
Figure 3.
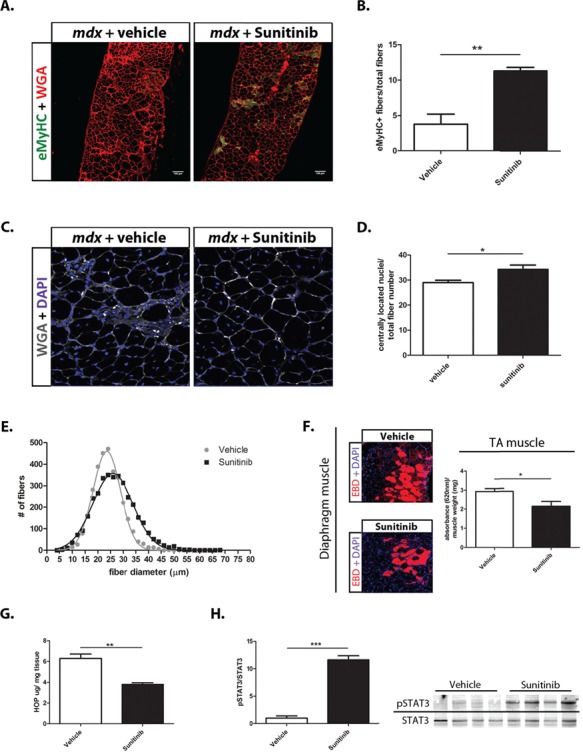
Sunitinib promotes muscle repair and improves markers of DMD disease progression. (A) Representative section of immunohistochemistry performed on 10 μm diaphragm muscle sections showing increased number of eMyHC (green) positive fibers in Sunitinib-treated muscle. WGA (red); scale bar, 100 μm. (B) Quantification of eMyHC positive (+) muscle fibers normalized to total fiber numbers of a whole mdx diaphragm muscle section (N = 4); Sunitinib treatment causes ~8% increase in eMyHC+ fibers compared to vehicle treatment. (C and D) CLN counts performed on WGA (grey) and DAPI (blue) immunolabeled 10 μm diaphragm muscle sections (N = 6); Sunitinib treatment increased CLNs by ~5% compared to vehicle treated. (E) Myofiber size distribution of Sunitinib- and vehicle-treated whole 10 μm sections diaphragm sections, measured using minimum Feret’s diameter (N = 4); Sunitinib-treated muscle shows a shift toward higher percentage of large fiber sizes compared to vehicle treated. (F) Representative sections of EBD (red) infiltration in Sunitinib-treated diaphragm muscle. EBD quantification performed on total GA muscle shows decreased EBD infiltration compared to vehicle treated (N = 4). (G) Hydroxyproline assay was performed to quantify the amount of fibrotic infiltration in whole GA muscle (N = 4); Sunitinib treatment decreases fibrosis as shown by a 2-fold decrease in collagen content in the mdx GA muscle, compared to vehicle treated. (H) Western blot analysis showing the STAT3 pathway is activated in response to Sunitinib treatment 1 h post final dose (6 week total dosing) in mdx diaphragm muscle. Data assessed for significance using unpaired t-test and statistical significance of mean ± SEM; *P < 0.05, **P < 0.01, ***P < 0.001.