

Abstract
To investigate the emotional problems (depressive and anxiety symptoms) of mothers of children with autism spectrum disorder (ASD) and explore the role of the mother's socioeconomic status (SES) and the core symptoms of the child on the mother's emotional problems.
This cross-sectional survey was performed in 180 mothers of children with ASD in Chang Sha city of China. The 7-item Generalized Anxiety Disorder Scale (GAD-7) and the 9-item Patient Health Questionnaire (PHQ-9) were used to assess the anxiety and depressive symptoms of the mothers of the autistic children. The education level and annual family income, as well as occupation, were be selected as components of the mother's SES. Autism Behaviour Checklist (ABC) and Social Responsiveness Scale (SRS) were used for the evaluation of the core symptoms of the children. A general information questionnaire was also used. The ordinal regression was used to examine the effect of the SES and children's core symptoms on maternal emotional problems.
The valid response rate was 92.7% (167 of 180 questionnaires were returned). Of the mothers studied, 72.5% and 80.2% had depressive and anxiety symptoms, respectively, and 67.1% suffered from both symptoms. Mother's SES was observed to be unrelated to maternal anxiety symptoms (P >.05). Only 1 component of the SES (junior high school education level) was related to depressive symptoms (OR = 0.31, 95% CI 0.12–0.80). SRS score under 115 (OR = 0.38, 95% CI 0.16–0.93) of autistic children was a protective factor against maternal anxiety symptoms. The borderline and mild behavioral problems (OR = 0.43, 95% CI 0.19–0.99; OR = 0.45, 95% CI 0.22–0.94, respectively) of autistic children were protective factors against maternal depressive symptoms.
Mothers of autistic children generally exhibited high levels of anxiety and depressive symptoms. The core symptoms of the autistic children were observed to be strongly associated with both maternal anxiety and depressive symptoms. Improvements in the core symptoms of children with ASD may help reduce maternal anxiety and depressive symptoms to some extent.
Keywords: anxiety, autism spectrum disorder, core symptoms, depression, socioeconomic status
1. Introduction
Autism spectrum disorder (ASD) is a kind of neurodevelopmental disorder characterized by impairments in social interaction and communication and restricted and repetitive patterns of behavior, interests, or activities.[1] Baxter et al [2] estimated that there are 52 million cases of ASD worldwide, which is equivalent to 1 in 132 individuals. The prevalence of ASD has increased. For example, the average annual increase in ASD prevalence was 9.3% per year from 1996 to 2010 in metropolitan Atlanta.[3] In China, a meta-analysis of 44 studies covering 30 of the 34 provinces/municipalities/autonomous regions from 2000 to 2016 showed that the pooled prevalence of ASD based on clinical diagnostic criteria was 3.92 per 1000, but the prevalence was lower than that in developed countries, and the national data were inadequate in the country.[4] Sun et al [5] estimated that approximately 13.7 million children would meet the diagnostic criteria of ASD and several related conditions in China, which would result in a heavy financial burden for the government and families. There is a lack of unified and effective approaches for the prevention and treatment of ASD in clinical practice. Therefore, most autistic children have a poor prognosis, and they lack the ability to study and work independently in adulthood; therefore, they have to rely on parental care for extended periods or their lifetime.[6]
As the primary caregiver of children with ASD, mothers usually face a variety of problems such as a heavy financial burden, discrimination, stigma and ineffective therapy.[7–10]An increased risk of anxiety and depressive symptoms in mothers of children with ASD was reported compared to the risk in mothers of children without ASD.[11–15] Ingersoll et al [13] found that mothers of children with ASD had significantly higher levels of depressed moods and parenting stress than mothers of children without ASD. The frequency of anxiety and depressive symptoms in 127 Iranian mothers of children with ASD was higher than that of the general female population in their country, and the children's illness affected all aspects of the mothers’ lives.[14] Additionally, between the 2 parents of autistic children, the mothers suffered from higher levels of anxiety and depressive symptoms than the fathers.[15] This finding indicates that significantly high levels of anxiety and depressive symptoms have been acknowledged in the mothers of children with ASD.
There is no standard for socioeconomic status (SES), which usually includes the education, occupation, and income of an individual.[16] Researchers have noted that lower SESs were related to higher odds of mental illness, such as depression and anxiety.[17,18] Zablotsky et al [19] reported that lower-income was a predictor of maternal emotional problems in mothers of children with ASD. Zhao et al[20] also found a negative relationship between educational background and the anxiety symptoms of parents of children with autism. More internal factors such as education and income decreased the stress of parents and families.[21] The occupational status of the mothers directly affects the family financial income.[22] However, the specific relation between the occupation and mental health of the mothers of autistic children remained unknown.
Many studies have reported that the behavioral problems of children with ASD were related to anxiety and depression as well as stress in the mothers.[11,22,23] Children's behavioral problems were positively correlated with maternal emotional problems and stress regardless of whether the total scores of the behavioral problems were evaluated by teachers or mothers.[24,25] Children's behavioral problems (not the daily living skills or the child's diagnosis) were significantly associated with increased parenting stress and related emotional symptoms in the mothers of children with autism and developmental delay.[11] The behavioral problems of autistic children were one of the risk factors for parental anxiety and depression in a sample of 84 mothers and 18 fathers.[26] Most studies in the literature have reported the relationship between stress and children's impairment in social interactions, but some different views are presented in this article. Two studies have reported that pro-social behaviors were independent predictors of high levels of maternal or parent-child stress.[27,28] However, Davis et al [29] reported that children's communication deficits were irrelevant to parent stress in parents of toddles with ASD. In our study, we jointly explored both mothers’ SES and the 2 core symptoms of the children, as potential contributors to maternal anxiety and depressive symptoms. In addition, the core symptoms of children were expressed in terms of total points of scales rather than grades in the direction of increasing severity, which was a shortcoming of previous studies. It is hard to provide exact evidence for the hypothesis of whether mothers of children with moderate-severe autistic symptoms experience the highest level of anxiety and depressive symptoms. This problem will be explored in our study.
The mental health status of mothers will, in turn, affect the child's recovery. Having good mental health helps mothers deal with the challenges associated with childcare. Therefore, in the current study, a cross-sectional investigation was performed to study the current states of related emotional symptoms in mothers of children with ASD. The SES and children's core symptom factors were utilized for potential predictors of maternal anxiety and depressive symptoms. Furthermore, how these factors contribute to maternal emotional problems was also studied.
2. Materials and methods
2.1. Research design and sample
Four autism rehabilitation centres were randomly selected for recruitment of autistic children in Changsha city, Hunan Province. A cross-sectional survey was conducted in those centres from March to November in 2018. All the mothers of children with ASD from those centres were recruited to the study (n = 180). The mothers were biological mothers of children with ASD and had only 1 autistic child. The inclusion criteria for the study participants were as follows:
-
(1)
children had been strictly diagnosed with an autistic disorder by the DSM-V or DSM-IV criteria (the pervasive developmental disorder-not otherwise specified (PDD-NOS) and Asperger Syndrome were excluded);
-
(2)
mothers spent at least 4 hours with the children every day and lived with the children for more than 6 months; and
-
(3)
mothers did not have a mental disease.13 questionnaires were excluded because of incomplete data.
Finally, sample size of the study was 167.
Ethics approval was provided by the Ethics Committee of Hunan Provincial Maternal and Child Health Care Hospital (EC20180318). Informed consent was obtained from the participants. All of the questionnaires were given to the 4 rehabilitation centres before the interview investigation began. The trained graduate students from Center South University School of Xiang Ya Public Health interviewed the mothers to help them fill in the questionnaires.
2.2. Data collection and measurements
2.2.1. General information and socioeconomic status (SES)
A self-designed questionnaire was used to obtain the mothers’ and children's demographic information. The basic informations obtained from children with ASD were age, gender and duration of illness to the study date. The questionnaire about the mothers included age, marital status, residence, and family financial burden. Family financial burden was the treatment costs, in terms of family income, associated with the illness since the ASD diagnosis. The socioeconomic status (SES) was based on self-reported education level (primary school or less, junior school, junior high school or university degree), annual family income (<20000, 20000–80000 and >80000 RMB) and occupation (employed and unemployed). The unemployed subjects in this study included those women who stay-at-home or want to apply for a job.
2.2.2. Anxiety and depressive symptoms of mothers
The emotional problems of the mothers were defined as depressive and anxiety symptoms in this study. Two screening tools of PHQ-9 (Personal Health Questionnaire for Depression)[30] and GAD-7 (General Anxiety Disorder Scale)[31] were used to assess the subjective depressive or anxiety symptoms of the mothers over the last 2 weeks. The PHQ-9 and GAD-7 are both answered on a 4-point Likert scale from (1) “0” not at all to (4) “3” nearly every day. The PHQ-9 consists of 9 items. The GAD-7 scale consists of 7 items. These scales are widely known as simple self-management tools for screening depressive or anxiety symptoms with good validity and reliability.[32] The PHQ-9 is scored as follows: scores of 0 to 4, 5 to 9, 10 to 14, and 15 to 27 corresponded to minimal, mild, moderate, and moderately severe or above symptoms. The GAD-7 is scored as follows: scores of 0 to 4, 5 to 9, 10 to 14, and 15 to 21 corresponded to minimal, mild, moderate, and severe symptoms, respectively. Higher scores indicate more depressive and anxiety symptoms.
2.2.3. Core symptoms of children with ASD
The Social Responsiveness Scale (SRS) and Autism Behaviour Checklists (ABC) were used to evaluate 2 core symptoms of children with ASD, and both were completed by the mothers. The ABC is a 57-item scale for children older than 18 months that is divided into 5 categories:
-
(1)
sensory,
-
(2)
relating,
-
(3)
body and object use,
-
(4)
language, and
-
(5)
social and self-help.
On the basis of the severity level, each item is rated from “1” to “4”. The sum of all items is the total score of the ABC. The screening cut-off score is 53, and the diagnosis cut-off score is 67.[33] In samples of Chinese children, when the cut-off was 31, the reliability and validity of the scale in mixed samples were equal to 1.[34] This cut-off was adopted considering the bias in this study due to the fact that mothers might misunderstanding the meaning of items or could not recognize children's autistic behaviors. This study used another Chinese investigation as a reference, so we defined scores of <30, 31 to 67, and >67 as corresponding to borderline, mild, and moderate to severe symptoms.[35]
The 65-item SRS was completed by rating items from “1” (not true) to “4” (almost always true) and was used to evaluate the social communication ability of the autistic children [36]. The SRS has 5 dimensions: social awareness, social cognition, social communication, social motivation, and autistic mannerisms. The range of SRS scores is from 0 to 195. The higher the scores the children had, the more severe their social communication problems were. According to a previous study,[37] 12 SRS items were excluded because 18 (10.8%) children had inadequate verbal ability (modified SRS scores: mean=131.23, SD= 25.94) in our study. According to the method of interquartile range, the SRS scores were divided into 3 groups: <115, 115 to 147, and >147.
2.3. Statistical analyses
Statistical analysis was performed using SPSS version 18.0 (SPSS, Inc., Chicago, IL). Descriptive statistics were applied to analyze social demographic data. The continuous data were described as the mean±SD. The categorical data were described as n (%). The 4 levels of anxiety and depressive symptoms were considered as dependent variables (minimal, mild, moderate and severe). The univariate ordinal regression was first conducted to examine whether the SES and/or children's core symptoms has an important impact on maternal emotional problems. The multivariate ordinal regression models were conducted to estimate the effect of SES and children's core symptoms on maternal emotional problems after adjusting different confounders, and the odds ratio (OR) and related 95% confidence interval (95% CI) were reported. The effects of the SES and children's core symptoms on mothers’ anxiety symptoms were presented in Tables 2 and 3, respectively. The effects of the SES and children's core symptoms on mothers’ depressive symptoms were presented in Tables 4 and 5, respectively. A P value of <.05 was considered statistically significant in our study. All statistical tests were 2-sided.
Table 2.
Ordinal logistic regression model of SES variables and anxiety (n = 167).
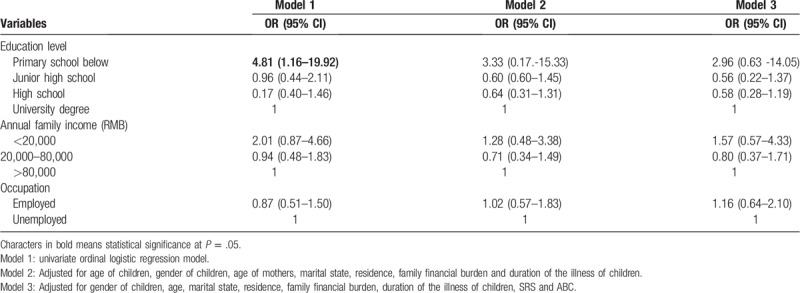
Table 3.
Ordinal logistic regression model of core symptoms of children variables and anxiety (n = 167).
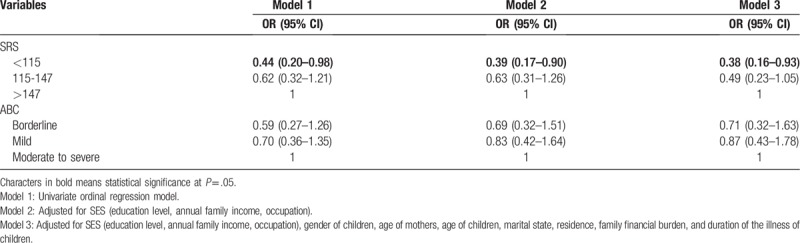
Table 4.
Ordinal logistic regression model of SES variables and depression (n = 167).
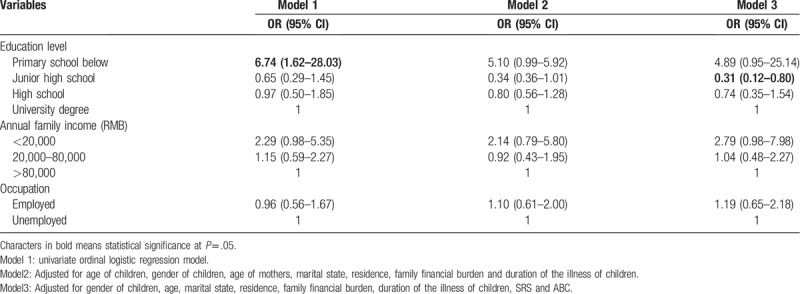
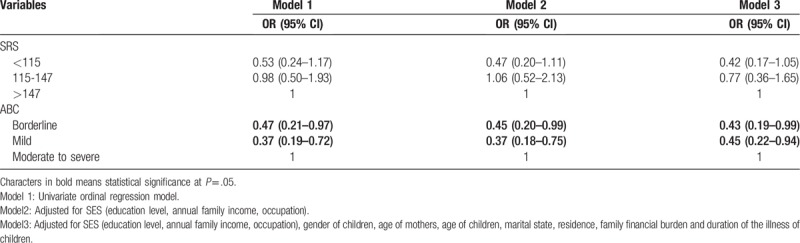
Table 5.
Ordinal logistic regression model of core symptoms of children and depression (n = 167).
3. Results
3.1. General information and SES of mothers of children with ASD
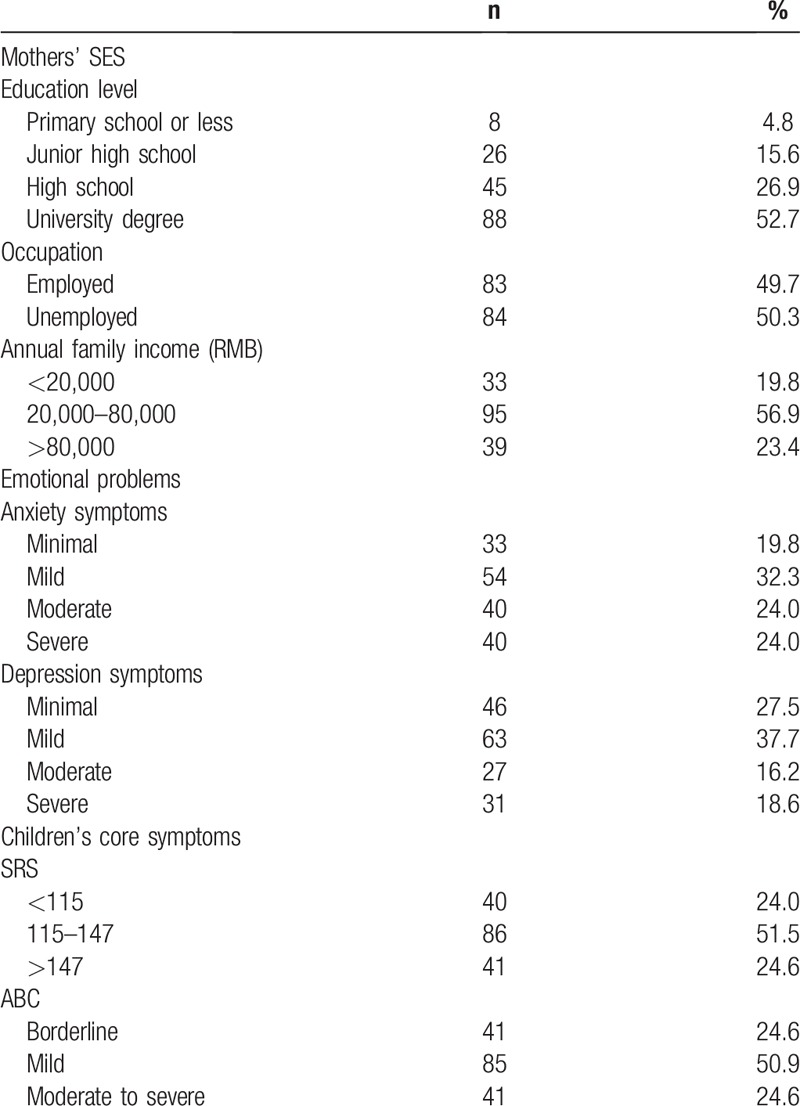
The 167 children with ASD and their mothers were recruited in the study. There were 122 boys (73.1%) and 45 girls (26.9%). The mean (SD) age of the children was 4.41 (1.76) years, range from 2 to 11 years old, most of them were 3 to 5 years old (66.5%). The mean (SD) value of the duration of illness was 24.98 (21.30) months, 80 (47.9%) less than 20 months, 45 (26.9%) between 20 to 36 months, and 42 (25.1%) more than 36 months. Among the 167 mothers, the mean (SD) age was 30.34 (4.65) years, range from 20 to 43 years old, most mothers were 27 to 33 years (52.7%). 165 (98.8%) were married and only 2 (1.2%) were divorced. Mothers with employment accounted for 49.7%. 71.3% of them lived in urban, and 52.7% of them had a university degree education level. 56.9% of them reported annual family income was 30,000 to 80,000 RMB per year, and 39 (23.4%) reported annual family income was more than 90,000 RMB. Unfortunately, 83 (49.7%) of them had a medium financial burden, and 69 (41.3%) of them reported they had a heavy financial burden.
3.2. Anxiety and depressive symptoms of mothers of children with ASD
The Cronbach's α of the PHQ-9 and GAD-7 scales were 0.928 and 0.929, respectively, which indicated high levels of internal consistency. The mean (SD) scores of the PHQ-9 and GAD-7 scales were 8.80 (6.45) and 9.64 (5.63), respectively. According to the scoring criteria of the PHQ-9 and GAD-7 scales, the total scores were divided into 4 groups (minimal symptoms, mild symptoms, moderate symptoms, and severe symptoms). It's observed 134 (80.2%) mothers had GAD-7 scores≥5 and 121 (72.5%) had PHQ-9 scores ≥5, and a total of 112 (67.1%) mothers suffered from anxiety and depressive symptoms (Table 1).
Table 1.
Distribution of mothers’ SES and emotional problems and children's core symptoms.
3.3. The core symptoms of children with ASD
The Cronbach's α of the ABC and SRS scales were 0.807 and 0.920, respectively. The ABC and SRS scales were applied to evaluate the behavioral problems and social responsive problems of the children, respectively. The mean (SD) scores of the SRS and ABC scales were 130.86 (25.62) and 56.93 (26.18), respectively. 85 (50.9%) of these children had mild behavioral problems. In total, 86 (51.5%) of children scored from 115 to 147 on the SRS scale. These findings illustrated that most of the children in the study had mild behavioral problems (Table 1).
3.4. The roles of SES and the children's core symptoms in maternal anxiety symptoms
The SES was defined as the mother's education level, annual family income and the mother's occupation in this study. As shown in Table 2, the univariate ordinal regression model reveals that an education level of primary school or below is significantly associated with maternal anxiety symptoms (in Model 1). However, the SES was not a significantly factor associated with maternal anxiety after adjusting general characteristic of mothers and children (in Model 2) and the core symptoms of the children (SRS and ABC) (in Model 3).
The univariate ordinal regression model showed the SRS score is a related factor of maternal anxiety symptoms (Table 3, Model 1). The SRS score remains as a significant factor for maternal anxiety symptoms after adjusting different confounding factors (in Model 2 and 3). As described in Model 3, after adjusting for SES and other general factors (e.g., age, gender, residence, marital status, family financial burden), mothers of children with SRS scores under 115 points were less likely to have anxiety symptoms (OR = 0.38, 95% CI 0.16 to 0.95).
3.5. The roles of SES and children's core symptoms in maternal depressive symptoms
The univariate ordinal regression indicated that an education level of primary school or below was significantly associated with depressive symptoms (Table 4, Model 1). Through multivariate ordinal models adjusted for the general characteristic of mothers and children (e,g., age of the children, the gender of the children), the effect of education level on maternal depressive symptoms was still significant in Model 2. As described in Model 3, after adjusting for all variables, including the core symptoms of the children (SRS and ABC), mothers with a junior high school education level had lower levels of depressive symptoms than mothers with a university degree education level (OR = 0.31, 95% CI 0.12–0.80).
The univariate ordinal regression indicated that ABC score was associated with maternal depressive (Table 5, Model 1). After adjusting for SES and other confounders, the ABC score remained as a significant factor for maternal depressive (in Model 2 and 3). The mothers of children with borderline (OR = 0.43, 95% CI 0.19 to 0.99) and mild behavioral problems (OR = 0.45, 95% CI 0.22–0.94) were less likely to have depressive symptoms than the reference groups (Model 3).
4. Discussion
4.1. The states of anxiety and depressive symptoms among mothers of children with ASD
In our study, the first aim was to report the states of anxiety and depressive symptoms in mothers of children with ASD. The overall prevalence of anxiety and depressive symptom in mothers with autistic children was at an elevated level. The positive rate (cut-off scores≥5) of depressive and anxiety symptoms were 72.5% and 80.2%, respectively. It seems that mothers of children with ASD were more easily effected by depressive and anxious symptoms.[11–13] Interestingly, anxiety and depressive symptoms among mothers with autistic children were more prevalent in the present study compared to that in those reported investigations. In previous studies, anxiety and depressive were assessed by the Self-Rating Anxiety Scale (SAS) and the Self-Rating Depression Scale (SDS); in an investigation conducted by Bitsika and colleagues, they found that approximately 45% of mothers had clinically significant anxiety, and 55% of them met the criteria for clinically significant depression.[15] By applying the Beck Depression Inventory (BDI) and Beck Anxiety Inventory (BAI) scales, 49.6% of mothers were noted to have depressive symptoms, and the prevalence of anxiety symptoms was 72.4%.[14] Elevated depression scores (BDI cut-off > 9) were more common in mothers of children with autism than in fathers of children with autism (50% vs 21%).[12] It should be noted that different research instruments have their own standard for evaluation. Even so, it is an observable fact that mothers of children with ASD suffer from poor mental health. The overall high level of anxiety and depressive symptoms revealed that psychiatric intervention is necessary for mothers of children with ASD.
4.2. The role of mothers’ SES in maternal anxiety and depressive symptoms
SES is a significant aspect of individual mental health; a low level of SES is associated with worse psychological health,[38,39] but there are limited studies for the association between SES and emotional problems in mothers with autistic children. Krakovich et al[21] identified education as an important factor for mental health of mothers with autistic children; mothers with a lower education level had higher odds of experiencing parenting stress. Most of mothers had inadequate knowledge about ASD in the early phases of the illness. Mothers with higher education levels begin to actively and intentionally raise awareness of ASD, actively carry out rehabilitation training for children, and relax physically and mentally to regulate their mood. One of the interesting findings in our study was that mothers with a primary school education level had significantly higher anxiety and depressive symptoms than mothers with a university degree education level in the univariate ordinal regression analysis. After adjusting for the gender of the children, age, marital status, residence, family financial burden, duration of the illness of children and SRS and ABC, only 1 component of SES (junior high school education) was a protective factor of depressive symptoms of mothers with autistic children when compared to higher education level group (university degree education). This may be partly explained by the fact that mothers with a higher level of education and intelligence generally have higher expectation of life, unfortunately, they have to face reality that their children catch the incurable disease and try to be realistic about what they can achieve. Even have high education, those mothers are still shrivel in the face of this disease and thus they feel guiltier, and gradually develop more emotional problems. Xu et al[40] reported that the average cost of rehabilitation for ASD children was 193.7% of the annual family income in Harbin City of China. The data in Changsha City is unknown. Parents of children with ASD had a substantial financial burden associated with rehabilitation training and medical illness.[41] According to the costs of the 4 rehabilitation centres in our study, it is estimated that every family spends at least 30,000 RMB per child every year for services in the rehabilitation centre. The expense of the treatment of autism is beyond the scope of medical insurance reimbursement in China. Therefore, mothers tended to believe that ASD was a threat rather than a challenge. Lu et al[42] reported that mothers of children with ASD always devoted all her time and give up work to assume responsibility for childcare, and they have no concern for their own mental health. Therefore, further studies should be conducted to examine the association between SES and maternal mental problems in populations of autistic children mothers. In our study, approximately 50.3% of mothers were unemployed. 91.0% of the mothers stated that their family faced medium-heavy level financial pressure during the children's rehabilitation treatment. The poor financial circumstances or high level of household debt would lead to negative feelings and moods. Therefore, the effect of occupation and family income on the mental health of mothers with autistic children also should be considered in further studies.
4.3. The role of the core symptoms of children in maternal anxiety and depressive symptoms
Data from ordinal regression models indicated that mothers with children who had more severe symptoms (higher ABC and SRS scores) were more likely to have higher levels of anxiety and depressive symptoms. Our findings are consisted with those of previous studies demonstrating higher odds of emotional related symptoms in mothers of children with ASD when children had more behavioral problems.[26,43]Another finding of our study was that the social responsive problems of children were relevant to maternal anxiety symptoms. Begeer et al[44] found that high-stress levels lead to the development of depressive symptoms, but in their study, there were no associations between social responsive problems and maternal stress. Our study provided new evidence for the association between maternal emotional problems, especially anxiety and depressive symptoms, and children's social interaction problems. Autism symptoms in children are characterized by deficiencies in functioning such as social communication impairment and repetitive stereotyped behaviours. Mothers generally take on the majority of the responsibility in terms of supporting and raising children, so they are especially affected by children's difficulty with normal communication and behaviour. In general, mothers spend a great deal of time with children for rehabilitation training, and they teach children to be polite or well behaved. However, the most difficult problem was how to handle the challenging behaviour of the children. The more serious a behaviour is, the worse the rehabilitation outcome is.[45] Many children made progress after rehabilitation training, but whether they can sustain the improvement is uncertain. The distress of children brought much worry to their mothers; they had more to worry about in terms of the children's safety, health and establishment of social relationships both in present and in the future. Those pressures from the children's illness would result in lower self-efficacy and quality of life of mothers, finally leading to an increase in anxiety and depressive symptoms.[46]
There are several limitations of this study should be acknowledged. First, the study was limited by self-reported data with possible recalling bias. Hence, the data of the child's autism characteristics might not conform to the actual situation of the child to some extent. Second, the study only investigated 3 components of SES, and the characteristics of individual-level may exist with a social and geographical gradient.[47] Individual and non-individual characteristics may influence the psychological status of mothers with autistic children. In addition, the anxiety and depressive symptoms of the mothers were short-term data that reflected the mental states in the past 2 weeks in this cross-sectional study. It is unclear whether there is a causal relationship between maternal mental problems and these related factors. Last but no least, anxiety and depressive symptoms were measured by GAD-7 and PHQ-9, to some extent, which may be limited in validity since they are 2 screening tools. The final diagnosis of anxiety or depression disorders should be performed by a psychiatrist or clinical psychologist.
5. Conclusion
In summary, our study revealed that mothers of children with ASD exhibited high levels of anxiety and depressive symptoms. A strong positive correlation between the autistic symptoms of children and maternal anxiety and depressive symptoms was recognized. Only 1 component of SES (education level) was related to maternal depressive symptoms. Nevertheless, statistically, we do not know whether mothers’ emotional problems are the cause or result of their children’ disease, which deserves further exploration. Furthermore, medical institutions should provide psychological support or medical help-seeking advices for those mothers to reduce their related emotional symptoms. Finally, I do believe that the most effective way to reduce their emotional problems is, of course, to completely overcome the major challenges of ASD.
Author contributions
Data curation: Wensu Zhou, Xiyue Xiong.
Formal analysis: Wensu Zhou, Xiyue Xiong, Huilan Xu.
Funding acquisition: Xiyue Xiong.
Investigation: Wensu Zhou, Dan Liu, Xiyue Xiong.
Methodology: Wensu Zhou, Dan Liu.
Project administration: Xiyue Xiong.
Resources: Dan Liu, Xiyue Xiong, Huilan Xu.
Software: Wensu Zhou, Huilan Xu.
Supervision: Xiyue Xiong, Huilan Xu.
Validation: Xiyue Xiong, Huilan Xu.
Visualization: Wensu Zhou, Dan Liu.
Writing – original draft: Wensu Zhou, Dan Liu.
Writing – review & editing: Wensu Zhou, Dan Liu, Xiyue Xiong, Huilan Xu.
Wensu Zhou orcid: 0000-0002-3871-1479.
Footnotes
Abbreviations: ABC = Autism Behaviour Checklist, ASD = autism spectrum disorder, GAD-7 = The 7-item anxiety scale, PHQ-9 = the 9-item depression scale, SES = socioeconomic status, SRS = Social Responsiveness Scale.
WZ and DL have equally contributed to this study.
This study was financially supported by the National Natural Science Foundation of China (81701356), science and technology programs of Changsha City (kq1801084). We sincerely appreciate mothers’ cooperation, as well as teachers’ support from autism rehabilitation centers.
The authors report no conflicts of interest.
References
- [1].Kroncke AP, Willard M, Huckabee H. Assessment of Autism Spectrum Disorder. 2016;Glendale, USA: Springer International Publishing, 345–373. [Google Scholar]
- [2].Baxter AJ, Brugha TS, Erskine HE, et al. The epidemiology and global burden of autism spectrum disorders. Psychol Med 2015;45:601–13. [DOI] [PubMed] [Google Scholar]
- [3].Braun KVN, Christensen D, Doernberg N, et al. Trends in the prevalence of autism spectrum disorder, cerebral palsy, hearing loss, intellectual disability, and vision impairment, metropolitan atlanta, 1991-2010. PLoS One 2015;10:1–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Wang F, Lu L, Wang SB, et al. The prevalence of autism spectrum disorders in China: a comprehensive meta-analysis. Int J Biol Sci 2018;14:717–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Sun X, Allison C, Auyeung B, et al. Service provision for autism in mainland China: a service providers’ perspective. Res Dev Disabil 2013;34:440–51. [DOI] [PubMed] [Google Scholar]
- [6].Lavelle TA, Weinstein MC, Newhouse JP, et al. Economic burden of childhood autism spectrum disorders. Pediatrics 2014;133:e520–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Tang L, Bie B. The stigma of autism in china: an analysis of newspaper portrayals of autism between 2003 and 2012. Health Commun 2016;31:445–52. [DOI] [PubMed] [Google Scholar]
- [8].Xiong N, Yang L, Yu Y, et al. Investigation of raising burden of children with autism, physical disability and mental disability in China. Res Dev Disabil 2011;32:306–11. [DOI] [PubMed] [Google Scholar]
- [9].Wang J, Zhou X, Xia W, et al. Autism awareness and attitudes towards treatment in caregivers of children aged 3-6 years in Harbin, China. Soc Psychiatry Psychiatr Epidemiol 2012;47:1301–8. [DOI] [PubMed] [Google Scholar]
- [10].Joshi G, Petty C, Wozniak J, et al. The heavy burden of psychiatric comorbidity in youth with autism spectrum disorders: a large comparative study of a psychiatrically referred population. J Autism Dev Disord 2010;40:1361–70. [DOI] [PubMed] [Google Scholar]
- [11].Estes A, Munson J, Dawson G, et al. Parenting stress and psychological functioning among mothers of preschool children with autism and developmental delay. Autism Int J Res Pract 2009;13:375–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Olsson MB, Hwang CP. Depression in mothers and fathers of children with intellectual disability. J Intellect Disabil Res 2001;45:535–43. [DOI] [PubMed] [Google Scholar]
- [13].Ingersoll B, Meyer K, Becker MW. Increased rates of depressed mood in mothers of children with ASD associated with the presence of the broader autism phenotype. Autism Res 2011;4:143–8. [DOI] [PubMed] [Google Scholar]
- [14].Kousha M, Attar HA, Shoar Z. Anxiety, depression, and quality of life in Iranian mothers of children with autism spectrum disorder. J Child Health Care 2016;20:405–14. [DOI] [PubMed] [Google Scholar]
- [15].Bitsika V, Sharpley CF, Bell R. The buffering effect of resilience upon stress, anxiety and depression in parents of a child with an autism spectrum disorder. J Dev Phys Disabil 2013;25:533–43. [Google Scholar]
- [16].Freeman A, Tyrovolas S, Ai K, et al. The role of socio-economic status in depression: results from the COURAGE (aging survey in Europe). BMC Public Health 2016;16:1098–106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Lorant V, Croux CS, Deliege D, et al. Depression and socio-economic risk factors: 7-year longitudinal population study. Br J Psychiatry 2007;190:293–8. [DOI] [PubMed] [Google Scholar]
- [18].Srijan S. Socioeconomic status and mental health: what is the causal relationship?: editorial comment to Kristian Tambs et al. ’Genetic and environmental contributions to the relationship between education and anxiety disorders. A twin study’ (1). Acta Psychiatrica Scandinavica 2012;125:187–8. [DOI] [PubMed] [Google Scholar]
- [19].Zablotsky B, Bradshaw CP, Stuart EA. The association between mental health, stress, and coping supports in mothers of children with autism spectrum disorders. J Autism Dev Disord 2013;43:1380–93. [DOI] [PubMed] [Google Scholar]
- [20].Zhao CM, Liu JC, Liu J, et al. The anxiety evaluation of parents of children with autism. Clin Med China 2011;27:878–9. [Google Scholar]
- [21].Krakovich TM, McGrew JH, Yu Y, et al. Stress in parents of children with autism spectrum disorder: an exploration of demands and resources. J Autism Dev Disord 2016;46:2042–53. [DOI] [PubMed] [Google Scholar]
- [22].Ouyang L, Grosse SD, Riley C, et al. A comparison of family financial and employment impacts of fragile X syndrome, autism spectrum disorders, and intellectual disability. Res Dev Disabil 2015;35:1518–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Supapak P, Margaret SM. Parenting stress in mothers of children with autism spectrum disorders. J Special Pediatr Nurs 2010;14:157–65. [DOI] [PubMed] [Google Scholar]
- [24].Hastings RP. Child behaviour problems and partner mental health as correlates of stress in mothers and fathers of children with autism. J Intellect Disabil Res 2003;47:4–5. [DOI] [PubMed] [Google Scholar]
- [25].Hastings RP, Kovshoff H, Ward NJ, et al. Systems analysis of stress and positive perceptions in mothers and fathers of pre-school children with autism. J Autism Dev Disord 2005;35:635–44. [DOI] [PubMed] [Google Scholar]
- [26].Junior SBM, Celestino MIO, Serra JPC, et al. Risk and protective factors for symptoms of anxiety and depression in parents of children with autism spectrum disorder. Dev Neurorehabil 2016;19:146–53. [DOI] [PubMed] [Google Scholar]
- [27].Beck A, Hastings RP, Daley D, et al. Pro-social behaviour and behaviour problems independently predict maternal stress. J Intellect Dev Disabil 2004;29:339–49. [Google Scholar]
- [28].Huang CY, Yen HC, Tseng MH, et al. Impacts of autistic behaviors, emotional and behavioral problems on parenting stress in caregivers of children with autism. J Autism Dev Disord 2014;44:1383–90. [DOI] [PubMed] [Google Scholar]
- [29].Davis NO, Carter AS. Parenting stress in mothers and fathers of toddlers with autism spectrum disorders: associations with child characteristics. J Autism Dev Disord 2008;38:1278–91. [DOI] [PubMed] [Google Scholar]
- [30].Kroenke K, Spitzer RL, Williams JBW. The PHQ-9 validity of a brief depression severity measure. J General Intern Med 2001;16:606–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Spitzer RL, Kroenke K, Williams JBW, et al. A brief measure for assessing generalized anxiety disorder. Arch Intern Med 2006;166:1092–7. [DOI] [PubMed] [Google Scholar]
- [32].Quon BS, Bentham WD, Unutzer J, et al. Prevalence of symptoms of depression and anxiety in adults with cystic fibrosis based on the Phq-9 and gad-7 screening questionnaires. Psychosomatics 2015;56:345–53. [DOI] [PubMed] [Google Scholar]
- [33].Krug DA, Arick J, Almond P. Behavior checklist for identifying severely handicapped individuals with high levels of autistic behavior. J Child Psychol Psychiatr 1980;21:221–9. [DOI] [PubMed] [Google Scholar]
- [34].Li LH, Zhong JM, Cai LY, et al. Comparison of clinical application of three autism rating scales. Chin J Contemp Pediatr 2005;7:59–62. [Google Scholar]
- [35].Juan YC, Ru ZY, Zhi S. Prevalence of autism spectrum disorders among 2-6 years old children in kindergartens of Chongqing city. Chin J Publ Health 2018;34:696–9. [Google Scholar]
- [36].Constantino JN, Gruber CP. Social ResponsivenessbScale (SRS). 2005;Los Angeles, CA: Western Psychological Services, 116–139. [Google Scholar]
- [37].Benson PR. Coping, distress, and well-being in mothers of children with autism. Res Autism Spectrum Dis 2010;4:217–28. [Google Scholar]
- [38].Mackenbach JP, Irina S, Roskam AJR, et al. Socioeconomic inequalities in health in 22 European countries. New Engl J Med 2008;358:124–67. [DOI] [PubMed] [Google Scholar]
- [39].Phetrasuwan S, Miles MS. Parenting stress in mothers of children with autism spectrum disorders. J Special Pediatr Nurs 2009;14:157–65. [DOI] [PubMed] [Google Scholar]
- [40].Xu ZB, Wang J, Sun XY, et al. A cross-sectional study on financial burden in families of children with autism spectrum disorder in Heilongjiang Province. Chin J School Health 2018;39:335–42. [Google Scholar]
- [41].Kogan MD, Strickland BB, Blumberg SJ, et al. A national profile of the health care experiences and family impact of autism spectrum disorder among children in the United States, 2005-2006. Pediatrics 2008;122:e1149–58. [DOI] [PubMed] [Google Scholar]
- [42].Lu M, Yang G, Skora E, et al. Self-esteem, social support, and life satisfaction in Chinese parents of children with autism spectrum disorder. Res Autism Spectrum Dis 2015;17:70–7. [Google Scholar]
- [43].Hou YM, Stewart L, Iao LS, et al. Parenting stress and depressive symptoms in Taiwanese mothers of young children with autism spectrum disorder: association with children's behavioural problems. J Appl Res Intellect Disabil Jarid 2018;31:1113–21. [DOI] [PubMed] [Google Scholar]
- [44].McStay RL, Dissanayake C, Scheeren A, et al. Parenting stress and autism: the role of age, autism severity, quality of life and problem behaviour of children and adolescents with autism. Autism Int J Res Pract 2014;18:502–10. [DOI] [PubMed] [Google Scholar]
- [45].Ericzn MJB, Frazee LBAS. Stress levels and adaptability in parents of toddlers with and without autism spectrum disorders. Res Pract Persons Severe Disabil 2005;30:194–204. [Google Scholar]
- [46].Hastings RP, Brown T. Behavior problems of children with autism, parental self-efficacy, and mental health. Am J Ment Retard 2002;107:22–32. [DOI] [PubMed] [Google Scholar]
- [47].Carrà G, Crocamo C, Bebbington P. Gambling, geographical variations and deprivation: findings from the adult psychiatric morbidity survey. Int Gambling Studies 2017;17:459–70. [Google Scholar]