
Fig. 3.
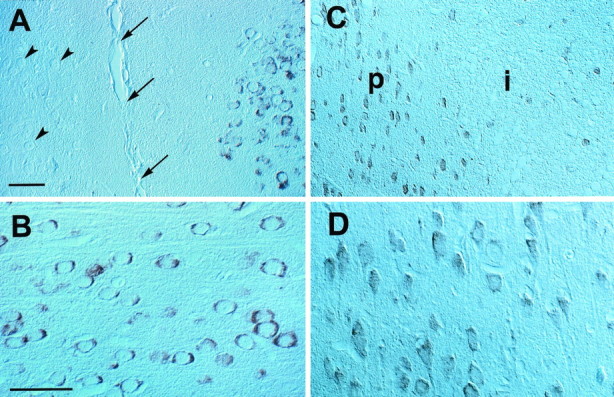
Effect of focal cerebral ischemia on COX-2 immunoreactivity in paraffin-embedded sections (7 μm thickness) of rats subjected to a 2 hr occlusion of the MCA. A, Some COX-2-immunoreactive cells are located in the intact cingulate cortex medial to ischemic lesion. This region corresponds to the border zone between the anterior cerebral artery and MCA. The arrowspoint to the midline (intrahemispheric fissure); thearrowheads point to unstained neurons in the contralateral side. B, High-power view of the cells depicted in A. These cells have the morphological characteristics of normal neurons, with a large round nucleus and a prominent nucleolus. The immunoreactivity is characteristically perinuclear (cf. Yamagata et al., 1993). C, Other COX-2-positive cells are located in the transitional region between normal and infarcted brain. These cells have an angular appearance, with a shrunken cytoplasm and nucleus. In alternate sections stained with hematoxylin and eosin, these cells correspond to neurons exhibiting distinct ischemic changes (“red neurons”). Therefore, COX-2 is expressed also in injured neurons at the periphery of the ischemic territory. The region in which these COX-2 neurons are located corresponds to the so-called ischemic penumbra. The positive cells observed within the infarct are most likely shrunken neurons.P, Anatomical location of the ischemic penumbra;i, infarct. D, High-power view of the COX-2-immunoreactive neurons depicted in C. Notice the cell shrinkage. Scale bars: A, C, 500 μm; B, D, 150 μm.