

Abstract
OBJECTIVES:
To compare the accuracy of the linear measurements made on pre- and posttreatment three-dimensional (3D) scanned digital models with conventional plaster study models.
MATERIALS AND METHODS:
The study was conducted on pre- and posttreatment study models of 132 patients. A 3D model scanner was used to scan the plaster models to form 3D digital models. The measurements were made on the plaster models using digital Vernier calipers, and the 3D digital models were assessed for similar measurement using a software of the model scanner. The intraclass correlation for intraoperator error showed good correlations between the measurements made on conventional plaster models and digital models.
RESULTS:
Although the comparison of the linear measurements made by conventional and digital methods on both pre- and posttreatment study models using intraclass coefficient showed a good correlation, analysis of variance showed significant mean differences in the measurements of multiple variables in both the groups. The number of variables showing significant differences was more in the pretreatment group. The measurements obtained by Vernier calipers were generally higher than those of scanned pre- and posttreatment study models.
CONCLUSION:
The linear measurements made by conventional and digital methods showed statistically significant mean differences. The accuracy of recording can be affected by the severity of pretreatment malocclusion, but the deviations were not large enough to contradict the use of the digital models for orthodontic records.
Keywords: Conventional plaster models, digital study models, three-dimensional model scanner, three-dimensional study models
Introduction
The digital study models provide an alternative to the conventional plaster models for orthodontic records used for diagnosis, treatment planning, and to assess treatment progress.[1,2] OrthoCAD services were one of the earliest methods to form three-dimensional digital models. The orthodontists these days are widely using the 3D digital models. These can be prepared by either scanning the plaster models indirectly or using the intraoral scanner directly in the patient.[3] The advantages of the digital models over the conventional stone models include a decreased requirement of space for physical storage, risk-free, and cost-free transfer, the great potential for data processing, and no risk of breakage.[4] The 3D study models can replace the physical study models to provide a good visualization of malocclusion and assess tooth material arch length discrepancy, interarch relationship, tooth dimensions, arch forms, and dimensions.[5,6,7,8,9,10,11] The 3D models may also be used for diagnostic setup and superimposition to compare the treatment results. The orthodontists can print the physical models from the scanned models whenever required. The 3D models are the last step in the complete digitalization or paperless orthodontics. The digitization of plaster models and X-rays (Orthopantomogram [OPG], lateral cephalogram, Intra Oral Periapical Radiograph [IOPA]) has been commonly referred to as “green orthodontics” in our department.
The assessment GOSLON and VAS (visual analog scale) ranking commonly used in cleft patients can be done with a high degree of reliability on the digital models.[12] Garib et al.[13] showed a degree of reliability in the superimposition of the maxillary models with the digital models. Ko et al.[14] concluded that the treatment decisions were not affected by the digital or plaster models in orthodontic records. Tomita et al.[15] compared the digital models obtained from the scans of the plaster models and intraoral scanner and found the latter to be more accurate.
Santoro et al.[16] and Zilberman et al.[17] compared the accuracy of measurements made on the plaster models and digital measurements with OrthoCAD and found that the measurements on the plaster models were more accurate and reproducible. Earlier studies have assessed the accuracy of the digital models[4,10,16,18,19,20]; however, the complexity of malocclusion may affect the identification of contact points in the digital models. Thus, it is essential to compare the accuracy of measurements on pre- and posttreatment conventional and digital study models. This study aimed to evaluate the reliability, validity, and accuracy of the measurements made on pre- and posttreatment conventional plaster and digital study models. Thus, the objective of this study was to compare the accuracy of the linear measurements made on pre- and posttreatment plaster and digital scanned models.
Materials and Methods
This observational retrospective study was conducted on pre- and posttreatment conventional plaster study models obtained from the records of the Unit of Orthodontics and Dentofacial Orthopedics, Postgraduate Institute of Medical Education and Research, Chandigarh. The appropriate ethical clearance was obtained from the ethical committee of the institution. The debonded cases of years 2012–2017 were scanned and evaluated in 2018. The sample consisted of randomly selected 132 debonded cases with pretreatment Angle's Class I and Class II malocclusion with severe crowding, all permanent teeth in both the arches and study models of good quality with no fractured teeth or air bubbles. The alginate impressions of patients were used to prepare the plaster models. The 3D study models were prepared using the Maestro 3D Dental model scanner (AGE Solutions Sr.l, Pontedera, Pisa, Italy) from the same plaster models. The mesiodistal width, transverse dimensions (IC-MAX = maxillary intercanine width, IM-MAX = maxillary intermolar width, IC-MAND = mandibular intercanine width, IM-MAND = mandibular intermolar width), total tooth material (TM-MAX = maxillary tooth material, TM-MAND = mandibular tooth material), occlusogingival height (OG), arch length (AL-MAX = maxillary arch length, AL-MAND = mandibular arch length), overjet, and overbite of all the pre- and posttreatment models of the debonded cases were compared. All the measurements were done on maxillary and mandibular teeth till the first molars designated according to FDI notation system. The tooth size (mesiodistal width) was measured on plaster models using digital Vernier calipers with efficiency of up to 0.1 mm. A calibrated periodontal probe was used to measure the overjet and overbite on the occluded models. The similar measurements were made on the digital models with the help of analysis tools provided by the manufacturer [Figures 1–3]. A single operator made all the measurements after calibration and standardization. The intraexaminer reliability was statistically assessed by intraclass coefficient after repeating 10% of the measurements after 3 weeks. All the parameters assessed for intraobserver reliability by intraclass coefficient showed a good correlation for the repeated measurements [Table 1].
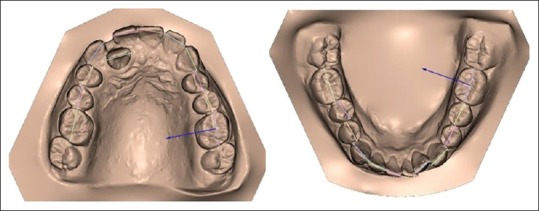
Figure 1.

Measurement of arch perimeter on digital maxillary and mandibular study models
Figure 3.
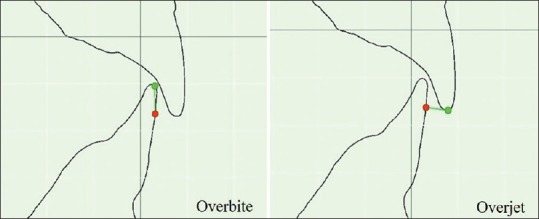
Measurement of overbite and overjet on digital study models
Table 1.
Intraexaminer reliability of conventional and digital methods
| Measurements | Intraclass correlation | |
|---|---|---|
| Manual | Digital | |
| 16 | 0.959 | 0.962 |
| 15 | 0.980 | 0.941 |
| 14 | 0.928 | 0.726 |
| 13 | 0.941 | 0.618 |
| 12 | 0.843 | 0.717 |
| 11 | 0.907 | 0.919 |
| 21 | 0.925 | 0.896 |
| 22 | 0.954 | 0.793 |
| 23 | 0.989 | 0.909 |
| 24 | 0.990 | 0.893 |
| 25 | 0.969 | 0.918 |
| 26 | 0.981 | 0.933 |
| 36 | 0.975 | 0.952 |
| 35 | 0.998 | 0.944 |
| 34 | 0.884 | 0.872 |
| 33 | 0.966 | 0.877 |
| 32 | 0.968 | 0.834 |
| 31 | 0.918 | 0.899 |
| 41 | 0.60 | 0.835 |
| 42 | 0.927 | 0.758 |
| 43 | 0.983 | 0.862 |
| 44 | 0.986 | 0.901 |
| 45 | 0.996 | 0.867 |
| 46 | 0.971 | 0.839 |
| IC-MAX | 0.821 | 0.874 |
| IM-MAX | 0.930 | 0.947 |
| IC-MAND | 0.943 | 0.947 |
| IM-MAND | 0.916 | 0.940 |
| TM-MAX | 0.823 | 0.892 |
| AL-MAX | 0.789 | 0.892 |
| TM-MAND | 0.847 | 0.827 |
| AL-MAND | 0.819 | 0.872 |
| OG | 0.959 | 0.956 |
| Overjet | 0.864 | 0.880 |
| Overbite | 0.847 | 0.879 |
16-46 – FDI tooth numbering system, IC-MAX – Maxillary intercanine width, IM-MAX – Maxillary intermolar width, IC-MAND – Mandibular intercanine width, IM-MAND – Mandibular intermolar width, TM-MAX – Maxillary tooth material, AL-MAX – Maxillary arch length, TM-MAND – Mandibular tooth material, AL-MAND – Mandibular arch length, OG – Occlusogingival height
Figure 2.
Measurement of mesiodistal width on digital maxillary and mandibular study models
Statistical analysis
Repeated measures analysis of variance and intraclass correlation coefficient were used to compare the pre- and posttreatment manual and digital measurements. All statistical tests were two-sided and were performed at a significance level of α = 0.05. The statistical analysis was performed using SPSS software version 25.0 (IBM Corp, Armonk, NY, USA).
Results
The comparison of linear measurements made by conventional and digital methods on both pre- and posttreatment study models using intraclass coefficient showed a good correlation [Table 2].
Table 2.
Intraclass correlation coefficient of conventional pre-treatment vs digital pre-treatment and conventional post-treatment vs digital post-treatment methods
| Measurements | Intraclass correlation | |
|---|---|---|
| Pre-Manual vs Pre-Digital | Post-Manual vs Post-Digital | |
| 16 | 0.936 | 0.943 |
| 15 | 0.913 | 0.935 |
| 14 | 0.923 | 0.835 |
| 13 | 0.923 | 0.866 |
| 12 | 0.971 | 0.916 |
| 11 | 0.958 | 0.939 |
| 21 | 0.948 | 0.951 |
| 22 | 0.962 | 0.941 |
| 23 | 0.910 | 0.908 |
| 24 | 0.918 | 0.916 |
| 25 | 0.872 | 0.926 |
| 26 | 0.947 | 0.937 |
| 36 | 0.864 | 0.920 |
| 35 | 0.898 | 0.895 |
| 34 | 0.876 | 0.846 |
| 33 | 0.828 | 0.798 |
| 32 | 0.919 | 0.880 |
| 31 | 0.921 | 0.962 |
| 41 | 0.865 | 0.875 |
| 42 | 0.916 | 0.919 |
| 43 | 0.919 | 0.892 |
| 44 | 0.866 | 0.929 |
| 45 | 0.931 | 0.909 |
| 46 | 0.936 | 0.932 |
| IC-MAX | 0.997 | 0.996 |
| IM-MAX | 0.997 | 0.994 |
| IC-MAND | 0.994 | 0.988 |
| IM-MAND | 0.996 | 0.994 |
| TM-MAX | 0.988 | 0.997 |
| AL-MAX | 0.840 | 0.970 |
| TM- MAND | 0.980 | 0.963 |
| AL- MAND | 0.947 | 0.983 |
| OG | 0.987 | 0.990 |
| Overjet | 0.996 | 0.994 |
| Overbite | 0.979 | 0.968 |
16-46 – FDI tooth numbering system, IC-MAX – Maxillary Intercanine width, IM-MAX – Maxillary Intermolar width, IC-MAND – Mandibular Intercanine width, IM-MAND – Mandibular Intermolar width, TM-MAX – Maxillary Tooth Material, AL-MAX – Maxillary Arch Length, TM-MAND – Mandibular Tooth Material, AL-MAND – Mandibular Arch Length, OG – Occlusogingival Height
Table 3 shows the comparison of the difference of means of the linear measurements made by conventional and digital methods which were significant for all the variables compared except tooth #15, 22, 25, 26, 31, 41, 42, 43, 45, and 46 (tooth numbering system – FDI notation), maxillary and mandibular intercanine width, maxillary intermolar width, maxillary arch length, and overjet. The manual measurements for all the variables compared were higher than the digital measurements except 16 and mandibular intermolar width. The difference in means of measurements made of pretreatment plaster study models and digital models were in the range of 0.013–0.32 mm.
Table 3.
Comparison of pre-treatment conventional and digital methods
| Manual (Mean±S.D) | Digital (Mean±S.D) | Mean Diff. | Significance | |
|---|---|---|---|---|
| 16 | 10.43±0.608 | 10.56±0.630 | -0.12303 | 0.002** |
| 15 | 6.85±0.507 | 6.80±0.485 | 0.04262 | 0.225 |
| 14 | 7.20±0.490 | 7.06±0.473 | 0.14136 | 0.000*** |
| 13 | 7.83±0.540 | 7.50±0.518 | 0.32323 | 0.000*** |
| 12 | 6.89±0.747 | 6.75±0.798 | 0.13828 | 0.000*** |
| 11 | 8.68±0.548 | 8.61±0.532 | 0.07061 | 0.010** |
| 21 | 8.69±0.549 | 8.65±0.571 | 0.04758 | 0.127 |
| 22 | 6.82±0.747 | 6.59±0.829 | 0.23068 | 0.000*** |
| 23 | 7.85±0.502 | 7.54±0.531 | 0.31662 | 0.000*** |
| 24 | 7.15±0.506 | 7.05±0.509 | 0.10061 | 0.005** |
| 25 | 6.83±0.559 | 6.76±0.548 | 0.07136 | 0.125 |
| 26 | 10.48±0.637 | 10.44±0.674 | 0.03379 | 0.353 |
| 36 | 10.88±0.567 | 10.72±0.604 | 0.15621 | 0.001*** |
| 35 | 7.23±0.492 | 7.05±0.510 | 0.18631 | 0.000*** |
| 34 | 7.18±0.493 | 7.03±0.558 | 0.15530 | 0.000*** |
| 33 | 6.86±0.501 | 6.73±0.553 | 0.12138 | 0.007** |
| 32 | 6.06±0.438 | 6.03±0.578 | 0.02923 | 0.551 |
| 31 | 5.40±0.416 | 5.34±0.454 | 0.06672 | 0.028* |
| 41 | 5.43±0.425 | 5.32±0.438 | 0.10652 | 0.000*** |
| 42 | 5.98±0.453 | 5.94±0.501 | 0.04394 | 0.282 |
| 43 | 6.87±0.470 | 6.80±0.508 | 0.07317 | 0.037 |
| 44 | 7.18±0.520 | 7.04±0.504 | 0.14227 | 0.000*** |
| 45 | 7.14±0.543 | 7.11±0.609 | 0.02262 | 0.647 |
| 46 | 10.80±0.567 | 10.81±0.601 | -0.01303 | 0.723 |
| IC-MAX | 33.84±3.574 | 33.80±3.423 | 0.04338 | 0.416 |
| IM-MAX | 50.88±2.979 | 50.90±2.959 | -0.02424 | 0.611 |
| IC-MAND | 25.03±2.753 | 25.21±2.833 | -0.17887 | 0.034* |
| IM-MAND | 43.97±3.062 | 44.79±3.060 | -0.81848 | 0.000*** |
| TM-MAX | 94.95±6.059 | 93.67±5.824 | 1.28061 | 0.000*** |
| AL-MAX | 93.89±5.352 | 94.33±5.606 | -0.43667 | 0.377 |
| TM-MAND | 86.11±5.398 | 85.03±5.461 | 1.08106 | 0.000*** |
| AL-MAND | 84.87±4.989 | 83.52±4.770 | 1.34470 | 0.005** |
| OG | 7.67±1.792 | 7.58±1.898 | 0.09037 | 0.000*** |
| Overjet | 3.76±3.041 | 3.94±2.976 | -0.13641 | 0.082 |
| Overbite | 4.57±2.075 | 4.22±2.063 | 0.35394 | 0.000*** |
*P=0.05; **P=0.01; ***P=0.001, 16-46 – FDI tooth numbering system, C-MAX – Maxillary Intercanine width, IM-MAX – Maxillary Intermolar width, IC-MAND – Mandibular Intercanine width, IM-MAND – Mandibular Intermolar width, TM-MAX – Maxillary Tooth Material, AL-MAX – Maxillary Arch Length, TM-MAND – Mandibular Tooth Material, AL-MAND – Mandibular Arch Length, OG – Occlusogingival Height
Table 4 shows the difference of the means of posttreatment linear measurements made by conventional and digital methods which were significant for all the following variables compared except tooth #16, 15, 14, 12, 11, 21, 22, 26, 36, 35, 34, 33, 32, 31, 41, 42, 44, 45, and 46, maxillary and mandibular intercanine width, and maxillary arch length. The manual measurements for all the variables compared were higher than the digital measurements except #16, 45, and 46, overjet, mandibular arch length, and mandibular intermolar width. The mean differences of measurements made of posttreatment plaster study models and digital models were in the range of 0.017–0.37 mm.
Table 4.
Comparison of post-treatment conventional and digital methods
| Manual (Mean±S.D) | Digital (Mean±S.D) | Mean Diff. | Significance | |
|---|---|---|---|---|
| 16 | 10.53±0.614 | 10.58±0.610 | -0.05333 | 0.131 |
| 15 | 6.87±0.494 | 6.85±0.533 | 0.01746 | 0.588 |
| 14 | 7.18±0.453 | 7.05±0.431 | 0.12886 | 0.014 |
| 13 | 7.90±0.547 | 7.53±0.480 | 0.37030 | 0.000*** |
| 12 | 7.06±0.686 | 6.96±0.639 | 0.10500 | 0.026 |
| 11 | 8.78±0.575 | 8.69±0.560 | 0.08515 | 0.014 |
| 21 | 8.80±0.551 | 8.70±0.580 | 0.09742 | 0.002 |
| 22 | 6.99±0.662 | 6.94±0.698 | 0.05031 | 0.210 |
| 23 | 7.95±0.533 | 7.69±0.525 | 0.26030 | 0.000*** |
| 24 | 7.21±0.457 | 7.06±0.470 | 0.15111 | 0.000*** |
| 25 | 6.93±0.512 | 6.82±0.497 | 0.10919 | 0.002** |
| 26 | 10.55±0.644 | 10.58±0.646 | -0.02530 | 0.517 |
| 36 | 10.97±0.568 | 10.95±0.579 | 0.01667 | 0.666 |
| 35 | 7.25±0.544 | 7.21±0.528 | 0.04484 | 0.290 |
| 34 | 7.09±0.470 | 6.99±0.402 | 0.09646 | 0.042 |
| 33 | 6.96±0.493 | 6.86±0.506 | 0.10108 | 0.051 |
| 32 | 5.99±0.484 | 6.04±0.468 | -0.04906 | 0.212 |
| 31 | 5.41±0.466 | 5.42±0.504 | -0.00864 | 0.723 |
| 41 | 5.40±0.410 | 5.39±0.428 | 0.01079 | 0.760 |
| 42 | 5.99±0.510 | 5.94±0.493 | 0.05545 | 0.106 |
| 43 | 6.98±0.466 | 6.74±0.520 | 0.23875 | 0.000*** |
| 44 | 7.09±0.484 | 6.99±0.526 | 0.10426 | 0.008** |
| 45 | 7.20±0.533 | 7.25±0.562 | -0.04934 | 0.229 |
| 46 | 10.95±0.570 | 10.99±0.625 | -0.04545 | 0.225 |
| IC-MAX | 35.28±2.408 | 35.20±2.271 | 0.08485 | 0.307 |
| IM-MAX | 50.73±2.972 | 50.95±2.911 | -0.22394 | 0.007** |
| IC-MAND | 26.04±2.569 | 26.14±2.431 | -0.10048 | 0.193 |
| IM-MAND | 43.68±2.846 | 44.51±2.774 | -0.83136 | 0.000*** |
| TM-MAX | 91.00±7.622 | 89.80±7.536 | 1.19394 | 0.000*** |
| AL-MAX | 91.14±7.105 | 91.37±7.520 | -0.22606 | 0.365 |
| TM-MAND | 81.09±6.590 | 80.65±6.601 | 0.44273 | 0.006** |
| AL-MAND | 81.63±6.159 | 82.26±6.697 | -0.62773 | 0.128 |
| OG | 7.75±1.735 | 7.66±1.833 | 0.08721 | 0.000*** |
| Overjet | 1.93±1.473 | 2.14±1.598 | -0.20273 | 0.000*** |
| Overbite | 2.60±1.315 | 2.26±1.283 | 0.34061 | 0.000*** |
**P=0.01; ***P=0.001, 16-46 – FDI tooth numbering system, IC-MAX – Maxillary Intercanine width, IM-MAX – Maxillary Intermolar width, IC-MAND – Mandibular Intercanine width, IM-MAND – Mandibular Intermolar width, TM-MAX – Maxillary Tooth Material, AL-MAX – Maxillary Arch Length, TM-MAND – Mandibular Tooth Material, AL-MAND – Mandibular Arch Length, OG – Occlusogingival Height
Out of the 24 mesiodistal tooth measurements made on pretreatment models, the differences were significant for 14 measurements, whereas only 5 tooth measurements showed significant mean differences in the posttreatment study models. Maxillary canines showed significant differences in the mesiodistal measurements in both pre- and post-treatment models. The intercanine width measurements did not show significant mean differences in the pre- and posttreatment models. The arch length measurements did not show significant mean differences in posttreatment models. The overjet measurement showed significant mean differences in the posttreatment models, whereas the overbite measurement showed significant mean differences in both pre- and posttreatment models.
Discussion
This study showed good reproducibility of the measurement in both plaster and digital models similar to the studies by Okunami et al.,[8] Zilberman et al.,[13] Stevens et al.,[20] Quimby et al.,[21] and Bell et al.[22] The mesiodistal measurements on the digital pre- and posttreatment study models in this study were generally lesser than the manual measurements, as concluded by Stevens et al.,[20] Mullen et al.,[23] and Redlich et al.[24] in their studies. The range of the difference of the means (0.013–0.32 in pretreatment and 0.017–0.37 in posttreatment models) was statistically significant although they were not clinically significant as intraoperator error according to a study varies between 0.10 and 0.48 mm which is larger than the errors recorded in comparison in this study.[22] The findings are similar to the study by Santoro et al.[16] where the digital measurements were lesser than manual, and the range of the mean difference was 0.016–0.32. El-Zanaty et al.[25] found a strong correlation in the mesiodistal measurements of all the teeth similar to this study where the digital and manual measurements show a strong correlation. A study by Scott et al.[26] evaluated and compared the ABO-cast radiograph evaluation scores by the automated manner by the Sure smile and hand grading. The automated scores were found to be significantly higher than hand grading.
The critical analysis showed that the mean differences were highest for maxillary canines, and the difference was statistically significant for both the groups. Thus, the mesiodistal measurement of maxillary canines (13, 23) on both pre- and post-treatment study models generally showed maximum deviation and should be considered with caution during measurement. The deviation in the measurements may be due to the curvature of the arch in the canine region. Although some of the transverse measurements may show significant differences, they were not clinically relevant. The intercanine width measurements did not show significant differences in pre- and posttreatment study models because locating the canine tip is much more comfortable. Occlusogingival digital measurements were also lesser than manual measurements similar to mesiodistal measurements and statistically significant but were not clinically relevant. The overbite measurements showed increased values for the manual measurements and the differences were statistically significant. Similarly, the study by Santoro et al.[12] also showed increased mean differences for overbite of 0.49 mm on average higher than 0.36 mm in this study. According to Sousa et al.,[5] the measurements of the arch length and arch width on the digital models were reliable. They found similar values for the linear measurements obtained from the digital models contrary to this study. The number of variables with a significant difference of means was lesser in the posttreatment study models than the pretreatment, thus showing lesser error/differences in the measurements on posttreatment digital models. The lesser errors in the posttreatment study models may be due to the malocclusion in the pretreatment models making the measurements difficult.
Conclusion
This study concludes excellent reliability and reproducibility of measurements made on the scanned digital models
The digital measurement values were generally lower than the manual measurements for most of the variables. The difference of the means between the digital and manual measurements was lesser in the posttreatment models. Hence, the accuracy of the measurements on posttreatment digital models was more
The maxillary canines at the transition of arch showed maximum mean differences in the mesiodistal measurements among all the teeth in both pre- and posttreatment models
The overbite measurements were affected in both the pre- and posttreatment models
The intercanine width measurements were least affected in pre- and posttreatment models
Although the differences in the manual and digital measurements were statistically significant for certain variables, they were not clinically relevant.
Thus, the digital models may replace the conventional plaster models and are acceptable for measurements and analysis without significant discrepancies.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Redmond WR. Digital models: A new diagnostic tool. J Clin Orthod. 2001;35:386–7. [PubMed] [Google Scholar]
- 2.Redmond WR. The digital orthodontic office: 2001. Semin Orthod. 2001;7:266–73. [Google Scholar]
- 3.Marcel TJ. Three-dimensional on-screen virtual models. Am J Orthod Dentofacial Orthop. 2001;119:666–8. doi: 10.1067/mod.2001.116502. [DOI] [PubMed] [Google Scholar]
- 4.Abizadeh N, Moles DR, O'Neill J, Noar JH. Digital versus plaster study models: How accurate and reproducible are they? J Orthod. 2012;39:151–9. doi: 10.1179/1465312512Z.00000000023. [DOI] [PubMed] [Google Scholar]
- 5.Sousa MVS, Vasconcelos EC, Janson G, Garib D, Pinzan A. Accuracy and reproducibility of 3-dimensional digital model measurements. Am J Orthod Dentofacial Orthop. 2012;142:269–73. doi: 10.1016/j.ajodo.2011.12.028. [DOI] [PubMed] [Google Scholar]
- 6.Naidu D, Freer TJ. Validity, reliability, and reproducibility of the iOC intraoral scanner: A comparison of tooth widths and Bolton ratios. Am J Orthod Dentofacial Orthop. 2013;144:304–10. doi: 10.1016/j.ajodo.2013.04.011. [DOI] [PubMed] [Google Scholar]
- 7.Tomassetti JJ, Taloumis LJ, Denny JM, Fischer JR., Jr A Comparison of 3 computerized Bolton tooth-size analyses with a commonly used method. Angle Orthod. 2001;71:351–7. doi: 10.1043/0003-3219(2001)071<0351:ACOCBT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 8.Okunami TR, Kusnoto B, BeGole E, Evans CA, Sadowsky C, Fadavi S. Assessing the American Board of Orthodontics objective grading system: Digital vs plaster dental casts. Am J Orthod Dentofacial Orthop. 2007;131:51–6. doi: 10.1016/j.ajodo.2005.04.042. [DOI] [PubMed] [Google Scholar]
- 9.Costalos PA, Sarraf K, Cangialosi TJ, Efstratiadis S. Evaluation of the accuracy of digital model analysis for the American Board of Orthodontics objective grading system for dental casts. Am J Orthod Dentofacial Orthop. 2005;128:624–9. doi: 10.1016/j.ajodo.2004.08.017. [DOI] [PubMed] [Google Scholar]
- 10.Horton HMI, Miller JR, Gaillard PR, Larson BE. Technique comparison for efficient orthodontic tooth measurements using digital models. Angle Orthod. 2010;80:254–61. doi: 10.2319/041709-219.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Burns A, Dowling AH, Garvey TM, Fleming GJP. The reliability of Little's Irregularity Index for the upper dental arch using three dimensional (3D) digital models. J Dent. 2014;42:1320–6. doi: 10.1016/j.jdent.2014.07.012. [DOI] [PubMed] [Google Scholar]
- 12.Fowler P, Bellardie H, Shaw B, Eyres P, Semb G, Thompson J. Reliability of a categorical scale (GOSLON) and a continuous scale (10-cm Visual Analog Scale) for assessing dental arch relationships using conventional plaster and 3D digital orthodontic study models of children with complete unilateral cleft lip and palate. Cleft Palate Craniofac J. 2019;56:84–9. doi: 10.1177/1055665618770054. [DOI] [PubMed] [Google Scholar]
- 13.Garib D, Miranda F, Yatabe MS, Lauris JRP, Massaro C, McNamara JA, et al. superimposition of maxillary digital models using the palatal rugae: Does ageing affect the reliability? Orthod Craniofac Res. 2019;22:183–93. doi: 10.1111/ocr.12309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ko HC, Liu W, Hou D, Torkan S, Spiekerman C, Huang GJ. Recommendations for clear aligner therapy using digital or plaster study casts. Prog Orthod. 2018;19:22. doi: 10.1186/s40510-018-0224-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tomita Y, Uechi J, Konno M, Sasamoto S, Iijima M, Mizoguchi I. Accuracy of digital models generated by conventional impression/plaster-model methods and intraoral scanning. Dent Mater J. 2018;37:628–33. doi: 10.4012/dmj.2017-208. [DOI] [PubMed] [Google Scholar]
- 16.Santoro M, Galkin S, Teredesai M, Nicolay OF, Cangialosi TJ. Comparison of measurements made on digital and plaster models. Am J Orthod Dentofacial Orthop. 2003;124:101–5. doi: 10.1016/s0889-5406(03)00152-5. [DOI] [PubMed] [Google Scholar]
- 17.Zilberman O, Huggare J, Parikakis KA. Evaluation of the validity of tooth size and arch width measurements using conventional and three-dimensional virtual orthodontic models. Angle Orthod. 2003;73:301–6. doi: 10.1043/0003-3219(2003)073<0301:EOTVOT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 18.Akyalcin S, Dyer DJ, English JD, Sar C. Comparison of 3-dimensional dental models from different sources: Diagnostic accuracy and surface registration analysis. Am J Orthod Dentofacial Orthop. 2013;144:831–7. doi: 10.1016/j.ajodo.2013.08.014. [DOI] [PubMed] [Google Scholar]
- 19.Wiranto MG, Engelbrecht WP, Tutein Nolthenius HE, van der Meer WJ, Ren Y. Validity, reliability, and reproducibility of linear measurements on digital models obtained from intraoral and cone-beam computed tomography scans of alginate impressions. Am J Orthod Dentofacial Orthop. 2013;143:140–7. doi: 10.1016/j.ajodo.2012.06.018. [DOI] [PubMed] [Google Scholar]
- 20.Stevens DR, Flores-Mir C, Nebbe B, Raboud DW, Heo G, Major PW. Validity, reliability, and reproducibility of plaster vs digital study models: Comparison of peer assessment rating and Bolton analysis and their constituent measurements. Am J Orthod Dentofacial Orthop. 2006;129:794–803. doi: 10.1016/j.ajodo.2004.08.023. [DOI] [PubMed] [Google Scholar]
- 21.Quimby ML, Vig KWL, Rashid RG, Firestone AR. The accuracy and reliability of measurements made on computer-based digital models. Angle Orthod. 2004;74:298–303. doi: 10.1043/0003-3219(2004)074<0298:TAAROM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 22.Bell A, Ayoub AF, Siebert P. Assessment of the accuracy of a three-dimensional imaging system for archiving dental study models. J Orthod. 2003;30:219–23. doi: 10.1093/ortho/30.3.219. [DOI] [PubMed] [Google Scholar]
- 23.Mullen SR, Martin CA, Ngan P, Gladwin M. Accuracy of space analysis with e-models and plaster models. Am J Orthod Dentofacial Orthop. 2007;132:346–52. doi: 10.1016/j.ajodo.2005.08.044. [DOI] [PubMed] [Google Scholar]
- 24.Redlich M, Weinstock T, Abed Y, Schneor R, Holdstein Y, Fischer A. A new system for scanning, measuring and analyzing dental casts based on a 3D holographic sensor. Orthod Craniofac Res. 2008;11:90–5. doi: 10.1111/j.1601-6343.2007.00417.x. [DOI] [PubMed] [Google Scholar]
- 25.El-Zanaty HM, El-Beialy AR, Abou El-Ezz AM, Attia KH, El-Bialy AR, Mostafa YA. Three-dimensional dental measurements: An alternative to plaster models. Am J Orthod Dentofacial Orthop. 2010;137:259–65. doi: 10.1016/j.ajodo.2008.04.030. [DOI] [PubMed] [Google Scholar]
- 26.Scott JD, English JD, Cozad BE, Borders CL, Harris LM, Moon AL, et al. Comparison of automated grading of digital orthodontic models and hand grading of 3-dimensionally printed models. Am J Orthod Dentofacial Orthop. 2019;155:886–90. doi: 10.1016/j.ajodo.2018.11.011. [DOI] [PubMed] [Google Scholar]