

Abstract
Background
About one‐third of women have urinary incontinence and up to one‐tenth have faecal incontinence after childbirth. Pelvic floor muscle training (PFMT) is commonly recommended during pregnancy and after birth for both prevention and treatment of incontinence.
This is an update of a review previously published in 2012.
Objectives
To determine the effectiveness of pelvic floor muscle training (PFMT) in the prevention or treatment of urinary and faecal incontinence in pregnant or postnatal women.
Search methods
We searched the Cochrane Incontinence Specialised Register (16 February 2017) and reference lists of retrieved studies.
Selection criteria
Randomised or quasi‐randomised trials in pregnant or postnatal women. One arm of the trial included PFMT. Another arm was no PFMT, usual antenatal or postnatal care, another control condition, or an alternative PFMT intervention.
Data collection and analysis
Review authors independently assessed trials for inclusion and risk of bias. We extracted data and checked them for accuracy. Populations included: women who were continent (PFMT for prevention), women who were incontinent (PFMT for treatment) at randomisation and a mixed population of women who were one or the other (PFMT for prevention or treatment). We assessed quality of evidence using the GRADE approach.
Main results
The review included 38 trials (17 of which were new for this update) involving 9892 women from 20 countries. Overall, trials were small to moderate sized, and the PFMT programmes and control conditions varied considerably and were often poorly described. Many trials were at moderate to high risk of bias. Other than two reports of pelvic floor pain, trials reported no harmful effects of PFMT.
Prevention of urinary incontinence: compared with usual care, continent pregnant women performing antenatal PFMT may have had a lower risk of reporting urinary incontinence in late pregnancy (62% less; risk ratio (RR) for incontinence 0.38, 95% confidence interval (CI) 0.20 to 0.72; 6 trials, 624 women; low‐quality evidence). Similarly, antenatal PFMT decreased the risk of urinary incontinence in the mid‐postnatal period (more than three to six months' postpartum) (29% less; RR 0.71, 95% CI 0.54 to 0.95; 5 trials, 673 women; moderate‐quality evidence). There was insufficient information available for the late (more than six to 12 months') postnatal period to determine effects at this time point.
Treatment of urinary incontinence: it is uncertain whether antenatal PFMT in incontinent women decreases incontinence in late pregnancy compared to usual care (RR 0.70, 95% CI 0.44 to 1.13; 3 trials, 345 women; very low‐quality evidence). This uncertainty extends into the mid‐ (RR 0.94, 95% CI 0.70 to 1.24; 1 trial, 187 women; very low‐quality evidence) and late (RR 0.50, 95% CI 0.13 to 1.93; 2 trials, 869 women; very low‐quality evidence) postnatal periods. In postnatal women with persistent urinary incontinence, it was unclear whether PFMT reduced urinary incontinence at more than six to 12 months' postpartum (RR 0.55, 95% CI 0.29 to 1.07; 3 trials; 696 women; very low‐quality evidence).
Mixed prevention and treatment approach to urinary incontinence: antenatal PFMT in women with or without urinary incontinence (mixed population) may decrease urinary incontinence risk in late pregnancy (26% less; RR 0.74, 95% CI 0.61 to 0.90; 9 trials, 3164 women; low‐quality evidence) and the mid‐postnatal period (RR 0.73, 95% CI 0.55 to 0.97; 5 trials, 1921 women; very low‐quality evidence). It is uncertain if antenatal PFMT reduces urinary incontinence risk late postpartum (RR 0.85, 95% CI 0.63 to 1.14; 2 trials, 244 women; low‐quality evidence). For PFMT begun after delivery, there was considerable uncertainty about the effect on urinary incontinence risk in the late postnatal period (RR 0.88, 95% CI 0.71 to 1.09; 3 trials, 826 women; very low‐quality evidence).
Faecal incontinence: six trials reported faecal incontinence outcomes. In postnatal women with persistent faecal incontinence, it was uncertain whether PFMT reduced incontinence in the late postnatal period compared to usual care (RR 0.68, 95% CI 0.24 to 1.94; 2 trials; 620 women; very low‐quality evidence). In women with or without faecal incontinence (mixed population), antenatal PFMT led to little or no difference in the prevalence of faecal incontinence in late pregnancy (RR 0.61, 95% CI 0.30 to 1.25; 2 trials, 867 women; moderate‐quality evidence). For postnatal PFMT in a mixed population, there was considerable uncertainty about the effect on faecal incontinence in the late postnatal period (RR 0.73, 95% CI 0.13 to 4.21; 1 trial, 107 women, very low‐quality evidence).
There was little evidence about effects on urinary or faecal incontinence beyond 12 months' postpartum. There were few incontinence‐specific quality of life data and little consensus on how to measure it. We found no data on health economics outcomes.
Authors' conclusions
Targeting continent antenatal women early in pregnancy and offering a structured PFMT programme may prevent the onset of urinary incontinence in late pregnancy and postpartum. However, the cost‐effectiveness of this is unknown. Population approaches (recruiting antenatal women regardless of continence status) may have a smaller effect on urinary incontinence, although the reasons for this are unclear. It is uncertain whether a population‐based approach for delivering postnatal PFMT is effective in reducing urinary incontinence. Uncertainty surrounds the effects of PFMT as a treatment for urinary incontinence in antenatal and postnatal women, which contrasts with the more established effectiveness in mid‐life women.
It is possible that the effects of PFMT might be greater with targeted rather than mixed prevention and treatment approaches and in certain groups of women. Hypothetically, for instance, women with a high body mass index are at risk factor for urinary incontinence. Such uncertainties require further testing and data on duration of effect are also needed. The physiological and behavioural aspects of exercise programmes must be described for both PFMT and control groups and how much PFMT women in both groups do, to increase understanding of what works and for whom.
Few data exist on faecal incontinence or costs and it is important that both are included in any future trials. It is essential that future trials use valid measures of incontinence‐specific quality of life for both urinary and faecal incontinence.
Keywords: Female, Humans, Pregnancy, Pelvic Floor, Exercise Therapy, Exercise Therapy/methods, Fecal Incontinence, Fecal Incontinence/prevention & control, Fecal Incontinence/therapy, Postnatal Care, Pregnancy Complications, Pregnancy Complications/prevention & control, Pregnancy Complications/therapy, Prenatal Care, Randomized Controlled Trials as Topic, Urinary Incontinence, Urinary Incontinence/prevention & control, Urinary Incontinence/therapy
How effective are pelvic floor muscle exercises undertaken during pregnancy or after birth for preventing or treating incontinence?
Review question
To assess whether doing pelvic floor muscle exercises (PFME) during pregnancy or after birth reduces incontinence. This is an update of a review published in 2012.
Background
More than one‐third of women experience unintentional (involuntary) loss of urine (urinary incontinence) in the second and third trimesters of pregnancy and about one‐third leak urine in the first three months after giving birth. About one‐quarter of women have some involuntary loss of flatus (wind) or faeces (anal incontinence) in late pregnancy and one fifth leak flatus or faeces one year after birth. PFME are commonly recommended by health professionals during pregnancy and after birth to prevent and treat incontinence. The muscles are strengthened and kept strong with regular PFME. Muscles are contracted several times in a row, more than once a day, several days a week and continued indefinitely.
How up‐to‐date is this review?
The evidence is current to 16 February 2017.
Study characteristics
We included 38 trials (17 new to this update) involving 9892 women from 20 countries. The studies included pregnant women or women who had delivered their baby within the last three months. Women reported leakage of urine, faeces, both urine or faeces, or no leakage. They were allocated randomly to receive PFME (to try and prevent incontinence or as a treatment for incontinence) or not and the effects were compared.
Study funding sources
Nineteen studies were publicly funded. One received grants from public and private sources. Three studies received no funding and 15 did not declare funding sources.
Key results
Pregnant women without urine leakage who did PFME to prevent leakage: women may report less urine leakage in late pregnancy and three to six months after childbirth. There was not enough information to determine whether these effects continued beyond the first year after the baby's birth.
Women with urine leakage, pregnant or after birth, who did PFME as a treatment: it was uncertain whether doing PFME during pregnancy reduced leakage in late pregnancy or in the year following childbirth. It was unclear if doing PFME helped women with leakage after giving birth.
Women with or without urine leakage (mixed group), pregnant or after birth, who did PFME to either prevent or treat leakage: women who began exercising during pregnancy were less likely to report leakage in late pregnancy and up to six months after birth, but it was uncertain if the effect lasted at one year following birth. For women who started PFME after delivery, the effect on leakage one year after birth was uncertain.
Leakage of faeces: few studies (only six) had evidence about leakage of faeces. One year after delivery, it was uncertain if PFME helped decrease leakage of faeces in women who started exercising following childbirth. It was also uncertain if women with or without leakage of faeces (mixed group) who started PFME while pregnant were less likely to leak faeces in late pregnancy or up to one year after birth.
There was little information about how PFME may affect leakage‐related quality of life. There were two reports of pelvic floor pain but no other harmful effects of PFME were noted. It is unknown if PFMEs offer value for money because no study had a health economics analysis. It is unknown if PFME offer value for money as no health economics data were identified.
Quality of the evidence
Overall, studies were not large and most had design problems, including limited details on how women were randomly allocated into groups, and poor reporting of measurements. Some of the problems were expected because it was impossible to blind health professionals or women to whether they were exercising or not. The PFME differed considerably between studies and were often poorly described. Evidence quality was generally low to very low.
Summary of findings
Summary of findings for the main comparison.
Antenatal pelvic floor muscle training compared to control for prevention of urinary and faecal incontinence
| Antenatal pelvic floor muscle training compared to control for prevention of urinary and faecal incontinence | ||||||
|
Patient or population: pregnant women who were continent when randomised Setting: hospital or outpatient settings in Canada, Italy, Mexico, Norway, Spain, Thailand, Turkey, UK and USA Intervention: antenatal PFMT Comparison: control (no PFMT or usual care) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with control | Risk with antenatal PFMT | |||||
| Urinary incontinence in late pregnancy | Study population | RR 0.38 (0.20 to 0.72) | 624 (6 RCTs) | ⊕⊕⊝⊝ Low1 | Upper and lower limits of the CI of summary statistic suggest clinical importance. | |
| 421 per 1000 | 160 per 1000 (84 to 303) | |||||
| Urinary incontinence mid‐postnatal period (> 3‐6 months) | Study population | RR 0.71 (0.54 to 0.95) | 673 (5 RCTs) | ⊕⊕⊕⊝ Moderate2 | Risk reduction is a clinically important effect but the upper limit of the CI is close to no effect. | |
| 251 per 1000 | 179 per 1000 (136 to 239) | |||||
| Urinary incontinence late postnatal period (> 6‐12 months) | Study population | RR 1.20 (0.65 to 2.21) | 44 (1 RCT) | ⊕⊕⊝⊝ Low3 | Wide CI including no effect. | |
| 440 per 1000 | 528 per 1000 (286 to 972) | |||||
| Faecal incontinence in late pregnancy | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Faecal incontinence mid‐postnatal period (> 3‐6 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Faecal incontinence late postnatal period (> 6‐12 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Incontinence‐specific quality of life assessed with: ICIQ‐SF Scale from: 0 to 10 (worse) | Mean 2.66, SD 4.1 | Mean 0.24, SD 1.2 | MD 2.42 lower (3.32 lower to 1.52 lower) | 152 (1 RCT) | ⊕⊕⊕⊝ Moderate4 | Measured in late postnatal period. Upper and lower limits of the CI of summary statistic suggest clinical importance in ICIQ‐SF (Nyström 2015). |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; ICIQ‐SF: International Consultation on Incontinence ‐ Short Form; MD: mean difference; PFMT: pelvic floor muscle training; RCT: randomised controlled trial; RR: risk ratio; SD: standard deviation. | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Downgraded two levels for serious inconsistency and imprecision (multiple small RCTs, fewer than 300 events, heterogeneous intervention and control groups).
2Downgraded one level for serious imprecision (multiple small RCTs, fewer than 300 events).
3Downgraded two levels for very serious imprecision (single, small trial with wide confidence interval).
4Downgraded one level for serious imprecision (single trial, fewer than 300 events).
The outcome measures relate to the presence of incontinence symptoms rather than absence. Symptoms of urinary and faecal incontinence were measured based on self‐report.
Summary of findings 2.
Antenatal pelvic floor muscle training compared to control for treatment of urinary and faecal incontinence
| Antenatal pelvic floor muscle training compared to control for treatment of urinary and faecal incontinence | ||||||
|
Patient or population: pregnant women who were incontinent when randomised Setting: health services or obstetric clinics in Brazil, Canada, the Netherlands and Turkey Intervention: antenatal PFMT Comparison: control (usual care) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with control | Risk with antenatal PFMT | |||||
| Urinary incontinence in late pregnancy | Study population | RR 0.70 (0.44 to 1.13) | 345 (3 RCTs) | ⊕⊝⊝⊝ Very low1 | Wide CI including no effect. | |
| 776 per 1000 | 543 per 1000 (341 to 877) | |||||
| Urinary incontinence mid‐postnatal period (> 3‐6 months) | Study population | RR 0.94 (0.70 to 1.24) | 187 (1 RCT) | ⊕⊝⊝⊝ Very low2 | Wide CL including no effect. | |
| 528 per 1000 | 496 per 1000 (369 to 654) | |||||
| Urinary incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.50 (0.13 to 1.93) | 869 (2 RCTs) | ⊕⊝⊝⊝ Very low3 | Wide CI including no effect. | |
| 232 per 1000 | 116 per 1000 (30 to 448) | |||||
| Faecal incontinence in late pregnancy | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Faecal incontinence mid‐postnatal period (> 3‐6 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Faecal incontinence late postnatal period (> 6‐12 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Incontinence‐specific quality of life (ICIQ‐SF) Scale from: 0 to 10 (worse) | Mean 4.7, SD 5.6 | Mean 1.2, SD 2.5 | MD 3.5 lower (6.13 lower to 0.87 lower) | 41 (1 RCT) | ⊕⊕⊝⊝ Low4 | MD suggests clinically important effect but the upper limit of the CI is close to no effect. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; ICIQ‐SF: International Consultation on Incontinence ‐ Short Form; MD: mean difference; PFMT: pelvic floor muscle training; RCT: randomised controlled trial; RR: risk ratio; SD: standard deviation. | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Downgraded three levels due to serious risk of selection bias (one trial with heavy weighting in the pooled estimate at high risk), inconsistency and indirectness, and very serious imprecision (fewer than 300 events, wide confidence interval, two trials without any details about PFMT interventions).
2Downgraded three levels due to serious risk of selection bias, indirectness and imprecision (singe trial, fewer than 300 events, wide confidence interval, no details about PFMT interventions).
3Downgraded three levels due to very serious risk of selection bias, inconsistency and imprecision (fewer than 300 events, wide confidence interval) and serious indirectness (no details about the PFMT intervention in one trial with about half the weighting in the pooled estimate).
4Downgraded two levels due to serious indirectness and imprecision (single trial, fewer than 300 participants, wide confidence interval).
The outcome measures relate to the presence of incontinence symptoms rather than absence. As this comparison addresses the effect of PFMT for treatment of existing continence symptoms, the data are "negative," that is continuing incontinence rather than cure. Symptoms of urinary and faecal incontinence were measured based on self‐report.
Summary of findings 3.
Antenatal pelvic floor muscle training compared to control for mixed prevention and treatment of urinary and faecal incontinence
| Antenatal pelvic floor muscle training compared to control for mixed prevention and treatment of urinary and faecal incontinence | ||||||
|
Patient or population: pregnant women some of who were incontinent symptoms and some who were not when randomised Setting: health services, obstetric clinics or hospitals in Brazil, China, France, Italy, Norway, UK or USA Intervention: antenatal PFMT Comparison: control (no PFMT, usual care or unspecified control) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with control | Risk with antenatal PFMT | |||||
| Urinary incontinence in late pregnancy | Study population | RR 0.74 (0.61 to 0.90) | 3164 (9 RCTs) | ⊕⊕⊝⊝ Low1 | RR suggests clinically important effect but the upper limit of the CI suggests lack of clinical importance. | |
| 575 per 1000 | 425 per 1000 (351 to 517) | |||||
| Urinary incontinence mid‐postnatal period (> 3‐6 months) | Study population | RR 0.73 (0.55 to 0.97) | 1921 (5 RCTs) | ⊕⊝⊝⊝ Very low2 | RR suggests clinically important effect but the upper limit of the CI suggests lack of clinical importance. | |
| 363 per 1000 | 265 per 1000 (200 to 352) | |||||
| Urinary incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.85 (0.63 to 1.14) | 244 (2 RCTs) | ⊕⊕⊝⊝ Low3 | RR suggests clinically important effect but the CI includes no effect. | |
| 448 per 1000 | 381 per 1000 (282 to 511) | |||||
| Faecal incontinence in late pregnancy | Study population | RR 0.61 (0.30 to 1.25) | 867 (2 RCTs) | ⊕⊕⊕⊝ Moderate4 | Wide CI including no effect. | |
| 43 per 1000 | 26 per 1000 (13 to 54) | |||||
| Faecal incontinence mid‐postnatal period (> 3‐6 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Faecal incontinence late postnatal period (> 6‐12 months) | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| Incontinence‐specific quality of life late postnatal period (> 6‐12 months) (ICIQ‐SF) Scale from: 0 to 10 (worse) | Mean 2.1, SD 3.3 | Mean 1.9, SD 3.7 | MD 0.2 lower (1.2 lower to 0.8 higher) | 190 (1 RCT) | ⊕⊕⊝⊝ Low5 | MD and CI suggest lack of clinically important effect. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; ICIQ‐SF: International Consultation on Incontinence ‐ Short Form; MD: mean difference; PFMT: pelvic floor muscle training; RCT: randomised controlled trial; RR: risk ratio; SD: standard deviation. | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Downgraded two levels due to serious inconsistency (statistically significant heterogeneity) and indirectness (limited details about PFMT intervention in two trials with more than one‐quarter of the weighting in the pooled estimate).
2Downgraded three levels due to serious risk of selection bias (no information about random allocation concealment in three trials carrying more than 50% of weighting in the pooled estimate), serious imprecision (statistically significant heterogeneity) and serious indirectness (includes two trials carrying about 40% of the weighting in the pooled estimate with no information about PFMT intervention).
3Downgraded two levels due to serious indirectness (no information about PFMT in one trial with more than two‐thirds of the weighting in the pooled estimate) and serious imprecision (fewer than 300 event).
4Downgraded one level due to serious imprecision (single trial with fewer than 300 events).
5Downgraded two levels due to serious indirectness (single trial, no information about PFMT intervention) and serious imprecision (fewer than 300 events).
The outcome measures relate to the presence of incontinence symptoms rather than absence. For those comparisons that addressed the effect of PFMT for treatment of existing continence symptoms, the data were "negative," that is continuing incontinence rather than cure. Symptoms of urinary and faecal incontinence were measured based on self‐report.
Summary of findings 4.
Postnatal pelvic floor muscle training compared to control for treatment of urinary and faecal incontinence
| Postnatal pelvic floor muscle training compared to control for treatment of urinary and faecal incontinence | ||||||
|
Patient or population: postnatal women who were incontinent when randomised Setting: health services or obstetric clinics in Canada, Republic of Korea, New Zealand and UK Intervention: postnatal PFMT Comparison: control (no PFMT or usual care) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with control | Risk with postnatal PFMT | |||||
| Urinary incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.55 (0.29 to 1.07) | 696 (3 RCTs) | ⊕⊝⊝⊝ Very low1 | RR suggests clinically important effect but the CI includes no effect. | |
| 724 per 1000 | 398 per 1000 (210 to 775) | |||||
| Faecal incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.68 (0.24 to 1.94) | 620 (2 RCTs) | ⊕⊝⊝⊝ Very low2 | RR suggests clinically important effect but the CI includes no effect. | |
| 137 per 1000 | 93 per 1000 (33 to 266) | |||||
| Incontinence‐specific quality of life assessed with: BFLUTS; 34 items (higher score worse) | Mean 21.22, SD 2.11 | Mean 19.56, SD 1.88 | MD 1.66 lower (3.51 lower to 0.19 higher) | 18 (1 RCT) | ⊕⊝⊝⊝ Very low3 | Wide CI including no effect. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). BFLUTS: British Female Lower Urinary Tract Symptoms questionnaire; CI: confidence interval; MD: mean difference; PFMT: pelvic floor muscle training; RCT: randomised controlled trial; RR: risk ratio; SD: standard deviation. | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Downgraded three levels due to very serious risk of selection bias (two trials with 90% of weighting in pooled estimate at high risk) and inconsistency (statistically significant heterogeneity), and serious indirectness (two trials with 90% of weighting in pooled estimate provide insufficient information about the intervention).
2Downgraded three levels due to very serious risk of selection bias (two trials with 100% of weighting in pooled estimate at high risk), inconsistency (statistically significant heterogeneity) and imprecision (fewer than 300 events, wide confidence interval) and serious indirectness (neither trial provides sufficient information about the intervention).
3Downgraded three levels due to very serious risk of selection bias and imprecision (fewer than 300 events, wide confidence interval).
The outcome measures relate to the presence of incontinence symptoms rather than absence. As this comparison addresses the effect of PFMT for treatment of existing continence symptoms, the data are "negative," that is continuing incontinence rather than cure. Symptoms of urinary and faecal incontinence were measured based on self‐report.
Summary of findings 5.
Postnatal pelvic floor muscle training compared to control for mixed prevention and treatment of urinary and faecal incontinence
| Postnatal pelvic floor muscle training compared to control for mixed prevention and treatment of urinary and faecal incontinence | ||||||
|
Patient or population: postnatal women some of whom had incontinent symptoms and some of whom had not when randomised Setting: health services or hospitals in Australia, China and Switzerland Intervention: postnatal PFMT Comparison: control (no PFMT or usual care) | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with control | Risk with postnatal PFMT | |||||
| Urinary incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.88 (0.71 to 1.09) | 826 (3 RCTs) | ⊕⊝⊝⊝ Very low1 | Wide CI including no effect. | |
| 294 per 1000 | 212 per 1000 (115 to 400) | |||||
| Faecal incontinence late postnatal period (> 6‐12 months) | Study population | RR 0.73 (0.13 to 4.21) | 107 (1 RCT) | ⊕⊝⊝⊝ Very low2 | Wide CI including no effect. | |
| 54 per 1000 | 39 per 1000 (7 to 226) | |||||
| Incontinence‐specific quality of life | Study population | ‐ | (0 studies) | ‐ | Not reported. | |
| ‐ | ‐ | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; PFMT: pelvic floor muscle training; RCT: randomised controlled trial; RR: risk ratio. | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Downgraded three levels due to serious inconsistency (statistically significant heterogeneity) and imprecision (fewer than 300 events, wide confidence interval).
2Downgraded three levels due to very serious risk of selection bias and imprecision (fewer than 300 events, wide confidence interval) and serious indirectness (no information about the PFMT intervention).
The outcome measures relate to the presence of incontinence symptoms rather than absence. For those comparisons that address the effect of PFMT for treatment of existing continence symptoms, the data are "negative," that is continuing incontinence rather than cure. Symptoms of urinary and faecal incontinence were measured based on self‐report.
Background
Accumulating epidemiological evidence suggests that women who have had a baby are at increased risk of developing urinary incontinence. It seems that both pregnancy and delivery are risk factors (Foldspang 1999; Milsom 2017; Rortveit 2003a; Rortveit 2003b; Viktrup 2006). Similarly, these women seem to be at greater risk of faecal incontinence, particularly those who have had vaginal deliveries (Eason 2002; MacArthur 2001; Pollack 2004; Sultan 1999).
Description of the condition
Urinary incontinence
Urinary incontinence (involuntary leakage of urine) is a common problem amongst adults living in the community (Milsom 2017). It is more frequent in women and pregnancy or the postnatal period may be the first time many women experience urinary incontinence. Stress urinary incontinence (involuntary urine leakage with physical exertion) and urgency urinary incontinence (involuntary leakage associated with, or immediately following, a sudden compelling need to void) are the two most common types of urine leakage in women. Many women have symptoms of both stress and urgency urinary incontinence. This is called mixed urinary incontinence. Of these types, stress urinary incontinence is most commonly associated with pregnancy and the postnatal period, although there is a small but significant increase in risk of urgency urinary incontinence (Milsom 2017).
It seems that the prevalence of urinary incontinence increases during pregnancy (particularly in the second trimester) and then gradually decreases during the first postpartum year (Milsom 2017). Variation is evident in prevalence estimates of all types of urinary incontinence during pregnancy but this may be as high as 58%, with stress urinary incontinence affecting about 31% of nulliparous women and 42% of parous women (Wesnes 2007). The prevalence of persistent urinary incontinence in the first three months following delivery is approximately 30% (Thom 2010).
Findings from moderate‐ to large‐sized cohorts of women suggest that factors associated with a greater risk of postpartum urinary incontinence are:
parity (Milsom 2017);
higher maternal body mass index (BMI) (Durnea 2017; Gyhagen 2013; Pizzoferrato 2014; Quiboeuf 2016; Svare 2014);
age (Quiboeuf 2016);
urinary incontinence before or during pregnancy (Durnea 2017; Gartland 2016; Pizzoferrato 2014; Svare 2014);
vaginal delivery (Gartland 2016; Gyhagen 2013);
operative vaginal deliveries or perineal or anal sphincter trauma (Durnea 2017; Gartland 2012; Svare 2014);
high birthweight of the baby (Gyhagen 2013; Pizzoferrato 2014; Wesnes 2017).
These associations have been observed anywhere between four to six months' postpartum through to 12 to 20 years following first delivery (Gartland 2012; Gyhagen 2013; Pizzoferrato 2014; Wesnes 2017).
Faecal incontinence
Faecal incontinence (involuntary loss of solid or liquid stool) is less common than urinary incontinence but is particularly distressing both psychologically and physically (Johanson 1996). Women may also experience involuntary loss of flatus (wind). The term anal incontinence is used to encompass involuntary loss of faeces or flatus.
The prevalence of faecal incontinence is difficult to estimate as the definition of this condition varies between studies, different assessment tools are used and because women may be reluctant to admit to faecal incontinence (MacArthur 2013). In addition, variation is also apparent in the time points at which faecal incontinence is measured during pregnancy and following delivery and in which groups of women (e.g. primiparous versus multiparous). For the purpose of this review, faecal incontinence was considered a generic term that encompassed involuntary loss of solid stool, liquid stool, flatus, or a combination of these.
Some form of faecal incontinence may be present during pregnancy in first‐time mothers, with a prevalence anywhere up to 12% to 35% for flatal incontinence and 2.0% to 9.5% for loss of formed stool (Johannessen 2016; Svare 2016). Persistent symptoms at three months' postpartum may be 19% to 46% for flatus and 2.4% to 8.0% for the involuntary loss of formed stool (Brown 2012; Signorello 2000). In the longer term, these rates seem to persist, with about 31% of primiparous women reporting involuntary loss of flatus at six and 12 years after delivery and 9% to 12% reporting loss of formed stool (MacArthur 2013). One systematic review by Bols 2010 suggested that the aetiological factor most strongly associated with postpartum faecal incontinence is a third‐ or fourth‐degree rupture of the external anal sphincter.
Description of the intervention
Pelvic floor muscle training
Pelvic floor muscle training (PFMT) refers to the performance of repeated voluntary contractions of the pelvic floor muscles (PFM), according to a protocol that outlines the frequency, intensity and progression of exercises, as well as the duration of the training period. A PFMT programme typically includes one or more sets of exercises per day, performed on at least several days of the week, for at least eight weeks. It is recommended that initial training be followed by maintenance PFM exercises to ensure duration of effect in the longer term (Bø 2004; Mørkved 2014).
In many countries, it is common for women to receive information about, and encouragement to perform, some PFM exercises during pregnancy and after delivery. During pregnancy, information on PFMT may be received from a health professional or obtained from other sources (e.g. leaflets and websites) but this advice may not lead to effective training if the exercise parameters and behaviour are insufficient. Nevertheless, we continued to use the term PFMT to make the review easier to read.
For women who are continent during pregnancy, PFMT is undertaken to prevent leakage. Women who develop symptoms of incontinence during pregnancy or postpartum may be referred to a health professional specifically for treatment and supervision of exercise.
Prevention of urinary and faecal incontinence with PFMT
Prevention is primary, secondary or tertiary prevention (Hensrud 2000). Primary prevention aims to remove the causes of a disease. As an example, a trial that compares two obstetric practices (e.g. liberal versus restrictive episiotomy policies) and the effect on the prevalence of postnatal incontinence amongst previously continent women is a primary prevention trial. Secondary prevention aims to detect asymptomatic dysfunction and treat it early to stop progression. A trial that compares a treatment to improve the muscular supports of the bladder with no treatment in postnatal women who had weak PFM but no urinary incontinence symptoms is classified as a secondary prevention trial. Tertiary prevention is the treatment of existing symptoms to prevent progression of disease.
Clinically, it may be difficult to screen all potential trial participants to see if a disease process is either absent altogether or present but asymptomatic. In addition, with a condition such as incontinence there might be more than one factor that could contribute to development of the problem, for example denervation, fascial deficits and poor muscle function. It is impractical to screen for all possible factors and, in many cases, there are no reliable or valid clinical tests available. Consequently, prevention trials may enrol people purely on the basis of the absence of symptoms. This is commonly the case in incontinence studies and the findings of these studies are probably a combination of primary and secondary prevention effects. This review makes no attempt to distinguish between primary and secondary effects and considers them together.
Treatment of urinary and faecal incontinence with PFMT
PFMT for the treatment of urinary incontinence was popularised by Arnold Kegel (Kegel 1948). However, in one review of the literature prior to 1949, Bø 2004 identified several records of the use of PFM exercise. PFMT was principally recommended in the treatment of stress and mixed urinary incontinence but was increasingly part of treatment offered to women with urgency urinary incontinence. The use of PFMT in the treatment of urinary incontinence is based on two functions of the PFM: support of the pelvic organs and a contribution to the sphincteric closure mechanism of the urethra. More detail about how PFMT might work to treat urinary incontinence can be found in the background to a previous Cochrane review of PFMT (Dumoulin 2014).
PFMT is used in the treatment of faecal incontinence, although there are fewer studies of its effectiveness than for urinary incontinence. Theoretically, the external anal sphincter muscle (which is continuous with the puborectalis muscle component of the PFM) could be trained in a similar way and it is unclear whether it is possible for people to know the difference between a voluntary external anal sphincter contraction and a voluntary PFM contraction (Norton 2012).
PFMT is recommended as a first‐line therapy for urinary incontinence (Abrams 2017; Dumoulin 2014). However, a wide range of options is available to treat urinary and faecal incontinence, including conservative interventions (PFM rehabilitation including use of electrical stimulation and biofeedback), lifestyle interventions, bladder training, anti‐incontinence devices, pharmaceutical interventions and surgery.
How the intervention might work
There are a variety of plausible reasons why PFMT might help prevent urinary incontinence. For example, trained muscle might be less prone to injury and previously trained muscle might be easier to retrain after damage as the appropriate motor patterns are already learned. It may be that previously trained muscle has a greater reserve of strength so that injury to the muscle itself, or its nerve supply, does not cause sufficient loss of muscle function to reach the threshold where reduced urethral closure pressure results in leakage. During pregnancy, training the PFM might help to counteract the increased intra‐abdominal pressure caused by the growing fetus, the hormonally mediated reduction in urethral closure pressure, and the increased laxity of fascia and ligaments in the pelvic area. A similar rationale might be used to support the use of PFMT to improve the function of the external anal sphincter and thus prevent faecal incontinence.
Essentially, a PFMT programme may be prescribed for women to:
increase strength (the maximum force generated by a muscle in a single contraction);
increase endurance (ability to contract repetitively, or to sustain a single contraction over time);
co‐ordinate muscle activity (such as the precontraction of PFM prior to a rise in intra‐abdominal pressure, or to suppress urgency);
address a combination of these (Bø 2014).
However, based on the plausible reasons above, strength training tends to be emphasised for pregnant and postnatal women. Characteristic features of strength training include low numbers of repetitions with high loads and one way to increase load is to increase the amount of voluntary effort with each near maximal voluntary contraction (Bø 2014).
There is a subgroup of women where there are particular uncertainties about whether the intervention might work and how it might work (Hilde 2013). These are women with avulsion (separation) of the PFM from the pelvic wall or other major defects in the PFM that are palpated or seen on imaging (e.g. ultrasound, magnetic resonance imaging). It is possible that these women might benefit from PFMT after the birth, helping the injury 'heal' (Hilde 2013). However, it is also possible that PFMT does not assist the return of function if the muscle no longer has the attachments that anatomically enable it to compress and lift the urethra with a muscle contraction.
Why it is important to do this review
Urinary and faecal incontinence are experienced by many women during pregnancy and following childbirth and can have a significant impact on quality of life (Handa 2007; Rogers 2017). With the high prevalence of incontinence in pregnant and postnatal women, this is potentially a 'costly' condition. There are direct costs borne by women, such as buying continence products, laundry costs and visits to a general practitioner or continence service. Less direct but no less important costs for women may include the social or physical activity limits they adopt to prevent embarrassment of leakage in public. Preventing or treating the condition with PFMT is likely to incur considerable cost to health services because supervised (e.g. several one‐to‐one contacts with a health professional) conservative therapies such as PFMT are more expensive than usual care (Wagner 2017). However, cost‐effectiveness modelling of non‐surgical treatments for stress urinary incontinence in women found more intensive forms of PFMT were likely to be worthwhile (Imamura 2010). It is unclear if it would offer greater value for money to prevent the condition than treat it.
Although PFMT is recommended as the first choice of conservative management for incontinence, uncertainties about its effectiveness in antenatal and postnatal women remain (Dumoulin 2017), such as whether PFMT might be more effective if targeted to specific groups, or more effective as a prevention or treatment intervention. Also, with increasing pressure on constrained healthcare budgets worldwide, it is important to clarify whether the intervention offers value for money to ensure efficient allocation of resources.
This review is a major update of Boyle 2012, which examined the effectiveness of PFMT for the prevention, treatment or mixed prevention and treatment of urinary and faecal incontinence in antenatal and postnatal women. Uncertainties identified in previous iterations of the review appear to have contributed to completion of some moderate‐ to large‐sized randomised controlled trials in this population (e.g. Fritel 2015). As several new trials have now been published with findings that could change the review outcomes, an update that was rigorous in terms of methods and analyses was required.
Since the last update of this review in 2012, other authors have published systematic reviews that address the effects of PFMT during pregnancy and after delivery for the prevention and treatment of urinary incontinence and the effects of antenatal PFMT on labour and delivery outcomes (Du 2015; Mørkved 2014).
Objectives
To determine the effectiveness of pelvic floor muscle training (PFMT) in the prevention or treatment of urinary and faecal incontinence in pregnant or postnatal women.
We wished to test the following comparisons.
-
Antenatal PFMT versus no PFMT, usual care or other control condition for the:
primary or secondary prevention of incontinence;
treatment of incontinence;
mixed prevention or treatment of incontinence (i.e. treating a mixed population with PFMT).
-
Postnatal PFMT versus no PFMT, usual care, or other control condition for the:
treatment of incontinence;
mixed prevention or treatment of incontinence.
Methods
Criteria for considering studies for this review
Types of studies
Randomised (including cluster and cross‐over) controlled trials and quasi‐randomised studies (e.g. allocation by alternation) were eligible for inclusion. We excluded other forms of controlled clinical trials.
Types of participants
Trials that recruited antenatal (i.e. pregnant) or postnatal women (i.e. women immediately following delivery or women with persistent urinary or faecal incontinence symptoms up to three months after their most recent delivery). Women could be with or without urinary, faecal, or both urinary and faecal incontinence symptoms at recruitment.
We compared three populations of women.
Prevention trials in antenatal women who were continent when randomised.
Treatment trials in antenatal or postnatal women who were incontinent when randomised.
Mixed prevention and treatment trials in antenatal or postnatal women where some women had incontinence symptoms and some did not when randomised.
Close attention was given to the distinction between treatment and prevention trials because the effect of PFMT might differ for these two purposes. For the trials that recruited antenatal or postnatal women, whether they had symptoms of incontinence or not, the PFMT intervention was a prevention strategy for the non‐symptomatic women and treatment for symptomatic women. The two effects could not be distinguished in these trials.
Types of interventions
One arm of all eligible trials included a PFMT programme to improve the function of the PFM, the external anal sphincter or both. PFMT was a programme of repeated voluntary PFM contractions, although this was a limited definition compared with the fuller ideal (Dumoulin 2014). All types of PFMT were considered, including variations in the purpose and timing of PFMT (e.g. PFMT for strengthening, PFMT for urgency suppression), ways of teaching PFMT, types of contractions (fast or sustained) and number of contractions.
Acceptable control interventions were usual antenatal and postnatal care, placebo treatment or no treatment. Usual antenatal or postnatal care in many countries included advice about PFMT. We included studies in which the control group had, or might have, received PFMT advice providing the PFMT arm was more intensive in some way than the control arm. For example, in the PFMT arm, women were taught the exercises by a health professional, whereas usual care involved distribution of a leaflet about PFMT on the postnatal wards.
Trials in which PFMT was combined with other physical therapy modalities such as biofeedback, electrical stimulation or multi‐modal exercise programmes were included. Studies where advice on strategies for symptoms of urgency and frequency (but without a scheduled voiding regimen characteristic of bladder training) were also eligible for inclusion. Trials in which PFMT was combined with another stand‐alone therapy such as bladder training or drug therapy (e.g. anticholinergic drug) were excluded. Trials of electrical stimulation (without PFMT) were excluded.
Types of outcome measures
With regards to prevention, it seemed that the most appropriate measure of outcome was the self‐reported absence of urinary or faecal incontinence symptoms. For treatment, a wider range of outcomes was considered important, although the self‐reporting of cure or improvement in urinary or faecal incontinence symptoms was thought to be most important. These outcomes are the opposite of each other, being either the presence or absence of incontinence symptoms. For consistency throughout the review, we chose to report presence of incontinence symptoms rather than absence. For the comparisons that addressed the effect of PFMT for treatment of existing continence symptoms, readers should be aware that the data were 'negative,' that is continuing incontinence rather than cure.
Primary outcomes
Self‐reported urinary or faecal incontinence.
Incontinence‐specific quality of life (e.g. International Consultation on Incontinence Questionnaire (ICIQ; 4 items, higher score worse), Incontinence Impact Questionnaire (IIQ; 30 items, higher score worse), Urogenital Distress Inventory (UDI; 19 items, higher score worse ) (Avery 2004; Avery 2007; Shumaker 1994).
Secondary outcomes
-
Women's observations:
severity of incontinence (e.g. Incontinence Index score, slight, moderate or severe (Sandvik 1993)).
-
Quantification of symptoms:
number of urinary or faecal incontinence episodes.
-
Clinician's measures:
loss of urine under stress test (e.g. cough or pad test).
-
Other quality of life and health status measures:
psychological measures (e.g. Hospital Anxiety and Depression Score (Zigmond 1983));
general health status (e.g. 36‐item Short Form (SF‐36) (Ware 1993)).
-
Health economics:
costs of intervention(s);
resource implications of differences in outcomes (e.g. differences in number of doctor visits, or referrals);
formal economic analysis (cost effectiveness, cost utility).
-
Adverse effects:
discomfort or pain associated with PFMT.
-
Other outcomes:
labour and delivery outcome (e.g. type of delivery, perineal trauma, episiotomy, length of second stage) for women who did antenatal PFMT;
sexual function;
pelvic organ prolapse;
non‐prespecified outcomes that were judged important when performing the review.
While not outcomes per se, we also extracted data on two particular variables that might help explain variations in PFMT effect:
PFM function (e.g. electromyography, vaginal or anal squeeze pressures);
Treatment adherence (e.g. surrogates such as class attendance, and more direct measures such as home exercise frequency).
Search methods for identification of studies
We imposed no restrictions on language of publication, publication status (i.e. full publication, grey literature, etc.) or any other restrictions on the searches described below.
Electronic searches
We drew on the search strategy developed for Cochrane Incontinence. We identified relevant trials from the Cochrane Incontinence Specialised Register, which is also described under the Cochrane Incontinence module in the Cochrane Library. The register contains trials identified from the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, MEDLINE In‐Process, MEDLINE Epub Ahead of Print, CINAHL, ClinicalTrials.gov, World Health Organization International Clinical Trials Registry Platform (WHO ICTRP), UK Clinical Research Network Portfolio and handsearching of journals and conference proceedings. Some of the trials in the Cochrane Incontinence Specialised Register are also contained in CENTRAL. The date of the last search was 16 February 2017.
The terms used to search the Cochrane Incontinence Specialised Register are given in Appendix 1.
Searching other resources
We searched for other possible relevant trials in the reference lists of relevant articles. We performed no tailored search for health economics studies.
Data collection and analysis
Selection of studies
Two review authors assessed all potentially eligible studies without prior consideration of the results. We resolved any disagreements by discussion and, where these were not resolved, a third review author had final responsibility. We included only randomised or quasi‐randomised controlled trials, and excluded trials that made comparisons other than those prespecified. Excluded studies are listed, with reasons for their exclusion, in the Characteristics of excluded studies.
Data extraction and management
Two review authors independently undertook data extraction onto a proforma and cross‐checked them. We resolved any differences by discussion. Where trial data were possibly collected but not reported, or data were reported in a form that could not be used in the formal comparisons, we sought further clarification from the trialists. We processed all included trial data as described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Assessment of risk of bias in included studies
Two review authors independently evaluated the methodological quality of the included trials using the 'Risk of bias' tool developed for Cochrane. We considered random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data and other bias and deemed each category at low, high or unclear risk of bias. Where there was insufficient information to make a clear decision, trials were rated at 'unclear risk.' Any disagreements were resolved by discussion.
Allocation (selection bias)
When considering random sequence bias, we assessed whether the method used to generate the allocation sequence in each study would allow an assessment of whether it produced comparable groups. We assessed the method as:
low risk of bias: any truly random process such as computer‐generated random number sequences;
high risk of bias: any non‐random process such as allocation by birth date or bed number;
unclear risk of bias.
For assessing allocation concealment, we determined the methods to conceal allocation to interventions prior to assignment and whether intervention allocation could have been foreseen in advance or during recruitment, or changed after assignment. We assessed the methods as:
low risk of bias: all forms of remote or web‐based allocation and sequentially numbered, sealed and opaque envelopes;
high risk of bias: open random allocation, envelopes where not all the above criteria were met (not sequentially numbered, unsealed, non‐opaque), all methods of alternation;
unclear risk of bias.
Blinding (performance bias and detection bias)
We did not have any criteria for performance bias as it was not considered feasible due to the nature of the intervention to blind the personnel or participants to group allocation. It is likely that this lack of blinding would unfortunately influence the results of the review.
We did not have any criteria for detection bias as it was not considered feasible to blind participants to the assessment of the two a priori outcomes of this review (prevalence of incontinence and incontinence quality of life) as both were self‐reported. We assessed blinding separately for other outcomes, such as the pad test and PFM function measures.
Incomplete outcome data (attrition bias)
For each outcome, we described the completeness of data, including attrition and exclusions from the analysis. In making a judgement about attrition bias, we considered the:
proportion of the total sample lost to follow‐up and the adequacy of any imputation methods used for missing data;
similarity in proportion of losses by group;
whether reasons were provided for losses and whether these differed by group;
if participants were analysed in the group to which they were assigned.
We assessed the methods as:
low risk of bias: trials with 10% or less loss to follow‐up and without a differential loss to follow‐up;
high risk of bias: trials with more than 20% loss to follow‐up without appropriate imputation methods or trials in which participants were not analysed in the group to which they were randomised;
unclear risk of bias: when the proportion of dropouts was between 10% and 20% without appropriate imputation methods (with no major differential or lack of similar reasons between groups) or when there was no reporting of losses to follow‐up.
Selective reporting (reporting bias)
For each included trial, we determined the possibility of selective outcome reporting bias and described what we found based on the following criteria:
low risk of bias: it was clear that all of the trial's prespecified outcomes were reported;
high risk of bias: not all of the trial's prespecified outcomes were reported, a primary outcome was not prespecified, outcomes of interest to the review and for which data were collected, were reported incompletely and so could not be used;
unclear risk of bias: a lack of detail in reporting made it difficult to assess whether all prespecified outcomes were presented.
Other bias
For each included study, we described any important concerns we had about other possible sources of bias that had not previously been considered in the categories above. In particular, we looked for a declaration of conflict of interest and the funding source. Other sources of bias were reported in the Characteristics of included studies.
Measures of treatment effect
For categorical outcomes, we related the numbers reporting an outcome to the numbers at risk in each group to derive a risk ratio (RR) and its 95% confidence interval (CI). For continuous variables, we used means and standard deviations (SD) to derive mean differences (MD). Where possible, data from different studies were pooled using a fixed‐effect model.
Some trials measured outcomes at more than one time point, usually in trials where PFMT began antenatally. There were some differences in the timing of outcome measures but, for the meta‐analysis, timing seemed to fall into the following clinical categories:
late pregnancy (from 20 weeks' gestation up to delivery);
early postnatal (zero to three months after delivery);
mid‐postnatal (more than three to six months after delivery);
late postnatal (more than six to 12 months after delivery);
medium term (more than one to five years after index delivery);
long‐term (more than five to 10 years after index delivery);
very long‐term (more than 10 years after index delivery).
Where a trial took measures at two time points within a single category (e.g. at eight and 12 months after delivery), we used the data from the longer time period. Few medium‐, long‐ and very long‐term data were available. Accordingly, these data were reported in text and not forest plots.
Unit of analysis issues
The primary unit of analysis was per women randomised.
For the meta‐analysis of multi‐arm studies, the data from the PFMT intervention arms were combined for comparison with the control arm. The mean and standard deviation for the combined data were calculated according to the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Dealing with missing data
Where possible, the trial data were analysed according to the intention‐to‐treat principle, that is by the randomised groups, and irrespective of whether women received treatment according to their randomised allocation. We did not impute missing outcome data.
Assessment of heterogeneity
The extent of heterogeneity was assessed in three ways: visual inspection of data plots, Chi² test for heterogeneity and the I² statistic (Higgins 2011). Possible explanations for the heterogeneity were sought and discussed.
Assessment of reporting biases
To minimise reporting bias, the review authors undertook a comprehensive search for eligible trials and were vigilant for duplication of data.
Data synthesis
We used the Mantel‐Haenszel methods with a fixed‐effect model approach in the meta‐analyses in this review, unless statistically significant heterogeneity (Chi² test, P < 0.10) in the comparison suggested a more conservative random‐effect model was indicated.
GRADE and 'Summary of findings' tables
We created 'Summary of findings' tables using the following outcomes:
urinary incontinence in late pregnancy (antenatal PFMT trials only);
urinary incontinence mid‐postnatal period (antenatal PFMT trials only);
urinary incontinence late postnatal period;
faecal incontinence in late pregnancy (antenatal PFMT trials only);
faecal incontinence mid‐postnatal period (antenatal PFMT trials only);
faecal incontinence late postnatal period;
incontinence‐specific quality of life.
For antenatal PFMT trials, we assessed the evidence in late pregnancy (postintervention effect) and the mid‐postnatal period (durability of effect postdelivery). In postnatal training trials, we assessed the evidence in the late postnatal period (sustained postintervention effect). We used the five GRADE considerations (study limitations, inconsistency of effect, imprecision, indirectness and publication bias) to assess the quality of the body of evidence as it related to the studies that contributed data to the meta‐analyses for the prespecified outcomes (Atkins 2004). We used methods and recommendations described in Section 8.5 and Chapter 12 of the Cochrane Handbook for Systematic Reviews of Interventions using GRADEpro GDT software (GRADEpro GDT; Higgins 2011). We justified all decisions to downgrade or upgrade the quality of studies using footnotes and made comments to aid the reader's understanding of the review where necessary.
Subgroup analysis and investigation of heterogeneity
In each comparison, trials were subgrouped according to the control comparison because, a priori, we thought it plausible that the size or direction of effect would be influenced by the control condition. The four subgroups were:
PFMT versus no PFMT;
PFMT versus unspecified control (i.e. the trialist gave insufficient information about the control condition to classify it as one of the others);
PFMT versus usual care;
PFMT (more intensive, e.g. addition of biofeedback) versus PFMT (less intensive).
Sensitivity analysis
Sensitivity analysis with respect to trial quality was planned, as there is some evidence that the adequacy of randomisation (sequence generation and allocation concealment) may have an impact on the findings of a meta‐analysis (Moher 1998). However, there were insufficient trials and too many other potential causes of heterogeneity to make this useful.
Results
Description of studies
Results of the search
The flow of literature through the assessment process is shown in the PRISMA flowchart (Figure 1).
Figure 1.
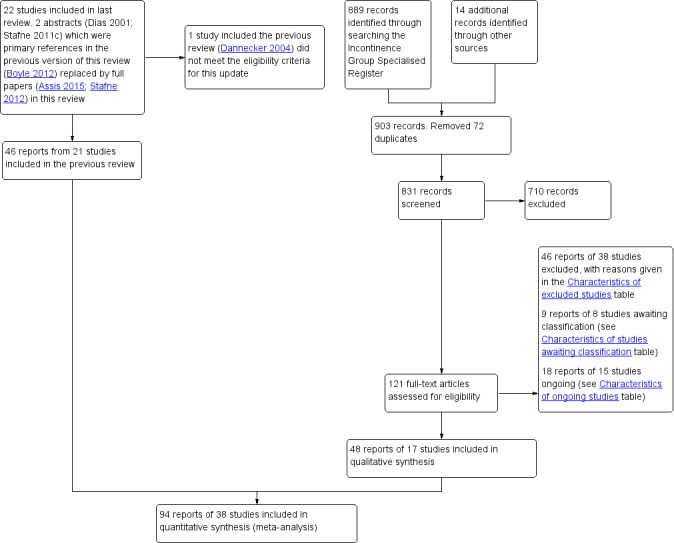
PRISMA study flow diagram.
The previous version of the review included 49 reports of 22 studies (Boyle 2012). The search update yielded 831 titles and abstracts and 121 records were obtained for further assessment. We included 48 reports from 17 new studies. The updated review now synthesises data from 94 reports of 38 studies that randomised 9892 women (4939 PFMT, 4953 controls) from 20 countries.
One trial included in the previous review did not meet the eligibility criteria for the intervention and was excluded from the update (Dannecker 2004; see Excluded studies). Forty‐six reports of 38 studies were excluded from the update and reasons are given in the Characteristics of excluded studies. In addition, 15 studies were classified as ongoing (see the Characteristics of ongoing studies) and eight require further assessment to determine eligibility (see the Characteristics of studies awaiting classification).
Three papers were published in Chinese and the data were extracted by translators for screening and further analysis (Kou 2013; Liu 2011; Wen 2010).
Included studies
The review includes 38 trials and further details are provided in the Characteristics of included studies.
Seven were primary or secondary prevention trials (i.e. none of the women had incontinence symptoms at the start of training) (Barakat 2011; Gaier 2010; Gorbea 2004; Kocaoz 2013; Pelaez 2014; Reilly 2002; Stothers 2002). Two trials provided subgroup data for women continent at randomisation (Mørkved 2003; Sampselle 1998). All nine investigated the effect of beginning PFMT antenatally.
Ten were treatment trials (i.e. all women had incontinence symptoms at the start of training). These investigated the effects of beginning PFMT antenatally and postnatally (Ahlund 2013; Cruz 2014; Dinc 2009; Dumoulin 2004; Glazener 2001; Kim 2012; Sangsawang 2016; Skelly 2004; Wilson 1998; Woldringh 2007).
Twenty‐one were mixed prevention or treatment trials as some women did, and others did not, have incontinence symptoms at the start of training. These trials investigated the effects of starting PFMT antenatally or postnatally (Assis 2015; Bø 2011; Chiarelli 2002; Dokmeci 2008; Ewings 2005; Fritel 2015; Frost 2014; Frumenzio 2012; Hilde 2013; Hughes 2001; Ko 2011; Kou 2013; Liu 2011; Meyer 2001; Miquelutti 2013; Mørkved 2003; Peirce 2013; Sampselle 1998; Sleep 1987; Stafne 2012; Wen 2010).
Twenty of the 38 studies were included in the previous version of this review (Assis 2015; Bø 2011; Chiarelli 2002; Dinc 2009; Dumoulin 2004; Ewings 2005; Glazener 2001; Gorbea 2004; Hughes 2001; Ko 2011; Meyer 2001; Mørkved 2003; Reilly 2002; Sampselle 1998; Skelly 2004; Sleep 1987; Stafne 2012; Stothers 2002; Wilson 1998; Woldringh 2007). Two trials were previously included in abstract form (Assis 2015; Stafne 2012).
The primary reference for eight trials was a conference abstract (Cruz 2014; Dokmeci 2008; Frost 2014; Frumenzio 2012; Gaier 2010; Hughes 2001; Skelly 2004; Stothers 2002). No further published reports were found for seven of these eight trials and one trialist kindly provided additional data from a thesis (Hughes 2001). One‐to‐one randomisation was assumed (the numbers in the intervention (139 women) and control (129 women) groups suggested this was likely) for one trial so that data could be used in the meta‐analysis (Skelly 2004).
Nineteen of the 38 included studies were publicly funded (university or national research funds or charitable trust) and one received grants from both public and private sources (Glazener 2001). Three studies did not receive any specific funding (Ahlund 2013; Barakat 2011; Kim 2012). Sixteen studies did not declare funding sources (Assis 2015; Bø 2011; Dokmeci 2008; Frost 2014; Frumenzio 2012; Gaier 2010; Gorbea 2004; Hughes 2001; Kim 2012; Kocaoz 2013; Kou 2013; Liu 2011; Pelaez 2014; Skelly 2004; Stothers 2002; Wen 2010). Fourteen trials declared no conflicts of interest (Ahlund 2013; Bø 2011; Chiarelli 2002; Dinc 2009; Dokmeci 2008; Fritel 2015; Glazener 2001; Hilde 2013; Ko 2011; Miquelutti 2013; Peirce 2013; Pelaez 2014; Sangsawang 2016; Stafne 2012). The remaining 14 trials did not report funding.
In all, 34 of the 38 trials contributed data to one or more meta‐analysis.
Settings
Women were recruited from various health services including antenatal and urology clinics, outpatient physiotherapy clinics, gynaecology and obstetric departments, and hospital settings in the following 20 countries: Australia (Chiarelli 2002), Brazil (Assis 2015; Cruz 2014; Miquelutti 2013), Canada (Dumoulin 2004; Skelly 2004; Stothers 2002), China (Ko 2011; Kou 2013; Liu 2011; Wen 2010), England (Ewings 2005; Glazener 2001; Reilly 2002; Sleep 1987), France (Fritel 2015), Ireland (Peirce 2013), Italy (Frumenzio 2012; Gaier 2010), Mexico (Gorbea 2004), Netherlands (Woldringh 2007), New Zealand (Glazener 2001; Wilson 1998), Norway (Bø 2011; Hilde 2013; Mørkved 2003; Stafne 2012), Republic of Korea (Kim 2012), Scotland (Glazener 2001), Spain (Barakat 2011; Pelaez 2014), Sweden (Ahlund 2013), Switzerland (Meyer 2001), Thailand (Sangsawang 2016), Turkey (Dinc 2009; Dokmeci 2008; Kocaoz 2013), and the US (Frost 2014; Sampselle 1998).
Sample characteristics
Parity (number of births)
Seven studies did not report parity or gravidity (Cruz 2014; Frost 2014; Frumenzio 2012; Kocaoz 2013; Skelly 2004; Stothers 2002; Wen 2010). Five of these were conference abstracts (Cruz 2014; Frost 2014; Frumenzio 2012; Skelly 2004; Stothers 2002). Trials that investigated the effects of antenatal PFMT for prevention of urinary incontinence recruited only continent women in their first pregnancy or having their first baby (or both), which trialists variously called nulliparous or primiparous women, or continent women regardless of parity (Barakat 2011; Gaier 2010; Gorbea 2004; Pelaez 2014; Reilly 2002). Trials testing antenatally for treatment of incontinence included women in their first pregnancy or nulliparae or multiparae women (Dinc 2009; Sangsawang 2016; Woldringh 2007). In trials of postnatal PFMT for treatment of urinary incontinence, all but one (Ahlund 2013, primiparous) recruited nulliparae or multiparae women (Dumoulin 2004; Glazener 2001; Kim 2012; Wilson 1998). In the mixed prevention and treatment studies investigating antenatal PFMT, most recruited women in their first pregnancy or who were having their first baby (Assis 2015; Bø 2011; Dokmeci 2008; Fritel 2015; Hughes 2001; Ko 2011; Miquelutti 2013; Mørkved 2003; Sampselle 1998). One included both nulliparae and multiparae (Stafne 2012). In the mixed prevention and treatment trials of postnatal PFMT, four included women who had just had their first baby (Hilde 2013; Liu 2011; Meyer 2001; Peirce 2013). The other three recruited mixed nulliparae and multiparae (Chiarelli 2002; Ewings 2005; Sleep 1987). In the trials with mixed parity samples, it is unknown if parity was comparable in six trials (Cruz 2014; Frumenzio 2012; Kocaoz 2013; Kou 2013; Skelly 2004; Stothers 2002). It was not comparable in one trial (Barakat 2011).
Age
Participant age was variously described, although five trials did not report this (Cruz 2014; Dokmeci 2008; Frost 2014; Peirce 2013; Skelly 2004). Three trials reported an age range, with women aged between their early 20s to early 40s (Kou 2013; Stothers 2002; Wen 2010). In two trials, about 50% to 60% of the women were aged 20 to 29 years (Chiarelli 2002; Ewings 2005). Median age was about 28 years in two trials (Hughes 2001; Reilly 2002) and 36 years in another trial (Dumoulin 2004). In the remaining 24 studies, the mean age was in the early 20s (Miquelutti 2013), mid to late 20s for 14 trials (Assis 2015; Dinc 2009; Fritel 2015; Gaier 2010; Gorbea 2004; Kocaoz 2013; Liu 2011; Meyer 2001; Mørkved 2003; Pelaez 2014; Sampselle 1998; Sangsawang 2016; Sleep 1987; Wilson 1998), and early 30s for 10 trials (Ahlund 2013; Barakat 2011; Bø 2011; Frumenzio 2012; Glazener 2001; Hilde 2013; Kim 2012; Ko 2011; Stafne 2012; Woldringh 2007). Age was comparable at baseline between groups in 29 trials but was unclear in the other nine (Cruz 2014; Dokmeci 2008; Frumenzio 2012; Kou 2013; Meyer 2001; Peirce 2013; Skelly 2004; Stothers 2002; Wen 2010).
Weight
Twenty‐two of the 38 trials reported bodyweight or BMI. For the women recruited antenatally, mean or median BMI was in the low to mid 20s (Barakat 2011; Bø 2011; Fritel 2015; Gaier 2010; Hughes 2001; Ko 2011; Miquelutti 2013; Mørkved 2003; Pelaez 2014; Reilly 2002; Sangsawang 2016; Stafne 2012; Woldringh 2007). Two trials reported that mean bodyweight in kilograms was in the mid 60s on average (Assis 2015, 67 kg; Gorbea 2004, 66 kg). About 30% of women had a BMI in the overweight or obese range in one trial that recruited women antenatally and in two that recruited women on postnatal wards (Chiarelli 2002; Ewings 2005; Kocaoz 2013). In three trials that recruited postnatal women with persistent incontinence symptoms, the mean or median BMI was in the normal range (Ahlund 2013; Dumoulin 2004; Kim 2012). BMI was about 26 kg/m² in one mixed treatment and prevention study which recruited women postnatally (Hilde 2013). BMI or bodyweight was comparable at baseline between groups for all of these trials, although two trials noted that weight gain in pregnancy differed significantly between the groups, being greater in either the PFMT group or in the control group (Barakat 2011; Gorbea 2004).
Type of delivery
Some details on delivery were given by 11 of 15 trials that began PFMT after delivery. In eight of these trials, all women delivered vaginally (Chiarelli 2002; Frost 2014; Hilde 2013; Kim 2012; Liu 2011; Peirce 2013; Sleep 1987; Wen 2010). In the study by Chiarelli 2002, all women had a forceps or ventouse delivery, while Peirce 2013 reported that about 39% of women had an instrumental delivery. The types of delivery appeared comparable across the PFMT and control groups in both trials. In the trials by Glazener 2001 and Wilson 1998, some women had a caesarean section (about 8% in Glazener 2001 and 18% in Wilson 1998) with the proportion of caesarean sections being similar in both the PFMT and control groups for both trials. Glazener 2001 also reported that about 14% of women in both the PFMT and control groups had assisted vaginal deliveries. In the remaining small trial by Meyer 2001, it was unclear if all 107 women delivered vaginally but it was reported that 30% of PFMT group and 16% of control group women had forceps delivery; this difference was not "statistically significant" (P = 0.10).
For the trials in which PFMT began antenatally, it is possible that the type of delivery was affected by PFMT. For these trials, the type of delivery was a possible confounder of the postnatal incontinence outcome but may itself be an outcome of importance. A short summary of the data is given here. The data are also reported in more detail in the analysis. Some details on the type of delivery, by group, were given by only 13 of the 23 trials in which PFMT began antenatally. In 11 trials, the delivery type was similar across both comparison groups (Barakat 2011; Fritel 2015; Frost 2014; Hughes 2001; Ko 2011; Miquelutti 2013; Mørkved 2003; Reilly 2002; Sampselle 1998; Stothers 2002; Woldringh 2007). However, in two trials, there seemed to be fewer vaginal deliveries in the PFMT group (Dinc 2009; Gorbea 2004). Miquelutti 2013 reported a "statistically significantly" longer duration of delivery in the PFMT group (MD 9.48, 95% CI 0.32 to 18.64; P < 0.05).
Exclusion criteria
The most common exclusion criterion (in 27 trials) was a comorbidity that contraindicated exercise in pregnancy or made PFMT difficult (or both), or might have altered the outcome of training, such as serious medical or neuromuscular conditions. Ten trials excluded women with high‐risk pregnancies (Bø 2011; Dokmeci 2008; Fritel 2015; Gorbea 2004; Ko 2011; Meyer 2001; Miquelutti 2013; Mørkved 2003; Sangsawang 2016; Stafne 2012). Sixteen trials included women with singleton pregnancies or excluded women with twins, or other multiple pregnancies or births (Ahlund 2013; Barakat 2011; Bø 2011; Cruz 2014; Fritel 2015; Gorbea 2004; Hilde 2013; Liu 2011; Meyer 2001; Miquelutti 2013; Mørkved 2003; Pelaez 2014; Sangsawang 2016; Stafne 2012; Stothers 2002; Wen 2010). Eight excluded women if the baby was stillborn or was very ill or died after birth (Chiarelli 2002; Ewings 2005; Glazener 2001; Hilde 2013; Mørkved 2003; Peirce 2013; Sleep 1987; Stafne 2012). Five excluded women if language difficulties meant it was difficult to seek informed consent (Chiarelli 2002; Dumoulin 2004; Ewings 2005; Peirce 2013; Woldringh 2007). An additional six outlined language requirements as part of their inclusion criteria (Bø 2011; Cruz 2014; Fritel 2015; Hilde 2013; Peirce 2013; Pelaez 2014). Four trials specifically excluded women who experienced pain with a PFM contraction (Dinc 2009; Ko 2011; Mørkved 2003; Sangsawang 2016).
Pelvic floor muscle training regimens and control interventions
The PFMT and control interventions are described in the Characteristics of included studies (overview) and in Table 11 (details of exercise parameters and adherence).
Table 1.
Pelvic floor muscle training programmes and adherence
| Study ID | Voluntary pelvic floor muscle contraction confirmed? | PFMT parameters | PFMT supervision | Control comparison | Adherence | Notes |
|
Ahlund 2013 (treatment trial) |
Vaginal palpation performed by study midwife: after randomisation and at each of the 3 visits to midwife (PFMT and control groups). | PFMT started with 3 fast contractions, followed by 3 sets of 8‐12 slow velocity, near maximal contractions, 6‐sec hold; 7 days per week for 6 months. Received written instructions on PFMT, but no information provided on PFMT progression. | Visit to the study midwife every 6th week (3 times during study period). | Usual care: written information describing PFM anatomy and PFMT. Received instructions on how to correctly perform PFM contraction (vaginal palpation) from midwife. | Women in the PFMT group were asked at each midwife visit how often they did PFMT; results not reported. | PFMT in lying or sitting positions. |
|
Assis 2015 (prevention trial) |
Perineometry (at 1st meeting), but unclear by whom (PFMT group). | 5‐10 slow PFM contractions with 6‐sec hold, rest 6 sec between contractions with 3 rapid contractions at the end (as per Mørkved 2003). Daily PFMT in 4 positions, and 1 group (27 women) had 5 supervised sessions with a physiotherapist. Received manual of home PFMT exercises and asked to complete an exercise diary. | Supervised PFMT (27 women): received up to 5 monthly supervised exercise sessions with physiotherapist (22, 26, 30, 34, 38 weeks' gestation). Unsupervised PFMT (27 women): trained to perform PFMT by physiotherapist (1 session). | Did not receive intervention and did not exercise. | Not reported, although it stated that no dropouts occurred throughout the duration of the study due to all women in the PFMT group complying with the exercise protocol. | PFMT in a variety of positions including left side lying, sitting, reclined sitting, sitting with legs crossed, standing. Translation (Portuguese). |
|
Barakat 2011 (prevention trial) |
Not reported. | PFMT included in the 7‐ to 8‐min cool‐down period as part of a 35‐ to 45‐min exercise session, 3 days per week for duration of pregnancy (potential mean of 85 sessions in total). No specific details provided about PFMT programme. | Group exercise classes, supervised by a qualified fitness specialist, with the assistance of an obstetrician. | Not reported. | Adherence to PFMT was 90%. | General exercises targeted major muscles of arms and abdomen to promote good posture and prevent low back pain, and in the 3rd trimester strengthen the muscles of labour and PF. 1 session of aerobic dance per week. Accompanied by music. |
|
Bø 2011 (mixed prevention and treatment trial) |
Participants did not have individual assessment of correct voluntary PFM contraction (due to pragmatic nature of study). Instructors were trained in how to explain a correct PFM contraction. | PFMT included as part of 15‐min strength training session within a 60‐min group exercise class. PFMT: 3 sets of 8‐12 maximal contractions, 6‐ to 8‐sec hold; strong verbal motivation to perform close to maximum PFM contractions. Women encouraged to participate in at least 2 out of 3 fitness classes per week for 12 weeks. Daily PFMT at home: 3 sets of 8‐12 close to maximum PFM contractions. Also encouraged to be physically active for at least 30 min per day. Received a specific PFMT brochure. | Group exercise classes, 2 or 3 per week for 12 weeks, led by certified aerobic instructors. Instructors were taught by a physiotherapist with > 20 years of experience in assessing, treating and researching women with PF dysfunction. | Usual antenatal care. | Mean adherence to exercise classes was 17.2 out of a possible 24 sessions. 40% (21/52) of women attended at least 80% of sessions. | PFMT integrated into aerobic dance class (accompanied by music): 5‐min warm‐up; 30‐min low‐impact aerobics; 15‐min strength training (including PFMT); 5‐min stretching and relaxation. PFMT in a variety of position including sitting, kneeling and standing. Informed of deep abdominal muscle co‐contraction during maximal PFM contraction. |
|
Chiarelli 2002 (mixed prevention and treatment trial) |
Visual inspection of perineum (PFMT group). | Maximum of 6 voluntary PFM contractions per set; 3‐6 sec hold; 3 sets per day; for 8 weeks. | PFMT taught 1‐to‐1 with physiotherapist. 1 (20 min) contact in hospital, and another (30 min) 8 weeks later at home or hospital. | Routine postnatal care; usual postnatal leaflet given; invitation to join postnatal class on ward; no restriction on PFMT if recommended by other health professional. | 84% (292/348) of women in the PFMT group and 58% (189/328) of controls were performing PFMT at "adequate" level at 3 months' postpartum. | Women were "asked if they were performing their PF exercises." |
|
Cruz 2014 (treatment trial) |
Not reported. | 5‐6 biweekly sessions. No specific details provided about PFMT. | Supervised by a physiotherapist. | Similar unsupervised PFMT at home. | Not reported. | Conference abstract. |
|
Dinc 2009 (treatment trial) |
Vaginal digital palpation (both PFMT and control groups). | Progressive PFMT programme. Level 1: 3 sets of 10 near maximal contractions; 3‐sec hold, 3‐sec rest; quick contraction, 1‐sec hold, 1‐sec rest; twice daily. Level 2: 3 sets of 10 near maximal contractions; 5‐sec hold, 5‐sec rest; quick contraction, 2‐sec hold, 2‐sec rest; twice daily. Level 3: 3 sets of 15 near maximal contractions; 10‐sec hold, 10‐sec rest; quick contraction, 2‐sec hold, 2‐sec rest; 3 per day. |
Trained by a researcher on how to do PFMT in accordance with booklet of PFM exercises. | Usual care: instructed on how to perform a correct PFM contraction, but did not receive training about exercises. | Not reported. | In 2nd stage of study, 68% of women in study group were contracting the proper muscle group. The rest were given more training and reassessed 1 week later. |
|
Dokmeci 2008 (mixed prevention and treatment trial) |
Not reported. | Not reported. | Not reported. | Not reported. | Not reported. | Conference abstract. |
|
Dumoulin 2004 (treatment trial) |
Not reported. | 8‐12 close to maximal voluntary PFM contraction per set; 6‐ to 8‐sec hold each with 3‐4 fast contractions at the end of each contraction; 6‐sec rest between contractions; 3 sets per day; 5 days per week; for 8 weeks. Also taught 'the knack' (voluntary PFM contraction prior to hard cough and maintained through cough until abdominal wall relaxed). | PFMT taught 1‐to‐1 with physiotherapist. Weekly physiotherapy appointments for 8 consecutive weeks. | Same number of physiotherapy contacts for relaxation massage of back and extremities; asked not to do PFMT at home. | Not reported. | In addition to PFMT 15 min of electrical stimulation (biphasic rectangular form, 50 Hz, pulse width 250 msec, duty cycle 6 sec on and 18 sec off for 1st 4 weeks, then 8 sec on and 24 sec off for next 4 weeks, at maximal tolerated current intensity) and 25 min of electromyographic biofeedback per appointment. |
|
Ewings 2005 (mixed prevention and treatment trial) |
Not reported. | 6 months. | PFMT taught 1‐to‐1 with physiotherapist in hospital. Invitation to attend PFMT class at 2 and 4 months postnatally. | Standard care including verbal promotion of PFMT and leaflet on PFMT. | Of 117 women in the PFMT group, 114 were visited by the physiotherapist in hospital, 21 attended the 2‐month PFMT group, and 5 attended the 4‐month group. | ‐ |
|
Fritel 2015 (mixed prevention and treatment trial) |
Vaginal digital palpation at each session (possibly by physiotherapist, but not stated; PFMT group). | 1 session per week (20‐30 min), total of 8 sessions between 6th and 8th month of pregnancy. Also 'the knack' (voluntary PFM contraction prior to increasing intra‐abdominal pressure). Provided with written information on PF anatomy and PFMT, and encouraged to perform daily PFMT at home, 10‐20 contractions. | Individually supervised by a physiotherapist or midwife at each session. In total, 37 different therapists (all trained by the same specialist physiotherapist) were involved in delivering the exercises. | Usual care, including written information on PF anatomy and PFMT (encouraged to perform daily at home, 10‐20 PFM contractions). | 69.3% (97/140) of women in the PFMT group completed all planned sessions, and 82.8% (116/140) completed at least 1 session (4‐8, median 8). At the end of pregnancy, women in both groups reported a similar frequency and duration of PFMT (including number of contractions). PFMT was performed daily at home by 4.3% (6/140) of PFMT women and 10.6% (15/142) of controls, at the end of pregnancy. | PFMT performed in standing (5 min) and lying (10 min). |
|
Frost 2014 (mixed prevention and treatment trial) |
Not reported. | Standard postpartum discharge instructions plus written and verbal instructions for PFMT. | Not reported. | Standard postpartum discharge instructions. | Not reported. | Conference abstract. |
|
Frumenzio 2012 (mixed prevention and treatment trial) |
Not reported. | 2 weekly session of Kegel exercises; 8 weeks. Daily home exercises (20 min) and stretching. | Not reported. | Did not receive any PFMT, no other details provided. | Not reported. | Conference abstract. |
|
Gaier 2010 (prevention trial) |
Not reported. | 12‐week PFMT programme. | PFMT supervised by a physiotherapist and midwife. | Routine care and PFM exercises, customary instruction at intake visit. | Not reported. | Conference abstract. |
|
Glazener 2001 (treatment trial) |
Not reported. | 8‐10 sessions of fast and slow voluntary PFM contraction per day with aim of 80‐100 per day; for up to 8 months. | PFMT taught 1‐to‐1 with nurse, health visitor or continence advisor. Visited at home at 5, 7 and 9 months' postnatally. | Usual antenatal and postnatal care that may have included advice on PFMT. | 78% (218/278) of women in the PFMT group and 48% (118/244) of controls had done some PFMT in the 11th postnatal month. Mean (SD) number of voluntary PFM contractions per day at 12 months' postnatal: PFMT group 20 (29) and controls 5 (15). | Frequency and urgency strategies added if needed at 7 or 9 months postnatally. 52.7% (394/747) of women at 6 years' follow‐up and 70.1% (471/672) of women at 12 years' follow‐up completed a questionnaire. About 50% of women in PFMT and control groups were performing any PFMT at both time points. Daily PFMT was undertaken by 6% (17/263) of PFMT women compared to 12% (29/253) of control women at 6 years; and 7% (15/227) of PFMT group compared to 8% (20/241) of control women at 12 years. |
|
Gorbea 2004 (prevention trial) |
Surface electromyography (electrodes either side of anus; PFMT group). | 10 voluntary PFM contraction; 8‐sec hold followed by 3 fast, 1‐sec contractions; 6‐sec rest between contractions; for up to 20 weeks. Asked to complete an exercise diary. | PFMT taught 1‐to‐1 with physiotherapist. Clinic appointments (1 hour each) weekly for 8 weeks, then weekly telephone calls. | Requested not to do PFMT during pregnancy or postnatally. | 63% attended all 8 physiotherapy appointments, 21% attended 7 appointments. | Electromyographic biofeedback at each appointment. |
|
Hilde 2013 (mixed prevention and treatment trial) |
Vaginal digital palpation (PFMT and control groups). | Progressive supervised PFM training programme (as per Mørkved 1997) for 16 weeks. Daily PFMT at home, 3 sets of 8‐12 close to maximal contractions. Customary written information on discharge from postnatal ward. Asked to complete an exercise diary. | Supervised exercise class from 6 weeks' postpartum, led by an experienced physiotherapist, once per week for 16 weeks. Class attendance was documented. | Usual care. Received customary written information on discharge from postnatal ward. At 6 weeks were instructed on how to perform a correct PFM contraction (verified with vaginal digital palpation). | 96% (72/75) of women in the PFMT group who completed the trial adhered to 80% of the class and daily home training. In the control group (retrospective questioning), 16.5% reported performing daily PFMT at home ≥ 3 times per week. | 4% (7/175) of women were unable to perform a voluntary PFM contraction at baseline. At baseline (6 weeks' postpartum) more women in the control group were performing PFMT ≥ 3 times or more per week. |
|
Hughes 2001 (mixed prevention and treatment trial) |
Vaginal digital palpation (PFMT and control groups). | Daily; for up to 11 months. | 1 individual session with physiotherapist, and 1 group PFMT session led by physiotherapist at 22‐25 weeks' gestation with maximum of 6 women per group. | Usual antenatal and postnatal care that may have included advice on PFMT (personal communication). | 79% (461/586) of women in PFMT group attended group PFMT session (personal communication). | 3.5% (16/460) of women who attended group PFMT session could not perform a voluntary PFM contraction after teaching, and 2.8% (13/460) of women could contract but not sustain a contraction (personal communication). Conference abstract. |
|
Kim 2012 (treatment trial) |
Perineometer (vaginal probe) used to ensure PFM contraction and assess control of contraction in both PFMT and control groups. Unclear if this was performed every session with the PFMT women. | 20 maximal voluntary PFM contractions, 10‐sec hold, 3 times per week; for 8 weeks (as part of a class), and daily at home. Progressed by changing position (prone, sitting and standing). Initial session included information on PFM anatomy and function. Also provided with a booklet which included a training programme and an exercise diary. | Supervised training sessions (1‐hour duration) with a specialist physiotherapist (23 in total, unclear if individual contacts or group classes). | Usual care. Received the same information and demonstration session as PFMT group and instructions on how to correctly perform PFM contraction (perineometer). Unsupervised, daily PFMT for 8 weeks. | Not reported. | PFMT integrated with trunk stabilisation exercises (progressive abdominal strengthening, bridging, and side‐bridge). |
|
Ko 2011 (mixed prevention and treatment trial) |
Observation of inward movement of perineum during contraction (PFMT group). | 3 repetitions of 8 PFM contractions, 6‐sec hold each, 2‐min rest between repetitions; repeated twice daily at home with additional training in groups once per week for 45 min for 12 weeks. Asked to complete an exercise diary. | Group training sessions (10 women) supervised by a physiotherapist once per week for 12 weeks. | Regular antenatal care and the customary written postpartum instructions that did not include PFMT from the hospital. Not discouraged from performing PFMT on their own. |
> 80% attended every training session and 0 were absent more than twice. At 35 gestational weeks, 87% of PFMT group reported practice of PFMT ≥ 75% of the time. |
Group training was performed in sitting and standing positions with legs apart to emphasise specific strength training of the PFM and relaxation of other muscles. |
|
Kocaoz 2013 (prevention trial) |
Observation of inward movement of perineum or digital vaginal palpation, or both (PFMT group). Vaginal digital palpation used to teach PFM contraction in 23.5% (16/68) of women. | 3 sets of 10 maximal voluntary PFM contractions at level 3 (2‐sec hold, 2‐sec rest for strength; 10‐sec hold, 10‐sec rest for endurance); 3 sessions per day during pregnancy and postpartum. Women received education about the anatomy and functions of the PFM and PFMT (unclear from whom) and were asked to complete an exercise diary (including progressions). | Exercise compliance was checked at every hospital visit (9‐10 visits on average, over a minimum of 12 weeks), and pregnant women were called once per month to encourage regular exercise. | Not instructed to do PFMT. Once data collection complete, controls received PFMT and a brochure with the relevant information during the 12th week home visit. | Women asked to record the number of times they did their exercises. No data reported. | Digital vaginal palpation was refused by 52/68 women due to concerns about pregnancy, cultural/religious reasons. Unclear if women progressed through levels 1‐3 or started at level 3, whether they did 3 sets of 10 exercises per day or 3 sets of 10 exercises 3 times per day, or how the sets were divided between endurance and strength training. |
|
Kou 2013 (mixed prevention and treatment trial) |
Not reported. | PFM (Kegel) exercises undertaken 2‐3 times per day for 20‐30 min or 150‐200 contractions (3‐sec hold then relax), performed until 12 months' postpartum. Biofeedback used twice per week (no further details available). | Not reported who supervised the programme, or the number and type of contacts with health professional(s). | Usual care: received standard postpartum information. | Not reported. | Translation (Chinese). |
|
Liu 2011 (mixed prevention and treatment trial) |
Not reported. | PFMT 2‐3 times per day, 15‐30 min each set (4‐ to 6‐sec hold, 10‐sec relaxation), started after birth and continued for ≥ 10 weeks. | Exercises taught by experienced midwives who also supervised the programme (number and type of contacts/visits unclear). | Usual care: standard postpartum information. Unclear if this included PFMT. | Not reported. | Translation (Chinese). Positions of exercises included supine, sitting or any other position, with legs slightly separated, with instructions to contract anus, vaginal and urinary tract while breathing in, and to relax with expiration. |
|
Meyer 2001 (mixed prevention and treatment trial) |
Not reported. | Up to 8 months; no details of PFMT provided. Each clinic session was followed by 20 min of biofeedback and 15 min of electrical stimulation. | 12 sessions (6 weeks) with a physiotherapist between 2 and 10 months postnatally. | No intervention. Women received PFMT education after 3rd assessment at 10 months' postpartum. | Not reported. | In addition to PFMT, 20 min of biofeedback and 15 min of electrical stimulation (vaginal electrode, biphasic rectangular waveform, pulse width 200‐400 msec, frequency 50 Hz, intensity 15‐15 mA, contraction time 6 sec, rest time 12 sec) per appointment. |
|
Miquelutti 2013 (mixed prevention and treatment trial) |
Instructed on correct contraction, but not verified (due to pragmatic nature of study). | PFMT (maximal rapid and sustained PFM contractions) performed as part of a class (50 min) for a median of 5 (range 2‐10) sessions between 18‐24 weeks' to 36‐38 weeks' gestation. Provided with an exercise guide and asked to do daily PFMT at home (30 rapid, 20 sustained (10‐sec hold) contractions), as well as 30‐min daily aerobic exercise (no specific examples provided). Received standard antenatal education and asked to complete an exercise diary. | Supervised by a trained study physiotherapists on a monthly basis. Either group or individual training sessions, depending on the number of women present. | Usual care: received standard antenatal and postnatal education (on labour, breastfeeding and pain relief) by trained physiotherapy, nursing and medial staff. | Analysis of adherence in intervention group was not possible as women failed to complete or return their exercise diaries. | PFMT performed in standing and sitting position. PFMT integrated into non‐aerobic exercise programme designed to reduce back pain. Included abdominal, stretching and relaxation exercises and exercises designed to promote venous return. |
|
Mørkved 2003 (mixed prevention and treatment) |
Vaginal digital palpation and observation of perineum (both PFMT and control groups). | 8‐12 near maximal voluntary PFM contractions; 6‐ to 8‐sec hold each, 3‐4 fast contractions at the end of each contraction; 6‐sec rest between contractions; twice daily at home; for ≤ 8 months. Also asked to attend weekly 60‐min PFMT class for 12 weeks. Women asked to complete an exercise diary. | Group training session (10‐15 women), once per week for 12 weeks, supervised by physiotherapists (5 in total). | Usual antenatal and postnatal care that may have included advice on PFMT. Correct PFM contraction verified. Not discouraged from doing PFMT on their own. | 19% (28/148) of PFMT women attended less than half the 12 weekly PFMT classes and did not return training diaries. | During exercise class voluntary PFM contraction undertaken in a range of body positions (lying, sitting, kneeling and standing with legs apart). PFMT interspersed with abdominal, back and thigh muscle exercises (accompanied by music). 62% (188/280) of women completed a questionnaire at 6‐year follow‐up, and 45% of women in both the former PFMT and control groups were doing PFMT at least weekly. |
|
Peirce 2013 (mixed prevention and treatment trial) |
Contraction assessed with anal biofeedback as part of training session (by obstetrician or specialist nurse); PFMT group. | Sets of 10 PFM contractions (Kegel exercises), 5‐sec hold; 10‐sec rest between contractions; twice daily for 5 min with biofeedback; for 3 months. Standard postpartum education by midwives or physiotherapists, including written information. Women asked to complete an exercise diary. | Biofeedback (electromyographic) training provided at initial session, but no further contact with health professionals. | Usual care: "conventional PFM training," but no details provided. Women asked to complete an exercise diary. | Poor adherence defined as performing < 70% of the intended home exercise sessions. 7/30 women in the PFMT group reported poor adherence. | The portable biofeedback machines were programmed to the electromyography setting with the work period set to 10 contractions (5‐sec duration) with a 10‐sec rest between each contraction. PFMT for treatment of FI. |
|
Pelaez 2014 (prevention trial) |
Instructed on correct contraction, but not formally verified. Women were asked to test themselves at home by stopping the flow of urine, digital palpation or using a mirror to observe the perineum (PFMT group). | PFMT programme, 3 times per week; for ≥ 22 weeks. Started with 1 set of 8 contractions increasing to 100; divided into different sets of slow (6 sec) and fast (5 as fast as possible) contractions. Unclear if this progression related to class or home exercises. Daily PFMT at home, 100 contractions in different sets. Received standard antenatal education about PFM. | Group training sessions (8‐12 women) designed and supervised by a physical activity and sport sciences graduate; 55‐ to 60‐min duration (10 min of PFMT); 70‐78 sessions in total. | Usual care: follow‐up by midwives, standard information about PFMT. Women were not asked not to do PFMT. | All women included in analysis attended ≥ 80% of exercise sessions. | PFMT integrated into supervised exercise programme; 30 min low‐impact aerobics including general strength training, PFMT and cool down (stretching, relaxation or massage); sometimes accompanied by music. PFMT in a variety of positions. Women wore heart rate monitors to control exercise intensity. |
|
Reilly 2002 (prevention trial) |
Unclear, but seems likely as physiotherapists gave individualised programmes to those unable to follow exercise regimen due to inability to do voluntary PFM contraction (PFMT group). | 8‐12 voluntary PFM contractions; 6‐sec hold each; 2‐min rest between each set of contractions; 3 sets of 8‐12 contractions twice daily; for about 20 weeks (as described by Bø 1995). Also asked to do voluntary PFM contraction with every cough and sneeze, and complete an exercise diary. | About 5 (monthly) contacts with physiotherapist between 20 weeks' gestation and delivery. | Usual antenatal and postnatal care that may have included advice on PFMT. Women appeared to have had same number of clinic visits as the PFMT group, and were asked if doing PFMT at each of these visits. | 43% (52/120) of women in the PFMT group did not return an exercise diary; 11% (13/120) completed < 28 days of PFMT; and 46% (55/120) completed ≥ 28 days. When asked postnatally, 28% (33/120) of PFMT women and 34% (37/110) of controls were doing occasional or no PFMT. | If unable to follow PFMT regimen then individualised programme until able to do so. 71% (164/230) of women completed a telephone questionnaire at 8‐year follow‐up, and 68.4% of women were doing PFMT, with 38% stating they were doing PFMT twice or more per week. |
|
Sampselle 1998 (mixed prevention and treatment trial) |
Yes, but unclear how or by whom (PFMT group). | PFMT tailored to individual ability. 30 maximal or near maximal voluntary PFM contraction per day; for ≤ 17 months. | Not reported. | Usual antenatal and postnatal care; no systematic PFMT programme. | At 35 weeks' gestation, 85% of women in the PFMT group reported to be doing PFMT 75% of the time. At 1 year, PFMT adherence reported to vary between 62% and 90%. | ‐ |
|
Sangsawang 2016 (treatment trial) |
Assessed by ability to stop or slow the flow of urine for 1‐2 sec (PFMT group). | 20 sets of PFM exercises, twice daily, at least 5 days per week, for 6 weeks. 1 set of PFM exercises was 1 slow contraction (10‐sec hold), followed by 10 fast contractions; no progression in number of contractions per set. Also received a handbook with information on stress UI, PFM function, instructions on PFMT and a urinary diary. | Supervised group sessions (4‐5 women) with a midwife; 45 min; once every 2 weeks for 6 weeks (3 sessions in total). | Usual care: from health professionals, obstetricians or midwives. Did not receive information about UI and received no training support about performing correct PFM exercises. | No women were excluded for failing to perform the PFMT for < 28 (of approximately 42) days. | PFMT performed in various positions including lying down, sitting and standing. |
|
Skelly 2004 (treatment trial) |
Not reported. | Not reported. | "One to one teaching about pelvic floor exercises." | "Conventional care (hand‐out information about pelvic muscle exercises)." | Not reported. | Conference abstract. |
|
Sleep 1987 (mixed prevention and treatment trial) |
Not reported. | As for controls with additional section in leaflet recommending a specific exercise each week that integrated voluntary PFM contraction with usual activities of daily living; up to 3 months. Asked to complete a daily exercise diary for 4 weeks. | 1‐to‐1 session with midwife co‐ordinator each postnatal day in hospital. | Usual antenatal and postnatal care including PFMT leaflet; might include PFMT at antenatal class or postnatal class on ward (or both); instructed to do voluntary PFM contraction as often as remembered and mid‐stream urine stop. | At 10 days postnatally, 78% of PFMT group and 68% of controls were doing some PFMT; with 58% of PFMT group and 42% of controls doing some PFMT at 3 months. | ‐ |
|
Stafne 2012 (mixed prevention and treatment trial) |
Vaginal digital palpation (PFMT group). | 8‐12 near maximal voluntary PFM contractions; 6‐ to 8‐sec hold each with 3 fast contractions at the end of each contraction. Asked to perform PFM exercises as part of a 45‐min home programme at least twice per week or a weekly 60‐min exercise class (or both). Received written information including brochure with an evidence‐based PFMT programme, and asked to complete an exercise diary. | Group training sessions (8‐15 women) supervised by physiotherapist, 60 min, once per week for 12 weeks | Usual care: received customary information from midwife or GP. Also given a detailed information brochure including evidence‐based PFMT programme. Women were not discouraged from exercising. | Adherence to the general exercise protocol (exercising ≥ 3 days per week, moderate to high intensity) was 55% (217/397) in the PFMT group and 10% (36/365) in the control group. 67% of the PFMT group performed PFMT ≥ 3 times per week compared to 40% in the control group | PFMT integrated into standardised exercise programme: 30‐ to 35‐min low‐impact aerobics; 20‐ to 25‐min strengthening exercises (including PFMT, 3 sets of 10 reps); 5‐ to 10‐min stretching and relaxation. PFMT performed in a variety of positions, with legs apart to emphasise specific strengthening of the PFM. |
|
Stothers 2002 (prevention trial) |
Not reported. | 12 contractions, 3 times daily. | Seen twice monthly throughout pregnancy, and every 3 months postnatally for 1 year. | "Other (placebo) including no pelvic floor exercises." | Not reported. | Conference abstract. |
|
Wen 2010 (mixed prevention and treatment trial) |
Assessment of PFM strength and contraction by an obstetrician (PFMT group; no further details) | Anal contraction; 3‐sec hold (while inhaling) followed by relaxation with 3‐5 faster contractions at the end of each contraction; 15‐30 min each set; twice daily; 6‐8 weeks. | Exercises taught by experienced midwives but unclear who supervised the programme of the number and type of contacts/visits. | Usual care: no other details provided other than "conventional guidance." | Not reported. | PFMT performed in a variety of positions including lying down, sitting or standing. Translation (Chinese). |
|
Wilson 1998 (treatment trial) |
Not reported. | Mix of fast and slow voluntary PFM contractions 8‐10 times per day with aim of 80‐100 voluntary PFM contraction daily; up to 9 months. | 1‐to‐1 sessions with physiotherapist at 3, 4, 6 and 9 months postnatally. | Usual PFMT as taught in antenatal and postnatal classes. | Mean (95% CI) number of daily voluntary PFM contraction at 12 months' postnatally was 86 (69‐104) in the PFMT group and 35 (30 to 40) in the control group. | Perineometry for biofeedback at each appointment. Mean time to teach PFMT to the PFMT group was 32 (95% CI 30 to 34) min. |
| Woldringh 2007 | Observation and palpation of perineal body by physiotherapists. Women also encouraged to practice self‐palpation (PFMT group). | Not reported. At each visit, women were asked about the frequency and duration of PFMT. | 1‐to‐1 30‐min sessions with physiotherapist. 4 in total: 3 antenatally and 1 at 6 weeks postnatally. In total, 25 physiotherapists (specialised in PFMT) were involved in delivering the exercises. | Usual antenatal and postnatal care including advice on PFMT; nearly two‐thirds received some instruction on PFMT. Women were also asked the same questions about frequency and duration of PFMT as the PFMT group | At 35 weeks' gestation, 6% reported no PFMT, 17% reported some PFMT, 40% were doing PFMT at low intensity and 37% were exercising intensively in the PFMT group vs 36% reported no PFMT, 25% reported some PFMT, 26% were doing PFMT at low intensity and 14% were exercising intensively in the control group. | ‐ |
CI: confidence interval; FI: faecal incontinence; min: minute; PF: pelvic floor; PFM: pelvic floor muscle; PFMT: pelvic floor muscle training; SD: standard deviation; sec: second; UI: urinary incontinence.
First, the PFMT programmes were classified by their possible physiological effect(s) (strength, endurance, co‐ordination or a combination), based on the described exercise parameters. Second, the amount of contact or supervision from health professionals (low fewer than five contacts; moderate six to 12 contacts; high more than 12 contacts), confirmation of a correct PFM contraction and nature of the control interventions were examined. Third, adherence data were considered to assess whether exercise behaviour was likely to support a physiological effect. Trials were classified according to whether they provided data for both the intervention and control groups, the intervention group only or neither group. The likely impact of the exercise programmes on PFM function and the clinical difference between the intervention and control conditions are considered in the Discussion.
We categorised 11 trials as providing strength training and six as probably strength training trials, 17 in all.
Eleven trials clearly provided exercise parameters that favoured strength training; short duration contractions of maximal or near maximal effort and a relatively small number of repetitions (Ahlund 2013; Bø 2011; Dinc 2009; Dumoulin 2004; Hilde 2013; Kim 2012; Kocaoz 2013; Miquelutti 2013; Mørkved 2003; Sampselle 1998; Stafne 2012). The exercise protocol described by Bø 1995 was the PFM strength training protocol on which the trials by Bø 2011, Mørkved 2003, and Dumoulin 2004 were based. Supervised treatment duration was only eight weeks in the trials by Dumoulin 2004 and Kim 2012 and this might have been insufficient for muscle hypertrophy to be established. In addition to strength training, Dumoulin 2004 included some co‐ordination type training. Women were encouraged to perform voluntary PFM contraction in conjunction with rises in intra‐abdominal pressure, such as with coughing or sneezing, also known as 'the Knack' (Miller 2008). Kim 2012 included trunk stabilisation exercises. With regard to contact with health professionals, this was low in two trials (fewer than five contacts) (Ahlund 2013; Miquelutti 2013), moderate (six to 12 contacts) in four (Dumoulin 2004; Kocaoz 2013; Mørkved 2003; Stafne 2012) and high (more than 12 contacts) in three (Bø 2011; Hilde 2013; Kim 2012). Four trials stated that PFMT was supervised in an exercise class (Bø 2011; Hilde 2013; Mørkved 2003; Stafne 2012). Eight trials confirmed a correct voluntary PFM contraction prior to training (Ahlund 2013; Dinc 2009; Hilde 2013; Kim 2012; Kocaoz 2013; Mørkved 2003; Sampselle 1998; Stafne 2012). Five of these also confirmed a correct contraction in the control group along with provision of usual antenatal and postnatal care (Ahlund 2013; Dinc 2009; Hilde 2013; Kim 2012; Mørkved 2003). In the remaining six trials, the control conditions were usual care, which may or may not have included PFMT or no PFMT as controls were asked not to train (Bø 2011; Dumoulin 2004; Kocaoz 2013; Miquelutti 2013; Sampselle 1998; Stafne 2012). With regard to adherence, five trials reported some information about exercise behaviour and four of these compared group exercise classes and home PFMT versus usual care (Bø 2011; Hilde 2013; Mørkved 2003; Stafne 2012). The fifth trial with adherence data compared standardised instruction and home PFMT with usual care (Sampselle 1998). In Stafne 2012, 67% of the PFMT group performed home PFMT at least three times per week compared to 40% of controls in late pregnancy. At six months' postpartum, Hilde 2013 found that 96% of the PFMT group who completed the trial adhered to 80% of the class and daily home training, whereas 16.5% of controls reported daily PFMT at home, three or more times per week. The other three trials reported data only for the intervention group, with adherence to PFMT of about 70% (Bø 2011) and 80% (Mørkved 2003), or 85% of PFMT women doing PFMT 75% of the time (Sampselle 1998).
Six trials described PFMT programmes that were characteristic of strength training but did not mention loading (effort) (Assis 2015; Chiarelli 2002; Gorbea 2004; Ko 2011; Peirce 2013; Reilly 2002). Two trials referenced the exercise protocols of other authors. Reilly 2002 cited Bø 1995 (strength and load training) and Ko 2011 cited Reilly 2002. The supervised treatment duration was only eight weeks in the trial by Chiarelli 2002 and this may have been insufficient for muscle hypertrophy to be established. In addition to strength training, women undertook some co‐ordination type training, daily biofeedback or participated in a weekly exercise class supervised by a physiotherapist (Ko 2011; Peirce 2013; Reilly 2002). In two trials, the control groups did not exercise (Assis 2015; Gorbea 2004). In the other four trials, controls were randomised to usual care which may or may not have included PFMT (Chiarelli 2002; Ko 2011; Peirce 2013; Reilly 2002). A correct PFM contraction for women in the exercise group was confirmed in five of the six trials (Assis 2015; Chiarelli 2002; Gorbea 2004; Ko 2011; Peirce 2013). However, none of the control groups appeared to have confirmation of a correct contraction. With regard to adherence, five of the six trials reported some information about exercise behaviour (Chiarelli 2002; Gorbea 2004; Ko 2011; Peirce 2013; Reilly 2002). Five trials offered individual supervision (Assis 2015; Chiarelli 2002; Gorbea 2004; Peirce 2013; Reilly 2002). One offered group sessions (Ko 2011). At three months' postpartum, Chiarelli 2002 reported that more women in the PFMT group (84%) compared to controls (58%) were doing "adequate" PFMT. Similarly, in Reilly 2002, about 75% of the PFMT group and 66% of the control group were doing more than occasional or no PFMT (27.5% in the PFMT group and 34% in the control group reported occasional or no PFMT). During the antenatal intervention period, nearly half the women in the PFMT group exercised for 28 days or more (which is approximately once per week over 20 weeks). The other three trials reported data only for the intervention group, with two reporting that over 80% of women attended most or all supervised visits (Gorbea 2004; Ko 2011). Ko 2011 and Peirce 2013 reported that more than three‐quarters of women in the PFMT group completed 70% or more of the prescribed exercise.
There was insufficient detail in the other 21 trials to classify them as providing strength or endurance training.
Seven trials provided some information about PFMT but could not be categorised (Glazener 2001; Kou 2013; Liu 2011; Pelaez 2014; Sangsawang 2016; Wen 2010; Wilson 1998). None had any description of effort (i.e. load). Supervised treatment was only six to eight weeks in two trials and this might have been insufficient for muscle hypertrophy to be established if strengthening was intended (Sangsawang 2016; Wen 2010). Five of the seven trials included variously described mixes of fast and slow contractions with relatively large numbers of sets (eight to 10 per day) and few repetitions per set (about 10) or exercise sets of 15‐ to 30‐minute duration (Glazener 2001; Pelaez 2014; Sangsawang 2016; Wen 2010; Wilson 1998). Overall, all appeared to recommend a large number of contractions per day (more than 100) or a minimum of 30 minutes of PFMT per day. The programmes might have affected strength or endurance, or both, depending on the number of contractions performed daily and the amount of voluntary effort with each contraction. The amount of contact with healthcare providers varied. In two trials, women participated in group exercise sessions, either three groups over a period of six weeks or a total of 70 to 80 groups over 22 weeks (Pelaez 2014; Sangsawang 2016). In another two trials, women had one‐to‐one sessions with health professionals, with three or four visits spread over eight to nine months (Glazener 2001; Wilson 1998). In three trials, the number and duration of contacts with healthcare providers was unknown (Kou 2013; Liu 2011; Wen 2010), although it is possible this was twice per week in the trial that included biofeedback (Kou 2013). Only three trials mention confirmation of correct PFM contraction, being verified by an obstetrician or by the women themselves using self‐palpation, mirror observation of the perineum or mid‐stream urine stoppage (Pelaez 2014; Sangsawang 2016; Wen 2010). In all trials, the control group received usual care that may have included advice or opportunities to do PFMT (e.g. in an antenatal class), with the exception of Sangsawang 2016 where women received usual care but no information on urinary incontinence or PFMT. Four trials provided some adherence data. The women in the trials by Glazener 2001 and Wilson 1998 were supervised individually and performed significantly more voluntary PFM contractions per day at 12 months' postpartum in the PFMT groups. The mean number of contractions was 20 (SD 29) and 86 (95% CI 69 to 104) per day in PFMT women, and 5 (SD 15) and 35 (95% CI 30 to 40) per day in control women. Glazener 2001 followed up women for six years after the index delivery. Similar proportions of women in both groups were doing some PFMT, 50% (132/263) in the intervention group and 50% (127/253) in the control group. The other two trials offered group supervision and reported adherence data for the training groups only. Pelaez 2014 reported that all PFMT women attended at least 80% of the exercise sessions (approximately 70 to 78 in total). In the trial by Sangsawang 2016, it appeared that all women had done PFMT for 28 days (of 42 in total).
Fourteen trials did not specify any details of the PFMT received by intervention group (Barakat 2011; Cruz 2014; Dokmeci 2008; Ewings 2005; Fritel 2015; Frost 2014; Frumenzio 2012; Gaier 2010; Hughes 2001; Meyer 2001; Skelly 2004; Sleep 1987; Stothers 2002; Woldringh 2007). Eight of these were conference abstracts (Cruz 2014; Dokmeci 2008; Frost 2014; Frumenzio 2012; Gaier 2010; Hughes 2001; Skelly 2004; Stothers 2002). Four trials mentioned that women were asked to do daily PFMT at home (Fritel 2015; Frumenzio 2012; Hughes 2001; Stothers 2002). One asked women to complete a daily exercise diary (Sleep 1987). Most trials provided one or more one‐to‐one supervisory sessions with a health professional, two invited women to one or two additional group sessions (Ewings 2005; Hughes 2001). Barakat 2011 provided PFMT within approximately 85 exercise classes over the course of pregnancy. Three trials confirmed a correct PFM contraction either by digital palpation or observation and palpation of the perineal body (Fritel 2015; Hughes 2001; Woldringh 2007). The control conditions were: no PFMT (Frumenzio 2012; Meyer 2001; Stothers 2002), usual care (which may or may not have included advice on PFMT) (Frost 2014; Gaier 2010; Hughes 2001; Skelly 2004), usual care that included advice about PFMT (Ewings 2005; Sleep 1987; Woldringh 2007), and PFMT at home (Cruz 2014; Fritel 2015). In two trials, the control condition was unclear (Barakat 2011; Dokmeci 2008). In five of the 14 trials, no information was provided about adherence, or the number of contacts with health professionals in either the intervention or control groups (Cruz 2014; Dokmeci 2008; Frost 2014; Frumenzio 2012; Gaier 2010). All were abstracts. Six of the 14 trials provided some information about exercise behaviour (Barakat 2011; Ewings 2005; Fritel 2015; Hughes 2001; Sleep 1987; Woldringh 2007). Three trials reported adherence data for both the intervention and control groups (Fritel 2015; Sleep 1987; Woldringh 2007). In the trial by Fritel 2015, 69% of women in the PFMT group completed all eight supervised weekly exercise sessions and 83% completed at least one. Fewer women in the PFMT group (4.3%) compared to controls (10.6%) were doing daily exercise at home at the end of pregnancy. Woldringh 2007 reported that 37% of the PFMT women were exercising intensively, compared to 14% of controls, at 36 weeks' gestation. Similarly, at three months' postpartum, Sleep 1987 reported that more women in the PFMT group (58%) compared to controls (42%) were doing some PFMT. The other three trials provided data only for the intervention group (Barakat 2011; Ewings 2005; Hughes 2001). Barakat 2011 reported "adherence to training in the experimental group was 90%" (a mean of 85 sessions in total) and Hughes 2001 (personal communication) observed that 79% of women assigned to PFMT attended the single group training session. In contrast, Ewings 2005 invited PFMT women to attend a class at two and four months postnatally and, of the 117 women, only 18% attended at two months and 4% attended at four months.
Outcome measures
Twenty‐five of the 38 trials clearly stated the primary outcome(s) of interest in the trial.
In 17 trials, it was self‐reported urinary incontinence (Assis 2015; Bø 2011; Chiarelli 2002; Cruz 2014; Ewings 2005; Fritel 2015; Glazener 2001; Gorbea 2004; Hilde 2013; Ko 2011; Kou 2013; Mørkved 2003; Pelaez 2014; Reilly 2002; Sangsawang 2016; Skelly 2004; Stafne 2012). Three used the International Consultation on Incontinence Questionnaire‐Short Form (ICIQ‐SF) (Cruz 2014; Fritel 2015; Pelaez 2014).
Three trials used loss of urine under stress test (Dumoulin 2004; Kocaoz 2013; Stothers 2002).
One trial used the Bristol Female Lower Urinary Tract Symptoms (BFLUTS; 34 question tool, higher score worse) questionnaire, quality of life domain (Kim 2012).
One trial combined data from a urinary diary and questionnaire to give an incontinence severity score (Woldringh 2007).
One trial used the unspecified "urinary condition score" (Liu 2011).
One trial used PFM strength (perineometry) (Ahlund 2013).
One trial used the occurrence of traumatic tears and use of episiotomy (Gaier 2010).
While there was some consistency in the choice of outcome measures by trialists, the differences in the measures or the way the data were reported limited the possibilities for combining results from individual trials.
Only three trials reported long‐term results after the first year (Glazener 2001; Mørkved 2003; Reilly 2002).
Excluded studies
Thirty‐eight trials were excluded for the following reasons.
Twenty‐eight studies did not collect any urinary or faecal incontinence outcome data (Agur 2005; Assis 2013; Barakat 2014; Barakat 2016; Dias 2011; Domingues 2015; Dougherty 1989; Golmakani 2015; Hou 2010; Huang 2014; Lekskulchai 2014; Li 2010; Liu 2013; Mahmoodi 2014; Morin 2015; NCT01696201; NCT01723293; NCT01753622; Nielsen 1988; Norton 1990; Oblasser 2016; Okido 2015; Perales 2016; Ruiz 2013; Siva 2014; Thorp 1994; Wang 2014; Zhu 2012).
Three trials compared the Epi‐No device versus control (Dannecker 2004; Dietz 2014; Kamisan Atan 2016). The women were recruited in very late pregnancy (33 to 37 weeks' gestation) and the primary purpose of the intervention was prevention of perineal trauma. In one trial, it seemed women did PFM contractions with the Epi‐No device in the vagina (Dannecker 2004). However, this was unclear in the other two (Dietz 2014; Kamisan Atan 2016).
Four trials included PFMT as part of an intervention but the actual comparisons were: active versus sham magnetic stimulation (Culligan 2005), one type of feedback versus another (Fynes 1999; Mahony 2004), and PFMT plus episiotomy versus caesarean section (Taskin 1996). Another trial compared abdominal exercise with no abdominal exercise (Gouldthorpe 2003).
One study was excluded because of internal inconsistencies and data discrepancies (Mason 2010).
One trial was listed in a trials register but there was no report of this trial available. There was no response to a letter sent to the principal investigator (Mason 1999).
Risk of bias in included studies
We have provided details for each trial in the Characteristics of included studies. A summary of the risk of bias for each individual trial is presented in Figure 2, while Figure 3 summarises the risk of bias across all trials included in the review.
Figure 2.
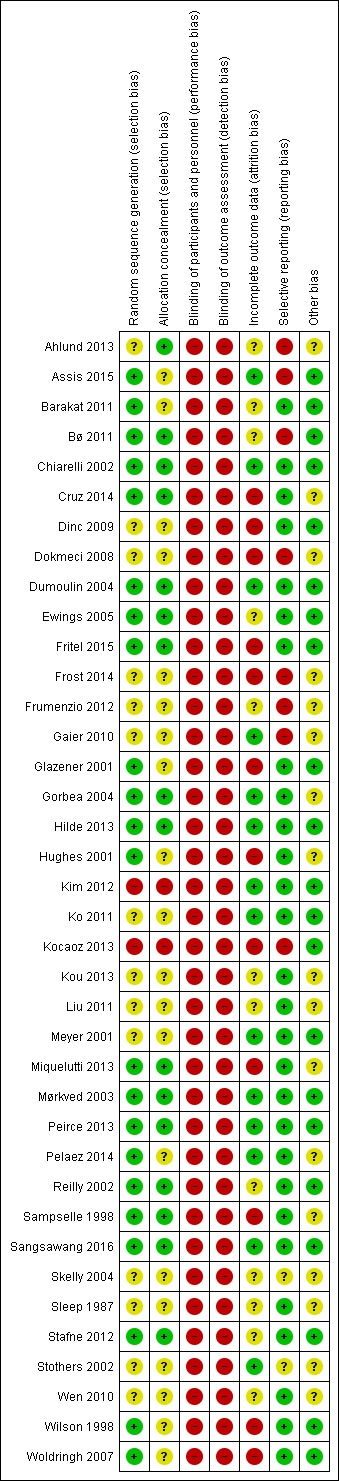
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Figure 3.
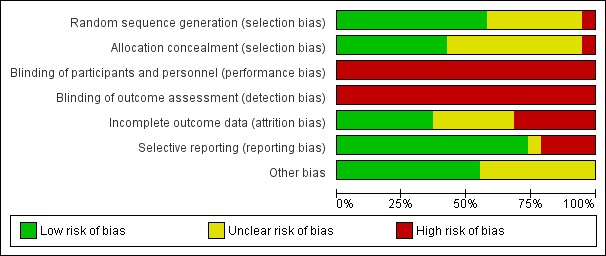
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Due to the brevity of reporting, it was difficult to assess the eight trials that were published as conference abstracts (Cruz 2014; Dokmeci 2008; Frost 2014; Frumenzio 2012; Gaier 2010; Hughes 2001; Skelly 2004; Stothers 2002). In addition, one of these abstracts did not report sample size (Skelly 2004). However, one‐to‐one randomisation was assumed. Three trials were small, with fewer than 25 women per comparison group (Dokmeci 2008; Dumoulin 2004; Kim 2012). Ten were of moderate size, with between 25 and 50 women per group (Ahlund 2013; Assis 2015; Barakat 2011; Cruz 2014; Dinc 2009; Frumenzio 2012; Gorbea 2004; Sampselle 1998; Sangsawang 2016; Stothers 2002). Twenty‐one trials allocated more than 50 women per group (Bø 2011; Chiarelli 2002; Ewings 2005; Fritel 2015; Frost 2014; Gaier 2010; Glazener 2001; Hilde 2013; Hughes 2001; Ko 2011; Kocaoz 2013; Kou 2013; Liu 2011; Meyer 2001; Miquelutti 2013; Mørkved 2003; Pelaez 2014; Reilly 2002; Stafne 2012; Wen 2010; Woldringh 2007). Three of these were large, that is, with more than 300 women per comparison group (Chiarelli 2002; Glazener 2001; Stafne 2012). Two were very large trials of more than 500 women per group (Hughes 2001; Sleep 1987). Peirce 2013 used block randomisation, meaning 30 women were allocated to PFMT and biofeedback and 90 women were included in the PFMT‐only group. Wilson and colleagues randomised just over 100 women to the control and individual treatment groups, with the individual treatment group being further randomised into three groups: PFMT only, PFMT with vaginal cones and vaginal cones only (Wilson 1998).
Twenty‐two of the 38 trials reported an a priori power calculation (Ahlund 2013; Assis 2015; Barakat 2011; Chiarelli 2002; Dinc 2009; Dumoulin 2004; Fritel 2015; Glazener 2001; Gorbea 2004; Hilde 2013; Kim 2012; Ko 2011; Meyer 2001; Miquelutti 2013; Mørkved 2003; Peirce 2013; Pelaez 2014; Reilly 2002; Sangsawang 2016; Sleep 1987; Stafne 2012; Woldringh 2007). One of the trials without a power calculation was a pilot trial (Ewings 2005).
Allocation
Random allocation generation
Twenty‐two trials provided enough information on random allocation generation for us to be reasonably sure that they had a low risk of bias (Assis 2015; Barakat 2011; Bø 2011; Chiarelli 2002; Cruz 2014; Dumoulin 2004; Ewings 2005; Fritel 2015; Glazener 2001; Gorbea 2004; Hilde 2013; Hughes 2001; Miquelutti 2013; Mørkved 2003; Peirce 2013; Pelaez 2014; Reilly 2002; Sampselle 1998; Sangsawang 2016; Stafne 2012; Wilson 1998; Woldringh 2007). Fourteen trials provided insufficient information for a judgement to be made, therefore these trials were at unclear risk of bias (Ahlund 2013; Dinc 2009; Dokmeci 2008; Frost 2014; Frumenzio 2012; Gaier 2010; Ko 2011; Kou 2013; Liu 2011; Meyer 2001; Skelly 2004; Sleep 1987; Stothers 2002; Wen 2010). Two trials were categorised as high risk of bias (Kim 2012; Kocaoz 2013). Kocaoz 2013 used methods suggestive of alternation and Kim 2012 provided participants with an envelope from which they drew one of two cards.
Random allocation concealment
Sixteen studies reported adequate allocation concealment and were at low risk of bias (Ahlund 2013; Bø 2011; Chiarelli 2002; Cruz 2014; Dumoulin 2004; Ewings 2005; Fritel 2015; Gorbea 2004; Hilde 2013; Miquelutti 2013; Mørkved 2003; Peirce 2013; Reilly 2002; Sampselle 1998; Sangsawang 2016; Stafne 2012). Two trials were at high risk of bias, being unable to adequately conceal randomisation (Kim 2012; Kocaoz 2013). The 22 remaining trials were at unclear risk of bias as insufficient information (e.g. not described or stated "randomised") was provided.
Blinding
Blinding of participants and therapists
Given the nature of the intervention, it was not feasible for the included trials to blind the treatment provider or participants to group allocation and so all 38 trials were at high risk of performance bias. The difficulty of blinding exercise‐based interventions is a common problem.
Blinding of outcome assessment
Because the two main outcomes of interest in this review, urinary incontinence and incontinence‐specific quality of life, are self‐reported, these are unblinded measures. As a result, all 38 trials were deemed to be at high risk of detection bias. Blinded outcome assessment should be possible for some secondary outcomes, such as pad testing, and 12 trials attempted this (Bø 2011; Chiarelli 2002; Cruz 2014; Dumoulin 2004; Fritel 2015; Glazener 2001; Hilde 2013; Kim 2012; Mørkved 2003; Reilly 2002; Sampselle 1998; Stothers 2002).
Incomplete outcome data
Reporting of dropout and withdrawal and analysis by intention to treat
Based on the criteria for assessment of attrition bias reported in the methods (see 'Assessment of risk of bias' in Included studies), 10 trials were at low risk of attrition bias (Assis 2015; Chiarelli 2002; Dumoulin 2004; Hilde 2013; Kim 2012; Ko 2011; Meyer 2001; Pelaez 2014; Sangsawang 2016; Stothers 2002). Another 10 were at unclear risk (Ahlund 2013; Barakat 2011; Frumenzio 2012; Kou 2013; Liu 2011; Reilly 2002; Skelly 2004; Sleep 1987; Stafne 2012; Wen 2010). Some trials did not report on losses to follow‐up and were at unclear risk of bias (Bø 2011; Frumenzio 2012; Kou 2013; Liu 2011; Skelly 2004; Wen 2010). Two of these were abstracts (Frumenzio 2012; Skelly 2004). The remaining 12 trials were at high risk. All trials appeared to analyse participants in the groups to which they were assigned.
Selective reporting
All outcomes appeared to have been reported in the majority of trials, with 28 of 38 trials assessed at low risk of bias in this domain. Eight trials were at high risk of bias. Six of these did not report all of the prespecified outcome measures (Ahlund 2013; Assis 2015; Bø 2011; Dokmeci 2008; Frumenzio 2012; Gaier 2010), and, of these, two also did not state the a priori primary outcome measure (Dokmeci 2008; Frumenzio 2012). A further two were at high risk due to not presenting data that related to a key outcome of the review (i.e. self‐reported urinary incontinence) (Frost 2014; Kocaoz 2013). Three of these were conference abstracts (Dokmeci 2008; Frost 2014; Frumenzio 2012). Two trials were at unclear risk of bias as it was uncertain if selective reporting had taken place (Skelly 2004; Stothers 2002).
Other potential sources of bias
From the 38 trials in this review, we considered 21 to be free of problems (such as conflict of interest) that could put them at risk of other bias. We considered the risk of other bias as unclear for 17 trials (Ahlund 2013; Cruz 2014; Dokmeci 2008; Frost 2014; Frumenzio 2012; Gaier 2010; Gorbea 2004; Hughes 2001; Kou 2013; Liu 2011; Miquelutti 2013; Pelaez 2014; Sampselle 1998; Skelly 2004; Sleep 1987; Stothers 2002; Wen 2010).
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5
There were some data available to explore the hypothesis that PFMT is better than usual antenatal and postnatal care, or no treatment, for the prevention or treatment of urinary and faecal incontinence. The primary analysis investigated the prevalence of urinary and faecal incontinence. Data for outcomes of secondary interest (in 'Other data' tables) are only briefly discussed to give an indication of whether the findings were broadly consistent with the pooled data, or not. Thirty‐four trials contributed data to one or more forest plots. The four trials that did not were by Ahlund 2013, Dokmeci 2008, Frost 2014, and Liu 2011.
The 'Summary of findings' tables present the selected outcomes for each of the five main comparisons.
Antenatal PFMT compared to control for prevention of urinary and faecal incontinence: Table 1.
Antenatal PFMT compared to control for treatment of urinary and faecal incontinence: Table 2.
Antenatal PFMT compared to control for mixed prevention and treatment of urinary and faecal incontinence: Table 3.
Postnatal PFMT compared to control for treatment of urinary and faecal incontinence: Table 4.
Postnatal PFMT compared to control for mixed prevention and treatment of urinary and faecal incontinence: Table 5.
Comparison 1: antenatal pelvic floor muscle training for prevention of incontinence
Ten trials reported antenatal PFMT for prevention of incontinence (Barakat 2011; Gaier 2010; Gorbea 2004; Kocaoz 2013; Mørkved 2003; Pelaez 2014; Reilly 2002; Sampselle 1998; Sangsawang 2016; Stothers 2002). Seven recruited nulliparous or primiparous or primigravid women during pregnancy (Gaier 2010; Gorbea 2004; Mørkved 2003; Pelaez 2014; Reilly 2002; Sampselle 1998; Sangsawang 2016). The other three recruited "pregnant women" or both primiparous and multiparous women (Barakat 2011; Kocaoz 2013; Stothers 2002). All women were continent at recruitment.
In all 10 trials, PFMT began during pregnancy. Controls were asked not to do PFMT, did not receive instruction on PFMT, received usual care that might have included information on PFMT, or the control condition was not specified (Barakat 2011; Gaier 2010; Gorbea 2004; Kocaoz 2013; Mørkved 2003; Pelaez 2014; Reilly 2002; Sampselle 1998; Sangsawang 2016; Stothers 2002).
Two of these trials were mixed prevention and treatment trials but published or unpublished data were available for women who were continent at recruitment (Mørkved 2003; Sampselle 1998). In Sampselle 1998, 54/72 women were continent based on a standing stress test at 20 weeks' gestation. After dropouts, there were unpublished data from 37 previously continent women (16 PFMT and 21 controls). Mørkved 2003 published data for 207/301 women who were continent before pregnancy and at 20 weeks' gestation. After dropouts, there were data from 193 previously continent women (94 PFMT and 99 controls). Neither trial was powered to find differences in the previously continent subgroup, as the subgroup sizes were small.
Primary outcome
Self‐reported urinary or faecal incontinence
Women randomised to PFMT were about 62% less likely to report urinary incontinence in late pregnancy compared to controls (RR 0.38, 95% CI 0.20 to 0.72; 6 trials, 624 women, random‐effects, I² = 78%, T² = 0.44; low‐quality evidence) (Analysis 1.1).
Analysis 1.1.
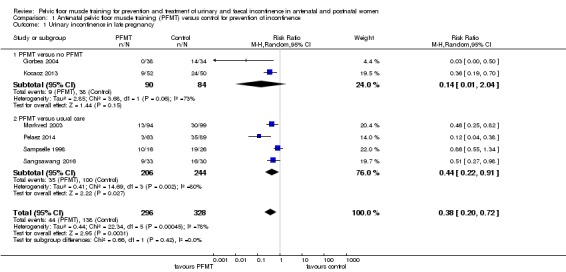
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 1 Urinary incontinence in late pregnancy.
There was statistically significant heterogeneity in this comparison and in both subgroups (PFMT versus no PFMT, PFMT versus usual care). A random‐effects model was used because of the heterogeneity. Two trials appeared to contribute most to the heterogeneity (Gorbea 2004; Pelaez 2014), and both found many fewer cases of urinary incontinence in the intervention than control groups. Gorbea 2004 was the only trial that specifically asked controls not to do PFMT during pregnancy. In addition, as none of the PFMT women reported urinary incontinence in late pregnancy, the point estimate and CIs were perhaps less stable given there were no events in one of the two comparison groups. In Pelaez 2014, the PFMT was very intensive and of longer duration than other trials in the same subgroup. The intervention included three supervised exercise classes per week for at least 22 weeks and 80% of women attended the maximum number of classes.
PFMT women were about 62% less likely to report urinary incontinence, compared to controls, in the early postpartum period (RR 0.38, 95% CI 0.17 to 0.83; 5 trials, 439 women, random‐effects, I² = 74%, T² = 0.55) (Analysis 1.2). There was statistically significant heterogeneity in this comparison, as well as in one subgroup (PFMT versus usual care), which included the trial by Pelaez 2014 (see above).
Analysis 1.2.
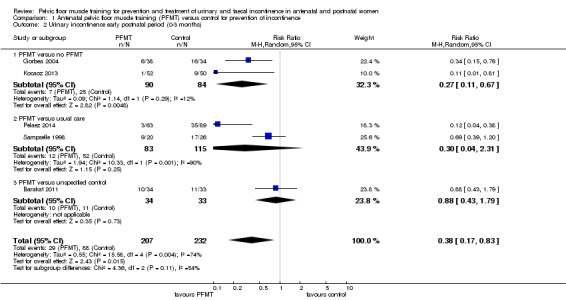
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 2 Urinary incontinence early postnatal period (0‐3 months).
PFMT women were still less likely than controls to have urinary incontinence in the mid‐postnatal period (three to six months), although the difference in risk had reduced to 29% (RR 0.71, 95% CI 0.54 to 0.95; 5 trials, 673 women, fixed‐effect, I² = 0%; moderate‐quality evidence) (Analysis 1.3). Overall, the pooled estimate favoured PFMT.
Analysis 1.3.
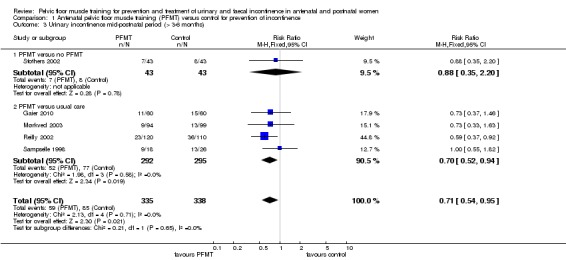
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 3 Urinary incontinence mid‐postnatal period (> 3‐6 months).
There were not enough participants (44 women; low‐quality evidence) in the trial by Sampselle 1998 to identify whether there was a difference in prevalence of urinary incontinence between PFMT women and women in the control group at 12 months' postpartum (RR 1.20, 95% CI 0.65 to 2.21) (Analysis 1.4).
Analysis 1.4.
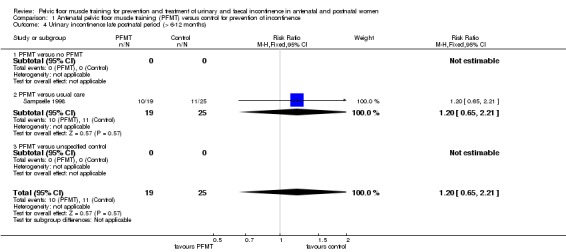
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 4 Urinary incontinence late postnatal period (> 6‐12 months).
Two trials measured incontinence at greater than five years (Mørkved 2003; Reilly 2002; seeTable 11 ). The pooled data suggested that the earlier effectiveness of PFMT did not persist in the long term (RR 1.07, 95% CI 0.77 to 1.48; 2 trials, 352 women, fixed‐effect, I² = 25%) (Analysis 1.6). Reilly 2002 found that 68.4% of women randomised to the intervention group were still performing PFMT, with 38% doing PFMT at least twice per week after eight years. Mørkved 2003 reported that the same number of women in the PFMT and control groups (45%) were exercising at least weekly, six years after the primary study. The lack of a difference in prevalence rates of incontinence in these three trials suggests that perhaps PFMT is not effective in the long term. There could be three immediately plausible explanations for this. The women may have stopped exercising, they may have had subsequent pregnancies or, as shown by Mørkved 2003, women were performing similar PFMT regimens regardless of which group they had initially been randomised.
Analysis 1.6.
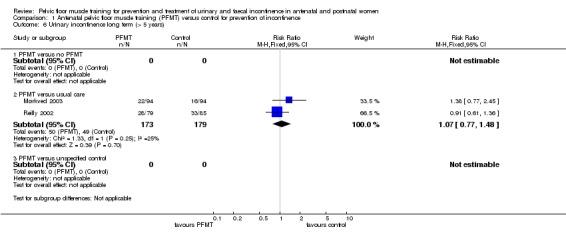
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 6 Urinary incontinence long term (> 5 years).
None of the 10 trials reported data on the prevalence of either antenatal or postpartum faecal incontinence.
Incontinence‐specific quality of life
Reilly 2002 (King's Health Questionnaire) and Pelaez 2014 (ICIQ‐SF) were the only two trials to mention incontinence‐specific quality of life. Pelaez 2014 found a difference between the two groups in favour of PFMT (MD ‐2.42, 95% CI ‐3.32 to ‐1.52; 2 trials, 152 women; moderate‐quality evidence) (Analysis 1.13; lower score indicates better incontinence‐specific quality of life). Reilly 2002 did not report their data but stated there was no difference between the groups on any of the eight subscales (Analysis 1.14).
Analysis 1.13.
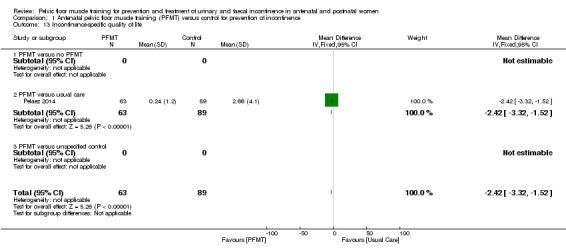
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 13 Incontinence‐specific quality of life.
Analysis 1.14.
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 14 Severity of incontinence.
Severity of incontinence
| Study | Measure of | Outcome measure | PFMT data | Control data | Difference |
|---|---|---|---|---|---|
| PFMT versus no PFMT | |||||
| Stothers 2002 | Frequency of leakage | Leakage episodes in 5 days | Mean 3.4, SD not reported, n=7 at 6 months postpartum | Mean 6.0, SD not reported, n=8 at 6 months postpartum | Not calculable |
| Stothers 2002 | Amount of leakage | Volume of urine loss (g) on stress test with standardised bladder volume | Mean 18, SD not reported, n=? at 6 months postpartum | Mean 38, SD not reported, n=? at 6 months postpartum | Not calculable |
| Stothers 2002 | Other leakage severity | Not measured | |||
| PFMT versus usual care | |||||
| Gorbea 2004 | Frequency of leakage | Less than weekly, weekly or daily urinary incontinence (not clear if self‐reported or from urinary diary) | 4 less than weekly, 2 weekly and none with daily leakage, n=38 at 6 weeks postpartum | 6 less than weekly, 8 weekly and 2 with daily leakage, n=34 at 6 weeks postpartum | Not calculated as validity/reliability of this measure not known |
| Gorbea 2004 | |||||
| Gorbea 2004 | Other leakage severity | Grade I, II or III leakage, where I=loss of urine with coughing or lifting, II=urine leakage when walking, and III=urine leakage when upright | 6 grade I, and none with grade II or III leakage, n=38 at 6 weeks postpartum | 10 grade I, 6 grade II, and none grade III leakage, n=34 at 6 weeks postpartum | Not calculated as validity/reliability of this measure not known |
| Pelaez 2014 | Frequency of leakage | Self‐reported leakage frequency categorised as never, once a week, 2‐3 times a week, once a day, several times a day, all the time (item 3, ICIQ‐SF) | 60 never, 3 once a week, n=63 at 36‐40 weeks gestation | 54 never, 18 once a week, 9 2‐3 times a week, 7 once a day, 1 several times a day, n=89 | Author reported p‐value 0.0001 |
| Pelaez 2014 | Amount of leakage | Self‐reported amount of leakage categorised as none, small, moderate, large (item 4, ICIQ‐SF) | 60 none, 3 small, n=63 at 36‐40 weeks gestation | 54 report none, 27 a small, 5 moderate, 3 large, n=89 | Author reported p‐value 0.0001 |
| Pelaez 2014 | Symptom bother | Symptom impact, numbered VAS 0‐10 (10 worse) (item 5, ICIQ‐SF) | Mean 0.10, SD 0.64, n=63 | Mean 0.97, SD 1.8, n=89 | Mean difference ‐0.87 (95% CI ‐1.28 to ‐0.46) |
| Reilly 2002 | Incontinence‐specific quality of life | King's Health Questionnaire | Not reported | Not reported | "No difference between the study groups on any of the 8 scales, and all mean scores were low" |
| Reilly 2002 | |||||
| Reilly 2002 | Other leakage severity | Mild, moderate or severe urinary incontinence (not clear how categorised) | 19 mild, 3 moderate and 1 severe, n=74 at 3 months postpartum | 30 mild, 5 moderate and 1 severe, n=74 at 3 months post partum | Not calculated as validity/reliability of this measure not known |
| Sampselle 1998 | Frequency of leakage | Not measured | |||
| Sampselle 1998 | Amount of leakage | Not measured | |||
| Sampselle 1998 | Other leakage severity | Average score from questionnaire re urine leakage with gentle cough, hard cough, sneeze and laugh scored 0 for none, 1 for dampness, 2 for wetness and 3 for soaked | Mean 0.30, standard deviation 0.44, n=16 at 12 months postpartum | Mean 0.32, standard deviation 0.41, n=21 at 12 months postpartum | Not calculated as validity/reliability of this measure not known |
| Sangsawang 2016 | Frequency of leakage | Bladder diary, number of leakages per week | Mean 12.4, SD 5.3, n=9 of 33 at 38 weeks gestation | Mean 23.1, SD 5.7, n=16 of 30 at 38 weeks gestation | Mean difference ‐8.9 (95% CI ‐13.7 to ‐4.0) |
| Sangsawang 2016 | Amount of leakage | Self‐reported: none, small (drops), moderate (wetting underwear), large (wetting outer clothing) | None 24, small 2, moderate 4, large 3 | None 14, small 2, moderate 8, large 6 | Author reported p‐value 0.03 |
| Sangsawang 2016 | Other leakage severity | Perceived severity on VAS (0‐10) | Mean 5.0, SD 0.9, n=9 of 33 | Mean 6.3, SD 1.2, n=16 of 30 | Mean difference ‐2.0 (95% CI ‐3.4 to ‐0.6) |
| PFMT versus unspecified control | |||||
| Barakat 2011 | Frequency of leakage | Self‐reported leakage frequency categorised as never, once a week, 2‐3 times a week, once a day, several times a day, all the time (item 3, ICIQ‐SF) | 24 never, 5 once a week, 2 2‐3 times a week, 2 once a day, 1 several times a day, n=34 | 22 never, 5 once a week, 1 2‐3 times a week, 2 once a day, 3 several times a day, n=33 | Author reported p‐value >0.05 |
| Barakat 2011 | Amount of leakage | Self‐reported amount of leakage categorised as none, small, moderate, large (item 4, ICIQ‐SF) | Not reported | Not reported | |
| Barakat 2011 | Other leakage severity | ||||
Secondary outcomes
Severity of incontinence
Seven of the 10 trials reported some data on symptom severity, such as frequency or amount of urine leakage (Analysis 1.14) (Barakat 2011; Gorbea 2004; Pelaez 2014; Reilly 2002; Sampselle 1998; Sangsawang 2016; Stothers 2002). The choice of measures (many of these of unknown validity) or the ways of reporting these were highly variable and data reporting was often incomplete. Two of the most recent trials used individual item scores from the ICIQ‐SF; frequency (item 3) and amount of leakage (item 4) (Barakat 2011; Pelaez 2014). There was a consistent pattern of effect in favour of PFMT, when compared to usual care, for frequency, amount and other urinary incontinence severity indices in two trials (Pelaez 2014; Sangsawang 2016).
Number of urinary or faecal incontinence episodes
None of the trials reported number of urinary or faecal incontinence episodes.
Loss of urine under stress test
Three trials reported whether women were continent or not based on a stress test (positive cough or one‐hour pad test) (Gorbea 2004; Kocaoz 2013; Reilly 2002). Women in the PFMT group were less likely to be incontinent in late pregnancy (RR 0.36, 95% CI 0.19 to 0.70; 1 trial, 102 women) or in the early postnatal period (RR 0.09, 95% CI 0.02 to 0.47; 2 trials, 174 women, fixed‐effect, I² = 0%) when compared with no treatment controls (Analysis 1.15; Analysis 1.16) (Gorbea 2004; Kocaoz 2013). There was no difference between PFMT versus usual care groups in the early postnatal period (RR 0.88, 95% CI 0.33 to 2.29; 1 trial, 148 women) (Analysis 1.16) (Reilly 2002). Two trials used the SF‐36 (Barakat 2011; Reilly 2002). In the general health domain, Reilly 2002 reported that the PFMT group scored significantly higher than the control group at three months' postpartum (MD 7.2, 95% CI 2.36 to 12.04), while Barakat 2011 found that women in the PFMT group were more likely to rate their health as very good (18/34 women in the PFMT group versus 9/33 women in the control group) (Analysis 1.17).
Analysis 1.15.
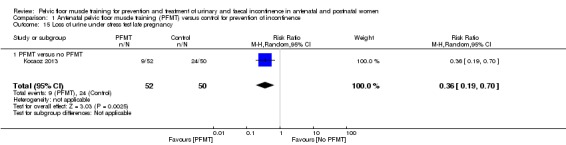
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 15 Loss of urine under stress test late pregnancy.
Analysis 1.16.
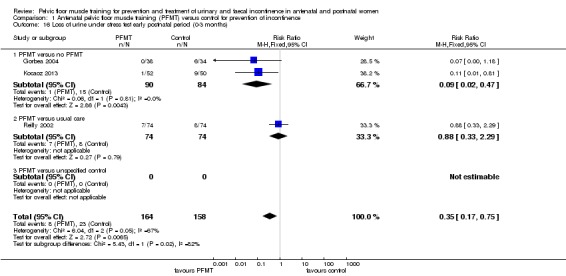
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 16 Loss of urine under stress test early postnatal period (0‐3 months).
Analysis 1.17.
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 17 Quality of life and health status measures.
Quality of life and health status measures
| Study | Outcome measure | PFMT data | Control data | Difference |
|---|---|---|---|---|
| PFMT versus usual care | ||||
| Reilly 2002 | SF‐36, general health scale (0=worst, 100=best) | Mean 84.4, SD 13.5, n=76 | Mean 77.2, SD 16.3, n=72 | Mean difference 7.2 (95% CI 12.04, 2.36) |
| PFMT versus unspecified control | ||||
| Barakat 2011 | Maternal perception of health status (presume an item derived from SF‐36). Rated as very bad, somewhat bad, good or very good | 1 very bad, 14 good, 18 very good, n=34 | 1 very bad, 5 somewhat bad, 18 good, 9 very good, n=33 | |
Other quality of life and health status measures
None of the trials reported other quality of life and health status measures.
Health economics
None of the trials reported health economic data.
Adverse effects
Only one trial noted any adverse events: two of 43 PFMT women withdrew due to pelvic floor pain (Stothers 2002). Barakat 2011 stated "there were no exercise‐related injuries experienced during pregnancy." No other trial reported whether there were adverse effects or not.
Other outcomes
Pelvic floor muscle function
Three trials measured PFM function (Gaier 2010; Gorbea 2004; Reilly 2002). However, Gaier 2010 reported no data. Measures were electromyography and vaginal squeeze pressure (Gorbea 2004; Reilly 2002). The lack of explanation of the type of electromyography and unusual presentation of the data in Gorbea 2004 made it difficult to interpret the findings. In Reilly 2002, mean vaginal squeeze pressure was not greater in the PFMT group than the control group (MD 1.00, 95% CI ‐1.31 to 3.31) (Analysis 1.18). Gaier 2010 reported significantly higher PFM strength in women doing PFMT. However, it was unclear how this was measured and the data were not given in the conference abstract.
Analysis 1.18.
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 18 Pelvic floor muscle function.
Pelvic floor muscle function
| Study | Outcome measure | PFMT data | Control data | Difference |
|---|---|---|---|---|
| PFMT versus no PFMT | ||||
| Gorbea 2004 | No or minimal contraction on electromyography. Not clear what type of electromyography or how categorised | 14 of 14 at 6 weeks postpartum | 10 of 12 at 6 weeks postpartum | Not calculated as validity/reliability of this measure not known |
| PFMT versus usual care | ||||
| Gaier 2010 | PF muscle strength (measure not reported) | Significantly higher in the training group at 12 weeks after delivery (p < 0.05) | ||
| Reilly 2002 | Vaginal squeeze pressure (need unit of measurement), early post‐natal | Mean 11.5, SD 7.8, n=68 | Mean 10.5, SD 5.5, n=64 | Mean difference 1.0 (95% CI ‐1.31 to 3.31) |
Delivery outcome
Five trials reported delivery outcome (Barakat 2011; Gaier 2010; Gorbea 2004; Reilly 2002; Stothers 2002). However, the data by Stothers 2002 were not reported by group. Three trials reported the number of caesarean sections (Barakat 2011; Gorbea 2004; Reilly 2002). There was no difference between PFMT and control groups in any of these trials (RR 1.28, 95% CI 0.89 to 1.85; 3 trials, 373 women, fixed‐effect, I² = 49%) (Analysis 1.19). Two trials reported type of vaginal delivery (normal or instrumental) (Barakat 2011; Reilly 2002). Two trials reported perineal trauma (Barakat 2011; Gaier 2010). There were no apparent differences between groups for either outcome (Analysis 1.20).
Analysis 1.19.
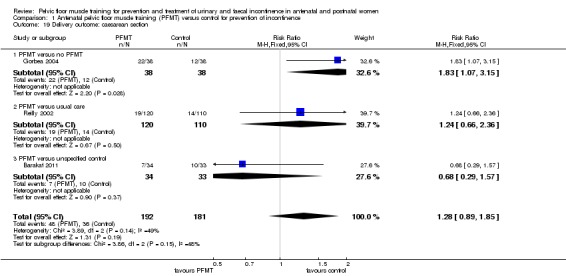
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 19 Delivery outcome: caesarean section.
Analysis 1.20.
Comparison 1 Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence, Outcome 20 Delivery outcome: other.
Delivery outcome: other
| Study | Outcome measure | PFMT data | Control data | Difference |
|---|---|---|---|---|
| PFMT versus no control | ||||
| Stothers 2002 | Type of delivery | 73.3% vaginal, 26.7% caesarean; not reported per group | ||
| Stothers 2002 | ||||
| PFMT versus usual care | ||||
| Gaier 2010 | Number with episiotomy | 2 of 65 | 6 of 62 | Relative risk 0.32 (95% CI 0.07 to 1.52) |
| Gaier 2010 | Perineal trauma | 0.5% | 4.2% | Unable to calculate |
| Reilly 2002 | Type of delivery | 78 normal vaginal, 13 ventouse, 8 forceps, n=120 | 72 normal vaginal, 22 ventouse, 2 forceps, n=110 | Relative risk for normal vaginal delivery 0.99 (95% CI 0.82 to 1.20) Relative risk for assisted vaginal delivery 0.80 (95% CI 0.47 to 1.36) |
| Reilly 2002 | ||||
| PFMT versus unspecified control | ||||
| Barakat 2011 | Type of delivery | 20 normal vaginal, 7 assisted vaginal, n=34 | 18 normal vaginal, 5 assisted vaginal, n=33 | Relative risk for normal vaginal delivery 1.08 (95% CI 0.71 to 1.64) Relative risk for assisted vaginal delivery 1.36 (95% CI 0.48 to 3.86) |
| Barakat 2011 | Perineal trauma | 22 intact perineum, 6 grade 1 tear, 5 grade 2 tear, 1 grade 3 tear, n=34 | 19 intact perineum, 6 grade 1 tear, 8 grade 2 tear, 0 grade 3 tear, n=33 | Relative risk for perineal tear 0.83 (95% CI 0.45 to 1.52) |
Any other outcome not prespecified but of interest
None of the trials reported any other outcomes not prespecified but of interest.
Comparison 2: antenatal pelvic floor muscle training for treatment of incontinence
Four trials reported antenatal PFMT for treatment of incontinence (Cruz 2014; Dinc 2009; Skelly 2004; Woldringh 2007). Two trials recruited primiparous and multiparous women (Dinc 2009; Woldringh 2007). Two trials reported as abstracts did not state parity (Cruz 2014; Skelly 2004). In all four trials, the control group received usual care.
Primary outcome
Self‐reported urinary or faecal incontinence
There was no difference in prevalence of urinary incontinence in late pregnancy (RR 0.70, 95% CI 0.44 to 1.13; 3 trials, 345 women, random‐effects, I² = 71%, T² = 0.11; very low‐quality evidence) (Analysis 2.1).
Analysis 2.1.
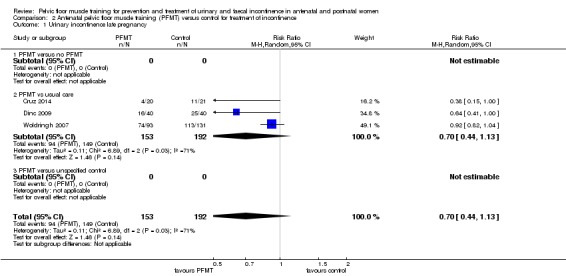
Comparison 2 Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 1 Urinary incontinence late pregnancy.
This comparison showed statistically significant heterogeneity; a random‐effects model was used to provide a more conservative estimate (Analysis 2.1).
There were no differences in the early postnatal period (RR 0.75, 95% CI 0.37 to 1.53; 2 trials, 292 women, random‐effects, I² = 65%, T² = 0.19) or mid‐postnatal period (RR 0.94, 95% CI 0.70 to 1.24; 1 trial, 187 women; very low‐quality evidence) (Analysis 2.2; Analysis 2.3).
Analysis 2.2.
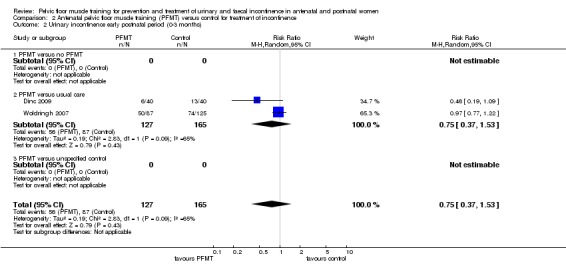
Comparison 2 Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 2 Urinary incontinence early postnatal period (0‐3 months).
Analysis 2.3.
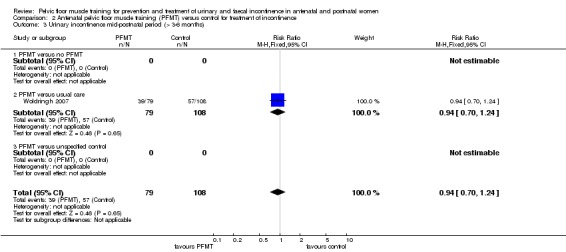
Comparison 2 Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 3 Urinary incontinence mid‐postnatal period (> 3‐6 months).
Two trials measured urinary incontinence in the late postnatal period. A random‐effects model was used because of statistically significant heterogeneity in this comparison and there was no difference between groups (RR 0.50, 95% CI 0.13 to 1.93; 2 trials, 869 women, random‐effects, I² = 94%, T² = 0.89; very low‐quality evidence) (Analysis 2.4) (Skelly 2004; Woldringh 2007). Skelly 2004 was available only as a conference abstract with limited data on which to base a risk of bias assessment and about half of the women randomised appeared to have urinary incontinence symptoms pre‐pregnancy. In Woldringh 2007, at 35 weeks' gestation, about two‐thirds of women in the control group were doing some form of PFMT, compared to 94% in the PFMT group. These, or other unknown reasons, could have contributed to the observed heterogeneity.
Analysis 2.4.
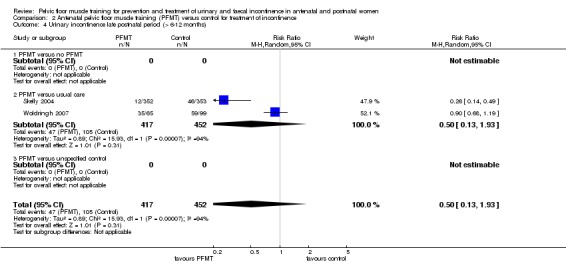
Comparison 2 Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 4 Urinary incontinence late postnatal period (> 6‐12 months).
None of the four trials reported data on the prevalence of either antenatal or postpartum faecal incontinence.
Incontinence‐specific quality of life
Two trials used a validated incontinence‐specific quality of life measure (Cruz 2014, ICIQ‐SF; Woldringh 2007, IIQ). Cruz 2014 found a better quality of life in PFMT women in late pregnancy (MD ‐3.50, 95% CI ‐6.13 to ‐0.87; 1 trial, 41 women, low‐quality evidence) (Analysis 2.14; lower score better). Woldringh 2007 categorised IIQ scores, which meant that it was not possible to interpret these data (Analysis 2.15).
Analysis 2.14.
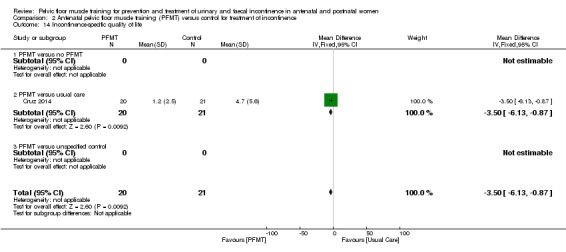
Comparison 2 Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 14 Incontinence‐specific quality of life.
Analysis 2.15.
Comparison 2 Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 15 Quality of life and health status measures.
Quality of life and health status measures
| Study | Outcome measure | PFMT data | Control data | Difference |
|---|---|---|---|---|
| PFMT versus usual care | ||||
| Woldringh 2007 | Incontinence Impact Questionnaire (IIQ), and data then dichotomised into impact versus no impact in four subscales ‐ impact on social relations, impact on emotional health, impact on recreational activities, and impact on physical activities (not clear how this was done) | Impact on social relations 2, on emotional health 11, on recreational activities 10, and on physical activities 4, n=65 at 12 months postpartum | Impact on social relations 5, on emotional health 14, on recreational activities 10, and on physical activities 7, n=99 at 12 months postpartum | Not calculated as validity/reliability of this measure not known |
| Woldringh 2007 | ||||
Secondary outcomes
Severity of incontinence
Woldringh 2007 reported on leakage severity, but the validity of this measure is unknown (Analysis 2.16).
Analysis 2.16.
Comparison 2 Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 16 Severity of incontinence.
Severity of incontinence
| Study | Measure of | Outcome measure | PFMT data | Control data | Difference |
|---|---|---|---|---|---|
| PFMT versus usual care | |||||
| Woldringh 2007 | Frequency of leakage | 7 day urinary diary | Not reported | Not reported | |
| Woldringh 2007 | Amount of leakage | Not measured | |||
| Woldringh 2007 | Other leakage severity | A combination of data from a 7 day bladder diary and a questionnaire (PRAFAB, Vierhout 1990), ending with a score between 0 and 10. Mild urinary incontinence 0 to 4, and moderate to severe incontinence 5 to 10 | 9 with moderate to severe leakage, n=65 at 12 months postpartum | 8 with moderate to severe leakage, n=99 at 12 months postpartum | Not calculated as validity/reliability of this measure not known |
Number of urinary or faecal incontinence episodes
None of the trials reported number of urinary or faecal incontinence episodes.
Loss of urine under stress test
None of the trials reported loss of urine under stress test.
Other quality of life and health status measures
None of the trials reported other quality of life and health status measures.
Health economics
None of the trials reported health economic data.
Adverse effects
None of the trials reported on adverse effects.
Other outcomes
Pelvic floor muscle function
Cruz 2014 found no difference between the groups in maximal vaginal squeeze pressure in the third trimester (Analysis 2.17).
Analysis 2.17.
Comparison 2 Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 17 Pelvic floor muscle function.
Pelvic floor muscle function
| Study | Outcome measure | PFMT data | Control data | Difference |
|---|---|---|---|---|
| PFMT versus usual care | ||||
| Cruz 2014 | Maximal vaginal squeeze pressure, in cm water (Peritron) | Mean 29.8, SD 18.8, n=20 in third trimester | Mean 24.2, SD 12.9, n=21 in third trimester | Mean difference 5.6 (95% CI ‐4.32 to 15.52) |
| Cruz 2014 | ||||
Comparison 3: antenatal pelvic floor muscle training for mixed prevention and treatment of incontinence
Eleven trials reported antenatal PFMT for mixed prevention and treatment of incontinence (Assis 2015; Bø 2011; Dokmeci 2008; Fritel 2015; Frumenzio 2012; Hughes 2001; Ko 2011; Miquelutti 2013; Mørkved 2003; Sampselle 1998; Stafne 2012). The control group consisted of usual care in seven trials (Bø 2011; Fritel 2015; Hughes 2001; Miquelutti 2013; Mørkved 2003; Sampselle 1998; Stafne 2012). There was no PFMT in two trials (Assis 2015; Ko 2011). Two did not specify the control group (Dokmeci 2008; Frumenzio 2012).
Nine trials were in women who were delivering their first baby (Assis 2015; Bø 2011; Dokmeci 2008; Fritel 2015; Hughes 2001; Ko 2011; Miquelutti 2013; Mørkved 2003; Sampselle 1998). One recruited both primiparous and multiparous women (Stafne 2012). Parity was not stated in Frumenzio 2012, which was an abstract.
Primary outcome
Self‐reported urinary or faecal incontinence
Women randomised to PFMT had about 26% less risk of urinary incontinence in late pregnancy (RR 0.74, 95% CI 0.61 to 0.90; 9 trials, 3164 women, random‐effects, I² = 82%, T² = 0.06; low‐quality evidence) (Analysis 3.1).
Analysis 3.1.
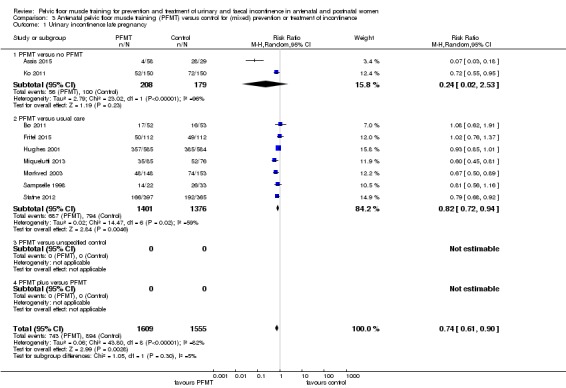
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 1 Urinary incontinence late pregnancy.
There was statistically significant heterogeneity in both subgroups (PFMT versus no exercise and PFMT versus usual care) in this comparison (Analysis 3.1). The point estimates favoured PFMT in all but two trials (Bø 2011; Fritel 2015). In the seven trials where the point estimates favoured PFMT, there was considerable variation with RR ranging from 0.07 to 0.93 (Assis 2015; Hughes 2001; Ko 2011; Miquelutti 2013; Mørkved 2003; Sampselle 1998; Stafne 2012). The data that appeared notably different, being markedly in favour of PFMT, were those from Assis 2015 for reasons unknown, although this was one of two trials in which controls were asked not to do PFMT. In the two trials where the point estimates did not favour PFMT, there were plausible explanations for no differences between the two groups. Participants in Bø 2011 were encouraged to attend at least two out of three possible exercise classes every week. These exercise classes were led by general fitness instructors who were taught by a physiotherapist how to deliver PFMT to women. It may be that the women in this trial considered the classes solely as general fitness and did not concentrate on the PFMT component. In Fritel 2015, the authors reported that at the end of pregnancy there was no difference in the frequency and duration of PFMT between groups, suggesting no difference in exercise adherence between the PFMT and usual care groups.
There was a difference in the prevalence of urinary incontinence between antenatal PFMT and control groups in the early postnatal (RR 0.80, 95% CI 0.67 to 0.95; 5 trials, 760 women, fixed‐effect, I² = 0%, T² = 0.00) (Analysis 3.2) and mid‐postnatal periods (RR 0.73, 95% CI 0.55 to 0.97; 5 trials, 1921 women, random‐effects, I² = 65%, T² = 0.06; very low‐quality evidence) (Analysis 3.3), but not in the late postnatal period (RR 0.85, 95% CI 0.63 to 1.14; 2 trials, 244 women, fixed‐effect, I² = 0%; low‐quality evidence) (Analysis 3.4).
Analysis 3.2.
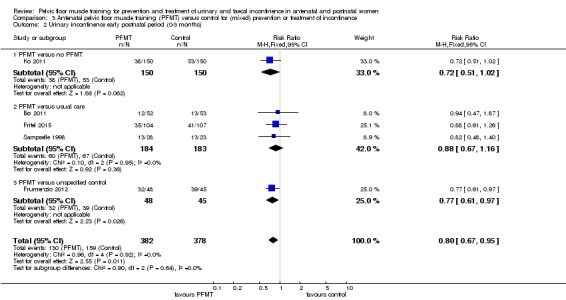
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 2 Urinary incontinence early postnatal period (0‐3 months).
Analysis 3.3.
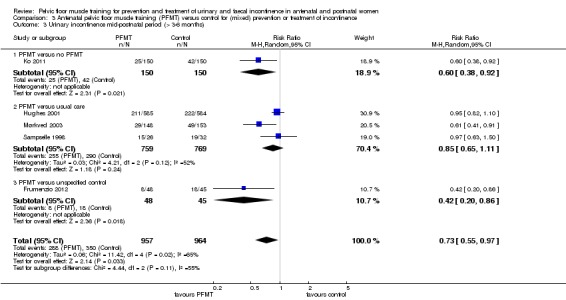
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 3 Urinary incontinence mid‐postnatal period (> 3‐6 months).
Analysis 3.4.
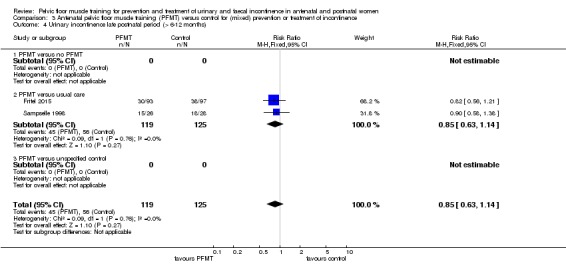
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 4 Urinary incontinence late postnatal period (> 6‐12 months).
In the mid‐postnatal period, while all the point estimates favoured PFMT, these varied considerably between the trials (RRs of 0.42 to 0.97). In the one trial with long‐term data (six years), Mørkved 2003, there was no difference between groups (RR 1.38, 95% CI 0.77 to 2.45; 1 trial, 188 women) (Analysis 3.6). Women in the control group were offered a description of the PFMT programme after the post‐treatment comparison and this and other events (such as subsequent births) may have contributed to a lack of difference.
Analysis 3.6.
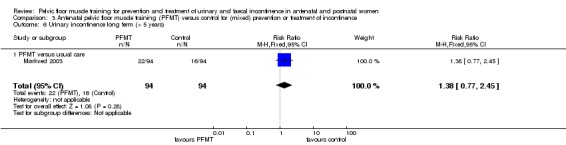
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 6 Urinary incontinence long term (> 5 years).
Two trials collected data on faecal incontinence in late pregnancy (Bø 2011; Stafne 2012). Bø 2011 also reported on faecal incontinence in the early postnatal period. There were no differences between PFMT and usual care groups at either time‐point (late pregnancy: RR 0.61, 95% CI 0.30 to 1.25; 2 trials, 867 women, fixed‐effect; moderate‐quality evidence; early postnatal: RR 0.36, 95% CI 0.04 to 3.37; 1 trial, 90 women) (Analysis 3.7; Analysis 3.8).
Analysis 3.7.
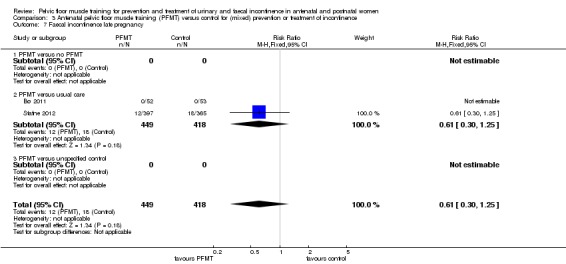
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 7 Faecal incontinence late pregnancy.
Analysis 3.8.
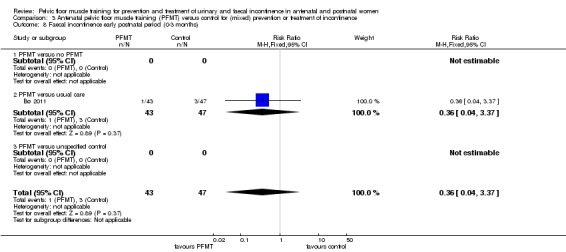
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 8 Faecal incontinence early postnatal period (0‐3 months).
Incontinence‐specific quality of life
Four trials used a validated incontinence‐specific quality of life measure (Fritel 2015, ICIQ‐SF and Contilife (higher score better); Dokmeci 2008; Ko 2011, IIQ‐7; Hughes 2001, BFLUTS questionnaire). Fritel 2015 (ICIQ‐SF) found no difference in incontinence‐specific quality of life between PFMT and usual care groups at any of three time points (late pregnancy, early and late (late: MD ‐0.20, 95% CI ‐1 to 0.81; 190 women, low‐quality evidence) postnatal periods) (Analysis 3.13; Analysis 3.14; Analysis 3.15). However, all point estimates were in favour of the PFMT group. The two trials that reported IIQ‐7 scores had contrasting findings. Ko 2011 found better quality of life in the PFMT group at each of three time points (late pregnancy, early and mid‐postnatal) compared to no PFMT, whereas Dokmeci 2008 stated there were no "statistically significant" differences in late pregnancy or early postpartum (no data provided) between PFMT and unspecified controls (Analysis 3.18). The overall score in the trial by Hughes 2001 was not reported.
Analysis 3.13.
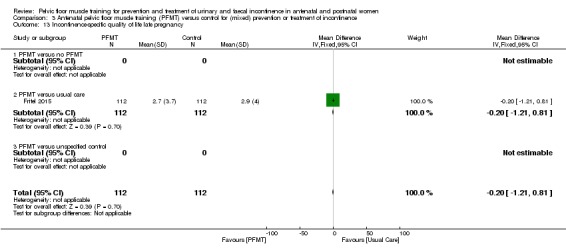
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 13 Incontinence‐specific quality of life late pregnancy.
Analysis 3.14.
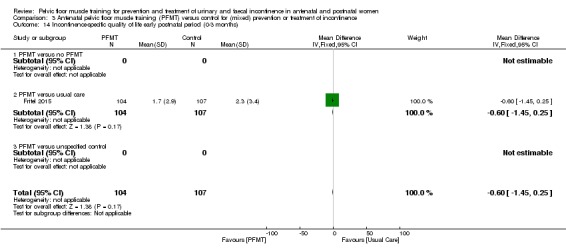
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 14 Incontinence‐specific quality of life early postnatal period (0‐3 months).
Analysis 3.15.
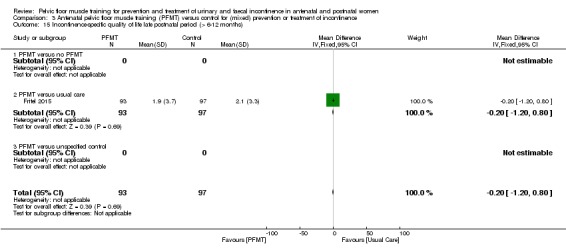
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 15 Incontinence‐specific quality of life late postnatal period (> 6‐12 months).
Analysis 3.18.
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 18 Quality of life and health status measures.
Quality of life and health status measures
| Study | Outcome measure | PFMT data | Control data | Difference |
|---|---|---|---|---|
| PFMT versus no PFMT | ||||
| Ko 2011 | UDI‐6 (0‐100) | Mean 3.44, SD 3.26, n=150 in late pregnancy; Mean 0.81, SD 1.36, n=150 at 0‐3 months postpartum; Mean 0.35, SD 0.84, n=150 at > 3‐6 months postpartum | Mean 4.66, SD 3.32, n=150 in late pregnancy; Mean 1.54, SD 1.59, n=150 at 0‐3 months postpartum; Mean 0.86, SD 1.14, n=150 at > 3‐6 months postpartum | Late pregnancy, mean difference ‐1.22 (95% CI ‐1.96 to ‐0.48); 0‐3 months postpartum, mean difference ‐0.73 (95% CI ‐1.06 to ‐0.40); > 3‐6 months postpartum, mean difference ‐0.51 (95% CI ‐0.74 to ‐0.28) |
| Ko 2011 | IIQ7 (0‐100) | Mean 3.77, SD 6.01, n=150 in late pregnancy; Mean 1.73, SD 3.57, n=150 at 0‐3 months postpartum; Mean 0.77, SD 2.07, n=150 at > 3‐6 months postpartum | Mean 5.28, SD 5.16, n=150 in late pregnancy; Mean 5.28, SD 5.61, n=150 at 0‐3 months postpartum; Mean 1.56, SD 2.20, n=150 at > 3‐6 months postpartum | Late pregnancy, mean difference ‐1.51 (95% CI ‐2.78 to ‐0.24); 0‐3 months postpartum, mean difference ‐3.55 (95% CI ‐4.61 to ‐2.49); > 3‐6 months postpartum, mean difference ‐0.79 (95% CI ‐1.27 to ‐0.31) |
| Ko 2011 | ||||
| Ko 2011 | ||||
| Ko 2011 | ||||
| Ko 2011 | ||||
| Ko 2011 | ||||
| Ko 2011 | ||||
| PFMT versus usual care | ||||
| Fritel 2015 | Female Pelvic Floor Questionnaire (FPFQ) bladder score (0‐10; 10 worse) | Mean 1.7, SD 1.3, n=112 in late pregnancy; Mean 0.8, SD 0.9, n=105 at 0‐3 months postpartum; Mean 0.9, SD 1.1, n=94 at > 6‐12 months postpartum | Mean 2.0, SD 1.4, n=111 in late pregnancy; Mean 0.9, SD 1.0, n=107 at 0‐3 months postpartum; Mean 1.0, SD 1.1, n=97 at > 6‐12 months postpartum | Late pregnancy, mean difference ‐0.30 (95% CI ‐0.65 to 0.05); 0‐3 months postpartum, mean difference ‐0.10 (95% CI ‐0.36 to 0.16); >6‐12 months postpartum, mean difference ‐0.10 (95% CI ‐0.41 to ‐0.12) |
| Fritel 2015 | FPFQ bowel score (0‐10) | Mean 1.3, SD 1.1, n=112 in late pregnancy; Mean 1.2, SD 1.2, n=104 at 0‐3 months postpartum; Mean 1.0, SD 1.0, n=94 at > 6‐12 months postpartum | Mean 1.4, SD 1.1, n=112 in late pregnancy; Mean 1.4, SD 1.2, n=107 at 0‐3 months postpartum; Mean 1.1, SD 1.0, n=97 > 6‐12 months postpartum | Late pregnancy, mean difference ‐0.10 (95% CI ‐0.39 to ‐0.19); 0‐3 months postpartum, mean difference ‐0.20 (95% CI ‐0.52 to 0.12); >6‐12 months postpartum, mean difference ‐0.10 (95% CI ‐0.38 to 0.18) |
| Fritel 2015 | FPFQ prolapse score (0‐10) | Mean 0.7, SD 1.2, n=112 in late pregnancy; Mean 0.3, SD 1.1, n=104 at 0‐3 months postpartum; Mean 0.4, SD 1.2, n=95 at > 6‐12 months postpartum | Mean 0.7, SD 1.4, n=112 in late pregnancy; Mean 0.5, SD 1.3, n=107 at 0‐3 months postpartum; Mean 0.4, SD 1.0, n=97 at > 6‐12 months postpartum | Late pregnancy, mean difference 0.00 (95% CI ‐0.34 to 0.34); 0‐3 months postpartum, mean difference ‐0.20 (95% CI ‐0.52 to 0.12); >6‐12 months postpartum, mean difference 0.00 (95% CI ‐0.31 to 0.31) |
| Fritel 2015 | Female Pelvic Floor Questionnaire sex score (0‐10; 10 worse) | Mean 2.7, SD 1.8, n=79 in late pregnancy; Mean 3.1, SD 2.1, n=73 at 0‐3 months postpartum; Mean 2.4, SD 1.8, n=86 at > 6‐12 months postpartum | Mean 3.1, SD 2.1, n=68 in late pregnancy; Mean 3.5, SD 2.2, n=77 at 0‐3 months postpartum; Mean 2.7, SD 2.0, n=83 at > 6‐12 months postpartum | Late pregnancy, mean difference ‐0.90 (95% CI ‐1.54 to ‐0.26); 0‐3 months postpartum, mean difference ‐0.40 (95% CI ‐1.09 to 0.29); >6‐12 months postpartum, mean difference ‐0.30 (95% CI ‐0.87 to 0.27) |
| Fritel 2015 | Contilife score (0‐10; 10 better) | Mean 9.3, SD 1.1, n=108 in late pregancy; Mean 9.6, SD 0.8, n=102 at 0‐3 months postpartum; Mean 9.5, SD 1.2, n=91 at > 6‐12 months postpartum | Mean 9.2, SD 1.3, n=109 in late pregancy; Mean 9.5, SD 0.8, n=101 at 0‐3 months postpartum; Mean 9.5, SD 1.0, n=89 at > 6‐12 months postpartum | Late pregnancy, mean difference 0.10 (95% CI ‐0.22 to 0.42); 0‐3 months postpartum, mean difference 0.10 (95% CI ‐0.12 to 0.32); >6‐12 months postpartum, mean difference 0.00 (95% CI ‐0.32 to 0.32) |
| Fritel 2015 | Sexually active | 83 of 112 at end of pregnancy; 74 of 104 at 0‐3 months postpartum; 89 of 95 at > 6‐12 months postpartum | 70 of 112 at end of pregnancy; 79 of 106 at 0‐3 months postpartum; 91 of 97 at > 6‐12 months postpartum | Late pregnancy, relative risk 1.19 (95% CI 0.99 to 1.42); 0‐3 months postpartum, relative risk 0.95 (95% CI 0.81 to 1.13); >6‐12 months postpartum, relative risk 1.0 (95% CI 0.93 to 1.07) |
| Fritel 2015 | EuroQoL‐5D (0‐100; 100 better) | Mean 76.4, SD 20.4, n=111 at end of pregnancy; Mean 82.8, SD 18.2, n=105 at 0‐3 months postpartum; Mean 86.8, SD 13.1, n=94 at > 6‐12 months postpartum | Mean 77.9, SD 16.3, n=112 at end of pregnancy; Mean 80.4, SD 17.0, n=107 at 0‐3 months postpartum; Mean 82.9, SD 14.8, n=97 at > 6‐12 months postpartum | Late pregnancy, mean difference ‐1.50 (95% CI ‐6.35 to 3.35); 0‐3 months postpartum, mean difference 2.40 (95% CI ‐2.34 to 7.14); >6‐12 months postpartum, mean difference 3.90 (95% CI ‐0.06 to 7.86) |
| Fritel 2015 | ||||
| Hughes 2001 | ||||
| Hughes 2001 | BFLUTs questionnaire: a negative effect on exercise in response to question "does incontinence affect physical activity?" | 47 of 585 at 6 months postpartum | 41 of 584 at 6 months postpartum | Relative risk 1.14 (95% CI 0.76 to 1.71) |
| Hughes 2001 | ||||
| Hughes 2001 | ||||
| Hughes 2001 | ||||
| Hughes 2001 | ||||
| Hughes 2001 | ||||
| Hughes 2001 | ||||
| Miquelutti 2013 | State Trait Anxiety Inventory (STAI) (20‐80; 50‐64 high; 65‐80 very high) | Trait anxiety 18 of 85 State anxiety 16 of 85 |
Trait anxiety 20 of 76 State anxiety 14 of 76 |
Trait anxiety, relative risk 0.80 (95% CI 0.46 to 1.40) State anxiety, relative risk 1.02 (95% CI 0.53 to 1.95) |
| Miquelutti 2013 | ||||
| Miquelutti 2013 | ||||
| Miquelutti 2013 | ||||
| Miquelutti 2013 | ||||
| Miquelutti 2013 | ||||
| Miquelutti 2013 | ||||
| Miquelutti 2013 | ||||
| Mørkved 2003 | Sexual satisfaction at 6 years post‐delivery | 34 of 94 | 17 of 94 | Relative risk 2.00 (95% CI 1.20 to 3.32) |
| Mørkved 2003 | ||||
| Mørkved 2003 | ||||
| Mørkved 2003 | ||||
| Mørkved 2003 | ||||
| Mørkved 2003 | ||||
| Mørkved 2003 | ||||
| Mørkved 2003 | ||||
| Stafne 2012 | Psychological General Well‐being Index (PGWBI) (0‐110; 110 better) | Total score at end of pregnancy: Mean 79.5 (95% CI 78.5 to 80.6), n=389 | Total score at end of pregnancy: Mean 78.5 (95% CI 77.5 to 79.6), n=361 | Mean difference 0.71 (95% CI ‐0.60 to 2.01) |
| Stafne 2012 | ||||
| Stafne 2012 | ||||
| Stafne 2012 | ||||
| Stafne 2012 | ||||
| Stafne 2012 | ||||
| Stafne 2012 | ||||
| Stafne 2012 | ||||
| PFMT versus unspecified control | ||||
| Dokmeci 2008 | UDI‐6 | No data | No data | Authors stated that there was a significant decrease in scores between first trimester and third trimester and between third trimester and 6 weeks postpartum |
| Dokmeci 2008 | IIQ‐7 | No data | No data | Authors stated that there were no significant differences observed during pregnancy or postpartum |
| Dokmeci 2008 | PISQ‐12 | No data | No data | Authors stated that there were no significant differences observed during pregnancy or postpartum |
| Dokmeci 2008 | ||||
| Dokmeci 2008 | ||||
| Dokmeci 2008 | ||||
| Dokmeci 2008 | ||||
| Dokmeci 2008 | ||||
Secondary outcomes
Severity of incontinence
Two trials reported some data on symptom severity, such as frequency or amount of urine leakage. None of the data suggested that PFMT was superior to control, or vice versa, at the primary endpoint of either three months' postpartum (Hughes 2001) or 12 months' postpartum (Sampselle 1998).
Number of urinary or faecal incontinence episodes
None of the trials reported number of urinary or faecal incontinence episodes.
Loss of urine under stress test
The single trial reporting pad test data (24 hour) found no difference between PFMT and usual care groups (Analysis 3.17) (Fritel 2015).
Analysis 3.17.
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 17 Loss of urine under stress test early postnatal period (0‐3 months).
Loss of urine under stress test early postnatal period (0‐3 months)
| Study | Measure | PFMT | Control | Difference |
|---|---|---|---|---|
| PFMT versus usual care | ||||
| Fritel 2015 | 24 hour pad test (g) | Mean 0.9, SD 1.6, n=78 at 2 months postpartum | Mean 1.3, SD 3.3, n=85 at 2 months postpartum | Mean difference ‐0.40 (95% CI ‐1.19 to 0.39) |
Other quality of life and health status measures
Other quality of life and health status measures included:
Urogenital Distress Index‐Short Form (UDI‐6) (Dokmeci 2008; Ko 2011);
Female Pelvic Floor questionnaire (bladder, bowel, prolapse and sex scores; Fritel 2015);
Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire (PISQ; higher score better) (Dokmeci 2008);
State Trait Anxiety Inventory (Miquelutti 2013);
Psychological General Wellbeing Index (Stafne 2012);
Euro‐QoL‐5D (Fritel 2015; higher score better).
There were no differences between groups for these other measures of well‐being (Analysis 3.18).
Three trials measured some aspect of sexual function in pregnancy, immediately postpartum and up to six years post‐index delivery (Dokmeci 2008; Fritel 2015; Mørkved 2003). Overall, there was no difference in sexual function or the proportion of women who were sexually active in late pregnancy and up to 12 months' postpartum (Dokmeci 2008; Fritel 2015). At six years, Mørkved 2003 found that PFMT women were twice as likely to report sexual satisfaction compared to controls (Analysis 3.18).
Health economics
None of the trials reported health economic data.
Adverse effects
Two trials reported no adverse effects (Fritel 2015; Miquelutti 2013).
Other outcomes
Pelvic floor muscle function
PFM function was measured using perineometry, electromyography and digital palpation (Assis 2015; Dokmeci 2008; Fritel 2015; Mørkved 2003). In the three trials that reported data, point estimates favoured PFMT women over controls (Assis 2015; Fritel 2015; Mørkved 2003). There were differences in favour of PFMT in both trials that measured vaginal squeeze pressures (Analysis 3.19) (Assis 2015; Mørkved 2003).
Analysis 3.19.
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 19 Pelvic floor muscle function.
Pelvic floor muscle function
| Study | Measure | PFMT | Control | Difference |
|---|---|---|---|---|
| PFMT versus no PFMT | ||||
| Assis 2015 | Perinometry, vaginal squeeze pressure (cm water), late pregnancy | Mean 9.45, SD 1.05, n=58 | Mean 4.7, SD 1.7, n=29 | Mean difference 4.75 (95% CI 4.07 to 5.43) |
| Assis 2015 | ||||
| PFMT versus usual care | ||||
| Fritel 2015 | Pelvic floor muscle strength, modified Oxford scale (0‐5; 5 better) | Mean 3.5, SD 1.5, n=105 at 2 months postpartum | Mean 3.3, SD 1.3, n=107 at 2 months postpartum | Mean difference 0.12 (95% CI ‐0.18 to 0.58) |
| Fritel 2015 | Change in pelvic floor muscle strength, baseline to 2 months postpartum | Mean 0.08, SD 1.32, n=101 | Mean ‐0.25, SD 1.11, n=103 | Mean difference 0.33 (95% CI ‐0.00 to 0.66) |
| Mørkved 2003 | Vaginal squeeze pressure (cm water) | Mean 29.5, 95% CI 26.8 to 32.2, n=143 at 3 months postpartum | Mean 25.6, 95% CI 23.2 to 27.9, n=146 at 3 months postpartum | Mean difference 3.90 (95% CI 0.35 to 7.45) |
| Mørkved 2003 | ||||
| PFMT versus unspecified control | ||||
| Dokmeci 2008 | Electromyography with vaginal electrode | No data | No data | Authors stated that "Maximum pelvic floor strength was increased significantly between first and third visits in PFMT group, p=0.03 and between first and post‐partum visits in control group, p=0.03." |
| Dokmeci 2008 | ||||
Delivery outcome
Six trials reported the number of caesarean sections, with no difference between groups (RR 0.95, 95% CI 0.79 to 1.14; 6 trials, 1899 women, fixed‐effect, I² = 25%, T² = 0.00) between PFMT and control groups (Analysis 3.20) (Bø 2011; Fritel 2015; Ko 2011; Miquelutti 2013; Mørkved 2003; Stafne 2012). Mørkved 2003 found no difference in the type of delivery, although women in the supervised antenatal PFMT group had a shorter second stage of labour. However, it is worth noting that fetal head circumference was also smaller in the PFMT group. Ko 2011 also reported rates of episiotomy among women and there was no difference between the groups (RR 0.86, 95% CI 0.53 to 1.39).
Analysis 3.20.
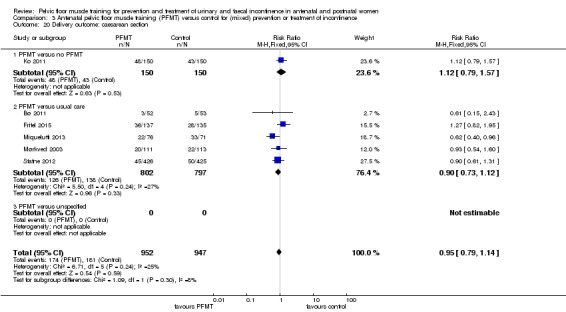
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 20 Delivery outcome: caesarean section.
Participant satisfaction and further treatment
Fritel 2015 reported no difference between the groups in the proportion of women who wanted further supervised training at 12 months' postpartum, or in the number of medical visits since delivery between the PFMT and usual care groups (Analysis 3.22).
Analysis 3.22.
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 22 Patient satisfaction and further treatment.
Patient satisfaction and further treatment
| Study | Measure | PFMT | Control | Difference |
|---|---|---|---|---|
| PFMT versus usual care | ||||
| Fritel 2015 | Additional postnatal pelvic floor muscle training | 50 of 92 at 12 months postpartum | 61 of 97 at 12 months postpartum | Relative risk 0.86 (95% CI 0.68 to 1.10) |
| Fritel 2015 | Medical visits since delivery | Mean 3.0, SD 2.5, n=84 at 12 months postpartum | Mean 3.0, SD 2.2, n=83 at 12 months postpartum | Mean difference 0.00 (95% CI ‐0.71 to 0.71) |
| PFMT versus unspecified control | ||||
| Frumenzio 2012 | Visual analogue scale patient satisfaction (0‐10) | Mean 7.6 | No data | Not able to calculate |
| Frumenzio 2012 | ||||
Comparison 4: postnatal pelvic floor muscle training for treatment of incontinence
Five trials reported postnatal PFMT for treatment of incontinence and provided supervised PFMT beginning at three or more months' postpartum as treatment for women with persistent urinary incontinence symptoms after delivery (Ahlund 2013; Dumoulin 2004; Glazener 2001; Kim 2012; Wilson 1998). The control group received usual care or were asked not to do PFMT (Ahlund 2013; Dumoulin 2004; Glazener 2001; Kim 2012; Wilson 1998).
Primary outcome
Self‐reported urinary or faecal incontinence
Women randomised to PFMT were about 22% less likely to have urinary incontinence after treatment compared to controls more than six and up to 12 months postdelivery (RR 0.78, 95% CI 0.69 to 0.87; 3 trials, 696 women, fixed‐effect). However, there was statistical heterogeneity in this comparison (I² = 90%) and when the more conservative random‐effects model was used there was no difference (RR 0.55, 95% CI 0.29 to 1.07; 696 women, I² = 90%, T² = 0.30; very low‐quality evidence) (Analysis 4.3).
Analysis 4.3.
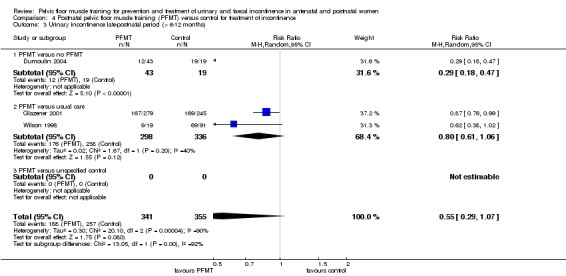
Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 3 Urinary incontinence late‐postnatal period (> 6‐12 months).
Women in all three studies were recruited at three months or more postpartum. In the case of Dumoulin 2004, women were recruited after completing an incontinence questionnaire at their annual gynaecological visit, so it seems likely many were much more than three months' postpartum at trial entry. Therefore, after a further two months' intervention, it seemed likely the postintervention outcome was between six and 12 months' postdelivery for most. For this reason, a decision was made to present the data from the trial in the late postnatal category (greater than six to 12 months) along with that from Glazener 2001 and Wilson 1998, who both measured outcome 12 months postdelivery.
In addition to possible differences in timing of outcome measurement, there were other obvious dissimilarities between the three studies. In Dumoulin 2004, women randomised to the control group were specifically asked not to do any PFMT, while women in the control group in Glazener 2001 and Wilson 1998 received usual postnatal care and some did PFMT. Glazener 2001 reported a mean of 20 PFM contractions every day in the PFMT group versus five PFM contractions every day in the control group. A total of 86 (PFMT) versus 35 (control) were performed in the trial by Wilson 1998. The second difference was that Dumoulin 2004 employed a strengthening PFMT regimen which incorporated electrical stimulation and biofeedback, while participants also had weekly contact with a physiotherapist for eight weeks. In contrast, Glazener 2001 and Wilson 1998 did not clearly aim their PFMT regimens at either strength or endurance and in both studies the intervention group had three or four contacts with health professionals over a six‐month period.
Glazener 2001 reported urinary incontinence prevalence at six years (RR 0.96, 95% CI 0.88 to 1.05; 1 trial, 516 women) and 12 years after the index delivery (RR 1.03, 95% CI 0.94 to 1.12; 1 trial, 471 women), with no difference between PFMT and control group at either time‐point (Analysis 4.5; Analysis 4.6).
Analysis 4.5.
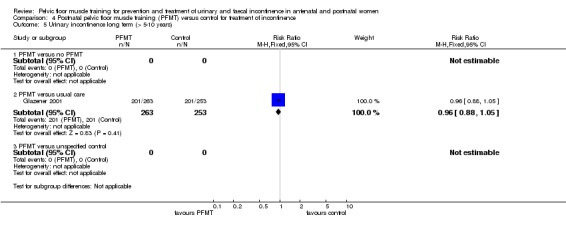
Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 5 Urinary incontinence long term (> 5‐10 years).
Analysis 4.6.
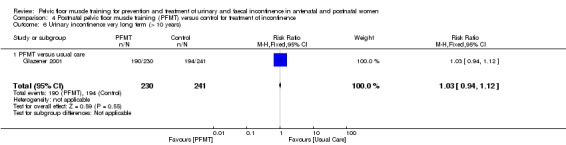
Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 6 Urinary incontinence very long term (> 10 years).
Two trials reported data on the prevalence of faecal incontinence one year after delivery (Glazener 2001; Wilson 1998). There was statistically significant heterogeneity, therefore a random‐effects model was used to give a more conservative estimate of effect (RR 0.68, 95% CI 0.24 to 1.94, random‐effects, I² = 74%, T² = 0.42; 2 trials, 620 women; very low‐quality evidence) (Analysis 4.9).
Analysis 4.9.
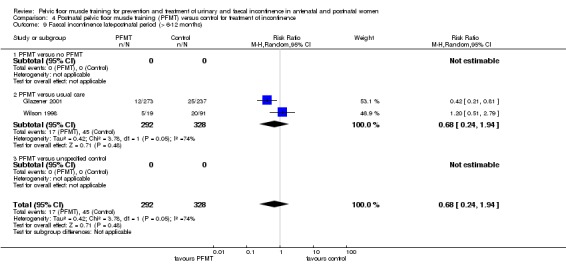
Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 9 Faecal incontinence late‐postnatal period (> 6‐12 months).
Glazener 2001 reported no difference in the prevalence of faecal incontinence at six years (RR 0.95, 95% CI 0.60 to 1.50; 509 women) and 12 years (RR 1.36, 95% CI 0.84 to 2.22; 1 trial, 468 women) post‐index delivery (Analysis 4.11; Analysis 4.12). At both these time points, Glazener 2001 reported that about 50% of women in both the intervention and control groups were doing "any" PFMT. When questioned about performing daily PFMT, it was interesting to note that only 6% of the PFMT group were exercising daily, compared to 12% of the control group at six years' follow‐up. After 12 years, 7% of the intervention group and 8% of the control group were performing daily PFMT (Table 11).
Analysis 4.11.
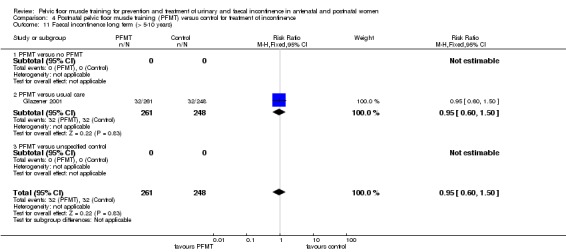
Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 11 Faecal incontinence long term (> 5‐10 years).
Analysis 4.12.
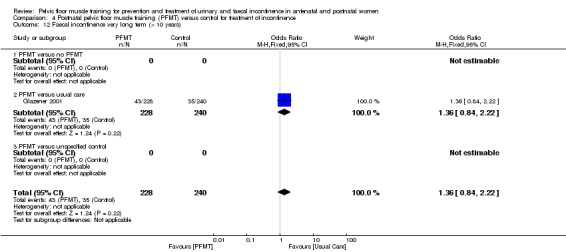
Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 12 Faecal incontinence very long term (> 10 years).
Incontinence‐specific quality of life
Two trials used incontinence‐specific quality of life measures (Dumoulin 2004: IIQ and UDI; Kim 2012: BFLUTS). Kim 2012 found no difference between PFMT and usual care groups post‐treatment (MD ‐1.66, 95% CI ‐3.51 to 0.19; 18 women) (Analysis 4.13). Dumoulin 2004 reported an improvement in IIQ and UDI score in women who were doing PFMT compared with women who were randomised to the control (no PFMT) group (Analysis 4.15).
Analysis 4.13.
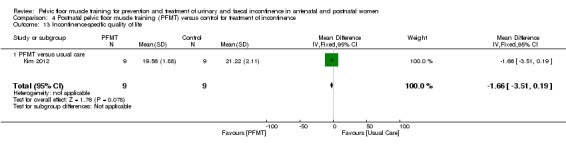
Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 13 Incontinence‐specific quality of life.
Analysis 4.15.
Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 15 Quality of life and health status measures.
Quality of life and health status measures
| Study | Outcome measure | PFMT data | Control data | Difference |
|---|---|---|---|---|
| Dumoulin 2004 | Change in Urogenital Distress Inventory Score (maximum score 57) | A: Median change 4, interquartile range 1 to 10, n=23 after 9 weeks PFMT B: Median change 7, interquartile range 3 to 8, n=20 after 9 weeks PFMT |
Median change 0, interquartile range ‐2.3 to 6.5, n=19 after 9 weeks of control condition | Not calculable |
| Dumoulin 2004 | Change in Incontinence Impact Questionnaire (maximum score 90) | A: Median change 10, interquartile range 2 to 16, n=23 after 9 weeks PFMT B: Median change 13, interquartile range 6 to 25, n=20 after 9 weeks PFMT |
Median change 0.5, interquartile range ‐6.5 to 5.0, n=19 after 9 weeks of control condition | Not calculable |
| Glazener 2001 | Hospital Anxiety and Depression Score ‐ anxiety score | Mean 6.1, 95% CI 5.6 to 6.5, n=238 at 12 months | Mean 6.8, 95% CI 6.3 to 7.3, n=219 at 12 months postpartum | Mean difference ‐0.79 (95% CI ‐1.43 to ‐0.05) |
| Glazener 2001 |
Secondary outcomes
Severity of incontinence
All five treatment trials reported some data on incontinence severity, for instance frequency or amount of urine leakage. None of the measures, or the methods of reporting these, were common to the five trials. The data suggest that women randomised to PFMT with symptoms of urinary incontinence might have had less severe symptoms than women in the control groups but this was not a consistent or clear‐cut finding (Analysis 4.14).
Analysis 4.14.
Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 14 Severity of incontinence.
Severity of incontinence
| Study | Measure of | Outcome measure | PFMT data | Control data | Difference |
|---|---|---|---|---|---|
| PFMT versus no PFMT | |||||
| Dumoulin 2004 | Frequency of leakage | Not measured | |||
| Dumoulin 2004 | Amount of leakage | Change, in grams, in 20 min pad test with standardised bladder volume | A: Median change 19.0, interquartile range 6.0 to 25.0, n=23 after 9 weeks of PFMT B: Median change 8, interquartile range 4.0 to 2.35, n=20 after 9 weeks of PFMT |
Median change 0, interquartile range ‐3.0 to 9.8, n=19 after 9 weeks of control condition | Not calculable |
| Dumoulin 2004 | Other leakage | Change in visual analogue scale for perceived burden of incontinence (Stach‐Lempinen et al 2001) | A: Median change 3.0, interquartile range 2.0 to 4.0, n=23 after 9 weeks of PFMT B: Median change 2.5, interquartile range 0.8 to 5.0, n=20 after 9 weeks of PFMT |
Median change 0, interquartile range ‐0.1 to 0.02, n=19 after 9 weeks of control condition | Not calculable |
| PFMT versus usual care | |||||
| Ahlund 2013 | Incontinence score (0‐20, 20 worse) | ICIQ‐FLUTS | Median 4.0, range 0 to 15, n=40 at 9 months postpartum | Median 4, range 0 to 12, n=42 at 9 months postpartum | Not calculable |
| Ahlund 2013 | Voiding score (0‐12, 12 worse) | ICIQ‐FLUTS | Median 1.0, range 0 to 5, n=40 at 9 months postpartum | Median 0.0, range 0 to 8, n=42 at 9 months postpartum | Not calculable |
| Ahlund 2013 | Incontinence score (0‐20, 20 worse) | ICIQ‐FLUTS | Median 4.0, range 0 to 15, n=40 at 9 months postpartum | Median 4, range 0 to 12, n=42 at 9 months postpartum | Not calculable |
| Glazener 2001 | Frequency of leakage | Not measured | |||
| Glazener 2001 | Amount of leakage | Using absorbent pads | 41 of 276 at 12 months postpartum | 55 of 245 at 12 months postpartum | Relative risk 0.66 (95% CI 0.46, 0.95) |
| Glazener 2001 | Other leakage severity | Visual analogue scale for severity of urine leakage | Mean 2.8, 95% CI 2.4 to 3.1, n=142 at 12 months postpartum | Mean 3.6, 95% CI 3.1 to 4.0, n=142 at 12 months postpartum | Mean difference ‐0.80 (95% CI ‐1.37 to ‐0.23) |
| Kim 2012 | Urinary symptoms (? range) | BFLUTS | Mean 40.56, SD 5.36, n=9 at between 8‐14 weeks postpartum | Mean 46.89, SD 3.62, n=9 at between 8‐14 weeks postpartum | |
| Kim 2012 | |||||
| Kim 2012 | |||||
| Wilson 1998 | Frequency of leakage | Not measured | |||
| Wilson 1998 | Amount of leakage | Urine loss on home pad test (Wilson et al 1989), in grams | Mean 2.1, 95% CI ‐0.3 to 4.5, n=18 at 12 months postpartum | Mean 2.6, 95% CI 0.1 to 5.1, n=82 at 12 months postpartum | Mean difference ‐0.50 (95% CI ‐3.81 to 2.81) |
| Wilson 1998 | Other leakage severity | Not measured | |||
Number of urinary or faecal incontinence episodes
None of the trials reported number of urinary or faecal incontinence episodes.
Loss of urine under stress test
None of the trials reported loss of urine under stress test.
Other quality of life and health status measures
Glazener 2001 used the Hospital Anxiety and Depression Scale to measure quality of life and found reduced anxiety in the PFMT group (Analysis 4.15).
Health economics
None of the trials reported health economic data.
Adverse effects
Dumoulin 2004 stated that none of the women in the PFMT group reported any adverse events (with PFMT or electrical stimulation).
Other outcomes
Pelvic floor muscle function
One trial measured PFM function using a dynamometer and three trials reported vaginal squeeze pressure (Ahlund 2013; Dumoulin 2004; Kim 2012; Wilson 1998). Dynamometer findings favoured the PFMT group, as did the vaginal squeeze pressure readings in two trials (Analysis 4.16) (Ahlund 2013; Dumoulin 2004; Kim 2012).
Analysis 4.16.
Comparison 4 Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence, Outcome 16 Pelvic floor muscle function.
Pelvic floor muscle function
| Study | Outcome measure | PFMT data | Control data | Difference |
|---|---|---|---|---|
| PFMT versus no PFMT | ||||
| Dumoulin 2004 | Maximal strength (Newtons, pelvic floor dynamometer, Dumoulin et al 2003) | A: Median change 0.7, range ‐0.2 to 2.3, n=23 after 9 weeks PFMT B: Median change 0.5, range ‐0.6 to 2.5, n=20 after 9 weeks PFMT |
Median change ‐0.5, range ‐1.7 to 1.0, n=19 after 9 weeks PFMT | Not calculable |
| Dumoulin 2004 | ||||
| Dumoulin 2004 | ||||
| PFMT versus usual care | ||||
| Ahlund 2013 | Maximal voluntary contraction (cm mercury, perineometer) | Median 26.0, estimated range 7 to 49, n=40 at 9 months postpartum | Median 18.2, estimated range 6 to 54, n=42 at 9 months postpartum | Not calculable |
| Ahlund 2013 | Endurance (secs, continuous contraction until pressure=0) | Median 26.7, estimated range 1 to 65, n =40 at 9 months postpartum | Median 23.4, estimated range 3 to 60, n=42 at 9 months postpartum | Not calculable |
| Ahlund 2013 | Oxford scale (0‐5, 0=no activity; 5, strong) | Median 4, estimated range 2 to 5, n=40 at 9 months postpartum | Median 3, estimated range 2 to 5, n=42 at 9 months postpartum | Not calculable |
| Kim 2012 | Maximal squeeze pressure (mm mercury, perineometer) | Mean 25.78, SD 10.74, n= 9 at between 8‐14 weeks postpartum | Mean 8.11, SD 2.57, n=9 at between 8‐14 weeks postpartum | Mean difference 17.67 (95% CI 10.46 to 24.88) |
| Kim 2012 | Holding time (sec, perineometer) | Mean 14.34, SD 3.08, n=9 at between 8‐14 weeks postpartum | Mean 8.89, SD 2.10, n=9 at between 8‐14 weeks postpartum | Mean difference 5.45 (95% CI 3.01 to 7.89) |
| Kim 2012 | ||||
| Wilson 1998 | Maximal vaginal squeeze pressure (cm water) | Mean 13.6, 95% CI 9.8 to 17.4, n=19 at 12 months postpartum | Mean 13.1, 95% CI 11.3 to 14.9, n=79 at 12 months postpartum | Mean difference 0.50 (95%CI ‐3.46 to 4.46) |
| Wilson 1998 | ||||
| Wilson 1998 | ||||
Any other outcome not prespecified but of interest
Wilson 1998 noted that the mean time to teach PFMT to the intervention group was 32 minutes (95% CI 30 to 34) but no further economic analysis was reported (Table 11).
Comparison 5: postnatal pelvic floor muscle training for mixed prevention and treatment of incontinence
Ten trials reported postnatal PFMT for mixed prevention and treatment of incontinence (Chiarelli 2002; Ewings 2005; Frost 2014; Hilde 2013; Kou 2013; Liu 2011; Meyer 2001; Peirce 2013; Sleep 1987; Wen 2010). These randomised women to postnatal PFMT versus usual care with the exception of one, in which the controls were asked to do no exercise (Meyer 2001). The trials recruited previously nulliparous women during their first pregnancy (Meyer 2001), women having their first baby (Hilde 2013; Liu 2011; Peirce 2013), or postnatal women of mixed parity (Chiarelli 2002; Ewings 2005; Sleep 1987). Three trials did not report this information (Frost 2014; Kou 2013; Wen 2010).
Primary outcome
Self‐reported urinary or faecal incontinence
The only information from the early postnatal period was from Frost 2014, a conference abstract. This trial did not contribute any data to the review but the authors stated that there were no significant differences in "urinary symptoms" at six to eight weeks' postpartum between the PFMT and control (usual care) groups.
There was no difference in the prevalence of urinary incontinence in women randomised to postnatal PFMT or control group in the:
mid‐postnatal period, up to six months (RR 0.95, 95% CI 0.75 to 1.19, random‐effects, I² = 65%, T² = 0.04; 5 trials, 2800 women) (Analysis 5.2) or
late postnatal period, more than six to 12 months (RR 0.88, 95% CI 0.71 to 1.09, fixed‐effect, I² = 50%, T² = 0.00; 3 trials, 826 women; very low‐quality evidence) (Analysis 5.3).
Analysis 5.2.
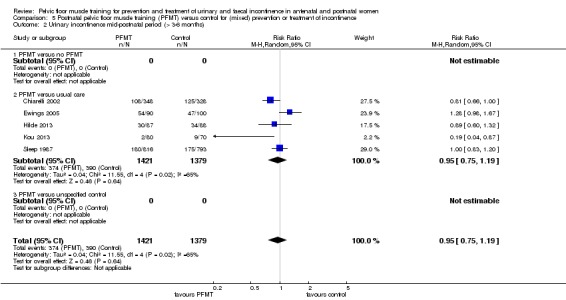
Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 2 Urinary incontinence mid‐postnatal period (> 3‐6 months).
Analysis 5.3.
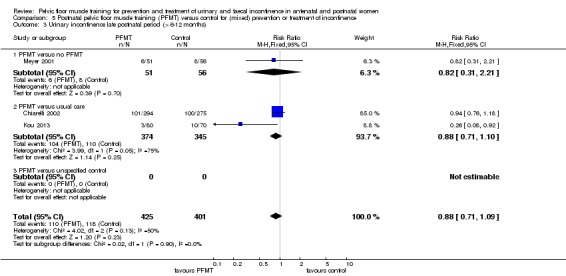
Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 3 Urinary incontinence late postnatal period (> 6‐12 months).
There was statistically significant heterogeneity in both comparisons. There was no detail of the PFMT programmes in three of the five trials contributing data to the mid‐postnatal comparison (Ewings 2005; Meyer 2001; Sleep 1987). In addition, there were other notable dissimilarities, including the risk profile of the recruited population (e.g. Chiarelli 2002) and the degree of contrast between PFMT and control groups in exercise supervision and prescription (e.g. Sleep 1987, low contrast; Kou 2013, high contrast). In the two trials with findings in favour of PFMT, the control groups were offered usual care, while the PFMT interventions were intensively supervised or enhanced with application of health behaviour theory (Chiarelli 2002; Kou 2013). In addition, Chiarelli 2002 recruited women who were at potentially increased risk of postnatal incontinence, such as those who had a large baby or a forceps delivery.
There was considerably less difference in PFMT and control groups in the other three trials for various reasons and none found a difference between the groups. All control groups received usual postnatal care that may have or did include information about PFMT. Ewings 2005 reported that 114/117 women randomised to PFMT received one‐to‐one instruction on PFMT but only 21 attended one group class, with five attending both available classes. There was no difference between groups. Hilde 2013 randomised women to PFMT delivered in a weekly exercise class plus home exercise, versus a home exercise control condition. Both groups had a correct PFM contraction confirmed prior to training. Sleep 1987 randomised women within 24 hours of delivery to an individual daily session with a midwife co‐ordinator while in hospital and home exercise, versus usual care that included postnatal classes taken by an obstetric physiotherapist. At three months' postpartum, the proportion of women doing PFMT was reasonably similar (58% with PFMT and 42% with control).
Chiarelli 2002 and Kou 2013 also contributed data to the late postpartum comparison with the addition of that from Meyer 2001. Women in the study by Meyer 2001 were randomised to either eight months of supervised PFM rehabilitation with a physiotherapist or no PFMT. Like Kou 2013, there was a high degree of contrast between the PFMT and control groups. However, unlike Kou 2013, Meyer 2001 found no difference between groups in the prevalence of urinary incontinence. Neither of these trials reported details of their randomisation procedures.
Two trials reported the prevalence of postnatal faecal incontinence (Meyer 2001; Sleep 1987). Neither demonstrated a difference between PFMT and control groups (at more than six to 12 months: RR 0.73, 95% CI 0.13 to 4.21; 1 trial, 107 women; very low‐quality evidence) (Analysis 5.6; Analysis 5.7; Analysis 5.8).
Analysis 5.6.
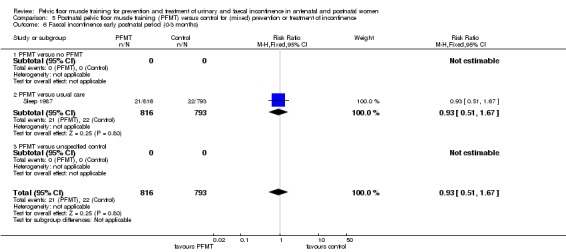
Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 6 Faecal incontinence early postnatal period (0‐3 months).
Analysis 5.8.
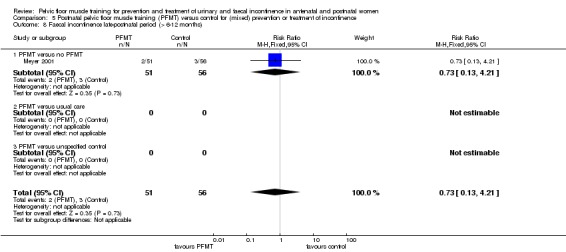
Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 8 Faecal incontinence late‐postnatal period (> 6‐12 months).
Incontinence‐specific quality of life
One of the 10 trials reported incontinence‐specific quality of life data, with no differences between PFMT and controls for faecal incontinence (Analysis 5.10; Analysis 5.13; Peirce 2013).
Analysis 5.13.
Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 13 Quality of life and health status measures.
Quality of life and health status measures
| Study | Measure of | Outcome measure | PFMT data | Control data | Difference |
|---|---|---|---|---|---|
| PFMT versus no PFMT | |||||
| Meyer 2001 | Sexual function | Reduced vaginal response at 10 months postpartum | 5 of 51 | 13 of 56 | Relative risk 0.42 (95% CI 0.16 to 1.10) |
| Meyer 2001 | |||||
| Meyer 2001 | |||||
| PFMT versus usual care | |||||
| Peirce 2013 | Faecal Incontinence Specific Quality of Life | Rockwood Faecal Incontinence Quality of Life Scale (low better, no total score, 4 domain scores) | Lifestyle: no data; coping/behaviour: no data, depression/self perception: no data, embarrassment: no data, n=30 |
Lifestyle: no data, coping/behaviour: no data, depression/self perception: no data, embarrassment: no data, n=90 | Lifestyle p =0.29, coping/behaviour p=0.27, depression/self perception p=089, embarrassment p=0.51 |
| Peirce 2013 | |||||
| Peirce 2013 | |||||
| Sleep 1987 | General wellbeing | 5 point Likhert scale in response to question "how are you feeling generally?" | 11 feeling not very well or not at all well, n=816 at 3 months postpartum | 18 feeling not very well or not at all well, n=793 at 3 months postpartum | Not calculated as validity/reliability of this measure not known |
| Sleep 1987 | Sexual function | Attempted sexual intercourse within 3 months of delivery | 714 of 819 | 681 of 792 | Relative risk 1.01 (95% CI 0.98 to 1.05) |
| Sleep 1987 | Sexual function | Dyspareunia at 3 months postpartum | 167 of 819 | 154 of 792 | Relative risk 1.05 (95% CI 0.86 to 1.28) |
Secondary outcomes
Severity of incontinence
Four trials reported some data on symptom severity (Hilde 2013; Liu 2011; Sleep 1987; Wen 2010).
At three months' postpartum, Sleep 1987 found no difference between the groups in frequency of leakage or the number of women using absorbent pads (often or always), whereas Liu 2011 reported less severe urinary incontinence (unspecified measure) in the PFMT group (Analysis 5.11).
Analysis 5.11.
Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 11 Severity of incontinence.
Severity of incontinence
| Study | Measure of | Outcome measure | PFMT data | Control data | Difference |
|---|---|---|---|---|---|
| PFMT versus usual care | |||||
| Hilde 2013 | Amount of leakage | Pad test, 1 min with standardised bladder volume (positive test 2g or more) | Median 4.0, range 2.0 to 80.0, n=87 at 6 months postpartum | Median 6.0, range 2.0 to 114.0, n=88 at 6 months postpartum | Mann Whitney‐U 213.5, z‐value ‐0.13, p‐value 0.90 |
| Hilde 2013 | |||||
| Hilde 2013 | |||||
| Liu 2011 | Urinary condition score, not specified (lower score better; 3 months postpartum) | Mean 2.2, SD 0.2, n=106 | Mean 2.8, SD 0.4, n=86 | Mean difference ‐0.60 (95% CI ‐0.69 to ‐0.51) | |
| Liu 2011 | Urinary condition score, not specified (lower score better; 6 months postpartum) | Mean 2.0, SD 0.4, n=106 | Mean 2.5, SD 0.4, n =86 | Mean difference ‐0.50 (95% CI ‐0.61 to ‐0.39) | |
| Liu 2011 | |||||
| Sleep 1987 | Frequency of leakage | Urine leakage once or more per week | 64 of 816 at 3 months postpartum | 57 of 793 at 3 months postpartum | Relative risk 1.09 (95% CI 0.77 to 1.54) |
| Sleep 1987 | Amount of leakage | Using absorbent pads sometimes or always | 38 of 815 at 3 months postpartum | 43 of 793 at 3 months postpartum | Relative risk 0.86 (95% CI 0.56 to 1.32) |
| Sleep 1987 | Other leakage severity | Not measured | |||
| Wen 2010 | Stress UI | Criteria from International Continence Society, 0‐5 (lower score better; 6 months postpartum) | Mean 2.84, SD 0.43, n=75 | Mean 2.50, SD 0.41, n=73 | Mean difference 0.34 (95% CI 0.20 to 0.48) |
| Wen 2010 | Stress UI | Criteria from International Continence Society, 0‐5 (lower score better; 12 months postpartum) | Mean 1.16, SD 0.38, n=75 | Mean 2.20, SD 0.39, n=73 | Mean difference ‐1.04 (95% CI ‐1.16 to ‐0.92) |
| Wen 2010 | Amount of leakage | Pad test (postive test more than 2g) | 7 of 75 at 12 months postpartum | 19 of 73 at 6 months postpartum | Relative risk 0.29 (95% CI 0.11 to 0.75) |
Number of urinary or faecal incontinence episodes
None of the trials reported number of urinary or faecal incontinence episodes.
Loss of urine under stress test
At six months' postpartum, Hilde 2013 found no difference between the groups for amount of leakage on pad test and the results for unspecified urinary incontinence severity were inconsistent (Liu 2011; Wen 2010). Pooled data from two studies found no difference in the risk of positive pad test between PFMT compared to usual care (RR 0.96, 95% CI 0.58 to 1.57; 2 trials, 85 women, fixed‐effect, I² = 0%) (Analysis 5.12) (Hilde 2013; Wen 2010). At 12 months, unspecified urinary incontinence severity was less in the PFMT group compared to usual care and fewer women in the PFMT groups had a positive pad test (Wen 2010).
Analysis 5.12.
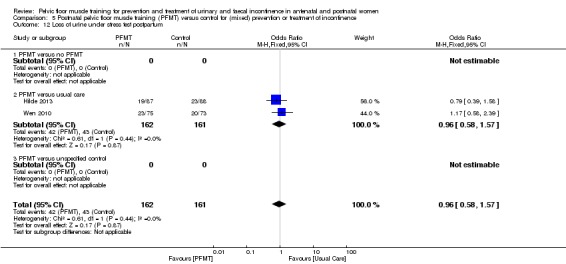
Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 12 Loss of urine under stress test postpartum.
Other quality of life and health status measures
Two trials measured some aspect of sexual function (Meyer 2001; Sleep 1987). Meyer 2001 noted fewer women in the PFMT group reported a diminished vaginal sexual response at 10 months' postpartum, while Sleep 1987 found no difference between groups in the proportion of women who had attempted or had pain with sexual intercourse at three months' postpartum (Analysis 5.13).
Health economics
None of the trials reported health economic data.
Adverse effects
Two trials collected data on adverse events, with none reported in either group or in those using biofeedback as an adjunct to PFMT (Hilde 2013; Peirce 2013).
Other outcomes
Pelvic floor muscle function
Two studies measured PFM function using the Oxford scale (Liu 2011; Wen 2010). The outcomes at three, six and 12 months' postpartum were in favour of the PFMT group compared to usual care. Three trials assessed vaginal squeeze pressure at six, 10 and 12 months' postpartum and found no difference between the groups (Hilde 2013; Kou 2013; Meyer 2001). Two trials measured anal pressure, in cm of water (Meyer 2001) or mmHg (Peirce 2013), and neither found a difference between PFMT and control groups (Analysis 5.14).
Analysis 5.14.
Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 14 Pelvic floor muscle function.
Pelvic floor muscle function
| Study | Outcome measure | PFMT data | Control data | Difference |
|---|---|---|---|---|
| PFMT versus no PFMT | ||||
| Meyer 2001 | Strength, vaginal squeeze pressure, in cm water (manometer, 10 months postpartum) | Mean 33, SD 22, n=51 | Mean 41, SD 27, n=56 | Mean difference ‐8.0 (95%CI ‐17.3 to 1.3) |
| Meyer 2001 | Mean anal squeeze pressure, in cm water (anorectal manometer, 10 months postpartum) | Mean 36, SD 20, n=51 | Mean 43, SD 24, n=56 | Mean difference ‐7.0 (95%CI ‐15.4 to 1.4) |
| Meyer 2001 | ||||
| PFMT versus usual care | ||||
| Hilde 2013 | Resting pressure, vaginal squeeze pressure (cm water, manometer) | n=87 at 6 months postpartum | n=88 at 6 months postpartum | Mean difference 1.3 (95% CI ‐1.0 to 3.6, p=0.257), reported by authors |
| Hilde 2013 | Strength, vaginal squeeze pressure (cm water, manometer) | n=87 at 6 months postpartum | n=88 at 6 months postpartum | Mean difference 3.3 (95% CI ‐1.4 to 8.0, p=0.172), reported by authors |
| Hilde 2013 | Endurance, vaginal squeeze pressure (cm sec, manometer) | n=87 at 6 months postpartum | n=88 at 6 months postpartum | Mean difference 29.8 (95% CI ‐10.6 to 70.2, p=0.148), reported by authors |
| Kou 2013 | Resting pressure, vaginal squeeze pressure (cm water) | Mean 33.7, SD 15.8, n=80 at 12 months postpartum | Mean 30.1, SD 15.3, n=70 at 12 months postpartum | Mean difference 3.60 (95% CI ‐1.38 to 8.58) |
| Kou 2013 | Vaginal squeeze pressure (cm water) | Mean 86.5, SD 14.8, n=80 at 12 months postpartum | Mean 60.4, SD 14.1, n=70 at 12 months postpartum | Mean difference 26.10 (95% CI 21.47 to 30.73) |
| Kou 2013 | Contraction time (sec) | Mean 5.9, SD 2.9, n=80 at 12 months postpartum | Mean 4.1, SD 2.6, n=70 at 12 months postpartum | Mean difference 1.80 (95% CI 0.92 to 2.68) |
| Liu 2011 | PF muscle tension (Oxford scale) | Mean 3.95, SD 0.32, n=106 at 3 months postpartum | Mean 3.02, SD 0.28, n=86 at 3 months postpartum | Mean difference 0.93 (95% CI 0.34 to 1.52) |
| Liu 2011 | PF muscle tension (Oxford scale) | Mean 4.73, SD 0.35, n=106 at 6 months postpartum | Mean 3.25, SD 0.41, n=86 at 6 months postpartum | Mean difference 1.48 (95% CI 1.37 to 1.59) |
| Liu 2011 | PF muscle tension (Oxford scale) | Mean 4.82, SD 0.38, n=106 at 12 months postpartum | Mean 3.43, SD 0.39, n=86 at 12 months postpartum | Mean difference 1.40 (95% CI 1.29 to 1.51) |
| Peirce 2013 | Mean anal resting pressure (mm Hg, anorectal manometer) | Mean 39, SD 13, n=30 at 3 months postpartum | Mean 43, SD 17, n=90 at 3 months postpartum | Mean difference ‐4.00 (95% CI ‐9.83 to 1.83) |
| Peirce 2013 | Mean anal squeeze pressure (mm Hg, anorectal manometer) | Mean 64, SD 17, n=30 at 3 months postpartum | Mean 62, SD 23, n=90 at 3 months postpartum | Mean difference 2.00 (95% CI ‐5.72 to 9.72) |
| Peirce 2013 | ||||
| Wen 2010 | PFMS (Oxford scale) | Mean 3.34, SD 0.35, n=75 at 6 months postpartum | Mean 3.25, SD 0.41, n=73 at 6 months postpartum | Mean difference 0.09 (95% CI ‐0.03 to 0.21) |
| Wen 2010 | PFMS (Oxford scale) | Mean 4.56, SD 0.38, n=75 at 12 months postpartum | Mean 3.46, SD 0.39, n=73 at 12 months postpartum | Mean difference 1.10 (95% CI 0.98 to 1.22) |
| Wen 2010 | ||||
Any other outcome not prespecified but of interest
One trial measured pelvic organ prolapse symptoms at six months' postpartum and found no difference between the groups (Analysis 5.15) (Hilde 2013).
Analysis 5.15.
Comparison 5 Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 15 Pelvic organ prolapse symptoms.
Pelvic organ prolapse symptoms
| Study | Measure | PFMT | Control | Difference |
|---|---|---|---|---|
| PFMT versus usual care | ||||
| Hilde 2013 | ICIQ‐Vag, bulging inside vagina (yes, no) | 8 of 87 at 6 months postpartum | 22 of 88 at 6 months postpartum | Mean difference 0.37 (95% CI 0.17 to 0.78) |
| Hilde 2013 | ICIQ‐Vag, bulging outside vagina (yes, no) | 5 of 87 at 6 months postpartum | 6 of 88 at 6 months postpartum | Mean difference 0.84 (95% CI 0.27 to 2.66) |
| Hilde 2013 | POP‐Q, stage 1 or 2 | 61 of 87 at 6 months postpartum | 64 of 88 at 6 months postpartum | Mean difference 0.88 (95% CI 0.46 to 1.70) |
Discussion
This review considers whether PFMT (as defined by the trialists) is better than usual antenatal or postnatal care for the prevention and treatment of urinary and faecal incontinence in childbearing women. Another Cochrane Review addressed a similar question (whether PFMT was better than no treatment, placebo or inactive control treatments) in women with urinary incontinence (Dumoulin 2014). This review specifically excluded trials that recruited antenatal or postnatal women.
Summary of main results
Is pelvic floor muscle training better than usual antenatal or postnatal care for the prevention and treatment of urinary and faecal incontinence?
There are three possible ways of delivering PFMT interventions to women during pregnancy and in the postpartum period. The first way is to provide PFMT for women who have no symptoms when PFMT begins (i.e. prevention). The second is to prescribe PFMT for women who have already developed symptoms of incontinence (i.e. treatment). The third is to provide PFMT for all women regardless of whether they have urinary incontinence symptoms or not when PFMT begins (i.e. mixed prevention and treatment approach). Comparisons were drawn within the following three populations of women.
Women who were continent when randomised to intervention groups, that is, prevention studies.
Women who were incontinent at randomisation, that is, treatment studies.
Trials including a mixed population, that is, some women were continent and some women were incontinent at randomisation.
Primary or secondary prevention of incontinence
Summary data from six trials suggested that PFMT during pregnancy decreased urinary incontinence in late pregnancy compared to usual care (RR 0.38, 95% CI 0.20 to 0.72; 624 women; low‐quality evidence). At between three months and up to six months following delivery (mid‐postpartum), summary data from five trials suggested that PFMT decreased the prevalence of urinary incontinence compared to usual care (RR 0.71, 95% CI 0.54 to 0.95; 673 women; moderate‐quality evidence). With only subgroup data from one small trial of 72 women, there were too few data from six months to one year after delivery (late postpartum) to comment meaningfully (Sampselle 1998). A single trial of 152 women suggested PFMT probably improved incontinence‐specific quality of life in late pregnancy compared to usual care (ICIQ‐SF: MD ‐2.42 , 95% CI ‐3.32 to ‐1.52 ; moderate‐quality evidence) (Pelaez 2014). None of the trials reported data on faecal incontinence in late pregnancy, or in the mid‐ and late postpartum periods (Table 1).
Two trials conducted a long‐term follow‐up of participants at eight and six years with no difference between PFMT and control groups (Analysis 1.6) (Mørkved 2003; Reilly 2002).
Treatment of incontinence
We expressed uncertainty about the effects of PFMT for treatment of urinary incontinence in antenatal and postnatal women below. The uncertainty arose from the lack of precision in the pooled estimate of effect; the CIs for the summary statistic were generally wide, and included a null effect.
Antenatal women
Based on summary data from three trials, we are uncertain whether PFMT decreased existing urinary incontinence in late pregnancy compared to usual care (RR 0.70, 95% CI 0.44 to 1.13; 345 women; very low‐quality evidence). We are equally uncertain whether PFMT to treat antenatal urinary incontinence reduced urinary incontinence in the mid‐ (RR 0.94, 95% CI 0.70 to 1.24; 1 trial, 187 women; very low‐quality evidence) or late (RR 0.50, 95% CI 0.13 to 1.93; 2 trials, 869 women; very low‐quality evidence) postnatal periods. Data from a single trial of 41 women suggested that PFMT may have improved incontinence‐specific quality of life in late pregnancy compared to usual care (ICIQ‐SF: MD ‐3.50, 95% CI ‐6.13 to ‐0.87; low‐quality evidence) (Cruz 2014). None of the trials reported data on faecal incontinence in late pregnancy, or in the mid‐ and late postpartum periods in this comparison (Table 2). Evidence in this comparison was particularly weak, with all trials limited by incomplete reporting of intervention and control conditions and trial methods. Two trials in this comparison were reported only as conference abstracts.
Postnatal women
Based on summary data from three trials, we were uncertain whether PFMT to treat postnatal urinary incontinence reduced urinary incontinence in the late postnatal period (RR 0.55, 95% CI 0.29 to 1.07; 696 women; very low‐quality evidence). We noted that two of the three trials that carried the greatest weighting in the pooled estimate compared PFMT (with limited supervision by a healthcare professional) with usual care and some women in the control groups were doing PFMT (Glazener 2001; Wilson 1998). There was no difference between groups in Wilson 1998 and close to no difference in Glazener 2001. In the third trial, Dumoulin 2004 compared a shorter and more intensively supervised PFMT intervention with no treatment and found a reduction in the risk of urinary incontinence in favour of PFMT. Based on the data from a single very small trial, we were uncertain whether urinary incontinence‐specific quality of life after treatment was improved with PFMT (BFLUTS: MD ‐1.66 , 95% CI ‐3.51 to 0.19; 18 women; very low‐quality evidence) (Kim 2012). Likewise, based on summary data from two trials, we are uncertain whether PFMT reduces faecal incontinence in the late postnatal period compared to usual care (RR 0.68, 95% CI 0.24 to 1.94; 620 women; very low‐quality evidence) (Glazener 2001; Wilson 1998) (Table 4).
Glazener 2001 carried out long‐term follow‐up of women at six and 12 years after the initial study. There was no difference in the prevalence of urinary incontinence between the PFMT and control groups at either of these time points suggesting that the possible benefits of PFMT were not upheld in the long term. Glazener and colleagues also measured faecal incontinence atsix and 12 years after delivery. These results did not show a difference but the CIs were wide, highlighting the need for more evidence in this area.
Trials with a mixed prevention and treatment approach
Antenatal women
Summary data from nine trials suggested that antenatal PFMT, delivered to a population of women with or without existing urinary incontinence symptoms, may have decreased the prevalence of urinary incontinence in late pregnancy (RR 0.74, 95% CI 0.61 to 0.90; 3164 women; low‐quality evidence). The two trials that compared PFMT to no training seemed to show a greater effect than the other seven trials that compared PFMT and usual care (Assis 2015; Ko 2011). Summary data from the mid‐postnatal period also favoured PFMT over control, although there was uncertainty about this effect (RR 0.73, 95% CI 0.55 to 0.97; 5 trials, 1921 women; very low‐quality evidence). Two trials reported data on urinary incontinence in the late postpartum period and there may have been no difference in urinary incontinence prevalence between PFMT and usual care, although there was uncertainty about this effect (RR 0.85, 95% CI 0.63 to 1.14; 244 women; low‐quality evidence).
Similarly, antenatal PFMT may have led to little or no difference in the prevalence of faecal incontinence in late pregnancy (RR 0.61, 95% CI 0.30 to 1.25; moderate‐quality evidence). There were no data for the prevalence of faecal incontinence in the mid‐ or late postnatal periods in this comparison. A single trial (ICIQ‐SF: MD ‐0.20, 95% CI ‐1.21 to 0.80; 190 women; low‐quality evidence) found that antenatal PFMT may have led to little or no difference in incontinence‐specific quality of life in the late postnatal period compared to usual care (Fritel 2015). However, it is important to note that in Fritel 2015, women in both groups reported a similar frequency and duration of PFMT (including the number of contractions) at the end of pregnancy. This suggested that the lack of difference between groups was because the control group was routinely doing adequate PFMT, which was encouraging in terms of delivering PFMT to the general population (Table 3).
Postnatal women
Based on summary data from three trials, we were uncertain whether postnatal PFMT, delivered to a population of women with or without existing urinary incontinence symptoms, reduced urinary incontinence in the late postnatal period (RR 0.88, 95% CI 0.71 to 1.09; 826 women; very low‐quality evidence). We were equally uncertain whether PFMT reduced faecal incontinence in the late postnatal period compared to no PFMT (RR 0.73, 95% CI 0.13 to 4.21; 1 trial, 107 women; very low‐quality evidence) (Meyer 2001). There were no incontinence‐specific quality of life data in this comparison (Table 5).
Delivery outcomes
Few adverse events were reported with PFMT. However, it was possible that PFMT during pregnancy might influence labour and delivery outcomes. This did not seem to be the case based on data from nine antenatal PFMT trials included in this review.
Three of the antenatal PFMT trials for the prevention of incontinence reported on delivery outcome (Barakat 2011; Gaier 2010; Gorbea 2004). The risk of caesarean section was not different (RR 1.28, 95% CI 0.89 to 1.85; 373 women) (Analysis 1.19). Gaier 2010 reported data on rates of episiotomy, with the control group receiving more episiotomies than the PFMT group, while Barakat 2011 reported rates of perineal trauma with no apparent difference in grades of perineal tear between the groups (Analysis 1.20).
Six of the antenatal PFMT trials for mixed prevention and treatment of incontinence reported on delivery outcome (Bø 2011; Fritel 2015; Ko 2011; Miquelutti 2013; Mørkved 2003; Stafne 2012). The risk of caesarean section was not different (RR 0.95, 95% CI 0.79 to 1.14; 1899 women) (Analysis 3.20). None of the three trials that reported data for the risk of assisted vaginal deliveries found a difference between the PFMT and control groups (Analysis 3.21) (Fritel 2015; Mørkved 2003; Stafne 2012). Two trials reported data on rates of episiotomy, with the control group receiving more episiotomies than the PFMT group (Analysis 3.21) (Ko 2011; Mørkved 2003). Du 2015 published a non‐Cochrane systematic review of antenatal PFMT and delivery outcomes where their findings appeared consistent with the above. Their review included more studies, as it contained trials that did not collect urinary incontinence or faecal incontinence data.
Analysis 3.21.
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 21 Delivery outcome: other.
Delivery outcome: other
| Study | Outcome measure | PFMT data | Control data | Difference |
|---|---|---|---|---|
| PFMT versus no PFMT | ||||
| Ko 2011 | Episiotomy | 99 of 150 | 104 of 150 | Relative risk 0.95 (95% CI 0.81 to 1.11) |
| Ko 2011 | Severe perineal lacerations | 10 of 150 | 10 of 150 | |
| Ko 2011 | ||||
| PFMT versus usual care | ||||
| Fritel 2015 | Spontaneous vaginal delivery | 72 of 137 | 72 of 135 | Relative risk 0.99 (95% CI 0.79 to 1.23) |
| Fritel 2015 | Assisted delivery | 29 of 137 | 35 of 135 | Relative risk 0.82 (95% CI 0.53 to 1.26) |
| Fritel 2015 | ||||
| Miquelutti 2013 | Vaginal delivery | 44 of 76 | 38 of 71 | Relative risk 1.08 (95% CI 0.81 to 1.44) |
| Miquelutti 2013 | Duration active phase labour (min) | Mean 284.5, SD 175, n=78 | Mean 254.2, SD 139.4, n=71 | Mean difference 30.3 (95% CI ‐40.9 to 101.4) |
| Miquelutti 2013 | Duration 2nd stage labour (min) | Mean 29.2, SD 23.3, n=78 | Mean 19.7, SD 13.0, n=71 | Mean difference 9.48 (95% CI 0.32 to 18.64) |
| Mørkved 2003 | Type of delivery (excluding twin pregnancy, preterm delivery, planned caesarean section and induced labour) | 91 normal vaginal deliveries, 15 asssisted vaginal deliveries, 5 emergency caesarean section, n=111 | 91 normal vaginal deliveries, 19 assisted vaginal deliveries, 3 emergency caesarean section, n=113 | Relative risk for normal vaginal delivery 1.02 (95% CI 0.90 to 1.15) Relative risk for assisted vaginal delivery 0.80 (95% CI 0.43 to 1.50) |
| Mørkved 2003 | Perineal trauma | 56 with episiotomy, and 7 with third or fourth degree tears, n=111 | 72 with episiotomy, and 9 with third or fourth degree tears, n=113 | Relative risk for episiotomy 0.79 (95% CI 0.63 to 1.00) |
| Mørkved 2003 | Duration 2nd stage labour (min) | Mean 40, 95% CI 33 to 47, n=111 | Mean 45, 95% CI 38 to 52, n=113 | Mean difference ‐5.00 (95% CI ‐14.79 to 4.79) |
| Stafne 2012 | Assisted vaginal delivery | 62 of 426 | 50 of 425 | Relative risk 1.24 (95% CI 0.87 to 1.75) |
| Stafne 2012 | Mean duration labour (min) | Mean 289, n=426? | Mean 281, n=425? | Unable to estimate |
| Stafne 2012 | Mean duration active 2nd stage labor (min) | Mean 32, n=426? | Mean 29, n=425? | Unable to estimate |
There were no data on labour or delivery outcomes reported in any of the trials of antenatal PFMT for treatment of incontinence.
Overall completeness and applicability of evidence
The self‐report measures of urinary and faecal incontinence were considered the most important outcomes in this review. However, there was variability in the way urinary and faecal incontinence were defined, how the questions were asked and how the data were presented. There were few incontinence‐specific quality of life data and little agreement about a standard measure. Further, some trials only partially reported a score (e.g. one domain of several included in the total score) or a statement about difference or lack of it, sometimes with a P value, as these data were collected but not reported or only partially reported this is a form of reporting bias.
Unfortunately, faecal incontinence data were rarely collected in the prevention or mixed prevention and treatment trials; only six studies presented data. Being a less common event than urinary incontinence, larger trials are needed to accurately document the effect of PFMT on this outcome and more trials must collect these data to enable a more precise effect estimate based on pooled data.
The usefulness of evidence was somewhat reduced by the short durations of follow‐up after intervention. This was particularly problematic in the antenatal PFMT trials, where the outcome was either measured at the end of pregnancy or in the three months postbirth. At three months' postpartum, there may not have been full resolution of many of the physiological changes associated with pregnancy and childbirth. A minimum follow‐up of six months postnatally is probably more useful to be sure how many cases of urinary or faecal incontinence are persistent. For treatment studies, while a postintervention measure is useful, data on the duration of effect (e.g. one year or longer) are needed. With regard to longer‐term follow‐up, only three studies provided data after five years (Glazener 2001; Mørkved 2003; Reilly 2002). Longer‐term data are difficult to interpret, as control groups may be offered a structured PFMT after the postintervention outcome is measured, women may have more children and so on. However, in the absence of longer‐term data about urinary and faecal incontinence and other variables (parity, bodyweight, etc.), there is an insufficient evidence base to begin to analyse and interpret.
Pregnancy and birth appear to be the most consistent and important factors associated with the development of urinary and faecal incontinence in women. Therefore, all women who have a child, or children, might be considered at risk of later incontinence. In addition, some women (such as those who have a connective tissue disorder, high BMI or an assisted delivery) might be at even greater risk (Durnea 2017; Svare 2014). The bulk of trials reviewed were undertaken in samples of antenatal women, principally those in their first pregnancy and most data were for urinary incontinence. The findings suggested that continent antenatal women benefited more from "structured" PFMT programmes (in terms of content and delivery) than women in usual care groups that may have incorporated some (or ad hoc) PFMT advice or teaching.
Trials of antenatal PFMT for mixed prevention and treatment also mostly recruited women having their first baby and showed a similar pattern of benefit of structured PFMT versus control conditions. However, the pooled data suggested less reduction in risk of urinary incontinence, upper CIs closer to one (i.e. no reduction in risk of urinary incontinence) and overall there was also more uncertainty about the effect.
Efforts to determine what value women, healthcare professionals and their professional organisations, provider and funding bodies give to this body of evidence about urinary incontinence prevention through structured and supervised antenatal PFMT (at least for first‐time mothers) are warranted. If the findings are considered sufficiently certain and of value, then changes to the current ad hoc delivery of PFMT advice in pregnancy within 'usual care' are needed. Alongside this, and to inform any decisions about the 'value' of antenatal PFMT for prevention of incontinence, investigations into health economics are needed. In the absence of such studies, there is no evidence about value for money. It is encouraging that one ongoing study identified in the search planned to collect and report economic data (Berghmans 2016).
We summarised data from all the trials. There were a few that we considered informed us enough about what was done in both PFMT and control groups that we were more confident in the estimate of differences in outcome. These were trials where sufficient information was provided about the intervention and control conditions such that it was possible to reach a judgement about:
the soundness of the physiology of the PFMT (i.e. whether the structured PFMT intervention was likely to strengthen muscle);
exercise behaviour in both groups (i.e. were both groups doing similar or quite different amounts of PFMT);
the degree of contrast between the two groups (e.g. did the PFMT group attend many exercise classes while the control group had none (high contrast), or did the PFMT group have one instruction session and the controls had none (low contrast)) (see Table 11 and Potential biases in the review process (heterogeneity)).
Four trials contained the necessary amount of information (Chiarelli 2002; Hilde 2013; Reilly 2002; Stafne 2012). All were at low risk of selection bias and had moderate to large sample sizes. Two examined the effect of antenatal PFMT for prevention of urinary and faecal incontinence (Reilly 2002; primiparous women with bladder neck hypermobility) and mixed prevention and treatment (Stafne 2012; healthy pregnant women, mixed parity) and two the effect of postnatal PFMT for mixed prevention and treatment of urinary and faecal incontinence (Chiarelli 2002, mixed parity, after ventouse or forceps delivery or baby weighing 4000 g or greater; Hilde 2013, primiparous women after vaginal delivery). Looking at the GRADE rated outcomes, data from these individual trials were consistent with the pooled estimates of effect. Antenatal training appeared to have clinically important reductions in urinary incontinence in late pregnancy and between more than three to six months postnatally (Reilly 2002; Stafne 2012). The effect of postnatal training for mixed prevention and treatment may not be clinically important at more than three to six months after delivery for urinary incontinence (Chiarelli 2002; Hilde 2013). However, it is possible that women at higher risk of postnatal incontinence benefited more (Chiarelli 2002).
Quality of the evidence
Overall, the evidence was moderate, low or even very low quality (see Table 1; Table 2; Table 3; Table 4; Table 5). The most common reasons for downgrading the evidence were:
imprecision, with few overall events contributing to the pooled analysis and wide CIs around the estimates of effect;
inconsistency, because many of the meta‐analyses demonstrated statistically significant heterogeneity (Chi² test P < 0.10) or had an I² > 50%;
indirectness, due to lack of clear reporting of the PFMT intervention or the control condition or both.
Some comparisons were downgraded for selection bias, arising from inadequate reporting of random sequence generation and random allocation. Most comparisons in the 'Summary of findings' tables were affected by more than one of the above and were downgraded twice or three times.
Trial quality and reporting
We evaluated methodological quality from the trial reports, which was limited when the only source of publication was from an abstract (see Included studies). In addition, abstracts reported few data.
The adequacy of reporting randomisation remains disappointing as fewer than half of the included trials reported both random sequence generation and allocation concealment and 13/38 studies described neither. The nature of the intervention means it was not feasible to blind the treatment provider or participants to group allocation (performance bias) in any of the included trials. The difficulty of blinding exercise‐based interventions is unavoidable. Furthermore, it is impossible to blind either of the primary outcomes in the review because both were self‐reported (prevalence of urinary incontinence or faecal incontinence and incontinence‐specific quality of life). Approximately three‐quarters of the trials (28/38) had a low risk of reporting bias but only just over half (21/38) were deemed to be low risk in terms of potential sources of other biases (Figure 2; Figure 3).
Based on the reported adequacy of randomisation, proportion and management of participant dropouts and withdrawals, and low risk of selective reporting or other biases, six trials appeared to be at low risk of bias (Chiarelli 2002; Dumoulin 2004; Hilde 2013; Mørkved 2003; Peirce 2013; Sangsawang 2016). However, this assessment did not take into account the quality of descriptions of the PFMT interventions or control conditions. If this was taken into account, the trial by Sangsawang 2016 would be downgraded in quality, as the intervention was of short duration and insufficient information was provided to determine the likely physiological effect of the PFMT. Sensitivity analysis on the basis of trial quality was not considered appropriate in view of the small number of trials contributing to each comparison.
Potential biases in the review process
We combined data from a diverse set of studies. This may inevitably impact on the applicability of our findings to practice. We summarise below the issues related to the heterogeneity of the studies we used.
Sources of heterogeneity
There were three notable sources of clinical heterogeneity. These were the variation in baseline characteristics (e.g. parity, type of delivery, type and duration of incontinence, if women were symptomatic when recruited), the PFMT programmes and the control care. To investigate the effects of baseline characteristics on treatment outcome would require an individual participant data meta‐analysis, which was beyond the scope of this review.
Variability of pelvic floor muscle training regimens
The content of PFMT programmes was often poorly described. Downgrading the evidence on the basis of inconsistency and indirectness was therefore inevitable in view of lack of information about PFMT and control conditions, PFMT content, and supervision of exercise programmes (see 'Summary of findings' tables).
More than half the trials provided insufficient information to be sure of the likely physiological effect of the exercise and only half reported confirmation of a correct PFM contraction prior to training (see PFMT regimens and control interventions, Included studies and Table 11). Consequently, it was difficult to evaluate the potential physiological efficacy of the exercise programmes. Including trials with a suboptimal exercise regimen alongside those with a sufficient regimen could adversely influence the pooled estimate of PFMT effect.
Alongside the physiological efficacy of the exercise, support for the behavioural aspects of exercise is also required. Behavioural support is commonly provided through supervision of exercise, and the extent of this varied markedly between trials. The least supervision was either one group or individual session to introduce the PFMT and the most was a mean of 85 classes between the sixth to 39th week of pregnancy (Table 11). Attendance was sometimes used as a surrogate for measuring adherence. It may be a good measure of adherence if the number of required attendances was sufficient to strengthen the PFM (Haskell 2007). However, if clinic attendance was less than twice per week, then it was likely that additional training needed to be completed at home to achieve a sufficient exercise regimen. Measurement of home exercise adherence then becomes a critical component of assessing the likely efficacy of the training. Half of the included trials reported some type of adherence data for women in the intervention or control groups but only nine studies asked women in both PFMT and control groups about their exercise behaviour (see Included studies). Adherence data should be collected in both study groups, although it is acknowledged that measuring it may change exercise behaviour. In turn, this may lead to an overestimate of the likely effect in 'real' life and may diminish the difference in effect between structured PFMT and control conditions.
Assessment of the interaction between quality and the effect of the intervention has been recommended but there were too few trials to conduct a formal sensitivity analysis by intervention quality (Herbert 2005). Rather than excluding or including trials on the basis of sufficiency of PFMT, or the likelihood that a clear‐cut comparison between PFMT and the control condition had been made, the preferred approach would be a sensitivity analysis on the basis of PFMT programme characteristics or amount of clinical difference between the PFMT and control interventions. However, more trials would be needed in each of the comparisons in the review before this was possible. We tried to distil information about the physiological and behavioural quality of the PFMT interventions, alongside the degree of contrast between the PFMT and control groups (see 'Sample characteristics' in Included studies and Summary of main results).
Variability of control conditions
The control conditions were also highly variable and usually poorly described, with many including a blanket statement about women in control groups receiving usual or standard care. However, it often it was unclear whether usual care encompassed advice about PFMT (i.e. written or verbal instructions) or a more ad hoc arrangement (see 'Sample characteristics' in Included studies, and Table 11).
Agreements and disagreements with other studies or reviews
The overall findings and conclusions in this updated review are generally the same as the previous version, despite this update containing more trials and substantially more data than the previous review and integrating the GRADE scores for assessing the quality of evidence (Boyle 2012). Since the last update of this review in 2012, one non‐Cochrane systematic review on the effects of PFMT during pregnancy and postpartum for the prevention and treatment of urinary incontinence has been published (Mørkved 2014). Although Mørkved 2014 considered the data in slightly different categories, they reported that PFMT during pregnancy and after delivery was effective in treating and preventing urinary incontinence, particularly when women adhered to a strength‐training protocol and were closely supervised. The findings of this review agreed with those of Mørkved 2014 relating to methodological factors such as the heterogeneity of the populations in the included trials, differences in reported outcome measures, and considerable variation in the PFMT and control conditions between trials.
Authors' conclusions
The findings from this review suggest that targeting continent antenatal women early in their pregnancy and offering a structured pelvic floor muscle training (PFMT) programme may prevent the onset of urinary incontinence in late pregnancy and postpartum. Population approaches, that is, recruiting antenatal women regardless of their continence status, might also reduce the prevalence of urinary incontinence in late pregnancy and postpartum but the effect may be less pronounced. However, the reasons for this are unclear. The findings about the effects of PFMT as a treatment for antenatal urinary incontinence are uncertain.
Similarly, it is uncertain whether a population‐based approach for delivery of postnatal PFMT (i.e. recruitment of women regardless of continence status immediately following delivery) is effective. It is possible that a 'high‐risk' approach (e.g. women who have an assisted delivery or deliver a large baby) leads to more clinical benefit than a population approach.
It is also unclear whether PFMT is an effective treatment for persistent urinary incontinence symptoms (i.e. women recruited at three months' postdelivery). This uncertainty around the efficacy of PFMT as a treatment for urinary incontinence in the immediate postnatal period is perhaps surprising given the summary findings of Dumoulin 2014, which suggested PFMT is an effective treatment for established urinary incontinence symptoms in non‐postnatal women.
We can suggest some plausible reasons for the differences in findings of the effectiveness of PFMT as a treatment for persistent postnatal urinary incontinence, compared to the findings of Dumoulin 2014, in non‐postnatal women. First, there are differences in the participants in the included trials. In this review, trials included postnatal women who may have altered physiological capabilities (muscle, nerve and connective tissue) consequent on the changes of pregnancy and delivery (Nygaard 2017). Postnatal women may find it particularly difficult to adopt or sustain exercise behaviour postdelivery, especially when they are distracted and occupied with caring for a new baby (Gillard 2010; Mason 2001). In contrast, Dumoulin 2014 reported outcomes from trials in non‐postnatal women, which may not have the same barriers. Second, there are differences in the comparator or control groups. In this review, the comparator group in the two large trials which carried the greatest weighting in the pooled estimate was usual care (which may have included PFMT), whereas the control group received no treatment in the majority of studies included in Dumoulin and colleagues' review (Analysis 4.3). It is possible that the potential lack of contrast between the intervention and control groups in this review contributed to the uncertainty surrounding the effect of PFMT as a treatment for postnatal urinary incontinence. Interestingly, in the one small study, which compared an intensively supervised strengthening PFMT programme to no treatment, rather than two larger trials that compared a minimally supervised PFMT programme with uncertain physiological effect, the benefit of PFMT was more marked (Analysis 4.3).
There are insufficient data on faecal incontinence to state whether or not PFMT is effective to prevent or treat this problem in pregnant or postpartum women. Furthermore, there are insufficient data to determine whether or not PFMT is effective to prevent urinary incontinence more than one year after birth. However, it is acknowledged that assessing the long‐term effects of PFMT is challenging, as women may go on to have subsequent pregnancies, be offered a specific PFMT programme if they had taken part in the control arm of a trial or initiate their own PFMT (Mørkved 2003).
Since the previous version of this review, 17 new studies have been added, most of which were small‐ to moderate‐sized trials (i.e. fewer than 500 women per arm). Unfortunately, the variability in rigour of methods and quality of reporting continued and this affords an opportunity to make some recommendations for further research (Boyle 2012).
First, the lack of faecal incontinence data was notable. It is encouraging to see some attention is being directed specifically towards investigations of faecal incontinence in antenatal and postnatal women (Johannessen 2017; Oakley 2016; Characteristics of studies awaiting classification). However, these studies are small and, therefore, unlikely to provide sufficient data for certainty about the effects of PFMT. Because fewer women may have faecal incontinence, every trial conducted on antenatal and postnatal incontinence must collect faecal as well as urinary incontinence data so we can learn more about this problem.
As there is insufficient evidence about the continuing effects of PFMT, trialists should, at a minimum, collect follow‐up data about antenatal training at three months' postpartum and about postnatal training at 12 months' postpartum. Ideally, for both antenatal and postnatal training, data should also be collected in both the intervention and control groups beyond one year.
The descriptions of the PFMT and control interventions and choice of outcome measures require attention. It is important that both the physiological and behavioural aspects of exercise are thoroughly described in both the intervention and control groups (Frawley 2017). In particular, there is a need to know what types of PFMT advice and behaviour occurs in the usual care group, as these details are infrequently measured or reported. In addition, it is recommended that all future trials collect valid measures of incontinence‐specific quality of life for both urinary incontinence and faecal incontinence (e.g. ICIQ‐SF for urinary incontinence and an agreed measure for faecal incontinence) (Avery 2007). In antenatal trials, the effect of PFMT on labour and delivery outcomes is worthy of further investigation. This would help to elucidate whether or not there are any associations between PFMT parameters, such as the type, frequency, intensity and duration of pelvic floor muscle (PFM) exercises and outcomes for mother and baby.
The evidence to date about the benefit of mixed prevention and treatment approaches is uncertain in antenatal populations and not at all clear in postnatal populations. However, these population approaches are probably the most common in clinical practice. It is possible that the effect of PFMT in these mixed approaches is diluted by some women who will never become incontinent and also those in whom PFMT is unlikely to be effective, such as those with denervation. Perhaps the focus in future population type trials should be to target women who are at heightened risk of developing urinary or faecal incontinence (such as women with a high body mass index or women who have had an assisted vaginal delivery).
The effect of PFMT for treatment of urinary and faecal incontinence, especially in antenatal women, is a high priority for further investigation. High‐quality health economics studies, alongside any future trials, are also a high priority.
Any further large pragmatic trials will ideally include process evaluation and fidelity checking, so some evaluation of treatment can be provided (Moore 2015).
Acknowledgements
We are grateful to Sue Bennett, Fiona Beyer, Dwayne Boyers, Chantale Dumoulin, Jemma Hudson, Andrea Lemos, Kate Walsh and Luke Vale for valuable comments on drafts of this review. We also thank Sheila Wallace for running the searches for this update.
We sincerely thank Hsin‐wen Wu and Xiaomei Yao for extracting data from the Chinese language papers. Unpublished data were kindly provided by Carolyn Sampselle and colleagues, Polly Hughes and Siv Mørkved. We acknowledge and thank Kate Fairbrother and Peter Herbison for their substantial contribution to a previous version of this review (Hay‐Smith 2008).
Appendices
Appendix 1. Search strategy
Terms used to search the Cochrane Incontinence Specialised Register are given below:
({design.rct*} or {design.cct*})
and
({intvent.prevent.pfe.} or {intvent.prevent.pfmt*} or {intvent.prevent.physicaltherapies} or {topic.urine.incon.prevent.} or {topic.urine.incon.prevent.postpartum.} or {topic.faecal.incon.prevent.} or {topic.faecal.incon.prevent.postobstet.} or {topic.urine.incon.postobstetric*} or {topic.faecal.incon.postobstetric*} or {topic.urine.incon.preg.} or {topic.urine.incon.stress.postnatal.} or {intvent.phys.biofeed*} or {intvent.phys.pfe*} or {topic.urine.incon.mixed.postnatal.} or {topic.urine.incon.mixed.preg.} or {topic.urine.incon.stress.preg.} or {topic.faecal.incon.preg.})
All searches were of the keyword field of Reference Manager 2012. The date of the last search was 16 February 2017.
Data and analyses
Comparison 1.
Antenatal pelvic floor muscle training (PFMT) versus control for prevention of incontinence
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Urinary incontinence in late pregnancy | 6 | 624 | Risk Ratio (M‐H, Random, 95% CI) | 0.38 [0.20, 0.72] |
| 1.1 PFMT versus no PFMT | 2 | 174 | Risk Ratio (M‐H, Random, 95% CI) | 0.14 [0.01, 2.04] |
| 1.2 PFMT versus usual care | 4 | 450 | Risk Ratio (M‐H, Random, 95% CI) | 0.44 [0.22, 0.91] |
| 2 Urinary incontinence early postnatal period (0‐3 months) | 5 | 439 | Risk Ratio (M‐H, Random, 95% CI) | 0.38 [0.17, 0.83] |
| 2.1 PFMT versus no PFMT | 2 | 174 | Risk Ratio (M‐H, Random, 95% CI) | 0.27 [0.11, 0.67] |
| 2.2 PFMT versus usual care | 2 | 198 | Risk Ratio (M‐H, Random, 95% CI) | 0.30 [0.04, 2.31] |
| 2.3 PFMT versus unspecified control | 1 | 67 | Risk Ratio (M‐H, Random, 95% CI) | 0.88 [0.43, 1.79] |
| 3 Urinary incontinence mid‐postnatal period (> 3‐6 months) | 5 | 673 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.71 [0.54, 0.95] |
| 3.1 PFMT versus no PFMT | 1 | 86 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.35, 2.20] |
| 3.2 PFMT versus usual care | 4 | 587 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.70 [0.52, 0.94] |
| 4 Urinary incontinence late postnatal period (> 6‐12 months) | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.20 [0.65, 2.21] |
| 4.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4.2 PFMT versus usual care | 1 | 44 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.20 [0.65, 2.21] |
| 4.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5 Urinary incontinence medium term (> 1‐5 years) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 5.1 PFMT versus no PFMT | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 PFMT versus usual care | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.3 PFMT versus unspecified control | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 Urinary incontinence long term (> 5 years) | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 6.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6.2 PFMT versus usual care | 2 | 352 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.07 [0.77, 1.48] |
| 6.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 7 Faecal incontinence late pregnancy | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 7.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 7.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 7.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 8 Faecal incontinence early postnatal period (0‐3 months) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 9 Faecal incontinence mid‐postnatal period (> 3‐6 months) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 10 Faecal incontinence late postnatal period (> 6‐12 months) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11 Faecal incontinence medium term (> 1‐5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12 Faecal incontinence long term (> 5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13 Incontinence‐specific quality of life | 1 | 152 | Mean Difference (IV, Fixed, 95% CI) | ‐2.42 [‐3.32, ‐1.52] |
| 13.1 PFMT versus no PFMT | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13.2 PFMT versus usual care | 1 | 152 | Mean Difference (IV, Fixed, 95% CI) | ‐2.42 [‐3.32, ‐1.52] |
| 13.3 PFMT versus unspecified control | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 14 Severity of incontinence | Other data | No numeric data | ||
| 14.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 14.2 PFMT versus usual care | Other data | No numeric data | ||
| 14.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 15 Loss of urine under stress test late pregnancy | 1 | 102 | Risk Ratio (M‐H, Random, 95% CI) | 0.36 [0.19, 0.70] |
| 15.1 PFMT versus no PFMT | 1 | 102 | Risk Ratio (M‐H, Random, 95% CI) | 0.36 [0.19, 0.70] |
| 16 Loss of urine under stress test early postnatal period (0‐3 months) | 3 | 322 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.35 [0.17, 0.75] |
| 16.1 PFMT versus no PFMT | 2 | 174 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.09 [0.02, 0.47] |
| 16.2 PFMT versus usual care | 1 | 148 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.33, 2.29] |
| 16.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 17 Quality of life and health status measures | Other data | No numeric data | ||
| 17.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 17.2 PFMT versus usual care | Other data | No numeric data | ||
| 17.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 18 Pelvic floor muscle function | Other data | No numeric data | ||
| 18.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 18.2 PFMT versus usual care | Other data | No numeric data | ||
| 18.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 18.4 PFMT plus vs PFMT | Other data | No numeric data | ||
| 19 Delivery outcome: caesarean section | 3 | 373 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.28 [0.89, 1.85] |
| 19.1 PFMT versus no PFMT | 1 | 76 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.83 [1.07, 3.15] |
| 19.2 PFMT versus usual care | 1 | 230 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.24 [0.66, 2.36] |
| 19.3 PFMT versus unspecified control | 1 | 67 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.68 [0.29, 1.57] |
| 20 Delivery outcome: other | Other data | No numeric data | ||
| 20.1 PFMT versus no control | Other data | No numeric data | ||
| 20.2 PFMT versus usual care | Other data | No numeric data | ||
| 20.3 PFMT versus unspecified control | Other data | No numeric data |
Comparison 2.
Antenatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Urinary incontinence late pregnancy | 3 | 345 | Risk Ratio (M‐H, Random, 95% CI) | 0.70 [0.44, 1.13] |
| 1.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 1.2 PFMT vs usual care | 3 | 345 | Risk Ratio (M‐H, Random, 95% CI) | 0.70 [0.44, 1.13] |
| 1.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 2 Urinary incontinence early postnatal period (0‐3 months) | 2 | 292 | Risk Ratio (M‐H, Random, 95% CI) | 0.75 [0.37, 1.53] |
| 2.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 2.2 PFMT versus usual care | 2 | 292 | Risk Ratio (M‐H, Random, 95% CI) | 0.75 [0.37, 1.53] |
| 2.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 3 Urinary incontinence mid‐postnatal period (> 3‐6 months) | 1 | 187 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.70, 1.24] |
| 3.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 3.2 PFMT versus usual care | 1 | 187 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.70, 1.24] |
| 3.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4 Urinary incontinence late postnatal period (> 6‐12 months) | 2 | 869 | Risk Ratio (M‐H, Random, 95% CI) | 0.50 [0.13, 1.93] |
| 4.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 4.2 PFMT versus usual care | 2 | 869 | Risk Ratio (M‐H, Random, 95% CI) | 0.50 [0.13, 1.93] |
| 4.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 5 Urinary incontinence medium term (> 1‐5 years) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 5.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6 Urinary incontinence long term (> 5 years) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 6.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 7 Faecal incontinence late pregnancy | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 8 Faecal incontinence early postnatal period (0‐3 months) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 9 Faecal incontinence mid‐postnatal period (> 3‐6 months) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 10 Faecal incontinence late postnatal period (> 6‐12 months) | 0 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 10.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 10.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 10.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 11 Faecal incontinence medium term (> 1‐5 years) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 11.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12 Faecal incontinence long term (> 5 years) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 12.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13 Faecal incontinence very long term (> 10 years) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 13.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 14 Incontinence‐specific quality of life | 1 | 41 | Mean Difference (IV, Fixed, 95% CI) | ‐3.5 [‐6.13, ‐0.87] |
| 14.1 PFMT versus no PFMT | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 14.2 PFMT versus usual care | 1 | 41 | Mean Difference (IV, Fixed, 95% CI) | ‐3.5 [‐6.13, ‐0.87] |
| 14.3 PFMT versus unspecified control | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 15 Quality of life and health status measures | Other data | No numeric data | ||
| 15.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 15.2 PFMT versus usual care | Other data | No numeric data | ||
| 15.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 16 Severity of incontinence | Other data | No numeric data | ||
| 16.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 16.2 PFMT versus usual care | Other data | No numeric data | ||
| 16.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 17 Pelvic floor muscle function | Other data | No numeric data | ||
| 17.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 17.2 PFMT versus usual care | Other data | No numeric data | ||
| 17.3 PFMT versus unspecified control | Other data | No numeric data |
Comparison 3.
Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Urinary incontinence late pregnancy | 9 | 3164 | Risk Ratio (M‐H, Random, 95% CI) | 0.74 [0.61, 0.90] |
| 1.1 PFMT versus no PFMT | 2 | 387 | Risk Ratio (M‐H, Random, 95% CI) | 0.24 [0.02, 2.53] |
| 1.2 PFMT versus usual care | 7 | 2777 | Risk Ratio (M‐H, Random, 95% CI) | 0.82 [0.72, 0.94] |
| 1.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 1.4 PFMT plus versus PFMT | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 2 Urinary incontinence early postnatal period (0‐3 months) | 5 | 760 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.80 [0.67, 0.95] |
| 2.1 PFMT versus no PFMT | 1 | 300 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.72 [0.51, 1.02] |
| 2.2 PFMT versus usual care | 3 | 367 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.67, 1.16] |
| 2.3 PFMT versus unspecified control | 1 | 93 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.77 [0.61, 0.97] |
| 3 Urinary incontinence mid‐postnatal period (> 3‐6 months) | 5 | 1921 | Risk Ratio (M‐H, Random, 95% CI) | 0.73 [0.55, 0.97] |
| 3.1 PFMT versus no PFMT | 1 | 300 | Risk Ratio (M‐H, Random, 95% CI) | 0.60 [0.38, 0.92] |
| 3.2 PFMT versus usual care | 3 | 1528 | Risk Ratio (M‐H, Random, 95% CI) | 0.85 [0.65, 1.11] |
| 3.3 PFMT versus unspecified control | 1 | 93 | Risk Ratio (M‐H, Random, 95% CI) | 0.42 [0.20, 0.86] |
| 4 Urinary incontinence late postnatal period (> 6‐12 months) | 2 | 244 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.85 [0.63, 1.14] |
| 4.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4.2 PFMT versus usual care | 2 | 244 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.85 [0.63, 1.14] |
| 4.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5 Urinary incontinence medium term (> 1‐5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6 Urinary incontinence long term (> 5 years) | 1 | 188 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.38 [0.77, 2.45] |
| 6.1 PFMT versus usual care | 1 | 188 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.38 [0.77, 2.45] |
| 7 Faecal incontinence late pregnancy | 2 | 867 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.30, 1.25] |
| 7.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 7.2 PFMT versus usual care | 2 | 867 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.30, 1.25] |
| 7.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 8 Faecal incontinence early postnatal period (0‐3 months) | 1 | 90 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.36 [0.04, 3.37] |
| 8.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 8.2 PFMT versus usual care | 1 | 90 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.36 [0.04, 3.37] |
| 8.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 9 Faecal incontinence mid‐postnatal period (> 3‐6 months) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 9.1 PFMT versus no PFMT | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.2 PFMT versus usual care | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 9.3 PFMT versus unspecified control | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10 Faecal incontinence late‐postnatal period (> 6‐12 months) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 10.1 PFMT versus no PFMT | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.2 PFMT versus usual care | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.3 PFMT versus unspecified control | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 11 Faecal incontinence medium term (> 1‐5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12 Faecal incontinence long term (> 5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13 Incontinence‐specific quality of life late pregnancy | 1 | 224 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐1.21, 0.81] |
| 13.1 PFMT versus no PFMT | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13.2 PFMT versus usual care | 1 | 224 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐1.21, 0.81] |
| 13.3 PFMT versus unspecified control | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 14 Incontinence‐specific quality of life early postnatal period (0‐3 months) | 1 | 211 | Mean Difference (IV, Fixed, 95% CI) | ‐0.60 [‐1.45, 0.25] |
| 14.1 PFMT versus no PFMT | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 14.2 PFMT versus usual care | 1 | 211 | Mean Difference (IV, Fixed, 95% CI) | ‐0.60 [‐1.45, 0.25] |
| 14.3 PFMT versus unspecified control | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 15 Incontinence‐specific quality of life late postnatal period (> 6‐12 months) | 1 | 190 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐1.20, 0.80] |
| 15.1 PFMT versus no PFMT | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 15.2 PFMT versus usual care | 1 | 190 | Mean Difference (IV, Fixed, 95% CI) | ‐0.20 [‐1.20, 0.80] |
| 15.3 PFMT versus unspecified control | 0 | 0 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 16 Severity of incontinence | Other data | No numeric data | ||
| 16.3 PFMT versus no PFMT | Other data | No numeric data | ||
| 16.4 PFMT versus usual care | Other data | No numeric data | ||
| 16.5 PFMT versus unspecified control | Other data | No numeric data | ||
| 17 Loss of urine under stress test early postnatal period (0‐3 months) | Other data | No numeric data | ||
| 17.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 17.2 PFMT versus usual care | Other data | No numeric data | ||
| 17.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 18 Quality of life and health status measures | Other data | No numeric data | ||
| 18.3 PFMT versus no PFMT | Other data | No numeric data | ||
| 18.4 PFMT versus usual care | Other data | No numeric data | ||
| 18.5 PFMT versus unspecified control | Other data | No numeric data | ||
| 19 Pelvic floor muscle function | Other data | No numeric data | ||
| 19.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 19.2 PFMT versus usual care | Other data | No numeric data | ||
| 19.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 19.4 PFMT plus vs PFMT | Other data | No numeric data | ||
| 20 Delivery outcome: caesarean section | 6 | 1899 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.95 [0.79, 1.14] |
| 20.1 PFMT versus no PFMT | 1 | 300 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.12 [0.79, 1.57] |
| 20.2 PFMT versus usual care | 5 | 1599 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.90 [0.73, 1.12] |
| 20.3 PFMT versus unspecified | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 21 Delivery outcome: other | Other data | No numeric data | ||
| 21.3 PFMT versus no PFMT | Other data | No numeric data | ||
| 21.4 PFMT versus usual care | Other data | No numeric data | ||
| 21.5 PFMT versus unspecified control | Other data | No numeric data | ||
| 22 Patient satisfaction and further treatment | Other data | No numeric data | ||
| 22.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 22.2 PFMT versus usual care | Other data | No numeric data | ||
| 22.3 PFMT versus unspecified control | Other data | No numeric data |
Analysis 3.16.
Comparison 3 Antenatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence, Outcome 16 Severity of incontinence.
Severity of incontinence
| Study | Measure of | Outcome measure | PFMT data | Control data | Difference |
|---|---|---|---|---|---|
| PFMT versus usual care | |||||
| Hughes 2001 | Frequency of leakage | Experiencing occasional or more than occasional urine leakage (not clear how measured) | 217 of 585 at 3 months postpartum | 210 of 584 at 3 months postpartum | Relative risk 1.03 (95% CI 0.89 to 1.20) |
| Hughes 2001 | Amount of leakage | Experiencing a drop or more than a drop of urine leakage (not clear how measured) | 228 of 585 at 3 months postpartum | 234 of 584 at 3 months postpartum | Relative risk 0.97 (95% CI 0.84 to 1.12) |
| Hughes 2001 | Other leakage severity | Not measured | |||
| Sampselle 1998 | Frequency of leakage | Not measured | |||
| Sampselle 1998 | Amount of leakage | Not measured | |||
| Sampselle 1998 | Other leakage severity | Average score from questionnaire re urine leakage with gentle cough, hard cough, sneeze and laugh scored 0 for none, 1 for dampness, 2 for wetness and 3 for soaked | Mean 0.38, SD 0.56, n=22 at 12 months postpartum | Mean 0.42, SD 0.49, n=24 at 12 months postpartum | Not calculated as validity/reliability of this measure not known |
Comparison 4.
Postnatal pelvic floor muscle training (PFMT) versus control for treatment of incontinence
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Urinary incontinence early postnatal period (0‐3 months) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 1.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 1.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 2 Urinary incontinence mid‐postnatal period (> 3‐6 months) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.1 PFMT plus versus PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 2.2 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 2.3 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 2.4 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 3 Urinary incontinence late‐postnatal period (> 6‐12 months) | 3 | 696 | Risk Ratio (M‐H, Random, 95% CI) | 0.55 [0.29, 1.07] |
| 3.1 PFMT versus no PFMT | 1 | 62 | Risk Ratio (M‐H, Random, 95% CI) | 0.29 [0.18, 0.47] |
| 3.2 PFMT versus usual care | 2 | 634 | Risk Ratio (M‐H, Random, 95% CI) | 0.80 [0.61, 1.06] |
| 3.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 4 Urinary incontinence medium term (> 1‐5 years) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 4.1 PFMT versus no PFMT | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 PFMT versus usual care | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.3 PFMT versus unspecified control | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 Urinary incontinence long term (> 5‐10 years) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 5.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.2 PFMT versus usual care | 1 | 516 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.88, 1.05] |
| 5.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6 Urinary incontinence very long term (> 10 years) | 1 | 471 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.94, 1.12] |
| 6.1 PFMT versus usual care | 1 | 471 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.94, 1.12] |
| 7 Faecal incontinence early postnatal period (0‐3 months) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 8 Faecal incontinence mid‐postnatal period (> 3‐6 months) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 9 Faecal incontinence late‐postnatal period (> 6‐12 months) | 2 | 620 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.24, 1.94] |
| 9.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 9.2 PFMT versus usual care | 2 | 620 | Risk Ratio (M‐H, Random, 95% CI) | 0.68 [0.24, 1.94] |
| 9.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 10 Faecal incontinence medium term (> 1‐5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11 Faecal incontinence long term (> 5‐10 years) | 1 | 509 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.95 [0.60, 1.50] |
| 11.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 11.2 PFMT versus usual care | 1 | 509 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.95 [0.60, 1.50] |
| 11.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12 Faecal incontinence very long term (> 10 years) | 1 | 468 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.36 [0.84, 2.22] |
| 12.1 PFMT versus no PFMT | 0 | 0 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12.2 PFMT versus usual care | 1 | 468 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.36 [0.84, 2.22] |
| 12.3 PFMT versus unspecified control | 0 | 0 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13 Incontinence‐specific quality of life | 1 | 18 | Mean Difference (IV, Fixed, 95% CI) | ‐1.66 [‐3.51, 0.19] |
| 13.1 PFMT versus usual care | 1 | 18 | Mean Difference (IV, Fixed, 95% CI) | ‐1.66 [‐3.51, 0.19] |
| 14 Severity of incontinence | Other data | No numeric data | ||
| 14.2 PFMT versus no PFMT | Other data | No numeric data | ||
| 14.3 PFMT versus usual care | Other data | No numeric data | ||
| 14.4 PFMT versus unspecified control | Other data | No numeric data | ||
| 15 Quality of life and health status measures | Other data | No numeric data | ||
| 16 Pelvic floor muscle function | Other data | No numeric data | ||
| 16.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 16.2 PFMT versus usual care | Other data | No numeric data | ||
| 16.3 PFMT versus unspecified control | Other data | No numeric data |
Comparison 5.
Postnatal pelvic floor muscle training (PFMT) versus control for (mixed) prevention or treatment of incontinence
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Urinary incontinence early postnatal period (0‐3 months) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2 Urinary incontinence mid‐postnatal period (> 3‐6 months) | 5 | 2800 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.75, 1.19] |
| 2.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 2.2 PFMT versus usual care | 5 | 2800 | Risk Ratio (M‐H, Random, 95% CI) | 0.95 [0.75, 1.19] |
| 2.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Random, 95% CI) | 0.0 [0.0, 0.0] |
| 3 Urinary incontinence late postnatal period (> 6‐12 months) | 3 | 826 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.71, 1.09] |
| 3.1 PFMT versus no PFMT | 1 | 107 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.82 [0.31, 2.21] |
| 3.2 PFMT versus usual care | 2 | 719 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.71, 1.10] |
| 3.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4 Urinary incontinence medium term (> 1‐5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 4.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5 Urinary incontinence long term (> 5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 5.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6 Faecal incontinence early postnatal period (0‐3 months) | 1 | 1609 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.51, 1.67] |
| 6.1 PFMT versus no PFMT | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 6.2 PFMT versus usual care | 1 | 1609 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.93 [0.51, 1.67] |
| 6.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 7 Faecal incontinence mid‐postnatal period (> 3‐6 months) | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7.1 PFMT versus no PFMT | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 PFMT versus usual care | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.3 PFMT versus unspecified control | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 Faecal incontinence late‐postnatal period (> 6‐12 months) | 1 | 107 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.73 [0.13, 4.21] |
| 8.1 PFMT versus no PFMT | 1 | 107 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.73 [0.13, 4.21] |
| 8.2 PFMT versus usual care | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 8.3 PFMT versus unspecified control | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 9 Faecal incontinence medium term (> 1‐5 years) | 0 | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 10 Incontinence‐specific quality of life | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 10.1 PFMT versus no PFMT | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.2 PFMT versus usual care | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 10.3 PFMT versus unspecified control | 0 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 11 Severity of incontinence | Other data | No numeric data | ||
| 11.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 11.2 PFMT versus usual care | Other data | No numeric data | ||
| 11.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 12 Loss of urine under stress test postpartum | 2 | 323 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.58, 1.57] |
| 12.1 PFMT versus no PFMT | 0 | 0 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 12.2 PFMT versus usual care | 2 | 323 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.58, 1.57] |
| 12.3 PFMT versus unspecified control | 0 | 0 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
| 13 Quality of life and health status measures | Other data | No numeric data | ||
| 13.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 13.2 PFMT versus usual care | Other data | No numeric data | ||
| 13.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 14 Pelvic floor muscle function | Other data | No numeric data | ||
| 14.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 14.2 PFMT versus usual care | Other data | No numeric data | ||
| 14.3 PFMT versus unspecified control | Other data | No numeric data | ||
| 14.4 PFMT plus versus PFMT | Other data | No numeric data | ||
| 15 Pelvic organ prolapse symptoms | Other data | No numeric data | ||
| 15.1 PFMT versus no PFMT | Other data | No numeric data | ||
| 15.2 PFMT versus usual care | Other data | No numeric data | ||
| 15.3 PFMT versus unspecified control | Other data | No numeric data |
What's new
Last assessed as up‐to‐date: 16 February 2017.
| Date | Event | Description |
|---|---|---|
| 21 December 2017 | New search has been performed | For this version, published in Issue 12, 2017, the following changes were made: 1. The search was updated to February 2017 and 17 new trials incorporated (taking the total number of included trials to 38 (involving 9892 women)). In addition, two abstracts which were the primary reference in the last version were replaced by full papers. 2. The GRADE method was implemented throughout the review to assess the quality of evidence; and a 'Summary of findings' table was added. 3. The comparisons and subgroups were substantially amended. 4. There has been a change in authorship. |
| 20 December 2017 | New citation required and conclusions have changed | 1. The overall findings are similar to the previous version of the review, with the exception of the evidence summary for the effectiveness of postnatal pelvic floor muscle training as a treatment for incontinence; we are less certain about this effect than previously. The findings altered because the way the data were grouped changed to report outcomes according to the time since the birth rather than time since intervention. This decision about timing of outcomes was made, a priori, when choosing outcomes for the 'Summary of findings' table. |
History
Review first published: Issue 4, 2008
| Date | Event | Description |
|---|---|---|
| 7 September 2012 | New search has been performed | Added 6 new studies |
| 7 September 2012 | New citation required but conclusions have not changed | Added 6 new studies |
| 18 April 2008 | Amended | Converted to new review format. |
| 3 March 2008 | New citation required and conclusions have changed | Substantive amendment |
| 11 September 2007 | New search has been performed | minor update |
Differences between protocol and review
1. In accordance with the latest Cochrane Handbook for Systematic Reviews of Interventions, this updated review now includes the use of GRADE to assess the quality of the body of evidence and includes 'Summary of findings' tables, which were not in the previous version of this review (Boyle 2012; Higgins 2011).
2. The way the data were grouped changed to report outcomes according to the time since the birth rather than time since intervention. This decision about timing of outcomes was made, a priori, when choosing outcomes for the 'Summary of findings' table.
3. A previously included trial was excluded (Dannecker 2004) (see the Characteristics of excluded studies).
Characteristics of studies
Characteristics of included studies [ordered by study ID]
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 98 postpartum primiparous women, 10‐16 weeks after delivery. Inclusion: normal term singleton vaginal delivery, stress UI. Exclusion: neurological bladder dysfunction or tumours in the genital area. Age, mean (SD), years: PFMT 33 (3.4); control 33 (3.9). Parity: primiparous. Delivery: not reported. BMI, mean (SD): PFMT 23 (3.5); control 23 (3.2). Incontinence at recruitment: 100% (as outlined in inclusion criteria). Setting: 4 different private antenatal clinics in the urban area of Stockholm, Sweden. |
|
| Interventions |
PFMT (n = 49): supervised home exercise programme (written instructions), daily exercises, for 6 months. Instructions from study midwife on how to perform correct PFM contraction, confirmed by vaginal palpation. Participants visited the midwife every 6 weeks (total of 3 times during the study period) for follow‐up of progress and to encourage PFMT. Control (n = 49): usual postnatal care. Instructions from study midwife on how to perform correct PFM contraction, confirmed by vaginal palpation. Received customary written postpartum instructions explaining PFM anatomy and recommendations around PFMT. |
|
| Outcomes | Measured at 3 (baseline) and 9 months' postpartum. Primary endpoint: 9 months' postpartum. UI at 9 months' postpartum: not reported. Primary outcome: PFM strength (maximal voluntary contraction) measured using perineometry (mmHg). Secondary outcomes: PFM endurance (sec), PFM strength using Oxford grading scale, self‐reported UI using ICIQ FLUTS short form questionnaire, general health form with 19 questions related to delivery, motherhood and current health status. |
|
| Notes | Losses to follow‐up at 9 months: PFMT 9/49; control 7/49 (total 16.3%). Funding: not specifically funded. Conflicts of interest: none declared |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported. |
| Allocation concealment (selection bias) | Low risk | "Allocated randomly through sequentially numbered and sealed envelopes." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. "A limitation of this study was that the midwife was not blinded during the project." |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 16.3% dropout; similar between groups; different reasons; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | High risk | Did not report data relating to adherence to the exercise programme and how women prioritised the exercises. |
| Other bias | Unclear risk | Study did not contribute any data to the forest plots. |
| Methods | 3‐arm, parallel, unblinded, RCT. | |
| Participants | 87 primiparous women. Inclusion: primiparous; ≤ 18 weeks' pregnant; aged 20‐35 years; and not presenting with diabetes, hypertension or UI prior to pregnancy. Exclusion: women who did not log their exercises, or gave up the collection of data. Age, mean (SD), years: PFMT (1) 26.3 (4.6); PFMT (2) 27.1 (5.4); control 26.6 (5.7). Parity: primiparous. Delivery: not measured as primary endpoint was during pregnancy. Weight, mean (kg), at 18 weeks: PFMT (1) 70.7 (18.4); PFMT (2) 65.5 (13.4); control 63.2 (9.6). Incontinence at recruitment: PFMT (1) 58.6%; PFMT (2) 51.7%; control 48.3%. Setting: Basic Health Units, Assis (Sao Paulo), Brazil. |
|
| Interventions |
PFMT 1 (n = 29): supervised home exercise programme, daily exercise at home, with up to 5 monthly visits from a physiotherapist (at 22, 26, 30, 34, and 38 weeks' gestation). Women received a manual of home exercises and were instructed on how to use it, as well as exercise and leakage diaries. PFMT 2 (n = 29): unsupervised PFMT, daily exercise at home as per the supervised group. Women received a manual of home exercises and were instructed on how to use it, as well as exercise and leakage diaries. Control (n = 29): no manual or supervision, and no exercise and leakage diaries. Unclear if instructed not to perform PFMT. Note: groups PFMT 1 and PFMT 2 were combined as the intervention group for comparison with controls. |
|
| Outcomes | Measured at baseline (up to 18 weeks' gestation), and at 22, 26, 30 and 34 weeks' gestation. Primary endpoint: 38 weeks' gestation. Primary outcome: self‐reported UI. Secondary outcome: PFM strength measured using perineometry (mmHg). |
|
| Notes | No dropouts. Funding: not reported. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated random number sequence. |
| Allocation concealment (selection bias) | Unclear risk | Prepared by 3rd party, sealed envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. Unclear if perineometry blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts. |
| Selective reporting (reporting bias) | High risk | Did not report UI severity (defined in methods as small, moderate and intense). |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm, parallel, unblinded, RCT (with unclear randomisation methods). | |
| Participants | 80 sedentary pregnant, primiparous and multiparous women. Inclusion: healthy, uncomplicated and singleton pregnancies. Exclusion: women who did not plan to give birth in the same obstetric department, did not receive medical follow‐up evaluations throughout their entire pregnancy, and who had experienced incontinence before pregnancy. Also, any type of absolute obstetric contraindication to aerobic exercise during pregnancy (such as haemodynamically significant heart disease, restrictive lung disease, incompetent cervix, multiple gestation, risk of premature labour, pre‐eclampsia/pregnancy‐induced hypertension, thrombophlebitis, recent pulmonary embolism (last 5 years), acquired infectious disease, retarded intrauterine development, serious blood disease, absence of antenatal control, or a combination). Age, mean (SD), years: PFMT 31 (3); control 30 (3). Parity: primiparous PFMT 65%; control 30%. Delivery: PFMT: 56.7% vaginal, 20.6% instrumental, 20.6% caesarean; control: 54.5% vaginal, 15.2% instrumental, 30.3% caesarean. BMI, mean (SD): PFMT 23.9 (3); control 24.8 (4). Incontinence at recruitment: none. Setting: obstetric department, Hospital de Fuenlabrada, Madrid, Spain. |
|
| Interventions |
PFMT (n = 40): approximately 7‐8 min of PFMT as part of a 35‐45 min multimodal physical conditioning programme. All sessions supervised by a qualified fitness specialist (working with groups of 10‐12 participants) with the assistance of an obstetrician, 3 days per week from the beginning of pregnancy (weeks 6‐9) to the end of the 3rd trimester (weeks 38‐39). Thus, an approximate 85 training sessions were originally planned for each participant in the event of no preterm delivery. No details of PFMT programme given and this appeared to have been introduced only in the 3rd trimester. Control (n = 40): unspecified, no information provided. |
|
| Outcomes | Measured "after delivery." Primary endpoint: not reported, but questionnaires given to participants "after delivery." Primary outcome: not reported. Other outcomes: self‐reported UI (ICIQ‐SF), maternal perception of health (SF‐36 King's Health Questionnaire), pregnancy outcomes. |
|
| Notes | Losses to follow‐up "after delivery": PFMT 6/40; control 7/40 (total 16.3%). Funding: no outside funding received. Conflicts of Interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Use of a random number table." |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 16.3% dropout; similar between groups (numbers and reasons); no mention of imputation for missing data. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) RCT, assessor‐blinded. | |
| Participants | 105 sedentary primiparous women. Inclusion: healthy and primiparous women with a singleton foetus, sedentary (defined as not having participated in regular exercise at least once per week, including significant amounts of walking) for the last 6 months, within the 1st 24 weeks of pregnancy, and able to understand verbal and written instructions in the Norwegian language. Exclusion: severe heart disease, pregnancy‐induced hypertension, history of ≥ 2 miscarriages, bleeding after 12 weeks' gestation, uncontrolled thyroid disease, pre‐eclampsia or other diseases that could affect participation. Age, mean (SD), in years: PFMT 31.2 (3.7); control 30.3 (4.4). Parity: 100% primiparous. Delivery: unclear, appeared to report delivery details for women with incontinence only. Of those with incontinence: PFMT 2 instrumental deliveries, 1 caesarean; control: 3 instrumental, 2 caesarean. BMI, mean (SD): PFMT 23.8 (3.8); control 23.9 (4.7). Incontinence at recruitment: UI: PFMT 27%, control 21%; flatus: PFMT 29%, control 23%; FI: PFMT 0, control 0. Setting: university‐conducted primary care study, single centre, Oslo, Norway. |
|
| Interventions |
PFMT (n = 52): as part of an aerobic fitness class (2‐3 times per week, 60 min), for at least 12 weeks. Progressive PFMT programme that was incorporated into 15 min of strength training which included PFMT. All sessions were led by instructors who were trained (which included instructions on how to explain a correct PFM contraction) by an experienced physiotherapist. Women were also encouraged to be physically active for at least 30 min per day and to increase their daily activity as much as possible. Women were given a book on general exercise during pregnancy with a specific PFMT pamphlet developed for pregnant women, explaining the anatomy of the pelvic floor, how to do a correct PFM contraction, and training prescription of 3 sets of 8‐12 close to maximum PFM contractions per day. Control (n = 53): usual antenatal care. |
|
| Outcomes | Measured before the start of the intervention (baseline, 12‐24 weeks' gestation), after the intervention (36‐38 weeks' gestation), and 6‐8 weeks' postpartum. Primary endpoint: not reported. Primary outcome: self‐reported UI and FI (flatus or anal incontinence, or both). Secondary outcomes: questions from the Severity Index and ICIQ‐SF. |
|
| Notes | Losses to follow‐up after the intervention (36‐38 weeks' gestation): PFMT 10/52; control 11/53 (total 20%). Losses to follow‐up 6‐8 weeks' postpartum: PFMT 9/52; control 6/53 (total 14.3%). Funding: not reported. Conflicts of interest: none declared. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "A statistical randomisation computer programme was used to perform a simple randomisation procedure (not block)." |
| Allocation concealment (selection bias) | Low risk | "A secretary not involved in the study assigned the participants to either the exercise group or the control group." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI and FI outcomes because they were participant reported. "The participants were asked not to reveal any information about group allocation to the principal investigator. The principal investigator was not involved in training the women, and was blinded to allocation while plotting and analysing the data... participants were interviewed by the blinded investigator and answered separate questions about incontinence." |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 14.3% dropout; differential loss (PFMT 17.3%, control 11.3%); similar reasons; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | High risk | Authors reported that only the overall prevalence of UI (primary outcome of this paper) was used in the statistical analysis of this study. However, it appeared that not all of the study's prespecified outcomes (such as questions relating to the severity of urinary tract symptoms as assessed by the Severity Index and ICIQ‐6) were reported. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 720 women recruited from postnatal wards. Inclusion: forceps or ventouse delivery or birth of baby weighing ≥ 4000 g. Exclusion: stillbirth or baby in neonatal intensive care unit, women with disabilities unable to perform PFMT, women who were not residents of Australia, women who could not speak English sufficiently to give consent. Age: PFMT 57% aged 20‐29 years; control 57% aged 20‐29 years. Parity: primiparous, PFMT 57%; control 57%. Delivery: PFMT 66% vaginal, 44% instrumental; control 65% vaginal, 45% instrumental. BMI: overweight or obese, PFMT 30%; control 32%. Incontinence prior to current pregnancy: PFMT 18%; control 17%. Setting: 3 hospitals in New South Wales, Australia. |
|
| Interventions |
PFMT (n = 370): taught 1‐to‐1 by a physiotherapist, over 2 visits in 8 weeks. Intervention also included discussion based on postnatal booklet (UI, pelvic floor function, PFMT, good bladder habits, type and amount of fluids, perineal care) and viewing perineum with hand mirror (for perineal trauma, haemorrhoids, and to practice perineal splinting for defecation) and practice of voluntary PFM contraction, the 'Knack', and transversus abdominus contraction. Postnatal pack also included red stick‐up dots, poster and partner information sheet in attempts to aid exercise adherence. Control (n = 350): usual postnatal care, no visit from physiotherapist. Hospital brochure available with general postnatal and PFMT advice, and invitation to join postnatal physiotherapy class held on wards. No restrictions on PFMT being recommended by other healthcare professionals. |
|
| Outcomes | Measured at 3 and 12 months' postpartum. Primary endpoint: 3 months' postpartum. Primary outcome: self‐reported UI (if answered occasionally, often, or always to a series of questions about stress or urgency UI). Secondary outcomes: incontinence severity (slight, moderate, severe), and self‐reported adherence. |
|
| Notes | Losses to follow‐up at 3 months: PFMT 22/370; control 22/350 (total 6.1%). Losses to follow‐up at 12 months: PFMT 49/370; control 50/350 (total 14%). In addition, at 12 months, 52 participants (PFMT 27; control 25) were pregnant and not included in the analysis. Funding: Medical Benefits Fund, Physiotherapy Foundation, and University of Newcastle Research Management Committee. Conflicts of interest: none declared. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Computer generated randomisation list contained the identification numbers for women in the trial." |
| Allocation concealment (selection bias) | Low risk | "The allocation to intervention or control group was placed by a research assistant in a sealed envelope marked with the corresponding study identification number." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible to blind participants. "Physiotherapist blinded to the women's allocation until interview at entry into the trial was complete." |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. "The interviewer was trained by PC and was blind to the group allocation of the women being interviewed" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 6.1% dropout; similar between groups; no reasons; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) RCT, nested into a cohort of 500 pregnant women. | |
| Participants | 79 pregnant women. Inclusion: UI in the current pregnancy (at 21‐26 weeks), single pregnancy, aged > 18 years, education to at least elementary school level and ability to understand the Portuguese language. Exclusion: previous urogenital surgery or diseases that may interfere with PFM strength (pelvic organ prolapse, neurological disorders, diabetes, pelvic or spinal injury). Age: not reported. Parity: not reported. Delivery: not reported. BMI: not reported. Incontinence at recruitment: 100% (refer to inclusion criteria). Setting: health service in Guarulhos (Sao Paulo), Brazil. |
|
| Interventions |
PFMT (n = 43): 5 or 6 biweekly sessions of PFMT supervised by a physiotherapist. Control (n = 36): instructed to perform a similar unsupervised PFMT at home. |
|
| Outcomes | Measured before beginning (2nd trimester of pregnancy) and after finishing (3rd trimester of pregnancy) the PFMT. Primary endpoint: not reported but presume after finishing PFMT (3rd trimester). Primary outcomes: self‐reported UI, urinary severity (ICIQ‐SF). Secondary outcome: PFM strength (perineometry). |
|
| Notes | Losses to follow‐up: PFMT 23/43; control 15/36 (total 48.1%). Funding: Sao Paulo Research Foundation (FAPESP) and National Council for Scientific Technological Development (CNPq). Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Computer‐generated sequence." |
| Allocation concealment (selection bias) | Low risk | "Opaque, sequentially numbered, sealed envelopes." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. Blinded PFM assessment. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 48.1% dropout; unclear if there was a differential between groups; no reasons; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Unclear risk | This was reported in a conference abstract with limited information about study methods. Initial estimated sample size was 74 (37 per group). The abstract states that 42 women were recruited but Table 1 in the abstract reports data for only 41 (20 in PFMT and 21 in control group) participants. This may have affected the power of the study. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 92 pregnant women. Inclusion: women 20‐34 weeks' gestation, complaints of stress/mixed UI, no genitourinary system pathology or UTI, who had at least primary school education. Exclusion: pregnancy complications, high risk for preterm labour, pain during PFMT, disease that could interfere with participation and were unable to attend for regular treatment. Age, mean (SD), years: PFMT 26.0 (4.8); control 27.7 (7.2). Parity: ≥ 1 pregnancy which reached term PFMT: 37.5%; control 47.5%. Delivery: spontaneous PFMT 88%; control 95.2%. BMI: not reported. Incontinence at recruitment: 100% women in trial incontinent at recruitment. Setting: obstetric clinic, single centre, Istanbul, Turkey. |
|
| Interventions |
PFMT (n = 46): trained by researcher how to do PFMT in accordance with booklet. Trained until all women were contracting the correct muscle group. Evaluated to check if performing PFMT correctly and retrained if not. Exercise session included 3 sets of exercise. Each set included contraction and relaxation of PFM, held for 10 sec, repeated 10 times. Duration of treatment not reported. Control (n = 46): usual antenatal care. |
|
| Outcomes | Measured at baseline (20‐34 weeks' gestation), intermediate evaluation (36‐38 weeks' gestation), and 6‐8 weeks' postpartum. Primary outcome: not reported. Outcomes: self‐reported leakage episodes, pad test (g, leakage), number of incontinence episodes per day, urgency and PFM strength (cm of water). |
|
| Notes | Losses to follow‐up after baseline evaluation PFMT 6/46; control 6/46 (total 13%). Losses to follow‐up by 6‐8 weeks' postpartum: PFMT 11/46; control 13/46 (total 26.1%). Funding: Research Fund of the University of Istanbul. Conflicts of interest: none declared. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomly allocated to a PFMT group or to control group using envelopes." |
| Allocation concealment (selection bias) | Unclear risk | "Randomly allocated to a PFMT group or to control group using envelopes." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. Unclear if pad test or PFM strength blinded. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 26.1% dropout; differential loss (PFMT 23.9%; control 28.3%); reasons provided, but not for each group; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 40 women recruited from antenatal outpatient clinic. Inclusion: nulliparous pregnant women. Exclusion: not reported. Age, mean (SD), years: not reported. Parity: nulliparous. Delivery: not reported. BMI: not reported. Incontinence at recruitment: not reported. Setting: antenatal outpatient clinic, Ankara Medical Faculty, Turkey. |
|
| Interventions |
PFMT (n = 20): unspecified, no information of PFMT programme provided. Control (n = 20): unspecified. Note: assumed, but not stated that the 40 participants were randomly allocated into 2 groups of 20. |
|
| Outcomes | Visits at weeks 12, 22 and 32 of gestation and week 6 postpartum. Primary endpoint: not reported. Primary outcome: not reported. Outcomes: lower urinary tract symptoms, sexual function and quality of life (UDI‐6, IIQ‐7, PISQ‐12), PFM activity (electromyographic biofeedback), valsalva‐urethral rotation angle measured using perineal ultrasound. |
|
| Notes | Losses to follow‐up: PFMT 9/20; control 7/20 (total 40%). Funding: not reported. Conflicts of interest: none declared. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomised." |
| Allocation concealment (selection bias) | Unclear risk | "Randomised." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. Un clear if ultrasound and electromyographic biofeedback blinded. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 40% dropout; similar between groups; no reasons; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | High risk | Difficult to assess. Report some of the outcome measures in results, but unclear if all are reported. |
| Other bias | Unclear risk | This was reported in a conference abstract with limited information about study methods, and did not contribute any data to the forest plots. |
| Methods | 3‐arm (parallel groups) RCT. | |
| Participants | 64 postnatal women with persistent stress UI symptoms (and urodynamic stress UI) ≥ 3 months after last delivery. Inclusion: aged < 45 years, premenopausal, symptoms of UI once per week ≥ 3 months after last delivery, willing to participate in trial. Exclusion: UI before pregnancy, previous surgery for stress UI, neurological or psychiatric disease, major medical conditions, taking medication that would interfere with evaluation or treatment, current pregnancy, inability to understand French or English instructions, moderate‐to‐severe pelvic organ prolapse (POP‐Q stage ≥ II), postvoid residual > 50 mL, < 5 g leakage on stress test (250 mL bladder volume and 20 min pad test with 10 jumping jacks substituted for standard jumping exercises), detrusor overactivity on urodynamics. Age, median (IQR), years: PFMT (1) 37 (34 to 29); PFMT (2) 36 (23 to 39); control 36 (34 to 38). Parity, median (IQR): PFMT 2 (2 to 2); PFMT (2) 2 (2 to 3); control 2 (1 to 3). Delivery: not reported. BMI, median (IQR): PFMT 22 (20 to 24); PFMT (2) 24 (23 to 26); control 24 (22 to 26). Incontinence at recruitment: all (refer to exclusion criteria). Setting: single‐centre, obstetrics clinic, Sainte‐Justine Hospital, Canada. |
|
| Interventions |
PFMT 1 (n = 23): as part of multimodal PF rehabilitation and transverse abdominis muscle contraction. PFMT 2 (n = 21): as part of multimodal PF rehabilitation programme taught by physiotherapist. In addition to home PFMT this group had 15 min of electrical stimulation and 25 min of PFMT with electromyographic feedback weekly for 8 weeks. Control (n = 20): relaxation massage of back and extremities by physiotherapist, asked not to exercise PFM at home. Same number of contacts with health professional as PFMT group. Offered treatment at end of study. Note: combined PFMT groups as the intervention group for comparison with control group. |
|
| Outcomes | Measured 9 weeks after intervention began. Primary endpoint: 9 weeks. Primary outcome: modified 20 min pad test with standardised bladder volume. Secondary outcomes: perceived burden of incontinence (visual analogue scale), UDI, IIQ, PFM dynamometry. |
|
| Notes | Losses to follow‐up at 9 weeks: PFMT 1/44; control 1/20 (total 3%). Funding: Canadian Institutes of Health Research and Laborie Medical Technologies Inc through a Canadian Institutes of Health Research‐Industry grant. C Dumoulin was supported by studentships from the Canadian Institutes of Health Research and from the Fonds de la Recherche en Santé du Quebec. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Stratified randomisation was performed using a balanced block randomisation schedule generated from a table of random numbers." |
| Allocation concealment (selection bias) | Low risk | "A research investigator who was not involved in any intervention or outcome assessment informed all participants of their group allocation, which was pre‐established by the randomisation schedule." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. "The participants were asked not to disclose their group allocation to the evaluators." Blinded pad test assessment. "A nurse‐assessor who was unaware of the treatment allocation of the participant administered the test." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 3% dropout; similar between groups; different reasons (2 women); no mention of imputation for missing data. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 234 women recruited from postnatal wards. Inclusion: women who delivered in a 19‐week period from November 2001 to March 2002, scored ≥ 9 on the SIFCRAT or already experiencing incontinence, or both. Exclusion: stillbirth, baby at high risk (e.g. very low birthweight), mother aged < 16 years, insufficient comprehension to complete study documentation, mother or midwife requesting treatment from physiotherapist for incontinence. Age: PFMT 48% aged 20‐29 years; control 45% aged 20‐29 years. Parity: primiparous, PFMT 39%; control 36%. Delivery: not reported. BMI: ≥ 26, PFMT 35%; control 39%. Incontinence at recruitment: PFMT 65%; control 62%. Setting: single centre, Taunton and Somerset Hospital, UK. |
|
| Interventions |
PFMT (n = 117): taught 1‐to‐1 with physiotherapist in hospital, with invitation to attend PFMT group at 2 and 4 months after delivery. No details of PFMT programme given. Control (n = 117): usual postnatal care including verbal promotion of postnatal PFMT and leaflet explaining how to do PFMT. |
|
| Outcomes | Measured at 6 months' postpartum. Primary endpoint: 6 months' postpartum. Primary outcome: some or no problem with stress UI (dichotomised response from single question from BFLUTS). |
|
| Notes | Losses to follow‐up at 6 months: PFMT 27/117; control 17/117 (total 18.8%). Funding: National Health Service (South West) R&D Project Grant Scheme. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Serially numbered opaque envelopes containing codes produced from computer generated pseudo‐random numbers." |
| Allocation concealment (selection bias) | Low risk | "Serially numbered opaque envelopes containing codes produced from computer generated pseudo‐random numbers." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 18.8% dropout; differential loss (PFMT 23.1%; control 14.5%); no reasons; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 282 nulliparous, pregnant women, 20‐28 weeks' gestation. Inclusion: nulliparous, aged ≥ 18 years, covered by health insurance, able to read French, carrying an uncomplicated singleton pregnancy, and with or without UI (including UI before pregnancy). Exclusion: previous delivery or abortion after 22 weeks' gestation, high‐risk pregnancy, any condition contraindicating further long‐distance travel, or previous PFMT < 6 months prior. Age, mean (SD), years: PFMT 29.4 (5.1); control 29.4 (5.1). Parity: nulliparous. Delivery: PFMT 52.6% vaginal, 21.2% instrumental, 26.2% caesarean section; control 52.9% vaginal, 25.7% instrumental, 21.3% caesarean section. BMI, mean (SD): PFMT 22.3 (4.4); control 22.6 (3.6) Incontinence at recruitment: PFMT 32.9%; control 37.3%. Setting: 5 university teaching hospitals (Nîmes, Poissy‐Saint‐Germain, Clermont‐Ferrand, Clamart and Saint‐Denis‐de‐la‐Réunion), France. |
|
| Interventions |
PFMT (n = 140): 1‐to‐1 sessions, 20‐30 min once per week, between 6th and 8th month of pregnancy (total of 8). An evaluation of PFM contraction was performed at each session through vaginal examination. PFMT supervised by 37 different therapists (physiotherapists and midwives who received an initial training course given by a physiotherapist specialising in PFM training), chosen by the woman from the list drawn up in each centre. Women were encouraged to perform daily PFM exercises at home. No specific instructions provided on the number or intensity of the contractions. However, note that abstract (Fritel and colleagues 2013) states women were given written information about UI and how to perform a series of 10 to 20 PFM contractions daily. Control (n = 142): written information on pelvic floor anatomy and PFM contraction exercises, at the time of inclusion. These instructions were also given to the PFMT group. |
|
| Outcomes | Measured at baseline (inclusion visit, 20‐28 weeks' gestation), end of pregnancy, and 2 and 12 months' postpartum. Primary endpoint: 12 months' postpartum. Primary outcome: self‐reported UI severity measured with ICIQ‐SF. Secondary outcomes: pelvic floor symptoms (Baessler Female Pelvic Floor Questionnaire, includes bladder, bowel, prolapse, sexual function scores), quality of life (Contilife, EuroQoL‐5D), clinical assessment of UI (24‐hour pad test at 2 months' postpartum), PFM strength (Laycock PFM digital palpation at 2 months' postpartum), questionnaire regarding frequency and duration of PFM contractions (end of pregnancy, 2 and 12 months' postpartum). |
|
| Notes | Losses to follow‐up at 12 months' postpartum: PFMT 47/140; control 45/142 (total 33%). Funding: French Ministry of Health. Conflicts of interest: none declared. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Women were randomly assigned to a group at a 1:1 ratio. Stratification was performed according to the centre. The randomised list was generated using the Proc Plan from SAS (block of six). The block sizes were blinded for research and health professionals (information not divulged in the study protocol)." |
| Allocation concealment (selection bias) | Low risk | "The random allocation sequence was secured in sequentially numbered sealed envelopes not accessible to the obstetrician." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. Blinded assessment of POP‐Q, PFM strength and pad test. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 33% dropout; similar between groups; no reasons; no mention of imputation for missing data (have done a non‐completers analysis). |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) RCT (with unclear randomisation methods and no mention of blinding). | |
| Participants | 128 pregnant women. Inclusion: primiparous, vaginal delivery, ≥ 18 years of age. Exclusion: not reported. Age: not reported. Parity: primiparous. Delivery: vaginal, not reported per group. BMI: not reported. Incontinence prior to current pregnancy: not reported. Setting: Queen's Medical Center, Honolulu, Hawaii. |
|
| Interventions |
PFMT (n = 64): standard postpartum discharge instructions plus written and verbal instructions for PFMT. No details of PFMT programme given. Control (n = 64): standard postpartum discharge instructions which likely included education about PFMT. |
|
| Outcomes | Measured at baseline (presumably antenatal) and 6‐8 weeks' postpartum (by telephone). Primary endpoint: presumably 6‐8 weeks' postpartum. Primary outcome: not reported. Outcomes: UI, urogenital distress, quality of life. |
|
| Notes | Losses to follow‐up at 6‐8 weeks' postpartum: PFMT 33/64; control 23/64 (total 44%). Funding: not reported. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomized clinical trial." |
| Allocation concealment (selection bias) | Unclear risk | "Randomized clinical trial." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 40% dropout; differential loss with nearly one‐third more from control group; no reasons; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | High risk | Difficult to assess. No data reported, so failed to present a key outcome that would have been expected to have been reported. Some data also not reported (currently being analysed); "The remaining data which was collected is in the process of being analysed and may or may not have a significant impact on results." |
| Other bias | Unclear risk | Reported in a conference abstract with limited information about study methods and did not contribute data to the forest plots. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 100 pregnant women. Inclusion: 38‐42 weeks' gestation. Exclusion: not reported. Age, mean (SD), years: total 32.6 (5). Parity: not reported. Delivery: not reported. BMI: not reported. Incontinence prior to pregnancy: UI: PFMT 16%; control 10% (note, unclear how many women were incontinent at recruitment). Setting: urology clinic, University Hospital, Perugia, Italy. |
|
| Interventions |
PFMT (n = 50): 8‐week programme, included 2 weekly sessions where Kegel exercises were taught (repeated daily at home for 20 min), and stretching exercises designed to correct agonist and antagonist muscle involvement. Control (n = 50): no pelvic or perineal rehabilitation. No other information provided. |
|
| Outcomes | Measured at baseline (38‐42 weeks' gestation), 3 and 6 months' postpartum. Primary endpoint: not reported. Primary outcome: not reported. Outcomes: number with UI, daily pad tests, stress tests, participant satisfaction (visual analogue scale). |
|
| Notes | Losses to follow‐up at 6 months. postpartum: PFMT 2/50; control 5/48 (total 7%). Funding: not reported. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomised study." |
| Allocation concealment (selection bias) | Unclear risk | "Randomised study." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. Unclear if stress test was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 7% dropout; differential loss (PFMT 4%; control 10%); no reasons; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | High risk | Did not report outcomes for number of daily pads or stress tests. |
| Other bias | Unclear risk | Reported in a conference abstract with limited information about study methods. |
| Methods | 2‐arm (parallel groups) RCT, open‐label. | |
| Participants | 127 healthy nulliparous women. Inclusion: nulliparous women. Exclusion: history of genitourinary or neuromuscular pathology, previous pregnancy and previous PFMT with a physiotherapist < 6 months before pregnancy. Age, mean (SD), years: PFMT 25.68 (4.22); control 26.79 (3.72). Parity: 100% nulliparous. Delivery: episiotomy PFMT 3%; control 9.5%. BMI, mean (SD): PFMT 22.19 (1.19); control 21.63 (1.64). Incontinence at recruitment: none. Setting: 2 outpatient physiotherapy clinics in a primary care setting, Italy. |
|
| Interventions |
PFMT (n = 65): 12‐week PFMT programme during pregnancy, supervised by a physiotherapist and a midwife. Control (n = 62): routine care and PFMT customary instruction at intake visit. |
|
| Outcomes | Measured at baseline, 12 weeks' postpartum, 6 months' postpartum. Primary endpoint: not reported. Primary outcomes: occurrence of traumatic tears and use of episiotomy. Secondary outcomes: PFM strength, PFM dysfunction (UI, FI and pelvic pain). |
|
| Notes | Dropouts after 1st assessment: PFMT 5/65; control 7/62 (total 9.4%). Unclear if any further dropouts following this time‐point. Funding: not reported. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Open‐label randomised clinical trial." |
| Allocation concealment (selection bias) | Unclear risk | "Open‐label randomised clinical trial." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Measure of UI and FI not reported. Presumably self‐reported as no indication of objective measure such as cough test. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 9.4% dropout; similar between groups; reasons provided, but not for each group; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | High risk | Did not report outcomes relating to FI and pelvic pain. |
| Other bias | Unclear risk | Reported in a conference abstract with limited information about study methods and few data. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 747 women with symptoms of UI at 3 months' postpartum. Inclusion: women with any UI in the preceding month. Exclusion: stillbirth, neonatal death. Age, mean (SD), years: PFMT 30 (5); control 29 (5). Parity: primiparous, PFMT 36%; control 37%. Delivery: PFMT 78.3% vaginal, 13.7% assisted, 8% caesarean; control 78.6% vaginal, 13.8% assisted, 7.6% caesarean. BMI: not reported. Incontinence at recruitment: all. Setting: 3 centres (Dunedin, Aberdeen, Birmingham) in 2 countries (New Zealand and UK). |
|
| Interventions |
PFMT (n = 371): home visit from nurse, health visitor or continence advisor at 5, 7 and 9 months for instruction and supervision of PFMT. Also education on PF anatomy. Frequency and urgency strategies were added at 2nd or 3rd visits if appropriate. Referral to primary care physician for women whose symptoms were not typical of stress, urgency or mixed UI, or had evidence of UTI. Control (n = 376): usual postnatal care that may have included advice on PFMT. |
|
| Outcomes | Measured at 12 months' postpartum and 6 years after index delivery. Primary endpoint: 12 months' postpartum. Primary outcome: self‐reported UI. Secondary outcomes: severity of incontinence (visual analogue scale), FI, use and frequency of PFMT, use of pads, general well‐being, Hospital Anxiety and Depression scale. |
|
| Notes | Losses to follow‐up at 12 months: PFMT 92/371; control 131/376 (total 29.9%). Losses to follow‐up at 6 years: PFMT 108/371; control 123/376 (total 30.9%). Funding: Wellbeing (grant sponsored by GlaxoWellcome) and Health Research Council of New Zealand. Conflicts of interest: none declared. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomisation was achieved with remote access to a computer programme in Dunedin. It registered each woman before presenting the allocation by using stratification by parity (four versus fewer), method of delivery (caesarean versus other) and frequency of incontinence (at least once per week versus less)." |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. "Intervention could not be performed blind." |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. "Collection of outcome data were by anonymised questionnaire which was identified by a study number and which could not be related back to trial allocation at time of data entry." |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 29.9% dropout; differential loss (PFMT 24.8%; control 34.8%; "differential loss to follow up confined to participants in one centre [Birmingham]"); few reasons provided ("women who did not respond at follow up were more likely to have had severe incontinence at baseline"); the impact of differential loss to follow‐up was explored with analyses stratified by centre. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 75 pregnant nulliparous women. Inclusion: aged 15‐35 years without stress UI at 20 weeks' gestation. Exclusion: multiple pregnancy, ≥ 2 caesarean births, oligohydramnios or polyhydramnios, cervical incompetence, maternal‐fetal iso‐immunisation, severe pregnancy‐induced hypertension, chronic degenerative conditions affecting pelvic floor function such as diabetes mellitus and multiple sclerosis. Age, mean (SD), years: PFMT 26 (6); 24 (7). Parity, mean (SD): PFMT 1.4 (0.8); control 1.4 (0.7). Delivery: PFMT 42.1% vaginal, 57.9% caesarean; control 64.7% vaginal, 35.3% caesarean Weight at 35 weeks' gestation, mean (SD), kg: PFMT 66 (7); control 66 (13). Incontinence at recruitment: none (see inclusion criteria). Setting: single‐centre, Mexico. |
|
| Interventions |
PFMT (n = 38): taught by physiotherapist. 8 × 1‐hour visits over 8 weeks, then weekly telephone calls. Also received information about anatomy and physiology of lower urinary tract, and biofeedback from surface electromyography electrodes (either side of anus) at clinic visits. Control (n = 34): requested not to perform PFMT during pregnancy or postpartum. |
|
| Outcomes | Measured at 28 and 35 weeks' gestation, and 6 weeks' postpartum. Primary endpoint: 6 weeks' postpartum. Primary outcome: self‐reported UI. Secondary outcomes: frequency and severity of UI, cough test, PFM activity (electromyography). |
|
| Notes | Losses to follow‐up: 3/75 (total 4%); data not available by group. Funding: not reported. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants names in sealed envelopes and assigned random numbers to divide them into 2 groups randomly. |
| Allocation concealment (selection bias) | Low risk | The sealed envelopes were held by the secretary who did not have any relationship to the study: she opened them and assigned the women to each group. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. Unclear if cough test and electromyography were blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 4% dropout; unclear if similar between groups; no reasons provided; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Unclear risk | Significant difference between groups with respect to weight gain during pregnancy (greater in the PFMT group) and self‐reported UI at 28 weeks' gestation (more prevalent in the PFMT group). |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 175 singleton primiparous women. Inclusion: singleton primiparous women who delivered vaginally after 32 weeks' gestation and able to speak and understand Scandinavian languages. Instrumental deliveries was noted as an inclusion in a secondary report (Bø and colleagues 2015; see Hilde 2013). Exclusion: prior abortion or stillbirth after gestational week 16; serious illness to mother or neonate; or perineal tearing graded as 3b, 3c or 4. Caesarean section noted as an exclusion criterion in secondary reports (Bø and colleagues 2013; Bø and colleagues 2015; see Hilde 2013), as were intrauterine fetal deaths/stillbirths (Bø and colleagues 2015; see Hilde 2013). Age, mean (SD), years: PFMT 29.5 (4.3); control 30.1 (4.0). Parity: primiparous. Delivery: all vaginal; 20% instrumental in total. BMI, mean (SD): PFMT 26.0 (4.1); control 25.3 (3.9). Incontinence at recruitment: UI PFMT 39.1%; control 50%. Setting: Akershus University Hospital, Norway. |
|
| Interventions |
PFMT (n = 87): supervised exercise class (once per week) led by an experienced physiotherapist, that included progressive PFMT programme (Bø 1990; Mørkved 1997), 16 weeks' duration. Women received individual instructions in how to perform a correct PFM contraction (including vaginal palpation and feedback). Also asked to perform daily PFMT at home (3 sets of 8‐12 contractions close to maximal contraction). All women were provided customary written information on discharge from postnatal ward and an exercise diary. Control (n = 88): individual instructions in how to perform a correct PFM contraction (including vaginal palpation and feedback) and a written leaflet containing information about PFMT and encouragement to perform these regularly. No further intervention provided. |
|
| Outcomes | Measured at 6 weeks' postpartum (baseline), and 6 months' postpartum. Primary endpoint: 6 months' postpartum. Primary outcome: self‐reported UI. Secondary outcomes: positive pad test (2 g); vaginal resting pressure, PFM strength and endurance (manometry). Stage of pelvic organ prolapse, bladder neck position and symptoms of pelvic organ prolapse (ICIQ‐vag) were outcomes included the secondary analysis (Bø and colleagues 2015; see Hilde 2013). |
|
| Notes | Losses to follow‐up at 6 months' postpartum: PFMT 12/87; control 3/88 (total 8.6%). Funding: Research Council of Norway. Conflicts of interest: none declared. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "The participants were stratified on major levator ani muscle defects being present or not at the very end of the baseline assessment and thereafter randomised into two groups (training or control) in blocks of 10. The randomisation sequence was computer‐generated and concealed." |
| Allocation concealment (selection bias) | Low risk | "Allocation of participants was administered outside the clinical room by a project midwife keeping the outcome assessors blinded for group allocation." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. All other outcomes blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 8.6% dropout; differential loss (PFMT 13.8%; control 3.4%); no reasons; imputation for missing data (missing values for continuous data were imputed by using the baseline value plus added change observed in the corresponding control group. For self‐reported UI, last observation carried forward was used). |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 1169 pregnant nulliparous women. Inclusion: pregnant nulliparous women at 20 weeks' gestation. Exclusion: diabetes, neurological conditions, previous bladder surgery or investigations. Age, median (IQR), years: PFMT 28 (24‐31); control 28 years (25‐31). Parity: all nulliparous. Delivery: PFMT 52.5% vaginal, 26.9% instrumental, 20.6% caesarean; control 54.8% vaginal, 23.5% instrumental, 21.7% caesarean. BMI, median (IQR): PFMT 23.2 (21.2‐26.3); control 23.5 (21.6‐25.7). Incontinence prior to pregnancy: PFMT 1.5%; control 1.4%. Incontinence by 20 weeks: PFMT 22%; control 30%. Setting: single centre, UK. |
|
| Interventions |
PFMT (n = 586): 1 individual appointment with a physiotherapist that included tuition in use of perineometer, information on anatomy/physiology, and vaginal palpation of voluntary PFM contraction, and 1 PFMT group session (maximum 6 women) with senior obstetric physiotherapist between 22 and 25 weeks. Written instructions for antenatal and postnatal daily home PFMT. No details of PFMT programme given. Control (n = 583): routine community antenatal care, including usual information about PFMT. |
|
| Outcomes | Measured at 6 weeks, and 3 and 6 months' postpartum. Primary endpoint: 6 months' postpartum. Primary outcome: not reported. Outcomes: BFLUTS, additional questions about bowel function. |
|
| Notes | Losses to follow‐up at 6 weeks' postpartum: PFMT 238/586; control 217/583 (total 38.9%). Losses to follow‐up at 3 months' postpartum: PFMT 178/586; control 139/583 (total 27.2%). Losses to follow‐up at 6 months' postpartum: PFMT 203/586; control 189/583 (total 33.5%). Funding: not reported. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomised using computer generated numbers." |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. Not reported if perineometry was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 33.5% dropout; similar between groups; no reasons; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results, and additional data were supplied by authors, from a thesis (as trial was reported as an abstract). |
| Other bias | Unclear risk | Reported in a conference abstract with limited information about study methods. |
| Methods | 2‐arm, parallel groups RCT. | |
| Participants | 20 women with UI symptoms, < 6 weeks' postpartum. Inclusion: UI after childbirth, as diagnosed by an urogynaecologist, < 6 weeks after normal vaginal delivery. Exclusion: genitourinary disease or infection, treatment administered for UI, obstetrical operation history. Age, mean (SD), years: PFMT 31.4 (2.8); control 32.0 (2.6). Parity, mean (SD), number: PFMT 1.4 (0.5); control 1.6 (0.5). Delivery: normal vaginal. BMI, mean (SD): PFMT 23.6 (1.8); control 24.6 (1.8). Incontinence at recruitment: all. Setting: Dong‐gu, Daejeon, Republic of Korea. |
|
| Interventions |
PFMT (n = 10): utilising trunk stabilisation (Koumantakis 2005), as part of a group session (3 times per week, 60 min) led by a specialist physiotherapist, over 8 weeks (23 in total). At the 1st session, the physiotherapist provided participants in both groups with information on basic anatomy and PFM function to facilitate a voluntary PFM contraction. Perineometry used to assist awareness and control of PFM contractions (but unclear if this was part of every session). Participants were instructed to perform the PFMT programme daily at home, and were provided with a home exercise training booklet and an exercise diary. Control (n = 10): women received the same information and demonstration session as described above for those in the supervised group sessions. They then followed the same PFMT programme, performing the same daily home exercises by themselves for an 8‐week period without physiotherapist supervision. |
|
| Outcomes | Measured at baseline (< 6 weeks' postpartum) and at 8 weeks' post‐treatment. Primary endpoint: 8 weeks' post‐treatment. Primary outcome: BFLUTS ‐ quality of life domain. Secondary outcomes: BFLUTS ‐ urinary symptoms domain; PFM strength (blinded perineometry, maximal vaginal squeeze pressure and holding time, mean of 3 trials). |
|
| Notes | Losses to follow‐up at 8 weeks postpartum: PFMT 1/10; control 1/10 (total 10%). These 2 participants were excluded from the data analysis due to "irregular participation in intervention sessions." Funding: no specific grants received from any funding agency. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | "An envelope with two cards was provided to each subject, and on each occasion, they simply drew out just one card without looking at the other." |
| Allocation concealment (selection bias) | High risk | "An envelope with two cards was provided to each subject, and on each occasion, they simply drew out just one card without looking at the other." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. Perineometry was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 10% dropout; similar between groups (numbers and reasons); no mention of imputation for missing data. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 300 nulliparous women at 16‐24 weeks' gestation. Inclusion: nulliparous women at 16‐24 weeks' gestation. Exclusion: multiparity, multiple gestations, severe pregnancy complications, high risk for preterm labour, pain during PFMT, women with diseases that could interfere with participation or women who would be unavailable for follow‐up. Women who performed PFMT before entry to the trial were also excluded. Age, mean, years: PFMT 32; control 31. Parity: all nulliparous. Delivery: PFMT 68% vaginal and of these 6% were instrumental, 32% caesarean; control 71% vaginal and of these 7% were instrumental, 29% caesarean. BMI prior to pregnancy, mean (SD): PFMT 21.78 (4.10); control 22.18 (3.38). Incontinence at recruitment: PFMT 27%; control 30%. Setting: obstetrics clinic at a university hospital, single centre, China. |
|
| Interventions |
PFMT (n = 150): group training (once per week, 45 min, approximately 10 women per group) with a physiotherapist for 12 weeks. Women individually instructed by a physiotherapist about pelvic floor anatomy and how to contract the PFM correctly before exercise. PFMT twice daily at home with exercise diaries to monitor compliance. Control (n = 150): received regular antenatal care and the customary written postpartum instructions that did not include PFMT from the hospital. |
|
| Outcomes | Measured at baseline (16‐24 weeks' gestation), 36 weeks' gestation, and 3 days', 6 weeks' and 6 months' postpartum. Primary outcome: self‐reported UI (unclear which of the questionnaires were used to derive these data). Secondary outcomes: IIQ‐7, UDI‐6, questions about frequency of urination (daily) and UI. |
|
| Notes | Losses to follow‐up: none. Funding: Medical Research Project, Chang Gung Memorial Hospital, Taiwan. Conflicts of interest: none declared. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomly allocated." |
| Allocation concealment (selection bias) | Unclear risk | "Randomisation was achieved by selection of sealed envelopes, which were opened at entry." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported (in an interview setting). |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data available for all 300 participants randomised. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups), quasi‐randomised (alternation) trial. | |
| Participants | 136 pregnant, continent women. Inclusion: able to attend pregnancy outpatient visits regularly, 14‐20 weeks' gestation during 1st attendance, aged 20‐35 years, completed at least elementary school, no UI complaints or UTI, BMI < 40, and no chronic disease (such as asthma) or genitourinary pathology (such as pelvic organ prolapse) requiring treatment. Exclusion: not reported. Age, mean (SD), years: PFMT 26.3 (4.8); control 25.7 (4.4). Parity: not reported. Delivery: not reported. BMI prior to pregnancy: < 20, 16.7%; 20‐24.9: 52.9%; 25‐29.9, 22.6%; 30‐39, 7.8%. Incontinence at recruitment: none. Based on negative 1‐hour pad test, urinary diary and self‐report. Setting: antenatal outpatient clinics of a women's maternity training and research hospital in Ankara, Turkey. |
|
| Interventions |
PFMT (n = 68): home exercise programme during pregnancy and postpartum, 3 sets of 10 exercises, 3 times per day. Women received education about functions of the PFM and PFMT, including the effect of pregnancy and vaginal delivery on incontinence, were taught the PFM exercises, and asked to observe the inward contraction of the perineum during contractions (frequency uncertain). Women completed an exercise diary, were phoned once per month to encourage adherence, and exercise compliance was checked at every hospital visit (9‐10 visits on average). Control (n = 68): not instructed to do PFMT. Once data collection complete, controls received PFMT and a brochure during the 12th week home visit. |
|
| Outcomes | Measured at baseline (unclear but possibly at 14‐20 weeks' gestation), 28 weeks' gestation, 32 weeks' gestation, 12 weeks' postpartum. Primary endpoint: 12 weeks' postpartum. Primary outcome: 1‐hour pad test. Secondary outcome: urinary diary. |
|
| Notes | Losses to follow‐up at 14‐20 weeks' gestation: PFMT 12/68; control 8/68 (total 14.7%). Losses to follow‐up at 28 weeks' gestation: PFMT 16/68; control 14/68 (total 22.1%). Losses to follow‐up at 32 weeks' gestation: PFMT 16/68; control 18/68 (total 25%). Losses to follow‐up at 12 weeks' postpartum: PFMT 16/68; control 18/68 (total 25%). Funding: not reported. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | "The pregnant women who were examined on odd days and even days were assigned to the intervention group and control group, respectively." |
| Allocation concealment (selection bias) | High risk | "The pregnant women who were examined on odd days and even days were assigned to the intervention group and control group, respectively." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | "The women were not informed as to which group they were in. The investigators were not blinded." |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported (urinary diary). Pad test not blinded. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 25% dropout; similar between groups (numbers and reasons); no mention of imputation for missing data. |
| Selective reporting (reporting bias) | High risk | Study did not report the primary outcome of the review (i.e. self‐reported UI). Other outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 150 women, 6 weeks' postpartum. Inclusion: women 6 weeks' postpartum, full‐term pregnancy, free of lochia with good healing following caesarean section or episiotomy. Exclusion: pace‐maker. Age, years: 23‐35. Parity: not reported. Delivery: not reported. BMI: not reported. Incontinence at recruitment: not reported, but women not recruited because of UI. Setting: People's Hospital of Kenli County, China. |
|
| Interventions |
PFMT (n = 80): combined with biofeedback. Biofeedback was used twice per week and PFMT (Kegel exercises) were undertaken 2‐3 times per day for 20‐30 min or 150‐200 contractions (3 sec hold then relax), performed until women were 12 months' postpartum. Not specified if a correct PFM contraction was confirmed, who supervised the programme, or the number and type of contacts with health professional(s). Control (n = 70): standard postpartum information. |
|
| Outcomes | Measured at baseline (6 weeks' postpartum), and 3, 6 and 12 months' postpartum. Primary endpoint: 12 months' postpartum. Primary outcome: self‐reported UI. Other outcomes: PFM tension and intensity (cm of water), PFM contraction time (sec), POP‐Q. |
|
| Notes | Losses to follow‐up not reported. Funding: not reported in translation. Conflicts of interest: not reported in translation. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomized into two groups." |
| Allocation concealment (selection bias) | Unclear risk | "Randomized into two groups." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Not possible for outcome (number with UI) but unclear if self‐report. Not reported if PFM tension and intensity, contraction time and POP‐Q blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Data not reported. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Unclear risk | Information from this study was obtained from a Chinese publication and it is possible some information was lost in translation. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 192 primiparous postpartum women. Inclusion: primiparous, cephalic presentation of baby, natural vaginal delivery at full term. Exclusion: multiparous women, multiple births, genitourinary surgery prior to or during pregnancy, oversized newborn, neuromuscular disease, caesarean section or vaginal surgery. Age, mean (SD), years: PFMT 26.2 (4.1); control 26.4 (4.5). Parity: primiparous. Delivery: all spontaneous vaginal. BMI: not reported. Incontinence at recruitment: not reported. Setting: Yeyang Maternity and Child Health Care, China. |
|
| Interventions |
PFMT (n = 106): 2‐3 times per day, 15‐30 min each set, started after birth and continued for ≥ 10 weeks. Exercises taught by experienced midwives who also supervised the programme (number and type of contacts/visits unclear). Not specified if a correct PFM contraction was confirmed. Control (n = 86): standard postpartum information. Unclear if this included PFMT. |
|
| Outcomes | Measured at 3, 6 and 12 months' postpartum. Primary endpoint: 12 months' postpartum. Primary outcome: "Urinary condition score." Other outcomes: PFM tension and intensity (Oxford score), pad test. |
|
| Notes | Losses to follow‐up not reported. If 1:1 randomisation, differential noted in numbers in intervention compared to control group (approximately 20%). Funding: not reported in translation. Conflicts of interest: not reported in translation. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Randomised into two groups." |
| Allocation concealment (selection bias) | Unclear risk | "Randomised into two groups." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Not possible for outcome (number with UI) but unclear if self‐report. Not reported if pad test, and PFM tension and intensity blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Data not reported. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Unclear risk | Information from this study was obtained from a Chinese publication and it is possible some information was lost in translation. This study did not contribute any data to the forest plots but did provide information on symptom severity. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 107 pregnant nulliparous women (unclear if this was number recruited or number analysed). Inclusion: pregnant nulliparous women at 12‐39 weeks' gestation at enrolment. Exclusion: pregnancy complications (twin gestation, diabetes, preterm labour, haemorrhage from low‐lying placenta), women beginning labour, history of UTIs. Age, mean (SD), years: 29 (4). Not reported by group. Parity: all nulliparous. Delivery: PFMT 30% instrumental; control 16% instrumental. BMI mean (SD): not reported. Incontinence at recruitment: PFMT 28%; control 32%. Setting: multiple clinics in single centre, Switzerland. |
|
| Interventions |
PFMT (n = 51): as part of a PFM rehabilitation programme, taught by a physiotherapist over 6 weeks (12 sessions). Begun at 2 months and ended before 10 months' postpartum. No details of PFMT programme given, but PFMT in clinic was followed by 20 min of biofeedback and 15 min of electrical stimulation. Control (n = 56): no postpartum PFM rehabilitation programme. Received PFMT education at 10 months' postpartum. |
|
| Outcomes | Measured at 10 months' postpartum. Primary endpoint: 10 months' postpartum. Primary outcome: not reported. Outcome measures: self‐reported UI or FI, sexual response, vaginal digital PFM palpation (graded 0‐5), ultrasonography (bladder volume, bladder neck position at rest, on Valsalva, and with voluntary PFM contraction, supine and standing), urodynamics (functional urethral length, maximal urethral closure pressure at stress (cm of water), area of continence at stress, mean value of pressure transmission ratio in central third of functional urethral length), vaginal and anal squeeze pressure. |
|
| Notes | No losses to follow‐up. Funding: Swiss National Fund for Scientific Research. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Assigned" in full publication; "randomly assigned" in abstract. |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI and FI self‐report outcomes because they were participant reported. Not reported if other measures were blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data available for all 107 participants randomised. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 205 nulliparous women. Inclusion: pregnant women with a single fetus, aged 16‐40 years, and gestational age of 18‐24 weeks. Exclusion: pathological conditions prior to pregnancy (heart conditions, diabetes, hypertension, bronchitis, asthma, HIV positive), pathological conditions of the pregnancy (gestational hypertension, gestational diabetes and pre‐eclampsia), contraindications to the practice of physical activity (persistent bleeding, preterm labour, incompetent cervix, acute febrile infection and fetal growth restriction) or indication for elective caesarean (placenta previa, cephalopelvic disproportion). Age, mean (SD), years: PFMT 22.9 (4.6); control 22.9 (5.1). Parity: nulliparous. Delivery: PFMT 57.9% vaginal; control 53.5% vaginal. Significant difference in length of delivery (longer in PFMT group). BMI, mean (SD): PFMT 25.4 (5.0); control 25.2 (5.3). Incontinence at recruitment: UI PFMT 50.4%; control 52.0%. Setting: Women's Integral Health Care Hospital, University of Campinas and 4 municipal primary healthcare centres in Campinas, São Paulo, Brazil. |
|
| Interventions |
PFMT (n = 103): either in groups or on an individual basis (50 min, median 5 (range 2‐10)) depending on the number of women present, supervised by a physiotherapist between 18‐24 weeks' and 36‐38 weeks' gestation. PFMT was additional to the routine activities offered at the antenatal clinic (but held on the same days as these antenatal visits). Each session included non‐aerobic exercises designed to reduce back pain, help venous return, prevent UI and minimise anxiety. Women also received standard antenatal education, and were instructed to perform daily PFMT at home as well as ≥ 30 min of aerobic exercise daily. Instructions provided on performance of correct PFM contraction, but this was not evaluated (due to the pragmatic nature of the study). Women were given an exercise guide (PFMT and general stretching) and asked to complete an exercise diary. Control (n = 102): usual care. Women participated in routine antenatal educational activities and received standard postnatal care and education from trained physiotherapy, nursing and medical staff (on the maternity ward). |
|
| Outcomes | Measured at baseline (18‐24 weeks' gestation), 28‐30 weeks' gestation, and 36‐38 weeks' gestation. Primary endpoint: 36‐38 weeks' gestation. Primary outcome: not reported. Outcomes: State‐Trait Anxiety Inventory, Pregnancy Physical Activity Questionnaire, self‐reported UI, lumbar pain as indicated on a body chart and quantified with a visual analogue scale, neonatal well‐being (Apgar scores in 1st and 5th min and perinatal scores from medical records). |
|
| Notes | Exclusions post‐randomisation: PFMT 6/103; control 2/102 (3.9%). Discontinuation at 28‐30 weeks' gestation: PFMT 3/103; control 1/102 (2%). Discontinuation after delivery: PFMT 19/103; control 29/103 (23.4%); need to check these numbers as flow‐chart appears to be incorrect in paper (Figure 1 of paper). Data on losses to follow‐up (reported on CONSORT flowchart, text and tables) were incongruent. Funding: Foundation for the support of research Sao Paulo and the Co‐ordination for the Improvement of Higher Education Personnel (CAPES). Conflicts of interest: none declared. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomisation was done by opening a sealed, opaque, consecutively numbered envelope containing the information on the group to which the participant was being allocated in accordance with a previously prepared, computer‐generated random sequence of numbers. The randomisation was 1:1, and the process and preparation of the envelopes containing the information were carried out by a person who was not directly involved with the study." |
| Allocation concealment (selection bias) | Low risk | "Randomisation was done by opening a sealed, opaque, consecutively numbered envelope containing the information on the group to which the participant was being allocated in accordance with a previously prepared, computer‐generated random sequence of numbers. The randomisation was 1:1, and the process and preparation of the envelopes containing the information were carried out by a person who was not directly involved with the study." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | "The study was not blinded to the evaluators." |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 27% dropout; slight differential loss (PFMT 24%; control 30%); similar reasons; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Unclear risk | Data on losses to follow‐up (reported on CONSORT flowchart, in the text and tables) were incongruent. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 301 pregnant nulliparous women. Inclusion: 18 weeks' gestation, aged ≥ 18 years, single live fetus at 18‐week ultrasound. Exclusion: pregnancy complications, high risk for preterm labour, pain during voluntary PFM contraction, ongoing UTI, diseases that could interfere with participation, lived too far from centre to attend weekly class. Age, mean (SD), years: PFMT 28 (5); control 27 (4). Parity: all nulliparous. Delivery: PFMT 74.3% vaginal, 17.6% instrumental, 8.1% caesarean; control 69.9% vaginal, 20.9% instrumental, 9.2% caesarean. BMI prior to pregnancy, mean (SD): PFMT 23 (3); control 23 (4). Incontinence at recruitment: PFMT 32%; control 31%. Setting: single centre, Norway. |
|
| Interventions |
PFMT (n = 148): supervised group exercise class (once per week, 60 min, 10‐15 women), led by a physiotherapist over a 12‐week period (from 20‐26 weeks' gestation). Class included a progressive PFMT programme (based on Bø 1999), and body awareness, breathing, relaxation and strength training for abdominal, back and thigh muscles. Women received individual instruction in pelvic floor anatomy and how to perform a correct PFM contraction from a physiotherapist, confirmed by digital vaginal palpation and observation of the perineum. Women were instructed to perform daily PFMT at home (2 sets of 8‐12 contractions), and were given exercise diaries to complete. Control (n = 153): customary information given by midwife or general practitioner. Women received individual instruction in pelvic floor anatomy and how to perform a correct PFM contraction from a physiotherapist, confirmed by digital vaginal palpation and observation of the perineum. Not discouraged from doing PFMT on their own. |
|
| Outcomes | Measured at 36 weeks' gestation and 3 months' postpartum. Primary endpoint: 3 months' postpartum. Primary outcome: self‐reported UI. Secondary outcomes: leakage episodes (3‐day urinary diary), change in leakage (Likert scale), vaginal digital palpation, vaginal squeeze pressure. |
|
| Notes | Losses to follow‐up at 3 months' postpartum: PFMT 5/148; control 7/153 (total 4%). Funding: Norwegian Fund for Postgraduate Training in Physiotherapy and the Norwegian Women's Public Health Association. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomisation was done in blocks of a maximum of 32 with the use of opaque, sealed envelopes. The envelopes were mixed thoroughly before they were stored in a larger envelope. Each participant drew and opened one envelope herself and was enrolled by the secretary in the secretary's office." |
| Allocation concealment (selection bias) | Low risk | "Randomisation was done in blocks of a maximum of 32 with the use of opaque, sealed envelopes. The professional staff involved in the training groups or the outcome assessments had no access to the randomisation procedure. A secretary with no other involvement in the trial prepared the envelopes." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. "The women were asked not to reveal any information about group allocation to the principal investigator doing the assessments." |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. Perineometry was blinded. "The principal assessor was not involved in the training of the women and was blinded to group allocation while making the assessments and plotting data." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 4.0% dropout; no differential; reasons provided, but not for each group; imputation for missing data (for the principal analysis the "missing last values were carried forward by their baseline values"). |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) block RCT. | |
| Participants | 120 postpartum women. Inclusion: primiparous, fluent in English, sustained a primary third‐degree tear during delivery (that was repaired immediately). Exclusion: women with an infant in the special care unit, a history of alcohol or illicit drug abuse, a positive viral status (hepatitis virus, HIV) and not fluent in English. Age, mean (SD), years: not reported. Parity: primiparous. Delivery: PFMT 60% spontaneous vaginal, 40%, assisted vaginal; control 63% spontaneous vaginal, 37% assisted vaginal. BMI, mean (SD): not reported. Incontinence at recruitment: not reported. Setting: labour ward and perineal clinic, National Maternity Hospital, Dublin. |
|
| Interventions |
PFMT plus biofeedback (n = 30): 2 sessions per day, 3 months' duration. Biofeedback training was undertaken in the perineal clinic and was delivered by either a specialist obstetrician, a specialist nurse, or a combination of both; no written information was provided. PFMT education was provided by senior midwives or physiotherapists on the postnatal ward and written information was provided, with women to perform standard Kegel exercises for 5 min. There was no mention of checking for a correct pelvic floor contraction and once given the programme it appeared that no further contact was made until the 3‐month follow‐up. Women were given an exercise diary to complete. PFMT alone (n = 90): women were educated on the ward before discharge, by senior midwives or physiotherapists. Written instructions were provided with women to perform standard Kegel exercises for 5 min, 2 sessions per day. |
|
| Outcomes | Measured at 3 months' postpartum (no baseline measures). Primary endpoint: 3 months' postpartum. Primary outcome: not reported. Outcomes: Cleveland Clinic continence score, Rockwood FI quality of life scale, manometry (mmHg), endoanal ultrasound. |
|
| Notes | No losses to follow‐up. Note block randomisation 1:3 (PFMT plus biofeedback 30, PFMT 90). Funding: Health Research Board of Ireland. Conflicts of interest: none declared. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Computer randomisation programme" (note randomisation in a ratio of 1:3). |
| Allocation concealment (selection bias) | Low risk | "Sealed, opaque envelopes." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of FI self‐report outcomes because they were participant reported. Unclear if manometry or ultrasound blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 169 pregnant primiparous women. Inclusion: healthy primiparous pregnant with singleton fetus, 10‐14 weeks' gestation, no UI, able to communicate in Spanish and able to provide informed written consent. Exclusion: planning not to give birth in Fuenlabrada University Hospital, and any contraindication according to the American College of Obstetricians and Gynecologists guidelines. Age, mean (SD), years: PFMT 29.9 (3.3); control 29.1 (4.5). Parity: primiparous. Delivery: not applicable as primary endpoint was during pregnancy. BMI prior to pregnancy, mean (SD): PFMT 23.6 (4.3); control 22.7 (3.8). Incontinence at recruitment: none (see inclusion criteria). Setting: Gynecology and Obstetrics Service of Fuenlabrada University Hospital, Madrid, Spain. |
|
| Interventions |
PFMT (n = 73): supervised exercise class (3 times per week, 60 min, 8‐12 women) designed and led by a physical activity and sport sciences graduate, at least 22 weeks' duration (about 70‐78 sessions in total). Class included a progressive PFMT programme (approximately 10 min of each session), low impact aerobics including general strength training, and stretching, relaxation and massage. All women received standard education and information on PFM anatomy and function, but a correct PFM contraction was not verified. Women were encouraged to perform 100 PFM contractions distributed in different sets every day (unclear if this was in reference to a home programme). Control (n = 96): usual care, which included follow‐up by midwifes including information about PFMT. Women were not asked not to do PFMT. |
|
| Outcomes | Measured at 36‐40 weeks' gestation. Primary endpoint: end treatment (36‐40 weeks' gestation). Primary outcomes: self‐reported UI and UI severity (measured with ICIQ‐SF). Secondary outcome: none. |
|
| Notes | Losses to follow‐up: PFMT 10/73; control 7/96 (total 10%). Funding: not reported. Conflicts of interest: none declared. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "A statistical randomisation computer programme was used." |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | "Non‐blinded design." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 10% dropout; slight differential loss (PFMT 13.7%; control 7.3%); similar reasons; no mention of imputation for missing data. Note uneven group size (PFMT 73, control 96). |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Unclear risk | Unclear how the randomisation process resulted in uneven group sizes (PFMT 73; control 96). This could possibly be due to immediate losses post‐randomisation from the PFMT group. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 268 primigravid women. Inclusion: 20 weeks' gestation, bladder neck hypermobility (> 5 mm linear movement following standardised Valsalva) on perineal ultrasound. Exclusion: pre‐pregnancy UI, neurological disorder. Age, median (range), years: PFMT 27 (17‐42); control 29 (16‐47). Parity: all primigravid. Delivery: PFMT 66.1% vaginal, 17.8% instrumental, 16.1% caesarean; control 65.5% vaginal, 21.8% instrumental, 12.7% caesarean. BMI, mean (SD): PFMT 25 (4); control 24 (4). Incontinence at recruitment: none. Setting: single centre, UK. |
|
| Interventions |
PFMT (n = 139): 1‐to‐1 monthly sessions with a physiotherapist, between 20 weeks' gestation and delivery. Progressive PFMT programme (based on that of Bø 1995) that included daily PFMT at home (2 sets of exercises) with women asked to complete an exercise diary. Women unable to follow PFMT protocol due to inability to contract the PFM had an individualised programme until they were able to follow the study regimen. Control (n = 129): likely to have received verbal advice on PFMT from midwives at antenatal classes. Probably monthly clinic visits for measurement of bladder neck mobility and vaginal squeeze pressure (perineometry). |
|
| Outcomes | At approximately 20 weeks' and 34 weeks' gestation, and 3 months' postpartum. PFM strength measured monthly from 20 weeks' gestation. Primary endpoint: 3 months' postpartum. Primary outcome: self‐reported UI. Secondary outcomes: 1‐hour ICS pad test at home, PFM strength (perineometry), bladder neck mobility with perineal US, joint hypermobility, striae (graded 1‐3), SF‐36, King's Health Questionnaire. |
|
| Notes | Losses to follow‐up at 3 months' postpartum: PFMT 19/139; control 19/129 (total 14.2% for primary outcome). Funding: Wellbeing. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Simple randomisation was used, from pseudo‐random numbers generated by computer." |
| Allocation concealment (selection bias) | Low risk | "Because women in the pelvic floor exercise group had to be referred to the physiotherapist, the allocation schedule was held by the study coordinator. The physiotherapist operated from separate premises." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. Pad test not blinded; perineometry and assessment of bladder neck mobility were blinded. "The observers carrying out the assessments of pelvic floor strength, bladder neck mobility and reported symptoms were blind to the allocation." |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 14.2% dropout; similar between groups; reasons provided, but not for each group; no mention of imputation for missing data. "101 withdrew from the study before completion: because of time and travel to the hospital, dislike of perineometry and ultrasound. Some women stayed in the study but refused perineometry. Analyses based on 230 women where there is info about main outcome." |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 72 primigravid women. Inclusion: 20 weeks' gestation, no history of genitourinary pathology, plan to remain in region for 12 months' postpartum, ability to read and understand English. Exclusion: history of genitourinary pathology (including severe incontinence) or neuromuscular pathology. Age, mean (SD), years: PFMT 28 (6); control 26 (5). Parity: all primigravid. Delivery: of the 46 with UI, 37 vaginal and 9 caesarean. Not reported by group. BMI: not reported. Incontinence at recruitment: PFMT 23%; control 21%. Setting: single centre, US. |
|
| Interventions |
PFMT (n = 34): standardised instruction in PFMT which included 30 maximal or near maximal voluntary PFM contractions per day; for up to 17 months. Control (n = 38): usual care with no systematic PFMT programme. |
|
| Outcomes | Measured at 35 weeks' gestation, 6 weeks' postpartum, and 6 and 12 months' postpartum. Primary endpoint: 12 months' postpartum. Primary outcome: not reported. Outcomes: best of 2 maximal voluntary PFM contractions measured using instrumented speculum (Newtons), severity of incontinence (mean score from questionnaire where 0 = none, 1 = damp, 2 = wet and 3 = soaked with gentle cough, hard cough, sneeze and laugh), self‐reported adherence. |
|
| Notes | Losses to follow‐up at 12 months' postpartum: PFMT 12/34; control 14/38 (total 36.1%). Funding: National Institutes of Health grants (R29‐NRO1950 and RO1‐NRO‐4007). Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Group allocation was by random assignment using a computer generated random numbers table." |
| Allocation concealment (selection bias) | Low risk | "Group assignment was conducted by a clerical member of the project staff." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. PFM strength blinded. "Investigator was blinded to participant group status... through the use of a second individual not involved in assessment of UI symptoms or muscle strength." |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 36.1% dropout; similar between groups; no reasons; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Unclear risk | Women who had a caesarean section were excluded from the analysis of PFM strength. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 70 pregnant primiparous women. Inclusion: primiparous, aged ≥ 18 years, 20‐30 weeks' gestation, singleton fetus and prepregnancy BMI < 30. Exclusion: stress UI during pregnancy, complications such as preterm labour, pregnancy‐induced hypertension, gestational diabetes mellitus, antenatal haemorrhage, pain during PFM contraction or diseases that could interfere with the participant. Age, mean (SD), years: PFMT 27.6 (SD 5.1); control 28.2 (5.0). Parity: primiparous. Delivery: not applicable as primary endpoint was during pregnancy. BMI prior to pregnancy, mean (SD): PFMT 21.7 (1.9); control 22.0 (1.9). Incontinence at recruitment: none. Setting: antenatal clinic, Department of Obstetrics and Gynecological Nursing, Srinakharinwirot University, Thailand (July‐October 2012). |
|
| Interventions |
PFMT (n = 35): supervised group PFMT programme (45 min, held once every 2 weeks, 4‐5 women) led by a midwife, 6 weeks' duration (a total of 3 sessions). All women received antenatal education about PFM function, PFM strengthening and how to perform PFM exercises. The ability to contract the PFM was assessed using the "stop test" (stop or slow urinary flow for 1‐2 sec). Women were instructed to perform 20 sets of exercises twice per day at home, at least 5 days per week, and were provided with a 25‐page PFMT handbook and a urinary dairy. Control (n = 35): usual antenatal care from health professionals, obstetricians or midwives (who were not involved in the study). Received information on diet, sleep, breastfeeding and antenatal exercise for the benefit of preparing for childbirth and were instructed in the "stop test." They did not receive information about stress UI during pregnancy and had no training to support the performance of correct PFMT. |
|
| Outcomes | Measured at baseline (20‐30 weeks' gestation) and 38 weeks' gestation. Primary endpoint: 38 weeks' gestation. Primary outcome: self‐reported UI (defined as involuntary leakage of urine on sneezing, coughing, effort or physical exertion, ≥ 1 times per week). Secondary outcomes: severity of UI comprised of frequency, volume of urine leakage (minimal = a few drops, moderate = wetting underwear, large = sufficient to dampen outer clothing) and perceived severity (visual analogue scale, 0‐10). |
|
| Notes | Losses to follow‐up at 38 weeks' gestation: PFMT 2/35; control 5/35 (total 10%). Funding: Supported by Faculty of Nursing, Srinakharinwirot University, Thailand. Conflicts of interest: none declared. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer generated, random numbers. |
| Allocation concealment (selection bias) | Low risk | Sealed, opaque envelopes. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 10% dropout; slight differential loss (PFMT 5.7%: control 14.3%); similar reasons; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | Unspecified number of women with antenatal UI, 705 women consented and interviewed. Inclusion: none reported in addition to above. Exclusion: none reported. Age: not reported. Delivery: not reported. BMI: not reported. Parity: not reported. Setting: single centre, Canada. |
|
| Interventions |
PFMT (n = ?): teaching about PFMT. No further details given. Control (n = ?): handout information about PFMT. |
|
| Outcomes | Measured at 1, 6 and 12 months' postpartum. Primary endpoint: not reported. Primary outcome: self‐reported UI. Secondary outcome: not reported. |
|
| Notes | Losses to follow‐up not reported. Funding: not reported. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported. |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI and FI self‐report outcomes because they were participant reported. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Not reported. |
| Selective reporting (reporting bias) | Unclear risk | Difficult to assess. Outcomes not clearly specified in text and probable that not all have been reported. |
| Other bias | Unclear risk | Reported in a conference abstract with limited information about study methods and results. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 1800 women recruited from postnatal wards. Inclusion: within 24 hours of delivery, vaginal delivery. Exclusion: stillbirth or seriously ill baby. Age, mean (SD), years: PFMT 27.1 (5.3); control 26.2 (5.3). Parity: primiparous, PFMT 49%; control 50%. Delivery: PFMT 83.6% vaginal, 16.4% instrumental; control 80.3% vaginal, 19.7% instrumental. BMI: not reported. Antenatal incontinence: PFMT 32%; control 29%. Setting: single centre, UK. |
|
| Interventions |
PFMT (n = 900): 1 individual session daily with midwife co‐ordinator while in hospital. 4‐week health diary including section recommending specific exercise each week that integrated voluntary PFM contraction with activities of daily living (also used to assess adherence). No further details of PFMT programme. Control (n = 900): usual antenatal and postnatal care that included instruction in PFMT at antenatal class and by obstetric physiotherapist in postnatal classes on the ward. PFMT instruction included awareness, voluntary PFM contraction as often as remembered, and mid‐stream urine stop. 4‐week health diary without additional section on PFMT. |
|
| Outcomes | Measured at 3 and 12 months' postpartum. Primary endpoint: 3 months' postpartum. Primary outcome: not reported. Outcomes: postal questionnaire to assess self‐reported UI and FI, frequency of leakage, perineal pain and severity of pain, time to resume sexual intercourse, dyspareunia, general well‐being, "use of PFM exercises." |
|
| Notes | Losses to follow‐up at 3 months' postpartum: PFMT 81/900; control 108/900 (total 11%). Funding: Oxford Region Health Authority. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Allocated at random." |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. "Community staff able to recognise women in intensive exercise group by possession of diary." |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI and FI self‐report outcomes because they were participant reported. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 10.6% dropout; similar between groups; no reasons; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Unclear risk | Unclear if the 2 groups were comparable at baseline in terms of undertaking regular PFMT during the last 6 months of pregnancy (PFMT 56.6%; control 45.6%) and UI during pregnancy (PFMT 32.0%; control 28.6%). |
| Methods | 2‐arm (parallel groups), 2‐centre RCT. | |
| Participants | 855 pregnant women at 18 weeks' gestation. Inclusion: aged ≥ 18 years, singleton live foetus. Exclusion: high‐risk pregnancy or diseases that could interfere with participation (or both), women who lived too far from the hospitals to attend weekly training groups (judged as more than 30‐min drive). Age, mean (SD), years: PFMT 30.5 (4.4); control 30.4 (4.3). Parity: nulliparous, PFMT 57.5%; control 56.1%. Delivery: not applicable as primary endpoint was during pregnancy. BMI, mean (SD): PFMT 24.7 (3.0); control 25.0 (3.4). Incontinence at recruitment: UI PFMT 40.1%; control 42.2%. FI PFMT 5.2%; control 4.0%. Flatal incontinence PFMT 27.5%; control 26.1%. Setting: 2 centres in Norway. Trondheim University Hospital (St. Olavs Hospital) and Stavanger University Hospital. |
|
| Interventions |
PFMT (n = 429): supervised group exercise class (once per week, 8‐15 women, 60 min), led by a physiotherapist over a 12‐week period. Class included a progressive PFMT programme that was included in a 20‐ to 25‐min block of strengthening exercises (in addition to 30‐35 min low‐impact aerobics and 5‐10 min of stretching). All women received written information on PFMT, individual instruction in PFM anatomy and how to perform a correct PFM contraction (confirmed by vaginal palpation) by a physiotherapist. Also encouraged to perform PFMT at home at least twice per week as part of a 45‐min home programme (written instructions provided) and complete an exercise diary. Control (n = 426): usual care including standard antenatal care and information provided by midwife or general practitioner. Women were not discouraged from doing PFMT. All women received the same written information and recommendations on PFMT as the intervention group, including detailed information about the pelvic floor and an evidence‐based PFMT programme. |
|
| Outcomes | Measured at baseline (18‐22 weeks' gestation) and end of treatment (32‐36 weeks' gestation). Primary endpoint: end of treatment (32‐36 weeks' gestation). Primary outcome: self‐reported UI and anal incontinence via a questionnaire that included Sandvik's severity index (UI) and St. Marks score (anal incontinence). Urinary leakage subclassified as UI, stress UI and urge UI with severity categorised as "urinary leakage < once per week" or "urinary leakage equal to or greater than once per week" (severe UI). Anal incontinence categorised into FI and flatal incontinence. Secondary outcomes: frequency, intensity and type of physical activity (including PFMT), training diary (intervention group only). Labour and delivery outcomes (Salvesen and colleagues 2014; see Stafne 2012). |
|
| Notes | Losses to follow‐up during pregnancy: PFMT 33/429; control 61/426 (total 11%). Funding: Norwegian Fund for Postgraduate Training in Physiotherapy and the Liaison Committee for Central Norway Health Authority, and the Norwegian University of Science and Technology. Conflicts of interest: none declared. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Concealed randomisation in blocks of 30 was performed at the Unit for Applied Clinical Research, Norwegian University of Technology and Science, by a web‐based computerised procedure. The staff involved with training or outcome assessments had no influence on the randomisation procedure." |
| Allocation concealment (selection bias) | Low risk | "Concealed randomisation in blocks of 30 was performed at the Unit for Applied Clinical Research, Norwegian University of Technology and Science, by a web‐based computerised procedure. The staff involved with training or outcome assessments had no influence on the randomisation procedure." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of anal incontinence and UI self‐report outcomes because they were participant reported. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 11% dropout; slight differential loss (PFMT 8%; control 14%); similar reasons; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias noted. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 86 pregnant women (unclear if this was number recruited, or number analysed). Inclusion: no further criteria reported. Exclusion: multiple birth, pre‐existing incontinence, medical conditions preventing exercise regimes during pregnancy. Age: range 24‐42 years. Parity: not reported. Delivery: 73.3% vaginal, 26.7% caesarean; not reported per group. BMI: not reported. Pre‐existing incontinence: none. Setting: single centre, Canada. |
|
| Interventions |
PFMT (n = 43): seen twice per month during pregnancy and every 3 months' postpartum for 1 year (possibly by a physiotherapist, but not explicitly stated). No further details given. Control (n = 43): same number of contacts. Treatment described as "other (placebo) including no pelvic floor exercises." |
|
| Outcomes | Measured at 6 and 12 months' postpartum. Primary endpoint: 6 months' postpartum. Primary outcome: mean urine loss on stress test with standardised bladder volume. Secondary outcome: not reported. |
|
| Notes | No losses to follow‐up for primary outcome. Adverse events: 2/43 women withdrew from PFMT due to pelvic floor pain. Funding: not reported. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not reported. |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. "The statistician and medical staff assessing questionnaires and assisting with pad testing were blinded to treatment assignment." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | UI self‐report data available for all 107 participants randomised. |
| Selective reporting (reporting bias) | Unclear risk | Difficult to assess. 1 prespecified outcome from methods reported, but possible other outcomes have not been. |
| Other bias | Unclear risk | Reported in a conference abstract with limited information about study methods and results. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 148 postpartum women. Inclusion: delivery via natural birth. Exclusion: multiple births, history of genitourinary disease prior to or during pregnancy, neuromuscular disease, caesarean section or vaginal surgery. Age, years: range 21‐35 in both groups. Parity: primiparous. Delivery: natural vaginal. BMI: not reported. Incontinence at recruitment: not reported. Setting: 1 hospital, China. |
|
| Interventions |
PFMT (n = 75): twice per day, 15‐30 min each set (anal contraction for at least 3 sec hold when inhaling, followed by relaxation with 3‐5 faster contractions at the end of each time), for > 6‐8 weeks. Exercises taught by experienced midwives but it was unclear who supervised the programme or the number and type of contacts/visits. An obstetrician assessed participants PFM strength and contraction (no further details provided). Control (n = 73): no details provided other than "conventional guidance." |
|
| Outcomes | Measured immediately following childbirth and at 6 and 12 months' postpartum. Primary endpoint: unclear. Primary outcome: not reported. Outcomes: stress UI (criteria of ICS, 0‐5), pad test (UI defined as > 2 g), PFM strength (Oxford scale). |
|
| Notes | Losses to follow‐up not reported. Funding: not reported in translation. Conflicts of interest: not reported in translation. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "Patients were randomised into two groups." |
| Allocation concealment (selection bias) | Unclear risk | "Patients were randomised into two groups." |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. Unclear if pad test and PFM strength blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Data not reported. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Unclear risk | Information from this study was obtained from a Chinese publication and it is possible some information was lost in translation. |
| Methods | 2‐arm (parallel groups) RCT (note: usual care vs individual treatment; the individual treatment group was further randomised into 3, producing 4 comparison groups in total). Stratified by parity (1‐3, ≥ 4), number of leakage episodes (< 1 per day, ≥ 1 per day), and type of delivery (vaginal, caesarean). |
|
| Participants | 230 women with UI symptoms, 3 months' postpartum. Inclusion: none reported in addition to above. Exclusion: none reported. Age, mean (95% CI), years: PFMT 29 (28.8‐29.2); control 27.8 (27.0‐28.7). Parity: primiparous, PFMT 28%; control 33%. Delivery: PFMT 82% vaginal (50% perineal trauma), 18% caesarean; control 83% (56% perineal trauma) vaginal, 17% caesarean. BMI: not reported. < 1 leakage episode per day: PFMT 89%; control 89%. Setting: single centre, New Zealand. |
|
| Interventions |
PFMT (n = 113): individual treatment: further randomised into (a) individualised PFMT (39 women), (b) individualised PFMT with vaginal cones (38 women) and (c) vaginal cones (36 women). In group (a) the PFMT comprised individual instruction by physiotherapist at 3, 4, 6 and 9 months' postpartum with use of perineometer at each visit for biofeedback. Women were to aim for 80‐100 voluntary PFM contractions daily, for up to 9 months. Control (n = 117): usual care comprising PFMT as taught by physiotherapists in antenatal classes (1 occasion) or daily classes on the postnatal wards (or audiotape at the weekend). |
|
| Outcomes | Measured at 12 months' postpartum. Primary endpoint: 12 months' postpartum. Primary outcome: not reported. Outcomes: postal questionnaire that included UI and FI, frequency of incontinence, frequency and amount of PFMT, general well‐being and sexual satisfaction. PFM strength (perineometry, mean of 3 maximal contractions) and home pad test. |
|
| Notes | Losses to follow‐up at 12 months: PFMT 59/113 (PFMT 20/38, PFMT with cones 24/38, cones 15/36); control 26/117 (total 37%). Funding: Health Research Council of New Zealand. Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Assignment was by means of a computer programme that used files stored in computer‐readable form to produce the next assignment. The assignment was stratified by parity (1‐3, or 4 or more). Number of incontinence episodes and type of delivery, and was blocked to produce even numbers after every 6 subjects in each of the strata." |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI and FI self‐report outcomes because they were participant reported; pad test unblinded; perineometry blinded. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 37.0% dropout; differential loss (PFMT 52.2%; control 22.2%); similar reasons but different proportions; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias were noted. |
| Methods | 2‐arm (parallel groups) RCT. | |
| Participants | 264 pregnant women. Inclusion: already affected by UI (≥ 2 leakage episodes in the last month). Exclusion: already receiving treatment for UI, comorbidity (type(s) not reported), insufficient knowledge of Dutch language. Age, mean (95% CI), years: PFMT 31.9 (31.1‐32.7); 32.6 (32.0‐33.3). Parity: nulliparous, PFMT 38%; control 34%. Delivery: ≥ 55.3% had vaginal births, exact data not reported. BMI, mean (95% CI): PFMT 24.0 (23.2‐24.8); control 23.5 (22.9‐24.1). UI before pregnancy: PFMT 53%; control 52%. Setting: multiple centres, the Netherlands. |
|
| Interventions |
PFMT (n = 112): taught by physiotherapists specialised in PFMT (using a treatment manual prepared for the study in accordance with guidelines from the Dutch Society of Physiotherapists). 4 × 30‐min visits with 3 between 23 and 30 weeks' gestation, and 1 × 6 weeks' postpartum. Included observation and palpation of perineal body with voluntary PFM contraction, information to raise awareness of PFM and encourage PFMT, self‐palpation encouraged. Also 40‐page handbook with information about incontinence, PFM function, detailed instructions on PFMT. No further details of PFMT. Control (n = 152): routine care for pregnant women. Nearly two‐thirds received some instruction on PFMT. |
|
| Outcomes | Measured at 35 weeks, 8 weeks' postpartum, 6 months' postpartum, and 12 months' postpartum. Primary endpoint: 12 months' postpartum. Primary outcome: severity of UI (combination of severity of urine loss from 7‐day bladder diary and score from PRAFAB questionnaire). Secondary outcome: IIQ. |
|
| Notes | Losses to follow‐up at 35 weeks: PFMT 19/112; control 21/152 (total 15%). Losses to follow‐up at 8 weeks' postpartum: PFMT 25/112; control 27/152 (total 20%). Losses to follow‐up at 6 months' postpartum: PFMT 33/112; control 44/152 (total 29%). Losses to follow‐up at 12 months' postpartum: PFMT 47/112; control 53/152 (total 38%). Funding: Netherlands Organisation for Health Research and Development (Zon‐MW Nr 2200.0052). Conflicts of interest: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Allocated to an intervention or control group by computerised randomisation." |
| Allocation concealment (selection bias) | Unclear risk | Not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Not feasible. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Unblinded reporting of UI self‐report outcomes because they were participant reported. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 37.9% dropout; slight differential loss (PFMT 42.0%; control 34.9%); similar reasons; no mention of imputation for missing data. |
| Selective reporting (reporting bias) | Low risk | Outcome measures described in methods were reported in results. |
| Other bias | Low risk | No other sources of bias were noted. |
BFLUTS: British Female Lower Urinary Tract Symptoms questionnaire; BMI: body mass index (kg/m²); CI: confidence interval; FI: faecal incontinence; ICIQ: International Consultation on Incontinence; ICIQ FLUTS: International Consultation on Incontinence‐Female Lower Urinary Tract Symptoms; ICIQ‐SF: International Consultation on Incontinence Questionnaire‐Short Form; ICS: International Continence Society; IIQ‐7: Incontinence Impact Questionnaire; IQR: interquartile range; min: minute; n: number of women; POP‐Q: Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire; PFM: pelvic floor muscle; PFMT: pelvic floor muscle training; PISQ‐12: Urinary Incontinence Sexual Questionnaire; POP‐Q: pelvic organ prolapse quantified; RCT: randomised controlled trial; SD: standard deviation; sec: second; SF‐36: 36‐item Short Form; SIFCRAT: Sandwell Incontinence Following Childbirth Risk Assessment Tool; UDI‐6: Urogenital Distress Index‐Short Form; UI: urinary incontinence; UTI: urinary tract infection.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Agur 2005 | RCT. Pregnant women. Usual care vs PFMT. Excluded because did not collect data on UI or FI; primary outcome of interest was duration of 2nd‐stage labour. |
| Assis 2013 | Quasi‐RCT. Postpartum, multiparous women. PFMT vs unspecified control. Excluded because UI or FI were not an outcome; assessed PFM function. |
| Barakat 2014 | RCT. Pregnant women. PFMT (in an exercise group) vs usual care. Excluded because it did not collect data on UI or FI; outcomes were maternal and fetal parameters. |
| Barakat 2016 | RCT. Healthy, pregnant women. PFMT (as part of an exercise group) vs usual care. Excluded because did not collect data on UI or FI; primary outcome was hypertension during pregnancy. |
| Culligan 2005 | RCT. Primigravid women. Sham vs active extracorporeal magnetic innervation after delivery; both groups did PFMT during pregnancy. Excluded because comparison of sham and active stimulation. |
| Dannecker 2004 | RCT. Primigravidae, pregnant women. PFMT with Epi‐No device vs no device. Excluded because the primary purpose of the study was to reduce perianal trauma. In addition, the maximum 3‐ to 4‐week duration of the intervention was deemed insufficient to change PFM strength (see also Dietz 2014). |
| Dias 2011 | RCT. Nulliparous pregnant women at 20 weeks' gestation. PFMT (in an exercise group and home exercises) vs control (no instruction on PFMT). Excluded because it did not collect data on UI or FI; assessed labour and newborn outcomes, including PFM strength. |
| Dietz 2014 | RCT. Primigravidae, pregnant women. Epi‐No vs unspecified control. Excluded because the Epi‐No device is designed to stretch the vagina and perineum, unclear if PFMT was part of the protocol (see Dannecker 2004), and did not collect data on UI or FI; outcome was levator avulsion. |
| Domingues 2015 | RCT (ongoing study). Pregnant women. PFMT (in an exercise group) vs no intervention. Excluded because UI or FI not stated as an outcome measure in trial protocol; assessment of preterm birth and pre‐eclampsia alongside other maternal and newborn measures. |
| Dougherty 1989 | RCT. Postnatal women within 6‐11 weeks of vaginal delivery. PFMT with intravaginal balloon device vs no treatment. Excluded because did not collect data on UI or FI. |
| Fynes 1999 | RCT. Postnatal women with FI following obstetric trauma. Sensory feedback vs audiovisual feedback (including electrical stimulation); both groups did PFMT. Excluded because comparison of 2 types of feedback. |
| Golmakani 2015 | RCT. Primiparous, postpartum women. PFMT vs usual care that included written instructions on PFMT. Excluded because did not collect data on UI or FI; outcomes were sexual self‐efficacy and PFM strength. |
| Gouldthorpe 2003 | RCT. Primiparous women. Abdominal muscle exercise vs no abdominal exercise. Excluded because not PFMT. |
| Hou 2010 | RCT. Postpartum women. PFMT with vaginal dumbbell and electrical stimulation vs PFMT with vaginal dumbbell. Excluded because no measure of UI or FI; outcome was PFM strength. |
| Huang 2014 | RCT. Primiparous women. PFMT vs control ("traditional nursing"). Excluded because did not collect data on UI or FI; assessed labour outcomes and PFM strength. |
| Kamisan Atan 2016 | RCT. Nulliparous, pregnant women. Epi‐No vs usual care. Excluded because the Epi‐No device is designed to stretch the vagina and perineum, unclear if PFMT was part of the protocol (see Dannecker 2004), and did not collect data on UI or FI; main outcomes were levator ani, anal sphincter and perineal trauma. |
| Lekskulchai 2014 | RCT. Nulliparous pregnant women (5‐12 weeks' pregnancy). PFMT vs non‐PFMT (routine antenatal care). Excluded because outcome of study was bladder neck descent on perineal ultrasound, no incontinence outcomes. |
| Li 2010 | RCT (no information provided about random sequence generation). Primiparous, pregnant women. PFMT vs no PFMT. Excluded as did not collect data on UI or FI; assessed labour outcomes and PFM strength. |
| Liu 2013 | RCT. Primigravidae, pregnant women. PFMT vs usual care. Excluded because no measure of UI or FI; outcome was PFM strength. |
| Mahmoodi 2014 | RCT. Primiparous, postnatal women. PFMT vs usual care. Excluded because did not collect data on UI or FI UI; outcome was postepisiotomy pain. |
| Mahony 2004 | RCT. Postnatal women with FI. Biofeedback vs biofeedback augmented with stimulation; both groups did PFMT. Excluded because comparison of 2 types of feedback. |
| Mason 1999 | RCT. Primiparous women recruited from postnatal wards. Conventional vs intensive physiotherapy. Excluded because cannot find any trial report (only record of trial on Medical Research Council trials database) and no response to letter to primary author. |
| Mason 2010 | RCT. Nulliparous, singleton pregnancy, no previous stress UI, 11‐14 weeks' pregnancy. PFMT vs usual care and instruction in PFMT. Excluded because there were internal inconsistencies in the data and the accuracy of the numbers was in doubt. |
| Morin 2015 | RCT. Primiparous, postnatal women with avulsion injury. PFMT vs usual care (plus a control arm of women without avulsion who received physiotherapy). Excluded because did not collect data on UI or FI; outcome was PFM morphometry. |
| NCT01696201 | RCT (ClinicalTrials.gov Identifier: NCT01696201; recruitment status unknown). Pregnant women. PFMT (as part of an exercise group) vs no intervention. Excluded because UI or FI not stated as an outcome measure; assessment of depression and other maternal and fetal measures. |
| NCT01723293 | RCT (ClinicalTrials.gov Identifier: NCT01723293; recruitment status unknown). Pregnant women. PFMT (as part of an exercise group) vs no intervention. Excluded because UI or FI not stated as an outcome measure; assessment of fetal heart rate and birth rate and type of delivery. |
| NCT01753622 | RCT (ClinicalTrials.gov Identifier: NCT01753622; recruitment status unknown). Pregnant women. PFMT (as part of an exercise group) vs no intervention. Excluded because UI or FI not stated as an outcome measure; assessment of depression, maternal weight gain and other maternal and fetal measures. |
| Nielsen 1988 | RCT. Primiparous women. PFMT vs no PFMT. Excluded because did not collect data on UI or FI. |
| Norton 1990 | RCT. Primiparous women 6 weeks' postnatal. PFMT vs vaginal cones vs controls. Excluded because did not collect data on UI or FI. |
| Oblasser 2016 | RCT. Postpartum women. Licensed PFMT vaginal ball vs usual care that included written PFMT exercises. Excluded as no formal PFMT provided to women in the intervention group. |
| Okido 2015 | RCT. Primigravidae, pregnant women. PFMT vs usual care. Excluded because did not collect data on UI or FI; outcomes were uteroplacental and fetoplacental blood flow. |
| Perales 2016 | RCT. Healthy, pregnant women. PFMT (as part of an exercise group) vs usual care. Excluded because did not collect data on UI or FI; primary outcomes were the effects of exercise on the maternal cardiovascular system and on risk factors for cardiovascular disease. |
| Ruiz 2013 | RCT. Pregnant women. PFMT (as part of an exercise group) vs usual care. Excluded because did not collect data on UI or FI; assessed gestational bodyweight gain and fetal outcomes. |
| Siva 2014 | RCT. Primigravidae, pregnant women. PFMT as part of a "motor relearning programme") vs PFMT. Excluded because did not collect data on UI or FI; outcome was PFM strength. |
| Taskin 1996 | Quasi‐randomised RCT (day of week). Primigravidae. Intervention PFMT with or without episiotomy or caesarean section. Excluded because of mixed intervention and inappropriate controls. |
| Thorp 1994 | RCT. Nulliparous women recruited through advertisement. Unclear if PFMT or vaginal cones vs controls. Excluded because it was unclear whether the intervention was PFMT or vaginal cones, neither were data on UI or FI collected. |
| Wang 2014 | RCT. Nulliparous, pregnant women. PFMT plus phone follow‐up once every 2 weeks vs PFMT. Excluded because did not collect data on UI or FI; assessed delivery outcomes and PFM strength. |
| Zhu 2012 | Quasi‐RCT. Postpartum women. PFMT with electrical stimulation vs usual care. Excluded as unclear when women were recruited after delivery. Possible that the women included in the study were > 12 months' postpartum at the time of recruitment because the mean age of the sample was 34 years, which is substantially higher than other trials conducted in a similar context (see Liu 2011 or Wen 2010). |
FI: faecal incontinence; PFM: pelvic floor muscle; PFMT: pelvic floor muscle training; RCT: randomised controlled trial; UI: urinary incontinence.
Characteristics of studies awaiting assessment [ordered by study ID]
| Methods | RCT. |
| Participants | 100 primiparous women. Inclusion: aged > 20 years, singleton gestation, planning to deliver at St. Paul's hospital, Vancouver, Canada. Exclusion: unable to understand English. |
| Interventions |
Educational workshop: covered PF anatomy, function and evidence‐based pregnancy‐related risk factors for PF disorders. Control: usual care. |
| Outcomes |
Primary outcome: PF knowledge questionnaire. Secondary outcomes: Pelvic Floor Distress Inventory, PFIQ, knowledge and frequency of PFMT, change in mode of delivery preference, global satisfaction rating with PF health. |
| Notes | Abstract referred to postpartum incontinence; awaiting full publication. |
| Methods | RCT. |
| Participants | 109 postpartum women with anal incontinence. Inclusion: aged > 18 years, anal incontinence at inclusion. Exclusion: inadequate Norwegian language skills, neurological conditions, already receiving PFMT, PFM pain/dysfunction, secondary sphincter repair, unable to attend treatment and follow‐up sessions. |
| Interventions |
PFMT: progressive PFMT programme, 6 months' duration, with 4‐6 individual appointments with specialised PF physiotherapist and electrical stimulation if indicated. Control: usual care: including individualised instruction on how to perform a PFM contraction and written information about PFMT. |
| Outcomes |
Primary outcome: anal incontinence (St. Mark's score). Secondary outcomes: anal sphincter defects (endoanal ultrasound defect score), anal sphincter length, anal sphincter mean strength (manometry), PFM muscle function and ability. |
| Notes |
| Methods | RCT. |
| Participants | 232 nulliparous women. Inclusion: not reported. Exclusion: not reported. |
| Interventions |
PFMT (84). Control (148): unknown. |
| Outcomes | Pelvic dysfunction, perineal trauma, episiotomy. |
| Notes | Abstract refers to postpartum incontinence but no data provided; awaiting full publication. |
| Methods | RCT. |
| Participants | 50 primiparous postpartum women who underwent primary perineal repair after obstetric anal sphincter injury. Inclusion: aged > 18 years, vaginal delivery at gestational age ≥ 27 completed weeks, ability to read and speak the English language. Exclusion: inability to comply with physiotherapy or clinic visits; unreliable transportation; inability to perform PFMT due to pre‐existing neurological, musculoskeletal or neuromuscular disorders; caesarean delivery; FI or anorectal surgery before pregnancy and delivery. |
| Interventions |
PFMT: including 4 sessions (60 min) with a certified PF physiotherapist, with biofeedback and behavioural therapy over 12 weeks, beginning at 6 weeks' postpartum. Control: usual care: but no PF physiotherapy or behavioural therapy. |
| Outcomes |
Primary outcome: FI assessed with the Faecal Incontinence Quality of Life Scale. Secondary outcomes: anal‐rectal manometry, vaginal electromyography, Faecal Incontinence Severity Index, Female Sexual Function Index, UDI‐6, IIQ‐7, General Health questionnaire (Short Form‐12). |
| Notes |
| Methods | RCT. |
| Participants | 324 postpartum women from 5 provinces in China. |
| Interventions |
Electrical stimulation and biofeedback (unclear if PFMT included) (n = 200). PFMT at home (n = 134). |
| Outcomes |
Primary outcomes: PF physiological indexes, POP‐Q at 6 and 12 months' postpartum. Other outcomes: quality of life (PFIQ‐7) and sexual function (PISQ‐12). |
| Notes | Need to evaluate methods from full paper (Chinese) which requires translation. |
| Methods | RCT. |
| Participants | 60 pregnant women. Inclusion: aged > 18 years, in 3rd trimester. Exclusion: twin or high‐risk pregnancies, urinary tract infections, prolapses, neuropathy, collagen tissue disease, neurological illnesses, diabetes, chronic pulmonary disease, history of pelvic surgery, high risk of early delivery. |
| Interventions |
PFMT (n = 30): 3 times per day, duration unspecified. Reminder telephone calls every 2 weeks. Control (n = 30): not specified, but no instruction on PFMT was given. |
| Outcomes | PFM strength (perineometry), voiding function (uroflowmetry), urinary symptoms and quality of life (UDI‐6, IIQ‐7, the Overactive Bladder Questionnaire), and voiding diaries. |
| Notes |
| Methods | Pilot RCT. |
| Participants | 70 primiparous women 22‐27 weeks' gestation. |
| Interventions |
PFMT (n = 35): web‐based PFM education programme with usual care. Control (n = 35): usual care. |
| Outcomes |
Primary outcomes: awareness and knowledge of PFM, confidence and belief about engaging in PFM exercises, adherence to a PFM exercise programme assessed by questionnaires. Other outcomes: medical conditions, self‐reported UI (diary) and access to services for treatment of UI, self‐reported levels of general exercise, knowledge of available treatment for UI. |
| Notes |
| Methods | Unknown. |
| Participants | Unknown. |
| Interventions |
PFMT. Control: unknown. |
| Outcomes | Unknown. |
| Notes | No further details of this research available. This Master's thesis has been requested and, if available, will require translation. |
FI: faecal incontinence; IIQ‐7: Incontinence Impact Questionnaire; min: minute; n: number of women; PF: pelvic floor; PFIQ: Pelvic Floor Impact Questionnaire; PISQ: Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire; PFM: pelvic floor muscle; PFMT: pelvic floor muscle training; POP‐Q, Pelvic Organ Prolapse Quantification; UDI‐6, Urogenital Distress Inventory ‐ Short Form; UI: urinary incontinence.
Characteristics of ongoing studies [ordered by study ID]
| Trial name or title | Effects of Pelvic Floor Muscle Training on Pelvic Floor Muscle Function in Women During their First Pregnancies Measured by Perineometer. |
| Methods | RCT (Australian New Zealand Clinical Trial Registry: ACTRN12609001005246). |
| Participants | 15 nulliparous women. Inclusion: 1st pregnancy, aged 18‐40 years. Exclusion: pregnancy complications. |
| Interventions |
PFMT: 30‐min sessions, once per week for 16 weeks, starting at 20 weeks' gestation. Control: no PFMT. |
| Outcomes |
Primary outcome: PFM function (perineometry and digital palpation). Secondary outcome: self‐reported UI. |
| Starting date | 2007. |
| Contact information | Cristine Ferreira, Av. Bandeirantes, 3900: Monte Alegre: CEP: 14049‐900 Ribeirão Preto/SP, Brazil. |
| Notes | Trial completed and paper in preparation for publication. |
| Trial name or title | Long Term Effects of Multidisciplinary Assessment and Pre‐ and Post‐partum Pelvic Floor Muscle Group Treatment in Primigravid with Stress Urinary Incontinence Compared to Care‐as Usual: a Randomised Controlled Trial (Motherfit). |
| Methods | RCT (Netherlands Trial Register: NTR5971). |
| Participants | 240 pregnant or postpartum women (or both) with stress UI. Inclusion: primigravid, UI (stress or mixed), motivated to participate in programme, competent to speak and understand Dutch language, able to access mApp or webApp. Exclusion: UI prior to pregnancy that continues into pregnancy, high‐risk pregnancy resulting in contraindication to high‐intensity PFM exercises, chronic neurological disorders or diseases related to UI, urinary tract infection, anti‐incontinence or urogynaecological surgery, women who were expected to be lost to follow‐up, recent pelvic physiotherapy (< 6 months), refusal to use a mApp or webApp. |
| Interventions |
PFMT (n = 40): as part of group training sessions. PFMT and general fitness, 8 sessions starting at 20 weeks' gestation, plus a further 8 sessions if UI persists postpartum. Individualised home PFMT programme (using a mApp or webApp to encourage adherence and compliance). Control (n = 40): usual care: which may or may not include PFMT. |
| Outcomes |
Primary outcome: UI (ICIQ‐SF) at 18 months' postpartum. Secondary outcomes: UI severity (Patient Global Impression of Severity), urinary (IIQ‐7) and general quality of life (EQ‐5D‐5L), cost and participant satisfaction at 18 months' postpartum. |
| Starting date | December 2016. |
| Contact information | Bary Berghmans, Maastricht University Medical Center (MUMC+), the Netherlands. |
| Notes |
| Trial name or title | Influence of the Practice of Pilates on the Incidence of Urinary Incontinence, Perineal Strength, Low Back Pain in the Third Trimester. |
| Methods | RCT (Brazilian Registry of Clinical Trials: UTN: U1111‐1155‐5315). |
| Participants | 80 primiparous women, 20‐25 weeks' gestation. Inclusion: reported UI prepregnancy and low back pain, single fetus. Exclusion: neurological disorders that resulted in cognitive deficits or motor disorders of the lower limbs, physical or mental (or both) limitations, restrictive lung or heart disease, regular physical exercise of Pilates in the past 6 months, prepregnancy BMI ≥ 30. |
| Interventions |
Pilates sessions (n = 40): 20 in total (twice per week), 60‐min duration. Guided walks (n = 40): 2‐3 times per week for 30 min, daily PFM strengthening exercises. |
| Outcomes |
Primary outcome: UI assessed with "urinary incontinence" questionnaire, low back pain assessed with visual analogue scale. Secondary outcome: PFM strength with surface electromyography. |
| Starting date | May 2014. |
| Contact information | Mariana Buen, Faculdade de Ciências Médicas da Universidade Estadual de Campinas, Brazil. |
| Notes | Recruitment status unknown, as registry last updated in September 2014. Awaiting full publication to determine if Pilates sessions included any voluntary PFM contractions. |
| Trial name or title | Effect of Postpartum Pelvic Floor Muscle Training with Ultrasound Biofeedback on Recovery of Pelvic Floor Muscle Function: a Randomized Controlled Trial. |
| Methods | 3‐arm RCT (UMIN Clinical Trial Registry: UMIN000015878). |
| Participants | 180 primiparous postpartum women. Inclusion: primiparous postpartum women. Exclusion: caesarean section, multiple birth or breech delivery, incontinence before pregnancy, neuropathic UI and FI, restricted physical activity, aged < 20 years. |
| Interventions |
PFMT with ultrasound biofeedback. PFMT without ultrasound biofeedback. Usual care. |
| Outcomes |
Primary outcome: PFM function assessed with ultrasound. Secondary outcomes: UI assessed with ICIQ‐SF and I‐QOL; FI assessed with FISI, FIQL and Wexner score; PFDI‐20, PFM exercise self‐efficacy scale, fatigue feelings (Jikakusho shirabe). |
| Starting date | December 2014. |
| Contact information | Megumi Haruna, Division of Health Sciences & Nursing, Graduate School of Medicine, University of Tokyo, Japan. |
| Notes | Registry updated in December 2016; recruitment completed. |
| Trial name or title | Effect of Pelvic Floor Muscle Training among Pregnant Black African Population on the Risk of Postpartum Urinary Incontinence, a Single Blind Randomized Control Trial. |
| Methods | RCT (Pan African Clinical Trials Registry: PACTR201407000834391). |
| Participants | 66 primiparous women, 14‐24 weeks' gestation. Inclusion: Black African descent, aged ≥ 18 years. Exclusion: pre‐existing UI, severe medical illness requiring recurrent hospital admissions or that would affect compliance to training programme, obstetrical conditions likely to lead to preterm delivery, history suggestive of collagen disorders. |
| Interventions |
PFMT (n = 33): supervised by a physiotherapist and continence nurse, up to 37 weeks' gestation. Control (n = 33): usual care. |
| Outcomes |
Primary outcome: UI at 6 weeks' postpartum assessed with the ICIQ‐SF. Other outcomes: effect of mode of delivery on incidence of postpartum UI and determining contributory factors (e.g. smoking, BMI, age, cultural practices) in this population on the incidence of postpartum UI. |
| Starting date | August 2014. |
| Contact information | Johnstone Miheso, Aga Khan University, Nairobi, Kenya. |
| Notes | Anticipated date of last follow‐up was March 2015. Unpublished thesis (Ngugi 2015; see Miheso 2014) related to this trial registry. |
| Trial name or title | Exercise Training in Pregnancy for Obese Women (ETIP): Study Protocol for a Randomised Controlled Trial. |
| Methods | RCT (ClinicalTrials.gov Identifier: NCT01243554). |
| Participants | 150 previously sedentary, pregnant women with prepregnancy BMI ≥ 30. Inclusion: aged ≥ 18 years, singleton live fetus at 11‐ to 14‐week ultrasound scan. Exclusion: pregnancy complications, high risk for preterm labour or diseases that would interfere with participation, and habitual exercise training (twice or more weekly). |
| Interventions |
PFMT (n = 75): as part of an exercise group, minimum 3 times per week. Daily PFMT at home and a 50‐min home exercise programme (endurance and strength training) at least once per week. Motivational interviews, 30 min each trimester. Control (n = 75): usual care: women not discouraged from exercising on their own. |
| Outcomes |
Primary outcome: gestational weight gain. Other outcomes: a variety of maternal outcomes (e.g. cardiac function, gestational diabetes, psychological well‐being, postnatal depression) including prevalence and severity of UI and FI, ultrasound of the PFM, and PFM strength; and fetal outcomes. |
| Starting date | September 2010. |
| Contact information | Trine Moholdt, Norwegian University of Science and Technology. |
| Notes | Study completed (according to trial registration). Awaiting publication of data relating to incontinence and PFM function. |
| Trial name or title | PERL 4: Promoting Effective Recovery from Labour. Self‐care to Prevent Birth‐Related Urinary Incontinence in Diverse Women. |
| Methods | RCT (ClinicalTrials.gov Identifier: NCT00763984). |
| Participants | 432 pregnant nulliparous or multiparous women of African American, Caucasian or Hispanic ethnicity. Inclusion: ≥ 18 years of age, able to understand and read English or Spanish, low risk antepartum (1st, 2nd or 3rd pregnancy), 16‐25 weeks' gestation, expecting a vaginal birth, have lost no more than a few drops of urine as often as every other day, no previous or current UI treatment, no history of serious medical or neurological conditions, do not have a chronic urinary tract infection. Exclusion: if participant does not meet all of the above criterion for inclusion. |
| Interventions |
PFMT: PFMT (as defined by the International Continence Society) and bladder training as part of a bladder health class. Women's knowledge, adoption and maintenance of PFMT and bladder training monitored. Control: usual care, which may include PFMT. Women's knowledge, adoption and maintenance of PFMT monitored. |
| Outcomes |
Primary outcome: incidence and severity of UI at 12 months' postpartum. 3‐year follow‐up period. |
| Starting date | October 2007. |
| Contact information | Carolyn Sampselle, School of Nursing, University of Michigan, USA. |
| Notes | Study complete (as verified on trial register in January 2015). Author contacted to confirm status of study, no response received. |
| Trial name or title | Reducing Perinatal Anal Incontinence through Early Pelvic Floor Muscle Training: a Prospective Pilot Study. |
| Methods | Feasibility RCT (ClinicalTrials.gov Identifier: NCT02270008). |
| Participants | 100 parous women. Inclusion: parous women, aged 20‐40 years, new obstetrician visit prior to 20 weeks' gestation, confirmed singleton live intrauterine pregnancy. Exclusion: history of anal incontinence or prolapse, history of surgery or procedures for urinary or anal incontinence or pelvic organ prolapse, tobacco use, diabetes mellitus, history of sexual trauma, chronic cough, chronic constipation, known connective tissue disorder. |
| Interventions |
PFMT: 1‐to‐1 with a trained nurse practitioner (1 session), with PFMT at home. Control: usual care: including written PFM exercises. |
| Outcomes |
Primary outcome: incidence of FI or flatal incontinence assessed with standardised questionnaires. Secondary outcome: PFMT compliance (exercise diary). |
| Starting date | October 2014. |
| Contact information | Deborah Karp, Emory University, USA. |
| Notes | Registry updated in January 2016; recruitment completed in June 2015. |
| Trial name or title | Bump on the Ball: Impact of a Prenatal Exercise and Education Programme on Birth Outcomes and Maternal Quality of Life. |
| Methods | RCT (ClinicalTrials.gov Identifier: NCT02334397). |
| Participants | 120 pregnant women. Inclusion: singleton, primiparous pregnancy, delivering at Prentice Women's Hospital, able to participate based on PARmedX for pregnancy criteria. Exclusion: non‐English or Spanish speaking, aged < 18 years, known condition requiring caesarean section, currently enrolled in any type of physiotherapy, unable to complete the programme secondary to medical limitations. |
| Interventions |
PFMT: as part of a fitness and education programme ("total control") that combines PFM and core muscle strengthening and education (around aspects of labour and delivery process), 1 class per week for 6 weeks. Women also to wear pedometers to monitor general activity. Control: no intervention. |
| Outcomes |
Primary outcomes: type of birth (spontaneous vs operative vaginal delivery) and indications for operative vaginal delivery. Secondary outcomes: obstetrical complications, level of concern about birthing experience (Penn State Worry Questionnaire), knowledge about birthing experience, PF symptoms (PFDI), sexual function (PISQ‐12), satisfaction with birthing experience, postpartum depression and risk factors (Edinburgh Postnatal Depression Score). |
| Starting date | February 2016. |
| Contact information | Christina Gaupp, Northwestern University, USA. |
| Notes | Estimated completion date June 2017 (for primary outcomes). |
| Trial name or title | Effect of Physical Exercise Programme on Fetoplacental Growth: a Randomised Controlled Trial. |
| Methods | RCT (ClinicalTrials.gov Identifier: NCT02420288). |
| Participants | 124 healthy pregnant women. Inclusion: able to exercise according to the American College of Obstetricians and Gynecologists guidelines, able to communicate in Spanish, giving birth at Hospital Universitario de Torrejón, Hospital Universitario de Puerta de Hierro or Hospital Universitario Severo Ochoa (Madrid, Spain). Exclusion: multiparous, obstetric complications, > 18 weeks' gestation, unable to attend the physical exercise programme, aged < 18 years or > 45 years. |
| Interventions |
PFMT: as part of a supervised exercise group, 3 times per week, 16‐38 weeks' gestation. Session duration 55‐60 min with 10 min PFMT. Control: no intervention. |
| Outcomes |
Primary outcomes: maternal weight gain during pregnancy, fetal and placental weight. Secondary outcomes: various maternal outcomes including postnatal depression, gestational diabetes and UI (measured with ICIQ‐SF), and fetal outcomes. |
| Starting date | November 2014. |
| Contact information | Ruben Barakat, Universidad Politecnica de Madrid. |
| Notes | Data collection for primary outcome completed in December 2016. Study completion date is documented as 2021. |
| Trial name or title | Obstetric Perineal Trauma, Pelvic Floor Symptoms and Early Physiotherapy Intervention. |
| Methods | RCT (ClinicalTrials.gov Identifier: NCT02682212). |
| Participants | 80 healthy postpartum women. Inclusion: primiparas after vaginal delivery at Landspitali University Hospital, aged ≥ 18 years, diagnosed UI at 6 weeks' postpartum, able to attend the intervention and answer the Australian Pelvic Floor Questionnaire. Exclusion: diseases or conditions that interfere with PF function (other than childbirth), unable to understand Icelandic, cognitive disabilities. |
| Interventions |
PFMT: delivered by a physiotherapist with vaginal/rectal pressure feedback once per week, plus daily home exercises, for 12 weeks. Control: usual care. |
| Outcomes |
Primary outcome: UI (Australian Female Pelvic Floor Questionnaire). Secondary outcomes: faecal/flatal incontinence, sexual dysfunction, quality of life (Australian Female Pelvic Floor Questionnaire), PFM strength. |
| Starting date | March 2016. |
| Contact information | Thora Steingrimsdottir, Landspitali University Hospital/University of Iceland, Reykjavik, Iceland. |
| Notes | Data collection for primary outcome completed in December 2016. Study completion date 2021. |
| Trial name or title | Iball and Pelvic Floor Muscle Training (iball). |
| Methods | RCT (ClinicalTrials.gov Identifier: NCT02865954). |
| Participants | 60 primiparous postpartum women. Inclusion: 3rd trimester of 1st pregnancy. Exclusion: currently seeing a pelvic health physiotherapist or participating in a PF fitness programme. |
| Interventions |
PFMT: iball (rehabilitation tool consisting of a device and mobile app) PFMT protocol, 16 weeks, starting approximately 6 weeks' postpartum. Control: usual care: including instructions on performing a correct PFM contraction. |
| Outcomes |
Primary outcome: acceptability of the iball intervention (qualitative). Secondary outcomes: PF examination (PERFECT criteria), UDI‐6 and IIQ‐7. |
| Starting date | October 2016. |
| Contact information | Sinead Dufour, McMaster University, Hamilton, Canada. |
| Notes |
| Trial name or title | Study about the Influence of Pelvic Floor Exercises Orientation Regarding Urinary Loss Prevention on Postpartum Period. |
| Methods | RCT (Brazilian Registry of Clinical Trials: UTN: U1111‐1125‐1467). |
| Participants | 300 postpartum women with self‐reported UI, dyspareunia and constipation. Inclusion: vaginal or caesarean delivery at Maternidade Carmela Dutra, Florianópolis, Brazil, during the study period, aged 18‐45 years. Exclusion: neurological UI, neurological disorder, history of urogenital cancer, cognitive deficits, blindness, illiteracy, episiotomy associated with local symptoms (excessive oedema, pain), drug dependency, no telephone for follow‐up contact. |
| Interventions |
PFMT. Control: not reported. |
| Outcomes |
Primary outcome: frequency and amount of UI (ICIQ‐SF). Secondary outcomes: frequency and intensity of dyspareunia (Female Sexual Function Index), constipation. |
| Starting date | September 2011. |
| Contact information | Cinara Sacomori, Universidade do Estado de Santa Catarina, Florianópolis, Brazil. |
| Notes | Registry last updated in January 2012, with recruitment ongoing. |
| Trial name or title | Impact of Pelvic Floor Physiotherapy during Pregnancy in Urinary Incontinence and Delivery. |
| Methods | RCT (Brazilian Registry of Clinical Trials: UTN: U1111‐1184‐9871). |
| Participants | 96 primiparous women. Inclusion: 12‐20 weeks' gestation, aged 12‐50 years. Exclusion: diabetes, fetal malformation, vaginal delivery unfeasible, UI. |
| Interventions |
PFMT (n = 48): once per week over 12 weeks (supervised by a physiotherapist), 12‐32 weeks' gestation. Perineal massage and elongation of PFM (supervised by a physiotherapist), once per week over 4 weeks, 34‐38 weeks' gestation. Control (n = 48): unspecified (but no physiotherapy intervention). |
| Outcomes |
Primary outcome: self‐reported UI (ICIQ‐SF). Secondary outcome: perineal laceration. |
| Starting date | July 2016. |
| Contact information | Lucas Schreiner, Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, Brazil. |
| Notes | Estimated date of last enrolment December 2017. |
| Trial name or title | Perineal Muscle Training versus Usual Prenatal Care in the Incidence of Avulsion of the Levator ani Muscle at First Birth of Mexican Women: Randomized Control Trial. |
| Methods | RCT (ClinicalTrials.gov Identifier: NCT02513420). |
| Participants | 228 pregnant women. Inclusion: pregnant women aged > 18 years with a single fetus, without contraindications to delivery, with no previous PF damage due to childbirth, with or without symptoms of PF dysfunction, < 33 weeks' gestation, physical and cognitive abilities to enable participation in programme. Exclusion: any contraindication to labour, avulsion of the levator ani muscle, previous pregnancies > 20 weeks' gestation delivered via caesarean section. |
| Interventions |
PFMT: perineal massage and PFMT from 33 weeks' gestation onwards, once per week until delivery. Control: usual care. |
| Outcomes | Levator ani avulsion (assessed by palpation and ultrasound), symptoms of PF dysfunction (Spanish Pelvic Floor Disability Index‐20 questionnaire), morphological changes of genital hiatus and perineal body, "accomplishment" of PFMT. |
| Starting date | July 2015. |
| Contact information | Daniel Velez‐Sanchez, Mexican College of Gynecology and Obstetrics. |
| Notes |
BMI: body mass index (kg/m²); FI: faecal incontinence; FIQL: Faecal Incontinence Quality of Life scale; FISI: Faecal Incontinence Severity Index; I‐QOL: ICIQ‐SF: Incontinence Quality of Life Scale Questionnaire; International Consultation on Incontinence Questionnaire‐Short Form; IIQ‐7: Incontinence Impact Questionnaire; min: minute; n: number of women; PERFECT: acronym with P = power (or pressure), E = endurance, R = repetitions, F = fast contractions and ECT = every contraction timed; PF: pelvic floor; PFDI‐20: Pelvic Floor Distress Inventory‐20; PFM: pelvic floor muscle; PFMT: pelvic floor muscle training; PISQ‐12: Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire; RCT: randomised controlled trial; UDI‐6: Urogenital Distress Index‐Short Form; UI: urinary incontinence.
Contributions of authors
All five authors screened trials for eligibility and discussed the overall conclusions.
SW and JHS: extracted and cross‐checked the data from the studies new to this review. SW: did most of the data entry, which was cross‐checked by JHS. SW and JHS: performed the GRADE assessment and prepared the 'Summary of findings' tables. JHS wrote the first draft of the protocol and the previous review. SW drafted the updated review, with assistance from JHS.
Sources of support
Internal sources
University of Otago, New Zealand.
External sources
-
National Institute for Health Research, UK.
This project was supported by the National Institute for Health Research (NIHR), via Cochrane Infrastructure funding to the Cochrane Incontinence Group. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, National Health Service or the Department of Health. The NIHR is the largest single funder of the Cochrane Incontinence Group.
Declarations of interest
SW: none known. RB: none known. JC: none known. SM: was an investigator on two of the included trials in the review and had no role in screening, quality assessment or data extraction for these trials. JHS: none known.
New search for studies and content updated (conclusions changed)
References
References to studies included in this review
- Ahlund S, Nordgren B, Wilander EL, Wiklund I, Friden C. Is home‐based pelvic floor muscle training effective in treatment of urinary incontinence after birth in primiparous women? A randomized controlled trial. Acta Obstetricia et Gynecologica Scandinavica 2013;92(8):909‐15. [sr‐incont48416] [DOI] [PubMed] [Google Scholar]
- Assis LC, Bernardes JM, Barbosa AM, Santini AC, Vianna LS, Dias A. Effectiveness of an illustrated home exercise guide on promoting urinary continence during pregnancy: a pragmatic randomized clinical trial [Portuguese]. Revista Brasileira de Ginecologia e Obstetricia 2015;37(10):460‐6. [sr‐incont69254] [DOI] [PubMed] [Google Scholar]; Assis LC, Dias A, Barbosa AMP, Santini ACM, Sousa VO, Vianna LS, et al. Contribution of early intensive prolonged pelvic floor exercises (Abstract number 782‐S). American Journal of Epidemiology 2011;173(Suppl 11):S196. [sr‐incont47327] [Google Scholar]; Dias A, Assis L, Barbosa A, Santini AC, Picelli‐Dias F. Effectiveness of perineal exercises in controlling urinary incontinence and improving pelvic floor muscle function during pregnancy (Abstract number 117). Neurourology and Urodynamics 2011;30(6):968. [Google Scholar]
- Barakat R, Pelaez M, Montejo R, Luaces M, Zakynthinaki M. Exercise during pregnancy improves maternal health perception: a randomized controlled trial. American Journal of Obstetrics and Gynecology 2011;204(5):402.e1‐7. [sr‐incont65194] [DOI] [PubMed] [Google Scholar]
- Bø K, Haakstad L. Is pelvic floor muscle training effective when taught in a general fitness class for pregnant women? A randomized controlled trial (Abstract number 200). International Urogynecology Journal 2009;20(Suppl 2):S238‐9. [Google Scholar]; Bø K, Haakstad LA. Is pelvic floor muscle training effective when taught in a general fitness class in pregnancy? A randomised controlled trial. Physiotherapy 2011;97(3):190‐5. [DOI] [PubMed] [Google Scholar]
- Chiarelli P, Cockburn J. Preventing urinary incontinence in postpartum women (Abstract). Neurourology and Urodynamics 2001;20(4):448‐9. [SR‐INCONT12109] [Google Scholar]; Chiarelli P, Cockburn J. Promoting urinary continence in women after delivery: randomised controlled trial (extended electronic version). BMJ 2002;324:1‐6. [SR‐INCONT14669] [DOI] [PMC free article] [PubMed] [Google Scholar]; Chiarelli P, Murphy B, Cockburn J. Acceptability of a urinary continence promotion programme to women in postpartum. BJOG 2003;110(2):188‐96. [SR‐INCONT15783] [PubMed] [Google Scholar]; Chiarelli P, Murphy B, Cockburn J. Promoting urinary continence in postpartum women: 12‐month follow‐up data from a randomised controlled trial. International Urogynecology Journal 2004;15(2):99‐105. [SR‐INCONT17410] [DOI] [PubMed] [Google Scholar]
- Cruz C, Riesco ML, Zanetti M. Supervised pelvic floor muscle training to treat urinary incontinence during pregnancy: a randomized controlled trial (Abstract number 403). Neurourology and Urodynamics 2014;33(6):867‐8. [RBR‐8xj48n; sr‐incont64412] [Google Scholar]
- Dinc A, Kizilkaya Beji N, Yalcin O. Effect of pelvic floor muscle exercises in the treatment of urinary incontinence during pregnancy and the postpartum period. International Urogynecology Journal2009; Vol. 20, issue 10:1223‐31. [SR‐INCONT35362] [DOI] [PubMed]
- Dokmeci F, Bayramov S, Tur BS, Bayramov V, Seval M, Gok H. Pelvic floor muscle training during pregnancy: a randomized single‐blind controlled study on improvement of antenatal and postpartum lower urinary tract symptoms (Abstract). Journal of Pelvic Medicine and Surgery 2008;14(4):304. [sr‐incont46744] [Google Scholar]
- Dumoulin C. Efficacite des traitements physiotherapiques pour l'incontinence urinaire d'effort chez la femme en periode postnatale [PhD thesis]. Montreal: University of Montreal, 2004. [Google Scholar]; Dumoulin C, Bourbonnais D, Morin M, Gravel D, Lemieux MC. Predictors of success for physiotherapy treatment in women with persistent postpartum stress urinary incontinence. Archives of Physical Medicine and Rehabilitation 2010;91(7):1059‐63. [DOI] [PubMed] [Google Scholar]; Dumoulin C, Lemieux MC, Bourbonnais D, Gravel D, Bravo G, Morin M. Physiotherapy for persistent postnatal stress urinary incontinence: a randomized controlled trial. Obstetrics and Gynecology 2004;104(3):504‐10. [DOI] [PubMed] [Google Scholar]; Dumoulin C, Martin C, Elliott V, Bourbonnais D, Morin M, Lemieux MC, et al. Randomized controlled trial of physiotherapy for postpartum stress incontinence: 7‐year follow‐up. Neurourology and Urodynamics 2013;32(5):449‐54. [sr‐incont48074] [DOI] [PubMed] [Google Scholar]; Dumoulin C, Morin M, Bourbonnais D, Lemieux M, Gravel D. Effect of adding deep abdominal muscle training to pelvic floor muscle training to treat stress urinary incontinence: a one‐year follow up (Abstract number 662). 34th Annual Meeting of the joint meeting of the International Continence Society and the International Urogynecological Association; 2004 Aug 23‐27; Paris. 2004. [Google Scholar]; Elliott V, Dumoulin C, Martin C, Morin M, Lemieux M, Bourbonnais D. Physical therapy for persistent postpartum stress urinary incontinence: a seven year follow‐up study (Abstract number 198). Neurourology and Urodynamics 2009;28(7):820‐1. [Google Scholar]
- Ewings P, Spencer S, Marsh H, O'Sullivan M. Obstetric risk factors for urinary incontinence and preventative pelvic floor exercises: cohort study and nested randomized controlled trial. Journal of Obstetrics and Gynaecology 2005;25(6):558‐64. [SR‐INCONT21250] [DOI] [PubMed] [Google Scholar]
- Fritel X, Fauconnier A, Savary D, Letouzey V, Gueye A, Campagne S, et al. Prevent postnatal urinary incontinence by prenatal pelvic floor muscle training? First results of the multicenter randomized study 3PN, prenatal pelvic floor prevention (Abstract number 263). Neurourology and Urodynamics 2012;31(6):1068‐9. [NCT00551551; sr‐incont46713] [Google Scholar]; Fritel X, Fauconnier A, Tayrac R, Amblard J, Cotte L, Fernandez H. Prevent postnatal urinary incontinence by prenatal pelvic floor exercise? Rationale and protocol of the multicenter randomized study PreNatal Pelvic floor Prevention (3PN) [French]. Journal de Gynecologie, Obstetrique et Biologie de la Reproduction 2008;37(5):441‐8. [NCT00551551; sr‐incont27753] [DOI] [PubMed] [Google Scholar]; Fritel X, Guilhot‐Gaudeffroy J, Tayrac R, Savary D, Deffieux X, Cotte L, et al. Prevention of postnatal urinary incontinence by antenatal pelvic floor muscle exercises, secondary per protocol analysis of the 3PN (prenatal pelvic floor prevention) randomized trial (Abstract number 5). Neurourology and Urodynamics 2013;32(6):528‐9. [NCT00551551; sr‐incont49222] [Google Scholar]; Fritel X, Tayrac R, Bader G, Savary D, Gueye A, Deffieux X, et al. Preventing urinary incontinence with supervised prenatal pelvic floor exercises: a randomized controlled trial. Obstetrics and Gynecology 2015;126(2):370‐7. [NCT00551551; sr‐incont68120] [DOI] [PubMed] [Google Scholar]
- Frost A, Trankel D, Shannon M. The efficacy of written and verbal pelvic floor exercise discharge instructions in reducing urinary incontinence among postpartum patients (Abstract). Journal of Women's Health Physical Therapy 2014;38(1):40. [sr‐incont61793] [Google Scholar]
- Frumenzio E, Giovannozzi S, Pietropaolo A, Salvini E, Bruno R, Lolli C, et al. Results of a prospective randomised study: role of pelvic‐perineal rehabilitation in post‐partum incontinence recovery (Abstract number 4). Neurourology and Urodynamics 2012;31(S1):S3. [sr‐incont46707] [Google Scholar]
- Gaier L, Lamberti G, Giraudo D. Pelvic floor muscle training during pregnancy to prevent urinary pelvic floor dysfunctions (Abstract). Neurourology and Urodynamics 2010;29(2S):64‐5. [Google Scholar]
- Geraerts I, Kampen M. Twelve‐year follow‐up of conservative management of postnatal urinary and faecal incontinence and prolapsed outcomes: randomised controlled trial. BJOG 2014;121(13):1741‐2. [DOI] [PubMed] [Google Scholar]; Glazener C, Elders A, MacArthur C, Lancashire RJ, Herbison P, Hagen S, et al. Childbirth and prolapse: long‐term associations with the symptoms and objective measurement of pelvic organ prolapse. BJOG 2013;120(2):161‐8. [DOI] [PubMed] [Google Scholar]; Glazener C, MacArthur C, Hagen S, Elders A, Lancashire R, Herbison G, et al. Twelve‐year follow‐up of conservative management of postnatal urinary and faecal incontinence and prolapse outcomes: randomised controlled trial. BJOG 2014;121(1):112‐20. [sr‐incont50467] [DOI] [PubMed] [Google Scholar]; Glazener C, MacArthur C, Wilson D, Hagen S, ProLong study group. Authors' reply: twelve‐year follow‐up of conservative management of postnatal urinary and faecal incontinence and prolapsed outcomes: randomised controlled trial. BJOG 2014;121(13):1742. [DOI] [PubMed] [Google Scholar]; Glazener CM, Herbison GP, MacArthur C, Grant A, Wilson PD. Randomised controlled trial of conservative management of postnatal urinary and faecal incontinence: six year follow up. BMJ 2005;330(7487):337‐40. [DOI] [PMC free article] [PubMed] [Google Scholar]; Glazener CM, Herbison GP, Wilson PD, MacArthur C, Lang GD, Gee H, et al. Conservative management of persistent postnatal urinary and faecal incontinence: a randomised controlled trial [Extended electronic version]. BMJ 2001;323:1‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]; Glazener CM, Herbison GP, Wilson PD, MacArthur C, Lang GD, Gee H, et al. Conservative management of persistent postnatal urinary and faecal incontinence: randomised controlled trial. BMJ 2001;323(7313):593‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]; Rennie AM, Wilson D, Glazener C, Gee H, Lang G, MacArthur C. A multicentre randomised trial of treatment of postnatal incontinence (Abstract). International Confederation of Midwives, 24th Triennial Congress; 1996 May 26‐31; Oslo. 1996:8. [Google Scholar]; Wilson PD, Glazener C, McGee M, Herbison P, MacArthur C, Grant A. Randomised controlled trial of conservative management of postnatal urinary and faecal incontinence: long term follow‐up study (Abstract). Neurourology and Urodynamics 2002;21(4):370. [Google Scholar]; Wilson PD, Herbison GP, Glazener CMA, Lang G, Gee H, MacArthur C. Postnatal incontinence: a multi centre, randomised controlled trial of conservative treatment (Abstract). Neurourology and Urodynamics 1997;16(5):349‐50. [Google Scholar]
- Gorbea Chavez V, Velazquez Sanchez MdP, Kunhardt Rasch JR. Effect of pelvic floor exercise during pregnancy and puerperium on prevention of urinary stress incontinence [Efecto de los ejercicios del piso pelvico durante el embarazo y el puerperio en la prevencion de la incontinencia urinaria de esfuerzo]. Ginecologia y Obstetricia de Mexico 2004;72(12):628‐36. [SR‐INCONT20384] [PubMed] [Google Scholar]
- Bø K, Hilde G, Stӕr‐Jensen J, Siafarikas F, Tennfjord MK, Engh ME. Postpartum pelvic floor muscle training and pelvic organ prolapse‐a randomized trial of primiparous women. American Journal of Obstetrics and Gynecology 2015;212(1):38.e1‐7. [NCT01069484; sr‐incont64837] [DOI] [PubMed] [Google Scholar]; Bø K, Hilde G, Tennfjord MK, Jensen JS, Siafarikas F, Engh ME. Randomized controlled trial of pelvic floor muscle training to prevent and treat pelvic organ prolapse in postpartum primiparous women (Abstract number 205). Neurourology and Urodynamics 2013;32(6):806‐7. [sr‐incont49200] [Google Scholar]; Hilde G, Stӕr‐Jensen J, Siafarikas F, Ellstrom Engh M, Bø K. Does pelvic floor muscle training enhance pelvic floor muscle recovery? An assessor blinded randomized controlled trial (Abstract number PP15). International Urogynecology Journal and Pelvic Floor Dysfunction 2014;25(1 Suppl 1):S17‐8. [sr‐incont64248] [Google Scholar]; Hilde G, Stӕr‐Jensen J, Siafarikas F, Ellstrom Engh M, Bø K. Effect of postpartum pelvic floor muscle training on urinary incontinence in primiparous women with and without major pelvic floor muscle defects. An assessor blinded randomised controlled trial (Abstract number 8). Neurourology and Urodynamics 2013;32(6):533‐4. [NCT01069484] [Google Scholar]; Hilde G, Stӕr‐Jensen J, Siafarikas F, Ellstrom Engh M, Bø K. Postpartum pelvic floor muscle training and urinary incontinence: a randomized controlled trial [Erratum appears in: Obstetrics and Gynecology 2014;124(3):639]. Obstetrics and Gynecology 2013;122(6):1231‐8. [NCT01069484; sr‐incont49471] [DOI] [PubMed] [Google Scholar]; Kolberg Tennfjord M, Hilde G, Stӕr‐Jensen J, Siafarikas F, Engh ME, Bø K. Effect of postpartum pelvic floor muscle training on vaginal symptoms and sexual dysfunction‐secondary analysis of a randomised trial. BJOG 2016;123(4):634‐42. [DOI] [PubMed] [Google Scholar]
- Hughes P. Personal communication2006. ; Hughes P, Jackson S, Smith P, Abrams P. Can antenatal pelvic floor exercises prevent postnatal incontinence (Abstract). Neurourology and Urodynamics 2001;20(4):447‐8. [SR‐INCONT12110] [Google Scholar]
- Kim EY, Kim SY, Oh DW. Pelvic floor muscle exercises utilizing trunk stabilization for treating postpartum urinary incontinence: randomized controlled pilot trial of supervised versus unsupervised training. Clinical Rehabilitation 2012;26(2):132‐41. [sr‐incont44514] [DOI] [PubMed] [Google Scholar]
- Ko PC, Liang CC, Chang SD, Lee JT, Chao AS, Cheng PJ. A randomized controlled trial of antenatal pelvic floor exercises to prevent and treat urinary incontinence. International Urogynecology Journal 2011;22(1):17‐22. [41029] [DOI] [PubMed] [Google Scholar]; Liang C, Ko P, Lin Y, Tseng L, Lo T, Wang AC. Effect of antenatal pelvic floor muscle exercises in prevention and treatment of urinary incontinence: a randomized controlled trial (Abstract number 208). Neurourology and Urodynamics 2010;29(6):1105‐6. [Google Scholar]
- Kocaoz S, Eroglu K, Sivaslioglu AA. Role of pelvic floor muscle exercises in the prevention of stress urinary incontinence during pregnancy and the postpartum period. Gynecologic and Obstetric Investigation 2013;75(1):34‐40. [sr‐incont49319] [DOI] [PubMed] [Google Scholar]
- Kou J‐L, Dang L‐J, Feng X‐Q. Clinical study on the treatment of postpartum rehabilitation to improve the pelvic floor function. Medical Innovation of China 2013;10(25):55‐7. [sr‐incont70278] [Google Scholar]
- Liu X‐B. Pelvic floor muscle training for prevention and treatment of postpartum urinary incontinence clinical observation. Guide of China Medicine 2011;9(2):21‐2. [sr‐incont70276] [Google Scholar]
- Meyer S, Hohlfeld P, Achtari C, Grandi P. Pelvic floor education after vaginal delivery. Obstetrics and Gynecology 2001;97(5 Pt 1):673‐7. [SR‐INCONT12119] [DOI] [PubMed] [Google Scholar]; Meyer S, Hohlfeld P, Grandi P, Megalo A. Is pelvic floor re‐education after vaginal delivery effective? A prospective double‐blind randomized study in primiparae (Abstract). Neurourology and Urodynamics1999; Vol. 18, issue 4:290. [SR‐INCONT9941]; Meyer S, Hohlfeld P, Grandi P, Megalo A. Is pelvic floor reeducation after vaginal delivery effective? A prospective double‐blind randomized study in primiparae (Abstract). International Urogynecology Journal and Pelvic Floor Dysfunction 1999;10 Suppl 1:39‐40. [SR‐INCONT9846]10207766 [Google Scholar]
- Miquelutti MA. Evaluating of an antenatal education program [PhD thesis]. Campinas, São Paulo: Universidade Estadual de Campinas, Faculdade de Ciências Médicas, 2012. [sr‐incont46712] [Google Scholar]; Miquelutti MA, Cecatti JG, Makuch MY. Developing strategies to be added to the protocol for antenatal care: an exercise and birth preparation program. Clinics (Sao Paulo, Brazil) 2015;70(4):231‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]; Miquelutti MA, Cecatti JG, Makuch MY. Evaluation of a birth preparation program on lumbopelvic pain, urinary incontinence, anxiety and exercise: a randomized controlled trial. BMC Pregnancy and Childbirth 2013;13:154. [NCT01155804; sr‐incont59873] [DOI] [PMC free article] [PubMed] [Google Scholar]; Miquelutti MA, Cecatti JG, Makuch MY. Evaluation of the efficacy of an antenatal birth preparation program (Abstract number O431). International Journal of Gynaecology and Obstetrics 2012;119(Suppl 3):S414. [sr‐incont64222] [Google Scholar]
- Mørkved S, Bø K, Schei B, Salvesen KÅ. Pelvic floor muscle training during pregnancy to prevent urinary incontinence: a single‐blind randomized controlled trial. Obstetrics and Gynecology 2003;101(2):313‐9. [SR‐INCONT15816] [DOI] [PubMed] [Google Scholar]; Mørkved S, Rommen K, Schei B, Salvesen KÅ, Bø K. No difference in urinary incontinence between training and control group six years after cessation of a randomized controlled trial, but improved sexual satisfaction in the training group (Abstract number 50). Neurourology and Urodynamics 2007;26(5):667. [Google Scholar]; Mørkved S, Salvesen KÅ. Does pelvic floor muscle training during pregnancy have an effect on labour? (Abstract). Neurourology and Urodynamics 2004;23(5/6):410‐1. [SR‐INCONT19001] [Google Scholar]; Mørkved S, Salvesen KÅ, Scheil B, Bø K. Prevention of urinary incontinence during pregnancy ‐ a randomized controlled trial of primiparous women (Abstract). International Urogynecology Journal and Pelvic Floor Dysfunction 2001;12 Suppl 3:1. [SR‐INCONT15713]11294524 [Google Scholar]; Salvesen KÅ, Mørkved S. Randomised controlled trial of pelvic floor muscle training during pregnancy. BMJ 2004;329(7462):378‐80. [SR‐INCONT17558] [DOI] [PMC free article] [PubMed] [Google Scholar]; Schei B, Mørkved S, Bø K. Does pelvic floor muscle training during pregnancy have an influence on sexual life after delivery? (Abstract number 176). Journal of Sexual Medicine 2011;8(Suppl s3):124‐5. [Google Scholar]
- O'Herlihy C. Early home feedback physiotherapy compared with pelvic floor exercises soon after third degree perineal tear: a randomised trial (Abstract number 63). International Urogynecology Journal and Pelvic Floor Dysfunction 2012;23(2 Suppl 1):S107. [Google Scholar]; Peirce C, Murphy C, Fitzpatrick M, Cassidy M, Daly L, O'Connell P, et al. Randomised controlled trial comparing early home biofeedback physiotherapy with pelvic floor exercises for the treatment of third‐degree tears (EBAPT Trial). BJOG 2013;120(10):1240‐7. [sr‐incont48563] [DOI] [PubMed] [Google Scholar]; Peirce C, O'Herlihy C, Murphy C, Fitzpatrick M, Cassidy M, Daly L, et al. Randomized trial comparing early home biofeedback physiotherapy with pelvic floor exercises following third degree perineal tears (Abstract). American Journal of Obstetrics and Gynecology 2012;206(1 Suppl 1):S298‐9. [sr‐incont46739] [DOI] [PubMed] [Google Scholar]
- Pelaez M, Gonzalez‐Cerron S, Montejo R, Barakat R. Pelvic floor muscle training included in a pregnancy exercise program is effective in primary prevention of urinary incontinence: a randomized controlled trial. Neurourology and Urodynamics 2014;33(1):67‐71. [NCT01578369; sr‐incont50396] [DOI] [PubMed] [Google Scholar]
- Agur WI, Steggles P, Waterfield M, Freeman RM. The long‐term effectiveness of antenatal pelvic floor muscle training: eight‐year follow up of a randomised controlled trial. BJOG 2008;115(8):985‐90. [27527] [DOI] [PubMed] [Google Scholar]; Reilly EIL, Freeman RM, Waterfield MR, Waterfield AE, Steggles P, Pedlar F. Can post partum stress incontinence be prevented? (Abstract). International Urogynecology Journal 2001;12 Suppl 3:1. [SR‐INCONT15712] [Google Scholar]; Reilly ETC, Freeman RM, Waterfield MR, Waterfield AE, Steggles P, Pedlar F. Prevention of postpartum stress incontinence in primigravidae with increased bladder neck mobility: a randomised controlled trial of antenatal pelvic floor exercises. BJOG 2002;109(1):68‐76. [SR‐INCONT12890] [DOI] [PubMed] [Google Scholar]; Reilly ETC, Pedler F, Steggles P, Waterfield AE, Freeman RM. Prevention of postpartum stress incontinence in at risk primigravidae (Abstract). International Urogynecology Journal and Pelvic Floor Dysfunction 1999;10 Suppl 1:2. [SR‐INCONT9837] [Google Scholar]; Udayasankar VJ, Steggles P, Freeman RM, Waterfield M, Adekanmi OA, Reilly ETC. Prevention of stress incontinence by ante‐natal pelvic floor exercises in primigravidae with bladder neck mobility: a three year follow‐up (Abstract). International Urogynaecology Journal 2002;13 Suppl 1:57‐8. [SR‐INCONT16343] [Google Scholar]
- Sampselle C, Miller J. Personal communication2006. ; Sampselle CM, Miller JM, Mims BL, Delancey JO, Ashton‐Miller JA, Antonakos CL. Effect of pelvic muscle exercise on transient incontinence during pregnancy and after birth. Obstetrics and Gynecology 1998;91(3):406‐12. [SR‐INCONT5452] [DOI] [PubMed] [Google Scholar]
- Sangsawang B, Sangsawang N. Is a 6‐week supervised pelvic floor muscle exercise program effective in preventing stress urinary incontinence in late pregnancy in primigravid women?: a randomized controlled trial. European Journal of Obstetrics, Gynecology, and Reproductive Biology 2016;197:103‐10. [sr‐incont70455] [DOI] [PubMed] [Google Scholar]
- Skelly J, Rush J, Eyles P, Burlock S, Morrow C, Fedorkow D. Postpartum urinary incontinence: regional prevalence and the impact of teaching pelvic muscle exercises to pregnant women with UI (Abstract number 552). 34th Annual Meeting of the International Continence Society and the International Urogynecology Association; 2004 Aug 23‐27; Paris. 2004. [Google Scholar]
- Sleep J, Grant A. Pelvic floor exercises in postnatal care. Midwifery 1987;3(4):158‐64. [SR‐INCONT2623] [DOI] [PubMed] [Google Scholar]
- Gustafsson MK, Stafne SN, Romundstad PR, Mørkved S, Salvesen K, Helvik AS. The effects of an exercise programme during pregnancy on health‐related quality of life in pregnant women: a Norwegian randomised controlled trial. BJOG2016; Vol. 123, issue 7:1152‐60. [sr‐incont69900] [DOI] [PubMed]; Hellenes OM, Vik T, Løhaugen GC, Salvesen KÅ, Stafne SN, Mørkved S, et al. Regular moderate exercise during pregnancy does not have an adverse effect on the neurodevelopment of the child. Acta Paediatrica 2015;104(3):285‐91. [sr‐incont69901] [DOI] [PubMed] [Google Scholar]; Mørkved S. Training during pregnancy ‐ effects of regular exercise during pregnancy in prevention of pregnancy‐related diseases and complications during labour. A randomised clinical trial. clinicaltrials.gov/show/NCT00476567 Date first received: 22 May 2007. [sr‐incont47816]; Salvesen KÅ, Stafne SN, Eggebo TM, Mørkved S. Does regular exercise in pregnancy influence duration of labor? A secondary analysis of a randomized controlled trial. Acta Obstetricia et Gynecologica Scandinavica 2014;93(1):73‐9. [sr‐incont61153] [DOI] [PubMed] [Google Scholar]; Songøygard KM, Stafne SN, Evensen KA, Salvesen KÅ, Vik T, Mørkved S. Does exercise during pregnancy prevent postnatal depression? A randomized controlled trial. Acta Obstetricia et Gynecologica Scandinavica 2012;91(1):62‐7. [sr‐incont69903] [DOI] [PubMed] [Google Scholar]; Stafne S, Salvesen K, Romundstad P, Torjusen I, Mørkved S. Does regular exercise including pelvic floor muscle training prevent urinary and anal incontinence during pregnancy? A randomised controlled trial. BJOG 2012;119(10):1270‐80. [sr‐incont45048] [DOI] [PubMed] [Google Scholar]; Stafne SN, Salvesen KÅ, Mørkved S. Does regular exercise in pregnancy increase lumbopelvic pain? (Abstract number RR‐PO‐312‐11‐Wed). Physiotherapy 2011a;97(Suppl S1):eS1171. [Google Scholar]; Stafne SN, Salvesen KÅ, Mørkved S. Does regular exercise in pregnancy prevent urinary incontinence? (Abstract number RR‐PL‐3377). Physiotherapy 2011b;97(Suppl S1):eS1170‐1. [Google Scholar]; Stafne SN, Salvesen KÅ, Romundstad PR, Eggebo TM, Carlsen SM, Mørkved S. Regular exercise during pregnancy to prevent gestational diabetes: a randomized controlled trial. Obstetrics and Gynecology 2012;119(1):29‐36. [sr‐incont69902] [DOI] [PubMed] [Google Scholar]; Stafne SN, Salvesen KÅ, Volloyhaug I, Mørkved S. Does a regular exercise program including pelvic floor muscle exercises prevent urinary incontinence in pregnancy? (Abstract number 100). Neurourology and Urodynamics 2011c;30(6):941‐2. [sr‐incont42181] [Google Scholar]
- Stothers L. A randomized controlled trial to evaluate intrapartum pelvic floor exercise as a method of preventing urinary incontinence (Abstract). Journal of Urology 2002;167(4 Suppl):106. [SR‐INCONT17623] [Google Scholar]
- Wen X‐H, Shi S‐Q, Wang J‐Y. Pelvic muscles exercise for postpartum stress urinary incontinence. China Practical Medicine 2010;5(15):72‐3. [sr‐incont70270] [Google Scholar]
- Wilson D, Herbison P, Borland M, Grant AM. A randomised controlled trial of physiotherapy treatment of postnatal urinary incontinence. 26th Congress of Obstetrics and Gynaecology; 1992 Jul 7‐10; Manchester (UK). 1992:162. [Google Scholar]; Wilson PD, Herbison GP. A randomized controlled trial of pelvic floor muscle exercises to treat postnatal urinary incontinence. International Urogynecology Journal and Pelvic Floor Dysfunction 1998;9(5):257‐64. [DOI] [PubMed] [Google Scholar]
- Woldringh C, Wijngaart M, Albers‐Heitner P, Lycklama a Nijeholt AAB, Lagro‐Janssen T. Pelvic floor muscle training is not effective in women with UI in pregnancy: a randomised controlled trial. International Urogynecology Journal and Pelvic Floor Dysfunction2007; Vol. 18, issue 4:383‐90. [DOI: 10.1007/s00192-006-0175-x] [DOI] [PubMed]
References to studies excluded from this review
- Agur W, Freeman R. Do antenatal pelvic floor training affect the outcome of labour? A randomised controlled trial (Abstract). Neurourology and Urodynamics 2005;24(5/6):510‐1. [SR‐INCONT20969] [DOI] [PubMed] [Google Scholar]
- Assis TR, Sa AC, Amaral WN, Batista EM, Formiga CK, Conde DM. The effect of an exercise program to strengthen pelvic floor muscles in multiparous women [Portuguese]. Revista Brasileira de Ginecologia e Obstetricia 2013;35(1):10‐5. [DOI] [PubMed] [Google Scholar]
- Barakat R, Perales M, Bacchi M, Coteron J, Refoyo I. A program of exercise throughout pregnancy. Is it safe to mother and newborn?. American Journal of Health Promotion 2014;29(1):2‐8. [DOI] [PubMed] [Google Scholar]
- Barakat R, Pelaez M, Cordero Y, Perales M, Lopez C, Coteron J, et al. Exercise during pregnancy protects against hypertension and macrosomia: randomized clinical trial. American Journal of Obstetrics and Gynecology 2016;214(5):649‐8. [DOI] [PubMed] [Google Scholar]
- Culligan P, Blackwell L, Murphy M, Ziegler C, Heit M. A blinded, sham‐controlled trial of postpartum extracorporeal magnetic innervation to restore pelvic muscle strength in primiparous patients (Abstract). Neurourology and Urodynamics 2004;23(5/6):451. [SR‐INCONT19008] [DOI] [PubMed] [Google Scholar]; Culligan PJ, Blackwell L, Murphy M, Ziegler C, Heit MH. A randomized, double‐blinded, sham‐controlled trial of postpartum extracorporeal magnetic innervation to restore pelvic muscle strength in primiparous patients. American Journal of Obstetrics and Gynecology 2005;192(5):1578‐82. [DOI] [PubMed] [Google Scholar]
- Dannecker C. The effect of the pelvic floor training device Epi‐No on the maternal pelvic floor function six months after childbirth ‐ follow‐up study of a randomised controlled trial [Einfluss des Geburtstrainers Epi‐No auf die mutterliche Beckenbodenfunktion sechs Monate nech Entbinding ‐ follow‐up einer prospektiven und randomisierten Studie]. Geburtshilfe und Frauenheilkunde 2004;64(11):1192‐8. [SR‐INCONT21149] [Google Scholar]
- Dias LA, Driusso P, Aita DL, Quintana SM, Bø K, Ferreira CH. Effect of pelvic floor muscle training on labour and newborn outcomes: a randomized controlled trial. Revista Brasileira de Fisioterapia 2011a;15(6):487‐93. [SRINCONT42964] [DOI] [PubMed] [Google Scholar]
- Dietz HP, Langer S, Kamisan Atan I, Shek KL, Caudwell‐Hall J, Guzman Rojas R. Does the Epi‐No prevent pelvic floor trauma? A multicentre randomised controlled trial (Abstract number 394). Neurourology and Urodynamics 2014;33(6):853‐5. [Google Scholar]
- Domingues MR, Bassani DG, Silva SG, Coll Cde V, Silva BG, Hallal PC. Physical activity during pregnancy and maternal‐child health (PAMELA): study protocol for a randomized controlled trial. Trials 2015;16:227. [DOI: 10.1186/s13063-015-0749-3] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dougherty MC, Abrams RM, Batich CD, Bishop KR, Gimptty P. Effect of exercise on the circumvaginal muscles (CVM) (Abstract). Neurourology and Urodynamics 1987;6(3):189‐90. [SR‐INCONT16393] [Google Scholar]; Dougherty MC, Bishop KR, Abrams RM, Batich CD, Gimotty PA. The effect of exercise on the circumvaginal muscles in postpartum women. Journal of Nurse‐Midwifery 1989;34(1):8‐14. [SR‐INCONT454] [DOI] [PubMed] [Google Scholar]
- Fynes M, Marshall K, Cassidy M, O'Connell R, O'Herlihy C. A prospective randomised study comparing the effect of augmented biofeedback with sensory biofeedback alone on faecal incontinence following obstetric trauma. 28th Annual Meeting of the International Continence Society (ICS); 1998 Sept 14‐17; Jerusalem, Israel1998:151. [SR‐INCONT5691] [DOI] [PubMed]; Fynes MM, Marshall K, Cassidy M, Behan M, Walsh D, O'Connell PR, et al. A prospective, randomized study comparing the effect of augmented biofeedback with sensory biofeedback alone on fecal incontinence after obstetric trauma. Diseases of the Colon and Rectum 1999;42(6):753‐8. [8121] [DOI] [PubMed] [Google Scholar]
- Golmakani N, Zare Z, Khadem N, Shareh H, Shakeri MT. The effect of pelvic floor muscle exercises program on sexual self‐efficacy in primiparous women after delivery. Iranian Journal of Nursing and Midwifery Research 2015;20(3):347‐53. [IRCT2013062313750N1; PMC4462060; sr‐incont67962] [PMC free article] [PubMed] [Google Scholar]; Zare Z, Golmakani N, Khadem N, Shareh H, Shakeri MT. The effect of pelvic floor muscle exercises on sexual quality of life and marital satisfaction in primiparous women after childbirth. Iranian Journal of Obstetrics, Gynecology and Infertility 2014;17(103):21‐32. [Google Scholar]
- Gouldthorpe H. A physiotherapy abdominal muscle assessment during and after pregnancy: Part 4 (Abstract). Australian and New Zealand Continence Journal. 9 2003; Vol. 9, issue 4:92. [SR‐INCONT17166]
- Hou S‐X. The clinical effects on biofeedback combined with electrical stimulation used in pelvic muscle recover therapy. Guide of China Medicine 2010;8(17):28‐9. [sr‐incont70279] [Google Scholar]
- Huang J. Effects of exercise of pelvic floor on childbirth outcome and pelvic floor function in primiparas. Hebei yi xue (Hebei Medicine) 2014;20(3):513‐6. [Google Scholar]
- Kamisan Atan I, Shek KL, Langer S, Guzman Rojas R, Caudwell‐Hall J, Daly JO, et al. Does the Epi‐No(©) birth trainer prevent vaginal birth‐related pelvic floor trauma? A multicentre prospective randomised controlled trial. BJOG 2016;123(6):995‐1003. [DOI] [PubMed] [Google Scholar]
- Lekskulchai O. Effect of antenatal pelvic floor exercises on bladder neck descent in nulliparous pregnant women (Abstract number 105). Neurourology and Urodynamics 2011;30(6):949‐50. [SRINCONT42182] [Google Scholar]; Lekskulchai O, Wanichsetakul P. Effect of pelvic floor muscle training (PFMT) during pregnancy on bladder neck descend and delivery. Journal of the Medical Association of Thailand 2014;97(Suppl 8):S156‐63. [PubMed] [Google Scholar]
- Li Y, Liu H‐S, Guo X‐J, Mai F‐M. Effect of functional exercise of prenatal pelvic floor muscles on pregnancy outcome. Xian Dai Sheng Wu Yi Xue Jin Zhan (Progress in Modern Biomedicine) 2010;10(11):2129‐31. [Google Scholar]
- Liu Y‐L, Zhou Y‐H, Ding H, Peng J, Chen S‐Q, Zhang J‐P. Effect of pelvic muscle training on pelvic floor function during pregnancy. Zhongshan da xue xue bao. Yi xue ke xue ban (Journal of Sun Yat‐sen University. Medical Sciences) 2013;34(5):777‐81. [sr‐incont70267] [Google Scholar]
- Mahmoodi F, Mobaraki A. Assessment of effects of Kegel exercises on reduction of perineal pain after episiotomy in primiparous women. Iranian Journal of Obstetrics, Gynecology and Infertility 2014;17(95):18‐25. [Google Scholar]
- Mahony R, Malone P, Nalty J, Cassidy M, O'Connell PR, O'Herlihy C. Prospective randomized comparison of intra‐anal electromyographic biofeedback and intra‐anal electromyographic biofeedback augmented with electrical stimulation of the anal sphincter. American Journal of Obstetrics and Gynecology 2003;189(6 Suppl):71. [DOI] [PubMed] [Google Scholar]; Mahony RT, Malone PA, Nalty J, Behan M, O'Connell PR, O'Herlihy C. Randomized clinical trial of intra‐analysis electromyographic biofeedback physiotherapy with intra‐anal electromyographic biofeedback augmented with electrical stimulation of the anal sphincter in the early treatment of postpartum fecal incontinence. American Journal of Obstetrics and Gynecology 2004;191(3):885‐90. [DOI] [PubMed] [Google Scholar]
- Mason M. A multicentre study to evaluate different pelvic floor exercise regimes. National Research Register1999. [SR‐INCONT6662]
- Mason L, Roe B, Wong H, Davies J, Bamber J. The role of antenatal pelvic floor muscle exercises in prevention of postpartum stress incontinence: a randomised controlled trial. Journal of Clinical Nursing 2010;19(19‐20):2777‐86. [SRINCONT40375] [DOI] [PubMed] [Google Scholar]
- Morin M, Kruger J, Wong V, Girard I, Sherburn M, Dumoulin C. Effect of physiotherapy on pelvic floor morphometry in women with and without avulsion injury of the puborectalis muscle after vaginal delivery: a randomised pilot study (Abstract number 15). Neurourology and Urodynamics 2015;34(S3):S39‐40. [Google Scholar]
- Barakat R, Perales M. Effect of a supervised exercise program during whole pregnancy on outcomes and level of depression. A randomized controlled trial. clinicaltrials.gov/show/NCT01696201 Date first received: 28 September 2012.
- Barakat R, Perales M. Effect of a specific exercise program during whole pregnancy on fetal heart rate response to maternal effort in third trimester. A randomised controlled trial. clinicaltrials.gov/show/NCT01723293 Date first received: 7 November 2012.
- Barakat R, Perales M. Effect of a supervised exercise program in obese and overweight pregnant women on outcomes and level of depression. A randomized controlled trial. clinicaltrials.gov/show/NCT01753622 Date first received: 20 December 2012.
- Nielsen CA, Sigsgaard I, Olsen M, Tolstrup M, Danneskiold‐Samsoee B, Bock JE. Trainability of the pelvic floor. A prospective study during pregnancy and after delivery. Acta Obstetricia et Gynecologica Scandinavica 1988;67(5):437‐40. [SR‐INCONT7395] [DOI] [PubMed] [Google Scholar]
- Norton P, Baker J. Randomized prospective trial of vaginal cones versus Kegel exercises in postpartum primiparous women. 11th Annual Meeting of the American Urogynecology Society; 1990 Oct 31‐Nov 3; Tarpon Springs (FL). 1990. [SR‐INCONT14572] [Google Scholar]; Norton P, Baker J. Randomized prospective trial of vaginal cones vs Kegel exercises in postpartum primiparous women (Abstract). Neurourology and Urodynamics 1990;9(4):434‐5. [SR‐INCONT5116] [Google Scholar]
- Oblasser C, McCourt C, Hanzal E, Christie J. Vibrating vaginal balls to improve pelvic floor muscle performance in women after childbirth: a protocol for a randomised controlled feasibility trial. Journal of Advanced Nursing 2016;72(4):900‐14. [DOI] [PubMed] [Google Scholar]
- Okido MM, Valeri FL, Martins WP, Ferreira CH, Duarte G, Cavalli RC. Assessment of foetal wellbeing in pregnant women subjected to pelvic floor muscle training: a controlled randomised study. International Urogynecology Journal 2015;26(10):1475‐81. [DOI] [PubMed] [Google Scholar]
- Perales M, Santos‐Lozano A, Sanchis‐Gomar F, Luaces M, Pareja‐Galeano H, Garatachea N, et al. Maternal cardiac adaptations to a physical exercise program during pregnancy. Medicine and Science in Sports and Exercise 2016;48(5):896‐906. [DOI] [PubMed] [Google Scholar]
- Ruiz JR, Perales M, Pelaez M, Lopez C, Lucia A, Barakat R. Supervised exercise‐based intervention to prevent excessive gestational weight gain: a randomized controlled trial. Mayo Clinic Proceedings 2013;88(12):1388‐97. [DOI] [PubMed] [Google Scholar]
- Siva PR, Kokila V, Kanchana MK, Suresh KS. Effectiveness of antenatal motor relearning approach of diaphragm, deep abdominal and pelvic floor muscles versus Kegels exercises on postpartum pelvic floor muscle strength. Indian Journal of Physiotherapy and Occupational Therapy 2014;8(1):193‐7. [sr‐incont67960] [Google Scholar]
- Taskin O, Wheeler JM, Yalcinoglu AI, Coksenim S. The effects of episiotomy and Kegel exercises on postpartum pelvic relaxation: a prospective controlled study. Journal of Gynecologic Surgery 1996;12(2):123‐7. [SRINCONT18347] [Google Scholar]
- Thorp JM, Stephenson H, Jones LH, Cooper G. Pelvic floor (Kegel) exercises: a pilot study in nulliparous women. International Urogynecology Journal 1994;5:86‐9. [Google Scholar]
- Wang X, Li G‐Y, Deng M‐L. Effect of persistent guidance of pelvic floor muscle training on the delivery outcome and pelvic muscle strength. Zhonghua Hu Li za Zhi [Chinese Journal of Nursing] 2013;48(4):308‐10. [Google Scholar]; Wang X, Li G‐Y, Deng M‐L. Pelvic floor muscle training as a persistent nursing intervention: effect on delivery outcome and pelvic floor myodynamia. International Journal of Nursing Sciences 2014;1(1):48‐52. [Google Scholar]
- Zhu X‐M, Jiang L‐Q. Effect of exercises and electrical stimulation of pelvic floor muscles on postpartum incontinence. Journal of Nursing (China) 2012;19(2A):49‐51. [Google Scholar]
References to studies awaiting assessment
- Han V, Hyakutake M, Cundiff G, Koenig N, Baerg L, Lee T, et al. Pregnancy‐associated pelvic floor health knowledge and reduction of symptoms: the PREPARED trial (Abstract number O‐GYN‐JM‐017). Journal of Obstetrics and Gynaecology Canada 2016;38(5):487. [DOI] [PubMed] [Google Scholar]; Koenig N. PREgnancy‐associated Pelvic Floor Health Knowledge And REDuction of Symptoms: the PREPARED trial. clinicaltrials.gov/show/NCT02947282 Date first received: 27 October 2016. [DOI] [PubMed]
- Johannessen HH, Wibe A, Stordahl A, Sandvik L, Mørkved S. Do pelvic floor muscle exercises reduce postpartum anal incontinence? A randomised controlled trial. BJOG 2017;124(4):686‐94. [DOI] [PubMed] [Google Scholar]
- Longo F, Montironi PL, Bar E, Frigerio S. Effects of pelvic floor muscle training during pregnancy. Techniques in Coloproctology 2013;17(1):143‐4. [Google Scholar]
- Oakley SH, Ghodsi VC, Crisp CC, Estanol MV, Westermann LB, Novicki KM, et al. Effects of physical therapy on pelvic floor symptoms and quality of life in postpartum women following severe perineal trauma: a randomized controlled trial. Female Pelvic Medicine & Reconstructive Surgery 2015;21(5 Suppl 1):S18. [Google Scholar]; Oakley SH, Ghodsi VC, Crisp CC, Estanol MV, Westermann LB, Novicki KM, et al. Impact of pelvic floor physical therapy on quality of life and function after obstetric anal sphincter injury: a randomized controlled trial. Female Pelvic Medicine and Reconstructive Surgery 2016;22:205‐13. [DOI] [PubMed] [Google Scholar]
- Sun Z, Zhu L, Lang J, Zhang Y, Liu G, Chen X, et al. Postpartum pelvic floor rehabilitation on prevention of female pelvic floor dysfunction: a multicenter prospective randomized controlled study. [Chinese]. Chung‐Hua Fu Chan Ko Tsa Chih [Chinese Journal of Obstetrics and Gynecology] 2015;50(6):420‐7. [PubMed] [Google Scholar]
- Sut HK, Kaplan PB. Effect of pelvic floor muscle exercise on pelvic floor muscle activity and voiding functions during pregnancy and the postpartum period. Neurourology & Urodynamics 2016;35(3):417‐22. [DOI] [PubMed] [Google Scholar]
- Wilson J. Evaluating Web‐based Pelvic Floor Muscle Education for Pregnant Women [PhD thesis]. Fremantle (Australia): The University of Notre Dame (Fremantle Campus), 2015. [Google Scholar]
- Zhou Y‐H. The Function of the Pregnancy on the Female Pelvic Floor and Study on the Effect of Pelvic Floor through Pelvic Floor Muscle Training During the Pregnancy [Masters thesis]. Guangzhou, Guangdong (China): Sun Yat‐Sen University, 2009. [Google Scholar]
References to ongoing studies
- Ferreira CHJ, Cavalcanti DLC. Effects of pelvic floor muscle training on pelvic floor muscle function in women during their first pregnancies measured by perineometer. anzctr.org.au/ACTRN12609001005246.aspx Date first received: 10 October 2009.
- Berghmans B. Long term effects of multidisciplinary assessment and pre‐ and post partum Pelvic Floor Muscle Group Treatment in primigravid with stress urinary incontinence compared to care‐as‐usual: a randomised controlled trial ‐ motherfit. trialregister.nl/trialreg/admin/rctview.asp?TC=5971 Date first received: 18 July 2016.
- Buen M. Clinical trial: influence of the practice of Pilates on the incidence of urinary incontinence, perineal strength low back pain in the third trimester. ensaiosclinicos.gov.br/rg/RBR‐4wkr8y/ Date first received: 9 April 2014.
- Haruna M, Asai Y. Effect of postpartum pelvic floor muscle training with ultrasound biofeedback on recovery of pelvic floor muscle function: a randomized controlled trial. UMIN Clinical Trials Registry (UMIN‐CTR) (available at: umin.ac.jp/ctr/index.htm) Date first received: 8 December 2014.
- Miheso J, Ngugi S. Effect of pelvic floor muscle training among pregnant black African population on the risk of postpartum urinary incontinence, a single blind randomized control trial. Pan African Clinical Trials Registry (PACTR) (available at: pactr.org) Date first received: 22 May 2014. ; Ngugi S. Effect of Pelvic Floor Muscle Training Among Pregnant Black African Population on the Risk of Postpartum Urinary Incontinence, a Single Blind Randomized Control Trial [Masters dissertation]. Nairobi (Kenya): Aga Khan University (Nairobi Campus), 2015. [Google Scholar]
- Garnaes KK, Mørkved S, Salvesen O, Moholdt T. Exercise training and weight gain in obese pregnant women: a randomized controlled trial (ETIP Trial). PLoS Medicine 2016;13(7):e1002079. [DOI] [PMC free article] [PubMed] [Google Scholar]; Moholdt TT, Salvesen K, Ingul CB, Vik T, Oken E, Mørkved S. Exercise training in pregnancy for obese women (ETIP): study protocol for a randomised controlled trial. Trials 2011;12:154. [DOI: 10.1186/1745-6215-12-154] [DOI] [PMC free article] [PubMed] [Google Scholar]; NCT01243554, Moholdt TT, Mørkved S. Exercise training in pregnancy. Good for the mother ‐ good for the child?. clinicaltrials.gov/show/NCT01243554 Date first received: 18 November 2010.
- Sampselle C, Davis CK. PERL 4: Promoting Effective Recovery from Labour. Self‐care to prevent birth‐related urinary incontinence in diverse women. clinicaltrials.gov/show/NCT00763984 Date first received: 1 October 2008.
- Karp D, Huber SA, Martinuzzi K. Reducing perinatal anal incontinence through early pelvic floor muscle training: a prospective pilot study. clinicaltrials.gov/show/NCT02270008 Date first received: 21 October 2014.
- Lewicky‐Gaupp C, Alverdy A. Bump on the ball: impact of a prenatal exercise & education program on birth outcomes & maternal quality of life. clinicaltrials.gov/show/NCT02334397 Date first received: 8 January 2015.
- Barakat RO, Vargas Terrones M. Effect of physical exercise program on fetoplacental growth: a randomized controlled trial. clinicaltrials.gov/show/NCT02420288 Date first received: 17 April 2015.
- Steingrimsdottir T, Geirsson RT, Bø K. Obstetric perineal trauma, pelvic floor symptoms and early physiotherapy intervention. clinicaltrials.gov/show/NCT02682212 Date first received: 15 February 2016.
- Dufour S. Use of iball mobile health technology in pelvic floor muscle training in the postpartum period: a pilot mixed methods study. clinicaltrials.gov/show/NCT02865954 Date first received: 15 August 2016.
- Sacomori C, Sperandio F. Study about the influence of pelvic floor exercises orientation regarding urinary loss prevention on postpartum period. ensaiosclinicos.gov.br/rg/RBR‐53wq87/ Date first received: 7 October 2011.
- Schreiner L. Impact of pelvic floor physiotherapy during pregnancy in urinary incontinence and delivery. ensaiosclinicos.gov.br/rg/RBR‐8nv3fg/ Date first received: 2 July 2016.
- Velez‐Sanchez D, Veloz MG. Perineal muscle training versus usual prenatal care in the incidence of avulsion of the levator ani muscle at first birth of Mexican women: randomized control trial. clinicaltrials.gov/show/NCT02513420 Date first received: 31 July 2015.
Additional references
- Abrams P, Andersson K‐E, Apostolidis A, Birder L, Bliss D, Brubaker L, et al. Evaluation and treatment of urinary incontinence, pelvic organ prolapse and faecal incontinence: recommendations of the International Scientific Committee, 6th International Consultation on Incontinence. In: Abrams P, Cardozo L, Wagg A, Wein A editor(s). Incontinence: 6th International Consultation on Incontinence, Tokyo, September 2016. 6th Edition. Vol. 1, Bristol (UK): International Continence Society (ICS) and International Consultation on Urological Diseases (ICUD), 2017:2549‐619. [Google Scholar]
- Atkins D, Best D, Briss PA, Eccles M, Falck‐Ytter Y, Flottorp S, and GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ 2004;328(7454):1490‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Avery K, Donovan J, Peters TJ, Shaw C, Gotoh M, Abrams P. ICIQ: a brief and robust measure for evaluating the symptoms and impact of urinary incontinence. Neurourology and Urodynamics 2004;23:322‐30. [DOI] [PubMed] [Google Scholar]
- Avery KN, Bosch JL, Gotoh M, Naughton M, Jackson S, Radley SC, et al. Questionnaires to assess urinary and anal incontinence: review and recommendations. Journal of Urology 2007;177:39‐49. [DOI] [PubMed] [Google Scholar]
- Bols EM, Hendriks EJ, Berghmans BC, Baeten CG, Nijhuis JG, Bie RA. A systematic review of etiological factors for postpartum fecal incontinence. Acta Obstetricia et Gynecologica Scandinavica 2010;89(3):302‐14. [DOI] [PubMed] [Google Scholar]
- Brown SJ, Gartland D, Donath S, MacArthur C. Fecal incontinence during the first 12 months postpartum. Complex causal pathways and implications for clinical practice. Obstetrics and Gynecology 2012;119:240‐9. [DOI] [PubMed] [Google Scholar]
- Bø K, Hagen RH, Kvarstein B, Jørgensen J, Larsen S. Pelvic floor muscle exercise for the treatment of female stress urinary incontinence. III. Effects of two different degrees of pelvic floor muscle exercises. Neurourology and Urodynamics 1990;9:489‐502. [Google Scholar]
- Bø K. Pelvic floor muscle exercise for the treatment of stress urinary incontinence. International Urogynecology Journal 1995;6:282‐91. [Google Scholar]
- Bø K, Talseth T, Holme I. Single blind, randomised controlled trial of pelvic floor exercise, electrical stimulation, vaginal cones, and no treatment in management of genuine stress incontinence. BMJ 1999;318:487‐93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bø K. Pelvic floor muscle training is effective in treatment of female stress urinary incontinence, but how does it work?. International Urogynecology Journal and Pelvic Floor Dysfunction 2004;15:76‐84. [DOI] [PubMed] [Google Scholar]
- Bø K. Measurement of pelvic floor muscle function and strength, and pelvic organ prolapse. In: Bø K, Berghmans B, Mørkved S, Kampen M editor(s). Evidence‐based physical therapy for the pelvic floor bridging science and clinical practice. 2nd Edition. London: Elsevier Health Sciences UK, 2014:44‐109. [Google Scholar]
- Du Y, Xu L, Ding L, Wang Y, Wang Z. The effect of antenatal pelvic floor muscle training on labor and delivery outcomes: a systematic review with meta‐analysis. International Urogynecology Journal 2015;26:1415‐27. [DOI] [PubMed] [Google Scholar]
- Dumoulin C, Hay‐Smith EJC, Mac Habee‐Seguin G. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database of Systematic Reviews 2014, Issue 5. [DOI: 10.1002/14651858.CD005654.pub3] [DOI] [PubMed] [Google Scholar]
- Dumoulin C, Adewuyi T, Booth J, Bradley C, Burgio K, Hagen S, et al. Adult conservative management. In: Abrams P, Cardozo L, Wagg A, Wein A editor(s). Incontinence: 6th International Consultation on Incontinence, Tokyo, September 2016. 6th Edition. Vol. 1, Bristol, UK: International Continence Society (ICS) and International Consultation on Urological Diseases (ICUD), 2017:1443‐628. [Google Scholar]
- Durnea CM, Khashan AS, Kenny LC, Durnea UA, Dornan JC, O'Sullivan SM, et al. What is to blame for postnatal pelvic floor dysfunction in primiparous women‐pre‐pregnancy or intrapartum risk factors?. European Journal of Obstetrics and Gynecology and Reproductive Biology 2017;214:36‐43. [DOI] [PubMed] [Google Scholar]
- Eason E, Labrecque M, Marcous S, Mondor M. Anal incontinence after childbirth. CMAJ 2002;166(3):326‐30. [PMC free article] [PubMed] [Google Scholar]
- Foldspang A, Mommsen S, Djurhuus JC. Prevalent urinary incontinence as a correlate of pregnancy, vaginal childbirth, and obstetric techniques. American Journal of Public Health 1999;89:209‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frawley HC, Dean SG, Slade SC, Hay‐Smith EJC. Is pelvic‐floor muscle training a physical therapy or a behavioural therapy? A call to name and report the physical, cognitive, and behavioural elements. Physical Therapy 2017;97(4):425‐37. [DOI] [PubMed] [Google Scholar]
- Gartland D, Donath S, MacArthur C, Brown SJ. The onset, recurrence and associated obstetric risk factors for urinary incontinence in the first 18 months after a first birth: an Australian nulliparous cohort study. BJOG 2012;119:1361‐9. [DOI] [PubMed] [Google Scholar]
- Gartland D, MacArthur C, Woolhouse H, McDonald E, Brown SJ. Frequency, severity and risk factors for urinary and faecal incontinence at 4 years postpartum: a prospective cohort. BJOG 2016;123:1203‐11. [DOI] [PubMed] [Google Scholar]
- Gillard S, Shamley D. Factors motivating women to commence and adhere to pelvic floor muscle exercises following a perineal tear at delivery: the influence of experience. Journal of the Association of Chartered Physiotherapists in Women's Health 2010;106:5‐18. [Google Scholar]
- McMaster University (developed by Evidence Prime Inc). GRADEpro GDT. Version 16 February 2017. Hamilton (ON): GRADE Working Group, McMaster University, 2015.
- Gyhagen M, Bullarbo M, Nielsen TF, Milsom I. A comparison of the long‐term consequences of vaginal delivery versus caesarean section on the prevalence, severity and bothersomeness of urinary incontinence subtypes: a national cohort study in primiparous women. BJOG 2013;120:1548‐55. [DOI] [PubMed] [Google Scholar]
- Handa VL, Zyczynski HM, Burgio KL, Fitzgerald MP, Borello‐France D, Janz NK, et al. The impact of fecal and urinary incontinence on quality of life 6 months after childbirth. American Journal of Obstetrics and Gynecology 2007;197(6):636.e1‐e6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haskell WL, Lee IM, Pate RR, Powell KE, Blair SN, Franklin BA, et al. American College of Sports Medicine, American Heart Association. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Circulation 2007;28:1081‐93. [DOI] [PubMed] [Google Scholar]
- Hensrud DD. Clinical preventive medicine in primary care: background and practice: 1. Rationale and current preventive practices. Mayo Clinic Proceedings 2000;75:165‐72. [DOI] [PubMed] [Google Scholar]
- Herbert RD, Bø K. Analysis of quality of interventions in systematic reviews. BMJ 2005;331(7515):507‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Higgins JPT, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
- Imamura M, Abrams P, Bain C, Buckley B, Cardozo L, Cody J, et al. Systematic review and economic modelling of the effectiveness and cost‐effectiveness of non‐surgical treatments for women with stress urinary incontinence. Health Technology Assessment 2010;14(40):1‐188, iii‐iv. [DOI: 10.3310/hta14400] [DOI] [PubMed] [Google Scholar]
- Johannessen HH, Wibe A, Stordahl A, Sandvik L, Backe B, Mørkved S. Prevalence and predictors of anal incontinence during pregnancy and 1 year after delivery: a prospective cohort study. BJOG 2016;121:269‐80. [DOI] [PubMed] [Google Scholar]
- Johanson JF, Lafferty J. Epidemiology of fecal incontinence: the silent affliction. American Journal of Gastroenterology 1996;91(1):33‐6. [PubMed] [Google Scholar]
- Kegel AH. Progressive resistance exercise in the functional restoration of the perineal muscles. American Journal of Obstetrics and Gynecology 1948;56:238‐48. [DOI] [PubMed] [Google Scholar]
- Koumantakis GA, Watson PJ, Oldham JA. Trunk muscle stabilization training plus general exercise versus general exercise only: randomized controlled trial of patients with recurrent low back pain. Physical Therapy 2005;85:209‐25. [PubMed] [Google Scholar]
- MacArthur C, Glazener CM, Wilson PD, Herbison GP, Gee H, Lang GD, et al. Obstetric practice and faecal incontinence three months after delivery. BJOG 2001;108(7):678‐83. [DOI] [PubMed] [Google Scholar]
- MacArthur C, Wilson D, Herbison P, Lancashire RJ, Hagen S, Toozs‐Hobson P, et al. on behalf of the ProLong study group. Faecal incontinence persisting after childbirth: a 12 year longitudinal study. BJOG 2013;120:169‐79. [DOI] [PubMed] [Google Scholar]
- Mason L, Glenn S, Walton I, Hughes C. Do women practise pelvic floor exercises during pregnancy or following delivery?. Physiotherapy 2001;87(12):662‐70. [DOI] [PubMed] [Google Scholar]
- Miller JM, Sampselle C, Ashton‐Miller J, Hong GR, Delancey JO. Clarification and confirmation of the Knack maneuver: the effect of volitional pelvic floor muscle contraction to preempt expected stress incontinence. International Urogynecology Journal and Pelvic Floor Dysfunction 2008;19(6):773‐82. [SR‐INCONT27428] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Milsom I, Altman D, Cartwright R, Lapitan MC, Nelson R, Sjöström S, et al. Epidemiology of urinary incontinence (UI) and other lower urinary tract symptoms (LUTS), pelvic organ prolapse (POP) and anal incontinence (AI). In: Abrams P, Cardozo L, Wagg A, Wein A editor(s). Incontinence: 6th International Consultation on Incontinence, Tokyo, September 2016. 6th Edition. Vol. 1, Bristol (UK): International Continence Society (ICS) and International Consultation on Urological Diseases (ICUD), 2017:1‐141. [Google Scholar]
- Moher D, Pham B, Jones A, Cook DJ, Jadad AR, Moher M, et al. Does quality of reporting of randomised trials affect estimates of intervention efficacy reported in meta‐analyses?. Lancet 1998;352(9128):609‐13. [DOI] [PubMed] [Google Scholar]
- Moore GF, Audrey S, Barker M, Bond L, Bonell C, Hardeman W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015;350:h1258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mørkved S, Bø K. Effect of post partum pelvic floor muscle exercise in prevention and treatment of urinary incontinence. International Urogynecology Journal 1997;8:217‐22. [DOI] [PubMed] [Google Scholar]
- Mørkved S, Bø K. Effect of pelvic floor muscle training during pregnancy and after childbirth on prevention and treatment of urinary incontinence: a systematic review. British Journal of Sports Medicine 2014;48(4):299‐310. [DOI] [PubMed] [Google Scholar]
- Norton C, Cody JD. Biofeedback and/or sphincter exercises for the treatment of faecal incontinence in adults. Cochrane Database of Systematic Reviews 2012, Issue 7. [DOI: 10.1002/14651858.CD002111.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nygaard IE, Clark E, Clark L, Egger MJ, Hitchcock R, Hsu Y, et al. Physical and cultural determinants of postpartum pelvic floor support and symptoms following vaginal delivery: a protocol for a mixed‐methods prospective cohort study. BMJ Open 2017;7(1):e014252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nyström E, Sjöström M, Stenlund H, Samuelsson E. ICIQ symptom and quality of life instruments measure clinically relevant improvements in women with stress urinary incontinence. Neurourology and Urodynamics 2015;34:747‐51. [DOI] [PubMed] [Google Scholar]
- Pizzoferrato AC, Fauconnier A, Quiboeuf E, Morel K, Schaal JP, Fritel X. Urinary incontinence 4 and 12 years after first delivery: risk factors associated with prevalence, incidence, remission, and persistence in a cohort of 236 women. Neurourology and Urodynamics 2014;33(8):1229‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollack J, Nordenstam J, Brismar S, Lopez A, Altman D, Zetterstrom J. Anal incontinence after vaginal delivery: a five‐year prospective cohort study. Obstetrics and Gynecology 2004;104(6):1397‐402. [DOI] [PubMed] [Google Scholar]
- Quiboeuf E, Saurel‐Cubizolles MJ, Fritel X, EDEN Mother‐Child Cohort Study Group. Trends in urinary incontinence in women between 4 and 24 months postpartum in the EDEN cohort. BJOG 2016;123(7):1222‐8. [DOI] [PubMed] [Google Scholar]
- Thomson Reuters. Reference Manager Professional Edition Version 12. New York (NY): Thomson Reuters, 2012.
- Rogers RG, Ninivaggio C, Gallagher K, Borders AN, Qualls C, Leeman LM. Pelvic floor symptoms and quality of life changes during first pregnancy: a prospective cohort study. International Urogynecology Journal2017; Vol. 28, issue 11:1701‐7. [DOI: 10.1007/s00192-017-3330-7] [DOI] [PMC free article] [PubMed]
- Rortveit G, Daltveit AK, Hannestad YS, Hunskaar S, the Norwegian EPICONT study. Urinary incontinence after vaginal delivery or caesarean section. New England Journal of Medicine 2003;348(10):900‐7. [DOI] [PubMed] [Google Scholar]
- Rortveit G, Daltveit AK, Hannestad YS, Hunskaar, S. Vaginal delivery parameters and urinary incontinence: the Norwegian EPICONT study. American Journal of Obstetrics and Gynecology 2003;189(5):1269‐74. [DOI] [PubMed] [Google Scholar]
- Sandvik H, Hunskaar S, Seim A, Hermstad R, Vanvik A, Bratt H. Validation of a severity index in female urinary incontinence and its implementation in an epidemiological survey. Journal of Epidemiology and Community Health 1993;47(6):497‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shumaker SA, Wyman JF, Uebersax JS, McClish D, Fantl JA. Health‐related quality of life measures for women with urinary incontinence: the Incontinence Impact Questionnaire and the Urogenital Distress Inventory. Quality of Life Research 1994;3:291. [DOI] [PubMed] [Google Scholar]
- Signorello LB, Harlow BL, Chekos AK, Repke JT. Midline episiotomy and anal incontinence: retrospective cohort study. BMJ 2000;320(7227):86‐90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sultan AH, Monga AK, Kumar D, Stanton SL. Primary repair of obstetric anal sphincter rupture using the overlap technique. British Journal of Obstetrics and Gynaecology 1999;106(3):318‐23. [DOI] [PubMed] [Google Scholar]
- Svare JA, Hansen BB, Lose G. Risk factors for urinary incontinence 1 year after first vaginal delivery in a cohort of primiparous Danish women. International Urogynecology Journal 2014;25:47‐51. [DOI] [PubMed] [Google Scholar]
- Svare JA, Hansen BB, Lose G. Prevalence of anal incontinence during pregnancy and 1 year after delivery in a cohort of primiparous women and a control group of nulliparous women. Acta Obstetricia et Gynecologica Scandinavica 2016;95:920‐5. [DOI] [PubMed] [Google Scholar]
- Thom DH, Rortveit G. Prevalence of postpartum urinary incontinence: a systematic review. Acta Obstetricia et Gynecologica Scandinavica 2010;89(12):1511‐22. [DOI] [PubMed] [Google Scholar]
- Viktrup L, Rortveit B, Lose G. Risk of stress urinary incontinence twelve years after the first pregnancy and delivery. Obstetrics and Gynecology 2006;108(2):248‐54. [DOI] [PubMed] [Google Scholar]
- Wagner TH, Moore KH, Subak LL, Wachter S, Dudding T. Economics of urinary & faecal incontinence, and prolapse. In: Abrams P, Cardozo L, Wagg A, Wein A editor(s). Incontinence: 6th International Consultation on Incontinence, Tokyo, September 2016. 6th Edition. Vol. 1, Bristol (UK): International Continence Society (ICS) and International Consultation on Urological Diseases (ICUD), 2017:2479‐511. [Google Scholar]
- Ware JE, Snow KK, Kosinski M, Gaudek B. SF‐36 Health Survey Manual and Interpretation Guide. Boston (MA): New England Medical Centre, 1993. [Google Scholar]
- Wesnes SL, Rortveit G, Bø K, Hunskaar S. Urinary incontinence during pregnancy. Obstetrics and Gynecology 2007;109(4):922‐8. [DOI] [PubMed] [Google Scholar]
- Wesnes SL, Hannestad Y, Rortveit G. Delivery parameters, neonatal parameters and incidence of urinary incontinence 6 months postpartum: a cohort study. Acta Obstetrica et Gynecologica Scandinavica2017; Vol. 96, issue 10:1214‐22. [DOI: 10.1111/aogs.13183; PUBMED: 28626856] [DOI] [PubMed]
- Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica 1983;67:361‐70. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
- Boyle R, Hay‐Smith EJC, Cody JD, Mørkved S. Pelvic floor muscle training for prevention and treatment of urinary and faecal incontinence in antenatal and postnatal women. Cochrane Database of Systematic Reviews 2012, Issue 10. [DOI: 10.1002/14651858.CD007471.pub2] [DOI] [PubMed] [Google Scholar]
- Hay‐Smith J, Mørkved S, Fairbrother KA, Herbison GP. Pelvic floor muscle training for prevention and treatment of urinary and faecal incontinence in antenatal and postnatal women. Cochrane Database of Systematic Reviews 2008, Issue 4. [DOI: 10.1002/14651858.CD007471] [DOI] [PubMed] [Google Scholar]