
Figure 1: Imaging and histopathologic findings.
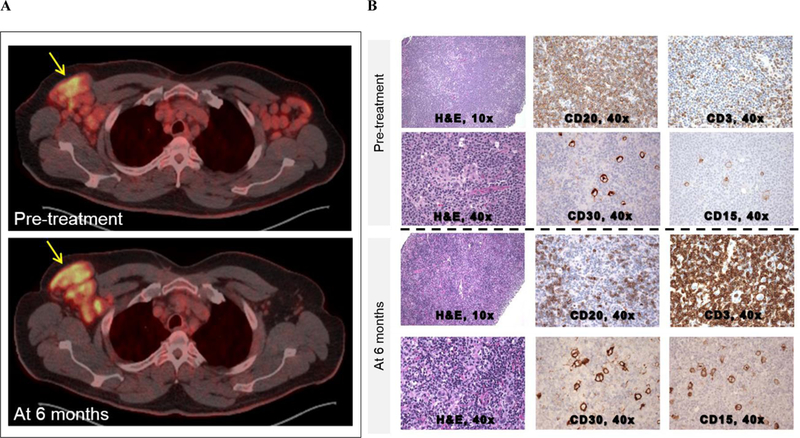
A-B: Patient 1
(A) Pre-treatment PET/CT showed enhancement of bilateral axillary LN with an SUV of 9.4 in the right axillary region. Repeat PET/CT after 6 months showed increased enhancement of the right axillary region (SUV 11.1) and near resolution of disease elsewhere. (B) Pre-treatment LN biopsy using hematoxylin and eosin (H&E) staining at 10x and CD20 and CD3 IHC staining at 40x. After the diagnosis of HL-RT was made, careful inspection of the H&E stain at 40x revealed Reed Sternberg cells amongst a background of diffuse CLL involvement. These Reed-Sternberg cells were positive for CD30 and CD15. After 6 months of treatment, there was a reduction in CLL involvement and more apparent visualization of Reed Sternberg cells.
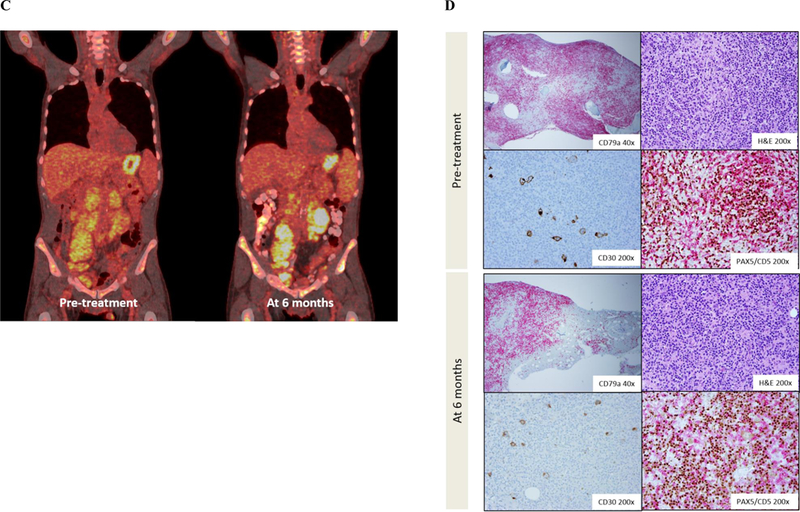
C-D: Patient 2
(C) Pre-treatment PET/CT showed diffuse enhancement of neck, mediastinal, abdominal and pelvic lymph nodes prior to treatment with acalabrutinib. Maximum SUV of 8.64 was seen in a left iliac node. After 6 months of acalabrutinib, PET/CT showed an interval increase in hypermetabolic activity in retroperitoneal and pelvic LNs. Maximum SUV of 11.16 was seen in retroperitoneal LNs near the left kidney. (B) Bone marrow biopsies were performed before and after 6 months of treatment. CD79a IHC staining of the pre-treatment biopsy at 40x showed extensive bone marrow involvement by CLL. H&E and CD30 stains at 200x revealed Reed Sternberg cells. Double staining for PAX5 (brown) and CD5 (red) highlighted Reed Sternberg cells weakly positive for CD5 amongst a background of CLL cells. Bone marrow biopsy after 6 months of acalabrutinib showed a decrease in CLL involvement and Reed Sternberg cells.