
Fig. 3.
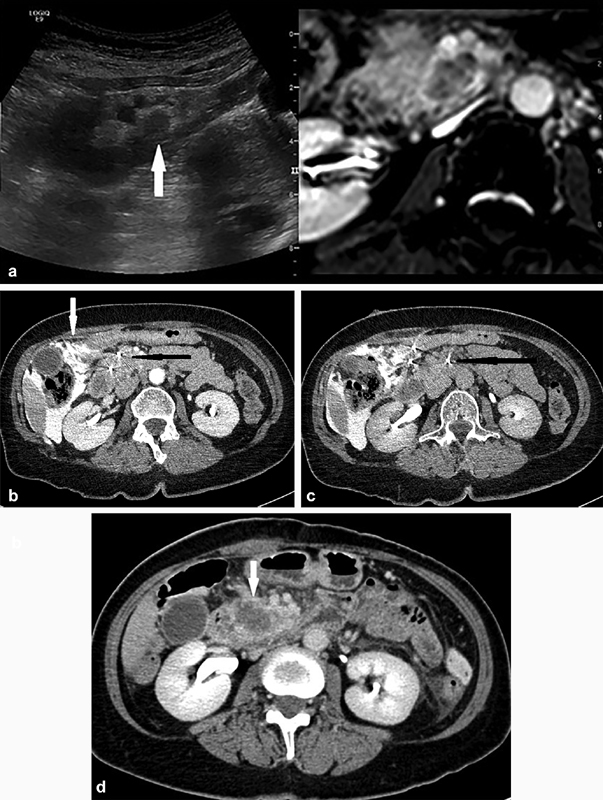
A 65-year old woman with neuroendocrine tumor in the pancreatic head and liver metastasis. The liver metastasis was successfully ablated using thermal ablation techniques with no evidence of short-term recurrence and improvement in symptoms. Decision for IRE was made at a multidisciplinary meeting for local disease control. ( a ) Ultrasound/MRI fusion image showing the hypoechoic lesion in the head of the pancreas (arrow), closely related to the superior mesenteric artery and vein anteriorly, as well as the inferior vena cava posteriorly. Probe placement under US/MRI fusion guidance in the caudal-cranial direction with position checked on CT. ( b ) CT image showing parallel needle placement (solid black arrow). Note the aggressive hydrodissection performed to create a safer window for placement of needles (white arrow). ( c ) To achieve adequate margins, a third probe was placed on the left of the superior mesenteric vessels, ∼2.0 cm away from the nearest ablation probe (black arrow). ( d ) Three-day postprocedure CT showing satisfactory ablation zone in the head of the pancreas (arrow) with no evidence of adjacent vessel injury.