

Abstract
Background
Foot orthoses have been shown to reduce the collapse of the longitudinal arch and to constrain soft tissue displacement under the heel. However, there has not been a study that has shown the effectiveness of both the arch and heel features in the same orthosis. This study quantitatively analyzed if the calcaneal pitch and the heel pad thickness will be affected by the use of an arch support and heel cup insole in a static weightbearing stance while wearing sports shoes.
Methods
Twenty-four (24) feet from 12 elite-level female soccer players with a mean age of 25 ± 3.99 years (20–33 years old) were studied. Lateral weightbearing radiographs with and without orthotics were obtained in order to measure the calcaneal pitch angle and heel fat pad thickness for each foot. A subjective outcome measure was used and the scores were classified as bad (0–2), fair (3–5), good (6–8), or excellent (9-10).
Results
The calcaneal pitch angle increased in all but three cases by an average of 1.05° (range, −1.14 to 3.19) after wearing orthotics (p < 0.01). The heel fat pad thickness increased in all cases with an average of 1.25 mm (range, 1.05 to 1.47; p < 0.01)). 9 of 12 subjects (75%) reported excellent (n = 2) or good (n = 7) overall subjective scores with insole wear.
Conclusion
Under static weightbearing conditions, the arch support and heel cup features of a foot orthosis help improve the height of the calcaneal pitch and the thickness of the heel fat pad, respectively.
Keywords: Foot orthoses, Arch support, Heel cup, Calcaneal pitch, Heel fat pad thickness
Introduction
Despite a lack of consensus, foot orthoses are widely used to treat various lower-limb problems,1,2 most notably symptomatic flat feet3,4 and plantar heel pain5,6. The arch and heel sections of a foot orthosis are the principal design features7 that allow it to alter loads between the plantar aspect of the foot and the orthotic surface.8,9 By applying an inversion moment at the rearfoot, an effective insole reduces calcaneal eversion as well as dorsiflexion of the joints forming the medial longitudinal arch.10 Authors have stressed the importance of correcting this malalignment dominated by protonation.11,12 The heel cup feature, on the other hand, provides more cushioning to the heel pad, further reducing the peak force at the instance of heel strike and even with just static standing.13
Orthoses have been shown to reduce foot protonation and thus the collapse of the longitudinal arch.14 It has also been shown that plantar heel fat pad thickness is increased when using a heel cup that constrains soft tissue displacement compared with no use of heel cup.13 However, there has not been a study that has shown the effectiveness of both the arch and heel features in the same orthosis.
The purpose of this study was to quantitatively analyze if the calcaneal pitch and the heel fat pad thickness will be affected by the use of an arch support and heel cup insole in a static weightbearing stance. It was hypothesized that such insoles will improve both the height of calcaneal pitch angle and thickness of the heel pad.
Materials and methods
This study was conducted from April to May 2018 at the Department of Sports Medicine, Kameda Medical Center. The study included 24 feet from 12 female football players competing in the top flight women's football association in Japan with a mean age of 25 ± 3.99 years (20–33 years old). Subjects were asked to wear sports shoes with and without Formthotics™ (Foot Science International, Christchurch, New Zealand) insoles (Fig. 1) while having lateral weight-bearing radiographs of their feet taken. The same sports medicine physician (H·O.) made and recorded all the radiographic measurements. Top players of the team and who had no known foot injuries or pathology were included in the study. Those with previous surgeries, injuries or known foot pathologies were excluded. Consent from the subjects and their team were obtained prior to inclusion in the study. This study was conducted with the formal approval of the human ethical committee of Kameda Medical Center No.19-054.
Fig. 1.

Formthotics™ (Foot Science International, Christchurch, New Zealand) insoles.
The radiographic parameter used to assess the effect of the arch support feature of the insole was the calcaneal pitch (Fig. 2), which was an angle formed by a line drawn extending from inferior portion of the calcaneocuboid joint to the inferior border of the calcaneus, a second line extending from the inferior aspect of the medial sesamoid bone to the inferior border.4,15 The difference in calcaneal pitch with and without the orthosis for each foot was then determined. To assess the heel cup feature of the insole, the heel fat pad thickness was measured on 2x magnification films, beginning from the lower vertex of the calcaneus (Fig. 3). The difference of the heel fat pad thickness while wearing sports shoes with the orthosis versus without orthosis while standing was then determined for each foot. Radiographic measurements were analyzed using the paired t-test.
Fig. 2.

Measurement of the calcaneal pitch.
Fig. 3.

Measurement of the heel fat pad thickness.
The subjective outcome of interest was an overall rating from a) foot slipping in the shoe, b) foot fatigue, c) perception of heel pain d)perception of ankle pain. Players were asked to rate all these parameters and give an overall score from a scale 0-2 bad, 3-5 fair, 6-8 good, 9-10 excellent.
Results
The calcaneal pitch angle increased in all but three feet when using sports shoes with the orthosis compared without the orthosis (Table 1). The mean increase with the orthosis was by 1.05° (range, 1.14 to 3.19; p < 0.01) (Fig. 4). The use of the orthosis also significantly increased heel fat pad thickness in all feet (Table 2) by an average of 1.25 mm (range, 1.05 to 1.47) compared when insole was not worn (p < 0.01) (Fig. 5). There overall subjective scores of players while wearing insole showed 9 of 12 subjects (75%) reporting excellent (n = 2) or good (n = 7) scores.
Table 1.
Calcaneal pitch angle difference.
| Calcaneal pitch angle (n = 24) | Foota | Without insole (degrees) | With insole (degrees) | Difference (degrees) |
|---|---|---|---|---|
| 1 | R | 13.17 | 13.01 | 0.16 |
| L | 22.03 | 22.62 | 0.59 | |
| 2 | R | 13.69 | 14.64 | 0.95 |
| L | 23.57 | 24.81 | 1.24 | |
| 3 | R | 20.36 | 19.22 | 1.14 |
| L | 15.81 | 17.16 | 1.35 | |
| 4 | R | 17 | 17.97 | 0.97 |
| L | 18.2 | 21.18 | 2.98 | |
| 5 | R | 19.36 | 18.98 | 0.38 |
| L | 20.24 | 20.71 | 0.47 | |
| 6 | R | 19.52 | 22.6 | 3.08 |
| L | 16.3 | 16.8 | 0.5 | |
| 7 | R | 10.58 | 12.74 | 2.16 |
| L | 21.01 | 22.11 | 1.1 | |
| 8 | R | 12.63 | 13.1 | 0.47 |
| L | 23.74 | 26.93 | 3.19 | |
| 9 | R | 19.4 | 19.84 | 0.44 |
| L | 15.04 | 16.27 | 1.23 | |
| 10 | R | 22.88 | 22.91 | 0.03 |
| L | 19.09 | 21.78 | 2.69 | |
| 11 | R | 18.81 | 18.92 | 0.11 |
| L | 17.73 | 19.75 | 2.02 | |
| 12 | R | 20.76 | 20.85 | 0.09 |
| L | 16.39 | 17.7 | 1.31 |
R – right foot; L – left foot.
Fig. 4.
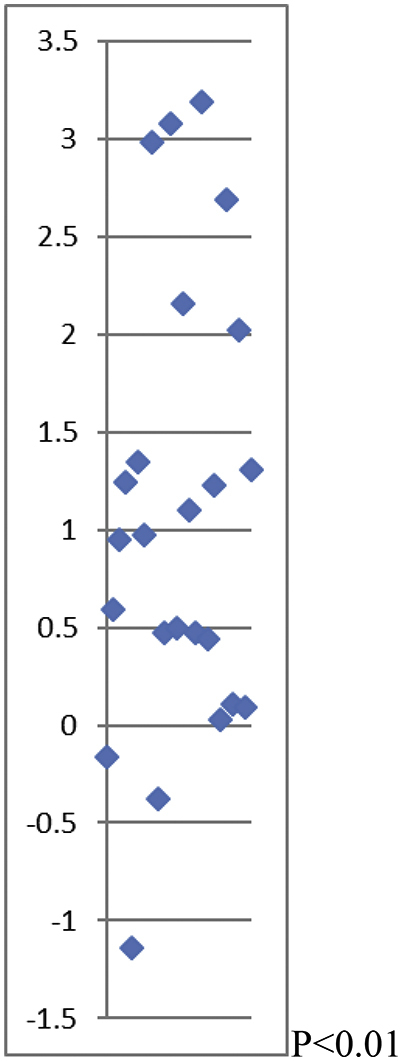
Calcaneal pitch angle difference (degrees).
Table 2.
Heel fat pad thickness (values from 2x magnification films).
| Heel fat pad thickness (n = 24) | Foota | Without insole (mm)** | With insole (mm)b | Difference |
|---|---|---|---|---|
| 1 | R | 21.37 | 29.36 | 7.99 |
| L | 22.71 | 26.7 | 3.99 | |
| 2 | R | 22.82 | 24.04 | 1.22 |
| L | 24.15 | 29.45 | 5.3 | |
| 3 | R | 23.09 | 29.15 | 6.06 |
| L | 24.04 | 28.13 | 4.09 | |
| 4 | R | 22.71 | 29.36 | 6.65 |
| L | 25.47 | 34.69 | 9.22 | |
| 5 | R | 25.37 | 34.77 | 9.4 |
| L | 17.38 | 24 | 6.62 | |
| 6 | R | 16.2 | 21.5 | 5.3 |
| L | 24.15 | 28.13 | 3.98 | |
| 7 | R | 24.04 | 28 | 3.96 |
| L | 24.04 | 30.7 | 6.66 | |
| 8 | R | 20.04 | 25.37 | 5.33 |
| L | 21.37 | 29.36 | 7.99 | |
| 9 | R | 24.02 | 27.02 | 3 |
| L | 25.37 | 29.36 | 3.99 | |
| 10 | R | 21.1 | 27.02 | 5.92 |
| L | 25.33 | 30.67 | 5.34 | |
| 11 | R | 24 | 29.3 | 5.3 |
| L | 18.7 | 24 | 5.3 | |
| 12 | R | 17.38 | 21.37 | 3.99 |
| L | 20.18 | 29.6 | 9.42 |
R – right foot; L – left foot
mm – millimeters.
Fig. 5.
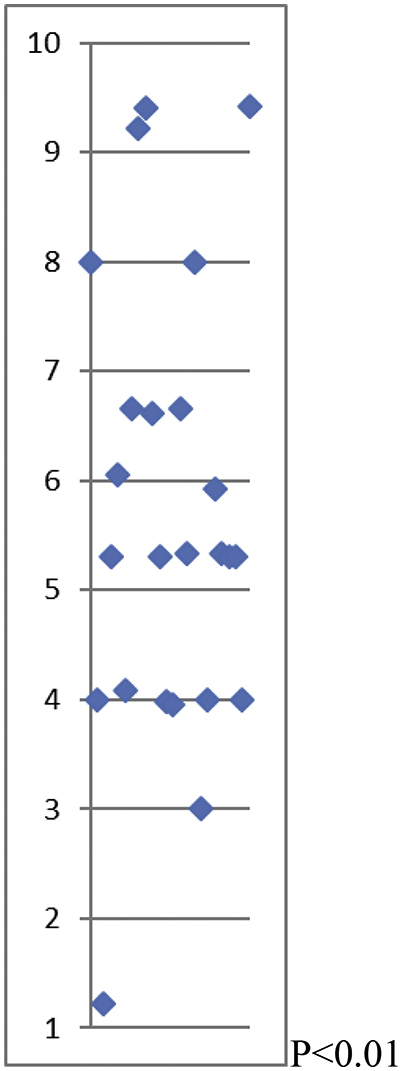
Heel fat pad thickness difference (mm) (values from 2x magnification films).
Discussion
This study has quantified the effects of a custom foot orthosis on static weightbearing based on measurements made on weightbearing lateral radiographs of the foot. As hypothesized, the use of sports shoes with this orthosis resulted in increased height of the longitudinal arch and thickness of the heel fat pad, as well as a subjective perception of pain relief.
The longitudinal arch of the foot, composed of medial and lateral parts, acts as a unit with the transverse arch, spreading the weight in all directions.6 The collapse of the medial longitudinal arch (MLA) leads to the clinical condition of flatfoot, which can be evaluated by indirect methods such as analyzing a footprint.15 However, direct methods such as radiographic parameters were defined as the gold standards by Saltzman and colleagues.16 Although there is still no consensus for MLA measurement in Orthopedics, there are suggested techniques such as the talo-horizontal angle, talo-first metatarsal angle (TFMA), and the calcaneal pitch.6,15 These radiographic parameters provide useful therapeutic guidance in clinical practice.17 Sensiba and colleagues found the calcaneal pitch to have the highest interobserver reliability among these parameters,18 prompting the authors to use it for the current study. The mean increase in calcaneal pitch by 1.05 suggests that the arch support feature of the insole is effective in restoring or improving the height of the MLA during static weightbearing.
Foot orthoses are also often applied for plantar heel pain5, with plantar fasciitis being the most common cause.19 As about 60% of the weight-bearing load is carried in the rear foot in static standing,13 the quality and thickness of the fat pad under the calcaneus are implicated as factors that influence the pressure under the heel.7,20 Therefore, the resulting increased heel fat pad thickness in all feet by an average of 1.25 mm is an indicator that the heel cup feature of the insole is effective in relieving pressure under the heel, which in turn can reduce or prevent plantar heel pain.
The current study has some limitations. First, it has a small sample size. A larger number of subjects will increase the power of the study and its conclusions. Second, the study only quantified the effects of the orthosis using static measurements, which may not reflect how the foot behaves dynamically. As such, it is desirable for further research to demonstrate the effects of the orthosis during dynamic movement, as well as to determine if the static measurements correlate with better performance during athletic activities.
Conclusion
Under static weightbearing conditions, the arch support and heel cup features of this orthosis help improve the height of the calcaneal pitch angle and the thickness of the heel pad, respectively.
Conflicts of interest
The authors declare that they have no conflicts of interest in this work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Footnotes
Supplementary data to this article can be found online at https://doi.org/10.1016/j.asmart.2019.07.001.
Appendix A. Supplementary data
The following is the Supplementary data to this article:
References
- 1.Sinclair J., Isherwood J., Taylor P.J. Effects of foot orthoses on Achilles tendon load in recreational runners. Clin Biomech. 2014;29(8):956–958. doi: 10.1016/j.clinbiomech.2014.07.004. [DOI] [PubMed] [Google Scholar]
- 2.Vtasalo J.T., Kvist M. Some biomechanical aspects of the foot and ankle in athletes with and without shin splints. Am J Sports Med. 1983;11(3):125–130. doi: 10.1177/036354658301100304. [DOI] [PubMed] [Google Scholar]
- 3.Chen T.H., Chou L.W., Tsai M.W. Effectiveness of a heel cup with an arch support insole on the standing balance of the elderly. Clin Interv Aging. 2014;9:351–356. doi: 10.2147/CIA.S56268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bok S.K., Kim B.O., Lim J.H. Effects of custom-made rigid foot orthosis on pes planus in children over 6 years old. Ann Rehabil Med. 2014;38(3):369–375. doi: 10.5535/arm.2014.38.3.369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rasenberg N., Riel H., Rathleff M.S. Efficacy of foot orthoses for the treatment of plantar heel pain: a systematic review and meta-analysis. Br J Sports Med. 2018;52:1040–1046. doi: 10.1136/bjsports-2017-097892. [DOI] [PubMed] [Google Scholar]
- 6.Akdoğan I., Akkaya S., Akkaya N. Comparison of the calcaneal pitch angle and modified projection area per length squared method for medial longitudinal arch evaluation of the foot. Balkan Med J. 2012;29:406–409. doi: 10.5152/balkanmedj.2012.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sweeney D., Nester C., Preece S. Effect of antipronation foot orthosis geometry on compression of heel and arch soft tissues. J Rehabil Res Dev. 2015;52(5):543–552. doi: 10.1682/JRRD.2014.12.0306. [DOI] [PubMed] [Google Scholar]
- 8.Che H., Nigg B.M., de Koning J. Relationship between plantar pressure distribution under the foot and insole comfort. Clin Biomech. 1994;9(6):335–341. doi: 10.1016/0268-0033(94)90062-0. [DOI] [PubMed] [Google Scholar]
- 9.Healy A., Dunning D.N., Chockalingam N. Effect of insole material on lower limb kinematics and plantar pressures during treadmill walking. Prosthet Orthot Int. 2012;36(1):53–62. doi: 10.1177/0309364611429986. [DOI] [PubMed] [Google Scholar]
- 10.Ferber R. The influence of custom foot orthoses on lower extremity running mechanics. Internat SportMed J. 2007;8(3):97–106. [Google Scholar]
- 11.Szames S.E., Forman W.M., Oster J. Sever's disease and its relationship to equinus: a statistical analysis. Clin Podiatr Med Surg. 1990;7:377–384. [PubMed] [Google Scholar]
- 12.Madden C.C., Mellion M.B. Sever's disease and other causes of heel pain in adolescents. Am Fam Physician. 1996;54:1995–2000. [PubMed] [Google Scholar]
- 13.Perhamre S., Lundin F., Klässbo M. A heel cup improves the function of the heel pad in Sever's injury:effects on heel pad thickness, peak pressure and pain. Scand J Med Sci Sport. 2012;22(4):516–522. doi: 10.1111/j.1600-0838.2010.01266.x. [DOI] [PubMed] [Google Scholar]
- 14.Kitaoka H.B., Luo Z.P., An K.N. Analysis of longitudinal arch supports in stabilizing the arch of the foot. Clin Orthop Relat Res. 1997;341:250–256. [PubMed] [Google Scholar]
- 15.Lee E.C., Kim M.O., Kim H.S. Changes in resting calcaneal stance position angle following insole fitting in children with flexible flatfoot. Ann Rehabil Med. 2017;41(2):257–265. doi: 10.5535/arm.2017.41.2.257. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Saltzman C.L., Nawoczenski D.A., Talbot K.D. Measurement of the medial longitudinal arch. Arch Phys Med Rehabil. 1995;76(1):45–49. doi: 10.1016/s0003-9993(95)80041-7. [DOI] [PubMed] [Google Scholar]
- 17.Bourdet C., Seringe R., Adamsbaum C. Flatfoot in children and adolescents. Analysis of imaging findings and therapeutic implications. Orthop Traumatol Surg Res. 2013;99(1):80–87. doi: 10.1016/j.otsr.2012.10.008. [DOI] [PubMed] [Google Scholar]
- 18.Sensiba P.R., Coffey M.J., Williams N.E. Inter- and intraobserver reliability in the radiographic evaluation of adult flatfoot deformity. Foot Ankle Int. 2010;31(2):141–145. doi: 10.3113/FAI.2010.0141. [DOI] [PubMed] [Google Scholar]
- 19.Taheri A., Jafarian F.S., Sadeghi-Demneh E. The effects of foot orthoses on pain management of people with plantar fasciitis. Clin Res Foot Ankle. 2015;3:2. [Google Scholar]
- 20.Ozdemir H., Söyüncü Y., Ozgörgen M. Effects of changes in heel fat pad thickness and elasticity on feel pain. J Am Podiatr Med Assoc. 2004;94(1):47–52. doi: 10.7547/87507315-94-1-47. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.