
Figure 7. Potential Strategies To Prevent Brain Metastasis.
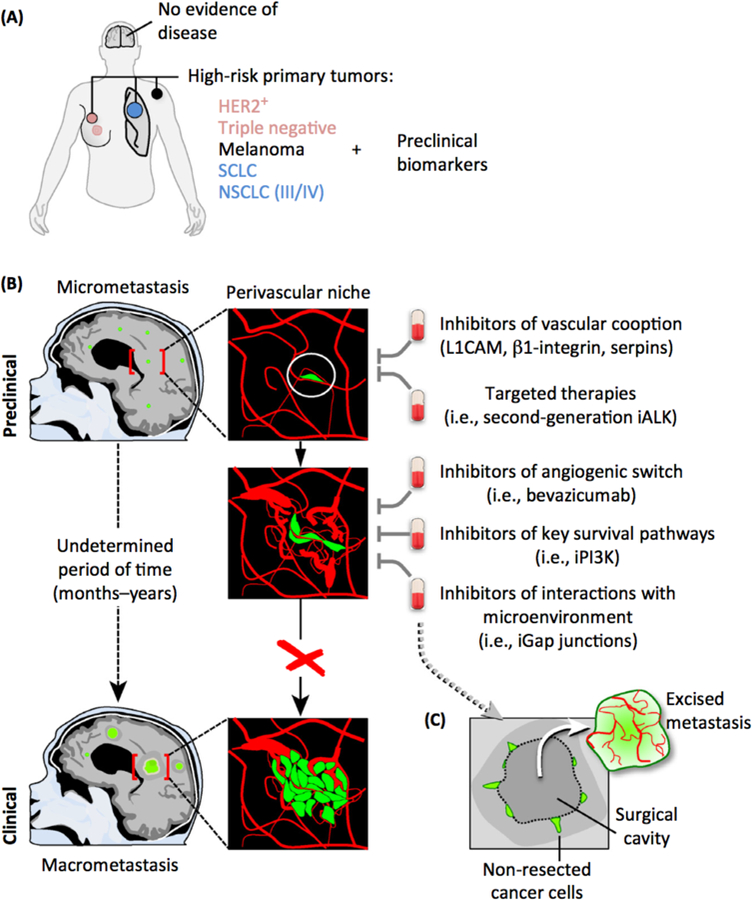
(A) Patients with HER2+ or triple-negative breast cancer, melanoma, small-cell lung cancer (SCLC), and stage IIV/IV non-scuamous non-small cell lung cancer (NSCLC) are at high risk for the development of brain metastasis during the progression of the disease. To guide clinical decisions in initiating brain metastasis-preventive trials, the discovery of biomarkers in preclinical models that could be translated to this group of patients will be a valuable resource. (B) Although clinically undetectable, brain micrometastasis might be present in asymptomatic patients with these high-risk tumors. Experimental findings suggest the importance of the interaction with the vasculature to allow metastasis-initiating cells to progress. Metastatic cells initially interact with pre-existing vessels (vascular cooption), and drugs targeting key mediators of this process will therefore impede their outgrowth. The efficacyof ALK inhibitors (iALK) that cross the blood-brain barrier (BBB) will allow targeting of cancer cells before they are detectable by imaging. Some micrometastases may have proliferated and started to influence the microenvironment, and at this point a VEGF-dependent switch from vascular cooption to angiogenesis is necessary to support the outgrowth of the metastatic lesion derived from lung cancer. Preventive trials with BBB-permeable Pl3K inhibitors might be considered because there is experimental evidence for their efficacy [41]. In addition, interaction with astrocytes could be targeted with blockers of gap junction communication (iGap junctions). (C) An alternative option will be to apply preventive therapies after neurosurgical resection, given the known ability of brain metastatic cells to infiltrate the tissue [57] and the likelihood that some cancer cells remain in surgical margins. In this sense the infiltrative phenotype of brain metastasis has been linked to reduced survval [167]. During reinitiation of local growth, the metastasis might follow the same principles and molecular regulation as during the inltial stages.