
Figure 1: hERG K+ channels: gating and physiology.
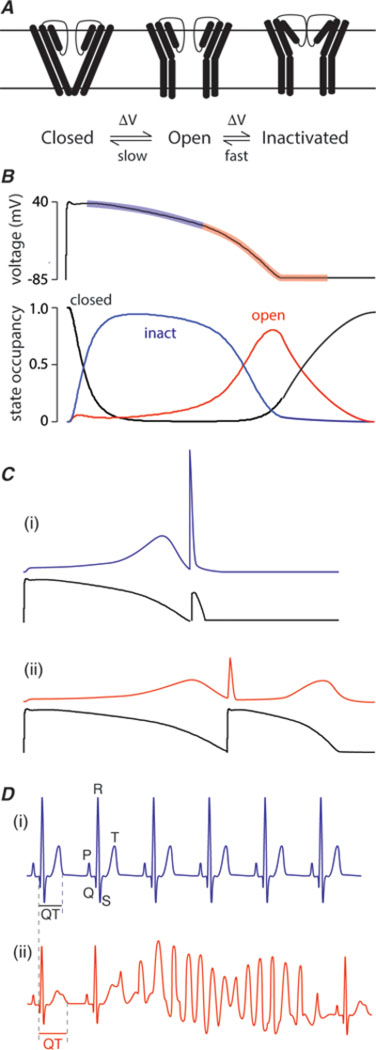
A. Simplified gating scheme for hERG K+ channels. Channels may exist in one of three main groups of states: closed states which are non-conducting, open states, which are conducting, or inactivated states, which are another non-conducting state that channels enter during a prolonged activating stimulus. The gating of hERG K+ channels is unusual in that (i) the kinetics of activation and deactivation are much slower than the kinetics of inactivation and recovery from inactivation. For example, at 0 mV, the time constant for activation is ~100 ms whereas the time constant for inactivation is ~2ms [47]. This is in marked contrast to the vast majority of voltage-gated ion channels where activation/deactivation are much more rapid than inactivation [48]. The second important feature of hERG K+ channel gating is that transitions between the open and inactivated states are voltage dependent.
B. As a consequence of their unusual gating kinetics, during the plateau phase of the cardiac myocyte action potential hERG K+ channels reside predominantly in the inactivated state (blue transparent region on action potential trace highlights the period when hERG K+ channels are predominantly inactivated). As the channels passing inward currents start to inactivate the membrane potential slowly starts to repolarize and this allows hERG K+ channels to recover from inactivation. The more the hERG K+ channels recover from inactivation the more outward current they pass and the more rapidly the membrane potential repolarizes (red transparent region on action potential trace). After the membrane potential has recovered to resting levels it still takes 200–300 ms for all the hERG K+ channels to return to the closed state.
C. (i) As a consequence of the slow deactivation of hERG K+ channels after the membrane potential has returned to the resting level, a premature stimulus (such as can occur with an ectopic beat) will result in a large “spike” of outward current through the still open hERG K+ channels, which then rapidly inactivate[26]. (ii) In patients with reduced hERG K+ channel activity, e.g. due to drug block, the reduced hERG K+ current results in a longer action potential as well as lower current response to premature beats [25].
D. (i) The surface electrocardiogram represents the summed activity of all the cells in the heart with the major deflections being the P-wave (represents atrial depolarization), QRS complex (represents ventricular depolarization) and the T-wave (represents ventricular repolarization). The duration of the interval from the start of the QRS complex to the end of the T-wave (QT interval) is usually ~400ms (at a heart rate of 60 beats per minute). (ii) Patients with reduced hERG K+ channel activity have prolonged QT intervals on their surface electrocardiogram and an increased risk of developing ventricular arrhythmias initiated by ectopic beats. In particular, they are prone to develop a particular arrhythmia called “torsades-de-pointes”.