

Summary
Few studies have assessed the extent of psychoactive drug consumption in the occupational setting. The trucking sector, in particular, is an important cause for concern, since psychoactive substance use has a relevant impact on the drivers’ health and safety, increasing the risk of injuries and traffic accidents, potentially affecting the general public health as well. A systematic review of the literature and meta-analysis was performed in order to provide Occupational Health Professionals and policy-makers with an updated epidemiological perspective regarding this important issue. The results showed a prevalence of overall drug consumption of 27.6% [95%CI 17.8-40.1], particularly high considering illicit CNS-stimulants (amphetamine consumption of 21.3% [95%CI 15.7-28.1], and cocaine consumption of 2.2% [95%CI 1.2-4.1]). It appears that truck-drivers choose stimulant substances as a form of performance enhancing drug, in order to increase productivity. However, chronic and high dose consumption has been shown to decrease driving skills, placing these professional drivers at risk for health and road safety. Further research is required, particularly in Europe, in order to fill the knowledge gap and improve the strength of evidence.
Keywords: Truck-drivers, Psychoactive drug consumption, Systematic review, Meta-analysis and meta-regression, Occupational health and wellbeing, Road safety
Introduction
Illicit drug and psychoactive substance misuse is an important contributor to the global burden of disease. According to data presented in the World Drug Review 2018 published by the United Nations Office on Drugs and Crime (UNODC), 5.6% of the global population aged 15-64 years has used drugs in the previous year. Moreover, medical and non-medical prescription drug abuse, especially opioids, is reaching epidemic proportions in many parts of the world [1].
These figures represent an increasing trend over the years, especially in developed countries. In its European Drug Report 2018, the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) has reported an annual prevalence of drug users equal to 7.4%, and drug-induced mortality surpassing 5 thousands deaths in EU countries [2]. Since working age population makes up most of the overall population, substance use among workers is of primary interest from an occupational perspective. Indeed, it can cause loss of productivity, workplace injuries, absenteeism and increased illness [3].
Few international and national surveys using a systematic approach have studied drug use in the workplace: the Center for Behavioral Health Statistics and Quality (CBHSQ) report regarding substance use and substance use disorder by industry published by the Substance Abuse and Mental Health Services Administration (SAMHSA) reported an annual prevalence of illicit drug use of 9.5% among workers in the USA between the years 2008-2012 [3]. In Europe, there is a lack of up-to-date and high quality epidemiological data about prevalence of drug use in the workplace. The trucking sector, in particular, is an important cause for concern: truck-drivers are a vulnerable working population due to a wide variety of hazards [4-6] including physical and ergonomic ones with the risk of developing musculoskeletal disorders [7], hypertension [8], obstructive sleep apnea (OSA) and sleep deprivation [9, 10], exposure to diesel exhaust and risk of developing lung cancer [11]. Stressful conditions due to irregular working schedules, night shifts, being distant from families for long periods [12], the need for constant mental alertness, and high productivity demands [13] increase risky behaviors such as smoking, drinking, using psychoactive substances, and having casual sexual contacts [14]. In particular, psychoactive drugs affect the functioning of the brain by delaying cognitive and executive functions, which may lead to impaired driving [15]. These can have a relevant impact on truck-drivers’ health, as well as on work safety, increasing the risk of injuries and traffic accidents [16, 17], often fatal: 21% of all lethal injuries occurred among “transportation and warehousing” workers in Iowa in 2005-2009 had a positive toxicology test for substance use [18]. Indeed, while the effects of ethanol on driving have been thoroughly studied by the literature, as shown in the previously published article by the Authors [19], the impact of other substances on driving is not as clear. The vast variety of substance classes, each with specific effects on physical and mental health, requires a detailed understanding of the interaction and effect on work specific tasks. Italian law has identified several occupational categories as at risk of harm to their and others’ health and safety, to which it prohibits drug use, even occasional [20]. Nevertheless, not much is known regarding on site health surveillance and drug testing in this occupational sector.
A comprehensive analysis of this issue can adequately inform policy-makers in order to address legislative shortcomings and implement preventive measures in the workplace, reducing in turn the contribution of work-related drug health problems arising from working conditions to the general public.
The aim of the present systematic review and meta-analysis is to provide Occupational Health Professionals and policy-makers with updated epidemiological data regarding drug consumption among truck-drivers, in order to reduce the knowledge gap, and in turn to allow the implementation of effective countermeasures taking place in the workplace. The reduction of drug-related health problems induced by working conditions will also beneficially contribute to public health. This study adds to the findings regarding alcohol consumption in this occupational category, presented in our previously published article, and significantly updates and expands, through a rigorous quantitative analysis, the work performed by Girotto and colleagues [4].
Materials and methods
SYSTEMATIC REVIEW
The current systematic review of the literature with meta-analysis and meta-regressions is reported according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines [21]. The study protocol was registered in the “International database of prospectively registered systematic reviews in health and social care” (PROSPERO database [22]; registration code CRD42016037077) [23]. The results of the study are reported in line with the PRISMA guidelines [24].
Briefly, a comprehensive pool of scholarly databases (namely, PubMed/MEDLINE (NLM), Scopus, SciVerse ScienceDirect, Science Citation Index Expanded (SCIE) and Social Sciences Citation Index from ISI/Web of Science, ProQuest Research Library, ABI/INFORM, CBCA), via the UNO per TUTTI Primo Central (Ex Libris) platform) was searched from inception using the following string of keywords: (truckers OR truck-drivers OR lorry OR commercial vehicles OR large good vehicles OR large vehicles OR heavy vehicles OR long vehicles OR trucking industry OR haul transport) AND (drugs OR psychostimulants OR psychoactive substances OR amphetamine OR benzodiazepines OR cocaine OR heroin OR opioids OR cannabis OR cannabinoids). Medical Subject Headings (MeSH) terms and wild-card option (truncated words) were used when necessary. Last search was carried out on 3rd December 2018. No language restriction or time filter were applied. Gray literature was consulted via Google Scholar. Further details of the search strategy are reported in Table I.
Tab. I.
Pooled drug consumption rates and respective ranges stratified according to the type of study (studies based on questionnaires, urine or saliva samples).
| Drug | Drug consumption | ||
|---|---|---|---|
| Questionnaire | Urine sample | Saliva sample | |
| Amphetamine | 21.3% [95%CI 15.7-28.1] | 3.8% [95%CI 1.7-8.2] | 1.3% [95%CI 0.7-2.4] |
| Benzodiazepines | 1.0% [95%CI 0.1-6.1] | 0.4% [95%CI 0.2-0.6] | NA |
| Cannabis | 5.9% [95%CI 3.5-9.8] | 2.1% [95%CI 1.0-4.3] | 0.5% [95% 0.3-1.0%] |
| Cocaine | 2.2% [95%CI 1.2-4.1] | 1.1% [95%CI 0.7-2.0] | 1.1% [95%CI 0.4-3.1] |
| Opioid | 4.3% [95%CI 0.6-26.4] | 2.0% [95%CI 0.6-6.6] | NA |
| OTC stimulants | 4.1% [95%CI 2.7-6.2] | 9.0% [95%CI 4.3-18.0] | NA |
| Overall drug consumption | 27.6% [95%CI 17.8-40.1] | 6.1% [95%CI 2.9-12.4] | 4.1% [95%CI 1.2-13.1] |
| Poliabuse | 2.7% [95%CI 0.2-25.6] | 0.6% [95%CI 0.1-4.8] | 0.3% [95%CI 0.1-0.7] |
NA: not available; OTC: over-the-counter.
Literature search was performed by 2 researchers independently (NLB and AR). In case of disagreement, consensus was reached through discussion and consultation. Based on the PECO criteria, articles were included if: 1) focused on truck-drivers (P = truck-drivers); 2) investigating drug consumption (E = exposure to abuse substances); 3) stratifying according to parameters such as age, gender, marital status, experience years, mean distance travelled (per trip), work-load, night-shift or educational level, in terms of primary schooling level (C = any comparison); and 4) reporting prevalence rate of drug consumption (O = drug consumption rate). Concerning the study design, articles were selected if devised as prevalence studies. Articles were excluded if not meeting with the above-stated PECO criteria and if designed as letter to editor, editorial, commentary, expert opinion, review article (of any type).
Reviews were, anyways, scanned for reducing the chance of missing potentially relevant articles. Relevant information was extracted from each included article by two researchers independently (NLB and AR). In case of disagreement, a third researcher (GD) acted as final referee. For data extraction, an ad hoc Excel spreadsheet was designed and utilized. Besides tables, relevant information was summarized by means of a narrative review.
METHODOLOGICAL APPRAISAL OF STUDIES QUALITY
Study quality was assessed utilizing the “Joanna Briggs Institute Critical Appraisal tools for use in JBI Systematic Reviews-Checklist for Prevalence Studies”. This tool explores different domains of quality: namely, 1) the appropriateness of the sample frame to address the target population; 2) the participants sampling technique; 3) the adequateness of the sample size; 4) the completeness of the description and details concerning the study subjects and the setting; 5) the coverage of the sample; 6) the validity of the methods; and 7) their reliability; 8) the appropriateness of the statistical analyses; and, finally, 9) the adequateness of the response rate. Based on the JBI tool, studies were deemed of high, medium and low quality, respectively.
META-ANALYSIS
For each outcome (amphetamine, benzodiazepines, cannabis, cocaine, heroin, opioid, OTC stimulants, overall drug consumption and poliabuse rates), effect size (ES) was computed pooling together the various prevalence rates, using the logit transformation approach.
Heterogeneity among studies was quantitatively assessed computing the I2 statistics. An amount greater than 50% was considered statistically significant [25, 26]. Based on the amount of heterogeneity, a fixed- or a random-effect model was chosen.
Publication bias was studied both by visually inspecting the funnel plot in terms of asymmetry and by computing the Egger’s regression test [27] and the Duval and Tweedie’s trim-and-fill analysis [28]. Sensitivity analyses and cumulative meta-analyses were further performed, in order to verify the reliability and the consistency of the findings.
All analyses were carried out with the commercial software Comprehensive Meta-Analysis (CMA version 3.0, for Windows).
For further details, the reader is referred to our previous publication [19].
Results
SYSTEMATIC REVIEW
The initial search resulted in a pool of 174,712 articles. After deleting duplicates, a set of 152,367 unique items was obtained. Screening titles and/or abstracts led to the exclusion of 153,132 items. A pool of articles was retrieved and accessed in full-text. Finally, 51 studies were included (Fig. 1).
Fig. 1.
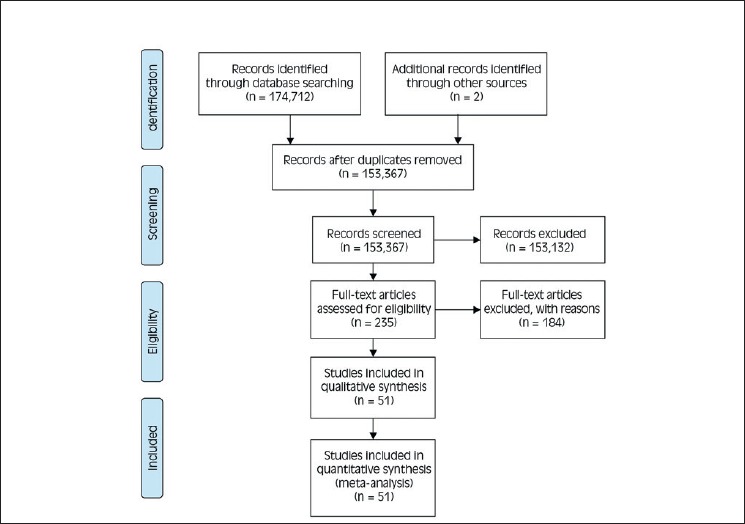
PRISMA 2009, flow diagram. The process of retrieving and selecting articles adopted in the present systematic review and meta-analysis.
Investigations were carried out between 1983 and 2018. Sample sizes ranged from 30 to 11,242 subjects, with a total of 43,673 participants. 31 studies investigated drug consumption among truck-drivers utilizing questionnaires, whilst 14 and 6 studies utilized urine and saliva samples, respectively. 35 studies were performed in the Americas (1 in Canada, 6 in the USA, and 28 in Brazil), 5 in Asia (3 in Thailand, 1 in Pakistan, and 1 in Iran), 5 in Europe (3 in Italy, 1 in France and 1 in Norway), 4 in Australia and 2 in Africa (1 in Morocco and 1 in Nigeria).
Age went from 33.5 to 43.85 years, with male percentage varying in the range 90.6-100.0%. Concerning the marital status, percentage of married subjects ranged from 62.0% to 94.9%. Percentage of truck-drivers with at least primary education varied between 35.2% and 100.0%, with schooling years going from 4.6 to 8.7 years. Work-load ranged from 7.8 to 14.8 hours, with mean distance travelled varying between 270 km and 1,159.7 km. Percentage of truck-drivers working for companies was highly variable, in the range 0-76%. Experience years went from 10 to 18.5 hours. Finally, percentage of truck-drivers doing night-shifts ranged from 10.7% to 33.0%.
Concerning the outcomes, amphetamine consumption ranged from 0.0% to 82.5%, whereas cannabis and cocaine use went from 0.0% to 29.9%, and from 0.1% to 8.9%, respectively. Heroin consumption varied between 0.1% and 0.9%. Opioid use ranged from 0.2% to 33.0%, while benzodiazepines consumption went from 0.0% to 2.1%. OTC stimulant use ranged from 4% to 13%, while poliabuse prevalence was more variable (0.0-8.9%). Finally, overall drug use was in the range 1.3-80.4%.
AMPHETAMINE CONSUMPTION
Based on questionnaires, the overall amphetamine consumption rate was 21.3% ([95%CI 15.7-28.1], z = – 6.94, p < 0.0001, k = 22) (Supplementary Fig. 1A). Due to the high statistically significant heterogeneity (I2 = 97.15%), a random-effect model was applied (I2 = 64.91%). No evidence of publication bias could be found. At the meta-regression analyses, significant moderators were found to be country (Q = 39.20, p < 0.0001, with the highest ES in Brazil, and the lowest ES in Nigeria) (Supplementary Fig. 2), age (coefficient = – 0.24, SE = 0.06 [95%CI – 0.36 to – 0.12], z = – 3.82, p = 0.0001) (Supplementary Fig. 3), marriage (coefficient = – 0.02, SE = 0.01 [95%CI – 0.04 to 0.00], z = – 1.99, p = 0.0470), experience years (coefficient = – 0.34, SE = 0.10 [95%CI – 0.54 to – 0.14], z = – 3.37, p = 0.0008) (Supplementary Fig. 4), working for companies (coefficient = – 0.04, SE = 0.01 [95%CI – 0.06 to – 0.01], z = – 2.72, p = 0.0065) and primary schooling level (coefficient = – 0.02, SE = 0.01 [95%CI – 0.03 to – 0.01], z = – 2.69, p = 0.0071). Male (p = 0.1040), mean distance (p = 0.7928) and work-load (p = 0.3804) were not statistically significant. For the other moderators, meta-regression analyses could not be run due to insufficient number of studies.
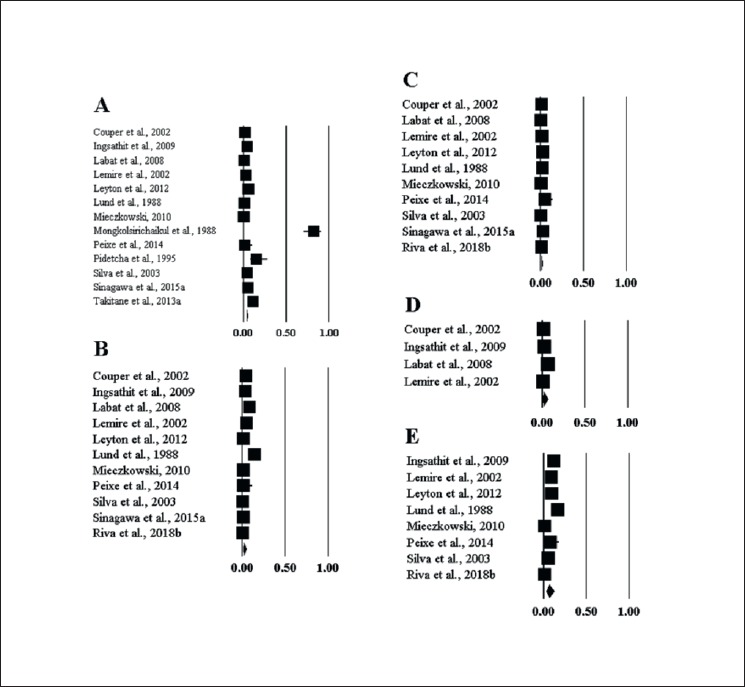
Supplementary Fig. 1.
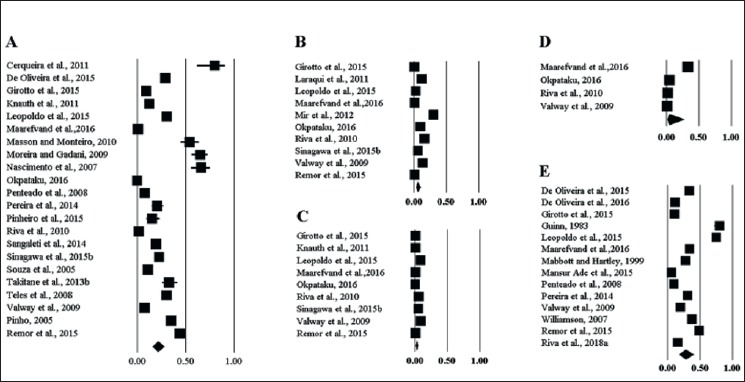
Forest plots of amphetamine (A), cannabis (B), cocaine (C), opioids (D) and overall drug (E) use prevalence based on questionnaires.
Supplementary Fig. 2.
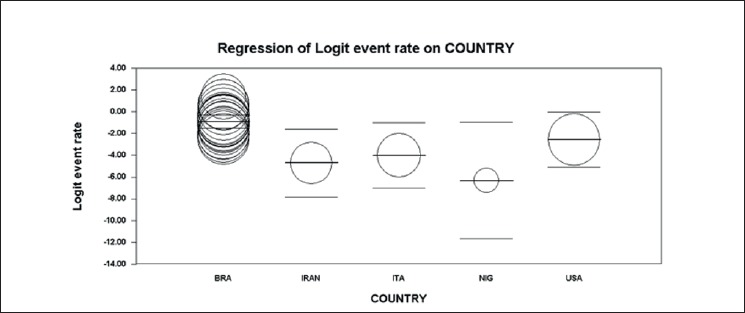
Meta-regression analysis of amphetamine use prevalence based on questionnaire, conducted for country as parameter.
Supplementary Fig. 3.
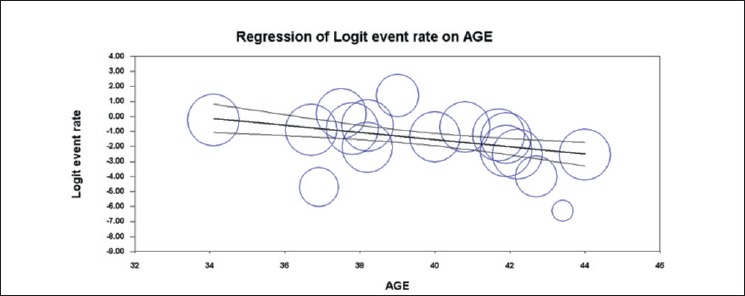
Meta-regression analysis of amphetamine use prevalence based on questionnaire, conducted for age as parameter.
Supplementary Fig. 4.
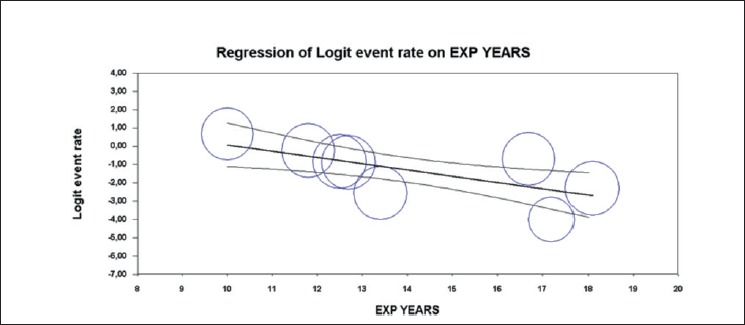
Meta-regression analysis of amphetamine use prevalence based on questionnaire, conducted for experience (in years) as parameter.
Based on studies utilizing urine samples, the overall amphetamine consumption rate was 3.8% ([95%CI 1.7-8.2], z = – 7.70, p < 0.0001, k = 13) (Supplementary Fig. 5A). Due to the high statistically significant heterogeneity (I2 = 97.36%), a random-effect model was carried out (I2 = 42.38%). No evidence of publication bias could be detected. At the meta-regression analyses, only country (Q = 23.64, p < 0.0001, with the highest ES in Thailand and the lowest ES in France) resulted a statistically significant moderator. Age (p = 0.1673), male (p = 0.0511) were not statistically significant moderators. For the other moderators, meta-regression analyses could not be run due to insufficient number of studies.
Supplementary Fig. 5.
Forest plots of amphetamine (A), cannabis (B), cocaine (C), opioids (D) and overall drug (E) use prevalence based on urine samples.
Based on studies utilizing saliva samples, the overall amphetamine consumption rate was 1.3% ([95%CI 0.7-2.4], z = – 13.63, p < 0.0001, k = 5) (Supplementary Fig. 6A). Due to the high statistically significant heterogeneity (I2 = 83.68%) a random-effect model was applied (I2 = 47.67%). No evidence of publication bias could be found. For all the moderators, meta-regression analyses could not be run due to insufficient number of studies.
Supplementary Fig. 6.
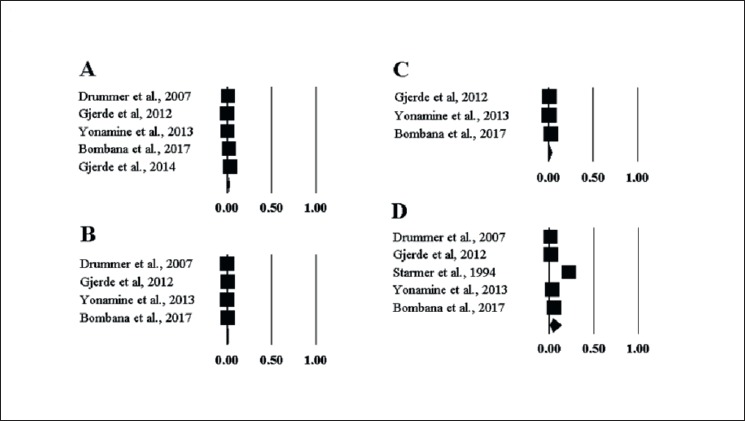
Forest plots of amphetamine (A), cannabis (B), cocaine (C) and overall drug (D) use prevalence based on saliva samples.
CANNABIS CONSUMPTION
Based on questionnaires, the overall cannabis consumption rate was 5.9% ([95%CI 3.5-9.8], z = – 9.88, p < 0.0001, k = 10) (Supplementary Fig. 1B). Due to the high statistically significant heterogeneity, (I2 = 96.81%), a random-effect model was carried out (I2 = 62.28%). No evidence of publication bias could be found. At the meta-regression analyses, a significant moderator was found to be only country (Q = 15.85, p = 0.0146, with the highest ES in Pakistan, and the lowest ES in Iran). Age (p = 0.1044), male (p = 0.5799), marriage (p = 0.5939), mean distance (p = 0.4235), experience years (p = 0.7688), working for companies (p = 0.2192), and primary schooling level (p = 0.3200) were not statistically significant. For the other moderators, meta-regression analyses could not be run due to insufficient number of studies.
Based on studies utilizing urine samples, the overall cannabis consumption rate was 2.1% ([95%CI 1.0-4.3], z = – 9.97, p < 0.0001, k = 11) (Supplementary Fig. 5B). Due to the high statistically significant heterogeneity (I2 = 97.62%), a random-effect model was chosen (I2 = 4.52). At the meta-regression analyses, only age (coefficient = – 0.50, SE = 0.09 [95%CI – 0.68 to – 0.33], z = – 5.56, p < 0.0001) resulted a statistically significant moderator. Country (Q = 3.97, p = 0.5537), male (p = 0.2427) were not statistically significant moderators. For the other moderators, meta-regression analyses could not be run due to insufficient number of studies.
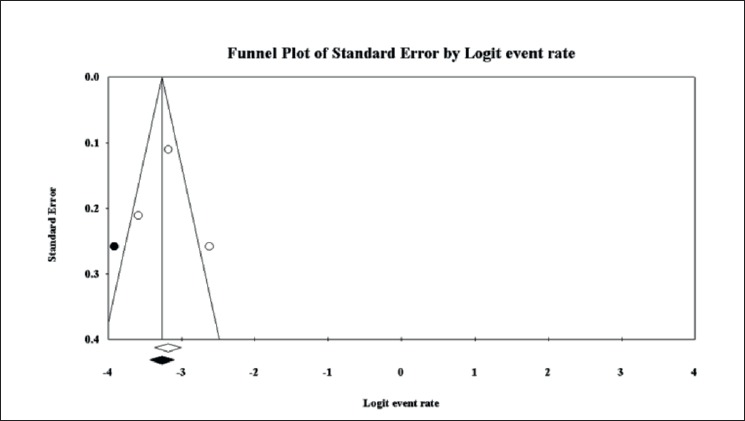
Based on studies utilizing saliva samples, the overall cannabis consumption rate resulted 0.5% ([95% 0.3-1.0%], z = – 15.69, p < 0.0001, k = 4) (Supplementary Fig. 6B). Due to the high statistically significant heterogeneity (I2 = 68.12%), a random-effect model was applied (I2 = 0.00%). The visual inspection of the funnel plot showed evidence of publication bias. At the Duval and Tweedie’s trim-and-fill analysis, 2 studies were censored, resulting in a “real” ES of 0.3% ([95%CI 0.1-0.7], Q = 33.21) (Supplementary Fig. 7). For all the moderators, meta-regression analyses could not be run due to insufficient number of studies.
Supplementary Fig. 7.
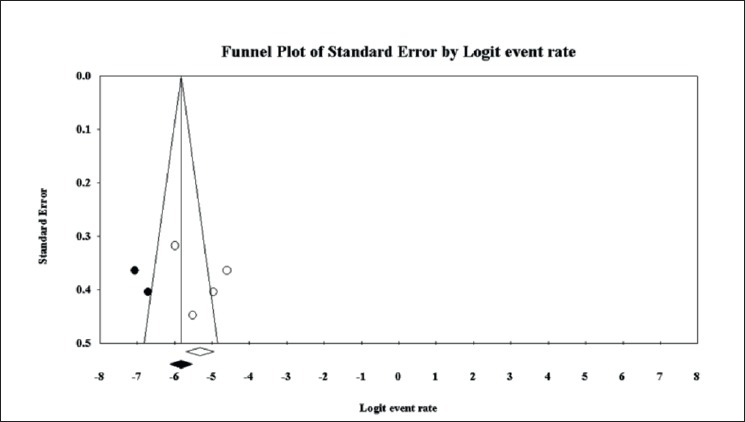
Funnel plot of cannabis use prevalence based on saliva samples. showing evidence of publication bias. In white observed effect sizes, in black imputed effect sizes.
COCAINE CONSUMPTION
Based on questionnaires, the overall cocaine consumption rate was 2.2% ([95%CI 1.2-4.1], z = – 11.75, p < 0.0001, k = 9) (Supplementary Fig. 1C). Due to the high statistically significant heterogeneity (I2 = 91.66%), a random-effect model was applied (I2 = 50.78%). No evidence of publication bias could be found. Country (Q = 6.06, p = 0.1951), age (p = 0.2460), male (p = 0.2433), marriage (p = 0.0541), mean distance (p = 0.8952), experience years (p = 0.2604), working for companies (p = 0.3851), primary schooling level (p = 0.5713) were not statistically significant moderators. For the other moderators, meta-regression analyses could not be run due to insufficient number of studies.
Based on studies utilizing urine samples, the overall cocaine consumption rate was 1.1% ([95%CI 0.7-2.0], z = – 15.59, p < 0.0001, k = 10) (Supplementary Fig. 5C). Due to the high statistically significant heterogeneity (I2 = 88.74%), a random-effect model was carried out (I2 = 19.33%). No evidence of bias was found. At the meta-regression analyses, no statistically significant moderators could be found. Country (Q = 6.47, p = 0.1668), age (p = 0.5273), male (p = 0.3568) were not statistically significant moderators. For the other moderators, meta-regression analyses could not be run due to insufficient number of studies.
Based on studies utilizing saliva samples, the overall cocaine consumption rate resulted 1.1% ([95%CI 0.4-3.1], z = – 8.29, p < 0.0001, k = 3) (Supplementary Fig. 6C). Due to the high statistically significant heterogeneity (I2 = 88.18%), a random-effect model was chosen (I2 = 0.00%). No evidence of bias publication could be found.
OPIOID CONSUMPTION
Based on questionnaires, the overall opioid consumption rate was 4.3% ([95%CI 0.6-26.4], z = – 2.92, p = 0.003, k = 4) (Supplementary Fig. 1D). Due to the high statistically significant heterogeneity (I2 = 98.12%), a random-effect model was performed (I2 = 0.00%). No evidence of publication bias could be found. At the meta-regression analyses, only age (coefficient = – 0.49, SE = 0.13 [95%CI – 0.75 to – 0.23], z = – 3.70, p = 0.0002) resulted a statistically significant moderator. For the other moderators, meta-regression analyses could not be run due to insufficient number of studies.
Based on studies utilizing urine samples, the overall opioid consumption rate was 2.0% ([95%CI 0.6-6.6], z = – 6.13, p < 0.0001, k = 4) (Supplementary Fig. 5D). Due to the high statistically significant heterogeneity (I2 = 95.97%), a random-effect model was chosen (I2 = 0.00%). No evidence of publication bias was found. It was not possible to compute meta-regressions due to insufficient number of studies/missing information.
BENZODIAZEPINES CONSUMPTION
Based on questionnaires, the overall benzodiazepines consumption rate was 1.0% ([95%CI 0.1-6.1], z = – 4.81, p < 0.0001, k = 2). Due to the high statistically significant heterogeneity (I2 = 70.57%), a random-effect model was carried out (I2 = 0.00%). Since there were only 2 studies, it was not possible to conduct a publication bias analysis and meta-regressions.
Based on studies utilizing urine samples, the overall benzodiazepines consumption rate was 0.4% [95%CI 0.2-0.6], z = – 21.71, p < 0.0001, k = 4). Due to the absence of heterogeneity (I2 = 0.00%), a fixed-effect model was applied. There was no evidence of publication bias. For all the moderators, meta-regression analyses could not be run due to insufficient number of studies.
OVER-THE-COUNTER STIMULANT CONSUMPTION
Based on questionnaires, the overall OTC stimulant consumption rate was 4.1% ([95%CI 2.7-6.2], z = – 14.09, p < 0.0001, k = 3). Due to the high statistically significant heterogeneity (I2 = 76.18%), a random-effect model was conducted (I2 = 28.35%). The visual inspection of the funnel plot gave evidence of publication bias. At the Duval and Tweedie’s trim-and-fill analysis, one study was censored, with a “real” ES of 3.5% ([95%CI 2.3-5.3], Q = 15.46) (Supplementary Fig. 8). For all moderators, meta-regression analyses could not be run due to insufficient number of studies.
Supplementary Fig. 8.
Funnel plot of over-the-counter stimulant use prevalence based on questionnaire, showing evidence of publication bias. In white observed effect sizes, in black imputed effect sizes.
Based on studies utilizing urine samples, the overall OTC stimulant consumption rate was 9.0% ([95%CI 4.3-18.0], k = 2). Due to the high statistically significant heterogeneity (I2 = 92.41%), a random-effect model was chosen (I2 = 0.00%). Since there were only 2 studies, it was not possible to conduct a publication bias analysis and meta-regressions.
POLIABUSE RATE
Based on questionnaires, the overall poliabuse rate was 2.7% ([95%CI 0.2-25.6], z = – 2.80, p = 0.005, k = 2). Due to the high statistically significant heterogeneity (I2 = 96.14%), a random-effect model was applied (I2 = 0.00%). Since there were only 2 studies, it was not possible to conduct a publication bias analysis and meta-regressions.
Based on studies utilizing urine samples, the overall poliabuse rate was 0.6% ([95%CI 0.1-4.8], z = – 4.77, k = 5). Due to the high statistically significant heterogeneity (I2 = 90.76%), a random-effect model was carried out (I2 = 0.00%). No evidence of publication bias could be found. At the meta-regression analyses, only country (Q = 17.45, p = 0.0002, with the highest ES in the USA and the lowest ES in Italy) resulted a statistically significant moderator. For the other moderators, meta-regression analyses could not be run due to insufficient number of studies.
Based on studies utilizing saliva samples, the overall poliabuse rate was 0.3% ([95%CI 0.1-0.7], z = – 12.98, p < 0.0001, k = 3). Due to the statistically significant heterogeneity (I2 = 61.68%), a random-effect model was performed (I2 = 0.00%). No evidence of publication bias could be found. For all moderators, meta-regression analyses could not be conducted due to insufficient number of studies.
OVERALL DRUG CONSUMPTION
Based on questionnaires, the pooled overall drug consumption rate was 27.6% ([95%CI 17.8-40.1], z = – 3.36, p = 0.001, k = 14) (Supplementary Fig. 1E). Due to the high statistically significant heterogeneity (I2 = 99.04%), a random-effect model was applied (I2 = 21.28%). There was no evidence of publication bias. At the meta-regression analyses, only age (coefficient = – 0.22, SE = 0.07 [95%CI – 0.36 to – 0.08], z = – 3.13, p = 0.0018) resulted a statistically significant moderator. On the contrary, country (Q = 1.47, p = 0.8326), male (p = 0.9460), marriage (p = 0.3583), mean distance (p = 0.9759), experience years (p = 0.1128), work-load (p = 0.9902), working for companies (p = 0.8486), and primary schooling level (p = 0.3112) were not statistically significant moderators. For the other moderators, meta-regression analyses could not be run due to insufficient number of studies.
Based on studies utilizing urine samples, the pooled overall drug consumption rate was 6.1% ([95%CI 2.9-12.4], p < 0.0001, k = 8) (Supplementary Fig. 5E). Due to the high statistically significant heterogeneity (I2 = 98.44%), a random-effect model was conducted (I2 = 0.00%). The visual inspection of the funnel plot showed evidence of publication bias. At the Duval and Tweedie’s trim-and-fill analysis, 1 study was censored, resulting in a “real” ES of 5.1% ([95% 2.4-10.1], Q = 543.42) (Supplementary Fig. 9). At the meta-regression analyses, only age (coefficient = – 0.36, SE = 0.09 [95%CI – 0.53 to – 0.19], z = – 4.13, p < 0.0001) resulted a statistically significant moderator. Country (Q = 1.65, p = 8003), and male (p = 0.8430) were not statistically significant moderators. For the other moderators, meta-regression analyses could not be run due to insufficient number of studies.
Supplementary Fig. 9.
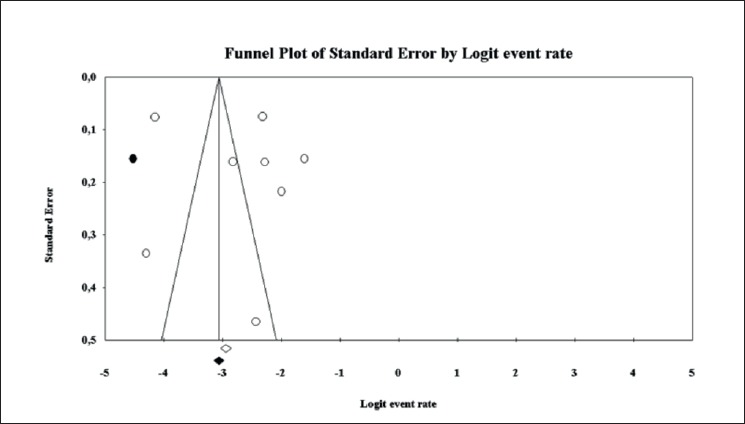
Funnel plot of overall drug use prevalence based on urine samples, showing evidence of publication bias. In white observed effect sizes, in black imputed effect sizes.
Based on studies utilizing saliva samples, the pooled overall drug consumption rate was 4.1% ([95%CI 1.2-13.1], z = – 4.90, p < 0.0001, k = 5) (Supplementary Fig. 6D). Due to the high statistically significant heterogeneity (I2 = 98.89%), a random-effect model was conducted (I2 = 0.00%). For all the moderators, meta-regression analyses could not be run due to insufficient number of studies.
Pooled drug consumption rates stratified according to the type of study are summarized in Table I.
STUDY QUALITY
Findings of the critical appraisal of included studies are shown in Table II.
Tab. II.
Critical appraisal of studies included in the present systematic review and meta-analysis.
| Study | Domain I | Domain II | Domain III | Domain IV | Domain V | Domain VI | Domain VII | Domain VIII | Domain IX |
|---|---|---|---|---|---|---|---|---|---|
| Bombana et al.
2017 [29] |
Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Cerqueira et al.
2011 [30] |
Yes | No | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Couper et al.
2002 [31] |
No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| De Oliveira et al.
2015 [32] |
Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| De Oliveira et al.
2016 [33] |
Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Drummer et al.
2007 [34] |
No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Girotto et al.
2015 [17] |
Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Gjerde et al.
2012 [35] |
No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Gjerde et al.
2014 [36] |
No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Guinn et al.
1983 [37] |
No | No | No | No | Yes | No | No | Yes | Yes |
| Ingsathit et al.
2009 [38] |
No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Knauth et al.
2011 [39] |
Yes | No | Yes | No | Yes | No | No | Yes | Yes |
| Korelitz et al.
1993 [16] |
Yes | No | Yes | No | Yes | Yes | Yes | Yes | Yes |
| Labat et al.
2008 [40] |
Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Laraqui et al.
2011 [41] |
Yes | No | Yes | Yes | Yes | No | No | Yes | Yes |
| Lemire et al.
2002 [42] |
No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes |
| Leopoldo et al.
2015 [43] |
Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Leyton et al.
2012 [44] |
Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Lund et al.
1988 [45] |
Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Maarefvand et al.
2016 [46] |
Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Mabbott and Hartley
1999 [47] |
Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | No |
| Mansur Ade et al.
2015 [48] |
No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes |
| Masson, Monteiro
2010 [49] |
Yes | No | No | Yes | Yes | No | No | Yes | Yes |
| Mieczkowski
2010 [50] |
No | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Mir et al.
2012 [51] |
Yes | Yes | Yes | No | Yes | No | No | Yes | Yes |
| Mongkolsirichaikul et al.
1988 [52] |
Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Moreira, Gadani
2009 [53] |
No | No | No | No | Yes | No | No | Yes | Yes |
| Nascimento et al.
2007 [54] |
Yes | No | No | No | Yes | No | No | Yes | Yes |
| Okpataku
2016 [55] |
Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Peixe et al.
2014 [56] |
Yes | No | No | Yes | Yes | Yes | Yes | Yes | No |
| Penteado et al.
2008 [57] |
Yes | No | Yes | Yes | Yes | No | No | Yes | Yes |
| Pereira et al.
2014 [58] |
Yes | No | No | Yes | Yes | No | No | Yes | Yes |
| Pidetcha et al.
1995 [59] |
No | No | No | No | Yes | Yes | Yes | Yes | Yes |
| Pinheiro et al.
2015 [60] |
Yes | No | No | Yes | Yes | No | No | Yes | Yes |
| Pinho
2005 [61] |
Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Remor et al.
2015 [62] |
Yes | No | Yes | Yes | Yes | No | No | Yes | Yes |
| Riva et al.
2010 [63] |
Yes | No | Yes | Yes | Yes | No | No | Yes | Yes |
| Riva et al.
2018 [64] |
Yes | No | Yes | Yes | Yes | No | No | Yes | Yes |
| Sangaleti et al.
2014 [65] |
Yes | No | Yes | Yes | Yes | No | No | Yes | Yes |
| Silva et al.
2003 [66] |
No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes |
| Sinagawa et al.
2014 [67] |
Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Souza et al.
2005 [68] |
Yes | No | Yes | Yes | Yes | No | No | Yes | Yes |
| Starmer et al.
1997 [69] |
No | No | Yes | No | Yes | Yes | Yes | Yes | Yes |
| Takitane et al.
2012 [70] |
Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Teles et al.
2008 [71] |
Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Valway et al.
2009 [72] |
Yes | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Williamson
2007 [73] |
Yes | No | Yes | Yes | Yes | No | No | Yes | Yes |
| Yonamine et al.
2012 [74] |
Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
Discussion
To the best of our knowledge, this is the first systematic review with meta-analysis and meta-regressions on drug consumption rate among truck-drivers. Considering the meta-analysis performed on data extracted from questionnaires, the findings show an increased prevalence of drug use among truck-drivers, especially central nervous system (CNS) stimulants, compared to the general population. In particular, the overall annual prevalence of amphetamine use among truck-drivers of 21.3%, compared to the estimated global prevalence of consumption in the general population of 0.7% [1], shows an almost 30-fold higher rate.
Similarly, but to a lesser degree, the results regarding cocaine use showed a higher prevalence (2.2%) compared to the general population (0.37%) [1]. In previous studies, stimulant consumption among truck-drivers has been associated with night shifts, length of travel and younger age [17, 75, 76]. Other authors have suggested that also external factors play a role, such as productivity-based payments [73]. In the present analysis, being younger and having less professional experience showed the most significant correlations with stimulant use.
Drivers often take stimulants as a form of Performance Enhancing Drugs (PEDs), in order to sustain ever increasing work-loads and busy work schedules. Several studies performed in controlled clinical settings have suggested that low dose amphetamines could improve psychomotor skills, such as driving ability, even in fatigued subjects [77]. However, chronic and high dose users, taken in real life settings, showed poorer compliance with traffic rules and working hours regulations [78], with an increased risk of traffic accidents [79], mainly as a consequence of after effects such as hypersomnolence and fatigue [80, 81]. Some authors have suggested that blood concentration above 0.27-0.53 mg/l is associated with psychomotor impairment [79]. Similar considerations have been made regarding cocaine use and its effects on psychomotor skills [82-85]. Amphetamine use has been estimated to increase the risk of fatal accidents by 5-times, causing in 2013 around half of all road traffic deaths caused by illicit drug consumption worldwide, resulting in around 20 thousand deaths [15].
The European Agency for Safety and Health at Work (EU-OSHA) has acknowledged the spread and normalization of stimulant use among certain groups of workers, particularly transportation workers, shift workers, and workers in high pressure, competitive or bullying work cultures [86]. It highlighted the need to evaluate the potential effect of non-medical drug used as cognitive enhancers in the workplace, and to consider the work environment and the interaction between workers and their working conditions as important factors in the use of PEDs.
Opiates, opioids, and CNS depressants, such as cannabinoids and benzodiazepines, showed a lower prevalence in the study population, and a smaller difference compared to the prevalence in the general population. In particular regarding cannabinoid use, the relatively high prevalence shown (5.9%), with the highest rates extracted from North American and European studies, follows the overall increasing rate of recreational and medical use of this type of drug in the general population: while an estimated 3.9% of the global population has used cannabinoids in the previous year, in North America the prevalence was higher at 13% [1], reaching over 14% in the European Union with an increasing trend of high-risk use, meaning consuming cannabinoids 20 or more days in the past month [2]. Many CNS depressant have been found to reduce lane control by increasing the standard deviation of lateral position (SDLP) [87-93]. Cannabis has been shown to impair cognitive, particularly affecting working memory and divided attention, and psychomotor performances, increasing the chance of road accidents [94]: according to systematic review and meta-analysis performed by Asbridge and collaborators, acute cannabis consumption among drivers doubles the risk of crashes compared to non-user [95].
Authors have suggested that tetrahydrocannabinol (THC) impairs mainly lateral control of the vehicle, while not affecting longitudinal control [96, 97]. Moreover, interaction between cannabis and alcohol has been shown to have an additive effect on driving performance [91, 94, 98, 99] causing an increased risk of road accidents [100]. Indeed, cannabinoids are estimated to cause one fifth of all road traffic deaths caused by illicit drug consumption [15]. The importance of cannabis use in the workplace may grow further as countries reform medicinal and recreational cannabinoid laws enabling an increase in the rate of consumption [101]. Concerning the results of opiate/opioid use among truck-drivers, the present analysis shows a prevalence of 4.3%, significantly higher compared to the rate of persons who use opiates and persons who use prescription opioids for non-medical purposes among the general population equal to 0.7% worldwide [1], and 0.4% in Europe [2].
However, similarly to cannabis, data show that there is a growing trend in the use of prescription drugs such as opioids and sedatives, for medical and non-medical reasons, reaching epidemic proportions in some Western countries. In particular, past-year users of opioids in North America have reached a prevalence of 4.2% [1], similar to the results found in the present study. Moreover, opioids cause most of the negative health impact of drug use, accounting for three quarters of deaths from drug use disorders in 2015 [1]. Although the role of opiates and opioid use in impairing driving ability is still unclear [102-106], there is suggestive evidence that opioids can cause an increased risk of vehicle collisions [1, 107].
Although the consumption of benzodiazepine was not found to be as common among truck-drivers, it must not be underestimated, as there is ample evidence of their impairing effect on driving skills, particularly regarding long-term benzodiazepines [108-110]. Moreover, non-medical use of benzodiazepines is the most common type of misuse of prescription drugs in the world [1].
Concerning drug testing for recent use, the results obtained through saliva sampling showed generally lower rates than those found on urine. This might be explained by the fact that urine drug testing can detect consumption occurred days or weeks before the sampling, resulting in low specificity for recent substance use. Research has suggested that saliva sampling has a stronger correlation with blood concentrations compared to urine, being also easier and faster to analyze and less intrusive to drivers [111-113]. However, there is a lack of conclusive evidence, with other authors considering urine testing as a more accurate method for identification of substance use and disorders in the workplace [114]. Based on the prevalence of overall drug use obtained through biological sampling, around 1 every 20 workers was driving under the influence of drugs. It is worth noting that the country of origin of the driver was an often found association with drug use. Indeed, considering the data obtained from the included studies, there appears to be a pattern of consumption of specific substances in different areas, such as prevalent stimulant use in South America, cannabis use in North America and Europe, and opioid use in parts of Asia, likely because of availability, as well as historic and cultural reasons.
Overall, the findings of the present study, adding to the results of the previously published systematic review and meta-analysis concerning at-risk drinking, show that substance use is widespread among truck-drivers globally, putting workers and the general public at an increased risk of harm.
The EU Action Plan on Drugs 2017-2020 states that, in order to reduce and prevent drug use, effective evidence-based prevention measures must take into consideration situational factors, including workplace conditions [115]. There is indeed an urgent necessity for updated epidemiological data and research studying effective Occupational Health Promotion programs, particularly in Europe, required in order to make and enforce effective policies, putting in place countermeasures such as regular worksite drug testing, which has been shown to deter drug use among workers [116], as well as assessing working conditions that facilitate drug consumption, such as excessive workloads demanded by companies.
STRENGTHS AND LIMITATIONS
The strengths of our study consist in its methodological rigor, reproducibility and transparency. We deposited a priori study protocol, which further corroborates our meta-analysis. However, despite its novelty and its methodological robustness, our study is not without limitations, which should be properly acknowledged.
The high statistically significant heterogeneity may affect the generalization of the findings and calls up for caution in their interpretation. For some outcomes, few studies were available. In some cases, such paucity limited the possibility of conducting a full extensive e series of analyses, including publication bias analysis and meta-regressions.
Conclusions
The present systematic review of the literature with meta-analysis and meta-regressions showed a relevant drug consumption rate among truck-drivers. As such, this study has practical implications for Occupational Physicians dealing with the health and wellbeing of truck-drivers. In particular, it appears that truck-drivers choose mainly stimulant substances as a form of performance enhancing drug, in order to increase productivity. However, chronic and high dose consumption has been shown to decrease driving skills, placing these professional drivers, as well as the general public, at risk.
Current literature is lacking in updated and reliable epidemiological data, especially in Europe. Therefore, further research in the field is urgently needed in order to provide Occupational Health Professionals with up-to-date data, necessary for the implementation of preventive programs and effective workplace measures. Moreover, this can be useful for decision and policy-makers in order to fill the gaps and shortcomings in the regulations.
Figures and tables
Acknowledgements
Funding sources: this research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Footnotes
Conflict of interest statement
None declared.
Authors’ contributions
GD, NLB and PD conceived the study, AM and AR performed a search of the literature, extracted and collected data, AM and AR critically appraised the literature, GD and NLB analyzed data, GD, NLB, AM, AR and PD drafted and revised the manuscript. All authors have read and approved the latest version of the manuscript.
References
- [1].The United Nations Office on Drugs and Crime (UNODC). World Drug Report 2018. Available online: www.unodc.org/wdr2018/prelaunch/WDR18_Booklet_2_GLOBAL.pdf.
- [2].European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). European Drug Report 2018: trends and developments. Available online: www.emcdda.europa.eu/system/files/publications/8585/20181816_TDAT18001ENN_PDF.pdf.
- [3].Substance Abuse and Mental Health Services Administration (SAMHSA); Center for Behavioral Health Statistics and Quality (CBHSQ). The CBHSQ report: substance use and substance use disorder, by industry. Available online: www.samhsa.gov/data/sites/default/files/report_1959/ShortReport-1959.pdf.
- [4].Girotto E, Mesas AE, de Andrade SM, Birolim MM. Psychoactive substance use by truck drivers: a systematic review. Occup Environ Med 2014;71:71-6. doi: 10.1136/oemed-2013-101452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Criezzle AM, Bigelow P, Adams D, Gooderham S, Myers AM, Thiffault P. Health and wellness of long-haul truck drivers and bus drivers: a systematic review and directions for future researches. J Transp Health 2017;7:90-109. doi: 10.1016/j.jth.2017.05.359. [Google Scholar]
- [6].Apostolopoulos Y, Sönmez S, Shattell MM, Belzer M. Worksite-induced morbidities among truck drivers in the United States. AAOHN J 2010;58(7):285-96. doi: 10.3928/08910162-20100625-01. [DOI] [PubMed] [Google Scholar]
- [7].van der Beek AJ. World at work: truck drivers. Occup Environ Med 2012;69:291-5. doi: 10.1136/oemed-2011-100342. [DOI] [PubMed] [Google Scholar]
- [8].Sieber WK, Robinson CF, Birdsey J, Chen GX, Hitchcock EM, Lincoln JE, Nakata A, Sweeney MH. Obesity and other risk factors: the national survey of U.S. long-haul truck driver health and injury. Am J Ind Med 2014;57:615-26. doi: 10.1002/ajim.22293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Guglielmi O, Magnavita N, Garbarino S. Sleep quality, obstructive sleep apnea, and psychological distress in truck drivers: a cross-sectional study. Soc Psychiatry Psychiatr Epidemiol 2018;53(5):531-6. doi: 10.1007/s00127-017-1474-x. [DOI] [PubMed] [Google Scholar]
- [10].Burns N. An integrative review of screening for obstructive sleep apnea in commercial vehicle drivers. Workplace Health Saf 2014;62:114-20. doi: 10.3928/21650799-20140219-05. [DOI] [PubMed] [Google Scholar]
- [11].Gamble JF, Nicolich MJ, Boffetta P. Lung cancer and diesel exhaust: an updated critical review of the occupational epidemiology literature. Crit Rev Toxicol 2012;42(7):549-98. doi: 10.3109/10408444.2012.690725. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Gay Anderson D, Riley P. Determining standards of care for substance abuse and alcohol use in long-haul truck drivers. Nurs Clin North Am 2008;43:357-65. doi: 10.1016/j.cnur.2008.04.003. [DOI] [PubMed] [Google Scholar]
- [13].Wagstaff AS, Sigstad Lie JA. Shift and night work and long working hours - a systematic review of safety implications. Scand J Work Environ Health 2011;37:173-85. doi: 10.5271/sjweh.3146. [DOI] [PubMed] [Google Scholar]
- [14].Zhang X, Chow EP, Wilson DP, Sun X, Zhao R, Zhang J, Jing J, Zhang L. Prevalence of HIV and syphilis infections among long-distance truck drivers in China: a data synthesis and meta-analysis. Int J Infect Dis. 2013,17:e2-e7. doi: 10.1016/j.ijid.2012.07.018. [DOI] [PubMed] [Google Scholar]
- [15].World Health Organization (WHO). Drug use and road safety: a policy brief. 2016. Available online: www.who.int/violence_injury_prevention/publications/road_traffic/Drug_use_and_road_safety.pdf.
- [16].Korelitz JJ, Fernandez AA, Uyeda VJ, Spivey GH, Browdy BL, Schmidt RT. Health habits and risk factors among truck drivers visiting a health booth during a trucker trade show. Am J Health Promot 1993;8:117-23. doi: 10.4278/0890-1171-8.2.117. [DOI] [PubMed] [Google Scholar]
- [17].Girotto E, de Andrade SM, Mesas AE, González AD, Guidoni CM. Working conditions and illicit psychoactive substance use among truck drivers in Brazil. Occup Environ Med 2015;72:764-9. doi: 10.1136/oemed-2015-102868. [DOI] [PubMed] [Google Scholar]
- [18].Ramirez M, Bedford R, Sullivan R, Anthony TR, Kraemer J, Faine B, Peek-Asa C. Toxicology testing in fatally injured workers: a review of five years of Iowa FACE cases. Int J Environ Res Public Health 2013;10:6154-68. doi: 10.3390/ijerph10116154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Bragazzi NL, Dini G, Toletone A, Rahmani A, Montecucco A, Massa E, Manca A, Guglielmi O, Garbarino S, Debarbieri N, Durando P. Patterns of harmful alcohol consumption among truck drivers: implications for occupational health and work safety from a systematic review and meta-analysis. Int J Environ Res Public Health 2018;15:1121 doi: 10.3390/ijerph15061121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Conferenza Unificata. Provvedimento 30 ottobre 2007, Intesa, ai sensi dell’articolo 8, comma 6, della legge 5 giugno 2003, n. 131, in materia di accertamento di assenza di tossicodipendenza. Available online: www.gazzettaufficiale.it/eli/id/2007/11/15/07A09622/sg.
- [21].Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ 2015;350:g7647 doi: 10.1136/bmj.g7647. [DOI] [PubMed] [Google Scholar]
- [22].Chien PF, Khan KS, Siassakos D. Registration of systematic reviews: PROSPERO. BJOG 2012;119:903-5. doi: 10.1111/j.1471-0528.2011.03242.x. [DOI] [PubMed] [Google Scholar]
- [23].Bragazzi NL, Dini G, Toletone A, Durando P. An Updated systematic review with meta-analysis examining prevalence of drugs and alcohol use among truck-drivers. PROSPERO 2016:CRD42016037077. Available online: www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42016037077.
- [24].Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009;6:e1000097 doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002;21:1539-58. doi: 10.1002/sim.1186. [DOI] [PubMed] [Google Scholar]
- [26].Huedo-Medina TB, Sánchez-Meca J, Marín-Martínez F, Botella J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol Methods 2006;11:193-206. doi: 10.1037/1082-989X.11.2.193. [DOI] [PubMed] [Google Scholar]
- [27].Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315(7109):629-34. doi: https://doi.org/10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Duval S, Tweedie R. Trim and fill: a simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000;56:455-63. doi: 10.1111/j.0006-341X.2000.00455.x. [DOI] [PubMed] [Google Scholar]
- [29].Bombana HS, Gjerde H, Dos Santos MF, Jamt REG, Yonamine M, Rohlfs WJC, Muñoz DR, Leyton V. Prevalence of drugs in oral fluid from truck drivers in Brazilian highways. Forensic Sci Int 2017;273:140-3. doi: 10.1016/j.forsciint.2017.02.023. [DOI] [PubMed] [Google Scholar]
- [30].Cerqueira GS, Siqueira RMP, Freitas APF, Leiros WSB, Freitas RM, Silva RC, Fragoso LM. Uso de anfetaminas entre caminhoneiros - um estudo transversal. Rev Inter 2011;4:76-86. [Google Scholar]
- [31].Couper FJ, Pemberton M, Jarvis A, Hughes M, Logan BK. Prevalence of drug use in commercial tractor-trailer drivers. J Forensic Sci 2002;47:562-7. [PubMed] [Google Scholar]
- [32].De Oliveira LG, de Souza LM, Barroso LP, Gouvêa MJ, de Almeida CV, Muñoz DR, Leyton V. Occupational conditions and the risk of the use of amphetamines by truck drivers. Rev Saude Publica 2015;49:61 doi: 10.1590/S0034-8910.2015049005944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].De Oliveira LG, Leopoldo K, Gouvea MJ, Barroso LP, Gouveia PA, Muñoz DR, Leyton V. Prevalence of at-risk drinking among Brazilian truck drivers and its interference on the performance of executive cognitive tasks. Drug Alcohol Depend 2016;166:218-25. doi: 10.1016/j.drugalcdep.2016.07.019. [DOI] [PubMed] [Google Scholar]
- [34].Drummer OH, Gerostamoulos D, Chu M, Swann P, Boorman M, Cairns I. Drugs in oral fluid in randomly selected drivers. Forensic Sci Int 2007;170:105-10. doi: 10.1016/j.forsciint.2007.03.028. [DOI] [PubMed] [Google Scholar]
- [35].Gjerde H, Christophersen AS, Normann PT, Pettersen BS, Sabaredzovic A, Samuelsen SO, Mørland J. Analysis of alcohol and drugs in oral fluid from truck drivers in Norway. Traffic Inj Prev 2012;13:43-8. doi:10.1080/15389588.2011.627957. [DOI] [PubMed] [Google Scholar]
- [36].Gjerde H, Sousa TR, De Boni R, Christophersen AS, Limberger RP, Zancanaro I, Oiestad EL, Normann PT, Mørland J, Pechansky F. A comparison of alcohol and drug use by random motor vehicle drivers in Brazil and Norway. Int J Drug Policy 2014;25:393-400. doi: 10.1016/j.drugpo.2014.01.019. [DOI] [PubMed] [Google Scholar]
- [37].Guinn B. Job satisfaction, counterproductive behavior and circumstantial drug use among long-distance truckers. J Psychoactive Drugs 1983;15:185-8. doi: 10.1080/02791072.1983.10471947. [DOI] [PubMed] [Google Scholar]
- [38].Ingsathit A, Woratanarat P, Anukarahanonta T, Rattanasiri S, Chatchaipun P, Wattayakorn K, Lim S, Suriyawongpaisal P. Prevalence of psychoactive drug use among drivers in Thailand: a roadside survey. Accid Anal Prev 2009;41:474-8. doi: 10.1016/j.aap.2009.01.010. [DOI] [PubMed] [Google Scholar]
- [39].Knauth DR, Pilecco FB, Leal AF, Seffner F, Teixeira AM. Staying awake: truck drivers’ vulnerability in Rio Grande do Sul, Southern Brazil. Rev Saude Publica 2012;46:886-93. doi: 0.1590/S0034-89102012000500016. [DOI] [PubMed] [Google Scholar]
- [40].Labat L, Fontaine B, Delzenne C, Doublet A, Marek MC, Tellier D, Tonneau M, Lhermitte M, Frimat P. Prevalence of psychoactive substances in truck drivers in the Nord-Pas-de-Calais region (France). Forensic Sci Int 2008;174:90-4. doi: 10.1016/j.forsciint.2007.03.004. [DOI] [PubMed] [Google Scholar]
- [41].Laraqui S, Laraqui O, Tripodi D, Manar N, Aoudi YE, Caubet A, Verger C, Ghailan T, Laraqui CH. Prevalence and risk factors of alertness disorders of professional drivers in Morocco. Sante Publique 2011;23:89-100. doi: 10.3917/spub.112.0089. [PubMed] [Google Scholar]
- [42].Lemire AM, Montégiani M, Dussault C. Alcohol and drug consumption by Québec truck drivers. In: Proceedings of the 16th International Conference on Alcohol, Drugs and Traffic Safety. Montreal, QC, Canada: 4-9 August 2002. [Google Scholar]
- [43].Leopoldo K, Leyton V, Oliveira LG. Alcohol use alone and in combination with other drugs among truck drivers on highways in São Paulo State, Brazil: a cross-sectional study. Cad Saude Publica 2015;31:1916-28. doi: 10.1590/0102-311X00047214. [DOI] [PubMed] [Google Scholar]
- [44].Leyton V, Sinagawa DM, Oliveira KC, Schmitz W, Andreuccetti G, De Martinis BS, Yonamine M, Munoz DR. Amphetamine, cocaine and cannabinoids use among truck drivers on the roads in the State of Sao Paulo, Brazil. Forensic Sci Int 2012;215:25-7. doi: 10.1016/j.forsciint.2011.03.032. [DOI] [PubMed] [Google Scholar]
- [45].Lund AK, Preusser DF, Blomberg RD, Williams AF. Drug use by tractor-trailer drivers. J Forensic Sci 1988;33(3):648-61.doi: 10.1520/JFS12474J. [PubMed] [Google Scholar]
- [46].Maarefvand M, Kassaie B, Ghiasvand H, Abolfathi Gharibdoosti R, Khubchandani J. Sexual and drug use risk behaviors of internal long distance truck drivers in Iran. Iran J Public Health 2016;45:606-13. [PMC free article] [PubMed] [Google Scholar]
- [47].Mabbott NA, Hartley LR. Patterns of stimulant drug use on Western Australian heavy transport routes. Transport Res Part F2 1999;115-30. doi: 10.1016/S1369-8478(99)00012-1. [Google Scholar]
- [48].Mansur Ade P, Rocha MA, Leyton V, Takada JY, Avakian SD, Santos AJ, Novo GC, Nascimento AL, Muñoz DR, Rohlfs WJ. Risk factors for cardiovascular disease, metabolic syndrome and sleepiness in truck drivers. Arq Bras Cardiol 2015;105:560-5. doi: 10.5935/abc.20150132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [49].Masson VA, Monteiro MI. Life style, health aspects and work among truck drivers. Rev Bras Enferm 2010;63:533-40. doi: 10.1590/S0034-71672010000400006. [DOI] [PubMed] [Google Scholar]
- [50].Mieczkowski T. Urinalysis and hair analysis for illicit drugs of driver applicants and drivers in the trucking industry. J Forensic Leg Med 2010;17:254-60. doi: 10.1016/j.jflm.2010.02.014. [DOI] [PubMed] [Google Scholar]
- [51].Mir MU, Khan I, Ahmed B, Abdul Razzak J. Alcohol and marijuana use while driving - an unexpected crash risk in Pakistani commercial drivers: a cross-sectional survey. BMC Public Health 2012;12:145 doi: 10.1186/1471-2458-12-145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [52].Mongkolsirichaikul D, Mokkhavesa C, Ratanabanangkoon K. The incidence of amphetamine use among truck drivers from various regions of Thailand. J Med Assoc Thai 1988;71:471-4. [PubMed] [Google Scholar]
- [53].Moreira RS, Gadani JAAB. A prevalência do uso de anfetaminas por caminhoneiros que passam pela cidade de Dourados-MS. Interbio 2009;3:27-34. [Google Scholar]
- [54].Nascimento EC, Nascimento E, Silva JP. Uso de álcool e anfetaminas entre caminhoneiros de estrada. Rev Saúde Pública 2007;41:290-3. [DOI] [PubMed] [Google Scholar]
- [55].Okpataku CI. Pattern and reasons for substance use among long-distance commercial drivers in a Nigerian city. Indian J Public Health 2015;59:259-63. doi: 10.4103/0019-557X.169649. [DOI] [PubMed] [Google Scholar]
- [56].Peixe TS, de Almeida RM, Girotto E, de Andrade SM, Mesas AE. Use of illicit drugs by truck drivers arriving at Paranaguá port terminal, Brazil. Traffic Inj Prev 2014;15:673-7. doi: 10.1080/15389588.2013.868893. [DOI] [PubMed] [Google Scholar]
- [57].Penteado RZ, Gonçalves CGO, Costa DD, Marques JM. Trabalho e saúde em motoristas de caminhãono interior de São Paulo. Saúde Soc 2008;17:35-45. [Google Scholar]
- [58].Pereira FGF, Aquino RA, Alencar VDM, Pordeus AMJ, Ataíde MBC. Relationship between work process and health of truckers. Rev Bras Promoç Saúde 2014;27:462-9. [Google Scholar]
- [59].Pidetcha P, Congpuong P, Putriprawan T, Rekakanakul R, Suwanton L, Tantrarongroj S. Screening for urinary amphetamine in truck drivers and drug addicts. J Med Assoc Thai 1995;78:554-8. [PubMed] [Google Scholar]
- [60].Pinheiro MP, Muniz LF, Da Silva MCV, Resill DP, Filho PCPT. Amphetamines consumption and alcohol for truck drivers. J Nurs UFPE On Line Recife 2015;9:8519-25. [Google Scholar]
- [61].Pinho RSN. Uso de estimulantes, queixa do sono e estado de humor em motoristas profissionais de caminhão. Dissertação (Mestrado em Ciências Farmacêuticas) - Universidade Federal do Ceará. Faculdade de Farmácia, Odontologia e Enfermagem, Fortaleza, 2005. [Google Scholar]
- [62].Remor KVT, Monteiro MTM, Rosa VD, Iacovski RB, Sakae TM, Galato D. Abusive Consumption of psychoactive substances by truck drivers. Med Clin Rev 2015;2:1. [Google Scholar]
- [63].Riva MM, Marchetti FA, Giupponi V, Mosconi G. Health surveillance of truck drivers: it is not just a question of drugs. Description of a one-year experience. Med Lav 2010;101:207-17. [PubMed] [Google Scholar]
- [64].Riva MM, Cantamessa F, Borleri D, Mosconi G. Occupational health and safety of road haulage company employees. Med Lav 2018;109:180-9. doi: 10.23749/mdl.v109i3.6827. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [65].Sangaleti CT, Trincaus MR, Baratieri T, Zarowy K, Ladika MB, Menon MU, Miyahara RY, Raimondo MI, Silveira JV, Bortolotto LA, Lopes HF, Consolim-Colombo FM. Prevalence of cardiovascular risk factors among truck drivers in the South of Brazil. BMC Public Health 2014;14:1063 doi: 10.1186/1471-2458-14-1063. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [66].Silva OA, Greve JMD, Yonamine M, Leyton V. Drug use by truck drivers in Brazil. Drug-Educ Prev Policy 2003;10:135-9. doi: org/10.1080/0968763021000057727. [Google Scholar]
- [67].Sinagawa DM, De Carvalho HB, Andreuccetti G, Do Prado NV, De Oliveira KC, Yonamine M, Muñoz DR, Gjerde H, Leyton V. Association between travel length and drug use among Brazilian truck drivers. Traffic Inj Prev 2015;16:5-9. doi: 10.1080/15389588.2014.906589. [DOI] [PubMed] [Google Scholar]
- [68].Souza JC, Paiva T, Reimão R. Sleep habits, sleepiness and accidents among truck drivers. Arquivos de Neuro-Psiquiatria 2005;63:925-30. doi: /S0004-282X2005000600004. [DOI] [PubMed] [Google Scholar]
- [69].Starmer GA, Mascord DJ, Tattam B, Zeleny R. Analysis for drugs in saliva. Canberra: Federal Office of Road Safety. 1994, report No. CR141, 1-66. [Google Scholar]
- [70].Takitane J, De Oliveira LG, Endo LG, De Oliveira KC, Muñoz DR, Yonamine M, Leyton V. Uso de anfetaminas por motoristas de caminhão em rodovias do Estado de São Paulo: um risco à ocorrência de acidentes de trânsito? Ciênc saúde coletiva 2013;18:1247-54. [PubMed] [Google Scholar]
- [71].Teles AS, Matos MA, Caetano KAA, Cost LA, França DDS, Pessoni GC, Brunini SM, Martins RMB. Comportamentos de risco para doenças sexualmente transmissíveis em caminhoneiros no Brasil. Rev Panam Salud Publica 2008;24:25-30. [DOI] [PubMed] [Google Scholar]
- [72].Valway S, Jenison S, Keller N, Vega-Hernandez J, Hubbard McCree D. Risk assessment and screening for sexually transmitted infections, HIV, and hepatitis virus among long-distance truck drivers in New Mexico, 2004-2006. Am J Public Health 2009;99:2063-8. doi: 10.2105/AJPH.2008.145383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [73].Williamson A. Predictors of psychostimulant use by long-distance truck drivers. Am J Epidemiol 2007;166:1320-6. doi: 10.1093/aje/kwm205. [DOI] [PubMed] [Google Scholar]
- [74].Yonamine M, Sanches LR, Paranhos BA, De Almeida RM, Andreuccetti G, Leyton V. Detecting alcohol and illicit drugs in oral fluid samples collected from truck drivers in the state of São Paulo, Brazil. Traffic Inj Prev 2013;14:127-31. doi: 10.1080/15389588.2012.696222. [DOI] [PubMed] [Google Scholar]
- [75].Sinagawa DM, De Carvalho HB, Andreuccetti G, Do Prado NV, De Oliveira KC, Yonamine M, Muñoz DR, Gjerde H, Leyton V. Association between travel length and drug use among Brazilian truck drivers. Traffic Inj Prev 2015;16:5-9. doi: 10.1080/15389588.2014.906589. [DOI] [PubMed] [Google Scholar]
- [76].Knauth DR, Pilecco FB, Leal AF, Seffner F, Teixeira AM. Staying awake: truck drivers’ vulnerability in Rio Grande do Sul, Southern Brazil. Rev Saude Publica 2012;46:886-93. [DOI] [PubMed] [Google Scholar]
- [77].Kelly E, Darke S, Ross J. A review of drug use and driving: epidemiology, impairment, risk factors and risk perceptions. Drug Alcohol Rev 2004;23:319-44. doi: 0.1080/09595230412331289482. [DOI] [PubMed] [Google Scholar]
- [78].Gustavsen I, Mørland J, Bramness JG. Impairment related to blood amphetamine and/or methamphetamine concentrations in suspected drugged drivers. Accid Anal Prev 2006;38:490-5. doi: 10.1016/j.aap.2005.11.005. [DOI] [PubMed] [Google Scholar]
- [79].Drummer OH, Gerostamoulos J, Batziris H, Chu M, Caplehorn J, Robertson MD, Swann P. The involvement of drugs in drivers of motor vehicles killed in Australian road traffic crashes. Accid Anal Prev 2004;36:239-48. [DOI] [PubMed] [Google Scholar]
- [80].Musshoff F, Madea B. Driving under the influence of amphetamine-like drugs. J Forensic Sci 2012;57:413-9. doi: 10.1111/j.1556-4029.2012.02055. [DOI] [PubMed] [Google Scholar]
- [81].Logan BK, Schwilke EW. Drug and alcohol use in fatally injured drivers in Washington State. J Forensic Sci 1996;41:505-10. [PubMed] [Google Scholar]
- [82].Coambs RB, McAndrews MP. The Effects of psychoactive substances on workplace performance. Macdonald S, Roman P. (eds.). Drug testing in the workplace. New York: Plenum Press; 1994, pp. 77-102. [Google Scholar]
- [83].McKim W. Drugs and behavior. Cliffs, NJ: Prentice-Hall; 1986. [Google Scholar]
- [84].Bolla K, Rothman R, Cadet JL. Dose-related neurobehavioral effects of chronic cocaine use. J Neuropsych Clin Neurosci 1999;11:361-9. doi: 10.1176/jnp.11.3.361. [DOI] [PubMed] [Google Scholar]
- [85].Burns M. Cocaine effects on performance. Utzelmann HD, Berghaus G, Kroj G. (eds.). Alcohol, drugs, and traffic safety-T’92: proceedings of the 12th International Conference on Alcohol, Drugs and Traffic Safety. Cologne: Verlag TUV Rheinland; 1993, pp. 612-9. [Google Scholar]
- [86].European Agency for Safety and Health at Work (EU-OSHA). A review on the future of work: performance-enhancing drugs. Available online: https://osha.europa.eu/sites/default/files/seminars/documents/Performance%20enhancing%20drugs.pdf.
- [87].Brookhuis KA, Volkerts ER, O’Hanlon JF. Repeated dose effects of lormetazepam and flurazepam upon driving performance. Eur J Clin Pharmacol 1990;39:83-7. [DOI] [PubMed] [Google Scholar]
- [88].Laurell H, Tornros J. The carry-over effects of triazolam compared with nitrazepam and placebo in acute emergency driving situations and in monotonous simulated driving. Acta Pharmacol Toxicol 1986;58:182-6. [DOI] [PubMed] [Google Scholar]
- [89].O’Hanlon JF, Volkerts ER. Hypnotics and actual driving performance. Acta Psychiatr Scand 1986;332:95-104. [DOI] [PubMed] [Google Scholar]
- [90].O’Hanlon JF, Haak TW, Blaauw GJ, Riemersma JB. Diazepam impairs lateral position control in highway driving. Science 1982;217:79-81. [DOI] [PubMed] [Google Scholar]
- [91].Ramaekers JG, Robbe HWJ, O’Hanlon JJ. Marijuana. Human Psychopharmacol 2000;15:551-8. [DOI] [PubMed] [Google Scholar]
- [92].Ray WA, Fought RL, Decker MD. Psychoactive drugs and the risk of injurious motor vehicle crashes in elderly drivers. Am J Epidemiol 1992;136:873-83. [DOI] [PubMed] [Google Scholar]
- [93].Robbe HWJ. Influence of marijuana on driving. CIP-Data Koninklinik Bibliothek. The Hague, Maastricht, The Netherlands: 1994 [Google Scholar]
- [94].Bondallaz P, Favrat B, Chtioui H, Fornari E, Maeder P, Giroud C. Cannabis and its effects on driving skills. Forensic Sci Int 2016;268:92-102. doi: 10.1016/j.forsciint.2016.09.007. [DOI] [PubMed] [Google Scholar]
- [95].Asbridge M, Hayden JA, Cartwright JL. Acute cannabis consumption and motor vehicle collision risk: systematic review of observational studies and meta-analysis. BMJ 2012;344:e536 doi: 10.1136/bmj.e536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [96].Hartman RL, Brown TL, Milavetz G, Spurgin A, Pierce RS, Gorelick DA, Gaffney G, Huestis MA. Cannabis effects on driving longitudinal control with and without alcohol. J Appl Toxicol 2016;36:1418-29. doi: 10.1002/jat.3295. [DOI] [PubMed] [Google Scholar]
- [97].Hartman RL, Brown TL, Milavetz G, Spurgin A, Pierce RS, Gorelick DA, Gaffney G, Huestis MA. Cannabis effects on driving lateral control with and without alcohol. Drug Alcohol Depend 2015;154:25-37. doi: 10.1016/j.drugalcdep.2015.06.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [98].Ronen A, Chassidim HS, Gershon P, Parmet Y, Rabinovich A, Bar-Hamburger R, Cassuto Y, Shinar D. The effect of alcohol, THC and their combination on perceived effects, willingness to drive and performance of driving and non-driving tasks. Accid Anal Prev 2010;42:1855-65. doi: 10.1016/j.aap.2010.05.006. [DOI] [PubMed] [Google Scholar]
- [99].Downey LA, King R, Papafotiou K, Swann P, Ogden E, Boorman M, Stough C. The effects of cannabis and alcohol on simulated driving: influences of dose and experience. Accid Anal Prev 2013;5:879-86. doi: 10.1016/j.aap.2012.07.016. [DOI] [PubMed] [Google Scholar]
- [100].Dubois S, Mullen N, Weaver B, Bédard M. The combined effects of alcohol and cannabis on driving: impact on crash risk. Forensic Sci Int 2015;248:94-100. doi: 10.1016/j.forsciint.2014.12.018. [DOI] [PubMed] [Google Scholar]
- [101].Goldsmith RS, Targin MC, Fanciullo GJ, Martin DW, Hartenbaum NP, White JM, Franklin P. Medical marijuana in the workplace: challenges and management options for occupational physicians. J Occup Environ Med 2015;57:518-25. doi: 10.1097/JOM.0000000000000454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [102].Strand MC, Vindenes V, Gjerde H, Mørland JG, Ramaekers JG. A clinical trial on the acute effects of methadone and buprenorphine on actual driving and cognitive function of healthy volunteers. Br J Clin Pharmacol 2019;85:442-53. doi: 10.1111/bcp.13818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [103].Strand MC, Fjeld B, Arnestad M, Mørland J. Can patients receiving opioid maintenance therapy safely drive? A systematic review of epidemiological and experimental studies on driving ability with a focus on concomitant methadone or buprenorphine administration. Traffic Inj Prev 2013;14:26-38. doi: 10.1080/15389588.2012.689451. [DOI] [PubMed] [Google Scholar]
- [104].Fishbain DA, Cutler RB, Rosomoff HL, Rosomoff RS. Are opioid-dependent/tolerant patients impaired in driving-related skills? A structured evidence-based review. J Pain Symptom Manage 2003;25:559-77. [DOI] [PubMed] [Google Scholar]
- [105].Galski T, Williams JB, Ehle HT. Effects of opioids on driving ability. J Pain Symptom Manage 2000;19:200-8. [DOI] [PubMed] [Google Scholar]
- [106].Kaye AM, Kaye A, Lofton EC. Basic concepts in opioid prescribing and current concepts of opioid-mediated effects on driving. Ochsner J 2013;13:525-32. [PMC free article] [PubMed] [Google Scholar]
- [107].Wickens CM, Mann RE, Brands B, Ialomiteanu AR, Fischer B, Watson TM, Matheson J, Stoduto G, Rehm J. Driving under the influence of prescription opioids: self-reported prevalence and association with collision risk in a large Canadian jurisdiction. Accid Anal Prev 2018;121:14-9. doi: 10.1016/j.aap.2018.08.026. [DOI] [PubMed] [Google Scholar]
- [108].Verster JC, Veldhuijzen DS, Patat A, Olivier B, Volkerts ER. Hypnotics and driving safety: meta-analyses of randomized controlled trials applying the on-the-road driving test. Curr Drug Saf 2006;1:63-71. [DOI] [PubMed] [Google Scholar]
- [109].Dubois S, Bédard M, Weaver B. The impact of benzodiazepines on safe driving. Traffic Inj Prev 2008;9:404-13. doi: 10.1080/15389580802161943. [DOI] [PubMed] [Google Scholar]
- [110].Van Laar MW, Volkerts ER. Driving and benzodiazepine use. Mol Diag Ther 1998;10:383. [Google Scholar]
- [111].Toennes SW, Kauert GF, Steinmeyer S, Moeller MR. Driving under the influence of drugs - evaluation of analytical data of drugs in oral fluid, serum and urine, and correlation with impairment symptoms. Forensic Sci Int 2005;152:149-55. doi: 10.1016/j.forsciint.2004.08.002. [DOI] [PubMed] [Google Scholar]
- [112].Vindenes V, Lund HM, Andresen W, Gjerde H, Ikdahl SE, Christophersen AS, Øiestad EL. Detection of drugs of abuse in simultaneously collected oral fluid, urine and blood from Norwegian drug drivers. Forensic Sci Int 2012;219:165-71. doi: 10.1016/j.forsciint.2012.01.001. [DOI] [PubMed] [Google Scholar]
- [113].Kelley-Baker T, Moore C, Lacey JH, Yao J. Comparing drug detection in oral fluid and blood: data from a national sample of nighttime drivers. Traffic Inj Prev 2014;15:111-8. doi: 10.1080/15389588.2013.796042. [DOI] [PubMed] [Google Scholar]
- [114].Casolin A. Comparison of urine and oral fluid for workplace drug testing. J Anal Toxicol 2016;40:479-85. doi: 10.1093/jat/bkw055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [115].European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). EU Action Plan on Drugs 2017-2020. Available online: www.emcdda.europa.eu/system/files/attachments/5642/eu-action-plan%27-on-drugs-2017-2020.pdf.
- [116].Carpenter CS. Workplace drug testing and worker drug use. Health Serv Res 2007;42:795-810. doi: 10.1111/j.1475-6773.2006.00632.x. [DOI] [PMC free article] [PubMed] [Google Scholar]