
Fig. 1.
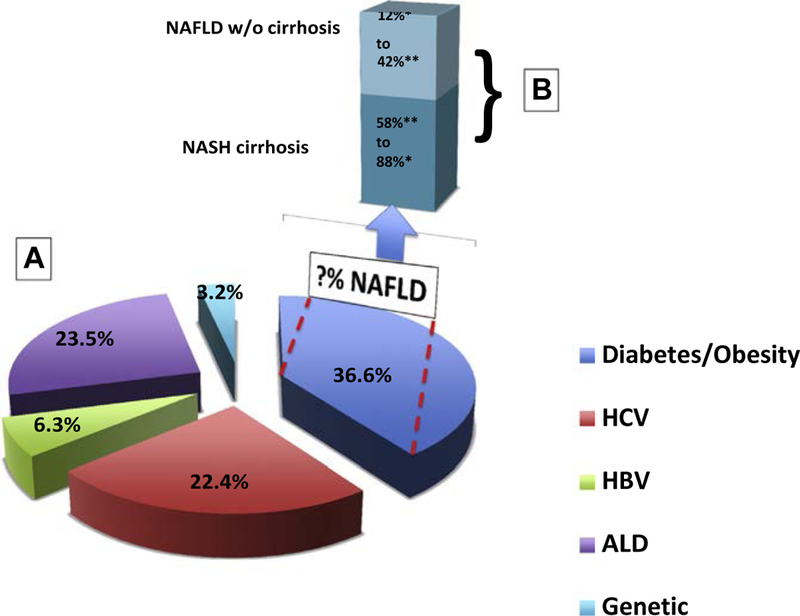
Risk factors for hepatocellular carcinoma (HCC) incidence in the United States. (A) Risk factors of HCC in the United States (presented as percentage). In a study by Welzel and colleagues of 6991 cases from the Surveillance, Epidemiology, and End Results (SEER)–Medicare databases from 1994 to 2007 the authors estimated the PAFs, that is, the proportions of cases that can be attributed to specific risk factors. The PAF owing to type 2 diabetes mellitus (T2DM) and/or obesity was the highest (36.6%), followed by alcohol-related disorders (23.5%), HCV (22.4%), HBV (6.3%), and rare genetic disorders (3.2%). Although the contribution of NAFLD is not exactly known, it is thought to contribute to the majority of the obesity and diabetes cases. (B) A breakdown of cases of HCC occurring in the setting of NAFLD in the presence or absence of cirrhosis to HCC. ALD, alcoholic liver disease; HBV, hepatitis B virus; HCV, hepatitis C virus; NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis. (Data from [A] Welzel TM, Graubard BI, Quraishi S, et al. Population-attributable fractions of risk factors for hepatocellular carcinoma in the United States. Am J Gastroenterol 2013;108(8):1314–21; [B] *Hashimoto E, Yatsuji S, Tobari M, et al. Hepatocellular carcinoma in patients with nonalcoholic steatohepatitis. J Gastroen-terol 2009;44 Suppl 19:89–95; and **Mittal S, Sada YH, El-Serag HB, et al. Temporal trends of non-alcoholic fatty liver disease-related hepatocellular carcinoma in the veteran affairs pop-ulation. Clin Gastroenterol Hepatol 2014;146(5):S–917.)