

Abstract
Background
Opioid drugs have been used for many years to relieve pain. Transdermal fentanyl offers one option for delivering and maintaining pain relief in patients with moderate or severe cancer pain.
Objectives
To determine the analgesic efficacy of transdermal fentanyl for relief of cancer pain, and to assess the adverse events associated with the use of transdermal fentanyl for relief of cancer pain.
Search methods
The following databases were searched: Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library 2013, Issue 4 of 12); MEDLINE (1966 to May 2013); EMBASE (1974 to May 2013; CANCERLIT (PubMED) (November 2012); and ClinicalTrials.gov (May 2013).
Selection criteria
Published randomised controlled trials (RCTs) using placebo or active comparators reporting on the analgesic effect of transdermal fentanyl in adults and children with cancer pain. Studies with fewer than 10 participants were excluded.
Data collection and analysis
Data were extracted independently by two review authors. We extracted any available data on the number or proportion of patients with ‘no worse than mild pain’ or treatment success (very satisfied, or very good or excellent on patient global impression scales), together with information about adverse events and withdrawals.
Main results
We identified nine studies meeting the inclusion criteria, including a Turkish study that is awaiting formal translation. There were 1244 participants randomised in classically designed RCTs, of whom 1197 had evaluable data, and 138 patients enrolled in an enriched enrolment, randomised withdrawal (EERW) trial. Overall, 600 participants were treated with transdermal fentanyl patches, 382 with various formulations of morphine, 36 with methadone, and 221 with paracetamol plus codeine. There were major sources of potential bias, including lack of blinding, small size, high levels of attrition, and inconsistent reporting.
We could not compare data in a meaningful analysis regarding adverse events such as nausea, abdominal pain, gastrointestinal bleeding, and confusion. These events may have been attributable to the underlying disease process.
There were insufficient comparable data for meta‐analysis to be undertaken or to produce numbers needed to treat (NNT) for the analgesic effect. In seven studies with 461 participants reporting pain intensity results after about two weeks, the mean or median pain scores were on the borderline of mild and moderate pain. Most participants would have had no worse than mild pain on treatment. Another reported that 77% of participants using transdermal fentanyl had an undefined successful outcome. Fewer participants experienced constipation with transdermal fentanyl (28%) than with oral morphine (46%), giving a risk ratio of 0.61 (95% CI 0.47 to 0.78); the NNT to prevent constipation was 5.5 (95% CI 3.8 to 10).
Authors' conclusions
The randomised trial literature for effectiveness of transdermal fentanyl is limited, but it is an important medicine. Most studies recruited fewer than 100 participants and did not provide data appropriate for meta‐analysis. Only a few reported how many patients had good pain relief but, where data were reported, a majority had no worse than mild pain within a reasonably short time period. The evidence pointed to a useful and significant reduction in complaints about constipation for transdermal fentanyl compared with oral morphine.
Plain language summary
Transdermal fentanyl for cancer pain
Fentanyl patches placed on the skin produced good pain relief for most people with moderate or severe cancer pain.
One person in two or three who gets cancer will suffer from pain that becomes moderate or severe in intensity. The pain tends to get worse as the cancer progresses. Morphine taken by mouth has been used since the 1950s for controlling cancer pain. Since that time a number of different drugs with morphine‐like actions have been produced for treating cancer pain, one of which is fentanyl. Fentanyl is particularly useful because it can be absorbed through the skin from patches. The ability of any drug to achieve consistent drug levels in the blood and the brain could, in theory, lead to better control of cancer pain. It also relieves the need to take medicines several times a day, as patches can often last for several days before changing.
We found nine studies involving 1244 patients. The studies were often small, used different study designs, and compared fentanyl with many different drugs. Most patients had pain that went from moderate or severe before transdermal fentanyl to no worse than mild pain when using transdermal fentanyl. Only 3 in 10 patients were constipated using transdermal fentanyl compared with 5 in 10 using oral morphine. We could not analyse the data in a meaningful way regarding harmful (adverse) events such as nausea, abdominal pain, gastrointestinal bleeding, and confusion. These events may have been attributable to the underlying disease processes.
The effect of the patch can continue after it has been taken off due to medicine that has been taken up by the skin. Used patches need to be disposed of carefully.
We could wish for more consistency in study design, and especially in study reporting, which should include the outcome of pain reduced to tolerable levels – no worse than mild pain – so that patients with cancer are not bothered by pain.
Background
Description of the condition
Cancer is a common disease. There is a greater than 1 in 3 risk of developing cancer over a person’s lifetime. In 2010 (the latest year for which statistics are available), approximately 325,000 people were diagnosed with cancer in the UK, or nearly 900 each day (Cancer Research UK). A recent review of the pharmacologic management of cancer pain reported that 24% to 62% of adult patients have pain at the time of cancer diagnosis, and almost all patients will be in pain in the terminal stages of the disease (Cleary 2007). Pain can be debilitating and have a serious impact on the quality of life of these patients.
Description of the intervention
Fentanyl patches are available as generic formulations and branded names include Fentalis®, Matrifen®, Mezolar®, Osmanil®, Tilofyl®, Victanyl®, Durogesic® and DTrans®. They are available as 8, 12, 25, 50, 75 and 100 micrograms (μg)/h transdermal patches. The 25, 50, 75, and 100 μg/h patches were first licensed in 1994, the 12 μg patch in 2005, and the 8 μg patch in 2010 (Patient information leaflet, Electronic medicines compendium). Transdermal fentanyl provides ‘rate controlled’ drug delivery over 72 hours at 25 μg per hour per 10 cm2. In addition to surface area, skin permeability and local blood flow determine absorption (Heiskanen 2009). In a study of 10 normal weight cancer patients compared to 10 cachectic (suffering from cancer cachexia, that is weak and underweight) cancer patients, absorption was impaired in the cachectic patients (Heiskanen 2009). The 'reservoir patch' is being phased out and replaced with a matrix design, as it was likely to leak if damaged or cut. Trials following replacement demonstrated no difference in pain intensity reduction or overall adverse effects. Satisfaction was improved, and wearability, adhesion, and comfort were improved (Cachia 2011).
How the intervention might work
Fentanyl is a synthetic opioid that acts at the mu opioid receptor. It takes 8 to 16 hours before the full effect of transdermal fentanyl is observed, and steady state is not observed until after two to four applications of the '72‐hour' patches. This is because initially there is depot accumulation of the drug within skin tissues (Jeal 1997). Levels in the blood fall gradually by approximately 50% within 16 hours of removal (Lehmann 1992). This prolonged elimination can be problematic with side effects such as hypoventilation, for example (Kornick 2003). Fentanyl is ideal for transdermal administration due to its lipophilicity (Cachia 2011). It is also highly potent and has a low molecular weight (Muijsers 2001), and differs from other opioids in penetration characteristics, for example through the dura (Moore 1982). A transdermal route of administration is useful in patients who are unable to swallow or who have gastrointestinal problems (Kornick 2003).
Why it is important to do this review
A previous meta‐analysis has compared the efficacy and safety of transdermal fentanyl and sustained release oral morphine (Clark 2004). This Canadian group, however, looked at both cancer and chronic non‐cancer pain, at a variety of study designs, including open label, uncontrolled trials, and randomised trials, and reported group mean results. Some of these study designs and methods are known to introduce bias, leading to overestimation of benefits. Another systematic review of transdermal opioids (fentanyl and buprenorphine) looked at evidence to support use of transdermal formulations as front line agents in moderate to severe cancer pain (Tassinari 2011), but did no quantitative analysis, while a systematic review of adverse events found reduced rates for some events for fentanyl and buprenorphine in a combined analysis compared with slow release morphine (Tassinari 2008).
This Cochrane Review is one of a series of reviews concerning individual drug interventions for cancer pain and will ultimately be included in an overview.
Objectives
To determine the analgesic efficacy of transdermal fentanyl for relief of cancer pain.
To assess the adverse events associated with the use of transdermal fentanyl for relief of cancer pain.
Methods
Criteria for considering studies for this review
Types of studies
Randomised (described as ‘randomised’ anywhere in the manuscript)
Ideally double blind, but open studies will be included as second tier evidence
Placebo or active controls, or both
Minimum of 10 participants per treatment arm
Studies with a minimum duration of 7 days for efficacy (it can take 'several 72‐hour patches to reach steady state' (Jeal 1997))
We excluded non‐randomised studies, studies of experimental pain, case reports and clinical observations. Studies had to be fully published or available as extended abstracts (for example from clinical trials websites); we did not include short (usually conference) abstracts.
Types of participants
Inpatients or outpatients with chronic pain of moderate to severe intensity, due to malignant disease (any stage)
Male or female
There were no limits on age
Types of interventions
Transdermal fentanyl (fentanyl patches) compared to placebo or active controls, in any dose, frequency, or duration of treatment.
Types of outcome measures
Pain had to be measured using a validated assessment tool. For pain intensity, for example, this could be a 100 mm visual analogue scale (VAS) (no pain to worst pain imaginable) or a four‐point categorical scale (none, mild, moderate, severe), and for pain relief a 100 mm VAS (no relief to complete relief), or five‐point categorical scale (none, a little, some, a lot, complete or words to that effect). Measures of ≥ 30% (moderate) and ≥ 50% (substantial) reduction of pain over baseline are recommended outcomes for chronic pain studies from the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) (Dworkin 2008). When considering Patient Global Impression of Change (PGIC), ≥ 30% reduction of pain over baseline equates to much improved or very much improved, and ≥ 50% to very much improved.
Primary outcomes
Number of participants with pain reduction of ≥ 30% from baseline
Number of participants with pain reduction of ≥ 50% from baseline
Number of participants with pain no worse than mild
Number of participants with PGIC of much improved or very much improved (or equivalent wording)
Secondary outcomes
Quality of life measures
Use of rescue medication
Patient satisfaction or preference
Adverse events: any, serious
Attrition: withdrawals due to lack of efficacy or adverse events (including death)
Search methods for identification of studies
Electronic searches
We searched the following databases:
the Cochrane Central Register of Controlled Trials (CENTRAL) (2013, Issue 4);
MEDLINE (1950 to 3 May 2013);
EMBASE (1974 to 3 May 2013);
CANCERLIT (PubMED) (searched to November 2012).
See Appendix 1, Appendix 2, and Appendix 3 for the MEDLINE, EMBASE, CENTRAL and CANCERLIT search strategies.
Searching other resources
Reference lists
All included studies
Key textbooks
Previous systematic reviews
Unpublished data
Personal communication with authors
Personal communication with pharmaceutical companies
Language
There was no language restriction.
Data collection and analysis
Selection of studies
Two review authors independently read the titles and abstracts of all studies identified by the searches, and excluded those that clearly did not meet the inclusion criteria. For the remaining studies, we read the full manuscript to assess if it should be included. We resolved discrepancies between review authors by discussion; if necessary a third review author would have been consulted. We did not anonymise studies before selection.
Data extraction and management
Two review authors independently extracted data using a standard form and agreed on the data before entry into RevMan (RevMan 2011). Data extracted included information about the number of participants treated and demographic details, type of cancer, drug and dosing regimen, study design (placebo or active control) and methods, study duration and follow‐up, analgesic outcome measures and results, withdrawals and adverse events.
Assessment of risk of bias in included studies
We assessed methodological quality using a validated scoring system (Jadad 1996) (Appendix 4). Two authors independently assessed risk of bias for each study using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011) and adapted from those used by the Cochrane Pregnancy and Childbirth Group, with any disagreements resolved by discussion. The following were assessed for each study.
Random sequence generation (checking for possible selection bias). The method used to generate the allocation sequence was assessed as: low risk of bias (any truly random process, e.g. random number table; computer random number generator); unclear risk of bias (method used to generate sequence not clearly stated). Studies using a non‐random process (e.g. odd or even date of birth; hospital or clinic record number) were excluded.
Allocation concealment (checking for possible selection bias). The method used to conceal allocation to interventions prior to assignment and whether intervention allocation could have been foreseen in advance of, or during recruitment, or changed after assignment, was assessed as: low risk of bias (e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes); unclear risk of bias (method not clearly stated). Studies that did not conceal allocation (e.g. open list) were excluded.
Blinding of outcome assessment (checking for possible detection bias). The methods used to blind study participants and outcome assessors from knowledge of which intervention a participant received were assessed as: low risk of bias (study stated that it was blinded and describes the method used to achieve blinding e.g. identical tablets; matched in appearance and smell); unclear risk of bias (study stated that it was blinded but does not provide an adequate description of how it was achieved); high risk of bias (studies that were not double blind).
Incomplete outcome data (checking for possible attrition bias due to the amount, nature and handling of incomplete outcome data). The methods used to deal with incomplete data were assessed as: low risk (< 10% of participants did not complete the study; or used ‘baseline observation carried forward’ analysis); unclear risk of bias (used 'last observation carried forward' analysis); high risk of bias (used 'completer' analysis).
Size of study (checking for possible biases confounded by small size). Studies were assessed as being at: low risk of bias (≥ 200 participants per treatment arm); unclear risk of bias (50 to 199 participants per treatment arm); high risk of bias (< 50 participants per treatment arm).
Measures of treatment effect
We used dichotomous data to calculate risk ratios (RR) with 95% confidence intervals (CI), and calculated numbers needed to treat to benefit (NNTs) as the reciprocal of the absolute risk reduction (McQuay 1998). For unwanted effects, the NNT becomes the number needed to treat to harm (NNH), and is calculated in the same manner.
We use the following terms to describe adverse outcomes in terms of harm or prevention of harm.
When significantly fewer adverse outcomes occur with fentanyl than with control (placebo or active) we use the term number needed to treat to prevent one event (NNTp).
When significantly more adverse outcomes occur with fentanyl compared with control (placebo or active) we use the term number needed to harm or cause one event (NNH).
We did not plan to use continuous data for the primary outcome because it is inappropriate where there is an underlying skewed distribution, as is usually the case with analgesic response.
Unit of analysis issues
The unit of randomisation was the individual patient.
Dealing with missing data
We planned to use intention‐to‐treat (ITT) analysis: participants who were randomised, took the study medication and gave a minimum of one post‐baseline assessment. Where there were missing participants or information, we assigned them to a zero improvement category where possible. We also looked for information about how data from withdrawals and dropouts were handled. In original studies, patients may have been analysed using ‘last observation carried forward' (that is their level of pain when stopping the medication), or returned to their baseline observation.
Where there were substantial numbers (> 10%) of participants missing from analyses, we comment on this. There were insufficient data for sensitivity analyses.
Assessment of heterogeneity
We planned to assess statistical heterogeneity using L'Abbé plots, a visual method for assessing differences in results of individual studies (L'Abbé 1987), and by use of the I2 statistic. We anticipated that there may be an effect of differences between patients, environment (inpatient versus outpatient) and outcome measures. We had planned to explore these with subgroup and sensitivity analyses where there were sufficient data, but the amount of data identified was, for the most part, inadequate for any more than basic analysis.
The aim of this review was to use dichotomous data of known utility (Moore 2010). The review does not depend on what authors of the original studies chose to report or not.
Data synthesis
We carried out data synthesis and statistical analysis using the Review Manager software (RevMan 2011). Where appropriate, we pooled data for each dichotomous outcome and calculated RRs with 95% CIs using the fixed‐effect model (Morris 1995), together with NNTs with 95% CIs (Cook 1995). We assumed a statistically significant benefit of active treatment over control when the lower limit of the 95% CI of the RR was greater than one, and of control over active treatment when the upper limit of the 95% CI was less than one. RR and NNH were calculated for adverse outcomes in the same way.
We planned to analyse studies carried out under double blind conditions separately from those that were not. We did not carry out pooled analysis where there would be fewer than 200 participants in the comparison (Moore 1998).
We planned to test for statistically significant differences between subgroups using the z test (Tramèr 1997).
Subgroup analysis and investigation of heterogeneity
We planned subgroup analysis for different types of cancer and different areas of the body, but were able only to distinguish differences in overall death rates between participants with primary cancers and those with metastatic disease.
Different doses were not considered as patients are titrated to effective dose.
Sensitivity analysis
We planned to carry out sensitivity analyses for duration of study, age of participants (< 18 years versus ≥ 18 years), and setting (inpatient versus outpatient), but there were insufficient data.
Results
Description of studies
All studies were identified using electronic database searches; no additional studies were found through communication with Janssen‐Cliag UK.
Included studies
We identified nine studies meeting the inclusion criteria (Ahmedzai 1997; Kongsgaard 1998; Kress 2008; Mercadante 2008; Mystakidou 2005; Oztürk 2008; Pistevou‐Gompaki 2004; van Seventer 2003; Wong 1997).
There were 1244 participants randomised in classically designed randomised controlled trials, of whom 1197 had evaluable data, and 138 patients enrolled in an enriched enrolment, randomised withdrawal (EERW) trial (Kongsgaard 1998). In total, 600 participants were treated with transdermal fentanyl patches, 382 with various formulations of morphine, 36 with methadone, and 221 with paracetamol plus codeine.
Details of individual studies are in the Characteristics of included studies table. The mean age of participants in the included studies was 59 to 65 years (range 18 to 91 years), and 57% were male. There were no studies in children.
Type of cancer
Two studies (Mystakidou 2005; Pistevou‐Gompaki 2004) specifically concentrated on the pain of bony metastasis; sites included thoracic spine, lumbar spine, cervical spine, thoracic and lumbar spine, pelvis, limbs, and scapula. The remaining studies enrolled participants with primary cancer; sites included lung, prostate, breast, stomach or gallbladder, kidney, uterus, liver, head and neck, pancreas, multiple myeloma, cervical, and other or unknown.
Life expectancy or performance status criteria
The majority of studies made some estimation of life expectancy or performance status criteria at enrolment.
Life expectancy > 1 month (Ahmedzai 1997).
Karnofsky performance ≥ 50 (Kongsgaard 1998; Kress 2008).
On Step 3 WHO opioids for pain (Kress 2008; Oztürk 2008).
Expected survival ≥ 3 months (Mercadante 2008; van Seventer 2003).
Study designs
The following study designs were used.
One randomised, double blind, placebo controlled EERW study: double blind period of nine days (Kongsgaard 1998).
One open label, active controlled, cross‐over study: 2 x 15 day treatment periods with no washout (Ahmedzai 1997).
Six open label, active controlled parallel studies: duration of treatment two weeks to three months (Kress 2008; Mercadante 2008; Mystakidou 2005; Oztürk 2008; Pistevou‐Gompaki 2004; van Seventer 2003; Wong 1997).
All studies except Pistevou‐Gompaki 2004 titrated the dose of medication at the start, and rescue medication was available.
Interventions
Transdermal fentanyl versus oral morphine
Transdermal fentanyl patch (TDF) every 72 hours versus sustained release oral morphine (SRM) every 12 hours (Ahmedzai 1997). N = 202 (TDF 122, SRM 122).
Fentanyl investigational matrix patch (FIT) versus standard opioid treatment (Durogesic patch (TDF) or Oramorph) (Kress 2008). N = 220 (FIT 117, Durogesic 65, Oramorph 38).
TDF versus SRM or oral methadone (Mercadante 2008). N = 108 (TDF 36, SRM 36, methadone 36).
TDF versus SRM (Oztürk 2008). N = 50 (TDF 25, SRM 25).
TDF every 72 hours versus SRM every 12 hours (van Seventer 2003). N = 131 (TDF 67, SRM 64).
TDF every 72 hours versus SRM every 12 hours (Wong 1997). N = 47 (TDF 20, SRM 20).
Transdermal fentanyl versus paracetamol and codeine
Radiotherapy plus: TDF every 72 hours or paracetamol plus codeine (P/C) four times daily (Mystakidou 2005). N = 460 (TDF 201, P/C 221).
Radiotherapy plus: TDF every 72 hours or paracetamol plus codeine (P/C) four times daily (Pistevou‐Gompaki 2004). N = 26 (TDF 13, P/C 13).
Transdermal fentanyl versus placebo
TDF or placebo (Kongsgaard 1998). N = 138 (TDF 47, placebo 48, not randomised 43).
Pain and analgesic measurement tools
Studies used a variety of pain and analgesic measurement tools. Almost half used a visual analogue scale (VAS) (Ahmedzai 1997; Kongsgaard 1998; Mystakidou 2005; Pistevou‐Gompaki 2004) and two used the Greek brief pain inventory (G‐BPI) 0 to 10 (Mystakidou 2005; Pistevou‐Gompaki 2004). A detailed list of tools for each study can be found in the Characteristics of included studies table.
Excluded studies
We excluded three studies (Ergenoglu 2010; Sarhan 2009; Wirz 2009); reasons for exclusion are provided in the Characteristics of excluded studies table.
Risk of bias in included studies
We assessed the methodological quality of each study using the Oxford Quality Scale (Jadad 1996), which awards points for adequate reporting of randomisation (2), blinding (2), and study withdrawals (1). Overall, the methodological quality of the included studies was poor, with a median score of two (range one to three); studies scoring three or more give more conservative estimates of effect. The results for each study can be found in the Characteristics of included studies section.
We also assessed each study using the Cochrane risk of bias tool. Overall findings are presented in the 'Risk of bias' graph (Figure 1), which reviews the authors' judgements about each risk of bias item presented as percentages across all included studies, and the 'Risk of bias' summary (Figure 2), which reviews the authors' judgements about each risk of bias item for each included study.
1.
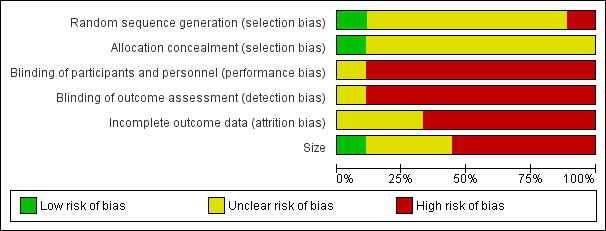
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
2.
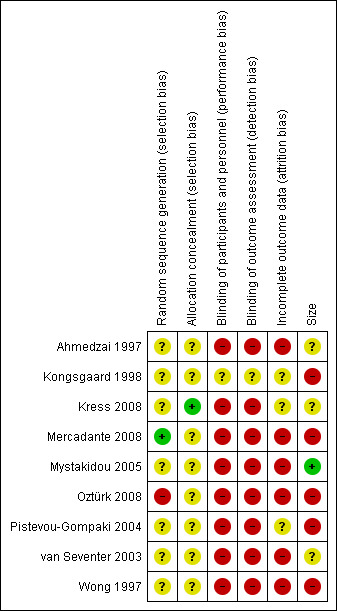
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
All studies reported that they were randomised, but only one properly described the method used to generate the random sequence (Mercadante 2008), and only one adequately described the method used to conceal the allocation (Kress 2008).
Blinding
Only one study (Kongsgaard 1998) was double blind, although there was an inadequate description of how sequence generation and allocation were achieved.
Incomplete outcome data
Five studies (Ahmedzai 1997; Mercadante 2008; Mystakidou 2005; Oztürk 2008; Wong 1997) analysed only participants who completed the study, and another (van Seventer 2003) used last observation carried forward imputation; these studies were considered to be at high risk of bias. Kongsgaard 1998 reported an ITT analysis, but in both this and Pistevou‐Gompaki 2004, the imputation method was unclear; these studies were considered to be at unknown risk of bias. Kress 2008 was not a true ITT analysis because participants with missing values for any analysis did not contribute to that analysis.
Other potential sources of bias
Treatment group size was an issue. Small studies are thought to be at increased risk of bias, probably because the conduct of small studies is more likely to be less rigorous, allowing critical criteria to be compromised. Only one of the treatment groups in this review was large enough to give a low risk of bias (Mystakidou 2005). Four studies (Ahmedzai 1997; Kress 2008; Oztürk 2008; van Seventer 2003) were judged to have an unclear risk of bias due to size, and four, notably including the only double blind placebo controlled trial (Kongsgaard 1998), were judged to carry a high risk of bias.
Effects of interventions
None of the studies we identified reported any of our pre‐specified primary outcomes. We were, however, able to make a judgement as to outcomes equivalent to no worse than mild pain.
No worse than mild pain
We examined reports to ascertain whether an outcome of no worse than mild pain was achieved, based on a VAS pain intensity of 30 mm or less on a 100 mm scale or the equivalent in other pain scales. Seven studies reported an outcome indicating achievement of this level of pain relief, for the most part apparently using data from completers, and all reporting mean outcomes (Kress 2008; Mercadante 2008; Mystakidou 2005; Oztürk 2008; Pistevou‐Gompaki 2004; van Seventer 2003; Wong 1997). Summary table A shows that for all seven studies, with 461 participants reporting pain intensity results after about two weeks, the mean or median pain scores were on the borderline of mild and moderate pain. The indications were therefore that most participants would have had no worse than mild pain on treatment.
In addition, Ahmedzai 1997 reported that 94/122 participants on transdermal fentanyl had a successful outcome (not clearly defined). Kongsgaard 1998 by contrast reported an outcome of no worse than moderate pain, but it was unclear what that meant.
Results for comparator drugs indicated a similar response with SRM, Durogesic patch, Oramorph, and methadone, and a slightly reduced response with paracetamol plus codeine.
| Summary table A: pain intensity | ||||
| Study | Number taking TDF | Mean pain intensity result | Scale | Timescale |
| Kress 2008 | 117 | 31 ± 2% of maximum | 100% | over 30 days |
| Mercadante 2006 | 36 | 3.0 (2.0 to 3.6) | out of 10 | 2 weeks |
| Mystakidou 2005 | 188 | 2 | out of 10 | 2 weeks |
| Ozturk 2008 | 22 | 3 (range 0 to 3) | out of 10 | 2 weeks |
| Pisetvou‐Gompaki 2004 | 13 | 3.5 | out of 10 | 2 weeks |
| van Seventer 2003 | 45 | approximately 3 | out of 10 | 2 weeks |
| Wong 1997 | 40 | 0.9 ± 0.1 | out of 4 | 2 weeks |
Adverse events
Summary table B below describes patients experiencing any adverse event, but it was not always possible to attribute the adverse event to a specific group.
| Summary table B: participants experiencing any adverse event (including death) | |||
| Study | Overall | Transdermal fentanyl | Comparator |
| Ahmedzai 1997 | No usable data | More events were reported during fentanyl treatment than morphine, although participants' perception was the reverse. Some events with fentanyl may have been due to morphine withdrawal | |
| Kongsgaard 1998 | No usable data | Nausea was most common adverse event: 15/138 during open label titration phase | Not reported |
| Kress 2008 | 130/220 | 72/117 | 58/103 (standard treatment: Durogesic or Oramorph) |
| Mercadante 2008 | No usable data | No important differences in symptom intensity between groups | |
| Mystakidou 2005 | No usable data | Constipation less frequent with fentanyl (≤ 18%) than paracetamol plus codeine (≤ 30%) | |
| Oztürk 2008 | No usable data | Impossible to tell if same patient is counted twice in adverse events table. Constipation less frequent in fentanyl group (27%) than sustained release morphine group (64%) | |
| Pistevou‐Gompaki 2004 | 8/26 | 5/13 | 3/13 (paracetamol plus codeine) |
| van Seventer 2003 | 115/131 | 61/67 | 54/64 (sustained oral release morphine) |
| Wong 1997 | No usable data | Some events (anorexia, nausea, insomnia) improved from baseline values with treatment | |
Specific adverse events
Constipation
In four studies (Ahmedzai 1997; Oztürk 2008; van Seventer 2003; Wong 1997) it was possible to compare the impact of constipation between TDF and SRM (Figure 3; Analysis 1.1). Fewer participants experienced constipation with TDF (28%) than with oral SRM (46%), giving a risk ratio of 0.61 (95% CI 0.47 to 0.78); the NNTp was 5.5 (3.8 to 10). This analysis was however conducted making assumptions about the primary data it was based upon. The numbers used were not ITT, they were based on completers and those who reported on adverse events. In Ahmedzai 1997 for example, data were taken from the 'bowel function' questionnaire rather than 'adverse events'. Data used from van Seventer 2003 were taken from patients reporting constipation at 28 days in Table 5 of that paper. Wong 1997 reported constipation in completers only.
3.
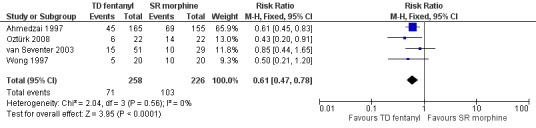
Forest plot of comparison: 1 Fentanyl versus sustained release morphine, outcome: 1.1 Constipation.
1.1. Analysis.
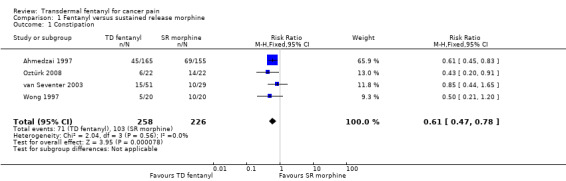
Comparison 1 Fentanyl versus sustained release morphine, Outcome 1 Constipation.
Reports of constipation were inconsistent. Constipation rates were much higher when bowel function was specifically asked about, using a questionnaire in Ahmedzai 1997 and direct questioning in van Seventer 2003, which may well skew the data. Using constipation reported as an adverse event in Ahmedzai 1997 and van Seventer 2003 gave a relative risk of 0.50 (0.34 to 0.74) and an NNTp of 8.2 (5.2 to 19).
Rash and pruritis
Rash and pruritis are adverse effects commonly associated with fentanyl patches. In the studies that reported on these the rates were low and symptoms improved with time. In the 161 participants who received skin assessments in the study by Ahmedzai 1997, five (3%) patients had erythema, eight had mild itching, and three (2%) had moderate itching at the patch site after the patches were removed. Over a two‐week period in Mystakidou 2005, 3/201 patients in the TDF group and 2/221 patients in the P/C group were noted as having rash or pruritis. In Wong 1997 two patients in the TDF group had itching and a skin rash which improved with time.
Other adverse events included nausea, vomiting, dry mouth, gastritis, abdominal pain, gastrointestinal haemorrhage, and confusion. It is difficult to say how many of these could be attributed to the underlying disease process, and no meaningful analysis was possible.
Serious adverse events
No serious adverse events were judged to be attributable to the study medications.
Death
The participants included in this review had an inherently high risk of mortality. It was impossible to accurately predict life expectancy, but most studies tried to ensure that those that enrolled would survive to the end of the study, based on their clinical condition at entry. Ahmedzai 1997 reported 14 deaths as a reason for study withdrawal (eight in the group fentanyl then morphine and six in the group morphine then fentanyl). Kress 2008 listed death as the reason for four participants withdrawing from the study (including one suicide). In addition, they reported that seven participants (6%) treated with the FIT patch and 12 (12%) treated with standard therapy died. There was one death reported in each of the SRM and TDF groups in Mercadante 2008. Seven of the withdrawals in Mystakidou 2005 were attributable to death; the group to which they belonged was not specified. Pistevou‐Gompaki 2004 reported one death due to advanced lung cancer in the fentanyl group, van Seventer 2003 reported seven deaths in the fentanyl group and four in the morphine group, and two patients died in the Wong 1997 study, although they are not attributed to a particular group. There were four deaths during the open label titration phase of Kongsgaard 1998, all attributed to disease progression. Oztürk 2008 did not report any deaths in the 15‐day study period. The number of participants who died is given in Summary table C.
Summary table C: deaths in studies where reported
| Study | Deaths | Timescale of study |
| Ahmedzai 1997 | 14/202 | 30 days |
| Kress 2008 | 23/220 | 30 days |
| Mercadante 2008 | 2/108 | 4 weeks |
| Mystakidou 2005 | 7/460 | 2 months |
| Oztürk 2008 | 0/50 | 15 days |
| Pistevou‐Gompaki 2004 | 1/26 | 3 months |
| van Seventer 2003 | 11/131 | 4 weeks |
| Wong 1997 | 2/47 | 2 weeks |
Over the period of all of the studies, almost 5% of the participants died. In studies lasting one month or less (participants with primary cancers) the death rate was 6.8%, and in those lasting two or three months (participants with bony metastases) it was 1.6%.
Withdrawal due to adverse events
Trials conducted in the palliative care setting inherently have a high dropout rate due to the frailty of the patients included. Most studies provided some information on withdrawals (Ahmedzai 1997; Kongsgaard 1998; Kress 2008; Mercadante 2008; Mystakidou 2005; Pistevou‐Gompaki 2004; van Seventer 2003). However, withdrawals were not always reported per treatment group and few data were reported according to ITT, as many patients were not accounted for.
Five studies reported withdrawal of participants due to adverse events (Ahmedzai 1997; Kress 2008; Mystakidou 2005; van Seventer 2003; Wong 1997). In three it was not clear whether participants withdrew whilst taking TDF or SRM (Ahmedzai 1997; Mystakidou 2005; Wong 1997). Furthermore, due to the unethical nature of prolonged washout, in the cross‐over study (Ahmedzai 1997) it was impossible to say whether adverse effects were due to morphine withdrawal in the TDF phase.
Summary table D lists the adverse event withdrawals described. Since not all studies reported adverse event withdrawals, and of those that did some did not specify in which group they occurred, it was possible to derive only a crude withdrawal rate of 9% from these studies. In only one study (van Seventer 2003) was there a clear difference in adverse event withdrawals between groups (TDF and SRM), but group numbers were too small to draw any conclusions.
Summary table D: adverse event withdrawals
| Study | Adverse event withdrawals |
| Ahmedzai 1997 | TDF/SRM 26/101, SRM/TDF 21/101 |
| Kongsgaard 1998 | 13/138 all during titration phase – i.e. on TDF |
| Kress 2008 | 26/220 in total (equally distributed between groups – FIT versus Durogesic or Oromorph) |
| Mercadante 2008 | TDF 0/36, SRM 1/36, methadone 2/36 |
| Mystakidou 2005 | 1/422 (did not state which group – TDF versus P/C) |
| Oztürk 2008 | None reported (0/50) ‐ TDF versus SRM |
| Pistevou‐Gompaki 2004 | None reported (0/24) – TDF versus P/C |
| van Seventer 2003 | TDF 3/67, SRM 23/64 |
| Wong 1997 | 2/47 (did not state which group – TDF versus SRM) |
| FIT ‐ fentanyl investigational matrix patch; P/C ‐ paracetamol plus codeine; SRM ‐ sustained release morphine; TDF ‐ transdermal fentanyl | |
Discussion
Summary of main results
For studies in cancer pain, it is useful to know what proportion of patients starting treatment are likely to be able to tolerate it, and what proportion of those who tolerate it are likely to obtain adequate pain relief. The studies did not report results in a way that unequivocally answers these questions.
None of our preferred outcomes were reported in any of the studies, but we were able to make a judgement of the number of participants who achieved a low pain state equivalent to 'no worse than mild pain'. It is clear that a majority of participants were able to continue with therapy for at least two to four weeks, and that the majority of those on therapy achieved this low pain state. This result is in general agreement with that for oral morphine (Wiffen 2013).
Overall completeness and applicability of evidence
Given the wide use of transdermal fentanyl in the palliative care setting, the evidence base for its use is limited. Studies enrolled patients who displayed heterogeneity in both the underlying malignancy and resultant pain. Two studies concentrated on painful bony metastasis, but again with heterogeneous primary cancer types. Comparator interventions ranged from a placebo control to paracetamol plus codeine and sustained relief oral morphine.
The only meaningful analysis when it came to adverse events concerned constipation. This analysis made a number of assumptions but seemed to favour transdermal fentanyl over oral morphine for lower rates of this troublesome side effect. Rash or pruritis is often quoted as a problem with transdermal fentanyl, but where reported in these studies it occurred at low rates and seemed to improve over time.
One of the useful outcomes from this systematic review is to highlight the inherent mortality of patients enrolled in these studies. Even though most studies included some measure of prognosis to ensure that life expectancy exceeded that of the proposed study duration, almost 7% of participants being treated for their primary cancer died over a study period of one month.
Quality of the evidence
The quality of evidence in these studies is severely limited. Overall, the methodological quality of the included trials was poor with a median quality score of two (range one to three) on the Oxford Quality Scale. Of the nine studies, only one was double blind and placebo controlled. It scored 3/5 on the Oxford Quality Scale due to failure to report the methods used to generate the random sequence and maintain blinding, and was judged to be at 'high risk of bias' using the risk of bias tool, owing to small sample size.
Potential biases in the review process
We are unaware of any potential biases in the review process.
Agreements and disagreements with other studies or reviews
This is the first systematic review looking at transdermal fentanyl in cancer pain compared to placebo or active controls. In a systematic review of adverse effects, comparing transdermal opiates with slow release morphine in moderate‐severe cancer pain, there was no overall difference in the adverse effect profile (Tassinari 2008). There was agreement with our finding that constipation was less of an issue in patients treated with transdermal fentanyl (taking into account the assumptions made concerning the primary literature upon which the analysis was based).
In their review of transdermal opioids in moderate to severe cancer pain, Tassinari 2011 concluded that slow release oral morphine was favoured, with transdermal opioids only recommended for use in selected patients. However, no quantitative analyses were undertaken.
In a recent systematic review of randomised trials evaluating the effectiveness of opioids in cancer pain, ‘fair evidence' was found for the effectiveness of transdermal fentanyl whereas other opioids were evaluated as being 'poorly efficacious' (Koyyalagunta 2012). This review excluded Kress 2008 because the ‘Cochrane score’ assigned to it did not meet the review's inclusion criteria. The included studies were van Seventer 2003, Mystakidou 2005, Mercadante 2008, and Marinangeli 2007. The latter study was a prospective randomised open label study looking at the influence of tramadol on dose adjustment of transdermal fentanyl in advanced cancer pain, and did not meet our inclusion criteria.
Authors' conclusions
Implications for practice.
Transdermal fentanyl is already widely used in the palliative care setting, but we found few studies of its use in cancer‐related pain. The studies were small, generally of poor quality, and none reported primary outcomes of importance to clinical practice. However, based on the end of treatment scores for people treated with transdermal fentanyl, we were able to make a judgement of the number of participants who achieved a state of 'no worse than mild pain'. We conclude that if patients were able to tolerate the medication and survived to the end of the study, pain appeared to be improved and the majority of patients would have no worse than mild pain.
In terms of side effects, lower rates of constipation have been demonstrated with transdermal fentanyl. These findings are however subject to the methodological weaknesses identified in the primary literature, and the analysis was conducted based on several assumptions. Rash and pruritis, commonly a concern with transdermal preparations, were in fact infrequent and improved with time. This review is unlikely to change current practice, but will hopefully stimulate further research in the area.
Implications for research.
Most studies in this review have very low methodological quality. Future studies should improve their design, use clinically important outcome measures, and be explicit in their methods of analysis so more meaningful comparisons can be made. Given the difficulty of conducting randomised controlled trials in the palliative care setting, observational studies that meet criteria for quality, validity and size could make a significant contribution to studies of cancer pain treatment (Hadley 2009). The single most important development would be the use of outcomes that are important to patients and relevant to clinical practice, namely achieving no worse than mild pain by, say, two weeks of treatment. The efficacy of transdermal fentanyl is comparable to morphine and it probably causes less constipation than morphine. However, clinical decision‐making based on this review would also need to take into account other factors, such as the balance of cost, preference, and speed of response needed (that is not for those who need rapid analgesic titration) when considering treatment for cancer pain.
What's new
| Date | Event | Description |
|---|---|---|
| 6 November 2018 | Review declared as stable | See Published notes. |
History
Protocol first published: Issue 12, 2012 Review first published: Issue 10, 2013
| Date | Event | Description |
|---|---|---|
| 17 November 2016 | Review declared as stable | See Published notes. |
Notes
A restricted search in November 2018 did not identify any potentially relevant studies likely to change the conclusions. We found only one small potentially relevant RCT, and we are aware of some NMA and TSA analyses that come to much the same conclusions as the current review. Therefore, this review has now been stabilised following discussion with the authors and editors. If appropriate, we will update the review if new evidence likely to change the conclusions is published, or if standards change substantially which necessitate major revisions.
Acknowledgements
This review received infrastructure support from the Oxford Pain Relief Trust. The authors would like to thank Hatun Bulut, a student at Wycliffe Hall, University of Oxford for her translation of Oztürk 2008.
Appendices
Appendix 1. MEDLINE (via Ovid) search strategy
exp Fentanyl/
(fentanyl or phentanyl or fentora or durogesic or duragesic or fentanest or sublimaze or r‐4263 or r4263).mp.
1 or 2
exp Neoplasms/
(neoplasm* or cancer* or carcinoma* or malignan* or tumor* or tumour* or adenocarcinoma* or choriocarcinoma* or leukemia* or leukaemia* or metasta* or sarcoma* or teratoma*).mp.
4 or 5
exp Pain/
Pain Management/
Pain Measurement/
pain*.mp.
7 or 8 or 9 or 10
3 and 6 and 11
randomized controlled trial.pt.
controlled clinical trial.pt.
randomized.ab.
placebo.ab.
drug therapy.fs.
randomly.ab.
trial.ab.
groups.ab.
13 or 14 or 15 or 16 or 17 or 18 or 19 or 20
12 and 21
Appendix 2. EMBASE (via Ovid) search strategy
exp fentanyl/
(fentanyl or phentanyl or fentora or durogesic or duragesic or fentanest or sublimaze or r‐4263 or r4263).mp.
1 or 2
exp neoplasm/
(neoplasm* or cancer* or carcinoma* or malignan* or tumor* or tumour* or adenocarcinoma* or choriocarcinoma* or leukemia* or leukaemia* or metasta* or sarcoma* or teratoma*).mp.
4 or 5
exp pain/
pain.mp.
7 or 8
randomized controlled trial/
random*.ti,ab.
factorial*.ti,ab.
assign*.ti,ab.
allocat*.ti,ab.
10 or 11 or 12 or 13 or 14
Appendix 3. CENTRAL search strategy
MeSH descriptor: [Fentanyl] explode all trees
(fentanyl or phentanyl or fentora or durogesic or duragesic or fentanest or sublimaze or r‐4263 or r4263):ti,ab,kw
#1 or #2
MeSH descriptor: [Neoplasms] explode all trees
(neoplasm* or cancer* or carcinoma* or malignan* or tumor* or tumour* or adenocarcinoma* or choriocarcinoma* or leukemia* or leukaemia* or metasta* or sarcoma* or teratoma*):ti,ab,kw
#4 or #5
MeSH descriptor: [Pain] explode all trees
pain or painful or analgesi*:ti,ab,kw
#7 or #8
#3 and #6 and #9
Limit #10 to Clinical Trials (CENTRAL)
CANCERLIT (PubMED)
#19 Search (#18) AND #9
#18 Search (#10 or #11 or #12 or #13 or #14 or #15 or #16 or #17)
#17 Search groups [tiab]
#16 Search trial [tiab]
#15 Search randomly [tiab]
#14 Search drug therapy [sh]
#13 Search placebo [tiab]
#12 Search randomized [tiab]
#11 Search controlled clinical trial [pt]
#10 Search randomized controlled trial [pt]
#9 Search (#8) AND #2 Filters: Cancer
#8 Search (((#7) OR #6) OR #5) OR #4 Filters: Cancer
#7 Search pain*[Title/Abstract] Filters: Cancer
#6 Search Pain Measurement[MeSH Major Topic] Filters: Cancer
#5 Search Pain Management[MeSH Major Topic] Filters: Cancer
#4 Search pain[MeSH Terms] Filters: Cancer
#3 Search (#1) OR #2 Filters: Cancer
#2 Search ((fentanyl or phentanyl or fentora or durogesic or duragesic or fentanest or sublimaze or r‐4263 or r4263).[Title/Abstract]) Filters: Cancer
#1 Search Fentanyl[MeSH Terms] Filters: Cancer
Appendix 4. Assessing methodological quality
Validated scoring system (Jadad 1996):
Was the study described as randomised? (1 point)
Is the randomisation appropriate? (1 point)
Deduct one point if the method of randomisation is inappropriate
Was the study described as double blind?
Is the blinding appropriate?
Deduct one point if the method of blinding is inappropriate
Was there a description of withdrawals and dropouts?
Appendix 5. Results for individual studies
| Study ID | Measures of efficacy | Adverse events and withdrawals |
| Ahmedzai 1997 | Pain control successful: TDF 94/122 SRM 99/122 End of trial preference N = 136: 14 no preference 73 TDF 49 SRM P = 0.037 |
Withdrawals: 110/202 completed 41 withdrew due to AE, 6 withdrew consent due to AE Adverse events (denominator not reported): Abdominal pain: TDF 18, SRM 0 Constipation: TDF 6, SRM 15 Diarrhoea: TDF 35, SRM 7 Dyspnea: TDF 10, SRM 5 Nausea: TDF 32, SRM 23 Somnolence/drowsiness TDF 17, SRM 19 Sweating: TDF 12, SRM 5 Vomiting: TDF 18, SRM 18 Death 14 |
| Kongsgaard 1998 | Dose titration phase: Failure to complete: 28/138, mainly due to progression of underlying disease (4 deaths, 13 AEs not related to fentanyl, 11 other) Not randomised due to inadequate pain control: 15/138 Double‐blind phase: Withdrawal due to lack of efficacy: TDF 9/47 Placebo 13/48 Unexpectedly high placebo response rate reduced sensitivity to show fentanyl superior to placebo at 5% significance level No significant difference between treatment group requirements for morphine Investigator evaluation of trial medication ‘good' or 'excellent’: TDF 30 Placebo 23 |
Withdrawals: 13 adverse event withdrawals during the titration phase, none in double blind phase Adverse events: Constipation: 3% throughout study Nausea: 9% during dose titration (similar to morphine during stabilisation 11%), 4% during double blind phase, 6% during follow‐up 1 participant (TDF) reported severe treatment events (nausea, somnolence, vomiting – titration phase) No respiratory depression |
| Kress 2008 | Non‐inferiority shown: Upper 95% CI limits of mean difference in relative PI area under curve between FIT patch and standard opioid treatment were less than 10% for both intention to treat and per protocol populations Subgroup analysis showed similar non‐inferiority between FIT and Durogesic patch and FIT and oral morphine Scores for tolerability endpoints similar in treatment groups |
Withdrawals Withdrawal of consent: 10 Adverse events: 26 'Other reasons': 14 (referral to another hospital/hospitalisation (5), death/suicide (3/1), lost to follow up (2). 8 participants took < 50% assigned medication (5 FIT and 3 Durogesic) Adverse events: FIT 10%, Std 14% Nausea: FIT 16/117, Std 15/103 Vomiting: FIT 4/117, Std 13/103 Constipation: FIT 7/117, Std 5/103 Dry mouth: FIT 3/117, Std 0/103 Gastritis: FIT 2/117, Std 1/103 Abdominal pain: FIT 2/117, Std 0/103 Gastrointestinal haemorrhage: FIT 2/117, Std 0/103 Death: FIT 7 patients (6%), Std 12 patients (12%). No deaths were considered related to the study treatment |
| Mercadante 2008 | No difference between groups for: number of days to reach dose stabilisation number of dose changes during titration use of rescue medication use of laxatives pain intensity use of non‐opioid analgesics No important differences between groups for QoL scores, symptom intensity, and distress score Within groups, some symptoms increased during SRM and ME not TDF. Distress score significantly increased during first two weeks of ME but did not require discontinuation and there was no difference in consumption of drugs to manage opioid effects |
Withdrawals: Unexpected death: TDF 1, SRM 1, ME 0 Switched to other opioids (mainly due to AEs): TDF 5, SRM 5, ME 4 Radiotherapy: TDF 1, SRM 0, ME 1 Change in chemotherapy regime: TDF 0, SRM 2, ME 0 Bowel obstruction: TDF 1, SRM 1, ME 0 Cerebral haemorrhage: TDF 0, SRM 0, ME 1 Lost to follow‐up: TDF 4, SRM 3, ME 4 Protocol violation: TDF 0, SRM 1, ME 1 Withdrew consent: TDF 0, SRM 1, ME 1 Adverse events No important differences in symptom intensity between groups |
| Mystakidou 2005 | Pain measures improved in both groups throughout study: TDF > P/C (P < 0.05), mean data Mean satisfaction scores showed progressive improvement in both groups Increased medication dosage during study: TDF 6.1% P/C 95.8% |
Exclusions: TDF: 11 did not adhere to protocol from baseline, 5 had severe anaemia, 10 did not receive palliative radiotherapy, 3 had acute intestinal obstruction P/C: 9 did not adhere to protocol from baseline, 2 had severe anaemia Withdrawals: Uncontrolled pain ‐ TDF 4, P/C 5 Adverse effects ‐ 1 (group not specified) Death ‐ 7 (group not specified) Adverse events: Frequencies of side effects higher in P/C group, and generally highest at 72 hours: Nausea: TDF 16/201, P/C 22/221 Constipation: TDF 37/201, P/C 66/221 Sleep disturbance: TDF 37/201, P/C 40/221 Vomiting: TDF 13/201, P/C 3/221 Rash/pruritis: TDF 3/201, P/C 0/221 Sweating: TDF 9/201, P/C 2/221 |
| Oztürk 2008 | Mean NRS at 15 days: TDF 3 (range 0 to 3), from baseline of 6.5 (5 to 8) SRM 3 (range 0 to 3), from baseline of 7 (6 to 8) ADLs were the same in both groups |
Withdrawals: 2 participants did not use plasters correctly, 4 required chemotherapy (3 in each group) Constipation: TDF 6/22, SRM 14/22 |
| Pistevou‐Gompaki 2004 | Significant improvement in all measures at 3 months. Mean pain scores fell gradually during radiotherapy to maximum reduction at 7 weeks post‐irradiation in both groups, which was maintained. Mean VAS decreased from 7.0 to 1.1 (mild pain) with TDF, and from 8.3 to 4.3 (moderate pain) with P/C; P < 0.01 G‐BPI domains (global quality of life, pain, and functioning) gradually improved to maximum at 4 weeks post‐irradiation, which was maintained QoL improvement > with TDF (74/100) than P/C (29/100); P < 0.001 |
Withdrawals: TDF ‐ 2/13 ‐ one died from advanced lung cancer, other lost to follow‐up Adverse events: TDF 4/11 nausea and vomiting (mild) P/C 3/13 nausea (treated with antiemetics) |
| van Seventer 2003 | Mean scores for pain intensity, amount of trouble/bother, sleep, and degree of interference all improved from baseline at 7, 28 days and endpoint. No significant difference between groups Absence of interruption of daily activities: TDF 88%, SRM 63% P = 0.012 During first week of treatment TDF group required more breakthrough relief |
Withdrawals: Overall: TDF 18/67, SRM 38/64 Death: TDF 7/67, SRM 4/64 AE: TDF 3/67, SRM 23/64 Insufficient response: TDF 2/67, SRM 1/64 Subject asymptomatic/cured: TDF 1/67, SRM 0/64 Subject ineligible to continue trial: TDF 2/67, SRM 4/64 Withdrew consent: TDF 1/67, SRM 5/64 Other: TDF 2/67, SRM 1/64 Adverse events: TDF showed favourable tolerability Constipation at 1 week: TDF 27%, SRM 57% Presence of troublesome side effects did not change, but incidence of those occurring "quite a bit" and "very much" was less with TDF (14%) than SRM (36%) Nausea worse in SRM group at week one, but not at the end Drowsiness increased in both groups. Worse in SRM at 7 days, but no difference at the end Daytime sleepiness increased in both groups, but less in TDF No respiratory depression |
| Wong 1997 | No significant differences in degree of pain improvement between stabilisation and treatment phases either within or between treatment groups Little improvement seen in activity status after treatment Breakthrough pain: no significant difference between groups Transdermal fentanyl easier for those with nausea, vomiting, dysphagia |
Withdrawals: 3 poor analgesic effect, 2 died during study, 2 adverse effect of treatment and inability to obtain assessment information (group not given) Adverse events: Drowsiness: TDF 5, SRM 6 (improved but 2 TDF still had at end of treatment) Insomnia: significantly reduced in both groups Itching and skin rash: TDF 2 (improved later) Pre‐existing nausea and vomiting improved, significantly in TDF group During final phase of treatment: Nausea and vomiting: TDF 2/20, SRM 4/20 Constipation: TDF 5/20, SRM 10/20 Insomnia: TDF 5/20, SRM 1/20 Drowsiness: TDF 2/20, SRM 6/20 |
| Abbreviations: ADL ‐ activities of daily living; AE ‐ adverse event; FIT ‐ fentanyl investigational matrix patch; QoL ‐ quality of life; P/C ‐ paracetamol plus codeine; SRM ‐ sustained release morphine; std ‐ standard; VAS ‐ visual analogue scale | ||
Data and analyses
Comparison 1. Fentanyl versus sustained release morphine.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Constipation | 4 | 484 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.47, 0.78] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Ahmedzai 1997.
| Methods | Multicentre, randomised, open, two period cross‐over study: each period lasted 15 days with no washout between periods. Initial opioid dose calculated using manufacturers recommendations, with dose titration at start of each period to achieve pain control Setting: Palliative care centres, UK Assessed at baseline and 8, 16, 23, 31 days, and by daily patient diary |
|
| Participants | Adult cancer patients requiring strong opioid analgesia and receiving stable dose of morphine for at least 48 hours Life expectancy > 1 month N = 202 Mean age 62 years (range 18 to 89) M 112, F 90 |
|
| Interventions | Transdermal fentanyl patch (new patch every 72 hours) Sustained release oral morphine, given every 12 hours One treatment for 15 days followed immediately by other for 15 days. Immediate release morphine was used freely to titrate pain at the start of study and at cross‐over Where possible other medication remained unchanged, but other analgesics allowed: e.g. NSAIDs, permitted radiotherapy, nerve blocks |
|
| Outcomes | Sleep, rescue medication, drowsiness using VAS, daily diary Pain and mood using Memorial Pain Assessment Card (MPAC), twice daily QoL (self‐rated) using EORTC QLQ‐C30 Performance status (clinician rated) using WHO scale Treatment preference Adverse events |
|
| Notes | Oxford Quality Score: R1, DB0, W1. Total = 2/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open study |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open study |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Appears to be a completer analysis. "Patients who withdrew before the end of the study were included in the analysis to the fullest extent possible" |
| Size | Unclear risk | 50 to 200 participants per treatment arm |
Kongsgaard 1998.
| Methods | Multicentre, enriched enrolment, randomised withdrawal study: 7 day stabilisation phase, 15 day open label titration phase, and 9 day double blind, placebo controlled, parallel group phase Assessment by daily patient diary and clinical visits at trial entry, beginning and end of double blind period, and 3 month intervals for follow‐up |
|
| Participants | Adult cancer patients with pain caused by malignancy recurring after potentially curative therapy, not currently amenable to curative therapy. Requiring equivalent of 60 to 300 mg oral morphine daily, with acceptable toxicity and pain relief (pain no worse than moderate, assessed by investigator using 7‐point scale at end of stabilisation phase). Karnofsky performance > 50 Site of cancer: head and neck, prostate, colon, lung, breast, uterus, gastrointestinal, liver, other Titration phase: N = 138 (131 enrolled after stabilisation, 7 directly) Mean age 59 years (range 24 to 83) M 85, F 53 |
|
| Interventions | Stabilisation phase: oral morphine (≥60 mg to ≤ 300 mg daily) titrated to provide adequate pain control with acceptable adverse effects 15 day dose‐titration period: fixed conversion table used to convert morphine to fentanyl and titration to maintain adequate pain control with acceptable adverse effects. New patch applied every 72 hours 9 day double blind period using fentanyl or placebo at same dose as at end of titration period (median dose 50 μg/h) Rescue medication (rapid release morphine) available. Medication for concurrent illness continued |
|
| Outcomes | Withdrawals due to inadequate analgesia (patient required x2 mean daily dose of rescue morphine that was administered at end of open treatment phase, or if no rescue morphine required at that stage, when patient required > 50% of mean morphine dose administered during stabilisation period) Patient diary card: Pain intensity using 100 mm VAS, x2 daily Rescue medication, daily Well‐being using 100 mm VAS, x2 daily Clinical visit: Investigator assessment of pain intensity using 7‐point scale (no pain‐intolerable pain) Investigator global assessment of trial medication (excellent, good, moderate, poor) Adverse events |
|
| Notes | Oxford Quality Score: R1, DB1, W1. Total = 3/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Method not described |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Method not described |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | ITT analysis, but imputation method not described. Withdrawals ˜ 10% |
| Size | High risk | < 50 participants per treatment arm |
Kress 2008.
| Methods | Multicentre, randomised, open, parallel group study: 30 days of treatment plus 7 days follow‐up Assessment by daily patient diary and weekly clinic visits Aim to determine non‐inferiority and compare safety of new formulation patch (FIT) with standard formulation patch and oral morphine. Participants switched to FIT using standardised conversion ratio, based on previous 24 hour intake or 12.5 μg/h if opioid naïve; previous analgesics phased out Dose adjustment allowed throughout study to meet needs of individual participants ITT – participants who took at least one dose of medication |
|
| Participants | Adult cancer patients (in or out patients) with chronic cancer‐related pain requiring long term (> 30 days) strong (WHO Step 3) opioid treatment, either step up or rotation. Karnofsky score >50/100 at baseline N = 220 Mean age 63 (±11) years M 132, F 88 |
|
| Interventions | Fentanyl Improved Transdermal (FIT) patch, n = 117 Standard opioid treatment, n = 103 (65 transdermal fentanyl (Durogesic patch), 38 Oramorph) New patches applied every 72 hours, oramorph given every 12 hours Dose adjustment permitted if breakthrough pain became regular (upward) or if significant adverse events were experienced alongside adequate pain control and no rescue medication (downward) Other treatment continued, including radiotherapy and chemotherapy, and both pharmacological and non‐pharmacological pain‐modulating interventions. Rescue medication: morphine, administered as preferred by participant or investigator |
|
| Outcomes | Patient diary: Pain intensity using 0 to 10 numerical rating scale, daily Tolerability (constipation, nausea sleep disturbance, daytime drowsiness), using 4‐point ordinal scale (absent, mild, moderate, severe) Rescue medication Adverse events, serious adverse events Primary endpoint was relative area under the curve of PI expressed as a % maximum possible area under the curve |
|
| Notes | Oxford Quality Score: R1, DB0, W1. Total = 2/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Low risk | Interactive voice response system |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open study |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open study |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | This was not a true ITT analysis patients with missing values did not contribute to that analysis ‐ 16% for primary endpoint ‐ but losses to each group approximately the same |
| Size | Unclear risk | 50 to 200 participants per treatment arm |
Mercadante 2008.
| Methods | Multicentre, randomised, open, parallel group study: 4 weeks Fixed starting dose of study medication, adjusted to balance analgesia and adverse effects Assessment at baseline and weekly intervals |
|
| Participants | Adult cancer patients requiring strong opioids who had received opioids for mild to moderate pain, including tramadol and codeine at doses of at least 300 mg and 180 mg respectively without adequate analgesia. Expected survival > 3 months Breast cancer was the most frequent diagnosis (16 patients), and mixed nociceptive‐neuropathic syndromes (18 patients) the most dominant pain type N = 108 Mean age 59 years (range 18‐78) (completers) M 36, F 34 (completers) |
|
| Interventions | Transdermal fentanyl patch, initially 0.6 mg/day 25 μg/h, n = 36 Sustained release oral morphine, initially 60 mg/day, n = 36 Oral methadone, 15 mg/day in 3 divided doses, n = 36 Rescue medication: oral morphine at 1/6 daily 24 hour oral equivalent requirement Use of other medication permitted, including those for palliation of symptoms |
|
| Outcomes | Symptoms associated with opioid therapy (e.g. nausea, drowsiness, confusion) using 4‐point scale (not at all, slight, a lot, severe) Constipation using 4‐point scale (0 = 1 passage every 1 to 2 days, 1 = one passage every 3 to 4 days, 2 = one passage > 4 days, 3 = rectal measures) Distress score calculated from sum of symptom intensities Pain intensity using numerical rating scale (0 to 10) Time to achieve dose stabilisation Number of daily dose changes Opioid escalation index QoL using Spitzer QoL index (activity, daily life, health perceptions, social support, behaviour rated on Likert 3‐point scale (0 to 2) Cost |
|
| Notes | Oxford Quality Score: R2, DB0, W1. Total = 3/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "computer generated" |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open study |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open study |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Completer analysis |
| Size | High risk | < 50 participants per treatment arm |
Mystakidou 2005.
| Methods | Ransomised, open label, parallel group study: 2 months All participants underwent palliative radiotherapy before randomisation. Fixed starting dose of study medication, adjusted to patient requirements Assessment at baseline, 3, 7, 14, 28 days, and 2 months |
|
| Participants | Adult cancer patients with painful bony metastasis and moderate/severe chronic cancer pain requiring strong opioids Primary cancer location: lung, kidney/bladder, gastrointestinal, breast, unknown, other) Site of bony metastasis: thoracic spine, lumbar spine, cervical spine, thoracic and lumbar spine, pelvis, femur, scapula Other metastases: brain, gastrointestinal, lung, adrenal N = 460 (422 eligible) Mean age 61 (25 to 88) years (eligible) M 219, F 203 (eligible) |
|
| Interventions | Transdermal fentanyl, initially 25 μg/h every 72 hours, n = 201 Paracetamol 500 mg plus codeine 30 mg, to maximum of 4 times per day, n = 221 Fentanyl dose was increased when treatment satisfaction ≤ 2 and pain score ≥ 3 Fentanyl‐treated participants could receive paracetamol and codeine twice in first 12 hours after patch application, as rescue medication |
|
| Outcomes | Diary cards: Greek brief pain inventory (G‐BPI), 0 to 10 Overall treatment satisfaction, 1 to 4 (not at all satisfied, fairly satisfied, satisfied, completely satisfied) QoL using VAS, 0 to 10 (0 = high, 10 = low) European Collaborative Oncology Group status Adverse events |
|
| Notes | Oxford Quality Score: R1, DB0, W1. Total = 2/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open study |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open study |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Completer analysis |
| Size | Low risk | ≥ 200 participants per treatment arm (before withdrawals) |
Oztürk 2008.
| Methods | Randomised, open label, parallel group. Duration 15 days | |
| Participants | Lung cancer requiring WHO step 3 opioids for pain; 18 of fentanyl patients were treated in hospital, and 16 of morphine patients were treated in hospital, others were visited by doctors at home N = 50 Mean age 55 years (completers, range not stated) M/F not reported |
|
| Interventions | Transdermal fentanyl patch Sustained relief oral morphine Starting level: Participants requiring 200 to 400 mg tramadol used 25 μg/h TDF patches Participants requiring 500 to 600 mg oral tramadol used 50 μg/h TDF patches 120 mg slow release morphine Dose increased if inadequate response to maximum 100 mg/h TDF or 180 mg SRM (41% and 23% changed, two participants in each group increased dose twice) Rescue medication: both groups given subcutaneous morphine if pain ‘unbearable’ (NRS > 3) |
|
| Outcomes | Pain: NRS (0‐10) ADLs using ECOG Adverse events |
|
| Notes | Oxford Quality Score: R1, DB0, W1. Total = 2/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open study |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open study |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Completer analysis |
| Size | High risk | 25 participants per treatment arm |
Pistevou‐Gompaki 2004.
| Methods | Multicentre, randomised, open, parallel group study All participants received palliative radiotherapy (unclear whether before or during medication) Assessed at baseline (before radiotherapy), at 2‐weekly intervals during and after radiotherapy, for 3 months |
|
| Participants | Adult cancer patients with painful bony metastasis. Moderate/severe pain refractory to common analgesics, no previous strong opioids Primary cancer location (lung, prostate, breast, stomach/gallbladder, kidney, multiple myeloma, unknown); site of bony metastasis (thoracic spine, lumbar spine, cervical spine, thoracic and lumbar spine, pelvis, limbs, scapula); other metastases (brain, lymph, lung, liver) N = 26 (24 eligible) Age range 54 to 72 years M 19, F 7 |
|
| Interventions | Radiotherapy plus: Transdermal fentanyl 25 μg/hour, every 72 hours, n = 13 Paracetamol 500 mg plus codeine 30 mg, x4 daily, n = 13 3 fentanyl and 2 paracetamol plus codeine participants also received iv bisphosphonates |
|
| Outcomes | Pain intensity using VAS (0 to 10) QoL using Greek brief pain inventory (G‐BPI) 0 to 10 |
|
| Notes | Oxford Quality Score: R1, DB0, W1. Total = 2/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open study |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open study |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Imputation method not described |
| Size | High risk | < 50 participants per treatment arm |
van Seventer 2003.
| Methods | Multicentre, randomised, open, parallel group study. Duration 4 weeks Assessements by investigator and participant at baseline, 7 and 28 days. Participants also kept a daily diary |
|
| Participants | Adults with moderate‐severe cancer related pain requiring opioid treatment, with life expectancy ≥ 3 months. Participants could be opioid naïve or using opioids for mild‐to‐moderate pain before entry. Participants using opioids for moderate‐to‐severe pain in 30 days preceding study entry were excluded N = 131 Mean age 65 (±12) years M 85, F 46 |
|
| Interventions | Transdermal fentanyl, initially 25 μg/h every 72 hours, n = 67 (dose increments of 25 μg/h to achieve adequate pain control) Sustained release oral morphine, initially 30 mg every 12 hours, n = 64 (dose increments of 30% to 50% 12 hours after previous administration to achieve adequate pain control) Rescue medication: 10 mg severedol every 2 to 4 hours, as required Concomitant medication recorded |
|
| Outcomes | Pain control using Shortened Wisconsin brief pain inventory: 11‐point scale (0 = no, 10 = extreme), daily Global assessment of pain relief, sleep, interruption of daily activities and caregiver's activities, troublesome side effects using 4‐point scale (1 = not at all, 4 = very much) at start and 28 days Overall assessment using 11‐point scale (0 = very poor, 10 = very good) Constipation using questionnaire (bowel function normal, constipated, diarrhoeal) at start, 7 and 28 days Adverse events |
|
| Notes | Oxford Quality Score: R1, DB0, W1. Total = 2/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not adequately described but states "centrally randomised" |
| Allocation concealment (selection bias) | Unclear risk | Method not adequately described but states "centrally randomised" |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open study |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open study |
| Incomplete outcome data (attrition bias) All outcomes | High risk | LOCF imputation |
| Size | Unclear risk | 50 to 200 participants per treatment arm |
Wong 1997.
| Methods | Randomised, open, parallel group study. Duration 7 day stabilisation phase (if necessary), 14 day treatment phase Assessment during stabilisation, at start of treatment phase, and in immediate and final phases of treatment |
|
| Participants | Adult cancer patients with estimated survival time ≥ 2 months, and pain requiring oral morphine or equivalent ≤ 404 mg per day Site of primary cancer: head and neck, liver, cervix, pancreas, lung, kidney, bladder Metastatic sites: bone, lung, liver Pain not directly related to disease or treatment: fentanyl 9, morphine 5 Location of pain: back, abdomen, lower extremities, head/neck, spine Type of pain: Fentanyl: somatic 18, visceral 8, deafferentation 7 Morphine: somatic 18, visceral 7, deafferentation 6 N = 47 (40 completed) Mean age 59 years (range 30 to 79) M 29, F 11 (completers) |
|
| Interventions | During stabilisation phase, current opioid was converted to immediate release morphine hydrochloride (if necessary), which was then converted using standard charts for treatment phase Transdermal fentanyl patch, every 3 days, n = 20 (completers) Controlled‐release morphine, every 12 hours, n = 20 (completers) Rescue medication: immediate release morphine |
|
| Outcomes | Pain intensity using 5‐point scale (no pain, mild, moderate, severe, excruciating) Frequency of pain using 4‐point scale (no pain, occasional, always, persistent) Degree of pain improvement using 5‐point scale (no pain, obvious, moderate, little, no improvement) Profile of mood state as effected by the pain using 4‐point scale (no, mild, moderate, severe interference) Quality of sleep using 4‐point scale (normal, occasionally awakened by pain, always awakened by pain, insomnia) Activity status using Eastern Cooperative oncology group (ECOG) 5‐point scale (0 = fully active, 4 = completely disabled) Use of rescue medication Patient satisfaction Treatment preference Adverse events |
|
| Notes | Oxford Quality Score: R1, DB0, W0 (withdrawals not reported per treatment arm). Total = 1/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not described |
| Allocation concealment (selection bias) | Unclear risk | Method not described |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Open study |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Open study |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Completer analysis |
| Size | High risk | < 50 participants per treatment group |
DB ‐ double blind; F ‐ female; FIT ‐ fentanyl investigational matrix patch; M ‐ male; N ‐ number of participants in study; n ‐ number of participants in treatment arm; QoL ‐ quality of life; R ‐ randomised; VAS ‐ visual analogue scale; W ‐ withdrawals
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Ergenoglu 2010 | Pain not due to cancer |
| Sarhan 2009 | Conference abstract |
| Wirz 2009 | Not a randomised controlled trial |
Contributions of authors
All authors contributed to writing the protocol. GH and SD carried out searches, study selection, data extraction, and analyses. All authors were involved in interpretation and writing the review. RAM and PW acted as arbitrators in the event of disagreement.
Sources of support
Internal sources
-
Oxford Pain Relief Trust, UK.
General institutional support
External sources
No sources of support supplied
Declarations of interest
RAM and SD have received research support from charities, government, and industry sources at various times. RAM has consulted for various pharmaceutical companies, and has received lecture fees from pharmaceutical companies related to analgesics and other healthcare interventions. PW and GH have no relevant interests to declare.
Stable (no update expected for reasons given in 'What's new')
References
References to studies included in this review
Ahmedzai 1997 {published data only}
- Ahmedzai S, Brooks D. Transdermal fentanyl versus sustained‐release oral morphine in cancer pain: preference, efficacy, and quality of life. The TTS‐Fentanyl Comparative Trial Group. Journal of Pain and Symptom Management 1997;13(5):254‐61. [DOI: 10.1016/S0885-3924(97)00082-1] [DOI] [PubMed] [Google Scholar]
Kongsgaard 1998 {published data only}
- Kongsgaard UE, Poulain P. Transdermal fentanyl for pain control in adults with chronic cancer pain. European Journal of Pain 1998;2(1):53‐62. [DOI] [PubMed] [Google Scholar]
Kress 2008 {published data only}
- Kress HG, Laage D, Hoerauf KH, Nolte T, Heiskanen T, Petersen R, et al. A randomized, open, parallel group, multicenter trial to investigate analgesic efficacy and safety of a new transdermal fentanyl patch compared to standard opioid treatment in cancer pain. Journal of Pain and Symptom Management 2008;36(3):268‐79. [DOI: 10.1016/j.jpainsymman.2007.10.023] [DOI] [PubMed] [Google Scholar]
Mercadante 2008 {published data only}
- Mercadante S, Porzio G, Ferrera P, Fulfaro F, Aielli F, Verna L, et al. Sustained‐release oral morphine versus transdermal fentanyl and oral methadone in cancer pain management. European Journal of Pain 2008;12(8):1040‐6. [DOI: 10.1016/j.ejpain.2008.01.013] [DOI] [PubMed] [Google Scholar]
Mystakidou 2005 {published data only}
- Mystakidou K, Katsouda E, Kouloulias V, Kouvaris J, Tsiatas M, Vlahos L. Comparison of transdermal fentanyl with codeine/paracetamol, in combination with radiotherapy, for the management of metastatic bone pain. Journal of Opioid Management 2005;1(4):204‐10. [DOI] [PubMed] [Google Scholar]
Oztürk 2008 {published data only}
- Oztürk T, Karadibak K, Catal D, Cakan A, Tugsavul F, Cirak K. Comparison of TD‐fentanyl with sustained‐release morphine in the pain treatment of patients with lung cancer. Agri 2008;20(3):20‐5. [PubMed] [Google Scholar]
Pistevou‐Gompaki 2004 {published data only}
- Pistevou‐Gompaki K, Kouloulias VE, Varveris C, Mystakidou K, Georgakopoulos G, Eleftheriadis N, et al. Radiotherapy plus either transdermal fentanyl or paracetamol and codeine for painful bone metastases: a randomised study of pain relief and quality of life. Current Medical Research and Opinion 2004;20(2):159‐63. [DOI: 10.1185/030079903125002829] [DOI] [PubMed] [Google Scholar]
van Seventer 2003 {published data only}
- Seventer R, Smit JM, Schipper RM, Wicks MA, Zuurmond WW. Comparison of TTS‐fentanyl with sustained‐release oral morphine in the treatment of patients not using opioids for mild‐to‐moderate pain. Current Medical Research and Opinion 2003;19(6):457‐69. [DOI: 10.1185/030079903125002045] [DOI] [PubMed] [Google Scholar]
Wong 1997 {published data only}
- Wong JO, Chiu GL, Tsao CJ, Chang CL. Comparison of oral controlled‐release morphine with transdermal fentanyl in terminal cancer pain. Acta Anaesthesiologica Sinica 1997;35(3):25‐32. [PubMed] [Google Scholar]
References to studies excluded from this review
Ergenoglu 2010 {published data only}
- Ergenoglu P, Ozbek H, Gunduz M, Isik G. Comparison of the analgesic efficacy of intravenous morphine infusion and transdermal fentanyl in oncology patients with mucositis [Mukozitli onkoloji hastalarinda intravenoz morfin infuzyonu ve transdermal fentanilin analjezik etkinliginin karsilastirilmasi]. Anatolian Journal of Clinical Investigation 2010;4(3):134‐40. [Google Scholar]
Sarhan 2009 {published data only}
- Sarhan T, Doghem M. A comparison of two trans‐dermal drug delivery systems; buprenorphine and fentanyl for chronic cancer pain management. European Journal of Pain. 6th Congress of the European Federation of IASP Chapters: Pain in Europe 6th, EFIC Lisbon Portugal. 2009; Vol. 13:S199.
Wirz 2009 {published data only}
- Wirz S, Wittmann M, Schenk M, Schroeck A, Schaefer N, Mueller M, et al. Gastrointestinal symptoms under opioid therapy: a prospective comparison of oral sustained‐release hydromorphone, transdermal fentanyl, and transdermal buprenorphine. European Journal of Pain 2009;13(7):737‐43. [DOI: 10.1016/j.ejpain.2008.09.005] [DOI] [PubMed] [Google Scholar]
Additional references
Cachia 2011
- Cachia E, Ahmedzai SH. Transdermal opioids for cancer pain. Current Opinion in Supportive and Palliative Care 2011;5(1):15‐9. [DOI: 10.1097/SPC.0b013e3283437a39] [DOI] [PubMed] [Google Scholar]
Cancer Research UK
- Cancer Research UK. Cancer incidence for all cancers combined. http://info.cancerresearchuk.org/cancerstats/incidence/all‐cancers‐combined/ [Accessed 22 May 2013].
Clark 2004
- Clark AJ, Ahmedzai SH, Allan LG, Camacho F, Horbay GL, Richarz U, et al. Efficacy and safety of transdermal fentanyl and sustained‐release oral morphine in patients with cancer and chronic non‐cancer pain. Current Medical Research and Opinion 2004;20(9):1419‐28. [DOI: 10.1185/030079904X2114] [DOI] [PubMed] [Google Scholar]
Cleary 2007
- Cleary JF. The pharmacologic management of cancer pain. Journal of Palliative Medicine 2007;10(6):1369‐94. [DOI: 10.1089/jpm.2007.9842] [DOI] [PubMed] [Google Scholar]
Cook 1995
- Cook RJ, Sackett DL. The number needed to treat: a clinically useful measure of treatment effect. BMJ 1995;310(6977):452‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Dworkin 2008
- Dworkin RH, Turk DC, Wyrwich KW, Beaton D, Cleeland CS, Farrar JT, et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. Journal of Pain 2008;9(2):105‐21. [DOI: 10.1016/j.jpain.2007.09.005] [DOI] [PubMed] [Google Scholar]
Electronic medicines compendium
- Durogesic® DTrans. http://www.medicines.org.uk/EMC/medicine/17088/ (Accessed 22 May 2013).
Hadley 2009
- Hadley G, Derry S, Moore RA, Wee B. Can observational studies provide a realistic alternative to randomized controlled trials in palliative care?. Journal of Pain & Palliative Care Pharmacotherapy 2009;23(2):106‐13. [DOI: 10.1080/15360280902899921] [DOI] [PubMed] [Google Scholar]
Heiskanen 2009
- Heiskanen T, Mätzke S, Haakana S, Gergov M, Vuori E, Kalso E. Transdermal fentanyl in cachectic cancer patients. Pain 2009;144(1‐2):218‐22. [DOI: 10.1016/j.pain.2009.04.012] [DOI] [PubMed] [Google Scholar]
Higgins 2011
- Altman DG, Antes G, Gøtzsche P, Higgins JPT, Jüni P, Lewis S, et al. Assessing risk of bias in included studies. In: Higgins JPT, Altman DG, Sterne JAC editor(s). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 (updated March 2011). Available from www.cochrane‐handbook.org. The Cochrane Collaboration, 2011. [Google Scholar]
Jadad 1996
- Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary?. Controlled Clinical Trials 1996;17(1):1‐12. [DOI: 10.1016/0197-2456(95)00134-4] [DOI] [PubMed] [Google Scholar]
Jeal 1997
- Jeal W, Benfield P. A review of its pharmacological properties and therapeutic efficacy in pain control. Drugs 1997;53(1):109‐38. [DOI] [PubMed] [Google Scholar]
Kornick 2003
- Kornick CA, Santiago‐Palma J, Moryl N, Payne R, Obbens EA. Benefit‐risk assessment of transdermal fentanyl for the treatment of chronic pain. Drug Safety 2003;26(13):951‐73. [DOI] [PubMed] [Google Scholar]
Koyyalagunta 2012
- Koyyalagunta D, Bruera E, Solanki DR, Nouri KH, Burton AW, Toro MP, et al. A systematic review of randomized trials on the effectiveness of opioids for cancer pain. Pain Physician 2012;15(3 Suppl):ES39‐58. [PubMed] [Google Scholar]
L'Abbé 1987
- L'Abbé KA, Detsky AS, O'Rourke K. Meta‐analysis in clinical research. Annals of Internal Medicine 1987;107(2):224‐33. [DOI] [PubMed] [Google Scholar]
Lehmann 1992
- Lehmann KA, Zech D. Transdermal fentanyl: clinical pharmacology. Journal of Pain and Symptom Management 1992;7 3 Suppl:S8‐16. [DOI] [PubMed] [Google Scholar]
Marinangeli 2007
- Marinangeli F, Ciccozzi A, Aloisio L, Colangeli A, Paladini A, Bajocco C, et al. Improved cancer pain treatment using combined fentanyl‐TTS and tramadol. Pain Pract 2007;7(4):307‐12. [DOI: 10.1111/j.1533-2500.2007.00155.x] [DOI] [PubMed] [Google Scholar]
McQuay 1998
- McQuay H, Moore R. An evidence‐based resource for pain relief. An evidence‐based resource for pain relief. Oxford: Oxford University Press, 1998. [ISBN: 0‐19‐263048‐2] [Google Scholar]
Moore 1982
- Moore RA, Bullingham RE, McQuay HJ, Hand CW, Aspel JB, Allen MC, et al. Dural permeability to narcotics: in vitro determination and application to extradural administration. British Journal of Anaesthetics 1982;54(10):1117‐28. [DOI] [PubMed] [Google Scholar]
Moore 1998
- Moore RA, Gavaghan D, Tramèr MR, Collins SL, McQuay HJ. Size is everything ‐ large amounts of information are needed to overcome random effects in estimating direction and magnitude of treatment effects. Pain 1998;78(3):209‐16. [DOI: 10.1016/S0304-3959(98)00140-7] [DOI] [PubMed] [Google Scholar]
Moore 2010
- Moore RA, Moore OA, Derry S, Peloso PM, Gammaitoni AR, Wang H. Responder analysis for pain relief and numbers needed to treat in a meta‐analysis of etoricoxib osteoarthritis trials: bridging a gap between clinical trials and clinical practice. Annals of the Rheumatic Diseases 2010;69(2):374‐9. [DOI: 10.1136/ard.2009.107805] [DOI] [PMC free article] [PubMed] [Google Scholar]
Morris 1995
- Morris JA, Gardner MJ. Calculating confidence intervals for relative risk, odds ratios and standardised ratios and rates. In: Gardner MJ, Altman DG editors editor(s). Statistics with Confidence ‐ Confidence Intervals and Statistical Guidelines. London: BMJ Books, 1995:50‐63. [DOI] [PMC free article] [PubMed] [Google Scholar]
Muijsers 2001
- Muijsers RB, Wagstaff AJ. Transdermal fentanyl: an updated review of its pharmacological properties and therapeutic efficacy in chronic cancer pain control. Drugs 2001;61(15):2289‐307. [DOI] [PubMed] [Google Scholar]
RevMan 2011
- The Nordic Cochrane Centre. The Cochrane Collaboration. Review Manager (RevMan). 5.1. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2011. [Google Scholar]
Tassinari 2008
- Tassinari D, Sartori S, Tamburini E, Scarpi E, Raffaeli W, Tombesi P, et al. Adverse effects of transdermal opiates treating moderate‐severe cancer pain in comparison to long‐acting morphine: a meta‐analysis and systematic review of the literature. Journal of Palliative Medicine 2008;11(3):492‐501. [DOI: 10.1089/jpm.2007.0200] [DOI] [PubMed] [Google Scholar]
Tassinari 2011
- Tassinari D, Drudi F, Rosati M, Maltoni M. Transdermal opioids as front line treatment of moderate to severe cancer pain: a systemic review. Palliative Medicine 2011;25(5):478‐87. [DOI: 10.1177/0269216311404274] [DOI] [PubMed] [Google Scholar]
Tramèr 1997
- Tramèr MR, Reynolds DJM, Moore RA, McQuay HJ. Impact of covert duplicate results on meta‐analysis: a case study. BMJ 1997;315(7109):635‐40. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wiffen 2013
- Wiffen PJ, Wee B, Moore RA. Oral morphine for cancer pain. Cochrane Database of Systematic Reviews 2013, Issue 7. [DOI: 10.1002/14651858.CD003868.pub3] [DOI] [PubMed] [Google Scholar]