
Figure 3.
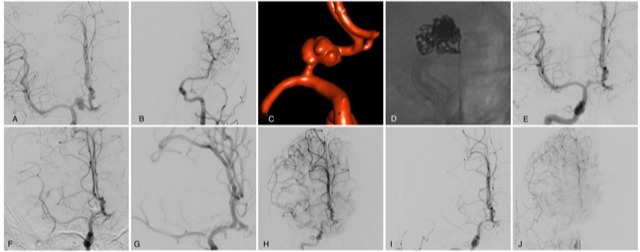
Case 1: Teenage patient with history of bicoronal craniotomy for craniopharyngioma resection followed by proton beam therapy who presented with (A) R ICA DSA showing 11 mm A1 aneurysm and (B) L CCA DSA showing hypoplastic left ACA. (C) 3-D rotational angiography shows fusiform and highly irregular morphology. (D) Unsubtracted DSA from treatment with single-stage pipeline with adjunctive coiling from R ACA into R ICA. Follow-up R CCA DSA at (E) 2 months shows dome occlusion of the aneurysm with residual neck filling and anterograde arterial phase filling of the jailed R MCA. (F) 6 months shows some ghosting across the M1, (G,H) increased ghosting at 12 months follow-up DSA after stopping Plavix with significant recruitment of pial collaterals from the ACA in the late arterial and parenchymal phase. (I) 24-month DSA arterial phase shows limited anterograde filling of the jailed MCA and (J) robust pial collaterals from ACA and ECA apparent on parenchymal phase runs. ACA, anterior cerebral artery; CCA, common carotid artery; DSA, digital subtraction angiography; ECA, external carotid artery; ICA, internal carotid artery; MCA, middle cerebral artery.