

Abstract
Background:
Cancer-related fatigue (CRF), is a common distressing symptom of cancer. What's more, “Three anti-fatigue acupoints” is one of the most important components of “Jin's 3-needle therapy” created by Rui Jin, a professor of Guangzhou University of Chinese Medicine, which can be used in the treatment of CRF. In this article, researchers will assess the safety and effect of acupuncture at 3 anti-fatigue acupoints on CRF in patients with cancer.
Methods:
Literature search for relevant articles up to October 2018 will be carried out in 9 databases: Cochrane Library, Embase, PubMed, VIP, CBM, CNKI, Wanfang Database, CiNii, and OASIS. The included literatures will be randomized controlled trials of acupuncture at 3 anti-fatigue acupoints on CRF in patients with cancer. The certain common scales, which reflect the patients’ fatigue degree or life quality will be the primary outcome measures. The secondary outcome measures will be defined with the blood index. After collecting the data, we will utilize Stata V.13.0. to perform data synthesis, subgroup analysis, partial sequence analysis, sensitivity analysis, and so on. A funnel plot will be used to assess reporting biases. And the funnel plot will be evaluated by the Egger and Begg tests. The quality of evidence will be judged by the grading of recommendations assessment, development, and evaluation.
Results:
The results of this systematic review and meta-analysis will be published in a peer-reviewed journal.
Conclusion:
Our study will provide the evidence for the clinical efficacy and safety of acupuncture at 3 anti-fatigue acupoints in the treatment of CRF.
Keywords: acupuncture, cancer-related fatigue, meta-analysis, protocol, systematic review
Key Points
This study will assess the clinical efficacy and safety of acupuncture at 3 anti-fatigue acupoints in the treatment of cancer-related fatigue.
Two reviewers will independently conduct the data extraction and risk f bias assessment.
The grading of recommendations assessment, development, and evaluation system will be applied to further evaluate study findings.
There may be a language bias, as both English and Chinese studies will be included.
There may be clinical heterogeneity due to variations in treatment frequency and duration and the use of additional therapies.
1. Introduction
1.1. Description of the condition
Cancer-related fatigue (CRF), is a common distressing symptom of cancer. Over 99% of patients experienced some levels of fatigue during treatment with radiation, chemotherapy, and biologic therapies.[1] Although fatigue is the most prevalent in patients undergoing chemotherapy or those with advanced diseases, it is also an important problem among cancer survivors.[2,3] Fatigue mostly resolves in the year after treatment completion, but approximately 30% of patients experience more persistent fatigue that may last for 10 years or more.[4] Studies have shown that CRF affects multiple aspects of individuals’ lives, such as performing activities of daily living, decreasing functional status, and limiting overall quality of life.[5,6] In addition, CRF is associated with decreased survival and interferes with employment, family life, social relationships as well as sexual life.[7–9] One of the consistent and key symptoms of CRF is seemingly the presence of emotional distress or mood disturbance.[10,11] It has been reported that erythropoietin can reduce the need for transfusions, decrease fatigue levels, and improve quality of life in patients receiving chemotherapy.[12–16] However, recent evidence has raised concerns regarding the safety of erythropoietin, suggesting it should not be used for the management of CRF.[17] Fortunately, traditional Chinese medicine (TCM), such as acupuncture, has been gradually acknowledged worldwide for the management of CRF.[18]
1.2. Description of the intervention
Acupuncture, as an indispensable part of TCM, has been proved to be effective for CRF management and should be recommended as a beneficial alternative therapy for CRF patients. The main therapeutic effects of acupuncture include dredging the meridians (channels and collaterals), regulating Yin and Yang, and strengthening the body's resistance to eliminate pathogenic factors.[19] Three anti-fatigue acupoints is an acupoint set consisting of Sishen Needle, Neiguan (PC6), Zusanli (ST36).[20] Sishen Needle is located on the parietal region, 1.5 cun anterior, posterior and lateral to Baihui, 4 acpoints totally, which is shown in Figure 1. PC6 is located 2 cun above the transverse crease of the wrist, between the tendons of palmaris longus and flexor carpi radialis. ST36 is located 3 cun directly below Dubi, and 1 finger-breath lateral to the anterior border of the tibia. Cun is defined based on the rules of traditional acupuncture as the width of the interphalangeal joint of the patient's thumb.[21] The location of PC6 and ST36 is shown in Figures 2 and 3. Several clinical trials have shown that PC6 or ST36 is effective in treating CRF.[22] However, the effect of acupuncture at 3 anti-fatigue acupoints in the treatment of CRF has not been investigated. In addition, there is insufficient evidence to support the widespread use of acupuncture at 3 anti-fatigue acupoints. Consequently, an examination of this therapy's effect on CRF is needed. Therefore, we aim to carry out a systematic review and meta-analysis to evaluate current evidence on the effects of acupuncture at 3 anti-fatigue acupoints in the treatment of CRF in patients with cancer. Researchers will include randomized controlled trials (RCTs) with no language restrictions that compare the effects of acupuncture or electroacupuncture with usual care or placebo acupuncture.
Figure 1.
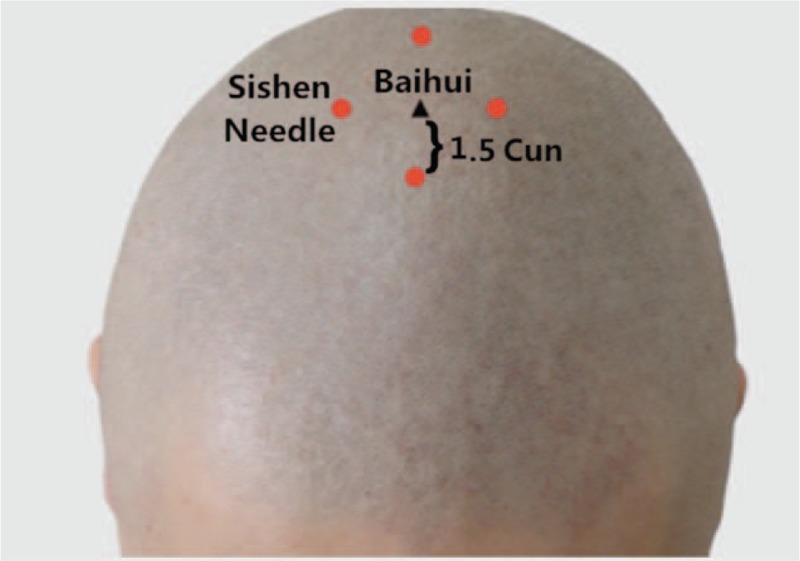
The location of Sishen Needle.
Figure 2.
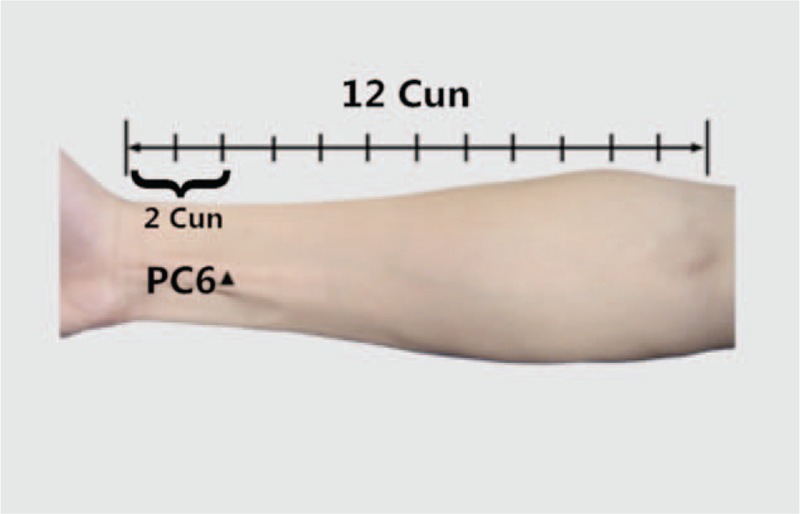
The location of PC6.
Figure 3.
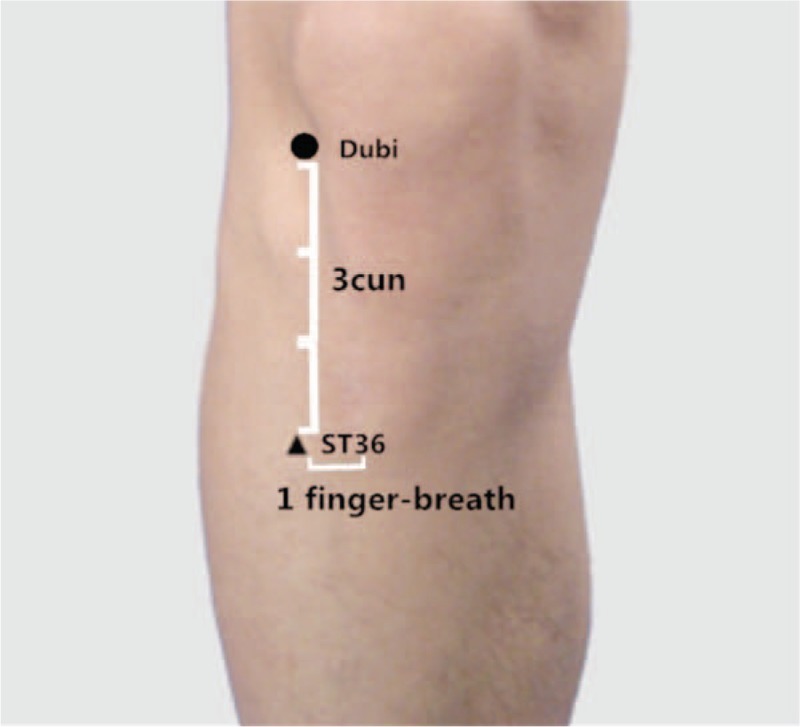
The location of ST36.
2. Methods
2.1. Selection criteria
2.1.1. Study type
Researchers will include all the RCTs of acupuncture at 3 anti-fatigue acupoints on CRF, without publication status. While others, such as non-RCTs, animal studies, case reports, will be excluded.
2.2. Participants
Regardless of types of cancer, gender, ages, nationalities, and educational status, the patients with CRF will be included. Firstly, the included participants should be diagnosed with cancer from cytological diagnosis, pathological diagnosis, or clinical diagnosis based on the past or current diagnosis standards or guidelines of cancer, such as New Standard for Diagnosis and Treatment of Malignant Tumors, which is formulated by China Cancer Association. Secondly, the included patients with cancer should conform to the definitions of CRF according to the diagnosis standards, such as International Classification of Diseases Tenth Edition.
2.3. Interventions
2.3.1. Experimental interventions
The intervention group included will use acupuncture at 3 anti-fatigue acupoints based on routine regimens of the control group, or only acupuncture at 3 anti-fatigue acupoints, which includes electroacupuncture and ordinary acupuncture. Acupuncture at 3 anti-fatigue acupoints is different from traditional acupuncture. Acupuncture at 3 anti-fatigue acupoints refers to only inserting needles into 3 acupoints (Sishen Needle, Neiguan, and Zusanli) at a time, while traditional acupuncture means selecting classic acupoints of channels and collaterals to resist fatigue. The time and frequency of treatment will not be restricted. If the intervention group uses electrical or manipulation stimulation at 3 anti-fatigue acupoints, it will be excluded.
2.4. Comparator interventions
The patients in control group will receive several interventions comprised of no treatment, placebo acupuncture, sham acupuncture, drug or other treatments (such as aerobic exercise, dietotherapy, and health education).
Several comparisons will be analyzed as following:
-
(1)
acupuncture at 3 anti-fatigue acupoints compared with no treatment;
-
(2)
acupuncture at 3 anti-fatigue acupoints compared with placebo acupuncture or sham acupuncture;
-
(3)
acupuncture at 3 anti-fatigue acupoints plus drug or other treatments compared with drug or other treatments;
-
(4)
acupuncture at 3 anti-fatigue acupoints plus drug or other treatments compared with placebo acupuncture or sham acupuncture plus drug or other treatments.
2.5. Outcome measures
The primary outcome measures will be certain common scales which reflect the patients’ fatigue degree or life quality, such as piper fatigue scale (PFS), brief fatigue inventory, fatigue symptom inventory, Karnofsky performance status, The Europe Organization for Research and Treatment of Cancer, Quality of Life Questionnaire-Core 30, and so on.
The secondary outcome measures will be the blood index such as 5-hydroxytryptamine (5-HT), interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), and interferon.
2.6. Information sources
2.6.1. Search strategy and identification of studies
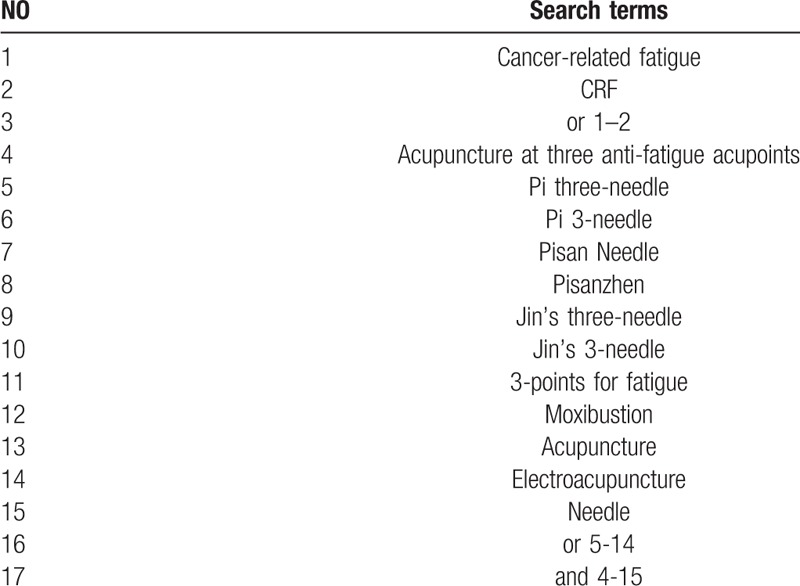
Related literatures published from inception to October 2018, will be retrieved from the following databases: Cochrane Library, Embase, PubMed, 4 Chinese databases (Chinese National Knowledge Infrastructure, Chinese Science and Technology Periodicals Database, Chinese BioMedical Database and Wanfang Database), a Japanese database (CiNii) and a Korean database (OASIS). The search terms will be “cancer-related fatigue” OR “CRF” AND “acupuncture at three anti-fatigue acupoints” OR “Pi three-needle” OR “Pi 3-needle” OR “Pisan Needle” OR “Pisanzhen” OR “Jin's three-needle” OR “Jin's 3-needle” OR “3-points for fatigue” OR “moxibustion” OR “acupuncture” OR “electroacupuncture” OR “needle.” In Chinese, Korean, and Japanese databases, we will use the corresponding translations of these search terms to perform electronic searches. Detailed search strategy is shown as Table 1.
Table 1.
Search strategy used in for the PubMed database.
Other resources including references list of anteriorly published reviews and relevant conference proceedings will be searched for potential eligible studies.
The reviewers (TL and YZX) will scan full articles independently. When divarication generates during the course and cannot be solved through discussion between 2 reviewers, the third reviewer (JY) will be consulted for arbitration. A Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart will be drawn to describe the study selection process and explain the reason for inclusion and exclusion (http://www.prisma-statement.org) (Fig. 4).
Figure 4.
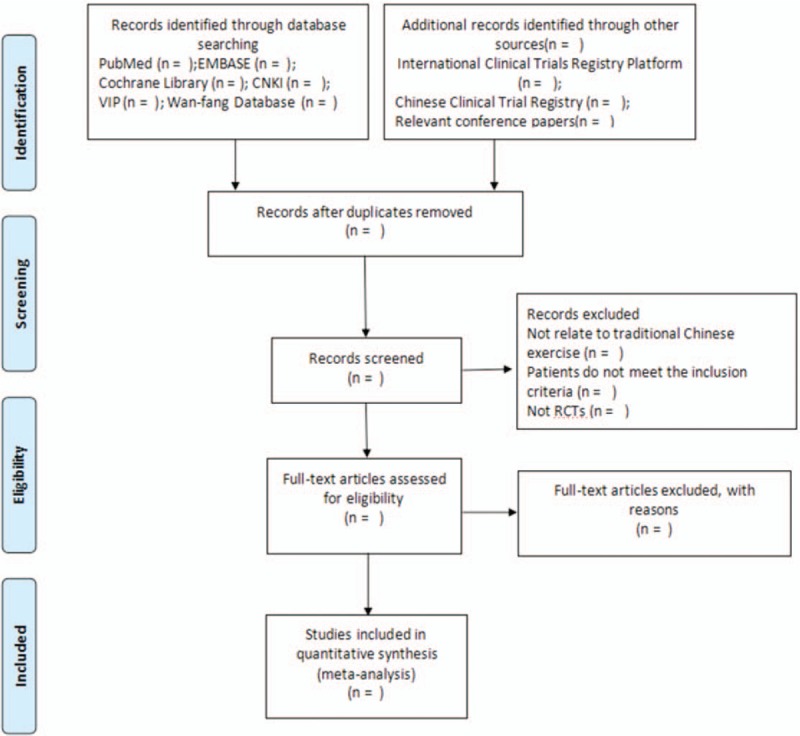
Flow diagram of the study selection process.
2.7. Selection of studies
The articles with repeated results, unclear outcome data or unavailable related information, will be excluded. The reviewers (TL and YZX) will review titles and abstracts to select potential eligible literature and scan full articles to select the literature which can conform to the inclusion criteria, independently. A third reviewer (JY) will solve the disagreement between 2 reviewers. Endnote V.X7 will be used for literature managements and duplication removals.
2.8. Data extraction and management
The reviewers (TL and YZX) will independently extract data by using a data extraction sheet. The data will include the following items: general information (first author and publication year), study design, randomization methods, allocation concealment, blind method, inclusion and exclusion criteria of participants, participant's characteristics (sex, age, and duration of disease), sample size, interventions, primary and secondary outcomes, outcome assessment methods, side effects, and follow-up. Any disagreements will be discussed by the reviewers to reach consensus, and if necessary, it will be consulted with the third reviewer.
2.9. Addressing missing data
Researchers will contact with the original authors by telephone or email to request incomplete or missing data when necessary. If the information cannot be supplemented sufficiently in this way, researchers will abandon it. The potential impact of missing data will be considered in the discussion section.
2.10. Risk of bias in included studies
For assessing the risk of bias, researchers will utilize Cochrane collaboration's tool, which contains the following domains: generation of random sequence, allocation concealment, blinding method of participants, blinding method of outcome assessors, selective outcome reporting, incomplete result, and other bias. In order to describe the risk of bias in each study clearly, researchers will categorize the risk into unclear, low or high.
2.11. Statistical analysis
2.11.1. Data synthesis and analysis
Stata V.13.0. software will be performed to analyze the data we obtained. We will calculate standard mean difference with 95% confidence intervals (CIs) for continuous outcomes and risk ratios with 95% CIs for dichotomous outcomes.
For assessing the heterogeneity, the Q and I2 test statistics will be performed. For the Q statistic, we will interpret the value of P < .1 as significant differences. For the I2 statistic, I2 > 50% indicates strong heterogeneity, I2 = 25% to 50% means moderate heterogeneity, and I2 < 25% represents no heterogeneity. If the data is considered as little heterogeneity, the fixed effect model will be adopted, or else the random effect model will be adopted.
2.12. Additional analyses
To explore the potential sources of heterogeneity, we will perform subgroup analysis, partial sequence analysis, and sensitivity analysis on the basis of various literature characteristics, such as locations of study, types of study, sample size, different participant conditions, different interventions and outcome measures, quality of study, and other related factors. We will use the extracted data to conduct quantitative analysis. But if the data is insufficient, qualitative analysis will replace it.
2.13. Assessment of reporting biases
When the included literatures are more than 10, we will use a funnel plot to assess the reporting bias. Egger and Begg tests will be utilized to evaluate funnel plot symmetry that P < .1 will be considered as showing statistical significance.
2.14. Quality of evidence
The quality of evidence of the included literatures will be judged by the grading of recommendations assessment, development, and evaluation. And the quality of evidence will be evaluated according to 4 levels: very low, low, moderate, or high.
2.15. Ethics and dissemination
Disseminating this systematic review and meta-analysis in a peer reviewed publication is our expected goal. The finding will furnish information about the safety and effect of acupuncture at 3 anti-fatigue acupoints on CRF in patients with cancer. As participants’ privacy will not be involved in this study, ethical approval is not required.
3. Discussion
According to TCM theories, acupuncture alone or in combination with moxibustion is often used to tonify qi and blood. To put acupuncture treatment into good use, it is of significance to select acupoints in treating CRF. Therefore, acupuncture at 3 anti-fatigue acupoints will be applied to the subjects in this study. Three anti-fatigue acupoints include Sishen Needle, PC6, ST36. Sishen Needle, is designated the sites 1.5 cun anterior, posterior left and right to Baihui (GV 20). It was suggested that Sishen Needle could regulate platelet 5-HT and plasma ACTH, which is helpful for the symptoms related to CRF.[23] In addition, ST36 is able to Tonify qi and blood, relieve abdominal discomforts and digestive or elimination dysfunctions.[24] Particularly, ST36 regulates immunity and reduces inflammation, which can improve the long term effects cause by related cancer treatments.[25,26] Another recent study concluded that acupuncture at ST36 and PC6 significantly lowered the level of the data of heart rate and oxygen consumption, indicating a fatigue relief.[27]
Consequently, acupuncture at 3 anti-fatigue acupoints is theoretical in treating CRF. Nevertheless, the efficacy of acupuncture at 3 anti-fatigue acupoints compared with pharmacological interventions remains unknown. Additionally, there is insufficient evidence that acupuncture at 3 anti-fatigue acupoints is able to treat CRF. The aim of this review is to systematically assess the effect of acupuncture at 3 anti-fatigue acupoints in the treatment of CRF in patients with cancer. Researchers hope to use enough studies to make sure that adequate power for the meta-analysis. Also, researchers expect to find out whether acupuncture at 3 anti-fatigue acupoints has a positive effect on primary prevention of CRF in patients with cancer. Generally speaking, this review will be the first to evaluate the impact of acupuncture at 3 anti-fatigue acupoints on primary prevention of CRF in patients with cancer. The outcome of this review may be beneficial to establish a better approach to prevent CRF in patients with cancer and provide reliable evidence for its application.
Author contributions
MXL, JY, YQY, and JTL conceived the study and drafted the protocol. YZX, TL, WJZ, LZL revised it. MXL, JY, YZX, and SLJ developed the search strategies, conducted data collection and analyzed independently. All authors have approved the final manuscript.
Conceptualization: Muxi Liao, Shuliang Ji.
Data curation: Yaqin Yang.
Investigation: Shuliang Ji.
Methodology: Wenjing Zhao.
Project administration: Tong Lin.
Resources: Jiao Yan.
Software: Zongyao Li.
Writing – original draft: Muxi Liao, Jiao Yan, Yizi Xie.
Writing – review and editing: Lizhu Lin, Jietao Lin.
Footnotes
Abbreviations: 5-HT = 5-hydroxytryptamine, CRF = cancer-related fatigue, RCTs = randomize controlled trials, TCM = Traditional Chinese medicine.
ML, YX, and JY contributed equally to this work.
This systematic review will be disseminated in a peer reviewed publication. Our findings will provide information about the safety of acupuncture at 3 anti-fatigue acupoints for cancer-related fatigue patients and their effect on cancer-related fatigue.
The protocol for this review has been registered in the PROSPERO network (registration number: CRD42018107785).
Not commissioned; externally peer reviewed.
This work is supported by grants from the High-level university construction project of Guangzhou University of Chinese Medicine. The grand number is No. A1-AFD18171Z11078.
The authors have no conflicts of interest to disclose.
References
- [1].Servaes P, Verhagen C, Bleijenberg G. Fatigue in cancer patients during and after treatment: prevalence, correlates and interventions. Eur J Cancer 2002;38:27–43. [DOI] [PubMed] [Google Scholar]
- [2].Butt Z, Rosenbloom SK, Abernethy AP, et al. Fatigue is the most important symptom for advanced cancer patients who have had chemotherapy. J Natl Compr Canc Netw 2008;6:448–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [3].Iop A, Manfredi AM, Bonura S. Fatigue in cancer patients receiving chemotherapy: an analysis of published studies. Ann Oncol 2004;15:712–20. [DOI] [PubMed] [Google Scholar]
- [4].Bower JE, Ganz PA, Desmond KA, et al. Fatigue in long-term breast cancinoma survivors: a longitudinal investigation. Cancer 2006;106:751–8. [DOI] [PubMed] [Google Scholar]
- [5].Borneman T. Assessment and management of cancer-related fatigue. J Hosp Palliat Nurs 2013;15:77–86. [Google Scholar]
- [6].Sood A, Barton DL, Bauer BA, et al. A critical review of complementary therapies for cancer-related fatigue. Integr Cancer Ther 2007;6:8–13. [DOI] [PubMed] [Google Scholar]
- [7].Cheville AL, Shen T, Chang M, et al. Appropriateness of the treatment of fatigued patients with stage IV cancer. Support Care Cancer 2013;21:229–33. [DOI] [PubMed] [Google Scholar]
- [8].Kirshbaum M. Cancer-related fatigue: a review of nursing interventions. Br J Community Nurs 2010;15:214–9. [DOI] [PubMed] [Google Scholar]
- [9].Scott JA, Lasch KE, Barsevick AM, et al. Patients’ experience with cancer-related fatigue: a review and synthesis of qualitative research. Oncol Nurs Forum 2011;38:E191–203. [DOI] [PubMed] [Google Scholar]
- [10].Storey DJ, Waters RA, Hibberd CJ, et al. Clinically relevant fatigue in cancer outpatients: the Edinburgh Cancer Center symptom study. Ann Oncol 2007;18:1861–9. [DOI] [PubMed] [Google Scholar]
- [11].Goldstedin D, Bennett B, Friedlander M, et al. Fatigue states after cancer treatment occur both in association with, and independent of, mood disorder: a longitudinal study. BMC Cancer 2006;6:240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Littlewood TJ, Bajetta E, Nortier JWR, et al. Effects of epoetin alfa on hematologic parameters and quality of life in cancer patients receiving nonplatinum chemotherapy: results of a randomized, double-blind, placebo-controlled trial. J Clin Oncol 2001;19:2865–74. [DOI] [PubMed] [Google Scholar]
- [13].Demetri G, Kris M, Wasde J, et al. Quality-of-life benefit in chemotherapy patients treated with epoetin alfa is independent of disease response or tumor type: results from a prospective community oncology study. J Clin Oncol 1998;16:3412–25. [DOI] [PubMed] [Google Scholar]
- [14].Glaspy J, Bukowski R, Steinberg D, et al. Impact of therapy with epoetin alfa on clinical outcomes in patients with nonmyeloid malignancies during cancer chemotherapy in community oncology practice. J Clin Oncol 1997;15:1218–34. [DOI] [PubMed] [Google Scholar]
- [15].Gabrilove JL, Cleeland CS, Livingston RB, et al. Clinical evaluation of once-weekly dosing of epoetin alfa in chemotherapy patients: improvements in hemoglobin and quality of life are similar to threetimes weekly dosing. J Clin Oncol 2001;19:2875–82. [DOI] [PubMed] [Google Scholar]
- [16].Österborg A, Brandberg Y, Molostova V, et al. Randomized doubleblind, placebo-controlled trial of recombinant human erythropoietin, epoetin beta, in hematologic malignancies. J Clin Oncol 2002;20:2486–94. [DOI] [PubMed] [Google Scholar]
- [17].Minton O, Richardson A, Sharpe M, et al. Drug therapy for the management of cancer-related fatigue. Cochrane Database Syst Rev 2010;7:CD006704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Lehmann H. Acupuncture in ancient China: how important was it really? J Integr Med 2013;11:45–53. [DOI] [PubMed] [Google Scholar]
- [19].Zhang Y, Lin L, Li H, et al. Effects of acupuncture on cancer-related fatigue: a meta-analysis. Support Care Cancer 2018;26:415–25. [DOI] [PubMed] [Google Scholar]
- [20].Zhou C, Tian H, Zeng B, et al. Clinical observation on acupuncture on three anti-fatigue acupoints in the treatment of cancer-induced fatigue in patients with breast cancer. Zhongyi Xuebao 2018;33:950–3. [Google Scholar]
- [21].Melchart D, Streng A, Hoppe A, et al. Acupuncture in patients with tension-type headache: randomized controlled trial. BMJ 2005;331:376–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Deng G, Chan Y, Sjoberg D, et al. Acupuncture for the treatment of post-chemotherapy chronic fatigue: a randomized, blinded, sham-controlled trial. Support Care Cancer 2013;21:1735–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Yuan Q, Li JN, Liu B, et al. Effect of jin-3-needling therapy on plasma corticosteroid, adrenocorticotrophic hormone and platelet 5-HT levels in patients with generalized anxiety disorder. Chin J Integr Med 2007;13:264–8. [DOI] [PubMed] [Google Scholar]
- [24].Grant SJ, Smith CA, de Silva N, et al. Defining the quality of acupuncture: the case of acupuncture for cancer-related fatigue. Integr Cancer Ther 2015;14:258–70. [DOI] [PubMed] [Google Scholar]
- [25].Yim YK, Lee H, Hong KE, et al. Electro-acupuncture at acupoint ST36 reduces inflammation and regulates immune activity in collagen-induced arthritic mice. Evid Based Complement Alternat Med 2007;4:51–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Kim SK, Bae H. Acupuncture and immune modulation. Auton Neurosci 2010;157:38–41. [DOI] [PubMed] [Google Scholar]
- [27].Lin ZP, Lan LW, He TY, et al. Effect of acupuncture stimulation on recovery ability of male elite basketball athletes. Am J Chin Med 2009;37:471–81. [DOI] [PubMed] [Google Scholar]