for all three patients with ocular myasthenia |
| Selective reporting (reporting bias) | Unclear risk | Primary endpoints were not specified |
| Other bias | Unclear risk | Insufficient information about study participants |
Mount 1964.
| Methods | Randomized parallel group double‐blind trial | |
| Participants | United States 43 participants (60% male) Mean age and range not reported. | |
| Interventions | Corticotropin (ACTH) 40 U twice daily for 6 days, 30 U twice daily for 1 day and 20 U twice daily for 1 day | |
| Outcomes | Change in range of eye movements between pre‐treatment and post‐treatment time points (10 days, 1 month, 3 months), with results reported separately for each eye. | |
| Notes | Primary outcome reported at 12 months | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Simply state that "each set [of vials] was identified only with a randomly assigned code number" |
| Allocation concealment (selection bias) | Low risk | Vials of medication labeled with code numbers, hospitals received assignment lists, patients assigned next available number and coded vial corresponding to this number was administered; "neither the patient, the nurses, nor the attending physicians knew what product was assigned" |
| Blinding (performance bias and detection bias) All outcomes | Low risk | "...corticotropin and the placebo (the same gel without the active ingredient) were bottled in identical 5ml vials ..." |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 22 patients assigned to placebo with results reported for 14 right eyes and 16 left eyes; 21 patients assigned to corticotropin with results reported for 15 right eyes and 14 left eyes |
| Selective reporting (reporting bias) | Low risk | Investigators planned to (and did) report outcome in terms of objectively measured range of eye movements |
| Other bias | Unclear risk | Insufficient information about study participants |
Characteristics of studies awaiting assessment [ordered by study ID]
Benatar 2016.
| Methods | Randomized, double‐blind, placebo‐controlled trial |
| Participants | United States and Canada 11 participants (male 6, female 5) Mean age was 62 (placebo group) and 64 (intervention group) Inclusion criteria
Exclusion criteria
|
| Interventions | Pyridostigmine for a period of 4 to 6 weeks, with dose escalated until efficacy or toxicity that could not be mitigated with a selective muscarinic antagonist; the maximum pyridostigmine dose permitted was 480 mg/day. Stage 1: Subjects whose symptoms failed to remit continued to take pyridostigmine and were randomized to either placebo or prednisone starting at 10 mg every other day, and titrated to a maximum of 40 mg/day over 16 weeks. Prednisone was started at a dose of 10 mg every other day; it was then initially increased to 10 mg/day, then 20 mg alternating with 10 mg, and so forth, with adjustments in dose made no more frequently than every 2 weeks. Dosage was titrated according to whether minimal manifestation status (MMS) had been attained and the presence and nature of adverse events. Stage 2: After the initial 16‐week period, participants who had not achieved MMS were crossed over to treatment with high‐dose prednisone (60 mg/day). The dose was tapered thereafter based on efficacy and safety/tolerability. Dosage was initially reduced to 50 mg/day, then 40 mg/day, and so forth down to 10 mg/day, with adjustments made every 2 weeks. After 2 weeks at 10 mg/day, the dose could be reduced to 10 mg every other day. For participants whose symptoms did remit during Stage 1, the study drug was tapered in a double‐blind manner in stage 2. This stage also lasted for 16 weeks. |
| Outcomes |
Primary outcome: treatment failure, defined as failure to achieve sustained MMS, progression to generalised myasthenia gravis, or toxicity leading to discontinuation of the study drug by week 16. Secondary outcomes: time to sustained MMS, change in ocular QMG score, changes in quality of life as measured by the 25‐item National Eye Institute Visual Function Questionnaire (NEI‐VFQ‐25), the 10‐item neuro‐ophthalmological supplement to the NEI‐VFQ‐25, and the 15‐item Myasthenia Gravis Quality‐of‐Life Scale (MG‐QOL‐15), each administered at baseline and week 16, as well as the occurrence of individual adverse events. |
| Notes |
Differences between protocol and review
For the 2010 update we revised the 'Risk of bias' methodology and stated outcomes that would be included in a 'Summary of findings' table. At the 2012 update, the RevMan categories for review authors 'Risk of bias' judgements changed (Higgins 2011).
The protocol gives details of methodology that the review authors would have followed had more data been available (Benatar 2006).
Contributions of authors
Michael Benatar and Henry Kaminski both evaluated each paper and extracted the relevant data. Michael Benatar wrote the first draft of the review. Henry Kaminski commented on and edited the draft to produce a final review. In 2010 both authors assessed 'Risk of bias' in the included studies. Both authors reviewed searches for updates and approved the text.
Declarations of interest
Dr Michael Benatar is the principal investigator on a RCT designed to compare the efficacy of prednisone plus pyridostigmine versus placebo plus pyridostigmine for the treatment of ocular myasthenia. He receives research funding from both the US National Institutes of Health (NIH) and the Food and Drug Administration for clinical trials in the field of MG.
Henry Kaminski is co‐investigator of the NIH‐sponsored trial of thymectomy for treatment of non‐thymomatous MG. He serves as consultant for Varleigh Limited, which is developing a drug for treatment of MG. He has served as a consultant for GlaxoSmithKline and serves on the Data and Safety Monitoring Board for a clinical trial sponsored by Cytokinetics. He receives royalties from Springer Publishing. He has performed legal consultations in cases related to MG.
Edited (no change to conclusions)
References
References to studies included in this review
Badrising 1996 {published data only}
- Badrising U, Brandenburg H, Hilten J, Brietl P, Wintzen A. Intranasal neostigmine as add‐on therapy in myasthenia gravis. Journal of Neurology 1996;243(Suppl):S59. [Google Scholar]
Mount 1964 {published data only}
- Mount FW. ACTH for ocular myasthenia. JAMA 1964;189:55. [PUBMED: 14149026] [DOI] [PubMed] [Google Scholar]
- Mount FW. Corticotropin in treatment of ocular myasthenia ‐ a controlled clinical trial. Archives of Neurology 1964;11:114‐24. [PUBMED: 14159267] [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
Benatar 2016 {published data only}
- Benatar M, McD ermott MP, Sanders DB, Wolfe GI, Barohn RJ, Nowak RJ, et al. Muscle Study Group. Efficacy of prednisone for the treatment of ocular myasthenia (EPITOME): a randomized controlled trial. Muscle & Nerve 2016;53:363–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
Additional references
Bever 1983
- Bever Jr CT, Aquino AV, Penn AS, Lovelace RE, Rowland LP. Prognosis of ocular myasthenia. Annals of Neurology 1983;14(5):516‐9. [DOI] [PubMed] [Google Scholar]
Bhanushali 2008
- Bhanushali MJ, Wuu J, Benatar M. Treatment of ocular symptoms in myasthenia gravis. Neurology 2008;71(17):1335‐8. [DOI] [PubMed] [Google Scholar]
Evoli 1988
- Evoli A, Tonali P, Bartoccioni E, Lo Monaco M. Ocular myasthenia: diagnostic and therapeutic problems. Acta Neurologica Scandinavica 1988;77(1):31‐5. [DOI] [PubMed] [Google Scholar]
Evoli 2001
- Evoli A, Batocchi AP, Minisci C, Schino C, Tonali P. Therapeutic options in ocular myasthenia gravis. Neuromuscular Disorders 2001;11(2):208‐16. [DOI] [PubMed] [Google Scholar]
Evoli 2003
- Evoli A, Tonali PA, Padua L, Monaco ML, Scuderi F, Batocchi AP, et al. Clinical correlates with anti‐MuSK antibodies in generalized seronegative myasthenia gravis. Brain 2003;126(10):2304‐11. [DOI] [PubMed] [Google Scholar]
Higgins 2008
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.0 [updated February 2008]. The Cochrane Collaboration, 2008. Available from www.cochrane‐handbook.org.
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Jaretzki 2000
- Jaretzki A, Barohn RJ, Ernstoff RM, Kaminski HJ, Keesey JC, Penn AS, et al. Myasthenia gravis. Recommendations for clinical research standards. Neurology 2000;55(1):16‐23. [DOI] [PubMed] [Google Scholar]
Kaminski 2003
- Kaminski HJ, editor. Myasthenia gravis and related disorders. Totowa, NJ: Humana Press, Inc, 2003. [Google Scholar]
Kawaguchi 2004
- Kawaguchi N, Kuwabara S, Nemoto Y, Fukutake T, Satomura Y, Arimura K, et al. Treatment and outcome of myasthenia gravis: retrospective multi‐center analysis of 470 Japanese patients, 1999‐2000. Journal of the Neurological Sciences 2004;224(1‐2):43‐7. [DOI] [PubMed] [Google Scholar]
Kupersmith 1996
- Kupersmith MJ, Moster M, Bhuiyan S, Warren F, Weinberg H. Beneficial effects of corticosteroids on ocular myasthenia gravis. Archives of Neurology 1996;53(8):802‐4. [DOI] [PubMed] [Google Scholar]
Kupersmith 2003
- Kupersmith MJ, Latkany R, Homel P. Development of generalized disease at 2 years in patients with ocular myasthenia gravis. Archives of Neurology 2003;60(2):243‐8. [DOI] [PubMed] [Google Scholar]
Kupersmith 2009
- Kupersmith, M. Ocular myasthenia gravis: treatment successes and failures in patients with long‐term follow‐up. Journal of Neurology 2009;256(8):1314‐20. [DOI] [PubMed] [Google Scholar]
Mee 2003
- Mee J, Paine M, Byrne E, King J, Reardon K, O'Day J. Immunotherapy of ocular myasthenia gravis reduces conversion to generalized myasthenia gravis. Journal of Neuro‐ophthalmology 2003;23(4):251‐5. [DOI] [PubMed] [Google Scholar]
Monsul 2004
- Monsul NT, Patwa HS, Knorr AM, Lesser RL, Goldstein JM. The effect of prednisone on the progression from ocular to generalized myasthenia gravis. Journal of the Neurological Sciences 2004;217(2):131‐3. [DOI] [PubMed] [Google Scholar]
Nakamura 1996
- Nakamura H, Taniguchi Y, Suzuki Y, Tanaka Y, Ishiguro K, Fukuda M, et al. Delayed remission after thymectomy for myasthenia gravis of the purely ocular type. Journal of Thoracic and Cardiovascular Surgery 1996;112(2):371‐5. [DOI] [PubMed] [Google Scholar]
Oosterhuis 1997
- Oosterhuis H. Myasthenia Gravis. The Netherlands: Groningen Neurological Press, 1997. [Google Scholar]
Ortiz 2008
- Ortiz S, Borchert, M. Long‐term outcomes of pediatric ocular myasthenia gravis. Ophthalmology 2008;115(7):1245‐48. [DOI] [PubMed] [Google Scholar]
Papapetropoulos 2003
- Papapetropoulos TH, Ellul J, Tsibri E. Development of generalized myasthenia gravis in patients with ocular myasthenia gravis. Archives of Neurology 2003;60(10):1491‐2. [DOI] [PubMed] [Google Scholar]
Papatestas 1987
- Papatestas AE, Genkins G, Kornfeld P, Eisenkraft JB, Fagerstrom RP, Pozner J, et al. Effects of thymectomy in myasthenia gravis. Annals of Surgery 1987;206(1):79‐88. [DOI] [PMC free article] [PubMed] [Google Scholar]
Schumm 1985
- Schumm F, Wietholter H, Fateh‐Moghadam A, Dichgans J. Thymectomy in myasthenia with pure ocular symptoms. Journal of Neurology, Neurosurgery and Psychiatry 1985;48(4):332‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sommer 1997
- Sommer N, Sigg B, Melms A, Weller M, Schepelmann K, Herzau V, et al. Ocular myasthenia gravis: response to long term immunosuppressive treatment. Journal of Neurology, Neurosurgery and Psychiatry 1997;62(2):156‐62. [DOI] [PMC free article] [PubMed] [Google Scholar]
Vincent 2001
- Vincent A, Palace J, Hilton‐Jones D. Myasthenia gravis. Lancet 2001;357(9274):2122‐8. [DOI] [PubMed] [Google Scholar]
Vincent 2003
- Vincent A, Bowen J, Newsom‐Davis J, McConville J. Seronegative generalized myasthenia gravis: clinical features, antibodies, and their targets. Lancet Neurology 2003;2(2):99‐106. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Benatar 2006
- Benatar M, Kaminski H. Medical and surgical treatment for ocular myasthenia. Cochrane Database of Systematic Reviews 2005, Issue 1. [DOI: 10.1002/14651858.CD005081] [DOI] [PMC free article] [PubMed] [Google Scholar]
Benatar 2011
- Benatar M, Kaminski H. Medical and surgical treatment for ocular myasthenia. Cochrane Database of Systematic Reviews 2006, Issue 2. [DOI: 10.1002/14651858.CD005081.pub2] [DOI] [PubMed] [Google Scholar]