

Abstract
Ostomy creation is a routine surgical procedure that has earned its place high in the surgeon's armamentarium in dealing with challenging situations. However, it is not without its complications. In this article, we review the common complications including parastomal hernia, prolapse, mucocutaneous junction separation with ischemia and stenosis, peristomal skin conditions, and infections. Additionally, we review conditions that arise in association with underlying Crohn's disease, such as peristomal inflammation, fistula formation, and pyoderma gangrenosum.
Keywords: Crohn’s disease, ostomy complications, parastomal hernia, stomal prolapse
Ostomy formation was introduced as early as the 1700s as a last resort for life-threatening conditions. It often served as a sole treatment for relieving colonic obstruction and sometimes to alleviate symptoms of severe colitis. Its original utilization was introduced by Littre as a ventral colostomy and has gone through numerous alterations, from tube to loop, ventral to lumbar, exteriorization, and delayed opening to the current practice of primary maturation, introduced by Dr. Brooke in 1951. Various modifications such as the mucosal grafted ileostomy by Dr. Turnbull and the continent ileostomy by Dr. Kock have had major contributions to the evolution and understanding in the surgical technique and function. A formal focus for the care of patients with ostomies (ostomates) cumulated to the first school of enterostomal therapy, established in 1961 at the Cleveland Clinic. 1 In the original literature, ostomies were referred to as “ anus artificial ”; however, it took the Greek-derived term “stoma,” meaning mouth or an opening. Up to now, it remains a vital part of gastrointestinal surgery. Performed in both the emergent and elective setting, its benefits range from providing a temporary palliation of an uncontrolled condition to sometimes a permanent solution. Although it may be simple to construct in some patients, if performed outside of the ideal conditions and without consideration of the substantial impact that the mere presence of an ostomy has on a patient's lifestyle, it may lead to an array of life-altering complications that hinder patient satisfaction and prompt repeat visits to the practitioner. 2 Furthermore, Crohn's patients who undergo an ostomy procedure are notorious for being plagued with frequent (up to 70%) and more severe complications. 3 4 Additionally, there is an association between stoma-related complication and Crohn's disease activity; hence, an ostomy may even serve as a window to the severity of the underlying inflammatory disease process. 5
Ostomy Planning and Education
The influence and importance of appropriate planning, education, and marking of a stoma site prior to surgery warrants specific mention. The location of the waistline, umbilicus, skin folds, and scars should all be considered in the ideal site placement of a stoma. The stoma should be placed within the rectus muscle to minimize the risk of parastomal hernia formation. In general, a spot in the center of a triangle connecting the umbilicus, anterior superior iliac spine, and the pubis is a good reference point, which ideally correlates to a summit of a bulge which exists just below the umbilicus. The patient should be examined while standing, sitting, and in supine positions and adjustments made in the ostomy site to avoid potential skin creases.
Several studies have shown preoperative stoma site marking, and familiarization with appliances and ongoing counseling by trained individuals provide a significant improvement in the overall experience. In a study of 105 patients by Person et al in which 52 were marked prior to surgery and 53 were not, quality of life, patient independence parameters, and complication rates were significantly better in favor of those who were marked. 6 This benefit is further reinforced with postoperative follow-up with a skilled wound ostomy continence (WOC) nurse. Common early complications that burden new ostomates such as skin irritation, leakage, and foul smell are issues that are alleviated by a WOC nurse. In a study of 796 ostomy nurses, they estimated that approximately 77% of their patients developed peristomal skin issues and the largest contributing factor was the lack of follow-up after hospital discharge. 7 8 Further, there is a psychological weight of getting an ostomy and alterations of body image and quality of life that is difficult to quantify, but relieved by the support provided by a WOC nurse. 2
Special Considerations for Obese Patients
With obesity being realized at epidemic proportions in the general population of United States and developed countries, similar trends are evidenced in inflammatory bowel disease (IBD) patients as well, with up to 41% of Crohn's patients meeting criteria as overweight or obese. 9 Obese patients suffer from higher complication rates from colorectal surgery, including higher risks of wound dehiscence, wound infection, and anastomotic leakage. They also suffer from higher stoma-related complications such as parastomal hernia, mucocutaneous separation, stoma retraction, and stomal prolapse. 10 11 The underlying cause of the higher complication rates may be systemic, but the body habitus of obese patients presents challenges that are not encountered in patients of normal weight. The aforementioned triangle of ideal placement may not be optimal due to the abdominal wall thickness lower in the abdomen and the inability of obese patients to see the ostomy in the lower abdomen. In general, the upper abdomen is preferred in obese individuals. Further, the segment of intestine to be brought up to serve as an ostomy may require more extensive mobilization than the nonobese patient as it has to travel a longer distance. Once an adequate conduit is created, the aperture in the abdominal wall needs to be made larger to accommodate a wider segment of intestine. Wound protectors have been shown to benefit the delivery of bowel through the subcutaneous tissue and fascia. 11 Further, a loop-end ostomy where the distal end of a loop ileostomy is closed and the ostomy matured 2 to 4 cm proximal to the closure site has been utilized in obese patients to decrease tension from the excess mesenteric weight and allow for adequate length without vascular compromise. 12
Parastomal Hernia
Parastomal hernia formation makes up the largest proportion of ostomy-related complications that may require surgical intervention, with reported rates up to 57%. 13 Urgent indications for repair remain in those seen with any hernia such as incarceration or strangulation; however, nonurgent indications are far more common. In general, repair in the elective setting is indicated for patients who suffer from symptoms such as intermittent obstruction, incarceration, pain, and difficulty in retaining an appliance on the stoma despite conservative measures such as ostomy belts, filler rings, and adhesives. There are numerous published studies and meta-analysis discussing repair; however, data are difficult to compare due to the high variety in classification and in practice. In an attempt to characterize hernias in a uniform manner, the European Hernia Society proposed a classification based on the hernia defect size (small is ≤5 cm) and the presence of a concomitant incisional hernia 14 ( Table 1 ; Fig. 1 ).
Table 1. European Hernia Society grid for classification of parastomal hernia.
| Parastomal hernia classification | Small ≤ 5 cm | Large >5 cm | |
|---|---|---|---|
| Concomitant incisional hernia | No | I | III |
| Yes | II | IV | |
| Primary | Recurrent | ||
Fig. 1.

Large parastomal hernia.
The simplest and perhaps the most attractive way to fix a parastomal hernia is by direct repair, which includes dissecting down to the fascial level and primary closure of the excess fascial defect around the bowel. However, as with any direct suture repair of a hernia, the recurrence rates are unacceptably high, with some studies showing rates of 46 to 100%. 2 Relocation of the hernia to another site provides better outcomes in the short term; however, longer follow-up results are unfavorable and recurrences range up to 40%. 15 In search of the cause for hernia formation, the high rate of recurrence over time has steered attention away from the traditionally believed causes of parastomal hernia formation such as an excessively large fascial aperture and emergency surgery. Rather, Nastro et al identified underlying patient-related factors such as respiratory comorbidities, obesity, diabetes, and surgery for malignancy at much higher rates in development of parastomal hernias than the traditional causes. 16
As with repair in non–ostomy-related hernias, recurrence rates with mesh repair compared favorably to direct repair in a systematic review by Hansson et al, ranging from only 6.9 to 17%. 17 Al Shakarchi and Williams confirmed similar results in a review of open non-mesh fascial repair versus mesh repair and found recurrence rates were substantially lower with use of mesh at 7.9 to 13.8%. The exact preference to onlay, sublay, or underlay was not able to be determined due to insufficient power in each arm. 18 With all the popular transversus abdominis release (TAR) with mesh placement has gained for large incisional hernias, a new method of open parastomal hernia repair with retromuscular mesh reinforcement is likely to gain further popularity as it maintains the biomechanics of a functional abdominal wall and is reinforced with synthetic mesh. 19
Several alternatives to traditional open repair with mesh have been proposed. The Sugarbaker technique, in which the bowel travels between a supportive mesh flap and the peritoneum prior to the exit site, has been widely modeled. 20 Laparoscopic parastomal hernia repair was also studied in a meta-analysis of 15 articles for a total of 469 patients by DeAsis et al. They reported an overall 17.4% recurrence rate, with a favorable 10.2% (95% confidence interval [CI]: 3.9–19.0) recurrence rate for a modified laparoscopic Sugarbaker approach, and a 27.9% (95% CI: 12.3–46.9) for the laparoscopic keyhole approach. 21 In a review for the Clinical Practice Guidelines for Ostomy Surgery prepared by the American Society of Colon and Rectal Surgeons, the committee concluded “ laparoscopic parastomal hernia repair with mesh may be a safe alternative to open mesh repair .” 22
Considering the high rates of parastomal hernia incidence and the challenges of repair, steps may be employed at the initial operation that would minimize the risk of hernia development. At the core of this approach is creating the stomal defect as small as possible and to bring the stoma through the rectus muscle. A technique that does not involve use of mesh, referred to as extraperitoneal colostomy, where the mobilized proximal colon is tunneled between the peritoneum and the abdominal wall muscles to the future stoma location, was introduced in 1958 and has been revisited as a preventive measure for parastomal hernia. A meta-analysis identified 347 patients who had an extraperitoneal colostomy construction and compared it to 701 patients with a traditional transperitoneal colostomy and found a significantly lower rate of hernia rate of 6.3% in the extraperitoneal group versus 17.8% of the traditional method without a change in stoma necrosis rates. 23
In regard to the use of a mesh at the initial operation, large pore light-weight synthetic mesh and biologic meshes have raised surgeons' comfort level in mesh placement in clean contaminated fields with relatively low infection rates, ranging from 0 to 13%. 2 In a meta-analysis of randomized controlled trials comparing prophylactic mesh versus no mesh on the incidence of parastomal hernia formation, mesh was found to favorably reduce the incidence of clinically detected hernia from 32.4 to 10.8% ( p = 0.001) and radiologically detected rates from 55.3 to 34.6% ( p = 0.01), without additional risk of stoma-related complications. 24 A second meta-analysis of 10 randomized trials of a total of 649 patients confirmed similar findings with prophylactic mesh placement resulting in a 65% ( p = 0.02) reduction in hernia repair requirement without increasing rates of parastomal infection, stomal stenosis, or necrosis. 25 The studies concluded that prophylactic mesh placement at the time of stoma creation reduces parastomal hernia formation and subsequent requirement for repair without an increase in mesh-related complications. The type of mesh placement and specific patient characteristics that benefit from those repair types are still subject to debate as further studies emerge for comparison.
Stomal Prolapse
Stomal prolapse, referring to an intussusception of the intestine through an ostomy, is a common complication that may be seen with both loop and end ostomies, although the highest rates are up to 42% for loop transverse colostomies. 26 The pathophysiology is poorly understood and was originally proposed to be related to conditions that raise intra-abdominal pressures and redundancy of proximate bowel segments. However, fixation of the bowel or mesentery as a preventive measure has not been shown to be effective in preventing prolapse. Furthermore, the defunctionalized distal limb of loop colostomies prolapses more frequently than the proximal limb, providing further evidence against a normal direction peristalsis as a contributing factor. 2 27 28 End-loop colostomies where the bowel is divided just distal to the ostomy defect is a viable prophylactic option to eliminate distal limb prolapse in high-risk situations. 2
Stoma prolapse may be categorized as “fixed,” in which the prolapsed tissue remains in eversion and the excessive length of bowel remains outside of the body at all times, or as the more common “sliding” prolapse, where the tissue intermittently protrudes out through the stoma orifice. Although the appearance of prolapse may be unsettling for the patient, surgical treatment is indicated mainly in those who suffer from symptoms ( Fig. 2 ). The most common complaint that leads to elective repair is problems with ostomy care, where the appliance does not adhere to the skin and fails to respond to conservative measures, further subjecting the prolapsed intestine itself to recurrent trauma and bleeding. Emergent indications include incarceration, obstruction, or actual strangulation of the prolapsed tissue. In case of acute prolapse with incarceration without strangulation, application of sugar onto the stoma to withdraw the edema and allow for gentle manipulation back into the peritoneum has been successfully employed. 27 29 Evidence of mucosal ischemia and strangulation warrants emergent surgical intervention. Extremely rare cases of parastomal evisceration have also been described where a patient suffers from parastomal hernia and a prolapse. 30
Fig. 2.

Stomal prolapse.
Stomal prolapse is generally treated with disconnection of the intestine just inside of mucocutaneous junction, eversion of the prolapsed segment, and resection of the redundant bowel. The ostomy is then rematured. The general recommendation is to disconnect the prolapsed ostomy just inside of the mucocutaneous junction to maintain the same size of the ostomy, or else a much wider ostomy is created. The rim of mucosa that is left on the skin should be very short (1–2 mm) and be able to survive with nutrients from the immediately surrounding skin. A Delorme-like technique without complete transection of the bowel and entry into the peritoneum may also be utilized in select cases, such as presence of ascites, presence of peritoneal dialysis catheter, or other conditions where avoidance of peritoneal entry is desired. In this technique, the mucosa is separated for the full length of the prolapse and plicating sutures are placed in the muscular wall from the mucocutaneous junction to the apex. 27 31 Most repairs and revisions of ostomies for prolapse are often possible with sedation and local anesthesia alone. 32
Mucocutaneous Separation/Retraction/Stomal Ischemia/Necrosis
Early postoperative mucocutaneous separation, retraction of the stoma, and necrosis of the stoma represent the range of complications that result from excessive tension, vascular compromise, or an inadequate fascial or skin defect creation. The end result, if left untreated, is stenosis and challenging ostomy care. In general, the blood supply is deemed adequate if a cut stoma has “nuisance” bleeding that requires a stitch or cauterization. If there is any doubt, it is much better to reopen the patient and provide either more length or a better vascularized segment than to subject the patient to an emergent laparotomy days after the initial operation or a stoma that retracts and has stenosis complicating ostomy care. In a high-quality, multicenter observational study of ostomy function, there was a strong association between ostomy protrusion above the skin surface and ability of the patient to successfully care for the ostomy. 33 One should aim for an ileostomy to protrude around 2 cm above the skin and a colostomy approximately 1 cm. In general, rates of stoma stricture/stenosis are 1 to 10%. 2 27 These rates are higher in Crohn's patients (likely due to inflammation and shorter mesentery) and those with polyposis syndromes. 34 35 36 Any late-onset stricture warrants a thorough investigation such an endoscopy through the stoma to rule out ongoing inflammation or an underlying malignancy.
In the setting where there is concern of ischemic within a few days after the operation, length of mucosal ischemia may be evaluated by insertion of a test tube into the stoma and evaluation of the mucosa with a light source. If the depth of ischemic mucosa extends below the fascia, then the concern for ischemia and full-thickness bowel involvement and perforation warrants a return trip to the operating room. If the ischemia is superficial to the fascial level, then the ostomy may be observed expecting stenosis and challenges with ostomy care. In general, the key to management of stomal strictures is prevention by ensuring adequate length with a tension-free mucocutaneous junction ( Fig. 3A , B ). A sustaining rod (ostomy bridge) in loop ileostomies was shown not to alter retraction rates in a multicenter, randomized controlled trial and in fact, ostomy necrosis or partial necrosis rates were higher in the rod group. In this study, the most compelling factor in suffering from ostomy necrosis was a high body mass index (BMI > 26), which was associated with a fivefold increase in odds ratio for severe stoma complications. 37 Unfortunately, once a stenosis does occur, repeat dilation only provides temporary relief and results in further fibrosis and restenosis. 38 Outside of the acute setting, stomal strictures require ostomy revision which may be performed either through the ostomy site if stenosis is at the distal end but only if adequate mobilization through the ostomy incision is possible. It generally requires a laparoscopic or open laparotomy to free up the proximal bowel and provide adequate length and ensure a viable blood supply. 28
Fig. 3.
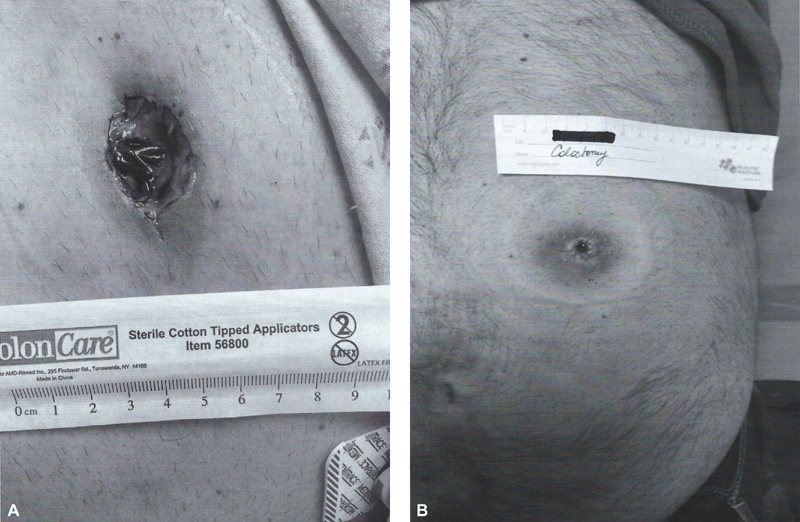
( A ) Mucocutaneous junction separation secondary to ischemia 2 days after surgery. ( B ) Ostomy stricture secondary to ischemia 3 months after surgery.
Peristomal Skin Irritation and Infection
Peristomal skin irritation or irritant contact dermatitis is the most frequently observed complication with rates up to 48.7% in a multicenter, retrospective study ( Fig. 4 ). It presents with erythema, pain, and skin ulceration usually as a direct result of (1) chemical dermatitis due to effluent or succus exposure or (2) desquamation of the skin caused by the trauma of frequent appliance changes. However, if simple erythema or early disease does not get addressed, the result of the aforementioned may lead to ulceration and full-thickness skin necrosis. 39
Fig. 4.

Peristomal contact dermatitis.
Once a peristomal skin irritation is identified, then it should be aggressively pursued and the impact of having a trained enterostomal nurse cannot be underestimated. The treatment usually starts with confirmation of appropriately sized opening of the appliance. It should be cut just to fit on the outer diameter of the stoma. There should not be a rim of visible skin outside of the mucocutaneous junction. Stomal adhesive paste and other skin protectants can be used to maintain the integrity of the skin and provide further adhesion to keep the appliance secured for a longer period. There are numerous other modalities that are used by experienced WOC nurses such as convex appliances, peristomal hernia belts, or custom-fitted ostomy appliances, which is beyond the scope of this article. The benefit of a WOC nurse regarding prevention of peristomal dermatitis was further reinforced by a study where the rates were significantly worse among patients without preoperative marking and education by a WOC nurse (22.9 vs. 46%, p < 0.001). In addition to the local skin issue, irritant contact dermatitis negatively affected quality of life on a Hope Quality of Life Ostomy Questionnaire with affected patients suffering a significantly lower quality of life total scores (mean: 6.64 [SD: 1.64], p = 0.02). 40 41
Other skin conditions include infectious sources. The dark, warm, moist environment of the peristomal skin yields itself to Candida albicans infections or bacterial infections and folliculitis with pathogenic skin flora such as Staphylococcus aureus . Most of these superficial infections may be treated with the appropriate antifungal/antibacterial powder and improved ostomy care. However, due caution is warranted as extreme cases of infection and peristomal necrotizing fasciitis have been reported, requiring extensive debridement and intense treatment. 42
In the setting of Crohn's disease and ulcerative colitis, where the prevalence of psoriasis is higher, 11.2 and 5.7%, respectively, versus 1.3 to 2% in the general population, an erythematous scaly plaque that goes beyond the appliance wafer should raise the suspicion for peristomal psoriasis. These are mostly treated with nongreasy topical steroids but may require systemic anti-inflammatory agents. 43
Further, trauma to the stoma from an ill-fitting appliance or other mechanical sources may lead to inflammatory granulomas and polyps ( Fig. 5 ). These can usually be treated with silver nitrate applications. However, patients with adenoma-forming conditions or underlying chronic inflammatory diseases such as Crohn's disease are at higher risks of developing carcinoma at an ostomy site. In a study of 36 primary adenocarcinomas at ileostomy sites, Metzger et al showed an average of 27 years between the index operation and the development of the parastomal malignant lesion. Hence, polyp development long after surgery usually warrants a biopsy and pathological evaluation. 44 45
Fig. 5.

Multiple granulomas from trauma from an ill-fitting appliance.
Peristomal Fistula, Ulceration, IBD
In addition to the aforementioned complications that may occur with any ostomate, Crohn's patients are subject to the development of issues that are exclusive to their underlying disease process. Peristomal fistulas, strictures, and recurrence of the disease process within a short distance from the ostomy are common reasons that make reconstruction of an ileostomy unusually frequent in Crohn's patients. 5 46 These patients may present with nonhealing ulcers or abscesses that eventually express bowel contents ( Fig. 6 ). In a study of 92 Crohn's patients with more than 5-year follow-up with a 30% reoperation rate, the preoperative clinical indication was prestomal recurrence in only 12%, while typical stomal complications leading to surgery were identified in the remaining 88%. However, in examination of the pathological specimen, 67% of the operated patients had evidence of ileal recurrence with a statistically significant association with fibrotic recurrence and stoma stenosis/retraction and a trend for association between penetrating recurrence and peristomal ulceration. Hence, the study concluded that most reoperations after ileostomy construction in Crohn's patients are at least associated with underlying recurrent inflammatory activity. 5
Fig. 6.

Peristomal fistula in a Crohn's patient—note two fistula openings and incision and drainage site.
Parastomal Pyoderma Gangrenosum
Pyoderma gangrenosum (PG) is an ulcerative, inflammatory skin disorder associated with underlying systemic disease up to 50% of cases. IBD, rheumatoid arthritis, and some hematologic malignancies may manifest with PG. 47 It occurs in approximately 1 to 5% of all IBD patients. 48 Clinically, parastomal PG appears as a painful superficial ulcer with a well-defined erythematous border ( Fig. 7 ). Strands of epidermis may be present and it often goes undiagnosed. It is attributed with the development of pustules and ulceration from local trauma or allergic reaction from the ostomy appliance. The diagnosis is made based on clinical evaluation by an experienced ostomy practitioner and is considered a diagnosis of exclusion. Biopsies are necessary to exclude other causes of nonhealing ulcerations, particularly skin neoplasms or infections. Medical treatment is not uniform and outside of general measures such as controlling the underlying disease, and avoiding trauma may be categorized into topical, systemic, and targeted therapy.
Fig. 7.

Pyoderma gangrenosum.
Topical therapy includes corticosteroids and direct injection of corticosteroids (Kenalog) into the lesion. Topical tacrolimus and dapsone have also been shown to be of benefit. Systemic therapy ranges from the first-line therapy corticosteroids to second-line agents such as cyclosporine and immunomodulators. The newer targeted therapy against tumor necrosis factor, interleukin 1, and others have changed the paradigm in favor of providing cure as opposed to just control; however, rates of complete healing only range at a challenging 47% with recurrence rates as high as 30%. 49
In general, PG is usually a representation of underlying ongoing inflammation and medical management is the first line of therapy. Surgery is reserved for situations where the lesion is being excised during an ostomy reversal or if the stoma is relocated for other reasons. 47
Footnotes
Conflict of Interest None declared.
References
- 1.Fazio V W, Church J M, Wu J S. New York, NY: Springer Science; 2012. Atlas of Intestinal Stomas; pp. 33–33. [Google Scholar]
- 2.Kwiatt M, Kawata M. Avoidance and management of stomal complications. Clin Colon Rectal Surg. 2013;26(02):112–121. doi: 10.1055/s-0033-1348050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Shabbir J, Britton D C. Stoma complications: a literature overview. Colorectal Dis. 2010;12(10):958–964. doi: 10.1111/j.1463-1318.2009.02006.x. [DOI] [PubMed] [Google Scholar]
- 4.Robertson I, Leung E, Hughes D et al. Prospective analysis of stoma-related complications. Colorectal Dis. 2005;7(03):279–285. doi: 10.1111/j.1463-1318.2005.00785.x. [DOI] [PubMed] [Google Scholar]
- 5.Ecker K W, Gierend M, Kreissler-Haag D, Feifel G. Reoperations at the ileostomy in Crohn's disease reflect inflammatory activity rather than surgical stoma complications alone. Int J Colorectal Dis. 2001;16(02):76–80. doi: 10.1007/s003840000279. [DOI] [PubMed] [Google Scholar]
- 6.Person B, Ifargan R, Lachter J, Duek S D, Kluger Y, Assalia A. The impact of preoperative stoma site marking on the incidence of complications, quality of life, and patient's independence. Dis Colon Rectum. 2012;55(07):783–787. doi: 10.1097/DCR.0b013e31825763f0. [DOI] [PubMed] [Google Scholar]
- 7.Prepared by the Standards Development Committee of the United Ostomy Association with the Assistance of Prospect Associates.National guidelines for enterostomal patient education Dis Colon Rectum 19943706559–563. [PubMed] [Google Scholar]
- 8.Colwell J C, McNichol L, Boarini J. North American wound, ostomy and continence and enterostomal therapy nurses current ostomy care practice related to peristomal skin issues. J Wound Ostomy Continence Nurs. 2017;44(03):257–261. doi: 10.1097/WON.0000000000000324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Back I R, Marcon S S, Gaino N M, Vulcano D SB, Dorna M S, Sassaki L Y. Body Composition in patients with Crohn's disease and ulcerative colitis. Arq Gastroenterol. 2017;54(02):109–114. doi: 10.1590/S0004-2803.201700000-02. [DOI] [PubMed] [Google Scholar]
- 10.De Raet J, Delvaux G, Haentjens P, Van Nieuwenhove Y. Waist circumference is an independent risk factor for the development of parastomal hernia after permanent colostomy. Dis Colon Rectum. 2008;51(12):1806–1809. doi: 10.1007/s10350-008-9366-5. [DOI] [PubMed] [Google Scholar]
- 11.Beck S J. Stoma issues in the obese patient. Clin Colon Rectal Surg. 2011;24(04):259–262. doi: 10.1055/s-0031-1295689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cataldo P A. Technical tips for stoma creation in the challenging patient. Clin Colon Rectal Surg. 2008;21(01):17–22. doi: 10.1055/s-2008-1055317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wang S, Wang W, Zhu B, Song G, Jiang C. Efficacy of prophylactic mesh in end-colostomy construction: a systemic review and meta-analysis of randomized controlled trials. World J Surg. 2016;40(10):2528–2536. doi: 10.1007/s00268-016-3576-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Śmietański M, Szczepkowski M, Alexandre J A et al. European Hernia Society classification of parastomal hernias. Hernia. 2014;18(01):1–6. doi: 10.1007/s10029-013-1162-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Riansuwan W, Hull T L, Millan M M, Hammel J P. Surgery of recurrent parastomal hernia: direct repair or relocation? Colorectal Dis. 2010;12(07):681–686. doi: 10.1111/j.1463-1318.2009.01868.x. [DOI] [PubMed] [Google Scholar]
- 16.Nastro P, Knowles C H, McGrath A, Heyman B, Porrett T R, Lunniss P J. Complications of intestinal stomas. Br J Surg. 2010;97(12):1885–1889. doi: 10.1002/bjs.7259. [DOI] [PubMed] [Google Scholar]
- 17.Hansson B M, Slater N J, van der Velden A S et al. Surgical techniques for parastomal hernia repair: a systematic review of the literature. Ann Surg. 2012;255(04):685–695. doi: 10.1097/SLA.0b013e31824b44b1. [DOI] [PubMed] [Google Scholar]
- 18.Al Shakarchi J, Williams J G. Systematic review of open techniques for parastomal hernia repair. Tech Coloproctol. 2014;18(05):427–432. doi: 10.1007/s10151-013-1110-z. [DOI] [PubMed] [Google Scholar]
- 19.Pauli E M, Juza R M, Winder J S. How I do it: novel parastomal herniorrhaphy utilizing transversus abdominis release. Hernia. 2016;20(04):547–552. doi: 10.1007/s10029-016-1489-3. [DOI] [PubMed] [Google Scholar]
- 20.Sugarbaker P H. Prosthetic mesh repair of large hernias at the site of colonic stomas. Surg Gynecol Obstet. 1980;150(04):576–578. [PubMed] [Google Scholar]
- 21.DeAsis F J, Lapin B, Gitelis M E, Ujiki M B. Current state of laparoscopic parastomal hernia repair: a meta-analysis. World J Gastroenterol. 2015;21(28):8670–8677. doi: 10.3748/wjg.v21.i28.8670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hendren S, Hammond K, Glasgow S C et al. Clinical practice guidelines for ostomy surgery. Dis Colon Rectum. 2015;58(04):375–387. doi: 10.1097/DCR.0000000000000347. [DOI] [PubMed] [Google Scholar]
- 23.Kroese L F, de Smet G H, Jeekel J, Kleinrensink G J, Lange J F. Systemic review and meta-analysis of extraperitoneal versus transperitoneal colostomy for preventing parastomal hernia. Dis Colon Rectum. 2016;59(07):688–695. doi: 10.1097/DCR.0000000000000605. [DOI] [PubMed] [Google Scholar]
- 24.Chapman S J, Wood B, Drake T M, Young N, Jayne D G. Systemic review and meta-analysis of prophylactic mesh during primary stoma formation to prevent parastomal hernia. Dis Colon Rectum. 2017;60(01):107–115. doi: 10.1097/DCR.0000000000000670. [DOI] [PubMed] [Google Scholar]
- 25.Cross A J, Buchwald P L, Frizelle F A, Eglinton T W. Meta-analysis of prophylactic mesh to prevent parastomal hernia. Br J Surg. 2017;104(03):179–186. doi: 10.1002/bjs.10402. [DOI] [PubMed] [Google Scholar]
- 26.Park J J, Del Pino A, Orsay C P et al. Stoma complications: the Cook County Hospital experience. Dis Colon Rectum. 1999;42(12):1575–1580. doi: 10.1007/BF02236210. [DOI] [PubMed] [Google Scholar]
- 27.Bafford A C, Irani J L. Management and complications of stomas. Surg Clin North Am. 2013;93(01):145–166. doi: 10.1016/j.suc.2012.09.015. [DOI] [PubMed] [Google Scholar]
- 28.Steel M CA, Wu J S. Late stomal complications. Clin Colon Rectal Surg. 2002;15(93):199–206. [Google Scholar]
- 29.Myers J O, Rothenberger D A. Sugar in the reduction of incarcerated prolapsed bowel. Report of two cases. Dis Colon Rectum. 1991;34(05):416–418. doi: 10.1007/BF02053694. [DOI] [PubMed] [Google Scholar]
- 30.Lolis E D, Savvidou P, Vardas K, Loutseti D, Koutsoumpas V. Parastomal evisceration as an extremely rare complication of a common procedure. Ann R Coll Surg Engl. 2015;97(07):e103–e104. doi: 10.1308/rcsann.2015.0017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Marrosu A, Paliogiannis P, Sassu M A, Attene F, Trignano M. Correction of an end colostomy prolapse with the Delorme technique. A case report. Ann Ital Chir. 2012;83(06):567–569. [PubMed] [Google Scholar]
- 32.Papadopoulos V, Bangeas P, Xanthopoulou K, Paramythiotis D, Michalopoulos A. Stoma prolapse handmade repair under local anesthesia with variation of Altemeier method in severe patients: a case report and review of the literature. J Surg Case Rep. 2017;2017(02):rjx027. doi: 10.1093/jscr/rjx027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Parmar K L, Zammit M, Smith A, Kenyon D, Less N P; Greater Manchester and Cheshire Colorectal Cancer Network.A prospective audit of early stoma complications in colorectal cancer treatment throughout the Greater Manchester and Cheshire colorectal cancer network Colorectal Dis 201113935–938. [DOI] [PubMed] [Google Scholar]
- 34.Kaidar-Person O, Person B, Wexner S D. Complications of construction and closure of temporary loop ileostomy. J Am Coll Surg. 2005;201(05):759–773. doi: 10.1016/j.jamcollsurg.2005.06.002. [DOI] [PubMed] [Google Scholar]
- 35.Takahashi K, Funayama Y, Fukushima K et al. Stoma-related complications in inflammatory bowel disease. Dig Surg. 2008;25(01):16–20. doi: 10.1159/000117818. [DOI] [PubMed] [Google Scholar]
- 36.Gadacz T R, McFadden D W, Gabrielson E W, Ullah A, Berman J J. Adenocarcinoma of the ileostomy: the latent risk of cancer after colectomy for ulcerative colitis and familial polyposis. Surgery. 1990;107(06):698–703. [PubMed] [Google Scholar]
- 37.Zindel J, Gygax C, Studer P et al. A sustaining rod increases necrosis of loop ileostomies: a randomized controlled trial. Int J Colorectal Dis. 2017;32(06):875–881. doi: 10.1007/s00384-017-2813-9. [DOI] [PubMed] [Google Scholar]
- 38.Nunoo R, Asgerisson T. Stomal strictures. Semin Colon Rectal Surg. 2012;23(01):10–12. [Google Scholar]
- 39.Kann B R. Early stomal complications. Clin Colon Rectal Surg. 2008;(21):23–30. doi: 10.1055/s-2008-1055318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Maydick-Youngberg D. A descriptive study to explore the effect of peristomal skin complications on quality of life of adults with a permanent ostomy. Ostomy Wound Manage. 2017;63(05):10–23. [PubMed] [Google Scholar]
- 41.Baykara Z G, Demir S G, Karadag A et al. A multicenter, retrospective study to evaluate the effect of preoperative stoma site marking on stomal and peristomal complications. Ostomy Wound Manage. 2014;60(05):16–26. [PubMed] [Google Scholar]
- 42.Peker K D, Ilhan B M. Rare complications of stomas: peristomal necrotizing fasciitis. Wounds. 2016;28(12):E47–E52. [PubMed] [Google Scholar]
- 43.Marshall C, Woodmansey S, Lyon C C. Peristomal psoriasis. Clin Exp Dermatol. 2017;42(03):282–286. doi: 10.1111/ced.13041. [DOI] [PubMed] [Google Scholar]
- 44.Metzger P P, Slappy A L, Chua H K, Menke D M. Adenocarcinoma developing at an ileostomy: report of a case and review of the literature. Dis Colon Rectum. 2008;51(05):604–609. doi: 10.1007/s10350-007-9188-x. [DOI] [PubMed] [Google Scholar]
- 45.Procaccino L, Rehman S, Abdurakhmanov A et al. Adenocarcinoma arising at ileostomy sites: Two cases and a review of the literature. World J Gastrointest Surg. 2015;7(06):94–97. doi: 10.4240/wjgs.v7.i6.94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Greenstein A J, Dicker A, Meyers S, Aufses A H., Jr Periileostomy fistulae in Crohn's disease. Ann Surg. 1983;197(02):179–182. doi: 10.1097/00000658-198302000-00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Lyon C C, Smith A J, Beck M H, Wong G A, Griffiths C E. Parastomal pyoderma gangrenosum: clinical features and management. J Am Acad Dermatol. 2000;42(06):992–1002. [PubMed] [Google Scholar]
- 48.Poritz L S, Lebo M A, Bobb A D, Ardell C M, Koltun W A. Management of peristomal pyoderma gangrenosum. J Am Coll Surg. 2008;206(02):311–315. doi: 10.1016/j.jamcollsurg.2007.07.023. [DOI] [PubMed] [Google Scholar]
- 49.Alavi A, French L E, Davis M D, Brassard A, Kirsner R S. Pyoderma gangrenosum: an update on pathophysiology, diagnosis and treatment. Am J Clin Dermatol. 2017;18(03):355–372. doi: 10.1007/s40257-017-0251-7. [DOI] [PubMed] [Google Scholar]