

Abstract
Breast implant-associated anaplastic large cell lymphoma (BIA-ALCL) is an emerging and indolent, but potentially fatal cancer of the immune system that can develop around textured-surface breast implants. The World Health Organization first recognized BIA-ALCL as a unique clinical entity in 2016. To date, over 600 confirmed cases have been reported worldwide. BIA-ALCL most commonly presents with disease confined to the capsule, as a seroma or a mass adjacent to the implant. While BIA-ALCL has a fairly indolent clinical course, with an excellent prognosis in early stage disease, disseminated cancer and death have also been reported. In this review, the authors focus on the early diagnosis and treatment, including reconstructing the breast following BIA-ALCL, and also discuss recently updated National Comprehensive Cancer Network guidelines. They also review the current epidemiology and risk factors associated with BIA-ALCL. Finally, they discuss important medicolegal considerations and the bioethics surrounding the continued use of textured-surface breast implants.
Keywords: breast implant-associated ALCL, anaplastic large cell lymphoma, non-Hodgkin lymphoma, CD30, double capsule, and Late Seroma
Breast implant-associated anaplastic large cell lymphoma (BIA-ALCL) is an emerging and indolent, but potentially fatal, T cell lymphoma associated with textured-surface breast implants. 1 Since Keech and Creech first described BIA-ALCL in 1997, 2 over 600 unique cases have been confirmed worldwide. 3 In 2011, the Food and Drug Administration (FDA) issued the first safety communication on breast implants, warning patients and physicians about the potential risk of BIA-ALCL. Since then, they have followed up with annual safety communication updates. 4 In 2016, the World Health Organization provisionally classified BIA-ALCL as a unique clinical entity. 5
Although the biological basis of the disease remains poorly understood, implant texturization, time and genetics in combination with other factors are all considered to contribute to pathogenesis. 6 BIA-ALCL most commonly presents as localized disease, as a seroma (80%) or mass (30%) adjacent to an implant. In most patients, BIA-ALCL follows an indolent course with an excellent prognosis when treated surgically; however, disseminated cancer and deaths from BIA-ALCL have also been reported. 7 8 Increased awareness of this emerging disease is necessary to facilitate early detection and treatment. Therefore, the purpose of this article is to increase physician awareness of the disease, and review the epidemiology, risk factors, clinical features, diagnostic work up, and current treatment recommendations for BIA-ALCL.
Epidemiology
Epidemiological studies of BIA-ALCL have been traditionally challenging and only recently has higher quality data on implant-specific risk become available. This is due, in part, to limitations in reporting to registries worldwide combined with incomplete breast implant sales data. 9 10 Other factors affecting epidemiological data include a lack of physician awareness of the disease or a paucity of necessary medical resources to effectively diagnose and treat. These are all important considerations that should be considered when interpreting epidemiologic outcomes in BIA-ALCL. Among women with textured breast implants, the absolute risk of developing BIA-ALCL is low; however, the relative risk when compared with the general population is high. The estimated lifetime risk of BIA-ALCL with textured implants, in general, ranges widely from 1:1,000 to 1:30,000 breast implants, these figures represent the average risk when sampling a given study population, which contains several texture manufacturers with both high and low risk devices. 11 12 Risk appears to narrow when reported as implant and manufacturer-specific risk.
BIA-ALCL does not exhibit a predilection for reconstructive over cosmetic augmentation patients. This suggests that a previous history of cancer (e.g., breast cancer) does not predispose to the development of BIA-ALCL. In addition, risk has not been linked to implant filling type (saline versus silicone). 13 Doren et al collected textured implant sales data in the United States to determine the epidemiology of BIA-ALCL, based upon only 100 known US cases at that time. 11 When comparing the number of textured implants sold to cases dealing with BIA-ALCL, they found a lifetime incidence of 2.03 per million patients or a prevalence of 1:30,000, which is 67.6 times higher than primary ALCL in the general population. Importantly, this was an average risk across two US manufacturers: Allergan Biocell and Mentor Siltex; the authors reported a sixfold difference between the manufacturers, which was statistically significant ( p = 0.001). They also found that there were approximately three million textured breast implants currently within the US market. In Australia, the Therapeutic Goods Administration (TGA) estimated a higher disease prevalence of 1 in 1000 to 1 in 10,000 women, with textured breast implants based upon the manufacturer mix of Australia. 12 Interestingly, the FDA-mandated Continued Access and Continued Access Reconstruction/Revision Expansion Trial, the largest prospective textured implant study to date, reports eight confirmed cases of BIA-ALCL to date, a risk of one in 2207 (95 percent CI, 1120 to 5112) with Allergan Biocell implants. 14 Loch-Wilkinson and colleagues investigated implant manufacturer-specific risks and found that higher surface texturization or macrotextured surfaces accounted for the majority (85%) of cases. 15 Recently, Magnusson et al updated the Australia-reported risk, noting an odds ratio for developing BIA-ALCL for Biocell (1:3345) implants compared with Siltex (1:86,029) implants of 16.52 (95 percent CI, 3.60 to 293.05; p < 0.0001). 16
Lymphoma Classification
Lymphoma is a cancer of the immune system developing from either B or T lymphocytes, natural killer cells, or plasma cells. It is the most common malignancy of the blood, affecting up to one in 50 in the general population. Broadly, lymphoma includes Hodgkin's lymphoma (10%), non-Hodgkin's lymphoma (NHL), multiple myeloma, and immunoproliferative diseases. 1 The family of ALCL is a type of NHL characterized by large anaplastic lymphoid cells that express the cell surface protein CD30. 17 CD30 is a marker for activated T-cells and occurs normally on ∼1 to 5% of circulating lymphocytes.
Peripheral T-cell lymphomas comprise less than 15% of all adult lymphomas and ALCL, a subset of peripheral T cell lymphoma comprising less than 2%. The 2016 revisions of the World Health Organization (WHO) classification of lymphoid neoplasms recognizes three distinct lymphoma forms of ALCL, including anaplastic lymphoma kinase (ALK)-positive systemic ALCL, ALK-negative systemic ALCL, and BIA-ALCL. 5 WHO also recognizes primary cutaneous ALCL (PC-ALCL) as a lymphoproliferative disorder. ALK expression is a result of the (2;5) translocation involving chromosomes 2p23 and 5q35, creating an oncogenic fusion protein of the ALK gene and nucleophosmin gene. 18 However, BIA-ALCL is an ALK-negative lymphoma. Oishi et al characterized BIA-ALCL as a triple negative genotype, meaning that it lacks characteristic gene rearrangements in ALK as well as TP63 and DUSP22 , which are typically found in other ALK-negative lymphomas. 19 As such, BIA-ALCL is a unique genetic subtype that is distinct from the other ALCL subtypes such as systemic and primary cutaneous.
Variability also exists between ALCL subtypes in terms of clinical aggressiveness. Systemic ALCL often follows an aggressive course with rapid evolution of disease when left untreated. The majority of patients with systemic ALCL are presented with disseminated stage III or IV disease. Systemic symptoms (B symptoms) are common and extra-nodal disease is present in 40 to 60% of patients. Of the systemic ALCLs, the presence of ALK (ALK-positive ALCL) is associated with a better prognosis. In contrast to systemic ALCL, PC-ALCL tends to not only be clinically indolent but also has an excellent prognosis, with disease-specific survival rates of 85% between 5 and 10 years. 20 Systemic spread is uncommon (∼5%); however, even with the presence of secondary spread to lymph nodes or when multifocal lesions are present, the prognosis of PC-ALCL appears to be unchanged and favorable. 21 While less aggressive, BIA-ALCL is provisionally classified as a systemic lymphoma by WHO. However, in its earliest stage confined to the effusion with no evidence of tissue infiltration, BIA-ALCL is indolent, likely becoming infiltrative at the later stages from increasing mutational burden. Advanced disease is the end of the spectrum of cancer stages, and these patients substantiate the World Health Organization classification of BIA-ALCL as a lymphoma rather than benign or lymphoproliferative.
Pathogenesis
In BIA-ALCL, no clear etiology leading to unregulated T cell clonal expansion has been identified. 22 Particulate matter from the textured device, presence of a subclinical biofilm, viral inoculation, induction after chronic mechanical abrasion to the breast pocket, as well as genetics have all been postulated. 6 23 24 Kadin et al have recently proposed an allergen-driven etiology. 25 The lack of a well-established animal model has complicated our understanding of the disease. 26 BIA-ALCL is not gender-specific as several cases of BIA-ALCL in transgender women (male to female) have been described. 27 Localized ALK- CD30+ ALCL has been described in limited case reports arising around a tibial metallic plate, dental implant, a shoulder repair, and a textured gluteal implant. 28 29 30 31 Interestingly, one case of an implant-associated ALK- CD30+ ALCL after bariatric surgery was reported, and the device was fabricated from elastopolymers similar to breast implants (Lap-Band AP; Allergan). 32 A case described by Engberg et al, presented with a unique skin ALCL in a single plague directly over an implanted chemotherapy port (product #0655640, Bard Access Systems) containing silicone and polyurethane. 33 In both of these later cases, patients had previously undergone treatment for lymphoproliferative disorders.
Implant Texturization
The association between textured-surface breast implants and BIA-ALCL is well established. To date, reported cases exclusively involve a clinical history of a textured device, whether through exposure to a textured tissue expander or a textured-surface breast implant in the clinical history. According to the 2018 FDA update, 457 unique medical device reports, which include nine patient deaths of BIA-ALCL, have been received with surface characteristics available for 334. 34 Of these, 92.8% were textured implants. Twenty-four cases of BIA-ALCL following smooth implants, reported to the FDA, had either minimal or no clinical history available and were unreliable. Out of 173 consecutive BIA-ALCL patients, Brody found all patients with known implant characteristics to have a history of textured implants. 35 Currently, the use of texturized devices appears to be the only modifiable risk factor for the development of BIA-ALCL.
Biofilm Theory
The biofilm hypothesis suggests that response to an endotoxin from a subclinical gram-negative biofilm may serve as the inciting event in BIA-ALCL. Subclinical infections with Helicobacter pylori or Chlamydia trachomatis have led to gastric and cervical cancers, but by very disparate pathways. 36 37
Textured breast implants have been shown to carry a higher bacterial load than smooth implants. 38 Once a threshold biofilm is reached, on both smooth and textured implants, propensity toward capsular contracture is potentiated. However, the concept that BIA-ALCL and capsular contracture share a common inciting factor remains underdeveloped and is not supported with clinical observation. Recent analyses of the bacterial biofilms of patients with BIA-ALCL initially suggested the bacteria Ralstonia pickettii ; however, BIA-ALCL patients do not appear to have a distinct microbiome. 39 Moreover, the study presents several limitations such as the following: the comparison of the microbiome of tumor specimens in some patients to non-tumor tissue in others; different handling and sterility of specimens (fresh vs formalin fixed); no information on concurrent antibiotic treatment of the patients, and finally the presence of Ralstonia spp . being found in both BIA-ALCL and non BIA-ALCL capsules. 40 The microbiome in tumor and non-tumor capsules is Staphylococcus spp . predominant. It is unclear how the microbiome might change for a patient with previous breast procedures, what role the surgery itself may play in manipulating the microenvironment, and how that may have confounded the study results. Therefore, microbiological investigations into BIA-ALCL should be considered with those factors in mind. Interestingly, R. pickettii is a spirochete that is typically found in water, and more specifically it is found as a contaminant in laboratory water sources. 41 Unfortunately, R. pickettii involvement continues to be propagated at scientific meetings and throughout the literature.
A link between bacterial biofilm and T cell hyperplasia has been established which has been demonstrated in both porcine models and humans. 42 Chronic biofilm infection of mammary prosthesis is associated with a T cell predominant lymphocytic infiltration, which is also directly related to the bacterial load around an implant. 38 Comparison of the capsules of textured and smooth implants in a porcine model demonstrated an increased number of lymphocytes with T cell predominance in textured implants. Kadin et al have shown that BIA-ALCL cells may be derived from Th1/Th17 cells in capsular tissues and seromas. 43 Th1/Th17 are antigen-driven memory t-cells, supporting the hypothesis that BIA-ALCL results from chronic bacterial antigen stimulation. Interestingly, continuous activation of JAK-STAT (discussed in genetics section) has also been shown to induce a Th1/Th17 phenotype in other cancers. 44
Inflammatory Model of Pathogenesis
Chronic inflammation is a well-established risk factor for the development of cancer. 45 Some evidence supports the theory that chronic inflammation plays a role in the development of BIA-ALCL. Bizjak et al proposed that in BIA-ALCL, chronic activation of local and systemic immune systems may cause neoplastic transformation. 46 Polyclonal activation of T-cells may result in monoclonal T cell expansion in a genetically at-risk host, ultimately leading to lymphoma. In the context of chronic inflammation, host genetic factors (e.g., JAK-STAT pathway, see Genetics section) in combination with other factors may influence the likelihood of malignant transformation. Future work in this area is warranted.
Microtrauma to the Breast Pocket
While biofilms may be present in patients with BIA-ALCL, the etiology is likely multifactorial in nature. Brody argues against the biofilm theory and suggests that the textured surface may act as the inciting stimulus as a result of chronic trauma inflected to the breast pocket which may lead to oncogenic transformation. 47 Tribology is the observed effect of friction between two objects. Orthopedic implants have been hypothesized to increase carcinogenicity via tribology although no investigation with relation to implants in BIA-ALCL has yet been reported.
Genetic Risk Factors
Genetics is also thought to play a major role in the pathogenesis of BIA-ALCL and may partially explain the rarity of the disease. 48 In a landmark study from Blombery et al, novel activating mutations in the JAK-STAT3 pathway were first described. 49 The JAK-STAT3 pathway is a major intracellular signaling pathway, and aberrant activation of the pathway has been shown to induce malignant transformation in other cancers including lymphomas. 50 Recent molecular genetics studies have increasingly discovered oncogenic mutations and aberrant activation of the pathway. 24 51 52 53 54 JAK-STAT3 involvement lends support to the inflammatory model of pathogenesis and suggests that similar fundamental driver gene mutations exist between BIA-ALCL and systemic ALK-negative ALCL, despite clinical differences. Importantly, aberrant activation in the JAK-STAT3 pathway has been shown to lead to tumorigenesis in other malignancies. 55 Moreover, constitutive JAK-STAT activation has also been shown to mechanistically link chronic inflammation and malignant transformation. 56 Therefore, we submit that the JAK-STAT pathway may be the mechanistic link between chronic inflammation and BIA-ALCL tumorigenesis. It is also important to note that some BIA-ALCL tumors have harbored other non-JAK-STAT pathway genetic mutations including TP53 and DNMT3A . 52 57 However, that does not necessarily preclude involvement of the JAK-STAT3 pathway in those cases. This is currently an active area of investigation in our laboratory.
Diagnosis and Treatment
Clinical Presentation
Onset of BIA-ALCL has been reported to be ranging between 2 and 28 years after breast implantation, most commonly occurring between 7 and 10 years. Unilateral disease is much more common than bilateral disease, which is rare, occurring approximately in 4.9% of patients. 58 BIA-ALCL arises adjacent to an implant, first as an effusion and then infiltrating into the luminal surface of the scar capsule. 7 The majority of patients (60–80%) present greater than one year after implantation with a periprosthetic effusion (delayed seroma); with far fewer presenting with an invasive mass (17–30%) or distant metastasis (1–3%). The finding of capsular contracture is both rare (8–10%) and may be non-specific for BIA-ALCL, and ipsilateral regional lymphadenopathy reportedly occurs in 8–16% of cases. 59
Diagnostic Workup
The National Comprehensive Cancer Network (NCCN) has standardized diagnosis and management guidelines for BIA-ALCL. 59 60 ( Fig. 1 ) The finding of seroma, presenting more than one year after placement of breast implants, should raise concerns for BIA-ALCL, prompting investigation. Textured surface breast implants have been uniquely associated with BIA-ALCL, but a suspicious fluid collection in any surface breast implant should be investigated. ( Fig. 2 ) First, a physical exam should include inspection and palpation of bilateral breast, axillae, neck, and chest wall. While the most common presentation of BIA-ALCL is peri-prosthetic fluid collection or mass, other rare and non-specific symptoms include the following: breast enlargement, skin rash, capsular contracture and lymphadenopathy. Ultrasound is the preferred initial imaging modality to investigate BIA-ALCL. Ultrasound can be used to define the extent of fluid collection (sensitivity 84%, specificity 75%), identify associated masses (sensitivity 46%, specificity 100%), and evaluate enlarged regional lymph nodes. Magnetic resonance imaging or positron emission tomography (PET) should be used if ultrasound is indeterminate. A small volume of peri-prosthetic fluid may be normal; however, seroma should be investigated with fine needle aspiration (FNA). FNA can be performed in clinics, under ultrasound guidance, or using interventional radiology. Seroma fluid should be aspirated for analysis along with samples of the capsule and any suspicious masses. As an uncommon and emerging disease, communication with the pathologist should include explicit directions to “rule-out BIA-ALCL.” Pathologic examination should include cytologic examination of seroma fluid with cell block cytology, CD30 immunohistochemistry, and flow cytometry to assess T cell receptor gene rearrangement. Cell block cytology demonstrates anaplastic large cells, and flow cytometry demonstrates a single T cell clonally expanded population. ( Fig. 3 ) If lymphoma diagnosis is indeterminate, additional hematopathologist consultation at a center with experience in this disease is recommended. If the pathology is negative, referral to a plastic surgeon for benign seroma management is considered appropriate. When pathology is positive, referral to a lymphoma oncologist with complete work-up and staging should follow. Physicians inexperienced with tumor extirpation may consider a surgical oncology consultation.
Fig. 1.
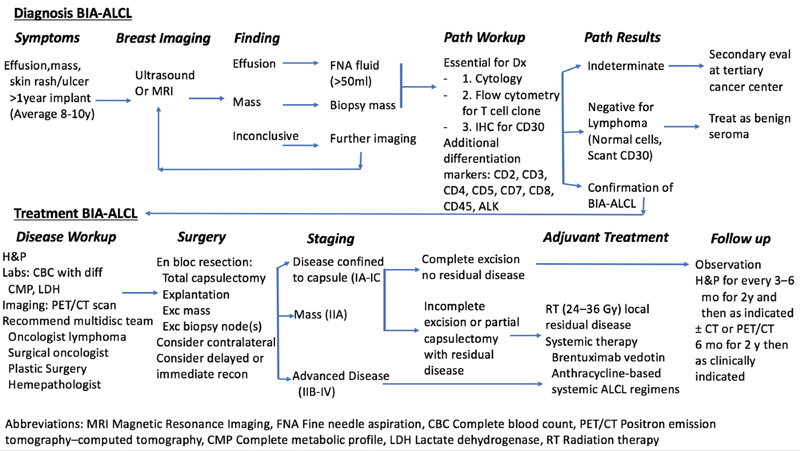
BIA-ALCL Disease Algorithm. Current evidence-based algorithm for achieving diagnosis, followed by treatment based on stage of disease. (Reprinted with permission from Clemens MW, Jacobsen ED, Horwitz SM. 2019 NCCN Consensus Guidelines on the Diagnosis and Treatment of Breast Implant-Associated Anaplastic Large Cell Lymphoma (BIA-ALCL). Aesthet Surg J. 39(S1) S3–S13, 2019.)
Fig. 2.

Smooth and a textured surface breast implant. To date, all known cases of BIA-ALCL worldwide with a known clinical history have involved a prior textured device. Therefore, a textured surface implant may be integral to the pathogenesis of BIA-ALCL.
Fig. 3.
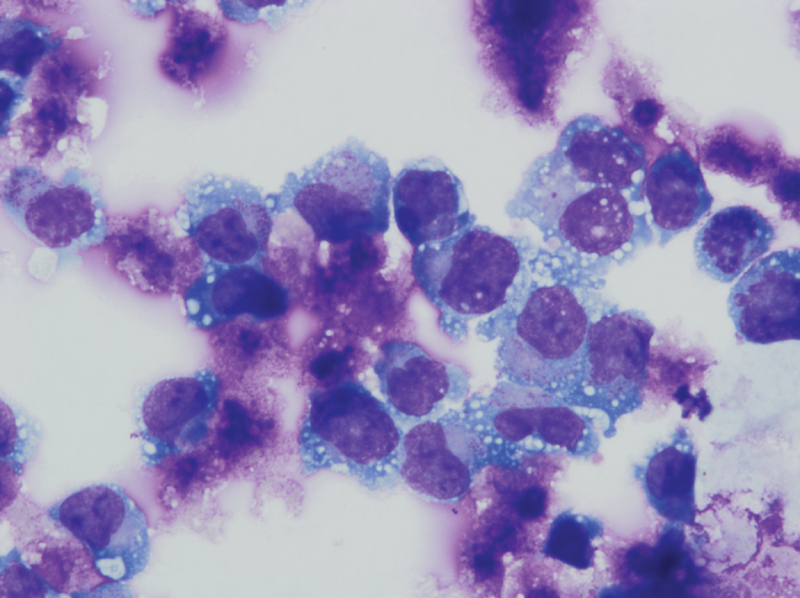
A malignant effusion in a BIA-ALCL patient demonstrates large pleomorphic anaplastic cells with prominent horseshoe-shaped nuclei and nuclear folding. (hematoxylin stain, 500X magnification) Positive anaplastic cytology, CD30 immunohistochemistry expression, and single T cell clonality demonstrated on flow cytometry are required for BIA-ALCL diagnosis.
A multidisciplinary team approach should be used following pathologic confirmation of BIA-ALCL. Routine laboratory tests include complete blood count, comprehensive metabolic panel, lactate dehydrogenase, Hepatitis B, and pregnancy test. Active BIA-ALCL is positive on PET, which is the preferred modality to evaluate for systemic spread to regional lymph nodes, and organ involvement in pathologically confirmed cases, and is performed prior to any surgical intervention. 61 Staging distinguishes localized from disseminated disease and is determined from a combination of imaging and pathologic findings at the time of surgery.
The following two staging systems may be used for BIA-ALCL: the Ann Arbor staging system and the MD Anderson BIA-ALCL tumor-node-metastasis (TNM) staging system. The Lunago revision to the Ann Arbor staging system is a lymphoma staging with stage IE disease limited to a single extra-nodal site (i.e., breast or capsule), and Stage IIE defining spread to local lymph nodes. 62 Using this system, most patients are nearly binary classified as having either early stage disease; 83 to 84% Stage IE, 10 to 16% Stage IIE. The MD Anderson (MDA) solid tumor BIA-ALCL TNM staging system is modeled after the American Joint Committee on Cancer (AJCC) TNM system for staging solid tumors. The TNM staging system may be more appropriate for patients who have BIA-ALCL, as this disease is more similar to other solid tumors than other lymphomas. Moreover, MDA TNM staging system has been shown to more accurately predict overall survival than the Ann Arbor Lymphoma staging system. 7
Treatment
BIA-ALCL, like any malignancy, should be treated as a part of a multidisciplinary team. 63 Treatment follows the established guidelines set forth by the NCCN, which was formulated on the best available evidence-based approaches. 60 Following prompt diagnosis, the current standard of care includes implant removal, complete capsulectomies, and excision of suspicious lymph nodes. ( Fig. 4 ) NCCN guidelines also recommend removal of the contralateral breast implant as 4.6% of cases have been presented with subclinical bilateral involvement. Surgery alone is effective for most cases limited to the implant capsule. ( Fig. 5 ) In the case of bilateral implants, the contralateral implant and capsule are recommended for removal to mitigate the risk of recurrence or contralateral disease. As an implant can drain into multiple lymph node basins, there is no role for sentinel lymph node biopsy. Excisional biopsies of clinically or radiographically enlarged lymph nodes should be performed, as ∼14% are pathologically involved.
Fig. 4.
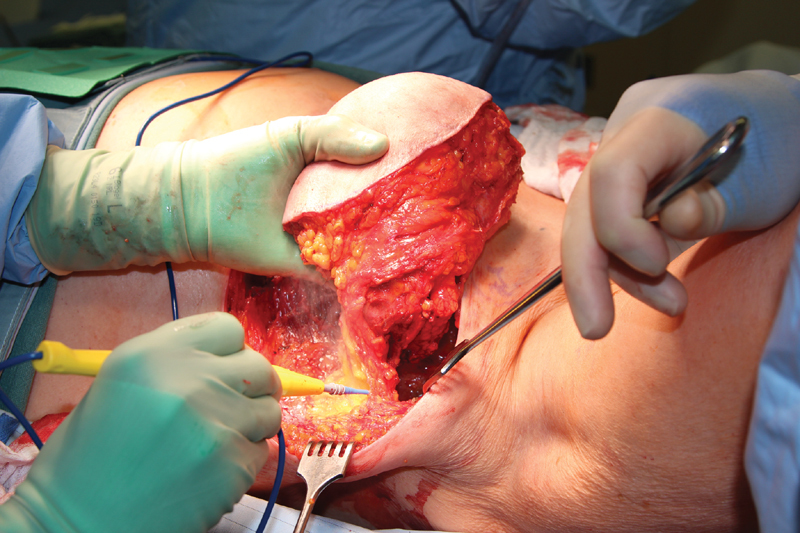
The treatment of BIA-ALCL is demonstrated with explantation of the device and total capsulectomy. The patient had a previous history of breast cancer which was treated with a mastectomy and prosthetic reconstruction. Following diagnosis of BIA-ALCL, the patient was not interested in further reconstruction and therefore a ellipse of skin was resected with the capsule for contouring of the chest skin.
Fig. 5.
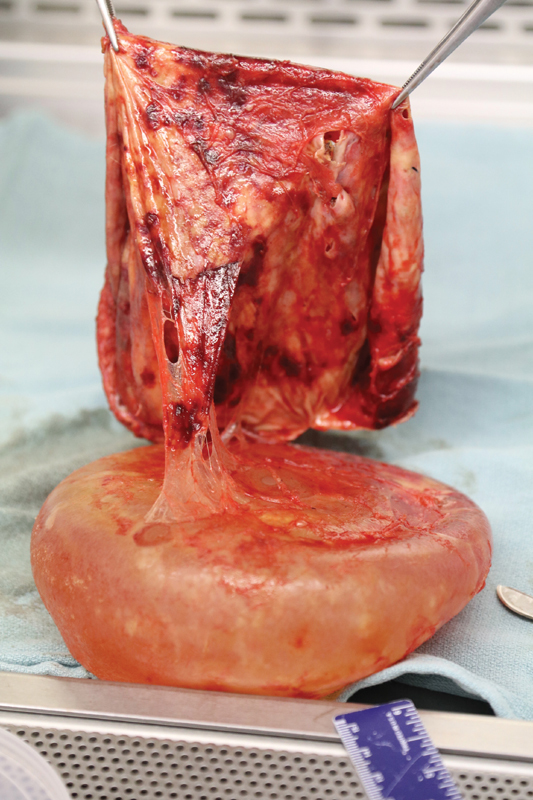
The capsule and implant of a BIA-ALCL patient are shown during evaluation by pathology. Note the thickened surface of the capsule which had developed into a mass.
Extirpative Therapy
Complete surgical resection is now the standard of care and is curative in the majority of cases. One retrospective analysis of 87 patients with BIA-ALCL estimated a median overall survival of 13 years after complete surgical excision. 7 Event-free survival was shown to be significantly higher with complete surgery (96%) than limited surgery (40%) and adjuvant therapy (chemotherapy 76%, radiation 82%). Optimal management of disseminated, persistent, or recurrent disease is unclear. Clemens et al compared different treatment regimens: surgery alone (40%), surgery and radiation (9%), surgery and chemotherapy (19%), surgery, chemotherapy and radiation (30%), and chemotherapy alone (2%). 7 Those treated with complete surgical excision had better overall survival and event-free survival than those treated with partial capsulectomy, systemic chemotherapy, or radiation ( Fig. 2 ).
Chemotherapy and Radiation
For patients with localized disease (Ann Arbor stage IE, MDA TNM Stage IA–IIA), no adjuvant chemotherapy or radiation is necessary. In patients with unresectable chest wall invasion or regional lymph node involvement (Stage IIE, MDA TNM Stage IIB–IV), adjunctive chemotherapy is recommended (NCCN). Patients who fail surgical therapy alone or with proven disseminated disease should be managed in the same way as de-novo ALK-negative systemic ALCL (NCCN). However, 32% of patients treated with systemic chemotherapy alone experience recurrence, suggesting this treatment may be insufficient in some cases.
Adjuvant radiation therapy should be considered in the case of positive margins, unresectable tumor extending into the chest wall, or residual disease. Metastatic disease may be treated with brentuximab, a monoclonal antibody directed at CD30 or an anthracycline based chemotherapeutic regimen (CHOP: cyclophosphamide, doxorubicin, vincristine, and prednisone). 60 64
Oncologic Follow-Up
Multidisciplinary consensus reports recommend clinical follow-up every six months for the two years following definitive treatment of BIA-ALCL. Annual ultrasounds may be continued for at least two years, with the addition of chest, abdominal, and pelvic computerized tomography scans, and contrast or PET scan every 6 months as clinically indicated.
Breast Reconstruction in BIA-ALCL
Lamaris et al recently described a novel, algorithmic approach to reconstructing the breast following BIA-ALCL, based on the experience they had gathered over 18 consecutive reconstructions. 65 In their case series, immediate reconstruction (smooth implant or autologous tissue) was reserved for patients with surgically resectable disease (Stage IA–IC). Alternatively, stage IA–IC patients also had the option of delaying reconstruction (smooth implant or autologous tissue or autologous fat grafting) until repeat PET imaging had been completed between 3 and6 months following oncologic resection. Advanced disease (Stage IIA–IV) was considered as a relative contraindication to immediate reconstruction. Patients with advanced disease typically undergo repeat imaging between 6 and 12 months following oncologic resection. If no evidence of residual or recurrent disease if found, delayed reconstruction using the same reconstructive adjuncts for immediate reconstruction may be undertaken. Overall, 96% of patients were either satisfied or highly satisfied with their reconstruction and no surgical complications were observed at long-term follow-up (42 months). As such, breast reconstruction remains a viable option in select cases following definitive treatment. 66
Prognosis
In general, with complete surgical resection, BIA-ALCL appears to be an indolent disease with good prognosis, unless it extends beyond the capsule and/or presents with a mass. Presence of a mass lesion, extracapsular extension, or bilateral disease are features associated with worse prognosis. One retrospective review of 60 patients with BIA-ALCL showed a higher rate of complete remission in patients without a mass (93%) than those with a mass present (72%). Although the majority of patients with BIA-ALCL have a relatively indolent clinical course, reports of death attributable to the disease emphasizes the importance of timely diagnosis and appropriate surgical treatment.
Medicolegal Considerations
In 2011, the FDA made recommendations to implant manufacturers after which a package insert warning regarding the existence of BIA-ALCL was added in the United States and Canada. 67 As awareness and understanding of the disease increases, the issue of informed consent becomes progressively apparent. Risk disclosure serves to respect patient autonomy and carries lasting consequences for both surgeon and patient. Informed consent should include both common (> 1 % of procedures) and rare (< 1 % of procedures) but serious adverse events. As awareness of the disease increases, inclusion of BIA-ALCL in consent for breast implant placement should be conducted without hesitation. 68 Informed consent examples including the risk of BIA-ALCL, developed by the American Society of Plastic Surgery (ASPS), are available on plasticsurgery.org.
Recent efforts have also been made to notify patients of the possible risk of BIA-ALCL. Roberts et al retroactively contacted 1,340 patients at risk for BIA-ALCL. 69 70 The authors found that contacting at-risk patients did not create an additional burden on their health care system. Given that new information regarding the safety and risks associated with textured devices occurred after many of the patients had their surgery, the study by Roberts et al can be seen as a model for retroactively completing the process of informed consent. Importantly, complications related to cosmetic breast implants may not always be covered by insurance. For this reason, cosmetic patients may be less likely to undergo BIA-ALCL screening. Unfortunately, Roberts et al also found that many of their patients actually incurred additional medical costs for removal of their textured device, which is problematic.
In 2006, the FDA recommended that all women with silicone breast implants undergo MRI three years after implant placement to evaluate for failure (rupture). However, lack of insurance coverage for this screening test decreased compliance. 71 In 2017, the FDA released an updated safety communication cautioning women with breast implants about BIA-ALCL. Included are the following recommendations for counseling: women with breast implants may have a very small but increased risk of developing BIA-ALCL in the capsule around the implant. BIA-ALCL most frequently occurs with textured implants and presents with late seroma but may also present with capsular contracture or masses. Women with implants should get routine mammography, perform regular self-breast exams, and visit a physician if changes occur. On July 24th, 2019, the US FDA requested Allergan perform a voluntary recall of Biocell textured tissue expanders and implants out of concern for a disproportionately higher risk of BIA-ALCL. 72 Allergan responded with a worldwide recall of these products. Importantly, this device recall only applies to future sales, and does not effect devices currently implanted. Screening and prophylactic implant removal is not recommended in asymptomatic individuals. 73 In accordance with the FDA recommendations, histologic confirmation of BIA-ALCL should be reported to the Patient Registry and Outcomes for Breast Implants and Anaplastic Large Cell Lymphoma Etiology and Epidemiology (PROFILE) registry of the American Society of Plastic Surgeons ( www.thepsf.org/profile ). To date, 288 US cases have been reported as of July 2019. There are currently 447 unique confirmed cases of BIA-ALCL outside of the United States. The US has confirmed 164 US cases, while 282 unique US cases have been reported to the PROFILE registry and confirmation is ongoing. There have been a total of 33 deaths worldwide directly attributable to disease. Using a registry of confirmed cases will help determine the exact role of breast implants in disease development and presence of genetic predisposition, and ascertain patient or implant modifiable risk factors.
Conclusion
BIA-ALCL is an emerging and indolent, but potentially fatal, lymphoma that can form around textured-surface breast implants usually a decade after implantation. 74 Over the last 20 years, basic science and clinical investigations from laboratories throughout the world have greatly increased our understanding of the disease. 75 NCCN guidelines include evidence-based guidelines that represent the most recent diagnostic and treatment guidelines available. 60 Current evidence supports that surgery plays a pivotal role in the management of BIA-ALCL, heavily influencing oncologic outcomes. Increasing physician awareness, continued biomedical research, and accurate reporting to implant registries are necessary to move our knowledge of the disease forward in order to improve patient safety.
Funding Statement
Funding Sources Dr. DeCoster is supported by a National Cancer Institute Surgeon-Scientist training grant (T32CA160003).
Footnotes
Conflicts of Interest None of the authors have associations or financial disclosures to report that create a conflict of interest with the information presented in this article. Dr. Clemens is a clinical investigator for Motiva US Safety Trial (Establishment Labs) and was a former Allergan consultant (2012–2015).
References
- 1.Clemens M W, Miranda R N. Coming of age: breast implant-associated anaplastic large cell lymphoma after 18 years of investigation. Clin Plast Surg. 2015;42(04):605–613. doi: 10.1016/j.cps.2015.06.006. [DOI] [PubMed] [Google Scholar]
- 2.Keech J A, Jr, Creech B J. Anaplastic T-cell lymphoma in proximity to a saline-filled breast implant. Plast Reconstr Surg. 1997;100(02):554–555. doi: 10.1097/00006534-199708000-00065. [DOI] [PubMed] [Google Scholar]
- 3.McCarthy C M, Loyo-Berríos N, Qureshi A Aet al. Patient registry and outcomes for breast implants and anaplastic large cell lymphoma etiology and epidemiology (PROFILE): initial report of findings, 2012-2018 Plast Reconstr Surg 2019143(3S A review of breast implant-associated anaplastic large cell lymphoma):65S–73S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Eaves F, 3rd, Nahai F. Anaplastic large cell lymphoma and breast implants: FDA report. Aesthetic Surg J. 2011;31(04):467–468. doi: 10.1177/1090820X11407872. [DOI] [PubMed] [Google Scholar]
- 5.Swerdlow S H, Campo E, Pileri S A et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127(20):2375–2390. doi: 10.1182/blood-2016-01-643569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Blombery P, Thompson E R, Prince H M.Molecular drivers of breast implant-associated anaplastic large cell lymphoma Plast Reconstr Surg 2019143(3S A review of breast implant-associated anaplastic large cell lymphoma):59S–64S. [DOI] [PubMed] [Google Scholar]
- 7.Clemens M W, Medeiros L J, Butler C E et al. Complete surgical excision is essential for the management of patients with breast implant-associated anaplastic large-cell lymphoma. J Clin Oncol. 2016;34(02):160–168. doi: 10.1200/JCO.2015.63.3412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Carty M J, Pribaz J J, Antin J H et al. A patient death attributable to implant-related primary anaplastic large cell lymphoma of the breast. Plast Reconstr Surg. 2011;128(03):112e–118e. doi: 10.1097/PRS.0b013e318221db96. [DOI] [PubMed] [Google Scholar]
- 9.Collett D J, Rakhorst H, Lennox P, Magnusson M, Cooter R, Deva A K.Current risk estimate of breast implant-associated anaplastic large cell lymphoma in textured breast implants Plast Reconstr Surg 2019143(3S A review of breast implant-associated anaplastic large cell lymphoma):30S–40S. [DOI] [PubMed] [Google Scholar]
- 10.Srinivasa D R, Mirnada R R, Kaura A et al. Global adverse event reports of breast implant-associated ALCL: an international review of 40 government authority databases. Plast Reconstr Surg. 2017;139(05):1029–1039. doi: 10.1097/PRS.0000000000003233. [DOI] [PubMed] [Google Scholar]
- 11.Doren E L, Miranda R N, Selber J C et al. U.S. epidemiology of breast implant-associated anaplastic large cell lymphoma. Plast Reconstr Surg. 2017;139(05):1042–1050. doi: 10.1097/PRS.0000000000003282. [DOI] [PubMed] [Google Scholar]
- 12.Australian Therapeutic Goods Administration. Breast implants and anaplastic large cell lymphoma-Update: TGA's review of textured breast implants and preliminary outcomes. Available athttps://www.tga.gov.au/alert/breast-implants-and-anaplastic-large-cell-lymphoma. Published 2019. Accessed July 13, 2019
- 13.Miranda R N, Aladily T N, Prince H M et al. Breast implant-associated anaplastic large-cell lymphoma: long-term follow-up of 60 patients. J Clin Oncol. 2014;32(02):114–120. doi: 10.1200/JCO.2013.52.7911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Clemens M W, McGuire P A. Discussion: a prospective approach to inform and treat 1340 patients at risk for BIA-ALCL. Plast Reconstr Surg. 2019;144(01):57–59. doi: 10.1097/PRS.0000000000005756. [DOI] [PubMed] [Google Scholar]
- 15.Loch-Wilkinson A, Beath K J, Knight R JW et al. Breast implant-associated anaplastic large cell lymphoma in Australia and New Zealand: high-surface-area textured implants are associated with increased risk. Plast Reconstr Surg. 2017;140(04):645–654. doi: 10.1097/PRS.0000000000003654. [DOI] [PubMed] [Google Scholar]
- 16.Magnusson M, Beath K, Cooter R et al. The epidemiology of breast implant-associated anaplastic large cell lymphoma in Australia and New Zealand confirms the highest risk for Grade 4 surface breast implants. Plast Reconstr Surg. 2019;143(05):1285–1292. doi: 10.1097/PRS.0000000000005500. [DOI] [PubMed] [Google Scholar]
- 17.Stein H, Mason D Y, Gerdes J et al. The expression of the Hodgkin's disease associated antigen Ki-1 in reactive and neoplastic lymphoid tissue: evidence that Reed-Sternberg cells and histiocytic malignancies are derived from activated lymphoid cells. Blood. 1985;66(04):848–858. [PubMed] [Google Scholar]
- 18.Morris S W, Kirstein M N, Valentine M Bet al. Fusion of a kinase gene, ALK, to a nucleolar protein gene, NPM, in non-Hodgkin's lymphoma Science 1994263(5151):1281–1284. [DOI] [PubMed] [Google Scholar]
- 19.Oishi N, Brody G S, Ketterling R P et al. Genetic subtyping of breast implant-associated anaplastic large cell lymphoma. Blood. 2018;132(05):544–547. doi: 10.1182/blood-2017-12-821868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Willemze R, Jaffe E S, Burg G et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105(10):3768–3785. doi: 10.1182/blood-2004-09-3502. [DOI] [PubMed] [Google Scholar]
- 21.Bekkenk M W, Geelen F A, van Voorst Vader P C et al. Primary and secondary cutaneous CD30(+) lymphoproliferative disorders: a report from the Dutch Cutaneous Lymphoma Group on the long-term follow-up data of 219 patients and guidelines for diagnosis and treatment. Blood. 2000;95(12):3653–3661. [PubMed] [Google Scholar]
- 22.Clemens M W, Nava M B, Rocco N, Miranda R N. Understanding rare adverse sequelae of breast implants: anaplastic large-cell lymphoma, late seromas, and double capsules. Gland Surg. 2017;6(02):169–184. doi: 10.21037/gs.2016.11.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Rastogi P, Riordan E, Moon D, Deva A K.Theories of etiopathogenesis of breast implant-associated anaplastic large cell lymphoma Plast Reconstr Surg 2019143(3S A review of breast implant-associated anaplastic large cell lymphoma):23S–29S. [DOI] [PubMed] [Google Scholar]
- 24.Di Napoli A, De Cecco L, Piccaluga P P et al. Transcriptional analysis distinguishes breast implant-associated anaplastic large cell lymphoma from other peripheral T-cell lymphomas. Mod Pathol. 2019;32(02):216–230. doi: 10.1038/s41379-018-0130-7. [DOI] [PubMed] [Google Scholar]
- 25.Kadin M E, Morgan J, Xu H et al. IL-13 is produced by tumor cells in breast implant-associated anaplastic large cell lymphoma: implications for pathogenesis. Hum Pathol. 2018;78:54–62. doi: 10.1016/j.humpath.2018.04.007. [DOI] [PubMed] [Google Scholar]
- 26.DeCoster R C, Vasconez H C, Butterfield T A.CRISPR/Cas9-mediated genomic editing: implications for engineering an animal model of breast implant-associated anaplastic large cell lymphomaPlast Reconstr Surg2019. Doi: 10.1097/PRS.0000000000006051 [epub ahead of print] [DOI] [PMC free article] [PubMed]
- 27.De Boer M, van der Sluis W B, de Boer J Pet al. Breast Implant-Associated Anaplastic Large-Cell Lymphoma in a Transgender Woman Aesthet Surg J 2017370883–87.. doi:10.1093/asj/sjx098 [DOI] [PubMed] [Google Scholar]
- 28.Palraj B, Paturi A, Stone R Get al. Soft Tissue Anaplastic Large T-Cell Lymphoma Associated with a Metallic Orthopedic Implant: Case Report and Review of the Current Literature J Foot Ankle Surg 20104906561–564.. doi:10.1053/j.jfas.2010.08.009 [DOI] [PubMed] [Google Scholar]
- 29.Yoon H J, Choe J Y, Jeon Y K.Mucosal CD30-Positive T-Cell Lymphoproliferative Disorder Arising in the Oral Cavity Following Dental Implants Internat J Surg Path 20152308656–661.. doi:10.1177/1066896915599059 [DOI] [PubMed] [Google Scholar]
- 30.Tuck M, Lim J, Lucar J, Benator D.Anaplastic large cell lymphoma masquerading as osteomyelitis of the shoulder: an uncommon presentationBMJ Case Rep2016. 2016. doi: 10.1136/bcr-2016-217317 [DOI] [PMC free article] [PubMed]
- 31.Mendes J, Jr, Mendes Maykeh V A, Frascino L F.Gluteal Implant-Associated Anaplastic Large Cell Lymphoma Plast Reconstr Surg 201914403610–613.. doi: 10.1097/PRS.0000000000005910 [DOI] [PubMed] [Google Scholar]
- 32.Manikkam Umakanthan J, McBride C L, Greiner Tet al. Bariatric Implant Associated Anaplastic Large-Cell Lymphoma J Onc Practice 20171312838–839.. doi:10.1200/jop.2017.026153 [DOI] [PubMed] [Google Scholar]
- 33.Engberg A K, Bunick C G, Subtil A, Ko C J, Girardi M.Development of a Plaque Infiltrated With Large CD30+ T Cells Over a Silicone-Containing Device in a Patient With History of Sézary Syndrome J Clin Onc 20133106e87–e89.. doi:10.1200/jco.2012.42.9241 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Food and Drug Administration. Medical device reports of breast implant-associated anaplastic large cell lymphoma. Available at:https://www.fda.gov/medical-devices/breast-implants/medical-device-reports-breast-implant-associated-anaplastic-large-cell-lymphoma. Published 2018. Accessed July 14, 2019
- 35.Brody G S, Deapen D, Taylor C R.Anaplastic large cell lymphoma occurring in women with breast implants: analysis of 173 cases Plast Reconstr Surg 201513503695–705.. Doi: 10.1097/PRS.0000000000001033 [DOI] [PubMed] [Google Scholar]
- 36.Wroblewski L E, Peek R M, Jr, Wilson K T. Helicobacter pylori and gastric cancer: factors that modulate disease risk. Clin Microbiol Rev. 2010;23(04):713–739. doi: 10.1128/CMR.00011-10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Zhu H, Shen Z, Luo H, Zhang W, Zhu X.Chlamydia trachomatis infection-associated risk of cervical cancer: A meta-analysisMedicine (Baltimore)2016. 95(13):e3077 [DOI] [PMC free article] [PubMed]
- 38.Jacombs A, Tahir S, Hu H et al. In vitro and in vivo investigation of the influence of implant surface on the formation of bacterial biofilm in mammary implants. Plast Reconstr Surg. 2014;133(04):471e–480e. doi: 10.1097/PRS.0000000000000020. [DOI] [PubMed] [Google Scholar]
- 39.Hu H, Johani K, Almatroudi A et al. Bacterial biofilm infection detected in breast implant-associated anaplastic large-cell lymphoma. Plast Reconstr Surg. 2016;137(06):1659–1669. doi: 10.1097/PRS.0000000000002010. [DOI] [PubMed] [Google Scholar]
- 40.Sorotos M, Longo B, Amorosi V, Santanelli di Pompeo F. Macrotextured breast implants with defined steps to minimize bacterial contamination around the device: experience in 42,000 implants. Plast Reconstr Surg. 2018;142(03):412e–413e. doi: 10.1097/PRS.0000000000004654. [DOI] [PubMed] [Google Scholar]
- 41.Walker J N, Hanson B, Pinkner C L et al. Insights into the microbiome of breast implants and periprosthetic tissue in breast implant-associated anaplastic large cell lymphoma. Sci Rep. 2019;9(01):10393. doi: 10.1038/s41598-019-46535-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Deva A K. Reply: Chronic biofilm infection in breast implants is associated with an increased T-cell lymphocytic infiltrate: implications for breast implant-associated lymphoma. Plast Reconstr Surg. 2015;135(06):1059e–1060e. doi: 10.1097/PRS.0000000000001243. [DOI] [PubMed] [Google Scholar]
- 43.Kadin M E, Deva A, Xu H et al. Biomarkers provide clues to early events in the pathogenesis of breast implant-associated anaplastic large cell lymphoma. Aesthet Surg J. 2016;36(07):773–781. doi: 10.1093/asj/sjw023. [DOI] [PubMed] [Google Scholar]
- 44.Seif F, Khoshmirsafa M, Aazami H, Mohsenzadegan M, Sedighi G. The role of JAK-STAT signaling pathway and its regulators in the fate of T helper cells. Cell Commun Signal. 2017;15(01):23. doi: 10.1186/s12964-017-0177-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Coussens L M, Werb Z.Inflammation and cancer Nature 2002420(6917):860–867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Bizjak M, Selmi C, Praprotnik S et al. Silicone implants and lymphoma: The role of inflammation. J Autoimmun. 2015;65:64–73. doi: 10.1016/j.jaut.2015.08.009. [DOI] [PubMed] [Google Scholar]
- 47.Brody G S. The case against biofilm as the primary initiator of breast implant-associated anaplastic large cell lymphoma. Plast Reconstr Surg. 2016;137(04):766e–767e. doi: 10.1097/01.prs.0000480003.80422.03. [DOI] [PubMed] [Google Scholar]
- 48.Oishi N, Miranda R N, Feldman A L.Genetics of Breast Implant-Associated Anaplastic Large Cell Lymphoma (BIA-ALCL) Aesthet Surg J 201939(77, Supplement_1):S14–S20. [DOI] [PubMed] [Google Scholar]
- 49.Blombery P, Thompson E R, Jones K et al. Whole exome sequencing reveals activating JAK1 and STAT3 mutations in breast implant-associated anaplastic large cell lymphoma anaplastic large cell lymphoma. Haematologica. 2016;101(09):e387–e390. doi: 10.3324/haematol.2016.146118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Thomas S J, Snowden J A, Zeidler M P, Danson S J. The role of JAK/STAT signalling in the pathogenesis, prognosis and treatment of solid tumours. Br J Cancer. 2015;113(03):365–371. doi: 10.1038/bjc.2015.233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Letourneau A, Maerevoet M, Milowich D et al. Dual JAK1 and STAT3 mutations in a breast implant-associated anaplastic large cell lymphoma. Virchows Arch. 2018;473(04):505–511. doi: 10.1007/s00428-018-2352-y. [DOI] [PubMed] [Google Scholar]
- 52.Di Napoli A, Jain P, Duranti E et al. Targeted next generation sequencing of breast implant- associated anaplastic large cell lymphoma reveals mutations in JAK/STAT signalling pathway genes, TP53 and DNMT3A. Br J Haematol. 2018;180(05):741–744. doi: 10.1111/bjh.14431. [DOI] [PubMed] [Google Scholar]
- 53.Blombery P, Thompson E, Ryland G L et al. Frequent activating STAT3 mutations and novel recurrent genomic abnormalities detected in breast implant-associated anaplastic large cell lymphoma. Oncotarget. 2018;9(90):36126–36136. doi: 10.18632/oncotarget.26308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Lechner M G, Megiel C, Church C H et al. Survival signals and targets for therapy in breast implant-associated ALK--anaplastic large cell lymphoma. Clin Cancer Res. 2012;18(17):4549–4559. doi: 10.1158/1078-0432.CCR-12-0101. [DOI] [PubMed] [Google Scholar]
- 55.Hodge D R, Hurt E M, Farrar W L. The role of IL-6 and STAT3 in inflammation and cancer. Eur J Cancer. 2005;41(16):2502–2512. doi: 10.1016/j.ejca.2005.08.016. [DOI] [PubMed] [Google Scholar]
- 56.Yu H, Pardoll D, Jove R. STATs in cancer inflammation and immunity: a leading role for STAT3. Nat Rev Cancer. 2009;9(11):798–809. doi: 10.1038/nrc2734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Pastorello R G, D'Almeida Costa F, Osório C ABT et al. Breast implant-associated anaplastic large cell lymphoma in a Li-FRAUMENI patient: a case report. Diagn Pathol. 2018;13(01):10. doi: 10.1186/s13000-018-0688-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Bautista-Quach M A, Nademanee A, Weisenburger D D, Chen W, Kim Y S. Implant-associated primary anaplastic large-cell lymphoma with simultaneous involvement of bilateral breast capsules. Clin Breast Cancer. 2013;13(06):492–495. doi: 10.1016/j.clbc.2013.08.009. [DOI] [PubMed] [Google Scholar]
- 59.Clemens M W, Horwitz S M. NCCN consensus guidelines for the diagnosis and management of breast implant-associated anaplastic large cell lymphoma. Aesthet Surg J. 2017;37(03):285–289. doi: 10.1093/asj/sjw259. [DOI] [PubMed] [Google Scholar]
- 60.Clemens M W, Jacobsen E D, Horwitz S M.2019 NCCN consensus guidelines on the diagnosis and treatment of breast implant-associated anaplastic large cell lymphoma (BIA-ALCL) Aesthet Surg J 201939(Supplement_1):S3–S13. [DOI] [PubMed] [Google Scholar]
- 61.Adrada B E, Miranda R N, Rauch G M et al. Breast implant-associated anaplastic large cell lymphoma: sensitivity, specificity, and findings of imaging studies in 44 patients. Breast Cancer Res Treat. 2014;147(01):1–14. doi: 10.1007/s10549-014-3034-3. [DOI] [PubMed] [Google Scholar]
- 62.Cheson B D, Fisher R I, Barrington S F et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. 2014;32(27):3059–3068. doi: 10.1200/JCO.2013.54.8800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Mehta-Shah N, Clemens M W, Horwitz S M. How I treat breast implant-associated anaplastic large cell lymphoma. Blood. 2018;132(18):1889–1898. doi: 10.1182/blood-2018-03-785972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Richardson K, Alrifai T, Grant-Szymanski K et al. Breast implant-associated anaplastic large-cell lymphoma and the role of brentuximab vedotin (SGN-35) therapy: A case report and review of the literature. Mol Clin Oncol. 2017;6(04):539–542. doi: 10.3892/mco.2017.1170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Lamaris G A, Butler C E, Deva A Ket al. Breast reconstruction following breast implant-associated anaplastic large cell lymphoma Plast Reconstr Surg 2019143(3S A review of breast implant-associated anaplastic large cell lymphoma):51S–58S. [DOI] [PubMed] [Google Scholar]
- 66.O'Neill A C, Zhong T, Hofer S OP. Implications of breast implant-associated anaplastic large cell lymphoma (BIA-ALCL) for breast cancer reconstruction: an update for surgical oncologists. Ann Surg Oncol. 2017;24(11):3174–3179. doi: 10.1245/s10434-017-6014-0. [DOI] [PubMed] [Google Scholar]
- 67.Health R, Food U S.Anaplastic large cell lymphoma (ALCL) in women with breast implants: preliminary FDA findings and analysesU S FDA website.2011
- 68.Reisman N R. Discussion: breast implant informed consent should include the risk of anaplastic large cell lymphoma. Plast Reconstr Surg. 2016;137(04):1123. doi: 10.1097/PRS.0000000000002026. [DOI] [PubMed] [Google Scholar]
- 69.Roberts J M, Carr L W, Jones A, Schilling A, Mackay D R, Potochny J D. A prospective approach to inform and treat 1,340 patients at risk for BIA-ALCL. Plast Reconstr Surg. 2019;144(01):46–54. doi: 10.1097/PRS.0000000000005703. [DOI] [PubMed] [Google Scholar]
- 70.Haddock N T, Teotia S S. Discussion: a prospective approach to inform and treat 1,340 patients at risk for BIA-ALCL. Plast Reconstr Surg. 2019;144(01):57–59. doi: 10.1097/PRS.0000000000005755. [DOI] [PubMed] [Google Scholar]
- 71.Chung K C, Malay S, Shauver M J, Kim H M. Economic analysis of screening strategies for rupture of silicone gel breast implants. Plast Reconstr Surg. 2012;130(01):225–237. doi: 10.1097/PRS.0b013e318254b43b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.US Food and Drug Administration. FDA Requests Allergan Voluntary Recall. Available at:https://www.fda.gov/medical-devices/safety-communications/fda-requests-allergan-voluntarily-recall-natrelle-biocell-textured-breast-implants-and-tissue. Accessed August 15, 2019
- 73.Aladily T N, Medeiros L J, Amin M B et al. Anaplastic large cell lymphoma associated with breast implants: a report of 13 cases. Am J Surg Pathol. 2012;36(07):1000–1008. doi: 10.1097/PAS.0b013e31825749b1. [DOI] [PubMed] [Google Scholar]
- 74.Leberfinger A N, Behar B J, Williams N C et al. Breast implant-associated anaplastic large cell lymphoma: a systematic review. JAMA Surg. 2017;152(12):1161–1168. doi: 10.1001/jamasurg.2017.4026. [DOI] [PubMed] [Google Scholar]
- 75.Miranda R N, Medeiros L J, Ferrufino-Schmidt M Cet al. Pioneers of breast implant-associated anaplastic large cell lymphoma: history from case report to global recognition Plast Reconstr Surg 2019143(3S A review of breast implant-associated anaplastic large cell lymphoma):7S–14S. [DOI] [PubMed] [Google Scholar]