
Figure 1.
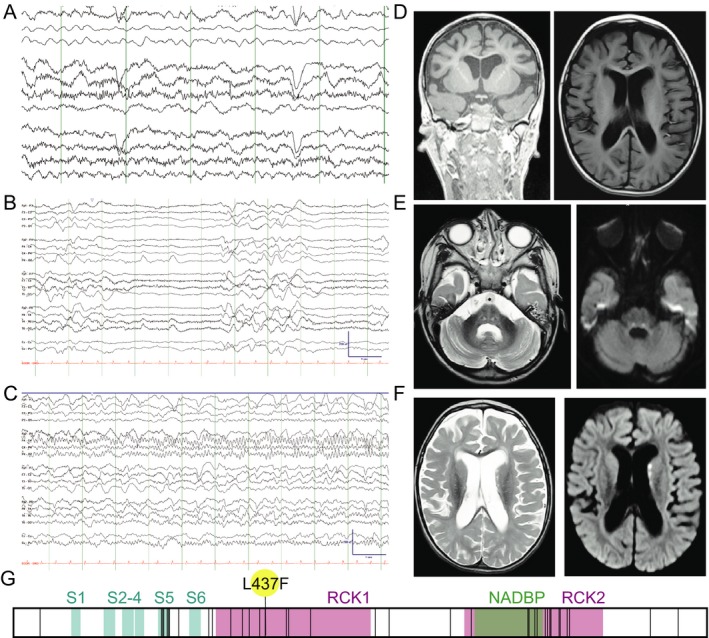
A proband with a de novo KCNT1‐L437F variant. (A–C) EEG at age 4 years old. (A) Awake cerebral electrical activity was characterized by a moderately disorganized background without a discernible posterior dominant rhythm. There was a moderate excess of delta activity diffusely. There were occasional small‐amplitude, multifocal spike wave discharges. (B) Deeper stages of sleep were marked by bursts of diffuse slowing alternating with epochs of severe (~10 μV) diffuse attenuation of voltage lasting 2–6 sec, giving the record a discontinuous appearance. (C) Example of an electroclinical focal seizure. On the video, the semiology was fairly stereotyped and characterized by a combination of upward and rightward eye deviation, eye blinking, change in breathing, chin quivering, jaw movements, and limb jerking. At the offset, the patient often coughed or sighed. Duration ~1–2 min. Electrographically, the onset was fairly stereotyped with focal rhythmic alpha activity in the right parietal region that typically spread (shown here) to the right posterior temporal region and then the remainder of the right hemisphere and then the left hemisphere. Offset was gradual and followed by diffuse background slowing. (D) Baseline MRI was notable for hydrocephalus ex vacuo. (E and F) MRI obtained at time of status dystonicus is notable for bilateral restricted diffusion in the basal ganglia, corticospinal, and pontine tracts. (G) Schematic of the KCNT1 coding sequence (from NM_020822.2) where all variants reported pathogenic in HGMD (6/24/19) are denoted by vertical lines superimposed on the transmembrane (S1–S6), regulator of potassium conductance (RCK), and NAD binding protein (NADBP) domains, with the proband variant (L437F) flagged.