

ABSTRACT
There have been various clinical studies on the effect of flaxseed-derived products on circulating inflammatory biomarkers, but the findings from these are contradictory. The aim of the present study was to clarify any association. A comprehensive literature search was conducted from inception to May 2018. From the eligible trials, 32 articles describing studies conducted on adults aged 18–70 y were selected for the meta-analysis. Meta-analyses using the random-effects model were performed to investigate the data and results showed significant effects of flaxseed intake on circulating high-sensitivity CRP (hs-CRP) [weighted mean difference (WMD) = −0.75; 95% CI: −1.19, −0.30; P < 0.001] and TNFα (WMD = −0.38; 95% CI: −0.75,–0.01; P = 0.04). However, no significant changes were found in IL6 concentration (WMD = −0.24; 95% CI: –0.70, 0.21; P = 0.28) and C-reactive protein (CRP) (WMD = −0.34; 95% CI:–0.89, 0.20; P = 0.22). Moreover, by eliminating 1 of the studies from the sensitivity analysis, changes in IL6 concentration were significant (WMD = −0.44; 95% CI: –0.81, –0.08). The changes in inflammatory biomarkers were dependent on study design (parallel or crossover), supplement type (flaxseed, flaxseed oil, or lignan), study quality (high or low), and participants’ age and BMI. According to this meta-analysis, flaxseed significantly reduced circulating concentrations of hs-CRP and TNFα, but did not affect IL6 and CRP. Further research is needed to examine the effect of different doses and long-term benefits of flaxseed and its derivatives on inflammatory factors.
Keywords: flaxseed, lignans, inflammatory markers, meta-analysis, randomized controlled trials, inflammatory disease
Introduction
According to previous relevant studies, the role of inflammation is critical in various diseases, including cardiovascular disease (CVD), chronic kidney disease, type 2 diabetes, chronic obstructive pulmonary disease, and cancer (1, 2). Predominant markers of inflammation such as TNFα, C-reactive protein (CRP), and IL6 are positively associated with various chronic disorders. TNFα and IL6 are the most important cytokines released in large amounts during inflammation and play critical roles as mediators in CVD and other chronic diseases. Also, they are potent stimulants for CRP production, which has been shown to be a strong risk factor for chronic disorders. Several therapeutic approaches including anti-inflammatory agents and monoclonal antibodies are being used in emerging clinical management in inflammation-related diseases (1, 3).
Evidence from several studies has shown that some dietary factors such as plant sterols, dietary fiber, isoflavones, phytoestrogens, lignans, and ω-3 PUFA including EPA, DHA, and α-linolenic acid (ALA) have revealed anti-inflammatory properties (4–6). According to epidemiologic studies, ALA can reduce the morbidity and mortality rate of CVD. The mechanism of action for this fatty acid is not clear yet, but anti-inflammatory properties are involved in the beneficial effects (7).
Flaxseed (linseed, Linum usitatissimum), an edible oil-rich seed/grain and 1 of the oldest arable crops, was recently acknowledged as a functional food (8). Flaxseed contains a high concentration of ALA, soluble fiber, lignan precursors, and other substances that may have many health benefits (9).
Flaxseed is the richest dietary source of the plant lignan secoisolariciresinol diglucoside (SDG), which is metabolized to the mammalian lignans enterodiol and enterolactone by colonic bacteria (10). According to various studies, CRP concentration can be reduced significantly by SDG (11).
Many clinical trials have been performed to determine the effect of flaxseed intervention (whole flaxseed, flaxseed oil, or lignans) on various inflammatory biomarkers in different chronic diseases (12, 13). Despite existing claims about the effects of flaxseed or its derivatives on inflammatory markers, the results of these studies remain conflicting. Thus, the present meta-analysis was conducted to summarize the available evidence regarding the effect of flaxseed or its derivatives on inflammatory markers (TNFα, IL6, CRP, and hs-CRP).
Methods
This research was conducted by following the guidelines and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement for reporting systematic reviews and meta-analyses of studies. Table 1 shows the population, intervention, comparator, outcome, and setting criteria used to perform the systematic review. According to the local legislation, ethical approval is not necessary for this study type (meta-analysis and systematic review). The study protocol was registered on PROSPERO (registration number: CRD42018095788).
TABLE 1.
PICOS (population, intervention, comparator, outcome, and setting) criteria used to perform the systematic review and meta-analyses1
| PICOS | Criteria |
|---|---|
| Population | Patients with chronic disease and healthy subjects |
| Intervention | Flaxseed and its derivatives |
| Comparator | Placebo group |
| Outcome | Circulating CRP, hs-CRP, IL6, and TNFα |
| Setting | Clinical trials |
CRP, C-reactive protein; hs-CRP, high-sensitivity CRP.
Study identification and selection
Two researchers (NB and MR) independently searched databases including the Cochrane Library, World Health Organization International Clinical Trial Registry Platform, PubMed, clinicaltrials.gov, Scopus, and ProQuest Digital Dissertations Database for randomized, placebo-controlled human trials that investigated the effect of flaxseed or its derivatives (in the form of whole or ground flaxseed, flaxseed oil, or lignan supplement) on inflammatory biomarkers. The search included all studies published as original full-text articles covering a period up to May 2018. The keywords flax* OR linseed* OR lignan* OR “Linum usitatissimum,” OR “flaxseed” OR “flaxseed oil” OR “secoisolariciresinol diglucoside” OR “SDG” in combination with “inflammation” OR “inflammatory” OR “C reactive protein” OR “C-reactive protein” OR “CRP” OR “high-sensitivity C-reactive protein” OR “hs-CRP” OR “interleukin-6” OR “interleukin 6” OR “IL-6” OR “tumor necrosis factor-” OR “tumor necrosis factor” OR “TNF-α” OR “TNF” were used in the literature search. The reference list of related articles was hand-searched for additional relevant studies. For studies to be included, they had to fulfill the following criteria: use of the randomized method [including intervention (flaxseed or its derivatives) and placebo group] and measurement of ≥1 of the primary outcomes. Trials with the following criteria were excluded: 1) observational studies (cohort studies, case-control studies, ecological studies, case reports, and case series), 2) nonclinical studies, uncontrolled trials, as well as those with insufficient data, and 3) flaxseed combined with other supplements or drugs.
Data extraction and quality assessment
An electronic database was created to collect all relevant data from the trials. The data were extracted independently by the 2 investigators (MR and NB), and in case of disagreement, ARA cross-examined doubtful data, with a decision being made after a consensus meeting. In the first screening, we evaluated the title and abstract of all the studies in endnote software (EndNote X6, Thomson Corporation) and duplicate studies were eliminated. The following characteristics were extracted: surname of the first author, study design, year of publication, sample size, gender and age mean, intervention dose, study duration, and inclusion and exclusion criteria. Data related to serum concentrations of CRP, hs-CRP, and TNFα as well as IL6 concentration before and after supplementation, were extracted for evaluating effects of the flaxseed intervention. The quality of the studies was assessed by both the researchers (MR and NB) according to the Jadad score (14) and Cochrane risk of bias tool (15). The Jadad score included randomization, blinding, description of withdrawals and dropouts, methods of randomization, and double-blinding status. The total score was the sum of the 5 points, which generated a scale from 0 to 5, with higher numbers representing better quality. The Cochrane risk of bias tool was used for quality assessment as follows: sequence generation, allocation and concealment, blinding, incomplete outcome data, selective outcome reporting, and other sources of bias. According to the Cochrane guideline handbook, the words “yes,” “no,” and “unclear” demonstrated the low, high, and unknown risk of bias, respectively.
Statistical analysis
The effect size, as estimated by the mean difference, was used to perform the fixed method meta-analysis. A random-effects meta-analysis was performed for each measurement, demonstrating a significant heterogeneity between the studies (16). Heterogeneity was assessed with the I2 index and by testing the null hypothesis that all studies share a common effect size. Heterogeneity was considered low if I2 < 30%, moderate if I2 = 30–75%, and high if I2 > 75% (17). For identifying the potential source of heterogeneity, stratified analyses were performed according to the following indicators: study quality according to the Jadad score (high or low), study design (parallel or crossover), age group (<30, 30–60, or >60 y), BMI categories (<25, 25–30, or >30 kg/m2) and supplement type (flaxseed, flaxseed oil, or lignan). Moreover, the meta-regression was performed based on study quality, study design, supplement type, age group, BMI, study duration (wk), and participants’ gender (percentage of male subjects recruited in the study) to identify possible sources of heterogeneity. Funnel plots were used to visually inspect for the presence of publication bias. In addition, for further investigation of publication bias, Begg's rank correlation and Egger's linear regression tests were used. All the analyses were carried out using Stata, version 12 SE (Stata Corp). A P value < 0.05 was considered to be statistically significant.
Results
Characteristics of the studies
From a total of 1004 records obtained through the systematic search, 32 articles were included in the final analysis. In these trials, the total number of participants was 1502, of whom 936 were included in the intervention groups and 566 in the control groups. The review flow diagram is shown in Figure 1, and the primary characteristics of all the 32 studies are outlined in Table 2. Flaxseed was tested in the form of whole flaxseed (18–23), golden flaxseed (12, 21, 24–28), flaxseed oil (29–45), and lignan (46–48) in the intervention groups with a dose of 360 mg (48) to 60 g (19). The trials varied in length from 2 (20) to 12 (30) wk with a median duration of 9.91 wk. Most of the trials (25 trials) had parallel study designs, but 7 studies had a crossover design. The quality of the included studies was diverse; 17 studies were high quality (Jadad score 3–5) (12, 19, 20, 25, 28, 29, 31, 32, 35, 36, 38, 39, 42, 43, 46–48) and 15 studies were low quality (18, 21–24, 26, 27, 30, 33, 34, 37, 40, 44, 45). Moreover, according to the Cochrane risk of bias tool, 13 articles were good quality, 13 articles were poor quality, and 6 articles were fair quality (Table 3). The eligible studies were conducted in the United States (12, 24, 25, 27, 28, 32, 44), Canada (18, 33, 46), Iran (22, 26, 29, 36–38, 42, 43), Brazil (19–21, 30, 35), Australia (31), Denmark (47), Greece (34, 40, 41), Finland (39), China (23, 48), and the United Kingdom (45).
FIGURE 1.

Search strategy for research evaluating the relations between intakes of flaxseed-derived products and circulating inflammatory markers. RCT, randomized clinical trial.
TABLE 2.
Characteristics of studies investigating the associations between flaxseed-derived product intakes and circulating inflammatory biomarkers
| First author, year (reference) | Country | Design | Participants (intervention/control) | Treatment duration/wk | Intervention | Disease name | Parameters | Quality score |
|---|---|---|---|---|---|---|---|---|
| Babajafari et al., 2018 (29) | Iran | Parallel | 49(25/24) Comp: 42 | 3 | 30 g FXO + ISP/30 g CO + ISP | Burn patients | hs-CRP | 3 |
| Barre et al., 2012 (46) | Canada | Crossover | 24 (24/24) | 6 | 600 mg LIG | T2DM | CRP, IL6, TNFα | 3 |
| Bloedon et al., 2008 (12) | United States | Parallel | 62(30/32) Comp: 58 | 10 | 40 g GF + LF & LC diet/WB + LF & LC diet | Dyslipidemia | hs-CRP, IL6 | 3 |
| de Oliveira et al., 2017 (30) | Brazil | Parallel | 52(27/25) Comp: 50 | 12 | 30 mL FXO/OO | OverWt or Obes | CRP | 1 |
| de Oliveira et al., 2017 (30) | Brazil | Parallel | 54(27/27) Comp: 52 | 12 | 30 mL FXO/SAO | OverWt or Obes | CRP | 1 |
| Demark et al., 2008 (28) | USA | Parallel | 81(40/41) Comp:78 | 3 | 30 g GF/Control (UD) | Prostate cancer patients | CRP | 3 |
| Demark et al., 2008 (28) | USA | Parallel | 81(40/41) Comp:78 | 3 | 30 g GF/LF | Prostate cancer patients | CRP | 3 |
| Dodin et al., 2008 (18) | Canada | Parallel | 199(101/98) Comp: 179 | 12 | 40 g FLX/WG | Menopausal women | CRP | 2 |
| Faintuch et al., 2011 (19) | Brazil | Crossover | 24(24/24) Comp: 24 | 2 | 30 g FF/MF | Obes | CRP | 3 |
| Faintuch et al., 2011 (19) | Brazil | Parallel | 20(11/9) Comp: 18 | 12 | 60 g FP/CF | Morbid obesity | CRP | 3 |
| Foster et al., 2013 (31) | Australia | Parallel | 24(12/12) Comp: 20 | 12 | 2 g FXO/OO | T2DM | CRP, IL6, TNFα | 4 |
| Hallund et al., 2008 (47) | Denmark | Crossover | 23(23/23) Comp: 22 | 6 | LF muffin with 500 mg LIG/without LIG | Postmenopausal women | IL6, CRP, TNFα | 3 |
| Hutchins et al., 2013 (27) | United States | Crossover | 41(41/41) Comp: 25 | 12 | 13 g GF/Control | OverWt or Obes | hs-CRP, IL6 | 1 |
| Hutchins et al., 2013 (27) | United States | Crossover | 41(41/41) Comp: 25 | 12 | 26 g GF/Control | OverWt or Obes | hs-CRP, IL6 | 1 |
| Karakas et al., 2016 (32) | United States | Parallel | 36(18/18) Comp: 34 | 6 | 3.5 g FXO/FO | PCOS | hs-CRP | 3 |
| Karakas et al., 2016 (32) | United States | Parallel | 36(18/18) Comp: 34 | 6 | 3.5 g FXO/SBO | PCOS | hs-CRP | 3 |
| Kaul et al., 2008 (33) | Canada | Parallel | 44(22/22) Comp: 44 | 12 | 2 g FXO/SFO | Healthy | CRP | 2 |
| Khalatbari et al., 2013 (26) | Iran | Parallel | 38(19/19) Comp:30 | 8 | 40 g GF/Control | HD | CRP | 1 |
| Kontogianni et al., 2013 (34) | Greece | Crossover | 53(53/53) Comp: 37 | 6 Washout: 6 | 15 mL FXO/OO | Healthy adults | hs-CRP, TNFα | 1 |
| Lemos et al., 2012 (35) | Brazil | Parallel | 20(11/9) Comp: 18 | 12 | 2 g FXO/MO | HD | CRP | 5 |
| Machado et al., 2015 (21) | Brazil | Parallel | 50(25/25) Comp: 41 | 11 | 28 g GF/WB | OW | CRP, IL6, TNFα | 1 |
| Machado et al., 2015 (21) | Brazil | Parallel | 50(25/25) Comp: 41 | 11 | 28 g BF/WB | OW | CRP, IL6, TNFα | 1 |
| Mirfatahi et al., 2016 (36) | Iran | Parallel | 38(19/19) Comp: 34 | 8 | 6 g FXO/MCT | HD | hs-CRP | 5 |
| Mirhashemi et al., 2016 (37) | Iran | Parallel | 60(30/30) Comp: 56 | 12 | 1 g ω3 FXO/PLA | DN | TNFα | 2 |
| Mirmasoumi et al., 2018 (38) | Iran | Parallel | 60(30/30) Comp:60 | 12 | 2 g FXO/PLA | PCOS | hs-CRP | 5 |
| Nordstrom et al., 1995 (39) | Finland | Parallel | 22(11/11) Comp: 22 | 12 | 30 g FXO/SAO | RA | CRP | 3 |
| Pan et al., 2009 (48) | China | Crossover | 73(73/73) Comp: 70 | 12 Washout: 8 | 360 mg LIG/RF | T2DM | CRP, IL6, | 5 |
| Paschos et al., 2007 (40) | Greece | Parallel | 40(20/20) Comp: 35 | 12 | 15 mL FXO/SAO | Dyslipidemia | TNFα | 1 |
| Rallidis et al., 2003 (41) | Greece | Parallel | 76(50/26) Comp: 76 | 12 | 15 mL FXO/SAO | Dyslipidemic | CRP, CRP | 1 |
| Rhee et al., 2011 (25) | United States | Crossover | 11(11/11) Comp: 9 | 12 Washout: 4 | 40 g GF/WB | Obes glucose intolerant | hs-CRP, IL6, TNFα | 3 |
| Ricklefs et al., 2017 (24) | United States | Parallel | 19(10/9) Comp: 17 | 8 | 28 g GF/9 g GP | T2DM | TNFα, CRP | 1 |
| Soleimani et al., 2017 (43) | Iran | Parallel | 60(30/30) Comp: 54 | 12 | 2 g ω3 FXO/PLA | DN | hs-CRP | 3 |
| Soleimani et al., 2017 (42) | Iran | Parallel | 60(30/30) Comp: 55 | 12 | 2 g ω3 FXO/PLA | DFU | hs-CRP | 3 |
| Vargas et al., 2011 (44) | United States | Parallel | 44(23/21) Comp: 34 | 6 | 3.5 g ω3 FXO/FO | PCOS | hs-CRP | 2 |
| Wallace et al., 2003 (45) | UK | Parallel | 16(8/8) Comp:16 | 12 | 9 g FXO/PLA | Healthy Adults | IL6, TNFα | 1 |
| Yari et al., 2016 (22) | Iran | Parallel | 50(25/25) Comp: 46 | 12 | 30 g BF + LM/LM | NAFLD | hs-CRP, TNFα | 1 |
| Zong et al., 2013 (23) | China | Parallel | 173(90/83) Comp: 173 | 12 | 30 g WF + LC/LC | MetS | hs-CRP, IL6, TNFα | 1 |
TABLE 3.
Quality assessment of clinical trials (according to the Cochrane guideline) investigating the associations between flaxseed-derived product intakes and circulating inflammatory biomarkers1
| First author, year (reference) | Random sequence generation | Allocation concealment | Blinding | Incomplete outcome data | Selective reporting | Other bias | Total quality |
|---|---|---|---|---|---|---|---|
| Barre et al., 2012 (46) | L | U | L | U | L | L | F |
| Babajafari et al., 2018 (29) | L | U | L | L | L | L | G |
| Bloedon et al., 2008 (12) | L | U | L | L | L | L | G |
| Oliveria et al., 2017 (30) | H | U | L | U | L | L | P |
| Demark et al., 2008 (28) | L | U | H | L | L | L | P |
| Dodin et al., 2008 (18) | L | L | L | U | L | L | F |
| Faintuch et al., 2011 (19) | L | L | L | L | L | L | G |
| Faintuch et al., 2011 (19) | L | U | L | L | L | L | G |
| Foster et.al., 2013 (31) | L | U | L | L | L | L | G |
| Hallund et al., 2008 (47) | U | U | L | L | L | L | F |
| Hutchins et al., 2013 (27) | L | U | H | U | L | U | P |
| Karakas et al., 2016 (32) | L | U | L | L | L | L | G |
| Kaul et al., 2008 (33) | L | U | L | L | L | L | G |
| Khalatbari et al., 2013 (26) | L | H | H | L | L | L | P |
| Kontogianni et al., 2013 (34) | L | U | L | U | L | L | F |
| Lemos et al., 2012 (35) | L | U | L | L | L | L | G |
| Machado et al., 2015 (21) | L | H | H | L | L | U | P |
| Mirfatahi et al., 2016 (36) | L | U | L | L | L | L | G |
| Mirhashemi et al., 2016 (37) | L | L | L | L | L | L | G |
| Mirmasoumi et al., 2018 (38) | L | L | L | L | L | L | G |
| Nordstrom et al., 1995 (39) | L | U | L | U | L | L | F |
| Pan et al., 2008 (48) | L | U | U | U | L | U | P |
| Paschos et al., 2007 (40) | L | H | H | L | L | L | P |
| Rallidis et al., 2003 (41) | L | U | U | U | L | U | P |
| Rhee et al., 2011 (25) | L | U | H | U | L | L | P |
| Ricklefs et al., 2017 (24) | L | H | H | U | L | U | P |
| Soleimani et al., 2017 (43) | L | L | L | L | L | L | G |
| Soleimani et al., 2017 (42) | L | U | L | L | L | L | G |
| Vargas et al., 2011 (44) | L | U | U | U | L | U | P |
| Wallace et al., 2003 (45) | L | U | L | L | L | U | F |
| Yari et al., 2016 (22) | L | U | H | L | L | L | P |
| Zong et al., 2013 (23) | L | U | H | L | L | L | P |
F, fair quality; G, good quality; H, high risk of bias; L, low risk of bias; P, poor quality; U, unclear risk of bias.
Meta-analysis of the effect of flaxseed or its derivatives on serum concentrations of TNFα
Overall, 11 studies, including 310 intervention and 317 control subjects, provided 12 effect sizes regarding the effect of flaxseed supplementation on serum concentration of TNFα (21–25, 31, 34, 37, 40, 46, 47). According to the meta-analysis, flaxseed had a significant effect on reducing serum concentration of TNFα, compared to the placebo groups (WMD = −0.38; 95% CI: −0.75, −0.01; P = 0.04; Figure 2). There was high level of heterogeneity among the studies (I2 = 80.0, P < 0.001). The subgroup analysis of study quality according to the Jadad score (high or low), study design (parallel or crossover), supplement type (flaxseed, flaxseed oil, or lignan), age group (<30, between 30 and 60, or >60 y), and BMI categories (<25, 25–30, or >30) showed that heterogeneity was significant within the low-quality studies (n = 9, I2 = 86.1, P < 0.001) with parallel design (n = 9, I2 = 86.8, P < 0.001), age 30–60 y (n = 5, I2 = 90.6, P < 0.001), and BMI < 25 (n = 4, I2 = 67.8, P = 0.02) and >30 (n = 4, I2 = 89.2, P < 0.001), as well as in trials supplemented by flaxseed (n = 3, I2 = 84.2, P = 0.004) (Table 4). The heterogeneity among the studies was not explained by study quality, study design, supplement type, age group, BMI, study duration, and participants’ gender in the meta-regression (Table 5). The sensitivity analysis suggested that this association disappeared following the exclusion of each of the trials by Rhee et al. (WMD = −0.42; 95% CI:–0.88, 0.03) (25), Machado et al. (WMD = −0.33; 95% CI:–0.72, 0.05, and = −0.32; 95% CI:–0.70, 0.06) (21), Yari et al. (22) (WMD = −0.27; 95% CI:–0.63, 0.08) (22), and Ricklefs et al. (WMD = −0.24; 95% CI: −0.56, 0.07) (24).
FIGURE 2.
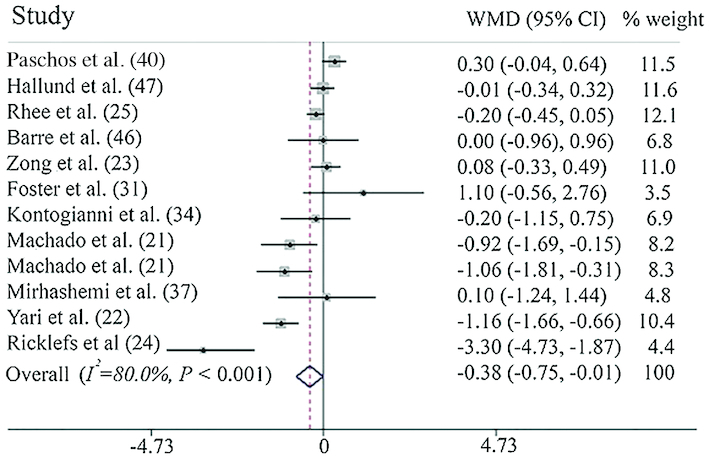
Forest plot summarizing the association between flaxseed or its derivatives vs. control on TNF-α concentration. TNF-α, Tumor necrosis factor alpha
TABLE 4.
Overall estimates of meta-analysis investigating the associations between flaxseed-derived product intakes and circulating inflammatory biomarkers1
| Outcomes | Subgroups | No. of effect size | References | WMD (95% CI) | P value | I2 (%) | P value for heterogeneity |
|---|---|---|---|---|---|---|---|
| TNFα, pg/mL | 12 | (18–22, 28, 31, 34, 37, 43, 44) | −0.38 (−0.75, 0.01) | 0.07 | 80.0 | <0.001 | |
| Study quality | High | 4 | (22, 28, 43, 44) | −0.10 (−0.30, 0.08) | 0.28 | 0.0 | 0.40 |
| Low | 7 | (18–21, 31, 34, 37) | −0.66 (−1.27, −0.05) | 0.03 | 86.1 | <0.001 | |
| Study design | Parallel | 7 | (18–21, 28, 34, 37) | −0.587 (−1.24, 0.06) | 0.07 | 86.8 | <0.001 |
| Crossover | 4 | (22, 31, 43, 44) | −0.128 (−0.32, 0.06) | 0.19 | 0.0 | 0.83 | |
| Supplement type | Flaxseed | 5 | (18–22) | −0.76 (−1.30, −0.22) | 0.006 | 84.2 | <0.001 |
| Flaxseed oil | 4 | (28, 31, 34, 37) | 0.26 (−0.04, 0.57) | 0.08 | 0.0 | 0.57 | |
| Lignan | 2 | (43, 44) | −0.01 (−0.34, 0.32) | 0.95 | – | – | |
| IL6, pg/mL | 11 | (10, 18, 20, 22, 28, 38, 42–45) | −0.24 (−0.70, 0.20) | 0.28 | 78.0 | <0.001 | |
| Study quality | High | 6 | (10, 22, 28, 43–45) | −0.40( −0.95, 0.14) | 0.14 | 74.0 | 0.002 |
| Low | 5 | (18, 20, 34, 42) | 0.006 (−0.92, 0.93) | 0.99 | 82.6 | <0.001 | |
| Study design | Parallel | 7 | (10, 18, 20, 28, 38, 42) | −0.11 (−0.64, 0.42) | 0.69 | 72.5 | 0.001 |
| Crossover | 4 | (22, 43–45) | −0.54 (−1.56, 0.47) | 0.29 | 88.7 | <0.001 | |
| Supplement type | Flaxseed | 5 | (10, 18, 20, 22) | −0.27 (−0.99, 0.45) | 0.46 | 87.9 | <0.001 |
| Flaxseed oil | 3 | (28, 38, 42) | −0.43 (−1.17, 0.31) | 0.25 | 9.0 | 0.33 | |
| Lignan | 3 | (43–45) | −0.02 (−0.42, 0.37) | 0.89 | 0.0 | 0.92 | |
| CRP, mg/L | 19 | (15–18, 21, 23, 25, 27, 28, 30, 32, 36, 38, 43–45) | −0.56 (−1.02, −0.10) | 0.01 | 75.6 | <0.001 | |
| Study quality | High | 10 | (16, 17, 25, 28, 32, 36, 43–45) | −0.57 (−1.31, 0.16) | 0.12 | 81.2 | <0.001 |
| Low | 9 | (15, 18, 21, 23, 27, 30, 38) | −0.52 (−1.11, 0.05) | 0.07 | 66.2 | 0.004 | |
| Study design | Parallel | 15 | (15, 16, 18, 21, 23, 25, 27, 28, 30, 32, 36, 38) | −0.51 (−1.05, 0.03) | 0.06 | 79.1 | <0.001 |
| Crossover | 4 | (17, 43–45) | −0.51 (−1.01, −0.01) | 0.04 | 54.7 | 0.08 | |
| Supplement type | Flaxseed | 9 | (15–18, 21, 23, 25) | −0.64 (−1.34, 0.06) | 0.07 | 71.2 | <0.001 |
| Flaxseed oil | 7 | (27, 28, 30, 32, 36, 38) | −0.56 (−1.44, 0.30) | 0.20 | 85.7 | <0.001 | |
| Lignan | 3 | (43–45) | −0.30 (−0.84, 0.23) | 0.27 | 0.0 | 0.95 | |
| hs-CRP, mg/L | 15 | (10, 19, 20, 22–24, 26, 31, 33, 35, 39, 41) | −0.68 (−1.21, −0.15) | 0.01 | 89.8 | <0.001 | |
| Study quality | High | 8 | (10, 23, 26, 33, 35, 39, 40) | −1.12 (−2.03, −0.22) | 0.01 | 87.4 | <0.001 |
| Low | 7 | (19, 20, 22, 24, 31, 41) | −0.06 (−0.60, 0.47) | 0.82 | 82.8 | <0.001 | |
| Study design | Parallel | 11 | (10, 19, 20, 23, 26, 33, 35, 39, 41) | −0.74 (−1.48, −0.01) | 0.04 | 91.5 | <0.001 |
| Crossover | 4 | (22, 24, 31) | −0.58 (−1.68, 0.50) | 0.29 | 84.3 | <0.001 | |
| Supplement type | Flaxseed | 5 | (10, 19, 20, 24) | −0.51 (−1.21, 0.18) | 0.15 | 88.5 | <0.001 |
| Flaxseed Oil | 10 | (22, 23, 26, 31, 33, 35, 39–41) | −0.81 (−1.85, 0.22) | 0.12 | 91.1 | <0.001 | |
CRP, C-reactive protein; hs-CRP, high-sensitivity CRP; WMD, weighted mean difference.
TABLE 5.
Meta-regression investigating the associations between flaxseed-derived product intakes and circulating inflammatory biomarkers1
| Variable | Coefficient | 95% CI | P value |
|---|---|---|---|
| TNFα, pg/mL | |||
| Study quality | 0.29 | −6.43, 7.01 | 0.89 |
| Study design | 0.20 | −5.73, 6.13 | 0.92 |
| Supplement type | 0.64 | −6.26, 7.56 | 0.78 |
| Age group | −0.16 | −7.47. 7.14 | 0.94 |
| BMI | −0.23 | −5.23, 4.76 | 0.89 |
| Time to follow, wk | 0.26 | −1.18, 1.71 | 0.60 |
| Gender, % of males | 0.002 | −0.10, 0.11 | 0.94 |
| IL6, pg/mL | |||
| Study quality | −0.69 | −17.14, 15.75 | 0.87 |
| Study design | −0.23 | −13.06, 12.60 | 0.94 |
| Supplement type | 0.57 | −15.27, 16.43 | 0.89 |
| Age group | −0.67 | −12.39, 11.04 | 0.82 |
| BMI | 0.31 | −14.42, 15.04 | 0.93 |
| Time to follow, wk | −0.27 | −8.43, 7.89 | 0.89 |
| Gender, % of males | −0.02 | −0.27, 0.22 | 0.74 |
| CRP, mg/L | |||
| Study quality | −1.63 | −11.37, 8.11 | 0.54 |
| Study design | 6.93 | −21.92, 35.79 | 0.41 |
| Supplement type | −1.60 | −5.62, 2.42 | 0.22 |
| Age group | 7.55 | −11.75, 26.86 | 0.23 |
| BMI | −4.91 | −14.65, 4.82 | 0.16 |
| Time to follow, wk | −0.07 | −0.25, 0.10 | 0.21 |
| Gender, % of males | −0.03 | −0.11, 0.04 | 0.23 |
| hs-CRP, mg/L | |||
| Study quality | −1.03 | −2.46, 0.39 | 0.14 |
| Study design | 0.39 | −1.12, 1.90 | 0.59 |
| Supplement type | 0.76 | −0.81, 2.33 | 0.31 |
| Age group | −0.46 | −1.80, 0.86 | 0.46 |
| BMI | 0.21 | −0.95, 1.39 | 0.69 |
| Time to follow, wk | −0.12 | −0.35, 0.10 | 0.27 |
| Gender, % of males | 0.005 | −0.02, 0.03 | 0.73 |
CRP, C-reactive protein; hs-CRP, high-sensitivity CRP.
Meta-analysis of the effect of flaxseed or its derivatives on serum concentration of IL6
A total of 11 effect sizes (n = 316 intervention and 301 control) were obtained from the trials that considered the effect of flaxseed supplementation on serum concentrations of IL6 (12, 21, 23, 25, 31, 41, 45–48). As shown in Figure 3, there was no association between flaxseed supplementation and IL6 concentration, compared to the placebo (WMD = −0.25; 95% CI:–0.70, 0.21; P = 0.28). High levels of heterogeneity were observed among the studies (I2 = 78.0, P < 0.001). The subgroup analysis of supplement type (flaxseed, flaxseed oil, or lignan), age group (<30, 30–60, or >60 y), and BMI categories (<25, 25−30, or >30) suggested that heterogeneity was significant in trials using flaxseed as a supplement (n = 6, I2 = 87.9, P < 0.001), with age < 30 y (n = 3, I2 = 90.1, P < 0.001) or > 60 y (n = 4, I2 = 84.2, P < 0.001) and BMI < 25 (n = 4, I2 = 85.3, P < 0.001) or > 30 (n = 2, I2 = 85.9, P < 0.001). In addition, according to the subgroup analysis, study quality and study design were not the source of heterogeneity and there was significant heterogeneity in all the subgroups of these variables. Moreover, meta-regression did not report study quality, study design, supplement type, age group, BMI, study duration (wk), and participants’ gender (percentage of male subjects) as sources of heterogeneity. The sensitivity analysis suggested a significant change in the results following the exclusion of the study by Machado et al. (21) (WMD = −0.44; 95% CI:–0.81, –0.08).
FIGURE 3.
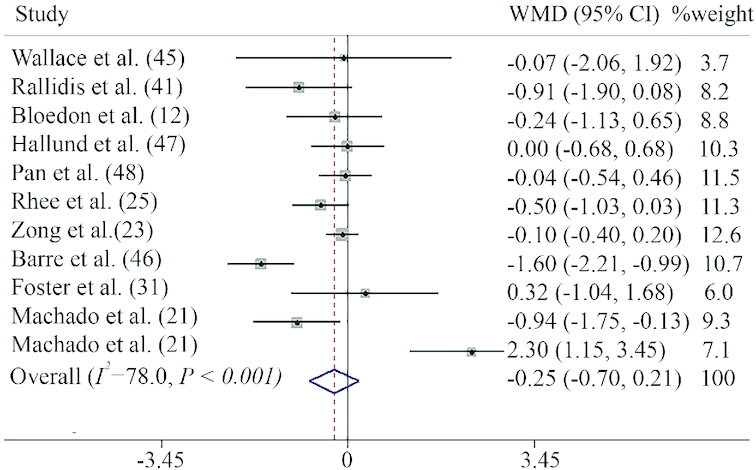
Forest plot summarizing the association between intake flaxseed or its derivatives on circulating IL-6 concentrations. WMD, weighted mean difference.
Meta-analysis of the effect of flaxseed or its derivatives on serum concentration of CRP
Ten trials, including 318 treatment and 327 controls, provided 12 effect sizes on serum concentration of CRP for the meta-analysis (18–21, 24, 28, 31, 33, 39, 46). These studies suggested no association between flaxseed consumption and CRP concentration (WMD = −0.34; 95% CI: −0.89, 0.20, P = 0.22, Figure 4). There was a moderate heterogeneity among the studies (I2 = 60.7%, P = 0.003). According to the subgroup analysis, there was a significant heterogeneity in the low-quality studies (n = 4, I2 = 72.9, P = 0.01) with parallel design (n = 10, I2 = 54.3, P = 0.02) and trials supplemented by flaxseed (n = 9, I2 = 67.0, P = 0.002). Further, stratifying the studies according to BMI resulted in a nonsignificant heterogeneity among studies in all the subgroups. However, the meta-regression did not report study quality, study design, supplement type, age group, BMI, study duration (wk), and participants’ gender (percentage of male subjects) as sources of heterogeneity. The sensitivity analysis did not provide any further information.
FIGURE 4.
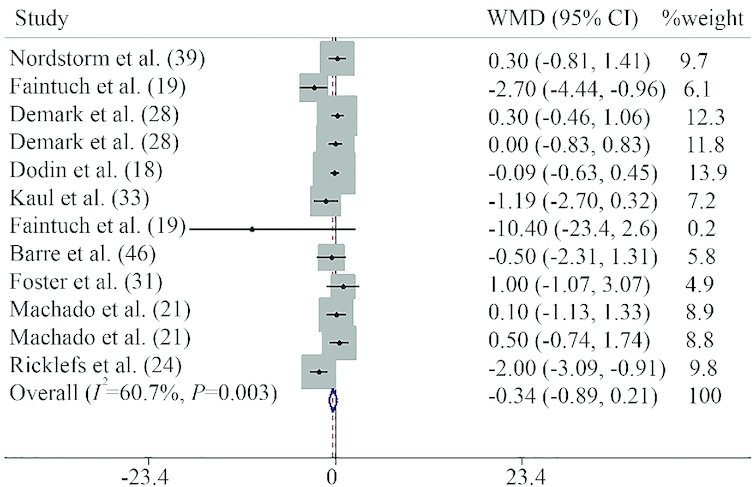
Forest plot summarizing the association between intake flaxseed or its derivatives on circulating CRP concentrations. CRP, C-reactive protein, WMD, weighted mean difference.
Meta-analysis of the effect of flaxseed or its derivatives on serum concentration of hs-CRP
In total, 19 studies (22 effect sizes; n = 699 intervention and 986 control) investigated the effect of flaxseed supplementation on serum concentration of hs-CRP (12, 22, 23, 25–27, 29, 30, 32, 34–36, 38, 41–44, 47, 48).
These studies suggested an inverse association between flaxseed consumption and hs-CRP concentration (mean difference = −0.75; 95% CI:–1.19, –0.30, P = 0.001, Figure 5). There was a high heterogeneity among the studies (I2 = 89.5%, P < 0.001). The subgroup analysis did not identify study quality (high or low), study design (parallel or crossover), age (<30, 30–60, or >60 y), and BMI (<25, 25–30, or >30) as sources of heterogeneity. According to the subgroup analysis, studies that used flaxseed and flaxseed oil as supplements had a high heterogeneity level (I2 = 88.7%, P < 0.001, and I2 = 91.0%, P < 0.001, respectively). However, heterogeneity was not evident among studies supplemented by flaxseed lignan (I2 = 0.0%, P = 0.95). The significant relation between flaxseed supplementation and hs-CRP concentration did not change in the sensitivity analysis.
FIGURE 5.
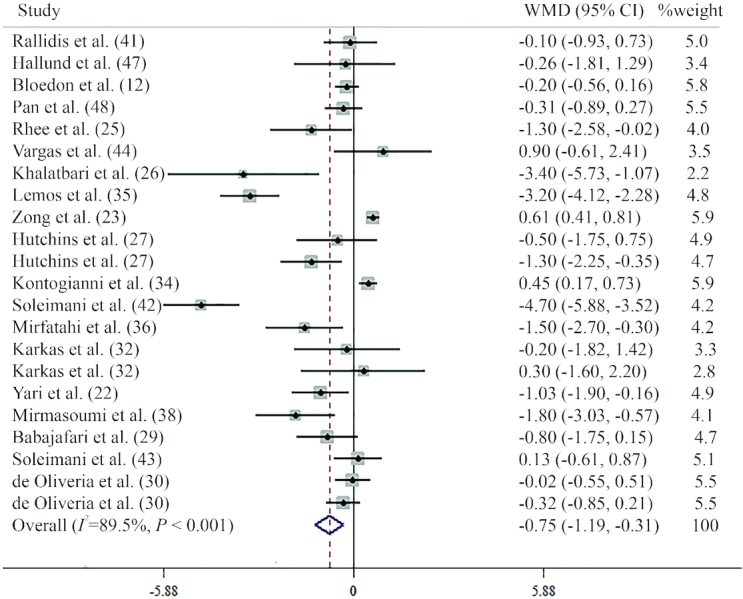
Forest plot summarizing the association between intake flaxseed or its derivatives on circulating hs-CRP concentration. hs-CRP, high-sensitivity CRP; WMD, weighted mean difference.
Publication bias
Visual inspection of the funnel plots demonstrated no publication bias of the trials in investigating the effect of flaxseed supplementation on TNFα (Egger's test P = 0.25; Begg's test P = 0.99) (Figure 6A), IL6 (Egger's test P = 0.87; Begg's test P = 0.99) (Figure 6B), and CRP (Egger's test P = 0.20; Begg's test P = 0.45) (Figure 6C) concentrations. Although the funnel plot (Figure 6D) and Begg's test (P = 0.31) did not show any publication bias of the trials in investigating the effect of flaxseed supplementation on hs-CRP concentration, the Egger's test was significant (P < 0.001).
FIGURE 6.
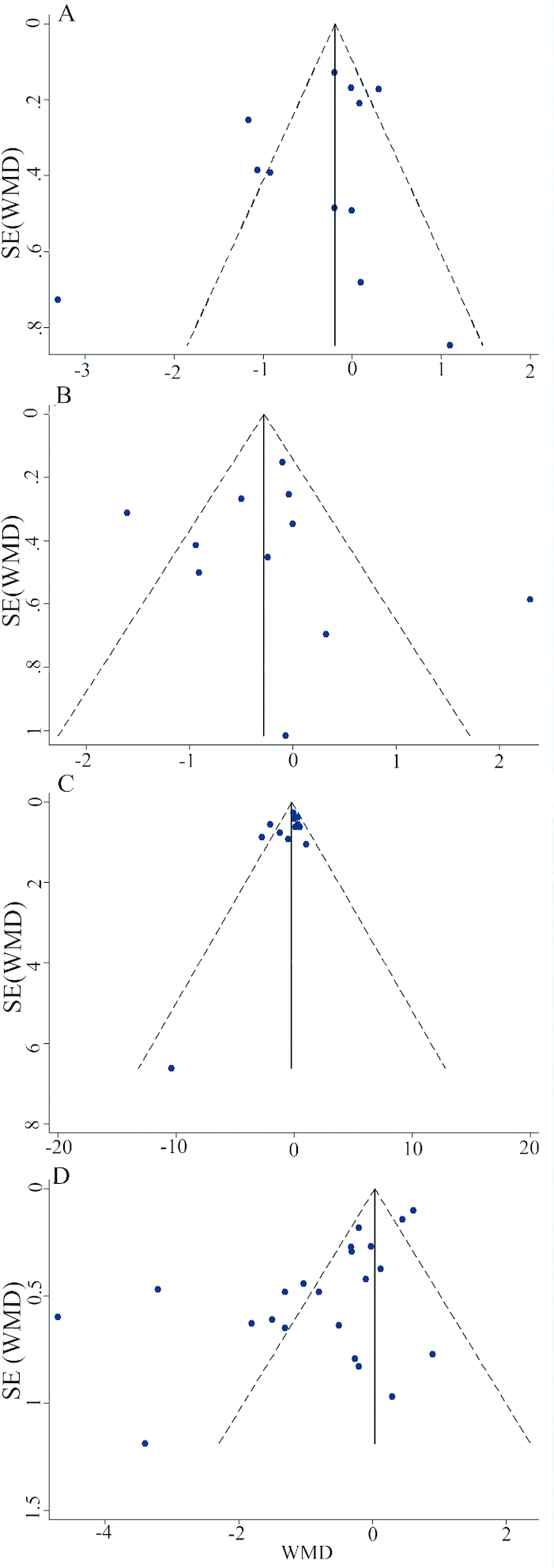
Funnel plots detailing publication bias in the selected studies of the relation between intakes of flaxseed-derived products and circulating TNFα (A), IL6 (B), CRP (C), and hs-CRP (D). Visual inspection of funnel plots indicates that there is no publication bias among studies. CRP, C-reactive protein; hs-CRP, high-sensitivity CRP; WMD, weighted mean difference.
Discussion
The present systematic review and meta-analysis revealed that flaxseed consumption had a beneficial effect on hs-CRP and TNFα, but not on IL6 and CRP. However, after excluding the study of Machado et al. (21), we found a significant inverse association between flaxseed and IL6 concentration. Flaxseed as 1 of the best sources of PUFA, especially ω-3, is widely established to have several beneficial effects on human health (49). There are 2 types of essential fatty acid for humans, including linoleic acid [18:2 (n–6)] from the n–6 family and ALA [18:3 (n–3)] from n–3 fatty acid family (50). Higher consumption of n–6 fatty acids compared to n–3 causes overproduction of proinflammatory agents such as series 2 eicosanoid-like prostaglandins and series 4 leukotrienes and low concentrations of anti-inflammatory agents, especially series 5 leukotrienes and series 3 prostaglandins (51). Because in many traditional and Western diets, less substrate is available for synthesis of the anti-inflammatory n–3 fatty acid family, supplementation of flaxseed or its derivatives has been shown to result in decreased production of PGE2, thromboxane B2, 5-hydroxyeicosatetraenoic acid, and leukotriene E4 by inflammatory cells (51). The amount of ALA in flaxseed is about 57%. Ground flaxseed has ALA, but flaxseed oil contains the highest amount (52). CRP is an indicator of general low-grade inflammation, and a higher concentration of CRP is associated with the increased risk of CVD (53), insulin resistance (54), and metabolic syndrome (55). In the current study, flaxseed or its derivatives reduced the hs-CRP concentration significantly. However, a pooled analysis did not reveal any significant change in the serum concentration of CRP after flaxseed supplementation. Macrophage infiltration into adipose tissue, which occurs as a result of obesity and chronic diseases, can increase the production of proinflammatory agents such as IL6, CRP, hs-CRP, and TNFα (56, 57). SDG is an active compound with antioxidant properties present in flax and is a precursor for other active metabolites such as enterolactone and lignans enterodiol (58). Studies have revealed that diets including a high amount of flaxseed can increase plasma concentration of these active compounds at a time interval of 2–3 wk (59). Flaxseed-related active compounds, especially SDG and its metabolites (enterolactone and lignans enterodiol), have shown anti-inflammatory and antioxidant activity, mainly through inhibition of lipid peroxidation. Moreover, some studies have suggested that the flaxseed lignan component can activate the nuclear element (erythroid-derived 2)-like 2, a transcription factor of the antioxidant and detoxifying genes, especially NAD(P)H quinone dehydrogenase 1 and heme oxygenase-1 (60). Furthermore, Rom et al. demonstrated that SDG administration reduces leukocyte adhesion and migration across the blood-brain barrier by ∼50% (61). On the other hand, flaxseed is 1 of the richest sources of soluble fiber. Dietary fiber has been shown to be fermented to SCFA (acetate, propionate, and butyrate) by intestinal bacteria. Previous studies have revealed that SCFA, especially propionate, can act as anti-inflammatory factors through interference in various inflammatory pathways, especially reduced TNFα-related gene expression (62). Furthermore, results of animal and human studies have shown that in humans and high-fat diet-fed rodents, consumption of flaxseed can improve critical aspects of the obese phenotype, including reduced adipocyte hypertrophy, T-cell accumulation, and monocyte chemoattractant protein-1 production, and reduce serum concentration and mononuclear cell secretion of IL6, IL1β, and TNFα (41, 63, 64). In our study, the effect of supplementation of flaxseed or its derivatives on TNFα was found to be significant, and excluding studies with high sample size and high effect size caused meaningful disappearance. However, we identified study design, study quality, age group, BMI, and intervention type (flaxseed, flaxseed oil, or lignan) as sources of the heterogeneity.
Our results also revealed that flaxseed or its derivatives had no effects on IL6 plasma concentration. However, supplement type, BMI, and age group were identified as sources of heterogeneity by the subgroup analysis. Interestingly, after removing Machado et al.’s study (21), we found a significant inverse association. It appears that the main causes of such contradictory findings in Machado et al.’s study are the age of participants and baseline serum concentration of inflammatory markers. In adolescents, serum concentrations of inflammatory factors are low (65). Nevertheless, previous studies have shown that in adult subjects and patients with high serum concentration of inflammatory markers, the effect of flaxseed is more significant on the reduction of inflammation (35). However, the stratified analysis did not show any difference in the effect of flaxseed on IL6 among the various age groups. Another reason for the contradiction in the study results with regard to the effect of flaxseed or its derivatives on inflammatory markers is the weights of the participants; it is clear that obese subjects have a high concentration of inflammatory markers because of the higher amounts of adipose tissue (66). Furthermore, several trials have shown that flaxseed is more likely to reduce systemic inflammatory markers in subjects with higher concentrations of inflammatory factors (i.e., CRP >3 mg/L or microinflammation) (36). The present study found that in subjects with higher BMI (>30), flaxseed resulted in significantly lower TNFα, CRP, and hs-CRP compared to the placebo; however, the changes were not significant in the other subgroups. In addition, flaxseed resulted in a nonsignificant reduction in the IL6 concentration in subjects with higher BMI. Because most of the studies did not report the results separately according to gender, the exact sex-specificity effect of flaxseed remains unclear. However, meta-regression did not find gender to be a source of heterogeneity.
To the best of the researchers’ knowledge, this study was the first comprehensive meta-analysis designed to analyze the effect of flaxseed or its derivatives on inflammatory biomarkers. The strengths of this study included the identification of randomized trials with a detailed search strategy and subgroup analysis of intervention type, study design, study quality score, age group, and BMI categories. The present study might have some limitations that should be considered. Firstly, in the included studies, sample populations were from different diseases and sometimes healthy people, which could affect the accuracy of the results. Secondly, the eligible studies were heterogeneous and the source of heterogeneity for some elements could not be identified, indicating that the effects of flaxseed were not uniform on inflammatory factors.
In conclusion, the current meta-analysis pooled results from 32 RCTs regarding the effects of consumption of flaxseed or its derivatives on main inflammatory factors. The results of this study showed that flaxseed or its derivatives could have anti-inflammatory effects on the human body. However, additional trials must be conducted in the future that include adequate durations, well-designed protocols, and larger sample sizes to demonstrate the beneficial effects of flaxseed consumption on inflammation.
Acknowledgments
The authors’ responsibilities were as follows—NB and ARA: study design and data collection; MR and ARA: meta-analysis; MR and NB: manuscript production; ARA: editing of the manuscript; and all authors: read and approved the final paper.
Notes
The authors reported no funding received for this study.
Author disclosures: MR, NBJ, NH, and ARA, no conflicts of interest
Abbreviations used: ALA, α-linolenic acid; CRP, C-reactive protein; CVD, cardiovascular disease; hs-CRP, high-sensitivity CRP; SDG, secoisolariciresinol diglucoside; WMD, weighted mean difference
References
- 1. Ren GY, Chen CY, Chen GC, Chen WG, Pan A, Pan CW, Zhang YH, Qin LQ, Chen LH. Effect of flaxseed intervention on inflammatory marker C-reactive protein: a systematic review and meta-analysis of randomized controlled trials. Nutrients. 2016;8(3):136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Fan L, Feng Y, Chen G-C, Qin L-Q, Fu C-l, Chen L-H. Effects of coenzyme Q10 supplementation on inflammatory markers: a systematic review and meta-analysis of randomized controlled trials. Pharmacol Res. 2017;119:128–36. [DOI] [PubMed] [Google Scholar]
- 3. Tracy R. Emerging relationships of inflammation, cardiovascular disease and chronic diseases of aging. Int J Obes. 2003;27(S3):S29. [DOI] [PubMed] [Google Scholar]
- 4. Micallef MA, Garg ML.. Anti-inflammatory and cardioprotective effects of n-3 polyunsaturated fatty acids and plant sterols in hyperlipidemic individuals. Atherosclerosis. 2009;204(2):476–82. [DOI] [PubMed] [Google Scholar]
- 5. Tardivo AP, Nahas-Neto J, Orsatti CL, Dias F, Poloni P, Schmitt E, Nahas EA. Effects of omega-3 on metabolic markers in postmenopausal women with metabolic syndrome. Climacteric. 2015;18(2):290–8. [DOI] [PubMed] [Google Scholar]
- 6. Zhao Y, Wang C.. Effect of ω-3 polyunsaturated fatty acid-supplemented parenteral nutrition on inflammatory and immune function in postoperative patients with gastrointestinal malignancy: A meta-analysis of randomized control trials in China. Medicine (Baltimore). 2018;97(16):e0472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Lanzmann-Petithory D. Alpha-linolenic acid and cardiovascular diseases. J Nutr Health Aging. 2001;5(3):179–83. [PubMed] [Google Scholar]
- 8. Pan A, Yu D, Demark-Wahnefried W, Franco OH, Lin X. Meta-analysis of the effects of flaxseed interventions on blood lipids. Am J Clin Nutr. 2009;90(2):288–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Touré A, Xueming X. Flaxseed lignans: source, biosynthesis, metabolism, antioxidant activity, bio‐active components, and health benefits. Compr Rev Food Sci F. 2010;9(3):261–9. [DOI] [PubMed] [Google Scholar]
- 10. Hu C, Yuan YV, Kitts DD. Antioxidant activities of the flaxseed lignan secoisolariciresinol diglucoside, its aglycone secoisolariciresinol and the mammalian lignans enterodiol and enterolactone in vitro. Food Chem Toxicol. 2007;45(11):2219–27. [DOI] [PubMed] [Google Scholar]
- 11. Adolphe JL, Whiting SJ, Juurlink BH, Thorpe LU, Alcorn J. Health effects with consumption of the flax lignan secoisolariciresinol diglucoside. Br J Nutr. 2010;103(7):929–38. [DOI] [PubMed] [Google Scholar]
- 12. Bloedon LT, Balikai S, Chittams J, Cunnane SC, Berlin JA, Rader DJ, Szapary PO. Flaxseed and cardiovascular risk factors: results from a double blind, randomized, controlled clinical trial. J Am Coll Nutr. 2008;27(1):65–74. [DOI] [PubMed] [Google Scholar]
- 13. Basch E, Mphil SB, Collins J, Dacey C, Harrison M, Szapary P. Flax and Flaxseed Oil (Linum usitatissimum): A Review. J Soc Integr Oncol. 2007;5(3):92–105. [DOI] [PubMed] [Google Scholar]
- 14. Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJM, Gavaghan DJ, McQuay HJ. Assessing the quality of reports of randomized clinical trials: is blinding necessary?. Control Clin Trials. 1996;17(1):1–12. [DOI] [PubMed] [Google Scholar]
- 15. Higgins JP, Altman DG, Cotzsche PC, Juni P, Moher D, Savovic J, Schulz KF, Weeks L, Sterne JA. The Cochrane collaborations tool for assessingrisk of bias in randomised trials. BMJ. 2011;343:d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. DerSimonian R, Laird N.. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–88. [DOI] [PubMed] [Google Scholar]
- 17. Higgins JP, Green S.. Cochrane Handbook for Systematic Reviews of Interventions: John Wiley & Sons, 2011. [Google Scholar]
- 18. Dodin S, Cunnane SC, Masse B, Lemay A, Jacques H, Asselin G, Tremblay-Mercier J, Marc I, Lamarche B, Legare F et al.. Flaxseed on cardiovascular disease markers in healthy menopausal women: a randomized, double-blind, placebo-controlled trial. Nutrition. 2008;24(1):23–30. [DOI] [PubMed] [Google Scholar]
- 19. Faintuch J, Bortolotto LA, Marques PC, Faintuch JJ, Franca JI, Cecconello I. Systemic inflammation and carotid diameter in obese patients: pilot comparative study with flaxseed powder and cassava powder. Nutr Hosp. 2011;26(1):208–13. [PubMed] [Google Scholar]
- 20. Faintuch J, Horie LM, Barbeiro HV, Barbeiro DF, Soriano FG, Ishida RK, Cecconello I. Systemic inflammation in morbidly obese subjects: response to oral supplementation with alpha-linolenic acid. Obes Surg. 2007;17(3):341–7. [DOI] [PubMed] [Google Scholar]
- 21. Machado AM, de Paula H, Cardoso LD, Costa NM. Effects of brown and golden flaxseed on the lipid profile, glycemia, inflammatory biomarkers, blood pressure and body composition in overweight adolescents. Nutrition. 2015;31(1):90–6. [DOI] [PubMed] [Google Scholar]
- 22. Yari Z, Rahimlou M, Eslamparast T, Ebrahimi-Daryani N, Poustchi H, Hekmatdoost A. Flaxseed supplementation in non-alcoholic fatty liver disease: a pilot randomized, open labeled, controlled study. Int J Food Sci Nutr. 2016;67(4):461–9. [DOI] [PubMed] [Google Scholar]
- 23. Zong G, Demark-Wahnefried W, Wu H, Lin X. Effects of flaxseed supplementation on erythrocyte fatty acids and multiple cardiometabolic biomarkers among Chinese with risk factors of metabolic syndrome. Eur J Nutr. 2013;52(5):1547–51. [DOI] [PubMed] [Google Scholar]
- 24. Ricklefs-Johnson K, Johnston CS, Sweazea KL. Ground flaxseed increased nitric oxide levels in adults with type 2 diabetes: A randomized comparative effectiveness study of supplemental flaxseed and psyllium fiber. Obes Med. 2017;5:16–24. [Google Scholar]
- 25. Rhee Y, Brunt A.. Flaxseed supplementation improved insulin resistance in obese glucose intolerant people: a randomized crossover design. Nutr J. 2011;10:44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Khalatbari Soltani S, Jamaluddin R, Tabibi H, Mohd Yusof BN, Atabak S, Loh SP, Rahmani L. Effects of flaxseed consumption on systemic inflammation and serum lipid profile in hemodialysis patients with lipid abnormalities. Hemodial Int. 2013;17(2):275–81. [DOI] [PubMed] [Google Scholar]
- 27. Hutchins AM, Brown BD, Cunnane SC, Domitrovich SG, Adams ER, Bobowiec CE. Daily flaxseed consumption improves glycemic control in obese men and women with pre-diabetes: a randomized study. Nutr Res. 2013;33(5):367–75. [DOI] [PubMed] [Google Scholar]
- 28. Demark-Wahnefried W, Polascik TJ, George SL, Switzer BR, Madden JF, Ruffin MT, Snyder DC, Owzar K, Hars V, Albala DM et al.. Flaxseed supplementation (not dietary fat restriction) reduces prostate cancer proliferation rates on men presurgery. Cancer Epidemiol Biomarkers Prev. 2008;17(12):3577–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Babajafari S, Akhlaghi M, Mazloomi SM, Ayaz M, Noorafshan A, Jafari P, Hojhabrimanesh A. The effect of isolated soy protein adjunctive with flaxseed oil on markers of inflammation, oxidative stress, acute phase proteins, and wound healing of burn patients; a randomized clinical trial. Burns. 2018;44(1):140–9. [DOI] [PubMed] [Google Scholar]
- 30. de Oliveira PA, Kovacs C, Moreira P, Magnoni D, Saleh MH, Faintuch J. Unsaturated Fatty Acids Improve Atherosclerosis Markers in Obese and Overweight Non-diabetic Elderly Patients. Obes Surg. 2017;27(10):2663–71. [DOI] [PubMed] [Google Scholar]
- 31. Foster M, Petocz P, Samman S. Inflammation markers predict zinc transporter gene expression in women with type 2 diabetes mellitus. J Nutr Biochem. 2013;24(9):1655–61. [DOI] [PubMed] [Google Scholar]
- 32. Karakas SE, Perroud B, Kind T, Palazoglu M, Fiehn O. Changes in plasma metabolites and glucose homeostasis during omega-3 polyunsaturated fatty acid supplementation in women with polycystic ovary syndrome. BBA Clin. 2016;5:179–85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Kaul N, Kreml R, Austria JA, Richard MN, Edel AL, Dibrov E, Hirono S, Zettler ME, Pierce GN. A Comparison of Fish Oil, Flaxseed Oil and Hempseed Oil Supplementation on Selected Parameters of Cardiovascular Health in Healthy Volunteers. J Am Coll Nutr. 2008;27(1):51–8. [DOI] [PubMed] [Google Scholar]
- 34. Kontogianni MD, Vlassopoulos A, Gatzieva A, Farmaki AE, Katsiougiannis S, Panagiotakos DB, Kalogeropoulos N, Skopouli FN. Flaxseed oil does not affect inflammatory markers and lipid profile compared to olive oil, in young, healthy, normal weight adults. Metabolism. 2013;62(5):686–93. [DOI] [PubMed] [Google Scholar]
- 35. Lemos JR, Alencastro MG, Konrath AV, Cargnin M, Manfro RC. Flaxseed oil supplementation decreases C-reactive protein levels in chronic hemodialysis patients. Nutr Res. 2012;32(12):921–7. [DOI] [PubMed] [Google Scholar]
- 36. Mirfatahi M, Tabibi H, Nasrollahi A, Hedayati M, Taghizadeh M. Effect of flaxseed oil on serum systemic and vascular inflammation markers and oxidative stress in hemodialysis patients: a randomized controlled trial. Int Urol Nephrol. 2016;48(8):1335–41. [DOI] [PubMed] [Google Scholar]
- 37. Mirhashemi SM, Rahimi F, Soleimani A, Asemi Z. Effects of omega-3 fatty acid supplementation on inflammatory cytokines and advanced glycation end products in patients with diabetic nephropathy: a randomized controlled trial. Iran J Kidney Dis. 2016;10(4):197–204. [PubMed] [Google Scholar]
- 38. Mirmasoumi G, Fazilati M, Foroozanfard F, Vahedpoor Z, Mahmoodi S, Taghizadeh M, Esfeh NK, Mohseni M, Karbassizadeh H, Asemi Z. The effects of flaxseed oil omega-3 fatty acids supplementation on metabolic status of patients with polycystic ovary syndrome: a randomized, double-blind, placebo-controlled trial. Exp Clin Endocrinol Diabetes. 2018;126(4):222–8. [DOI] [PubMed] [Google Scholar]
- 39. Nordstrom DC, Honkanen VE, Nasu Y, Antila E, Friman C, Konttinen YT. Alpha-linolenic acid in the treatment of rheumatoid arthritis. A double-blind, placebo-controlled and randomized study: flaxseed vs. safflower seed. Rheumatol Int. 1995;14(6):231–4. [DOI] [PubMed] [Google Scholar]
- 40. Paschos GK, Zampelas A, Panagiotakos DB, Katsiougiannis S, Griffin BA, Votteas V, Skopouli FN. Effects of flaxseed oil supplementation on plasma adiponectin levels in dyslipidemic men. Eur J Nutr. 2007;46(6):315–20. [DOI] [PubMed] [Google Scholar]
- 41. Rallidis LS, Paschos G, Liakos GK, Velissaridou AH, Anastasiadis G, Zampelas A. Dietary alpha-linolenic acid decreases C-reactive protein, serum amyloid A and interleukin-6 in dyslipidaemic patients. Atherosclerosis. 2003;167(2):237–42. [DOI] [PubMed] [Google Scholar]
- 42. Soleimani A, Taghizadeh M, Bahmani F, Badroj N, Asemi Z. Metabolic response to omega-3 fatty acid supplementation in patients with diabetic nephropathy: A randomized, double-blind, placebo-controlled trial. Clin Nutr. 2017;36(1):79–84. [DOI] [PubMed] [Google Scholar]
- 43. Soleimani Z, Hashemdokht F, Bahmani F, Taghizadeh M, Memarzadeh MR, Asemi Z. Clinical and metabolic response to flaxseed oil omega-3 fatty acids supplementation in patients with diabetic foot ulcer: A randomized, double-blind, placebo-controlled trial. J Diabetes Complications. 2017;31(9):1394–400. [DOI] [PubMed] [Google Scholar]
- 44. Vargas ML, Almario RU, Buchan W, Kim K, Karakas SE. Metabolic and endocrine effects of long-chain versus essential omega-3 polyunsaturated fatty acids in polycystic ovary syndrome. Metabolism. 2011;60(12):1711–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Wallace FA, Miles EA, Calder PC. Comparison of the effects of linseed oil and different doses of fish oil on mononuclear cell function in healthy human subjects. Br J Nutr. 2003;89(5):679–89. [DOI] [PubMed] [Google Scholar]
- 46. Barre DE, Mizier-Barre KA, Stelmach E, Hobson J, Griscti O, Rudiuk A, Muthuthevar D. Flaxseed lignan complex administration in older human type 2 diabetics manages central obesity and prothrombosis-an invitation to further investigation into polypharmacy reduction. J Nutr Metab. 2012;2012:585170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Hallund J, Tetens I, Bugel S, Tholstrup T, Bruun JM. The effect of a lignan complex isolated from flaxseed on inflammation markers in healthy postmenopausal women. Nutr Metab Cardiovasc Dis. 2008;18(7):497–502. [DOI] [PubMed] [Google Scholar]
- 48. Pan A, Demark-Wahnefried W, Ye X, Yu Z, Li H, Qi Q, Sun J, Chen Y, Chen X, Liu Y et al.. Effects of a flaxseed-derived lignan supplement on C-reactive protein, IL-6 and retinol-binding protein 4 in type 2 diabetic patients. Br J Nutr. 2009;101(8):1145–9. [DOI] [PubMed] [Google Scholar]
- 49. Hansen C. From fish to flaxseed. Reducing cardiac risk with omega-3 fatty acids. Adv Nurse Pract. 2006;14(5):51–3.; quiz 4. [PubMed] [Google Scholar]
- 50. Harris WS, Assaad B, Poston WC. Tissue omega-6/omega-3 fatty acid ratio and risk for coronary artery disease. Am J Cardiol. 2006;98(4A):19i–26i. [DOI] [PubMed] [Google Scholar]
- 51. Calder PC. n-3 polyunsaturated fatty acids, inflammation, and inflammatory diseases. Am J Clin Nutr. 2006;83(6 Suppl):1505S–19S. [DOI] [PubMed] [Google Scholar]
- 52. Oomah BD. Flaxseed as a functional food source. J Sci Food Agric. 2001;81(9):889–94. [Google Scholar]
- 53. Karakas M, Koenig W. CRP in cardiovascular disease. Herz. 2009;34(8):607–13. [DOI] [PubMed] [Google Scholar]
- 54. Dandona P, Aljada A, Bandyopadhyay A. Inflammation: the link between insulin resistance, obesity and diabetes. Trends Immunol. 2004;25(1):4–7. [DOI] [PubMed] [Google Scholar]
- 55. Nishida M, Moriyama T, Ishii K, Takashima S, Yoshizaki K, Sugita Y, Yamauchi-Takihara K. Effects of IL-6, adiponectin, CRP and metabolic syndrome on subclinical atherosclerosis. Clin Chim Acta. 2007;384(1-2):99–104. [DOI] [PubMed] [Google Scholar]
- 56. Lee D-E, Kehlenbrink S, Lee H, Hawkins M, Yudkin JS. Getting the message across: mechanisms of physiological cross talk by adipose tissue. Am J Physiol Endocrinol Metab. 2009;296(6):E1210–E29. [DOI] [PubMed] [Google Scholar]
- 57. Xu H, Barnes GT, Yang Q, Tan G, Yang D, Chou CJ, Sole J, Nichols A, Ross JS, Tartaglia LA. Chronic inflammation in fat plays a crucial role in the development of obesity-related insulin resistance. J Clin Invest. 2003;112(12):1821–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Prasad K. Antioxidant activity of secoisolariciresinol diglucoside-derived metabolites, secoisolariciresinol, enterodiol, and enterolactone. Int J Angiol. 2000;9(4):220–5. [DOI] [PubMed] [Google Scholar]
- 59. Kinniry P, Amrani Y, Vachani A, Solomides CC, Arguiri E, Workman A, Carter J, Christofidou-Solomidou M. Dietary flaxseed supplementation ameliorates inflammation and oxidative tissue damage in experimental models of acute lung injury in mice. J Nutr. 2006;136(6):1545–51. [DOI] [PubMed] [Google Scholar]
- 60. Lee JC, Bhora F, Sun J, Cheng G, Arguiri E, Solomides CC, Chatterjee S, Christofidou-Solomidou M. Dietary flaxseed enhances antioxidant defenses and is protective in a mouse model of lung ischemia-reperfusion injury. Am J Physiol Lung Cell Mol Physiol. 2008;294(2):L255–L65. [DOI] [PubMed] [Google Scholar]
- 61. Rom S, Zuluaga-Ramirez V, Reichenbach NL, Erickson MA, Winfield M, Gajghate S, Christofidou-Solomidou M, Jordan-Sciutto KL, Persidsky Y. Secoisolariciresinol diglucoside is a blood-brain barrier protective and anti-inflammatory agent: implications for neuroinflammation. J Neuroinflammation. 2018;15(1):25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Sa'ad H, Peppelenbosch MP, Roelofsen H, Vonk RJ, Venema K. Biological effects of propionic acid in humans; metabolism, potential applications and underlying mechanisms. Biochim Biophys Acta. 2010;1801(11):1175–83. [DOI] [PubMed] [Google Scholar]
- 63. Baranowski M, Enns J, Blewett H, Yakandawala U, Zahradka P, Taylor CG. Dietary flaxseed oil reduces adipocyte size, adipose monocyte chemoattractant protein-1 levels and T-cell infiltration in obese, insulin-resistant rats. Cytokine. 2012;59(2):382–91. [DOI] [PubMed] [Google Scholar]
- 64. Zhao G, Etherton TD, Martin KR, Gillies PJ, West SG, Kris-Etherton PM. Dietary α-linolenic acid inhibits proinflammatory cytokine production by peripheral blood mononuclear cells in hypercholesterolemic subjects. Am J Clin Nutr. 2007;85(2):385–91. [DOI] [PubMed] [Google Scholar]
- 65. Kelly AS, Wetzsteon RJ, Kaiser DR, Steinberger J, Bank AJ, Dengel DR. Inflammation, insulin, and endothelial function in overweight children and adolescents: the role of exercise. J Pediatr. 2004;145(6):731–6. [DOI] [PubMed] [Google Scholar]
- 66. Recasens M, Ricart W, Fernández-Real JM. Obesity and inflammation. Rev Med Univ Navarra. 2004;48(2):49–54. [PubMed] [Google Scholar]