
Fig. 4.
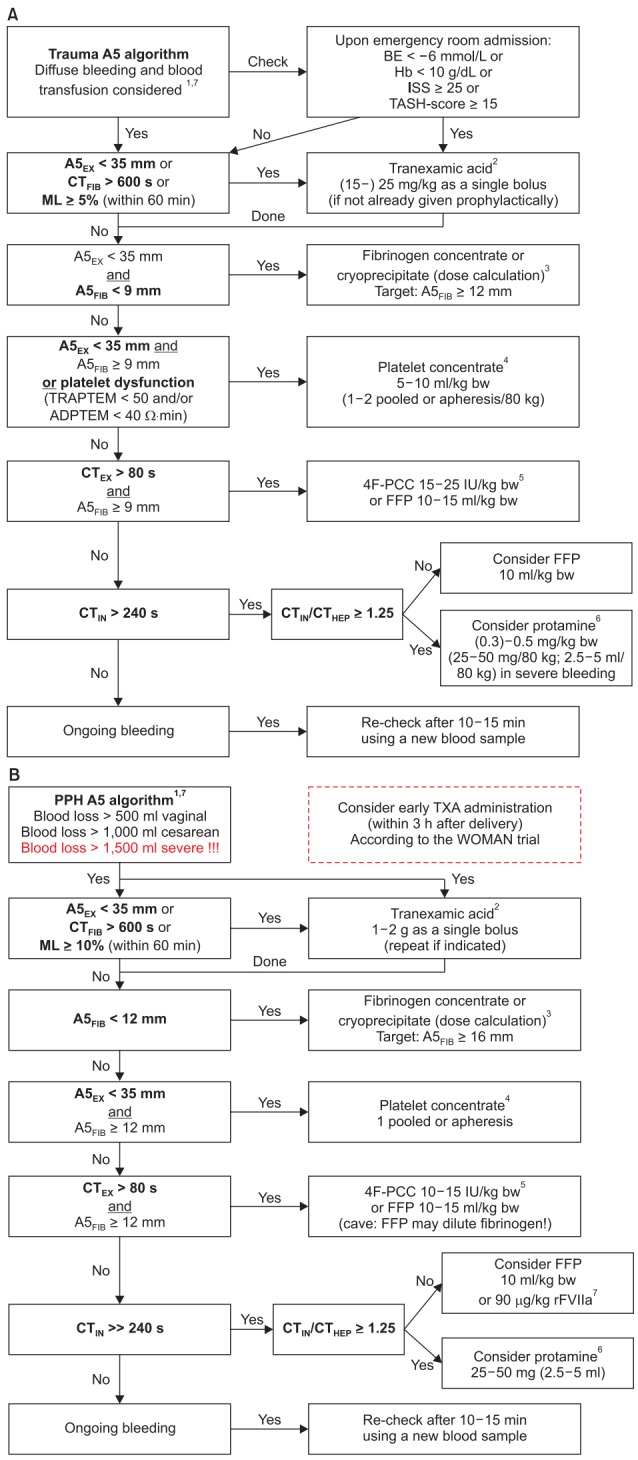
Evidence-based algorithms for ROTEM (A5)-guided bleeding management in (A) trauma/orthopedic surgery and (B) obstetrics/postpartum hemorrhage. Algorithm footnotes: 1Check basic conditions: Temp. > 35℃; pH > 7.3; Cai2+ > 1 mmol/L; Hb ≥ 7 g/dl. 2Antifibrinolytic therapy [105,142-146,153,157,195]: Prophylactic administration of TXA can be given within 3 h after trauma or delivery [142-144,195]. Continuous infusion of TXA can be performed in trauma [142-144]. CTFIB > 600 s represents a flat-line in FIBTEM. EACA can be used instead of TXA (based on local practice). 3Fibrinogen dose calculation (stepwise approach; see Table 2): Fibrinogen dose (g) = targeted increase in A5FIB (mm) × body weight (kg)/ 160. Correction factor (140–160 mm kg/g) depends on the actual plasma volume. 10 U Cryoprecipitate ≈ 2 g Fibrinogen concentrate. 4Platelet concentrate transfusion: Check platelet function with ROTEM platelet (ADPTEM and TRAPTEM) or Multiplate, if available [168-169]. Cave: Platelet transfusion might not improve platelet function in TIC [170]. Consider compensation by increased A5FIB ≥ 12 mm. Consider TXA (25 mg/kg) and/or desmopressin (DDAVP; 0.3 µg/kg) in patients with dual antiplatelet therapy and/or ADPTEM < 30 Ω∙min. Expected increase per pooled/apheresis PC per 80 kg: 8–10 mm in A5EX. A5EX 28–35 mm or ADPTEM < 40 Ω∙min: 1 pooled or apheresis platelet concentrate. A5EX 20–28 mm or (ADPTEM < 40 Ω∙min and TRAPTEM < 50 Ω∙min): 2 pooled or apheresis platelet concentrates. A5EX < 20 mm: 2 platelet concentrates + fibrinogen substitution (≥ 4 g). 5If 4-factor prothrombin-complex-concentrate (4F-PCC) is not available: 10–15 ml FFP /kg bw or 45–90 µg rFVIIa /kg bw (if patient is normothermic and pH > 7.3, and Cai2+ > 1 mmol/L, and A5EX ≥ 35 mm, and A5FIB ≥ 9 mm but FFP is not effective to decrease CTEX ≤ 80 s and CTHEP ≤ 240 s). Consider acquired hemophilia A in early severe bleeding, EXTEM and FIBTEM are normal but CTIN and CTHEP are significantly prolonged (see Fig. 6). Therapy: rFVIIa. 6Protamine: Endogenous HLE might occur in severe trauma and shock. Hemodynamic stabilization is the most important therapy. However, protamine administration might be considered in severe bleeding. 7Simultaneous interventions: Maximal three interventions at the same time (in first analysis and severe bleeding). Maximal two interventions at the same time (in second analysis and moderate to severe bleeding). Only one intervention at the same time (in second or later analysis and mild to moderate bleeding). ISS: injury severity score, TASH: trauma associated sever hemorrhage, A5EX: amplitude of clot firmness 5 min after coagulation time (CT) in EXTEM, CTFIB: CT in FIBTEM (CTFIB > 600 s reflects a flatline in FIBTEM), ML: maximum lysis (within 1 h run time), A5FIB: amplitude of clot firmness 5 min after CT in FIBTEM, bw: body weight, CTEX: CT in EXTEM, 4F-PCC: four factor prothrombin complex concentrate, IU: international units, FFP: fresh frozen plasma, CTIN: CT in INTEM, CTHEP: CT in HEPTEM, PPH: postpartum hemorrhage, TXA: tranexamic acid, rFVIIa: activated recombinant factor VII, Cai2+: ionized Calcium concentration, EACA: epsilon-aminocaproic acid, TIC: trauma-induced coagulopathy, HLE: heparin-like effect. Courtesy of Klaus Görlinger, Germany.