
FIGURE 1.
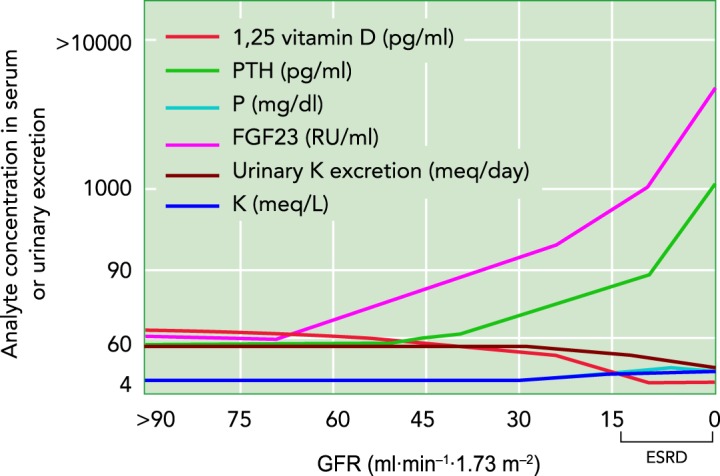
Impairment of the kidneys’ ability to maintain body homeostasis when GFR, and potentially nephron number, is declining
CKD stages 2, 3, 4, and 5 correspond to GFR values (in ml·min−1·1.73 m−2) of 60-89, 30-59, 15-29, and 0-15 (=ESRD), respectively. The blood levels of phosphaturic fibroblast growth factor 23 (FGF23) and parathyroid hormone (PTH) rise with decreasing GFR, and thus filtered phosphate, to maintain renal phosphate excretion and plasma phosphate concentrations. Hyperphosphatemia occurs in CKD stages 4 and 5, primarily as a result of the reduction in GFR. FGF23 inhibits renal conversion of inactive vitamin D to active 1,25 vitamin D, whereas PTH increases this conversion. Blood levels of FGF23 rise in CKD stage 2 and before PTH, the latter increasing in CKD stage 3, thus causing a decrease in active 1,25 vitamin D. Urinary potassium excretion decreases starting in CKD stage 4; serum potassium concentrations increase but remain within normal range through adaptive renal and non-renal mechanisms. Of note, serum potassium and phosphorous graphically overlap to a large extent. Adapted from Ref. 47, with permission from Kidney Research and Clinical Practice, and Ref. 52, with permission from the Journal of the American Society of Nephrology.