

Gastroesophageal reflux disease (GERD) is characterized by prolonged and repeated exposure of the esophageal mucosa to acidic gastric contents, often resulting in ulcerative and erosive damage to the esophagus. Patients typically experience symptoms of heartburn and regurgitation, although symptoms alone do not predict the presence of esophageal mucosal injury (1). The pathologic reflux can be confirmed using 24-hr ambulatory esophageal pH monitoring, and normalization of 24-hr reflux measurement correlates with symptom relief and endoscopic healing (2, 3). The newest and most effective agents currently available for the treatment of acid-related diseases are drugs classified as proton pump inhibitors (PPIs). Rabeprazole is one of the newer drugs in the PPI class, sharing a substituted benzimidazole like omeprazole and lansoprazole (4). Although rabeprazole has the same mechanism of action as other PPIs, its differing molecular structure results in small, but potentially clinically significant, differences in chemical and physical properties (5). The rapid activation compared with other PPIs may account for rabeprazole’s faster inhibition of H+, K+-adenosine triphosphatase activity and acid secretion in vitro (6).
This Case Report describes a man aged 64 years with “cluster GERD” who participated in the study entitled, “A Study of Rabeprazole 20 mg q.d. in Patients with GERD Whose Symptoms Were Not Resolved with Lansoprazole 30 mg q.d.” His GERD symptoms were controlled with rabeprazole, 20 mg q.d., after unsuccessful treatment with lansoprazole, 30 mg q.d. This study was approved by the VA Greater Los Angeles Healthcare System Institutional Review Board.
CASE REPORT
A Caucasian man aged 64 years originally presented to the outpatient gastroenterology clinic in 1997 for further evaluation of GERD symptoms. The patient had a history of esophageal dilatation in 1975 after 2 years of dysphagia. He underwent another dilatation in 1976, which resulted in esophageal rupture and surgical repair via thoracotomy. Occasional, poor esophageal motility and weak lower esophageal sphincter pressure were documented in 1995 and 1997 by esophageal manometry. Symptoms of GERD were subsequently developed and included intermittent heartburn that occurred sporadically but persisted for several days in a “cluster-like” fashion. The patient had been previously treated with cisapride but discontinued treatment due to diarrhea. Metoclopramide treatment resulted in mental status changes and was also discontinued.
In 1997, an esophagogastroduodenoscopy revealed hiatal hernia at 40–42 cm, and diverticula in the midesophagus, but no esophageal stricture. The patient described his symptoms as burning pain in the epigastrium lasting for 3–4 days per week interspersed with a few days of no symptoms and occurring approximately five or six times per year in a “cluster-like” fashion. Between these episodes, the patient was asymptomatic. The patient described his pain as incapacitating at times, often leading him to take over-the-counter antacids for transient relief. He also noted acid regurgitation in the mouth with a prominent nocturnal pattern and complained of an occasional “globus-like” sensation. The patient continued to have episodes of significant reflux symptoms despite being treated with omeprazole, 20 mg b.i.d., since 1998. He stated that symptoms often occurred at night and was given ranitidine, 150 mg q.h.s., in addition to omeprazole. The patient then complained that ranitidine treatment resulted in nausea, and the dosage was reduced to 75 mg q.h.s. The patient also ate small meals several times a day and practiced lifestyle modifications to minimize his symptoms. An upper endoscopy performed in September 2000 revealed hiatal hernia, Barrett’s esophagus, esophageal stricture, and poor esophageal motility. Intraluminal esophageal pH testing revealed that the patient experienced an esophageal pH <4 for 11% of a 24-hr period while on omeprazole.
Gastroesophageal reflux symptoms were assessed using the Gastroesophageal Symptom Assessment Scale (GSAS) questionnaire (Table 1). Positive findings of GERD on the GSAS included heartburn with a burning retrosternal discomfort, an acid or sour taste in the mouth, a feeling of pressure or lump in the throat, bloating, flatulence, and halitosis in the week immediately prior to assessment. The patient also indicated that each of the symptoms was distressing and interfered with his daily activities (total GSAS symptom score of 12 of 24 in eight different symptom categories).
Table 1.
Gastroesophageal Symptom Assessment Scale Results
| Lansoprazole, 30 mg q.d. |
Rabeprazole, 20 mg q.d. |
|||||||
|---|---|---|---|---|---|---|---|---|
| Baseline |
Week 2 |
Week 1 |
Week 2 |
|||||
| Symptom | Symptom frequency* |
Symptom score |
Symptom frequency* |
Symptom score |
Symptom frequency* |
Symptom score |
Symptom frequency* |
Symptom score |
| Heartburn or burning pain inside your chest or breast bone | 4 | 2 | 4 | 2 | 2 | 1 | 1 | 0 |
| A feeling of pressure or discomfort inside your chest | 1 | 1 | – | – | – | – | – | – |
| Food coming back into your mouth | 0 | 2 | – | – | – | – | – | – |
| An acid or sour taste in your mouth | 7 | 1 | 4 | 1 | 2 | 1 | – | – |
| Frequent gurgling in your stomach or belly | – | – | – | – | – | – | – | – |
| Feeling of pressure or lump in your throat | 7 | 3 | – | – | – | – | – | – |
| Nausea or feeling like you were going to vomit | – | – | – | – | – | – | – | – |
| Burning pain in your throat | – | – | – | – | – | – | – | – |
| Bloating or feeling like you had to loosen your belt or unbutton your pants/skirt | 3 | 1 | 2 | 1 | – | – | – | – |
| Belching | – | – | – | – | – | – | – | – |
| Flatulence or passing gas from below | 6 | 0 | – | – | 4 | 0 | 4 | 0 |
| Feeling full after eating a little | – | – | – | – | – | – | – | – |
| Bad breath | 7 | 2 | – | – | – | – | – | – |
| coughing | – | – | 6 | 1 | – | – | – | – |
| Hoarseness | – | – | 1 | 0 | 4 | 0 | – | – |
Response to the question, symptom frequency: “How many times this week [did you experience symptoms]?” symptom score: “If you have this symptom, how much did it distress or bother you?” 0 = not at all; 1 = somewhat; 2 = quite a bit; 3 = very much.
Initially in the research study, the patient was switched from omeprazole to lansoprazole at a standard dose of 30 mg q.d. to be taken approximately 30 min before breakfast for 2 weeks, during which time the patient continued to experience GERD symptoms. After the 2-week course of lansoprazole, 30 mg q.d., the GSAS survey was repeated, revealing a symptom score of 5 of 15 in five different symptom categories, including heartburn, burning retrosternal discomfort, acid or sour taste in the mouth, bloating, coughing, and hoarseness (Table 1). Compliance with the PPI regimen was evaluated with a patient dose diary, and pill counts were performed at each clinic visit. In addition, the patient underwent 24-hr ambulatory pH monitoring. He continued to have abnormal acid reflux (time with pH <4) for 11.7% of a 24-hr period (Figure 1).
Fig 1.
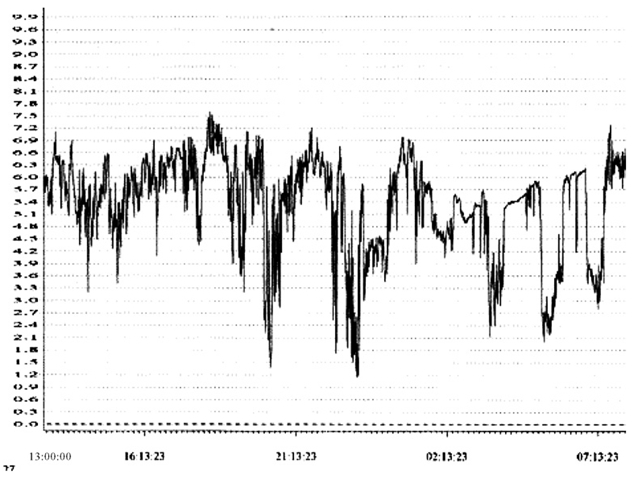
Twenty-four-hour pH reading after 2 weeks of lansoprazole, 30 mg q.d.
After a 2-week washout period, the patient was switched from lansoprazole to rabeprazole, 20 mg q.d. in the morning (30 min before breakfast), and scheduled for a follow-up visit after 1 week of daily treatment for reassessment using the GSAS questionnaire and confirmation of treatment compliance, as described above. After 1 week of rabeprazole treatment (20 mg q.d.), the patient had a GSAS symptom score of 2 in four different symptom categories. At the end of a 2-week treatment period, a repeat GSAS questionnaire was administered (Table 1), and 24-hr ambulatory pH monitoring was performed. The final symptom score on the GSAS was 0 of 6 in two categories (heartburn or burning retrosternal discomfort and flatulence), demonstrating that 2 weeks of rabeprazole therapy resulted in complete resolution of the patient’s reflux symptoms. Moreover, 24-hr ambulatory pH monitoring indicated a reduction of abnormal acid reflux time to 7.5% (Figure 2). Furthermore, as shown in Figure 2, there was improved control of nighttime esophageal acidity. The patient continued treatment with rabeprazole, 20 mg q.d., with occasional use of an antacid to control nocturnal GERD symptoms. He has continued on rabeprazole therapy successfully for more than 12 months.
Fig 2.

Twenty-four-hour pH reading after 2 weeks of rabeprazole, 20 mg q.d.
DISCUSSION
This case describes a unique pattern of GERD symptoms that we have termed “cluster GERD.” Cluster GERD is best defined as several consecutive days of reflux symptoms experienced by patients intermittently (i.e., several consecutive days of reflux symptoms occurring interspersed with periods of no reflux lasting from a few days to up to approximately 2 months) at least several times a year during the course of their illness. Many patients with GERD take medication only in response to symptoms and are poorly compliant with continuous maintenance therapy (7-9). In a study by Schindlbeck et al. (8), 39% of patients with GERD on continuous maintenance therapy stopped taking their medication, whereas 61% continued to take medication, either on demand or regularly. Of the group that stopped taking medication entirely, almost one third actually had their symptoms completely disappear. The poor compliance illustrated by this study suggests that there is a large percentage of patients who experience recurrent and intermittent GERD-like symptoms that may or may not seek medical attention.
The patient discussed here had a history of esophageal injury and, prior to enrolling in the study, had intermittent symptoms of reflux interspersed with periods with no reflux symptoms. The intermittent symptom profile and the availability of over-the-counter acid suppressants may deter patients with cluster GERD from seeking medical attention. In general, these patients will experience complete resolution of their symptoms with over-the-counter antacids, and it is unlikely that there is significant esophageal injury. Inciting agents, such as certain types of foods, beverages, or stress, may “trigger” heartburn symptoms to occur. The determinants of this disorder as well as its prevalence clearly need further investigation.
In this case, rabeprazole treatment resulted in complete symptom resolution, whereas lansoprazole failed to resolve GERD symptoms. Possible explanations of this phenomenon include reduced bioavailability for lansoprazole and/or increased efficacy with rabeprazole. Because this report describes an open-label treatment with rabeprazole after the patient completed a 2-week washout period with lansoprazole, the contribution of unrecognized psychological influences that may have contributed to the improved symptom scores on the final GSAS questionnaire cannot be excluded completely. Despite the possible bias influencing subjective testing, esophageal pH measurements indeed indicate an objective improvement in esophageal pH with rabeprazole over lansoprazole—most notably in the nocturnal hours—suggesting perhaps that rabeprazole was more effective for relief of nocturnal reflux in this patient.
The canalicular space of the parietal cell is an acidic compartment with a maximal acidity of pH <1.0 (7). Rabeprazole, having the highest pKa within the PPI class, has the theoretical advantage of being the first to be acidified or protonated and, in vitro, has been shown to act more rapidly (6, 10, 11). In general, the newer PPIs (pantoprazole and rabeprazole) that have been introduced onto the U.S. market have a greater likelihood of inhibiting gastric acid secretion for a full 24-hr period and, therefore, can be dosed once per day, generally in the morning. Rabeprazole has been shown to provide rapid, potent, and sustained inhibition of gastric acid secretion in Helicobacter pylori-positive subjects and inhibition of peptone-meal stimulated gastric acid secretion superior to omeprazole in H. pylori-negative subjects (12, 13).
In a short-term study of 20 patients with GERD, both 20 mg q.d. and 40 mg q.d. rabeprazole normalized acid reflux time by day 7 of treatment (14). Additionally, no significant difference in efficacy or side effects was found, with both dosages being well tolerated. Consequently, the recommended standard dose of rabeprazole, 20 mg q.d., was used in the patient described in this report, with notable improvement of acid reflux time as well as elimination of GERD symptoms.
This report is the first to describe the symptoms of “cluster GERD” in a patient with recurrent and intermittent reflux disease followed by periods of complete remission who responded completely to rabeprazole in both symptom relief and improvement in esophageal pH. Further investigations are necessary to better characterize and treat this disorder, which may be more common than previously appreciated.
ACKNOWLEDGMENTS
This research was funded by a research grant from Eisai Inc., Teaneck, New Jersey, and Janssen Pharmaceutica Inc., Titusville, New Jersey.
REFERENCES
- 1.Voutilainen M, Sipponen P, Mecklin JP, Juhola M, Farkkila M: Gastroesophageal reflux disease: prevalence, clinical, endoscopic and histopathological findings in 1,128 consecutive patients referred for endoscopy due to dyspeptic and reflux symptoms. Digestion 61:6–13,2000 [DOI] [PubMed] [Google Scholar]
- 2.Sabesin SM, Berlin RG. Humphries TJ, et al. : Famotidine relieves symptoms of gastroesophageal reflux disease and heals erosions and ulcerations. Results of a multicenter, placebo-controlled, doseranging study. USA Merck Gastroesophageal Reflux Disease Study Group. Arch Intern Med 151:2394–2400, 1991 [PubMed] [Google Scholar]
- 3.Wesdorp IC, Dekker W, Festen HP: Efficacy of famotidine 20 mg twice a day versus 40 mg twice a day in the treatment of erosive or ulcerative reflux esophagitis. Dig Dis Sci 38:2287–2293, 1993 [DOI] [PubMed] [Google Scholar]
- 4.Kovacs TOG, Sytnik B, Humphries TJ, et al. : A low dose of a new proton pump inhibitor LY307640 (E3810) effectively inhibits acid secretion in humans. Gastroenterology 110:A161, 1996. (abstr) [Google Scholar]
- 5.Morii M, Hamatani K, Takeguchi N: The proton pump inhibitor, E3810, binds to the N-terminal half of the alpha-subunit of gastric H+, K+-ATPase. Biochem Pharmacol 49:1729–1734, 1995 [DOI] [PubMed] [Google Scholar]
- 6.Besancon M, Simon A, Sachs G, Shin JM: Sites of reaction of the gastric H, K-ATPase with extracytoplasmic thiol reagents. J Biol Chem 272:22438–22446, 1997 [DOI] [PubMed] [Google Scholar]
- 7.Hungin AP, Rubin G, O’Flanagan H:Factors influencing compliance in long-term proton pump inhibitor therapy in general practice. Br J Gen Pract 49:463–464, 1999 [PMC free article] [PubMed] [Google Scholar]
- 8.Schindlbeck NE, Klauser AG, Berghammer G, Londong W, Muller-Lissner SA: Three year follow up of patients with gastroesophageal reflux disease. Gut 33:1016–1019, 1992 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Dent J, Brun J, Fendrick AM, et al. : An evidence-based appraisal of reflux disease management—The Genval Workshop Report. Gut 44(Suppl 2):S1–S16, 1999 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Horn J: The proton-pump inhibitors: similarities and differences. Clin Ther 22:266–280, 2000 [DOI] [PubMed] [Google Scholar]
- 11.Williams MP, Pounder RE: Review article: the pharmacology of rabeprazole. Aliment Pharmacol Ther 13(Suppl 3):3–10, 1999 [DOI] [PubMed] [Google Scholar]
- 12.Ohning GV, Barbuti RC, Kovacs TO, et al. : Rabeprazole produces rapid, potent, and long-acting inhibition of gastric acid secretion in subjects with Helicobacter pylori infection. Aliment Pharmacol Ther 14:701–708, 2000 [DOI] [PubMed] [Google Scholar]
- 13.Ohning GV, Walsh JH, Pisegna JR, et al. : Rabeprazole is superior to omeprazole for the inhibition of peptone meal-stimulated gastric acid secretion in Helicobacter pylori-negative subjects. Ailment Pharmacol Ther 17:1109–1114, 2003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Robinson M, Maton PN, Rodriguez S, Greenwood B, Humphries TJ: Effects of oral rabeprazole on oesophageal and gastric pH in patients with gastro-oesophageal reflux disease. Ailment Pharmacol Ther 11:973–980, 1997 [DOI] [PubMed] [Google Scholar]