

Abstract
Background:
Physicians and medical students in the world do not have high awareness of fecal microbiota transplantation (FMT). This study aimed to explore the recognition and attitude of postgraduate medical students towards FMT and to create awareness for it.
Methods:
A self-administered questionnaire was distributed to first-year Chinese postgraduate medical students across six medical universities. Basic descriptive statistical analyses were performed.
Results:
A total of 1828 eligible questionnaires were included into analysis. 47.76% of students did not know FMT prior to this survey. Respondents with a high-level recognition of FMT were more willing to donate feces or receive FMT therapy than those with a low-level recognition (80.26% vs. 69.62%, p = 0.000 and 56.80% vs. 41.45%, p = 0.000). The respondents from a leading institution of FMT in China showed better awareness compared with others, and 42.26% of them knew about FMT from medical lectures. The main reasons for respondents not supporting FMT were: limited reported clinical evidence (67.94%), raw technology (42.56%), and lack of analysis of patient willingness or cost-effectiveness (36.71%). However, the life-saving value (84.41%), the automatic purification system (38.68%), low expenses (36.00%), and convenient delivering ways (35.67%) were the major considerations for supporting FMT.
Conclusions:
This study revealed the low recognition level of postgraduate medical students about FMT. Therefore, medical education should not neglect the knowledge of FMT. Studies of FMT and standardized FMT should be carried out to promote its development.
Keywords: attitude, fecal microbiota transplantation, knowledge, medical education, postgraduate medical students, recognition
Background
Fecal microbiota transplantation (FMT) refers to the delivery of a large amount of gut microbiota (fecal suspension or purified fecal microbiota) from a healthy donor into the gastrointestinal tract (GI) of a patient to treat diseases by restoring gut microbiota.1–3 Its use was first clearly documented as a treatment for food poisoning, severe vomiting, and diarrhea in ancient traditional Chinese medicine during the fourth century.4 As the most effective therapy for refractory Clostridoides (Clostridium) difficile infection (CDI),5 FMT has been strongly recommended for patients who suffer multiple recurrences of CDI with appropriate antibiotic treatments.6 The therapeutic potential of FMT in inflammatory bowel disease (IBD),7,8 irritable bowel syndrome (IBS),9,10 metabolic syndrome,11,12 hepatic disease,13,14 cancer,15,16 and other diseases17,18 has also caught the attention of researchers in recent years. A number of clinical trials are currently underway to explore the efficacy of FMT in microbiota-related diseases.
As with any therapy, a new clinical therapeutic application depends not only on its efficacy but also on the recognition and attitudes of physicians and patients. FMT is still in the investigation phase, lacking adequate data on efficacy and safety. Physician’s and patient’s perceptions of FMT are discrepant. A questionnaire survey evaluating gastroenterologists perceptions of FMT in Australia indicated that 90% of gastroenterologists would refer patients with CDI for FMT if it was easily available, 37% for ulcerative colitis (UC), 13% for Crohn’s disease (CD), and 6% for IBS.19 The biggest concern of most gastroenterologists was the lack of supportive evidence and safety issues for FMT.19 Also, another questionnaire survey conducted in China showed that 71.9% of Chinese physicians had heard of FMT prior to the survey, but only 45.6% had an awareness of FMT.20 The major concerns of the physicians included acceptability of FMT among the patients (79.2%), absence of standardized guidelines (56.9%), and administration and ethics (46.5%).20 With regard to the ethical problems of FMT, Ma and colleagues21 developed a questionnaire to assess Chinese physicians perceptions and attitudes toward ethical and social challenges raised by FMT. Results showed that 89% of all respondents believed FMT is a promising treatment model for some diseases, from which 88% of respondents chose clinical efficacy as the primary reason for recommending FMT. The high expectation of the patients and pressure on clinicians (33%) were reported as the most frequent reasons for not recommending FMT.21 In contrast, patient’s knowledge and attitude toward FMT directly reflected the acceptance of FMT. A survey focusing on evaluating patients attitudes toward the use of FMT in the treatment of CDI exhibited that 85% of respondents chose to receive FMT, and 15% chose antibiotics alone.22 In addition, a survey carried out in New York revealed the poor awareness of most patients towards FMT (12%). However, 77% of patients were open to undergoing the procedure if medically indicated,23 and if recommended by a physician (94%, p < 0.001).22 This is similar to another study that indicated specialists were likely to change the patient’s opinion towards FMT.24 Therefore, a physician’s perceptions of FMT indirectly affects patient’s acceptance.
As an important reserve of future physicians and medical researchers, the recognition and attitude of postgraduate medical students reflects the structure of medical education, as well as determining future physicians perceptions towards FMT. Therefore, we designed this questionnaire to assess the recognition and attitude of the postgraduate medical students towards FMT. To the best of the authors’ knowledge, this is the first survey that focuses on the recognition and attitude of postgraduate medical students towards FMT. We hope that the results of this survey reflect the current attitudes of Chinese postgraduate medical students towards FMT, and also provide recommendations for existing medical education.
Methods
Study design, setting, and participants
This study was a questionnaire survey among the first-year postgraduate medical students from six medical universities in China including: Nanjing Medical University (NJMU), Jiangxi Medical College of Nanchang University (NCU), Guangxi Medical University (GXMU), Hubei University of Chinese Medicine, Ningxia Medical University, and the West China College of Medicine of Sichuan University. The questionnaire was pilot tested for interpretation of items constructed, and the importance of content, among ten first-year postgraduate students from NJMU. Questionnaires were then anonymously distributed by electronic and paper form to 2113 first-year postgraduate medical students at the six universities from August 2018 to October 2018. They completed the questionnaires voluntarily and independently, under anonymous and uncompensated conditions. In this article, we use ‘postgraduate students’ and ‘participants’ interchangeably to refer all the respondents, without trying to differentiate between them.
Questionnaire design
A self-administered questionnaire was developed according to our experience in performing FMT and practice guidelines. It consisted of 16 questions aiming to evaluate postgraduate medical students recognition and attitudes towards FMT. Specifically, items about knowledge of FMT among the participants included four single-choice questions and one single-choice question on how they learnt about FMT for the first time. The choices for the four recognition questions about the definition, donor, indications, and origin of FMT were answered by ‘known’ and ‘unknown’. Participants who chose ‘known’ scored 1 point, while ‘unknown’ scored 0. The higher total score represented a higher recognition level of FMT. Items related to the reasons for supporting or not supporting FMT if participants themselves were medical workers or researchers, the willingness to donate feces, and to accept FMT therapy. Reasons for refusing to donate feces were included with regards to their attitudes toward FMT through multiple-choice questions. Furthermore, the significance of gut microbiota in preventing and treating disease was described through 4 scales as ‘very important’, ‘more important’, ‘important’, and ‘not important’. Participants responses were analyzed to assess whether their perceptions of gut microbiota differed from those of FMT.
The participants were also asked to provide their demographics including gender, university, specialty, work seniority, and health status. These factors were further analyzed as possible reasons influencing the recognition level of the postgraduate medical students of FMT.
Statistical analysis
Data collection and its statistical analysis was carried out using the SPSS software system (SPSS for Windows, Version 23.0, SPSS Inc., Chicago). The paper questionnaires were double-typed by the encoder and the electronic ones were imported directly. The data analysis excluded incomplete items regarding gender, specialty, work seniority, health status, or any choice questions. The categorical data obtained was presented as frequency counts and percentages. Kruskal–Wallis H test was used to evaluate univariate factors associated with the recognition of FMT. Factors affecting the recognition level of FMT with p < 0.10 on univariate analysis were analyzed by multinomial logistics regression subsequently. In particular, the participants were divided into two groups based on the total recognition score: (1) low recognition level group: total recognition score <2, (2) high recognition level group: total recognition score ⩾2. Pearson Chi-squared test was used to detect the differences in the cognitive level of FMT among various universities and specialties. The participants willingness to donate feces and accept FMT therapy in different groups was also investigated using the Pearson Chi-squared test. For all analyses, p < 0.05 was considered statistically significant.
Ethical statement
This study was reviewed and approved by the Second Affiliated Hospital of Nanjing Medical University Institutional Review Board ([2017] KY No.009). All participants completed it voluntarily, under anonymous and uncompensated conditions, and gave written consent through a proper term.
Results
A total of 2113 paper and electronic questionnaires were issued and 2052 were returned, with a recovery rate of 97.11%. Among them, there were 1828 valid questionnaires (some questionnaires with missing items), and the effective rate was 89.08%. The participant’s demographics and health description are shown in Table 1. In particular, non-clinical medicine specialties (307, 16.8%) included Preventive Medicine (88, 28.7%), Basic Medicine (147, 47.9%), Nursing (49, 16.0%), and others (23, 7.5%). Clinical medicine specialties(1521, 83.2%) were further clustered into 22 groups for the subsequent analysis: gastroenterology (96, 6.3%), cardiology (88, 5.8%), endocrinology and rheumatology (63, 4.1%), pulmonology (46, 3.0%), nephrology (34, 2.2%), hematology (35, 2.3%), ophthalmology, otorhinolaryngology and stomatology (174, 11.4%), gynecology, obstetrics and pediatrics (161, 10.6%), neurology and pathergasiology (72, 4.7%), traditional Chinese medicine (73, 4.8%), radiology (73, 4.8%), oncology (86, 5.7%), anesthesiology (61, 4.0%), general surgery (112, 7.4%), osteology (64, 4.2%), urinary surgery (47, 3.1%), neurosurgery (35, 2.3%), other surgery (52, 3.4%), lemology and dermato-venerology (43, 2.8%), geriatrics and rehabilitation science (32, 2.1%), emergency medicine and intensive care medicine (24, 1.6%), and others (50, 3.3%).
Table 1.
Participants demographics and health description (n = 1828).
| Items | n (%) | |
|---|---|---|
| Gender | Female | 1149 (62.9%) |
| Male | 679 (37.1%) | |
| Specialty | Clinical medicine | 1521 (83.2%) |
| Non-clinical medicine | 307 (16.8%) | |
| University | Nanchang University | 747 (40.9%) |
| Nanjing Medical University | 478 (26.1%) | |
| Guangxi Medical University | 318 (17.4%) | |
| Other Universities | 285 (15.6%) | |
| Work seniority | <1 year | 1617 (88.5%) |
| ⩾1 year | 211 (11.5%) | |
| Health status | Good | 1262 (69.0%) |
| Sub-health | 566 (31.0%) |
Recognition of first-year postgraduate medical students of FMT
Items used to detect the recognition of first-year postgraduate medical students of FMT are shown in Table 2. Each question answered by ‘known’ represented one recognition score. There are four questions, with a maximum score of 4 and a minimum score of 0. The higher total score represented a higher recognition level of FMT. The distribution of total recognition scores of participants are listed in Table 2. The awareness rates of participants from different specialties (clinical medicine versus non-clinical medicine versus clinical medicine subspecialties) on each question are shown in Table 2 and Supplementary Table 1. A Kruskal–Wallis H test was taken to explore whether gender, specialty, work seniority, university, or health status can make a difference in total recognition scores. We found that gender (H = 5.392, p = 0.020), specialty (H = 12.840, p = 0.000), university (H = 94.479, p = 0.000) and health status (H = 3.959, p = 0.047) can influence the distribution of total recognition scores. But there was no significant difference in total recognition scores between participants who had different work seniority (H = 0.000, p = 0.989). The pairwise comparisons made among various universities indicated that the distribution of total cognitive scores of postgraduate medical students in NJMU was significantly different from that of NCU, GXMU, and the other universities, with corresponding p values of 0.000, 0.000, 0.001. Factors (gender, university, specialty, and health status) affecting the recognition level of FMT with p < 0.10 on univariate analysis were analyzed by multinomial logistics regression. The statistical results suggested that university (p = 0.000) and specialty (p = 0.026) makes a difference to the recognition level of FMT.
Table 2.
Distribution of total cognitive scores of first-year postgraduate medical students of FMT (n = 1828).
| Question | Known (%) | M (Q1, Q3) | Clinical medicine (%) | Non-clinical medicine (%) |
|---|---|---|---|---|
| 1.FMT refers to the delivery of fecal microbiota from a healthy donor into a patients intestinal tract | 955 (52.24%) | 1 (0, 1) | 829 (54.50%) | 126 (41.04%) |
| 2.Donors for FMT may come from relatives or other people | 694 (37.96%) | 1 (0, 1) | 594 (39.05%) | 100 (32.57%) |
| 3.FMT is currently used to treat Clostridium difficile infections and other diseases | 297 (16.25%) | 0 (0, 0) | 253 (16.63%) | 44 (14.33%) |
| 4.The medical history of FMT dates back at least 1700 years to China | 114 (6.24%) | 0 (0, 0) | 100 (6.61%) | 14 (4.56%) |
M: Median.
As referred to above, participants were divided into two groups according to the total recognition score at the cut off score of 2. There were 1129 (61.8%) postgraduate medical students in the group of low-level of recognition and 699 (38.2%) in the group of high-level recognition. Pearson Chi-squared test showed a significant difference (χ2 = 51.045, p = 0.000) between clinical medicine subspecialties and non-clinical medicine in the recognition level of FMT (Supplementary Table 1). In short, students who had majored in gastroenterology had higher recognition levels of FMT than those majoring in other clinical medicine subspecialties and non-clinical medicine. The recognition levels of FMT among ophthalmology, otorhinolaryngology and stomatology, neurology and pathergasiology, radiology, traditional Chinese medicine, and general surgery was low and similar to non-clinical medicine. In contrast, that of the other 16 clinical medicine subspecialties was higher when compared with non-clinical medicine. Furthermore, respondents from NJMU had the highest recognition level of FMT while respondents from NCU had the lowest (χ2 = 80.960, p = 0.000). The results of the pairwise comparison are shown in Figure 1.
Figure 1.
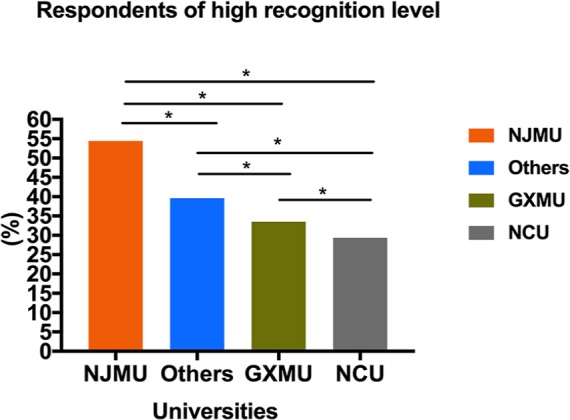
The recognition level of postgraduate medical students of FMT among various universities.
Learning about FMT for the first time
The first approach for respondents to learn about FMT is detailed in Figure 2. Unfortunately, quite a large number of postgraduate medical students (44.64%) did not know anything about FMT prior to this survey. It is worth mentioning that many postgraduate medical students (42.26%), from NJMU primarily, learned about FMT from medical lectures. In addition, half of the participants (51.93%) from the other five universities first learned about FMT from this survey, and medical lectures are an important way for them to learn about FMT (19.70%), which was even higher than the mass media (Figure 2B).
Figure 2.

Approaches to learning about FMT for the first time. All respondents’ approaches to primarily knowing about FMT (a). Approaches of respondents from other universities versus NJMU to knowing about FMT for the first time (b).
Attitudes of first-year postgraduate medical students toward FMT
From the perspective of clinicians and researchers, the main reason for respondents supporting or not supporting FMT are displayed in Figure 3(a) and (b). Our results indicated that the majority of the participants (n = 1347, 73.69%) were willing to donate their feces, while only 481 (26.31%) were unwilling or uncertain about it. With regard to the reasons for unwillingness (only the unwilling or uncertain respondents answered the multiple choices question, n = 481), and of interest, 37.42% of participants said they were afraid of microorganisms. A number of respondents (33.47%) considered donating feces troublesome, 32.64% felt ashamed of this topic because it hampered their privacy, and 19.13% were unwilling to become donors due to lack of confidence in the existing technology. More participants (80.26%) in the high recognition level group were willing to donate feces when compared with those in the low recognition level group (69.62%). The proportion of participants willing to donate feces showed a significant difference (χ2 = 25.199, p = 0.000) in different recognition level groups. This indicated that the higher the recognition level on FMT, the higher the willingness to become a donor for FMT.
Figure 3.

Reasons for supporting FMT (a) and not supporting FMT (b).
Out of 1828 postgraduate medical students 47.32% of participants were willing to receive FMT therapy if they had the disease, on their physician’s recommendation. But 52.68% of participants felt uncertain about receiving FMT therapy, or refused it even if the physicians recommended it. Similarly, we found that there was a significant difference in the proportion of participants willing to receive FMT therapy between different recognition level groups (χ2 = 40.768, p = 0.000). 56.80% of respondents in the high recognition level group compared with only 41.45% in the low recognition level group, were willing to receive FMT therapy.
Significance of microbiota in the prevention and treatment of disease
Despite the varying levels of recognition and attitudes of participants towards FMT, the overwhelming majority of participants (n = 1816, 99.34%) thought that disturbing and restoring gut microbiota played an important role in the pathogenesis and prevention of disease. Specifically, 56.73% chose ‘very important’, 33.37% chose ‘more important’, 9.25% chose ‘important’, and only 0.66% thought it is unimportant.
Discussion
This study found that nearly half of the postgraduate medical students had not heard about FMT prior to this survey. Less than half of postgraduate medical students know the concept of FMT, let alone its donor, indications and historical origin. All of the results indicated that postgraduate medical students had poor recognition of FMT. This finding was similar to the survey conducted by Orduna and colleagues using social networks that revealed the poor knowledge of FMT in the general population.25As an important reserve of future physicians and medical researchers, the reasons that postgraduate medical students have the same low awareness of FMT as the general population need to be explored further. First, FMT is a relatively new technique that lacks substantial clinical evidence about its efficacy and safety for related diseases, and has only been written into the guidelines for the treatment of recurrent CDI.5 Second, there is no universal and standardized FMT procedure for donor selection, laboratory preparation, and delivering methods. The ethical problems of FMT are also of great considerations among the clinicians. Finally, the insufficient promotion due to the above problems further affects the recognition of physicians and the general population of FMT. FMT has not been the mainstream treatment and, therefore, has not been offered in many centers, which is indirectly confirmed by this study with the recognition level of FMT varying among the six universities. The reasons why students from NJMU have the highest rate of recognition on FMT could be due to the fact that the leading FMT center is supported by this university, and the Chinese fmtBank, which provides national non-profit FMT service, is also supported by NJMU.
The results demonstrate that postgraduate medical students who have high recognition levels of FMT show a more positive attitudes toward FMT and are more likely to receive FMT therapy or to donate their feces than those who have a low recognition level. Online research also showed that a high proportion (86%) wanted to receive more information about FMT.25 The data suggests that the popularization of FMT shows great significance to promote acceptance, not only among the postgraduate medical students, but also the clinicians and the general population. Among 44.64% of respondents who knew about FMT from this survey, medical lectures (25.6%) are the most common approach for respondents from NJMU and other universities to learn about FMT, followed by mass media (18.8%). This indicated that medical lectures and mass media are important ways to promote FMT. Medical universities can influence the perceptions of postgraduate students towards FMT through lectures or extended classroom teaching. Although the mass media is also a powerful way to disseminate knowledge, the coverage of this emerging therapy is limited, with varying degrees of depth and attention. Some respondents had heard about FMT prior to this survey, but it was limited to the concept of FMT. Therefore, some deeper FMT related knowledge should be included in the popularization of FMT, such as the indications, methodology, and origin of FMT. Only correct science popularization can better improve postgraduate medical students understanding of FMT, therefore promoting them to refer more materials. An observation that warrants discussion is that 99.34% of participants affirmed the importance of gut microbiota in spite of having low recognition of FMT. It was also surprising that 37.42% of participants were not willing to donate feces as donors because of their fear of microorganisms. These two contradictory results indicated that postgraduate medical students need to correctly understand microorganisms and the efficacy of FMT in the reconstruction of gut microbiota. Moreover, it is not surprising that postgraduate medical students specializing in clinical medicine have higher recognition levels when compared with those in non-clinical medicine. However, this study indicated that only participants focusing on gastroenterology knew more about FMT. Owing to the multiple indications of FMT and the multidisciplinary cooperative medical model of the future, the objective of popularizing FMT should not be limited to those who majored in gastroenterology. Therefore, both mass media and medical lectures should contribute in improving the quality and breadth of the popular science of FMT.
Promoting the development of FMT is the long-standing goal of our team. This study indicated that the life-saving value of FMT was the primary reason for postgraduate medical students supporting FMT, which reflected the conclusion that the efficacy of FMT is undoubtedly the greatest factor determining the acceptability of FMT.20 The limited amount of reported clinical evidence prevented them from supporting FMT, therefore more clinical research focused on the efficacy and long-term adverse events of FMT is required. Raw technology was also a concern on the application of FMT, because the standardized, humanized, strict laboratory procedures, and clinical operation flow is crucial for guaranteeing the success of FMT.26 Therefore, the advent of an automatic purification system for enriching microbiota from stool samples (GenFMTer, FMT medical, Nanjing, China)26 and promising delivery methods were also the focus of participants in this study. FMT can be delivered through the upper-gut, mid-gut, and lower-gut.27 For example, colonic transendoscopic enteral tubing is a very effective and convenient way for the frequent delivery of FMT to the whole colon.28,29 Appropriate delivery methods of FMT according to individual characteristics can satisfy patients and reduce side effects.28,29 Improvement in aesthetics, the cost-effectiveness analysis, and the analysis of the willingness of the patients are other ways to promote FMT.
FMT is a breakthrough in therapeutics in microbiota related diseases in recent years. Investigations into patients and physicians perception of FMT have been initiated. To the best of the authors’ knowledge this is the first self-administered questionnaire survey to assess the perceptions of postgraduate medical students toward FMT. This survey revealed the lack of recognition of postgraduate medical students of FMT. The education of the cutting-edge science of FMT should be highlighted in traditional medical education. This study has some limitations. As a cross-sectional study, the participants we surveyed were first-year postgraduate medical students, and we lack longitudinal comparison data for different grades. More studies about the differences in recognition of FMT among postgraduates in different grades, and between postgraduates and gastroenterologists, need to be instigated. Research is also required to investigate further whether the recognition and attitude of postgraduate medical students towards FMT can be improved by strengthening the education of FMT and promoting the standardization of FMT.
Conclusion
To the best of the authors’ knowledge, this self-administered questionnaire survey is the first investigation to assess the perceptions of postgraduate medical students toward FMT in China. Postgraduate medical students recognition of FMT was generally lower than expected. Therefore, the profound and extensive popularization of FMT, especially the development of medical lectures about FMT, is required for postgraduate medical students to correctly establish the knowledge of FMT and further promote the development of FMT in China. The requirement to carry out studies on identifying the efficacy and safety of FMT and standardized FMT cannot be understated.
Supplemental Material
Supplemental material, Data1 for The recognition and attitudes of postgraduate medical students toward fecal microbiota transplantation: a questionnaire study by Xia Wu, Min Dai, Heena Buch, Jianling Bai, Wenwu Long, Chuyan Long, Xianyan Tang, Hua Tu, Renjie Zhang, Cairong Zhu, Shaoqi Yang, Bota Cui, Guozhong Ji and Faming Zhang in Therapeutic Advances in Gastroenterology
Supplemental Material
Supplemental material, Questionnaire for The recognition and attitudes of postgraduate medical students toward fecal microbiota transplantation: a questionnaire study by Xia Wu, Min Dai, Heena Buch, Jianling Bai, Wenwu Long, Chuyan Long, Xianyan Tang, Hua Tu, Renjie Zhang, Cairong Zhu, Shaoqi Yang, Bota Cui, Guozhong Ji and Faming Zhang in Therapeutic Advances in Gastroenterology
Supplemental Material
Supplemental material, Supplementary_table for The recognition and attitudes of postgraduate medical students toward fecal microbiota transplantation: a questionnaire study by Xia Wu, Min Dai, Heena Buch, Jianling Bai, Wenwu Long, Chuyan Long, Xianyan Tang, Hua Tu, Renjie Zhang, Cairong Zhu, Shaoqi Yang, Bota Cui, Guozhong Ji and Faming Zhang in Therapeutic Advances in Gastroenterology
Acknowledgments
Faming Zhang, Bota Cui and Guozhong Ji designed the study. Xia Wu and Min Dai drafted the manuscript. Faming Zhang and Heena Buch have been involved in the revision of the manuscript. Xia Wu, Min Dai, Jianling Bai, Wenwu Long, Chuyan Long, Xianyan Tang, Hua Tu, Renjie Zhang, Cairong Zhu, Shaoqi Yang, and Heena Buch were responsible for data acquisition and Xia Wu conducted the statistical analyses. Jianling Bai provided statistical consultation. All of the authors have read and approved the final version of this manuscript. The authors would like to thank all of the participants for their time and effort.
Footnotes
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by public donated Intestine Initiative Foundation; Jiangsu Province Medical Innovation Team (Faming Zhang); National Natural Science Foundation of China (81873548); Top-notch talent research projects (LGY2017080); Project of Jiangsu Provincial Science and Technology Department (BE2018751).
Conflict of interest statement: Faming Zhang invented the concept of GenFMTer and transendoscopic enteral tubing and devices related to it. Other authors declare that there are no conflicts of interest.
ORCID iD: Faming Zhang  https://orcid.org/0000-0003-4157-1144
https://orcid.org/0000-0003-4157-1144
Data accessibility statement: All data generated or analyzed during this study are included in this published article and its supplementary information files.
Supplemental material: Supplemental material for this article is available online.
Contributor Information
Xia Wu, Medical Center for Digestive Diseases, The Second Affiliated Hospital of Nanjing Medical University, Nanjing, China.
Min Dai, Medical Center for Digestive Diseases, The Second Affiliated Hospital of Nanjing Medical University, Nanjing, China.
Heena Buch, Medical Center for Digestive Diseases, The Second Affiliated Hospital of Nanjing Medical University, Nanjing, China.
Jianling Bai, Department of Biostatistics, School of Public Health, Nanjing Medical University, Nanjing, China.
Wenwu Long, Jiangxi Medical College of Nanchang University, Nanchang, China.
Chuyan Long, Medical Center for Digestive Diseases, The Second Affiliated Hospital of Nanjing Medical University, Nanjing, China.
Xianyan Tang, Department of Epidemiology and Biostatistics, School of Public Health, Guangxi Medical University, Guangxi Zhuang Autonomous Region, China.
Hua Tu, Department of Gastroenterology, Hubei Provincial Hospital Traditional Chinese Medicine, Wuhan, China.
Renjie Zhang, Hubei University of Chinese Medicine, Wuhan, China.
Cairong Zhu, West China School of Public Health and West China Fourth Hospital, Sichuan University, Chengdu, China.
Shaoqi Yang, Department of Gastroenterology, General Hospital of Ningxia Medical University, Yinchuan, China.
Bota Cui, Medical Center for Digestive Diseases, The Second Affiliated Hospital of Nanjing Medical University, Nanjing, China.
Guozhong Ji, Medical Center for Digestive Diseases, The Second Affiliated Hospital of Nanjing Medical University, Nanjing, China.
Faming Zhang, Medical Center for Digestive Diseases, The Second Affiliated Hospital of Nanjing Medical University, 121 Jiang Jia Yuan, Nanjing, 210011, China; Key Lab of Holistic Integrative Enterology, Nanjing Medical University, 121 Jiang Jia Yuan, Nanjing, 210011, China.
References
- 1. Brandt LJ. American journal of gastroenterology lecture: intestinal microbiota and the role of fecal microbiota transplant (FMT) in treatment of C. difficile infection. Am J Gastroenterol 2013; 108: 177–185. [DOI] [PubMed] [Google Scholar]
- 2. Borody TJ, Campbell J. Fecal microbiota transplantation: techniques, applications, and issues. Gastroenterol Clin North Am 2012; 41: 781–803. [DOI] [PubMed] [Google Scholar]
- 3. Cammarota G, Ianiro G, Gasbarrini A. Fecal microbiota transplantation for the treatment of Clostridium difficile infection: a systematic review. J Clin Gastroenterol 2014; 48: 693–702. [DOI] [PubMed] [Google Scholar]
- 4. Zhang F, Luo W, Shi Y, et al. Should we standardize the 1,700-year-old fecal microbiota transplantation? Am J Gastroenterol 2012; 107: 1755; author reply pp. 1755–1756. [DOI] [PubMed] [Google Scholar]
- 5. Surawicz CM, Brandt LJ, Binion DG, et al. Guidelines for diagnosis, treatment, and prevention of Clostridium difficile infections. Am J Gastroenterol 2013; 108: 478–498; quiz 499. [DOI] [PubMed] [Google Scholar]
- 6. McDonald LC, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the infectious diseases society of America (IDSA) and society for healthcare epidemiology of America (SHEA). Clin Infect Dis 2018; 66: 987–994. [DOI] [PubMed] [Google Scholar]
- 7. Rossen NG, Fuentes S, van der Spek MJ, et al. Findings from a randomized controlled trial of fecal transplantation for patients with ulcerative colitis. Gastroenterology 2015; 149: 110–118. e4. [DOI] [PubMed] [Google Scholar]
- 8. He Z, Li P, Zhu J, et al. Multiple fresh fecal microbiota transplants induces and maintains clinical remission in Crohn’s disease complicated with inflammatory mass. Sci Rep 2017; 7: 4753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Johnsen PH, Hilpusch F, Cavanagh JP, et al. Faecal microbiota transplantation versus placebo for moderate-to-severe irritable bowel syndrome: a double-blind, randomised, placebo-controlled, parallel-group, single-centre trial. Lancet Gastroente-rol Hepatol 2018; 3: 17–24. [DOI] [PubMed] [Google Scholar]
- 10. Pinn DM, Aroniadis OC, Brandt LJ. Is fecal microbiota transplantation the answer for irritable bowel syndrome? A single-center experience. Am J Gastroenterol 2014; 109: 1831–1832. [DOI] [PubMed] [Google Scholar]
- 11. Kootte RS, Levin E, Salojarvi J, et al. Improvement of insulin sensitivity after lean donor feces in metabolic syndrome is driven by baseline intestinal microbiota composition. Cell Metab 2017; 26: 611–619.e6. [DOI] [PubMed] [Google Scholar]
- 12. Vrieze A, Van Nood E, Holleman F, et al. Transfer of intestinal microbiota from lean donors increases insulin sensitivity in individuals with metabolic syndrome. Gastroenterology 2012; 143: 913–916.e7. [DOI] [PubMed] [Google Scholar]
- 13. Ren YD, Ye ZS, Yang LZ, et al. Fecal microbiota transplantation induces hepatitis B virus e-antigen (HBeAg) clearance in patients with positive HBeAg after long-term antiviral therapy. Hepatology 2017; 65: 1765–1768. [DOI] [PubMed] [Google Scholar]
- 14. Mullish BH, McDonald JAK, Thursz MR, et al. Fecal microbiota transplant from a rational stool donor improves hepatic encephalopathy: a randomized clinical trial. Hepatology 2017; 66: 1354–1355. [DOI] [PubMed] [Google Scholar]
- 15. Routy B, Le Chatelier E, Derosa L, et al. Gut microbiome influences efficacy of PD-1-based immunotherapy against epithelial tumors. Science 2018; 359: 91–97. [DOI] [PubMed] [Google Scholar]
- 16. Wang Y, Wiesnoski DH, Helmink BA, et al. Fecal microbiota transplantation for refractory immune checkpoint inhibitor-associated colitis. Nat Med. Epub ahead of print 12 November 2018. DOI: 10.1038/s41591-018-0238-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Kang DW, Adams JB, Gregory AC, et al. Microbiota transfer therapy alters gut ecosystem and improves gastrointestinal and autism symptoms: an open-label study. Microbiome 2017; 5: 10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. He Z, Cui BT, Zhang T, et al. Fecal microbiota transplantation cured epilepsy in a case with Crohn’s disease: the first report. World J Gastroenterol 2017; 23: 3565–3568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Paramsothy S, Walsh AJ, Borody T, et al. Gastroenterologist perceptions of faecal microbiota transplantation. World J Gastroenterol 2015; 21: 10907–10914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Ren RR, Sun G, Yang YS, et al. Chinese physicians’ perceptions of fecal microbiota transplantation. World J Gastroenterol 2016; 22: 4757–4765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Ma Y, Yang J, Cui B, et al. How Chinese clinicians face ethical and social challenges in fecal microbiota transplantation: a questionnaire study. BMC Med Ethics 2017; 18: 39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Zipursky JS, Sidorsky TI, Freedman CA, et al. Patient attitudes toward the use of fecal microbiota transplantation in the treatment of recurrent Clostridium difficile infection. Clin Infect Dis 2012; 55: 1652–1658. [DOI] [PubMed] [Google Scholar]
- 23. Park L, Mone A, Price JC, et al. Perceptions of fecal microbiota transplantation for Clostridium difficile infection: factors that predict acceptance. Ann Gastroenterol 2017; 30: 83–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Zeitz J, Bissig M, Barthel C, et al. Patients’ views on fecal microbiota transplantation: an acceptable therapeutic option in inflammatory bowel disease? Eur J Gastroenterol Hepatol 2017; 29: 322–330. [DOI] [PubMed] [Google Scholar]
- 25. Orduna P, Lopez SY, Schmulson M, et al. A survey using the social networks revealed poor knowledge on fecal microbiota transplantation. J Neurogastroenterol Motil 2015; 21: 294–295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Cui B, Li P, Xu L, et al. Step-up fecal microbiota transplantation (FMT) strategy. Gut Microbes 2016; 7: 323–328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Zhang F, Cui B, He X, et al. Microbiota transplantation: concept, methodology and strategy for its modernization. Protein Cell 2018; 9: 462–473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Peng Z, Xiang J, He Z, et al. Colonic transendoscopic enteral tubing: a novel way of transplanting fecal microbiota. Endosc Int Open 2016; 4: E610–E613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Long C, Yu Y, Cui B, et al. A novel quick transendoscopic enteral tubing in mid-gut: technique and training with video. BMC Gastroenterol 2018; 18: 37. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, Data1 for The recognition and attitudes of postgraduate medical students toward fecal microbiota transplantation: a questionnaire study by Xia Wu, Min Dai, Heena Buch, Jianling Bai, Wenwu Long, Chuyan Long, Xianyan Tang, Hua Tu, Renjie Zhang, Cairong Zhu, Shaoqi Yang, Bota Cui, Guozhong Ji and Faming Zhang in Therapeutic Advances in Gastroenterology
Supplemental material, Questionnaire for The recognition and attitudes of postgraduate medical students toward fecal microbiota transplantation: a questionnaire study by Xia Wu, Min Dai, Heena Buch, Jianling Bai, Wenwu Long, Chuyan Long, Xianyan Tang, Hua Tu, Renjie Zhang, Cairong Zhu, Shaoqi Yang, Bota Cui, Guozhong Ji and Faming Zhang in Therapeutic Advances in Gastroenterology
Supplemental material, Supplementary_table for The recognition and attitudes of postgraduate medical students toward fecal microbiota transplantation: a questionnaire study by Xia Wu, Min Dai, Heena Buch, Jianling Bai, Wenwu Long, Chuyan Long, Xianyan Tang, Hua Tu, Renjie Zhang, Cairong Zhu, Shaoqi Yang, Bota Cui, Guozhong Ji and Faming Zhang in Therapeutic Advances in Gastroenterology