

Abstract
Background
Computer users frequently complain about problems with seeing and functioning of the eyes. Asthenopia is a term generally used to describe symptoms related to (prolonged) use of the eyes like ocular fatigue, headache, pain or aching around the eyes, and burning and itchiness of the eyelids. The prevalence of asthenopia during or after work on a computer ranges from 46.3% to 68.5%. Uncorrected or under‐corrected refractive error can contribute to the development of asthenopia. A refractive error is an error in the focusing of light by the eye and can lead to reduced visual acuity. There are various possibilities for optical correction of refractive errors including eyeglasses, contact lenses and refractive surgery.
Objectives
To examine the evidence on the effectiveness, safety and applicability of optical correction of refractive error for reducing and preventing eye symptoms in computer users.
Search methods
We searched the Cochrane Central Register of Controlled Trials (CENTRAL); PubMed; Embase; Web of Science; and OSH update, all to 20 December 2017. Additionally, we searched trial registries and checked references of included studies.
Selection criteria
We included randomised controlled trials (RCTs) and quasi‐randomised trials of interventions evaluating optical correction for computer workers with refractive error for preventing or treating asthenopia and their effect on health related quality of life.
Data collection and analysis
Two authors independently assessed study eligibility and risk of bias, and extracted data. Where appropriate, we combined studies in a meta‐analysis.
Main results
We included eight studies with 381 participants. Three were parallel group RCTs, three were cross‐over RCTs and two were quasi‐randomised cross‐over trials. All studies evaluated eyeglasses, there were no studies that evaluated contact lenses or surgery. Seven studies evaluated computer glasses with at least one focal area for the distance of the computer screen with or without additional focal areas in presbyopic persons. Six studies compared computer glasses to other types of glasses; and one study compared them to an ergonomic workplace assessment. The eighth study compared optimal correction of refractive error with the actual spectacle correction in use. Two studies evaluated computer glasses in persons with asthenopia but for the others the glasses were offered to all workers regardless of symptoms. The risk of bias was unclear in five, high in two and low in one study. Asthenopia was measured as eyestrain or a summary score of symptoms but there were no studies on health‐related quality of life. Adverse events were measured as headache, nausea or dizziness. Median asthenopia scores at baseline were about 30% of the maximum possible score.
Progressive computer glasses versus monofocal glasses One study found no considerable difference in asthenopia between various progressive computer glasses and monofocal computer glasses after one‐year follow‐up (mean difference (MD) change scores 0.23, 95% confidence interval (CI) −5.0 to 5.4 on a 100 mm VAS scale, low quality evidence). For headache the results were in favour of progressive glasses.
Progressive computer glasses with an intermediate focus in the upper part of the glasses versus other glasses In two studies progressive computer glasses with intermediate focus led to a small decrease in asthenopia symptoms (SMD −0.49, 95% CI −0.75 to −0.23, low‐quality evidence) but not in headache score in the short‐term compared to general purpose progressive glasses. There were similar small decreases in dizziness. At medium term follow‐up, in one study the effect size was not statistically significant (SMD −0.64, 95% CI −1.40 to 0.12). The study did not assess adverse events.
Another study found no considerable difference in asthenopia between progressive computer glasses and monofocal computer glasses after one‐year follow‐up (MD change scores 1.44, 95% CI −6.95 to 9.83 on a 100 mm VAS scale, very low quality evidence). For headache the results were inconsistent.
Progressive computer glasses with far‐distance focus in the upper part of the glasses versus other glasses One study found no considerable difference in number of persons with asthenopia between progressive computer glasses with far‐distance focus and bifocal computer glasses after four weeks' follow‐up (OR 1.00, 95% CI 0.40 to 2.50, very low quality evidence). The number of persons with headache, nausea and dizziness was also not different between groups.
Another study found no considerable difference in asthenopia between progressive computer glasses with far‐distance focus and monofocal computer glasses after one‐year follow‐up (MD change scores −1.79, 95% CI −11.60 to 8.02 on a 100 mm VAS scale, very low quality evidence). The effects on headaches were inconsistent.
One study found no difference between progressive far‐distance focus computer glasses and trifocal glasses in effect on eyestrain severity (MD −0.50, 95% CI −1.07 to 0.07, very low quality evidence) or on eyestrain frequency (MD −0.75, 95% CI −1.61 to 0.11, very low quality evidence).
Progressive computer glasses versus ergonomic assessment with habitual (computer) glasses One study found that computer glasses optimised for individual needs reduced asthenopia sum score more than an ergonomic assessment and habitual (computer) glasses (MD −8.9, 95% CI −16.47 to −1.33, scale 0 to 140, very low quality evidence) but there was no effect on the frequency of eyestrain (OR 1.08, 95% CI 0.38 to 3.11, very low quality evidence).
We rated the quality of the evidence as low or very low due to risk of bias in the included studies, inconsistency in the results and imprecision.
Authors' conclusions
There is low to very low quality evidence that providing computer users with progressive computer glasses does not lead to a considerable decrease in problems with the eyes or headaches compared to other computer glasses. Progressive computer glasses might be slightly better than progressive glasses for daily use in the short term but not in the intermediate term and there is no data on long‐term follow‐up. The quality of the evidence is low or very low and therefore we are uncertain about this conclusion. Larger studies with several hundreds of participants are needed with proper randomisation, validated outcome measurement methods, and longer follow‐up of at least one year to improve the quality of the evidence.
Plain language summary
Eyeglasses, contact lenses or eye surgery for preventing and treating eye symptoms in computer users
What is the aim of this review?
Computer users frequently complain about problems with their eyes, or headaches. Eyeglasses, contact lenses or surgery of the eye might help to decrease or prevent these symptoms. We examined the effects of these interventions on eye symptoms and quality of life.
Key messages
Computer glasses with specific types of lenses are no different to other types of computer glasses in terms of eye symptoms. Computer glasses might improve eye symptoms more than glasses designed for daily use in the short term but not at six months follow‐up and there is no evidence on long‐term follow‐up. Due to the very low quality of the evidence we are uncertain about this conclusion. There are no studies on contact lenses or eye surgery to decrease eye symptoms of computer users. Randomised studies are needed with hundreds of participants that better measure symptoms at one‐year follow‐up.
What was studied in the review?
We found eight studies with 381 participants. All studies evaluated eyeglasses. We found no studies evaluating contact lenses or surgery. Two studies looked at progressive computer glasses where the focus gradually changes from nearby to the distance of the computer screen but one did not report any data. Two studies examined progressive computer glasses in which the focus also extended a couple of meters beyond the computer screen. Five studies looked at progressive computer glasses whose focus gradually changed to far distance. One study examined if the spectacles that participants already had could be improved and whether that influenced their computer vision, but the study did not provide data. We judged the risk of bias to be unclear in four studies, high in two and low in another study.
What are the main results of the review?
Progressive computer glasses compared to other types of computer glasses One study found no difference in eye symptoms after one year between progressive computer glasses and computer glasses with only one focus.
Progressive computer glasses including middle distance focus in the upper part of the glasses compared to other types of glasses Two studies found a small difference in eye symptoms between progressive computer glasses including middle distance focus and progressive glasses for everyday use when the glasses had been used for a period of one week to one month. There was no difference in dizziness between the two kinds of glasses. Another study found no difference in eye symptoms after one year between progressive computer glasses and computer glasses with only one focus.
Progressive computer glasses including far‐away focus in the upper part of the glasses compared to other types of glasses Two different studies found no difference in eye symptoms after one month between computer glasses including a far‐away focus and bifocal or trifocal computer glasses. Another study found that after one year glasses with only one focus were just as good as computer glasses. One study compared progressive computer glasses to an assessment of the participant's computer work station and own (computer) glasses and found an improvement of asthenopia symptom‐score of about 40%.
How up‐to‐date is this review?
We searched for studies that had been published up to 20 December, 2017.
Summary of findings
Background
Description of the condition
Computer vision syndrome (CVS) is defined by the American Optometric Association as "the complex of eye and vision problems related to near work which are experienced during or related to computer use" (AOA 2011). As a major complaint in people with CVS, asthenopia is a formal diagnostic term (ICD‐10, H53.1) and is nearly synonymous with the more familiar word 'eyestrain' (Rosenfield 2011). The reported prevalence of asthenopia during or after work on a computer ranges from 46.3% to 68.5% (Bhanderi 2008; Dain 1988; Sanchez 1996). Two broad categories of asthenopic symptoms were described by Sheedy 2003 as:
(1) internal symptoms including eyestrain, eye ache, headache, double vision and blur, which are generally caused by refractive, accommodative or vergence anomalies; and
(2) external symptoms including burning, irritation, ocular dryness and tearing, which are caused by holding the eyelids open, glare, gazing up, trying to read a small font and flickering of visual display units (VDUs). The symptoms seem highly related to dry‐eye symptoms.
A refractive error, or refraction error, is an error in the focusing of light by the eye which is a frequent reason for reduced visual acuity. Uncorrected or under‐corrected refractive error can be major contributing factors to VDU‐related asthenopia (Daum 1988; Rosenfield 2012; Rosner 1989; Sheedy 1992; Wiggins 1992). Some studies have observed that individuals who have refractive error (even when corrected) are more likely to develop asthenopia (Bergqvist 1994; Bhanderi 2008; Nakaishi 1999).
Besides the discomfort related to asthenopia and experienced during computer operation, eye symptoms may also have a significant economic impact. For instance, such symptoms can increase the number of errors made during computer use and increase the need for more frequent breaks. It has been estimated that the provision of appropriate refractive correction alone could produce at least a 2.5% increase in productivity among those who use a computer in their work (Daum 2004).
Description of the intervention
There are various possibilities for optical correction of refractive errors including eyeglasses, contact lenses and refractive surgery. These can be categorised as follows.
-
Eyeglasses for optical correction may have:
monofocal glasses that are used to meet the need of correction for one field of vision, either for distance, intermediate (computer), or near vision;
bifocal glasses that contain two different prescriptions in the same lens, where there is a visible segment in the lens that can be used for near vision;
trifocal glasses that contain three focal points, usually for distance, intermediate and near vision; a trifocal lens has an added segment above the bifocal for viewing objects in the intermediate zone;
progressive glasses that provide the smoothest transition from long distance vision to intermediate vision to near vision, including all the in‐between corrections. There are no visible segments and the glasses provide gradual or progressive powers of correction (from top to bottom). Modified progressive glasses are also called progressive occupational glasses or progressive computer glasses. Several occupational lens designs have been developed for computer users who have a high intermediate‐vision demand coupled with a high near‐vision demand (Mancil 2010). They have a larger intermediate zone than regular progressive glasses, leaving no or less space for distance. Progressive computer glasses are generally not suitable for driving or regular wear.
Contact lenses are corrective lenses placed on the cornea of the eye to improve vision. There are two general categories of contact lenses, soft and rigid gas permeable. Just as with eyeglasses there are monofocal and bifocal or multifocal contact lenses.
-
Refractive surgery includes:
corneal refractive surgery using several laser and non‐laser refractive surgical procedures that can be used to modify the shape of the cornea and correct myopia, hyperopia, astigmatism and presbyopia. The mainstay of refractive surgery is currently laser refractive surgery, which can be broadly divided into lamellar ablation (LASIK); and surface (photorefractive keratectomy (PRK), laser epithelial keratomileusis (LASEK), and Epi‐LASIK) ablation (Sakimoto 2006). In the lamellar procedure the surgeon cuts a thin flap of the corneal tissue. The flap is lifted like a hinged door, targeted corneal tissue is removed using a computer‐controlled beam of light (a laser) and then the flap is replaced. In the surface procedure the cornea is reshaped by removing corneal tissue with a laser without first cutting a flap into the cornea.
intraocular lenses (IOLs), which are lenses that are implanted in the eye. There are IOLs that are used for replacing the lens of the eye after cataract surgery. Also, various types of implantable lenses are available as an alternative to laser refractive surgery when correcting (high) refractive errors, either as a replacement for, or placed in front of, the lens of the eye. IOLs come in two varieties, monofocal and multifocal intraocular lenses.
How the intervention might work
To achieve and maintain clear and single vision of relatively small targets throughout the computer task, it is important that the retinal image is focused appropriately. The presence of refractive errors will significantly reduce visual acuity and correcting them will reduce or prevent eye symptoms.
Except for people who have uncorrected myopia (nearsighted people), the closer an object (including the computer) is to the eyes the harder the eyes have to work to accommodate. When visual demands exceed the capacity of visual accommodation, there might be an increase in symptoms such as eyestrain and headache (Rosenfield 2011; Zhang 2008). Optical correction of refractive error can relieve or remove accommodative strain and improve visual capacity to reduce or prevent eye symptoms during computer use, especially during prolonged or multi‐tasking computer use.
In older individuals, accommodation is reduced and a near correction might be needed. As computer users usually interact visually with other tasks and persons within the entire operating area, a large visual range is desirable. This is probably best achieved with progressive glasses. Progressive glasses enable a wearer to have a wider, larger area of view that can be fixated at that viewing distance with little head movement. Some progressive lens designs address the specific occupational vision needs of computer users with large intermediate viewing zones. Progressive glasses are well accepted by people who use computers 20% to 50% of the work day (Bachman 1992; Horgen 2004; Krefman 1991; Sheedy 2005). Progressive glasses have been proven to be very successful in presbyopic people (Bachman 1992; Barcik 2010; Blehm 2005); and are considered to be the best solution so far for people who work with computers (Barcik 2010). Some studies have indicated that presbyopic patients generally prefer progressive glasses compared to their usual glasses for computer work, and that they have fewer eye symptoms (Bachman 1992; Butzon 1997; Butzon 2002; Hanks 1996).
Why it is important to do this review
There is a high incidence of eye problems among computer users, threatening long‐term visual health and productivity. Appropriate interventions like refractive error correction to minimise symptoms will not only result in improved visual health for computer users, but possibly also in financial benefit, as occupational efficiency will be improved as well. Computer users who have asthenopic symptoms, with or without glasses, probably should have their refractive errors corrected (Edema 2010). It is necessary, however, to know which optical intervention may best meet their needs. Although there are various possible interventions for correcting refractive error in computer users with CVS there is a lack of consensus regarding the effectiveness of interventions.
There are several published studies on these optical interventions that describe successful outcomes for computer users. However, we are aware of only two systematic reviews that have studied ergonomic interventions for computer uses, among which were computer glasses (Brewer 2006; Leyshon 2010). Both reviews stated that the evidence regarding effectiveness of computer glasses was insufficient to draw firm conclusions. Consequently, this Cochrane review exhaustively summarises the evidence regarding the effectiveness, safety and applicability of computer glasses and other optical interventions, which can help clinicians or computer users to select the most appropriate optical intervention. In addition, this Cochrane review can help develop healthcare policies and programmes including occupational health guidelines and regulations.
Objectives
To examine the evidence on the effectiveness, safety and applicability of optical correction of refractive error for reducing and preventing eye symptoms in computer users.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised and quasi‐randomised controlled trials. The unit of randomisation could be the individual computer user or groups of individuals but all included studies used the individual level randomisation. 'Quasi‐randomised' refers to a situation in which the investigator allocates individuals to groups using methods lacking strict randomisation, for example by means of date of birth, hospital record number or alternation. We included both parallel RCTs and cross‐over RCTs in which the participants are randomised to the order of getting the intervention first or the comparison condition first.
We excluded other, non‐randomised types of studies such as controlled before‐after studies, cohort studies, case‐control studies, cross‐sectional studies, or case series, as these are inclined toward confounding and bias.
Types of participants
Study participants included male or female computer users with a refractive error who used a computer for at least four hours per day. We included studies where participants had one or more of the following types of refractive errors: myopia, hyperopia, astigmatism or presbyopia. See Appendix 1 for an explanation.
We were interested in two types of participants for this review.
(1) Those with symptoms that were treated by correcting refractive error.
(2) Those without symptoms in whom the refractive error was corrected to prevent symptoms.
For this review, eye symptoms associated with computer use were defined as a condition characterised by at least one of the clinical signs noted above (Sheedy 2003).
There were no restrictions on race, gender, age or type of computer. We also intended to include studies in which participants had refractive error after a cataract extraction and intraocular lens implantation but we did not identify such studies.
We excluded studies that only included participants with existing strabismus (including vergence disorders and latent strabismus (heterophoria), which may give rise to prism correction), amblyopia or other ocular pathology. See Appendix 1 for an explanation of key terms.
Types of interventions
We included studies in which any intervention for optical correction of refractive error (that is eyeglasses, contact lenses or refractive surgery) for reducing or preventing eye symptoms in computer users was compared with another optical intervention, sham intervention or no intervention. We list all possible interventions for refractive error corrections in Appendix 2. We also included studies in which an optical intervention was compared to a non‐optical intervention, like a rest break, exercises or eyedrops.
We excluded studies in which prism corrections were the intervention, as they correct binocular problems instead of refractive errors. We also excluded studies of combined interventions, unless we could distinguish between effects of refractive error correction and alternative treatment.
Types of outcome measures
Primary outcomes
Patient‐reported symptoms of asthenopia, i.e. internal symptoms related to use of the eyes including eyestrain, eye ache, headache, diplopia and blur; and external symptoms including burning, irritation, ocular dryness and tearing, measured with a questionnaire or interview. If a study reported more than one outcome for asthenopia and did not use a summary score, we chose the outcome that best matched asthenopia or eye‐strain for inclusion in the meta‐analysis and disregarded the other outcomes.
Health‐related quality of life (HQoL) measured with vision‐ or occupation‐specific questionnaires or generic questionnaires.
Secondary outcomes
Reading speed in words per minute.
Font size readable: depicts visual acuity at computer‐using distance.
Visual acuity: refers to near visual acuity by visual chart with own correction versus new correction.
Compliance with optical correction: refers to continued use of glasses or contact lenses for a certain period of time for computer use, or wearing time per day.
Accommodative response (AR) values.
Near point of convergence.
Difference in refractive error between own correction and intervention correction.
Adverse outcomes: worsening of headaches, dizziness, or nausea, and worsening of peripheral image blur (aberrations of unwanted astigmatism, defocus error and higher aberration) (Mok 2011).
Economic data: sick leave days and productivity, time of sustained computer work without symptoms, as well as cost of optical refractive error correction.
We included studies that reported one of the primary outcomes, as well as studies that only reported one or more of our secondary outcomes.
Search methods for identification of studies
We present our search strategy for MEDLINE through PubMed in Appendix 3. Based on this strategy we developed search strategies for the other databases. We used the most sensitive and precision‐maximising search strategy as recommended by Cochrane (Chapter 6 of the Cochrane Handbook for Systematic Reviews of Interventions;Higgins 2011). We combined database subject headings (e.g. MeSH terms) and free text terms; and placed no restrictions on date, language or publication type.
Electronic searches
We searched the following electronic databases, from inception to 20 December 2017.
The Cochrane Central Register of Controlled Trials (CENTRAL) (which contains the Cochrane Eyes and Vision Group and the Cochrane Work Trials Registers) in the Cochrane Library;
MEDLINE through PubMed;
ISI Web of Knowledge;
Embase;
and OSH update (CISDOC, HSELINE, IRSST, NIOSHTIC, NIOSHTIC‐2, RILOSH) until 22 June 2017.
Searching other resources
We searched the World Health Organization (WHO) International Clinical Trials Registry Platform (apps.who.int/trialsearch, accessed on 20 December 2017) using the following search terms: 'computer vision syndrome', '(refraction OR refractive) AND computer'.
We checked the reference lists of included papers and we used the Science Citation Index‒Expanded database to identify any additional relevant publications that cited our included studies.
We also used the yield of a preliminary search at the protocol stage of this review including five major mainland China databases, using keywords in Chinese: CNKI (China National Knowledge Infrastructure), VIP (Wei Pu Information), Wang Fang Data, CMCI (Chinese Medical Citation Index), CBM (Chinese Biologic Medical database). These databases were probably searched until June 2012; however, due to difficulties in contacting the original co‐authors, we are not sure. Since we had no indication that this revealed additional publications we did not put effort into updating this search. Information about the initial search strategy as reported in the protocol of this review can be found in Appendix 4.
Data collection and analysis
Selection of studies
Two authors (PH; and CT or JV) independently screened all references for eligibility of inclusion using the pre‐defined inclusion criteria regarding design, participants and the intervention. We first screened references via title and abstract, and retrieved and screened in full text those articles that were not excluded. We contacted the authors of potentially eligible conference abstracts, to trace full‐text publications of the studies. In cases where no full‐text publication could be identified, we used the information in the abstract to judge eligibility of the study. For two publications (one in Russian — Feigin 2003; and one in Chinese — Guo 2010) a native speaker assisted in assessment of the eligibility.
The two review authors resolved any disagreements by discussion; and the third review author arbitrated if disagreement persisted. We documented justification for exclusion of studies at full‐text stage.
Data extraction and management
Two review authors (PH; and CT or JV) independently extracted data for each included study. We used a standardised, tailored data extraction form, including items about general information (study design, setting, duration of follow‐up, funding), methods (e.g. randomisation and blinding), participants, interventions and comparisons, outcomes and results. When applicable, we compared multiple reports and publications of the same study for completeness and possible discrepancies.
One author (PH or JV) entered data into Review Manager 5 (RevMan 5) software (Review Manager 2014); and the data were checked by another (PH or JV).
Assessment of risk of bias in included studies
Two review authors (PH; and CT or JV) independently assessed risk of bias in included studies using the recommended tool in Chapter 8 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We resolved disagreements through discussion and, if necessary, the third author made the final decision.
We evaluated the following domains for each study: sequence generation; allocation concealment; blinding of participants and personnel; blinding of outcome assessors; incomplete outcome data; selective reporting; and other sources of bias (among others baseline imbalances). We assessed the risk of detection bias separately for primary and secondary outcomes. We reported the judgment for each criterion (low/high/unclear risk of bias), as well as support for each judgement.
In cases where we did not succeed in retrieving additional information from study authors we had to base our assessment of methodological quality on the available information.
We considered a study at low risk of bias if the domains 'selection bias', 'performance bias' and 'detection bias' were assessed as low risk and none of the other domains was at high risk.
Measures of treatment effect
We expressed dichotomous results as risk ratios (RRs) with their 95% confidence intervals (CIs) and continuous data as (standardised) mean differences ([S]MD) with their 95% CI, where possible. We used standardised mean differences (SMD) with 95% CI when studies assessed the same outcome but measured it in different ways. We calculated SMDs from a paired analysis according to the methods described in chapter 16 of the Cochrane Handbook (Higgins 2011).
In case of severe baseline imbalances, we would have used the adjusted effect estimates based on an ANCOVA analysis. In the absence of a reported ANCOVA analysis we used the change scores as the second best option as suggested by Fu 2013. We then chose the estimate with a correlation of 0.7 as the results reported in this review.
If in future updates of this review we can include studies with results that cannot be plotted, we will describe these results in the ‘Characteristics of included studies’ table, or we will enter the data into ‘Additional tables’.
Unit of analysis issues
As symptoms of asthenopia are binocular the unit of analysis is the individual. For some of our secondary outcomes, like refraction and accommodation, the likely unit of analysis is one eye or 'per eye'. If an included study reported such an outcome and the unit of randomisation had been the individual, the study would have been considered a cluster‐randomised trial. In this case we would have extracted data from analyses that properly account for the non‐independence of the clustered design but there was no need to do this in the current version of this review. If included studies in future updates of this review employ a cluster‐randomised design and make no allowance for the clustering effect, we will make an estimation based on a conservative estimate of the intra‐cluster correlation coefficient of 0.1 as found in implementation research (Campbell 2001).
For cross‐over trials that reported continuous outcomes, we used a paired analysis when reported by the authors and put the MD between intervention and control condition and its standard error into the RevMan 5 data‐tables and used the generic inverse variance method for calculating the effect estimate. If the authors had not reported these paired analysis, we would have calculated them based on a reported or imputed correlation between the outcomes of the intervention and the control condition, as advised in Chapter 16 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). For dichotomous outcomes, we adjusted the confidence intervals for the paired analysis according to Elbourne 2002.
When multiple arms of a study were included in the same meta‐analysis we divided the number of participants in the control condition evenly across the study arms to prevent double counting of participants.
Dealing with missing data
We contacted corresponding authors of included studies with missing data to request missing information needed for data analysis (Bachman 1992; Butzon 1997; Butzon 2002; Cagnie 2017; Daum 2014; Horgen 2004; Jaschinski 2015b; Zeried 2007). We pre‐specified that in case of no response within four weeks, we would use the available data. This was the case for all studies except Jaschinski 2015b and Cagnie 2017. We investigated dropouts, missing at follow‐up and withdrawn study participants. We analysed only the available data and ignored data that are assumed to be missing at random. We would have imputed missing data assumed not to be missing at random with replacement values, and we would have treated these as if they were observed, according to the methods provided in Section 16.1 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
For paired analysis with dichotomous outcome data that presented results as from a parallel trial, we calculated odds ratios (ORs) and confidence intervals adjusted for the paired analysis according to Elbourne 2002, based on an assumed correlation coefficient of 0.23.
Following the recommendations by Fu 2013 for change scores from baseline to follow‐up, we calculated change scores with imputed correlation coefficients for a fair correlation (0.7). We examined the effect of the assumptions of the correlation coefficients on our final conclusions.
Assessment of heterogeneity
We assessed clinical heterogeneity based on the similarity of the population, intervention, outcome and follow‐up. We considered populations as similar when they fell into one of the pre‐defined categories of participants (as stated in Types of participants), regardless of occupation or type of work. We considered participants with and without presbyopia as different. We considered interventions as similar if they fell into one of the pre‐defined categories of interventions (as stated in Types of interventions and Appendix 2). We considered the various outcome categories as different but we considered all patient‐reported complaints of asthenopia as similar. We regarded follow‐up times of less than three months, three months to one year and more than one year as different.
We planned a test for statistical heterogeneity by means of the Chi² statistic as implemented in the forest plot in Review Manager 5 software (Review Manager 2014). The significance level would be set at 0.10. Moreover, we planned to quantify the degree of heterogeneity using the I² statistic, where an I² value of 25% to 50% indicates a low degree of heterogeneity, 50% to 75% a moderate degree of heterogeneity and more than 75% a high degree of heterogeneity (Higgins 2003).
We planned to explore potential sources of heterogeneity but there were too few studies to do so. We only considered subgroup analyses to explore clinical heterogeneity, as specified below, if there were at least five studies in a comparison.
Assessment of reporting biases
If in a future update of this review there are more than 10 included studies available in a particular comparison, we will use funnel plots to assess possible selective publication and alternative explanations for funnel plot asymmetry (such as clinical or methodological heterogeneity, statistical artefacts, chance, relationship between trial size and effect size) according to Egger 1998.
Data synthesis
We pooled data from studies judged to be clinically homogeneous using Review Manager 5 software (Review Manager 2014). In cases of statistical heterogeneity we would have used a random‐effects model; otherwise a fixed‐effect model. In cases of substantial clinical or statistical heterogeneity or if pooling of data had not been feasible, we would have explored the source of heterogeneity and presented a qualitative summary rather than pooling the data.
The GRADE approach as described in the Cochrane Handbook for Systematic Reviews of Interventions was used to summarise findings and to present the quality of evidence in ‘Summary of findings’ tables (Higgins 2011). The downgrading of the quality of a body of evidence for a specific outcome was based on five factors: 1. limitations in studies; 2. indirectness of evidence; 3. inconsistency of results; 4. imprecision of results; 5. publication bias. The GRADE approach specifies four levels for the quality of evidence: high, moderate, low and very low.
Subgroup analysis and investigation of heterogeneity
If there is sufficient data available in a future update of this review, we will conduct subgroup analyses or meta‐regression to explore the following sources of heterogeneity.
Type of refractive errors: hyperopia versus myopia versus astigmatism
Type of computer: desktop versus laptop versus tablet versus Personal Digital Assistant (PDA).
People who have had cataract surgery versus those without cataract surgery, as they do not have accommodation at all.
Sensitivity analysis
We planned to perform sensitivity analyses to determine the impact of excluding studies with lower methodological quality, industry funding, and those only reported in abstracts or unpublished at the time of this review. However, this was not possible, because we did not have enough studies in each comparison‐outcome combination. In the case of missing data, we employed sensitivity analyses using different approaches to impute missing data.
Results
Description of studies
Results of the search
We identified 5809 references by searching electronic databases and identified 16 additional records through other sources (mainly identified by the initial search performed by the authors of the protocol of this review; see Appendix 4). After removing duplicates 5182 records remained. We excluded 5146 records based on title and abstract; and we listed one study as ongoing (NCT02775396). We screened 35 full‐text articles of which eight studies met our inclusion criteria.
We present the study flow in Figure 1.
1.
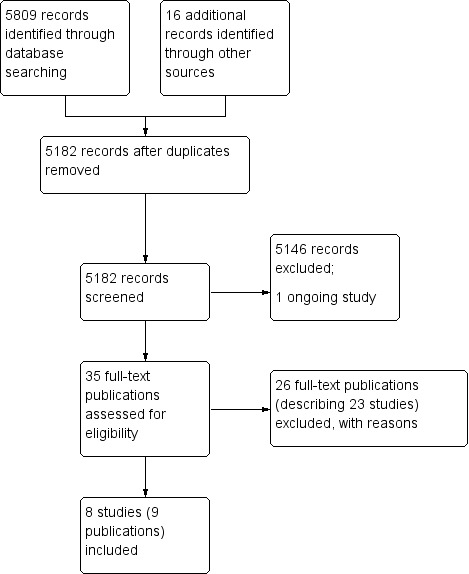
PRISMA Study flow diagram.
Included studies
We included six randomised controlled studies (Bachman 1992; Cagnie 2017; Daum 2014; Horgen 2004; Jaschinski 2015b; Zeried 2007) and two quasi‐randomised studies (Butzon 1997; Butzon 2002) with a total of 386participants. For two of the included studies there was no full‐text publication, so our description and analyses of these studies are based on the information as presented in a conference abstract and a trial register record/study protocol (Daum 2014; Zeried 2007). See also the Characteristics of included studies table.
Study design
Five studies had a cross‐over design in which the order of the interventions was randomised (Bachman 1992; Butzon 1997; Butzon 2002; Jaschinski 2015b; Zeried 2007).
Bachman 1992 divided the participants randomly into a group which used the intervention first and a group which used the control eyeglasses first. The first period of four weeks was immediately followed by the second period of four weeks without a wash‐out period. The second period was followed by a one‐week period in which the preferred glasses were worn. The outcome was evaluated after all three periods. The authors presented the data only as if a parallel trial was performed. We adjusted the confidence interval based on an assumed correlation of 0.23 according to the method presented by Elbourne 2002.
Butzon 1997 used a 'counterbalanced order' of allocating the interventions, which we understood as alternating order. Two types of eyeglasses were worn during three weeks each, without a wash‐out period in between. After this six‐week intervention period, both eyeglasses were used during another three weeks. The authors presented the results as a non‐significant difference based on a paired t‐test but did not provide a P value. We took a P value of 0.1 as an estimate and calculated the mean difference (MD) and standard error (SE) based on this value for our data‐analysis.
Butzon 2002 also alternated the order of the interventions. Both intervention periods lasted three weeks without a wash‐out period in between. The authors presented the results based on a ANOVA analysis and a P value for the F‐test. We took the square root of the F‐test as the input for a paired t‐test to calculate the SE for the mean difference. For the dichotomous results we used the adjustment of the confidence interval as proposed by Elbourne 2002.
Jaschinski 2015b randomly assigned the order of the intervention or control for the first week of the trial. For the next three weeks, participants crossed over to the alternative condition each week. The outcomes were assessed at the end of each week and for some outcomes on a daily basis during weeks three and four. The authors called the first two weeks the adaptation phase and the last two weeks the test phase. However, they did not use a wash‐out period between any of the periods. They presented the results for the last two weeks of the test phase based on a paired analysis and we took the reported MD and SE of these results for our data‐analysis.
Zeried 2007 did not provide enough data for an analysis.
Three other studies had a parallel design in which participants were randomised to either one of four study groups (Horgen 2004), one of three study groups (Daum 2014), or one of two study groups (Cagnie 2017).
Participants
Participants were recruited from the workforce of a pharmaceutical company (N = 30) (Butzon 2002), financial holding (N = 35) (Cagnie 2017), call centre (N = 51) (Daum 2014), tax office (N = 23) (Jaschinski 2015b), and telecommunication companies (N = 24 and N = 158) (Butzon 1997 and Horgen 2004). Another study included respondents to an advertisement (N = 29) (Bachman 1992); and one study did not mention where participants were recruited (N = 36) (Zeried 2007).
Five studies were conducted in the USA (Bachman 1992; Butzon 1997; Butzon 2002; Daum 2014; Zeried 2007); one in Belgium (Cagnie 2017); one in Germany (Jaschinski 2015b); and one in Norway (Horgen 2004).
For six studies the age of the participants was within a comparable age range, as follows: a mean age of 52.3 years (range 42 to 64) (Bachman 1992); 53 years (range 47 to 66) (Butzon 1997); 51.1 (SD 4.2) in intervention group and 53.7 (SD 4.0) in control group (Cagnie 2017); 51.1 years (range 40 to 65) (Daum 2014); 55 years (range 46 to 61) (Jaschinski 2015b); and age range 37 to 57 without a mean provided (Butzon 2002). Participants in Zeried 2007 had a lower mean age of 27.7 years (no range provided). Horgen 2004 did not report any age characteristics of the studied population.
The estimated mean time spent at a computer was described in two studies: 5.5 and 5.1 hours per day respectively for Bachman 1992 and Zeried 2007. Daum 2014 included participants who worked at a computer for at least six hours a day and three other studies included participants who worked at a computer for at least four hours a day (Butzon 1997; Butzon 2002; Cagnie 2017). The remaining two studies provided no information about the time spent at a computer (Horgen 2004; Jaschinski 2015b). However, Jaschinski 2015b included employees that 'worked primarily at the computer' and reported a mean daily duration of work of 7.9 ± 1.6 hours; whereas in Horgen 2004 the intervention was used over four hours a day, indicating a duration of computer work lasting more than four hours a day. None of the included studies specified the type of computer or computer screen used.
Six studies included only presbyopic participants (Bachman 1992; Butzon 1997; Cagnie 2017; Daum 2014; Horgen 2004; Jaschinski 2015b). In Bachman 1992 refractive error of study participants ranged from spherical +4.75 to −4.75 diopters and cylindrical 0 to −2.75 diopters but the authors did not report the additional power for reading distance.
In the study by Daum 2014 participants were described as myopic astigmats (means spherical −1.32 dioptres, cylindrical −0.74 dioptres) requiring a mean addition of +1.72 diopters. In the third study by Horgen 2004 the only information about participants' refractive error was that it did not exceed spherical −6.00 dioptres.
In the study of Jaschinski 2015b the refractive error was averaged across the two eyes and had a spherical component of −0.90 ± 2.66 D (range −6.25 D to +4.00 D), a cylindrical refraction of −0.90 ± 0.69 D (range 0 to −2.75 D), and an additional power for near of 2.06 ± 0.41 D (range 1.00 D to 2.50 D).
Butzon 1997 and Cagnie 2017 did not provide information about the refractive error of the participants, except that they needed a near add power of at least +1.50 D.
Butzon 2002 also mainly included presbyopic participants but as they used a minimum age of 37 as inclusion criterion, their population consisted of some non‐presbyopes as well.
Finally, Zeried 2007 did not report data on study participants' absolute refractive error.
Interventions and comparators
In all eight included studies the intervention was correction of refractive error with eyeglasses and aimed at treatment of symptoms rather than at prevention. We did not find any studies that had evaluated the effect of contact lenses or refractive surgery.
Various types of glasses from different manufacturers were used in which the number and surface of the focal areas in the lens were specifically adapted for use with computer screens. The adaptations varied from just one focus at the distance of the computer screen to focal areas that gradually changed from nearby to far away but that still included a larger surface of the area that focuses on the computer screen. In six studies, interventions were progressive computer glasses (Bachman 1992; Butzon 1997; Cagnie 2017; Daum 2014; Horgen 2004; Jaschinski 2015b). All but two types of glasses in the control groups were designed as specific computer glasses. The two types that were designed for all‐purpose use were gradually progressive glasses without a specific larger area that focusses on the computer screen (Jaschinski 2015b; Cagnie 2017); and general purpose bifocal glasses that have a focus for nearby and one for far away (Daum 2014).
We categorised the computer glasses as follows.
Monofocal computer glasses denoted as C+ meaning that they focus on the computer screen.
Bifocal computer glasses, denoted as N/C+ meaning that they have separate areas for focus nearby and on the computer screen.
Progressive computer glasses denoted as N/C+ meaning that they have focal areas ranging from nearby to the computer screen.
Progressive computer glasses with a focus at an intermediate distance (< 6 metres) in the upper part of the glasses denoted as N/C+/IM.
Progressive computer glasses with a focus at far distance (≥ 6 metres, optical infinity) in the upper part of the glasses denoted as N/C+/F.
The brand used by Daum 2014 was Essilor computer glasses without further specification and the brand used by Horgen 2004 was Essilor Interview glasses. The brand of progressive intermediate‐range computer glasses used by Horgen 2004 was Zeiss Gradal RD, the brand used by Cagnie 2017 was Zeiss Officelens Plus, and the brand used by Jaschinski 2015b was Zeiss Officelens Individual. The brand of progressive far‐distance range computer glasses used by Bachman 1992, Butzon 1997 and Horgen 2004 was American Optical TruVision Technica. The brand of general purpose progressive glasses used by Jaschinski 2015b was Zeiss Progressive Individual 2 and Cagnie 2017 used Zeiss Precision Plus; and the brand of trifocal glasses used in Butzon 1997 was Vision‐Ease CRT DataLite. The brands of the monofocal computer glasses used by Horgen 2004 and bifocal computer glasses used by Bachman 1992 were not specified.
In the Butzon 2002 study, computer glasses were compared to an ergonomic self‐assessment tool (wearing habitual refractive error correction). Computer glasses were provided according to individual needs and characteristics: progressive computer glasses (American Optical TruVision Technica or SOLA Access); bifocal computer glasses (brand not specified); or trifocal computer glasses (Vision‐Ease CRT DataLite).
Two studies compared best refractive error correction with the habitual refractive error correction. Daum 2014 additionally compared full to habitual correction with bifocal glasses. The other study by Zeried 2007 evaluated the best correction of refractive error with habitual correction of refractive error without specifying the types of glasses used.
Altogether this resulted in the following direct comparisons.
Progressive computer glasses vs. monofocal computer glasses (Horgen 2004) and vs. general purpose bifocal glasses (Daum 2014).
Progressive intermediate‐distance range computer glasses vs. general purpose progressive glasses (Jaschinski 2015b; Cagnie 2017) and vs. monofocal computer glasses Horgen 2004.
Progressive far‐distance range computer glasses vs. monofocal glasses (Horgen 2004), vs. bifocal computer glasses (Bachman 1992), and vs. trifocal computer glasses (Butzon 1997).
Best refractive error correction vs. habitual refractive error correction (Daum 2014; Zeried 2007).
Computer glasses vs. ergonomic self‐assessment tool (using habitual refractive error correction) (Butzon 2002).
Outcomes
All studies reported our primary outcome 'patient‐reported symptoms of asthenopia'.
The studies reported asthenopia in different ways which we all considered as similar. When studies had reported more than one outcome for asthenopia and did not provide a sum score we took the outcome that best resembled eye strain such as in Butzon 1997. Bachman 1992 reported the number of symptoms that improved. Butzon 1997 measured the frequency and severity of eyestrain with a 0 to 10 Likert scale anchored as 0 (mild), 5 (moderate) and 10 (severe) strain and 0 (monthly), 5 (weekly) and 10 (daily) symptoms. Butzon 2002 measured the total sum score of 14 asthenopia‐related symptoms with a 10‐point Likert scale resulting in a scale ranging from 0 to 140. In addition, the authors reported the frequency of eyestrain or tired eyes (yes/no). Cagnie 2017 used the Visual Fatigue Questionnaire (VFQ) to measure visual fatigue on a patient‐reported VAS ranging from 0 to 10. Daum 2014 used the Convergence Insufficiency Symptom Survey. Horgen 2004 reported intensity of visual symptoms on a 100 mm VAS scale. Jaschinski 2015b used the average over a week of the average rating of seven specific questions on eye symptoms that could be answered on a scale ranging from 1 to 6 (with 6 indicating more problems) on a daily basis. To be able to calculate a SMD for Jaschinski 2015b we first calculated a correlation coefficient based on the reported SE of the MD of 0.09 and reported SDs of the intervention and control group of 0.38 and 0.65 according to chapter 16 in the Cochrane Handbook (Higgins 2011). Zeried 2007 measured visual comfort by a phone survey not further specified before and after one hour of work on the participant's own computer.
The median baseline scores for the four intervention groups in Horgen 2004 and the two groups in Jaschinski 2015b amounted to 29% of the maximum attainable score.
Horgen 2004 had considerable baseline differences for this outcome. Therefore, we also used the change scores in addition to the outcome values at follow‐up. We subtracted the end‐scores from the baseline scores which means that a higher score means a bigger change and a more favourable result. Because no SDs for the change scores were reported and the authors could not be contacted, we imputed the standard deviations based on the calculations according to the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), assuming a correlation between baseline and follow‐up of 0, 0.7 and 0.9. Horgen 2004 reported the outcomes only in figures and we extracted the MD and SDs from these figures. For Butzon 2002 we had to extract data from a figure too, and we calculated change scores in the same way because of baseline differences.
None of the included studies reported our primary outcome 'health‐related quality of life'. According to his study protocol Daum 2014 was supposed to have used the National Eye Institute Refractive Quality of Life survey. However the authors reported no results.
Of our secondary outcomes, four studies reported on our predefined adverse event of headaches (Bachman 1992; Butzon 2002, Horgen 2004, Jaschinski 2015b). None of the studies reported on peripheral image blur. Three studies reported on additional adverse events of nausea (Bachman 1992; Butzon 2002) and dizziness (Bachman 1992, Jaschinski 2015b).
Two studies addressed compliance with optical correction (Butzon 1997; Horgen 2004); and another study evaluated the difference in refractive error between own and intervention correction (Zeried 2007). Economic data on productivity were provided in two studies (Daum 2014; Zeried 2007). None of the studies reported reading speed, font size readable, near vision visual acuity, accommodative response or near point of convergence.
Length of follow‐up
Horgen 2004 presented results for long‐term follow‐up: using eyeglasses for a period of 12 months.
Cagnie 2017 evaluated the effect of eyeglasses after one month, three months and six months (short and medium‐term follow‐up). We only used the one month and six months' follow‐up data to prevent the same study contributing data twice to the same meta‐analysis.
The other studies had a short‐term follow‐up only. In Bachman 1992 each pair of eyeglasses was used for a period of four weeks in random order, followed by one week of direct comparison. Butzon 1997 and Butzon 2002 used a period of three weeks for the intervention after which the groups crossed over to the other intervention. Zeried 2007 followed the participants during the one‐month cross‐over period and three months after the study. Duration of the intervention period was 10 weeks in Daum 2014. Jaschinski 2015b first used an adaptation period of two weeks and then a two‐week test period in which the intervention was alternated, which effectively leads to a one‐week follow‐up. After this test period there was an eight‐week follow‐up period in which the participants could use the glasses according to their preference.
Funding
Five studies received financial support from representatives of the optical industry (Bachman 1992; Butzon 2002; Daum 2014; Jaschinski 2015b; Zeried 2007); and Horgen 2004 was supported by the Norwegian Optometric Research Foundation. Butzon 1997 received a grant from a telecommunication company. Cagnie 2017 did not declare any funding sources.
Excluded studies
We excluded 26 publications describing 23 studies at full‐text stage. Reasons for exclusion of these studies are presented in the 'Characteristics of excluded studies' table. The main reason for exclusion was that authors did not use randomisation.
Risk of bias in included studies
We present a summary of the 'Risk of bias' assessments in Figure 2 and Figure 3.
2.
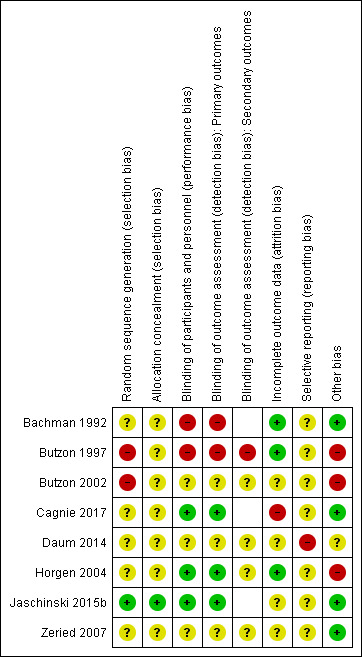
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
3.
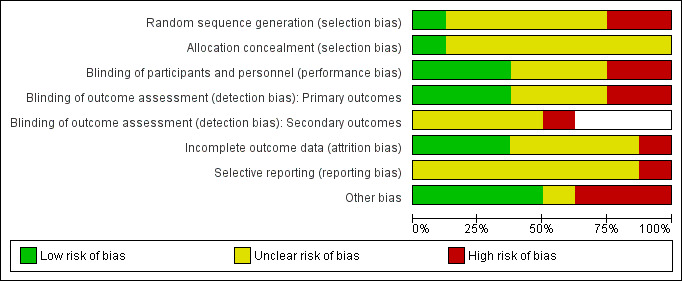
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Allocation
Except for the study by Jaschinski 2015b, none of the studies provided details on the procedure of randomisation or methods used to ensure concealment of allocation; therefore we judged the risk of selection bias to be unclear in five studies. In Jaschinski 2015b we judged randomisation procedures to be adequate and thus the risk of bias to be low. In the two remaining studies we judged random sequence generation to be at high risk of bias and concealment of allocation to be at unclear risk of bias (Butzon 1997; Butzon 2002).
Blinding
We considered two studies to be at high risk of performance bias because blinding of the intervention was impossible due to a visible difference between aspects of bifocal glasses and progressive glasses and no attempt was made to explain to the participants that both glasses were considered equally effective (Bachman 1992; Butzon 1997), For the same reason, we judged the risk of detection bias for the primary outcome (participant‐reported symptoms) to be high in these two studies. Even though optical characteristics of computer glasses make them unsuitable for use all‐day long (Cagnie 2017; Jaschinski 2015b) and thus participants could notice the difference, the authors presented them as equally valid and made them look completely similar. Therefore, we judged the risk of performance bias to be low in these two studies. We judged the risk of performance bias and detection bias of primary outcomes to be unclear in three studies (Butzon 2002; Daum 2014; Zeried 2007); and low in the two remaining studies (Horgen 2004; Jaschinski 2015b). Five studies reported secondary outcomes (Butzon 1997; Butzon 2002; Daum 2014; Horgen 2004; Zeried 2007). We judged the risk of detection bias to be high for the secondary outcomes in one study (Butzon 1997); and unclear in the remaining four studies.
Incomplete outcome data
We judged one study to be at high risk of attrition bias due to persons missing for reasons related to the type of interventions (Cagnie 2017). We considered four studies to be at unclear risk of attrition bias because there was no information about completeness of outcome data (Butzon 2002; Daum 2014; Jaschinski 2015b; Zeried 2007). We judged the risk of attrition bias to be low in the other three studies (Bachman 1992; Butzon 1997; Horgen 2004).
Selective reporting
For two studies we identified a study protocol (Daum 2014; Zeried 2007). As registration of the protocol was post hoc for the study of Zeried 2007, we judged the risk of reporting bias for this study to be unclear. For Daum 2014, results for outcomes not listed in the protocol were presented and therefore we judged the risk of reporting bias to be high. No study protocol was identified for the remaining six studies; we therefore considered them to be at an unclear risk of bias (Bachman 1992; Butzon 1997; Butzon 2002; Cagnie 2017; Horgen 2004; Jaschinski 2015b).
Other potential sources of bias
The Horgen 2004 study did not provide any information on characteristics of included participants. Based on the data presented in figures, we suspect that there were baseline differences between intervention and control groups. Therefore we judged this study to be at a high risk of other bias. We also judged Butzon 1997 and Butzon 2002 to be at high risk of other bias because in these cross‐over studies there was no wash‐out period between the interventions and therefore a carry‐over effect can not be excluded. The study by Daum 2014 reported no information on the study groups and therefore we had no alternative but judge the study to be at unclear risk of other bias. We judged the risk of other bias to be low in the remaining four studies (Bachman 1992; Cagnie 2017; Jaschinski 2015b; Zeried 2007).
Overall risk of bias
Based on risk of bias for allocation concealment, detection and attrition bias, we judged one study to be at an overall low risk of bias (Jaschinski 2015b); and two studies to be at an overall high risk of bias (Bachman 1992; Butzon 1997). The remaining five studies we judged to be at an overall unclear risk of bias because these studies had an unclear risk of bias for all key domains.
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5; Table 6; Table 7
Summary of findings for the main comparison. Progressive computer glasses versus monofocal computer glasses.
| Various progressive computer glasses compared with monofocal computer glasses for asthenopia | |||||
|
Patient or population: computer workers Settings: workplace Intervention: progressive computer glasses Comparison: monofocal computer glasses | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk2 | Corresponding risk | ||||
| Monofocal computer glasses | Progressive computer glasses | ||||
| Asthenopia (change from baseline to 12 months) VAS scale 0 to 100 12 months' follow‐up |
The mean asthenopia change score in the control group was 2.51 | The mean asthenopia change score in the intervention group was 0.23 score points higher (4.97 lower to 5.00 higher) | 186 (1) | ⊕⊕⊝⊝ low1 | Change scores based on imputed correlation coefficient (0.7). Sensitivity analysis revealed no change |
| Headache (change from baseline to 12 months) VAS scale 0 to 100 12 months' follow‐up |
The mean headache change score in the control group was −3.42 | The mean headache change score in the intervention group was 11.02 score points higher (5.17 higher to 16.87 higher) | 186 (1) | ⊕⊝⊝⊝ low1 | Change scores based on imputed correlation coefficient (0.7) |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval | |||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | |||||
1 We downgraded the quality of evidence with one level because of risk of bias and with one level because of imprecision (less than 300 participants).
2 This is the mean change score in the control group.
Summary of findings 2. Progressive computer glasses with intermediate distance focus versus progressive glasses for daily use.
| Progressive computer glasses with intermediate focus compared with progressive glasses for daily use for asthenopia | |||||
|
Patient or population: computer workers Settings: workplace Intervention: progressive computer glasses with intermediate distance focus Comparison: progressive glasses for daily use | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk2 | Corresponding risk | ||||
| Progressive glasses for daily use | Progressive computer glasses | ||||
| Asthenopia (two different scales), Short term follow‐up |
The standardized mean asthenopia score in the intervention group was 0.49 SD lower (0.75 lower to 0.23 lower) | 58 (2) | ⊕⊕⊝⊝ low1 | One cross‐over trial, (paired analysis) and one parallel trial | |
| Asthenopia Medium term follow‐up (6 months) |
The standardized mean asthenopia score in the intervention group was 0.64 SD lower (1.40 lower to 0.12 higher) | 35 (1) |
⊕⊕⊝⊝ low1 | ||
| Headache scale 1 to 6 1‐week follow‐up |
The mean headache score in the control group was 1.8 | The mean headache change score in the intervention group was 0.24 score points lower (0.55 lower to 0.07 higher) | 23 (1) | ⊕⊕⊝⊝ low1 | Cross‐over trial, paired analysis |
| Dizziness score 1 to 6 1‐week follow‐up |
The mean dizziness score in the control group was 1.08 | The mean dizziness score in the intervention group was 0.29 score points lower (0.51 lower to 0.07 lower) | 23 (1) | ⊕⊕⊝⊝ low1 | Cross‐over trial, paired analysis |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval | |||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | |||||
1 We downgraded the quality of evidence with two levels because of imprecision (less than 300 participants).
2 This is the mean change score in the control group
Summary of findings 3. Progressive computer glasses with intermediate distance focus versus monofocal computer glasses.
| Progressive computer glasses plus intermediate focus compared with monofocal computer glasses for asthenopia | |||||
|
Patient or population: computer workers Settings: workplace Intervention: progressive computer glasses with intermediate distance focus Comparison: monofocal computer glasses | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk2 | Corresponding risk | ||||
| Monofocal computer glasses | Progressive computer glasses | ||||
| Asthenopia (change from baseline to 12 months) VAS scale 0 to 100 12 months' follow‐up |
The mean asthenopia change score in the control group was 2.51 | The mean asthenopia change score in the intervention group was 1.44 score points higher (6.95 lower to 9.83 higher) | 64 (1) | ⊕⊕⊝⊝ low1 | Change scores based on imputed correlation coefficient (0.7). Sensitivity analysis revealed no change |
| Headache (change from baseline to 12 months) VAS scale 0 to 100 12 months' follow‐up |
The mean headache change score in the control group was −3.42 | The mean headache change score in the intervention group was 10.73 score points higher (2.02 higher to 19.44 higher) | 64 (1) | ⊕⊝⊝⊝ very low3 | Change scores based on imputed correlation coefficient (0.7). Sensitivity analysis revealed different results for values of 0 and 0.9 |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval | |||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | |||||
1 We downgraded the quality of evidence with one level because of risk of bias and with one level because of imprecision (less than 300 participants).
2 This is the mean change score in the control group.
3 We downgraded the quality of evidence with one level because of risk of bias and with one level because of imprecision (less than 300 participants) and with one level again because of inconsistency in the sensitivity analysis.
Summary of findings 4. Progressive computer glasses with far distance focus compared to bifocal computer lenses.
| Progressive computer glasses with far distance focus compared to bifocal computer glassesfor preventing and treating asthenopia | ||||||
|
Patient or population: computer workers Setting: workplace Intervention: progressive computer glasses with far distance focus Comparison: bifocal computer glasses | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with Bifocal computer glasses | Risk with Progressive computer glasses | |||||
| Asthenopia (improvement of symptoms after 4 weeks) | Study population | RR 1.00 (0.80 to 1.24) | 38 (1 RCT) | ⊕⊝⊝⊝ very low 1 2 | Cross‐over trial, events during intervention and during control per total group at risk | |
| 895 per 1000 | 895 per 1000 (716 to 1000) | |||||
| Headache (improvement of symptoms after 4 weeks) | Study population | OR 1.43 (0.27 to 7.55) | 36 (1 RCT) | ⊕⊝⊝⊝ very low 1 2 | ||
| 778 per 1000 | 833 per 1000 (486 to 964) | |||||
| Nausea (improvement of symptoms after 4 weeks) | Study population | RR 1.29 (0.68 to 2.45) | 8 (1 RCT) | ⊕⊝⊝⊝ very low 1 2 | ||
| 750 per 1000 | 968 per 1000 (510 to 1000) | |||||
| Dizziness (improvement of symptoms after 4 weeks) | Study population | RR 1.00 (0.25 to 4.00) | 8 (1 RCT) | ⊕⊝⊝⊝ very low 1 2 | ||
| 500 per 1000 | 500 per 1000 (125 to 1000) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; OR: Odds ratio; | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect | ||||||
1 We downgraded the quality of evidence with two levels because of unclear risk of selection bias, high risk of performance bias and detection bias.
2 We downgraded the quality of evidence with one level because of very small sample size, i.e. the optimal information size not reached.
Summary of findings 5. Progressive computer glasses with far distance focus versus trifocal computer glasses.
| Progressive computer glasses plus far distance focus compared with trifocal computer glasses for asthenopia | |||||
|
Patient or population: computer workers Settings: workplace Intervention: progressive computer glasses with far distance focus Comparison: trifocal computer glasses | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk2 | Corresponding risk | ||||
| Trifocal computer glasses | Progressive computer glasses | ||||
| Asthenopia (eyestrain severity) Likert scale 0 to 10 3 weeks follow‐up |
The mean asthenopia score in the control group was 1.46 | The mean asthenopia score in the intervention group was 0.5 score points lower (1.46 lower to 0.46 higher) | 24 (1) | ⊕⊝⊝⊝ very low1 | Cross‐over trial, unpaired analysis |
| Asthenopia (eyestrain frequency) Likert scale 0 to 10 3 weeks' follow‐up |
The mean asthenopia score in the control group was 2.51 | The mean asthenopia score in the intervention group was 0.75 score points lower (2.45 lower to 0.95 higher) | 24 (1) | ⊕⊝⊝⊝ very low1 | Cross‐over trial, unpaired analysis |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval | |||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | |||||
1 We downgraded the quality of evidence with two levels because of high risk of bias and with one level because of imprecision (less than 300 participants).
2 This is the mean change score in the control group.
3 We downgraded the quality of evidence with one level because of risk of bias and with one level because of imprecision (less than 300 participants) and with one level again because of inconsistency in the sensitivity analysis.
Summary of findings 6. Progressive computer glasses with far distance focus versus monofocal computer glasses.
| Progressive computer glasses plus far distance focus compared with monofocal computer glasses for asthenopia | |||||
|
Patient or population: computer workers Settings: workplace Intervention: progressive computer glasses with far‐distance focus Comparison: monofocal computer glasses | |||||
| Outcomes | Illustrative comparative risks* (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk2 | Corresponding risk | ||||
| Monofocal computer glasses | Progressive computer glasses | ||||
| Asthenopia (change from baseline to 12 months) VAS scale 0 to 100 12 months' follow‐up |
The mean asthenopia change score in the control group was 2.51 | The mean asthenopia change score in the intervention group was 1.79 score points lower (11.60 lower to 8.02 higher) | 64 (1) | ⊕⊕⊝⊝ low1 | Change scores based on imputed correlation coefficient (0.7). Sensitivity analysis revealed no change |
| Headache (change from baseline to 12 months) VAS scale 0 to 100 12 months' follow‐up |
The mean headache change score in the control group was −3.42 | The mean headache change score in the intervention group was 8.21 score points higher (4.55 lower to 20.97 higher) | 64 (1) | ⊕⊝⊝⊝ very low3 | Change scores based on imputed correlation coefficient (0.7). Sensitivity analysis revealed different results for values of 0 and 0.9 |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval | |||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | |||||
1 We downgraded the quality of evidence with one level because of risk of bias and with one level because of imprecision (less than 300 participants).
2 This is the change score in the control group.
3 We downgraded the quality of evidence with one level because of risk of bias and with one level because of imprecision (less than 300 participants) and with one level again because of inconsistency in the sensitivity analysis.
Summary of findings 7. Computer glasses versus Ergonomic assessment plus habitual (computer) glasses.
| Computer glasses adapted to need compared with ergonomic assessment plus habitual (computer) glasses | ||||||
|
Patient or population: computer workers Settings: workplace Intervention: computer glasses Comparison: ergonomic assessment plus habitual glasses | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative Effect (RR 95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk2 | Corresponding risk | |||||
| Ergonomics | Computer glasses | |||||
| Asthenopia, summed score scale 1 to 140 3 weeks' follow‐up |
The mean asthenopia score in the control group was 24 | The mean asthenopia score in the intervention group was 8.9 score points lower (16.47 lower to 1.33 lower) | 24 (1) | ⊕⊝⊝⊝ very low1 | Cross‐over trial, paired analysis | |
| Asthenopia Change score 3 weeks' follow‐up |
The mean asthenopia change score in the control group was 20.4 | The mean asthenopia change score in the intervention group was 17.5 score points lower (23.5 lower to 11.5 lower | 24 (1) | ⊕⊝⊝⊝ very low1 | Change scores calculated based on correlation of 0.7. Sensitivity analysis did not reveal big differences | |
| Eyestrain (yes/no) 3 weeks' follow‐up | 690 per 1000 | 657 per 1000 (463 to 927) | RR 0.95 (95% CI 0.67 to 1.34) | 24 (1) | ⊕⊝⊝⊝ very low1 | Cross‐over trial |
| Headache (yes/no) 3 weeks' follow‐up | 461 per 1000 | 424 per 1000 (240 to 752) | RR 0.92 (95% CI 0.52 to 1.63) | 24 (1) |
⊕⊝⊝⊝ very low1 | Cross‐over trial |
| Upset stomach (yes/no) 3 weeks' follow‐up | 115 per 1000 | 57 per 1000 (16 to 206) | RR 0.50 (95% CI 0.14 to 1.79) | 24 (1) |
⊕⊝⊝⊝ very low1 | Cross‐over trial |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval | ||||||
| GRADE Working Group grades of evidence High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | ||||||
1 We downgraded the quality of evidence with two levels because of high risk of bias and with one level because of imprecision (less than 300 participants).
2 This is the mean change score in the control group.
There were no studies on prevention restricted to people without previous complaints. All studies included people with a certain level of eye complaints. However, none of the studies were treatment studies in the sense that a person came to see a physician or optometrist to ask for help with eye problems.
Presbyopic persons
1. Optical intervention versus another optical intervention
1.1 Eyeglasses
1.1.1 All progressive computer glasses (range N/C+/all additional ranges) versus monofocal computer glasses
We first analysed all types of progressive computer glasses with a nearby and computer‐distance focus regardless of other focal distances. To this end we combined three arms of Horgen 2004, which evaluated three different types of progressive computer glasses and compared these to monofocal glasses. We also evaluated these arms separately (see paragraphs 1.1.3, 1.1.5 and 1.1.6).
1.1.1.1 Patient reported symptoms of asthenopia ‐ long term follow up (1 year)
All three study arms with progressive computer glasses in the Horgen 2004 study did not have a substantial difference in the intensity of visual symptoms after one‐year follow‐up on a 100 mm VAS scale for symptoms compared to monofocal glasses (change score assumed correlation 0.7, MD 0.23, 95% CI −4.97 to 5.43, Analysis 1.1) at 12‐months follow‐up. Using different correlation coefficients for the calculation of the SDs of the change values did not make a difference (Analysis 1.2; Analysis 1.3). It seems reasonable to assume that the difference in end scores as presented in Analysis 1.4 is a result of the differences in baseline scores and that therefore the change scores present the treatment effects better.
1.1. Analysis.
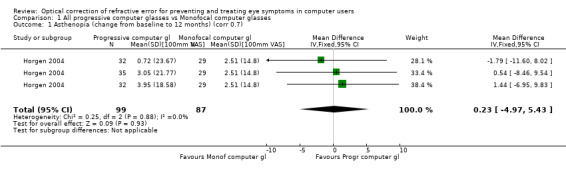
Comparison 1 All progressive computer glasses vs Monofocal computer glasses, Outcome 1 Asthenopia (change from baseline to 12 months) (corr 0.7).
1.2. Analysis.
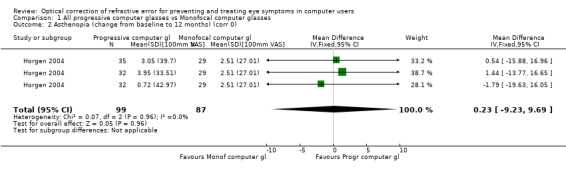
Comparison 1 All progressive computer glasses vs Monofocal computer glasses, Outcome 2 Asthenopia (change from baseline to 12 months) (corr 0).
1.3. Analysis.
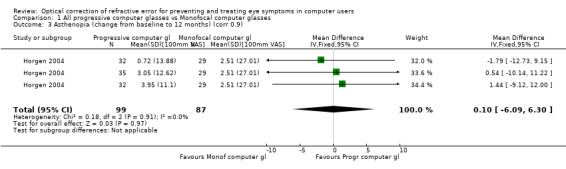
Comparison 1 All progressive computer glasses vs Monofocal computer glasses, Outcome 3 Asthenopia (change from baseline to 12 months) (corr 0.9).
1.4. Analysis.
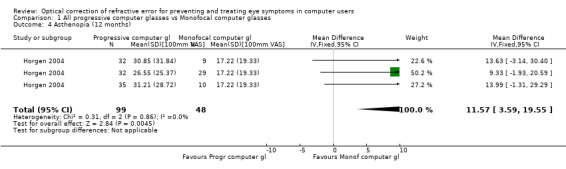
Comparison 1 All progressive computer glasses vs Monofocal computer glasses, Outcome 4 Asthenopia (12 months).
1.1.1.2 Adverse effects ‒ long‐term follow‐up (1 year)
In the same study by Horgen 2004, progressive computer glasses reduced headache intensity on a 100 mm VAS scale at 12‐months follow‐up (MD 11.02, 95% CI 5.17 to 16.87, change values (with r = 0.7, Analysis 1.5) compared to monofocal glasses. There was no considerable change of this result when changing the assumed correlation coefficients to r = 0 or r = 0.9 (Analysis 1.6; Analysis 1.7). Here too, the change scores present the treatment effects better than the end scores presented in Analysis 1.8).
1.5. Analysis.
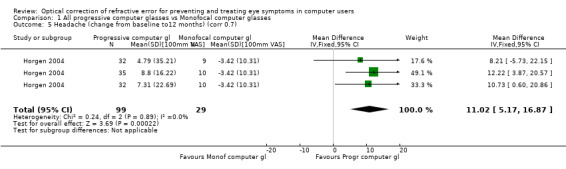
Comparison 1 All progressive computer glasses vs Monofocal computer glasses, Outcome 5 Headache (change from baseline to12 months) (corr 0.7).
1.6. Analysis.
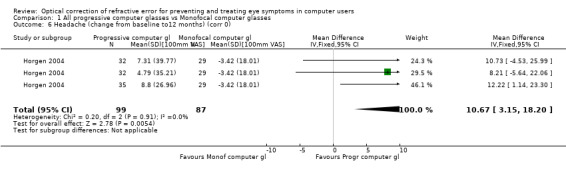
Comparison 1 All progressive computer glasses vs Monofocal computer glasses, Outcome 6 Headache (change from baseline to12 months) (corr 0).
1.7. Analysis.
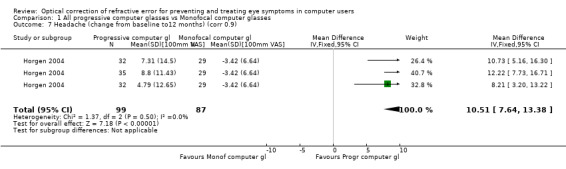
Comparison 1 All progressive computer glasses vs Monofocal computer glasses, Outcome 7 Headache (change from baseline to12 months) (corr 0.9).
1.8. Analysis.
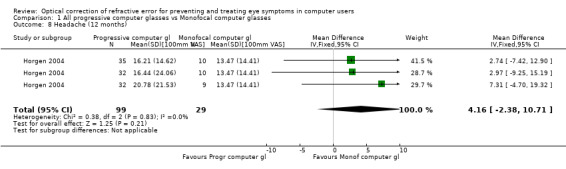
Comparison 1 All progressive computer glasses vs Monofocal computer glasses, Outcome 8 Headache (12 months).
1.1.1.3 Compliance ‒ long‐term follow‐up (1 year)
Compliance varied from 3.4 to 5.6 hours per day, with the best compliance for progressive computer glasses (N/C+) without any additional focus. The monofocal glasses were used 4.2 hours/day. The results could not be combined in a meta‐analysis because the authors did not report SDs.
1.1.2 Progressive computer glasses (range N/C+) versus general purpose bifocal glasses
1.1.2.1 Patient‐reported symptoms of asthenopia ‒ short‐term follow‐up (10 weeks)
The study by Daum 2014 reported greater visual comfort for subjects using progressive glasses compared to bifocal glasses (Chi² test, P = 0.004) but did not provide the data. The study did not report adverse effects.
1.1.2.2 Economic data ‒ short‐term follow‐up (10 weeks)
The study by Daum 2014 reported no significant difference in productivity between progressive glasses and bifocal glasses based on production and quality indicators but did not report any data to support this.
1.1.3 Progressive computer glasses (range N/C+) versus monofocal computer glasses
1.1.3.1 Patient‐reported symptoms of asthenopia ‒ long‐term follow‐up (1 year)
Horgen 2004 found no considerable difference in the intensity of visual symptoms after one‐year follow‐up (MD 0.54, 95% CI −8.46 to 9.54, change values r = 0.7, 100 mm VAS scale, Analysis 2.1). Using different correlation coefficients for the calculation of the SDs of the change values did not make a considerable difference (Analysis 2.2; Analysis 2.3). We present the end scores in Analysis 2.4.
2.1. Analysis.
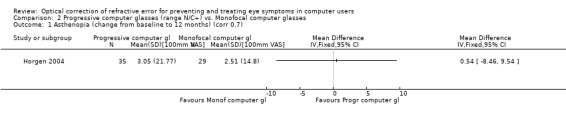
Comparison 2 Progressive computer glasses (range N/C+) vs. Monofocal computer glasses, Outcome 1 Asthenopia (change from baseline to 12 months) (corr 0.7).
2.2. Analysis.
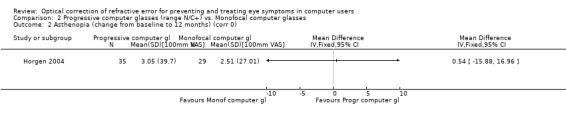
Comparison 2 Progressive computer glasses (range N/C+) vs. Monofocal computer glasses, Outcome 2 Asthenopia (change from baseline to 12 months) (corr 0).
2.3. Analysis.
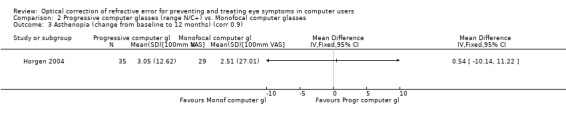
Comparison 2 Progressive computer glasses (range N/C+) vs. Monofocal computer glasses, Outcome 3 Asthenopia (change from baseline to 12 months) (corr 0.9).
2.4. Analysis.
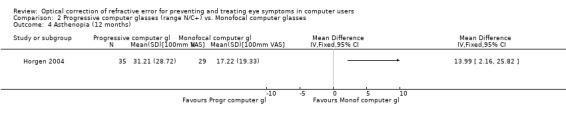
Comparison 2 Progressive computer glasses (range N/C+) vs. Monofocal computer glasses, Outcome 4 Asthenopia (12 months).
1.1.3.2 Adverse effects ‒ long‐term follow‐up (1 year)
In the same study by Horgen 2004, progressive computer glasses reduced headache intensity (MD 12.22, 95% CI 5.67 to 18.77, change values r = 0.7, Analysis 2.5) compared to monofocal glasses . This effect remained also when using correlation coefficients r = 0 and r = 0.9 (Analysis 2.6 and Analysis 2.7). We present the end scores in Analysis 2.8.
2.5. Analysis.
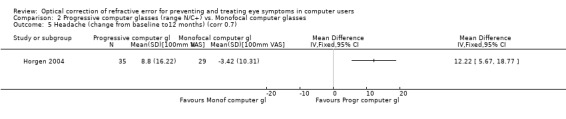
Comparison 2 Progressive computer glasses (range N/C+) vs. Monofocal computer glasses, Outcome 5 Headache (change from baseline to12 months) (corr 0.7).
2.6. Analysis.
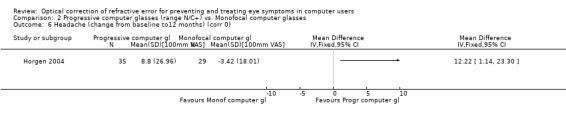
Comparison 2 Progressive computer glasses (range N/C+) vs. Monofocal computer glasses, Outcome 6 Headache (change from baseline to12 months) (corr 0).
2.7. Analysis.
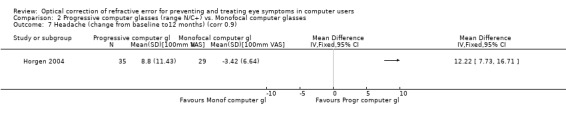
Comparison 2 Progressive computer glasses (range N/C+) vs. Monofocal computer glasses, Outcome 7 Headache (change from baseline to12 months) (corr 0.9).
2.8. Analysis.
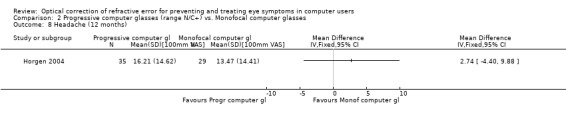
Comparison 2 Progressive computer glasses (range N/C+) vs. Monofocal computer glasses, Outcome 8 Headache (12 months).
1.1.3.3 Compliance ‒ long‐term follow‐up (1 year)
Horgen 2004 reported a mean difference in the total wearing time per day of 1.4 hours in favour of the progressive glasses compared to the monofocal glasses and reported that this was statistically significant but did not provide standard deviations.
1.1.4 Progressive computer glasses containing intermediate distance focus (range N/C+/IM) versus general purpose progressive glasses
1.1.4.1 Patient reported symptoms of asthenopia ‒ short‐term follow‐up
Two studies (Jaschinski 2015b; Cagnie 2017) combined in a meta‐analysis found a difference between progressive computer glasses and general purpose progressive glasses in eyestrain symptoms (SMD −0.49, 95% CI −0.75 to −0.23, Analysis 3.1).
3.1. Analysis.
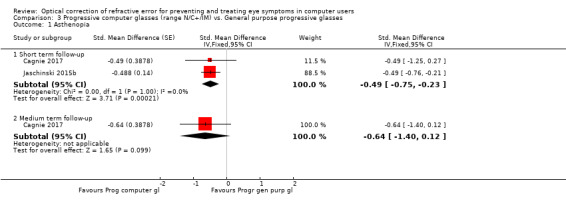
Comparison 3 Progressive computer glasses (range N/C+/IM) vs. General purpose progressive glasses, Outcome 1 Asthenopia.
1.1.4.1 Patient reported symptoms of asthenopia ‒ medium‐term follow‐up
Cagnie 2017 found a non‐significant effect of progressive computer glasses on eye strain compared to general purpose progressive glasses (SMD −0.64, 95% CI −1.40 to 0.12) at six months' follow‐up (Analysis 3.1).
1.1.4.2 Adverse effects ‒ short‐term follow‐up (1 month)
Jaschinski 2015b found no difference for headache (MD −0.24, 95% CI −0.55 to 0.07; Analysis 3.2) but did find a small difference in dizziness in favour of the progressive computer glasses compared to general purpose progressive glasses after one week of wearing (MD −0.29, 95% CI −0.51 to −0.07; Analysis 3.3).
3.2. Analysis.
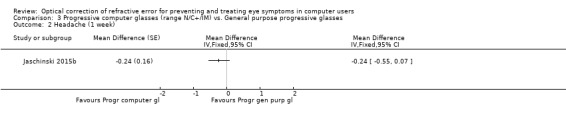
Comparison 3 Progressive computer glasses (range N/C+/IM) vs. General purpose progressive glasses, Outcome 2 Headache (1 week).
3.3. Analysis.
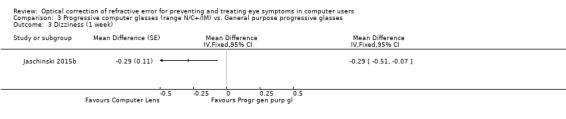
Comparison 3 Progressive computer glasses (range N/C+/IM) vs. General purpose progressive glasses, Outcome 3 Dizziness (1 week).
1.1.5 Progressive computer glasses containing intermediate distance focus (range N/C+/IM) versus monofocal computer glasses
1.1.5.1 Patient reported symptoms of asthenopia ‒ long‐term follow‐up (1 year)
The study by Horgen 2004 found no considerable difference in the intensity of visual symptoms after one‐year follow‐up (MD 1.44, 95% CI −6.95 to 9.83, change values r = 0.7, 100 mm VAS scale, Analysis 4.1). Using different correlation coefficients for the calculation of the SDs of the change values did not make a difference (Analysis 4.2; Analysis 4.3). We present the end scores in Analysis 4.4.
4.1. Analysis.
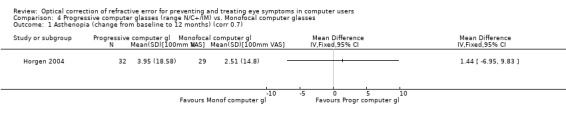
Comparison 4 Progressive computer glasses (range N/C+/IM) vs. Monofocal computer glasses, Outcome 1 Asthenopia (change from baseline to 12 months) (corr 0.7).
4.2. Analysis.
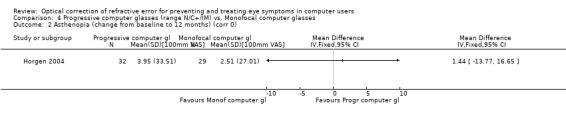
Comparison 4 Progressive computer glasses (range N/C+/IM) vs. Monofocal computer glasses, Outcome 2 Asthenopia (change from baseline to 12 months) (corr 0).
4.3. Analysis.
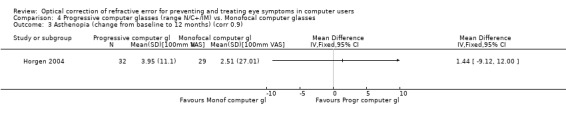
Comparison 4 Progressive computer glasses (range N/C+/IM) vs. Monofocal computer glasses, Outcome 3 Asthenopia (change from baseline to 12 months) (corr 0.9).
4.4. Analysis.
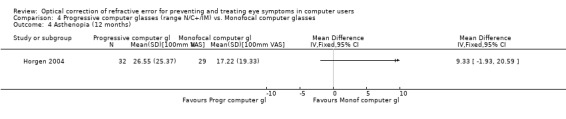
Comparison 4 Progressive computer glasses (range N/C+/IM) vs. Monofocal computer glasses, Outcome 4 Asthenopia (12 months).
1.1.5.2 Adverse effects ‒ long‐term follow‐up (1 year)
In the same study by Horgen 2004 progressive computer glasses resulted in less headache (MD 10.73, 95% CI 2.02 to 19.44, 100 mm VAS scale, change values r = 0.7, Analysis 4.5) when compared to monofocal computer glasses. However, the result depended on the imputed values of the correlation coefficients with r = 0 showing no statistically significant result (Analysis 4.6) and r = 0.9 showing a more statistically precise result (MD 10.73, 95% CI 5.16 to 16.30; Analysis 4.7). We present the end scores in Analysis 4.8.
4.5. Analysis.
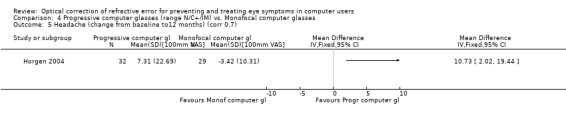
Comparison 4 Progressive computer glasses (range N/C+/IM) vs. Monofocal computer glasses, Outcome 5 Headache (change from baseline to12 months) (corr 0.7).
4.6. Analysis.
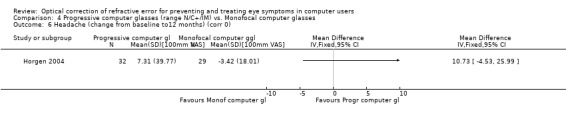
Comparison 4 Progressive computer glasses (range N/C+/IM) vs. Monofocal computer glasses, Outcome 6 Headache (change from baseline to12 months) (corr 0).
4.7. Analysis.
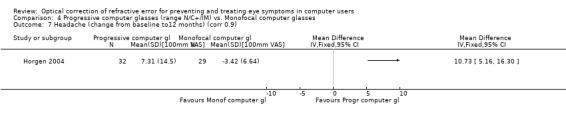
Comparison 4 Progressive computer glasses (range N/C+/IM) vs. Monofocal computer glasses, Outcome 7 Headache (change from baseline to12 months) (corr 0.9).
4.8. Analysis.
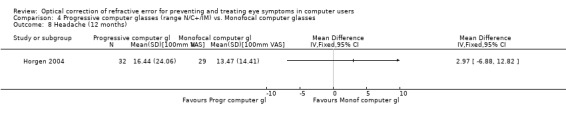
Comparison 4 Progressive computer glasses (range N/C+/IM) vs. Monofocal computer glasses, Outcome 8 Headache (12 months).
1.1.5.3 Compliance ‒ long‐term follow‐up (1 year)
Horgen 2004 reported a mean difference in the total wearing time per day of 0.2 hours in favour of the progressive glasses compared to the monofocal glasses and reported that this was statistically significant but did not provide standard deviations.
1.1.6 Progressive computer glasses containing far distance focus (range N/C+/F) versus monofocal glasses
1.1.6.1 Patient‐reported symptoms of asthenopia ‒ long‐term follow‐up (1 year)
The study by Horgen 2004 found no considerable difference in the intensity of visual symptoms after one year follow‐up (MD −1.79, 95% CI −11.60 to 8.02, 100 mm VAS scale, change values r = 0.7, Analysis 5.1) between the two types of glasses. Using different correlation coefficients for the calculation of the SDs of the change values did not make a difference (Analysis 5.2; Analysis 5.3). We present the end scores in Analysis 5.4.
5.1. Analysis.
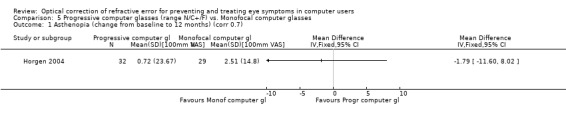
Comparison 5 Progressive computer glasses (range N/C+/F) vs. Monofocal computer glasses, Outcome 1 Asthenopia (change from baseline to 12 months) (corr 0.7).
5.2. Analysis.
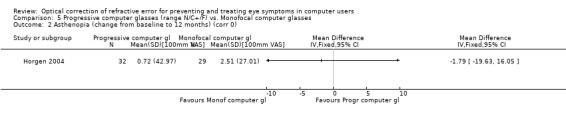
Comparison 5 Progressive computer glasses (range N/C+/F) vs. Monofocal computer glasses, Outcome 2 Asthenopia (change from baseline to 12 months) (corr 0).
5.3. Analysis.
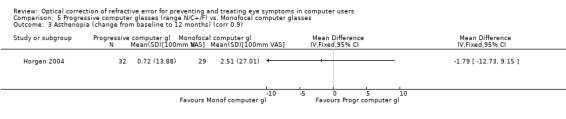
Comparison 5 Progressive computer glasses (range N/C+/F) vs. Monofocal computer glasses, Outcome 3 Asthenopia (change from baseline to 12 months) (corr 0.9).
5.4. Analysis.
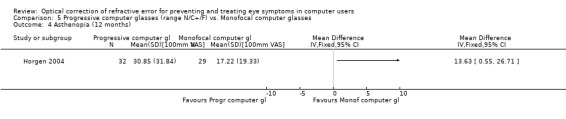
Comparison 5 Progressive computer glasses (range N/C+/F) vs. Monofocal computer glasses, Outcome 4 Asthenopia (12 months).
1.1.6.2 Adverse effects ‒ long‐term follow‐up (1 year)
In the same study by Horgen 2004, there was no effect of the lens type on headache intensity on a 100 mm VAS scale at 12‐months follow‐up (MD 8.21, 95% CI −4.55 to 20.97, change values r = 0.7, Analysis 5.5) but the result depended on the imputed values of the correlation coefficients with r = 0 showing no statistically significant result (Analysis 5.6), but r = 0.9 showing a statistically significant beneficial effect for the progressive glasses (MD 8.21, 95% CI 3.20 to 13.22, Analysis 5.7). We present the end scores in Analysis 5.8.
5.5. Analysis.
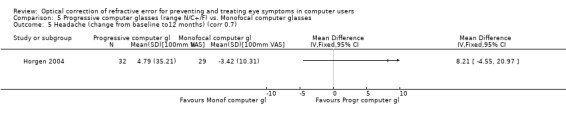
Comparison 5 Progressive computer glasses (range N/C+/F) vs. Monofocal computer glasses, Outcome 5 Headache (change from baseline to12 months) (corr 0.7).
5.6. Analysis.
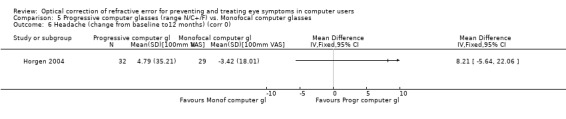
Comparison 5 Progressive computer glasses (range N/C+/F) vs. Monofocal computer glasses, Outcome 6 Headache (change from baseline to12 months) (corr 0).
5.7. Analysis.
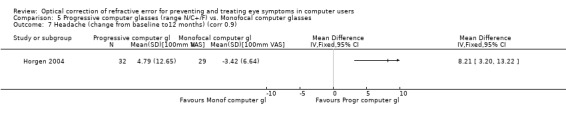
Comparison 5 Progressive computer glasses (range N/C+/F) vs. Monofocal computer glasses, Outcome 7 Headache (change from baseline to12 months) (corr 0.9).
5.8. Analysis.
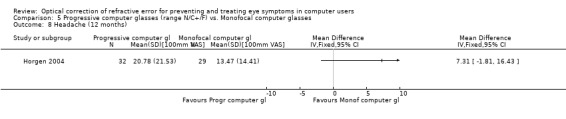
Comparison 5 Progressive computer glasses (range N/C+/F) vs. Monofocal computer glasses, Outcome 8 Headache (12 months).
1.1.6.3 Compliance ‒ long‐term follow‐up (1 year)
Horgen 2004 reported a mean difference in total wearing time per day of −0.8 hours for the progressive glasses compared to the monofocal glasses and reported that this was statistically significant but did not provide standard deviations (Analysis 5.9).
5.9. Analysis.
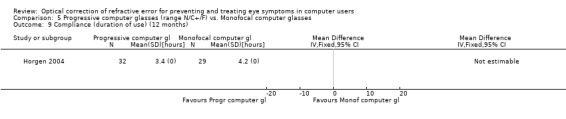
Comparison 5 Progressive computer glasses (range N/C+/F) vs. Monofocal computer glasses, Outcome 9 Compliance (duration of use) (12 months).
1.1.7 Progressive computer glasses containing far‐distance focus (range N/C+/F) versus bifocal computer glasses
1.1.7.1 Patient‐reported symptoms of asthenopia ‒ short‐term follow‐up (1 month)
Bachman 1992 found no difference in eyestrain for progressive glasses compared to alternative glasses (bifocal and single vision glasses were not separated in this analysis by the study authors) (OR 1.00, 95% CI 0.40 to 2.50; Analysis 6.1).
6.1. Analysis.
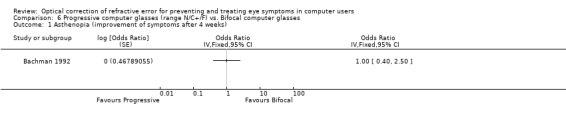
Comparison 6 Progressive computer glasses (range N/C+/F) vs. Bifocal computer glasses, Outcome 1 Asthenopia (improvement of symptoms after 4 weeks).
1.1.7.2 Adverse effects ‒ short‐term follow‐up (1 month)
Bachman 1992 found no considerable difference in headache (OR 1.00, 95% CI 0.17 to 5.94; Analysis 6.2), nausea (OR 1.33, 95% CI 0.33 to 5.40; Analysis 6.3), or dizziness (OR 1.00, 95% CI 0.40 to 2.50; Analysis 6.4) while wearing progressive computer glasses compared to bifocal computer glasses.
6.2. Analysis.
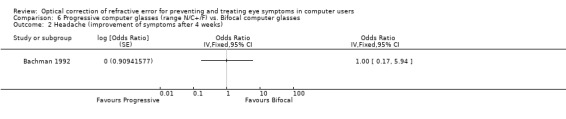
Comparison 6 Progressive computer glasses (range N/C+/F) vs. Bifocal computer glasses, Outcome 2 Headache (improvement of symptoms after 4 weeks).
6.3. Analysis.
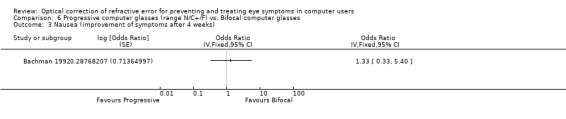
Comparison 6 Progressive computer glasses (range N/C+/F) vs. Bifocal computer glasses, Outcome 3 Nausea (improvement of symptoms after 4 weeks).
6.4. Analysis.
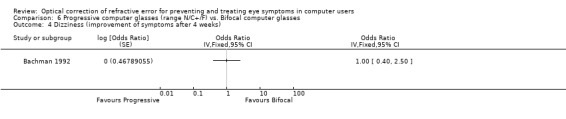
Comparison 6 Progressive computer glasses (range N/C+/F) vs. Bifocal computer glasses, Outcome 4 Dizziness (improvement of symptoms after 4 weeks).
1.1.8 Progressive computer glasses containing far distance focus (range N/C+/F) versus trifocal glasses
1.1.8.1 Outcome asthenopia ‒ short‐term follow‐up (3 weeks)
The study by Butzon 1997 found no considerable difference in asthenopia measured as severity of eyestrain (scale from 0 to 10, MD −0.50, 95% CI −1.07 to 0.07; Analysis 7.1) or measured as frequency of eyestrain (MD −0.75, 95% CI −1.61 to 0.11; Analysis 7.2) between the use of progressive computer glasses containing far‐distance focus and trifocal glasses. The study did not report adverse effects.
7.1. Analysis.
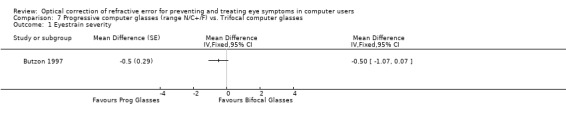
Comparison 7 Progressive computer glasses (range N/C+/F) vs. Trifocal computer glasses, Outcome 1 Eyestrain severity.
7.2. Analysis.
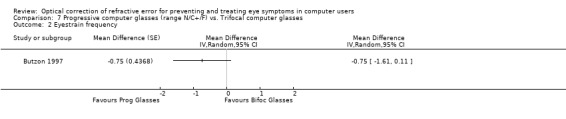
Comparison 7 Progressive computer glasses (range N/C+/F) vs. Trifocal computer glasses, Outcome 2 Eyestrain frequency.
1.1.8.2 Compliance ‒ short‐term follow‐up (3 weeks)
Butzon 1997 reported that during the intervention period participants wore progressive glasses for 74.6% and trifocal glasses for 73.8% of the work day respectively (no SDs provided). During the three‐week period in which participants directly compared the eyeglasses, they reported wearing the progressive glasses during 50% and trifocal glasses during 55% of the day (both at work and at home) (T = 0.82; P > 0.05).
1.2 Contact lenses
We did not identify any studies in which contact lenses were compared to another optical intervention in presbyopic persons.
1.3 Refractive surgery
We did not identify any studies in which refractive surgery was compared to an optical intervention in presbyopic persons.
2. Optical intervention vs. non‐optical intervention
2.1 Eyeglasses
2.1.1 Computer glasses versus ergonomic self‐assessment plus habitual refraction correction
2.1.1.1 Outcome asthenopia ‒ short‐term follow‐up (3 weeks)
The study by Butzon 2002 found a small beneficial effect of computer glasses on eyestrain severity (MD −8.90, 95% CI −16.47 to −1.33, scale from 0 to 140) compared to ergonomic self‐assessment (Analysis 8.1). The authors also report frequency of eyestrain at each measurement point. There was no considerable difference in eyestrain between the eyeglasses and the ergonomics group (OR 1.08, 95% CI 0.38 to 3.11, Analysis 8.2).
8.1. Analysis.
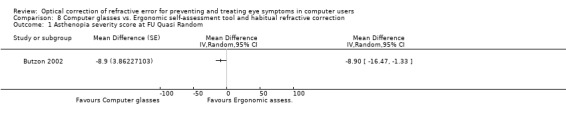
Comparison 8 Computer glasses vs. Ergonomic self‐assessment tool and habitual refractive correction, Outcome 1 Asthenopia severity score at FU Quasi Random.
8.2. Analysis.
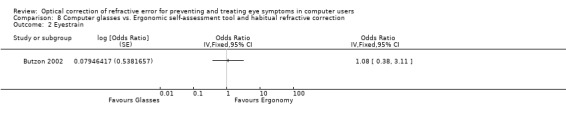
Comparison 8 Computer glasses vs. Ergonomic self‐assessment tool and habitual refractive correction, Outcome 2 Eyestrain.
2.1.1.2 Adverse outcomes ‒ short‐term follow‐up (3 weeks)
In the same study by Butzon 2002, the authors measured the frequency of headaches and upset stomach and there were no differences in the frequency between the eyeglasses and the ergonomics group (headache: OR 0.99, 95% CI 0.38 to 2.58, Analysis 8.3; upset stomach: OR 0.68, 95% CI 0.18 to 2.56, Analysis 8.4).
8.3. Analysis.
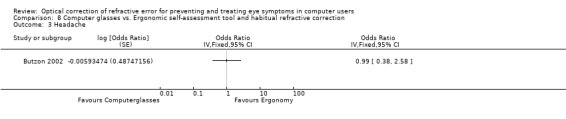
Comparison 8 Computer glasses vs. Ergonomic self‐assessment tool and habitual refractive correction, Outcome 3 Headache.
8.4. Analysis.
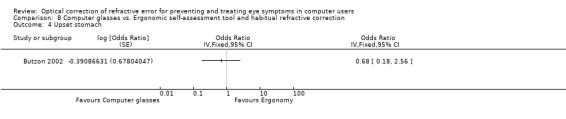
Comparison 8 Computer glasses vs. Ergonomic self‐assessment tool and habitual refractive correction, Outcome 4 Upset stomach.
2.2 Contact lenses
We did not identify any studies in which contact lenses were compared to a non‐optical intervention in presbyopic persons.
2.3 Refractive surgery
We did not identify any studies in which refractive surgery was compared to a non‐optical intervention in presbyopic persons.
Non‐presbyopic persons
1. Optical intervention versus optical intervention
1.1. Eyeglasses
1.1.1 Optimal versus habitual eyeglasses
1.1.1.1 Patient‐reported symptoms of asthenopia ‒ short‐term follow‐up (1 month)
Zeried 2007 reported a relationship between visual symptoms and the number of eyes with an uncorrected refractive error (no, one, or both eyes). The authors reported median values of the visual symtom index of 86.7, 91.1 and 84.4 for no, one or both eyes with an uncorrected refractive error of at least 0.50 dioptres, respectively (P = 0.029). However, the authors did not provide a more detailed explanation about the scoring of the visual symptom index. The study did not report adverse effects.
1.1.1.2 Difference in refractive error between optimal correction and own correction ‒ short‐term follow‐up (1 month)
Zeried 2007 reported a median difference in refractive error between best and habitual correction of 0.8 dioptres (SD 0.57, range 0 to 3.03 dioptres). It is, however, unclear whether this concerns the difference in one eye, or whether both eyes are taken into account.
1.1.1.3 Economic data ‒ short‐term follow‐up (1 month)
Zeried 2007 reported a relationship between productivity and the number of eyes with an uncorrected refractive error of at least 0.50 diopters (P = 0.001). The authors concluded that a low or absent degree of optical blur in at least one eye was related to the amount of work per hour. The authors did not present more detailed data.
1.2 Contact lenses
We did not identify any studies in which contact lenses were compared to another optical intervention in non‐presbyopic persons.
1.3 Refractive surgery
We did not identify any studies in which refractive surgery was compared to an optical intervention in non‐presbyopic persons.
2. Optical intervention versus non‐optical intervention
We did not identify any studies in which an optical intervention (either eyeglasses, contact lenses or refractive surgery) was compared to a non‐optical intervention in non‐presbyopic persons.
Quality of the evidence
We applied GRADE to all comparison‐outcome combinations and started with 'high quality' because we only included randomised controlled trials. We downgraded all comparisons because of risk of bias except for the comparison based on Jaschinski 2015b. We downgraded the comparisons that were based on Bachman 1992, Butzon 1997 and Butzon 2002 twice because of high risk of bias. We did not downgrade for indirectness because all comparisons were direct answers to the review question. We downgraded the quality of the evidence for comparisons in Horgen 2004 because of inconsistency in the results. We then downgraded all comparisons because of imprecision due to a low number of participants. We did not downgrade because of publication bias because we had only single‐study comparisons (and thus were not able to examine publication bias).
We did not rate the quality of the evidence of the studies that did not provide data and whose authors did not respond to our queries.
Discussion
Summary of main results
We identified eight studies that evaluated refractive error correction by means of eyeglasses. Six of these studied specially designed computer glasses in a presbyopic population and one studied the effect of correcting the refractive error in the best possible way in non‐presbyopic people. There are no studies on contact lenses or surgery. All of the included studies aimed at decreasing symptoms but none were in a treatment setting in which participants had asked for help. All studies focused on people at work who were symptomatic to a certain degree.
We found very low quality evidence that there is no considerable difference in asthenopia in the long term between the use of any type of progressive computer glasses and monofocal computer glasses (Table 1) but progressive computer glasses might reduce headache about 10% more than monofocal glasses. Progressive computer glasses might lead to better visual comfort than general purpose bifocal glasses but there are no quantitative data to support this.
There is low‐quality evidence that progressive computer glasses including intermediate distance focus may reduce asthenopia a little compared to progressive glasses for daily use in the short term but not in the intermediate term (Table 2). For the same type of glasses there is very low quality evidence of no considerable difference when compared to monofocal computer glasses in the long term (Table 3). For headache the results are in favour of the progressive glasses but the evidence is of very low quality. Progressive computer glasses might also decrease nausea and dizziness by about 10% but the evidence is of very low quality.
There is very low quality evidence that progressive computer glasses that include far‐distance focus do not have a considerable effect on asthenopia or headaches compared to bifocal computer glasses (Table 4) or trifocal glasses in the short term (Table 5) or compared to monofocal computer glasses (Table 6) in the long term.
There is very low quality evidence that individually adapted computer glasses might reduce asthenopia severity by about 40% more than ergonomic self‐assessment combined with habitual eyeglasses (Table 7). But there is no evidence of an effect on eyestrain frequency or on frequency of headaches or upset stomach.
Optimal correction of refractive error might lead to less asthenopia and better productivity than sub‐optimal refractive error correction but there are insufficient data to support this.
Overall completeness and applicability of evidence
It is unclear if the interventions in the included studies were all aimed at treating symptoms or at preventing symptoms. Having symptoms was an inclusion criterion in only two studies — Butzon 2002 and Jaschinski 2015b — but unclear in the other studies. It is therefore unclear if these interventions would work in a strictly preventive situation where only participants without symptoms would be included. It might, however, be difficult to find such a population in practice. Besides, as CVS is a collective term for eye and vision problems related to computer use, it covers a wide range of symptoms and there are no standardised diagnostic criteria, although asthenopia, a major complaint in people with CVS, is a formal diagnostic term.
We did not include musculoskeletal complaints such as neck and back pain in our review because we restricted the outcome to asthenopia. However, many authors include these complaints in what they call CVS. Neck complaints can be caused by both the ergonomic design of the workplace and the design of multifocal glasses. In the first update of this review, we will include these symptoms as a primary outcome in addition to asthenopia.
In seven of the included studies the intervention of interest is a specific type of eyeglasses: progressive computer glasses. Designs of progressive glasses are changing over time because of developments in knowledge and techniques. The American Optical TruVision Technical glasses are outdated and not available anymore. However, other eyeglasses such as the Essilor Interview glasses are still on the market — but it might be possible that whilst the name has not changed, the glasses have.
Only one of the seven included studies conducted a long‐term follow‐up where the other studies were evaluated over a period ranging from three to four weeks to six months, which we believe is insufficient to evaluate both beneficial and adverse effects.
Studies were conducted mainly in North America and Europe and studies from other continents are missing.
Quality of the evidence
Quality of the evidence is low to very low for all outcomes identified due to downgrading for risk of bias, inconsistency and imprecision; (see also Table 1; Table 2; Table 3; Table 5; Table 4; Table 6; Table 7). We found only small single studies for each comparison, which is why we downgraded the quality of evidence due to imprecision. In addition, the studies lacked good descriptions of the randomisation and allocation concealment processes.
Study authors assessed outcomes with questionnaires of questionable validity; and each study used its own questionnaire. Unfortunately, the studies we identified provide generally little data, as two studies were published only as a conference abstract and study protocol (Daum 2014; Zeried 2007), and one did not present quantitative results for the relevant comparisons (Horgen 2004). Our attempts to obtain additional information from study authors failed. Lack of data hampered the assessment of methodological quality of the studies, as well as analysis and interpretation of results. All in all, this led to the conclusion that the quality of the evidence was low to very low.
The cross‐over studies lacked a good rationale for the suitability of the cross‐over design. None of the cross‐over studies used a wash‐out period and we can imagine that being used to one type of eyeglasses causes problems when there is a sudden change to another type. Only one study used a habituation period. Given that asthenopia symptoms can change over time, it would be important to properly randomise participants but two studies used alternation instead of randomisation.
The study by Jaschinski 2015b allowed participants in the intervention group to choose a preferred 'maximum intermediate distance' between one and four metres and this could have diminished the contrast between intervention and control group. However, the viewing distance on the computer screen was always included in this type of glasses and we had included various distances within our category 'intermediate' (< 6 meters). Therefore we think that this has not biased the results of this study or our review.
Besides the fact that the identified studies are small and all but one had a high or unclear risk of bias, there is also possible influence by the optical industry because five studies were funded by producers of optical lenses, who have a big financial interest in promoting the quality of their product. As such, one would expect to see an overestimation of the effect but most studies found the eyeglasses having no considerable effects on asthenopia.
Potential biases in the review process
The author team changed considerably during the review process. However, the new authors redid all essential steps, which ensures uniformity in the review process.
The new author team also redesigned the systematic search strategies. The redesigned search strategy we used missed three of the included studies because none of these studies used a word indicating randomisation (Bachman 1992; Butzon 1997; Butzon 2002). However, as we searched many databases, grey literature and checked references, we believe that we identified all relevant randomised studies on optical correction for asthenopia in computer users.
We had to extract data from figures for two studies (Butzon 2002; Horgen 2004). We also calculated change values for these two studies because there were large baseline imbalances. To be able to calculate the SDs for these change values, we had to impute correlation coefficients. Since we had no data to make inferences about the magnitude of these, we conducted sensitivity analyses using various values of the correlation coefficient. Sometimes this led to inconsistent results, all of which we reported. This also led us to downgrade the quality of the evidence.
We had no preconceived categorisation of the various types of glasses that were designated as computer glasses by the authors. We classified all glasses that had a focus at the computer distance as computer glasses. We then made a distinction between progressive glasses (that gradually change focus) and those that have a sharp distinction between the focal areas of the lens. For the progressive glasses we made a distinction between including more focal areas than the computer distance and classified these as computer, computer plus intermediate or computer plus far distance. Since all interventions had different comparisons or follow‐up time, we could not pool any study results. Even though arbitrary, we believe that our categorisation is the best possible.
We searched for reports in any language and the original team searched a number of Chinese databases but this lead to no more included studies additional to those that had been published in English. We identified one article published in Russian and one in Chinese and we asked native speakers to assess their eligibility to this Cochrane review. Both judged their respective studies to be ineligible. Consequently, we believe that we avoided language bias effectively.
Agreements and disagreements with other studies or reviews
We are aware of two systematic reviews reporting on the effect of refractive error correction on asthenopia in computer users (Brewer 2006; Leyshon 2010). These systematic reviews studied the effect of several ergonomic interventions one of which was refractive error correction. The review by Brewer 2006 focused on computer workers without symptoms and thus on the prevention of visual and musculoskeletal symptoms. Whereas the study population of interest in the Leyshon 2010 review was computer workers with musculoskeletal disorders of the upper limb, neck, low back, and eye. Both reviews identified the same four primary studies on refractive error correction. We also identified these four studies and considered them for inclusion in our review.
Three non‐randomised studies that we excluded from this systematic review studied the effect of eyeglasses on visual symptoms (Aarås 1998; Guo 2010; Wallin 1994). All of these non‐randomised studies reported a positive effect of eyeglasses on visual symptoms. Of these, one study compared different types of eyeglasses and found a beneficial effect of progressive glasses compared to monofocal glasses (Guo 2010).
In the EU, there has been regulation in force since 1990 (90/270/EEC) that requires employers to provide workers with special corrective appliances if normal corrective appliances cannot be used (European Council 1990). However, there is no supporting evidence review and there are no criteria to assess if normal corrective glasses cannot be used. In practice, in most countries in the EU, this means that workers would be prescribed computer glasses as defined in this review. This could be any type of glasses that have a larger focal area for the distance of the computer screen than glasses that are in everyday use. Nowadays, most elderly people use multifocal glasses that have gradually changing focal areas ranging from nearby to the far distance. The only difference with computer glasses is that computer glasses would have a larger focal area for the computer distance than multifocal glasses for everyday use. In addition, the use of computers is not confined to the workplace anymore but ubiquitous also at home. The use of standalone computers is also rapidly changing to laptops, tablets and mobile phones for which the computer glasses might not be the most appropriate aid. Therefore, some authors have suggested that this EU legal requirement might be outdated (Johnson 2012). However, in a survey of stakeholders' opinions, both employers and trade unions questioned if these legal requirements should be updated (Niskanen 2015).
Authors' conclusions
Implications for practice.
We found low to very low quality evidence that progressive computer glasses with or without focal areas for intermediate or long distance do not have a considerable effect on asthenopia or on headache compared to monofocal, bifocal, or trifocal glasses in persons with presbyopia who work with computers. However, progressive computer glasses also including intermediate or far‐distance focus might have a small beneficial effect in the short term compared to glasses for daily use but it is unclear if this can be sustained in the long term. A proportion of participants in all studies had complaints of asthenopia at the start of the study and it is unclear if the results are also applicable to a situation in which participants would have no asthenopia at the start of the intervention. There are no studies that have used computer glasses as a treatment for people that ask for help with their asthenopia.
There are insufficient data to draw conclusions on the effect of best possible optical correction.
Implications for research.
There is a need for parallel group randomised studies that should better report their methods to enable judgement of the risk of bias. The risk of bias in studies can be decreased by blinding participants and providers, which can be achieved by providing the intervention eyeglasses in exactly the same frame with a code and not presenting them as superior. A uniform standardised outcome measure for asthenopia should be used, like the Computer Vision Questionnaire (del Mar Seguí 2015). Studies should be conducted in participants who clearly suffer from asthenopia or in participants who are clearly free from these complaints but at risk of developing them, such as older workers.
Cross‐over studies should at least properly randomise the order of the interventions and include habituation and wash‐out periods. The results should be reported as intra‐person differences with the standard deviations.
Given that most studies included in this review show no evidence of a considerable effect, the effect size is expected to be small. This means that studies are needed with at least several hundred participants to have enough power to detect small effect sizes.
Follow‐up of the participants to assess the outcomes should be at least a year because we would like to know if these optical corrections work in the long run.
New studies should clearly describe the construction of the eyeglasses that they provide for computer work and a rationale as to why this would decrease symptoms. Given that most workers have various tasks that require various focal areas, glasses with focal areas for nearby, computer distance and distance beyond the computer are probably the most useful.
Acknowledgements
We would like to acknowledge the guidance and support of Cochrane Work, in particular Leena Isotalo and Kaisa Neuvonen for their help in designing and conducting the searches, and Jani Ruotsalainen for assisting with screening retrieved references. We also would like to thank René Spijker, Information Specialist at Cochrane Netherlands, for running the search updates in 2016 and 2017. Furthermore we would like to thank the native speakers that assisted in judging eligibility of the articles in Russian and Chinese.
The protocol for this review was designed and written by Hong‐Hao Li, Pauline Heus, Ling Li, Juan Yang, Jie Kuang, You‐Ping Li, and Tao Xiong; and was published in May 2012. In 2014, the author team preparing the review changed considerably. We are much indebted to the former authors for their contribution to the protocol.
Finally we would like to thank the peer reviewers: Carel Hulshof, Enembe Okokon and Anneli Ojajärvi for providing feedback on the protocol, and Kerry Dwan, Simon Turner, Miguel Sergio Kabilio, John Broderick, and Carel Hulshof for providing feedback on the review and Jason Elliot‐Smith and Jani Ruotsalainen for copy editing the review text.
Appendices
Appendix 1. Terms and their explanations
| Terms | Explanations |
| Myopia (nearsightedness) |
the image of distant objects focuses in front of the retina in the unaccommodated eye, resulting in difficulty in seeing distant objects clearly |
| Hyperopia (farsightedness) | the image of distant objects focuses behind the retina in the unaccommodated eye, resulting in difficulty in seeing close objects clearly; |
| Astigmatism | the eye produces an image with multiple focal points or lines, i.e. distorted vision resulting from an irregularly curved cornea |
| Presbyopia | a vision condition in which the crystalline lens of the eye loses its flexibility, which makes it difficult for patients to focus on close objects. It differs from the other disorders in that it is linked to ageing and occurs almost universally |
| Vergence | simultaneous movement of both eyes in opposite directions to obtain or maintain binocular single vision |
| Latent strabismus or heterophoria |
the tendency, controllable by muscular effort, for one or both eyes to exhibit strabismus |
| Amblyopia (lazy eye) | a disorder of the visual system that is characterised by a vision deficiency in an eye that is otherwise physically normal, or out of proportion to associated structural abnormalities of the eye |
| Strabismus (squint) | a disorder in which the two eyes do not line up in the same direction |
Appendix 2. Possible interventions to be included
| Optical correction of refractive error |
Eyeglasses | Unifocal/Single glasses |
Spherical and/or toric (i.e. cylindrical) |
| Bifocal glasses Trifocal glasses Multifocal/progressive glasses |
Spherical and/or toric with addition(s) for near and or intermediate distances | ||
| Contact lenses | Unifocal | Spherical and/or toric | |
| Orthokeratology, which refers to the use of rigid gas‐permeable contact lenses, normally worn only at night, to improve vision through the reshaping of the cornea. | |||
| Multifocal | Spherical and/or toric with addition for near and or intermediate distances | ||
| Refractive surgery |
Lenses, Intraocular (IOLs) | Anterior chamber IOLs, Posterior chamber IOLs | |
| Corneal Surgery, Laser | lamellar (LASIK, intraLASIK/FemtoLASIK) and surface (photorefractive keratectomy [PRK], laser epithelial keratomileusis [LASEK], and Epi‐LASIK) ablation | ||
| Keratotomy, Radial | A procedure that consists of making numerous radial incisions which extended from the pupil to the periphery of the cornea in a pattern like the spokes of a wheel. |
Appendix 3. Search strategy
| database | search strategy |
| PubMed (1966 ‐ January 11, 2017) | Search #1 AND #2 AND #3 #3 (randomized controlled trial[pt] OR controlled clinical trial[pt] OR randomized[tiab] OR placebo[tiab] OR clinical trials as topic [mesh: noexp] OR randomly[tiab] OR trial[ti]) NOT (Animals[Mesh] NOT Humans[Mesh]) #2 computers[Mesh] OR "computer terminals"[Mesh] OR "computer screen"[tw] OR "computer screens"[tw] OR "display screen"[tw] OR "display screens"[tw] OR "computer monitor"[tw] OR "computer monitors"[tw] OR "PC monitor"[tw] OR "PC monitors"[tw] OR "computer display"[tw] OR "computer use"[tw] OR "visual display unit"[tw] OR "visual display units"[tw] OR "video display unit"[tw] OR "video display units"[tw] OR vdu[tw] OR vdus[tw] OR "screen‐based equipment"[tw] OR sbe[tw] OR sbes[tw] OR "computer work"[tw] OR "office work"[tw] OR "near work"[tw] #1 "Refractive Errors"[Mesh] OR "Presbyopia"[Mesh] OR "Hyperopia"[Mesh] OR "Myopia"[Mesh] OR "Astigmatism"[Mesh] OR "Asthenopia"[Mesh] OR "refractive error"[tw] OR "refractive errors"[tw] OR ametropia[tw] OR presbyopia[tw] OR farsight*[tw] OR longsight*[tw] OR myopia*[tw] OR nearsight*[tw] OR "visual discomfort"[tw] OR eyestrain[tw] OR "eye fatigue" OR "visual fatigue"[tw] OR "blurred vision"[tw] OR "doubled vision"[tw] OR "computer vision syndrome"[tw] OR CVS[tw] OR "visual symptom"[tw] OR "eye ache"[tw] OR diplopia[tw] OR "eye problems"[tw] OR "vision problems"[tw] OR "visual symptoms"[tw] OR "visual complaints"[tw] OR "ocular complaints"[tw] OR "asthenopic symptoms"[tw] OR "dry eye"[tw] OR "dry eyes"[tw] OR "accommodation, ocular"[Mesh] OR "visual acuity"[Mesh] |
| EMBASE (unique NOT Medline, until January 11, 2017) | #1 'refraction error'/exp OR 'presbyopia'/exp OR 'hypermetropia'/exp OR 'myopia'/exp OR 'astigmatism'/exp OR 'asthenopia'/exp OR 'accommodation'/exp OR 'visual acuity'/exp OR 'refractive error'/de OR 'refractive error' OR ametropia OR 'presbyopia'/de OR presbyopia OR farsight* OR longsight* OR myopia* OR nearsight* OR 'visual discomfort' OR 'ocular discomfort' OR eyestrain OR 'eye fatigue' OR 'visual fatigue' OR 'blurred vision'/de OR 'blurred vision' OR 'doubled vision' OR 'computer vision syndrome' OR 'cvs' OR 'visual symptom' OR 'eye ache' OR 'diplopia'/de OR diplopia OR 'eye problems' OR 'vision problems' OR 'visual symptoms' OR 'visual complaints' OR 'ocular complaints' OR 'asthenopic symptoms' OR 'dry eye'/de OR 'dry eye' OR 'schirmer test'/de OR 'schirmer test' OR 'tear film'/de OR 'tear film' OR blinking OR 'visual performance' OR 'visual disorder'/de OR 'visual disorder' OR 'vision'/de #2 'computer'/exp OR 'computer terminal'/exp OR 'computer screen' OR 'display screen' OR 'computer monitor' OR 'pc monitor' OR 'computer display' OR 'computer use' OR 'visual display unit'/de OR 'visual display unit' OR 'video display unit' OR 'vdu' OR 'vdus' OR 'screen‐based equipment' OR 'sbe' OR 'sbes' OR 'computer work' OR 'office work' OR 'near work' OR 'work'/de OR 'work' OR 'worker'/de OR 'worker' OR 'employee'/de OR 'employee' #3 'randomized controlled trial (topic)'/de OR 'crossover procedure'/de OR 'double blind procedure'/de OR 'single blind procedure'/de OR random* OR factorial* OR crossover* OR cross NEAR/1 over* OR placebo* OR doubl* NEAR/1 blind* OR singl* NEAR/1 blind* OR assign* OR allocat* OR volunteer* #4 #1 AND #2 AND #3 #4 NOT ([medline]/lim NOT [embase]/lim) #4 AND [embase]/lim |
| CENTRAL (until January 11, 2017) | #1 MeSH descriptor: [Refractive Errors] explode all trees #2 MeSH descriptor: [Presbyopia] explode all trees #3 MeSH descriptor: [Hyperopia] explode all trees #4 MeSH descriptor: [Myopia] explode all trees #5 MeSH descriptor: [Astigmatism] explode all trees #6 MeSH descriptor: [Asthenopia] explode all trees #7 MeSH descriptor: [Accommodation, Ocular] explode all trees205 #8 MeSH descriptor: [Visual Acuity] explode all trees #9 #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 #10 "refractive error" #11 "refractive errors" #12 ametropia #13 presbyopia #14 farsight* #15 longsight* #16 myopia* #17 nearsight* #18 "visual discomfort" #19 eyestrain #20 "eye fatigue" #21 "visual fatigue" #22 "blurred vision" #23 "doubled vision" #24 "computer vision syndrome" #25 CVS #26 "visual symptom" #27 "eye ache" #28 diplopia #29 "eye problems" #30 "vision problems" #31 "visual symptoms" #32 "visual complaints" #33 "ocular complaints" #34 "asthenopic symptoms" #35 "dry eye" #36 "schirmer test" #37 "dry eyes" #38 "ocular discomfort" #39 "tear film" #40 blinking #41 {or #10‐#40} #42 #9 or #41 #43 MeSH descriptor: [Computers] explode all trees #44 MeSH descriptor: [Computer Terminals] explode all trees #45 "computer screen" #46 "computer screens" #47 "display screen" #48 "display screens" #49 "computer monitor" #50 "computer monitors" #51 "PC monitor" #52 "PC monitors" #53 "computer display" #54 "computer use" #55 "visual display unit" #56 "visual display units" #57 "video display unit" #58 "video display units" #59 (vdu) #60 (vdus) #61 "screen‐based equipment" #62 (sbe) #63 (sbes) #64 "computer work" #65 "office work" #66 "near work" #67 {or #43‐#66} #68 #42 and #67 #69 #68 limit to trials |
| OSH‐update (CISDOC HSELINE IRSST NIOSHTIC NIOSHTIC‐2 RILOSH; until June 22 2017 |
#1 GW{"refraction error" OR "refractive error" OR "refractive errors" OR hypermetropia OR astigmatism OR asthenopia OR ametropia OR presbyopia OR farsight* OR longsight* OR myopia* OR nearsight* OR "visual discomfort" OR "ocular discomfort" OR eyestrain OR "eye fatigue" OR "visual fatigue" OR "blurred vision" OR "doubled vision" OR "computer vision syndrome" OR "CVS" OR "visual symptom" OR "eye ache" OR diplopia OR "eye problems" OR "vision problems" OR "visual symptoms" OR "visual complaints" OR "ocular complaints" OR "asthenopic symptoms" OR "dry eye" OR "dry eyes" OR "schirmer test" OR "tear film" OR "blinking" OR "visual performance" OR "visual disorder" OR "vision" OR "accommodation" OR "visual acuity"} #2 GW{computer* OR "computer terminal" OR "computer screen" OR "display screen" OR "computer monitor" OR "PC monitor" OR "computer display" OR "computer use" OR "visual display unit" OR "video display unit" OR "vdu" OR "vdus" OR "screen‐based equipment" OR "sbe" OR "sbes" OR "computer work" OR "office work" OR "near work" OR work OR worker OR employe*} #3 GW{intervent* OR random*} OR TW{trial*} #4 #1 AND #2 AND #3 #5 DC{OUBIB OR OUCISD OR OUHSEL OR OUISST OR OUNIOC OR OUNIOS OR OURILO} #6 #4 AND #5 |
| WoS (until January 11, 2017) | # 6 #4 NOT #5 Indexes=SCI‐EXPANDED, SSCI, A&HCI Timespan=All years # 5 TS=(animal* NOT human*) Indexes=SCI‐EXPANDED, SSCI, A&HCI Timespan=All years # 4 #1 AND #2 AND #3 Indexes=SCI‐EXPANDED, SSCI, A&HCI Timespan=All years # 3 TS=("randomized controlled trial" OR "controlled clinical trial" OR placebo OR "clinical trials" OR randomly OR intervent*) OR TI=trial Indexes=SCI‐EXPANDED, SSCI, A&HCI Timespan=All years # 2 TS=(computer* OR "computer terminal" OR "computer screen" OR "display screen" OR "computer monitor" OR "PC monitor" OR "computer display" OR "computer use" OR "visual display unit" OR "video display unit" OR "vdu" OR "vdus" OR "screen‐based equipment" OR "sbe" OR "sbes" OR "computer work" OR "office work" OR "near work" OR work OR worker OR employe*) Indexes=SCI‐EXPANDED, SSCI, A&HCI Timespan=All years # 1 TS=("refraction error" OR "refractive error" OR "refractive errors" OR hypermetropia OR astigmatism OR asthenopia OR ametropia OR presbyopia OR farsight* OR longsight* OR myopia* OR nearsight* OR "visual discomfort" OR "ocular discomfort" OR eyestrain OR "eye fatigue" OR "visual fatigue" OR "blurred vision" OR "doubled vision" OR "computer vision syndrome" OR "CVS" OR "visual symptom" OR "eye ache" OR diplopia OR "eye problems" OR "vision problems" OR "visual symptoms" OR "visual complaints" OR "ocular complaints" OR "asthenopic symptoms" OR "dry eye" OR "dry eyes" OR "schirmer test" OR "tear film" OR "blinking" OR "visual performance" OR "visual disorder" OR "vision" OR "accommodation" OR "visual acuity") Indexes=SCI‐EXPANDED, SSCI, A&HCI Timespan=All years |
Appendix 4. Information about the initial search strategy
(as presented in the protocol of this review)
Electronic searches
We will search the following electronic databases, from inception to date.
The Cochrane Central Register of Controlled Trials (CENTRAL) (which contains the Cochrane Eyes and Vision Group Trials Register), MEDLINE through PubMed, ISI Web of Knowledge and EMBASE.
We will also search the Cochrane Occupational Safety and Health Specialized Register. This register contains reports of trials identified from regular searches of MEDLINE and by handsearches.
We will search the WHO International Clinical Trials Registry Platform and clinical trials registries for ongoing studies.
We will also search five major mainland China academic literature databases using keywords in Chinese: CNKI (China National Knowledge Infrastructure) (1979 to 2012), VIP (Wei Pu Information) (1989 to 2012), Wang Fang Data (1980 to 2012), CMCI (Chinese Medical Citation Index) (1994 to 2012), CBM (Chinese Biologic Medical database) (1978 to 2012).
We will search the US Centers for Disease Control and Prevention, the National Institute for Occupational Safety and Health (NIOSHTIC‐2), and the International Occupational Safety and Health Information Centre (CIS) databases.
We will search the following websites to identify additional unpublished and ongoing studies:UK National Research Register (NRR) Archive, China Occupational Disease Network.
Search strategy
The search strategy for MEDLINE through PubMed is shown below; search strategies for the other databases were developed based on this strategy. #1 “refractive errors”[mh] OR presbyopia[mh] OR hyperopia[mh] OR myopia[mh] OR astigmatism[mh] OR asthenopia[mh] OR “refractive error”[tw] OR “refractive errors” [tw] OR ametropia[tw] OR presbyopia[tw] OR farsight*[tw] OR longsight*[tw] OR myopia*[tw] OR nearsight*[tw] OR “visual discomfort”[tw] OR eyestrain[tw] OR “eye fatigue” OR “visual fatigue”[tw] OR “blurred vision”[tw] OR “doubled vision”[tw] OR “computer vision syndrome”[tw] OR CVS[tw] OR “visual symptom”[tw] OR “eye ache” [tw] OR diplopia[tw] OR “eye problems”[tw] OR “vision problems”[tw] OR “visual symptoms”[tw] OR “visual complaints”[tw] OR “ocular complaints”[tw] OR “asthenopic symptoms”[tw] OR “dry eye”[tw] OR “dry eyes”[tw] OR “accomodation,ocular”[mh] OR “visual acuity”[mh]
#2 computers[mh] OR “computer terminals”[mh]OR “computer screen”[tw] OR “computer screens”[tw] OR “display screen”[tw] OR “display screens”[tw] OR “display screen”[tw] OR “display screens”[tw] OR “computer monitor”[tw] OR “computer monitors”[tw] OR “PC monitor”[tw] OR “PC monitors”[tw] OR “computer display”[tw] OR “computer use”[tw] OR “visual display unit”[tw] OR “visual display units”[tw] OR “video display unit”[tw] OR “video display units”[tw] OR vdu[tw] OR vdus[tw] OR “screen‐based equipment” [tw] OR sbe[tw] OR sbes[tw] OR “computer work”[tw] OR “office work”[tw] OR “near work”[tw]
#3 (“Randomized Controlled Trial”[pt] OR “Controlled Clinical Trial”[pt] OR “Randomized Controlled Trials as Topic”[mh] OR “Random Allocation”[mh] OR “Double‐Blind Method”[mh] OR “Single‐Blind Method”[mh] OR “Clinical Trial”[pt] OR “Clinical Trials as Topic”[mh] OR “clinical trial”[tw] OR ((singl*[tw] OR doubl*[tw] OR trebl*[tw] OR tripl*[tw]) AND (mask*[tw] OR blind*[tw])) OR “latin square”[tw] OR Placebos[mh] OR placebo*[tw] OR random*[tw] OR “Research Design”[mh:noexp] OR “Comparative Study”[pt] OR “Evaluation Studies as Topic”[mh] OR “Follow‐up Studies”[mh] OR “Prospective Studies”[mh] OR “Cross‐over Studies”[mh] OR control[tw] OR controls*[tw] OR controla*[tw] OR controle*[tw] OR controli*[tw] OR controll*[tw] OR control’*[tw] OR prospectiv*[tw] OR volunteer*[tw]) NOT (Animals[mh] NOT Humans[mh])
#4 #1 AND #2 AND #3
Data and analyses
Comparison 1. All progressive computer glasses vs Monofocal computer glasses.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Asthenopia (change from baseline to 12 months) (corr 0.7) | 1 | 186 | Mean Difference (IV, Fixed, 95% CI) | 0.23 [‐4.97, 5.43] |
| 2 Asthenopia (change from baseline to 12 months) (corr 0) | 1 | 186 | Mean Difference (IV, Fixed, 95% CI) | 0.23 [‐9.23, 9.69] |
| 3 Asthenopia (change from baseline to 12 months) (corr 0.9) | 1 | 186 | Mean Difference (IV, Fixed, 95% CI) | 0.10 [‐6.09, 6.30] |
| 4 Asthenopia (12 months) | 1 | 147 | Mean Difference (IV, Fixed, 95% CI) | 11.57 [3.59, 19.55] |
| 5 Headache (change from baseline to12 months) (corr 0.7) | 1 | 128 | Mean Difference (IV, Fixed, 95% CI) | 11.02 [5.17, 16.87] |
| 6 Headache (change from baseline to12 months) (corr 0) | 1 | 186 | Mean Difference (IV, Fixed, 95% CI) | 10.67 [3.15, 18.20] |
| 7 Headache (change from baseline to12 months) (corr 0.9) | 1 | 186 | Mean Difference (IV, Fixed, 95% CI) | 10.51 [7.64, 13.38] |
| 8 Headache (12 months) | 1 | 128 | Mean Difference (IV, Fixed, 95% CI) | 4.16 [‐2.38, 10.71] |
| 9 Compliance (duration of use) (12 months) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected |
1.9. Analysis.
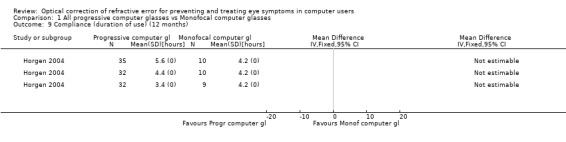
Comparison 1 All progressive computer glasses vs Monofocal computer glasses, Outcome 9 Compliance (duration of use) (12 months).
Comparison 2. Progressive computer glasses (range N/C+) vs. Monofocal computer glasses.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Asthenopia (change from baseline to 12 months) (corr 0.7) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2 Asthenopia (change from baseline to 12 months) (corr 0) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3 Asthenopia (change from baseline to 12 months) (corr 0.9) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4 Asthenopia (12 months) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5 Headache (change from baseline to12 months) (corr 0.7) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6 Headache (change from baseline to12 months) (corr 0) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7 Headache (change from baseline to12 months) (corr 0.9) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 8 Headache (12 months) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 9 Compliance (duration of use) (12 months) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected |
2.9. Analysis.
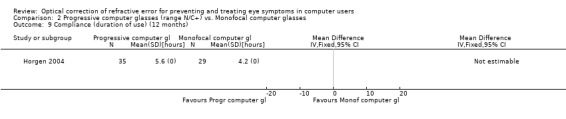
Comparison 2 Progressive computer glasses (range N/C+) vs. Monofocal computer glasses, Outcome 9 Compliance (duration of use) (12 months).
Comparison 3. Progressive computer glasses (range N/C+/IM) vs. General purpose progressive glasses.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Asthenopia | 2 | Std. Mean Difference (Fixed, 95% CI) | Subtotals only | |
| 1.1 Short term follow‐up | 2 | Std. Mean Difference (Fixed, 95% CI) | ‐0.49 [‐0.75, ‐0.23] | |
| 1.2 Medium term follow‐up | 1 | Std. Mean Difference (Fixed, 95% CI) | ‐0.64 [‐1.40, 0.12] | |
| 2 Headache (1 week) | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 3 Dizziness (1 week) | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected |
Comparison 4. Progressive computer glasses (range N/C+/IM) vs. Monofocal computer glasses.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Asthenopia (change from baseline to 12 months) (corr 0.7) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2 Asthenopia (change from baseline to 12 months) (corr 0) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3 Asthenopia (change from baseline to 12 months) (corr 0.9) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4 Asthenopia (12 months) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5 Headache (change from baseline to12 months) (corr 0.7) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6 Headache (change from baseline to12 months) (corr 0) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7 Headache (change from baseline to12 months) (corr 0.9) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 8 Headache (12 months) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 9 Compliance (duration of use) (12 months) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected |
4.9. Analysis.
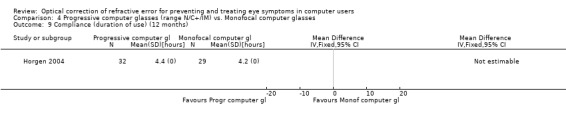
Comparison 4 Progressive computer glasses (range N/C+/IM) vs. Monofocal computer glasses, Outcome 9 Compliance (duration of use) (12 months).
Comparison 5. Progressive computer glasses (range N/C+/F) vs. Monofocal computer glasses.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Asthenopia (change from baseline to 12 months) (corr 0.7) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2 Asthenopia (change from baseline to 12 months) (corr 0) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3 Asthenopia (change from baseline to 12 months) (corr 0.9) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4 Asthenopia (12 months) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5 Headache (change from baseline to12 months) (corr 0.7) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6 Headache (change from baseline to12 months) (corr 0) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7 Headache (change from baseline to12 months) (corr 0.9) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 8 Headache (12 months) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 9 Compliance (duration of use) (12 months) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected |
Comparison 6. Progressive computer glasses (range N/C+/F) vs. Bifocal computer glasses.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Asthenopia (improvement of symptoms after 4 weeks) | 1 | Odds Ratio (Fixed, 95% CI) | Totals not selected | |
| 2 Headache (improvement of symptoms after 4 weeks) | 1 | Odds Ratio (Fixed, 95% CI) | Totals not selected | |
| 3 Nausea (improvement of symptoms after 4 weeks) | 1 | Odds Ratio (Fixed, 95% CI) | Totals not selected | |
| 4 Dizziness (improvement of symptoms after 4 weeks) | 1 | Odds Ratio (Fixed, 95% CI) | Totals not selected |
Comparison 7. Progressive computer glasses (range N/C+/F) vs. Trifocal computer glasses.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Eyestrain severity | 1 | Mean Difference (Fixed, 95% CI) | Totals not selected | |
| 2 Eyestrain frequency | 1 | Mean Difference (Random, 95% CI) | Totals not selected |
Comparison 8. Computer glasses vs. Ergonomic self‐assessment tool and habitual refractive correction.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Asthenopia severity score at FU Quasi Random | 1 | Mean Difference (Random, 95% CI) | Totals not selected | |
| 2 Eyestrain | 1 | Odds Ratio (Fixed, 95% CI) | Totals not selected | |
| 3 Headache | 1 | Odds Ratio (Fixed, 95% CI) | Totals not selected | |
| 4 Upset stomach | 1 | Odds Ratio (Fixed, 95% CI) | Totals not selected |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Bachman 1992.
| Methods | Cross‐over randomised controlled trial | |
| Participants | 29 respondents to an advertisement in the university’s weekly newspaper that asked for presbyopic volunteers who worked at a visual display terminal (VDT) for 20 or more hours per week. Mean age 52.3 years, range 42 to 64 Male/Female: 7/22 Mean time spent at a VDT per day: 5.52 hours ± 1.25 (SD?) (type of computer not described) Refractive error: range of spherical power: +4.75 to −4.75 dpt; range of cylinders: 0 to −2.75 dpt Country: USA |
|
| Interventions | Eyeglasses: progressive addition glasses were compared with flat top bifocal glasses in n = 26 participants and with single vision glasses in n = 3 participants, each type of eyeglasses was worn for a period of 4 weeks, followed by a direct comparison for 1 week. | |
| Outcomes | At baseline and during each intervention period patients reported the effect of the intervention on symptoms (headache, eyestrain, back pain, neck pain, nausea and dizziness). Other aspects that were judged by the patients were: clarity of VDU screen work and desk work (paper and other objects), adjustments in position required to see clearly, utility of distance vision, usefulness away from the desk. At the end of the study (week 9) overall preference (intervention or control lens) was assessed. Participants took several measurements at their work station and viewing angle to computer screen was calculated. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, yet method of randomisation not described. |
| Allocation concealment (selection bias) | Unclear risk | No information about concealment of allocation. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No information on blinding, however blinding is not possible due to the type of intervention. |
| Blinding of outcome assessment (detection bias) Primary outcomes | High risk | Participants, who are unblinded, are the outcome assessors. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Data of all participants for all outcomes were reported. |
| Selective reporting (reporting bias) | Unclear risk | No study protocol. However, all outcomes stated in methods were reported at results section of the publication. |
| Other bias | Low risk | No indication of other bias. |
Butzon 1997.
| Methods | Quasi‐randomised cross‐over study | |
| Participants | 24 presbyopic volunteers from research and development personnel of a telecommunications equipment company who were age 47 or older wearing a full‐time multifocal lens design, needing a near add power of at least S+1.50 dioptres, that worked at a computer for 4 hours per day or more. Mean age: 53 years, range 47 to 66 Male/Female: 19/5 Mean time spent at a VDT per day: at least 4 hours (type of computer not described) Refractive error: not described, near add power of at least S+1.50 dioptres Country: USA |
|
| Interventions | Eyeglasses: progressive computer glasses (Technica by American Optical) vs. trifocal computer glasses (Datalite CRT trifocal by Vision‐Ease); each type of eyeglasses was worn for a period of 3 weeks, followed by a direct comparison during 3 weeks | |
| Outcomes | Frequency and severity of symptoms at baseline and after each intervention period (3 and 6 weeks). Wearing time of the eyeglasses expressed as % of the working day. | |
| Notes | Authors did not respond to our request for information about the allocation method. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Intervention and comparison in "counterbalanced order". |
| Allocation concealment (selection bias) | Unclear risk | Intervention and comparison in a "counterbalanced order"; no attempt to concealment reported. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Blinding not possible because of differences in visual aspect of the eyeglasses: progressive vs. trifocal. |
| Blinding of outcome assessment (detection bias) Primary outcomes | High risk | No blinding of outcome assessment, as participants are outcome assessors. |
| Blinding of outcome assessment (detection bias) Secondary outcomes | High risk | No blinding of outcome assessment, as participants are outcome assessors. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 24 participants who all completed the study and answered all questionnaires. |
| Selective reporting (reporting bias) | Unclear risk | No study protocol. All outcomes mentioned in the methods section are reported. |
| Other bias | High risk | No wash‐out period between interventions. |
Butzon 2002.
| Methods | Quasi‐randomised cross‐over study | |
| Participants | 26 symptomatic computer users aged 37 or older, who wore eyeglasses at the computer and had an eye examination in past year (20/20 vision at distance and near) and who worked at computer for at least four hours per day. Age range (37 to 57) Male/Female: 7/23 Mean time spent at a VDT per day: at least 4 hours (type of computer not described) Refractive error: not described Country: USA |
|
| Interventions | Eyeglasses vs. non‐optical intervention: computer glasses (progressive (n = 15 Technica by American Optical; n = 8 Access by SOLA), bifocal (n = 1) or trifocal (n = 1, Datlite CRT) glasses) vs. ergonomic self assessment tool (ESAT) with habitual refraction; 3 weeks duration of each intervention period. | |
| Outcomes | Frequency and severity of 14 symptoms at baseline and after each intervention period (3 and 6 weeks) | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Intervention and comparison in a "planned alternating order". |
| Allocation concealment (selection bias) | Unclear risk | Intervention and comparison in a "planned alternating order"; no attempt at concealment reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No attempt at blinding reported. |
| Blinding of outcome assessment (detection bias) Primary outcomes | Unclear risk | No attempt at blinding reported. |
| Blinding of outcome assessment (detection bias) Secondary outcomes | Unclear risk | No attempt at blinding reported. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 26 of 30 participants completed the study and answered all questionnaires. Three persons missing from computer glasses‒ESAT sequence, and one from the ESAT‒computer glasses sequence; no further information on participants not completing the study. |
| Selective reporting (reporting bias) | Unclear risk | No study protocol. All outcomes mentioned in the Methods section are reported. |
| Other bias | High risk | No wash‐out period between interventions, and baseline imbalance: the computer glasses‒ESAT sequence had a symptom score of 34.5 and the ESAT‒computer glasses had a score of 43.1. |
Cagnie 2017.
| Methods | Randomised controlled trial, 2 groups, parallel | |
| Participants | 35 computer workers who are between 45 and 65 years of age, recruited from the employee population of a financial holding in Ghent (Belgium), performing computer work for at least 4 h a day and 20 h a week, experiencing work‐related neck/shoulder pain or discomfort of more than 30 days during the last year and having a difference in spectacle correction for presbyopia and myopia of minimum 1.5 dioptres. Mean age ± SD (intervention vs. control group): 51.09 ± 4.19 years vs. 53.67 ± 3.97 years Male/Female: 21/14 Country: Belgium |
|
| Interventions | Eyeglasses: progressive computer glasses (n=17 randomised, n=15 analyzed) vs. general purpose progressive glasses (n=18 randomised, n=13 analyzed). | |
| Outcomes | Visual fatigue (visual fatigue questionnaire‐ VFQ), self‐perceived pain (numeric rating scale ‐ NRS) and disability (neck disability index ‐ NDI) at baseline (with old glasses), and 1 week, 3 months and 6 months after wearing new glasses. In addition, Forward Head Angle and Pressure Pain Thresholds were assessed during and after a VDU task before and 6 months after wearing the new lenses. A short questionnaire concerning the satisfaction about the study lenses was completed at the end of the study. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Block randomization, yet method not described.Authors responded: "We had an envelope for males and an envelope for females with each 6 sheets. In the envelope for males, there were 6 sheets, 3 with the letter A (was similar to VDU glasses) and 3 with the letter B (was similar to normal glasses). All 6 consecutive male participants took one sheet and pending of the letter they took, they were assigned to the VDU or normal glasses group. The same procedure was performed for the females." |
| Allocation concealment (selection bias) | Unclear risk | No information on concealment of allocation. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | The authors communicated that: "Patients were not informed by the type of glasses. All glasses looked similar and had similar frames (typical silhouette glasses have no ‘frame’). Although the participants were not informed, they easily knew afterwards to which group they were allocated, as VDU lenses can only be used during VDU work, whereas progressive lenses can be used all day long (this was also mentioned in the discussion section). Subjects didn't know which type of glasses were intended to have a more beneficial effect." |
| Blinding of outcome assessment (detection bias) Primary outcomes | Low risk | See blinding of participants performance bias. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 5/18 dropouts in control group; 2/17 dropouts in intervention group. In both groups are reasons related to type of intervention. |
| Selective reporting (reporting bias) | Unclear risk | No trial register record or study protocol available. Outcomes listed in methods were reported results for. |
| Other bias | Low risk | No indication of other bias. |
Daum 2014.
| Methods | Randomised controlled trial, 3 groups, parallel | |
| Participants | 51 volunteers who are 40 years of age or older, recruited from the employee population of a call centre, with corrected visual acuity at near (40 cm) of at least 20/40 or better in each eye, at least 0.50D vector dioptric difference in refractive error in their habitual correction in both eyes, stereopsis of at least 40 seconds at 40 cm (corrected, Randot), and use a computer for at least 6 hours per day. Mean age 51.1 years; range: 40 to 65 Male/Female: 2/49 Refractive error: means S−1.32D, C−0.74D, add +1.72D Country: USA |
|
| Interventions | Eyeglasses: habitual refractive error (bifocals) vs. fully corrected refractive error (bifocals) vs. Essilor computer glasses. | |
| Outcomes | Post intervention (10 weeks) visual comfort (Convergence Insufficiency Symptom Survey and National Eye Institute Refractive Quality of Life survey) and productivity (productivity in a given day is defined as: Number of calls * Efficiency in answering calls * Accuracy in answering calls * Proportion of time on job) were assessed. | |
| Notes | Data‐extraction based on study protocol and a conference abstract; no full text available. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information on method of randomisation. |
| Allocation concealment (selection bias) | Unclear risk | No information on method of randomisation. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | No information on who is masked in what way. |
| Blinding of outcome assessment (detection bias) Primary outcomes | Unclear risk | No information on who is masked in what way. |
| Blinding of outcome assessment (detection bias) Secondary outcomes | Unclear risk | No information on who is masked in what way. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No information. |
| Selective reporting (reporting bias) | High risk | There were outcomes reported In the conference abstract that were not in the study protocol. |
| Other bias | Unclear risk | No information on individual study groups. |
Horgen 2004.
| Methods | Randomised controlled trial, 4 groups, parallel | |
| Participants | About 360 visual display unit (VDU) users were drawn from the total workforce of Alcatel Telecom and Nexans Companies in Oslo, of which 158 participated. No information about patient characteristics was provided. Country: Norway |
|
| Interventions | Eyeglasses: three different types of specially designed VDU progressive glasses (Interview (Essilor), Gradal HR (Zeiss), Technica (American Optical)) were compared with single vision glasses. | |
| Outcomes | At baseline, after six months and one year: questionnaire concerning visual conditions, working conditions and discomfort in different body areas, based on the Nordic Questionnaire with some additional optometric questions. It also dealt with psychological factors at work and at home. Other outcomes: total wearing time per day and possible confounding factors were documented as well. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of randomisation is not described: "The subjects were divided into four test groups by a stratified randomization procedure". |
| Allocation concealment (selection bias) | Unclear risk | No information on allocation concealment. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "The subjects were not informed about which type of lens they received, only that the lenses were specially designed for computer work". |
| Blinding of outcome assessment (detection bias) Primary outcomes | Low risk | "The subjects were not informed about which type of lens they received, only that the lenses were specially designed for computer work". Even though symptoms were self‐reported, participants did not know to which group they belonged. |
| Blinding of outcome assessment (detection bias) Secondary outcomes | Unclear risk | Unclear who assessed secondary outcome. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | "There were nine dropouts in the study". These were equally divided over the four intervention groups. No intention to treat analysis. |
| Selective reporting (reporting bias) | Unclear risk | No study protocol. All outcomes mentioned in the methods section are reported. All results with 95% confidence intervals are presented in figures. |
| Other bias | High risk | No information on patient characteristics and possible baseline imbalances. Looking at the presented figures, baseline differences are suspected. |
Jaschinski 2015b.
| Methods | Cross‐over randomised controlled trial | |
| Participants | 23 employees of a tax office, who habitually used general purpose progressive glasses for their office work and indicated higher ocular and musculoskeletal strain in a questionnaire as part of a previous field study. Mean age 55 (standard deviation 4) years; range: 46 to 61 Male/Female: 10/13 Mean daily duration of work (primarily at the computer) 7.9 ± 1.6 hours (range 4 to 10 hours) Refractive error: spherical component was −0.90 ± 2.66 D averaged across the two eyes (range −6.25 D = +4.00 D); cylindrical refraction −0.90 ± 0.69 D (range 0 to −2.75 D); additional power for near 2.06 ± 0.41 D (range 1.00 D to 2.50 D) Country: Germany |
|
| Interventions | Eyeglasses: progressive computer glasses vs. general purpose progressive glasses. Participants switched glasses every week over a one‐month period , followed by a period of eight more weeks of free use of the spectacles. | |
| Outcomes | Participant‐reported symptoms of asthenopia at the end of the working day, weekly administration of questionnaire during first four weeks of intervention period. Daily administration of subset of presumably most relevant questions during third and fourth week, the actual test period of the study. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Author correspondence: "the random assignment was produced by the software EXCEL". |
| Allocation concealment (selection bias) | Low risk | Author correspondence: "The random order was not generated by the experimenters of our research Institute, but by the company ZEISS, that participated in the study. The experimenters were not informed of the assignment of the type of lens to the participants". |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "Neither the experimenters nor the participants were aware of this assignment to ensure a double‐masked condition as much as possible. We intended for the participants to evaluate the two types of lenses purely based on their perception and experience without being influenced by information about the features and purposes of these lenses. The experimenters were neutral, as they were not informed about the type of lenses and did not communicate with the participants about the lenses; however, it was almost inevitable that participants noticed the blurred distance vision with the computer vision PALs, which can occur when looking outside the window. These conditions cannot be avoided, if realistic office conditions are to be investigated." |
| Blinding of outcome assessment (detection bias) Primary outcomes | Low risk | See Blinding of participants. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Cross‐over study of 23 participants, no information about lost to follow‐up or incomplete outcome data. |
| Selective reporting (reporting bias) | Unclear risk | No study protocol or trial registration; results were reported for more outcomes than were listed in Methods section of the publication. |
| Other bias | Low risk | No indication of other bias. |
Zeried 2007.
| Methods | Cross‐over randomised controlled trial | |
| Participants | 36 computer workers of ≥ 19 years of age, who had a visual acuity of ≥ 20/40 and used a computer for at least 1 hr/day. | |
| Interventions | Eyeglasses: habitual correction and best correction (correcting optical blur) were each worn for a period of 1 month in a randomised order. | |
| Outcomes | Visual comfort (phone survey before and after 1 hour of work on participant's own computer, 5 times during each 1‐month period of the study and 3 times 3 months after the experimental portion of the study is completed); uncorrected refractive error; undesirable reactions (short survey at each visit); time and accuracy in completing editing and data entry tasks (4‐hour test once every 1‐month study period). | |
| Notes | There is no full‐text publication of this study (confirmed by authors). Data extraction was based on study registration information and a conference abstract. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information on method of randomisation. |
| Allocation concealment (selection bias) | Unclear risk | No information. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | "Double blind". Protocol states "subjects and doctors are masked". Unclear how this was done. |
| Blinding of outcome assessment (detection bias) Primary outcomes | Unclear risk | "Double blind". Protocol states "subjects and doctors are masked". Unclear how this was done. |
| Blinding of outcome assessment (detection bias) Secondary outcomes | Unclear risk | "Double blind". Protocol states "subjects and doctors are masked". Unclear how this was done. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No information, probably no drop‐outs. |
| Selective reporting (reporting bias) | Unclear risk | Unclear, as study protocol was registered post hoc. |
| Other bias | Low risk | No indication of other bias. |
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Aarås 1998 | Wrong study design (no randomisation). |
| Balci 2001 | Wrong study design (no randomisation). |
| Daum 2003 | Probably participants did not use a computer for at least 4 hours a day; authors did not respond to request for information. |
| Daum 2007a | Probably participants did not use a computer for at least 4 hours a day; authors did not respond to request for information. |
| Daum 2007b | Study was terminated because principal investigator left the university; no publications. |
| Feigin 2003 | Intervention not relevant (spectral filters instead of refractive error correction), probably non‐random assignment. |
| Guo 2010 | Wrong study design (no randomisation). |
| Heatly 2005 | Wrong patient population. |
| Jaschinski 2015 | Not an intervention study. |
| Kojima 2011 | Wrong study design (no randomisation). |
| Lazarus 1996 | Intervention is not only refractive error correction but a correction with prisms as well. |
| Lie 1994 | Intervention is not refractive error correction. |
| Lin 2017 | Intervention is filter in glasses, not refractive error correction. |
| Lodin 2012 | Wrong patient population. |
| Palm 1987 | Wrong study design (no randomisation). |
| Potvin 1998 | Wrong study design (no randomisation). |
| Rosenfield 2012 | No randomisation. |
| Scullica 1995 | Intervention is not a correction of refractive error. |
| Vidal‐Lopez 2015 | Wrong patient population. |
| Wallin 1994 | Wrong study design (no randomisation). |
| Weidling 2015 | Wrong study design (no randomisation). |
| Wiggins 1991 | Wrong patient population: volunteers involved, not using a computer for at least 4 hours a day. |
| Wiggins 1992 | Wrong patient population: volunteers involved, not using a computer for at least 4 hours a day. |
Characteristics of ongoing studies [ordered by study ID]
NCT02775396.
| Trial name or title | Effects of Wearing Progressive Addition Lens on Working Distance and Refractive Status in Adult Computer Users |
| Methods | Cross‐over randomised controlled trial |
| Participants | Hong Kong Chinese, pre‐presbyopic, adult (18 to 40 years of age) computer users (computer usage > 2 hours/day) with spherical‐equivalent refractive errors between plano and −9.00D and cylindrical power ≤ 2.50D. Persons with visual acuity worse than 0 logMAR, anisometropia more than 2.00D, abnormal accommodative function, wearing rigid contact lens, and a history of ocular surgery and pathology were excluded. |
| Interventions | Eyeglasses: single‐vision glasses vs. progressive addition glasses designed for handheld digital display devices. |
| Outcomes | Working distance and refractive status. |
| Starting date | September 2014 (final data collection date for primary outcome measure: April 2015). |
| Contact information | Chea‐su Kee, PhD, The Hong Kong Polytechnic University |
| Notes | Trial registration number: NCT02775396 |
Differences between protocol and review
We used a different search strategy than the one the authors of the protocol for this review initially developed (Li 2012). We applied different search terms for identifying randomised controlled trials and we did not search any Chinese databases or websites. The decision not to use the Chinese databases or websites was based on the change of the author team and, as a consequence, lack of access and language abilities to do so. We did not do any handsearching as the journals that were mentioned to be handsearched in the protocol were already included in PubMed. Besides, we searched in Cochrane CENTRAL which contains the specialised registers of Cochrane Eyes and Vision and Cochrane Work. Although the protocol stated ithat we would search the World Health Organization (WHO) International Clinical Trials Registry Platform and clinical trials registries to identify ongoing studies, we only searched the WHO international Clinical Trials Registry Platform, as it incorporates datasets from all major trial registries. Similarly we did not run searches in the UK National Research Register (NRR) Archive or China Occupational Disease Network. Information about the initial search strategy as reported in the protocol of this review can be found in Appendix 4.
We extended our secondary outcome 'adverse events' with the addition of symptoms of dizziness and nausea.
Although we stated in the protocol that we would not assess the domain of blinding of the participants and personnel, we eventually did, as blinding is possible when the interventions assessed are a type of eyeglasses.
Due to the way we presented our results, some sources of heterogeneity that we mentioned in the protocol that we would explore with subgroup analyses or meta‐regression are no longer relevant: prevention versus treatment will be unlikely to be found because all studies will be a mixture of patients with and without symptoms; it will be unlikely that a comparison between glasses, lenses and surgery can be made; the duration of the intervention is similar to the follow‐up time and we take that already into account
Contributions of authors
Conceiving the review idea: Hong‐Hao Li (author of protocol) Designing the review: Hong‐Hao Li, Pauline Heus Co‐ordinating the review: Hong‐Hao Li from Apr 16 2012 to Oct 23, 2014, and Christina Tikka and Pauline Heus from Oct 23 2014 onwards. Data collection for the review ‐ Undertaking additional searches: Pauline Heus ‐ Organizing retrieval of papers: Christina Tikka, Pauline Heus ‐ Screening retrieved papers against inclusion criteria: Christina Tikka, Pauline Heus, Jos Verbeek ‐ Appraising quality of papers: Christina Tikka, Pauline Heus, Jos Verbeek ‐ Extracting data from papers: Christina Tikka, Pauline Heus, Jos Verbeek ‐ Writing to authors for additional information: Christina Tikka, Pauline Heus, Jos Verbeek
Data management for the review ‐ Entering data into RevMan 5: Pauline Heus, Jos Verbeek ‐ Analysis and interpretation of data: Jos Verbeek, Pauline Heus,Christina Tikka ‐ Writing the review: Pauline Heus, Jos Verbeek, Christina Tikka, (from the first author team Hong‐Hao Li and Ling Li contributed to background and methods sections)
Sources of support
Internal sources
-
Chinese Cochrane Center, China.
Methodology
Cochrane Netherlands, Netherlands.
Cochrane Work, Finland.
External sources
No sources of support supplied
Declarations of interest
Pauline Heus: None known.
Christina Tikka: None known.
Jos Verbeek: None known.
New
References
References to studies included in this review
Bachman 1992 {published data only}
- Bachman WG. Computer‐specific spectacle lens design preference of presbyopic operators. Journal of Occupational Medicine 1992;34(10):1023‐7. [PubMed] [Google Scholar]
Butzon 1997 {published data only}
- Butzon SP, Eagels SR. Prescribing for the moderate‐to‐advanced ametropic presbyopic VDU user. A comparison of theTechnica Progressive and Datalite CRT trifocal. Journal of the American Optometric Association 1997;68(8):495‐502. [PubMed] [Google Scholar]
Butzon 2002 {published data only}
- Butzon SP, Sheedy JE, Nilsen E. The efficacy of computer glasses in reduction of computer worker symptoms. Optometry 2002;73(4):221‐30. [PubMed] [Google Scholar]
Cagnie 2017 {published data only}
- Cagnie B, Meulemeester K, Saeys L, Danneels L, Vandenbulcke L, Castelein B. The impact of different lenses on visual and musculoskeletal complaints in VDUworkers with work‐related neck complaints:a randomized controlled trial. Environmental Health and Preventive Medicine 2017;22(1):2‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Daum 2014 {published data only}
- Daum KM, Amick III BC, Barnwell MM, DeRango K, Hately WW, Hodur N, et al. Real‐world workplace return on investment of a computer‐specific vision intervention benefit for presbyopes. https://vii‐production.s3.amazonaws.com/uploads/research_article/pdf/511e6b8b155851cb5d000004/1009p_ICO_2009_Daum.pdf (accessed 04 August 2015).
- Daum KM, Barnwell MM, DeRango K, Tarantino G, Torrey J, Hunt L, et al. Real‐world workplace return on investment of a computer‐specific vision intervention benefit for presbyopes. Investigative Ophthalmology & Visual Science 2014;55(13):162. [Google Scholar]
Horgen 2004 {published data only}
- Horgen G, Aaras A, Thoresen M. Will visual discomfort among visual display unit (VDU) users change in development when moving from single vision lenses to specially designed VDU progressive lenses?. Optometry and Vision Science 2004;81(5):341‐9. [DOI] [PubMed] [Google Scholar]
Jaschinski 2015b {published data only}
- Jaschinski W, König M, Mekontso TM, Ohlendorf A, Welscher M. Comparison of progressive addition lenses for general purpose and for computer vision: an office field study. Clinical and Experimental Optometry 2015;98(3):234‐43. [DOI] [PubMed] [Google Scholar]
Zeried 2007 {published data only}
- Zeried FM, Daum KM. Effects of optical blur on the performance and comfort of computer users. Investigative Ophthalmology & Visual Science 2007;48(13):1004. [Google Scholar]
References to studies excluded from this review
Aarås 1998 {published data only}
- Aarås A, Horgen G. Relationship between visual discomfort and musculoskeletal disorders (msd) for vdu workers. American Academy of Optometry Annual Meeting; 2004. Tampa (Fl): American Academy of Optometry, 2004:Poster 22.
- Aarås A, Horgen G, Bjorset HH, Ro O, Thoresen M. Musculoskeletal, visual and psychosocial stress in VDU operators before and after multidisciplinary ergonomic interventions. Applied Ergonomics 1998;29(5):335‐54. [DOI] [PubMed] [Google Scholar]
- Aarås A, Horgen G, Bjorset HH, Ro O, Walsoe H. Musculoskeletal, visual and psychosocial stress in VDU operators before and after multidisciplinary ergonomic interventions. A 6 years prospective study‐‐Part II. Applied Ergonomics 2001;32(6):559‐71. [DOI] [PubMed] [Google Scholar]
- Horgen G, Aarås A. Optometric examination and correction of VDU workers. Advances in Occupational Ergonomics and Safety 1998;2:517‐20. [Google Scholar]
Balci 2001 {published data only}
- Balci R, Aghazadeh F. Influence of VDT monitor positions on discomfort and performance of users with or without bifocal lenses. Journal of Human Ergology 2001;27(1‒2):62‐9. [PubMed] [Google Scholar]
Daum 2003 {published data only}
- Daum KM, Clore KA, Simms SS, Vesely JW, Wilczek DD, Spittle BM, Good GW. Effects of improvements in visual status of computer users on productivity. Investigative Ophthalmology & Visual Science May 2003;44:770. [Google Scholar]
Daum 2007a {published data only}
- Daum KM, Zeried FM. Effects of different add powers on the comfort and productivity of computer users with fixed or free head movement. Investigative Ophthalmology & Visual Science 2007;48(13):1005. [Google Scholar]
Daum 2007b {published data only}
- NCT00585026. Randomized clinical trial of bifocal lenses versus computer‐specific progressive addition lenses. clinicaltrials.gov/show/NCT00585026 (first received 2 January 2008).
Feigin 2003 {published data only}
- Feigin AA. Role of spectral filters for refraction dynamics in computer users. Vestnik Oftalmologii 2003;119(2):39‐40. [PubMed] [Google Scholar]
Guo 2010 {published data only}
- Guo Q, Han Q. Analysis of the effects of progressive addition lenses on VDT operators visual fatigue. International Journal of Ophthalmology 2010;10(2):351‐2. [Google Scholar]
Heatly 2005 {published data only}
- Heatley CJ, Spalton DJ, Hancox J, Kumar A, Marshall J. Fellow eye comparison between the 1CU accommodative intraocular lens and the Acrysof MA30 monofocal intraocular lens. American Journal of Ophthalmology 2005;140(2):207‐13. [DOI] [PubMed] [Google Scholar]
Jaschinski 2015 {published data only}
- Jaschinski W, König M, Mekontso TM, Ohlendorf A, Welscher M. Computer vision syndrome in presbyopia and beginning presbyopia:effects of spectacle lens type. Clinical and Experimental Optometry 2015;98(3):228‐33. [DOI] [PubMed] [Google Scholar]
Kojima 2011 {published data only}
- Kojima T, Ibrahim OM, Wakamatsu T, Tsuyama A, Ogawa J, Matsumoto Y, et al. The impact of contact lens wear and visual display terminal work on ocular surface and tear functions in office workers. American Journal of Ophthalmology 2011;152(6):933‐40. [DOI] [PubMed] [Google Scholar]
Lazarus 1996 {published data only}
- Lazarus SM. The use of yoked base‐up and base‐in prism for reducing eye strain at the computer. Journal of the American Optometric Association 1996;67(4):204‐8. [PubMed] [Google Scholar]
Lie 1994 {published data only}
- Lie I, Watten RG. VDT work, oculomotor strain, and subjective complaints: An experimental and clinical study. Ergonomics 1994;37(8):1419‐33. [DOI] [PubMed] [Google Scholar]
Lin 2017 {published data only}
- Lin JB, Gerratt BW, Bassi CJ, Apte RS. Short‐wavelength light‐blocking eyeglasses attenuate symptoms of eye fatigue. Investigative Ophthalmology & Visiual Science 2017;58:442‐447. [DOI] [PubMed] [Google Scholar]
Lodin 2012 {published data only}
- Lodin C, Forsman M, Richter H. Eye‐ and neck/shoulder‐discomfort during visually demanding experimental near work. Work 2012;41(Suppl 1):3388‐92. [doi: 10.3233/WOR‐2012‐0613‐3388; PUBMED: PMID: 22317236] [DOI] [PubMed] [Google Scholar]
Palm 1987 {published data only}
- Palm B. Work Distance and Optical Correction. International Scientific Conference on Work with Display Units; 1986 May 12‐15; Stockholm, Sweden. Amsterdam: Elsevier Science Publishers B.V., 1986:522‐5.
Potvin 1998 {published data only}
- Potvin R. Putting glasses on the computer ‐ treating computer vision syndrome with the pc‐magni‐viewer TM. American Academy of Optometry Annual Meeting; 1998; San Fransisco. San Francisco (CA): American Academy of Optometry, 1998:Poster 93.
Rosenfield 2012 {published data only}
- Rosenfield M, Hue JE, Huang RR, Bababekova Y. The effects of induced oblique astigmatism on symptoms and reading performance while viewing a computer screen. Ophthalmic & Physiological Optics 2012;32(2):142‐8. [DOI] [PubMed] [Google Scholar]
Scullica 1995 {published data only}
- Scullica L, Rechichi C, Moja CA. Protective filters in the prevention of asthenopia at a video display terminal. Perceptual and Motor Skills 1995;80(1):299‐303. [DOI] [PubMed] [Google Scholar]
Vidal‐Lopez 2015 {published data only}
- Vidal‐Lopez J, Javaloyes‐Moreno B, Benlloch‐Fornes J. The effect of low power glasses at close distances on visual performance. Perceptual and Motor Skills 2015;121(2):528‐36. [DOI] [PubMed] [Google Scholar]
Wallin 1994 {published data only}
- Wallin JA, Zhu Z, Jacobsen JL, Jacobsen SD. A preliminary study of the effects of computer glasses on reported VDT user symptoms: a field study. Journal of Safety Research 1994;25(2):67‐76. [Google Scholar]
Weidling 2015 {published data only}
- Weidling P, Jaschinski W. The vertical monitor position for presbyopic computer users with progressive lenses: how to reach clear vision and comfortable head posture. Ergonomics 2015;58(11):1813‐29. [DOI] [PubMed] [Google Scholar]
Wiggins 1991 {published data only}
- Wiggins NP, Daum KM. Visual discomfort and astigmatic refractive errors in VDT use. Journal of the American Optometric Association 1991;62(9):680‐4. [PubMed] [Google Scholar]
Wiggins 1992 {published data only}
- Wiggins NP, Daum KM, Snyder CA. Effects of residual astigmatism in contact lens wear on visual discomfort in VDT use. Journal of the American Optometric Association 1992;63(3):177‐81. [PubMed] [Google Scholar]
References to ongoing studies
NCT02775396 {published data only}
- NCT02775396. Effects of Wearing Progressive Addition Lens on Working Distance and Refractive Status in Adult Computer Users. clinicaltrials.gov/show/NCT02775396 (first received 17 May 2016).
Additional references
AOA 2011
- The American Optometric Association (AOA). Computer Vision Syndrome (CVS). www.aoa.org/x5374.xml (accessed 1 September 2011).
Barcik 2010
- Barcik A, Siedlecki D. Optical performance of the eye with progressive addition lens correction. Optik 2010;121(21):1937‐40. [Google Scholar]
Bergqvist 1994
- Bergqvist UO, Knave BG. Eye discomfort and work with visual display terminals. Scandinavian Journal of Work, Environment & Health 1994;20(1):27‐33. [DOI] [PubMed] [Google Scholar]
Bhanderi 2008
- Bhanderi DJ, Choudhary S, Doshi VG. A community‐based study of asthenopia in computer operators. Indian Journal of Ophthalmology 2008;56(1):51‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Blehm 2005
- Blehm C, Vishnu S, Khattak A. Computer vision syndrome: A review. Survey of Ophthalmology 2005;50(3):259. [DOI] [PubMed] [Google Scholar]
Brewer 2006
- Brewer S, Eerd D, Amick III BC, Irvin E, Daum KM, Gerr F, et al. Workplace interventions to prevent musculoskeletal andvisual symptoms and disorders among computer users: A systematic review. Journal of Occupational Rehabilitation 2006;16(3):325‐58. [DOI] [PubMed] [Google Scholar]
Campbell 2001
- Campbell MK, Mollison J, Grimshaw JM. Cluster trials in implementation research: estimation of intracluster correlation coefficients and sample size. Statistics in Medicine 2001;20(3):391‐9. [DOI] [PubMed] [Google Scholar]
Dain 1988
- Dain SJ, McCarthy AK, Chan‐Ling T. Symptoms in VDU operators. American Journal of Optometry and Physiological Optics 1988;65(3):162‐7. [DOI] [PubMed] [Google Scholar]
Daum 1988
- Daum KM, Good G, Tijerina L. Symptoms in video display terminal operators and the presence of small refractive erro. Journal of the American Optometric Association 1988 Sep;59(9):691‐7. [PubMed] [Google Scholar]
Daum 2004
- Daum KM, Clore KA, Simms SS, Vesely JW, Wilczek DD, Spittle BM, et al. Productivity associated with visual status of computer users. Optometry 2004;75(1):33‐7. [DOI] [PubMed] [Google Scholar]
del Mar Seguí 2015
- Mar Seguí M, Cabrero‐Garcıa J, Crespoa A, Verduc J, Rondad E. A reliable and valid questionnaire was developed to measure computer vision syndrome at the workplace. Journal of Clinical Epidemiology 2015;68(6):662‐73. [DOI] [PubMed] [Google Scholar]
Edema 2010
- Edema OT, Akwukwuma VVN. Asthenopia and use of glasses among visual display terminal (VDU) users. International Journal of Tropical Medicine 2010;5(2):16‐9. [Google Scholar]
Egger 1998
- Egger M, Smith GD. Bias in location and selection of studies. BMJ 1998;316(7124):61‐6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Elbourne 2002
- Elbourne DR, Altman DG, Higgins JPT, Curtin F, Worthington HV, Vail A. Meta‐analysis involving cross‐over trials: methodological issues. International Journal of Epidemiology 2002;31(1):140‐9. [DOI] [PubMed] [Google Scholar]
European Council 1990
- European Council. Council Directive 90/270/EEC of 29 May 1990 on the minimum safety and health requirements for work with display screen equipment (fifth individual Directive within the meaning of Article 16 (1) of Directive 89/391/EEC).. EU Publication 1990.
Fu 2013
- Fu R, Vandermeer BW, Shamliyan TA, O'Neil ME, Yazdi F, Fox SH, et al. Handling of continuous outcomes in quantitative synthesis. Methods guide for comparative effectiveness reviews. Rockvile, MD, US: Agency for Healthcare Research and Quality, 2013. [PubMed] [Google Scholar]
Hanks 1996
- Hanks A, Kris M, Hartley LP, Peachey G, Simon A. A clinical wearer study of the sola access lens. Clinical and Experimental Optometry 1996;79(2):67‐73. [Google Scholar]
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327(7414):557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S, (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Johnson 2012
- Jonsson C. Visual ergonomics and computer work‐‐is it all about computer glasses?. Work 2012;41(Suppl 1):3577‐9. [DOI: 10.3233/WOR-2012-0638-3577.; PUBMED: 22317265.] [DOI] [PubMed] [Google Scholar]
Krefman 1991
- Krefman RA. A comparative evaluation of readables to single vision lenses. Journal of the American Optometric Association 1991;62(9):676‐9. [PubMed] [Google Scholar]
Leyshon 2010
- Leyshona R, Chalovab K, Gersonb L, Savtchenkob A, Zakrzewskib R, Howiec A, et al. Ergonomic interventions for office workers with musculoskeletal disorders: A systematic review. Work 2010;35(3):335‐48. [DOI] [PubMed] [Google Scholar]
Mancil 2010
- Mancil GL, Bailey IL, Campbell JB, Cho MH, Rosenbloom AA, Sheedy JE. Care of the patient with presbyopia. Reference guide for clinicians. www.aoa.org/documents/optometrists/CPG‐17.pdf. St. Louis, MO: American Optometric Association 2011, (accessed prior to 13 January 2018):26.
Mok 2011
- Mok AK‐H, Chung CS‐T, Kwok TW‐K. A simple clinical test for perception of progressive addition lens peripheral image blur. A pilot study. Journal of Optometry 2011;4(1):30‐4. [Google Scholar]
Nakaishi 1999
- Nakaishi N, Yamada Y. Abnormal tear dynamics and symptoms of eyestrain in operators of visual display terminals. Occupational and Environmental Medicine 1999;56(1):6‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Niskanen 2015
- Niskanen T, Lehtelä J. Finnish discourses of the stakeholders on development of the implementation of EU legislation concerned with occupational safety and health in computer work. International Journal of Occupational Safety and Ergonomics 2015;21(4):413‐25. [DOI: 10.1080/10803548.2015.1086194; PUBMED: 26327151.] [DOI] [PubMed] [Google Scholar]
Review Manager 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Rosenfield 2011
- Rosenfield M. Computer vision syndrome: a review of ocular causes and potential treatments. Ophthalmic & Physiological Optics 2011;31(5):502‐15. [DOI] [PubMed] [Google Scholar]
Rosner 1989
- Rosner M, Belkin M. Video display units and visual function. Survey of Ophthalmology 1989;33(6):515‐22. [DOI] [PubMed] [Google Scholar]
Sakimoto 2006
- Sakimoto T, Rosenblatt MI, Azar DT. Laser eye surgery for refractive errors. Lancet 2006;367(9520):1432‐47. [DOI] [PubMed] [Google Scholar]
Sanchez 1996
- Sanchez‐Roman FR, Perez‐Lucio C, Juarez‐Ruiz C, Velez‐Zamora NM, Jimenez‐Villarruel M. Risk factors for asthenopia among computer terminal operators. Salud Publica de Mexico 1996;38(3):189‐96. [PubMed] [Google Scholar]
Sheedy 1992
- Sheedy JE. Vision problems at video display terminals: a survey of optometrists. Journal of the American Optometric Association 1992;63(10):687‐92. [PubMed] [Google Scholar]
Sheedy 2003
- Sheedy JE, Hayes JN, Engle J. Is all asthenopia the same?. Optometry and Vision Science 2003;80(11):732‐9. [DOI] [PubMed] [Google Scholar]
Sheedy 2005
- Sheedy JE, Hardy RF. The optics of occupational progressive lenses. Optometry 2005;76(8):432‐41. [DOI] [PubMed] [Google Scholar]
Zhang 2008
- Zhang Y, Liang H, Hao C, Fan L. Computer Vision Syndrome: A widely spreading but largely unknown epidemic among computer users. Computers in Human Behavior 2009;11(24):2026–42. [Google Scholar]
References to other published versions of this review
Li 2012
- Li HH, Heus P, Li L, Yang J, Kuang J, Li YP, Xiong T. Optical correction of refractive error for preventing and treating eye symptoms in computer users. Cochrane Database of Systematic Reviews 2012, Issue 5. [DOI: 10.1002/14651858.CD009877] [DOI] [PMC free article] [PubMed] [Google Scholar]