

Abstract
Medical claims were analyzed from 2,810 military children who visited a civilian emergency department (ED) or hospital from 2000–2014 with behavioral health as the primary diagnosis and TRICARE as the primary/secondary payer. Visit prevalence was estimated annually and categorized: 2000–2002 (pre-deployment), 2003–2008 (first post-deployment), 2009–2014 (second post-deployment). Age was categorized: preschoolers (0–4 years), school-aged (5–11 years), adolescents (12–17 years). During Afghanistan and Iraq wars, 2,562 military children received 4,607 behavioral health visits. School-aged children’s mental health visits increased from 61 to 246 from pre-deployment to the second post-deployment period. Adolescents’ substance use disorder (SUD) visits increased almost 5-fold from pre-deployment to the first post-deployment period. Mental disorders had increased odds (OR=2.93, 95% CI: 1.86–4.61) of being treated during hospitalizations than in EDs. Adolescents had increased odds of SUD treatment in EDs (OR=2.92, 95% CI: 1.85–4.60) compared to hospitalizations. Implications for integrated behavioral health and school behavioral health interventions are discussed.
Keywords: military children, behavioral health care, Military Health System beneficiaries, military medicine, mixed effects model, Afghanistan and Iraq wars
Introduction
Over two million American children have experienced a parent deploying to Afghanistan or Iraq; more than 41,000 had a parent injured and more than 3,700 experienced the death of a parent.1,2 Military children have unique experiences associated with their parents’ military service.3 The military lifestyle exposes them to frequent relocations, changes in schools and communities, prolonged family separations, parental deployment, post-deployment physical and psychological injuries of their parents, and post-deployment reintegration difficulties of military families.3–5 As a result, military children are at risk for behavioral health problems, including anxiety, mood, and substance use disorders. Given the demands and uncertainty of the military lifestyle, these behavioral health problems can endure across developmental stages and result in the need for behavioral health services. The need for behavioral health services by military children can potentially impact the work performance or attendance, enlistment and re-enlistment decisions of military parents, and increase military family stress, and thus, is of significant concern for senior military leadership and defense policymakers.
Children of deployed service members are more likely to have behavioral health problems than their same-aged peers.6 Common behavioral health conditions among military children include sleep problems, depression, anxiety, substance use, and suicidal ideation,7–10 which may differ by age, gender, and developmental level. Parental report on the Child Behavior Checklist revealed that preschool military children (ages 3–5 years) of a deployed parent exhibited higher levels of both internalizing (i.e., emotional reactivity, anxiousness/depression, somatic complaints, withdrawal) and externalizing (i.e., attention difficulties, aggression) behaviors compared to same-aged peers without a deployed parent and children aged 1.5–3 years regardless of parent’s deployment status.11 Among school-aged children of Persian Gulf War veterans, girls were found to have increased tearfulness/sadness and boys had more discipline problems.12 Parental deployment is also associated with increased behavioral (18%) and stress (19%) disorders among military children ages 3–8 years.4 Military children ages 4–16 years of deployed parents also reported significantly more psychosocial difficulties than same-aged peers without a deployed parent based on parental and self-report.13
Given the majority of school-aged military children and adolescents attend civilian schools,14 recent investigations compared rates of behavioral health problems between military and nonmilitary students. On the Pediatric Symptom Checklist, school-aged military children scored high risk for emotional and behavioral problems at 2.5 times higher than national norms.15 Military adolescents who attend civilian schools have higher rates of negative social and emotional outcomes, including violence and victimization, gang affiliation, substance use and abuse, depression, and suicidal ideation than nonmilitary students who attend the same schools.9,10,16,17 Stress from a parental deployment also results in elevated anxiety and self-reports of low quality of life in military school-age children, which subsequently impacts social, emotional, and academic functioning.18 Having a family member deployed is also associated with decreased positive well-being and increased feelings of sadness or hopelessness among 7th, 9th and 11th grade military adolescents compared to non-military peers.9 Boys were less likely to report experiencing sadness or hopelessness, depressive symptoms, and suicidal ideation (9th and 11th graders only) compared to girls.9
Behavioral health service use by military children also increases during parental deployments. Despite an overall decrease in pediatric outpatient visits in FY2007 and FY2008, military children ages 3–8 years had an 11% increase in behavioral health outpatient visits during parental deployments, with older children having higher rates than younger children.4 Boys had decreased rates of outpatient behavioral health care visits compared to girls.4 Attention-deficit (30.1%), adjustment (14.6%), and autistic (12.1%) disorders were the most common primary diagnoses associated with these outpatient visits.7 From 2003–2006, parental deployment was associated with increased visits for acute stress reaction, and adjustment, behavioral, and mood disorders.19 Larson et al.20 found increased rates of pediatric specialist visits for psychiatric conditions with a 12% (under age 12) and 18% (over age 12) increase for military children of deployed service members. Afghanistan and Iraq deployments are also associated with a 17.2% increase in antidepressant prescriptions and a 10% increase in antianxiety prescriptions for children of active duty service members, but a decrease in use of health care in military treatment facilities (MTFs),21 suggesting increased behavioral health service utilization during parental deployments in civilian medical facilities.
Despite a wealth of evidence on behavioral health problems military children experience, few studies focus on behavioral health treatment received by military children. Current behavioral health treatment evidence on military children primarily focuses on children under age 821 or those who receive care in military treatment facilities.4,22,23 Limited evidence exists on behavioral health treatment received by military children in civilian acute care facilities providing care via the Military Health System (MHS) purchased care component, which is contracted care provided to military service members, retirees, and family members from all branches of military service by TRICARE-approved civilian facilities and providers in TRICARE regional networks.24,25 This study fills this knowledge gap by examining trends in behavioral health treatment received by military children age 17 and younger in civilian emergency departments (EDs) and inpatient facilities from 2000–2014. ED visits and acute psychiatric care for behavioral health conditions experienced by military children suggest the need for emergency services and/or intensive inpatient care for crises related to a danger to self or others, exacerbation of a current behavioral health condition, an undiagnosed and/or untreated behavioral health condition, or limited access to outpatient or specialty pediatric behavioral health care despite access to health care in MTFs. With more than 50% of military children receiving treatment from non-military pediatricians,8 examining behavioral health treatment received in civilian acute care facilities is important for understanding behavioral health care needs of military children and developing targeted behavioral health interventions.
Given the U. S. has been at war for more than 15 years, many military children have only lived during wartime and may experience emotional distress not only from actual parental deployments, but from the possibility of parental deployment based on the experiences of neighboring military families and friends. Additionally, risk for behavioral health problems occurring during parental deployment persists and even increases after parental deployment.23 Thus, more evidence is needed to understand trends in behavioral health treatment received by military children who may have been directly or indirectly impacted by the Afghanistan and Iraq wars.
Methods
This longitudinal study was a part of a larger study, Behavioral Health Care by Military Health System Beneficiaries in Civilian Medical Facilities,25 analyzing medical claims data from the South Carolina Revenue and Fiscal Affairs Office (RFA), which stores and maintains medical claims from all health care systems in South Carolina. Per the RFA data use agreement, patients and health care facilities were de-identified. The University of South Carolina Institutional Review Board approved this study. See Wooten et al.25 for a detailed description of adult and child MHS beneficiaries receiving behavioral health care in civilian medical facilities in South Carolina from 2000–2014.
Setting
MHS beneficiaries are well-represented in South Carolina. As of 2014, 243,202 MHS beneficiaries resided in South Carolina of which 125,059 were TRICARE Prime enrollees and 8,556 were TRICARE Reserve Select enrollees.26 Wooten et al.25 provides a detailed description of TRICARE enrollees. Although the number of military school-aged children in South Carolina varied over time, the highest recent prevalence reported was 23,710 in 2012.27
Sample population
The sample included medical claims for all child dependents of military service members from all branches of military service who visited an ED, inpatient facility, or ambulatory care facility in South Carolina from January 1, 2000 to December 31, 2014, with behavioral health disorders, including both mental health and substance use disorders, as the primary diagnosis and TRICARE listed as the primary or secondary payer. A total of 2,810 patients who were 17 years old and younger with a combined 5,004 behavioral health visits were included in the analytic sample.
War and deployment-related time periods
The study observation period was January 1, 2000 to December 31, 2014, a total of 15 years, and included all electronically captured medical claims data available in South Carolina during this timeframe. The observation period also included the current war periods: Operation Enduring Freedom (OEF) in Afghanistan from October 7, 2001 to December 28, 2014 and Operation Iraqi Freedom (OIF) in Iraq from March 19, 2003 to August 31, 2010.28 To estimate child behavioral health treatment trends during OEF/OIF, the 15-year study period was categorized into deployment-related time periods: pre-deployment (2000–2002), first post-deployment period (2003–2008), and second post-deployment period (2009–2014). Post-deployment periods were divided equally in 6-year increments. The rationale for deployment-related time periods parallels increased war-related violence and troop surges (i.e., increased number of U. S. armed forces) in Afghanistan and Iraq war zones. The Iraq invasion (2003) and Iraq troop surge (2007) occurred during the first post-deployment period, which exposed military children to pre-deployment activities, training, and preparation as well as prolonged parental separations.29 The Iraq drawdown (2009) and Afghanistan troop surge (2011) occurred during the second post-deployment period,29 which meant some military children had already been exposed to multiple, lengthy deployments and multiple post-deployment reintegrations. Thus, the second post-deployment period potentially represents cumulative exposure to deployment-related activities by military children and intermittent adjustments and readjustments by military families to pre-deployment, deployment, and post-deployment activities. Because OEF began in late 2001 and there was a 12-months boots on the ground deployment policy,29 2003 is the first calendar year that deployed military parents would have redeployed home and military children were exposed to parental physical and/or psychological combat-related injuries. Trends in child behavioral health treatment and visit characteristics were also estimated annually from 2000–2014. (See supplemental tables S1, S2, and S3).
Measures
Demographics.
Age group categorized as preschoolers (0–4 years), school-aged children (5–11 years), and adolescents (12–17 years); gender (male/female) and race (White, Black, Hispanic, Other) were estimated based on the child patient’s age at first behavioral health visit on a medical claim during the 15-year observation period.
Visit type.
Visit type was categorized as inpatient hospitalizations and ED visits, which were ED visits resulting in a hospitalization in the same facility. Outpatient ED visits were those in which patients received ED services and were discharged home from the ED without being admitted into the hospital. ED visits and outpatient ED visits were combined into the ED visit variable.
Behavioral health bed-days.
Behavioral health bed-days, categorized as less than or equal to 7 days, 8–14 days, or greater than or equal to 15 days, were identified based on hospital discharges and calculated by taking the difference in days between the admission and discharge dates. Mental health and substance use disorder (SUD) bed-days were also computed.
Behavioral health treatment.
The dependent variable was receipt of behavioral health treatment defined as inpatient hospitalizations and ED visits for primary diagnoses of behavioral health disorders, including mental health disorders and/or SUDs. Major Diagnostic Codes (MDC) 19 (mental diseases/disorders) and 20 (alcohol/other drug disorders) were used to identify inpatient hospitalizations and ED visits for behavioral health diagnoses on a medical claim. MDCs are formed by dividing all possible primary diagnoses, defined by the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM) codes, into 25 mutually exclusive diagnostic categories, which are primarily a claims and administrative data element unique to the United States medical reimbursement system. For consistency across both inpatient hospitalizations and ED visits, an algorithm of ICD-9-CM diagnosis codes corresponding to MDC 19 and 20 was created. Specifically, MDC 19 was defined by ICD-9-CM codes 290.x, 293.x – 302.x, 306.x – 315.x (excluding 307.81 tension headache) and 317.x – 319.x. MDC 20 was defined by ICD-9 codes: 291.x, 292.x, 303.x – 305.x. Mental health treatment was defined by MDC 19 and substance use treatment by MDC 20.
Behavioral health diagnoses.
Behavioral health diagnoses were identified within MDC 19 and 20 using ICD-9-CM codes designated as the primary diagnosis to better assess prevalence and patterns of behavioral health treatment (i.e., measured as inpatient hospitalizations and ED visits) during the Afghanistan and Iraq wars. Most mental health and SUDs were derived using algorithms from Case Definitions for the Armed Forces Health Surveillance Center,30 which is used for conducting epidemiological reports on alcohol and SUDs, and psychosocial problems among military service members. For mental health disorders, these included adjustment, anxiety, mood, personality, and bipolar disorders; psychosis, posttraumatic stress disorder (PTSD), and schizophrenia. Psychosocial problems were defined by V-codes (V40.xx, V61.0x, V61.1x, V61.2x, V62.8-V62.82, V62.84-V62.85, 995.8x) related to marital and family relationships, maltreatment, and life circumstances. Alcohol use disorder (AUD) was also defined by this algorithm and alcohol dependence was assessed using ICD-9 code 303.xx. Drug dependence and abuse were divided into categories based on ICD-9 codes: opioid/combination opioid-type dependence (304.0x, 304.7x); sedative, hypnotic, or anxiolytic dependence (304.1x); cocaine dependence (304.2x); cannabis dependence (304.3x); other specified drug dependence (304.6x); combinations of drug dependence excluding opioid type (304.8x); unspecified drug dependence (304.9x); tobacco use disorder (305.1); nondependent cannabis abuse (305.2x); nondependent sedative, hypnotic or anxiolytic abuse (305.4x); nondependent opioid abuse (305.5x); nondependent cocaine abuse (305.6x); nondependent amphetamine or related acting sympathomimetic abuse (305.7); and nondependent mixed or unspecified drug abuse (305.9x).
Statistical analyses
Behavioral health treatment was defined by number of inpatient hospitalizations, ED visits, and unique patients annually and categorized by pre-deployment (2000–2002), first post-deployment (2003–2008), and second post-deployment (2009–2014) periods for any behavioral health, mental health, and substance use treatment (SUT). Additional behavioral health visit characteristics for child MHS beneficiaries included mean age, age group, sex, race, visit type, mean behavioral health bed-days, and bed-day frequencies. Annual frequencies of behavioral health visits were plotted by type of behavioral health treatment (mental health, substance use, any behavioral health), visit type (inpatient hospitalization, ED), and by deployment-related time periods (pre-deployment, first post-deployment, second post-deployment) during OEF/OIF. For behavioral health diagnoses, categorized by mental health and SUDs, prevalence was computed by age group for the total observation period and prevalence was calculated as the number of total visits with a mental health and/or SUD listed as the primary diagnosis divided by the number of total visits for a specific age group. Due to small mental health visit totals for preschoolers, and preschoolers and school-aged children for SUD visits, prevalence of ICD-9-CM diagnostic codes were examined rather than MDC 19 and 20 for these age groups.
To estimate trends in behavioral health treatment during the Afghanistan and Iraq wars, two mixed effects models were estimated. For mental health treatment, a mixed effects model was estimated with deployment-related time periods (2000–2002, 2003–2008, 2009–2014), age group (5–11, 12–14, 15–17 years), sex, race, mental health bed-days, and visit type as predictors and mental health treatment (yes/no) for the total observation period (2000–2014) as the outcome for school-aged children (5–11 years) and adolescents (12–17 years). For SUT, a mixed effects model including only adolescents was estimated with deployment-related time periods (2000–2002, 2003–2008, 2009–2014), age group (12–14, 15–17 years), sex, race, SUD bed-days, and visit type as predictors and SUT for the total observation period (2000–2014) as the outcome. Preschool children (0–4 years) were excluded from both mixed effects models due to low sample size (n=41) and cell counts. Only military adolescents were included in the SUT model because they utilized 98.1% of SUT. All descriptive statistics were conducted using SAS/STAT 9.4 and mixed effects models were estimated using lme4 package in R 3.3.1.31
Results
A total of 5,004 behavioral health visits were received by 2,810 unique child MHS beneficiaries from 2000–2014 in civilian acute care facilities. Of the 2,810 unique child patients, 41 (1.5%) were preschoolers, 473 (16.8%) were school-aged children, and 2,296 (81.7%) were adolescents based on the patient’s first visit during the 15-year observation period. Mean age was 13.8 years for the total sample and 2.1 years for preschoolers, 8.9 years for school-aged children, and 15.0 years for adolescents. Boys comprised 47.0% and girls were 53.0% of the sample. Supplemental Tables S1, S2, and S3 (available online) report behavioral health treatment characteristics by sex, race, visit type, bed-days, and unique number of child patients annually.
Behavioral health bed-days
Mean bed-days were 10.4 (sd=28.2) days for behavioral health hospitalizations collectively; however, SUD hospitalizations resulted in a much longer stay on average (21.5 days) compared to mental health hospitalizations (10.1 days, sd=27.9). Bed-days varied by mental health and SUD hospitalizations. On average, bed-days for bipolar disorder were 13.4 days, and bed-days for depression, adjustment, and anxiety disorders were 9.0, 7.0, and 6.0 days, respectively. For adolescents, mean hospital bed-days for mixed or unspecified drug abuse was 33.8 days, compared to a mean of 32.1 days for AUDs and 16.8 days for cannabis abuse. Most (58.4%) SUD hospitalizations lasted < 7 days and almost one-third (29.9%) lasted ≥ 15 days. Only 11.7% of SUD hospitalizations lasted 8–14 days. Number of bed-days for mental health hospitalizations were predominantly < 7 days (60.3%) with 31.5% lasting 8–14 days, and 8.2% lasting ≥ 15 days. Supplement 1 provides more detailed results on behavioral health treatment by child MHS beneficiaries from 2000–2014.
Behavioral health treatment during Afghanistan (OEF) and Iraq (OIF) wars
During the Afghanistan and Iraq wars (2002–2014), 4,607 behavioral health visits were received by 2,562 unique child MHS beneficiaries in civilian acute care facilities. Behavioral health visit prevalence remained above 205, ranging from 205 to 300 annually from 2003–2014 compared to 132, 156, and 174 from 2000–2003 (Table S1). There were spikes in both visits and unique child patients during 6 of the last 10 years of OEF (i.e., 2006, 2008, 2009, 2011, 2013, 2014). Number of unique child patients receiving behavioral health treatment remained above 200 (ranging 205–300) during OEF/OIF and annual ED visits for behavioral health conditions remained above 150 (ranging 151–232) from 2008–2014 (see Table S1). Annual behavioral health visits remained over 280 (ranging 283–466) from 2003–2014. The number of unique child patients also increased from pre-deployment (n=422) to first post-deployment (n=1,076) and second post-deployment (n=1,312) periods. Figure 1 displays the frequency of behavioral health treatment in civilian health facilities annually by mental health and substance use for school-aged children and adolescents (ages 5–17 years) and by OEF and OIF. Figure 2 displays the frequency of behavioral health treatment by visit type (emergency department, inpatient hospitalization) for school-aged children and adolescents (ages 5–17 years) and by OEF and OIF.
Figure 1:
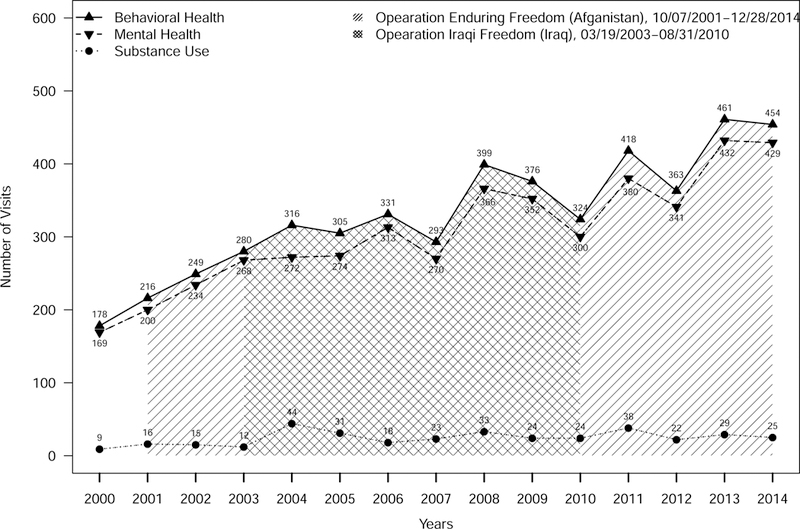
Behavioral health care for school-aged children and adolescent Military Health System beneficiaries during Afghanistan and Iraq Wars, by type of behavioral health disorder (5–17 year olds)
Figure 2:
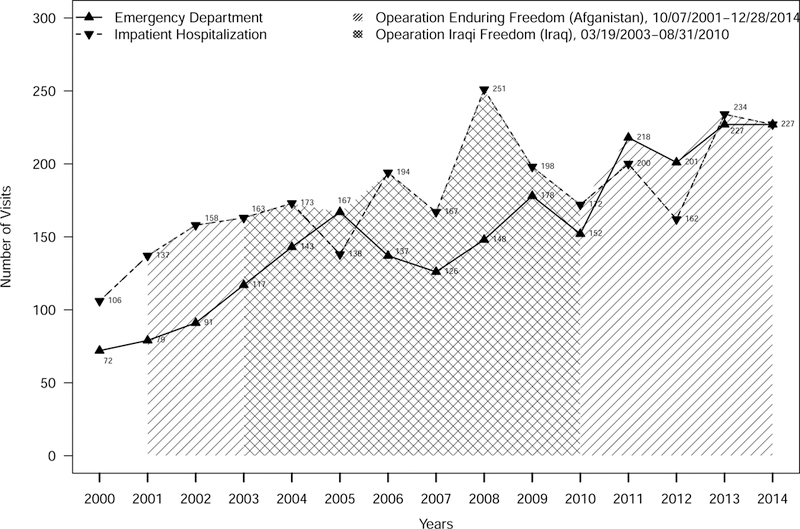
Behavioral health care by school-aged children and adolescent Military Health System beneficiaries during Afghanistan and Iraq Wars, by type of behavioral health visit (5–17 year olds)
Table 1 reports behavioral health visit characteristics by deployment-related time periods: pre-deployment (2000–2002), first post-deployment (2003–2008), and second post-deployment (2009–2014). The distribution of behavioral health visits by age and gender were similar across pre-deployment and post-deployment periods. Prevalence of behavioral health visits received by school-aged children and adolescents increased from the first to second post-deployment periods. Although adolescents received an overwhelming majority of care (81.7%), school-aged children had the largest increase in behavioral health care over time from 61 (12.9%) visits between 2000–2002 to 247 (52.3%) between 2009–2014. Positive trends were also observed for both Blacks and Whites for whom the number of behavioral health visits more than tripled from pre-deployment to the second post-deployment period. ED visits increased by 20% over 12 years of war from 243 during pre-deployment to 1,220 during the second post-deployment period. A positive trend was observed in ED visits for both post-deployment periods, increasing from 35.5% of visits in the pre-deployment period to 48.2% in the second post-deployment period for mental health visits, and from 70.0% to 82.2% for SUD visits.
Table 1.
Sociodemographic characteristics of child Military Health System beneficiaries receiving behavioral health treatment in South Carolina Health Systems, 2000–2014, by pre-deployment and post-deployment periods1
| Characteristics | Pre-deployment Period2 | First Post-deployment Period | Second Post-deployment Period | All Years |
|---|---|---|---|---|
| 2000–2002 n = 646 (12.9% of total visits) |
2003–2008 n = 1,943 (38.8% of total visits) |
2009–2014 n = 2,415 (48.3% of total visits) |
2000–2014 n = 5,004 |
|
| Patients3 (% of patients) | 422 (15) | 1,076 (38.3) | 1,312 (46.7) | 2,810 |
| Age (m, sd)4 | 14.0 (2.9) | 13.9 (3.1) | 13.6 (3.2) | 13.8 (3.1) |
| Age | ||||
| 0–4 | 3 (7.3) | 19 (46.3) | 19 (46.3) | 41 (1.5) |
| 5–11 | 61 (12.9) | 164 (34.8) | 247 (52.3) | 472 (16.8) |
| 12–17 | 358 (15.6) | 893 (38.9) | 1,046 (45.5) | 2,297 (81.7) |
| Sex | ||||
| Male | 198 (15.0) | 517 (39.2) | 605 (45.8) | 1,320 (47.0) |
| Female | 224 (15.0) | 559 (37.5) | 707 (47.5) | 1,490 (53.0) |
| Race | ||||
| Black | 100 (15.4) | 236 (36.4) | 312 (48.2) | 648 (23.1) |
| White | 281 (14.3) | 779 (39.7) | 904 (46.0) | 1,964 (69.9) |
| Hispanic | 13 (22.4) | 17 (29.3) | 28 (48.3) | 58 (2.1) |
| Other 5 | 28 (20.0) | 44 (31.4) | 68 (48.6) | 140 (5.0) |
| Visit Type | ||||
| Emergency Department | 243 (10.5) | 855 (36.9) | 1,220 (52.6) | 2,318 (46.32) |
| Inpatient Hospitalizations | 403 (15.0) | 1,088 (40.5) | 1,195 (44.5) | 2,686 (53.68) |
| Hospital Bed-days6 (m, sd) | 9.2 (28.9) | 9.7 (26.0) | 11.5 (29.9) | 10.4 (28.2) |
| ≤ 7 days | 313 (77.7) | 673 (61.9) | 633 (53.0) | 1,619 (69.1) |
| 8–14 days | 69 (17.1) | 301 (27.7) | 460 (38.5) | 830 (30.9) |
| ≥ 15 days | 21 (5.2) | 114 (10.5) | 102 (8.5) | 237 (8.8) |
Behavioral health treatment includes all visits for MDC 19 (mental health disorders and diseases) and MDC 20 (alcohol/other drugs).
Although Operation Enduring Freedom (Afghanistan) began in 2001, given the 12-month deployment policy, 2003 was the first eligible post-deployment year.
Unique child patients per pre-deployment and post-deployment periods.
Mean age of unique patients based on age on first behavioral health claim during the time period.
Other = American Indian, Asian, Pacific Islander/Alaska Native, and other racial/ethnic groups.
Bed-days = Number of days child patients were in the hospital for inpatient care.
Mental health treatment.
During OEF/OIF (2002–2014), approximately 4,266 mental health visits were received by 2,422 child MHS beneficiaries in civilian acute care facilities. Mental health visit prevalence remained above 184, ranging from 184 to 280 annually from 2003–2014 compared to 125, 149, and 166 from 2000–2003 (Table S2). Table 2 reports mental health visit characteristics by pre-deployment (2000–2002), first post-deployment (2003–2008), and second post-deployment (2009–2014) periods. The distribution of mental health visits by age and gender were similar across pre-deployment and post-deployment periods. Prevalence of mental health visits received by school-aged children and adolescents increased from the first to second post-deployment periods. Although adolescents received an overwhelming majority of care (80.4%), school-aged children had the largest increase in mental health care over time from 61 (13.0%) visits between 2000–2002 to 246 (52.5%) between 2009–2014. Positive trends were also observed for both Blacks and Whites for whom the number of mental health visits more than tripled from pre-deployment (2000–2002) to the second post-deployment period (2009–2014). ED visits increased by 20% over 12 years of war from 215 during pre-deployment to 1,086 during the second post-deployment period. For mental health hospitalizations, mean bed-days increased chronologically from 8.7 days in the pre-deployment period to 11.0 days in the second post-deployment period. Overall, there were positive trends in mental health treatment for ED visits, inpatient hospitalizations, and mental health bed-days.
Table 2.
Sociodemographic characteristics of child Military Health System beneficiaries receiving mental health treatment in South Carolina Health Systems, 2000–2014, by pre-deployment and post-deployment periods1
| Characteristics | Pre-deployment Period2 | First Post-deployment Period | Second Post-deployment Period | All Years |
|---|---|---|---|---|
| 2000–2002 n = 606 (13.1% of total visits) |
2003–2008 n = 1,780 (38.4% of total visits) |
2009–2014 n = 2,252 (48.6% of total visits) |
2000–2014 n = 4,638 |
|
|
Patients3 (% of patients) |
402 (15.5) | 976 (37.7) | 1,212 (46.8) | 2,590 |
| Age (m, sd)4 | 13.9 (2.9) | 13.7 (3.1) | 13.5 (3.2) | 13.8 (3.1) |
| 0–4 | 3 (7.9) | 17 (44.7) | 18 (47.4) | 38 (1.5) |
| 5–11 | 61 (13.0) | 162 (34.5) | 246 (52.5) | 469 (18.1) |
| 12–17 | 338 (16.2) | 797 (38.3) | 948 (45.5) | 2,083 (80.4) |
| Sex | ||||
| Male | 186 (15.6) | 453 (38.1) | 550 (46.3) | 1,189 (45.9) |
| Female | 216 (15.4) | 523 (37.3) | 662 (47.3) | 1,401 (54.1) |
| Race | ||||
| Black | 96 (16.0) | 213 (35.6) | 290 (48.4) | 599 (23.1) |
| White | 267 (14.8) | 705 (39.1) | 830 (46.1) | 1,802 (69.6) |
| Hispanic | 13 (24.1) | 14 (25.9) | 27 (50.0) | 54 (2.1) |
| Other 5 | 26 (19.3) | 44 (32.6) | 65 (48.2) | 135 (5.2) |
| Visit Type | ||||
| Emergency Department | 215 (10.6) | 728 (35.9) | 1,086 (48.2) | 2,029 (43.8) |
| Inpatient Hospitalizations | 391 (15.0) | 1,052 (40.3) | 1,166 (44.7) | 2,609 (56.3) |
|
Mental Health Bed-Days6 (m, sd) |
8.7 (28.0) | 9.6 (26.1) | 11.0 (29.3) | 10.1 (27.9) |
| ≤ 7 days | 303 (77.5) | 653 (62.1) | 618 (53.0) | 1,574 (60.3) |
| 8–14 days | 69 (17.7) | 295 (28.0) | 457 (39.2) | 821 (31.5) |
| ≥ 15 days | 19 (4.9) | 104 (9.9) | 91 (7.8) | 214 (8.2) |
Mental health treatment includes all visits for MDC 19 (mental health disorders and diseases).
Although Operation Enduring Freedom (Afghanistan) began in 2001, given the 12-month deployment policy, 2003 was the first eligible post-deployment year.
Unique child patients per pre-deployment and post-deployment periods.
Mean age of unique patients based on age on first behavioral health claim during the time period.
Other = American Indian, Asian, Pacific Islander/Alaska Native, and other racial/ethnic groups.
Bed-days = Number of days child patients were hospitalized for mental health disorders.
Substance use treatment.
During OEF/OIF (2002–2014), approximately 341 SUD visits were received by 214 child MHS beneficiaries in civilian acute care facilities. SUD visit prevalence remained relatively consistent from 2004–2014 with the highest prevalence in 2004 (n=14) and 2011 (n=39; see Table S2). Table 3 reports SUD visit characteristics by pre-deployment (2000–2002), first post-deployment (2003–2008), and second post-deployment (2009–2014) periods. The distribution of SUD visits was concentrated among adolescents and increased almost 5-fold from pre-deployment to the first post-deployment period, but remained relatively stable between the two post-deployment periods. Boys had the highest prevalence of SUD visits for pre-deployment and both post-deployment periods. Although White children had the highest prevalence of SUD visits during both post-deployment periods, the prevalence of SUD visits remained stable for both Whites and Blacks during both post-deployment periods. ED visits more than quadrupled over 12 years of war from 28 during pre-deployment to 134 during the second post-deployment period. For SUD hospitalizations, mean bed-days were similar in the pre-deployment (24.1 days) and second post-deployment periods (27.0 days), but were twice those in the first post-deployment period (12.8 days).
Table 3.
Sociodemographic characteristics of child Military Health System beneficiaries receiving substance use treatment in South Carolina Health Systems, 2000–2014, by pre-deployment and post-deployment periods1
| Characteristics | Pre-deployment Period2 | First Post-deployment Period | Second Post-deployment Period | All Years |
|---|---|---|---|---|
| 2000–2002 n = 40 (10.9% of total visits) |
2003–2008 n = 163 (44.5% of total visits) |
2009–2014 n = 646 (12.9% of total visits) |
2000–2014 n = 366 |
|
| Patients3 (% of patients) | 20 (9.0) | 100 (45.5) | 100 (45.5) | 220 |
| Age (m, sd)4 | 15.6 (1.3) | 15.4 (2.5) | 15.5 (1.9) | 15.5 (2.2) |
| 0–4 | 0 (0) | 2 (66.7) | 1 (33.3) | 3 (1.4) |
| 5–11 | 0 (0) | 2 (66.7) | 1 (33.3) | 3 (1.4) |
| 12–17 | 20 (9.4) | 96 (44.9) | 98 (45.8) | 214 (97.3) |
| Sex | ||||
| Male | 12 (9.2) | 64 (48.9) | 55 (41.9) | 131 (59.6) |
| Female | 8 (9.0) | 36 (40.5) | 45 (50.5) | 89 (40.5) |
| Race | ||||
| Black | 4 (8.2) | 23 (46.9) | 22 (44.9) | 162 (73.6) |
| White | 14 (8.6) | 74 (45.7) | 74 (45.7) | 49 (22.3) |
| Hispanic | 0 (0) | 3 (3.0) | 1 (1.0) | 4 (1.8) |
| Other 5 | 2 (10.0) | 0 (0.0) | 3 (3.0) | 5 (2.3) |
| Visit Type | ||||
| Emergency Department | 28 (9.7) | 127 (43.9) | 134 (46.4) | 289 (100.0) |
| Inpatient Hospitalizations | 12 (30.0) | 36 (22.1) | 29 (17.8) | 77 (21.0) |
|
Substance Use Disorder Bed-Days6 (m, sd) |
24.1 (49.8) | 12.8 (18.0) | 27.0 (39.5) | 19.9 (33.4) |
| ≤ 7 days | 10 (83.3) | 20 (55.6) | 15 (51.7) | 45 (58.4) |
| 8–14 days | 0 (0) | 6 (16.7) | 3 (10.3) | 9 (11.7) |
| ≥ 15 days | 2 (16.7) | 10 (27.8) | 11 (37.9) | 23 (29.9) |
Substance use treatment includes all visits for MDC 20 (alcohol/drug use).
Although Operation Enduring Freedom (Afghanistan) began in 2001, given the 12-month deployment policy, 2003 was the first eligible post-deployment year.
Unique child patients per pre-deployment and post-deployment periods.
Mean age of unique patients based on age on first behavioral health claim during the time period.
Other = American Indian, Asian, Pacific Islander/Alaska Native, and other racial/ethnic groups.
Bed-days = Number of days child patients were hospitalized for substance use disorders.
Behavioral health diagnoses.
Based on primary diagnoses, preschool children were treated for a variety of mental health diagnoses, including post-concussion syndrome; sleep terror, autistic, tic, anxiety, sleep, and attention deficit disorder with hyperactivity. School-aged children received behavioral health treatment most frequently for mood (19.1%), bipolar (8.7%), adjustment (5.5%), and anxiety (5.0%) disorders. Similarly, adolescents received behavioral health treatment most frequently for mood (44.1%), bipolar (9.6%), adjustment (5.6%), and anxiety (5.3%) disorders. Less commonly treated conditions in school-aged children and adolescents included psychosocial problems, personality disorder, PTSD, and schizophrenia. SUDs were rarely treated in preschool and school-aged children. Among adolescents, AUD (37.9%), nondependent mixed or unspecified drug abuse (21.7%), and non-dependent cannabis abuse (14.8%) were the most frequently treated SUDs. SUDs for which adolescents were less commonly treated included cocaine abuse/dependence, opioid abuse/dependence, amphetamine abuse, and alcohol dependence.
Mixed effects models estimating trends in receipt of behavioral health treatment
Tables 4 and 5 present results of two mixed effects models examining trends in mental health and SUT from 2000–2014. The mental health treatment model examined trends in both school-aged children (5–11 years) and adolescents (12–14 years, 15–17 years). Given an overwhelming majority (98.1%) of SUT was received by adolescents, the SUT model only examined trends in military adolescents (12–17 years).
Table 4.
Mixed effects model predicting probability of mental health treatment by school-aged children and adolescent Military Health System beneficiaries, 2000–2014
| Characteristics | Mental Health Treatment | ||
| OR | 95% Confidence Limit | ||
| Lower | Upper | ||
| Time (ref=2000–2002) | |||
| 2003–2008 | 0.83 | 0.56 | 1.22 |
| 2009–2014 | 0.98 | 0.66 | 1.45 |
| Age (ref = 5 – 11 years) | |||
| 12 – 14 years | 0.13*** | 0.05 | 0.38 |
| 15 – 17 years | 0.03*** | 0.01 | 0.09 |
| Sex (ref=Male) | |||
| Female | 2.45*** | 1.92 | 3.12 |
| Race (ref=White) | |||
| Black | 1.36* | 1.01 | 1.84 |
| Other | 1.51 | 0.84 | 2.71 |
| Visit Type (ref = Emergency Department) | |||
| Inpatient Hospitalization | 2.93*** | 1.86 | 4.61 |
| Mental Health Bed-Days (ref = ≤7 days) | |||
| 8 −14 days | 2.88** | 1.37 | 6.05 |
| ≥ 15 days | 0.54 | 0.28 | 1.04 |
p < .001.
p < .01.
p < .05.
Table 5.
Mixed effects model predicting probability of substance use treatment by adolescent Military Health System beneficiaries, 2000–2014
| Characteristics | Substance Use Treatment | ||
|---|---|---|---|
| OR | 95% Confidence Limit | ||
| Lower | Upper | ||
| Time (ref=2000–2002) | |||
| 2003–2008 | 1.18 | 0.80 | 1.75 |
| 2009–2014 | 1.01 | 0.68 | 1.49 |
| Age (ref = 12–14) | |||
| 15 – 17 years | 4.05*** | 2.89 | 5.66 |
| Sex (ref=Male) | |||
| Female | 0.40*** | 0.31 | 0.51 |
| Race (ref=White) | |||
| Black | 0.71* | 0.52 | 0.97 |
| Other | 0.66 | 0.37 | 1.19 |
| Visit Type (ref = Inpatient hospitalization) | |||
| Emergency Department | 2.92*** | 1.85 | 4.60 |
| SUD Bed Days (ref = ≤7 days) | |||
| 8 −14 days | 0.35** | 0.17 | 0.73 |
| ≥ 15 days | 1.87 | 0.97 | 3.60 |
p < .001.
p < .01.
p < .05.
Mental health treatment.
Compared to the pre-deployment time period (2000–2002), no significant change in use of mental health treatment by military school-aged children (5–11) and adolescents (12–17) occurred during the first (2003–2008; OR=0.83, 95% CI: 0.56–1.22) or second (2009–2014; OR=0.98, 95% CI: 0.66–1.45) post-deployment periods in civilian acute care facilities. However, receiving mental health treatment differed by age, sex, race, bed-days and visit type over deployment-related time periods. Trends are plotted in Figure 3. Younger adolescents (12–14 years) were 87% less likely (OR=0.13, 95% CI: 0.05–0.38) and older adolescents (15–17 years) were 2% less likely (OR=0.98, 95% CI: 0.66–1.45) to receive mental health treatment compared to school-aged children (5–11 years). During the Afghanistan and Iraq wars, military adolescents consistently received mental health treatment less often than school-aged children (see Figure 3a). Girls had 2.45 greater odds (OR=2.45, 95% CI: 1.92–3.12) of receiving mental health treatment compared to boys, and consistently received mental health treatment more often than boys over time (see Figure 3b). Black children were 36% more likely (OR=1.36, 95% CI: 1.01–1.84) to receive mental health treatment than White children. Between the first and second post-deployment period, racial/ethnic minority children were consistently more likely to receive mental health treatment compared to White children (see Figure 3c). School-aged children and adolescents had almost triple the odds of being hospitalized (OR=2.93, 95% CI: 1.86–4.61) for mental health treatment than being treated in EDs. Compared to hospital stays for ≤ 7 days, mental health hospitalizations had 2.88 greater odds (OR=2.88, 95% CI: 1.37–6.05) of being for 8–14 days (see Figure 3d). During the Afghanistan and Iraq wars, mental health hospitalizations for both school-aged children and adolescents was consistently more likely to be for 8–14 days than for ≤ 7 days (see Figure 3e).
Figure 3:
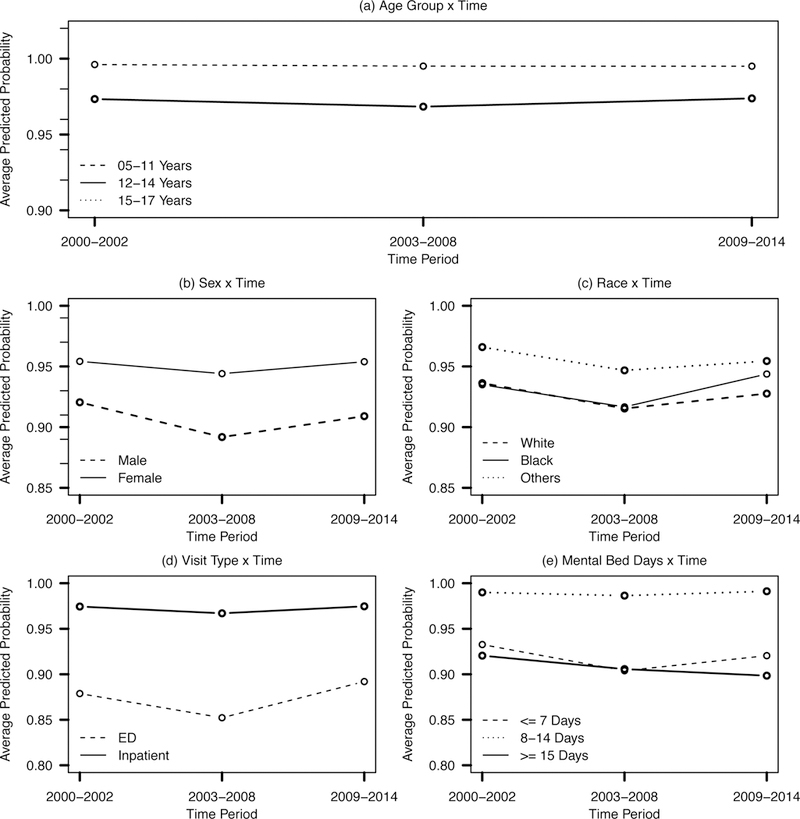
Trends in probability of mental health treatment by school-aged children and adolescent Military Health System beneficiaries, based on deployment-related time periods from 2000–2014, by demographic characteristics, estimated from mixed effects model.
Substance use treatment.
Compared to the pre-deployment time period (2000–2002), no significant change in use of SUT by military adolescents (12–17 years) occurred during the first (2003–2008; OR=1.18, 95% CI: 0.80–1.75) or second (2009–2014; OR=1.01, 95% CI: 0.68–1.49) post-deployment periods in civilian acute care facilities. However, receiving SUT differed by age, sex, race, bed-days and visit type over deployment-related time periods. Trends are plotted in Figure 4. Older adolescents (15–17 years) had more than four times the odds (OR=4.05, 95% CI: 2.89–5.66) of receiving SUT compared to younger adolescents (12–14 years) and were consistently more likely to received SUT over time (see Figure 4a). Girls had 60% lower odds of receiving SUT (OR=0.40, 95% CI: 0.32–0.51) than boys, who consistently received SUT more often than girls during deployment-related time periods (see Figure 3b). Racial/ethnic minority children were consistently less likely to receive SUT than White children (see Figure 4c). Black adolescents were 29% less likely (OR=0.71, 95% CI: 0.52–0.97) to receive SUT than White adolescents during the Afghanistan and Iraq wars. Military adolescents had almost three times greater odds (OR=2.92, 95% CI: 1.85–4.60) of being seen in the ED for SUDs than being hospitalized (see Figure 4d). Compared to hospital stays for ≤ 7 days, SUD hospitalizations were 65% less likely (OR=0.35, 95% CI: 0.17–0.73) to be for 8–14 days (see Figure 4e).
Figure 4:
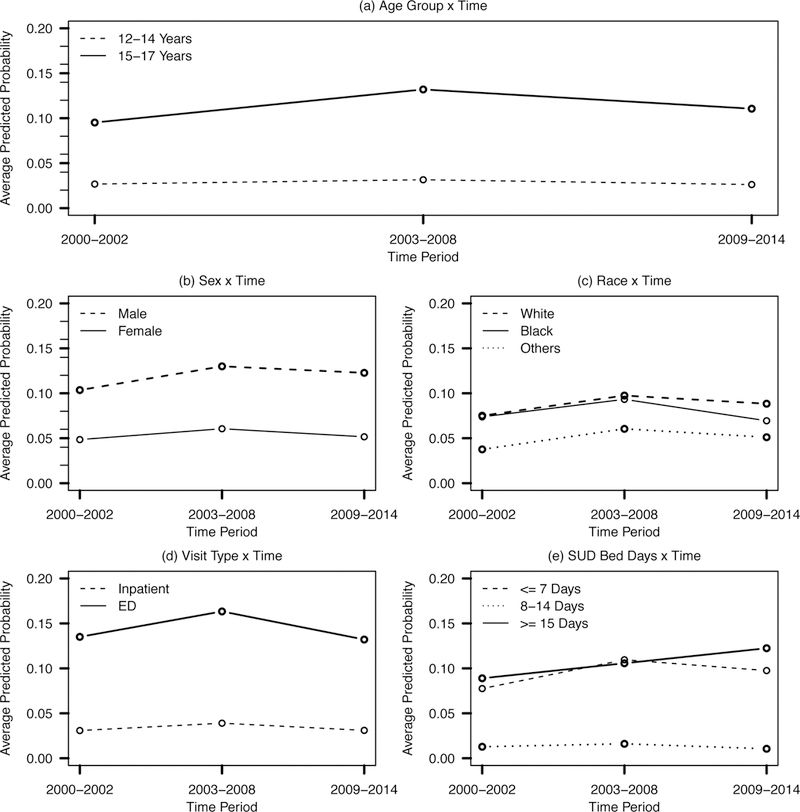
Trends in probability of substance use treatment by adolescent Military Health System beneficiaries, based on deployment-related time periods from 2000–2014, by demographic characteristics, estimated from mixed effects model
Discussion
This study examined trends in behavioral health treatment among military children in civilian acute care facilities and identified behavioral health conditions for which military children were most frequently treated during the Afghanistan and Iraq wars. Although no significant change in purchased behavioral health care changed over deployment-related time periods, ED visits increased by 20% for mental health disorders and more than quadrupled for SUDs from pre-deployment to the second post-deployment period. Mental health conditions were most frequently treated during inpatient hospitalizations (56.4%), whereas a large majority (78.8%) of SUT occurred in the ED. During the Afghanistan and Iraq wars, military adolescents received the majority of behavioral health treatment for AUD, mood and bipolar disorders, nondependent mixed/unspecified drug and non-dependent cannabis abuse. Older adolescents (15–17 years) had more than four times greater odds of receiving SUT than younger adolescents (12–14 years). Girls and Blacks were more likely to receive mental health treatment compared to boys and Whites, respectively. These findings build upon and extend prior research on behavioral health treatment for military children, have implications for the provision of behavioral health treatment for military children in the purchased care component of the MHS, and targeted behavioral health promotion and prevention of behavioral health crises among military school-aged children and adolescents.
Afghanistan and Iraq wars were ongoing for 13 years of the 15-year study period examined in this study. Thus, it is important to note that most military children in this study have only known a life of individual and family stressors associated with the high military operations tempo that includes war, domestic terrorism, mass shootings, and parental deployments. From 2003–2014, 2,562 military children received 4,607 behavioral health visits. School-aged children’s mental health visits increased from 61 to 246 from pre-deployment to the second post-deployment period and were more likely to be inpatient hospitalizations. Adolescents received an overwhelming majority of care (81.7%) and were more likely to receive ED services for substance use problems. During the first post-deployment period, the Iraq invasion (2003) and Iraq troop surge (2007) occurred, which increased troops on the ground to 149,000 and 165,000, respectively.29 This is a period when military children may have been directly and indirectly exposed to preparations for parental deployments, prolonged parental separations, and changing family dynamics, which may account for the increase in mental health visits for school-aged children and ED visits for adolescents. During the second post-deployment period, the Iraq drawdown to 141,000 troops and the Afghanistan surge to 100,000 troops occurred,29 which may have exposed military children to multiple, lengthy deployments, short dwell times (i.e., time between deployments), multiple family readjustments, and physical and psychological injuries (e.g., traumatic brain injury, PTSD, amputations) resulting in significant physical and psychological changes in military parents, marital discord, and possibly financial difficulties. Throughout OEF/OIF, military children were exposed to military funerals and 24-hour mainstream and social media war coverage. All these military and wartime stressors may have increased social and emotional difficulties among military children that resulted in behavioral health crises and need for behavioral health treatment in acute care facilities. Given the patriotism and collectivism of military culture, military children whose parents did not deploy may have experienced emotional distress because their friends’ parents and neighbors may have deployed and thus, they feared the deployment or even death of their parents or other family members in the military. Gilreath and colleagues10 found that military adolescents with a sibling in the military reported high levels of lifetime substance use (i.e., alcohol, prescription drugs, tobacco, marijuana, other drugs) ranging from 45.8% to 17.3%. The findings build upon current evidence regarding behavioral health problems and need for behavioral health treatment by military children who were directly and indirectly affected by the current wars.
Adolescents received an overwhelming majority of behavioral health treatment during the Afghanistan and Iraq wars. Specifically, adolescents received 80.4% of mental health and 97.3% of SUD visits. SUT for adolescents increased almost 5-fold from pre-deployment (2000–2002) to the first post-deployment period (2003–2008), and ED visits more than quadrupled over 12 years of war. Adolescence is a developmental stage involving physical, social, and interpersonal transformations as well as expressions of independence.32 Current evidence suggests that military adolescents are at increased risk for developing maladaptive coping mechanisms, such as social withdrawal and substance use in response to psychological and physiological stressors of developmental transitions and additional social and familial obligations related to a parental deployment.10,33–36 Thus, high levels of behavioral health treatment by military adolescents may have resulted from difficult adaptations to parental deployments coupled with normative stressors related to developmental milestones and the middle-to-high school transition. For military adolescents, stress during a parental deployment may be exacerbated by the redefining of family roles and responsibilities, as well as concerns about the safety of the deployed parent.36,37 Older adolescents (15–17 years) may be acutely aware of family deployment stressors and may assume more family and caregiver responsibilities, which may result in substance use and in part account for increased use of SUT compared to younger adolescents (12–14 years). Barnes, Davis, and Treiber38 found higher heart rate, blood pressure, and perceived stress among military adolescents with a family member deployed compared to military adolescents with no family member deployed and civilian adolescents, suggesting adolescents also have psychophysiological reactions to family member deployments.
Adolescents received SUT most frequently for AUD, nondependent mixed/unspecified drug and non-dependent cannabis abuse in the ED. In the 2015 National Survey on Drug Use and Health (NSDUH)39 data from South Carolina, approximately 60% of adolescents perceived no risk in binge drinking 1–2 times weekly and 76.5% perceived no risk in smoking marijuana monthly.39 NSDUH data also indicated that underage drinkers are more likely than drinkers aged 21 or older to use illicit drugs within two hours of alcohol use.40 High rates of lifetime and past 30-day alcohol (41.1% and 21%, respectively) and marijuana (26.6% and 14.2%, respectively) use were also reported by military adolescents in California10 and in this study, a significant proportion of military adolescents in South Carolina were treated for AUD (37.9%), mixed/unspecified drug abuse (21.7%), and non-dependent cannabis abuse (14.8%). The high rate of ED visits for SUT (78.8%) among military adolescents in this study is the same rate as ED visits for alcohol misuse among underage drinkers (aged 12–20) in Nationwide Emergency Department Sample data.41 These findings underscore the need for screening, brief intervention, and referral to outpatient SUT to assist in the early identification of substance use problems in military adolescents.
Both school-aged children and adolescents were most frequently treated for mood, bipolar, adjustment, and anxiety disorders. Primary diagnoses for which military children received behavioral health treatment in South Carolina are consistent with commonly reported behavioral health problems in military school-aged children and adolescents in prior research.7–10 In California, 22.9% of military adolescents self-reported depressive symptoms;9 and in this study 19.1% of adolescents were treated for mood disorders. Similar to this study, pediatric medical records also identified mood, adjustment, and anxiety disorders as commonly treated disorders among military children.7,42 Although similarities were found in primary diagnoses associated with behavioral health treatment by military school-aged children and adolescents, prior research suggests developmental differences in social and emotional responses of school-aged children to a parental deployment compared to adolescents. Military school-aged children may exhibit more internalizing behaviors such as emotional dysregulation and academic difficulties whereas adolescents may engage in more externalizing behaviors such as anger, defiance, and substance use.33 Thus, high rates of SUT among adolescents may be an artifact of their tendency to engage in more externalizing behaviors than school-aged children. Developmental differences in stress responses underscore the need for developmentally-appropriate prevention and intervention strategies for military school-aged children and adolescents.
No significant changes found in behavioral health treatment during the Afghanistan and Iraq wars may in part be an artifact of the military force structure in South Carolina. Although South Carolina has large military and veteran populations representing all branches of military service,43 between 2004–2009, 14 Army installations accounted for 80% of OEF/OIF deployments by active duty Soldiers44 and none of them were in South Carolina,a which has two large military installations providing basic combat training to the majority of new recruits in the U. S. Army and U. S. Marine Corps. During the Afghanistan and Iraq wars, the Army had the largest number of service members returning with physical and psychological injuries45 and thus, these 14 Army installations may also have had the largest number of military children receiving behavioral health treatment. Future research in national trends in behavioral health treatment utilization by military children are needed to better understand patterns of use from pre-deployment to post-deployment.
Noteworthy strengths of this study include the use of objective longitudinal medical claims data examining 15-year trends in behavioral health treatment by military children in a state with large military and veteran populations. These data included all emergency department and inpatient hospitalization claims for child MHS beneficiaries who received behavioral health treatment that was paid for through the purchased care component of the MHS. However, behavioral health treatment by military children may be underestimated because outpatient visits in pediatrician offices of civilian providers were not available in these data. These clinical data also included only demographic characteristics, medical diagnoses, and procedure codes. Future research should examine individual, family, and school factors associated with behavioral health treatment by military children. Small sample sizes in the mixed effect models may have resulted in limited statistical power to detect a significant difference in behavioral health treatment over time.
Implications for Behavioral Health
Children and adolescents spend a significant portion of their time in school settings, which gives school staff a critical role in identifying and addressing behavioral health concerns that may arise with military-connected students. Most military children attend civilian schools;46 however, school staff are often ill-prepared to respond to their military and deployment-related stressors.34,35 Cederbaum and colleagues9 suggest that school personnel be better trained to screen for and identify military-connected student’s mental health problems, and that schools develop clear guidelines on mental health referral procedures. School behavioral health (SBH) programs can also provide prevention and intervention training that can better prepare school staff and military parents to address behavioral health crises among military children.47 Faran and colleagues47 describe a comprehensive SBH program, the Child and Family Behavioral Health System of the U. S. Army, that embeds behavioral health specialists in schools, which gives school staff, military parents and students greater access to behavioral health services. Findings from the current study suggest a greater need for the integration of SBH programs in schools to potentially prevent behavioral health crises among school-aged children and adolescents, and subsequently their need for acute behavioral health services. Family and caregiver stress related to parental deployment has been associated with behavioral health problems in both military school-aged children and adolescents.15 Family-centered interventions, such as Families OverComing Under Stress (FOCUS),48 was found effective in reducing emotional and behavioral problems and increasing prosocial behaviors in military youth ages 3–17, and such programs can potentially increase peer and social networks, reduce family and caregiver stress, and normalize help-seeking behaviors among military children and families. A systematic review of behavioral health interventions for military youth found positive treatment outcomes, but noteworthy methodological limitations in their evaluations.49 Future research evaluating the effectiveness of behavioral health interventions for military youth should employ more rigorous research methods to improve the quality of evidence on behavioral health treatment outcomes among military youth.
Given that most military children attend civilian schools and receive care from non-military pediatricians,8,14,46 study findings also have implications for behavioral health treatment within the purchased care component of the MHS. Integrated and enhanced referral behavioral health models in primary care have been effective in reducing risky drinking in older adults and veterans.50,51 Integrated behavioral health in pediatric clinics and school-based behavioral health interventions may facilitate early identification and referral to treatment of military children with mental health problems, which may reduce the need for inpatient hospitalizations. Given marijuana is the primary substance abused by civilian adolescents receiving outpatient SUT,40 referral of military adolescents to outpatient SUT from the ED may potentially prevent future behavioral health crises and costly ED visits for alcohol misuse and non-dependent cannabis abuse. Developmentally-appropriate substance abuse prevention programs targeting military adolescents could also prevent the need for ED services for substance use problems. As military operations continue in Afghanistan, Iraq and other parts of the world, it is critical to increase military children’s access to preventive interventions promoting screening, brief intervention, and referral to outpatient treatment for behavioral health conditions.
Supplementary Material
Acknowledgements:
This study was funded by the National Institute on Drug Abuse (NIDA #K01DA037412, PI: Nikki R. Wooten, PhD). Data are from the records of the South Carolina Revenue and Fiscal Affairs Office (SC RFA), Health and Demographics, whose authorization to release these data does not imply endorsement of this study or its findings by either the Division of Research and Statistics or the Data Oversight Council. The authors acknowledge programming assistance from Mr. Chris Finney, SC RFA, Health and Demographics Division, in creating the data extract used in this study and research assistance from Tamara L. Grimm, MSW.
Footnotes
Presentation Information: This study was presented as an oral presentation at the annual meeting of the Society for Social Work and Research, New Orleans, LA, January 14–17, 2017.
Fort Benning, Fort Bliss, Fort Bragg, Fort Campbell, Fort Carson, Fort Hood, Fort Irwin, Fort Knox, Fort Lewis, Fort Polk, Fort Riley, Fort Shaer, Fort Stewart, Fort Wainwright
Conflict of Interest Statement: Dr. Wooten is a lieutenant colonel in the U. S. Army Reserves and Mr. Moore is a lieutenant junior grade in the U. S. Naval Reserves, but neither conducted this study as a part of their official military duties. All other authors report no conflicts of interest. The opinions and assertions herein are those of the authors and do not necessarily reflect the official views of the Department of Defense, NIDA, or the National Institutes of Health.
Contributor Information
Nikki R. Wooten, University of South Carolina, College of Social Work.
Jordan A. Brittingham, University of South Carolina, Arnold School of Public Health.
Nahid S. Sumi, University of South Carolina, Arnold School of Public Health.
Ronald O. Pitner, University of South Carolina, College of Social Work.
Kendall D. Moore, University of South Carolina, Department of Psychology.
References
- 1.U. S. Department of Defense. Report on the impact of deployment of members of the Armed Forces on their dependent children Washington, DC: Author; 2010. [Google Scholar]
- 2.Sogomonyan F, Cooper J. Trauma faced by children in military families: What every policymaker should know New York, NY: Columbia University;2010. [Google Scholar]
- 3.De Pedro KMT, Astor RA, Benbenishty R, et al. The children of military service members. Review of Educational Research 2011;81(4):566–618. [Google Scholar]
- 4.Gorman GH, Eide M, Hisle-Gorman E. Wartime military deployment and increased pediatric mental and behavioral health complaints. Pediatrics 2010:1058–1066. [DOI] [PubMed] [Google Scholar]
- 5.White CJ, de Burgh HT, Fear NT, et al. The impact of deployment to Iraq or Afghanistan on military children: A review of the literature. International Review of Psychiatry 2011;23(2):210–217. [DOI] [PubMed] [Google Scholar]
- 6.Sullivan K, Capp G, Gilreath T, et al. Substance abuse and other adverse outcomes for military-connected youth in California: Results from a large-scale normative population survey. JAMA Pediatrics 2015;169(10):922–928. [DOI] [PubMed] [Google Scholar]
- 7.Gorman GH, Eide M, Hisle-Gorman E. Wartime military deployment and increased pediatric mental and behavioral health complaints. Pediatrics 2010;126(6):1058–1066. [DOI] [PubMed] [Google Scholar]
- 8.Flake EM, Davis BE, Johnson PL, et al. The psychosocial effects of deployment on military children. Journal of Developmental & Behavioral Pediatrics 2009;30(4):271–278 [DOI] [PubMed] [Google Scholar]
- 9.Cederbaum JA, Gilreath TD, Benbenishty R, et al. Well-being and suicidal ideation of secondary school students from military families. Journal of Adolescent Health 2014;54(6):672–677. [DOI] [PubMed] [Google Scholar]
- 10.Gilreath TD, Cederbaum JA, Astor RA, et al. Substance use among military-connected youth: The California healthy kids survey. American Journal of Preventive Medicine 2013;44(2):150–153. [DOI] [PubMed] [Google Scholar]
- 11.Chartrand MM, Frank DA, White LF, et al. Effect of parents’ wartime deployment on the behavior of young children in military families. Archives of Pediatric & Adolescent Medicine 2008;162(11):1009–1014. [DOI] [PubMed] [Google Scholar]
- 12.Kelley ML. The effects of military-induced separation on family factors and child behavior. American journal of Orthopsychiatry 1994;64(1):103–111. [DOI] [PubMed] [Google Scholar]
- 13.Aranda MC, Middleton LS, Flake E, et al. Psychosocial screening in children with wartime-deployed parents. Military Medicine 2011;176(4):402–407. [DOI] [PubMed] [Google Scholar]
- 14.Astor R, De Pedro K, Gilreath T, et al. The promotional role of school and community contexts for military students. Clinical Child Family Psychological Review 2013;16(3):233–244. [DOI] [PubMed] [Google Scholar]
- 15.Flake EM, Davis BE, Johnson PL, et al. The psychosocial effects of deployment on military children. Journal of Developmental & Behavioral Pediatrics 2009;30(4):271–278. [DOI] [PubMed] [Google Scholar]
- 16.Gilreath TD, Astor RA, Cederbaum JA, et al. Prevalence and correlates of victimization and weapon carrying among military-and nonmilitary-connected youth in Southern California. Preventive medicine 2014;60:21–26. [DOI] [PubMed] [Google Scholar]
- 17.Reed SC, Bell JF, Edwards TC. Weapon carrying, physical fighting and gang membership among youth in Washington state military families. Maternal and Child Health Journal 2014. [DOI] [PubMed] [Google Scholar]
- 18.Chandra A, Martin LT, Hawkins SA, et al. The impact of parental deployment on child social and emotional functioning: Perspectives of school staff. Journal of Adolescent Health 2010;46(3):218–223. [DOI] [PubMed] [Google Scholar]
- 19.Mansfield AJ, Kaufman JS, Marshall SW, et al. Deployment and the use of mental health services among U.S. Army wives. New England Journal of Medicine 2010;362(2):101–109. [DOI] [PubMed] [Google Scholar]
- 20.Larson M, Mohr BA, Lorenz L, et al. General and specialist health care utilization in military children of Army service members who are deployed. In: MacDermid Wadsworth S, Riggs DS, eds. Military deployment and its consequences for families New York, NY: Springer; 2014:87–110. [Google Scholar]
- 21.Larson M, Mohr BA, Adams RS, et al. Association of military deployment of a parent or spouse and changes in dependent use of health care services. Medical Care 2012;50:821–828. [DOI] [PubMed] [Google Scholar]
- 22.Eide M, Gorman G, Hisle-Gorman E. Effects of parental military deployment on pediatric outpatient and well-child visit rates. Pediatrics 2010;126(1):22. [DOI] [PubMed] [Google Scholar]
- 23.Hisle-Gorman E, Eide M, Coll EJ, et al. Attention deficit hyperactivity disorder and medication use by children during parental military deployments. Military Medicine 2014;179(5):573–578. [DOI] [PubMed] [Google Scholar]
- 24.U. S. Department of Defense; Military health system review Washington, DC: Author; 2014. [Google Scholar]
- 25.Wooten NR, Brittingham JA, Pitner RO, et al. Purchased behavioral health care received by military health system beneficiaries in civilian medical facilities, 2000–2014. Military Medicine 2018;183(7–8):e278–e290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Defense Health Agency; Evaluation of the TRICARE program: Access, cost, and quality (Fiscal Year 2015 report to Congress) Washington, DC: 2015. [Google Scholar]
- 27.South Carolina Education Oversight Committee; Educational performance of military-connected children Columbia, SC: Author; 2015. [Google Scholar]
- 28.Torreon BUS periods of war and dates of recent conflicts Washington, DC: Congressional Research Service; 2015. [Google Scholar]
- 29.Belasco A The cost of Iraq, Afghanistan, and other Global War on Terror Operations since 9/11 Washington, DC: Congresional Research Service; 2014. [Google Scholar]
- 30.Armed Forces Health Surveillance Center [AFHSC]. AFHSC surveillance case definitions Silver Spring, MD: Armed Forces Health Surveillance Branch; 2012. [Google Scholar]
- 31.Bates D, Mächler M, Bolker B, et al. Fitting linear mixed-effects models using lme4 arXiv preprint arXiv:14065823 2014. [Google Scholar]
- 32.Seiffge-Krenke I Stress, coping, and relationships in adolescence. Psychology Press; 2013. [Google Scholar]
- 33.Lincoln A, Swift E, Shorteno-Fraser M. Psychological adjustment and treatment of children and families with parents deployed in military combat. Journal of Clinical Psychology 2008;64(8):984–992. [DOI] [PubMed] [Google Scholar]
- 34.Mmari KN, Roche KM, Sudhinaraset M, et al. When a parent goes off to war: Exploring the issues faced by adolescents and their families. Youth & Society 2008;40(4):455–475. [Google Scholar]
- 35.Mmari K, Bradshaw C, Sudhinaraset M, et al. Exploring the role of social connectedness among military youth: Perceptions from youth, parents, and school personnel. Child and Youth Care Forum 2010;39(5):351–366. [Google Scholar]
- 36.Huebner AJ, Mancini JA. Adjustments among adolescents in military families when a parent is deployed: A final report submitted to the Military Family Research Institute and the Department of Defense Quality of Life Office. Falls Church, VA: Virginia Tech, Department of Human Development;2005. [Google Scholar]
- 37.Bradshaw CP, Sudhinaraset M, Mmari K, et al. School transitions among military adolescents: A qualitative study of stress and coping. School Psychology Review 2010;39(1):84. [Google Scholar]
- 38.Barnes VA, Davis H, Treiber FA. Perceived stress, heart rate, and blood pressure among adolescents with family members deployed in Operation Iraqi Freedom. Military Medicine 2007;172(1):40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Substance Abuse and Mental Health Services Administration [SAMHSA]. Behavioral health barometer: South Carolina, 2015 Rockville, MD: SAMHSA; 2015. [Google Scholar]
- 40.Substance Abuse and Mental Health Services Administration. Behavioral health barometer: United States, 2015 Rockville, MD: SAMHSA;2015. [PubMed] [Google Scholar]
- 41.Naeger S Emergency department visits involving underage alcohol use: 2010 to 2013. Rockville, MD: Health Statistics and Quality, Substance Abuse and Mental Health Services Administration;2016. [PubMed] [Google Scholar]
- 42.Davis BE. Parental wartime deployment and the use of mental health services among young military children. Pediatrics 2010:peds. 2010-2543. [DOI] [PubMed] [Google Scholar]
- 43.National Center for Veterans Analysis and Statistics; 2015 Profile of unique veteran users 2016. Available at https://www.va.gov/vetdata/; accessed March 15, 2016. [Google Scholar]
- 44.Resnick A, Jacobson M, Kadiyala S, et al. How deployments affect the capacity and utilization of Army treatment facilities Santa Monica, CA: 2014. [PMC free article] [PubMed] [Google Scholar]
- 45.U. S. Government Accountability Office. Army needs to improve oversight of Warrior Transition Units Washington, DC: GAO; 2016. [Google Scholar]
- 46.Capp G, Benbenishty R, Moore H, et al. Partners at learning: A service-learning approach to serving public school students from military families. Military Behavioral Health 2017:1–10. [Google Scholar]
- 47.Faran ME, Johnson PL, Ban P, et al. The evolution of a school behavioral health model in the US Army. Child and Adolescent Psychiatric Clinics of North America 2015;24(2):415–428. [DOI] [PubMed] [Google Scholar]
- 48.Lester P, Liang L- J, Milburn N, et al. Evaluation of a family-centered preventive intervention for military families: Parent and child longitudinal outcomes. Journal of the American Academy of Child & Adolescent Psychiatry 2016;55(1):14–24. [DOI] [PubMed] [Google Scholar]
- 49.Moore KD, Fairchild AJ, Wooten NR, et al. Evaluating behavioral health interventions for military-connected youth: A systematic review. Military Medicine 2017;182(11–12):e1836–e1845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Wooten N, Tavakoli AS, Al-Barwani MB, et al. Comparing behavioral health models for reducing risky drinking among older male veterans. The American Journal of Drug and Alcohol Abuse 2017;43(5):545–555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Krahn D, Bartels S, Coakley E, et al. PRISM-E: Comparison of integrated care and enhanced specialty referral models in depression outcomes. Psychiatric Services 2006;57(7):946–953. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.