
Figure 5.
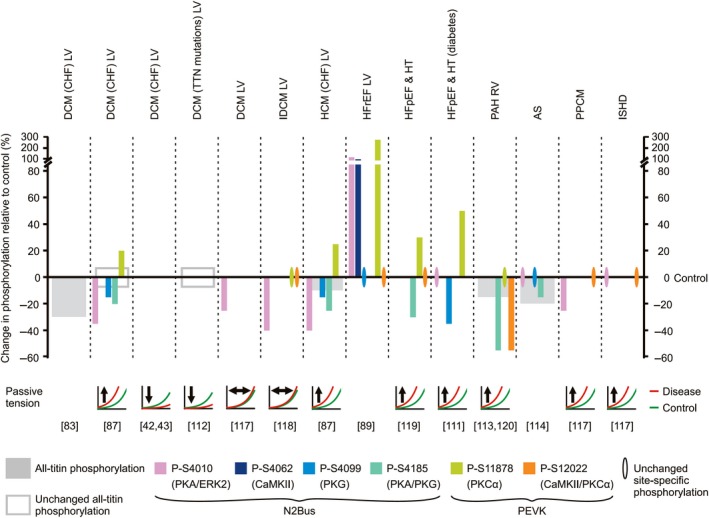
Changes in titin phosphorylation in human failing hearts and relationship with alterations in cardiomyocyte passive tension. The size of the bars indicates the relative amount of change in phosphorylation in failing vs. nonfailing hearts (for some conditions, an average value is shown). The relative changes are as indicated by the respective study authors and therefore, magnitude comparisons between studies may not be plausible. Note the absence of hyperphosphorylation of all‐titin. Also, note the general pattern of hypophosphorylation at one or more N2Bus sites and hyperphosphorylation at PEVK site S11878, whereas phosphorylation at S12022 mostly remains unaltered. For those studies where titin‐based passive tension was measured, the direction of change (arrow) in disease (red lines) relative to healthy heart samples (green lines) is indicated. Protein kinases known to target individual phosphosites are listed in parentheses. References are in square brackets. DCM, dilated cardiomyopathy; CHF, congestive heart failure; IDCM, idiopathic DCM; HCM, hypertrophic cardiomyopathy; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; HT, hypertensive heart disease; PAH, pulmonary arterial hypertension; AS, aortic stenosis; PPCM, peripartum cardiomyopathy; ISHD, ischemic heart disease. LV, left ventricle; RV, right ventricle.