
Figure 6d.
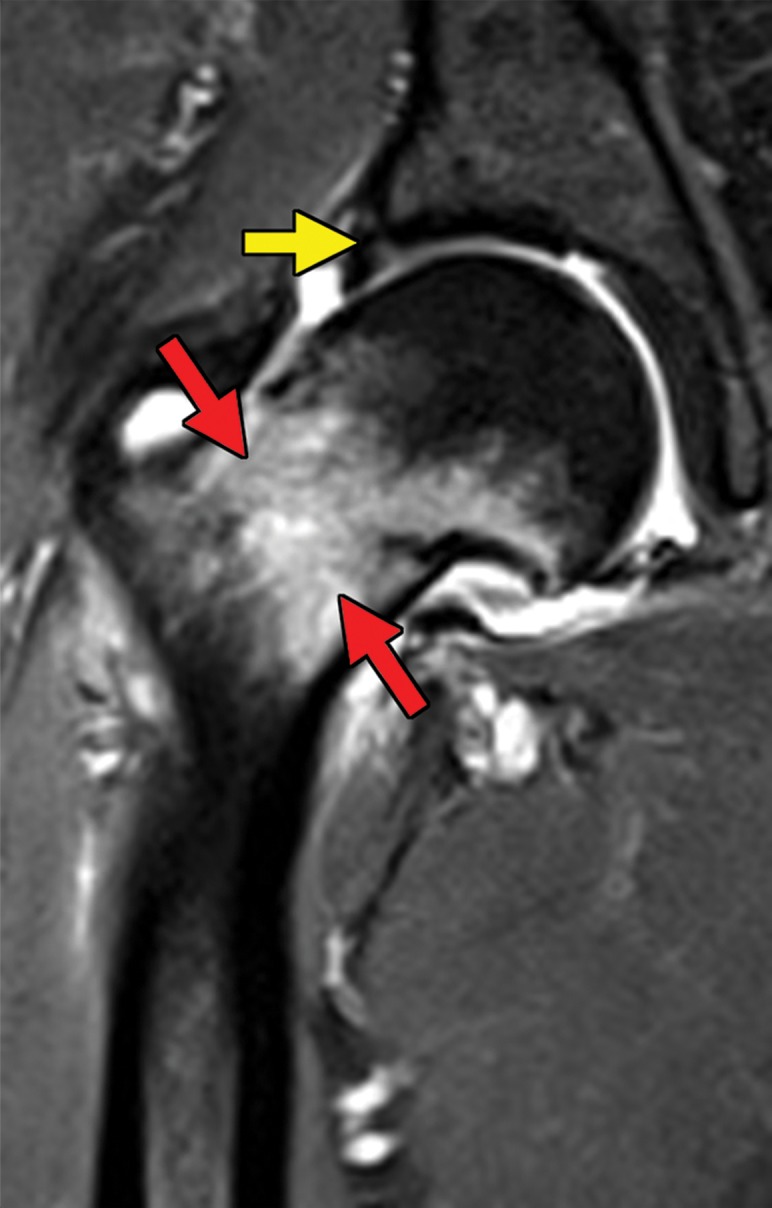
Metastatic RCC and hip pain in a 63-year-old man. (a) Radiograph of the right hip shows no abnormalities. (b) 99mTc methylene diphosphonate bone scintigram shows lesions in the right humerus and the clavicle (arrows) and the right hip (dashed square). (c) Detail image of the right hip corresponding to the dashed square in b shows abnormal uptake in the right femoral head (red arrow) and a small area of increased uptake in the acetabulum (yellow arrow). (d, e) Coronal fat-saturated T2-weighted fast spin-echo MR images at the level of the femoral head (d) and the ischial tuberosity (e) show marrow edema in the femoral neck (red arrows in d) corresponding to the abnormality on the bone scan due to an insufficiency fracture. Mild degenerative changes are noted in the right acetabulum (yellow arrow in d), corresponding to the focus of uptake in the right acetabulum in c, but there is no evidence of metastasis. A metastasis in the right ischium (red arrow in e) is clearly shown on the MR images but not detected on the bone scintigram (black arrow in c).