

Abstract
Background
Schönlein-Henoch purpura is a systemic vasculitis that affects vessels of a small caliber and rarely reported in the literature.
Case presentation
We report on a 35-year-old woman who developed palpable purpura with necrotizing cutaneous lesions on the lower limbs at 27 weeks of gestation. She also complained of epigastric pain and arthralgias. Histologic examination of a skin biopsy showed leukocytoclastic vasculitis with intravascular fibrin thrombi. The direct immunofluorescence analysis evidenced vascular deposits of IgA and C3 in the upper and mid-dermis. These findings were consistent with Schönlein-Henoch purpura. There was no evidence of renal involvement or placental dysfunction. The patient was treated with low-dose oral corticosteroids and a healthy infant was delivered by cesarean section. Examination of the placenta and the navel string disclosed no signs of vasculitis or infarction.
Conclusions
Schönlein-Henoch purpura is rarely reported in pregnancy. Treatment with orally administred corticosteroids may lead to a beneficial outcome for mother and newborn.
Background
Schönlein-Henoch purpura (SHP) is a systemic vasculitis that affects vessels of a small caliber [1]. The vascular purpura is usually confined to the lower limbs and is associated, at varying degrees, with joint, gastrointestinal and renal involvement [2].
In 1990, the American College of Rheumatology defined SHP by the presence of 2 ore more of the following criteria: age of disease onset (20 years or younger); palpable purpura; acute abdominal pain and granulocytic infiltration in the walls of arterioles or venules [3]. Focusing on the pathogenic role of IgA immune complexes in SHP, the Chapel Hill Consensus Group view the diagnosis as a small vessel vasculitis with predominant IgA vascular deposits [4]. SHP was first defined and is more commonly reported in children. There is a peak incidence between 2 and 5 years of age. Boys are more frequently affected. The incidence of SHP in the 2 to 14-year-old population is about 14 cases out of 100 000 per year [5]. The onset of SHP during pregnancy is very rare. Using an electronic literature research of MEDLINE and the National Library of Medicine PubMed we found case reports including patients with SHP in pregnancy exclusively in Journals for gynecology, internal medicine, pathology, pediatric and general medicine respectively, from 1976 to the present. Therefore, we report on a patient who developed SHP at 27 weeks of gestation with successful outcome for mother and child.
Case presentation
A 35-year-old unipara in the 31st week of gestation was admitted with a 4 week history of purpura on the legs. She also complained of epigastric pain and arthralgias, mainly in the knees.
Examination revealed crops of non tender palpable purpura on the legs, 1 to 3 mm in diameter (Fig 1). On the anterior aspects of the lower legs, the lesions subsequently coalesced to large plaques with a necrotic ulcerating center. A few scattered purpuric lesions were present on the abdomen.
Figure 1.

Numerous lesions of palpable purpura on the legs.
Biopsy of a skin lesion showed leukocytoclastic vasculitis (Fig 2 and Fig 3) with intravascular fibrin thrombi. The direct immunofluorescence analysis evidenced vascular deposits of IgA and C3 in the upper and mid-dermis. These findings, together with the gastrointestinal and articulary symptoms, led to the diagnosis of Schönlein-Henoch purpura.
Figure 2.
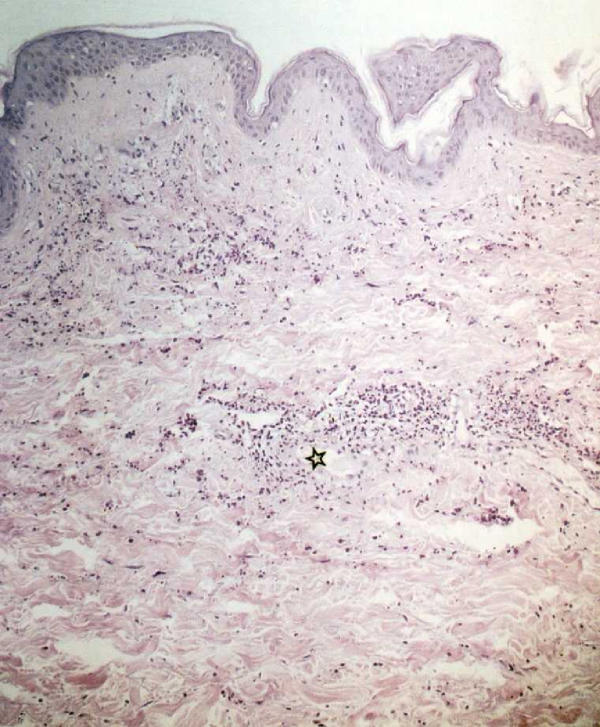
Leucocytoclastic vasculitis in the upper and mid-dermis. Asterisk marks the area of higher magnification (Fig 2b).
Figure 3.
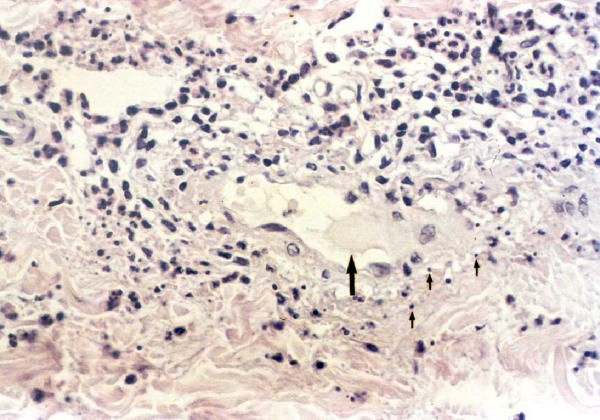
Leucocytoclastic vasculitis. Fibrin thrombi (large arrow) in the lumen of the vessel featuring a destroyed wall. Note the nuclear dust in a perivascular arrangement (small arrows).
Laboratory data were: red blood cell count 3,14 T/l, hemoglobin 9,8 g/dl, hematocrit 29,1%, white blood cell count 9,96 G/l, platelets 236 G/l, ESR 84/94 mm, serum creatinine 0,73 mg/dl and urea 7 mg/dl. Liver parameters and electrolytes were within normal range. Repeated urinanalysis showed no proteinuria or haematuria. Stool guaiacs were repeatedly negative.
Findings from the following tests were negative or within normal range: antinuclear antibodies, ANCA, C3, C4, antiphospholipid antibodies, serum immunoglobulin A, M, and G respectively, ASLO, virus serologies including hepatitis A, B and C. The circulating immuncomplexes were slightly raised (1,89 μg/ml, normal < 1,5 μg/ml). The gynecological examination showed an ultrasound-estimated gestation age of 31 weeks with a normal blood flow in the umbilical artery. The patient's blood pressure ranged from 100/70 to 120/80 mm Hg. Because of the necrotizing cutaneous lesions, treatment with low-dose oral corticosteroids (methylprednisolon 20 mg/day, i.e. 0,25 mg/kg body weight) was started. The lesions rapidly resolved and the corticosteroid dosage was tapered off progressively. After one month, treatment was stopped. Subsequent antepartum course was unremarkable. Repeated controls of kidney function and blood pressure showed normal results. At 38 weeks of gestation, a healthy male infant weighting 4100 g was delivered by cesarean section.
Histologic examination of the placenta and the navel string showed no vasculitis or infarction (Fig 4). Direct immunofluorescence did not evidence deposits of immunoreactants.
Figure 4.
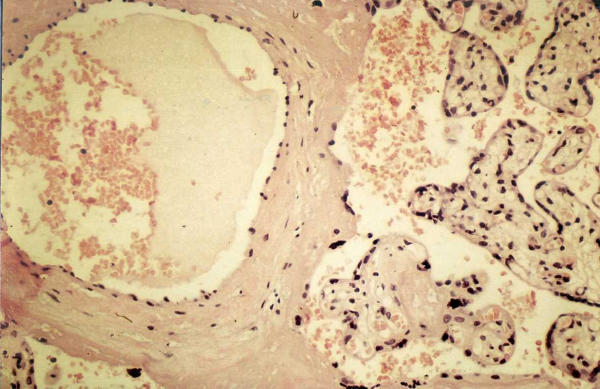
Placenta. Regular morphology of the placenta tissue without evidence of an inflammatory process.
Conclusions
Schönlein-Henoch purpura is a distinctive clinical syndrome. The skin lesions consist of recurrent purpuric papules, sometimes necrotizing, on the lower limbs. Spread of the rash to the trunk seems to be a predictive factor for renal involvement [6]. Initial symptoms may be accompanied by fever. Histological examination discloses leukocytoclastic vasculitis in the upper and mid-dermis. The direct immunofluorescence analysis of fresh lesions shows deposits of IgA and C3 in the capillary walls [7]. In older lesions, these immunoreactants may lack.
Arthralgias occur in up to two thirds of patients, usually affecting knees and ankles. Arthritis is rarely observed [8]. Gastrointestinal symptoms are frequent, appear usually at the beginning of the disease and last for a few days. They include colicky pain, nausea, vomiting, diarrhea, constipation and occult or gross gastrointestinal bleeding. Endoscopic examination discloses an erosive-haemorrhagic gastroenteritis, most often in the duodenum [9]. During the acute course of SHP, neurological symptoms may occur. Headache seems to be the most frequent symptom, convulsions are rare [10]. The reported incidence of nephritis associated with SHP varies according to the population studied. Renal involvement occurs in 25 to 50% of children. The glomerulonephritis usually leads to proteinuria and microhaematuria.
More rarely, a nephritic syndrome, macrohaematuria or arterial hypertension appear [11]. Glomerular changes consist of segmental and focal mesangial and/or endothelial proliferation and diffuse mesangial IgA deposits. Although acute renal failure is rare, end-stage renal disease may develop after a long latency period of up to 20 years after diagnosis of SHP [12]. This indicates that careful clinical and laboratory supervision is necessary even after complete healing of skin lesions. If the kidneys are spared, prognosis of SHP is excellent. Relapses of purpura, abdominal pain and arthralgias occur over 3 to 6 weeks before resolution of the disease.
SHP in adulthood differs from the pediatric form of the disease. Adults have more pronounced and chronic skin lesions [13] and renal involvement is more frequent and severe than in childhood [14]. However, long term outcome of SHP seems equally good in patients of both age groups [6,14].
Occurrence of SHP during pregnancy is exceptional. To the best of our knowledge, nine cases have previously been reported. Four patients were already known to have SHP before pregnancy [15-18]. Three woman developed SHP for the first time during gestation, at 11, 17 and 23 weeks respectively [19-21]. In two patients, diagnosis was made in the post-partum period [22,23].
Symptomatology of SHP in pregnant woman has no specific characteristics. Diagnosis may be difficult when renal, articular or gastrointestinal involvement preceed the cutaneous manifestations since many aspects of SHP may masquerade as preeclampsia or eclampsia, especially hypertension, nephrotic syndrome, abdominal pain, headache and convulsions.
The effect of pregnancy on the course of preexistant SHP remains to be evaluated. Analysis of the four observations reported in the literature shows: aggravation of the disease in two patients [15,17], diminution of proteinuria in one patient [16] and total disparition of symptoms in one patient [18]. The only obstetrical complication of SHP related in the literature is pregnancy-induced hypertension and its possible consequences (preeclampsia, eclampsia). If kidneys are spared, obstetrical prognosis is good. There is probably no risk of IgA vasculitis in the fetus as these immunoglobulins cannot cross the normal placenta. Examination of the placenta in one case showed no vasculitis or infarction [17] and this observation was confirmed in our patient.
The pathogenesis of SHP remains poorly understood. The similarity of the histologic findings in SHP to those of Arthus reaction suggest an immune-complex mediated disorder [24]. It is postulated that various antigenic stimuli cause elevation of circulating IgA and that complement activation leads to necrotizing vasculitis. SHP has been reported after bacterial infections (β-hemolytic Streptococcus, Legionella, Salmonella, Helicobacter pylori, etc) [25,26], viral infections (Hepatitis A and B, EBV, Parvovirus, etc) [27,28], vaccinations (influenza) [29] and intake of drugs (Penicillin, acetylsalicylic acid, enalapril, etc) [30,31].
The efficacy of corticosteroids and immunsuppressants (azathioprine, cyclophosphamide) in the treatment of SHP is subject to controversy, especially when the kidneys are involved [32]. Some cases of SHP were successfully treated by dapsone or plasmapheresis [17,33]. Little experience exists concerning treatment of SHP during pregnancy, although corticosteroids and plasmapheresis have been used.
Abbreviations
Schönlein-Henoch purpura: SHP
Competing interests
None declared
Acknowledgments
Acknowledgements
Written consent was obtained from the patient for publication of the patient's details. We acknowledge the excellent technical assistance of Barbara Brückler.
Contributor Information
Robert Feldmann, Email: fer@der.khl.magwien.gv.at.
Walter Rieger, Email: riw@der.khl.magwien.gv.at.
Paul G Sator, Email: sap@der.khl.magwien.gv.at.
Friedrich Gschnait, Email: gsf@der.khl.magwien.gv.at.
Friedrich Breier, Email: brf@der.khl.magwien.gv.at.
References
- Jennette CJ, Milling DM, Falk RJ. Vasculitis affecting the skin. Arch Dermatol. 1994;130:899–906. [PubMed] [Google Scholar]
- Piette WW. What is Schönlein-Henoch purpura and why should we care ? Arch Dermatol. 1997;133:515–518. [PubMed] [Google Scholar]
- Mills JA, Michel BA, Bloch DA, Calabrese LH, Hunder GG, Arend WP, Edworthy SM, Fauci AS, Leavitt RY, Lie JT, Lightfoot RW, Jr, Masi AT, McShane DJ, Stevens MB, Wallace SL, Zvaifler NJ. The American College of Rheumatology 1990 criteria for the classification of Henoch-Schönlein purpura. Arthritis Rheum. 1990;33:1114–1121. doi: 10.1002/art.1780330809. [DOI] [PubMed] [Google Scholar]
- Jennette JC, Falk RJ, Andrassy K, Bacon PA, Churg J, Gross WL, Hagen EC, Hoffman GS, Hunder GG, Kallenberg CGM, McCluskey RT, Sinico RA, Rees AJ, van Es LA, Waldherr R, Wiik A. Nomenclature of systemic vasculitides. Arthritis Rheum. 1994;37:187–192. doi: 10.1002/art.1780370206. [DOI] [PubMed] [Google Scholar]
- Nielsen HA. Epidemiology of Schönlein-Henoch purpura. Acta Pathol Scand. 1988;77:125–131. doi: 10.1111/j.1651-2227.1988.tb10610.x. [DOI] [PubMed] [Google Scholar]
- Tancrede-Bohin E, Ochonisky S, Vignon-Pennamen MD, FlageuI B, Morel P, Rybojad M. Schönlein-Henoch purpura in adult patients. Arch Dermatol. 1997;133:438–442. doi: 10.1001/archderm.133.4.438. [DOI] [PubMed] [Google Scholar]
- Helander SD, De Castro FR, Gibson LE. Henoch-Schönlein purpura: clinicopathologic correlation of cutaneous vascular IgA deposits and the relationship to leukocytoclastic vasculitis. Acta Derm Venereol. 1995;75:125–129. doi: 10.2340/0001555575125129. [DOI] [PubMed] [Google Scholar]
- Cream JJ, Gumpel JM, Peachy RDG. Schoenlein-Henoch purpura in the adult: a study of 77 adults with anaphylactoid or Schoenlein-Henoch purpura. QJ Med. 1970;39:461–484. [PubMed] [Google Scholar]
- Vogt M, Maier M, Benz Z, Kaufmann V, Riemann JF. Schönlein-Henoch-Syndrom mit schwerer Abdominalbeteiligung beim Erwachsenen. Dtsch Med Wschr. 1996;121:871–875. doi: 10.1055/s-2008-1043081. [DOI] [PubMed] [Google Scholar]
- Ostergaard JR, Storm K. Neurological manifestations of Schönlein-Henoch purpura. Acta Paediatr Scand. 1992;80:339–342. doi: 10.1111/j.1651-2227.1991.tb11859.x. [DOI] [PubMed] [Google Scholar]
- Schmaldienst S, Winkler S, Breiteneder S, Hörl WH. Severe nephrotic syndrome in a patient with Schönlein-Henoch purpura: complete remission after cyclosporin. Nephrol Dial Transplant. 1997;12:790–792. doi: 10.1093/ndt/12.4.790. [DOI] [PubMed] [Google Scholar]
- Goldstein AR, White RHR, Akuse R, Chantler C. Long term follow-up of childhood Henoch-Schönlein nephritis. Lancet. 1992;339:280–282. doi: 10.1016/0140-6736(92)91341-5. [DOI] [PubMed] [Google Scholar]
- Michel BA, Hunder GG, Bloch DA, Calabrese LH. Hypersensitivity vasculitis and Henoch-Schönlein purpura: a comparison between the 2 disorders. J Rheumatol. 1992;19:721–728. [PubMed] [Google Scholar]
- Blanco R, Martinez-Taboada VM, Rodriguez-Valverde V, Garcia-Fuentes M, Gonzalez-Gay MA. Henoch-Schönlein purpura in adulthood and Childhood. Arthritis Rheum. 1997;40:859–864. doi: 10.1002/art.1780400513. [DOI] [PubMed] [Google Scholar]
- Plauche WC. Henoch-Schönlein (anaphylactoid) nephropathy in pregnancy. Obstet Gynecol. 1980;56:515–517. [PubMed] [Google Scholar]
- Ray M, Posen GA. Henoch-Schönlein purpura in pregnancy. Can Med Assoc J. 1985;132:1385–1386. [PMC free article] [PubMed] [Google Scholar]
- Joseph G, Holtman JS, Kosfeld RE, Blodgett WA, Liu YK. Pregnancy in Henoch-Schönlein purpura. Am J Obstet Gynecol. 1987;157:911–912. doi: 10.1016/s0002-9378(87)80087-x. [DOI] [PubMed] [Google Scholar]
- Merill J, Lahita RG. Henoch-Schönlein purpura remitting in pregnancy and during sex steroid therapy. Br J Rheumatol. 1994;33:586–588. doi: 10.1093/rheumatology/33.6.586. [DOI] [PubMed] [Google Scholar]
- McCoy MJ. Henoch-Schönlein purpura and pregnancy. Am J Obstet Gynecol. 1981;141:469–470. doi: 10.1016/0002-9378(81)90616-5. [DOI] [PubMed] [Google Scholar]
- Siroty R. Case report: Henoch-Schönlein purpura in pregnancy. J Med Soc J. 1985;82:535–536. [PubMed] [Google Scholar]
- Ekoukou D, Karaoui B, Bazin C. Purpura rhumatoide (ou syndrome de Schönlein-Henoch) et grossesse. J Gynecol Obstet Biol Reprod (Paris) 1997;26:197–201. [PubMed] [Google Scholar]
- Wilks RL, Abdella TN, Alfano CA. Henoch-Schönlein purpura associated with eclampsia. J Reprod Med. 1993;38:645–646. [PubMed] [Google Scholar]
- Miyata M, Kumakawa H, Funabashi Y, Suenaga K, Hanzawa S, Takahashi M, Ogata M, Kasukawa R. Henoch-Schönlein purpura associated with pregnancy in a patient with chronic thyroiditis. Fukushima J Med Sci. 1994;40:45–49. [PubMed] [Google Scholar]
- Lie JT. Nomenclature and classification of vasculitis: plus ca change, plus c'est la même chose. Arthritis Rheum. 1994;37:181–186. doi: 10.1002/art.1780370205. [DOI] [PubMed] [Google Scholar]
- Bull PW, Scott JT, Breathnach SM. Henoch-Schoenlein purpura associated with legionnaires' disease. Br Med J Clin Res Ed. 1987;294:220. doi: 10.1136/bmj.294.6566.220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reinauer S, Megahed M, Goerz G, Ruzicka T, Borchard F, Susanto F, Reinauer H. Schönlein-Henoch purpura associated with gastric Helicobacter pylori infection. J Am Acad Dermatol. 1995;33:876–879. doi: 10.1016/0190-9622(95)90426-3. [DOI] [PubMed] [Google Scholar]
- Garty BZ, Danon YL, Nitzan M. Schoenlein-Henoch purpura associated with hepatitis A infection. Am J Dis Child. 1985;139:547. doi: 10.1001/archpedi.1985.02140080017017. [DOI] [PubMed] [Google Scholar]
- Lefrère JJ, Couroucé AM, Müller JY, Clark M, Soulier JP. Human parvovirus and purpura. Lancet. 1985;2:730. doi: 10.1016/s0140-6736(85)92509-7. [DOI] [PubMed] [Google Scholar]
- Patel U, Bradley JR, Hamilton DV. Henoch-Schönlein purpura after influenza vaccination. Br Med J Clin Res Ed. 1988;296:1800. [PMC free article] [PubMed] [Google Scholar]
- Wakefield IR, Hunter DA. Antibiotic associated Henoch-Schoenlein purpura syndrome. Br J Clin Pract. 1988;42:525–526. [PubMed] [Google Scholar]
- Moots RJ, Keeling PJ, Morgan SH. Adult Schönlein-Henoch purpura after enalapril. Lancet. 1992;340:304–305. doi: 10.1016/0140-6736(92)92391-r. [DOI] [PubMed] [Google Scholar]
- De Pree C, Schifferli JA, Masouyé I, Bernard P. Schoenlein-Henoch de I'adulte – aspects actuels. Schweiz Rundschau Med Phase. 1994;83:975–979. [PubMed] [Google Scholar]
- Ledermann JA, Hoffbrand BI. Dapsone in allergic vasculitis: its use in Henoch-Schönlein disease following vaccination. J R Soc Med. 1983;76:613–614. doi: 10.1177/014107688307600717. [DOI] [PMC free article] [PubMed] [Google Scholar]