
Figure 1. Illustration of quantitative measures of MEPG and TM perforation conditions.
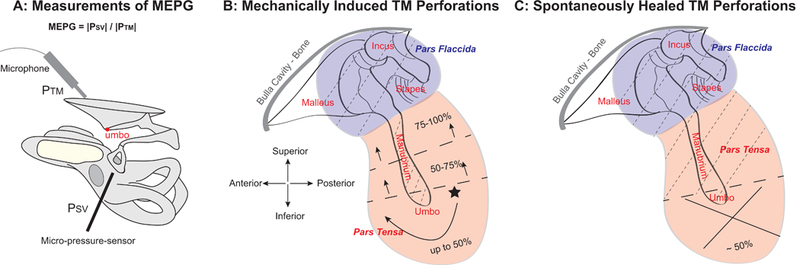
(A) Experimental approach for simultaneous measurements of PTM and PSV using an ultrasound Sokolich probe-tube microphone and a micro-pressure sensor positioned close to the TM and in the SV next to the stapes, respectively. ME pressure gain was defined as MEPG = |PSV| / |PTM|. PTM: pressure at the TM; PSV: pressure in the SV next to the stapes.; SV: scala vestibuli. (B) Diagram of mechanically induced TM perforations re size and location. The initial perforation was made at a location in the inferior pars tensa (star) using a 200-μm diameter sterilized pin, and was then subsequently enlarged to the desired size, i.e., ~ <1/8 (10%), 1/4 (25%), 1/2 (50%), 3/4 (75%), and 100%, by carefully expanding the edges of the existing perforation clockwise until the pars tensa was completely removed, leaving only the pars flaccida, the TM directly on top of the manubrium, and the ossicular chain intact. (C) Diagram of a ~50% TM perforation at the inferior location of the pars tensa, which spontaneously-healed up to 4 weeks. Dashed lines in panels B & C indicate areas of the TM that were left intact.