

Abstract
Background
Cough causes concern for parents and is a major cause of outpatient visits. Cough can impact quality of life, cause anxiety, and affect sleep in children and their parents. Honey has been used to alleviate cough symptoms. This is an update of reviews previously published in 2014, 2012, and 2010.
Objectives
To evaluate the effectiveness of honey for acute cough in children in ambulatory settings.
Search methods
We searched CENTRAL (2018, Issue 2), which includes the Cochrane Acute Respiratory Infections Group's Specialised Register, MEDLINE (2014 to 8 February 2018), Embase (2014 to 8 February 2018), CINAHL (2014 to 8 February 2018), EBSCO (2014 to 8 February 2018), Web of Science (2014 to 8 February 2018), and LILACS (2014 to 8 February 2018). We also searched ClinicalTrials.gov and the World Health Organization International Clinical Trial Registry Platform (WHO ICTRP) on 12 February 2018. The 2014 review included searches of AMED and CAB Abstracts, but these were not searched for this update due to lack of institutional access.
Selection criteria
Randomised controlled trials comparing honey alone, or in combination with antibiotics, versus no treatment, placebo, honey‐based cough syrup, or other over‐the‐counter cough medications for children aged 12 months to 18 years for acute cough in ambulatory settings.
Data collection and analysis
We used standard methodological procedures expected by Cochrane.
Main results
We included six randomised controlled trials involving 899 children; we added three studies (331 children) in this update.
We assessed two studies as at high risk of performance and detection bias; three studies as at unclear risk of attrition bias; and three studies as at unclear risk of other bias.
Studies compared honey with dextromethorphan, diphenhydramine, salbutamol, bromelin (an enzyme from the Bromeliaceae (pineapple) family), no treatment, and placebo. Five studies used 7‐point Likert scales to measure symptomatic relief of cough; one used an unclear 5‐point scale. In all studies, low score indicated better cough symptom relief.
Using a 7‐point Likert scale, honey probably reduces cough frequency better than no treatment or placebo (no treatment: mean difference (MD) ‐1.05, 95% confidence interval (CI) ‐1.48 to ‐0.62; I² = 0%; 2 studies; 154 children; moderate‐certainty evidence; placebo: MD ‐1.62, 95% CI ‐3.02 to ‐0.22; I² = 0%; 2 studies; 402 children; moderate‐certainty evidence). Honey may have a similar effect as dextromethorphan in reducing cough frequency (MD ‐0.07, 95% CI ‐1.07 to 0.94; I² = 87%; 2 studies; 149 children; low‐certainty evidence). Honey may be better than diphenhydramine in reducing cough frequency (MD ‐0.57, 95% CI ‐0.90 to ‐0.24; 1 study; 80 children; low‐certainty evidence).
Giving honey for up to three days is probably more effective in relieving cough symptoms compared with placebo or salbutamol. Beyond three days honey probably had no advantage over salbutamol or placebo in reducing cough severity, bothersome cough, and impact of cough on sleep for parents and children (moderate‐certainty evidence). With a 5‐point cough scale, there was probably little or no difference between the effects of honey and bromelin mixed with honey in reducing cough frequency and severity.
Adverse events included nervousness, insomnia, and hyperactivity, experienced by seven children (9.3%) treated with honey and two children (2.7%) treated with dextromethorphan (risk ratio (RR) 2.94, 95% Cl 0.74 to 11.71; I² = 0%; 2 studies; 149 children; low‐certainty evidence). Three children (7.5%) in the diphenhydramine group experienced somnolence (RR 0.14, 95% Cl 0.01 to 2.68; 1 study; 80 children; low‐certainty evidence). When honey was compared with placebo, 34 children (12%) in the honey group and 13 (11%) in the placebo group complained of gastrointestinal symptoms (RR 1.91, 95% CI 1.12 to 3.24; I² = 0%; 2 studies; 402 children; moderate‐certainty evidence). Four children who received salbutamol had rashes compared to one child in the honey group (RR 0.19, 95% CI 0.02 to 1.63; 1 study; 100 children; moderate‐certainty evidence). No adverse events were reported in the no‐treatment group.
Authors' conclusions
Honey probably relieves cough symptoms to a greater extent than no treatment, diphenhydramine, and placebo, but may make little or no difference compared to dextromethorphan. Honey probably reduces cough duration better than placebo and salbutamol. There was no strong evidence for or against using honey. Most of the children received treatment for one night, which is a limitation to the results of this review. There was no difference in occurrence of adverse events between the honey and control arms.
Plain language summary
Honey for acute cough in children
Review question
Can honey reduce cough symptoms caused by bacteria and viruses in children?
Background
Cough causes concern for parents and is a major reason for outpatient visits. Honey is believed to prevent growth of germs and reduce inflammation.
Search date
We searched databases to 8 February 2018 and trial registers to 12 February 2018.
Study characteristics
We included six small trials involving 899 children aged 12 months to 18 years conducted in Iran, Israel, the USA, Brazil, and Kenya. This update included three new trials conducted between 2007 and 2016 that involved 331 children.
Study funding sources
Two studies were supported by pharmaceutical manufacturers; one by a university research centre; one by the Honey Board of Israel and non‐government agencies; and one by USA National Honey Board. One study did not report funding sources.
Key results
We compared honey to over‐the‐counter cough preparations, bromelin (a pineapple enzyme) mixed with honey, fake treatment (placebo), and no treatment.
Honey probably reduces cough symptoms more than placebo and salbutamol (a drug that opens lung airways) when given for up to three days. Honey is probably more effective at providing cough relief and reducing the impact of cough on children's sleep at night than no treatment.
There may be little or no difference between the effects of honey and dextromethorphan (an ingredient in over‐the‐counter cough remedies) or honey and bromelin with honey on all cough symptoms. Honey may be better than diphenhydramine (an antihistamine) at relieving and reducing children's cough.
The parents of seven children given honey and two given dextromethorphan reported side effects in their children, such as not falling asleep easily, restlessness, and becoming overexcited. The parents of three children in the diphenhydramine group reported that their children were often sleepy. The parents of nine children given salbutamol, seven given honey, and six given placebo reported diarrhoea. The parents of four children who received salbutamol and one child given honey reported rash.
We found no evidence for or against the use of honey to relieve cough in children. Using honey for infants aged up to 12 months is not advised because of poor immunity against bacteria that may be present, which can cause paralysis. Most of the children received honey for just one night, which is a limitation to the results of this review.
Quality of the evidence
Overall, evidence quality was low to moderate. Some studies did not blind participants.
Summary of findings
Background
Description of the condition
Cough is a normal protective mechanism (Landau 2006), and a means by which the respiratory system rids itself of excessive secretions and foreign bodies (Cuestas 2017). Cough can be caused by bacterial or viral infections, the presence of an irritant or allergen in the respiratory tract, or both (Ma 2017). Respiratory infections can be situated along the upper or lower respiratory tract, and the resulting cough can be either productive or unproductive of sputum. Unproductive cough is usually referred to as 'dry' cough. Children with dry cough tend to have minimal airway secretions (Chang 2005).
Cough can be classified as acute or chronic. Chronic cough lasts for more than three weeks (Smith 2016). Acute cough from upper respiratory tract infection (URTI) is a very common symptom seen in primary care settings or by general practitioners (Butler 2005; Derebery 2013). Most coughs from URTIs are caused by viral infections (Braman 2006; Butler 2005). Cough is cause for parental concern (Hay 2003), and a major reason for outpatient visits for both children and adults (Kigen 2015; Kusel 2007). Cough can impact on quality of life (French 2002), cause anxiety, and affect the sleep of children and their parents. For these reasons, immediate remedy for cough is often sought by parents and carers of children with cough.
Description of the intervention
Many people use over‐the‐counter (OTC) cough medications, and general practitioners in primary care settings often recommend these as first‐line treatments (Kigen 2015). Although many OTC cough preparations are available, there is no good evidence regarding their efficacy (Chang 2014; Smith 2014). In children, OTC cough medications may be associated with serious adverse events such as death, altered consciousness, and arrhythmias (CDC 2007; Gunn 2001; Kelly 2004). Study findings vary in reported relief of cough symptoms, with several studies finding no effect compared with placebo (Banderali 1995; Freestone 1997; Kurth 1978; Smith 2014).
Cough mixtures contain a variety of drugs with differing modes of action, which makes them difficult to compare (Morice 1998). Over‐the‐counter cough medications may contain dextromethorphan hydrobromide, phenylephrine hydrochloride, chlorpheniramine maleate, and methylparaben (El‐Gindy 2005).
Honey is a sweet, viscous liquid with a complex chemical composition of approximately 25 carbohydrates (Sanz 2004), free amino acids (Hermosin 2003; Suárez‐Luque 2002), vitamins and trace elements (Golob 2005; Hernández 2005; Nanda 2003; Tuzen 2007; Yao 2003). Honey also contains compounds that function as antioxidants such as flavonoids and carotenoids, polyphenol, phenolic acids, vitamin C, and glucose oxydase enzymes (Khalil 2010; Nagai 2006).
How the intervention might work
Honey confers antibacterial (Lusby 2005; Mullai 2007), antiviral (Shahzad 2012; Watanabe 2014; Zeina 1996), antifungal (Ahmed 2013b; Irish 2006; Kuncic 2012), and anti‐inflammatory properties (Tonks 2003). Studies of the antimicrobial effect of honey show that it has broad‐spectrum antimicrobial effects on various gram‐negative and gram‐positive bacteria (Agbaje 2006; Katrina 2014). Honey is reported to be active against certain bacteria that have been isolated from the upper respiratory tract such as Staphylococcus aureus, Enterococcus faecalis,Candida albicans,Klebsiella pneumoniae,Pseudomonas aeruginosa,Escherichia coli, Salmonella spp., and Shigella dysenteriae (Adeleye 2003; Kousalya 2010; Mullai 2007). Honey has antiviral effects against Varicella zoster virus (Shahzad 2012), influenza virus (Watanabe 2014), and rubella virus (Zeina 1996). It is believed that the antibacterial activities of honey are intrinsic and not dependent on any external factors such as geographical location or its source (Katrina 2014).
Honey has been used in traditional medicine to treat cough (Adeleye 2003), and in modern medicine to treat infected wounds (Lusby 2005; Molan 2006); it is also an ingredient in some cough syrups (Zeina 1996). However, the use of honey in infants aged under 12 months is restricted because of babies' poor immunity against Clostridium botulinum, a possible contaminant in honey (Küplülü 2006; Nevas 2002).
Why it is important to do this review
Identification of ineffective preparations for cough could reduce costs for consumers and healthcare providers (Smith 2014). Cochrane Reviews have assessed the effectiveness of OTC cough medications (Chang 2014; Smith 2014), but none have studied honey for cough relief.
If effective, honey may save significant annual expenditure on OTC cough medications (Dicpinigaitis 2011). Previous versions of this review were inconclusive about the effectiveness of using honey to treat acute cough in children (Oduwole 2010; Oduwole 2012; Oduwole 2014a). The aim of this review was to examine the comparative effectiveness of honey to relieve acute cough in children.
Objectives
To evaluate the effectiveness of honey for acute cough in children in ambulatory settings.
Methods
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs).
Types of participants
We included children aged 12 months to 18 years with cough caused by acute viral or bacterial URTI. We excluded studies that included participants with chronic cough (lasting for more than three weeks). We also excluded studies with sample sizes of fewer than 10 per intervention.
Types of interventions
Studies that compared:
-
honey only versus:
honey‐based cough syrup;
non‐honey cough syrup;
placebo; and
no treatment;
honey plus antibiotics versus antibiotics alone; and
honey plus antibiotics versus non‐honey cough syrups plus antibiotics
were eligible for inclusion.
Types of outcome measures
Primary outcomes
Duration of cough.
Symptomatic relief of cough (frequency of cough, reduction in severity, and less bothersome cough).
Secondary outcomes
Improvement in quality of sleep at night for children (cough impact on sleep score).
Improvement in quality of sleep at night for caregiver (cough impact on sleep score).
Improvement in quality of life (e.g. school attendance and playing).
Adverse effects.
Improvement in appetite.
Cost of honey alone compared with other cough syrups.
Search methods for identification of studies
Electronic searches
For this update we searched the Cochrane Central Register of Controlled Trials (CENTRAL; 2018, Issue 2), part of the Cochrane Library (searched 8 February 2018), which includes the Cochrane Acute Respiratory Infections Group's Specialised Register, MEDLINE (Ovid) (October 2014 to 8 February 2018), Embase (Elsevier) (October 2014 to 8 February 2018), CINAHL (Cumulative Index to Nursing and Allied Health Literature) (EBSCO) (October 2014 to 8 February 2018), Web of Science (Clarivate Analytics) (October 2014 to 8 February 2018), and LILACS (Latin American and Caribbean Health Sciences Literature) (BIREME) (October 2014 to 8 February 2018). The 2014 version of this review included searches of AMED (Appendix 1) and CAB Abstracts (Appendix 2), but these were not searched for this update due to lack of institutional access to those databases. Details of previous searches are in Appendix 3.
We used the search strategy in Appendix 4 to search MEDLINE and CENTRAL, and modified terms to search Embase (Appendix 5), CINAHL (Appendix 6), Web of Science (Appendix 7), and LILACS (Appendix 8). We did not combine the MEDLINE search string with the Cochrane Highly Sensitive Search Strategies for identifying randomised trials in MEDLINE (Lefebvre 2011), because we found very few results. We imposed no language or publication restrictions.
Searching other resources
We searched the World Health Organization International Clinical Trials Registry Platform (WHO ICTRP) (apps.who.int/trialsearch/) and ClinicalTrials.gov (www.clinicaltrials.gov) on 12 February 2018. We checked the reference lists of all relevant articles obtained from our search and those from previously published systematic reviews to identify additional articles. We also contacted the authors of studies added for this update for information and unpublished data (Ahmadi 2013; Paul 2007; Waris 2014).
Data collection and analysis
Selection of studies
Two review authors (OO, EU) independently screened search results using Covidence for eligible studies based on a priori inclusion criteria (Covidence). Any disagreements were resolved by consensus.
Data extraction and management
One review author (OO) independently extracted and entered data into Review Manager 5 (Review Manager 2014). Ahmadi 2013 was translated from Farsi to English for assessment. Another review author (EU) checked data extraction for accuracy and completeness. Any disagreements were resolved by consensus.
Assessment of risk of bias in included studies
Two review authors (OO, EU) assessed risk of bias of the included trials using Cochrane's 'Risk of bias' tool. We assessed random sequence generation, allocation concealment, blinding, selective reporting, and other sources of bias, and recorded the assessment in the 'Risk of bias' tables. We ranked the studies as low, unclear, or high risk of bias, as recommended in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Measures of treatment effect
We used one‐way analysis of variance (ANOVA) to compare treatment effects for cough duration, cough symptoms, and quality of sleep. We presented estimates of effects as mean differences (MD) derived from parents' subjective assessment of cough symptoms and cough impact on sleep quality using validated questions on a 7‐point Likert scale (Likert 1932).
We used the mean and standard deviation (SD) to analyse pair‐wise comparisons of treatment effect between honey and placebo and honey and salbutamol on cough duration. We also analysed pair‐wise comparisons of other outcomes using generic inverse variance in Review Manager 5 (Review Manager 2014). We estimated MD between children's Likert scores at baseline and postintervention for frequency of cough, bothersome cough, and cough impact on quality of sleep for child and parent. We used the MD and standard error (SE) for the pair‐wise comparison of treatment effect between honey and dextromethorphan, honey and diphenhydramine, honey and no treatment, honey and placebo, honey and salbutamol, and honey and bromelin. We used the Mantel‐Haenszel method to analyse the risk ratio (RR) for adverse events in Review Manager 5 (Review Manager 2014). We presented results for other measures of effects not presented as MD in Table 6.
1. Pre‐ and postintervention comparison of honey on cough frequency and severity expressed as medians.
| Study ID | Cough |
Honey (N = 29) |
Bromelin
(pineapple extract) + honey (N = 31) |
P value | Certainty of the evidence |
| Peixoto 2016 | Frequency of cough1 | ||||
| Before, median (P25 to P75) After, median (P25 to P75) Mean ± SD |
3 (2 to 4) 1 (1 to 1) 1.76 ± 0.87 |
3 (2 to 3) 1 (1 to 1) 1.71 ± 0.78 |
0.832 0.943 |
⊕⊕⊕⊝ MODERATE 4 | |
| Severity of cough1 | |||||
| Mean ± SD assessed with: unvalidated 5‐point cough scale from 0 to 4 |
‐0.86 ± 0.45 | ‐0.97 ± 0.62 | 0.322 0.223 | ⊕⊕⊕⊝ MODERATE 4 | |
|
Honey (N = 63) |
Diphenhydramine (N = 63) |
||||
| Ahmadi 2013 | Proportion of children with reduction in frequency and severity of daytime cough5 | 84.1% (N = 53) |
58.7% (N = 37) | "< 0.02" | ⊕⊕⊕⊝ MODERATE 4 |
| Proportion of children with reduction in frequency and severity of nighttime cough5 | 79.4% (N = 50) |
58.7% (N = 37) | "< 0.02" | ⊕⊕⊕⊝ MODERATE 4 | |
SD: standard deviation P: percentile
1Assessed on an unvalidated 5‐point cough scale from 0 to 4; lower score is better. 2Student's t test. 3Chi². 4Downgraded by one level for risk of bias and imprecision. 5Assessed on a 7‐point Likert scale from 0 to 6; lower score is better.
Unit of analysis issues
There were no unit of analysis issues.
Dealing with missing data
We contacted the lead author of Paul 2007 and obtained the SE of the mean. We used PEPI version 3, Abramson 1999, to calculate the SE of the mean for Shadkam 2010 and Microsoft 2007 for both Cohen 2012 and Waris 2014. We also contacted the authors of Waris 2014 and Peixoto 2016 to request unpublished data. Ahmadi 2013 was translated from Farsi to English.
We performed an intention‐to‐treat analysis by including all randomised children in the analysis according to methods provided in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We assumed that all missing participants did not improve.
Assessment of heterogeneity
We considered heterogeneity statistically significant when the I² statistic was ≥ 50%. We used the random‐effects model for meta‐analysis when the I² statistic was > 50%.
Assessment of reporting biases
We could not test for asymmetry using a funnel plot because we included fewer than 10 studies.
Data synthesis
We used the fixed‐effect model to combine data from four included studies (Cohen 2012; Paul 2007; Shadkam 2010; Waris 2014). We used the mean and SE to analyse pair‐wise comparisons of treatment effect between honey and placebo and honey and salbutamol on cough duration.
We used Review Manager 5 to perform an inverse‐variance meta‐analysis using a fixed‐effect model for differences in mean between pre‐ and postintervention (Review Manager 2014). We conducted pair‐wise comparisons of postintervention scores between honey and dextromethorphan, honey and diphenhydramine, honey and no treatment, honey and placebo, and honey and salbutamol. We used a random‐effects model in the presence of heterogeneity.
We extracted the estimates of effects (MD) and SE of the mean for each outcome and calculated 95% confidence intervals (CIs) of the MDs using generic inverse variance. We used the Mantel‐Haenszel method to analyse the RR for adverse events.
We combined the mean score of the three honey groups (eucalyptus, citrus, or Labiatae) and compared these to the placebo group in Cohen 2012.
Peixoto 2016 treated honey as a placebo and compared it to bromelin (a pineapple enzyme) mixed with honey. We presented the placebo arm as a honey intervention for Peixoto 2016. Because data for honey and bromelin were presented as medians, data were tabulated for presentation (Table 6).
We could not include Ahmadi 2013 in the meta‐analyses because the results were reported as a proportion of children with reduced cough score. We presented the results in Table 6.
GRADE and 'Summary of findings' table
We created 'Summary of findings' tables for the following outcomes:
duration of cough;
symptomatic relief of cough (frequency of cough, reduction in severity, and less bothersome cough);
improvement in quality of sleep at night for children (cough impact on sleep score);
improvement in quality of sleep at night for caregivers (cough impact on sleep score); and
adverse effects.
We used the five GRADE considerations (study limitations, consistency of effect, imprecision, indirectness, and publication bias) to assess the quality of a body of evidence as it relates to the studies that contribute data to the meta‐analyses for the prespecified outcomes (Atkins 2004). We used methods and recommendations described in Section 8.5 and Chapter 12 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), employing GRADEpro GDT software (GRADEpro GDT 2015). We justified all decisions to downgrade the quality of studies in footnotes, and made comments to aid readers' understanding of the review where necessary.
Subgroup analysis and investigation of heterogeneity
Data were available from six small studies, and investigation of sources of heterogeneity was not feasible. We used a random‐effects model to investigate possible sources of heterogeneity. We performed subgroup analyses for different types of honey.
Sensitivity analysis
We did not perform a sensitivity analysis because we included only five trials in the meta‐analyses.
Results
Description of studies
Results of the search
Our updated 2018 search yielded 321 records. After removal of duplicates, we screened 299 records by title and abstract, and excluded 290 records. We assessed nine full‐text records and excluded three studies that did not meet our inclusion criteria. This update included three additional studies (Ahmadi 2013; Peixoto 2016; Waris 2014), bringing the total number of included studies to six. We included two studies in the qualitative analysis (Ahmadi 2013; Peixoto 2016), and four in the meta‐analyses (Cohen 2012; Paul 2007; Shadkam 2010; Waris 2014). See Figure 1.
1.
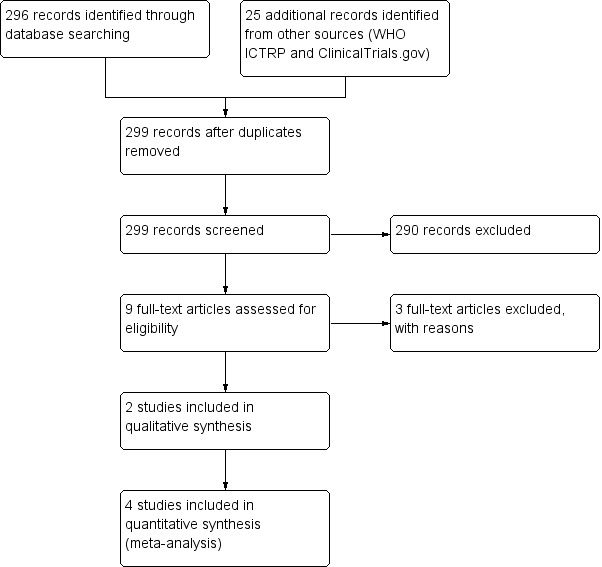
Study flow diagram (2018 update).
Included studies
We included six RCTs involving 899 children (Ahmadi 2013; Cohen 2012; Paul 2007; Peixoto 2016; Shadkam 2010; Waris 2014). Of these, three were added for this update (N = 331) (Ahmadi 2013; Peixoto 2016; Waris 2014). Ahmadi 2013 was published in Farsi and was translated for analysis. In our protocol we proposed to include children aged from 2 to 18 years. We decided to include studies with children aged 12 months to 18 years because very few clinical trials were available on honey for acute cough in children. We also think that it is best for physicians to decide whether or not to prescribe honey to children aged up to 12 months based on the available evidence.
Study populations
The age of participants ranged from 12 months to 16 years. We obtained proportions of boys and girls from available data only.
Ahmadi 2013 randomised 126 children aged from 2 to 5 years (48% boys, 52% girls) with viral URTI with cough for up to 2 days. Study duration was two years (2010 to 2012).
Cohen 2012 randomised 300 children aged 12 to 71 months (54% boys, 46% girls) with URTI who "were ill with a mean ± SD of 2.8 ± 2.0 before enrolment". Study duration was a year (January 2009 to December 2009).
Paul 2007 randomised 108 children aged 2 to 16 years (105 completed the study; 47% boys, 53% girls) with URTI "characterized by the presence of rhinorrhoea and cough for 7 or fewer days’ duration. Other symptoms may have included but were not limited to congestion, fever, sore throat, myalgias, and headache". Study duration was six months (September 2005 to March 2006).
Peixoto 2016 randomised 60 children aged 2 to 15 years (43% boys, 57% girls) "with irritative cough for at least 24 hours, which led to the need for medical consultation" and no history of chronic disease. The study start date was June 2011 and the estimated completion date was March 2012, however the actual study completion date is unclear.
Shadkam 2010 randomised 160 children aged 24 to 60 months (139 completed the study; 49% boys, 51% girls) with URTI‐induced cough. The study started in December 2008 and ended in May 2009.
Waris 2014 randomised 145 children aged 12 months to 12 years (51% boys, 49% girls) with uncomplicated acute upper respiratory infection. Waris 2014 enrolled participants from December 2010 to February 2012.
No studies enrolled children with comorbidities.
Study settings
Studies by Ahmadi 2013 and Shadkam 2010 were conducted in Iran; Cohen 2012 in Israel; Paul 2007 in the USA; Peixoto 2016 in Brazil; and Waris 2014 in Kenya.
Five were single‐centre studies (Ahmadi 2013; Paul 2007; Peixoto 2016; Shadkam 2010; Waris 2014). Cohen 2012 enrolled participants from six study centres.
All studies recruited participants from paediatric outpatient clinics.
Interventions
Honey mixed with distilled lukewarm water (Ahmadi 2013).
Three different types of honey: eucalyptus (family Myrtaceae), Labiatae (family Labiatae), or citrus (family Rutaceae) honeys (Cohen 2012).
Buckwheat honey (Paul 2007).
Honey was placebo and compared to bromelin (Ananas comosus, pineapple extract) mixed with honey (Peixoto 2016).
Natural honey from Kafi‐Abad (a village in Yazd, Iran) (Shadkam 2010).
"the darkest locally available honey" (Kenya) (Waris 2014).
Comparators
Ahmadi 2013 compared honey and diphenhydramine. Children received interventions three times a day, the last dose one hour before bed at night.
Cohen 2012 compared three types of honey to placebo ("Silan date extract was selected as the placebo because its structure, brown color, and taste are similar to that of honey" p. 466) ("Parents were instructed to administer 10 g of their child’s treatment product within 30 minutes of the child going to sleep" p. 466). Treatment could also be given with a non‐caffeinated beverage.
Paul 2007 compared honey to dextromethorphan and no treatment. Parents were told that their child’s treatment could be given with a non‐caffeinated beverage administered within 30 minutes of the child going to sleep.
Peixoto 2016 compared honey alone (labelled as placebo) to bromelin (Ananas comosus (pineapple)) mixed with honey. Two treatment regimens were administered: children up to 20 kg received 5 mL; those weighing > 20 kg received 1 mL for every 5 kg of additional weight.
Shadkam 2010 compared honey to dextromethorphan, diphenhydramine, and no treatment. Treatment regimens were administered before sleep.
Waris 2014 compared honey to salbutamol and placebo. The interventions were administered three times daily for five days.
Study funding sources
All included studies declared no conflicts of interest.
Source of funding for Ahmadi 2013 was not declared.
Cohen 2012 reported "This study was supported in part by a research grant from the Israel Ambulatory Pediatric Association, Materna Infant Nutrition Research Institute, and the Honey Board of Israel. The funders had no role in the study design, data collection or analysis, decision to publish, or preparation of the manuscript" (p. 465).
Peixoto 2016 was funded by Hebron Indústrias Químicas (a pharmaceutical manufacturer) (p. 416).
Paul 2007 reported "This work was supported by an unrestricted research grant from the National Honey Board, an industry‐funded agency of the US Department of Agriculture" (p. 1145).
Shadkam 2010 was "fully funded by the Department of Research Administration, Shahid Sadoughi University of Medical Sciences (SSUMS) in Yazd, Iran" (p. 791).
Waris 2014 indicated that "Universal Corporation Ltd prepared all study drugs and at no cost" (p. 55).
Excluded studies
We excluded three studies after assessment for this update: Cohen 2017 compared honey‐based cough syrup to non‐honey‐based cough syrup; Ayazi 2017 was a quasi‐RCT; Baker 2016 was a commentary on our review. We had previously excluded two studies, Gilbert 2008 and Warren 2007, from our 2010 review (Oduwole 2010); and two studies, Ahmed 2013a and Miceli Sopo 2014, from the 2014 update (Oduwole 2014a).
Studies awaiting classification
We had previously identified two studies that were awaiting classification (Ahmadi 2013; Peixoto 2016), which we included in this update.
Ongoing studies
We identified two ongoing studies (NCT03218696; UMIN000020651). A study identified as ongoing in 2014 was published, but was excluded because it was a quasi‐RCT (Ayazi 2017).
Risk of bias in included studies
Two review authors independently assessed the methodological quality of all included studies according to the methods described in the Cochrane Handbook for Systematic Reviews of Interventions (Figure 2; Figure 3) (Higgins 2011).
2.
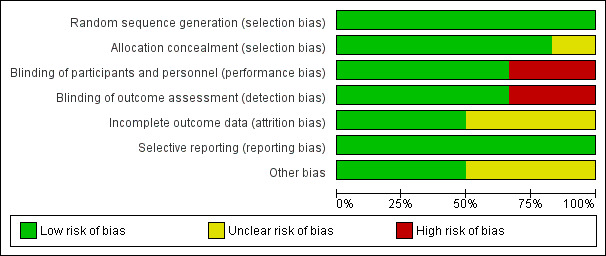
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.
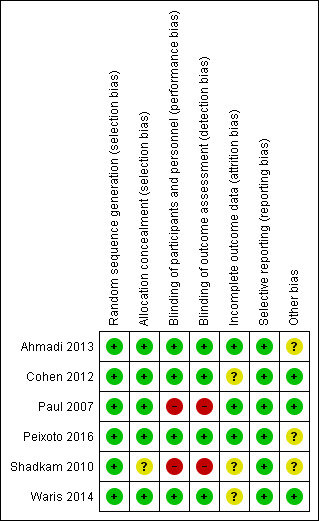
'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
Allocation
We rated all six included studies as at low risk of bias for sequence generation. We assessed five studies as at low risk for allocation concealment bias (Ahmadi 2013; Cohen 2012; Paul 2007; Peixoto 2016; Waris 2014). We rated Shadkam 2010 as at unclear risk of bias for this domain.
Blinding
We rated four studies as at low risk for performance and detection bias (Ahmadi 2013; Cohen 2012; Peixoto 2016; Waris 2014). We assessed two studies as at high risk of bias for this domain (Paul 2007; Shadkam 2010). There was partial blinding in Paul 2007; only the no‐treatment group was aware of receiving no intervention. We rated Paul 2007 as at high risk of bias for this domain because all outcomes were subjective: participants knowing they received no treatment could have influenced performance and assessment of the outcomes.
Incomplete outcome data
We assessed three studies as at low risk of bias of attrition bias (Ahmadi 2013; Paul 2007; Peixoto 2016). We assessed three studies as at unclear risk of attrition bias (Cohen 2012; Shadkam 2010; Waris 2014). In Cohen 2012, attrition was significantly higher in the eucalyptus honey (19%) and citrus honey (18%) groups than Labiatae honey (3%) and placebo (5%) groups. It was unclear if reasons for attrition were related to the study. Shadkam 2010 reported that children were either lost to follow‐up or were withdrawn for violating the protocol (but did not state to which group children lost to follow‐up or withdrawn belonged).
Selective reporting
We rated all studies as at low risk of bias for selective reporting; all outcomes proposed in the methods sections were reported in results. We obtained protocols of two included studies (Ahmadi 2013; Peixoto 2016); both reported all outcomes proposed.
Other potential sources of bias
We assessed two studies as at low risk of bias (Cohen 2012; Paul 2007; Waris 2014), and three studies as at unclear risk of bias for this domain (Ahmadi 2013; Peixoto 2016; Shadkam 2010). In Shadkam 2010, "Some of the questions put to mothers were answered by the paediatrician because the questions were ambiguous", which could have influenced outcome assessment. Ahmadi 2013 reported results as the proportion of children with reduced cough symptoms instead of actual mean reduction in cough scores of children as reported by other studies. In addition, the study protocol was registered retrospectively after completion of the study (Ahmadi 2013). It is unclear if the authors had planned to report results as proportion of children with reduced cough score. It is also not clear if the two outcomes (cough frequency and severity) listed in the methods section of the published paper and protocol was their original intention (Ahmadi 2013). Peixoto 2016 used an unvalidated cough scale.
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5
Summary of findings for the main comparison. Honey compared to dextromethorphan for acute cough in children.
| Honey compared to dextromethorphan for acute cough in children | ||||||
| Patient or population: acute cough in children Setting: ambulatory Intervention: honey Comparison: dextromethorphan | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with dextromethorphan | Risk with honey | |||||
| Duration of cough | ‐ | ‐ | ‐ | ‐ | ‐ | Not assessed |
| Frequency of cough1 | The mean frequency of cough (reduction in frequency of cough score) was ‐1.54. | MD 0.07 score lower (1.07 lower to 0.94 higher) | ‐ | 149 (2 RCTs) | ⊕⊕⊝⊝ LOW 2, 3 | Follow‐up: mean 1 day |
| Severity of cough1 | The mean severity of cough (reduction in severity of cough score) was ‐1.52. | MD 0.13 score lower (1.25 lower to 0.99 higher) | ‐ | 149 (2 RCTs) | ⊕⊕⊝⊝ LOW 2, 3 | Follow‐up: mean 1 day |
| Bothersome cough1 | The mean bothersome cough (reduction in bothersome nature of cough score) was ‐1.94. | MD 0.29 score higher (0.56 lower to 1.14 higher) | ‐ | 69 (1 RCT) | ⊕⊕⊕⊝ MODERATE 5 | Follow‐up: mean 1 day |
| Cough impact on children's sleep1 | The mean cough impact on children's sleep (cough impact on children' sleep score) was ‐1.75. | MD 0.03 score higher (1.12 lower to 1.19 higher) | ‐ | 149 (2 RCTs) | ⊕⊕⊝⊝ LOW 2, 3 | Follow‐up: mean 6 days |
| Cough impact on parents' sleep1 | The mean cough impact on parents' sleep (cough impact on parents' sleep score) was ‐1.97. | MD 0.16 score lower (0.84 lower to 0.53 higher) | ‐ | 149 (2 RCTs) | ⊕⊕⊝⊝ LOW 2, 3 | Follow‐up: mean 1 day |
| Adverse events | Population | |||||
| Nervousness, insomnia, hyperactivity | 3 per 100 | 8 per 100 (2 to 32) |
RR 2.94 (0.74 to 11.71) | 149 (2 RCTs) | ⊕⊕⊝⊝ LOW 4 | Follow‐up: mean 1 day |
| Stomachache, nausea, and vomiting | 1 per 100 | 7 per 100 (0 to 100) |
RR 4.86 (0.24 to 97.69) | 69 (1 RCT) | ⊕⊕⊝⊝ LOW 5 | |
| Drowsiness | 1 per 100 | 4 per 100 (0 to 100) | RR 2.92 (0.12 to 69.20) | 69 (1 RCT) | ⊕⊕⊝⊝ LOW 5 | |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; RCT: randomised controlled trial; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Assessed on a 7‐point Likert scale from 0 to 6; lower score is better. 2Downgraded by one level because of study limitations: it was unclear if Shadkam 2010 concealed allocation; there was no blinding, which could increase the risk of bias in the study outcomes. 3Downgraded by one level for serious heterogeneity, which could be due to difference in dextromethorphan dose. In Paul 2007, 8.5 mg/2.5 mL dextromethorphan was given compared to 7.5 mg/2.5 mL given to children aged under 5 years by Shadkam 2010. 4Downgraded by two levels for risk of bias, inconsistency, and imprecision; the studies were underpowered to detect differences. 5Downgraded by two levels for very serious imprecision. Data were available from only Paul 2007, which had a small sample size.
Summary of findings 2. Honey compared to diphenhydramine for acute cough in children.
| Honey compared to diphenhydramine for acute cough in children | ||||||
| Patient or population: acute cough in children Setting: ambulatory Intervention: honey Comparison: diphenhydramine | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with diphenhydramine | Risk with honey | |||||
| Cough duration | ‐ | ‐ | ‐ | ‐ | ‐ | Not assessed |
| Frequency of cough1 | The mean frequency of cough (reduction in cough frequency score) was ‐1.73. | MD 0.57 lower (0.9 lower to 0.24 lower) | ‐ | 80 (1 RCT) | ⊕⊕⊝⊝ LOW 2, 3 | Follow‐up: mean 1 day |
| Severity of cough1 | The mean severity of cough (reduction in cough severity score) was ‐1.83. | MD 0.6 lower (0.94 lower to 0.26 lower) | ‐ | 80 (1 RCT) | ⊕⊕⊝⊝ LOW 2, 3 | Follow‐up: mean 1 day |
| Cough impact on children's sleep1 | The mean cough impact on children's sleep (cough impact on children' sleep score) was ‐1.64. | MD 0.55 score lower (0.87 lower to 0.23 lower) | ‐ | 80 (1 RCT) | ⊕⊕⊝⊝ LOW 2, 3 | Follow‐up: mean 6 days |
| Cough impact on parents' sleep1 | The mean cough impact on parents' sleep (cough impact on parents' sleep score) was ‐1.89. | MD 0.48 lower (0.76 lower to 0.2 lower) | ‐ | 80 (1 RCT) | ⊕⊕⊝⊝ LOW 2, 3 | Follow‐up: mean 1 day |
| Adverse event: Somnolence | Population | 1 per 100 (0 to 20) | RR 0.14 (0.01 to 2.68) | 80 (1 RCT) | ⊕⊕⊝⊝ LOW 2, 3 | Follow‐up: mean 1 day |
| 8 per 100 | ||||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; RCT: randomised controlled trial; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Assessed on a 7‐point Likert scale from 0 to 6; lower score is better. 2Downgraded by one level because of study limitations: it was unclear if Shadkam 2010 concealed allocation; there was no blinding, which could increase the risk of bias in the study outcomes. 3Downgraded by one level for serious imprecision: data were from one small study (Shadkam 2010).
Summary of findings 3. Honey compared to no treatment for acute cough in children.
| Honey compared to no treatment for acute cough in children | ||||||
| Patient or population: acute cough in children Setting: ambulatory Intervention: honey Comparison: 'no treatment' | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with no treatment | Risk with honey | |||||
| Cough duration | ‐ | ‐ | ‐ | ‐ | ‐ | Not assessed |
| Frequency of cough1 | The mean frequency of cough (reduction in cough frequency score) was ‐0.98. | MD 1.05 lower (1.48 lower to 0.62 lower) | ‐ | 154 (2 RCTs) | ⊕⊕⊕⊝ MODERATE 2, 3 | Follow‐up: mean 1 day |
|
Severity of cough1 assessed with: 7‐point Likert scale Scale from 0 to 6 |
The mean severity of cough (reduction in severity of cough score) was ‐1.13. | MD 1.03 score lower (1.59 lower to 0.47 lower) | ‐ | 154 (2 RCTs) | ⊕⊕⊕⊝ MODERATE 2, 3 | Follow‐up: mean 1 day |
| Bothersome cough1 assessed with: 7‐point Likert scale Scale from 0 to 6 | The mean bothersome cough (reduction in bothersome nature of cough score) was ‐1.30. | MD 0.93 score lower (1.98 lower to 0.12 higher) | ‐ | 74 (1 RCT) | ⊕⊕⊝⊝ LOW 2, 4 | Follow‐up: mean 1 day |
| Cough impact on children's sleep1 assessed with: 7‐point Likert scale Scale from 0 to 6 | The mean cough impact on children's sleep (cough impact on children' sleep score) was ‐1.28. | MD 1.04 score lower (1.57 lower to 0.51 lower) | ‐ | 154 (2 RCTs) | ⊕⊕⊕⊝ MODERATE 2, 3 | Follow‐up: mean 6 days |
|
Cough impact on parents' sleep1 assessed with: 7‐point Likert scale Scale from 0 to 6 |
The mean cough impact on parents' sleep (cough impact on parents' sleep score) was ‐1.46. | MD 0.88 score lower (1.23 lower to 0.52 lower) | ‐ | 154 (2 RCTs) | ⊕⊕⊕⊝ MODERATE 2, 3 | Follow‐up: mean 1 day |
| Adverse events | Population | |||||
| Nervousness, insomnia, hyperactivity | 1 per 100 | 6 per 100 (1 to 33) | RR 9.40 (1.16 to 76.20) | 154 (2 RCTs) | ⊕⊕⊝⊝ LOW 2, 4 | Follow‐up: mean 1 day |
| Stomachache, nausea, and vomiting | 1 per 100 | 7 per 100 (0 to 62) | RR 5.90 (0.27 to 127.14) | 74 (1 RCT) | ⊕⊕⊝⊝ LOW 2, 4 | |
| Drowsiness | 1 per 100 | 4 per 100 (0 to 53) | RR 3.43 (0.14 to 87.09) | 74 (1 RCT) | ⊕⊕⊝⊝ LOW 2, 4 | |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; RCT: randomised controlled trial; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Assessed on a 7‐point Likert scale from 0 to 6; lower score is better. 2Downgraded by one level for risk of bias. Participants in the no‐treatment arm were not blinded; knowledge of receiving no treatment may have influenced assessment of this subjective outcome (Paul 2007; Shadkam 2010). 3Downgraded by one level for imprecision and risk of bias. 4Downgraded by one level for serious imprecision: data from one small study (Paul 2007).
Summary of findings 4. Honey compared to placebo for acute cough in children.
| Honey compared to placebo for acute cough in children | ||||||
| Patient or population: acute cough in children Setting: ambulatory Intervention: honey Comparison: placebo | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with placebo | Risk with honey | |||||
| Day 1 | ||||||
| Frequency of cough1 | The mean frequency of cough (reduction in cough frequency score) was ‐0.99. | MD 1.62 score lower (3.02 lower to 0.22 lower) | ‐ | 402 (2 RCT) | ⊕⊕⊕⊝ MODERATE 2 | Follow‐up: mean 1 day |
| Severity of cough1 | The mean severity of cough (reduction in severity of cough score) was ‐0.80. | MD 1.07 score lower (2.43 lower to 0.3 higher) | ‐ | 402 (2 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Bothersome cough (mean improvement score)1 | The mean bothersome cough (reduction in bothersome nature of cough) was ‐1.08. | MD 1.4 score lower (2.82 lower to 0.03 higher) | ‐ | 402 (2 RCTs) | ⊕⊕⊕⊝ MODERATE 2 | |
| Cough impact on children's sleep1 | The mean cough impact on children's sleep (cough impact on children' sleep score) was ‐1.03. | MD 1.21 score lower (2.61 lower to 0.19 higher) | ‐ | 402 (2 RCTs) | ⊕⊕⊕⊝ MODERATE 2 | Follow‐up: mean 6 days |
| Cough impact on parents' sleep1 | The mean cough impact on parents' sleep (cough impact on parents' sleep score) was ‐1.44. | MD 1.29 score lower (2.71 lower to 0.13 higher) | ‐ | 402 (2 RCTs) | ⊕⊕⊕⊝ MODERATE 2 | Follow‐up: mean 1 day |
| Day 3 | ||||||
| Frequency of cough1 | The mean frequency of cough (reduction in frequency of cough score) was ‐0.9. | MD 1.13 score lower (1.71 lower to 0.55 lower) | ‐ | 102 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | Follow‐up: mean 6 days |
| Severity of cough1 | The mean severity of cough (reduction in severity of cough score) was ‐1.08. | MD 0.85 score lower (1.41 lower to 0.29 lower) | ‐ | 102 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Bothersome cough1 | The mean bothersome cough (reduction in bothersome nature of cough score) was ‐0.99. | MD 1.33 score lower (1.87 lower to 0.79 lower) | ‐ | 102 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Cough impact on children's sleep1 | The mean cough impact on children's sleep (cough impact on children's sleep score) was ‐0.46. | MD 0.93 score lower (1.42 lower to 0.44 lower) | ‐ | 102 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Cough impact on parents' sleep3 | The mean cough impact on parents' sleep (cough impact on parents' sleep score) was ‐1.04. | MD 0.88 score lower (1.38 lower to 0.38 lower) | ‐ | 102 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Day 5 | ||||||
| Cough duration | The mean cough duration was 5.18 days. | MD 0.72 days lower (1.31 lower to 0.13 lower) | ‐ | 102 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | Follow‐up: mean 6 days; assessed with: 7‐point Likert scale Scale from 0 to 6 |
| Frequency of cough1 | The mean frequency of cough (reduction in frequency of cough score) was ‐1.95. | MD 0.48 score lower (2.95 lower to 1.99 higher) | ‐ | 102 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Severity of cough1 | The mean severity of cough (reduction in severity of cough score) was ‐1.96. | MD 0.43 score lower (2.21 lower to 1.35 higher) | ‐ | 102 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Bothersome cough1 | The mean bothersome cough (reduction in bothersome nature of cough score) was ‐1.85. | MD 0.51 score lower (3.01 lower to 1.99 higher) | ‐ | 102 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Cough impact on children's sleep1 | The mean cough impact on children's sleep (cough impact on children' sleep score) was ‐1.68. | MD 0.55 score lower (1.79 lower to 0.69 higher) | ‐ | 102 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Cough impact on parents' sleep | The mean cough impact on parents' sleep (cough impact on parents' sleep score) was ‐1.54. | MD 0.57 score lower (1.59 lower to 0.45 higher) | ‐ | 102 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Adverse events | Population | |||||
| Stomachache, nausea, and vomiting | 11 per 100 | 21 per 100 (12 to 35) | RR 1.91 (1.12 to 3.24) | 402 (2 RCTs) | ⊕⊕⊕⊝ MODERATE2 | Follow‐up: mean 6 days |
| Diarrhoea | 13 per 100 | 12 per 100 (4 to 34) | RR 0.92 (0.33 to 2.55) | 102 (1 RCT) | ⊕⊕⊝⊝ LOW 3 | |
| Tachycardia | 2 per 100 | 4 per 100 (0 to 37) | RR 1.58 (0.15 to 16.86) | 102 (1 RCT) | ⊕⊕⊝⊝ LOW 3 | |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; RCT: randomised controlled trial; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Assessed on a 7‐point Likert scale from 0 to 6; lower score is better. 2Downgraded by one level for serious imprecision. 3Downgraded by two levels for very serious imprecision: Waris 2014 was insufficiently powered to detect differences.
Summary of findings 5. Honey compared to salbutamol for acute cough in children.
| Honey compared to salbutamol for acute cough in children | ||||||
| Patient or population: acute cough in children Setting: ambulatory Intervention: honey Comparison: salbutamol | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with salbutamol | Risk with honey | |||||
| Day 1 | ||||||
| Frequency of cough (mean improvement score)1 | The mean frequency of cough (reduction in frequency of cough score) was ‐0.52. | MD 0.26 lower (3.14 lower to 2.62 higher) | ‐ | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | Follow‐up: mean 6 days |
| Severity of cough (mean improvement score)1 | The mean severity of cough (reduction in severity of cough score) was ‐0.74. | MD 0.1 lower (0.39 lower to 0.19 higher) | ‐ | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Bothersome cough (mean improvement score)1 | The mean bothersome cough (reduction in bothersome nature of cough score) was ‐1.00. | MD 0.21 lower (0.9 lower to 0.48 higher) | ‐ | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Cough impact on children's sleep1 | The mean cough impact on children's sleep (cough impact on children' sleep score) was ‐1.24. | MD 0.09 higher (0.05 lower to 0.23 higher) | ‐ | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Cough impact on parents' sleep1 | The mean cough impact on parents' sleep (cough impact on parents' sleep score) was ‐1.22. | MD 0.05 higher (0.03 lower to 0.13 higher) | ‐ | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Day 3 | ||||||
| Frequency of cough1 | The mean frequency of cough (reduction in frequency of cough score) was ‐1.34. | MD 0.69 lower (1.13 lower to 0.25 lower) | ‐ | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | Follow‐up: mean 4 days |
| Severity of cough1 | The mean severity of cough (reduction in severity of cough score) was ‐1.59. | MD 0.34 lower (0.64 lower to 0.04 lower) | ‐ | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Bothersome cough1 | The mean bothersome cough (reduction in bothersome nature of cough score) was ‐2.08. | MD 0.24 lower (0.38 lower to 0.1 lower) | ‐ | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Cough impact on children's sleep1 | The mean cough impact on children's sleep (cough impact on children' sleep score) was ‐2.25. | MD 0.31 higher (0.13 higher to 0.49 higher) | ‐ | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | Follow‐up: mean 6 days |
| Cough impact on parents' sleep1 | The mean cough impact on parents' sleep (cough impact on parents' sleep score) was ‐2.13. | MD 0.21 higher (0.06 higher to 0.36 higher) | ‐ | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | Follow‐up: mean 4 days |
| Day 5 | ||||||
| Cough duration assessed (days) | The mean cough duration was 5 days. | MD 0.54 days lower (0.98 lower to 0.1 lower) | ‐ | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | Follow‐up: mean 6 days |
| Frequency of cough (mean improvement score)1 | The mean frequency of cough (reduction in frequency of cough score) was ‐2.19. | MD 0.54 lower (1.03 lower to 0.05 lower) | ‐ | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Severity of cough (mean improvement score)1 | The mean severity of cough (reduction in severity of cough score) was ‐2.08. | MD 0.41 lower (0.78 lower to 0.04 lower) | ‐ | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Bothersome cough (mean improvement score)1 | The mean bothersome cough (reduction in bothersome nature of cough score) was ‐2.47. | MD 0.27 lower (0.48 lower to 0.06 lower) | ‐ | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Cough impact on children's sleep1 | The mean cough impact on children's sleep (cough impact on children's sleep score) was ‐2.47. | MD 0.15 higher (0.04 higher to 0.26 higher) | ‐ | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Cough impact on parents' sleep1 | The mean cough impact on parents' sleep (cough impact on parents' sleep score) was ‐2.33. | MD 0.04 higher (0.01 higher to 0.07 higher) | ‐ | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Adverse events | Population | |||||
| Stomachache, nausea, and vomiting | 30 per 100 | 53 per 100 (31 to 88) | RR 1.74 (1.04 to 2.92) | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | Follow‐up: mean 6 days |
| Rash | 9 per 100 | 2 per 100 (0 to 15) | RR 0.19 (0.02 to 1.63) | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| Tachycardia | 2 per 100 | 4 per 100 (0 to 39) | RR 1.51 (0.14 to 16.10) | 100 (1 RCT) | ⊕⊕⊝⊝ LOW 3 | |
| Diarrhoea | 21 per 100 | 12 per 100 (5 to 30) | RR 0.59 (0.24 to 1.45) | 100 (1 RCT) | ⊕⊕⊕⊝ MODERATE 2 | |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; RCT: randomised controlled trial; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: We are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: Our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low certainty: We have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Assessed on a 7‐point Likert scale from 0 to 6; lower score is better. 2Downgraded by one level for serious imprecision. Data were from one small study (Waris 2014). 3Downgraded by two levels for very serious imprecision. Data were from one small study (Waris 2014).
Primary outcomes
1. Duration of cough
Only one study assessed duration of cough in comparison to salbutamol and placebo (Waris 2014). The effect of honey on cough duration was compared to salbutamol after five days of treatment; moderate‐certainty evidence indicated that cough was relieved sooner in children who received honey (mean difference (MD) ‐0.54, 95% confidence interval (CI) ‐0.98 to ‐0.10; 1 study, N = 100; Analysis 1.13). Compared with placebo, honey also provided faster cough relief (MD ‐0.72, 95% CI ‐1.31 to ‐0.13; 1 study, N = 102; Analysis 1.8; moderate‐certainty evidence).
1.13. Analysis.
Comparison 1 Pair‐wise comparison, Outcome 13 Honey versus salbutamol (Day 5).
1.8. Analysis.
Comparison 1 Pair‐wise comparison, Outcome 8 Honey versus placebo (Day 5).
2. Symptomatic relief of cough (frequency of cough, reduction in severity, and less bothersome)
2.1 Frequency of cough (pre‐ and postintervention comparison)
Four studies used a 7‐point Likert scale to report cough frequency (Ahmadi 2013; Cohen 2012; Paul 2007; Shadkam 2010; Waris 2014). Caregivers' responses to the questionnaire on cough symptoms ranged from 'extremely' (6 points) to 'not at all' (0 points) (lower score indicated better cough symptom relief). Pre‐ and postintervention comparison for each treatment arm showed that honey was more effective in reducing the frequency of cough in six studies. Four studies were meta‐analysed (moderate‐certainty evidence) (Cohen 2012; Paul 2007; Shadkam 2010; Waris 2014). Data from two studies are presented in Table 6 (moderate‐certainty evidence, one study with unclear cough scales) (Ahmadi 2013; Peixoto 2016).
When the effect of honey on cough symptoms was compared after a five‐day treatment to the night before the first dose of intervention (pre‐ and postintervention cough score) using the 7‐point Likert scale, honey reduced cough frequency to a greater extent (MD ‐2.65, 95% CI ‐4.32 to ‐0.98; 1 study, N = 57; moderate‐certainty evidence) than salbutamol (MD ‐2.19, 95% CI ‐3.55 to ‐0.83; 1 study, N = 43; moderate‐certainty evidence) and placebo (MD ‐1.95, 95% CI ‐4.42 to 0.52; 1 study, N = 45; moderate‐certainty evidence; Analysis 2.1).
2.1. Analysis.
Comparison 2 Pre‐ and postintervention comparison, Outcome 1 Cough frequency (mean reduction in frequency).
When the frequency of cough on Day 1 of treatment was assessed, parents of children in the honey group rated their children's coughs to be slightly less frequent (MD ‐1.71, 95% CI ‐2.28 to ‐1.13; I² = 0%; 4 studies, N = 357; moderate‐certainty evidence) compared to children who received dextromethorphan (MD ‐1.54, 95% CI ‐2.30 to ‐0.78; 2 studies, N = 74; moderate‐certainty evidence), placebo (MD ‐0.99, 95% CI ‐1.79 to ‐0.18; I² = 0%; 2 studies, N = 120; moderate‐certainty evidence), no treatment (MD ‐0.98, 95% CI ‐1.38 to ‐0.59; I² = 17%; 2 studies, N = 79; low‐certainty evidence), and salbutamol (MD ‐0.52, 95% CI ‐6.28 to 5.24; 1 study, N = 43; moderate‐certainty evidence), but not better than diphenhydramine (MD ‐1.73, 95% CI ‐2.72 to ‐0.74; 1 study, N = 40; low‐certainty evidence; Analysis 2.1).
2.2 Reduction in severity
Similarly, honey reduced the severity of cough in children postintervention on a 7‐point Likert scale (MD ‐1.65, 95% CI ‐2.39 to ‐0.91; I² = 0%; 4 studies, N = 357; moderate‐certainty evidence) to a greater extent than dextromethorphan (MD ‐1.52, 95% CI ‐2.24 to ‐0.80; I² = 29%; 2 studies, N = 74; moderate‐certainty evidence), no treatment (MD ‐1.13, 95% CI ‐1.54 to ‐0.72; I² = 2%; 2 studies, N = 79; low‐certainty evidence), placebo (MD ‐0.80, 95% CI ‐1.47 to ‐0.13; I² = 0%; 2 studies, N = 120; moderate‐certainty evidence), or salbutamol (MD ‐0.74, 95% CI ‐2.87 to 1.39; 1 study, N = 43; moderate‐certainty evidence), but not diphenhydramine (MD ‐1.83, 95% CI ‐2.88 to ‐0.78; 1 study, N = 40; low‐certainty evidence; Analysis 2.2).
2.2. Analysis.
Comparison 2 Pre‐ and postintervention comparison, Outcome 2 Severity of cough (mean reduction in severity).
Honey also reduced cough severity on Day 5 (MD ‐2.62, 95% CI ‐5.04 to ‐0.20; 1 study, N = 57; moderate‐certainty evidence) better than salbutamol (MD ‐2.08, 95% CI ‐4.21 to 0.05; 1 study, N = 43; moderate‐certainty evidence) or placebo (MD ‐1.96, 95% CI ‐3.74 to ‐0.18; 1 study, N = 45; moderate‐certainty evidence; Analysis 2.2).
Peixoto 2016 expressed results as medians and showed no difference between honey and bromelin (honey + pineapple) (moderate‐certainty evidence; Table 6).
2.3 Less bothersome cough
Children's cough was less bothersome in the honey group after one day of treatment (MD ‐2.22, 95% CI ‐3.24 to ‐1.21; I² = 0%; 3 studies, N = 317; moderate‐certainty evidence) compared with the dextromethorphan (MD ‐1.94, 95% CI ‐3.05 to ‐0.83; 1 study, N = 34; moderate‐certainty evidence), no treatment (MD ‐1.30, 95% CI ‐2.07 to ‐0.53; 1 study, N = 39; low‐certainty evidence), placebo (MD ‐1.08, 95% CI ‐2.06 to ‐0.10; I² = 0%; 2 studies, N = 120; moderate‐certainty evidence), and salbutamol groups (MD ‐1.00, 95% CI ‐4.28 to 2.28; 1 study, N = 43; moderate‐certainty evidence; Analysis 2.3).
2.3. Analysis.
Comparison 2 Pre‐ and postintervention comparison, Outcome 3 Bothersome cough (mean reduction in bothersome cough).
On Day 5, honey reduced bothersome cough to a greater extent (MD ‐2.74, 95% CI ‐5.27 to ‐0.21; 1 study, N = 57) than salbutamol (MD ‐2.47, 95% CI ‐4.73 to ‐0.21; 1 study, N = 43; moderate‐certainty evidence) or placebo (MD ‐1.85, 95% CI ‐3.56 to ‐0.14; 1 study, N = 45; moderate‐certainty evidence; Analysis 2.3).
Subgroup analysis comparing types of honey
Effect of different types of honey on cough symptoms
When we compared different types of honey in a subgroup analysis, dark honey from Kenya reduced cough frequency to a greater extent (MD ‐2.65, 95% CI ‐4.32 to ‐0.98; Waris 2014, N = 57; moderate‐certainty evidence) than natural honey from Iran (MD ‐2.16, 95% CI ‐3.40 to ‐0.92; Shadkam 2010, N = 40; low‐certainty evidence), citrus honey (MD ‐1.95, 95% CI ‐3.55 to ‐0.35; Cohen 2012, N = 75; moderate‐certainty evidence), buckwheat honey (MD ‐1.89, 95% CI ‐2.96 to ‐0.81; Paul 2007, N = 35; moderate‐certainty evidence), Labiatae honey (MD ‐1.82, 95% CI ‐3.30 to ‐0.34; Cohen 2012, N = 75; moderate‐certainty evidence), and eucalyptus honey (MD ‐1.77, 95% CI ‐3.22 to ‐0.32; Cohen 2012, N = 75; moderate‐certainty evidence; Analysis 2.1).
On treatment Day 1, dark honey from Kenya reduced children's cough severity to a greater extent (MD ‐2.62, 95% CI ‐5.04 to ‐0.20; 1 study, N = 57; moderate‐certainty evidence) than natural honey from Iran (MD ‐2.33, 95% CI ‐3.67 to ‐0.99; 1 study, N = 40; low‐certainty evidence), buckwheat honey (MD ‐1.80, 95% CI ‐2.88 to ‐0.72; 1 study, N = 35; moderate‐certainty evidence), Labiatae honey (MD ‐1.94, 95% CI ‐3.07 to ‐0.81; 1 study, N = 75; moderate‐certainty evidence), eucalyptus honey (MD ‐1.78, 95% CI ‐2.82 to ‐0.74; 1 study, N = 75; moderate‐certainty evidence), and citrus honey (MD ‐1.77, 95% CI ‐2.74 to ‐0.80; 1 study, N = 75; moderate‐certainty evidence; Analysis 2.2).
Dark honey from Kenya reduced bothersome cough to some extent (MD ‐2.74, 95% CI ‐5.27 to ‐0.21; 1 study, N = 57; moderate‐certainty evidence) more than buckwheat honey (MD ‐2.23, 95% CI ‐3.50 to ‐0.96; 1 study, N = 35; moderate‐certainty evidence), citrus honey (MD ‐2.16, 95% CI ‐4.20 to ‐0.12; 1 study, N = 75; moderate‐certainty evidence), Labiatae honey (MD ‐2.07, 95% CI ‐4.03 to ‐0.11; 1 study, N = 75; moderate‐certainty evidence), or eucalyptus honey (MD ‐2.00, 95% CI ‐3.82 to ‐0.18; 1 study, N = 75; moderate‐certainty evidence; Analysis 2.3).
Secondary outcomes
1. Improvement in quality of sleep at night for children (cough impact on sleep score)
Caregivers' Likert scores for cough impact on children's sleep were reduced to a greater extent in the honey group (MD ‐2.23, 95% CI ‐2.87 to ‐1.59; I² = 0%; 4 studies, N = 357; moderate‐certainty evidence) than in the dextromethorphan (MD ‐1.75, 95% CI ‐2.46 to ‐1.04; I² = 1%; 2 studies, N = 74; moderate‐certainty evidence), diphenhydramine (MD ‐1.64, 95% CI ‐2.58 to ‐0.70; 1 study, N = 40; low‐certainty evidence), no treatment (MD ‐1.28, 95% CI ‐1.81 to ‐0.76; I² = 60%; 2 studies, N = 79; moderate‐certainty evidence), or placebo groups (MD ‐1.03, 95% CI ‐2.05 to 0.00; I² = 0%; 2 studies, N = 120; moderate‐certainty evidence). After children received dark Kenyan honey, salbutamol, or placebo for five days, caregivers' Likert scores for cough impact on their children's sleep were reduced to a greater extent in the honey group (MD ‐2.32, 95% CI ‐3.63 to ‐1.01; 1 study, N = 57; moderate‐certainty evidence) than in the salbutamol (MD ‐2.47, 95% CI ‐3.84 to ‐1.10; 1 study, N = 43; moderate‐certainty evidence) and placebo groups (MD ‐1.68, 95% CI ‐2.63 to ‐0.73; 1 study, N = 45; moderate‐certainty evidence; Analysis 2.4).
2.4. Analysis.
Comparison 2 Pre‐ and postintervention comparison, Outcome 4 Children's sleep (mean reduction in cough impact on sleep score).
2. Improvement in quality of sleep at night for caregiver (cough impact on sleep score)
At postintervention, cough impact on parents' sleep was also improved to a greater extent by honey (measured on a 7‐point Likert scale) (MD ‐2.25, 95% CI ‐2.89 to ‐1.61; I² = 0%; 4 studies, N = 357; moderate‐certainty evidence) than by dextromethorphan (MD ‐1.97, 95% CI ‐2.77 to ‐1.17; I² = 0%; 2 studies, N = 74; moderate‐certainty evidence), diphenhydramine (MD ‐1.89, 95% CI ‐2.97 to ‐0.81; 1 study, N = 40; low‐certainty evidence), no treatment (MD ‐1.46, 95% CI ‐2.06 to ‐0.87; I² = 2%; 2 studies, N = 79; low‐certainty evidence), or placebo (MD ‐1.44, 95% CI ‐2.28 to ‐0.61; I² = 0%; 2 studies, N = 120; moderate‐certainty evidence).
On Day 5 of treatment, honey improved the quality of sleep of caregivers to a greater extent (MD ‐2.29, 95% CI ‐3.86 to ‐0.72; 1 study, N = 57; moderate‐certainty evidence) than placebo (MD ‐1.54, 95% CI ‐2.60 to ‐0.48; 1 study, N = 45; moderate‐certainty evidence) but not salbutamol (MD ‐2.33, 95% CI ‐3.91 to ‐0.75; 1 study, N = 43; moderate‐certainty evidence; Analysis 2.5).
2.5. Analysis.
Comparison 2 Pre‐ and postintervention comparison, Outcome 5 Parents' sleep (mean reduction in cough impact on sleep score).
Combined improvement score
When the scores of each intervention were combined across all categories, children in the honey group had reduced cough symptoms to a greater extent (MD ‐10.60, 95% CI ‐14.43 to ‐6.77; I² = 0%; 3 studies, N = 317; moderate‐certainty evidence) than those in the dextromethorphan (MD ‐8.39, 95% CI ‐10.95 to ‐5.84; 1 study, N = 34; low‐certainty evidence), no treatment (MD ‐6.41, 95% CI ‐8.82 to ‐3.99; 1 study, N = 39; low‐certainty evidence), or placebo groups (MD ‐7.11, 95% CI ‐10.78 to ‐3.44; I² = 0%; 2 studies, N = 132; moderate‐certainty evidence). Likewise, after five days treatment with honey, salbutamol, or placebo, honey reduced cough to a greater extent (MD ‐12.68, 95% CI ‐14.06 to ‐11.30; 1 study, N = 57; moderate‐certainty evidence) than salbutamol (MD ‐11.37, 95% CI ‐17.55 to ‐5.19; 1 study, N = 43; moderate‐certainty evidence) or placebo (MD ‐8.69, 95% CI ‐14.17 to ‐3.21; 1 study, N = 45; moderate‐certainty evidence; Analysis 2.6).
2.6. Analysis.
Comparison 2 Pre‐ and postintervention comparison, Outcome 6 Combined reduction in symptoms score.
3. Improvement in quality of life (e.g. school attendance and playing)
None of the included studies assessed the effect of honey on children's quality of life.
4. Adverse effects
Reported adverse events included mild reactions (nervousness, insomnia, and hyperactivity), gastrointestinal symptoms (stomachache, nausea, diarrhoea, and vomiting), rash, tachycardia, drowsiness, and somnolence. The difference observed in adverse events in comparisons of honey versus dextromethorphan, honey versus diphenhydramine, honey versus salbutamol, and honey versus placebo were not statistically significant. Seven children (9.3%) from the honey group compared to two (2.7%) from the dextromethorphan group experienced reactions such as nervousness, insomnia, and hyperactivity (risk ratio (RR) 2.94, 95% CI 0.74 to 11.71; I² = 0%; 2 studies, N = 149; low‐certainty evidence; Analysis 3.1). Two children (2.7%) from the honey group had gastrointestinal symptoms compared to none from the dextromethorphan group (RR 4.86, 95% CI 0.24 to 97.69; 1 study, N = 69; low‐certainty evidence; Analysis 3.1). One (1.3%) child in the honey group experienced drowsiness (RR 2.92, 95% CI 0.12 to 69.20; I² = 0%; 1 study, N = 69; low‐certainty evidence; Analysis 3.1). Three children (7.5%) experienced somnolence in the diphenhydramine group, but this result was not significantly different from the honey group (RR 0.14, 95% CI 0.01 to 2.68; 1 study, N = 80; low‐certainty evidence; Analysis 3.2). No adverse effects were reported for the no‐treatment group.
3.1. Analysis.
Comparison 3 Adverse events, Outcome 1 Honey versus dextromethorphan.
3.2. Analysis.
Comparison 3 Adverse events, Outcome 2 Honey versus diphenhydramine.
A total of 34 children (12%) in the honey group compared to 13 children (11%) from the placebo group experienced gastrointestinal symptoms (RR 1.91, 95% CI 1.12 to 3.24; I² = 0%; 2 studies, N = 402; moderate‐certainty evidence; Analysis 3.3). Similarly, more gastrointestinal symptoms probably occurred with honey than with salbutamol (RR 1.74, 95% CI 1.04 to 2.92; 1 study, N = 100; moderate‐certainty evidence).
3.3. Analysis.
Comparison 3 Adverse events, Outcome 3 Honey versus placebo.
Diarrhoea was reported in the salbutamol (N = 9, 21%), honey (N = 7, 12%), and placebo (N = 6, 13%) groups. The risk of diarrhoea was similar in the honey group compared to the placebo group (RR 0.92, 95% CI 0.33 to 2.55; 1 study, N = 102; low‐certainty evidence; Analysis 3.3). The risk of diarrhoea probably increased to a greater extent in the salbutamol group than in the honey group (RR 0.59, 95% CI 0.24 to 1.45; 1 study, N = 100; moderate‐certainty evidence; Analysis 3.4).
3.4. Analysis.
Comparison 3 Adverse events, Outcome 4 Honey versus salbutamol.
The risk of rash in the salbutamol group was probably higher than in the honey group (RR 0.19, 95% CI 0.02 to 1.63; 1 study, N = 100; moderate‐certainty evidence; Analysis 3.4). Two children in the honey group had tachycardia compared to one in the placebo group (RR 1.58, 95% CI 0.15 to 16.86; 1 study, N = 102; low‐certainty evidence; Analysis 3.3) and one in the salbutamol group (RR 1.51, 95% CI 0.14 to 16.10; 1 study, N = 100; low‐certainty evidence; Analysis 3.4).
5. Improvement in appetite
None of the included studies assessed improvement in appetite as an outcome.
6. Cost of honey alone compared with other cough syrups
None of the included studies assessed cost of treatment as an outcome.
Pair‐wise comparison of honey and dextromethorphan
There was no difference between honey and dextromethorphan in reducing cough frequency (MD ‐0.07, 95% CI ‐1.07 to 0.94; I² = 87%; 2 studies, N = 149; low‐certainty evidence), cough severity (MD ‐0.13, 95% CI ‐1.25 to 0.99; I² = 85%; 2 studies, N = 149; low‐certainty evidence), bothersome cough (MD 0.29, 95% CI ‐0.56 to 1.14; 1 study, N = 69; moderate‐certainty evidence), impact of cough on children's sleep (MD 0.03, 95% CI ‐1.12 to 1.19; I² = 84%; 2 studies, N = 149; low‐certainty evidence), and parents' sleep (MD ‐0.16, 95% CI ‐0.84 to 0.53; I² = 59%; 2 studies, N = 149; low‐certainty evidence; Analysis 1.1).
1.1. Analysis.
Comparison 1 Pair‐wise comparison, Outcome 1 Honey versus dextromethorphan.
Pair‐wise comparison of honey versus diphenhydramine
Honey may be better than diphenhydramine in reducing cough frequency (MD ‐0.57, 95% CI ‐0.90 to ‐0.24; 1 study, N = 80; low‐certainty evidence), cough severity (MD ‐0.60, 95% CI ‐0.94 to ‐0.26; 1 study, N = 80; low‐certainty evidence), cough impact on children's sleep (MD ‐0.55, 95% CI ‐0.87 to ‐0.23; 1 study, N = 80; low‐certainty evidence), and cough impact on parents' sleep (MD ‐0.48, 95% CI ‐0.76 to ‐0.20; 1 study, N = 80; low‐certainty evidence; Analysis 1.2).
1.2. Analysis.
Comparison 1 Pair‐wise comparison, Outcome 2 Honey versus diphenhydramine.
Ahmadi 2013 reported that the frequency and severity of night‐ and daytime coughing was significantly reduced by 79.4% and 84.1% in the group receiving honey, and 58.7% and 58.7% in the group receiving diphenhydramine, quote: "P < 0.02" (Table 6).
Pair‐wise comparison of honey versus no treatment
Moderate‐certainty evidence showed that the effect of honey was probably better than no treatment in reducing cough frequency (MD ‐1.05, 95% CI ‐1.48 to ‐0.62; I² = 0%; 2 studies, N = 154), cough severity (MD ‐1.03, 95% CI ‐1.59 to ‐0.47; I² = 63%; 2 studies, N = 154), cough impact on children's sleep (MD ‐1.04, 95% CI ‐1.57 to ‐0.51; I² = 7%; 2 studies, N = 154), and cough impact on parents' sleep (MD ‐0.88, 95% CI ‐1.23 to ‐0.52; I² = 26%; 2 studies, N = 154). However, honey was no different than no treatment in resolving bothersome cough (MD ‐0.93, 95% CI ‐1.98 to 0.12; 1 study, N = 74; low‐certainty evidence; Analysis 1.3).
1.3. Analysis.
Comparison 1 Pair‐wise comparison, Outcome 3 Honey versus no treatment.
Pair‐wise comparison of honey versus placebo
Moderate‐certainty evidence showed that honey probably reduces the duration of cough more than placebo (MD ‐0.72, 95% CI ‐1.31 to ‐0.13; 1 study, N = 102).
After a one‐night honey intervention, the available evidence showed that honey reduced cough frequency to a greater extent than placebo (MD ‐1.62, 95% CI ‐3.02 to ‐0.22; I² = 0%; 2 studies, N = 402; moderate‐certainty evidence). Honey also had a greater effect in reducing cough severity (MD ‐1.07, 95% CI ‐2.43 to 0.30; I² = 50%; 2 studies, N = 402; moderate‐certainty evidence) and bothersome cough (MD ‐1.40, 95% CI ‐2.82 to 0.03; I² = 6%; 2 studies, N = 402; moderate‐certainty evidence) than placebo, but the difference was not statistically significant. Caregivers reported that honey improved quality of sleep better than placebo for parents (MD ‐1.29, 95% CI ‐2.71 to 0.13; I² = 73%; 2 studies, N = 402; moderate‐certainty evidence) and their children (MD ‐1.21, 95% CI ‐2.61 to 0.19; I² = 78%; 2 studies, N = 402; moderate‐certainty evidence). The difference between intervention groups was not statistically significant (Analysis 1.4).
1.4. Analysis.
Comparison 1 Pair‐wise comparison, Outcome 4 Honey versus placebo (Day 1).
On Day 3 of honey versus placebo treatment, moderate‐certainty evidence showed that honey reduced cough frequency (MD ‐1.13, 95% CI ‐1.71 to ‐0.55; 1 study, N = 102), cough severity (MD ‐0.85, 95% CI ‐1.41 to ‐0.29; 1 study, N = 102), bothersome cough (MD ‐1.33, 95% CI ‐1.87 to ‐0.79; 1 study, N = 102), impact of cough on children's sleep (MD ‐0.93, 95% CI ‐1.42 to ‐0.44; 1 study, N = 102), and impact of cough on parents' sleep to a greater extent than placebo (MD ‐0.88, 95% CI ‐1.38 to ‐0.38; 1 study, N = 102; Analysis 1.6).
1.6. Analysis.
Comparison 1 Pair‐wise comparison, Outcome 6 Honey versus placebo (Day 3).
Honey reduced cough duration to a greater extent than placebo (MD ‐0.72, 95% CI ‐1.31 to ‐0.13; 1 study, N = 102; moderate‐certainty evidence).
On the fifth day of treatment, moderate‐certainty evidence showed there was no significant difference between honey and placebo in reducing cough frequency (MD ‐0.48, 95% CI ‐2.95 to 1.99; 1 study, N = 102), cough severity (MD ‐0.43, 95% CI ‐2.21 to 1.35; 1 study, N = 102), bothersome cough (MD ‐0.51, 95% CI ‐3.01 to 1.99; 1 study, N = 102), cough impact on children's sleep (MD ‐0.55, 95% CI ‐1.79 to 0.69; 1 study, N = 102), and cough impact on parents' sleep (MD ‐0.57, 95% CI ‐1.59 to 0.45; 1 study, N = 102; Analysis 1.8).
Pair‐wise comparison of honey versus salbutamol
After the first night of treatment, honey reduced cough frequency (MD ‐0.26, 95% CI ‐3.14 to 2.62; 1 study, N = 100; moderate‐certainty evidence), cough severity (MD ‐0.10, 95% CI ‐0.39 to 0.19; 1 study, N = 100; moderate‐certainty evidence), and bothersome cough (MD ‐0.21, 95% CI ‐0.90 to 0.48; 1 study, N = 100; moderate‐certainty evidence) more than salbutamol, but the difference was not statistically significant. However, salbutamol reduced cough impact on children's sleep (MD 0.09, 95% CI ‐0.05 to 0.23; 1 study, N = 100; moderate‐certainty evidence) and cough impact on parents' sleep (MD 0.05, 95% CI ‐0.03 to 0.13; 1 study, N = 100; moderate‐certainty evidence) more than honey. The difference was not statistically significant (Analysis 1.9).
1.9. Analysis.
Comparison 1 Pair‐wise comparison, Outcome 9 Honey versus salbutamol (Day 1).
On Day 3 of the intervention, honey reduced cough frequency (MD ‐0.69, 95% CI ‐1.13 to ‐0.25; 1 study, N = 100; moderate‐certainty evidence), cough severity (MD ‐0.34, 95% CI ‐0.64 to ‐0.04; 1 study, N = 100; moderate‐certainty evidence), and bothersome cough to a greater extent than salbutamol (MD ‐0.24, 95% CI ‐0.38 to ‐0.10; 1 study, N = 100; moderate‐certainty evidence). Salbutamol probably reduced the impact of cough on children's sleep (MD 0.31, 95% CI 0.13 to 0.49; 1 study, N = 100; moderate‐certainty evidence) and impact of cough on parents' sleep (MD 0.21, 95% CI 0.06 to 0.36; 1 study, N = 100; moderate‐certainty evidence; Analysis 1.11).
1.11. Analysis.
Comparison 1 Pair‐wise comparison, Outcome 11 Honey versus salbutamol (Day 3).
Moderate‐certainty evidence showed that honey reduced cough duration (MD ‐0.54, 95% CI ‐0.98 to ‐0.10; 1 study, N = 100), cough frequency (MD ‐0.54, 95% CI ‐1.03 to ‐0.05; 1 study, N = 100), cough severity (MD ‐0.41, 95% CI ‐0.78 to ‐0.04; 1 study, N = 100), and bothersome cough more than salbutamol on Day 5 (MD ‐0.27, 95% CI ‐0.48 to ‐0.06; 1 study, N = 100). Salbutamol reduced cough impact on children's sleep (MD 0.15, 95% CI 0.04 to 0.26; 1 study, N = 100) and parents' sleep to a greater extent than honey (MD 0.04, 95% CI 0.01 to 0.07; 1 study, N = 100; Analysis 1.13).
Pair‐wise comparison of honey versus bromelin + honey
There was no difference between the effect of honey alone and bromelin with honey on cough frequency (moderate‐certainty evidence; Table 6).
Discussion
Summary of main results
We included six small trials (899 children). Honey was given for one night only in four studies (Cohen 2012; Paul 2007; Peixoto 2016; Shadkam 2010). One study administered honey three times on one day (Ahmadi 2013), and one study administered honey three times daily for five days (Waris 2014). Giving honey for a day was better in relieving cough severity and bothersome cough when compared to no treatment, but the effect was not statistically significantly different from the use of other interventions. However, this evidence was derived from five small studies, two of which had a high risk of performance and detection bias.
Moderate‐certainty evidence showed that honey probably reduces cough duration to a greater extent than salbutamol or placebo. Honey group participants were first to get total relief of cough compared to salbutamol or placebo.
Honey probably relieves cough symptoms and improves sleep quality for both children and parents better than no treatment. Honey may resolve bothersome cough to a greater extent than no treatment, but the difference was not statistically significant. Honey probably reduces cough frequency better than placebo when given to children for a day. Honey probably reduces cough severity, bothersome cough, and impact of cough on both children's and parents' sleep to a greater extent than placebo, but the difference was not statistically significant.
The effect estimate showed that after one night of administration honey may reduce cough symptoms and improve sleep quality of children and their parents better than diphenhydramine. Honey probably had little effect or no difference compared to dextromethorphan or salbutamol for symptomatic relief of cough, resolving bothersome cough, and improving sleep quality for both children and parents.
When we compared types of honey, dark honey from Kenya probably reduced cough frequency and cough severity to a greater extent than the other types of honey. However, dark Kenyan honey was administered three times daily compared to other types of honey that were administered once at night; this may have contributed to the effect size of the African honey.
Three days of honey administration was probably more effective than one day of treatment in relieving symptomatic cough and resolving the bothersome nature of cough when compared with salbutamol or placebo. However, salbutamol probably improved sleep quality for children and parents more than honey.
There is probably little or no difference between honey alone and bromelin (pineapple enzyme extract) mixed with honey for relieving cough symptoms.
On Day 5 of administration, there was probably little or no difference between honey versus placebo or honey versus salbutamol for symptomatic relief of cough and reduction of cough impact on the sleep quality of children and their parents.
No serious adverse events were reported in any of the treatment groups. Non‐severe adverse events such as stomachache, nausea, and vomiting were probably more common in the honey groups than no‐treatment and placebo groups, but comparable with dextromethorphan, diphenhydramine, and salbutamol groups. There was probably little or no difference in numbers of events in the honey, no‐treatment, placebo, dextromethorphan, diphenhydramine, and salbutamol groups for other non‐severe adverse events such as rash and tachycardia.
Overall completeness and applicability of evidence
The available evidence shows that honey may be better than placebo and salbutamol in reducing cough duration for children with acute cough. However, as the data for this evidence were from a small study, the applicability of this evidence is uncertain.
We also found that giving honey for three days is probably more effective in relieving symptoms of cough when compared to placebo or salbutamol. However, salbutamol was more effective in reducing the impact of cough on sleep quality of children and their parents. The administration of honey beyond three days had no advantage over salbutamol or placebo in the reduction of cough severity and bothersome cough. This evidence was generated from a small study, and as such caution is required in its application.
Overall, the direction of effect was in favour of honey compared to no treatment, placebo, dextromethorphan, diphenhydramine, and salbutamol for relieving symptomatic cough and resolving bothersome cough, but it was not better than dextromethorphan, diphenhydramine, and salbutamol at improving the quality of sleep in children and their parents. Other outcomes such as improvements in appetite, school attendance, and playing were not reported. We cannot generalise on the applicability of our findings because most children in this review received treatment for one night, even though an acute cough may last for more than one week.
Waris 2014 reported that they used the darkest honey they could find; it is believed that the darker the honey, the more the antioxidant property (Cohen 2012). However, there is insufficient evidence to support this estimate of effect.
Quality of the evidence
We included six small RCTs that we assessed as at overall low risk of bias (Figure 2). We assessed two studies as at high risk of bias relating to blinding (overall, we assessed the certainty of the evidence as low to moderate certainty for outcomes measured; Table 1; Table 2; Table 3; Table 4; Table 5). This was largely due to imprecision of the effect estimate, heterogeneity, and high risk of bias of some of the studies. We rated the certainty of the evidence as moderate to low for all outcomes for the comparisons of honey to dextromethorphan, no treatment, bromelin, and placebo. However, we rated the certainty of evidence as low for honey versus diphenhydramine on symptomatic relief of cough. We assessed two included studies as at high risk of bias of performance and detection bias (Paul 2007; Shadkam 2010). We rated Paul 2007 as at high risk for performance bias because they did not blind the no‐treatment arm of their study. Shadkam 2010 did not blind participants and investigators for all treatment arms. We assessed Cohen 2012 and Waris 2014 as at low risk of bias for all domains except for attrition bias, which we judged as unclear. We rated Ahmadi 2013 as unclear risk of bias for selective reporting and other bias because results were presented as the proportion of children with reduced cough instead of the actual mean symptom scores reported by the other included studies. In addition, the scale used for measurement was not clear (a 7‐point Likert‐like scale was used for cough assessment), and the protocol was registered retrospectively after completion of study. African honey was administered thrice daily for five days compared to one night for other honey types; this may have been responsible for its higher effect on cough symptoms. Also, most studies measured all outcomes using a 7‐point Likert scale, except Peixoto 2016, which used an unvalidated 5‐point cough scale; for this reason we rated Peixoto 2016 as at unclear risk of other bias. These scales are qualitative ordinal scales; as a result, symptom scores may be subjective.
Potential biases in the review process
Due to limitations in the design and reporting of the included studies, conclusive evidence for or against the use of honey in the treatment of cough symptoms and their impact on sleep remains elusive. Data from two studies could not be meta‐analysed because of the way results were presented (Ahmadi 2013; Peixoto 2016). Peixoto 2016 also used an unvalidated cough scale, and the cough scale used by Ahmadi 2013 was unclear. We were unable to conduct sensitivity analyses to determine publication bias because there were too few studies. We screened, extracted, and reported data according to the methods in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). Most included studies were underpowered. The risk of bias for attrition was unclear in three studies because the studies only stated the proportion of children lost to follow‐up in each treatment group, but no clear information on the reason for the loss (Cohen 2012; Shadkam 2010; Waris 2014).
We did not limit electronic searches by language or publication.
Agreements and disagreements with other studies or reviews
An overview of reviews of honey for treating cough included three reviews (Nitsche 2016). Of the three reviews included in the overview, Oduwole 2014a and Oduwole 2014b are earlier versions of this review, and Smith 2014 is a Cochrane Review that assessed over‐the‐counter remedies for acute cough in community settings. The conclusions reported by Nitsche 2016 were similar to the findings of this review. We also identified a related study (Mulholland 2011), but we did not think it was relevant to our review, and moreover, the review had no included studies.
Authors' conclusions
Implications for practice.
We found that giving honey for up to three days is probably more effective in relieving cough symptoms compared to placebo or salbutamol. However, to an extent, salbutamol was more effective in relieving the impact of cough on the quality of sleep of children and their parents. The administration of honey beyond three days probably had no advantage over salbutamol or placebo in the reduction of cough severity and bothersome cough.
When given for one day, honey is probably more effective in reducing cough frequency, cough severity, and impact of cough on sleep for both children and parents than no treatment. Honey may also resolve bothersome cough to a greater extent than no treatment. Honey probably reduces cough frequency more effectively than placebo. Honey probably also reduces cough severity, resolves bothersome cough, and improves sleep quality for both children and their parents to a greater extent than placebo. Its effect on cough frequency, cough severity, and quality of sleep for children and their parents is also likely to be better than with diphenhydramine, an over‐the‐counter cough remedy. Its effect may be comparable to dextromethorphan (another over‐the‐counter drug) for reducing cough frequency, cough severity, and the impact of cough on sleep quality of children and their parents. There was probably little or no difference between honey and bromelin mixed with honey for reducing cough frequency and severity. One of the included studies assessed the effect of honey on cough duration; the available evidence suggests that honey reduces cough duration to a greater extent than placebo or salbutamol. There was no difference in the occurrence of non‐severe adverse events between honey and the various control arms.
These findings are from six small studies, two of which were at high risk of performance and detection bias with moderate‐ to low‐certainty evidence, and may not be generalisable.
Implications for research.
We advocate for more high‐quality, large randomised controlled trials evaluating the effectiveness of honey in relieving acute cough in children. Randomised controlled trials need to look at dosage, longer treatment times, and follow‐up of participants, and measure other important secondary outcomes relevant to caregivers such as cost of the intervention and quality of life of the children.
What's new
| Date | Event | Description |
|---|---|---|
| 17 December 2018 | Amended | Amendment made to Table 4. The superscripts 'moderate certainty evidence' were corrected for Day 3 and Day 5. |
History
Protocol first published: Issue 2, 2008 Review first published: Issue 1, 2010
| Date | Event | Description |
|---|---|---|
| 8 February 2018 | New citation required but conclusions have not changed | Our conclusions remain unchanged. |
| 8 February 2018 | New search has been performed | Searches updated. We included three new trials (Ahmadi 2013; Peixoto 2016; Waris 2014), and excluded three new trials (Ayazi 2017; Baker 2016; Cohen 2017). One study is awaiting classification (IRCT2014090819037N1), and two studies are ongoing (NCT03218696; UMIN000020651). |
| 4 November 2014 | New citation required and minor changes | Our conclusions remain unchanged. |
| 4 November 2014 | New search has been performed | Searches updated. We included one new trial (Cohen 2012), and excluded two new trials (Ahmed 2013a; Miceli Sopo 2014). Two studies are awaiting classification (IRCT201110247882N1; NCT01356693), and one study is ongoing (IRCT2014090819037N1). |
| 11 January 2012 | New search has been performed | Searches updated. We included one new trial (Shadkam 2010). |
| 11 January 2012 | New citation required but conclusions have not changed | Our conclusions remain unchanged. |
Acknowledgements
The review authors wish to thank Liz Dooley, Ann Jones, and David Honeyman from the Cochrane Acute Respiratory Infections Group for their contributions. We would also like to acknowledge the comments of the following referees: Matthew Thompson, Clare Jeffrey, Peter Molan, Jenny Wilkinson, David Gregory, Teresa Neeman, Mark Jones, and Lisa Baniran. We wish to thank Milad Tavakoli for translating Ahmadi 2013 from Farsi to English. We would also like to thank the authors of Paul 2007, Shadkam 2010, and Waris 2014 for their prompt responses to our requests for further information and clarification about their studies.
Appendices
Appendix 1. AMED (Ovid) search strategy
1 cough/ 2 cough*.tw. 3 1 or 2 4 honey/ 5 honey*.tw. 6 4 or 5 7 3 and 6
Appendix 2. CAB Abstracts (Thomson Reuters) search strategy
Topic=(cough*) AND Topic=(honey*)Timespan=2009‐2011. Databases=CAB Abstracts.
Appendix 3. Previous searches
For the 2014 update we searched the Cochrane Central Register of Controlled Trials (CENTRAL) (2014, Issue 10), which contains the Cochrane Acute Respiratory Infections Group's Specialised Register, MEDLINE (January 2012 to October week 4, 2014), EMBASE (January 2012 to October 2014), CINAHL (January 2012 to October 2014), Web of Science (2011 to October 2014), AMED (2011 to October 2014), LILACS (2011 to October 2014) and CAB abstracts (2011 to January 2014).
Our initial 2009 search covered CENTRAL (The Cochrane Library 2009, Issue 2), MEDLINE (1950 to April Week 2, 2009), Embase (1990 to April 2009), CINAHL (1982 to April 2009), Web of Science (2000 to April 2009), AMED (1985 April 2009) and LILACS (1982 to April 2009). The search was then updated in January 2012 to cover the period April 2009 to January 2012.
Appendix 4. CENTRAL and MEDLINE (Ovid) search strategy
1 Cough/ 2 cough*.tw 3 cough*.tw 4 Honey/ 5 honey*.tw. 6 4 or 5 7 3 and 6
Appendix 5. Embase (Elsevier) search strategy
#7. #3 AND #6 #6. #4 OR #5 #5. honey*:ab,ti #4. 'honey'/de #3. #1 OR #2 #2. cough*:ab,ti #1. 'coughing'/exp
Appendix 6. CINAHL (EBSCO) search strategy
S7 S3 and S6 S6 S4 or S5 S5 TI honey* or AB honey* S4 (MH "Honey") S3 S1 or S2 S2 TI cough* or AB cough* S1 (MH "Cough")
Appendix 7. Web of Science (Clarivate Analytics) search strategy
Topic=(cough*) AND Topic=(honey*)
Appendix 8. LILACS (BIREME) search strategy
(mh:cough OR cough* OR tos OR tosse) AND (mh:honey OR honey* OR miel OR mel) AND db:("LILACS")
Data and analyses
Comparison 1. Pair‐wise comparison.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Honey versus dextromethorphan | 2 | Mean Difference (Random, 95% CI) | Subtotals only | |
| 1.1 Frequency of cough (mean reduction in cough frequency) | 2 | 149 | Mean Difference (Random, 95% CI) | ‐0.07 [‐1.07, 0.94] |
| 1.2 Severity of cough (mean reduction in severity of cough) | 2 | 149 | Mean Difference (Random, 95% CI) | ‐0.13 [‐1.25, 0.99] |
| 1.3 Bothersome cough (mean reduction in bothersome cough) | 1 | 69 | Mean Difference (Random, 95% CI) | 0.29 [‐0.56, 1.14] |
| 1.4 Children's sleep (mean reduction in cough impact on sleep score) | 2 | 149 | Mean Difference (Random, 95% CI) | 0.03 [‐1.12, 1.19] |
| 1.5 Parents' sleep (mean reduction in cough impact on sleep score) | 2 | 149 | Mean Difference (Random, 95% CI) | ‐0.16 [‐0.84, 0.53] |
| 1.6 Combined cough score (reduction in combined cough score) | 1 | 69 | Mean Difference (Random, 95% CI) | 2.32 [‐1.24, 5.88] |
| 2 Honey versus diphenhydramine | 1 | Mean Difference (Random, 95% CI) | Subtotals only | |
| 2.1 Frequency of cough (mean reduction in cough frequency) | 1 | 80 | Mean Difference (Random, 95% CI) | ‐0.57 [‐0.90, ‐0.24] |
| 2.2 Severity of cough (mean reduction in severity of cough) | 1 | 80 | Mean Difference (Random, 95% CI) | ‐0.6 [‐0.94, ‐0.26] |
| 2.3 Children's sleep (mean reduction in cough impact on sleep score) | 1 | 80 | Mean Difference (Random, 95% CI) | ‐0.55 [‐0.87, ‐0.23] |
| 2.4 Parents' sleep (mean reduction in cough impact on sleep score) | 1 | 80 | Mean Difference (Random, 95% CI) | ‐0.48 [‐0.76, ‐0.20] |
| 3 Honey versus no treatment | 2 | Mean Difference (Random, 95% CI) | Subtotals only | |
| 3.1 Frequency of cough (mean reduction in frequency of cough) | 2 | 154 | Mean Difference (Random, 95% CI) | ‐1.05 [‐1.48, ‐0.62] |
| 3.2 Severity of cough (mean reduction in severity of cough) | 2 | 154 | Mean Difference (Random, 95% CI) | ‐1.03 [‐1.59, ‐0.47] |
| 3.3 Bothersome cough (mean reduction in bothersome cough) | 1 | 74 | Mean Difference (Random, 95% CI) | ‐0.93 [‐1.98, 0.12] |
| 3.4 Children's sleep (mean reduction in cough impact on sleep score) | 2 | 154 | Mean Difference (Random, 95% CI) | ‐1.04 [‐1.57, ‐0.51] |
| 3.5 Parents' sleep (mean reduction in cough impact on sleep score) | 2 | 154 | Mean Difference (Random, 95% CI) | ‐0.88 [‐1.23, ‐0.52] |
| 3.6 Combined reduction in symptoms score | 1 | 74 | Mean Difference (Random, 95% CI) | ‐4.31 [‐6.77, ‐1.85] |
| 4 Honey versus placebo (Day 1) | 2 | Mean Difference (Random, 95% CI) | Subtotals only | |
| 4.1 Frequency of cough (mean reduction in frequency of cough) | 2 | 402 | Mean Difference (Random, 95% CI) | ‐1.62 [‐3.02, ‐0.22] |
| 4.2 Severity of cough (mean reduction in severity of cough) | 2 | 402 | Mean Difference (Random, 95% CI) | ‐1.07 [‐2.43, 0.30] |
| 4.3 Bothersome cough (mean reduction in bothersome cough) | 2 | 402 | Mean Difference (Random, 95% CI) | ‐1.40 [‐2.82, 0.03] |
| 4.4 Children's sleep (mean reduction in cough impact on sleep score) | 2 | 402 | Mean Difference (Random, 95% CI) | ‐1.21 [‐2.61, 0.19] |
| 4.5 Parents' sleep (mean reduction in cough impact on sleep score) | 2 | 402 | Mean Difference (Random, 95% CI) | ‐1.29 [‐2.71, 0.13] |
| 5 Honey versus placebo (Day 2) | 1 | Mean Difference (Random, 95% CI) | Subtotals only | |
| 5.1 Frequency of cough (mean reduction in frequency of cough) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.71 [‐1.22, ‐0.20] |
| 5.2 Severity of cough (mean reduction in severity of cough) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.63 [‐1.36, 0.10] |
| 5.3 Bothersome cough (mean reduction in bothersome cough) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐1.11 [‐1.79, ‐0.43] |
| 5.4 Children's sleep (mean reduction in cough impact on sleep score) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.69 [‐1.43, 0.05] |
| 5.5 Parents' sleep (mean reduction in cough impact on sleep score) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.87 [‐1.59, ‐0.15] |
| 6 Honey versus placebo (Day 3) | 1 | Mean Difference (Random, 95% CI) | Subtotals only | |
| 6.1 Frequency of cough (mean reduction in frequency of cough) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐1.13 [‐1.71, ‐0.55] |
| 6.2 Severity of cough (mean reduction in severity of cough) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.85 [‐1.41, ‐0.29] |
| 6.3 Bothersome cough (mean reduction in bothersome cough) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐1.33 [‐1.87, ‐0.79] |
| 6.4 Children's sleep (mean reduction in cough impact on sleep score) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.93 [‐1.42, ‐0.44] |
| 6.5 Parents' sleep (mean reduction in cough impact on sleep score) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.88 [‐1.38, ‐0.38] |
| 7 Honey versus placebo (Day 4) | 1 | Mean Difference (Random, 95% CI) | Subtotals only | |
| 7.1 Frequency of cough (mean reduction in frequency of cough) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐1.16 [‐1.83, ‐0.49] |
| 7.2 Severity of cough (mean reduction in severity of cough) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.88 [‐1.59, ‐0.17] |
| 7.3 Bothersome cough (mean reduction in bothersome cough) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.90 [‐1.76, ‐0.04] |
| 7.4 Children's sleep (mean reduction in cough impact on sleep score) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.7 [‐1.25, ‐0.15] |
| 7.5 Parents' sleep (mean reduction in cough impact on sleep score) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.90 [‐1.51, ‐0.29] |
| 8 Honey versus placebo (Day 5) | 1 | Mean Difference (Random, 95% CI) | Subtotals only | |
| 8.1 Cough duration (mean number of days) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.72 [‐1.31, ‐0.13] |
| 8.2 Frequency of cough (mean reduction in frequency of cough) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.48 [‐2.95, 1.99] |
| 8.3 Severity of cough (mean reduction in severity of cough) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.43 [‐2.21, 1.35] |
| 8.4 Bothersome cough (mean reduction in bothersome cough) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.51 [‐3.01, 1.99] |
| 8.5 Children's sleep (mean reduction in cough impact on sleep score) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.55 [‐1.79, 0.69] |
| 8.6 Parents' sleep (mean reduction in cough impact on sleep score) | 1 | 102 | Mean Difference (Random, 95% CI) | ‐0.57 [‐1.59, 0.45] |
| 9 Honey versus salbutamol (Day 1) | 1 | Mean Difference (Random, 95% CI) | Subtotals only | |
| 9.1 Frequency of cough (mean reduction in frequency of cough) | 1 | 100 | Mean Difference (Random, 95% CI) | ‐0.26 [‐3.14, 2.62] |
| 9.2 Severity of cough (mean reduction in severity of cough) | 1 | 100 | Mean Difference (Random, 95% CI) | ‐0.1 [‐0.39, 0.19] |
| 9.3 Bothersome cough (mean reduction in bothersome cough) | 1 | 100 | Mean Difference (Random, 95% CI) | ‐0.21 [‐0.90, 0.48] |
| 9.4 Children's sleep (mean reduction in cough impact on sleep score) | 1 | 100 | Mean Difference (Random, 95% CI) | 0.09 [‐0.05, 0.23] |
| 9.5 Parents' sleep (mean reduction in cough impact on sleep score) | 1 | 100 | Mean Difference (Random, 95% CI) | 0.05 [‐0.03, 0.13] |
| 10 Honey versus salbutamol (Day 2) | 1 | Mean Difference (Random, 95% CI) | Subtotals only | |
| 10.1 Frequency of cough (mean reduction in frequency of cough) | 1 | 100 | Mean Difference (Random, 95% CI) | ‐0.67 [‐1.35, 0.01] |
| 10.2 Severity of cough (mean reduction in severity of cough) | 1 | 100 | Mean Difference (Random, 95% CI) | ‐0.42 [‐1.16, 0.32] |
| 10.3 Bothersome cough (mean reduction in bothersome cough) | 1 | 100 | Mean Difference (Random, 95% CI) | ‐0.27 [‐0.52, ‐0.02] |
| 10.4 Children's sleep (mean reduction in cough impact on sleep score) | 1 | 100 | Mean Difference (Random, 95% CI) | 0.17 [‐0.04, 0.38] |
| 10.5 Parents' sleep (mean reduction in cough impact on sleep score) | 1 | 100 | Mean Difference (Random, 95% CI) | 0.03 [‐0.00, 0.06] |
| 11 Honey versus salbutamol (Day 3) | 1 | Mean Difference (Random, 95% CI) | Subtotals only | |
| 11.1 Frequency of cough (mean reduction in frequency of cough) | 1 | 100 | Mean Difference (Random, 95% CI) | ‐0.69 [‐1.13, ‐0.25] |
| 11.2 Severity of cough (mean reduction in severity of cough) | 1 | 100 | Mean Difference (Random, 95% CI) | ‐0.34 [‐0.64, ‐0.04] |
| 11.3 Bothersome cough (mean reduction in bothersome cough) | 1 | 100 | Mean Difference (Random, 95% CI) | ‐0.24 [‐0.38, ‐0.10] |
| 11.4 Children's sleep (mean reduction in cough impact on sleep score) | 1 | 100 | Mean Difference (Random, 95% CI) | 0.31 [0.13, 0.49] |
| 11.5 Parents' sleep (mean reduction in cough impact on sleep score) | 1 | 100 | Mean Difference (Random, 95% CI) | 0.21 [0.06, 0.36] |
| 12 Honey versus salbutamol (Day 4) | 1 | Mean Difference (Random, 95% CI) | Subtotals only | |
| 12.1 Frequency of cough (mean reduction in frequency of cough) | 1 | 100 | Mean Difference (Random, 95% CI) | ‐0.61 [‐0.96, ‐0.26] |
| 12.2 Severity of cough (mean reduction in severity of cough) | 1 | 100 | Mean Difference (Random, 95% CI) | ‐0.43 [‐0.78, ‐0.08] |
| 12.3 Bothersome cough (mean reduction in bothersome cough) | 1 | 100 | Mean Difference (Random, 95% CI) | ‐0.3 [‐0.59, ‐0.01] |
| 12.4 Children's sleep (mean reduction in cough impact on sleep score) | 1 | 100 | Mean Difference (Random, 95% CI) | 0.22 [0.05, 0.39] |
| 12.5 Parents' sleep (mean reduction in cough impact on sleep score) | 1 | 100 | Mean Difference (Random, 95% CI) | 0.15 [0.04, 0.26] |
| 13 Honey versus salbutamol (Day 5) | 1 | Mean Difference (Random, 95% CI) | Subtotals only | |
| 13.1 Cough duration (mean number of days) | 1 | 100 | Mean Difference (Random, 95% CI) | ‐0.54 [‐0.98, ‐0.10] |
| 13.2 Frequency of cough (mean reduction in frequency of cough) | 1 | 100 | Mean Difference (Random, 95% CI) | ‐0.54 [‐1.03, ‐0.05] |
| 13.3 Severity of cough (mean reduction in severity of cough) | 1 | 100 | Mean Difference (Random, 95% CI) | ‐0.41 [‐0.78, ‐0.04] |
| 13.4 Bothersome cough (mean reduction in bothersome cough) | 1 | 100 | Mean Difference (Random, 95% CI) | ‐0.27 [‐0.48, ‐0.06] |
| 13.5 Children's sleep (mean reduction in cough impact on sleep score) | 1 | 100 | Mean Difference (Random, 95% CI) | 0.15 [0.04, 0.26] |
| 13.6 Parents' sleep (mean reduction in cough impact on sleep score) | 1 | 100 | Mean Difference (Random, 95% CI) | 0.04 [0.01, 0.07] |
1.5. Analysis.
Comparison 1 Pair‐wise comparison, Outcome 5 Honey versus placebo (Day 2).
1.7. Analysis.
Comparison 1 Pair‐wise comparison, Outcome 7 Honey versus placebo (Day 4).
1.10. Analysis.
Comparison 1 Pair‐wise comparison, Outcome 10 Honey versus salbutamol (Day 2).
1.12. Analysis.
Comparison 1 Pair‐wise comparison, Outcome 12 Honey versus salbutamol (Day 4).
Comparison 2. Pre‐ and postintervention comparison.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Cough frequency (mean reduction in frequency) | 4 | Mean Difference (Fixed, 95% CI) | Subtotals only | |
| 1.1 Honey | 4 | 357 | Mean Difference (Fixed, 95% CI) | ‐1.71 [‐2.28, ‐1.13] |
| 1.2 Dextromethorphan | 2 | 74 | Mean Difference (Fixed, 95% CI) | ‐1.54 [‐2.30, ‐0.78] |
| 1.3 Diphenhydramine | 1 | 40 | Mean Difference (Fixed, 95% CI) | ‐1.73 [‐2.72, ‐0.74] |
| 1.4 Placebo | 2 | 120 | Mean Difference (Fixed, 95% CI) | ‐0.99 [‐1.79, ‐0.18] |
| 1.5 Salbutamol Day 1 | 1 | 43 | Mean Difference (Fixed, 95% CI) | ‐0.52 [‐6.28, 5.24] |
| 1.6 No treatment | 2 | 79 | Mean Difference (Fixed, 95% CI) | ‐0.98 [‐1.38, ‐0.59] |
| 1.7 Buckwheat honey | 1 | 35 | Mean Difference (Fixed, 95% CI) | ‐1.89 [‐2.96, ‐0.81] |
| 1.8 Natural honey from Kafi‐Abad (Iran) | 1 | 40 | Mean Difference (Fixed, 95% CI) | ‐2.16 [‐3.40, ‐0.92] |
| 1.9 Eucalyptus honey | 1 | 75 | Mean Difference (Fixed, 95% CI) | ‐1.77 [‐3.22, ‐0.32] |
| 1.10 Labiatae honey | 1 | 75 | Mean Difference (Fixed, 95% CI) | ‐1.82 [‐3.30, ‐0.34] |
| 1.11 Citrus honey | 1 | 75 | Mean Difference (Fixed, 95% CI) | ‐1.95 [‐3.55, ‐0.35] |
| 1.12 Salbutamol Day 5 | 1 | 43 | Mean Difference (Fixed, 95% CI) | ‐2.19 [‐3.55, ‐0.83] |
| 1.13 African honey Day 5 | 1 | 57 | Mean Difference (Fixed, 95% CI) | ‐2.65 [‐4.32, ‐0.98] |
| 1.14 Placebo Day 5 | 1 | 45 | Mean Difference (Fixed, 95% CI) | ‐1.95 [‐4.42, 0.52] |
| 2 Severity of cough (mean reduction in severity) | 4 | Mean Difference (Fixed, 95% CI) | Subtotals only | |
| 2.1 Honey | 4 | 357 | Mean Difference (Fixed, 95% CI) | ‐1.65 [‐2.39, ‐0.91] |
| 2.2 Dextromethorphan | 2 | 74 | Mean Difference (Fixed, 95% CI) | ‐1.52 [‐2.24, ‐0.80] |
| 2.3 Diphenhydramine | 1 | 40 | Mean Difference (Fixed, 95% CI) | ‐1.83 [‐2.88, ‐0.78] |
| 2.4 Salbutamol Day 1 | 1 | 43 | Mean Difference (Fixed, 95% CI) | ‐0.74 [‐2.87, 1.39] |
| 2.5 No treatment | 2 | 79 | Mean Difference (Fixed, 95% CI) | ‐1.13 [‐1.54, ‐0.72] |
| 2.6 Placebo | 2 | 120 | Mean Difference (Fixed, 95% CI) | ‐0.80 [‐1.47, ‐0.13] |
| 2.7 Buckwheat honey | 1 | 35 | Mean Difference (Fixed, 95% CI) | ‐1.80 [‐2.88, ‐0.72] |
| 2.8 Natural honey from Kafi‐Abad (Iran) | 1 | 40 | Mean Difference (Fixed, 95% CI) | ‐2.33 [‐3.67, ‐0.99] |
| 2.9 Eucalyptus honey | 1 | 75 | Mean Difference (Fixed, 95% CI) | ‐1.78 [‐2.82, ‐0.74] |
| 2.10 Labiatae honey | 1 | 75 | Mean Difference (Fixed, 95% CI) | ‐1.94 [‐3.07, ‐0.81] |
| 2.11 Citrus honey | 1 | 75 | Mean Difference (Fixed, 95% CI) | ‐1.77 [‐2.74, ‐0.80] |
| 2.12 Salbutamol Day 5 | 1 | 43 | Mean Difference (Fixed, 95% CI) | ‐2.08 [‐4.21, 0.05] |
| 2.13 African honey Day 5 | 1 | 57 | Mean Difference (Fixed, 95% CI) | ‐2.62 [‐5.04, ‐0.20] |
| 2.14 Placebo Day 5 | 1 | 45 | Mean Difference (Fixed, 95% CI) | ‐1.96 [‐3.74, ‐0.18] |
| 3 Bothersome cough (mean reduction in bothersome cough) | 3 | Mean Difference (Fixed, 95% CI) | Subtotals only | |
| 3.1 Honey | 3 | 317 | Mean Difference (Fixed, 95% CI) | ‐2.22 [‐3.24, ‐1.21] |
| 3.2 Dextromethorphan | 1 | 34 | Mean Difference (Fixed, 95% CI) | ‐1.94 [‐3.05, ‐0.83] |
| 3.3 Salbutamol Day 1 | 1 | 43 | Mean Difference (Fixed, 95% CI) | ‐1.0 [‐4.28, 2.28] |
| 3.4 No treatment | 1 | 39 | Mean Difference (Fixed, 95% CI) | ‐1.30 [‐2.07, ‐0.53] |
| 3.5 Placebo | 2 | 120 | Mean Difference (Fixed, 95% CI) | ‐1.08 [‐2.06, ‐0.10] |
| 3.6 Buckwheat honey | 1 | 35 | Mean Difference (Fixed, 95% CI) | ‐2.23 [‐3.50, ‐0.96] |
| 3.7 Eucalyptus honey | 1 | 75 | Mean Difference (Fixed, 95% CI) | ‐2.0 [‐3.82, ‐0.18] |
| 3.8 Labiatae honey | 1 | 75 | Mean Difference (Fixed, 95% CI) | ‐2.07 [‐4.03, ‐0.11] |
| 3.9 Citrus honey | 1 | 75 | Mean Difference (Fixed, 95% CI) | ‐2.16 [‐4.20, ‐0.12] |
| 3.10 Salbutamol Day 5 | 1 | 43 | Mean Difference (Fixed, 95% CI) | ‐2.47 [‐4.73, ‐0.21] |
| 3.11 African honey Day 5 | 1 | 57 | Mean Difference (Fixed, 95% CI) | ‐2.74 [‐5.27, ‐0.21] |
| 3.12 Placebo Day 5 | 1 | 45 | Mean Difference (Fixed, 95% CI) | ‐1.85 [‐3.56, ‐0.14] |
| 4 Children's sleep (mean reduction in cough impact on sleep score) | 4 | Mean Difference (Random, 95% CI) | Subtotals only | |
| 4.1 Honey | 4 | 357 | Mean Difference (Random, 95% CI) | ‐2.23 [‐2.87, ‐1.59] |
| 4.2 Dextromethorphan | 2 | 74 | Mean Difference (Random, 95% CI) | ‐1.75 [‐2.46, ‐1.04] |
| 4.3 Diphenhydramine | 1 | 40 | Mean Difference (Random, 95% CI) | ‐1.64 [‐2.58, ‐0.70] |
| 4.4 No treatment | 2 | 79 | Mean Difference (Random, 95% CI) | ‐1.28 [‐1.81, ‐0.76] |
| 4.5 Placebo | 2 | 120 | Mean Difference (Random, 95% CI) | ‐1.03 [‐2.05, 0.00] |
| 4.6 Salbutamol Day 5 | 1 | 43 | Mean Difference (Random, 95% CI) | ‐2.47 [‐3.84, ‐1.10] |
| 4.7 African honey Day 5 | 1 | 57 | Mean Difference (Random, 95% CI) | ‐2.32 [‐3.63, ‐1.01] |
| 4.8 Placebo Day 5 | 1 | 45 | Mean Difference (Random, 95% CI) | ‐1.68 [‐2.63, ‐0.73] |
| 5 Parents' sleep (mean reduction in cough impact on sleep score) | 4 | Mean Difference (Fixed, 95% CI) | Subtotals only | |
| 5.1 Honey | 4 | 357 | Mean Difference (Fixed, 95% CI) | ‐2.25 [‐2.89, ‐1.61] |
| 5.2 Dextromethorphan | 2 | 74 | Mean Difference (Fixed, 95% CI) | ‐1.97 [‐2.77, ‐1.17] |
| 5.3 Diphenhydramine | 1 | 40 | Mean Difference (Fixed, 95% CI) | ‐1.89 [‐2.97, ‐0.81] |
| 5.4 No treatment | 2 | 79 | Mean Difference (Fixed, 95% CI) | ‐1.46 [‐2.06, ‐0.87] |
| 5.5 Placebo | 2 | 120 | Mean Difference (Fixed, 95% CI) | ‐1.44 [‐2.28, ‐0.61] |
| 5.6 Salbutamol Day 5 | 1 | 43 | Mean Difference (Fixed, 95% CI) | ‐2.33 [‐3.91, ‐0.75] |
| 5.7 African honey Day 5 | 1 | 57 | Mean Difference (Fixed, 95% CI) | ‐2.29 [‐3.86, ‐0.72] |
| 5.8 Placebo Day 5 | 1 | 45 | Mean Difference (Fixed, 95% CI) | ‐1.54 [‐2.60, ‐0.48] |
| 6 Combined reduction in symptoms score | 3 | Mean Difference (Fixed, 95% CI) | Subtotals only | |
| 6.1 Honey | 3 | 317 | Mean Difference (Fixed, 95% CI) | ‐10.60 [‐14.43, ‐6.77] |
| 6.2 Dextromethorphan | 1 | 34 | Mean Difference (Fixed, 95% CI) | ‐8.39 [‐10.95, ‐5.84] |
| 6.3 No treatment | 1 | 39 | Mean Difference (Fixed, 95% CI) | ‐6.41 [‐8.82, ‐3.99] |
| 6.4 Placebo | 2 | 132 | Mean Difference (Fixed, 95% CI) | ‐7.11 [‐10.78, ‐3.44] |
| 6.5 Honey Day 5 | 1 | 57 | Mean Difference (Fixed, 95% CI) | ‐12.68 [‐14.06, ‐11.30] |
| 6.6 Placebo Day 5 | 1 | 45 | Mean Difference (Fixed, 95% CI) | ‐8.69 [‐14.17, ‐3.21] |
| 6.7 Salbutamol Day 5 | 1 | 43 | Mean Difference (Fixed, 95% CI) | ‐11.37 [‐17.55, ‐5.19] |
Comparison 3. Adverse events.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Honey versus dextromethorphan | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 Nervousness, insomnia, hyperactivity | 2 | 149 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.94 [0.74, 11.71] |
| 1.2 Stomachache, nausea, and vomiting | 1 | 69 | Risk Ratio (M‐H, Fixed, 95% CI) | 4.86 [0.24, 97.69] |
| 1.3 Drowsiness | 1 | 69 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.92 [0.12, 69.20] |
| 2 Honey versus diphenhydramine | 1 | 80 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.14 [0.01, 2.68] |
| 2.1 Somnolence | 1 | 80 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.14 [0.01, 2.68] |
| 3 Honey versus placebo | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3.1 Stomachache, nausea, and vomiting | 2 | 402 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.91 [1.12, 3.24] |
| 3.2 Diarrhoea | 1 | 102 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.92 [0.33, 2.55] |
| 3.3 Tachycardia | 1 | 102 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.58 [0.15, 16.86] |
| 4 Honey versus salbutamol | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 4.1 Stomachache, nausea, and vomiting | 1 | 100 | Risk Ratio (M‐H, Random, 95% CI) | 1.74 [1.04, 2.92] |
| 4.2 Rash | 1 | 100 | Risk Ratio (M‐H, Random, 95% CI) | 0.19 [0.02, 1.63] |
| 4.3 Tachycardia | 1 | 100 | Risk Ratio (M‐H, Random, 95% CI) | 1.51 [0.14, 16.10] |
| 4.4 Diarrhoea | 1 | 100 | Risk Ratio (M‐H, Random, 95% CI) | 0.59 [0.24, 1.45] |
| 5 Honey versus no treatment | 2 | 302 | Odds Ratio (M‐H, Fixed, 95% CI) | 6.99 [1.55, 31.58] |
| 5.1 Nervousness, insomnia, hyperactivity | 2 | 154 | Odds Ratio (M‐H, Fixed, 95% CI) | 9.40 [1.16, 76.20] |
| 5.2 Stomachache, nausea, and vomiting | 1 | 74 | Odds Ratio (M‐H, Fixed, 95% CI) | 5.90 [0.27, 127.14] |
| 5.3 Drowsiness | 1 | 74 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.43 [0.14, 87.09] |
3.5. Analysis.
Comparison 3 Adverse events, Outcome 5 Honey versus no treatment.
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Ahmadi 2013.
| Methods | Study design: RCT Study duration: 2010 to November 2012 |
|
| Participants |
Exclusion criteria Onset of otitis or sinusitis symptoms; onset of symptoms of lower respiratory tract involvement; adding a bacterial infection (purulent nasal discharge, high fever, difficulty breathing, periorbital oedema, facial pain); not using recommended treatments; adding other drugs to recommended treatment; conflicting reports of the carers of the participants |
|
| Interventions |
Treatment group
Control group
Honey was given in the same volume, frequency, and duration of use as diphenhydramine. |
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Not described but likely done. Randomisation was done by the hospital pharmacist who was not involved in the study. |
| Allocation concealment (selection bias) | Low risk | Not described but probably done. Quote: "The classification of patients was done by the hospital pharmacist" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Honey was placed in glasses similar to those belonging to diphenhydramine and with a similar concentration, mixed with distilled lukewarm water. The honey and diphenhydramine mixtures were prepared by the pharmacist, who was not part of the study. The paediatricians and parents were unaware of the nature of the treatment each child received. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "the treating doctor and the mother were unaware of the nature of the medication (honey or diphenhydramine)"; "In order to prevent the confounding factor of mother’s anxiety or her personal situation, her reports were only accepted if they were corroborated by the reports of a third person close to the child" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All children randomised to treatment arms completed the 2‐day study. |
| Selective reporting (reporting bias) | Low risk | Both outcomes listed in the methods section were reported. |
| Other bias | Unclear risk | Results were presented as the proportion of children with reduced symptom cough instead of the actual mean symptom scores. Furthermore, the scale used for measurement was not clear (a 7‐point Likert‐like scale was used for cough assessment). The protocol was registered retrospectively after completion of the study. |
Cohen 2012.
| Methods | Study design: RCT Study duration: January 2009 to December 2009 |
|
| Participants |
Exclusion criteria Quote: "children were excluded if they had signs or symptoms of asthma, pneumonia, laryngotracheobronchitis, sinusitis, and/or allergic rhinitis. Children were also excluded if they had used any cough or cold medication or honey on the night before entering the study" |
|
| Interventions |
Treatment group
Control group
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was in blocks of 4. |
| Allocation concealment (selection bias) | Low risk | The envelopes containing the codes for the study preparations were stored at the office of the Ministry of Agriculture, Extension service, Beekeeping Department and were not opened until after the statistical analysis was completed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | The 3 honeys and the placebo were prepared by someone not involved in the study; interventions were packed in small plastic containers marked A, B, C, and D and distributed to the paediatric community clinics. Silan date extract was used as a placebo because its structure, brown colour, and taste are similar to that of honey. The parents, physicians, and investigators did not know the content of the preparation that was dispensed. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | The parents, physicians, and investigators did not know the content of the preparation that was dispensed. Interventions were packed in small plastic containers marked A, B, C, and D and distributed to the paediatric community clinics. Silan date extract was used as a placebo because its structure, brown colour, and taste are similar to that of honey. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 14 (19%), 13 (18%), 2 (3%), and 4 (5%) children were lost to follow‐up in the eucalyptus honey, citrus honey, Labiatae honey, and placebo groups, respectively. The authors stated that the reasons for loss to follow‐up were unknown. However, attrition was significantly high in the eucalyptus honey and citrus honey groups. It is unclear if the reasons for attrition in the treatment groups were related to the study or not and if the reasons were similar. |
| Selective reporting (reporting bias) | Low risk | All outcomes listed in the protocol were reported. |
| Other bias | Low risk | Not detected |
Paul 2007.
| Methods | RCT | |
| Participants |
Exclusion criteria Quote: "patients were excluded if they had signs or symptoms of a more treatable disease (e.g., asthma, pneumonia, laryngotracheobronchitis, sinusitis, allergic rhinitis). They were also ineligible when they had a history of reactive airways disease, asthma, or chronic lung disease or were using a drug known to inhibit the metabolism of dextromethorphan, such as selective serotonin reuptake inhibitors. Subjects were also excluded if on the prior evening they had taken a medication that included an antihistamine or dextromethorphan hydrobromide within 6 hours of bedtime or dextromethorphan polistirex within 12 hours of bedtime on the evening prior to or on the day of enrolment" (p. 1141) |
|
| Interventions |
Treatment group
Control group
Parents were instructed that their child’s treatment could be given with a non‐caffeinated beverage and should be administered within 30 minutes of the child going to sleep. Intervention and control were in a 10‐millilitre opaque syringe and kept in brown paper bags. |
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Not described but probably done. Quote: "The randomisation sequence was constructed by a statistician not affiliated with the study and was then used by the study coordinators to assign treatment group" |
| Allocation concealment (selection bias) | Low risk | Not described but probably done. Treatment allocation was concealed in 10‐millilitre opaque syringe and kept in brown paper bags. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | The syringes used for all 3 treatment groups were opaque and placed in a brown paper bag to conceal the treatments from the investigators. The no‐treatment group was not blinded to their treatment, but the honey and dextromethorphan arms were blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Although all participants were given syringes in brown paper bags, the no‐treatment group had empty syringes, which could influence the assessment of the outcome. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2 children from the no‐treatment group were lost to follow‐up; 1 was withdrawn from the dextromethorphan group because the participant did not take the treatment. |
| Selective reporting (reporting bias) | Low risk | All outcomes were adequately reported. |
| Other bias | Low risk | It is unclear whether any of the no‐treatment group revealed to any of the assessors during phone conversations that they were given no treatment. Children lost to follow‐up or withdrawn were not included in the final analysis. |
Peixoto 2016.
| Methods | RCT | |
| Participants |
Exclusion criteria Children with history of obstructive pulmonary disease, cystic fibrosis, neuropathies, heart disease, diabetes, or identifiable primary or secondary immunodeficiencies |
|
| Interventions |
Treatment group
Control group
Quote: "the quality of the honey was certified in both groups and approved by the regulatory agencies and the National Health Surveillance Agency (Anvisa) for sale; the honey had been recently produced and underwent strict bacteriological control" |
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was carried out according to a table generated in Microsoft Excel. |
| Allocation concealment (selection bias) | Low risk | Not described but very likely. Treatments were labelled A and B. Quote: "Neither the investigator nor the patient, nor the family knew which product was used"; "The treatment groups were revealed only after the analysis of the study results" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: "neither the investigator nor the patient, nor the family knew which product was used. The treatment groups were revealed only after the analysis of the study results" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "neither the investigator nor the patient, nor the family knew which product was used. The treatment groups were revealed only after the analysis of the study results" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants randomised were included in the final analysis. |
| Selective reporting (reporting bias) | Low risk | All outcomes listed in the study protocol and methods section were reported. |
| Other bias | Unclear risk | Used an unvalidated 5‐point cough scale that differed from the cough scale used by the other included studies |
Shadkam 2010.
| Methods | RCT | |
| Participants |
Exclusion criteria "asthma, pneumonia, laryngotracheobronchitis, sinusitis, allergic rhinitis, chronic lung disease, congenital heart disease, malignancy, and diabetes were not included in the study. antihistamine, diphenhydramine, or dextromethorphan 4 hours before sleep or had consumed cytochrome P450 inhibitors simultaneously (i.e. serotonin‐reabsorption selective inhibitors) were also excluded from the study. Parents were also excluded if they were using a drug and herbal that had an effect on sleeping, such as sedatives" |
|
| Interventions |
Treatment group
Control group
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomisation was by random numbers table. |
| Allocation concealment (selection bias) | Unclear risk | It was not clear whether treatment allocation was concealed. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Neither the investigators nor caregivers were blinded to treatments given, which could greatly influence the assessment of outcome. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Neither the investigators nor caregivers were blinded to treatments given, which could greatly influence the assessment of outcome. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 7 participants from the honey group, 4 from the dextromethorphan group, 6 from the diphenhydramine group, and 4 from the no‐treatment group were either lost to follow‐up or withdrawn for violating the protocol. Attrition was high for the honey and diphenhydramine groups. Participants were excluded from analysis for not visiting the physician as scheduled or using the drugs inappropriately. The proportion of children who did not visit physician as scheduled or violated protocol per group was unclear. |
| Selective reporting (reporting bias) | Low risk | All outcomes listed in the protocol were reported. |
| Other bias | Unclear risk | Some of the questions put to mothers were answered by the paediatrician because the questions were ambiguous, which could also have influenced the assessment of outcomes. Since mothers were filling in the questionnaire in the presence of the physician, it is unclear if this could have influenced the assessment of outcomes (p. 788) |
Waris 2014.
| Methods | RCT | |
| Participants |
Exclusion criteria Prior use (48 hours) of any cough mixture, study agents, oral antihistamines, nasal decongestants, steroids, or antibiotics. Other exclusions were any past history of atopy, asthma, or any chronic lung disease as well as hospitalisation for lower respiratory tract infection in the past 6 months. |
|
| Interventions |
Treatment group
Control group
|
|
| Outcomes |
|
|
| Notes |
|
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Dispensing study drugs was undertaken following a random order previously generated by a statistician not involved in care of study participants. |
| Allocation concealment (selection bias) | Low risk | Not described, but risk of bias unlikely. All 3 study drugs were prepared, bottled, packaged, and labelled as Study Drug A, B, and C by Universal Corporation Ltd, who also held the code until after statistical analysis was completed. |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | All 3 study drugs were prepared, bottled, packaged, and labelled as Study Drug A, B, and C by Universal Corporation Ltd, who also held the code until after statistical analysis was completed. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | All 3 study drugs were prepared, bottled, packaged, and labelled as Study Drug A, B, and C by Universal Corporation Ltd, who also held the code until after statistical analysis was completed. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 13%, 7%, and 5% of children in the placebo, honey, and salbutamol groups, respectively, were lost to follow‐up or were in violation of study protocol. It is unclear if the reasons for not completing the study were the same across study groups. It is possible that more participants in the placebo group left because their condition worsened. |
| Selective reporting (reporting bias) | Low risk | Not detected |
| Other bias | Low risk | Unlikely |
ITT: intention‐to‐treat; OTC: over‐the‐counter; RCT: randomised controlled trial; SD: standard deviation; URTI: upper respiratory tract infection
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Ahmed 2013a | Not an RCT; this was a feasibility study of honey for the treatment of cough in children |
| Ayazi 2017 | Quasi‐RCT |
| Baker 2016 | Not an RCT; commentary on a previous version of this review (Oduwole 2014a) |
| Cohen 2017 | Wrong intervention: compared polysaccharide‐resin‐honey to carbocysteine syrup. The study examined honey‐based cough syrup (polysaccharide‐resin‐honey) versus a non‐honey‐based cough syrup (carbocysteine syrup). We would have included this study if the comparisons had been polysaccharide‐resin‐honey versus honey alone/polysaccharide‐resin alone or carbocysteine syrup + honey versus carbocysteine syrup alone. |
| Gilbert 2008 | Not an RCT |
| Miceli Sopo 2014 | Wrong intervention: compared honey and milk versus dextromethorphan and honey and milk versus levodropropizine |
| Warren 2007 | Not an RCT |
RCT: randomised controlled trial
Characteristics of studies awaiting assessment [ordered by year of study]
IRCT2014090819037N1.
| Methods | Randomised clinical trial |
| Participants | Children aged 2 to 12 years |
| Interventions | 2 types of honey versus diphenhydramine |
| Outcomes | Cough frequency, bothersome nature of cough, and severity |
| Notes | Completed |
Characteristics of ongoing studies [author‐defined order]
NCT03218696.
| Trial name or title | Comparison of a protective cough syrup against placebo on night cough in children 1 to 5 years coughing since 1 to 2 days due to common cold |
| Methods | Randomised controlled trial |
| Participants | Children aged 1 to 5 years (i.e. 1 day before the 6th birthday, males and females) Inclusion criteria: cough attributed to infection of the upper respiratory tract present in the child for not more than 2 days |
| Interventions | Cough syrup containing specific plant extracts (Poliflav MA) and honey versus placebo |
| Outcomes | Primary
Secondary
(Time frame: First and only night of treatment) |
| Starting date | September 2017 |
| Contact information | Prof Herman A Cohen Email: hermanc@clalit.org.il Affiliation: Clalit Health Services |
| Notes | This study is not yet open for participant recruitment (November 2017). |
UMIN000020651.
| Trial name or title | Effectiveness of honey and expectorant for nocturnal cough in children with acute upper respiratory infection: a prospective interventional study |
| Methods | Parallel randomised |
| Participants | Children aged 2 to 16 years Inclusion criteria:
|
| Interventions | Honey (5 g for those age 2 to 5 years, 10 g for those aged 6 years and above) orally before bedtime for a week versus carbocysteine (30 mg/kg/day) and ambroxol (0.9 mg/kg/day) orally for a week |
| Outcomes | Primary outcome: change in frequency of nocturnal cough on the next day when honey or expectorant had been given prior to bedtime compared to that on the first day of presentation when no medication had been given Secondary outcomes: Change in severity of nocturnal cough, bothersome cough, appetite, and quality of sleep at night on the next day when honey or expectorant had been given prior to bedtime compared to that on the first day of presentation when no medication had been given. Improvement of nocturnal cough 1 week after honey or expectorant had been given prior to bedtime compared to that on the first day of presentation when no medication had been given |
| Starting date | 25 January 2016 |
| Contact information | Name: Kazushi Agata; Shun Kishibe Address: 1163 Tatemachi, Hachioji, Tokyo, Japan; 2‐8‐29 Musashidai, Fuchu‐shi, Tokyo, Japan Email: tokyoseki2016@gmail.com; jemstone625@gmail.com Affiliation: Tokyo Medical University Hachioji Medical Center Pediatrics; Tokyo Metropolitan Children's Medical Center Pediatric Emergency Medicine |
| Notes |
Differences between protocol and review
An inclusion criterion in our protocol was the inclusion of children aged from two to 18 years because of safety concerns for infants less than two years (Oduwole 2008). However, we included participants aged from 12 months because most included studies enrolled children aged from 12 months and over. Studies have reported that only infants aged less than 12 months are at risk when given honey due to poor immunity against Clostridium botulinum (Küplülü 2006), thus our safety concern was no longer valid. Including children aged less than two years did not change the conclusions of subsequent review updates (Oduwole 2012; Oduwole 2014a), from the first publication (Oduwole 2010).
We were unable to assess the effect of honey on children's quality of life, improvement in appetite, and cost of honey alone compared with other cough syrups because none of the included studies reported these outcomes.
Contributions of authors
Dr Olabisi Oduwole (OO) prepared the main text of this update and wrote the methods section of the update based on a template developed by the Cochrane Acute Respiratory Infections Group. OO and Dr Ekong Udoh (EU) selected studies and extracted data. Prof Martin Meremikwu (MM), OO, Prof Angela Oyo‐Ita (AO), and EU revised the text. All review authors contributed to this update and read and agreed upon the final version.
Declarations of interest
Olabisi Oduwole: none known. Ekong E Udoh: none known. Angela Oyo‐Ita: none known. Martin M Meremikwu: none known.
Edited (no change to conclusions)
References
References to studies included in this review
Ahmadi 2013 {published data only}
- Ahmadi M, Moosavi SM, Zakeri S. Comparison of the effect of honey and diphenhydramine on cough alleviation in 2‐5 year‐old children with viral upper respiratory tract infection. Journal of Gorgan University of Medical Science 2013;15(2):8‐13. [Google Scholar]
Cohen 2012 {published data only}
- Cohen HE, Rozen J, Kristal H, Laks Y, Berkovitch M, Uziel Y, et al. Effect of honey on nocturnal cough and sleep quality: a double‐blind, randomised, placebo‐controlled study. Pediatrics 2012;130(3):465‐71. [DOI: 10.1542/peds.2011-3075] [DOI] [PubMed] [Google Scholar]
Paul 2007 {published and unpublished data}
- Paul IM, Beiler J, McMonagle A, Shaffer ML, Duda L, Berlin CM Jr. Effect of honey, dextromethorphan, and no treatment on nocturnal cough and sleep quality for coughing children and their parents. Archives of Pediatrics and Adolescent Medicine 2007;161(12):1140‐6. [DOI] [PubMed] [Google Scholar]
Peixoto 2016 {published data only}
- Peixoto DM, Rizzo JA, Schor D, Silva AR, Cavalcanti de Oliveira D, Solé D, et al. Use of honey associated with Ananas comosus (Bromelin) in the treatment of acute irritative cough [Uso do mel de abelha associado ao Ananas comosus (Bromelin) no tratamentoda tosse irritativa aguda]. Revista Paulista de Pediatria 2016;34(4):412‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Shadkam 2010 {published data only}
- Shadkam MN, Mozaffari‐Khosravi H, Mozayan MR. A comparison of the effect of honey, dextromethorphan, and diphenhydramine on nightly cough and sleep quality in children and their parents. Journal of Alternative and Complementary Medicine (New York, NY) 2010;16(7):787‐93. [DOI: 10.1089/acm.2009.0311] [DOI] [PubMed] [Google Scholar]
Waris 2014 {published data only}
- Waris A, Macharia WM, Njeru EK, Essajee F. Randomised double blind study to compare effectiveness of honey, salbutamol and placebo in treatment of cough in children with common cold. East African Medical Journal 2014;91(2):50‐6. [PubMed] [Google Scholar]
References to studies excluded from this review
Ahmed 2013a {published data only}
- Ahmed N, Sutcliffe A, Tipper C. Feasibility study: honey for treatment of cough in children. Pediatric Reports 2013;5(e8):31‐4. [DOI: 10.4081/pr.2013.e8] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ayazi 2017 {published data only}
- Ayazi P, Mahyar A, Yousef‐Zanjani M, Allami A, Esmailzadehha N, Beyhaghi T. Comparison of the effect of two kinds of Iranian honey and diphenhydramine on nocturnal cough and the sleep quality in coughing children and their parents. PLoS ONE 2017;12(1):e0170277. [DOI: 10.1371/journal.pone.0170277] [DOI] [PMC free article] [PubMed] [Google Scholar]
Baker 2016 {published data only}
- Baker SJ. Honey for acute cough in children. Paediatrics and Child Health 2016;21(4):199‐200. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cohen 2017 {published data only}
- Cohen HA, Hoshen M, Gur S, Bahir A, Laks Y, Blau H. Efficacy and tolerability of a polysaccharide‐resin‐honey based cough syrup as compared to carbocysteine syrup for children with colds: a randomized, single‐blinded, multicenter study. World Journal of Pediatrics 2017;13(1):27‐33. [DOI: 10.1007/s12519-016-0048-4] [DOI] [PubMed] [Google Scholar]
Gilbert 2008 {published data only}
- Gilbert G. Single dose of honey effective for cough in kids. Journal of the National Medical Association 2008;100(4):459. [Google Scholar]
Miceli Sopo 2014 {published data only}
- Miceli Sopo S, Greco M, Monaco S, Varrasi G, Lorenzo G, Simeone G, Milk Honey Study Group. Effect of multiple honey doses on non‐specific acute cough in children. An open randomised study and literature review. Allergologia et Immunopathologia 2014;43(5):449‐55. [DOI] [PubMed] [Google Scholar]
Warren 2007 {published data only}
- Warren MD, Pont SJ, Barkin SL, Callahan ST, Caples TL, Carroll KN, et al. The effect of honey on nocturnal cough and sleep quality for children and their parents. Archives of Pediatrics and Adolescent Medicine 2007;161(12):1149‐53. [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
IRCT2014090819037N1 {published data only}
- IRCT2014090819037N1. Comparison of the effect of two kinds of Iranian honey and diphenhydramine on nocturnal cough and sleep quality in coughing children and their parents. apps.who.int/trialsearch/Trial2.aspx?TrialID=IRCT2014090819037N1 (first received 23 September 2013).
References to ongoing studies
NCT03218696 {unpublished data only}
- NCT03218696. Comparison of a protective cough syrup against placebo on night cough in children 1‐5 years coughing since 1‐2 days due to common cold. clinicaltrials.gov/ct2/show/NCT03218696 (first received 14 July 2017).
UMIN000020651 {unpublished data only}
- UMIN000020651. Effectiveness of honey and expectorant for nocturnal cough in children with acute upper respiratory infection: a prospective interventional study. rctportal.niph.go.jp/en/detail?trial_id=UMIN000020651 (first received 25 January 2016).
Additional references
Abramson 1999 [Computer program]
- Abramson JH, Gahlinger PM. Computer Programs for Epidemiologists: PEPI version 3. Llanidloes: Brixton Books, 1999.
Adeleye 2003
- Adeleye IA, Opiah L. Antimicrobial activities of local cough mixtures on upper respiratory tract bacterial pathogens. West Indian Medical Journal 2003;52(3):188‐90. [PubMed] [Google Scholar]
Agbaje 2006
- Agbaje EO, Ogunsanya T, Aiwerioba OR. Conventional use of honey as antibacterial agent. Annals of African Medicine 2006;5(2):78‐81. [Google Scholar]
Ahmed 2013b
- Ahmed M, Djebli N, Aissat S, Khiati B, Meslem A, Bacha S. In vitro activity of natural honey alone and in combination with curcuma starch against Rhodotorula mucilaginosa in correlation with bioactive compounds and diastase activity. Asian Pacific Journal of Tropical Biomedicine 2013;3(10):816‐21. [DOI] [PMC free article] [PubMed] [Google Scholar]
Atkins 2004
- Atkins D, Best D, Briss PA, Eccles M, Falck‐Ytter Y, Flottorp S, et al. GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ 2004;328(7454):1490. [DOI] [PMC free article] [PubMed] [Google Scholar]
Banderali 1995
- Banderali G, Riva E, Fiocchi A, Cordaro CI, Giovannini M. Efficacy and tolerability of levodropropizine and dropropizine in children with non‐productive cough. Journal of International Medical Research 1995;23(3):175‐83. [DOI] [PubMed] [Google Scholar]
Braman 2006
- Braman SS. Postinfectious cough: ACCP evidence‐based clinical guidelines. Chest 2006;129(Suppl 1):138‐46. [DOI] [PubMed] [Google Scholar]
Butler 2005
- Butler CC, Hood K, Kinnersley P, Robling M, Prout H, Houston H. Predicting the clinical course of suspected acute viral upper respiratory tract infection in children. Family Practice 2005;22(1):92‐5. [DOI] [PubMed] [Google Scholar]
CDC 2007
- Centers for Disease Control and Prevention. Infant death associated with cough and cold medications ‐ two states, 2005. MMWR. Morbidity and Mortality Weekly Report 2007;56(1):1‐4. [PubMed] [Google Scholar]
Chang 2005
- Chang AB. Cough: are children really different to adults?. Cough 2005;1:7. [DOI: 10.1186/1745-9974-1-7] [DOI] [PMC free article] [PubMed] [Google Scholar]
Chang 2014
- Chang CC, Cheng AC, Chang AB. Over‐the‐counter (OTC) medications to reduce cough as an adjunct to antibiotics for acute pneumonia in children and adults. Cochrane Database of Systematic Reviews 2014, Issue 3. [DOI: 10.1002/14651858.CD006088.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Covidence [Computer program]
- Veritas Health Innovation. Covidence. Version accessed prior to 16 August 2017. Melbourne, Australia: Veritas Health Innovation.
Cuestas 2017
- Cuestas G, Rodríguez V, Doormann F, Bellia Munzón P, Bellia Munzón G. Foreign body in the esophagus as a cause of respiratory symptoms in children. Clinical cases [Cuerpo extraño en el esófago como causa de síntomas respiratorios en el niño. Casos clínicos]. Archivos Argentinos de Pediatria 2017;115(2):e126‐30. [DOI: 10.5546/aap.2017.e126] [DOI] [PubMed] [Google Scholar]
Derebery 2013
- Derebery MJ, Dicpinigaitis PV. New horizons: current and potential future self‐treatments for acute upper respiratory tract condition. Postgraduate Medicine 2013;125(1):82‐96. [DOI: 10.3810/pgm.2013.01.2605] [DOI] [PubMed] [Google Scholar]
Dicpinigaitis 2011
- Dicpinigaitis PV. Cough: an unmet clinical need. British Journal of Pharmacology 2011;163(1):116‐24. [DOI: 10.1111/j.1476-5381.2010.01198.x] [DOI] [PMC free article] [PubMed] [Google Scholar]
El‐Gindy 2005
- El‐Gindy A, Emara S, Mesbah MK, Hadad GM. Liquid chromatography and chemometric‐assisted spectrophotometric methods for the analysis of two multicomponent mixtures containing cough suppressant drugs. Journal of AOAC International 2005;88(4):1069‐80. [PubMed] [Google Scholar]
Freestone 1997
- Freestone C, Eccles R. Assessment of the antitussive efficacy of codeine in cough associated with common cold. Journal of Pharmacy and Pharmacology 1997;49(10):1045‐9. [DOI] [PubMed] [Google Scholar]
French 2002
- French CT, Irwin RS, Fletcher KE, Adam TM. Evaluation of a cough‐specific quality‐of‐life‐questionnaire. Chest 2002;121(4):1123‐31. [DOI] [PubMed] [Google Scholar]
Golob 2005
- Golob T, Dobersek U, Kump P, Necemer M. Determination of trace and minor elements in Slovenian honey by total reflection x‐ray fluorescence spectroscopy. Food Chemistry 2005;91(4):593‐600. [Google Scholar]
GRADEpro GDT 2015 [Computer program]
- GRADE Working Group, McMaster University. GRADEpro GDT. Version accessed prior to 16 August 2017. Hamilton (ON): GRADE Working Group, McMaster University, 2015.
Gunn 2001
- Gunn VL, Taha SH, Liebelt EL, Serwint JR. Toxicity of over‐the‐counter cough and cold medications. Pediatrics 2001;108(3):e52. [DOI] [PubMed] [Google Scholar]
Hay 2003
- Hay AD, Wilson A, Fahey T, Peters TJ. The duration of acute cough in pre‐school children presenting to primary care: a prospective cohort study. Family Practice 2003;20(6):696‐705. [DOI] [PubMed] [Google Scholar]
Hermosin 2003
- Hermosin I, Chicon RM, Cabezudo MD. Free amino acid composition and botanical origin of honey. Food Chemistry 2003;83(2):263‐8. [Google Scholar]
Hernández 2005
- Hernández OM, Fraga JMG, Jiménez AI, Jiménez F, Arias JJ. Characterization of honey from the Canary Islands: determination of the mineral content by atomic absorption spectrophotometry. Food Chemistry 2005;93(3):449‐58. [Google Scholar]
Higgins 2011
- Higgins JP, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Irish 2006
- Irish J, Carter DA, Shokohi T, Blair SE. Honey has an antifungal effect against Candida species. Medical Mycological 2006;44(3):289–91. [DOI: 10.1080/13693780500417037] [DOI] [PubMed] [Google Scholar]
Katrina 2014
- Katrina B, Calvin S. Antibacterial compounds of Canadian honeys target bacterial cell wall inducing phenotype changes, growth inhibition and cell lysis that resemble action of B‐lactam antibiotics. PLoS ONE 2014;9(9):e106967. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kelly 2004
- Kelly LF. Pediatric cough and cold preparations. Pediatrics in Review 2004;25(4):115‐23. [DOI] [PubMed] [Google Scholar]
Khalil 2010
- Khalil MI, Sulaiman SA, Boukraa L. Antioxidant properties of honey and its role in preventing health disorder. Open Nutraceuticals Journal 2010;3:6‐16. [Google Scholar]
Kigen 2015
- Kigen G, Busakhala N, Ogaro F, Chesire E, Saat N, Too R, et al. A review of the ingredients contained in over the counter (OTC) cough syrup formulations in Kenya. Are they harmful to infants?. PLoS ONE 2015;10(11):e0142092. [DOI: 10.1371/journal.pone.0142092] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kousalya 2010
- Kousalya K, Thirumurugu S, Arumainayagam DC, Manavalan R, Vasantha J, Reddy CU. Antimicrobial resistance of bacterial agents of the upper respiratory tract in south Indian population. Journal of Advanced Pharmaceutical Technology & Research 2010;1(2):207‐15. [PUBMED: PMC3255429] [PMC free article] [PubMed] [Google Scholar]
Kuncic 2012
- Kuncic MK, Jaklic D, Lapanje A, Gunde‐Cimerman N. Antibacterial and antimycotic activities of Slovenian honeys. British Journal of Biomedical Science 2012;69(4):154‐8. [PUBMED: 23304790] [PubMed] [Google Scholar]
Kurth 1978
- Kurth W. Secure therapeutic effectiveness of the traditional antitussive agent Mintetten in a double‐blind study [Gesicherte therapeutische wirksamkeit des traditionellen antitussivums mintetten im doppelblindversuch]. Medizinische Welt 1978;29(48):1906‐9. [PubMed] [Google Scholar]
Kusel 2007
- Kusel MM, Klerk N, Holt PG, Landau Ll, Sly PD. Occurrence and management of acute respiratory illnesses in early childhood. Pediatric Infectious Disease Journal 2007;43(3):139‐46. [DOI] [PubMed] [Google Scholar]
Küplülü 2006
- Küplülü O, Göncüoglu M, Özdemir H, Koluman A. Incidence of Clostridium botulinum spores in honey in Turkey. Food Control 2006;17(3):222‐4. [Google Scholar]
Landau 2006
- Landau LI. Acute and chronic cough. Paediatric Respiratory Reviews 2006;7(1):64‐7. [DOI] [PubMed] [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JP, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Likert 1932
- Likert R. A technique for measurement of attitude. Archives of Psychology 1932;140:1‐55. [Google Scholar]
Lusby 2005
- Lusby PE, Coombes AL, Wilkinson JM. Bactericidal activity of different honeys against pathogenic bacteria. Archives of Medical Research 2005;36(5):464‐7. [DOI] [PubMed] [Google Scholar]
Ma 2017
- Ma TT, Zhuang Y1, Gong HY, Yii AC, Wang XY, Shi HZ. Predictive value of respiratory symptoms for the diagnosis of pollen‐induced seasonal asthma among children and adults in Inner Mongolia. Therapeutics and Clinical Risk Management 2017;4(13):967‐74. [DOI: 10.2147/TCRM.S138355] [DOI] [PMC free article] [PubMed] [Google Scholar]
Microsoft 2007 [Computer program]
- Microsoft. Microsoft Excel. 2007.
Molan 2006
- Molan PC. The evidence supporting the use of honey as a wound dressing. International Journal of Lower Extremity Wounds 2006;5(1):40‐54. [DOI] [PubMed] [Google Scholar]
Morice 1998
- Morice A, Abdul‐Manap R. Drug treatments for coughs and colds. Prescriber 1998;17(9):74‐9. [Google Scholar]
Mulholland 2011
- Mulholland S, Chang AB. Honey and lozenges for children with non‐specific cough. Cochrane Database of Systematic Reviews 2011, Issue 2. [DOI: 10.1002/14651858.CD007523.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Mullai 2007
- Mullai V, Menon T. Bactericidal activity of different types of honey against clinical and environmental isolates of Pseudomonas aeruginosa. Journal of Alternative and Complementary Medicine 2007;13(4):439‐41. [DOI] [PubMed] [Google Scholar]
Nagai 2006
- Nagai T, Inoue R, Kanamori N, Suzuki N, Nagashima T. Characterization of honey from different floral sources. Its functional properties and effect of honey species on storage meat. Food Chemistry 2006;97(2):256‐62. [Google Scholar]
Nanda 2003
- Nanda V, Sarkar BC, Sharma HK, Bawa AS. Physico‐chemical properties and estimation of mineral content in honey produced from different plants in Northern India. Journal of Food Composition and Analysis 2003;16(5):613‐9. [Google Scholar]
Nevas 2002
- Nevas M, Heilm S, Lindström M, Horn H, Koivulehto K, Korkeala H. High prevalence of Clostridium botulinum types A and B in honey samples detected by polymerase chain reaction. International Journal of Food Microbiology 2002;72(1‐2):45‐52. [DOI] [PubMed] [Google Scholar]
Nitsche 2016
- Nitsche MP, Carreño M. Is honey an effective treatment for acute cough in children? [Miel versus no tatramiento o placebo para la tos aguda en ninos]. Medwave 2016;16(Suppl 2):e6454. [DOI: 10.5867/medwave.2016.6454] [DOI] [PubMed] [Google Scholar]
Review Manager 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Sanz 2004
- Sanz ML, Gonzalez M, Lorenzo C, Sanz J, Matinez‐Castro I. Carbohydrate composition and physico chemical properties of artisanal honeys from Madrid (Spain): occurrence of Echium sp honey. Journal of the Science of Food and Agriculture 2004;84(12):1577‐84. [Google Scholar]
Shahzad 2012
- Shahzad A, Cohrs RJ. In vitro antiviral activity of honey against varicella zoster virus (VZV): a translational medicine study for potential remedy for shingles. Translational Biomedicine 2012;3(2):2. [DOI: 10.3823/434.] [DOI] [PMC free article] [PubMed] [Google Scholar]
Smith 2014
- Smith SM, Schroeder K, Fahey T. Over‐the‐counter (OTC) medications for acute cough in children and adults in community settings. Cochrane Database of Systematic Reviews 2014, Issue 11. [DOI: 10.1002/14651858.CD001831.pub5] [DOI] [PMC free article] [PubMed] [Google Scholar]
Smith 2016
- Smith JA, Woodcock A. Chronic cough. New England Journal of Medicine 2016;375:1544‐51. [DOI: 10.1056/NEJMcp1414215] [DOI] [PubMed] [Google Scholar]
Suárez‐Luque 2002
- Suárez‐Luque S, Mato I, Huidobro JF, Simal‐Lozano J, Sancho MT. Rapid determination of minority organic acids in honey by high‐performance liquid chromatography. Journal of Chromatography 2002;955(2):207‐14. [DOI] [PubMed] [Google Scholar]
Tonks 2003
- Tonks AJ, Cooper RA, Jones KP, Blair S, Parton J, Tonks A. Honey stimulates inflammatory cytokine production from monocytes. Cytokine 2003;21(5):242‐7. [DOI] [PubMed] [Google Scholar]
Tuzen 2007
- Tuzen M, Silici S, Mendil D, Soylak M. Trace element levels in honeys from different regions of Turkey. Food Chemistry 2007;103(2):325‐30. [Google Scholar]
Watanabe 2014
- Watanabe K, Rahmasari R, Matsunaga A, Haruyama T, Kobayashi N. Anti‐influenza viral effects of honey in vitro: potent high activity of manuka honey. Archives of Medical Research 2014;45(5):359‐65. [DOI: 10.1016/j.arcmed.2014.05.006] [DOI] [PubMed] [Google Scholar]
Yao 2003
- Yao L, Datta N, Tomas‐Barberan FA, Ferreres F, Martos I, Singanusong R. Flavonoids, phenolic acids and abscisic acid in Australian and New Zealand leptospermum honeys. Food Chemistry 2003;81(2):159‐68. [Google Scholar]
Zeina 1996
- Zeina B, Othman O, Al‐Assad S. Effects of honey versus thyme on rubella virus survival in vitro. Journal of Alternative and Complementary Medicine 1996;2(3):345‐8. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Oduwole 2008
- Oduwole O, Meremikwu MM, Oyo‐Ita A, Udoh EE. Honey for acute cough in children. Cochrane Database of Systematic Reviews 2008, Issue 2. [DOI: 10.1002/14651858.CD007094] [DOI] [PMC free article] [PubMed] [Google Scholar]
Oduwole 2010
- Oduwole O, Meremikwu MM, Oyo‐Ita A, Udoh EE. Honey for acute cough in children. Cochrane Database of Systematic Reviews 2010, Issue 1. [DOI: 10.1002/14651858.CD007094.pub2] [DOI] [PubMed] [Google Scholar]
Oduwole 2012
- Oduwole O, Meremikwu MM, Oyo‐Ita A, Udoh EE. Honey for acute cough in children. Cochrane Database of Systematic Reviews 2012, Issue 3. [DOI: 10.1002/14651858.CD007094.pub3] [DOI] [PubMed] [Google Scholar]
Oduwole 2014a
- Oduwole O, Meremikwu MM, Oyo‐Ita A, Udoh EE. Honey for acute cough in children. Cochrane Database of Systematic Reviews 2014, Issue 12. [DOI: 10.1002/14651858.CD007094.pub4] [DOI] [PubMed] [Google Scholar]
Oduwole 2014b
- Oduwole O, Meremikwu MM, Oyo‐Ita A, Udoh EE. Honey for acute cough in children. Evidence‐based Child Health 2014;9(2):401‐44. [DOI: 10.1002/ebch.1970] [DOI] [PubMed] [Google Scholar]