

Abstract
Introduction
Acquired nasopharyngeal stenosis after radiotherapy for NPC is rare. We report a case of bilateral choanal stenosis and nasopharygeal stenosis in patient treated with chemo radiotherapy for undifferentieted nasopharnygeal carcinoma.
Case Report
A 68 years old man treated for undifferentiated nasopharyngeal carcinoma with chemo-radiotherapy 10 years before. He complained of complete nasal obstruction, rhinorrhea, anosmia, snoring and hearing loss. Clinical examination and imaging revealed bilateral choanal stenosis and nasopharyngeal stenosis. Patient underwent a transnasal endoscopic resection for scar tissue with stenting of posterior choanae. Restenosis was noted just after stent removal. Second endoscopic resection of stenosis was done, followed by application of mitomycin-C without stenting. Several months later, the patient has good airflow, a patent nasopharynx without reccurence of stenosis.
Discussion
The use of topical mitomycin-C may prove useful in the treatment and prevention of subsequent restenosis and scar formation in larynx and tracheal. Mitomycin-C application has being shown useful in treating nasopharyngeal stenosis. It is safely used topically in various surgical sites without major side effect.
Conclusion
Nasopharyngeal stenosis is an unusual complication of radiotherapy that can be successfully treated with combine two modalities: surgical and mitomycin-C as an adjunct.
Keywords: Nasopharyngeal carcinoma, Stenosis, Radiotherapy, Mitomycin C
Introduction
Choanal stenosis, usually a congenital anomaly in children, has recently been recognized as a late complication of radiation therapy for nasopharyngeal carcinoma. [1]. We report a case of nasopharyngeal stenosis post-radiotherapy and challenges in its treatment. We also review literature on treatment options and described our management of this patient which was successfully treated by combine two modalities: surgery and mitomycin-C applied topically.
Case Report
A 68 year-old man presented with complete nasal obstruction, rhinorrhea, anosmia, snoring and hearing loss. He was treated 10 years before by chemo-radiotherapy for undifferentiated nasopharyngeal carcinoma.
On examination, the air flow was absent on the both side of nasal cavity. Rigid endoscopic nasal examination revealed pale mucous with lot of rhinorrhea and bilateral choanal stenosis. There was no local or regional recurrence. Otoscopic examination revealed bilateral serous otitis media. The pure tone audiogram shown severe mixed hearing loss and both tympanometry were of Type C. A computer tomography scan of nose and paranasal sinuses showed a soft tissue density lesion occupying bilateral choanae and confirmed the diagnosis of nasopharyngeal stenosis (Fig. 1a, b).
Fig. 1.
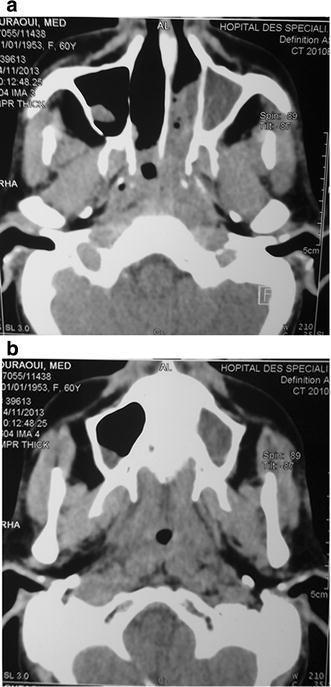
a, b CT scan showing the nasopharyngeal and bilateral choanal stenosis
Patient underwent a transnasal endoscopic resection of scar tissue and the posterior choanae was stented by tutor. Transtympanic aerator was established in both ears. Restenosis were noted just after sent removal. Few months later, second release of stenosis was done with removal of posterior wall of septum and wide resection of fibrosis tissue, topical mitomycin-C was applied to surgical wound without stent insertion. Follow up with clinical examination, endoscopic control and imaging was favorable without restenosis after several months of recoil (Fig. 2).
Fig. 2.
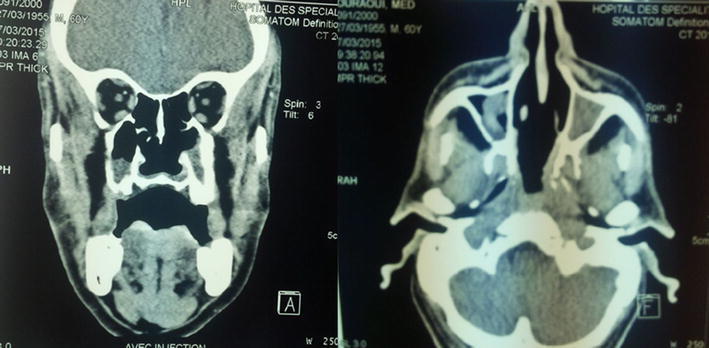
CT scan showing the post operative result after surgical desobstruction and mitomycine C application
Discussion
Choanal stenosis is a well recognized late complication of radiotherapy for nasopharyngeal carcinoma [2]. However velopharyngeal stenosis following radiotherapy is rare. The pathogenesis of postradiotherapy choanal stenosis is uncertain. It is thought that it may appear as a result of severe mucosal reaction that occurs after radiotherapy followed by fibrosis and scar tissue formation [3]. The literature reports that the majority of the cases were due to tertiary syphilis infection of oropharyngeal and oral cavity. Other rare cause includes rhinoscleroma, lupus, dyphteria and tuberculosis [4].
The rate of choanal stenosis after radiotherapy for NPC range from 7 to 15 % [5, 6]. Nasopharyngeal stenosis is rare. There is no relationship between the stage of nasopharyngeal carcinoma, the dosage or technique of irradiation delivered to patient and the occurrence of choanal or nasopharyngeal stenosis [6].
Clinically, the severity of symptoms is closely related to the degree of stenosis: patient with nasopharyngeal stenosis can present with a varying severity of mouth breathing, snoring, rhinorhea, anosmia, hyponasality, dysphagia, otalgia and loss of hearing [6].
As in our case, nasopharyngeal stenosis was not obvious on endoscopic examination because it was obscure by the choanal stenosis and the computer tomography scan confirmed the diagnosis.
Treatment of choanal stenosis and nasopharygeal stenosis is challenging due the high incidence of recurrence.
Various methods and procedure for reparing this problem have been described from mucosal flaps with stent positioning to recent radiofrequency excision with mitomycin-C application [2]; but none has shown clearly superior results in treating this difficult problem.
Authors revealed that a repeat operation is performed of 10–20 % patients [1]. As in our case, first intervention using transnasal endoscopic resection of scar tissue and stenting of posterior choanae had failed [1–7].
Our patient underwent a transnasal endoscopic excision of velopharyngeal scar tissue and widening of posterior choanal stenosis with a resection of posterior septum, mitomycin-C applied topically to the surgical wound without any stenting under general anesthesia. We practice 10 days after a second mitomycine C application.
Surgeons whom do not advocate post-operative stenting often have to perform serial dilatations or revision endoscopy to remove crusting [8].
Also, Hussein et al. [2] had reported a successful management of a velopharyngeal stenosis case by transnasal endoscopic excision of scar tissue and widening of choanal stenosis using Surgitron® with application of mitomycin-C and stenting.
The use of topical mitomycin-C may prove useful in the treatment and prevention of subsequent restenosis and scar formation in larynx and tracheal. It can also reduce the risk of synechiae formation after endoscopic sinus surgery [6].
Mitomycin-C application has being shown useful in treating nasopharyngeal stenosis [2]. It is an antineoplastic antibiotic that acts as alkylating agent by inhibiting cell division, protein synthesis and fibroplast proliferation [9]. It is safely used topically in various surgical sites without major side effect [10].
Conclusion
Choanal stenosis is a well-recognized late complication of radiotherapy for nasopharyngeal carcinoma; however nasopharyngeal stenosis is very exceptional. Systematic endoscopic examination is recommended in follow up of all patients treated for NPC even cured. The treatment of this complication is challenging due the high incidence of recurrence. Mitomycin-C has being shown useful adjunct to surgical technique in managing nasopharyngeal stenosis.
Compliance with Ethical Standards
Conflict of interest
The authors declare no conflict of interest.
References
- 1.Lee SC, Tang P, Singh A, Kumar SS, Singh S. Velopharyngeal stenosis, a late complication of radiotherapy. Auris Nasus Larynx. 2009;36:709–711. doi: 10.1016/j.anl.2009.02.002. [DOI] [PubMed] [Google Scholar]
- 2.Hussein J, Tan TS, Chong AW, Narayanan P, Omar R. Velopharyngeal and choanal stenosis after radiotherapy for nasopharyngeal carcinoma. Auris Nasus Larynx. 2013;40(40):323–326. doi: 10.1016/j.anl.2012.05.004. [DOI] [PubMed] [Google Scholar]
- 3.Ku PKM, Tong MCF, Tsang SS, Van Hasselt A. Acquired posterior choanal stenosis and atresia: management of this unusual complication after radiotherapy for nasopharyngeal carcinoma. Am J Otolarngol. 2001;22:225–229. doi: 10.1053/ajot.2001.24816. [DOI] [PubMed] [Google Scholar]
- 4.Bonfils P, De Preobrajenski N, Florent A, Bensimon JL. Sténose choanale post-radique: une complication rare de la radiothérapie des carcinomes nasopharyngés. Cancer/Radiothér. 2007;11:143–145. doi: 10.1016/j.canrad.2006.10.004. [DOI] [PubMed] [Google Scholar]
- 5.Alon EE, Lipschitz N, Bedrin L, Gluck I, Talmi Y, Wolf M, Yakirevitch A. Delayed sino-nasal complications of radiotherapy for nasopharyngeal carcinoma. Otolaryngol Head Neck Surg. 2014;151(2):354–358. doi: 10.1177/0194599814530858. [DOI] [PubMed] [Google Scholar]
- 6.Singh B. Bilateral choanal atresia: key to success with the transnasal approach. J Laryngol Otol. 1990;104:482–484. doi: 10.1017/S0022215100112939. [DOI] [PubMed] [Google Scholar]
- 7.Giannoni C, Sulek M, Friedman EM, Duncan NO. Acquired nasopharyngeal stenosis. Arch Otolaryngol Head Neck Surg. 1998;124:163–167. doi: 10.1001/archotol.124.2.163. [DOI] [PubMed] [Google Scholar]
- 8.Van Den Abbeele T, Francois M, Narcy P. Transnasal endoscopic treatment of choanal atresia without prolonged stenting. Arch Otolaryngol Head Neck Surg. 2002;128:936–940. doi: 10.1001/archotol.128.8.936. [DOI] [PubMed] [Google Scholar]
- 9.Jones LM, Guillory VL, Mair EA. Total nasopharyngeal stenosis: treatment with laser excision, nasopharyngeal obturators and topical mitomycin-C. Otolaryngol Head Neck Surg. 2005;133(5):795–798. doi: 10.1016/j.otohns.2005.07.005. [DOI] [PubMed] [Google Scholar]
- 10.Rosseneu S, Afzal N, Yerushalmi B, Ibarguen-Secchia E, Lewindon P, Cameron D, et al. Topical application of mitomycin-C in oesophageal strictures. J Pediatr Gastroenterol Nutr. 2007;44:336–341. doi: 10.1097/MPG.0b013e31802c6e45. [DOI] [PubMed] [Google Scholar]