
Figure 4.
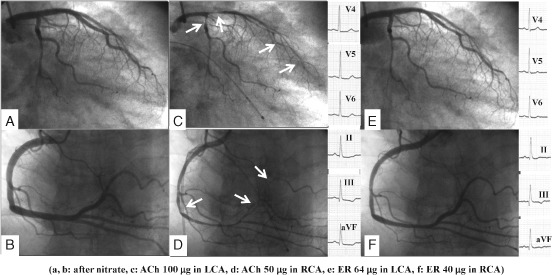
A case of CSA showing different coronary responses between ACh and ER in a female. Patient is a 70‐year‐old female complaining of rest angina at early morning and midnight. Frequent sublingual nitroglycerine suppressed her chest pain. Her coronary angiogram (A, B) was normal. IC injection of 100 µg ACh (C) provoked diffuse spasm at both proximal LAD and LCX, accompanied by more than usual chest pain and ischemic ECG change (ST‐segment depression in leads V4 through V6 at 1.0 mV). In the RCA, 50 µg ACh (D) induced diffuse spasm at distal portion accompanied by usual chest pain and ischemic ECG change (ST‐segment depression in II through III aVF leads at 1.0 mV). However, after the spontaneous spasm relief induced by ACh, IC administration of ER 64/40 µ (E, F) did not provoke spasm in both coronary arteries. Neither chest pain nor ischemic ECG change were recognized during the ER spasm provocation test. Abbreviations: ACh, acetylcholine; CSA, coronary spastic angina; ECG, electrocardiographic; ER, ergonovine; IC, intracoronary; LAD, left anterior descending artery; LCX, left circumflex artery; RCA, right coronary artery.