

Abstract
Aim
The aim of this investigation was to develop a standardised method for using the inverse planning module in Leksell GammaPlan.
Methods
Leksell GammaPlan version 10 and higher contains an inverse planning module, consisting of functions to automatically fill a target volume with shots and subsequently optimise their resulting dosimetry. A standardised method for using the inverse planning module was developed for metastases, using the following optimisation parameter weightings: {coverage 0.9, selectivity 0.1, gradient index (GI) 0.2, }. 25 plans produced using these parameters were compared to manually produced clinical plans. Additionally, the 25 plans were manually adjusted to match the coverage of the clinical plans, and comparison of the PCI, GI and BOT was made.
Results
The average parameters for plans produced using the optimisation module were; coverage 98.7%; Paddick conformity index (PCI) 0.85; GI 2.75, compared to coverage 99.5%; PCI 0.83; GI 2.70 for manual clinical plans with BOT 21% shorter than clinical plans on average. The average parameters for the plans produced by the optimisation module after manual adjustment to match the coverage of the clinical plans were: coverage 99.5, PCI 0.83, GI 2.73 with BOT 16% shorter than clinical plans on average.
Conclusions
The standardised method for using the optimisation module has potential for shortening treatment times and planning times.
Keywords: Gamma Knife, inverse planning, optimiser, stereotactic radiosurgery
Introduction
Gamma Knife treatments are traditionally forward planned, with users positioning shots and adjusting their collimation and weighting manually, a process which requires considerable skill and experience. Version 10 of the Leksell GammaPlan (LGP) treatment planning system (Elekta Instrument AB, Stockholm, Sweden) included an interactive Inverse Planning (IP) module, which consists of two separate functions:
An auto-fill function, which uses a geometric packing approach to fill the target volume with shots. The user determines whether the use of composite shots is permitted. If the use of composite shots is permitted, the user selects whether the auto-fill function favours large or small shots. If the use of composite shots is not allowed, then the user selects which collimation sizes are permitted.
- An optimisation function which adjust the weights, positions and collimation setting of the shots, using a simulated annealing algorithm to maximise the following cost function:

Where C is coverage, S is selectivity, α, β and γ are user defined parameters and Grad and Time are defined as shown in Figure 1. Therefore increasing α penalises poor coverage, decreasing α penalises poor selectivity, increasing β penalises poor gradient index and increasing γ penalises poor beam on time.1
Figure 1.
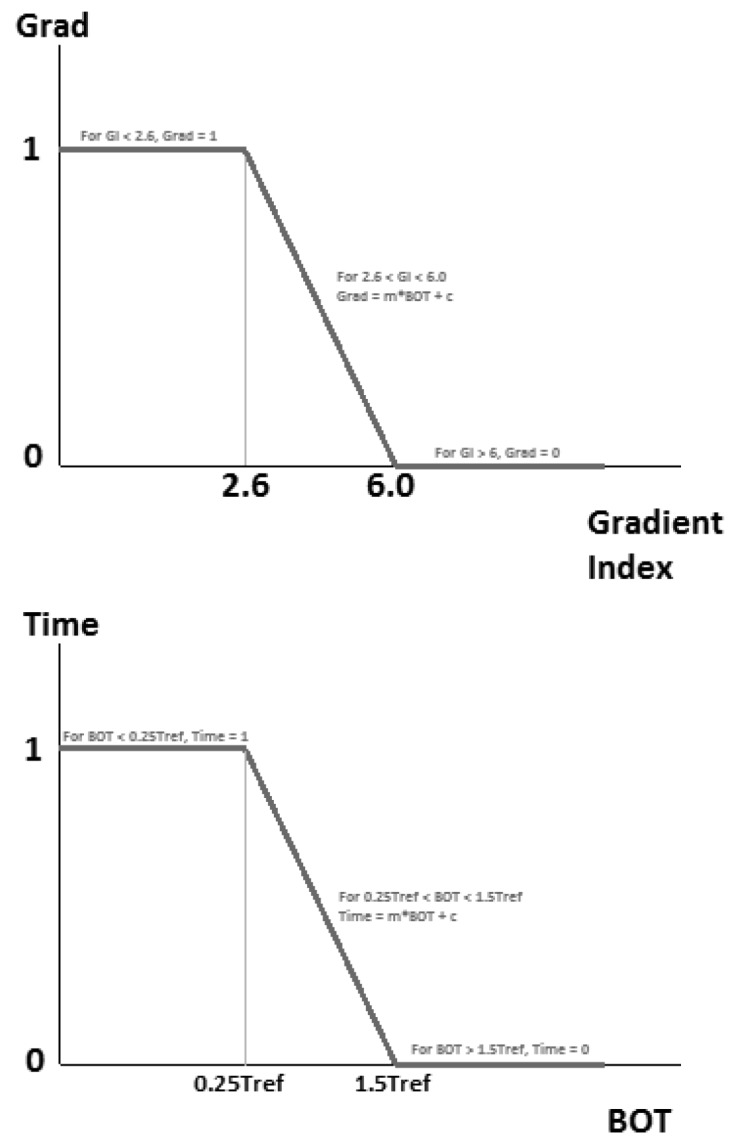
The definition of Grad is shown in the top image. Gradient indices above 2.6 are penalised (this has been changed to 2,3 in versions 11.0.2 and later). The definition of the Time parameter is shown in the bottom image. Tref is defined as the BOT at the start of the optimisation.
In version 11.0.2, the lower limit at which the gradient index parameter has a value >1 was changed from 2.6 to 2.3.2
The aim of this study was to produce a standardised method for using the IP module that could be used by both experienced and inexperienced planners to consistently produce clinically acceptable plans.
Methods and Materials
This study was performed using LGP version 11.0.3.
All plan comparisons in this study were based on target coverage, PCI, GI and BOT, defined as follows:3,4



Where PIV is the prescription isodose volume, PIV(50) is the volume of the half prescription isodose and TV is the target volume.
Shot filling
A preliminary investigation into the IP’s ‘Fill’ function performed prior to this study indicated that it tends to produce sets of shots that the authors believe to be a poor starting point for the subsequent optimiser function If composite shots are permitted, it was found that the resulting shot distribution contained many highly complex shots consisting of multiple collimator sizes. This is undesirable as it leads to long treatment times, high GI and less conformal lower isodoses. Not permitting the use of composite shots avoids this problem, however the geometric packing approach used by the autofill function does not allow for overlap of shots, which is necessary to create an efficient plan.5 Consequently, using the autofill function in this manner produces shot combinations with a high proportion of small shots. To illustrate this, for the sample of 25 cases described in section 2.3.1, the average shot size proportions for the clinical plans were 16mm: 20%, 8mm: 64%, 4mm:16% whereas using the autofill function they were 16mm: 3%, 8mm: 16%, 4mm: 81%.
Therefore, in this study, the auto fill function was not used. Instead, for all treatment plans produced in this study, the preliminary step of filling the target volume was performed manually by placing a number of shots at the centre of the target volume and the optimisation function was used with ‘lock collimator settings’ selected so that only the positions and weightings of the shots were optimised.
Optimal initial shot combinations
A sample of 15 previously treated single metastatic clinical cases (all single target volume) was selected from an audit of metastases patients treated at our centre, which covered a period from June 2013 to March 2014. The cases were chosen in order to cover a range of target volumes from 0.8 cm2 to 11 cm2, which is representative of the range of target volumes treated at our centre, excluding those whose size would mean that they would be treated using a single shot, thus negating any benefit of using the optimisation module. All of the volumes in the sample were typical spherically shaped metastatic volumes.
A preliminary investigation indicated that 15 shots of each collimator size was sufficient for the optimiser to produce a clinically acceptable plan. Based on this, each case was planned with a starting shot combination of fifteen 16mm shots, fifteen 8mm shots and fifteen 4mm shots to provide a baseline plan for comparison. All shots were placed centrally in the target volume. Subsequent plans were created for each case, decreasing the number of shots until degradation in plan quality was observed. For each case the starting shot combination with the lowest number of shots, which did not result in degradation in optimised plan quality was determined. Recommended values for the optimiser’s cost function parameters themselves had yet to be determined: as such these parameters were iteratively adjusted manually during this initial planning study.
Recommended optimiser settings
Minimum iteration requirements
For this and the following investigation a sample of 27 patient cases was used, taken from metastases patients previously treated at our centre. The cases were chosen to cover a wide range of treatment volumes. A different set of cases was used compared to those in section 2.2 in order to independently test the validity of the starting shot combinations in Table 1. During the investigations it became apparent that the volume of one of the targets was so small that it could only be reasonably planned using a single shot, so this target was excluded on the basis that there would be no benefit in using the optimiser in this case. A second target was excluded due to its irregular shape, leaving a final sample of 25 cases. Two cases were selected to investigate the number of iterations which the optimisation module needed to run for. These two cases were selected as the target volumes were large and therefore might reasonably be expected to require more iterations to optimise. Plans were produced by running the optimisation module for a range of numbers of iterations from 100 to 10,000. The optimisation parameters were fixed at coverage: 0.9, GI: 0.2 and BOT: 0 (note that the default parameters are coverage: 0.5, GI: 0.25 and BOT: 0), which initial experience had indicated tended to yield reasonably satisfactory plans.
Table 1.
Recommended initial shot combinations for the optimiser.
| Target volume (cm2) | 16mm shots | 8mm shots | 4mm shots |
| <1 | 0 | 3 | 3 |
| 1-2.5 | 2 | 6 | 5 |
| 2.5-3.5 | 4 | 10 | 6 |
| 3.5-6 | 6 | 12 | 0 |
| >6 | 12 | 8 | 0 |
Coverage versus selectivity parameter values
The coverage and selectivity parameters in the optimisation module are competing parameters- as one increases from zero to one, the other automatically decreases from one towards zero. From the sample of 25 cases, a further four were selected to represent the full range of target volumes in the sample. Three plans were produced for each case with the coverage parameter value set to 0.95, 0.9 and 0.85. For all plans the GI and BOT parameter were set at 0, and the optimisation module was run for 3,000 iterations.
GI parameter
The same four cases from section 2.3.2 were used to investigation the optimal weighting of the GI parameter. Plans were produced using the recommended settings determined in sections 2.3.1 and 2.3.2 for GI parameter values of 0.1, 0.2, 0.3 and 0.4.
Comparison with manually produced clinical plans
For each of the 25 cases, 4 plans were produced:
Plan 1: Optimisation module run for 3,000 iterations using the parameters determined in sections 2.3.2 and 2.3.3.
Plan 2: Plan 1 optimised for a further 3,000 iterations with the BOT parameter set to 0.05 in addition to the parameters determined in sections 2.3.2 and 2.3.3.
Plan 3: Optimisation module run for 3,000 iterations using the parameters determined in sections 2.3.2 and 2.3.3 and BOT set to 0.05.
Plan 4: The most optimal plan of plans 1-3 was chosen and manually adjusted to match the coverage of the manually produced clinical plan
The rationale for the method above was as follows. It was reasoned that coverage, PCI and GI should not be compromised for the sake of BOT, therefore the BOT parameter was not used in plan 1. In addition, some control of the BOT is provided by the starting shot combinations. However, it may be possible to reduce BOT without compromising the plan quality, hence the production of plan 2. The nature of the BOT term in the optimisation module means that the weight assigned to the BOT parameter is dependent on the BOT when the optimisation is started. For this reason it was decided to also produce plan 3, with BOT included in the optimisation from the start, as this may result in a superior plan in some cases. Plan 4 was produced as this simulates how the optimiser may be used clinically, and to enable a more meaningful comparison with the manually produced clinical plans.
Results
Optimal initial shot combinations
Figures 2-4 show the number of shots for each collimator setting from the plan with the lowest number of shots which maintained equivalent plan quality to the baseline plan (fifteen shots of each collimator setting). Each figure also shows the recommended initial number of shots for that collimator setting (denoted by the dashed line). The recommended number of 8mm and 4mm starting shots deviates from the trend for small volumes to prevent an excessive number of shots being used for these volumes. The combined recommended initial shot combinations are shown in Table 1.
Figure 2.
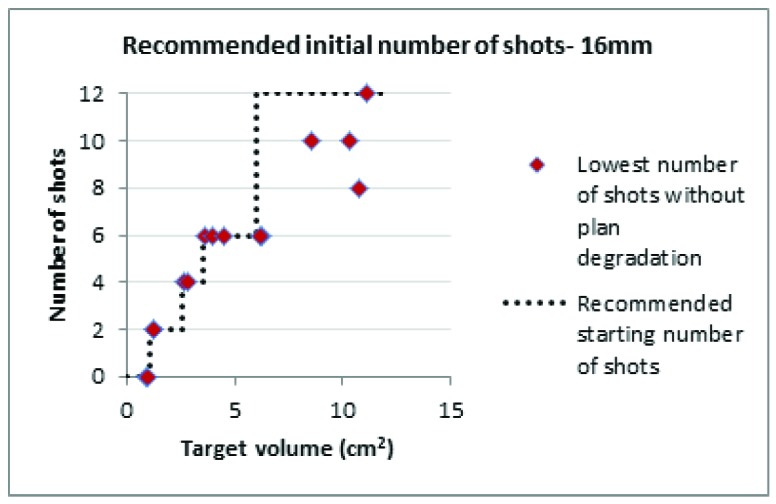
Recommended initial number of 16mm shots.
Figure 3.
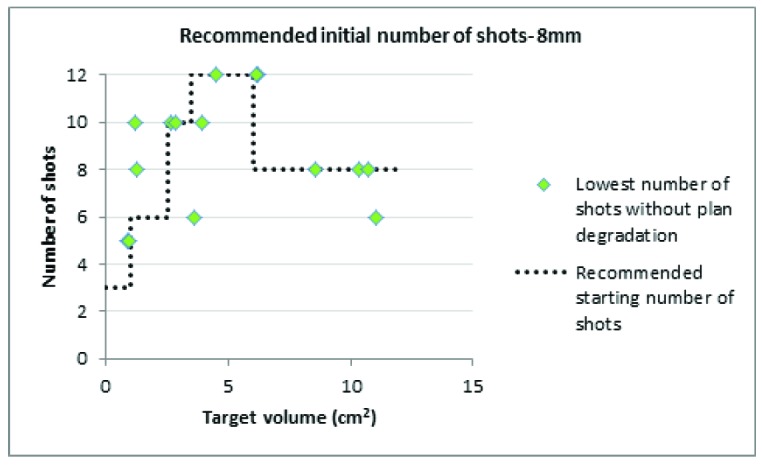
Recommended initial number of 8mm shots.
Figure 4.
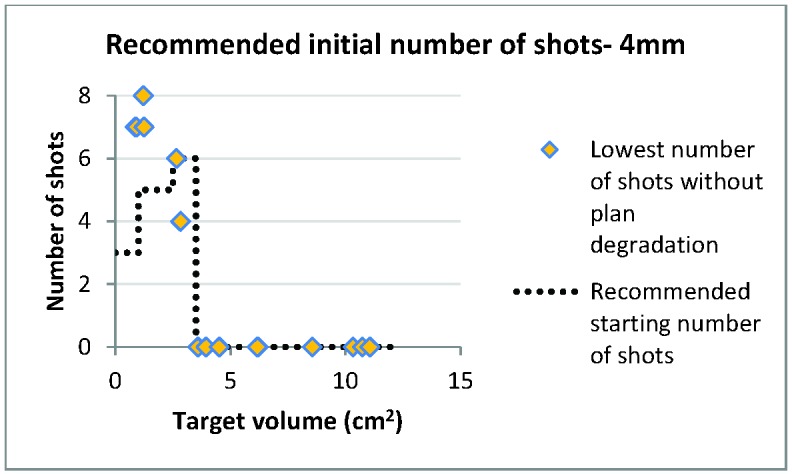
Recommended initial number of 4mm shots.
Table 2.
Variation in plan quality with number of iterations.
| Number of iterations | Coverage | PCI | GI | BOT |
| 100 | 62.3 | 0.58 | 3.01 | 31.3 |
| 500 | 98.6 | 0.70 | 2.70 | 45.1 |
| 1000 | 98.7 | 0.80 | 2.75 | 41.9 |
| 1500 | 98.7 | 0.84 | 2.75 | 39.9 |
| 2000 | 99.1 | 0.84 | 2.74 | 39.8 |
| 2500 | 98.9 | 0.85 | 2.75 | 39.7 |
| 3000 | 99.0 | 0.86 | 2.74 | 40.0 |
| 5000 | 99.0 | 0.87 | 2.72 | 39.5 |
| 10000 | 99.0 | 0.87 | 2.71 | 39.7 |
3.2 Ideal optimisation module settings
3.2.1 Minimum iteration requirements
Table 2 shows the variation in plan quality with the number of iterations of the optimiser. Based on these results, it was decided that running the optimisation module for 3,000 iterations was adequate for the subsequent investigations as any improvements observed from running >3,000 iterations were minimal.
3.2.2 Coverage versus selectivity parameters
Table 3 shows the variation in plan quality with changes in coverage versus selectivity parameters. Based on these results, it was decided to use a value of 0.9 for the coverage parameter (0.1 for selectivity), as coverage begins to drop off rapidly below this value.
3.2.3 GI parameter
Table 4 shows variation in plan quality with increase in the optimiser’s GI weighting factor. Based on these results, it was decided that a starting GI parameter value of 0.2 represented the best compromise between decreasing the GI and maintaining selectivity.
3.3 IP versus manual plans
Table 5 summarises how the plans produced using the inverse planning module compared to the manually created clinical plans.
The plans produced using the standardised method (plans 1-3) resulted in inferior coverage and gradient index, and superior PCI and BOT versus the manually produced clinical plans. Manual adjustment of these plans to match the coverage of the clinical plan resulted in a decrease in PCI, an improvement in the GI and an increase in BOT. The manually optimised plans had a superior BOT to the clinical plans, with no statistically significant differences in PCI or GI. The study was powered to be able to detect a mean difference in PCI of 0.016 and a mean difference in GI of 0.07.
Table 3.
Variation in plan quality versus coverage/selectivity parameters. Coverage, selectivity, PCI, GI and BOT are all averaged across all plans. 95% confidence intervals in brackets.
| Optimiser settings coverage/selectivity | Coverage | Selectivity | PCI | GI | BOT |
| 0.95/0.05 | 99.3 (99.1-99.5) | 0.82 (0.78-0.86) | 0.81 (0.77-0.85) | 3.11 (2.93-3.29) | 48.0 (29.9-66.1) |
| 0.90/0.10 | 98.7 (98.5-98.9) | 0.83(0.76-0.90) | 0.82 (0.75-0.89) | 2.95 (2.87-3.03) | 42.0 (27.7-56.3) |
| 0.85/0.15 | 97.5 (96.4-98.6) | 0.87 (0.83-0.90) | 0.85 (0.8-0.9) | 3.18 (3.13-3.33) | 43.5 (23.8-63.2) |
Table 4.
Average results of the GI parameter investigation. 95% confidence intervals in brackets.
| GI parameter value | Coverage | Selectivity | PCI | GI | BOT |
| 0.1 | 98.6 (98.2-99.0) | 0.84 (0.79-0.89) | 0.83 (0.77-0.89) | 2.77 (2.70-2.84) | 45.8 (36.6-55.0) |
| 0.2 | 98.7 (98.4-99.0) | 0.82 (0.76-0.88) | 0.81 (0.75-0.87) | 2.69 (2.55-2.83) | 46.5 (30.1-62.9) |
| 0.3 | 98.9 (98.6-99.2) | 0.81 (0.74-0.88) | 0.80 (0.73-0.87) | 2.68 (2.59-2.77) | 47.7 (31.8-63.6) |
| 0.4 | 98.7 (98.3-99.1) | 0.79 (0.73-0.85) | 0.78 (0.72-0.84) | 2.61 (2.55-2.67) | 50.8 (36.0-65.6) |
Table 5.
Mean results comparing the plans produced using the standardized method (plans 1-3) and manually adjusted standardized method plan with the manually planned clinical plans (n=25). Values in italics represent the range and values in brackets the p-value from a pair t-test versus the clinical plans.
| Coverage | PCI | GI | Clinical BOT/BOT | |
| Clinical plans (planned manually) | 99.5: 98.6-99.9 | 0.829: 0.65-0.91 | 2.700: 2.48-2.92 | 1.000 |
| Best standardised method plan (1, 2 or 3) | 98.7 (<0.001): 97.0-99.4 | 0.850 (0.012): 0.66-0.91 | 2.754 (0.04): 2.54-3.02 | 1.212 (0.0019): 0.56-1.80 |
| Manually adjusted plan (4) | 99.5(n/a): 98.6-99.9 | 0.827 (0.73): 0.61-0.90 | 2.731 (0.24): 2.55-2.96 | 1.160 (0.017): 0.53-1.85 |
The BOT for the manually adjusted optimizer plans was on average 16% less than the clinical plans (ranging from 85% less to 47% more). Shorter treatment times mean that treatments are easier to tolerate for patients. This is particularly important for patients being treated in a mask on the Icon™ model Gamma Knife rather than a frame as mask-based treatments can often be prolonged due to patients struggling to remain within the tolerance of the high-definition motion management (HDMM) device. It is also important for patients with multiple targets, as these treatments are likely to be lengthy. Plan efficiency also becomes increasingly important as the sources decay over time, decreasing the dose rate.
Discussion
These results demonstrate that the optimiser settings and initial shot filling recommendations presented here constitute a well-prescribed method for using the IP module, which inexperienced planners could use to produce plans which only require minor manual adjustment in order to be clinically acceptable. Manual planning is a skill which takes time to learn, and the method outlined here may be easier for new planners to learn.
The inverse planning module has a number of limitations which should be highlighted. It cannot be used in summation mode, but must be used in 1-to-1 dose mode. This limits its usefulness for close neighbouring targets where the dose from shots in one target contributes significantly to the other. The optimisation module does not adjust the prescription isodose, which is a strategy used in manual planning, in particular for small target volumes. The impact of changing the prescription isodose used for optimisation was not investigated here and is an avenue for future investigation.
This study considered only metastases. Metastases are the most common condition treated at our centre, so were chosen as the focus for this study. In addition to this, metastases generally have a regular, approximately spherical shape, and therefore it was thought that producing a solution would be more straightforward. Investigating more challenging sites such as acoustic neuroma and meningioma presents an avenue for future work.
The study did not include metastases with irregular volumes and very small metastases which would typically be planned using a single shot, so the method described here may not be appropriate for these situations.
Conclusions
Using the inverse planning module in Leksell Gamma Plan with the starting shot combinations and optimisation parameters outlined in this study has the potential reduce planning time, reduce treatment time, and make planning more accessible to inexperienced planners.
Acknowledgements
Authors’ disclosure of potential conflicts of interest
Dr. Wright reports personal fees received by his employer from Elekta Instruments AB, Stockholm, Sweden, outside the submitted work. Dr Wright attended user group meetings of early Icon adopters organized by and hosted by Elekta. Furthermore, Dr Wright participated in work for Elekta validating developments and new software releases for Icon and GammaPlan, for which payments have been received by his employer from Elekta. Elekta has not been involved in any way in the compilation of this manuscript, nor does the company have any knowledge of the work described in this manuscript.
Peter Fallows and Peter Bownes have nothing to disclose.
Author contributions
Conception and design: Peter Fallows, Gavin Wright
Data collection: Peter Fallows
Data analysis and interpretation: Peter Bownes, Peter Fallows, Gavin Wright
Manuscript writing: Peter Fallows, Gavin Wright
Final approval of manuscript: Peter Bownes, Peter Fallows, Gavin Wright
References
- 1. Inverse Planning in Leksell GammaPlan 10 , Elekta Instrument AB, 2010 [Google Scholar]
- 2. Elekta , Release Notes for Leksell Gammaplan 11.0.2, doc 1521809 rev1, 2016 [Google Scholar]
- 3. Paddick I, Gamma Knife Centre, Cromwell Hospital, London. A simple scoring ratio to index the conformity of radiosurgical treatment plans. Technical note. J Neurosurg (Suppl 3) 2000;93:219-222 [DOI] [PubMed] [Google Scholar]
- 4. Paddick I, Lippitz B, Gamma Knife Centre, Cromwell Hospital, London A simple dose gradient measurement tool to complement the conformity index, Neurosurgery (Suppl) 2006;105:194-201 [DOI] [PubMed] [Google Scholar]
- 5. Wright G, Hatfield P, Loughrey C, Reiner B, Bownes P, St James’s Institute of Oncology, St James’s University Hospital, Leeds A method for scoring treatment time efficiency of Gamma Knife radiosurgical treatment plans for brain metastases, Medical Physics 2013;40(2) [DOI] [PubMed] [Google Scholar]