

Purpose of review
Hyperventilation is commonly used in neurological patients to decrease elevated intracranial pressure (ICP) or relax a tense brain. However, the potentially deleterious effects of hyperventilation may limit its clinical application. The aim of this review is to summarize the physiological and outcome evidence related to hyperventilation in neurological patients.
Recent findings
Physiologically, hyperventilation may adversely decrease cerebral blood flow (CBF) and the match between the cerebral metabolic rate and CBF. In patients with severe traumatic brain injury (TBI), prolonged prophylactic hyperventilation with arterial carbon dioxide tension (PaCO2) less than 25 mmHg or during the first 24 h after injury is not recommended. Most patients (>90%) with an aneurysmal subarachnoid hemorrhage undergo hyperventilation (PaCO2 <35 mmHg); however, whether hyperventilation is associated with poor outcomes in this patient population is controversial. Hyperventilation is effective for brain relaxation during craniotomy; however, this practice is not based on robust outcome evidence.
Summary
Although hyperventilation is commonly applied in patients with TBI or intracranial hemorrhage or in those undergoing craniotomy, its effects on patient outcomes have not been proven by quality research. Hyperventilation should be used as a temporary measure when treating elevated ICP or to relax a tense brain. Outcome research is needed to better guide the clinical use of hyperventilation in neurological patients.
Keywords: craniotomy, hyperventilation, hypocapnia, intracranial hemorrhage, outcome, traumatic brain injury
INTRODUCTION
Hyperventilation is frequently used in neurological patients based on the fact that the hyperventilation-induced hypocapnia has profound effects on cerebral physiology. It is well known that carbon dioxide (CO2) is a powerful modulator of cerebral vasomotor tone, and hypocapnia leads to cerebral vasoconstriction, whereas hypercapnia causes cerebral vasodilation.
We use hyperventilation to decrease elevated intracranial pressure (ICP) [1] and relax a tense brain (i.e. to make it smaller and softer) [2,3] because hypocapnia leads to reduced cerebral blood flow (CBF) [4] and cerebral blood volume (CBV) [5]. Interestingly, this common practice is not based on robust evidence [6]. In contrast, a randomized controlled trial (RCT) performed in patients with severe head injury suggested that prolonged prophylactic hyperventilation may be deleterious [7]. One major concern with multihour and forced hyperventilation is hypocapnia-induced CBF reduction [4,8].
Therefore, hyperventilation is a double-edged sword that brings both benefits and risks. As ventilation is an adjustable physiological variable, it is pertinent to understand how to best manage ventilation to avoid doing more harm than good. The present review aims to summarize the relevant physiology and outcome evidence related to hyperventilation in neurological patients.
Box 1.
no caption available
PHYSIOLOGICAL EFFECTS OF HYPERVENTILATION ON NORMAL AND INJURED BRAIN
Hyperventilation lowers ICP and relaxes the brain [5]. These two phenomena are related: ICP is the ICP measured with the cranium closed and is determined by all of the contents of the cranium, whereas brain relaxation refers to the size and firmness of the brain in relation to the capacity of the bony cranium typically assessed by the surgeon during craniotomy [2]. Hyperventilation leads to cerebral vasoconstriction-related reduction of the CBV, one of the components of the intracranial contents; thereby, it decreases ICP and relaxes the brain.
It is notable that CBF and CBV are related but different: CBF is the blood volume that perfuses the brain per unit time (i.e. a dynamic concept), whereas CBV is the volume of the blood within the brain (i.e. a static concept). In healthy volunteers, hyperventilation leads to an approximately 30% decrease in CBF but only a 7% decrease in the CBV when arterial blood CO2 partial pressure (PaCO2) is decreased from normocapnia (∼41 mmHg) to hypocapnia (∼25 mmHg) [9]. In patients with TBI, hyperventilation leads to an approximately 34% decrease in CBF and a 9% decrease in CBV when the PaCO2 is decreased from ∼40 to ∼30 mmHg for 30 min [10]. The different magnitudes of change in CBF and CBV highlight that CBF and CBV are different but related measurements.
Hypocapnia induced by hyperventilation may increase cerebral metabolic activity through several different mechanisms. Hypocapnia increases neuronal excitability and seizure duration, which leads to increased oxygen and glucose consumption, excitatory amino acids production, and a switch to anaerobic metabolism [11–13]. Alkalosis may also lead to a leftward shift of the oxygen–hemoglobin dissociation curve and an inhibition of the usual negative feedback by which a low pH limits the production of endogenous organic acids [14]. These effects of hyperventilation, in addition to the CBF reduction-related decrease in oxygen supply, tilts the cerebral consumption–supply balance further towards more demand than supply [11].
The effects of hyperventilation on a normal brain or an injured brain in patients with acute cerebral injury are different. Although hyperventilation reduces CBF in both the normal and the injured brain [15–18], the CBF reduction is more profound in the normal than the injured brain because hyperventilation redistributes CBF from normal brain tissues to injured brain tissues [13,19]. This is consistent with the observation that luxury perfusion (i.e. regional hyperemia) mainly occurs in the injured brain in patients with acute cerebral injury [20].
Studies have suggested that hyperventilation may adversely affect cerebral metabolism or oxygenation in patients with TBI [17,21]. Coles et al.[22] showed that hyperventilation (PaCO2 from 36 to 29 mmHg for 10 min) led to a slightly increased cerebral metabolic rate of oxygen (CMRO2) from 78 to 81 μmol/100 ml/min in patients with TBI. Soustiel et al. found that following moderate hyperventilation (PaCO2 from 36 to 32 mmHg for 20 min), jugular venous oxygen saturation (SvjO2) and the cerebral metabolic rate of lactate and oxygen decreased, whereas the cerebral metabolic rate of glucose increased in patients with TBI [21]. These findings were corroborated by a different study that showed that hyperventilation (PaCO2 from 36 to 29 mmHg for 10 min) led to a decrease in SvjO2 from 72 to 60% and an increase in arteriovenous oxygen content differences (AVDO2) from 3.7 to 5.6% in patients with TBI [17]. However, although decreased, the SvjO2 values in these studies were still within the normal range.
In contrast, some studies did not find a significant impact of hyperventilation on cerebral metabolic activity in patients with TBI [10,17,23,24]. Brandi et al.[23] showed that 50 min of moderate hyperventilation (PaCO2 from 35 to 30 mmHg) did not change the glucose, lactate, or pyruvate profiles in the extracellular fluid of the brain in patients with TBI, although brain tissue oxygen tension measured by a Clark-type microcatheter was slightly decreased from 32 to 30 mmHg (the normal range > 15 mmHg). Diringer et al.[24] showed that the global CMRO2 did not change, although the global oxygen extraction fraction increased from 0.31 to 0.45 and from 0.23 to 0.44 in patients with severe TBI following moderate (PaCO2 = 30 mmHg less than 24 h) and severe (PaCO2 = 25 mmHg for 1–5 days) hyperventilation, respectively.
In summary, hyperventilation has significant effects on cerebral physiology, including cerebral blood flow, blood volume, and metabolic activity. Hyperventilation-related reduction of CBF may lead to suboptimal or insufficient cerebral perfusion, whereas CBV reduction causes brain relaxation and ICP reduction. The consequences of the impact on cerebral metabolic activity remain to be determined. The physiological effects of hyperventilation on normal and injured brains are illustrated in Fig. 1.
FIGURE 1.
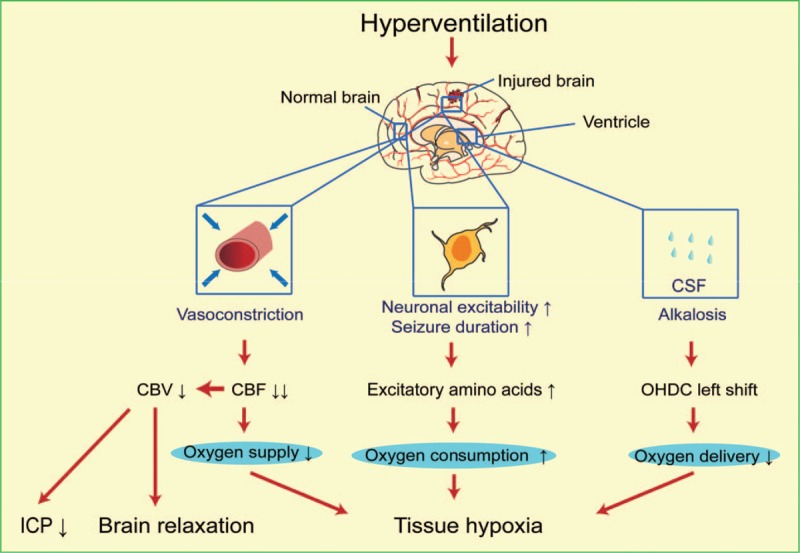
The effects of hyperventilation in an injured brain. Hyperventilation causes cerebral vasoconstriction, which reduces cerebral blood flow and volume to decrease the oxygen supply in both normal and injured areas. Hyperventilation decreases the intracranial pressure and relaxes the brain. Hyperventilation increases neuronal excitability and seizure duration, which contribute to damaged brain metabolism. Hyperventilation also causes cerebrospinal fluid to alkalinize, pH to rise, and oxygen delivery to decrease. CSF, cerebrospinal fluid; CBV, cerebral blood volume; CBF, cerebral blood flow; OHDC, oxygen-hemoglobin dissociation curve; ICP, intracranial pressure.
HYPERVENTILATION IN TRAUMATIC BRAIN INJURY
One of the therapeutic priorities in patients with TBI is to control the ICP because intracranial hypertension, which occurs frequently in this patient population, threatens the integrity of the brain and adversely affects the neurological outcome. Hyperventilation is a commonly used therapeutic option for ICP reduction [25]. In Europe, early prophylactic hyperventilation (targeting a PaCO2 ≤ 35 mmHg within 24 h after TBI) is still applied in more than half of patients with TBI [26]. However, prolonged and overzealous prophylactic hyperventilation may do more harm than good. In patients with severe TBI, one guideline does not recommend prolonged prophylactic hyperventilation targeting a PaCO2 ≤ 25 mmHg [27]. This guideline also suggests that hyperventilation targeting a PaCO2 ≤ 35 mmHg should be avoided during the first 24 h after injury but is recommended as a temporizing measure for ICP reduction after 24 h [27].
A systematic review based on six studies concluded that both hypocapnia and hypercapnia after cerebral injury are associated with poor patient outcomes [28]. One RCT compared two different levels of PaCO2 (25 vs. 35 mmHg) based on different ventilation protocols for 5 days in 77 patients with severe closed head injury [7]. The numbers of cases with a favorable outcome (defined as good and moderate disability according to the Glasgow Outcome Scale) were significantly different after 3 months (3 vs. 10) and 6 months (4 vs. 12) but not after 12 months (7 vs. 12) between groups with a PaCO2 of 25 and 35 mmHg, respectively. These outcome differences occurred only in patients with a severe head injury with a motor score more than 3 but not 3 or less on the Glasgow Coma Scale (GCS). In this study, the authors did not distinguish between adult and pediatric patients; they also kept the PaCO2 at 30–35 mmHg in the control group, a level that was actually the result of moderate hyperventilation. Despite these limitations, this RCT is unique in investigating the effect of hyperventilation on neurological outcomes in head-injured patients.
One multicenter retrospective study found that an arrival PaCO2 < 30 mmHg or > 49 mmHg was associated with reduced rates of survival or good outcomes (defined as discharge to home, jail, or a psychiatric facility; rehabilitation; or signing out against medical advice) in intubated patients with TBI [29]. A different retrospective study showed that children with an admission PaCO2 between 36 and 46 mmHg had a greater discharge survival compared with those with either admission hypocapnia or hypercapnia [30]. Cold et al. showed that hyperventilation (PaCO2 from 36 to 26 mmHg) increased the frequency of regional CBF less than 15 ml/100 g/min, a critically low level related to poor outcomes including dementia, vegetative survival or death, from 0.1 to 3% in patients with acute comatose head injury [31].
However, not every study demonstrated a detrimental effect of hyperventilation in patients with TBI. One study investigated the relationship between different PaCO2 levels at admission and mortality in 492 patients with severe TBI and intubation before hospital arrival. This study showed that patients with a PaCO2 ranging from 30 to 35 mmHg had the lowest mortality (16.1%), whereas patients with a PaCO2 more than 45 mmHg had the highest mortality (36.2%). The mortality in patients with a PaCO2 level less than 30 mmHg and 36–45 mmHg was 25.2 and 26.6%, respectively. There were no significant differences in the discharge GCS, functional independence measure score, or intensive care unit length of stay among the groups [32].
The overall evidence suggests that prolonged excessive ventilation may lead to worse outcomes in patients with TBI. Prolonged prophylactic hyperventilation targeting a PaCO2 less than 25 mmHg or during the first 24 h after injury when the CBF is frequently decreased to a critically low level is not recommended. Hyperventilation should be used as a temporary measure to reduce the ICP in this patient population, and when it is applied, the adequacy of tissue perfusion and oxygenation should be simultaneously monitored based on parameters such as SjvO2 and brain tissue oxygen partial pressure [27].
HYPERVENTILATION IN PATIENTS WITH HEMORRHAGIC STROKE
Spontaneous intracranial hemorrhage is associated with a high mortality and disability [33]. Hyperventilation is frequently applied in this patient population to temporarily decrease an elevated ICP and prevent an impending herniation [34].
Hyperventilation may further deteriorate an already decreased CBF in subarachnoid hemorrhage (SAH). Von Helden et al.[35] showed that hyperventilation (PaCO2 from 35 to 28 mmHg for 20 min) dropped the SjvO2 from 60 to 50% and increased the mean blood flow velocity from 88 to 160 cm/s in the first 3 days in patients with an SAH. They also showed that, during the same degree of hyperventilation, a SjvO2 below 55% was observed in more than 50% of comatose patients secondary to intracerebral hemorrhage, SAH, and head injury [35].
There is limited evidence pertaining to the effect of hyperventilation on neurological outcomes in patients with intracranial hemorrhage. One study found that hypocapnia (PaCO2 <35 mmHg) occurred in 92% of ventilated patients with aneurysmal SAH (n = 102) [36]. This study also showed that the duration (7 days) of hypocapnia was associated with unfavorable outcomes (Glasgow Outcome Scale < 4) and symptomatic vasospasm, but the ICU length of stay and hospital mortality were not associated with this duration [36]. A different study found that 78% of patients with PaCO2 more than 48 or less than 30 mmHg had unfavorable neurological outcomes (modified Rankin scale score 3–6), whereas 23% of patients with PaCO2 between 30 and 48 mmHg had the same outcome [37]. Both studies suggested deleterious effects associated with hyperventilation in patients with SAH.
However, not every study demonstrated a detrimental effect of hyperventilation in patients with intracranial hemorrhage. A retrospective study performed in 1099 patients with endovascular coiling or surgical clipping for SAH found that neither blood pressure (MAP < 60 mmHg) nor end-tidal CO2 (< 30 mmHg) was significantly associated with the Glasgow Outcome Scale at discharge or three months after discharge [38▪].
Different studies showed that hypercapnia (PaCO2 from 30 to 40, 50, and 60 mmHg at a 15 min interval) via hypoventilation increased CBF (from 77 to 98, 124, and 143% of baseline, respectively) and improved the brain metabolism profile (brain tissue oxygen saturation increased from 94 to 99%, 105, and 111% of baseline, respectively) in patients with SAH [39,40]. However, the therapeutic effect of hypercapnia in this patient population remains to be further determined [39–41].
In summary, the effect of hyperventilation in patients with intracranial hemorrhage remains controversial. Prolonged and nondiscriminative use of hyperventilation may do more harm than good. The value of hypoventilation remains elusive.
HYPERVENTILATION DURING CRANIOTOMY
Hyperventilation is commonly used during craniotomy to render a smaller and softer brain to improve the operating condition (i.e. brain relaxation) [2]. However, the concern is whether hypocapnia may compromise cerebral perfusion of the normal brain at the same time. Clearly, optimal operating conditions and cerebral perfusion should be balanced during the management of ventilation.
A multicenter randomized crossover trial compared normal ventilation (PaCO2 37 mmHg) with hyperventilation (PaCO2 25 mmHg) in patients who underwent supratentorial brain tumor surgery (n = 275). The trial found that hyperventilation decreased the ICP from 16 to 12 mmHg, decreased the risk of increased brain bulk by 45%, and improved brain relaxation, as assessed by surgeons [3].
In summary, hyperventilation is still a common method to induce brain relaxation during craniotomy. There is still a lack of evidence on the relationship between hyperventilation and neurological outcome in patients having craniotomy.
CLINICAL IMPLICATIONS
Hyperventilation has been used in neurological patients for decades; however, whether its application has improved patient outcomes remains unclear. Hyperventilation rapidly reduces ICP and relaxes the brain. However, it also decreases CBF in both normal and injured brains. The overriding principle in the clinical application of hyperventilation is the balance between the therapeutic effects on intracranial hypertension and the deleterious effect of CBF reduction. Although still lacking quality evidence, hyperventilation should only be selectively used in situations where its therapeutic effects outweigh its deleterious effect. It is ideal to have a monitor that assesses the adequacy of cerebral perfusion during the application of hyperventilation [42].
CONCLUSION
Hyperventilation is commonly used in neurological patients to decrease ICP and relax the brain. The therapeutic effect and the deleterious effect associated with hyperventilation should be balanced in decision-making. Hyperventilation appears to be well tolerated when applied during craniotomy; however, its effects on neurological outcomes in patients with TBI or intracranial hemorrhage remain unclear. How to best use hyperventilation in neurological patients clearly needs further research.
Acknowledgements
The authors would like to thank Dr Lingzhong Meng from the Department of Anesthesiology at Yale University School of Medicine for his gracious help in improving the quality of this manuscript.
Financial support and sponsorship
None.
Conflicts of interest
There are no conflicts of interest.
REFERENCES AND RECOMMENDED READING
Papers of particular interest, published within the annual period of review, have been highlighted as:
▪ of special interest
▪▪ of outstanding interest
REFERENCES
- 1.Kinoshita K. Traumatic brain injury: pathophysiology for neurocritical care. J Intensive Care 2016; 4:29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Li J, Gelb AW, Flexman AM, et al. Definition, evaluation, and management of brain relaxation during craniotomy. Br J Anaesth 2016; 116:759–769. [DOI] [PubMed] [Google Scholar]
- 3.Gelb AW, Craen RA, Rao GS, et al. Does hyperventilation improve operating condition during supratentorial craniotomy? A multicenter randomized crossover trial. Anesth Analg 2008; 106:585–594. table of contents. [DOI] [PubMed] [Google Scholar]
- 4.Meng L, Gelb AW. Regulation of cerebral autoregulation by carbon dioxide. Anesthesiology 2015; 122:196–205. [DOI] [PubMed] [Google Scholar]
- 5.Akca O. Optimizing the intraoperative management of carbon dioxide concentration. Curr Opin Anaesthesiol 2006; 19:19–25. [DOI] [PubMed] [Google Scholar]
- 6.Laffey JG, Kavanagh BP. Hypocapnia. N Engl J Med 2002; 347:43–53. [DOI] [PubMed] [Google Scholar]
- 7.Muizelaar JP, Marmarou A, Ward JD, et al. Adverse effects of prolonged hyperventilation in patients with severe head injury: a randomized clinical trial. J Neurosurg 1991; 75:731–739. [DOI] [PubMed] [Google Scholar]
- 8.Adams RW, Gronert GA, Sundt TM, Jr, Michenfelder JD. Halothane, hypocapnia, and cerebrospinal fluid pressure in neurosurgery. Anesthesiology 1972; 37:510–517. [DOI] [PubMed] [Google Scholar]
- 9.Fortune JB, Feustel PJ, deLuna C, et al. Cerebral blood flow and blood volume in response to O2 and CO2 changes in normal humans. J Trauma 1995; 39:463–471. discussion 471-462. [DOI] [PubMed] [Google Scholar]
- 10.Diringer MN, Yundt K, Videen TO, et al. No reduction in cerebral metabolism as a result of early moderate hyperventilation following severe traumatic brain injury. J Neurosurg 2000; 92:7–13. [DOI] [PubMed] [Google Scholar]
- 11.Godoy DA, Seifi A, Garza D, et al. Hyperventilation Therapy for Control of Posttraumatic Intracranial Hypertension. Front Neurol 2017; 8:250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Carey BJ. Hypocapnia. N Engl J Med 2002; 347:1533.author reply 1533. [DOI] [PubMed] [Google Scholar]
- 13.Curley G, Kavanagh BP, Laffey JG. Hypocapnia and the injured brain: more harm than benefit. Crit Care Med 2010; 38:1348–1359. [DOI] [PubMed] [Google Scholar]
- 14.Hood VL, Tannen RL. Protection of acid-base balance by pH regulation of acid production. N Engl J Med 1998; 339:819–826. [DOI] [PubMed] [Google Scholar]
- 15.Stringer WA, Hasso AN, Thompson JR, et al. Hyperventilation-induced cerebral ischemia in patients with acute brain lesions: demonstration by xenon-enhanced CT. AJNR Am J Neuroradiol 1993; 14:475–484. [PMC free article] [PubMed] [Google Scholar]
- 16.Ojha BK, Jha DK, Kale SS, Mehta VS. Trans-cranial Doppler in severe head injury: evaluation of pattern of changes in cerebral blood flow velocity and its impact on outcome. Surg Neurol 2005; 64:174–179. discussion 179. [DOI] [PubMed] [Google Scholar]
- 17.Coles JP, Minhas PS, Fryer TD, et al. Effect of hyperventilation on cerebral blood flow in traumatic head injury: clinical relevance and monitoring correlates. Crit Care Med 2002; 30:1950–1959. [DOI] [PubMed] [Google Scholar]
- 18.Jagersberg M, Schaller C, Bostrom J, et al. Simultaneous bedside assessment of global cerebral blood flow and effective cerebral perfusion pressure in patients with intracranial hypertension. Neurocrit Care 2010; 12:225–233. [DOI] [PubMed] [Google Scholar]
- 19.Darby JM, Yonas H, Marion DW, Latchaw RE. Local ‘inverse steal’ induced by hyperventilation in head injury. Neurosurgery 1988; 23:84–88. [DOI] [PubMed] [Google Scholar]
- 20.Broich K, Alavi A, Cruz J, et al. Evidence of ‘regional hyperemia’ in patients with severe closed head injury using single-photon emission computed tomography. J Stroke Cerebrovasc Dis 1994; 4:271–274. [DOI] [PubMed] [Google Scholar]
- 21.Soustiel JF, Mahamid E, Chistyakov A, et al. Comparison of moderate hyperventilation and mannitol for control of intracranial pressure control in patients with severe traumatic brain injury–a study of cerebral blood flow and metabolism. Acta Neurochir (Wien) 2006; 148:845–851. discussion 851. [DOI] [PubMed] [Google Scholar]
- 22.Coles JP, Fryer TD, Coleman MR, et al. Hyperventilation following head injury: effect on ischemic burden and cerebral oxidative metabolism. Crit Care Med 2007; 35:568–578. [DOI] [PubMed] [Google Scholar]
- 23.Brandi G, Stocchetti N, Pagnamenta A, et al. Cerebral metabolism is not affected by moderate hyperventilation in patients with traumatic brain injury. Crit Care 2019; 23:45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Diringer MN, Videen TO, Yundt K, et al. Regional cerebrovascular and metabolic effects of hyperventilation after severe traumatic brain injury. J Neurosurg 2002; 96:103–108. [DOI] [PubMed] [Google Scholar]
- 25.Ghajar J, Hariri RJ, Narayan RK, et al. Survey of critical care management of comatose, head-injured patients in the United States. Crit Care Med 1995; 23:560–567. [DOI] [PubMed] [Google Scholar]
- 26.Neumann JO, Chambers IR, Citerio G, et al. The use of hyperventilation therapy after traumatic brain injury in Europe: an analysis of the BrainIT database. Intensive Care Med 2008; 34:1676–1682. [DOI] [PubMed] [Google Scholar]
- 27.Carney N, Totten AM, O’Reilly C, et al. Guidelines for the management of severe traumatic brain injury, fourth edition. Neurosurgery 2017; 80:6–15. [DOI] [PubMed] [Google Scholar]
- 28.Roberts BW, Karagiannis P, Coletta M, et al. Effects of PaCO2 derangements on clinical outcomes after cerebral injury: A systematic review. Resuscitation 2015; 91:32–41. [DOI] [PubMed] [Google Scholar]
- 29.Davis DP, Idris AH, Sise MJ, et al. Early ventilation and outcome in patients with moderate to severe traumatic brain injury. Crit Care Med 2006; 34:1202–1208. [DOI] [PubMed] [Google Scholar]
- 30.Ramaiah VK, Sharma D, Ma L, et al. Admission oxygenation and ventilation parameters associated with discharge survival in severe pediatric traumatic brain injury. Childs Nerv Syst 2013; 29:629–634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Cold GE. Does acute hyperventilation provoke cerebral oligaemia in comatose patients after acute head injury? Acta Neurochir (Wien) 1989; 96:100–106. [DOI] [PubMed] [Google Scholar]
- 32.Warner KJ, Cuschieri J, Copass MK, et al. The impact of prehospital ventilation on outcome after severe traumatic brain injury. J Trauma 2007; 62:1330–1336. discussion 1336–1338. [DOI] [PubMed] [Google Scholar]
- 33.Caceres JA, Goldstein JN. Intracranial hemorrhage. Emerg Med Clin North Am 2012; 30:771–794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Ravishankar N, Nuoman R, Amuluru K, et al. Management strategies for intracranial pressure crises in subarachnoid hemorrhage. J Intensive Care Med 2018; [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 35.von Helden A, Schneider GH, Unterberg A, Lanksch WR. Monitoring of jugular venous oxygen saturation in comatose patients with subarachnoid haemorrhage and intracerebral haematomas. Acta Neurochir Suppl (Wien) 1993; 59:102–106. [DOI] [PubMed] [Google Scholar]
- 36.Solaiman O, Singh JM. Hypocapnia in aneurysmal subarachnoid hemorrhage: incidence and association with poor clinical outcomes. J Neurosurg Anesthesiol 2013; 25:254–261. [DOI] [PubMed] [Google Scholar]
- 37.Yokoyama S, Hifumi T, Okazaki T, et al. Association of abnormal carbon dioxide levels with poor neurological outcomes in aneurysmal subarachnoid hemorrhage: a retrospective observational study. J Intensive Care 2018; 6:83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38▪.Akkermans A, van Waes JA, Peelen LM, et al. Blood pressure and end-tidal carbon dioxide ranges during aneurysm occlusion and neurologic outcome after an aneurysmal subarachnoid hemorrhage. Anesthesiology 2019; 130:92–105. [DOI] [PubMed] [Google Scholar]; This study describes the relationship between the blood pressure, end-tidal carbon dioxide, and the neurological outcome in patients with aneurysmal subarachnoid hemorrhage. This study is a large-scale newest study, may have import different opinions that low blood pressure and low or high end-tidal carbon dioxide have no relationship with neurological outcome.
- 39.Westermaier T, Stetter C, Kunze E, et al. Controlled hypercapnia enhances cerebral blood flow and brain tissue oxygenation after aneurysmal subarachnoid hemorrhage: results of a phase I study. Neurocrit Care 2016; 25:205–214. [DOI] [PubMed] [Google Scholar]
- 40.Westermaier T, Stetter C, Kunze E, et al. Controlled transient hypercapnia: a novel approach for the treatment of delayed cerebral ischemia after subarachnoid hemorrhage? J Neurosurg 2014; 121:1056–1062. [DOI] [PubMed] [Google Scholar]
- 41.Manley GT, Hemphill JC, Morabito D, et al. Cerebral oxygenation during hemorrhagic shock: perils of hyperventilation and the therapeutic potential of hypoventilation. J Trauma 2000; 48:1025–1032. discussion 1032–1023. [DOI] [PubMed] [Google Scholar]
- 42.Meng L, Gelb AW, Alexander BS, et al. Impact of phenylephrine administration on cerebral tissue oxygen saturation and blood volume is modulated by carbon dioxide in anaesthetized patients. Br J Anaesth 2012; 108:815–822. [DOI] [PMC free article] [PubMed] [Google Scholar]