
Figure 1.
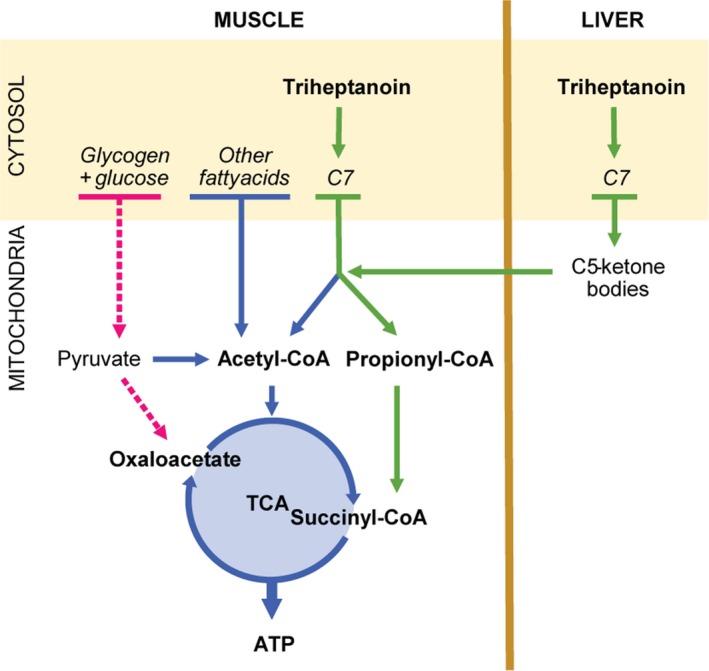
The suggested principles of treatment with triheptanoin in McArdle disease. The pyruvate pool is depleted in patients with McArdle disease due to the block in glycogenolysis. This may reduce levels of oxaloacetate in the tricarboxylic acid cycle (TCA), which slows the turnover rate of the TCA and limits the entry of acetyl‐CoA to the TCA. Almost all naturally occurring fatty acids have an even number of carbons. They are metabolized through beta‐oxidation cleaving off two carbons at a time producing acetyl‐CoA. Triheptanoin is a triglyceride of three 7‐carbon fatty acids (C7). The final step in the metabolism of odd number carbon fatty acids, such as C7, produces both acetyl‐CoA and propionyl‐CoA, which are converted to succinyl‐CoA, an intermediate of the TCA. The supplied succinyl‐CoA can potentially replenish the pool of TCA intermediates, boost the turnover of the TCA and enhance oxidative phosphorylation through increased metabolism of fatty acids and other substrates passing through the cycle. The liver can convert C7 to 5‐carbon (C5) ketone bodies, which are readily exported from the liver to the muscle. The breakdown of C5‐ketone bodies in the muscle produces acetyl‐CoA and propionyl‐CoA and contributes to the delivery of intermediates to the TCA.